Embed Size (px)
Citation preview

Can Helicobacter pylori serology still be applied as a surrogatemarker to identify peptic ulcer disease in dyspepsia?
H. H.-X. XIA 1 , J . S. KALANTAR 1 , H. M. MITCHELL 2 & N. J. TALLEY 1
1Department of Medicine, The University of Sydney, Nepean Hospital, and 2School of Microbiology and Immunology,
The University of New South Wales, Australia
Accepted for publication 16 November 1999
INTRODUCTION
Peptic ulcer continues to be a common disease that
causes a substantial socioeconomic burden and negat-
ively impacts on quality of life.1, 2 The mortality from
peptic ulcer disease due to perforation or bleeding is still
of concern; the annual rate is 50 per million (or 850
deaths) in Australia and 67 per million (or 4000
deaths) in the UK.3±5 Helicobacter pylori infection has
been reported to be present in up to 80±100% of
patients with duodenal ulcer and 60±95% of patients
with gastric ulcer.6, 7 There are convincing data that
eradication of H. pylori infection leads to cure of
H. pylori-associated peptic ulcer and prevents ulcer
complications.6±10 Thus, identi®cation of H. pylori-
associated peptic ulcer is now an important issue for
both general practitioners and gastroenterologists.
Based on UK data that noninvasive screening of
patients for H. pylori infection using a urea breath test
or serology is useful for identifying peptic ulcer disease
amongst patients with dyspepsia,11±14 the British Soci-
ety of Gastroenterology has recommended that nonin-
vasive H. pylori testing be employed in patients with
dyspepsia prior to referring for an upper endoscopy.15 It
has further been suggested that H. pylori-negative
patients who are younger than 45 years do not require
an upper endoscopy if there are no alarm features.15 On
the other hand, the European Study Group has
recommended that patients with dyspepsia under
SUMMARY
Background: Helicobacter pylori infection and associated
peptic ulcer disease (PUD) has become less common in
some countries.
Aim: To determine if H. pylori serology alone or com-
bined with a history of ingestion of non-steroidal anti-
in¯ammatory drugs (NSAIDs) and an age threshold can
be used as an indirect ulcer test.
Methods: Two hundred and ®fty-two consecutive Aus-
tralian patients (121 males, mean age 52 years)
referred for endoscopy were enrolled. Blood was tested
by a validated ELISA. At endoscopy, eight biopsies were
taken for CLO-testing, culture and histology. NSAID use
over the prior 3 months was recorded.
Results: One hundred and six (42%) patients were
seropositive for H. pylori, 48 (19%) patients had PUD
and 30 (12%) used NSAIDs. Serology alone had a
sensitivity of 52% and a speci®city of 60% for identifying
PUD; the sensitivity and speci®city were 60% and 55%,
respectively, when combined with a history of NSAID
use. Serology, regardless of NSAID use, would have
saved 23% in endoscopy workload but would have
missed 17% of PUD cases if an age threshold of
< 45 years was chosen for omitting endoscopy.
Conclusions: Serology was a poor ulcer test despite an
excellent performance for detecting H. pylori. A strategy
combining serology and an age threshold with a history
of NSAID use to reduce endoscopy workloads may not
always be appropriate.
Correspondence to: Professor N. J. Talley, Department of Medicine, The
University of Sydney, Nepean Hospital, PO Box 63, Penrith NSW 2751,
Australia.E-mail: [email protected]
Aliment Pharmacol Ther 2000; 14: 615±624.
Ó 2000 Blackwell Science Ltd 615

45 years of age should receive empirical anti-H. pylori
therapy if noninvasive H. pylori testing is positive and
there are no alarm symptoms.16 The American Gast-
roenterological Association and an Asian Paci®c Con-
sensus Party have supported a similar `test and treat'
approach.17, 18 It is assumed that this approach will
reduce endoscopy workloads and will be cost-effect-
ive.16, 19, 20
Recent randomized controlled trials have reported that
H. pylori eradication is not of symptomatic bene®t for
patients with nonulcer dyspepsia.21, 22 While not all
studies agree,23 empirical anti-H. pylori therapy appears
not to be justi®able, at present, for all H. pylori-positive
patients with nonulcer dyspepsia if symptom relief is the
primary goal. Moreover, over several decades the
prevalence of H. pylori infection appears to have been
declining in developed countries, presumably due to an
improvement in living standards such as reduced
crowding in families.24, 25 Correspondingly, the inci-
dence of H. pylori-associated diseases such as peptic
ulcer and gastric cancer have also decreased.3, 26, 27
The prevalence of H. pylori infection and the incidence
of associated diseases will probably fall further as
effective eradication therapy for H. pylori infection is
more widely applied.7, 16±18, 28 Indeed, there have been
increasing reports of H. pylori-negative gastric and
duodenal ulcer.29±34 This will impact on a management
strategy that relies on noninvasive H. pylori testing.
In this prospective study, we aimed to determine
whether serology alone or combined with a history of
use of non-steroidal anti-in¯ammatory drugs (NSAIDs)
is a useful tool for identifying peptic ulcer disease
amongst patients presenting with upper gastrointestinal
complaints.
PATIENTS AND METHODS
Patients
Two hundred and ®fty-two consecutive patients referred
to the Nepean Hospital endoscopy unit in Australia
because of upper gastrointestinal symptoms were
enrolled. They were 121 males and 131 females, with a
mean age of 52.1 years (range 18±86 years). All patients
had no documented history of anti-H. pylori therapy in
the prior year. Use of NSAIDs over the prior 3 months
was recorded, based on an interview by a gastroenterol-
ogist (J.S.K.). Patients who had used aspirin or nonaspirin
NSAIDs for at least 3 days at any dosage during this
period of time were considered to be NSAID users.
Treatment with H2-receptor antagonists or proton pump
inhibitors over the prior 4 weeks was also recorded.
At endoscopy, a mucosal break with depth in the
stomach or duodenum was de®ned as an active ulcer,
whereas a healed ulcer was de®ned as present if there
was evidence of scarring or deformity. Re¯ux oesoph-
agitis was identi®ed by the presence of oesophageal
mucosal breaks.
All patients gave informed consent. The study was
approved by the Wentworth Area Health Service Ethics
Committee.
Serological assay
Blood samples (10 mL) were obtained from each
patient, and an enzyme-linked immunosorbent assay
kit, pylori DTect ELISA (Diagnostic Technology, Sydney,
Australia), which was validated in our laboratory, was
applied for the serological detection of H. pylori infec-
tion; of the patients included in the present study, 209
had been used previously to validate the kit.35
Con®rmation of H. pylori infection
At the time of endoscopic examination, eight biopsies
were obtained from each patient using a standard
mapping protocol.36 These included three biopsies taken
at the antrum within 2 cm of the pylorus along the
lesser curvature, two from midway between pylorus and
cardio±oesophageal junction at the greater curvature,
two from the deepest portion of the dome of the fundus
when retro¯exing the endoscope and one from the
angulus at the lesser curvature. One antral biopsy was
used for a rapid urease test (CLO-test; Delta West Pty
Ltd, Bentley, Western Australia). Three biopsies (one
each from the antrum, body and fundus) were cultured
on horse blood agar plates for 5±7 days under micro-
aerophilic conditions. Colonies suspected of being
H. pylori were Gram stained, and then urease activity
was tested. The remaining four biopsies were examined
for Helicobacter-like organisms by histology according to
the revised Sydney System after staining with haemat-
oxylin and eosin (H&E) as well as Giemsa.37 The
endoscopist and pathologist were unaware of the
serological status.
To establish the gold standard, H. pylori status was
only de®ned to be positive if a patient was shown to be
positive by one of the following: (i) culture (ii) the CLO-
616 H. H.-X. XIA et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624

test and histology on one or more biopsies, or
(iii) histology on at least two biopsies.38
Statistical analysis
The seroprevalence of H. pylori infection between
different groups of patients was assessed using the
Chi-squared test, with Yates's correction if required. All
P-values calculated were two-tailed; the alpha level of
signi®cance was set at P < 0.05.
RESULTS
Seroprevalence of H. pylori infection in peptic ulcer disease
and other endoscopic ®ndings
Overall, 106 (42.1%) of the 252 patients were seropos-
itive and 146 (57.9%) were seronegative. Thirteen of
the seropositive patients were negative, and four of the
seronegative patients were positive by the gold stan-
dard. Thus, the pylori DTect ELISA had a sensitivity and
speci®city of 96% and 92%, respectively, for the
detection of H. pylori infection. The prevalence of
H. pylori infection determined by the serology and
biopsy based tests is shown in Figure 1. The seropreva-
lence of H. pylori infection was signi®cantly higher in
males than in females (50% vs. 34%, P � 0.01), and
appeared to increase with age, with the rate being
signi®cantly higher in patients ³ 45 years of age than
those < 45 years of age (48% vs. 31%, P � 0.02)
(Table 1).
At endoscopy, 48 (19%) patients were diagnosed
as having chronic peptic ulcer disease (13 with duo-
denal ulcer, 29 with gastric ulcer and six with duo-
denal and gastric ulcers), 129 (51.2%) patients had
nonulcer dyspepsia (75 normal mucosa, 54 macro-
scopic gastroduodenitis), and two (0.8%) patients had
gastric cancer. The remaining 73 (29%) patients had
de®nite gastro-oesophageal re¯ux disease (seven
Barrett's oesophagus and 66 re¯ux oesophagitis).
The seroprevalence of H. pylori infection (52.1%) in
patients with peptic ulcer disease was not signi®cantly
different from the seroprevalence (44%) in patients
with a normal mucosa (Table 1). The lowest sero-
prevalence (30.1%) occurred in gastro-oesophageal
re¯ux disease; this was signi®cantly lower than in
peptic ulcer disease (v2 � 5.87, OR � 2.52, 95%CI
1.18±5.36, P < 0.02), but was not signi®cantly
different from the seroprevalence in nonulcer
dyspepsia (Table 1).
Overall, 69% of duodenal ulcer cases, 41% of gastric
ulcer cases and 67% of cases with both duodenal and
gastric ulcer were seropositive for H. pylori. The
seroprevalence was not signi®cantly different between
males and females with peptic ulcer disease (Table 1).
However, the seroprevalence in gastric ulcer and gastric
and duodenal ulcer appeared to be related to age; none
(0%) of the seven patients younger than 45 years was
seropositive for H. pylori, compared with a seropreva-
lence of 57.1% (16/28) in gastric ulcer patients
45 years or older (P � 0.01, Fisher's Exact Test, two-
tail) (Table 1).
Figure 1. Prevalence of H. pylori infec-
tion in 252 patients with dyspepsia and
re¯ux symptoms, according to age, as
determined by serology and biopsy-based
tests (BBT).
H. PYLORI SEROLOGY FOR IDENTIFYING PEPTIC ULCER DISEASE 617
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624
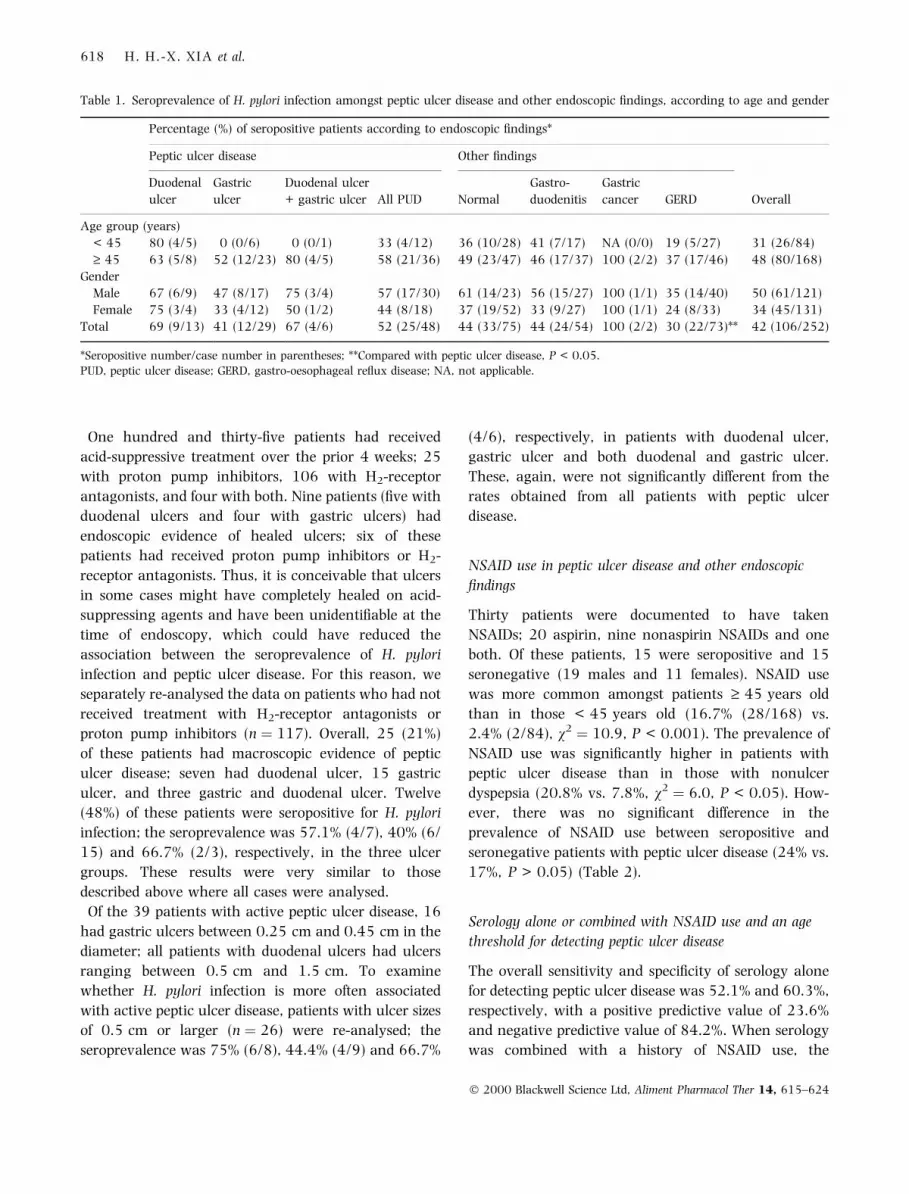
One hundred and thirty-®ve patients had received
acid-suppressive treatment over the prior 4 weeks; 25
with proton pump inhibitors, 106 with H2-receptor
antagonists, and four with both. Nine patients (®ve with
duodenal ulcers and four with gastric ulcers) had
endoscopic evidence of healed ulcers; six of these
patients had received proton pump inhibitors or H2-
receptor antagonists. Thus, it is conceivable that ulcers
in some cases might have completely healed on acid-
suppressing agents and have been unidenti®able at the
time of endoscopy, which could have reduced the
association between the seroprevalence of H. pylori
infection and peptic ulcer disease. For this reason, we
separately re-analysed the data on patients who had not
received treatment with H2-receptor antagonists or
proton pump inhibitors (n � 117). Overall, 25 (21%)
of these patients had macroscopic evidence of peptic
ulcer disease; seven had duodenal ulcer, 15 gastric
ulcer, and three gastric and duodenal ulcer. Twelve
(48%) of these patients were seropositive for H. pylori
infection; the seroprevalence was 57.1% (4/7), 40% (6/
15) and 66.7% (2/3), respectively, in the three ulcer
groups. These results were very similar to those
described above where all cases were analysed.
Of the 39 patients with active peptic ulcer disease, 16
had gastric ulcers between 0.25 cm and 0.45 cm in the
diameter; all patients with duodenal ulcers had ulcers
ranging between 0.5 cm and 1.5 cm. To examine
whether H. pylori infection is more often associated
with active peptic ulcer disease, patients with ulcer sizes
of 0.5 cm or larger (n � 26) were re-analysed; the
seroprevalence was 75% (6/8), 44.4% (4/9) and 66.7%
(4/6), respectively, in patients with duodenal ulcer,
gastric ulcer and both duodenal and gastric ulcer.
These, again, were not signi®cantly different from the
rates obtained from all patients with peptic ulcer
disease.
NSAID use in peptic ulcer disease and other endoscopic
®ndings
Thirty patients were documented to have taken
NSAIDs; 20 aspirin, nine nonaspirin NSAIDs and one
both. Of these patients, 15 were seropositive and 15
seronegative (19 males and 11 females). NSAID use
was more common amongst patients ³ 45 years old
than in those < 45 years old (16.7% (28/168) vs.
2.4% (2/84), v2 � 10.9, P < 0.001). The prevalence of
NSAID use was signi®cantly higher in patients with
peptic ulcer disease than in those with nonulcer
dyspepsia (20.8% vs. 7.8%, v2 � 6.0, P < 0.05). How-
ever, there was no signi®cant difference in the
prevalence of NSAID use between seropositive and
seronegative patients with peptic ulcer disease (24% vs.
17%, P > 0.05) (Table 2).
Serology alone or combined with NSAID use and an age
threshold for detecting peptic ulcer disease
The overall sensitivity and speci®city of serology alone
for detecting peptic ulcer disease was 52.1% and 60.3%,
respectively, with a positive predictive value of 23.6%
and negative predictive value of 84.2%. When serology
was combined with a history of NSAID use, the
Table 1. Seroprevalence of H. pylori infection amongst peptic ulcer disease and other endoscopic ®ndings, according to age and gender
Percentage (%) of seropositive patients according to endoscopic ®ndings*
Peptic ulcer disease Other ®ndings
Duodenal
ulcer
Gastric
ulcer
Duodenal ulcer
+ gastric ulcer All PUD Normal
Gastro-
duodenitis
Gastric
cancer GERD Overall
Age group (years)
< 45 80 (4/5) 0 (0/6) 0 (0/1) 33 (4/12) 36 (10/28) 41 (7/17) NA (0/0) 19 (5/27) 31 (26/84)
³ 45 63 (5/8) 52 (12/23) 80 (4/5) 58 (21/36) 49 (23/47) 46 (17/37) 100 (2/2) 37 (17/46) 48 (80/168)
Gender
Male 67 (6/9) 47 (8/17) 75 (3/4) 57 (17/30) 61 (14/23) 56 (15/27) 100 (1/1) 35 (14/40) 50 (61/121)
Female 75 (3/4) 33 (4/12) 50 (1/2) 44 (8/18) 37 (19/52) 33 (9/27) 100 (1/1) 24 (8/33) 34 (45/131)
Total 69 (9/13) 41 (12/29) 67 (4/6) 52 (25/48) 44 (33/75) 44 (24/54) 100 (2/2) 30 (22/73)** 42 (106/252)
*Seropositive number/case number in parentheses; **Compared with peptic ulcer disease, P < 0.05.
PUD, peptic ulcer disease; GERD, gastro-oesophageal re¯ux disease; NA, not applicable.
618 H. H.-X. XIA et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624
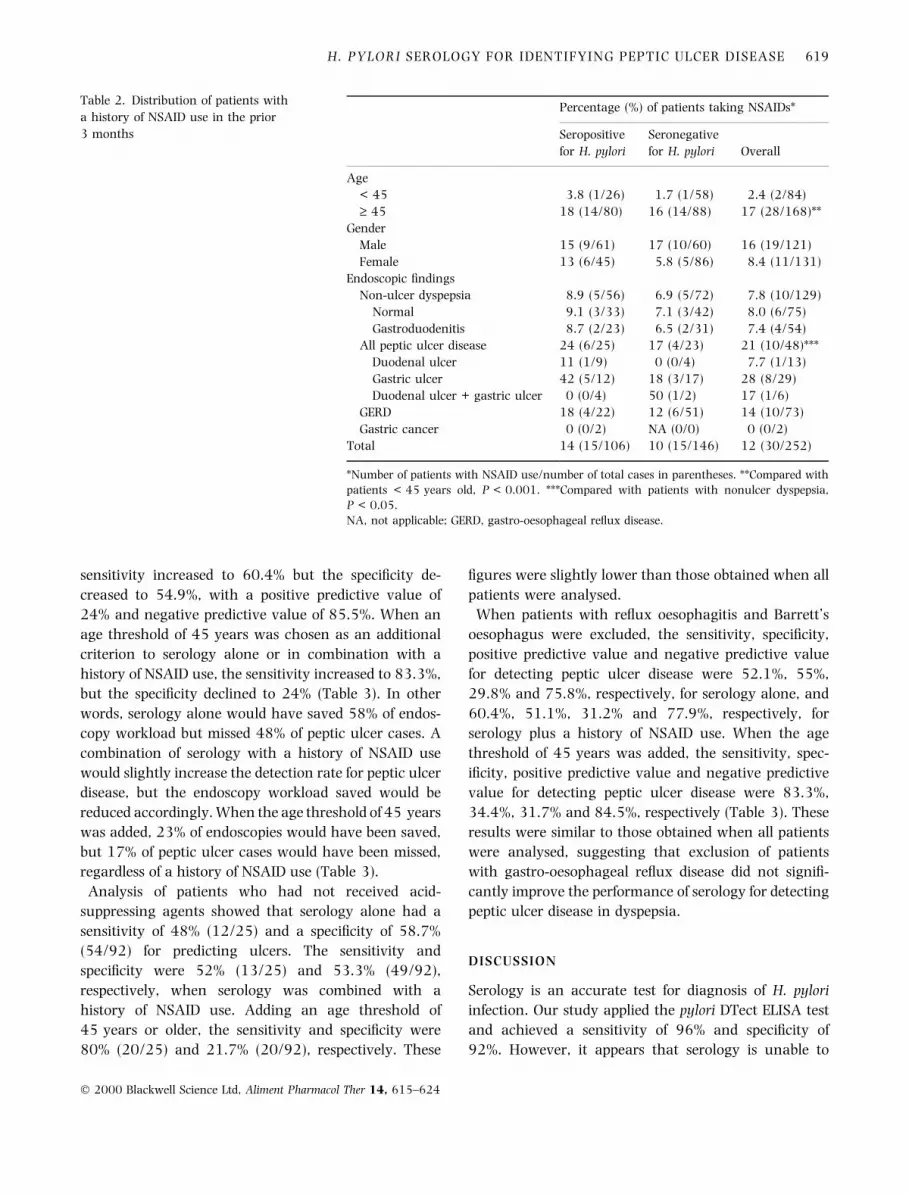
sensitivity increased to 60.4% but the speci®city de-
creased to 54.9%, with a positive predictive value of
24% and negative predictive value of 85.5%. When an
age threshold of 45 years was chosen as an additional
criterion to serology alone or in combination with a
history of NSAID use, the sensitivity increased to 83.3%,
but the speci®city declined to 24% (Table 3). In other
words, serology alone would have saved 58% of endos-
copy workload but missed 48% of peptic ulcer cases. A
combination of serology with a history of NSAID use
would slightly increase the detection rate for peptic ulcer
disease, but the endoscopy workload saved would be
reduced accordingly. When the age threshold of 45 years
was added, 23% of endoscopies would have been saved,
but 17% of peptic ulcer cases would have been missed,
regardless of a history of NSAID use (Table 3).
Analysis of patients who had not received acid-
suppressing agents showed that serology alone had a
sensitivity of 48% (12/25) and a speci®city of 58.7%
(54/92) for predicting ulcers. The sensitivity and
speci®city were 52% (13/25) and 53.3% (49/92),
respectively, when serology was combined with a
history of NSAID use. Adding an age threshold of
45 years or older, the sensitivity and speci®city were
80% (20/25) and 21.7% (20/92), respectively. These
®gures were slightly lower than those obtained when all
patients were analysed.
When patients with re¯ux oesophagitis and Barrett's
oesophagus were excluded, the sensitivity, speci®city,
positive predictive value and negative predictive value
for detecting peptic ulcer disease were 52.1%, 55%,
29.8% and 75.8%, respectively, for serology alone, and
60.4%, 51.1%, 31.2% and 77.9%, respectively, for
serology plus a history of NSAID use. When the age
threshold of 45 years was added, the sensitivity, spec-
i®city, positive predictive value and negative predictive
value for detecting peptic ulcer disease were 83.3%,
34.4%, 31.7% and 84.5%, respectively (Table 3). These
results were similar to those obtained when all patients
were analysed, suggesting that exclusion of patients
with gastro-oesophageal re¯ux disease did not signi®-
cantly improve the performance of serology for detecting
peptic ulcer disease in dyspepsia.
DISCUSSION
Serology is an accurate test for diagnosis of H. pylori
infection. Our study applied the pylori DTect ELISA test
and achieved a sensitivity of 96% and speci®city of
92%. However, it appears that serology is unable to
Table 2. Distribution of patients with
a history of NSAID use in the prior
3 months
Percentage (%) of patients taking NSAIDs*
Seropositive
for H. pylori
Seronegative
for H. pylori Overall
Age
< 45 3.8 (1/26) 1.7 (1/58) 2.4 (2/84)
³ 45 18 (14/80) 16 (14/88) 17 (28/168)**
Gender
Male 15 (9/61) 17 (10/60) 16 (19/121)
Female 13 (6/45) 5.8 (5/86) 8.4 (11/131)
Endoscopic ®ndings
Non-ulcer dyspepsia 8.9 (5/56) 6.9 (5/72) 7.8 (10/129)
Normal 9.1 (3/33) 7.1 (3/42) 8.0 (6/75)
Gastroduodenitis 8.7 (2/23) 6.5 (2/31) 7.4 (4/54)
All peptic ulcer disease 24 (6/25) 17 (4/23) 21 (10/48)***
Duodenal ulcer 11 (1/9) 0 (0/4) 7.7 (1/13)
Gastric ulcer 42 (5/12) 18 (3/17) 28 (8/29)
Duodenal ulcer + gastric ulcer 0 (0/4) 50 (1/2) 17 (1/6)
GERD 18 (4/22) 12 (6/51) 14 (10/73)
Gastric cancer 0 (0/2) NA (0/0) 0 (0/2)
Total 14 (15/106) 10 (15/146) 12 (30/252)
*Number of patients with NSAID use/number of total cases in parentheses. **Compared with
patients < 45 years old, P < 0.001. ***Compared with patients with nonulcer dyspepsia,
P < 0.05.
NA, not applicable; GERD, gastro-oesophageal re¯ux disease.
H. PYLORI SEROLOGY FOR IDENTIFYING PEPTIC ULCER DISEASE 619
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624

Ta
ble
3.
Th
ev
alu
eo
fp
osi
tiv
eH
.py
lori
sero
log
ya
lon
eo
rw
ith
ah
isto
ryo
fN
SA
IDu
sea
ta
na
ge
thre
sho
ldo
f4
5y
ears
for
iden
tify
ing
pep
tic
ulc
erd
isea
sein
pa
tien
tsw
ith
up
per
ga
stro
inte
stin
al
sym
pto
ms
H.
pylo
ri
sero
log
yN
SA
IDu
seA
ge
³4
5y
ears
H.
pylo
rise
rolo
gy
/
NS
AID
use
H.
pylo
rise
rolo
gy
/
ag
e³
45
yea
rs
H.
pylo
rise
rolo
gy
/NS
AID
use
/ag
e³
45
yea
rs
+±
+±
+±
+±
+±
+±
All
pati
ents
*
Wit
hp
epti
cu
lcer
s(n
=4
8)
25
23
10
38
36
12
29
19
40
84
08
Wit
ho
ut
pep
tic
ulc
ers
(n=
20
4)
81
12
32
01
84
13
27
29
21
12
15
45
01
55
49
Sen
siti
vit
y(%
)5
22
17
56
08
38
3
Sp
eci®
city
(%)
60
90
55
55
25
24
Lik
elih
oo
dra
tio
1.3
2.1
1.2
1.3
1.1
1.1
Po
siti
ve
pre
dic
tiv
ev
alu
e(%
)2
43
32
12
42
12
1
Neg
ati
ve
pre
dic
tiv
ev
alu
e(%
)8
48
38
68
58
68
6
En
do
sco
py
sav
ed(%
)5
88
83
34
82
32
3
Pat
ien
tsw
ith
dysp
epsi
aon
ly**
Wit
hp
epti
cu
lcer
s(n
=4
8)
25
23
10
38
36
12
29
19
40
84
08
Wit
ho
ut
pep
tic
ulc
ers
(n=
13
1)
59
72
10
12
18
64
56
46
78
64
58
64
5
Sen
siti
vit
y(%
)5
22
17
56
08
38
3
Sp
eci®
city
(%)
55
92
34
51
34
34
Lik
elih
oo
dra
tio
1.2
2.8
1.1
1.2
1.3
1.3
Po
siti
ve
pre
dic
tiv
ev
alu
e(%
)3
05
03
03
13
23
2
Neg
ati
ve
pre
dic
tiv
ev
alu
e(%
)7
67
67
97
88
58
5
En
do
sco
py
sav
ed(%
)5
38
93
64
83
03
0
*All
pa
tien
ts(n
=2
52
)w
ith
up
per
ga
stro
inte
stin
al
sym
pto
ms
are
incl
ud
ed;
**P
ati
ents
wit
hg
ast
ro-o
eso
ph
ag
eal
re¯
ux
dis
ease
(n=
73
)w
ere
excl
ud
ed.
620 H. H.-X. XIA et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624
accurately predict peptic ulcer disease; in the present
study, serology missed 48% of peptic ulcer cases. Even
when serology was combined with a history of NSAID
use, this approach missed 40% of peptic ulcer cases,
despite potentially saving 50% in endoscopy workloads
if such a strategy was applied. When an age threshold of
45 years was added, one-quarter of endoscopy work-
loads would be saved, but one-®fth of ulcer cases would
be missed.
Eradication of H. pylori infection cures H. pylori-
associated peptic ulcer disease, leading to a substantial
decrease in the number with peptic ulceration.7±10
Therefore, while the overall prevalence of peptic ulcer
cases, particularly duodenal ulcer cases, is decreasing,
the proportion of H. pylori negative peptic ulcer cases is
increasing, leading to a high percentage of patients with
peptic ulcer disease who are missed by serology. In the
present study, the low prevalence of duodenal ulcer
disease may be due to the fact that anti-H. pylori therapy
has been used to treat duodenal ulcer for more than a
decade in Australia.39
Many previous studies have recommended an age
threshold of 45 years or greater before referring patients
with upper gastrointestinal symptoms for endos-
copy.12±14, 40 These studies have shown that 93±
100% of peptic ulcer patients under 45 years old were
seropositive for H. pylori.13, 14, 40 However, the present
study observed that only 33% (4/12) of young ulcer
patients were seropositive for H. pylori, which means
that up to 70% of ulcer patients under 45 years old
would have been missed if serology had been used as
screening tool in this population (Table 1). It is also
notable that in this age group all seven patients with
gastric ulcer were missed by serology testing. Therefore,
factors other than H. pylori infection are likely to play a
role in peptic ulcer disease, particularly gastric ulcer, in
this young population.29±34
Whether serology can be applied as a screening tool for
peptic ulcer disease depends in part on the seropreva-
lence of H. pylori infection in patients with peptic ulcer
disease. Duodenal ulcers may occasionally be due to
NSAIDs.29±34 On the other hand, gastric ulcer disease is
more strongly linked to NSAIDs.30, 31 Thus, a higher
prevalence of gastric ulcer contributes to an increased
number of H. pylori-negative peptic ulcer cases.30, 31
The different results observed between the present study
and others may be due in part to the different
distribution (i.e. ratio of gastric ulcer cases over
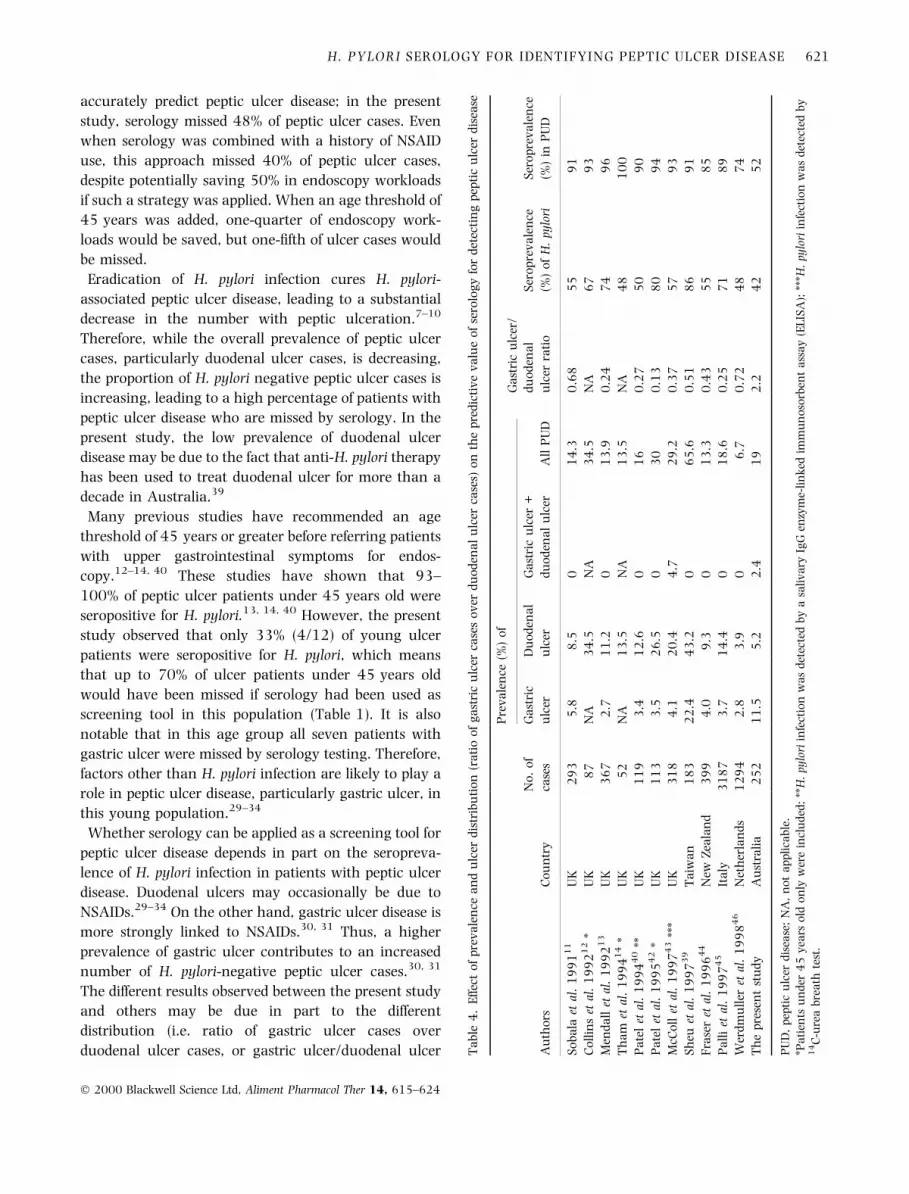
duodenal ulcer cases, or gastric ulcer/duodenal ulcer Ta
ble
4.
Eff
ect
of
pre
va
len
cea
nd
ulc
erd
istr
ibu
tio
n(r
ati
oo
fg
ast
ric
ulc
erca
ses
ov
erd
uo
den
al
ulc
erca
ses)
on
the
pre
dic
tiv
ev
alu
eo
fse
rolo
gy
for
det
ecti
ng
pep
tic
ulc
erd
isea
se
Pre
va
len
ce(%
)o
fG
ast
ric
ulc
er/
Au
tho
rsC
ou
ntr
y
No
.o
f
case
s
Ga
stri
c
ulc
er
Du
od
ena
l
ulc
er
Ga
stri
cu
lcer
+
du
od
ena
lu
lcer
All
PU
D
du
od
ena
l
ulc
erra
tio
Ser
op
rev
ale
nce
(%)
of
H.
pylo
ri
Ser
op
rev
ale
nce
(%)
inP
UD
So
ba
laet
al.
19
91
11
UK
29
35
.88
.50
14
.30
.68
55
91
Co
llin
set
al.
19
92
12
*U
K8
7N
A3
4.5
NA
34
.5N
A6
79
3
Men
da
llet
al.
19
92
13
UK
36
72
.71
1.2
01
3.9
0.2
47
49
6
Th
am
etal
.1
99
41
4*
UK
52
NA
13
.5N
A1
3.5
NA
48
10
0
Pa
tel
etal
.1
99
44
0**
UK
11
93
.41
2.6
01
60
.27
50
90
Pa
tel
etal
.1
99
54
2*
UK
11
33
.52
6.5
03
00
.13
80
94
McC
oll
etal
.1
99
74
3**
*U
K3
18
4.1
20
.44
.72
9.2
0.3
75
79
3
Sh
euet
al.
19
97
39
Ta
iwa
n1
83
22
.44
3.2
06
5.6
0.5
18
69
1
Fra
ser
etal
.1
99
64
4N
ewZ
eala
nd
39
94
.09
.30
13
.30
.43
55
85
Pa
lli
etal
.1
99
74
5It
aly
31
87
3.7
14
.40
18
.60
.25
71
89
Wer
dm
ull
eret
al.
19
98
46
Net
her
lan
ds
12
94
2.8
3.9
06
.70
.72
48
74
Th
ep
rese
nt
stu
dy
Au
stra
lia
25
21
1.5
5.2
2.4
19
2.2
42
52
PU
D,
pep
tic
ulc
erd
isea
se;
NA
,n
ot
ap
pli
cab
le.
*Pa
tien
tsu
nd
er4
5y
ears
old
on
lyw
ere
incl
ud
ed;
**H
.py
lori
infe
ctio
nw
as
det
ecte
db
ya
sali
va
ryIg
Gen
zym
e-li
nk
edim
mu
no
sorb
ent
ass
ay
(EL
ISA
);**
*H.
pylo
riin
fect
ion
wa
sd
etec
ted
by
14
C-u
rea
bre
ath
test
.
H. PYLORI SEROLOGY FOR IDENTIFYING PEPTIC ULCER DISEASE 621
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624

ratio) of peptic ulcer disease in these countries
(Table 4).12±14, 41±46 In the UK, the gastric ulcer/
duodenal ulcer ratio ranges from 0 to 0.68. In Taiwan,
New Zealand, Italy and the Netherlands, the ratios were
0.51, 0.43, 0.25 and 0.75, respectively. However, in
the present study, the gastric ulcer/duodenal ulcer ratio
was 2.2 (Table 4). It appears that an increased gastric
ulcer/duodenal ulcer ratio is associated with a decreased
seroprevalence of H. pylori infection in peptic ulcer
disease.
Intake of NSAIDs is common and may contribute to a
substantial proportion of H. pylori negative peptic ulcer
cases. Studies carried out in Sydney several years ago by
Borody et al. found that 38% of gastric ulcer cases and
6% of duodenal ulcer cases were H. pylori negative,
and that 66% of H. pylori negative gastric ulcer cases
and 44% of H. pylori negative duodenal ulcer cases had
taken NSAIDs.29, 32 Nensey et al. from the USA showed
that 23% of their duodenal ulcer cases were H. pylori
negative, of whom 83% had taken NSAIDs.33 It has
been also reported, in the USA and in Finland, that 60%
and 81%, respectively, of H. pylori negative gastric ulcer
patients had a history of NSAID use.30, 31 The present
study was able to identify NSAID use in only 21% of
patients with peptic ulcer disease and the rate was only
17% in seronegative patients with peptic ulcer disease.
One major reason may be that we only recorded recent
use of NSAIDs (in the 3 months prior to the enrolment).
There is also a possibility that some patients were
unaware that they were taking NSAIDs. One study has
shown that 13% of patients who claimed to have not
used aspirin had objective evidence of current aspirin
intake, as determined by platelet cyclooxygenase activ-
ity.47 While NSAID use is a major risk factor for peptic
ulcer disease, the present study suggests that a recent
history of NSAID use only minimally improves the
sensitivity of serology for identifying peptic ulcer disease
in practice.
The present study evaluated patients with upper
gastrointestinal symptoms referred for endoscopy to a
teaching hospital in Australia. Because the prevalence
of peptic ulcer disease is likely to be lower in general
practice, the performance of the serology in the general
practice setting may be even poorer. For example, if the
prevalence of peptic ulcer disease in dyspepsia is 10% in
general practice rather than 19% as observed in the
present study population, then the positive predictive
value of serology for identifying peptic ulcer disease
would decrease from 24% to 13%, despite an increase of
the negative predictive value from 83% to 92% (with
the same sensitivity of 52.1% and speci®city of 60.3%).
On the other hand, in populations with a prevalence of
peptic ulcer disease of 30%, the positive predictive value
would increase to 36% although the negative predictive
value would decrease to 75%. Therefore, H. pylori
serology appears to be unable to adequately serve as an
indirect marker of peptic ulcer disease when, in a given
population, the seroprevalence of H. pylori is low in
peptic ulcer disease.
In conclusion, serology achieved a relatively low
detection rate for peptic ulcer disease in this population
despite a high sensitivity and speci®city for identifying
H. pylori infection. A strategy combining serology and
an age threshold with a history of NSAID use to reduce
endoscopy workloads may no longer be appropriate in
some parts of the world.
ACKNOWLEDGEMENT
The authors thank Mr Stuart Howell for statistical
analysis.
REFERENCES
1 Jensen DM. Economic and health aspects of peptic ulcer
disease and H2-receptor antagonists. Am J Med 1986; 81:
42±8.
2 Wilhelmsen I, Berstad A. Quality of life and relapse of duo-
denal ulcer before and after eradication of Helicobacter pylori.
Scand J Gastroenterol 1994; 29: 874±9.
3 Sonnenberg A. Temporal trends and geographical variations
of peptic ulcer disease. Aliment Pharmacol Ther 1995;
9(Suppl. 2): 3±12.
4 Hugh TB, Kelly MD. Why are Australian peptic ulcer death
rates rising? Med J Aust 1991; 155: 136.
5 Axon A, Forman D. Helicobacter gastroduodenitis: a serious
infectious disease. Antibiotic treatment may prevent deaths in
the decades ahead. Br Med J 1997; 314: 1430±1.
6 Korman MG, Tytgat GNJ. Helicobacter pylori and peptic ulcer.
Scand J Gastroenterol 1995; 30(Suppl. 210): 92±6.
7 Consensus Development Panel on Helicobacter pylori in Peptic
Ulcer Disease. Helicobacter pylori in peptic ulcer disease. J Am
Med Assoc 1994; 272: 65±9.
8 Coghlan JG, Gilligan D, Humphries H, et al. Campylobacter
pylori and recurrence of duodenal ulcerÐa 12-month follow-
up study. Lancet 1987; ii: 1109±11.
9 Rauws EA, Tytgat GNJ. Cure of duodenal ulcer associated
with eradication of Helicobacter pylori. Lancet 1990; 335:
1233±5.
10 Graham DY, Hepps KS, Ramirez FC, Lew GM, Saeed ZA.
Treatment of Helicobacter pylori reduces the rebleeding in
peptic ulcer disease. Scand J Gastroenterol 1993; 28:
939±42.
622 H. H.-X. XIA et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624

11 Sobala GM, Crabtree JE, Pentith JA, et al. Screening dyspepsia
by serology to Helicobacter pylori. Lancet 1991; 338: 94±6.
12 Collins JSA, Bamford KB, Sloan JM, Collins BJ, Moorehead RJ,
Gary Love AH. Screening for Helicobacter pylori antibody could
reduce endoscopy workload in young dyspeptic patients. Eur J
Gastroenterol Hepatol 1992; 4: 991±3.
13 Mendall MA, Goggin PM, Marrero JM, et al. Role of Helicob-
acter pylori serology in screening prior to endoscopy. Eur J
Gastroenterol Hepatol 1992; 4: 713±7.
14 Tham TCK, McLaughlin N, Hughes DF, et al. Possible role of
Helicobacter pylori serology in reducing endoscopy workload.
Postgrad Med J 1994; 70: 809±12.
15 Axon ATR, Bell GD, Jones RH, Quine MA, McCloy RF.
Guidelines on appropriate indications for upper gastrointesti-
nal endoscopy. Br Med J 1995; 310: 853±6.
16 The European Helicobacter pylori Study Group. Current Euro-
pean concepts in the management of Helicobacter pylori in-
fection. The Maastricht Consensus Report. Gut 1997; 41:
8±13.
17 Anonymous. American Gastroenterological Association med-
ical position statement: evaluation of dyspepsia. Gastroente-
rology 1998; 114: 579±81.
18 Lam SK, Talley NJ. Helicobacter pylori Consensus. Report of the
1997 Asia Paci®c Consensus Conference on the management
of Helicobacter pylori infection. J Gastroenterol Hepatol 1998;
13: 1±12.
19 Sonnenberg A, Townsend WF. Costs of duodenal ulcer ther-
apy with antibiotics. Arch Intern Med 1995; 155: 922±8.
20 Briggs AH, Sculpher MJ, Logan RPH, Aldous J, Ramsay ME,
Baron JH. Cost effectiveness of screening for and eradication of
Helicobacter pylori in management of dyspeptic patients under
45 years of age. Br Med J 1996; 312: 1321±5.
21 Blum AL, Talley NJ, O'Morain C, et al. Lack of effect of treating
Helicobacter pylori infection in patients with nonulcer dys-
pepsia. N Engl J Med 1998; 339: 1875±81.
22 Talley NJ, Janssens J, Lauritsen K, Racz I, Bolling-Sternevald E.
Eradication of Helicobacter pylori in functional dyspepsia:
randomised double blind placebo controlled trial with 12
months' follow up. Br Med J 1999; 318: 833±7.
23 McColl K, Murray L, El-Omar E, et al. Symptomatic bene®ts
from eradicating Helicobacter pylori infection in patients with
nonulcer dyspepsia. N Engl J Med 1998; 339: 1869±74.
24 Haruma K, Okamoto S, Kawaguchi H, et al. Reduced incidence
of Helicobacter pylori infection in young Japanese persons be-
tween the 1970s and the 1990s. J Clin Gastroenterol 1997;
25: 583±6.
25 Sipponen P, Helske T, Jarvinen P, Hyvarinen H, Seppala K,
Siurala M. Fall in the prevalence of chronic gastritis over 15
years: analysis of outpatient series in Finland from 1977,
1985, and 1992. Gut 1994; 35: 1167±71.
26 Tytgat GNJ. No Helicobacter pylori, no Helicobacter pylori-
associated peptic ulcer disease. Aliment Pharmacol Ther
1995; 9(Suppl. 1): 39±42.
27 Sipponen P, Kimura K. Intestinal metaplasia, atrophic gastritis
and stomach cancer: trends over time. Eur J Gastroenterol
Hepatol 1994; 6(Suppl. 1): S79±83.
28 Xia HH-X, Talley NJ. Prospects for improved therapy for
Helicobacter pylori infection. Exp Opin Invest Drugs 1996; 5:
959±76.
29 Borody TJ, Brandl S, Andrews P, Jankiewicz E, Ostapowicz N.
Helicobacter pylori-negative gastric ulcer. Am J Gastroenterol
1992; 87: 1403±6.
30 Laine L, Marin-Sorensen M, Weinstein WM. Non-steroidal
anti-in¯ammatory drug-associated gastric ulcers do not re-
quire Helicobacter pylori for their development. Am J Gastro-
enterol 1992; 87: 1398±402.
31 Hyvarinen H, Salmenkyla S, Sipponen P. Helicobacter pylori-
negative duodenal and pyloric ulcer: role of NSAIDs. Digestion
1996; 57: 305±9.
32 Borody TJ, George LL, Brandl S, et al. Helicobacter pylori-
negative duodenal ulcer. Am J Gastroenterol 1991; 86:
1154±7.
33 Nensey YM, Schubert TT, Bologna SD, Ma CK. Helicobacter
pylori-negative duodenal ulcer. Am J Med 1991; 91: 15±8.
34 Talley NJ. Is Helicobacter pylori negative duodenal ulcer a
separate disease? In: Malfertheiner P, Ditschuneit H, eds.
Helicobacter Pylori, Gastritis, and Peptic Ulcer. Berlin: Springer-
Verlag, 1990: 340±4.
35 Xia HH-X, Kalantar JS, Ma Wyatt J, et al. High sensitivity and
speci®city of a laboratory-based serological test, pylori DTect
ELISA, for detection of Helicobacter pylori infection. Diag
Microbiol Infect Dis 2000; 36: 69±74.
36 Xia HH-X, Kalantar J, Talley NJ. Metronidazole- and clari-
thromycin-resistant Helicobacter pylori in dyspeptic patients in
Western Sydney as determined by testing multiple isolates
from different gastric sites. J Gastroenterol Hepatol 1998; 13:
1044±9.
37 Dixon MF, Genta RM, Yardley JH, Correa P and the partici-
pants in the International Workshop on the Histopathology of
Gastritis, Houston 1994. Classi®cation and grading of gastri-
tis. The Updated Sydney System. Am J Surg Pathol 1996; 20:
1161±81.
38 Thijs JC, van Zwet AA, Thijs WJ, et al. Diagnostic tests for
Helicobacter pylori: a prospective evaluation of their accuracy,
without selecting a single test as the gold standard. Am J
Gastroenterol 1996; 91: 2125±9.
39 Sheu B-S, Shiesh S-C, Yang H-B, Chen C-Y, Lin X-Z. Im-
plications Helicobacter pylori serological titer for the histo-
logical severity of antral gastritis. Endoscopy 1997; 29:
27±30.
40 Patel P, Mendall MA, Khulusi S, et al. Salivary antibodies to
Helicobacter pylori: screening dyspeptic patients before endos-
copy. Lancet 1994; 344: 511±2.
41 Marshall BJ, Goodwin CS, Warren JR, et al. Prospective dou-
ble-blind trial of duodenal ulcer relapse after eradication of
Campylobacter pylori. Lancet 1988; ii: 1437±42.
42 Patel P, Khulusi S, Mendall MA, et al. Prospective screening of
dyspeptic patients by Helicobacter pylori serology. Lancet
1995; 346: 1315±8.
43 McColl KEL, El-Nujumi A, Murray L, et al. The Helicobacter
pylori breath test: a surrogate marker for peptic ulcer disease
in dyspeptic patients. Gut 1997; 40: 302±6.
H. PYLORI SEROLOGY FOR IDENTIFYING PEPTIC ULCER DISEASE 623
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624

44 Fraser AG, Ali MR, McCullough S, Yeates NJ, Haystead A.
Diagnostic tests for Helicobacter pyloriÐcan they help select
patients for endoscopy? NZ Med J 1996; 109: 95±8.
45 Palli D, Vaira D, Menegatti M, Saieva C on behalf of the Italian
Helicobacter pylori Study Group. A serological survey of Heli-
cobacter pylori infection in 3281 Italian patients endoscoped
for upper gastrointestinal systems. Aliment Pharmacol Ther
1997; 11: 719±28.
46 Werdmuller BFM, V/Der Putten ABMM, Veenedaal RA,
Lamers CBHW, Loffeld RJLF. Can screening for IgG antibodies
against Helicobacter pylori be used in clinical practice? Omit
endoscopy in seropositive or negative patients? Dig Dis Sci
1998; 43: 2296±300.
47 Lanas A, Serano P, Bajador E, Esteva F, Benito R, Sainz R.
Evidence of aspirin use in both upper and lower gastrointes-
tinal perforation. Gastroenterology 1997; 112: 683±9.
624 H. H.-X. XIA et al.
Ó 2000 Blackwell Science Ltd, Aliment Pharmacol Ther 14, 615±624





























