Embed Size (px)
Citation preview
BOARD OF DIRECTORS – PUBLIC MEETING
AGENDA
Thursday 26 November 2020 MS Teams
10.00 – 12.30
No. Approx. time
Item Director
Please note this meeting will be live-streamed on the internet so care should be taken not to use people’s names in questions unless their permission has been given in advance.
10.00 Employee of the month awards Verbal Chair
MEETING ADMINISTRATION
1 10.10 Welcome and introduction, apologies and declarations of interest
Verbal Chair
2 10.15 Minutes of the previous meeting 24 September 2020
Enclosure Chair
3 10.20 Matters arising and actions log Enclosure Chair
STRATEGIC ITEMS
4 10.25 Board Assurance Framework and Corporate Objectives 2020/21 To review/discuss
Enclosure CEO
PERFORMANCE
5 10.40 Integrated Performance Report including COVID update To review/discuss
Enclosure
CFO
QUALITY ITEMS
6 11.00 Infection Prevention & Control Board Assurance To note
Enclosure CN
7 11.10 Quality Account 2019/20 To receive/endorse
Enclosure CN
8 11.25 Serious Incidents Report Q2 2020/21 To note
Enclosure MD
01 P
art 1
Pub
lic B
oard
Age
nda
2011
26
Page 1 of 300

9 11.35 Mortality Report Q2 2020/21 To note
Enclosure MD
GOVERNANCE ITEMS
10 11.45 Emergency Planning Resilience and Response Annual Report To receive/endorse
Enclosure COO
11 12.00 Guardian of Safe Working Q1 2020/21 To note
Verbal MD
12 12.10 Local Clinical Excellence Awards To note
Enclosure MD
13 12.20 Standing Financial Instructions and Board Standing Orders To approve
Enclosure Trust Secretary
14 12.30 Close of Board Meeting
Date of next meeting: 28 January 2021
Note: Questions from Governors and/or the public will be taken on each item during the meeting. Any other, general questions should be submitted to the following email address for a response outside the Board meeting:
[email protected] Resolution: That the remainder of the meeting shall be held in private because publicity would be prejudicial
to the public interest, by reason of the confidential nature of the business to be transacted in accordance with the Public Bodies (Admissions to Meetings) Act 1960 s1(2)
Page 2 of 300
1
MINUTES OF BOARD MEETING
Thursday 24 September 2020
Present:
Peter Horn Trust Chair (Chair)
Siobhan Melia Chief Executive
Stephen Lightfoot Non-Executive Director (NED)
Janice Needham Non-Executive Director (NED)
Elizabeth Woodman Non-Executive Director (NED)
David Parfitt Non-Executive Director (NED)
Maggie Ioannou Non-Executive Director (NED)
Mike Jennings Chief Financial Officer
Donna Lamb Chief Nurse
Sara Lightowlers Medical Director
Kate Pilcher Chief Operating Officer
In Attendance
Caroline Haynes Director of HR and Organisational Development
Diarmaid Crean Chief Digital and Technology Officer
Zoe Smith Trust Secretary (minutes)
20/124 Employee of the month
The Chair introduced the winners of the Trust’s July and August employee of the month awards.
Julia Fairhall, Area Head of Central Nursing and Governance, had been awarded July employee of
the month for her outstanding nursing leadership during challenging times. Wilma Thomas, Team
Lead in the Carers Health Team, was August’s employee of the month. Wilma and part of her team
had been redeployed earlier during the pandemic and she had been instrumental in setting up the
Trust’s drive thru COVID testing site in Bognor as well as supporting her team through
redeployment. The Board gave their thanks to Julia and Wilma and congratulated them on their
awards.
20/125 Welcome and introduction, apologies and declarations of interest
The Chair welcomed attendees. Some Board members were in attendance at Brighton General
Hospital, others were attending via MS Teams and the meeting was being live streamed on YouTube.
Stephen Lightfoot declared that he had been appointed as Chair of the Medicines and Healthcare
products Regulatory Agency. The Trust Secretary undertook to update the Trust’s Register of
Interests.
20/126 Minutes of the previous meeting 30 July 2020
The minutes of the previous meeting were agreed as a true and accurate record subject to an
amendment to the minute of BoD 20/112 Safer Staffing recognising the direct impact of registered
nurse staffing levels on patient safety.
02 P
art 1
Pub
lic B
oard
Min
utes
200
924
Page 3 of 300

2
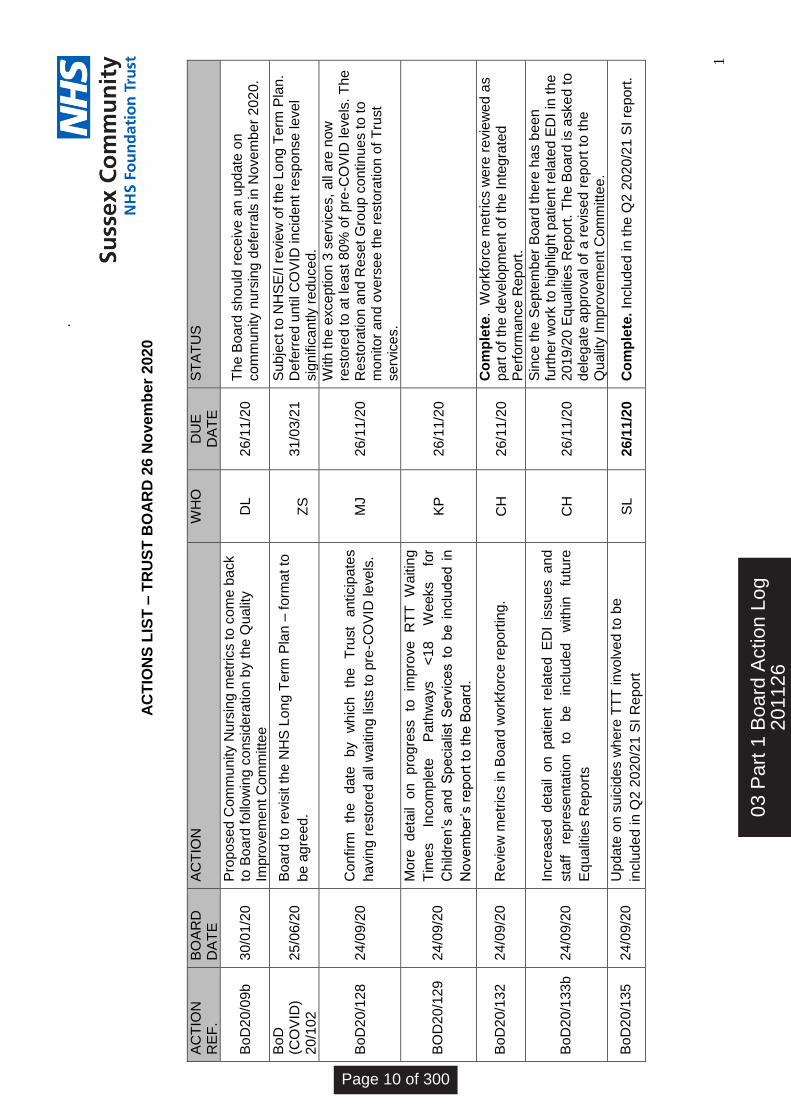
20/127 Matters arising and action log
The action log was reviewed and updated.
20/128 Reset and Restoration Plans
Mike Jennings (MJ) reported on the Trust’s reset and restoration plans highlighting the link to health
inequalities prevention. It was noted that there was currently that no financial element within the
plans. The Sussex Integrated Care System (ICS) would submit its financial plan on 5th October 2020
following which the Board would need to consider the Trust’s plan.
MJ stated that the Trusts’ plans reflected the current COVID situation. Estates issues related to
COVID safety restricted the number of patients who could be seen in some settings and the potential
impact of a second wave was unknown. Restoring previous activity levels did not necessarily mean
clearing all waiting lists. Those in most clinical need would be prioritised and the Trust would
communicate with patients.
Action: MJ to confirm the date by which the Trust anticipates having restored all waiting lists to
pre-COVID levels.
There was discussion of home working and of the need to offer comprehensive support to staff as
COVID continues.
In relation to the impact of COVID on children’s and other preventative services, specifically the
Healthy Child Programme, Kate Pilcher (KP) confirmed that there were mechanisms in place with
partners to ensure children’s safety and undertook to ensure that restoration was being effectively
monitored at a service level within the Trust.
Executives reported on work planned to better understand population health and health inequality
issues, noting that individual patients with particular risk factors or vulnerabilities would be
identified as part of clinical prioritisation. The Chair underlined the Board’s interest in this area and
the need for a particular emphasis on health inequalities as part of the Trust’s Phase 3 work, as well
as the importance of communicating with patients.
20/129 Operational Performance Report
KP introduced the item highlighting particular areas of variation and assurance, both adverse and
favourable, as shown in the report.
Responding to questions from Non-Executive Directors, KP confirmed that
The reduction in average length of stay was supported under new guidance through
increased system working although it was not possible to say whether this improvement
could be sustained after the end of this financial year;
Continuing Health Care assessments were now taking place in the community with any care
provided prior to the assessment funded by the CCG, irrespective of the assessment
outcome.
Page 4 of 300
3
In relation to wellbeing, members noted increased staff referrals to Time to Talk in the context of
the national focus on NHS staff wellbeing. There was discussion of funding for the planned Time to
Talk trajectory and members heard that the Trust did not currently fully meet the national target.
The funding to do this would be determined in 2021/22.
KP provided an update on work to address diagnostics underperformance both within the Trust and
across the system, including the development of a network of Community Diagnostic Hubs as part of
the national cancer strategy.
Responding to a NED question, KP highlighted specific issues impacting certain services within
Referral to Treatment (RTT) Waiting Times Incomplete Pathways less than 18 Weeks for Children’s
and Specialist Services. For example, dental services had been affected by lack of access to
anaesthetics and system work to improve neurodevelopmental pathway had been paused during
COVID. More detail on progress being made to improve performance in this area would be included
in the next report to the Board.
Action: More detail on progress to improve RTT Waiting Times Incomplete Pathways less than 18
Weeks for Children’s and Specialist Services to be included in November’s report to the Board.
There were no operational or IT risks scored above 15. The COVID risk, currently rated 12, was due
to be reviewed and would be rescored as necessary.
The Board noted the Operational Performance report and thanked KP for the high quality of the
reporting.
20/130 Quality Report
Donna Lamb (DL) introduced the item highlighting two areas of adverse assurance - community
nursing deferrals and falls risk assessments - both of which had been discussed by the Quality
Improvement Committee.
With regard to community nursing deferrals, an audit was being undertaken to understand the
reasons for the recent increase; for example, whether this was a recording issue or a failure to apply
standard operating procedures. Work was also ongoing to understand the patient experience of
deferrals. Action would be taken once the findings were received.
NEDs voiced some frustration with ongoing adverse assurance on deferrals, highlighting staff
concerns that this impacts on patient safety. The Chair noted that this would come back to the
Board through Quality Improvement Committee in November.
There was discussion about demand and capacity in the community nursing service and Siobhan
Melia (SMe) reported on the recent appointment of a Head of Data Engineering to support
improvement of data and reporting within the Trust.
02 P
art 1
Pub
lic B
oard
Min
utes
200
924
Page 5 of 300
4
DL acknowledged the need for clear action to address falls risk assessment performance. She
reported that, as well as undertaking a process mapping exercise to address any improvements
required in recording, the Trust was also scoping a Falls Lead role. Notwithstanding the recording of
falls risks assessments, Sara Lightowlers (SL) highlighted the significant improvement achieved by the
Trust in falls performance despite an increasingly acute and complex patient cohort.
The Board noted the Quality Report including the actions being taken in the two areas of adverse
variance and agreed proposals to report back to Board in November.
20/131 Finance Report
Mike Jennings (MJ) introduced the item noting the Trust’s break even forecast under the current
financial regime. October 2020 onwards would see a more constrained financial environment and
therefore increased financial risk.
Advance payments to the Trust had resulted in a healthy cash position which meant no liquidity
concerns going into winter. This cash position was expected to unwind at the end of the year.
Responding to a NED question about prepayments to suppliers, MJ confirmed that the Trust had
entered into pre-payment arrangements with a handful of suppliers in line with national guidance. It
kept supplier resilience under constant review and no pre-paid supplier had been identified as at
risk.
As Chair of the Resources Committee, Stephen Lightfoot noted that the Trust’s capital programme
had been maintained to Month 5. A system based financial regime from M7 meant increased risk
and the Committee would continue to oversee the capital programme on behalf the Board.
The Board noted the Trust’s Month 5 Finance Report.
20/132 Workforce Report
Caroline Haynes (CH) introduced the Workforce Report highlighting the focus on embedding new
ways of working and on staff retention as well as the spotlight on the NHS People Plan aligned to the
objectives of the Trust’s workforce strategy.
In response to questions from NEDs, CH stated that:
Improvements in recruitment and retention over recent months were the result of a
combination of Trust actions and the ‘COVID effect’;
The Trust had been highly rated for the quality of its student nurse placements and
recognised the importance of converting these into Band 5 nurses as discussed at the
Quality Improvement Committee
The Trust was committed to developing the right environment for BAME staff to be
appointed to senior roles, as well as to meeting targets for senior BAME appointments
There was discussion of the Trust’s Workforce risk in the context of a positive performance report.
Page 6 of 300
5
Members noted that the risk was now workforce resilience (as a result of pandemic) rather than
vacancies. CH committed to review the metrics in Board workforce reporting.
Action: CH to review the metrics in Board workforce reporting.
SMe noted the impact of COVID on both workforce and performance and suggested the COVID 19
dashboard be reinstated as part of Board reporting. Members discussed the balance of outcomes
versus operational detail in Board reporting and agreed to keep the metrics reported to the Board
under review.
Responding to a question from Martin Ensom, Deputy Lead Governor and observer at the meeting,
about whether the Trust could maintain its improved vacancy rate, CH reported on mechanisms
already in place to support staff and consideration being given to a ‘Thinking of Leaving Us’ helpline.
The Board noted the Workforce Report.
20/133 Annual Equality Report
CH introduced the Trust’s Annual Equality Report 2019-20 highlighting the further work to be done
to respond to the requirements of the Phase 3 COVID response letter.
Acknowledging the 2019-20 report’s focus on staff Equality Diversity and Inclusion (EDI) and the
need to broaden the scope of the Trust’s EDI work programme going forward, CH confirmed that the
Trust continued to comply with the patient related EDI requirements previously reported to the
board including, for example, pastoral care and interpreting services .
DL referred to known problems with the Trust’s patient data. An Executive Equality Diversity and
Inclusion Steering Group would lead the Trust’s approach to addressing this and other aspects of the
EDI agenda in line with the Trust’s Patient Experience and Population Health strategic goals and the
requirements of the Phase 3 COVID response letter.
NEDs commended the clear report which demonstrated the Trust’s commitment to EDI as well as
reflecting the richness and depth of its EDI activity with staff. Expanded reporting on the Trust’s EDI
activity as it affects patients was requested along with more information on representation,
specifically whether SCFT staff were representative of the communities served and whether senior
staff were representative of the wider staff and/or of the community.
Members heard that while SCFT staffing was more or less representative of the population it served,
there were large variations in the size of BAME populations across the Trust’s footprint. In addition,
while there was under-representation of BAME staff at Agenda for Change 8A and above, this group
was over represented among medical staff. It was suggested therefore that the Trust could usefully
consider how it compares to other Trusts with a similar demographic.
Commenting that COVID had raised the profile of equalities in ways which were not foreseeable,
SMe proposed increased co-production with NEDs on future EDI reporting.
02 P
art 1
Pub
lic B
oard
Min
utes
200
924
Page 7 of 300
6
The Board noted the report. On behalf of the Board, the Chair commended the progress made and
underlined the further work to be done in highlighting patient related EDI issues and the need for
increased detail on staff representation to be included within future reports.
ACTION: Increased detail on patient related EDI issues and staff representation to be included
within future Equalities Reports
20/134 Information Governance and Caldicott Annual Report
Diarmaid Crean introduced the item, giving credit to Lindsay Wells, Head of Information
Governance, the report’s author. He highlighted that the Trust had met its stretching statutory and
mandatory training target of 95% and that the Trust had reported only two Information Governance
Serious Incidents to the Information Commissioner’s Office, both of which had been closed with no
further action.
Members discussed the need for a comparator for the number of IG incidents reported by the Trust
as well as the potential for increased risk of breaches as a result of increased homeworking. As
Caldicott Guardian, SL stated that although the Health Record Keeping training target had not been
met due to COVID, the quality of the Trusts’ health records was assured through audit.
The Board noted the report.
20/135 Serious Incidents Report Q1 2020/21
SL introduced the Serious Incidents (SI) Report Q1 2020/21 confirming that the reduction in the
number of reported SIs was a national phenomenon related to reduced activity and that the Trust
had maintained its mechanisms for review of incidents and SI reports throughout the pandemic.
In relation to suicides where the Trust’s Time to Talk (TTT) service been involved, SL noted that the
theme emerging appeared to be around the processing of appointments rather than quality of
patient care and commented that many TTT patients were also under the care of the mental health
provider and/or had attended an acute hospital.
ACTION: Update on suicides where TTT involved to be included in Q2 2020/21 SI Report to Board
SL reported on clarification of Reporting of Injuries Diseases and Dangerous Occurrences Regulations
(RIDDOR) guidance in relation to COVID 19 and provided assurance that any concerns or complaints
raised retrospectively would be dealt with as Serious Incidents where appropriate.
The Board was assured that the Trust had a robust process for monitoring incidents, that the Trust’s
increasing incident rate was in line with the national picture and that the Trust would review the
number of suicides in which its Time to Talk Service was involved to understand if it was an outlier.
20/136 Infection Prevention and Control Annual Report
Page 8 of 300
7
DL introduced the Infection Prevention and Control (IPC) Annual Report highlighting that there had been no cases of Meticillin Resistant Staphylococcus Aureus (MRSA) blood stream infection (BSI) or of Trust apportioned Clostridium difficile infection. Hand hygiene audits showed good compliance and the IPC team were effective in ensuring that any changes to national guidance were communicated to and embedded with frontline staff.
There was discussion of the number of incidents involving patients’ own equipment. Recognising
that that this was as a result of GP prescribing decisions, members agreed the need to reduce the
risk to SCFT staff.
The Board thanked the IPC team and noted that the framework for infection prevention and control
continued to be effective and robust.
20/137 Mortality Report Q1 2020/21
SL introduced the Mortality Report contrasting the national COVID picture with 9 deaths of SCFT
patients caused by COVID and confirming that there had been no deaths within the Trust related to
Serious Incidents.
NEDs asked about visitors for patients at the end of life. SL confirmed that in line with national
guidance one visitor was allowed at the end of life, for a restricted amount of time and subject to
being arranged in advance where possible to minimise the number of visitors at the same time.
The Board noted the report.
20/138 Medical Revalidation and Appraisal Annual Report
The Board noted the report including the Statement of Compliance at Appendix 1. The Chief
Executive would sign this on behalf of the Board following the meeting.
20/139 Duty of Candour Annual Report
The Board noted the report which included the significant improvements made since the previous
year’s report and outlined further actions to be taken to support staff.
20/140 Staff Flu Campaign 2020/21
DL presented a briefing on the Trust’s staff flu campaign highlighting the Healthcare Worker Flu
Vaccination Best Management Checklist included at Appendix A of the report.
20/141 Any Other Business
The Chair noted that the NHS COVID app for England was now available.
Meeting closed.
Date of next meeting: 26 November 2020
02 P
art 1
Pub
lic B
oard
Min
utes
200
924
Page 9 of 300

1
.
A
CT
ION
S L
IST
– T
RU
ST
BO
AR
D 2
6 N
ove
mb
er
202
0
AC
TIO
N
RE
F.
BO
AR
D
DA
TE
A
CT
ION
W
HO
D
UE
D
AT
E
ST
AT
US
Bo
D2
0/0
9b
30/0
1/2
0
Pro
po
sed
Com
mu
nity N
urs
ing
metr
ics to
com
e b
ack
to B
oard
fo
llow
ing
co
nsid
era
tio
n b
y t
he Q
ualit
y
Impro
ve
me
nt C
om
mitte
e
D
L
26/1
1/2
0
Th
e B
oard
sh
ou
ld r
ece
ive
an
upd
ate
on
co
mm
unity n
urs
ing
defe
rra
ls in
Nove
mb
er
202
0.
Bo
D
(CO
VID
) 2
0/1
02
25/0
6/2
0
Bo
ard
to r
evis
it th
e N
HS
Lon
g T
erm
Pla
n –
form
at to
be a
gre
ed.
Z
S
31/0
3/2
1
Su
bje
ct to
NH
SE
/I r
evie
w o
f th
e L
ong
Term
Pla
n.
De
ferr
ed u
ntil C
OV
ID in
cid
en
t re
spo
nse
leve
l sig
nific
antly r
edu
ced.
BoD
20/1
28
24/0
9/2
0
Co
nfirm
th
e
date
b
y
wh
ich
th
e
Tru
st
anticip
ate
s
havin
g r
esto
red a
ll w
aitin
g lis
ts to
pre
-CO
VID
le
ve
ls.
M
J
26/1
1/2
0
With
th
e e
xce
ptio
n 3
serv
ice
s,
all
are
now
re
sto
red to
at
least
80%
of
pre
-CO
VID
le
ve
ls.
The
R
esto
ratio
n a
nd
Reset G
roup
co
ntin
ue
s to
to
m
on
ito
r a
nd
ove
rse
e t
he r
esto
ration
of T
rust
se
rvic
es.
BO
D2
0/1
29
24/0
9/2
0
Mo
re
deta
il o
n
pro
gre
ss
to
imp
rove
R
TT
W
aitin
g
Tim
es
Incom
ple
te
Path
wa
ys
<1
8
Weeks
for
Ch
ildre
n’s
and
Sp
ecia
list
Se
rvic
es t
o b
e i
nclu
de
d i
n
No
ve
mb
er’s r
epo
rt t
o t
he B
oard
.
KP
2
6/1
1/2
0
Bo
D2
0/1
32
24/0
9/2
0
Re
vie
w m
etr
ics in
Bo
ard
wo
rkfo
rce
re
po
rtin
g.
CH
2
6/1
1/2
0
Co
mp
lete
. W
ork
forc
e m
etr
ics w
ere
re
vie
we
d a
s
part
of
the d
eve
lopm
ent of
the In
teg
rate
d
Pe
rfo
rma
nce R
epo
rt.
Bo
D2
0/1
33b
2
4/0
9/2
0
Incre
ase
d d
eta
il o
n pa
tie
nt
rela
ted E
DI
issu
es a
nd
sta
ff
repre
senta
tion
to
b
e
inclu
de
d
with
in
futu
re
Eq
ualit
ies R
ep
ort
s
CH
2
6/1
1/2
0
Sin
ce t
he S
epte
mb
er
Boa
rd th
ere
has b
ee
n
furt
her
wo
rk t
o h
igh
ligh
t p
atie
nt re
late
d E
DI
in th
e
201
9/2
0 E
qu
alit
ies R
ep
ort
. T
he B
oard
is a
ske
d t
o
dele
ga
te a
pp
rova
l of
a r
evis
ed r
epo
rt t
o t
he
Qu
alit
y I
mpro
ve
me
nt C
om
mitte
e.
Bo
D2
0/1
35
24/0
9/2
0
Up
da
te o
n s
uic
ides w
here
TT
T in
vo
lve
d t
o b
e
inclu
de
d in
Q2
20
20
/21 S
I R
epo
rt
SL
26/1
1/2
0
Co
mp
lete
. In
clu
de
d in
the
Q2 2
02
0/2
1 S
I re
port
.
03 P
art 1
Boa
rd A
ctio
n Lo
g20
1126
Page 10 of 300

BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number: 04
Report Title: Corporate Objectives & BAF 2020/21 Q2 Report
Purpose:
Approval Assurance x Discussion Briefing
Summary: Sussex Community NHS Foundation Trust’s 2019-22 strategy, designed to achieve ‘excellent care at the heart of the community’, has five strategic goals. From these a set of annual corporate objectives for 2020-21 were provisionally agreed by the Board in March 2020. These were reviewed in September 2020 and a set of revised corporate objectives for the remainder of 2020-21 was agreed by the Trust Board on 5 November 2020. The Board Assurance Framework (BAF) records and reports on the key risks to delivery of the Trust’s strategic goals 2019-22, the controls in place, sources and levels of assurance and any gaps in controls or assurance. The SCFT BAF has been redesigned to provide better view of the totality of risks to the Trust’s strategic goals as well as better oversight of individual thematic risks, controls and assurances. The BAF is presented alongside the revised Corporate Objectives for 2020-21. The normal quarterly cycle of reporting the BAF and progress against delivery of the corporate objectives to public meetings of the Board will resume from January 2021. A Board Assurance Framework (BAF) Guide is provided at Appendix 3 which details the key stages leading up to the presentation of the BAF, and information on how the BAF template is populated
Recommendation:
The Board is asked to note the Board Assurance Framework Q2 2020/21.
Previously reviewed by: Siobhan Melia, Chief Executive
Relevance to Trust’s Strategic Goals: All - Population Health; Quality Improvement; Patient Experience; Thriving Staff; Value and Sustainability
Relevance to CQC Domains: All - Safe; Caring; Responsive; Effective; Well Led
04 C
S C
orpo
rate
Obj
ectiv
esan
d B
AF
Page 11 of 300
Equality and Diversity: One of the Trust’s strategic goals is to improve health and care outcomes, including meeting the needs of diverse communities and tackling health inequalities. Ensuring services can meet the needs of all segments of the population by developing systematic approaches to the collection and understanding of equalities data is one of the corporate objectives for the remainder of 2020-21.
Report author: Zoe Smith, Trust Secretary
Report owner: Siobhan Melia, Chief Executive
Page 12 of 300
TRUST BOARD
26 November 2020
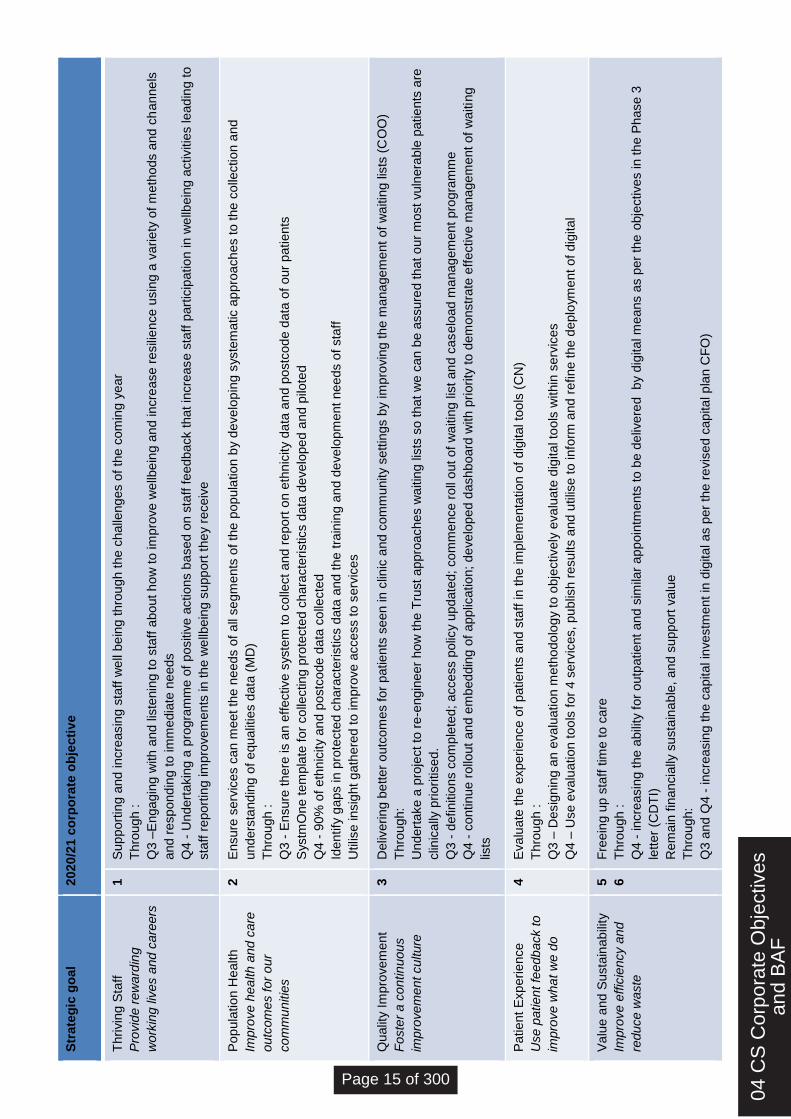
2020/21 Corporate Objectives and Board Assurance Framework 1. 2020/21 Corporate Objectives
Sussex Community NHS Foundation Trust’s 2019-2022 strategy, designed to achieve ‘excellent care at the heart of the community’, has five strategic goals:
1. Thriving Staff
Provide rewarding working lives and careers
2. Population Health
Improve health and care outcomes for our communities
3. Quality Improvement
Foster a continuous improvement culture
4. Patient Experience
Use patient feedback to improve what we do
5. Value and Sustainability
Improve efficiency and reduce waste
Each year the Trust agrees a set of annual corporate objectives which contribute to the delivery of these strategic goals. The Trust’s initial 2020/21 corporate objectives were agreed by the Board in March 2020 on a provisional basis due to the uncertainty created by the COVID situation at that time. These provisional objectives were reviewed by the Board again in September 2020 in the context of the learning from the Trust’s reset plans following the first stages of the pandemic response and various external factors, including the ongoing response to the pandemic and the requirements set out within the NHS Improvement and NHS England phase 3 letter. A set of revised corporate objectives has now been agreed for the remainder of 2020-21. These are shown at Appendix 1. 2. Board Assurance Framework (BAF)
This report also provides the board with the Board Assurance Framework (BAF) as at Q2 2020-21 (Appendix 2) to provide assurance to the Board that there are systems and controls in place to mitigate risks which may threaten the delivery of the Trust’s strategic goals. The Board Assurance Framework (BAF) records and reports on the key risks to delivery of the Trust’s strategic goals 2019-22, the controls in place, sources and levels of assurance and any gaps in controls or assurance. Following a pause in BAF production as part of reducing the burden for COVID and the Board’s review of the Trust’s corporate objectives for 2020-21, the SCFT BAF
04 C
S C
orpo
rate
Obj
ectiv
esan
d B
AF
Page 13 of 300
has been redesigned to provide better view of the totality of risks to the Trust’s strategic goals as well as better oversight of individual thematic risks, controls and assurances. A Board Assurance Framework (BAF) Guide is provided at Appendix 3 which details the key stages leading up to the presentation of the BAF, and information on how the BAF template is populated. 3. Corporate Objective and BAF Reporting Cycle
A report on progress against trajectory for each of the corporate objectives will be presented, alongside the BAF, to meetings of the Trust Board in public on a quarterly basis from January 2021. A review of progress against the Trust’s strategic goals as at end of Year 2 of the three year strategy will be presented to the Board in March 2021.
4. Recommendation
The Board is asked to:
Note the Corporate Objectives for the remainder of 2020-21
Note the Quarter 2 2020-21 BAF
Page 14 of 300
Str
ate
gic
go
al
2020
/21 c
orp
ora
te o
bje
cti
ve
Thrivin
g S
taff
Pro
vid
e r
ew
ard
ing
work
ing liv
es a
nd c
are
ers
1
Sup
port
ing a
nd incre
asin
g s
taff
we
ll be
ing t
hro
ugh t
he c
halle
ng
es o
f th
e c
om
ing y
ear
Thro
ugh :
Q3 –
Enga
gin
g w
ith a
nd
lis
tenin
g t
o s
taff
about h
ow
to im
pro
ve w
ellb
ein
g a
nd incre
ase r
esili
ence u
sin
g a
varie
ty o
f m
eth
ods a
nd
ch
an
ne
ls
and r
esp
ond
ing to im
media
te n
eeds
Q4 -
Undert
akin
g a
pro
gra
mm
e o
f positiv
e a
ctions b
ased o
n s
taff
feedback that in
cre
ase s
taff
part
icip
atio
n in w
ellb
ein
g a
ctivitie
s lead
ing to
sta
ff r
eport
ing im
pro
vem
ents
in th
e w
ellb
ein
g s
upp
ort
the
y r
eceiv
e
Pop
ula
tion H
ealth
Impro
ve h
ea
lth a
nd
care
outc
om
es for
our
com
mu
nitie
s
2
Ensure
serv
ices c
an
meet th
e n
eeds o
f a
ll se
gm
ents
of th
e p
op
ula
tio
n b
y d
evelo
pin
g s
yste
matic a
ppro
ach
es to the
colle
ction a
nd
unders
tand
ing o
f equa
litie
s d
ata
(M
D)
Thro
ugh :
Q3 -
Ensure
there
is a
n e
ffective s
yste
m to c
olle
ct a
nd
report
on e
thn
icity d
ata
an
d p
ostc
od
e d
ata
of
our
patients
Systm
One tem
pla
te f
or
co
llecting
pro
tecte
d c
hara
cte
ristics d
ata
de
velo
pe
d a
nd p
ilote
d
Q4 -
90%
of
eth
nic
ity a
nd p
ostc
ode d
ata
co
llecte
d
Identify
gaps in p
rote
cte
d c
hara
cte
ristics d
ata
and
the
tra
inin
g a
nd d
eve
lopm
ent needs o
f sta
ff
Utilis
e insig
ht g
ath
ere
d t
o im
pro
ve a
ccess to s
erv
ices
Qualit
y I
mpro
vem
ent
Foste
r a c
ontin
uous
impro
ve
me
nt culture
3
Deliv
erin
g b
etter
outc
om
es for
patien
ts s
een in c
linic
and c
om
munity s
ett
ings b
y im
pro
vin
g th
e m
anagem
ent
of
wa
itin
g lis
ts (
CO
O)
Thro
ugh:
Undert
ake a
pro
ject to
re
-engin
eer
ho
w t
he T
rust appro
aches w
aitin
g lis
ts s
o t
hat
we c
an b
e a
ssure
d th
at o
ur
most vuln
era
ble
patie
nts
are
clin
ically
priori
tise
d.
Q3 -
definitio
ns c
om
ple
ted;
access p
olic
y u
pdate
d; co
mm
ence r
oll
out of
wa
itin
g lis
t an
d c
aselo
ad m
anag
em
ent pro
gra
mm
e
Q4 -
continue r
ollo
ut
an
d e
mbeddin
g o
f applic
ation;
de
ve
lop
ed d
ashb
oard
with p
riority
to d
em
onstr
ate
eff
ective m
anagem
ent of
waitin
g
lists
Patient
Exp
erie
nce
Use p
atien
t fe
edb
ack to
impro
ve
wha
t w
e d
o
4
Evalu
ate
the e
xperi
ence o
f patients
and s
taff
in th
e im
ple
menta
tion o
f d
igital to
ols
(C
N)
Thro
ugh :
Q3 –
Desig
nin
g a
n e
valu
ation m
eth
odo
log
y t
o o
bje
ctively
eva
luate
dig
ita
l to
ols
within
serv
ices
Q4 –
Use e
valu
ation t
oo
ls f
or
4 s
erv
ices, pu
blis
h r
esu
lts a
nd u
tilis
e t
o info
rm a
nd r
efine th
e d
eplo
ym
ent of
dig
ital
Valu
e a
nd
Susta
inab
ility
Impro
ve e
ffic
iency a
nd
reduce w
aste
5
6
Fre
ein
g u
p s
taff
tim
e to c
are
Thro
ugh :
Q4 -
incre
asin
g t
he a
bili
ty f
or
outp
atient
an
d s
imila
r ap
poin
tments
to b
e d
eliv
ere
d
by d
igital m
eans a
s p
er
the
obje
ctives in th
e P
hase 3
lett
er
(CD
TI)
Rem
ain
fin
ancia
lly s
usta
ina
ble
, an
d s
upp
ort
valu
e
Thro
ugh:
Q3 a
nd
Q4 -
incre
asin
g th
e c
apital in
vestm
ent in
dig
ital as p
er
the r
evis
ed c
ap
ita
l p
lan C
FO
)
04 C
S C
orpo
rate
Obj
ectiv
esan
d B
AF
Page 15 of 300

Page 16 of 300
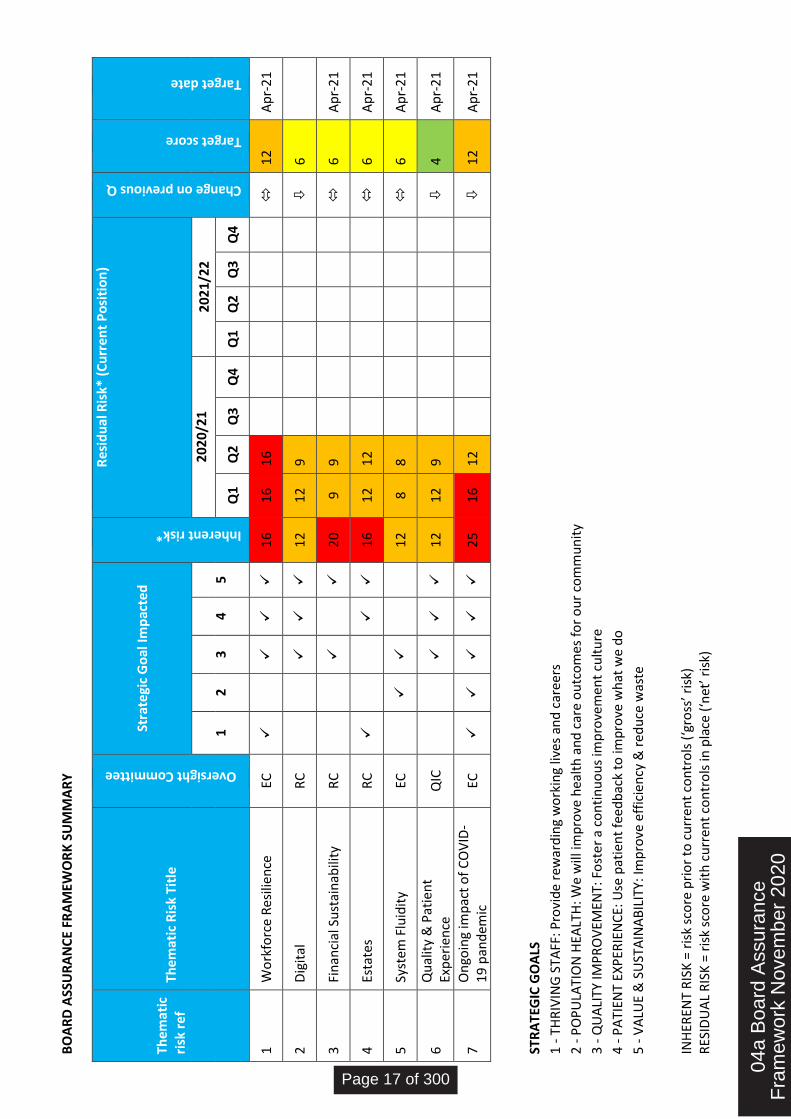
INH
EREN
T R
ISK
= r
isk
sco
re p
rio
r to
cu
rren
t co
ntr
ols
(‘g
ross
’ ris
k)
RES
IDU
AL
RIS
K =
ris
k sc
ore
wit
h c
urr
ent
con
tro
ls in
pla
ce (
‘net
’ ris
k)
BO
AR
D A
SSU
RA
NC
E FR
AM
EWO
RK
SU
MM
AR
Y
The
mat
ic
risk
ref
Th
emat
ic R
isk
Titl
e
Oversight Committee
Stra
tegi
c G
oal
Imp
acte
d
Inherent risk*
Re
sid
ual
Ris
k* (
Cu
rren
t P
osi
tio
n)
Change on previous Q
Target score
Target date
1 2
3 4
5
20
20/
21
2
021
/22
Q1
Q2
Q3
Q4
Q1
Q2
Q3
Q4
1 W
ork
forc
e R
esili
ence
EC
16
16
1
6
1
2
Ap
r-2
1
2 D
igit
al
RC
1
2 1
2
9
6
3 Fi
nan
cial
Su
stai
nab
ility
R
C
2
0 9
9
6
Ap
r-2
1
4 Es
tate
s
RC
1
6 1
2
12
6 A
pr-
21
5 Sy
stem
Flu
idit
y EC
12
8 8
6 A
pr-
21
6 Q
ual
ity
& P
atie
nt
Exp
erie
nce
Q
IC
12
12
9
4 A
pr-
21
7 O
ngo
ing
imp
act
of
CO
VID
-1
9 p
and
emic
EC
2
5 1
6
12
12
A
pr-
21
STR
ATE
GIC
GO
ALS
1 -
TH
RIV
ING
STA
FF: P
rovi
de
rew
ard
ing
wo
rkin
g liv
es a
nd
car
eers
2 -
PO
PU
LATI
ON
HEA
LTH
: We
will
imp
rove
hea
lth
an
d c
are
ou
tco
mes
fo
r o
ur
com
mu
nit
y
3 -
QU
ALI
TY IM
PR
OV
EMEN
T: F
ost
er
a co
nti
nu
ou
s im
pro
vem
ent
cult
ure
4 -
PA
TIEN
T EX
PER
IEN
CE:
Use
pat
ien
t fe
edb
ack
to im
pro
ve w
hat
we
do
5 -
VA
LUE
& S
UST
AIN
AB
ILIT
Y: Im
pro
ve e
ffic
ien
cy &
red
uce
was
te
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 17 of 300
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
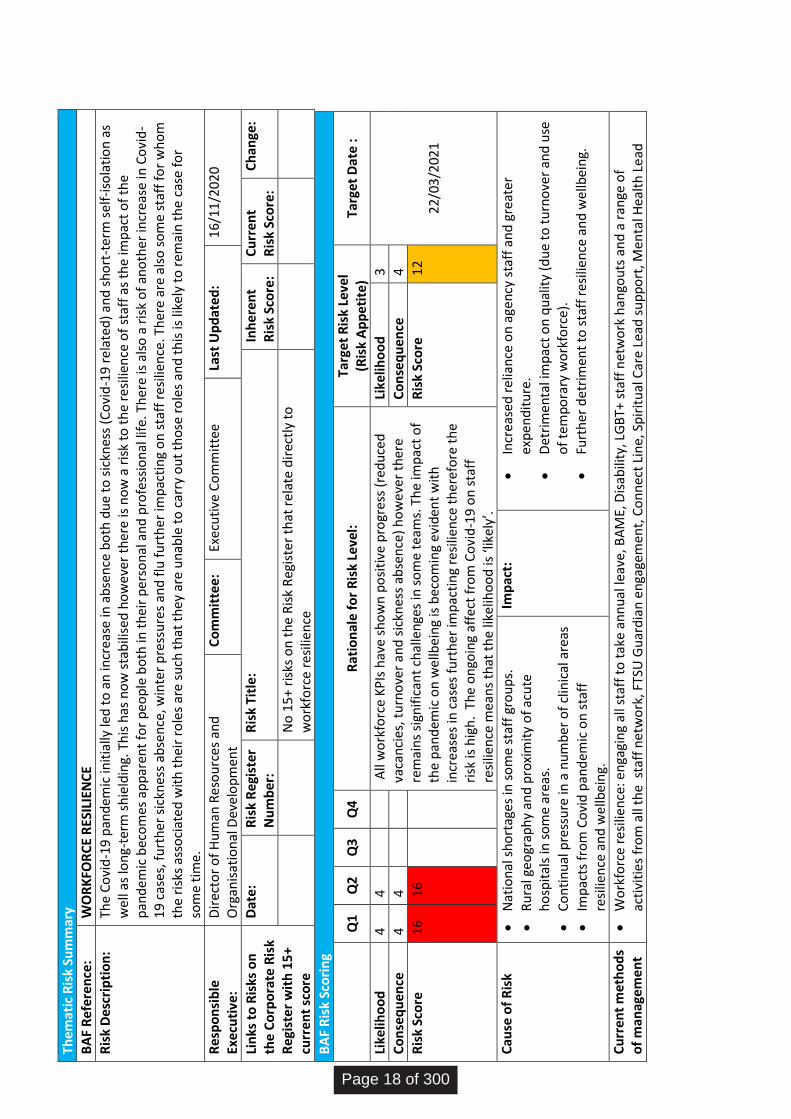
WO
RK
FOR
CE
RES
ILIE
NC
E
Ris
k D
esc
rip
tio
n:
The
Co
vid
-19
pan
dem
ic in
itia
lly le
d t
o a
n in
crea
se in
ab
sen
ce b
oth
du
e to
sic
knes
s (C
ovi
d-1
9 r
elat
ed)
and
sh
ort
-ter
m s
elf
-iso
lati
on
as
we
ll as
lon
g-te
rm s
hie
ldin
g. T
his
has
no
w s
tab
ilise
d h
ow
eve
r th
ere
is n
ow
a r
isk
to t
he
resi
lien
ce o
f st
aff
as t
he
imp
act
of
the
pan
dem
ic b
eco
mes
ap
par
ent
for
peo
ple
bo
th in
th
eir
per
son
al a
nd
pro
fess
ion
al li
fe. T
her
e is
als
o a
ris
k o
f an
oth
er in
crea
se in
Co
vid
-1
9 c
ases
, fu
rth
er s
ickn
ess
abse
nce
, win
ter
pre
ssu
res
and
flu
fu
rth
er im
pac
tin
g o
n s
taff
res
ilien
ce. T
her
e ar
e al
so s
om
e st
aff
for
wh
om
th
e ri
sks
asso
ciat
ed w
ith
th
eir
role
s ar
e su
ch t
hat
th
ey a
re u
nab
le t
o c
arry
ou
t th
ose
ro
les
and
th
is is
like
ly t
o r
emai
n t
he
cas
e fo
r so
me
tim
e.
Re
spo
nsi
ble
Ex
ecu
tive
: D
irec
tor
of
Hu
man
Res
ou
rces
an
d
Org
anis
atio
nal
Dev
elo
pm
ent
C
om
mit
tee:
Ex
ecu
tive
Co
mm
itte
e
Last
Up
dat
ed
: 1
6/1
1/2
02
0
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egi
ster
N
um
ber
: R
isk
Titl
e:
Inh
eren
t R
isk
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
ange
:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to
wo
rkfo
rce
resi
lien
ce
BA
F R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
4
4
A
ll w
ork
forc
e K
PIs
hav
e sh
ow
n p
osi
tive
pro
gres
s (r
edu
ced
va
can
cies
, tu
rno
ver
and
sic
knes
s ab
sen
ce)
ho
wev
er t
her
e re
mai
ns
sign
ific
ant
chal
len
ges
in s
om
e te
ams.
Th
e im
pac
t o
f th
e p
and
emic
on
wel
lbei
ng
is b
eco
min
g e
vid
ent
wit
h
incr
ease
s in
cas
es f
urt
her
imp
acti
ng
resi
lien
ce t
her
efo
re t
he
risk
is h
igh
. Th
e o
ngo
ing
affe
ct f
rom
Co
vid
-19
on
sta
ff
resi
lien
ce m
ean
s th
at t
he
like
liho
od
is ‘l
ike
ly’.
Like
liho
od
3
22
/03
/202
1
Co
nse
qu
ence
4
4
C
on
seq
uen
ce
4
Ris
k Sc
ore
1
6
16
R
isk
Sco
re
12
Cau
se o
f R
isk
Nat
ion
al s
ho
rtag
es in
so
me
staf
f gr
ou
ps.
Ru
ral g
eogr
aph
y an
d p
roxi
mit
y o
f ac
ute
h
osp
ital
s in
so
me
area
s.
Co
nti
nu
al p
ress
ure
in a
nu
mb
er o
f cl
inic
al a
reas
Imp
acts
fro
m C
ovi
d p
and
emic
on
sta
ff
resi
lien
ce a
nd
wel
lbei
ng.
Imp
act:
Incr
ease
d r
elia
nce
on
age
ncy
sta
ff a
nd
gre
ate
r ex
pen
dit
ure
.
Det
rim
enta
l im
pac
t o
n q
ual
ity
(du
e to
tu
rno
ver
and
use
o
f te
mp
ora
ry w
ork
forc
e).
Furt
her
det
rim
ent
to s
taff
res
ilien
ce a
nd
wel
lbei
ng.
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
Wo
rkfo
rce
resi
lien
ce: e
nga
gin
g al
l sta
ff t
o t
ake
ann
ual
leav
e, B
AM
E, D
isab
ility
, LG
BT+
sta
ff n
etw
ork
han
gou
ts a
nd
a r
ange
of
acti
viti
es f
rom
all
the
sta
ff n
etw
ork
, FTS
U G
uar
dia
n e
nga
gem
ent,
Co
nn
ect
Lin
e, S
pir
itu
al C
are
Lead
su
pp
ort
, Men
tal H
ealt
h L
ead
Page 18 of 300
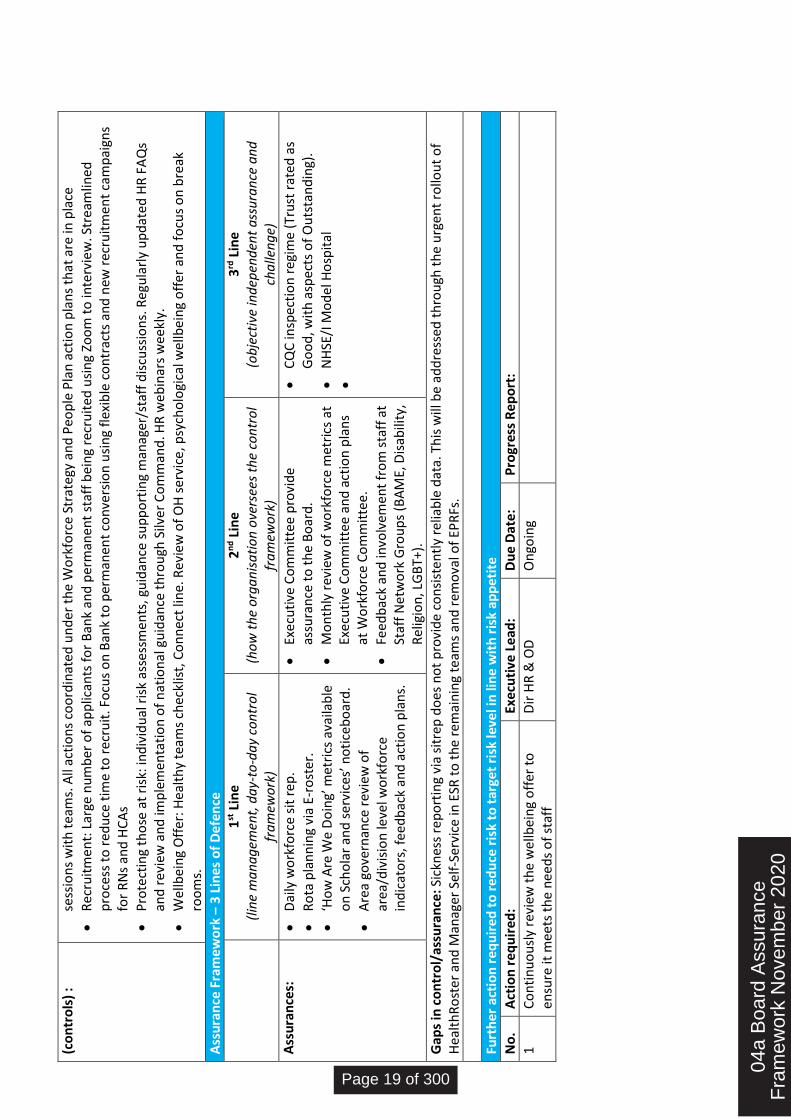
(co
ntr
ols
) :
se
ssio
ns
wit
h t
eam
s. A
ll ac
tio
ns
coo
rdin
ated
un
der
th
e W
ork
forc
e St
rate
gy a
nd
Peo
ple
Pla
n a
ctio
n p
lan
s th
at a
re in
pla
ce
Rec
ruit
men
t: L
arge
nu
mb
er o
f ap
plic
ants
fo
r B
ank
and
per
man
ent
staf
f b
ein
g re
cru
ited
usi
ng
Zoo
m t
o in
terv
iew
. Str
eam
lined
p
roce
ss t
o r
edu
ce t
ime
to r
ecru
it. F
ocu
s o
n B
ank
to p
erm
anen
t co
nve
rsio
n u
sin
g fl
exib
le c
on
trac
ts a
nd
new
rec
ruit
men
t ca
mp
aign
s fo
r R
Ns
and
HC
As
Pro
tect
ing
tho
se a
t ri
sk: i
nd
ivid
ual
ris
k as
sess
men
ts, g
uid
ance
su
pp
ort
ing
man
ager
/sta
ff d
iscu
ssio
ns.
Reg
ula
rly
up
dat
ed H
R F
AQ
s an
d r
evie
w a
nd
imp
lem
enta
tio
n o
f n
atio
nal
gu
idan
ce t
hro
ugh
Silv
er C
om
man
d. H
R w
ebin
ars
wee
kly.
Wel
lbei
ng
Off
er: H
ealt
hy
team
s ch
eckl
ist,
Co
nn
ect
line.
Rev
iew
of
OH
ser
vice
, psy
cho
logi
cal w
ellb
ein
g o
ffer
an
d f
ocu
s o
n b
reak
ro
om
s.
Ass
ura
nce
Fra
mew
ork
– 3
Lin
es o
f D
efe
nce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Dai
ly w
ork
forc
e si
t re
p.
Ro
ta p
lan
nin
g vi
a E-
rost
er.
‘Ho
w A
re W
e D
oin
g’ m
etri
cs a
vaila
ble
o
n S
cho
lar
and
se
rvic
es’ n
oti
ceb
oar
d.
Are
a go
vern
ance
rev
iew
of
area
/div
isio
n le
vel w
ork
forc
e in
dic
ato
rs, f
eed
bac
k an
d a
ctio
n p
lan
s.
Exe
cuti
ve C
om
mit
tee
pro
vid
e as
sura
nce
to
th
e B
oar
d.
Mo
nth
ly r
evie
w o
f w
ork
forc
e m
etri
cs a
t Ex
ecu
tive
Co
mm
itte
e a
nd
act
ion
pla
ns
at W
ork
forc
e C
om
mit
tee.
Feed
bac
k an
d in
volv
emen
t fr
om
sta
ff a
t St
aff
Net
wo
rk G
rou
ps
(BA
ME,
Dis
abili
ty,
Rel
igio
n, L
GB
T+).
CQ
C in
spec
tio
n r
egim
e (T
rust
rat
ed a
s G
oo
d, w
ith
asp
ects
of
Ou
tsta
nd
ing)
.
NH
SE/I
Mo
del
Ho
spit
al
Gap
s in
co
ntr
ol/
assu
ran
ce: S
ickn
ess
rep
ort
ing
via
sitr
ep d
oes
no
t p
rovi
de
con
sist
entl
y re
liab
le d
ata.
Th
is w
ill b
e ad
dre
ssed
th
rou
gh t
he
urg
ent
rollo
ut
of
Hea
lth
Ro
ste
r an
d M
anag
er S
elf-
Serv
ice
in E
SR t
o t
he
rem
ain
ing
team
s an
d r
emo
val o
f EP
RFs
.
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
equ
ired
: Ex
ecu
tive
Le
ad:
Du
e D
ate:
P
rogr
ess
Re
po
rt:
1 C
on
tin
uo
usl
y re
view
th
e w
ellb
ein
g o
ffer
to
en
sure
it m
eets
th
e n
eed
s o
f st
aff
Dir
HR
& O
D
On
goin
g
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 19 of 300
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
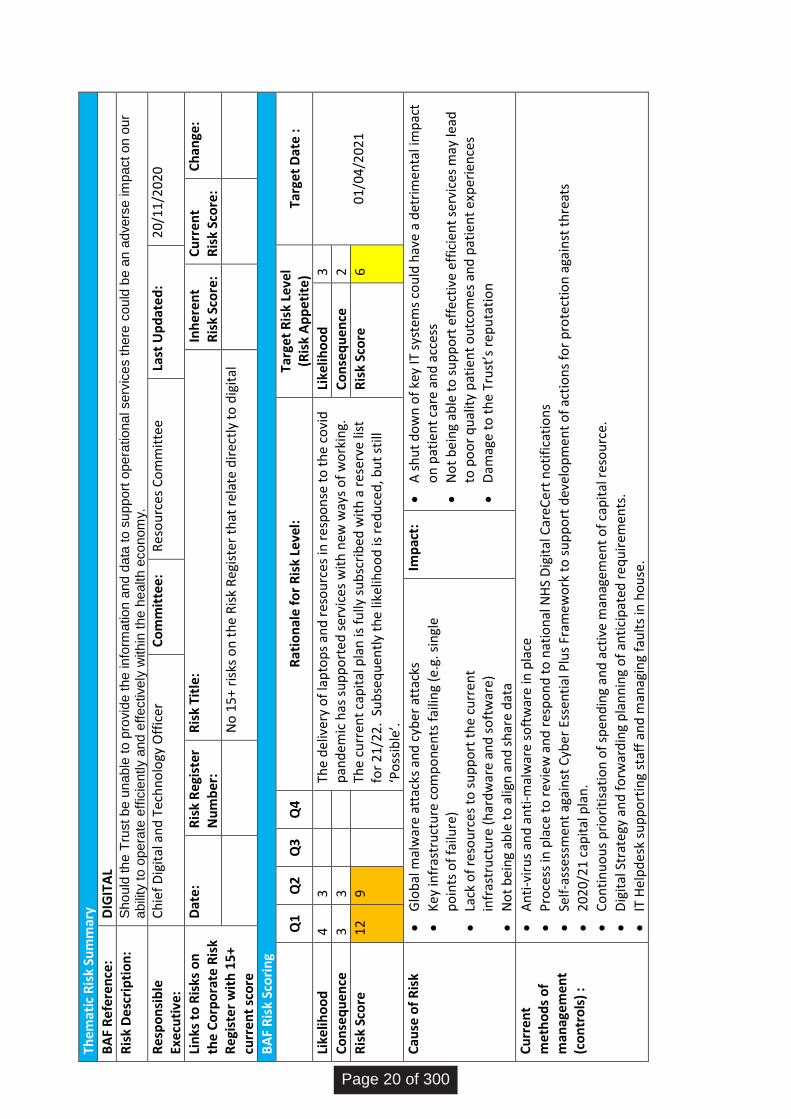
DIG
ITA
L
Ris
k D
esc
rip
tio
n:
Sh
ou
ld th
e T
rust
be
un
able
to p
rovid
e t
he in
form
atio
n a
nd
data
to s
up
po
rt o
pe
ratio
na
l se
rvic
es t
he
re c
ou
ld b
e a
n a
dve
rse
im
pact
on
ou
r a
bili
ty t
o o
pera
te e
ffic
iently a
nd
eff
ective
ly w
ith
in t
he h
ealth
eco
nom
y.
Re
spo
nsi
ble
Ex
ecu
tive
: C
hie
f D
igit
al a
nd
Tec
hn
olo
gy O
ffic
er
Co
mm
itte
e:
Res
ou
rces
Co
mm
itte
e
Last
Up
dat
ed
: 2
0/1
1/2
020
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egi
ster
N
um
ber
: R
isk
Titl
e:
Inh
eren
t R
isk
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
ange
:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to d
igit
al
BA
F R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
4
3
Th
e d
eliv
ery
of
lap
top
s an
d r
eso
urc
es in
res
po
nse
to
th
e co
vid
p
and
emic
has
su
pp
ort
ed s
ervi
ces
wit
h n
ew w
ays
of
wo
rkin
g.
The
curr
ent
cap
ital
pla
n is
fu
lly s
ub
scri
bed
wit
h a
res
erve
list
fo
r 2
1/2
2.
Sub
seq
uen
tly
the
like
liho
od
is r
edu
ced
, bu
t st
ill
‘Po
ssib
le’.
Like
liho
od
3
01/
04/2
021
C
on
seq
uen
ce
3 3
Co
nse
qu
ence
2
Ris
k Sc
ore
1
2 9
Ris
k Sc
ore
6
Cau
se o
f R
isk
Glo
bal
mal
war
e at
tack
s an
d c
yber
att
acks
Ke
y in
fras
tru
ctu
re c
om
po
nen
ts f
ailin
g (e
.g. s
ingl
e p
oin
ts o
f fa
ilure
)
Lack
of
reso
urc
es t
o s
up
po
rt t
he
curr
ent
infr
astr
uct
ure
(h
ard
war
e an
d s
oft
war
e)
No
t b
ein
g ab
le t
o a
lign
an
d s
har
e d
ata
Imp
act:
A s
hu
t d
ow
n o
f ke
y IT
sys
tem
s co
uld
hav
e a
det
rim
enta
l im
pac
t o
n p
atie
nt
care
an
d a
cces
s
No
t b
ein
g ab
le t
o s
up
po
rt e
ffec
tive
eff
icie
nt
serv
ices
may
lead
to
po
or
qu
alit
y p
atie
nt
ou
tco
mes
an
d p
atie
nt
exp
erie
nce
s
Dam
age
to t
he
Tru
st’s
rep
uta
tio
n
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
(co
ntr
ols
) :
An
ti-v
iru
s an
d a
nti
-mal
war
e so
ftw
are
in p
lace
Pro
cess
in p
lace
to
rev
iew
an
d r
esp
on
d t
o n
atio
nal
NH
S D
igit
al C
areC
ert
no
tifi
cati
on
s
Self
-ass
essm
ent
agai
nst
Cyb
er E
sse
nti
al P
lus
Fram
ewo
rk t
o s
up
po
rt d
evel
op
men
t o
f ac
tio
ns
for
pro
tect
ion
aga
inst
th
reat
s
202
0/21
cap
ital
pla
n.
Co
nti
nu
ou
s p
rio
riti
sati
on
of
spen
din
g an
d a
ctiv
e m
anag
emen
t o
f ca
pit
al r
eso
urc
e.
Dig
ital
Str
ate
gy a
nd
fo
rwar
din
g p
lan
nin
g o
f an
tici
pat
ed r
eq
uir
emen
ts.
IT H
elp
des
k su
pp
ort
ing
staf
f an
d m
anag
ing
fau
lts
in h
ou
se.
Page 20 of 300
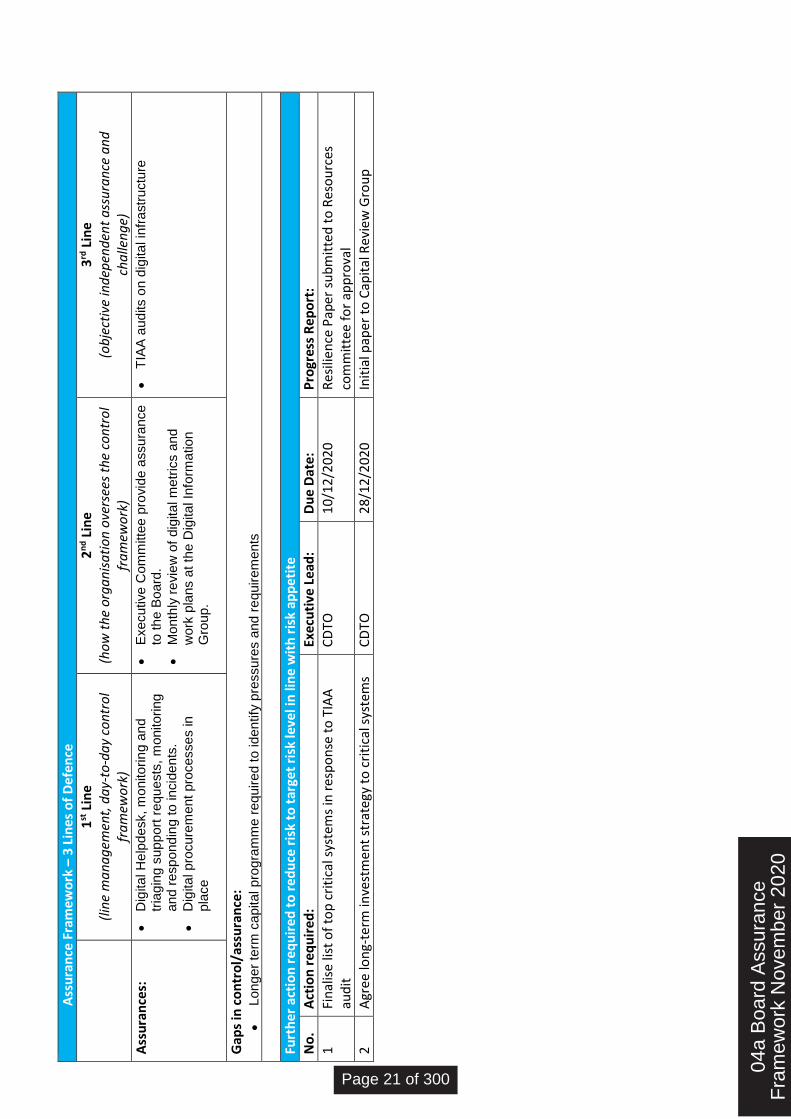
A
ssu
ran
ce F
ram
ewo
rk –
3 L
ines
of
De
fen
ce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Dig
ita
l H
elp
de
sk, m
onito
rin
g a
nd
tr
iag
ing s
upp
ort
re
qu
ests
, m
onito
rin
g
and r
esp
ond
ing
to
in
cid
en
ts.
Dig
ita
l p
rocu
rem
ent
pro
ce
sse
s in
p
lace
Exe
cu
tive
Co
mm
itte
e p
rovid
e a
ssu
ran
ce
to
th
e B
oard
.
Mon
thly
re
vie
w o
f d
igita
l m
etr
ics a
nd
w
ork
pla
ns a
t th
e D
igita
l In
form
atio
n
Gro
up
.
TIA
A a
ud
its o
n d
igita
l in
fra
str
uctu
re
Gap
s in
co
ntr
ol/
assu
ran
ce:
Lon
ge
r te
rm c
apita
l p
rog
ram
me
re
quire
d t
o id
en
tify
pre
ssu
res a
nd
re
quir
em
ents
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
equ
ired
: Ex
ecu
tive
Lea
d:
Du
e D
ate:
P
rogr
ess
Re
po
rt:
1 Fi
nal
ise
list
of
top
cri
tica
l sys
tem
s in
res
po
nse
to
TIA
A
aud
it
CD
TO
10
/12
/202
0
Res
ilien
ce P
aper
su
bm
itte
d t
o R
eso
urc
es
com
mit
tee
for
app
rova
l
2 A
gree
lon
g-te
rm in
vest
men
t st
rate
gy t
o c
riti
cal s
yste
ms
CD
TO
28
/12
/202
0
Init
ial p
aper
to
Cap
ital
Rev
iew
Gro
up
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 21 of 300
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
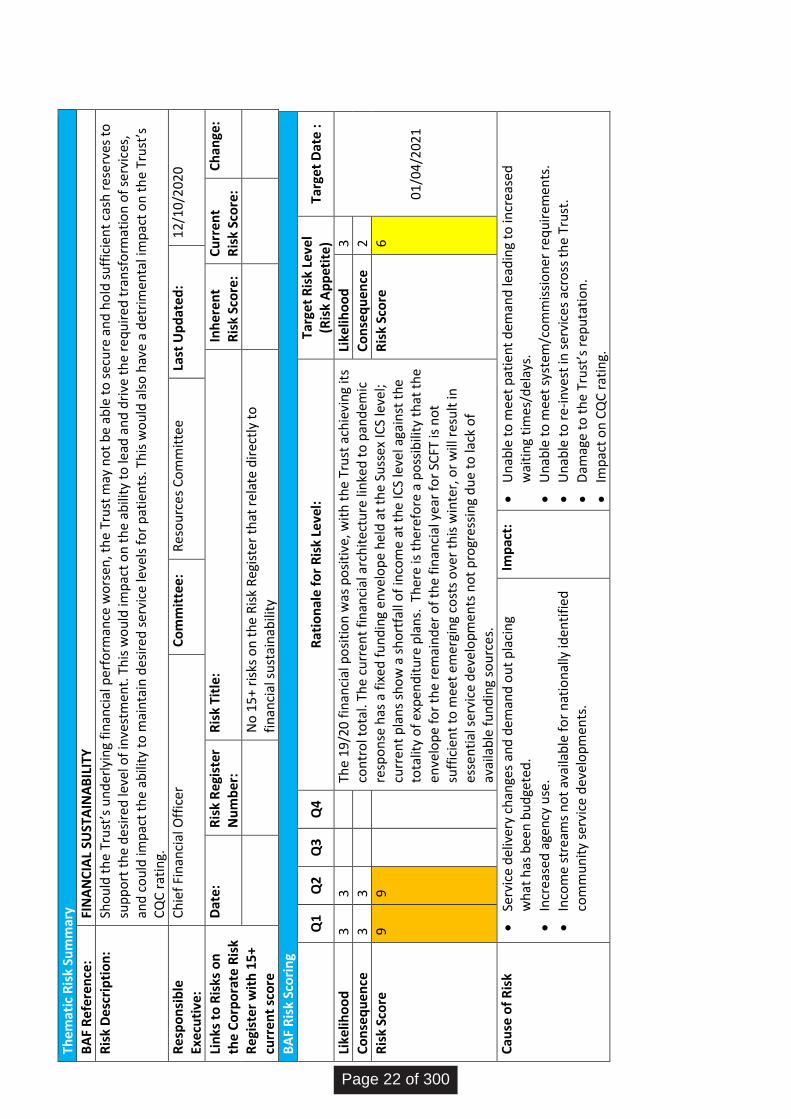
FIN
AN
CIA
L SU
STA
INA
BIL
ITY
Ris
k D
esc
rip
tio
n:
Sho
uld
th
e Tr
ust
’s u
nd
erly
ing
fin
anci
al p
erfo
rman
ce w
ors
en, t
he
Tru
st m
ay n
ot
be
able
to
sec
ure
an
d h
old
su
ffic
ien
t ca
sh r
ese
rves
to
su
pp
ort
th
e d
esir
ed le
vel o
f in
vest
men
t. T
his
wo
uld
imp
act
on
th
e ab
ility
to
lead
an
d d
rive
th
e re
qu
ired
tra
nsf
orm
atio
n o
f se
rvic
es,
and
co
uld
imp
act
the
abili
ty t
o m
ain
tain
des
ired
ser
vice
leve
ls f
or
pat
ien
ts. T
his
wo
uld
als
o h
ave
a d
etri
men
tal i
mp
act
on
th
e Tr
ust
’s
CQ
C r
atin
g.
Re
spo
nsi
ble
Ex
ecu
tive
: C
hie
f Fi
nan
cial
Off
icer
C
om
mit
tee:
R
eso
urc
es C
om
mit
tee
La
st U
pd
ate
d:
12
/10
/202
0
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egi
ster
N
um
ber
: R
isk
Titl
e:
Inh
eren
t R
isk
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
ange
:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to
fin
anci
al s
ust
ain
abili
ty
BA
F R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
3
3
Th
e 1
9/2
0 f
inan
cial
po
siti
on
was
po
siti
ve, w
ith
th
e Tr
ust
ach
ievi
ng
its
con
tro
l to
tal.
The
curr
ent
fin
anci
al a
rch
ite
ctu
re li
nke
d t
o p
and
emic
re
spo
nse
has
a f
ixe
d f
un
din
g e
nve
lop
e h
eld
at
the
Suss
ex IC
S le
vel;
curr
ent
pla
ns
sho
w a
sh
ort
fall
of
inco
me
at t
he
ICS
leve
l aga
inst
th
e to
talit
y o
f ex
pen
dit
ure
pla
ns.
Th
ere
is t
her
efo
re a
po
ssib
ility
th
at t
he
enve
lop
e fo
r th
e re
mai
nd
er o
f th
e fi
nan
cial
yea
r fo
r SC
FT is
no
t su
ffic
ien
t to
mee
t em
ergi
ng
cost
s o
ver
this
win
ter,
or
will
res
ult
in
esse
nti
al s
ervi
ce d
evel
op
men
ts n
ot
pro
gres
sin
g d
ue
to la
ck o
f av
aila
ble
fu
nd
ing
sou
rces
.
Like
liho
od
3
01
/04
/202
1
Co
nse
qu
ence
3
3
C
on
seq
uen
ce
2
Ris
k Sc
ore
9
9
R
isk
Sco
re
6
Cau
se o
f R
isk
Serv
ice
del
iver
y ch
ange
s an
d d
eman
d o
ut
pla
cin
g w
hat
has
bee
n b
ud
gete
d.
Incr
ease
d a
gen
cy u
se.
Inco
me
stre
ams
no
t av
aila
ble
fo
r n
atio
nal
ly id
enti
fied
co
mm
un
ity
serv
ice
dev
elo
pm
ents
.
Imp
act:
Un
able
to
mee
t p
atie
nt
dem
and
lead
ing
to in
crea
sed
w
aiti
ng
tim
es/d
elay
s.
Un
able
to
mee
t sy
stem
/co
mm
issi
on
er r
equ
irem
ents
.
Un
able
to
re
-in
vest
in s
ervi
ces
acro
ss t
he
Tru
st.
Dam
age
to t
he
Tru
st’s
rep
uta
tio
n.
Imp
act
on
CQ
C r
atin
g.
Page 22 of 300
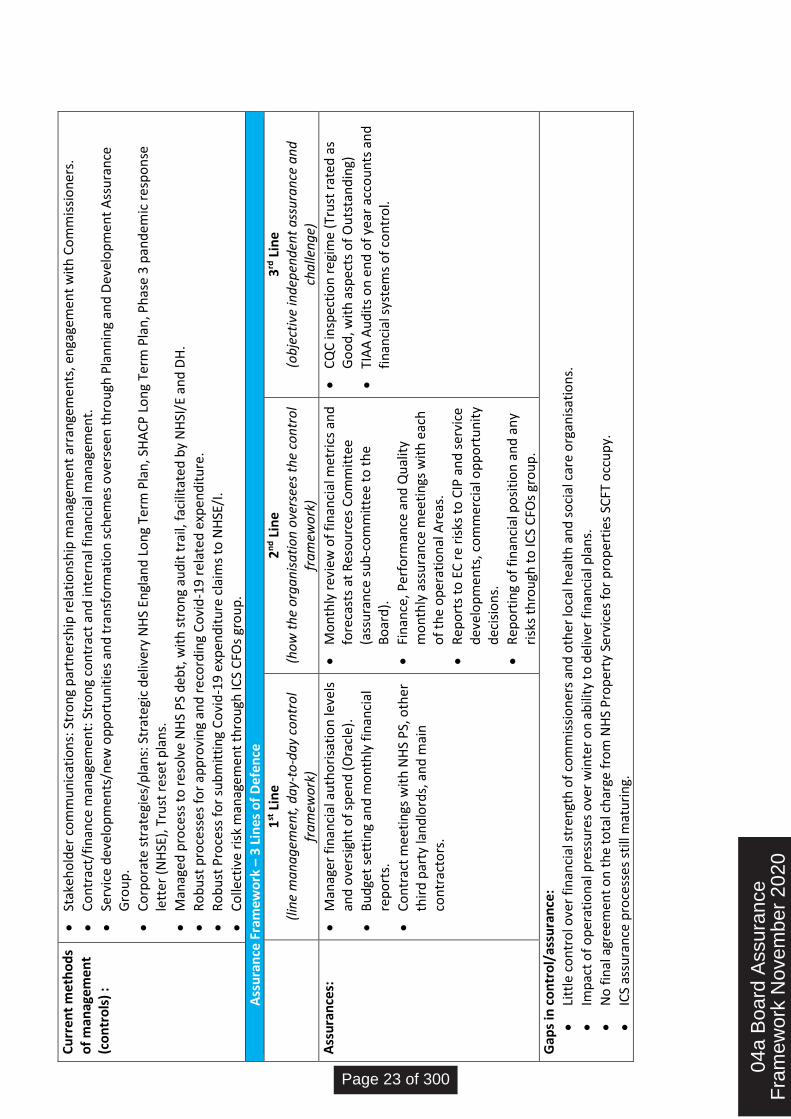
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
(co
ntr
ols
) :
Stak
eho
lder
co
mm
un
icat
ion
s: S
tro
ng
par
tner
ship
rel
atio
nsh
ip m
anag
emen
t ar
ran
gem
ents
, en
gage
men
t w
ith
Co
mm
issi
on
ers.
Co
ntr
act/
fin
ance
man
agem
ent:
Str
on
g co
ntr
act
and
inte
rnal
fin
anci
al m
anag
emen
t.
Serv
ice
dev
elo
pm
ents
/new
op
po
rtu
nit
ies
and
tra
nsf
orm
atio
n s
chem
es o
vers
een
th
rou
gh P
lan
nin
g an
d D
evel
op
men
t A
ssu
ran
ce
Gro
up
.
Co
rpo
rate
str
ateg
ies/
pla
ns:
Str
ate
gic
del
iver
y N
HS
Engl
and
Lo
ng
Term
Pla
n, S
HA
CP
Lo
ng
Term
Pla
n, P
has
e 3
pan
dem
ic r
esp
on
se
lett
er (
NH
SE),
Tru
st r
ese
t p
lan
s.
Man
aged
pro
cess
to
re
solv
e N
HS
PS
deb
t, w
ith
str
on
g au
dit
tra
il, f
acili
tate
d b
y N
HSI
/E a
nd
DH
.
Ro
bu
st p
roce
sses
fo
r ap
pro
vin
g an
d r
eco
rdin
g C
ovi
d-1
9 r
ela
ted
exp
end
itu
re.
Ro
bu
st P
roce
ss f
or
sub
mit
tin
g C
ovi
d-1
9 e
xpen
dit
ure
cla
ims
to N
HSE
/I.
Co
llect
ive
risk
man
agem
ent
thro
ugh
ICS
CFO
s gr
ou
p.
A
ssu
ran
ce F
ram
ewo
rk –
3 L
ines
of
De
fen
ce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Man
ager
fin
anci
al a
uth
ori
sati
on
leve
ls
and
ove
rsig
ht
of
spen
d (
Ora
cle)
.
Bu
dge
t se
ttin
g an
d m
on
thly
fin
anci
al
rep
ort
s.
Co
ntr
act
mee
tin
gs w
ith
NH
S P
S, o
ther
th
ird
par
ty la
nd
lord
s, a
nd
mai
n
con
trac
tors
.
Mo
nth
ly r
evie
w o
f fi
nan
cial
met
rics
an
d
fore
cast
s at
Res
ou
rces
Co
mm
itte
e (a
ssu
ran
ce s
ub
-co
mm
itte
e to
th
e B
oar
d).
Fin
ance
, Per
form
ance
an
d Q
ual
ity
mo
nth
ly a
ssu
ran
ce m
eeti
ngs
wit
h e
ach
o
f th
e o
per
atio
nal
Are
as.
Rep
ort
s to
EC
re
ris
ks t
o C
IP a
nd
ser
vice
d
evel
op
men
ts, c
om
mer
cial
op
po
rtu
nit
y d
ecis
ion
s.
Rep
ort
ing
of
fin
anci
al p
osi
tio
n a
nd
an
y ri
sks
thro
ugh
to
ICS
CFO
s gr
ou
p.
CQ
C in
spec
tio
n r
egim
e (T
rust
rat
ed a
s G
oo
d, w
ith
asp
ects
of
Ou
tsta
nd
ing)
TIA
A A
ud
its
on
en
d o
f ye
ar a
cco
un
ts a
nd
fi
nan
cial
sys
tem
s o
f co
ntr
ol.
Gap
s in
co
ntr
ol/
assu
ran
ce:
Litt
le c
on
tro
l ove
r fi
nan
cial
str
engt
h o
f co
mm
issi
on
ers
and
oth
er lo
cal h
ealt
h a
nd
so
cial
car
e o
rgan
isat
ion
s.
Imp
act
of
op
erat
ion
al p
ress
ure
s o
ver
win
ter
on
ab
ility
to
del
iver
fin
anci
al p
lan
s.
No
fin
al a
gree
men
t o
n t
he
tota
l ch
arge
fro
m N
HS
Pro
per
ty S
ervi
ces
for
pro
per
ties
SC
FT o
ccu
py.
ICS
assu
ran
ce p
roce
sses
sti
ll m
atu
rin
g.
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 23 of 300
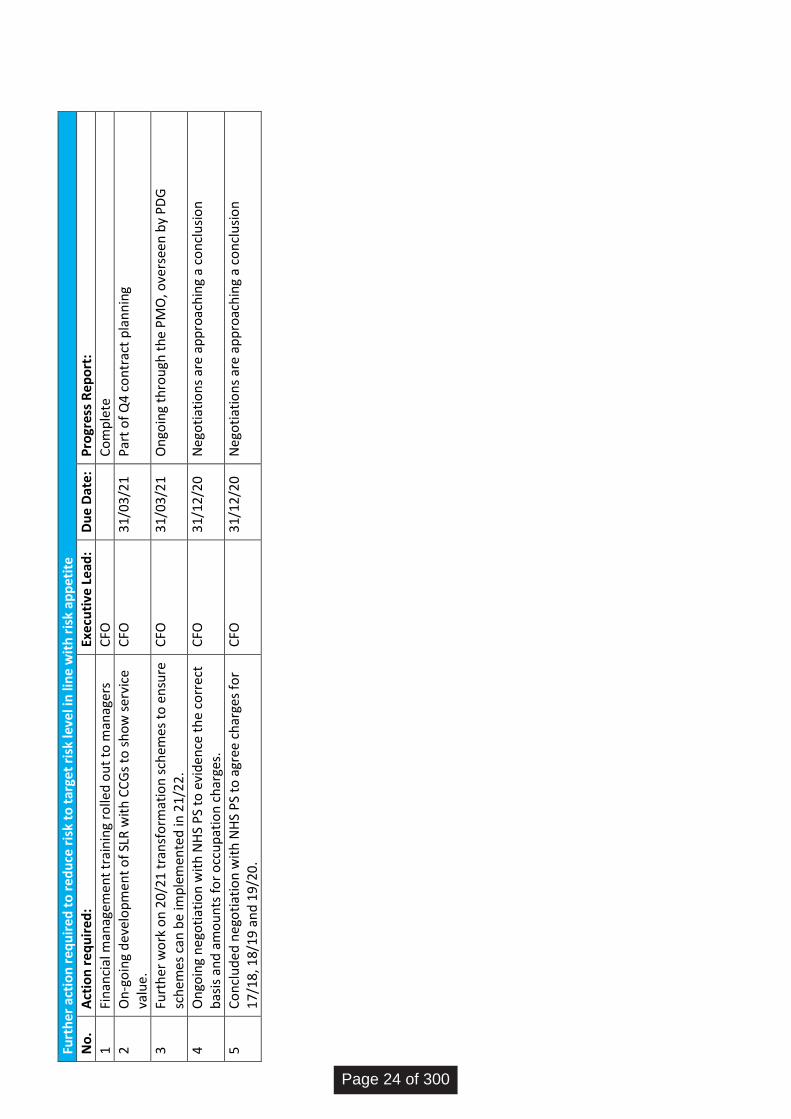
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
eq
uir
ed:
Exec
uti
ve L
ead
: D
ue
Dat
e:
Pro
gres
s R
ep
ort
:
1 Fi
nan
cial
man
agem
ent
trai
nin
g ro
lled
ou
t to
man
ager
s C
FO
C
om
ple
te
2 O
n-g
oin
g d
evel
op
men
t o
f SL
R w
ith
CC
Gs
to s
ho
w s
ervi
ce
valu
e.
CFO
3
1/0
3/2
1
Par
t o
f Q
4 c
on
trac
t p
lan
nin
g
3 Fu
rth
er w
ork
on
20/
21 t
ran
sfo
rmat
ion
sch
emes
to
en
sure
sc
hem
es c
an b
e im
ple
men
ted
in 2
1/2
2.
CFO
3
1/0
3/2
1
On
goin
g th
rou
gh t
he
PM
O, o
vers
een
by
PD
G
4 O
ngo
ing
neg
oti
atio
n w
ith
NH
S P
S to
evi
den
ce t
he
corr
ect
bas
is a
nd
am
ou
nts
fo
r o
ccu
pat
ion
ch
arge
s.
CFO
3
1/1
2/2
0
Neg
oti
atio
ns
are
app
roac
hin
g a
con
clu
sio
n
5 C
on
clu
ded
neg
oti
atio
n w
ith
NH
S P
S to
agr
ee c
har
ges
for
17/
18, 1
8/19
an
d 1
9/20
. C
FO
31
/12
/20
N
ego
tiat
ion
s ar
e ap
pro
ach
ing
a co
ncl
usi
on
Page 24 of 300
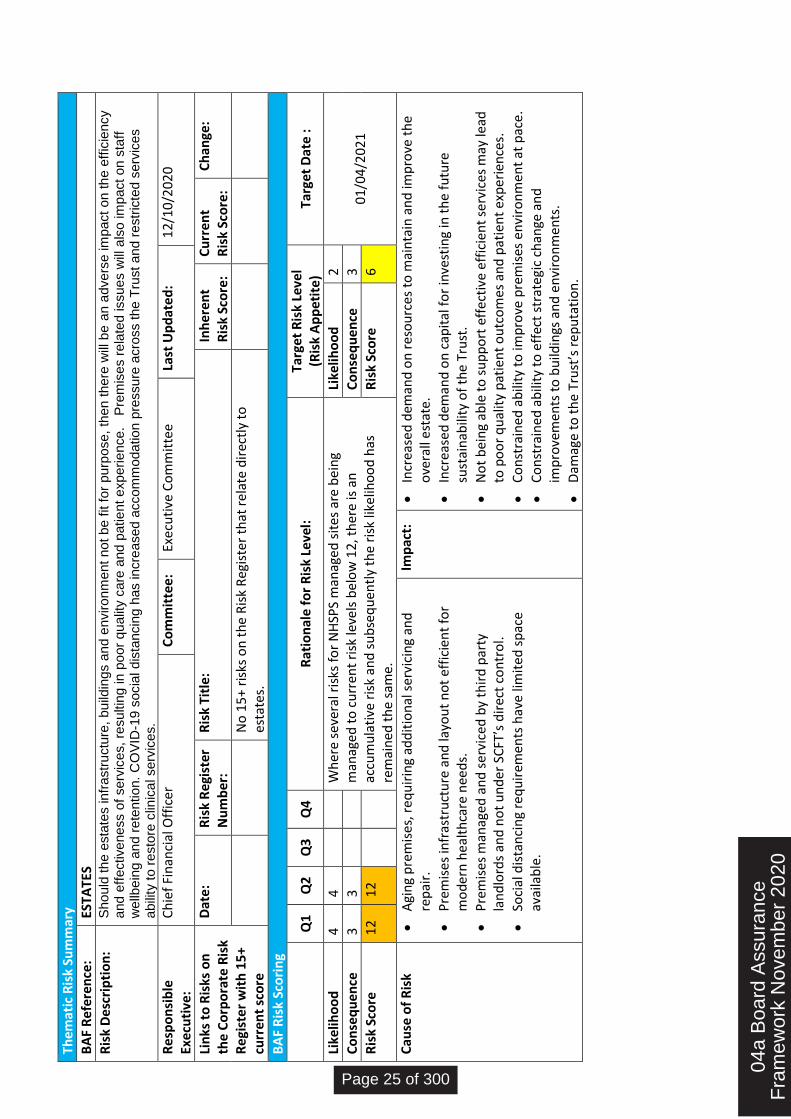
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
ESTA
TES
Ris
k D
esc
rip
tio
n:
Sh
ou
ld th
e e
sta
tes in
fra
str
uctu
re,
bu
ildin
gs a
nd
en
viro
nm
ent
no
t b
e f
it f
or
pu
rpo
se
, th
en
th
ere
will
be a
n a
dve
rse
im
pact
on
th
e e
ffic
iency
and
eff
ective
ne
ss o
f se
rvic
es,
resu
ltin
g in
po
or
qu
alit
y c
are
and
patie
nt e
xp
erie
nce
.
Pre
mis
es r
ela
ted
issu
es w
ill a
lso
im
pact
on
sta
ff
we
llbe
ing
an
d r
ete
ntio
n.
CO
VID
-19 s
ocia
l d
ista
ncin
g h
as in
cre
ase
d a
cco
mm
oda
tio
n p
ressu
re a
cro
ss t
he
Tru
st
an
d r
estr
icte
d s
erv
ice
s
abili
ty t
o r
esto
re c
linic
al se
rvic
es.
Re
spo
nsi
ble
Ex
ecu
tive
: C
hie
f Fi
nan
cial
Off
icer
C
om
mit
tee:
Ex
ecu
tive
Co
mm
itte
e
Last
Up
dat
ed
: 1
2/1
0/2
02
0
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egi
ster
N
um
ber
: R
isk
Titl
e:
Inh
eren
t R
isk
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
ange
:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to
esta
tes.
BA
F R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
4
4
W
her
e se
vera
l ris
ks f
or
NH
SPS
man
aged
sit
es a
re b
ein
g m
anag
ed t
o c
urr
ent
risk
leve
ls b
elo
w 1
2, t
her
e is
an
ac
cum
ula
tive
ris
k an
d s
ub
seq
uen
tly
the
risk
like
liho
od
has
re
mai
ned
th
e sa
me.
Like
liho
od
2
01
/04
/202
1
Co
nse
qu
ence
3
3
C
on
seq
uen
ce
3
Ris
k Sc
ore
1
2
12
R
isk
Sco
re
6
Cau
se o
f R
isk
Agi
ng
pre
mis
es, r
eq
uir
ing
add
itio
nal
ser
vici
ng
and
re
pai
r.
Pre
mis
es
infr
astr
uct
ure
an
d la
you
t n
ot
effi
cien
t fo
r m
od
ern
hea
lth
care
nee
ds.
Pre
mis
es m
anag
ed a
nd
se
rvic
ed b
y th
ird
par
ty
lan
dlo
rds
and
no
t u
nd
er S
CFT
’s d
irec
t co
ntr
ol.
Soci
al d
ista
nci
ng
req
uir
emen
ts h
ave
limit
ed s
pac
e av
aila
ble
.
Imp
act:
Incr
ease
d d
eman
d o
n r
eso
urc
es t
o m
ain
tain
an
d im
pro
ve t
he
ove
rall
est
ate.
Incr
ease
d d
eman
d o
n c
apit
al f
or
inve
stin
g in
th
e fu
ture
su
stai
nab
ility
of
the
Tru
st.
No
t b
ein
g ab
le t
o s
up
po
rt e
ffec
tive
eff
icie
nt
serv
ices
may
lead
to
po
or
qu
alit
y p
atie
nt
ou
tco
mes
an
d p
atie
nt
exp
erie
nce
s.
Co
nst
rain
ed a
bili
ty t
o im
pro
ve p
rem
ises
en
viro
nm
ent
at p
ace
.
Co
nst
rain
ed a
bili
ty t
o e
ffec
t st
rate
gic
chan
ge a
nd
im
pro
vem
ents
to
bu
ildin
gs a
nd
en
viro
nm
ents
.
Dam
age
to t
he
Tru
st’s
rep
uta
tio
n.
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 25 of 300
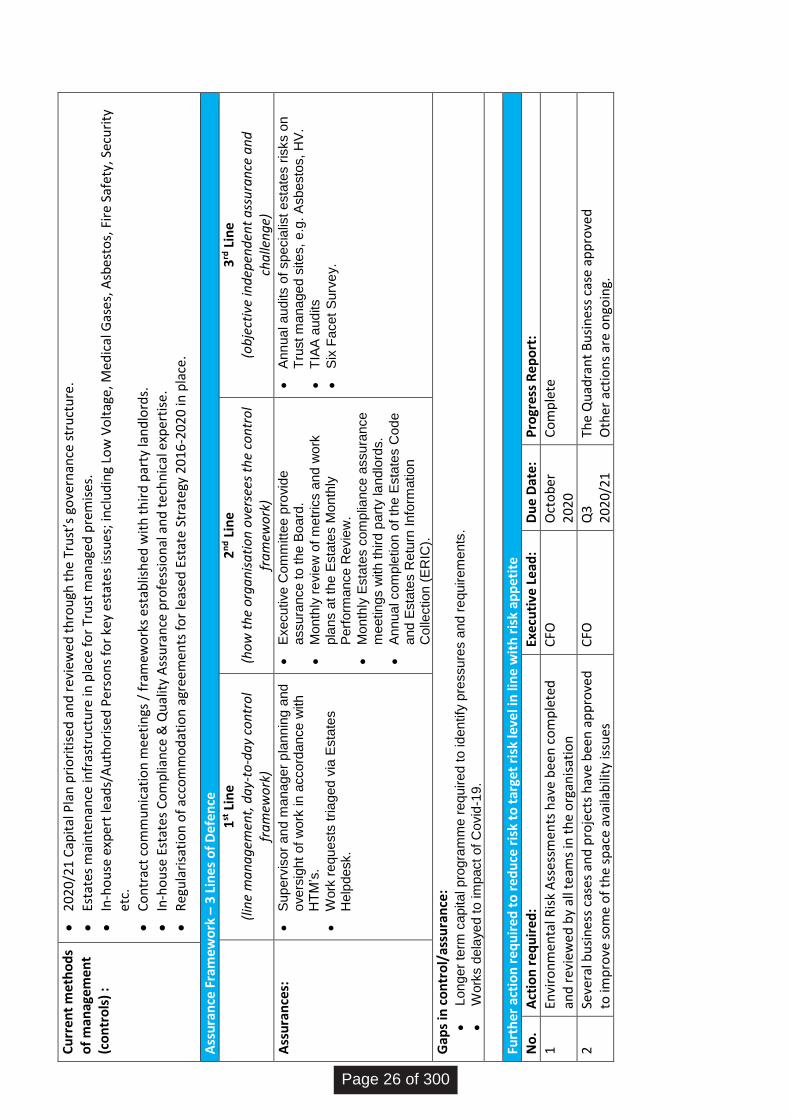
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
(co
ntr
ols
) :
202
0/21
Cap
ital
Pla
n p
rio
riti
sed
an
d r
evie
we
d t
hro
ugh
th
e Tr
ust
’s g
ove
rnan
ce s
tru
ctu
re.
Esta
tes
mai
nte
nan
ce in
fras
tru
ctu
re in
pla
ce f
or
Tru
st m
anag
ed p
rem
ises
.
In-h
ou
se e
xper
t le
ads/
Au
tho
rise
d P
erso
ns
for
key
est
ate
s is
sues
; in
clu
din
g Lo
w V
olt
age,
Med
ical
Gas
es, A
sbes
tos,
Fir
e Sa
fety
, Sec
uri
ty
etc.
Co
ntr
act
com
mu
nic
atio
n m
eeti
ngs
/ f
ram
ewo
rks
esta
blis
hed
wit
h t
hir
d p
arty
lan
dlo
rds.
In-h
ou
se E
stat
es C
om
plia
nce
& Q
ual
ity
Ass
ura
nce
pro
fess
ion
al a
nd
tec
hn
ical
exp
erti
se.
Reg
ula
risa
tio
n o
f ac
com
mo
dat
ion
agr
eem
ents
fo
r le
ased
Est
ate
Str
ate
gy 2
016
-202
0 in
pla
ce.
Ass
ura
nce
Fra
mew
ork
– 3
Lin
es o
f D
efe
nce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Su
pe
rvis
or
an
d m
ana
ge
r p
lann
ing a
nd
o
ve
rsig
ht
of
wo
rk in
acco
rda
nce
with
H
TM
’s.
Work
re
qu
ests
tria
ged
via
Esta
tes
He
lpd
esk.
Exe
cu
tive
Co
mm
itte
e p
rovid
e
assu
ran
ce
to
th
e B
oa
rd.
Mon
thly
re
vie
w o
f m
etr
ics a
nd
wo
rk
pla
ns a
t th
e E
sta
tes M
on
thly
P
erf
orm
ance
Revie
w.
Mon
thly
Esta
tes c
om
plia
nce
assu
ran
ce
m
eetin
gs w
ith
th
ird
pa
rty la
ndlo
rds.
An
nu
al co
mp
letio
n o
f th
e E
sta
tes C
od
e
and
Esta
tes R
etu
rn I
nfo
rmatio
n
Co
llectio
n (
ER
IC).
An
nu
al a
ud
its o
f sp
ecia
list
esta
tes r
isks o
n
Tru
st m
ana
ge
d s
ite
s,
e.g
. A
sb
esto
s,
HV
.
TIA
A a
ud
its
Six
Fa
ce
t S
urv
ey.
Gap
s in
co
ntr
ol/
assu
ran
ce:
Lon
ge
r te
rm c
apita
l p
rog
ram
me
re
quire
d t
o id
en
tify
pre
ssu
res a
nd
re
quir
em
ents
.
Work
s d
ela
ye
d t
o im
pact
of
Co
vid
-19
.
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
equ
ired
: Ex
ecu
tive
Le
ad:
Du
e D
ate:
P
rogr
ess
Re
po
rt:
1 En
viro
nm
enta
l Ris
k A
sses
smen
ts h
ave
bee
n c
om
ple
ted
an
d r
evie
we
d b
y al
l te
ams
in t
he
org
anis
atio
n
CFO
O
cto
ber
2
02
0
Co
mp
lete
2 Se
vera
l bu
sin
ess
case
s an
d p
roje
cts
hav
e b
een
ap
pro
ved
to
imp
rove
so
me
of
the
spac
e av
aila
bili
ty is
sues
C
FO
Q3
2
02
0/2
1
The
Qu
adra
nt
Bu
sin
ess
case
ap
pro
ved
O
ther
act
ion
s ar
e o
ngo
ing.
Page 26 of 300
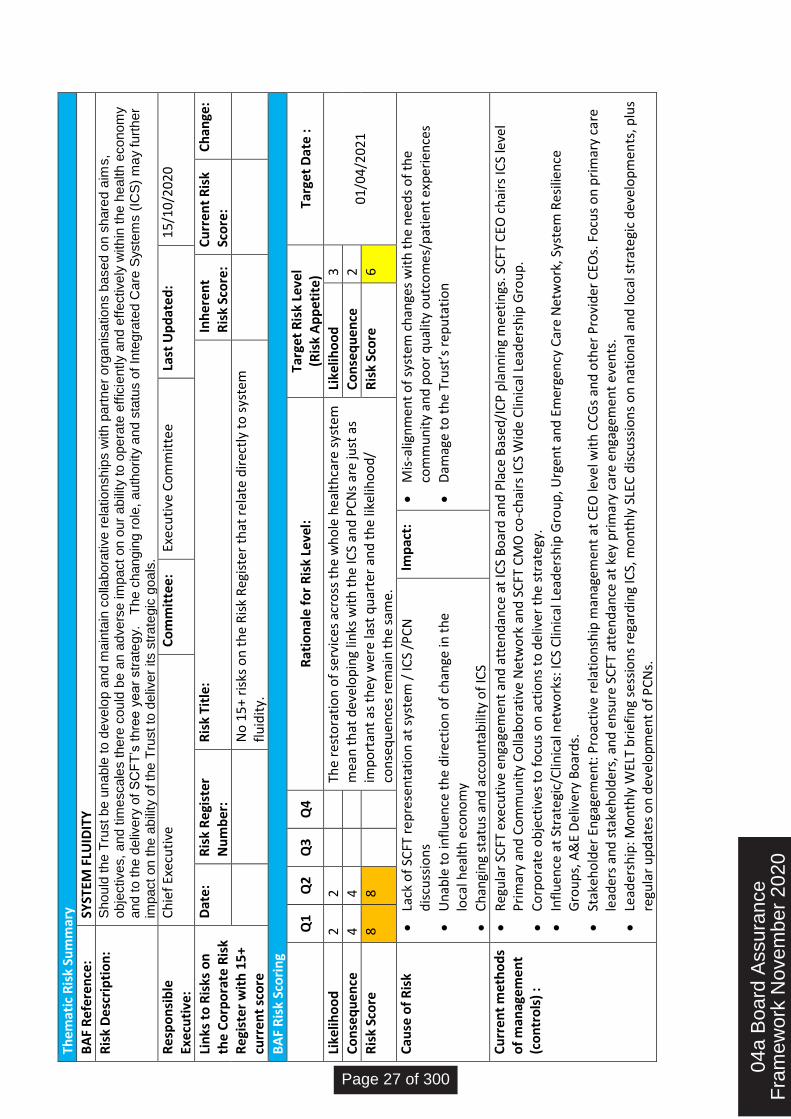
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
SYST
EM F
LUID
ITY
Ris
k D
esc
rip
tio
n:
Sh
ou
ld th
e T
rust
be
un
able
to d
eve
lop
an
d m
ain
tain
co
llab
ora
tive
re
latio
nsh
ips w
ith
pa
rtn
er
org
anis
atio
ns b
ase
d o
n s
hare
d a
ims,
obje
ctive
s,
an
d t
ime
sca
les t
he
re c
ou
ld b
e a
n a
dve
rse
im
pact
on
ou
r a
bili
ty t
o o
pe
rate
eff
icie
ntly a
nd
eff
ective
ly w
ith
in t
he h
ea
lth
eco
no
my
and t
o th
e d
eliv
ery
of
SC
FT
’s t
hre
e y
ea
r str
ate
gy.
T
he c
han
gin
g r
ole
, a
uth
ori
ty a
nd
sta
tus o
f In
tegra
ted C
are
Syste
ms (
ICS
) m
ay f
urt
he
r im
pact
on
th
e a
bili
ty o
f th
e T
rust
to d
eliv
er
its s
tra
teg
ic g
oa
ls.
Re
spo
nsi
ble
Ex
ecu
tive
: C
hie
f Ex
ecu
tive
C
om
mit
tee:
Ex
ecu
tive
Co
mm
itte
e
Last
Up
dat
ed
: 1
5/1
0/2
020
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egis
ter
Nu
mb
er:
Ris
k Ti
tle:
In
her
ent
Ris
k Sc
ore
: C
urr
ent
Ris
k Sc
ore
: C
han
ge:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to s
yste
m
flu
idit
y.
BA
F R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
2
2
Th
e re
sto
rati
on
of
serv
ices
acr
oss
th
e w
ho
le h
ealt
hca
re s
yste
m
mea
n t
hat
dev
elo
pin
g lin
ks w
ith
th
e IC
S an
d P
CN
s ar
e ju
st a
s im
po
rtan
t as
th
ey w
ere
last
qu
arte
r an
d t
he
likel
iho
od
/ co
nse
qu
ence
s re
mai
n t
he
sam
e.
Like
liho
od
3
01
/04
/202
1
Co
nse
qu
ence
4
4
C
on
seq
uen
ce
2
Ris
k Sc
ore
8
8
R
isk
Sco
re
6
Cau
se o
f R
isk
Lack
of
SCFT
rep
rese
nta
tio
n a
t sy
stem
/ IC
S /P
CN
d
iscu
ssio
ns
Un
able
to
infl
uen
ce t
he
dir
ecti
on
of
chan
ge in
th
e lo
cal h
ealt
h e
con
om
y
Ch
angi
ng
stat
us
and
acc
ou
nta
bili
ty o
f IC
S
Imp
act:
Mis
-alig
nm
ent
of
syst
em c
han
ges
wit
h t
he
nee
ds
of
the
com
mu
nit
y an
d p
oo
r q
ual
ity
ou
tco
mes
/pat
ien
t ex
per
ien
ces
Dam
age
to t
he
Tru
st’s
rep
uta
tio
n
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
(co
ntr
ols
) :
Reg
ula
r SC
FT e
xecu
tive
en
gage
men
t an
d a
tte
nd
ance
at
ICS
Bo
ard
an
d P
lace
Bas
ed/I
CP
pla
nn
ing
mee
tin
gs. S
CFT
CEO
ch
airs
ICS
leve
l P
rim
ary
and
Co
mm
un
ity
Co
llab
ora
tive
Net
wo
rk a
nd
SC
FT C
MO
co
-ch
airs
ICS
Wid
e C
linic
al L
ead
ersh
ip G
rou
p.
Co
rpo
rate
ob
ject
ives
to
fo
cus
on
act
ion
s to
del
iver
th
e st
rate
gy.
Infl
uen
ce a
t St
rate
gic/
Clin
ical
net
wo
rks:
ICS
Clin
ical
Lea
der
ship
Gro
up
, Urg
ent
and
Em
erge
ncy
Car
e N
etw
ork
, Sys
tem
Re
silie
nce
G
rou
ps,
A&
E D
eliv
ery
Bo
ard
s.
Stak
eho
lder
En
gage
men
t: P
roac
tive
rel
atio
nsh
ip m
anag
emen
t at
CEO
leve
l wit
h C
CG
s an
d o
ther
Pro
vid
er C
EOs.
Fo
cus
on
pri
mar
y ca
re
lead
ers
and
sta
keh
old
ers,
an
d e
nsu
re S
CFT
att
end
ance
at
key
pri
mar
y ca
re e
nga
gem
ent
even
ts.
Lead
ersh
ip: M
on
thly
WEL
T b
rief
ing
sess
ion
s re
gard
ing
ICS,
mo
nth
ly S
LEC
dis
cuss
ion
s o
n n
atio
nal
an
d lo
cal s
trat
egi
c d
evel
op
men
ts, p
lus
regu
lar
up
dat
es
on
dev
elo
pm
ent
of
PC
Ns.
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 27 of 300
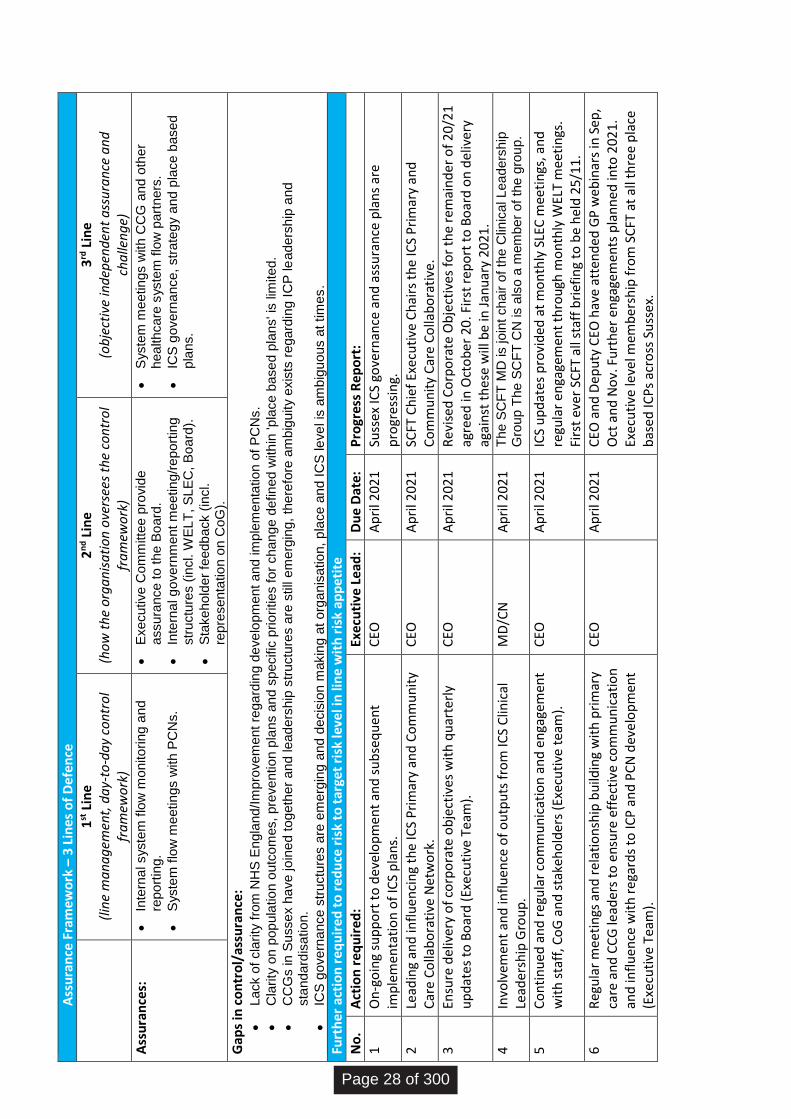
A
ssu
ran
ce F
ram
ewo
rk –
3 L
ines
of
De
fen
ce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Inte
rna
l syste
m flo
w m
onito
rin
g a
nd
repo
rtin
g.
Syste
m f
low
me
etin
gs w
ith
PC
Ns.
Exe
cu
tive
Co
mm
itte
e p
rovid
e
assu
ran
ce
to
th
e B
oa
rd.
Inte
rna
l g
ove
rnm
ent
me
etin
g/r
ep
ort
ing
str
uctu
res (
incl. W
EL
T,
SL
EC
, B
oa
rd).
Sta
ke
ho
lder
feed
ba
ck (
incl.
repre
se
nta
tio
n o
n C
oG
).
Syste
m m
eetin
gs w
ith
CC
G a
nd
oth
er
hea
lth
ca
re s
yste
m f
low
part
ners
.
ICS
go
ve
rna
nce
, str
ate
gy a
nd p
lace
base
d
pla
ns.
Gap
s in
co
ntr
ol/
assu
ran
ce:
Lack o
f cla
rity
fro
m N
HS
En
gla
nd
/Im
pro
ve
me
nt
reg
ard
ing
de
ve
lop
me
nt
an
d im
ple
me
nta
tio
n o
f P
CN
s.
Cla
rity
on p
op
ula
tio
n o
utc
om
es,
pre
ve
ntio
n p
lan
s a
nd
sp
ecific
prio
ritie
s f
or
ch
an
ge
de
fin
ed w
ith
in 'p
lace
base
d p
lans' i
s lim
ite
d.
CC
Gs in
Su
sse
x h
ave
jo
ine
d to
ge
the
r a
nd
le
ad
ers
hip
str
uctu
res a
re s
till
em
erg
ing,
the
refo
re a
mb
igu
ity e
xis
ts r
ega
rdin
g I
CP
le
ade
rsh
ip a
nd
sta
nd
ard
isa
tio
n.
ICS
go
ve
rna
nce
str
uctu
res a
re e
me
rgin
g a
nd
decis
ion m
akin
g a
t o
rga
nis
atio
n, p
lace
an
d I
CS
le
ve
l is
am
big
uo
us a
t tim
es
.
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
equ
ired
: Ex
ecu
tive
Le
ad:
Du
e D
ate:
P
rogr
ess
Re
po
rt:
1 O
n-g
oin
g su
pp
ort
to
dev
elo
pm
ent
and
su
bse
qu
ent
imp
lem
enta
tio
n o
f IC
S p
lan
s.
CEO
A
pri
l 202
1
Suss
ex IC
S go
vern
ance
an
d a
ssu
ran
ce p
lan
s ar
e p
rogr
essi
ng.
2 Le
adin
g an
d in
flu
enci
ng
the
ICS
Pri
mar
y an
d C
om
mu
nit
y C
are
Co
llab
ora
tive
Net
wo
rk.
CEO
A
pri
l 202
1
SCFT
Ch
ief
Exe
cuti
ve C
hai
rs t
he
ICS
Pri
mar
y an
d
Co
mm
un
ity
Car
e C
olla
bo
rati
ve.
3 En
sure
del
iver
y o
f co
rpo
rate
ob
ject
ives
wit
h q
uar
terl
y u
pd
ates
to
Bo
ard
(Ex
ecu
tive
Te
am).
C
EO
Ap
ril 2
021
R
evis
ed C
orp
ora
te O
bje
ctiv
es f
or
the
rem
ain
der
of
20/
21
ag
reed
in O
cto
ber
20
. Fir
st r
epo
rt t
o B
oar
d o
n d
eliv
ery
agai
nst
th
ese
will
be
in J
anu
ary
2021
.
4 In
volv
emen
t an
d in
flu
ence
of
ou
tpu
ts f
rom
ICS
Clin
ical
Le
ader
ship
Gro
up
. M
D/C
N
Ap
ril 2
021
T
he S
CF
T M
D is jo
int
ch
air o
f th
e C
linic
al L
ea
ders
hip
G
roup
Th
e S
CF
T C
N is a
lso
a m
em
ber
of
the
gro
up
.
5 C
on
tin
ued
an
d r
egu
lar
com
mu
nic
atio
n a
nd
en
gage
men
t w
ith
sta
ff, C
oG
an
d s
take
ho
lder
s (E
xecu
tive
tea
m).
C
EO
Ap
ril 2
021
IC
S u
pd
ates
pro
vid
ed a
t m
on
thly
SLE
C m
eeti
ngs
, an
d
regu
lar
en
gage
men
t th
rou
gh m
on
thly
WEL
T m
eeti
ngs
. Fi
rst
ever
SC
FT a
ll st
aff
bri
efin
g to
be
hel
d 2
5/1
1.
6 R
egu
lar
mee
tin
gs a
nd
rel
atio
nsh
ip b
uild
ing
wit
h p
rim
ary
care
an
d C
CG
lead
ers
to e
nsu
re e
ffec
tive
co
mm
un
icat
ion
an
d in
flu
ence
wit
h r
egar
ds
to IC
P a
nd
PC
N d
eve
lop
men
t (E
xecu
tive
Tea
m).
CEO
A
pri
l 202
1
CEO
an
d D
epu
ty C
EO h
ave
atte
nd
ed G
P w
eb
inar
s in
Sep
, O
ct a
nd
No
v. F
urt
her
en
gage
men
ts p
lan
ned
into
20
21
. Ex
ecu
tive
leve
l mem
ber
ship
fro
m S
CFT
at
all t
hre
e p
lace
b
ased
ICP
s ac
ross
Su
ssex
.
Page 28 of 300
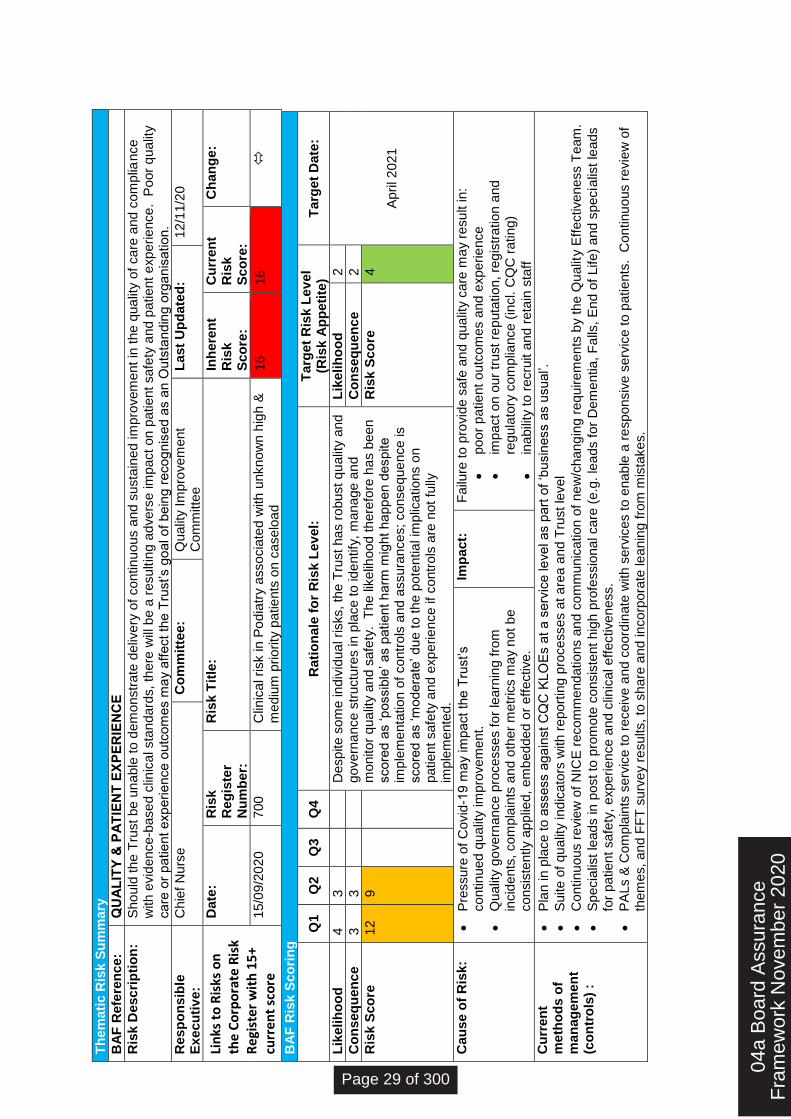
Th
em
ati
c R
isk S
um
ma
ry
BA
F R
efe
ren
ce
:
QU
AL
ITY
& P
AT
IEN
T E
XP
ER
IEN
CE
Ris
k D
esc
rip
tio
n:
S
ho
uld
th
e T
rust
be
un
able
to d
em
onstr
ate
deliv
ery
of
co
ntin
uou
s a
nd
su
sta
ined
im
pro
vem
ent
in t
he q
ua
lity o
f ca
re a
nd
co
mp
lian
ce
w
ith
evid
ence
-base
d c
linic
al sta
nd
ard
s,
the
re w
ill b
e a
re
su
ltin
g a
dve
rse
im
pact
on
patie
nt
sa
fety
an
d p
atie
nt
exp
erie
nce
. P
oor
qu
alit
y
ca
re o
r p
atie
nt e
xp
erie
nce
outc
om
es m
ay a
ffe
ct
the
Tru
st’s g
oa
l o
f b
ein
g r
eco
gn
ise
d a
s a
n O
uts
tan
din
g o
rga
nis
atio
n.
Re
sp
on
sib
le
Ex
ec
uti
ve
:
Ch
ief
Nu
rse
C
om
mit
tee:
Qu
alit
y I
mp
rove
ment
Co
mm
itte
e
La
st
Up
da
ted
: 1
2/1
1/2
0
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Da
te:
Ris
k
Re
gis
ter
Nu
mb
er:
Ris
k T
itle
: In
he
ren
t R
isk
Sc
ore
:
Cu
rre
nt
Ris
k
Sc
ore
:
Ch
an
ge
:
15/0
9/2
02
0
700
C
linic
al risk in
Po
dia
try a
sso
cia
ted
with
unkn
ow
n h
igh
&
me
diu
m p
rio
rity
pa
tie
nts
on
ca
se
loa
d
16
16
BA
F R
isk
Sc
ori
ng
Q
1
Q2
Q3
Q4
Ra
tio
na
le f
or
Ris
k L
ev
el:
T
arg
et
Ris
k L
ev
el
(R
isk A
pp
eti
te)
Ta
rge
t D
ate
:
Lik
eli
ho
od
4
3
De
sp
ite
so
me
in
div
idu
al ri
sks,
the
Tru
st
ha
s r
obu
st
qu
alit
y a
nd
g
ove
rna
nce
str
uctu
res in
pla
ce
to
id
en
tify
, m
ana
ge
an
d
mo
nito
r q
ua
lity a
nd s
afe
ty.
Th
e lik
elih
ood
th
ere
fore
ha
s b
ee
n
sco
red
as ‘p
ossib
le’ a
s p
atie
nt
ha
rm m
ight
ha
pp
en d
esp
ite
im
ple
me
nta
tio
n o
f co
ntr
ols
and
assu
ran
ce
s;
co
nse
qu
en
ce
is
sco
red
as ‘m
ode
rate
’ d
ue
to
th
e p
ote
ntia
l im
plic
atio
ns o
n
patie
nt
sa
fety
an
d e
xp
erie
nce
if
co
ntr
ols
are
not
fully
im
ple
me
nte
d.
Lik
eli
ho
od
2
Ap
ril 2
021
Co
ns
eq
ue
nc
e
3
3
Co
ns
eq
ue
nc
e
2
Ris
k S
co
re
12
9
Ris
k S
co
re
4
Ca
us
e o
f R
isk:
Pre
ssu
re o
f C
ovid
-19
ma
y im
pact
the
Tru
st’s
co
ntin
ued
qu
alit
y im
pro
ve
me
nt.
Qu
alit
y g
ove
rna
nce
pro
ce
sse
s f
or
learn
ing
fro
m
incid
ents
, co
mp
lain
ts a
nd
oth
er
me
tric
s m
ay n
ot b
e
co
nsis
tently a
pp
lied
, em
bed
de
d o
r e
ffe
ctive
.
Imp
act:
F
ailu
re t
o p
rovid
e s
afe
an
d q
ua
lity c
are
ma
y r
esu
lt in
:
poo
r p
atie
nt
outc
om
es a
nd
exp
erie
nce
imp
act
on
ou
r tr
ust
rep
uta
tio
n,
reg
istr
atio
n a
nd
re
gu
lato
ry c
om
plia
nce
(in
cl. C
QC
ra
tin
g)
ina
bili
ty t
o r
ecru
it a
nd
re
tain
sta
ff
Cu
rre
nt
me
tho
ds
of
ma
na
ge
me
nt
(co
ntr
ols
) :
Pla
n in
pla
ce
to
asse
ss a
ga
inst
CQ
C K
LO
Es a
t a
se
rvic
e le
ve
l a
s p
art
of
‘bu
sin
ess a
s u
su
al’.
Su
ite
of
qu
alit
y in
dic
ato
rs w
ith
re
port
ing p
roce
sse
s a
t a
rea a
nd
Tru
st
leve
l
Co
ntin
uo
us r
evie
w o
f N
ICE
re
co
mm
end
atio
ns a
nd
co
mm
unic
atio
n o
f n
ew
/ch
ang
ing r
eq
uire
me
nts
by t
he
Qu
alit
y E
ffe
ctive
ne
ss T
eam
.
Sp
ecia
list
lead
s in
post
to p
rom
ote
co
nsis
tent
hig
h p
rofe
ssio
na
l ca
re (
e.g
. le
ad
s f
or
De
me
ntia
, F
alls
, E
nd
of
Life
) a
nd s
pecia
list
lea
ds
for
pa
tie
nt
sa
fety
, e
xp
eri
en
ce
an
d c
linic
al e
ffe
ctive
ne
ss.
PA
Ls &
Co
mp
lain
ts s
erv
ice
to r
ece
ive
an
d c
oord
ina
te w
ith
se
rvic
es t
o e
nab
le a
re
sp
on
siv
e s
erv
ice
to
pa
tie
nts
. C
on
tin
uo
us r
evie
w o
f th
em
es,
an
d F
FT
su
rve
y r
esu
lts,
to s
ha
re a
nd in
co
rpo
rate
le
an
ing
fro
m m
ista
ke
s.
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 29 of 300
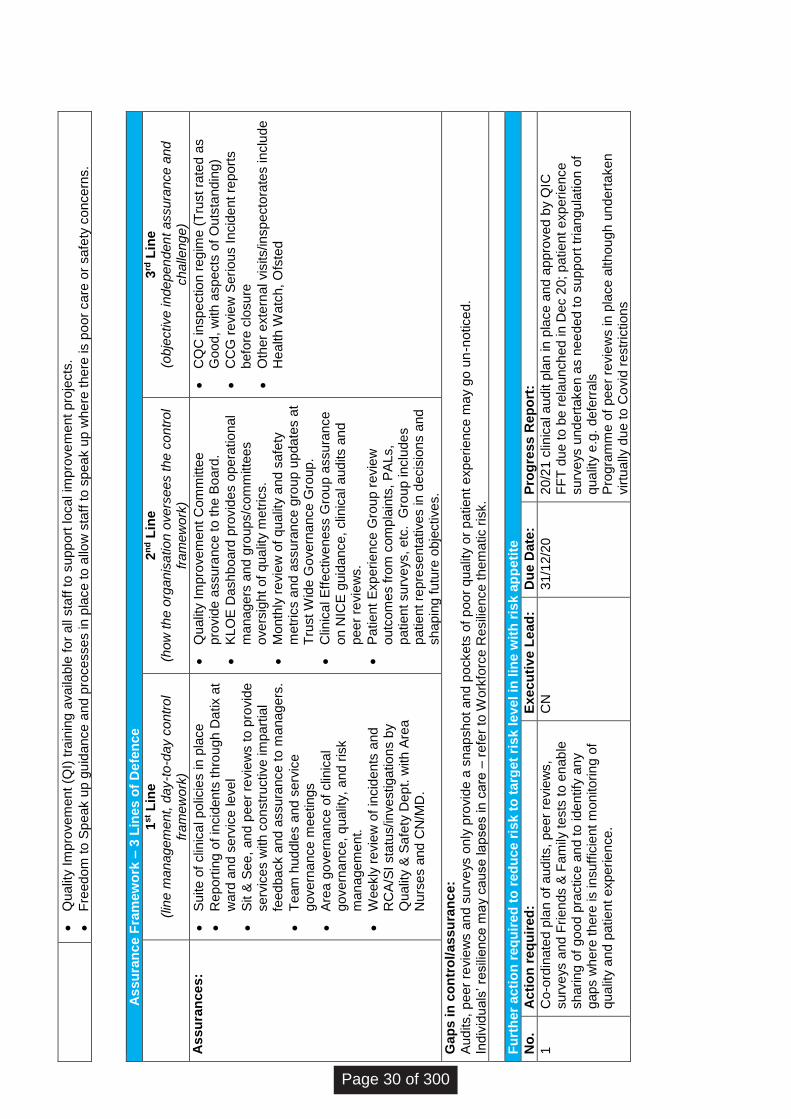
Qu
alit
y I
mp
rove
me
nt
(QI)
tra
inin
g a
va
ilab
le f
or
all
sta
ff to
su
pp
ort
lo
ca
l im
pro
ve
me
nt
pro
jects
.
Fre
ed
om
to S
pe
ak u
p g
uid
ance
an
d p
roce
sse
s in
pla
ce
to
allo
w s
taff
to s
pea
k u
p w
he
re t
here
is p
oo
r ca
re o
r sa
fety
co
nce
rns.
A
ss
ura
nc
e F
ram
ew
ork
– 3
Lin
es o
f D
efe
nc
e
1
st L
ine
(lin
e m
an
ag
em
ent,
day-t
o-d
ay c
ontr
ol
fra
me
wo
rk)
2n
d L
ine
(h
ow
th
e o
rga
nis
atio
n o
ve
rse
es t
he
co
ntr
ol
fra
me
wo
rk)
3rd
Lin
e
(obje
ctive
in
de
pen
den
t assu
ran
ce
an
d
ch
alle
ng
e)
As
su
ran
ce
s:
Su
ite
of
clin
ica
l p
olic
ies in
pla
ce
Re
port
ing
of
incid
en
ts t
hro
ug
h D
atix a
t w
ard
an
d s
erv
ice
le
ve
l
Sit &
Se
e,
an
d p
eer
revie
ws t
o p
rovid
e
se
rvic
es w
ith
co
nstr
uctive
im
part
ial
feed
ba
ck a
nd
assu
ran
ce
to
ma
na
ge
rs.
Te
am
hud
dle
s a
nd
se
rvic
e
gove
rna
nce
me
etin
gs
Are
a g
ove
rna
nce
of
clin
ica
l g
ove
rna
nce
, q
ualit
y,
an
d r
isk
ma
na
ge
me
nt.
Weekly
re
vie
w o
f in
cid
ents
and
R
CA
/SI
sta
tus/in
ve
stig
atio
ns b
y
Qu
alit
y &
Sa
fety
De
pt. w
ith
Are
a
Nu
rse
s a
nd
CN
/MD
.
Qu
alit
y I
mp
rove
me
nt
Co
mm
itte
e
pro
vid
e a
ssu
ran
ce
to
th
e B
oard
.
KL
OE
Da
sh
bo
ard
pro
vid
es o
pe
ratio
nal
ma
na
ge
rs a
nd
gro
ups/c
om
mitte
es
ove
rsig
ht
of
qua
lity m
etr
ics.
Mon
thly
re
vie
w o
f q
ua
lity a
nd s
afe
ty
me
tric
s a
nd
assu
ran
ce
gro
up u
pda
tes a
t T
rust W
ide G
ove
rna
nce
Gro
up
.
Clin
ica
l E
ffe
ctive
ness G
rou
p a
ssu
ran
ce
o
n N
ICE
gu
idan
ce
, clin
ica
l a
ud
its a
nd
p
ee
r re
vie
ws.
Pa
tie
nt
Exp
erie
nce
Gro
up
re
vie
w
outc
om
es f
rom
com
pla
ints
, P
AL
s,
patie
nt
su
rve
ys,
etc
. G
rou
p in
clu
de
s
patie
nt
rep
rese
nta
tive
s in
de
cis
ions a
nd
sh
ap
ing f
utu
re o
bje
ctive
s.
CQ
C in
sp
ectio
n r
eg
ime
(T
rust
rate
d a
s
Go
od
, w
ith
asp
ects
of
Ou
tsta
nd
ing)
CC
G r
evie
w S
eri
ous I
ncid
en
t re
po
rts
befo
re c
losu
re
Oth
er
exte
rna
l vis
its/in
sp
ecto
rate
s in
clu
de
He
alth
Wa
tch
, O
fste
d
Ga
ps
in
co
ntr
ol/
ass
ura
nc
e:
A
ud
its,
pe
er
revie
ws a
nd
su
rve
ys o
nly
pro
vid
e a
sn
ap
sh
ot
an
d p
ocke
ts o
f p
oo
r q
ualit
y o
r p
atie
nt
exp
eri
ence
ma
y g
o u
n-n
otice
d.
Indiv
idu
als
’ re
sili
ence
ma
y c
ause
la
pse
s in
ca
re –
re
fer
to W
ork
forc
e R
esili
ence
th
em
atic r
isk.
Fu
rth
er
ac
tio
n r
eq
uir
ed
to
re
du
ce
ris
k t
o t
arg
et
ris
k l
ev
el in
lin
e w
ith
ris
k a
pp
eti
te
No
. A
cti
on
re
qu
ire
d:
E
xe
cu
tiv
e L
ea
d:
D
ue
Date
:
Pro
gre
ss
Re
po
rt:
1
Co-o
rdin
ate
d p
lan
of
aud
its,
pe
er
revie
ws,
su
rve
ys a
nd
Fri
en
ds &
Fa
mily
tests
to
en
ab
le
sh
arin
g o
f g
oo
d p
ractice
an
d to
id
en
tify
an
y
gap
s w
he
re t
here
is in
su
ffic
ient
mo
nito
rin
g o
f q
ua
lity a
nd p
atie
nt
exp
eri
en
ce
.
CN
3
1/1
2/2
0
20/2
1 c
linic
al a
ud
it p
lan
in
pla
ce
and
ap
pro
ve
d b
y Q
IC
FF
T d
ue
to
be
re
laun
ch
ed in
Dec 2
0; p
atie
nt
exp
eri
ence
su
rve
ys u
nd
ert
ake
n a
s n
ee
ded
to
su
pp
ort
tri
ang
ula
tio
n o
f q
ua
lity e
.g.
defe
rra
ls
Pro
gra
mm
e o
f p
ee
r re
vie
ws in
pla
ce
alth
ou
gh u
nd
ert
ake
n
virtu
ally
du
e to
Co
vid
re
str
ictio
ns
Page 30 of 300
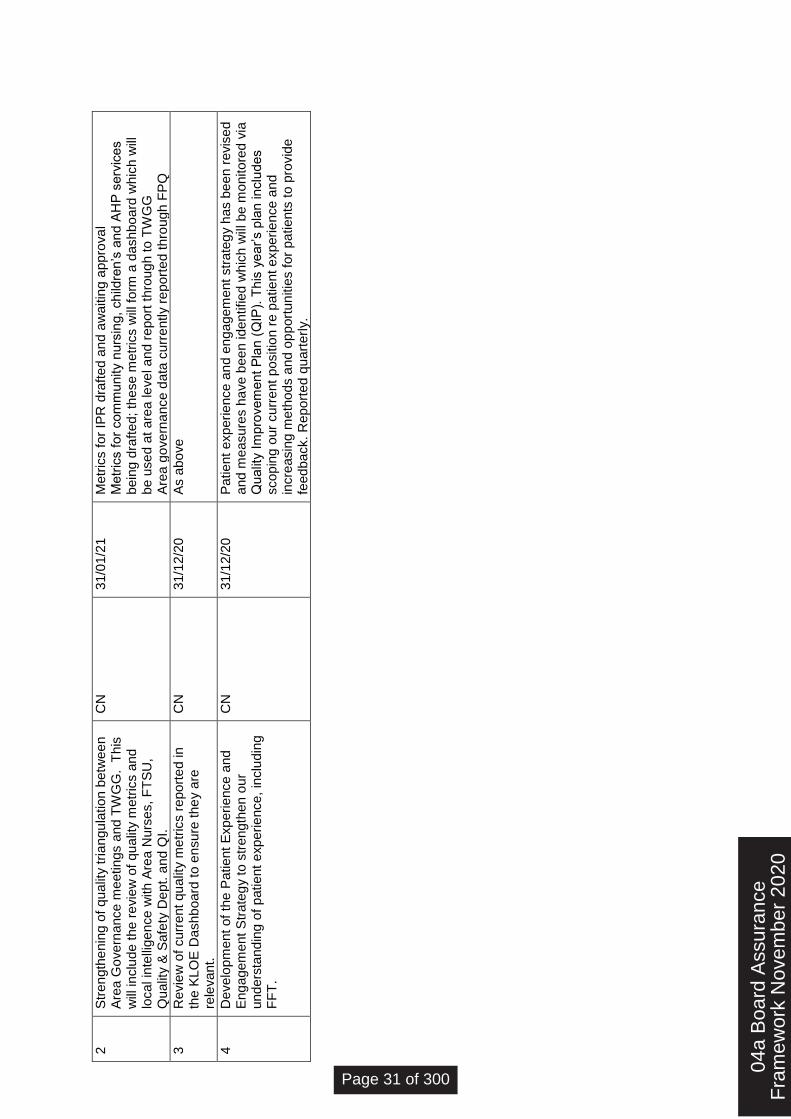
2
Str
en
gth
en
ing o
f q
ua
lity t
ria
ngu
latio
n b
etw
ee
n
Are
a G
ove
rna
nce
me
etin
gs a
nd
TW
GG
. T
his
w
ill in
clu
de t
he r
evie
w o
f q
ua
lity m
etr
ics a
nd
lo
ca
l in
telli
ge
nce
with
Are
a N
urs
es,
FT
SU
, Q
ualit
y &
Sa
fety
De
pt. a
nd Q
I.
CN
3
1/0
1/2
1
Metr
ics f
or
IPR
dra
fte
d a
nd
aw
aitin
g a
ppro
va
l M
etr
ics f
or
co
mm
unity n
urs
ing,
ch
ildre
n’s
and
AH
P s
erv
ice
s
bein
g d
raft
ed;
the
se
me
tric
s w
ill f
orm
a d
ash
bo
ard
wh
ich
will
b
e u
se
d a
t a
rea
le
ve
l a
nd r
epo
rt t
hro
ug
h to
TW
GG
A
rea g
ove
rna
nce
da
ta c
urr
ently r
ep
ort
ed
th
rou
gh
FP
Q
3
Re
vie
w o
f cu
rre
nt
qu
alit
y m
etr
ics r
epo
rte
d in
th
e K
LO
E D
ash
bo
ard
to
en
su
re t
he
y a
re
rele
va
nt.
CN
3
1/1
2/2
0
As a
bo
ve
4
De
ve
lop
me
nt
of
the
Pa
tie
nt
Exp
eri
ence
and
E
ng
age
me
nt
Str
ate
gy t
o s
tre
ng
then
our
und
ers
tan
din
g o
f p
atie
nt
exp
erie
nce
, in
clu
din
g
FF
T.
CN
3
1/1
2/2
0
Pa
tie
nt
exp
eri
ence
an
d e
ng
age
me
nt
str
ate
gy h
as b
ee
n r
evis
ed
a
nd
me
asu
res h
ave
be
en
id
en
tifie
d w
hic
h w
ill b
e m
onito
red
via
Q
ualit
y I
mp
rove
me
nt
Pla
n (
QIP
). T
his
ye
ar’s p
lan in
clu
des
sco
pin
g o
ur
cu
rre
nt
positio
n r
e p
atie
nt e
xp
erie
nce
an
d
incre
asin
g m
eth
ods a
nd o
pp
ort
un
itie
s f
or
pa
tie
nts
to
pro
vid
e
feed
ba
ck.
Re
po
rte
d q
ua
rte
rly.
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 31 of 300
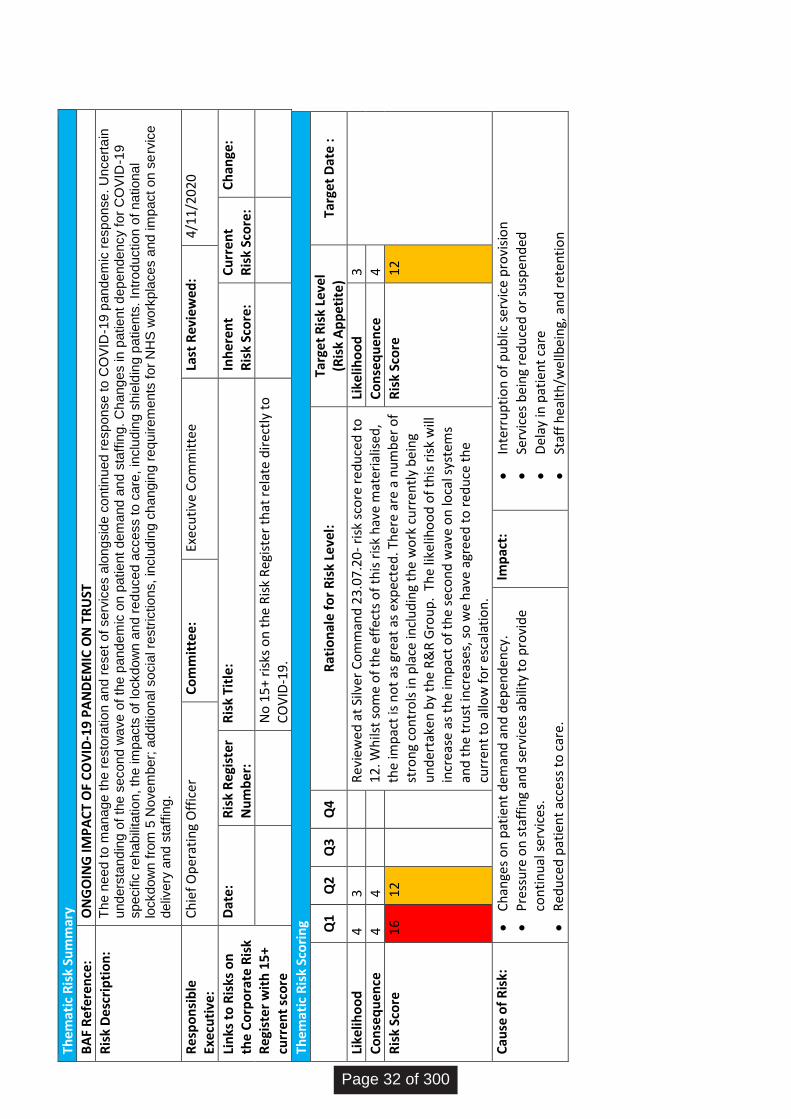
The
mat
ic R
isk
Sum
mar
y
BA
F R
efe
ren
ce:
ON
GO
ING
IMP
AC
T O
F C
OV
ID-1
9 P
AN
DEM
IC O
N T
RU
ST
Ris
k D
esc
rip
tio
n:
Th
e n
ee
d t
o m
ana
ge
th
e r
esto
ratio
n a
nd
re
se
t o
f se
rvic
es a
lon
gsid
e c
ontin
ued
re
sp
on
se
to
CO
VID
-19 p
and
em
ic r
esp
on
se
. U
nce
rta
in
und
ers
tan
din
g o
f th
e s
eco
nd
wa
ve
of
the
pa
nd
em
ic o
n p
atie
nt
dem
and
an
d s
taff
ing.
Ch
ang
es in
patie
nt d
epe
nde
ncy f
or
CO
VID
-19
sp
ecific
re
ha
bili
tatio
n, th
e im
pacts
of
lockd
ow
n a
nd r
ed
uce
d a
cce
ss t
o c
are
, in
clu
din
g s
hie
ldin
g p
atie
nts
. In
tro
ductio
n o
f n
atio
na
l lo
ckd
ow
n f
rom
5 N
ove
mb
er;
ad
ditio
na
l so
cia
l re
str
ictio
ns,
inclu
din
g c
ha
ng
ing
re
qu
ire
me
nts
fo
r N
HS
wo
rkp
lace
s a
nd
im
pact
on
se
rvic
e
deliv
ery
and
sta
ffin
g.
Re
spo
nsi
ble
Ex
ecu
tive
: C
hie
f O
per
atin
g O
ffic
er
Co
mm
itte
e:
Exe
cuti
ve C
om
mit
tee
La
st R
evie
wed
: 4
/11/
2020
Lin
ks t
o R
isks
on
th
e C
orp
ora
te R
isk
Re
gist
er
wit
h 1
5+
curr
ent
sco
re
Dat
e:
Ris
k R
egi
ster
N
um
ber
: R
isk
Titl
e:
Inh
eren
t R
isk
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
ange
:
No
15
+ ri
sks
on
th
e R
isk
Reg
iste
r th
at r
ela
te d
irec
tly
to
CO
VID
-19
.
The
mat
ic R
isk
Sco
rin
g
Q
1 Q
2 Q
3 Q
4 R
atio
nal
e f
or
Ris
k Le
vel:
Ta
rget
Ris
k Le
vel
(Ris
k A
pp
etit
e)
Targ
et D
ate
:
Like
liho
od
4
3
R
evie
wed
at
Silv
er C
om
man
d 2
3.0
7.2
0-
risk
sco
re r
ed
uce
d t
o
12
. Wh
ilst
som
e o
f th
e ef
fect
s o
f th
is r
isk
hav
e m
ater
ialis
ed,
the
imp
act
is n
ot
as g
reat
as
exp
ecte
d. T
her
e ar
e a
nu
mb
er o
f st
ron
g co
ntr
ols
in p
lace
incl
ud
ing
the
wo
rk c
urr
entl
y b
ein
g u
nd
erta
ken
by
the
R&
R G
rou
p.
The
likel
iho
od
of
this
ris
k w
ill
incr
ease
as
the
imp
act
of
the
seco
nd
wav
e o
n lo
cal s
yste
ms
and
th
e tr
ust
incr
ease
s, s
o w
e h
ave
agre
ed
to
red
uce
th
e cu
rren
t to
allo
w f
or
esc
alat
ion
.
Like
liho
od
3
Co
nse
qu
ence
4
4
C
on
seq
uen
ce
4
Ris
k Sc
ore
1
6
12
R
isk
Sco
re
12
Cau
se o
f R
isk:
Ch
ange
s o
n p
atie
nt
dem
and
an
d d
epen
den
cy.
Pre
ssu
re o
n s
taff
ing
and
ser
vice
s ab
ility
to
pro
vid
e co
nti
nu
al s
ervi
ces.
Red
uce
d p
atie
nt
acce
ss t
o c
are
.
Imp
act:
Inte
rru
pti
on
of
pu
blic
ser
vice
pro
visi
on
Serv
ices
bei
ng
red
uce
d o
r su
spen
ded
Del
ay in
pat
ien
t ca
re
Staf
f h
ealt
h/w
ellb
ein
g, a
nd
ret
en
tio
n
Page 32 of 300
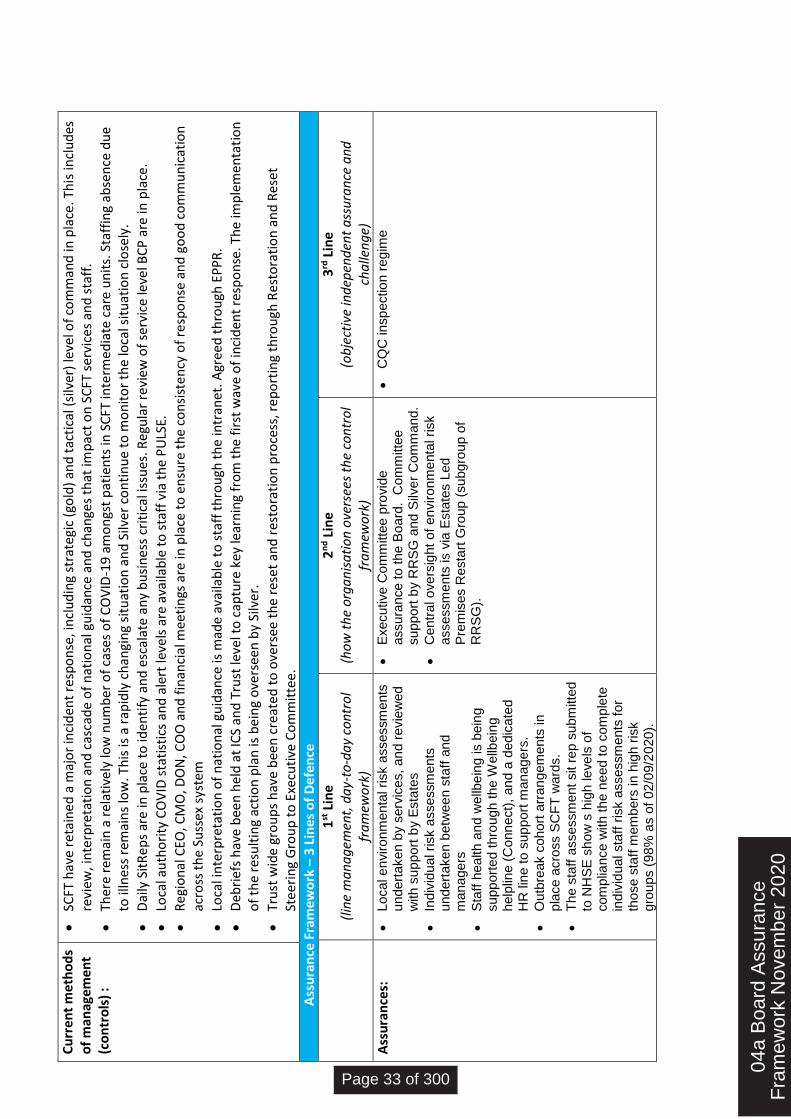
Cu
rren
t m
eth
od
s o
f m
anag
eme
nt
(co
ntr
ols
) :
SCFT
hav
e re
tain
ed a
maj
or
inci
den
t re
spo
nse
, in
clu
din
g st
rate
gic
(go
ld)
and
tac
tica
l (si
lver
) le
vel o
f co
mm
and
in p
lace
. Th
is in
clu
des
re
view
, in
terp
reta
tio
n a
nd
cas
cad
e o
f n
atio
nal
gu
idan
ce a
nd
ch
ange
s th
at im
pac
t o
n S
CFT
se
rvic
es a
nd
sta
ff.
Ther
e re
mai
n a
rel
ativ
ely
low
nu
mb
er o
f ca
ses
of
CO
VID
-19
am
on
gst
pat
ien
ts in
SC
FT in
term
edia
te c
are
un
its.
Sta
ffin
g ab
sen
ce d
ue
to il
lnes
s re
mai
ns
low
. Th
is is
a r
apid
ly c
han
gin
g si
tuat
ion
an
d S
ilver
co
nti
nu
e to
mo
nit
or
the
loca
l sit
uat
ion
clo
sely
.
Dai
ly S
itR
ep
s ar
e in
pla
ce t
o id
enti
fy a
nd
esc
alat
e an
y b
usi
nes
s cr
itic
al is
sues
. Reg
ula
r re
view
of
serv
ice
leve
l BC
P a
re in
pla
ce.
Loca
l au
tho
rity
CO
VID
sta
tist
ics
and
ale
rt le
vels
are
ava
ilab
le t
o s
taff
via
th
e P
ULS
E.
Reg
ion
al C
EO, C
MO
, DO
N, C
OO
an
d f
inan
cial
mee
tin
gs a
re in
pla
ce t
o e
nsu
re t
he
con
sist
en
cy o
f re
spo
nse
an
d g
oo
d c
om
mu
nic
atio
n
acro
ss t
he
Suss
ex s
yste
m
Loca
l in
terp
reta
tio
n o
f n
atio
nal
gu
idan
ce is
mad
e av
aila
ble
to
sta
ff t
hro
ugh
th
e in
tran
et. A
gree
d t
hro
ugh
EP
PR
.
Deb
rief
s h
ave
bee
n h
eld
at
ICS
and
Tru
st le
vel t
o c
aptu
re k
ey le
arn
ing
fro
m t
he
firs
t w
ave
of
inci
den
t re
spo
nse
. Th
e im
ple
men
tati
on
o
f th
e re
sult
ing
acti
on
pla
n is
bei
ng
ove
rsee
n b
y Si
lver
.
Tru
st w
ide
gro
up
s h
ave
bee
n c
reat
ed
to
ove
rsee
th
e re
set
and
re
sto
rati
on
pro
cess
, re
po
rtin
g th
rou
gh R
est
ora
tio
n a
nd
Res
et
Stee
rin
g G
rou
p t
o E
xecu
tive
Co
mm
itte
e.
A
ssu
ran
ce F
ram
ewo
rk –
3 L
ines
of
De
fen
ce
1
st L
ine
(lin
e m
an
ag
emen
t, d
ay-
to-d
ay
con
tro
l fr
am
ewo
rk)
2n
d L
ine
(ho
w t
he
org
an
isa
tio
n o
vers
ees
the
con
tro
l fr
am
ewo
rk)
3rd
Lin
e (o
bje
ctiv
e in
dep
end
ent
ass
ura
nce
an
d
cha
llen
ge)
Ass
ura
nce
s:
Lo
ca
l e
nviro
nm
enta
l risk a
sse
ssm
ents
u
nd
ert
ake
n b
y s
erv
ice
s,
an
d r
evie
we
d
with
su
ppo
rt b
y E
sta
tes
Indiv
idu
al ri
sk a
sse
ssm
ents
u
nd
ert
ake
n b
etw
ee
n s
taff
an
d
ma
na
ge
rs
Sta
ff h
ea
lth
an
d w
ellb
ein
g is b
ein
g
su
pp
ort
ed
th
rou
gh
the
We
llbein
g
help
line (
Co
nn
ect)
, an
d a
de
dic
ate
d
HR
lin
e t
o s
up
port
ma
na
ge
rs.
Ou
tbre
ak c
oho
rt a
rra
ng
em
ents
in
p
lace
acro
ss S
CF
T w
ard
s.
Th
e s
taff
asse
ssm
ent
sit r
ep
su
bm
itte
d
to N
HS
E s
ho
w s
hig
h le
ve
ls o
f com
plia
nce
with
th
e n
eed
to
co
mp
lete
in
div
idu
al sta
ff r
isk a
sse
ssm
ents
fo
r th
ose
sta
ff m
em
bers
in
hig
h r
isk
gro
up
s (
98
% a
s o
f 0
2/0
9/2
020
).
Exe
cu
tive
Co
mm
itte
e p
rovid
e
assu
ran
ce
to
th
e B
oa
rd.
Co
mm
itte
e
su
pp
ort
by R
RS
G a
nd
Silv
er
Co
mm
and
.
Ce
ntr
al o
ve
rsig
ht
of
en
viro
nm
enta
l risk
asse
ssm
ents
is v
ia E
sta
tes L
ed
P
rem
ise
s R
esta
rt G
roup
(su
bg
rou
p o
f R
RS
G).
CQ
C in
sp
ectio
n r
eg
ime
04a
Boa
rd A
ssur
ance
Fra
mew
ork
Nov
embe
r 20
20
Page 33 of 300

Gap
s in
co
ntr
ol/
assu
ran
ce:
On
go
ing c
ha
ng
es in
natio
na
l g
uid
an
ce
an
d u
nkn
ow
n im
pact
of
natio
na
l lo
ckd
ow
n r
estr
ictio
ns in
re
sp
onse
to
an
y in
cre
asin
g in
num
bers
.
On
go
ing r
isk o
f o
utb
rea
ks w
ith
in S
CF
T s
erv
ice
s/
an
d w
ith
in s
taff
gro
ups/t
ea
ms w
hic
h c
ou
ld r
esu
lt in
lo
ca
lise
d B
C in
cid
en
ts. L
ack o
f re
sili
ence
in
Tru
st's
VP
N
infr
astr
uctu
re.
Ga
p in
un
de
rsta
nd
ing
of
inte
rna
l tr
igg
ers
fo
r e
sca
latin
g th
e e
me
rge
ncy r
esp
on
se
in
th
e c
ase
of
a s
eco
nd
wa
ve
or
ad
ditio
na
l w
inte
r p
ressu
res.
N
atio
na
l a
nd r
eg
ion
al ch
alle
ng
es in
th
e a
va
ilab
ility
of
CO
VID
te
sts
.
Furt
her
act
ion
req
uir
ed t
o r
edu
ce r
isk
to t
arge
t ri
sk le
vel i
n li
ne
wit
h r
isk
app
etit
e
No
. A
ctio
n r
equ
ired
: Ex
ecu
tive
Le
ad:
Du
e D
ate:
P
rogr
ess
Re
po
rt:
1 Si
lve
r re
view
of
trig
gers
fo
r an
esc
alat
ed
em
erge
ncy
res
po
nse
. C
hie
f O
per
atin
g O
ffic
er
31
/3/2
021
S
up
ers
ede
d b
y r
etu
rn t
o n
atio
na
l L
eve
l 4
in
cid
ent
resp
on
se
.
Page 34 of 300
Page 1 of 4 Version 1.2 (Updated 2 Nov 2020)
Board Assurance Framework (BAF) Guide The BAF informs the Board about risks to the Trust’s Strategic goals and the new BAF template consists of two sections
the BAF Summary, showing the link between all the thematic risks and the Trust’s Strategic Goals; and
an overview of each thematic risk, providing further detail on the risk scoring, control methods, levels of assurance, relevant risks from the Risk Register, rationale for the current risk level, and a status update on any further actions. There are currently 7 thematic risks on the Trust’s Risk Register.
This guide includes the following table, on the key stages leading up to the presentation of the BAF, and information on how the BAF template is populated.
Key steps in the production of the BAF document
Updating the Thematic Risks
Each of the Thematic Risks has an Executive Director ‘Responsible Owner’.
The live records of the Thematic Risks are maintained on Datix and these will be reviewed and updated by the Responsible Owner as/when required.
These will then be monitored and reported on in monthly risk reports, through the normal governance/assurance reporting to the Executive Committee.
Links to Risk Register
Live risks are identified and evaluated as per the Trust’s Risk Management Policy and reported through Trust Wide Governance Group (TWGG) to Executive Committee (EC) for assurance to the Board. Feedback from TWGG/EC will enable the Risk team to have the most relevant up to date knowledge to ensure that the operational risks relevant to each thematic risk are included on the BAF.
Inputting onto the BAF template
The Risk team provide updates from the thematic risks and ‘Links to the Risk Register’ to the Trust Secretary (owner of the BAF).
Oversight of BAF before review at Executive/Board level
Each thematic risk is individually reviewed by the applicable oversight Committee (i.e. as identified on the BAF Summary).
The BAF document will be reviewed in its entirety, for the purposes of quality control and consistency checking at the Risk Oversight Group (ROG).
The Executive Committee will also review the BAF prior to presentation at Public Board meetings.
Quarterly presentation at Board meeting
The BAF is presented at the Trust’s Public Board meetings quarterly to provide assurance to the Board about the management of risks to the Trust’s achievement of its Strategic Goals.
04b
BA
F g
uide
Page 35 of 300
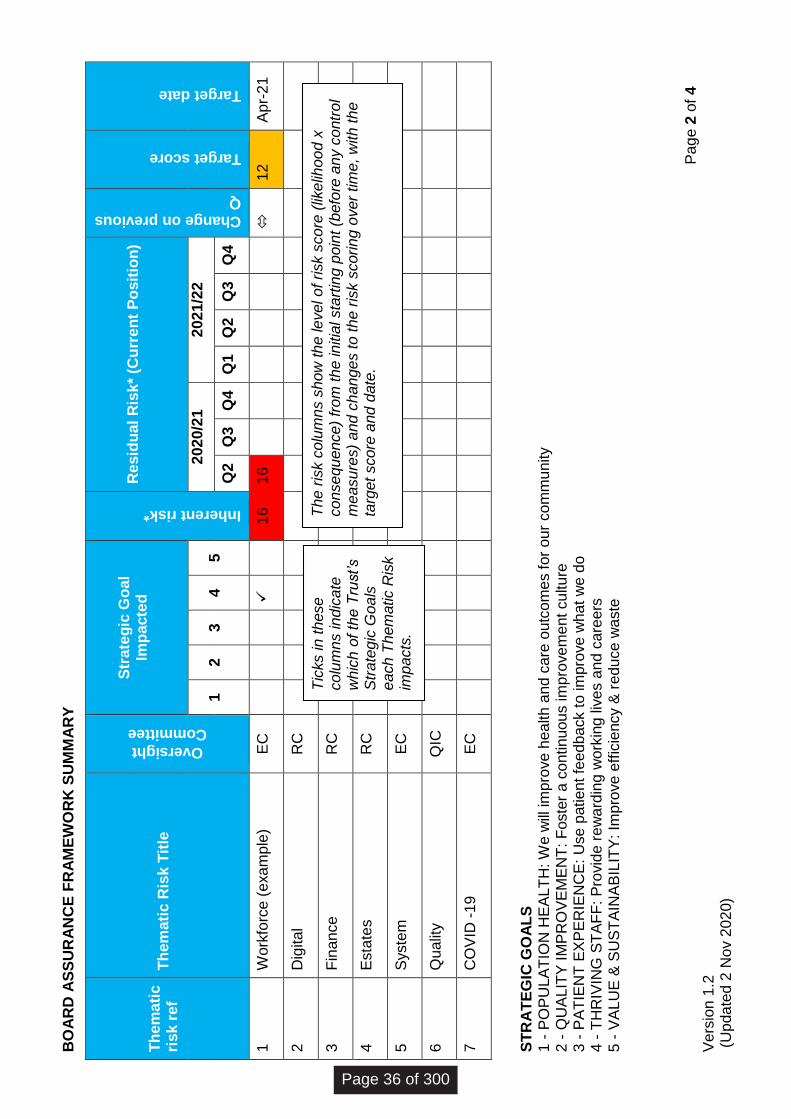
Pag
e 2
of
4
Vers
ion 1
.2
(U
pdate
d 2
Nov 2
020)
BO
AR
D A
SS
UR
AN
CE
FR
AM
EW
OR
K S
UM
MA
RY
Th
em
ati
c
risk r
ef
Th
em
ati
c R
isk T
itle
Oversight
Committee
Str
ate
gic
Go
al
Imp
acte
d
Inherent risk*
Resid
ual
Ris
k*
(Cu
rren
t P
osit
ion
)
Change on previous
Q
Target score
Target date
1
2
3
4
5
2020/2
1
2021/2
2
Q2
Q3
Q4
Q1
Q2
Q3
Q4
1
Work
forc
e (
exam
ple
) E
C
16
16
12
Apr-
21
2
Dig
ital
RC
3
Fin
ance
RC
4
Esta
tes
RC
5
Syste
m
EC
6
Qualit
y
QIC
7
CO
VID
-19
EC
ST
RA
TE
GIC
GO
AL
S
1 -
PO
PU
LA
TIO
N H
EA
LT
H: W
e w
ill im
pro
ve h
ealth a
nd c
are
outc
om
es f
or
our
com
munity
2 -
QU
ALIT
Y I
MP
RO
VE
ME
NT
: F
oste
r a c
ontinuous im
pro
vem
ent culture
3 -
PA
TIE
NT
EX
PE
RIE
NC
E:
Use p
atient fe
edback t
o im
pro
ve w
hat
we d
o
4 -
TH
RIV
ING
ST
AF
F: P
rovid
e r
ew
ard
ing
work
ing liv
es a
nd c
are
ers
5 -
VA
LU
E &
SU
ST
AIN
AB
ILIT
Y: Im
pro
ve e
ffic
iency &
reduce w
aste
Tic
ks in t
hese
colu
mn
s indic
ate
w
hic
h o
f th
e T
rust’s
Str
ate
gic
Goals
each T
hem
atic R
isk
impacts
.
The r
isk c
olu
mns s
how
the level of risk s
core
(lik
elih
ood x
consequence)
from
the initia
l sta
rtin
g p
oin
t (b
efo
re a
ny c
ontr
ol
measure
s)
and c
hanges to the r
isk s
coring o
ver
tim
e, w
ith the
targ
et
score
and d
ate
.
Page 36 of 300
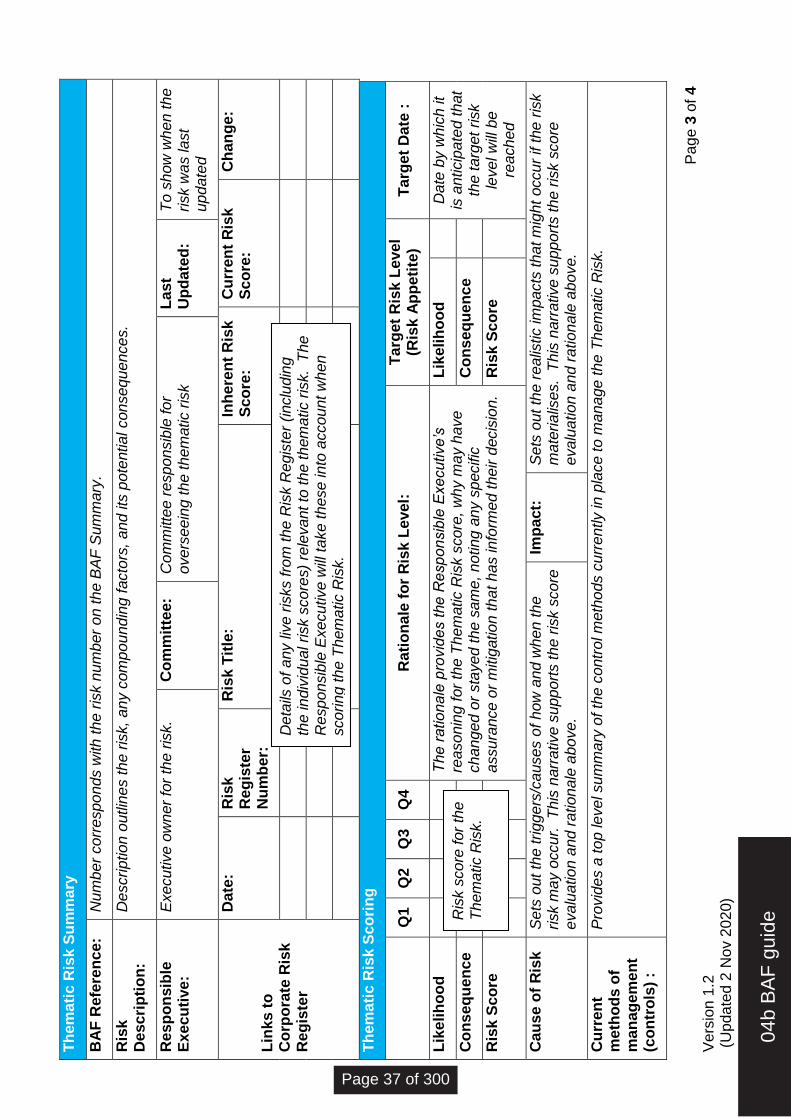
Pag
e 3
of
4
Vers
ion 1
.2
(U
pdate
d 2
Nov 2
020)
Th
em
ati
c R
isk S
um
mary
BA
F R
efe
ren
ce:
N
um
ber
corr
esponds w
ith t
he r
isk n
um
ber
on t
he B
AF
Sum
mary
.
Ris
k
Descri
pti
on
:
Description o
utlin
es t
he r
isk,
any c
om
poundin
g f
acto
rs,
and its
pote
ntial consequences.
Resp
on
sib
le
Execu
tive:
E
xecutive o
wner
for
the r
isk.
Co
mm
itte
e:
Com
mitte
e r
esponsib
le for
overs
eein
g the them
atic r
isk
Last
Up
date
d:
To s
how
when the
risk w
as last
update
d
Lin
ks t
o
Co
rpo
rate
Ris
k
Reg
iste
r
Date
: R
isk
Reg
iste
r N
um
ber:
Ris
k T
itle
: In
here
nt
Ris
k
Sco
re:
Cu
rren
t R
isk
Sco
re:
Ch
an
ge:
Th
em
ati
c R
isk S
co
rin
g
Q
1
Q2
Q3
Q4
Rati
on
ale
fo
r R
isk L
evel:
T
arg
et
Ris
k L
evel
(R
isk A
pp
eti
te)
Targ
et
Date
:
Lik
elih
oo
d
The r
ationale
pro
vid
es the R
esponsib
le E
xecutive’s
re
asonin
g f
or
the T
hem
atic R
isk s
core
, w
hy m
ay h
ave
changed o
r sta
yed the s
am
e, noting a
ny s
pecific
assura
nce o
r m
itig
ation that
has info
rmed t
heir d
ecis
ion.
Lik
elih
oo
d
D
ate
by w
hic
h it
is a
nticip
ate
d that
the targ
et risk
level w
ill b
e
reached
Co
nseq
uen
ce
Co
nseq
uen
ce
Ris
k S
co
re
Ris
k S
co
re
Cau
se o
f R
isk
Sets
out th
e triggers
/causes o
f how
and w
hen the
risk m
ay o
ccur.
T
his
narr
ative s
upport
s the r
isk s
core
evalu
ation a
nd r
ationale
above.
Imp
act:
S
ets
out th
e r
ealis
tic im
pacts
that m
ight
occur
if t
he r
isk
mate
rialis
es. T
his
narr
ative s
upport
s the r
isk s
core
evalu
ation a
nd r
ationale
above.
Cu
rren
t m
eth
od
s o
f m
an
ag
em
en
t (c
on
tro
ls)
:
Pro
vid
es a
top level sum
mary
of th
e c
ontr
ol m
eth
ods c
urr
ently in p
lace to m
anage the T
hem
atic R
isk.
Deta
ils o
f any liv
e r
isks fro
m the R
isk R
egis
ter
(inclu
din
g
the indiv
idual risk s
core
s)
rele
vant to
the t
hem
atic r
isk. T
he
Responsib
le E
xecutive w
ill t
ake t
hese into
account w
hen
scoring the T
hem
atic R
isk.
Ris
k s
core
for
the
Them
atic R
isk.
04b
BA
F g
uide
Page 37 of 300
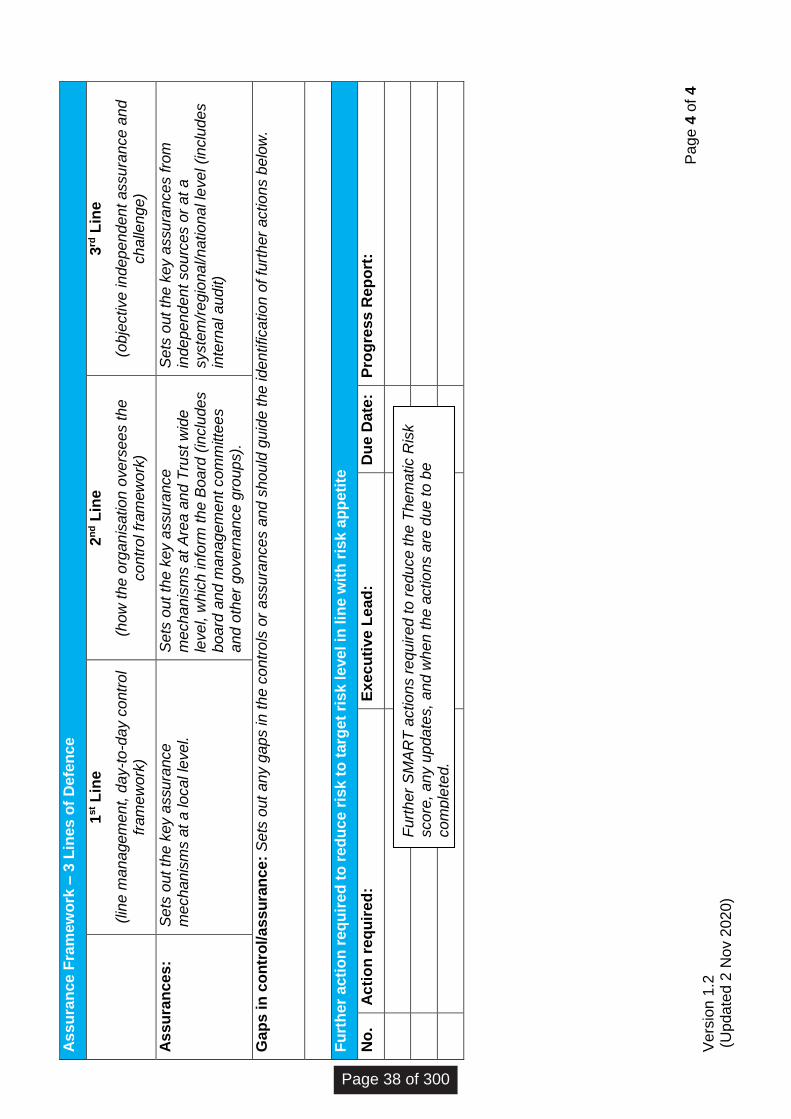
Pag
e 4
of
4
Vers
ion 1
.2
(U
pdate
d 2
Nov 2
020)
As
su
ran
ce F
ram
ew
ork
– 3
Lin
es o
f D
efe
nce
1
st L
ine
(lin
e m
anagem
ent, d
ay-t
o-d
ay c
ontr
ol
fram
ew
ork
)
2n
d L
ine
(how
the o
rganis
ation o
vers
ees the
contr
ol fr
am
ew
ork
)
3rd
Lin
e
(obje
ctive independent assura
nce a
nd
challe
nge)
As
su
ran
ces:
S
ets
out th
e k
ey a
ssura
nce
m
echanis
ms a
t a local le
vel.
Sets
out th
e k
ey a
ssura
nce
m
echanis
ms a
t A
rea a
nd T
rust w
ide
level, w
hic
h info
rm t
he B
oard
(in
clu
des
board
and m
anagem
ent com
mitte
es
and o
ther
govern
ance g
roups).
Sets
out th
e k
ey a
ssura
nces fro
m
independent
sourc
es o
r at
a
syste
m/r
egio
nal/national le
vel (inclu
des
inte
rnal audit)
Gap
s in
co
ntr
ol/
assu
ran
ce:
Sets
out
any g
aps in t
he c
ontr
ols
or
assura
nce
s a
nd s
hould
guid
e the identification o
f fu
rther
actions b
elo
w.
Fu
rth
er
acti
on
req
uir
ed
to
red
uce r
isk t
o t
arg
et
risk l
evel in
lin
e w
ith
ris
k a
pp
eti
te
No
. A
cti
on
req
uir
ed
:
Execu
tive L
ead
:
Du
e D
ate
:
Pro
gre
ss R
ep
ort
:
Furt
her
SM
AR
T a
ctions r
equired t
o r
educe the T
hem
atic R
isk
score
, any u
pdate
s,
and w
hen the a
ctions a
re d
ue t
o b
e
com
ple
ted.
Page 38 of 300
TRUST BOARD 26 November 2020
Agenda Item Number:
Report Title: SCFT Integrated Performance Report (IPR) - Month 06 (September 2020) Reported November 2020
Purpose:
Approval Assurance Discussion Briefing x
Summary: The Board approved the Integrated Performance Report (IPR) format at the October 2020 Board Meeting following detailed discussions. The IPR sets out details of the Trust’s performance using a balanced scorecard covering key metrics for each topic (Quality, Operational Performance, Workforce and Finance). The IPR Balanced Scorecard includes narrative for each topic area focused on identified adverse exceptions only. Each section also has a ‘spotlight’ slide providing additional narrative for each area focusing on key developments.
Recommendation:
The Board is asked to:
Note current operational performance
Discuss areas of exception for M06 (September data) specifically:
Operational Performance: Adverse Variation and Favourable Assurance: MT102 RTT referral to treatment waiting time incomplete pathways less than 18 weeks Adverse Variation and Favourable Assurance: MT031 Diagnostic Waits < 6 weeks Workforce: Favourable Variation and Adverse Assurance: MT429 Total Staff in Post Finance: Favourable Variation and Adverse Assurance: MT514 BPP (%)
Note current operational performance risks are for the present month M08
(November)
Previously reviewed by: Relevant Executive Directors
05 IP
R F
ront
shee
t v3
2011
20
Page 39 of 300
Relevance to Trust’s Strategic Goals: Relevant to all Trust Strategic Goals
Relevance to CQC Domains: Relevant to all CQC domains
Equality and Diversity: An equality impact assessment has been carried out and no impacts identified
Report author: Ceri Davies Deputy Director of Strategic Planning and Performance Ed Rothery Director of Finance and Performance Performance Team Executive Directors for each section
Report owner: Mike Jennings Chief Financial Officer
Page 40 of 300

Inte
grat
ed
Pe
rfo
rman
ce R
ep
ort
Mo
nth
06
Se
pte
mb
er
20
20
(re
po
rte
d N
ove
mb
er
20
20
)
Mik
e Je
nn
ings
Ch
ief
Fin
anci
al O
ffic
er a
nd
D
epu
ty C
hie
f Ex
ecu
tive
05 IP
R_2
021_
M06
_fin
al
Page 41 of 300
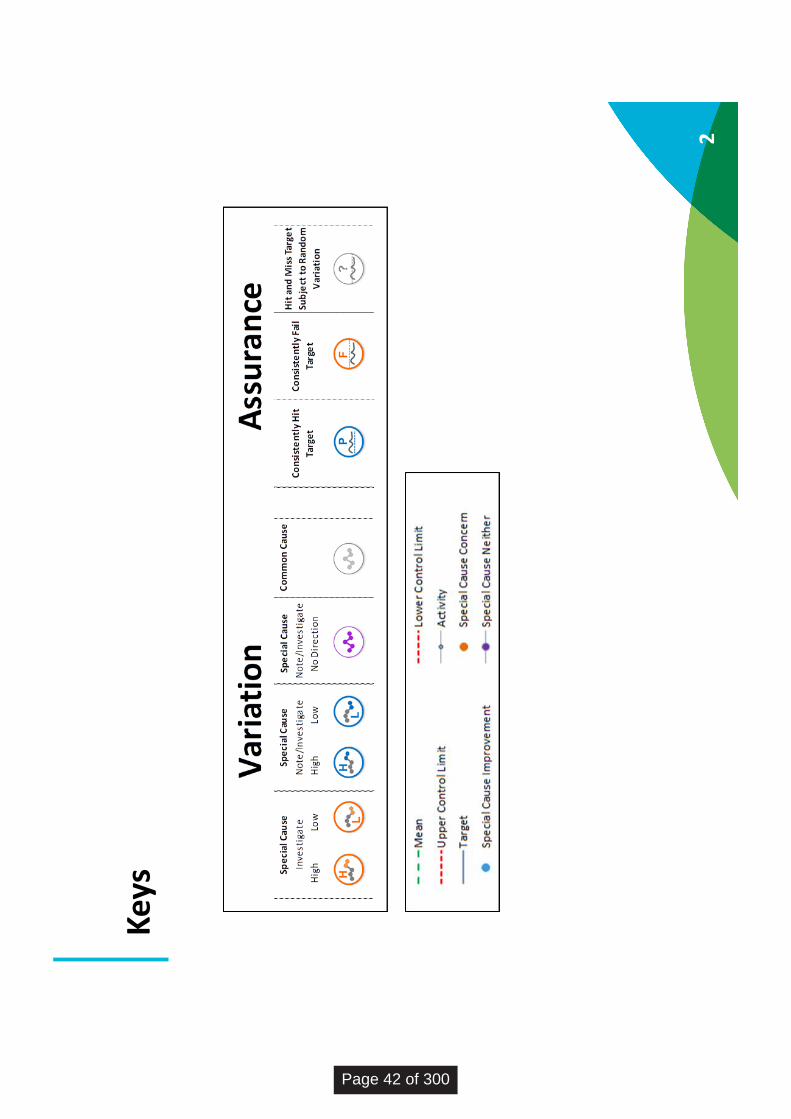
Key
s
2
Page 42 of 300
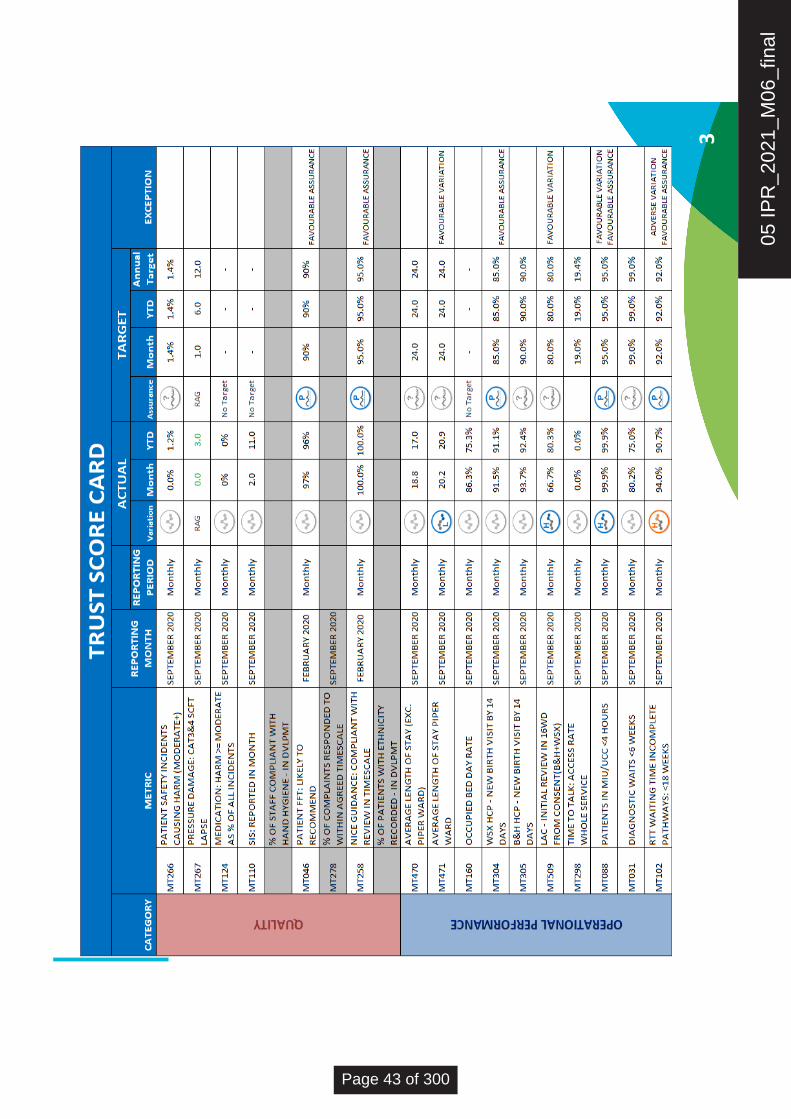
3
05 IP
R_2
021_
M06
_fin
al
Page 43 of 300
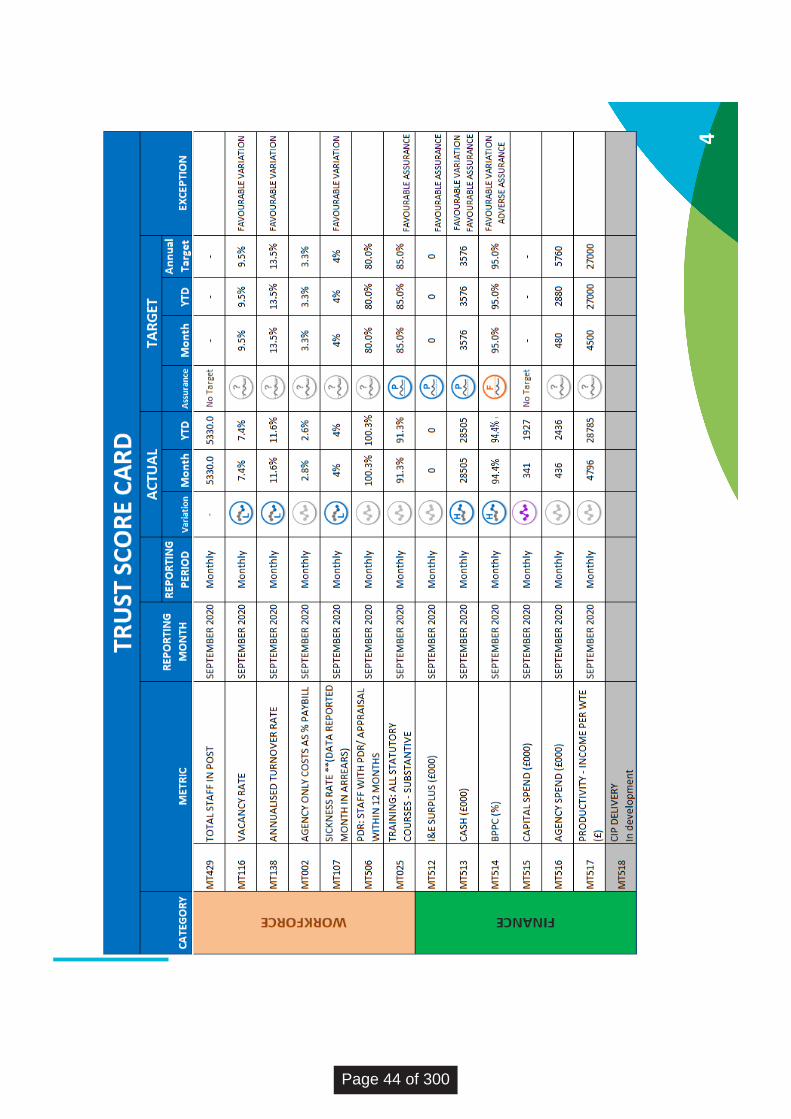
4
Page 44 of 300

Qu
alit
y R
ep
ort
5
05 IP
R_2
021_
M06
_fin
al
Page 45 of 300
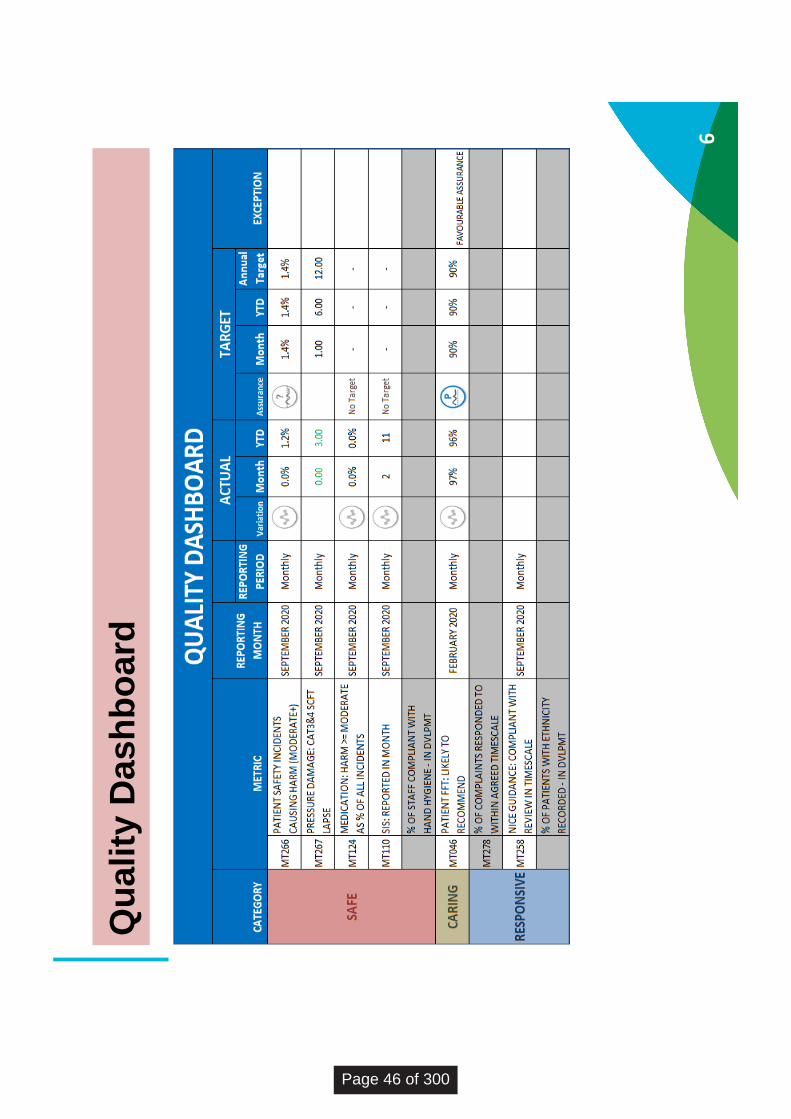
6
Qu
ality
Dash
bo
ard
Page 46 of 300
7
Qu
ality
Ex
ce
pti
on
Rep
ort
No
ad
vers
e ex
cep
tio
ns
to r
epo
rt
05 IP
R_2
021_
M06
_fin
al
Page 47 of 300

8
Qu
ality
Sp
otl
igh
t R
ep
ort
Follo
win
g d
iscussio
n a
t th
e B
oard
, an a
ction w
as t
aken to a
mend the Q
ualit
y m
etr
ics p
resente
d
in the IP
R P
roto
type a
nd these w
ere
pre
sente
d to the Q
ualit
y Im
pro
vem
ent C
om
mitte
e (
QIC
) on
19
thN
ovem
ber
for
dis
cussio
n a
nd a
ppro
val.
The Q
IC h
as r
equeste
d the follo
win
g c
hanges:
MT
258 N
ICE
Guid
ance: C
om
plia
nt w
ith R
evie
w in T
imescale
s s
hould
be m
oved fro
m the
responsiv
e to the e
ffective d
om
ain
% o
f patients
with e
thnic
ity r
ecord
ed (
metr
ic in d
evelo
pm
ent should
be m
oved fro
m r
esponsiv
e
to w
ell
led
% o
f S
taff C
om
plia
nt w
ith H
and H
ygie
ne (
metr
ic in d
evelo
pm
ent)
was d
iscussed a
nd it w
as
agre
ed it w
ill r
em
ain
in the s
afe
dom
ain
These c
hanges w
ill b
e a
ctioned for
the n
ext re
port
ing r
ound
Page 48 of 300

Op
era
tio
nal
P
erf
orm
ance
Re
po
rt
9
05 IP
R_2
021_
M06
_fin
al
Page 49 of 300
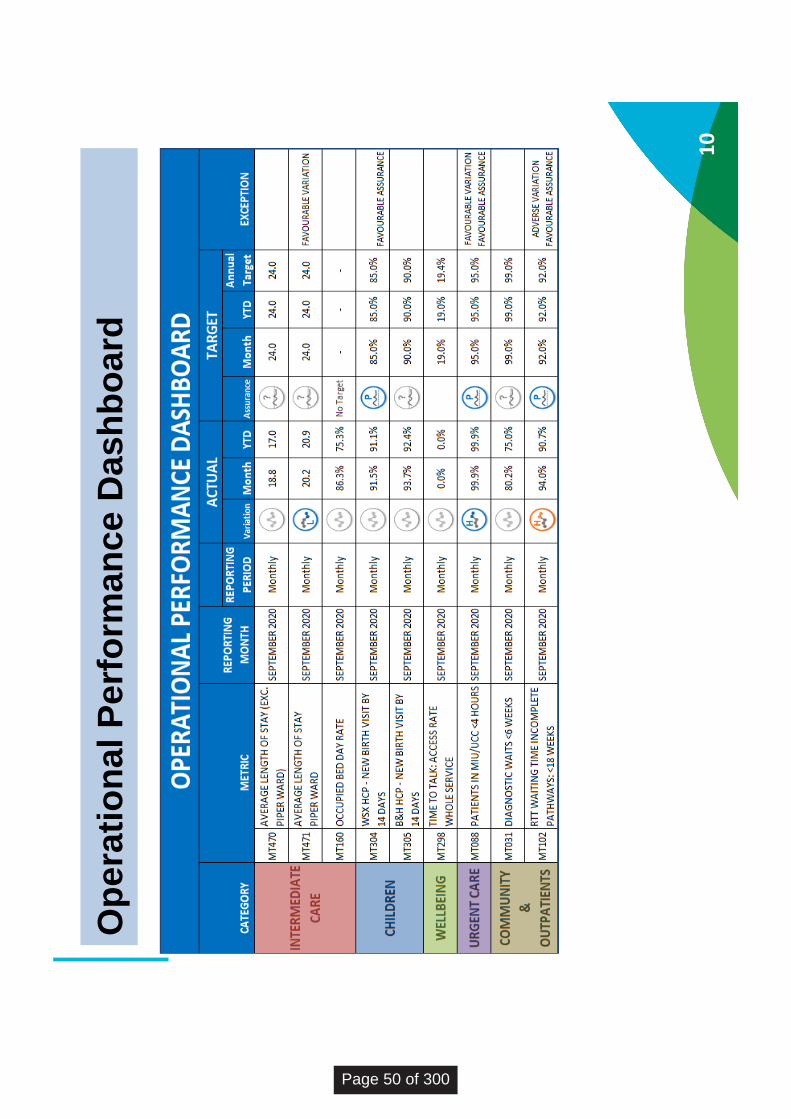
10
Op
era
tio
na
l P
erf
orm
an
ce
Dash
bo
ard
Page 50 of 300
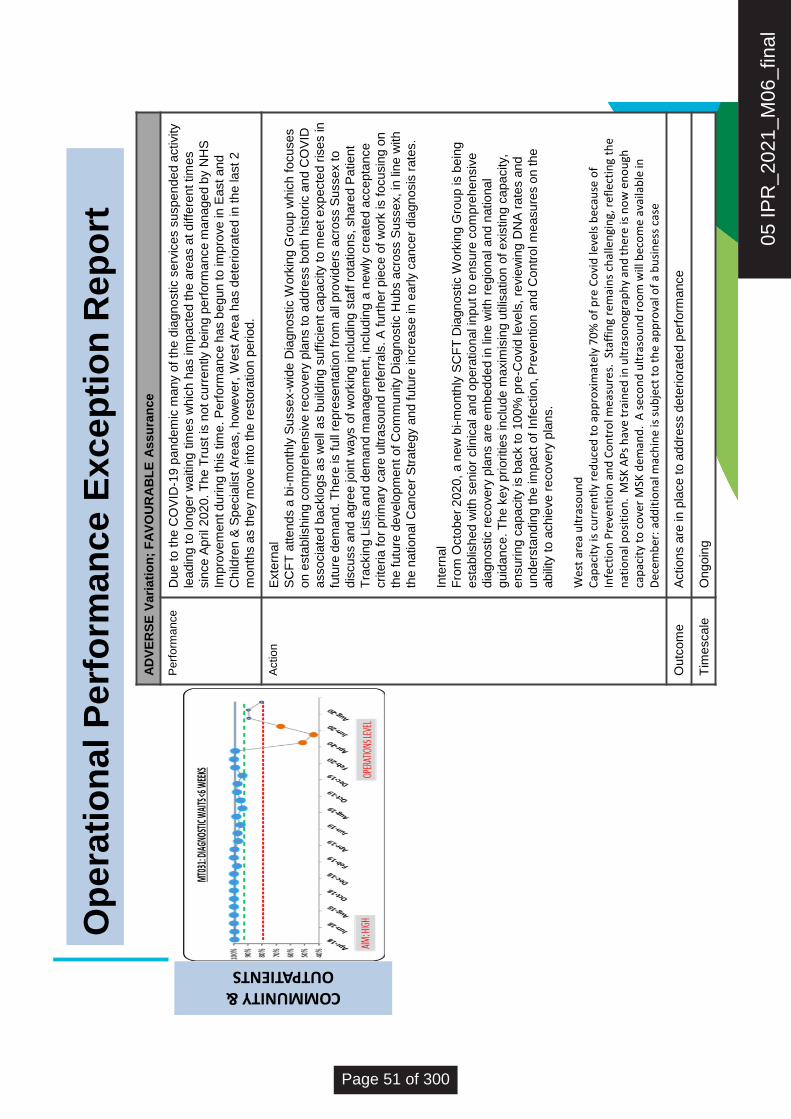
11
Op
era
tio
na
l P
erf
orm
an
ce
Exce
pti
on
Re
po
rtCOMMUNITY & OUTPATIENTS
AD
VE
RS
E V
ari
ati
on
; F
AV
OU
RA
BL
EA
ssu
ran
ce
Pe
rfo
rma
nce
Du
e to
th
e C
OV
ID-1
9 p
andem
ic m
any o
f th
e d
iagnostic s
erv
ices s
uspended a
ctivity
lead
ing t
o lo
ng
er
wa
itin
g t
ime
s w
hic
h h
as im
pacte
d th
e a
rea
s a
t d
iffe
ren
t tim
es
sin
ce
Ap
ril 2
02
0. T
he T
rust is
not cu
rre
ntly b
ein
g p
erf
orm
ance
ma
na
ge
d b
y N
HS
Imp
rove
me
nt d
urin
g t
his
tim
e. P
erf
orm
ance
has b
eg
un
to
im
pro
ve
in
Ea
st a
nd
Ch
ildre
n &
Sp
ecia
list
Are
as, h
ow
eve
r, W
est A
rea h
as d
ete
rio
rate
d in
th
e la
st
2
month
s a
s they
move into
the r
esto
ration p
eriod.
Actio
nE
xte
rna
l
SC
FT
atte
nd
s a
bi-
mo
nth
ly S
usse
x-w
ide D
iagn
ostic W
ork
ing G
roup
wh
ich
fo
cu
se
s
on e
sta
blis
hin
g c
om
pre
he
nsiv
e r
eco
ve
ry p
lans t
o a
dd
ress b
oth
his
toric a
nd
CO
VID
asso
cia
ted
backlo
gs a
s w
ell
as b
uild
ing s
uff
icie
nt ca
pa
city
to m
eet e
xp
ecte
d r
ise
s in
futu
re d
em
and
. T
here
is f
ull
repre
se
nta
tio
n fro
m a
ll p
rovid
ers
acro
ss S
usse
x to
dis
cu
ss a
nd
agre
e jo
int w
ays
of w
ork
ing in
clu
din
g s
taff
ro
tatio
ns, sh
are
d P
atie
nt
Tra
ckin
g L
ists
and
de
ma
nd
ma
na
ge
me
nt,
inclu
din
g a
ne
wly
cre
ate
d a
cce
pta
nce
crite
ria
fo
r p
rim
ary
ca
re u
ltra
so
un
d r
efe
rra
ls. A
fu
rth
er
pie
ce
of w
ork
is f
ocu
sin
g o
n
the fu
ture
deve
lopm
ent o
f C
om
mu
nity
Dia
gn
ostic H
ub
s a
cro
ss S
usse
x, in
lin
e w
ith
the n
atio
na
l C
an
ce
r S
tra
teg
y a
nd
fu
ture
in
cre
ase
in
early c
ance
r d
iagn
osis
ra
tes.
Inte
rna
l
Fro
m O
cto
be
r 2
02
0,
a n
ew
bi-
mo
nth
ly S
CF
T D
iagn
ostic W
ork
ing G
roup
is b
ein
g
esta
blis
hed
with
se
nio
r clin
ica
l a
nd
op
era
tio
na
l in
pu
t to
ensu
re c
om
pre
he
nsiv
e
dia
gn
ostic r
eco
ve
ry p
lans a
re e
mb
ed
de
d in
lin
e w
ith
re
gio
na
l a
nd
natio
na
l
guid
an
ce
. T
he k
ey
prioritie
s in
clu
de
ma
xim
isin
gu
tilis
atio
n o
f e
xis
tin
g c
apa
city,
ensu
ring
ca
pa
city
is b
ack to
100
% p
re-C
ovid
leve
ls,
revie
win
g D
NA
ra
tes a
nd
und
ers
tand
ing th
e im
pact o
f In
fectio
n, P
reve
ntio
n a
nd
Co
ntr
ol m
easu
res o
n t
he
abili
ty t
o a
ch
ieve
re
co
ve
ry p
lans.
Wes
t ar
ea u
ltra
sou
nd
C
apac
ity
is c
urr
entl
y re
du
ced
to
ap
pro
xim
atel
y 7
0%
of
pre
Co
vid
leve
ls b
ecau
se o
f In
fect
ion
Pre
ven
tio
n a
nd
Co
ntr
ol m
easu
res.
Staf
fin
g re
mai
ns
chal
len
gin
g, r
efle
ctin
g th
e n
atio
nal
po
siti
on
. M
SK A
Ps
hav
e tr
ain
ed in
ult
raso
no
grap
hy
and
th
ere
is n
ow
en
ou
gh
cap
acit
y to
co
ver
MSK
dem
and
. A
sec
on
d u
ltra
sou
nd
ro
om
will
bec
om
e av
aila
ble
in
Dec
emb
er:
add
itio
nal
mac
hin
e is
su
bje
ct t
o t
he
app
rova
l of
a b
usi
nes
s ca
se
Ou
tco
me
Actio
ns a
re in
pla
ce
to
add
ress d
ete
rio
rate
d p
erf
orm
ance
Tim
esca
leO
ngo
ing
05 IP
R_2
021_
M06
_fin
al
Page 51 of 300

12
Op
era
tio
na
l P
erf
orm
an
ce
Exce
pti
on
Re
po
rtCOMMUNITY & OUTPATIENTS
AD
VE
RS
E V
ari
ati
on
; F
AV
OU
RA
BL
EA
ssu
ran
ce
Pe
rfo
rma
nce
Du
e to
th
e C
OV
ID-1
9p
an
de
mic
ma
ny o
utp
atie
nt se
rvic
es s
usp
en
de
d a
ctivity le
ad
ing
to
lon
ge
r w
ait t
ime
s in
so
me
se
rvic
es. T
he
Tru
st
is n
ot cu
rre
ntly b
ein
g p
erf
orm
an
ce m
an
ag
ed
by N
HS
Im
pro
ve
me
nt d
uri
ng
th
is tim
e. P
erf
orm
an
ce
is im
pro
vin
g m
on
th o
n m
on
th fo
llow
ing
the
re
sto
ratio
n p
eri
od
.
Actio
n•
De
nta
l S
erv
ice
s:T
he
re w
as n
o a
cce
ss to
pro
ce
du
res th
at re
qu
ire
d g
en
era
l a
na
esth
esia
(GA
) d
uri
ng
wa
ve
on
e o
f th
e p
an
de
mic
an
d a
cce
ss r
em
ain
s lim
ite
d, a
lth
ou
gh
imp
rovin
g.
SC
FT
are
wo
rkin
g w
ith
th
e in
de
pe
nd
en
t se
cto
r to
in
cre
ase
acce
ss to
GA
slo
ts a
nd
ne
igh
bo
uri
ng A
cu
te T
rusts
ha
ve
co
mm
itte
d to
pro
vid
ing
in
cre
ase
d a
cce
ss. S
lots
with
in
Acu
te T
rusts
are
no
t ye
t b
ack to
pre
CO
VID
activity b
ut a
re in
cre
asin
g.
•C
ha
iley C
linic
al S
erv
ice
s: A
ll C
on
su
lta
nt le
d c
linic
s s
top
pe
d d
uri
ng
wa
ve
on
e. T
he
te
am
is n
ow
wo
rkin
g th
rou
gh
th
e b
acklo
g a
s c
linic
s h
ave
re
sta
rte
d a
s p
art
of re
se
t a
nd
reco
ve
ry. C
hild
ren
with
th
e lo
ng
est w
aits a
re b
ein
g p
rio
ritise
d, to
ge
the
r w
ith
th
ose
with
mo
re u
rge
nt clin
ica
l ne
ed
s. A
fu
ll re
vie
w o
f a
ll o
utp
atie
nt clin
ics is
als
o u
nd
erw
ay.
•C
hild
De
ve
lop
me
ntS
erv
ice
s: T
he
re w
as a
re
du
ctio
n in
Co
nsu
lta
nt clin
ics d
uri
ng
wa
ve
on
e. T
he
se
rvic
e is n
ow
op
era
tin
g to
gre
ate
r ca
pa
city a
nd
ad
dre
ssin
g lo
ng
est w
aits a
s a
pri
ori
ty, to
ge
the
r w
ith
th
ose
with
mo
re u
rge
nt clin
ica
l ne
ed
s. A
ll C
hild
De
ve
lop
me
nt
Ce
ntr
es m
et th
e ta
rge
t in
Se
pte
mb
er.
•M
SK
de
ma
nd
is b
ack to
pre
-co
vid
le
ve
ls, a
nd
RT
T c
om
plia
nt.
•R
he
um
ato
log
y: R
TT
co
mp
lian
tb
ut re
du
ce
d c
on
su
lta
nt co
ve
r is
lik
ely
to
im
pa
ct o
n te
am
ca
pa
city
in D
ece
mb
er.
•P
ain
Asse
ssm
ent a
nd
Clin
ica
l Eva
lua
tio
n(P
AC
E):
Th
ere
is a
co
ho
rt o
f lo
ng
wa
itin
g
pa
tie
nts
bu
ilt u
p d
uri
ng
Co
vid
an
d a
lso
an
In
cre
ase
in r
efe
rra
l n
um
be
rs.A
ve
rag
e r
efe
rra
l
nu
mb
ers
ove
r th
e la
st th
ree
mo
nth
sa
re 1
60
co
mp
are
d to
a p
re C
ovid
ave
rag
e o
f 1
00
. A
po
ten
tia
l ca
use
is th
at d
em
an
d h
as in
cre
ase
d b
eca
use
of
pa
tie
nt re
du
ce
d m
ob
ility
du
rin
g lo
ckd
ow
n. A
lso
, it is n
ot p
ossib
le to
ru
n fa
ce
to fa
ce
gro
up
pa
in m
an
ag
em
ent
cla
sse
s a
t p
rese
nt.
Lo
ng
est w
aitin
gp
atie
nts
ha
ve
all
no
w b
ee
n o
ffe
red
ap
po
intm
ents
.
Th
e w
aitin
g lis
tis
estim
ate
d to
be
gro
win
g b
y a
pp
roxim
ate
ly 5
pe
r w
ee
k. R
TT
is a
rou
nd
68
% b
ut co
ntin
ue
s to
im
pro
ve
. A
sse
ssm
en
ts o
f clin
ica
l ha
rm h
ave
be
en
co
mp
lete
d a
s
req
uir
ed
.T
his
sh
ow
s n
on
e a
re lik
ely
to
ha
ve
su
sta
ine
d h
arm
an
d a
ll h
ave
a fo
rma
l
clin
ica
l ha
rm r
evie
w d
ate
se
t. L
ocu
m C
on
su
lta
nt se
ssio
ns a
re b
ein
g s
et u
p to
wo
rk
thro
ug
h th
e b
acklo
g.
Ad
ditio
na
l ca
pa
city h
as b
ee
n s
ou
rce
d fro
m r
eg
ula
r co
nsu
lta
nts
an
d
a lo
cu
m. T
his
sh
ou
ld b
e s
uff
icie
nt to
cle
ar
the
cu
rre
nt 1
8 w
ee
k w
aits.
Th
e t
ea
m is a
lso
wo
rkin
g th
rou
gh
op
tio
ns fo
r d
eliv
eri
ng
pa
in m
an
ag
em
en
t cla
sse
s v
irtu
ally
.
Ou
tco
me
Actio
ns a
re in
pla
ce
to
ad
dre
ss d
ete
rio
rate
d p
erf
orm
an
ce
.
Tim
esca
leO
ng
oin
g
Page 52 of 300
13
Op
era
tio
na
l S
po
tlig
ht
Rep
ort
As
ym
pto
mati
c S
taff
Testi
ng
On 1
6th
Novem
ber
2020, N
HS
Engla
nd a
nd N
HS
Im
pro
vem
ent publis
hed a
sta
ndard
opera
ting
pro
cedure
for
rollo
ut of la
tera
l flow
devic
es for
asym
pto
matic s
taff testing.
Overa
ll aim
: T
o r
oll
out re
gula
r te
sting o
f all
asym
pto
matic N
HS
sta
ff u
sin
g late
ral flow
devic
es
(LF
Ds)
on n
asal sw
ab s
am
ple
s w
ith im
media
te e
ffect.
Each N
HS
org
anis
ation is r
equired to
:
•Take d
eliv
ery
of sta
ff testing k
its a
nd a
rrange d
eliv
ery
to a
ll patient fa
cin
g fro
nt lin
e s
taff
•E
nsure
that sta
ff u
nders
tand h
ow
to s
elf a
dm
inis
ter
the test
•E
sta
blis
h a
help
lin
e o
r dro
p-in a
ssis
tance p
oin
t fo
r sta
ff m
em
bers
havin
g d
ifficulty p
erf
orm
ing
the s
elf-a
dm
inis
tere
d test
•E
sta
blis
h a
mechanis
m for
sta
ff to r
etu
rn their w
eekly
results s
heets
•P
rovid
e info
rmation for
sta
ff m
em
bers
on w
hat to
do if th
ey test positiv
e a
nd w
here
they w
ill g
et
their s
wab test fo
r confirm
ato
ry P
CR
•A
gre
e w
ho is the d
esig
nate
d la
bora
tory
for
confirm
ato
ry P
CR
testing
•D
evelo
p a
mechanis
m for
record
ing a
nd r
eport
ing r
esults for
sta
tuto
ry p
urp
oses in lin
e w
ith t
he
sta
ndard
opera
ting p
rocedure
At th
e tim
e o
f w
riting, S
CF
T is p
lannin
g to g
o liv
e w
ith the p
rogra
mm
e o
n W
ednesday 2
5th
Novem
ber,
with testing k
its b
ein
g d
eliv
ere
d to fro
ntlin
e p
atient fa
cin
g s
taff o
n 2
3rd
and 2
4th
Novem
ber.
05 IP
R_2
021_
M06
_fin
al
Page 53 of 300

Wo
rkfo
rce
Re
po
rt
14
Page 54 of 300
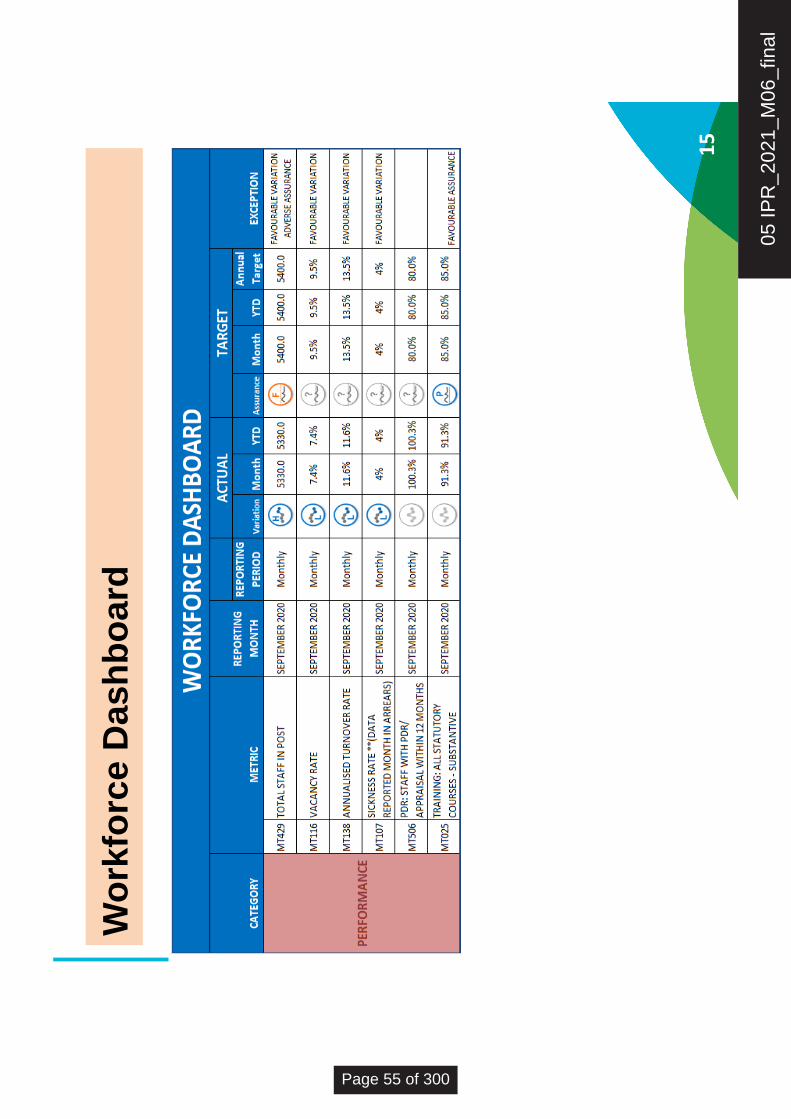
15
Wo
rkfo
rce
Dash
bo
ard
05 IP
R_2
021_
M06
_fin
al
Page 55 of 300
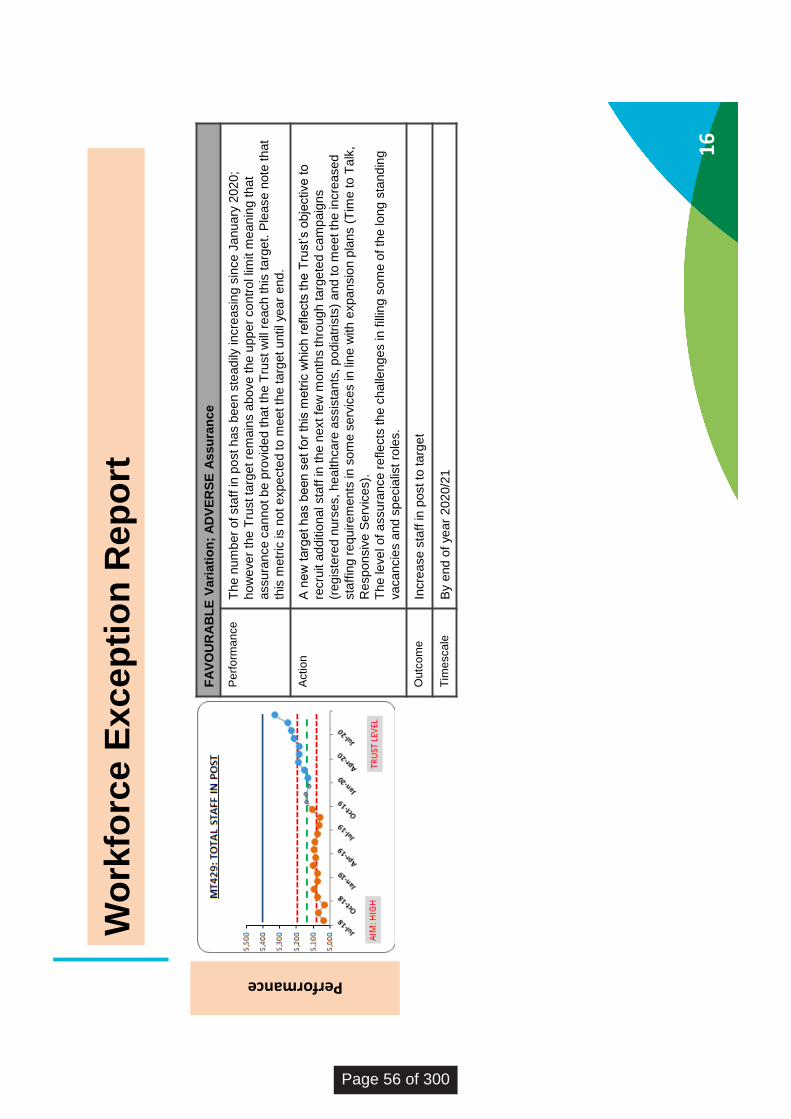
16
Wo
rkfo
rce
Exc
ep
tio
n R
ep
ort
FA
VO
UR
AB
LE
Va
ria
tio
n;
AD
VE
RS
E A
ssu
ran
ce
Pe
rfo
rma
nce
Th
e n
um
ber
of sta
ff in
po
st h
as b
ee
n s
tead
ily in
cre
asin
g s
ince
Ja
nu
ary
202
0;
how
eve
r th
e T
rust ta
rge
t re
ma
ins a
bo
ve
th
e u
pp
er
co
ntr
ol lim
it m
ean
ing th
at
assu
ran
ce
ca
nn
ot b
e p
rovid
ed
th
at
the
Tru
st w
ill r
each
th
is t
arg
et. P
lease
no
te th
at
this
me
tric
is n
ot
exp
ecte
d to
me
et th
e t
arg
et u
ntil ye
ar
end
.
Actio
nA
new
targ
et has b
een s
et fo
r th
is m
etr
ic w
hic
h r
eflects
the T
rust’s o
bje
ctive to
recru
it a
dditio
na
l sta
ff in
th
e n
ext
few
mo
nth
s th
rou
gh
ta
rge
ted
ca
mp
aig
ns
(re
gis
tere
d n
urs
es, h
ea
lth
ca
re a
ssis
tants
, p
od
iatr
ists
) a
nd
to
me
et th
e in
cre
ase
d
sta
ffin
g r
equ
ire
me
nts
in
so
me
se
rvic
es in
lin
e w
ith
exp
an
sio
n p
lans (
Tim
e to
Ta
lk,
Re
sp
on
siv
e S
erv
ice
s).
Th
e le
ve
l o
f a
ssu
ran
ce
re
fle
cts
th
e c
halle
ng
es in
fill
ing s
om
e o
f th
e lo
ng
sta
nd
ing
va
ca
ncie
s a
nd
sp
ecia
list
role
s.
Ou
tco
me
Incre
ase
sta
ff in
po
st to
ta
rge
t
Tim
esca
leB
y e
nd
of ye
ar
202
0/2
1
Performance
Page 56 of 300
17
Wo
rkfo
rce
Sp
otl
igh
t R
ep
ort
Sp
otl
igh
t o
n s
taff
re
de
plo
ym
en
t d
uri
ng
ph
as
e o
ne
of
the
Co
vid
-19
pa
nd
em
ic
Ove
rvie
w
As p
art
of th
e c
ovid
-19
re
sp
on
se t
he T
rust
wa
s r
equ
este
d to
sca
le b
ack a
nu
mb
er
of
se
rvic
es a
nd
fo
cu
s r
eso
urc
es in
se
rvic
es
tha
t w
ou
ld b
e m
ost im
pa
cte
d b
y C
ovid
. S
taff
we
re d
ep
loye
d to
su
pp
ort
in
hig
h p
rio
ry a
rea
s a
nd
te
am
s a
cro
ss th
e T
rust.
As p
art
of o
ur
lea
rnin
g fro
m th
e r
ed
ep
loym
ent p
roce
ss, fe
edb
ack w
as s
ou
gh
t fr
om
th
ose
in
vo
lve
d in
clu
din
g o
pe
rationa
l
ma
na
gers
, sta
ff r
ed
ep
loye
d, a
nd
sta
ff w
ork
ing in
th
e c
en
tra
l re
de
plo
ym
ent te
am
(ta
ctica
l te
am
). T
he
fe
ed
back f
ocu
se
d o
n w
ha
t
we
nt
we
ll a
nd
wh
at
co
uld
be
im
pro
ve
d in
fu
ture
. I
nfo
rma
tion w
as g
ath
ere
d t
ho
ugh
fe
edb
ack s
essio
n w
ith
ma
na
gers
, a
su
rve
y
se
nt to
th
e 4
50
re
de
plo
ye
d s
taff
an
d a
fo
cu
s g
rou
p w
ith
th
e ta
ctica
l te
am
.
Mo
st
of th
e s
taff
re
de
plo
ye
d w
ere
fro
m C
hild
ren &
Sp
ecia
list s
erv
ice
s w
ho
we
nt to
ad
ult s
erv
ice
s (
48
% to
West,
26
% to
Ce
ntr
al, 1
0%
to
Ea
st,
an
d 7
% to
Co
mm
unity S
wa
bb
ing)
with
th
e m
ajo
rity
wo
rkin
g in
Re
sp
on
siv
e s
erv
ice
s a
nd
IC
Us.
Sta
ff
work
ed
in r
ole
s s
uch
as n
urs
es (
31
% )
th
era
pis
ts (
26
%),
un
regis
tere
d c
linic
al (2
5%
) an
d a
dm
in (
14
%).
Fe
ed
ba
ck
fro
m s
taff
Th
e s
urv
ey h
ad
a 3
3%
re
sp
on
se r
ate
(1
46
re
sp
on
ses)
an
d in
clu
de
d 9
90
co
mm
ents
. M
an
y s
taff
co
mm
en
ted th
at
the
y h
ad
mix
ed
fe
elin
gs a
bo
ut re
de
plo
ym
en
t d
urin
g C
ovid
. A
th
em
e w
as t
ha
t it w
as b
oth
a p
ositiv
e a
nd
ne
ga
tive
exp
erie
nce; n
ega
tive
initia
lly b
ut p
ositiv
e o
nce
th
ey w
ere
mo
re fa
mili
ar
with
th
e w
ork
th
ey w
ere
do
ing.
•6
1%
of
sta
ff r
ep
ort
ed
an
ove
rall
po
sitiv
e o
r n
eu
tra
l e
xp
erie
nce
•2
4%
a n
ega
tive
exp
erie
nce
Th
ere
we
re a
ra
nge
of re
aso
ns w
hy s
taff
did
no
t w
an
t to
be
re
de
plo
ye
d a
ga
in. T
he
ma
in th
em
es r
ela
ted
to
fle
xib
ility
, la
ck o
f
su
pp
ort
, im
pa
ct o
n th
eir s
ub
sta
ntive
se
rvic
e a
nd
no
t fe
elin
g a
s th
ou
gh
th
ey w
ere
ne
ed
ed b
ut th
ere
we
re a
lso
ma
ny p
ositiv
e
co
mm
ents
.
•9
1*
sta
ff w
ou
ld e
ith
er
co
nsid
er
or
like
to
be
re
de
plo
ye
d a
ga
in
•6
2*
sta
ff r
ep
ort
ed
th
ey w
ou
ld h
ave
re
se
rva
tio
ns
* S
om
e s
ele
cte
d m
ore
than o
ne a
nsw
er
Fe
ed
ba
ck
fro
m o
pe
rati
on
al m
an
ag
ers
Ma
na
ge
rs r
ep
ort
ed
th
at th
ere
we
re c
ha
llenge
s w
ith
th
eir a
bili
ty to
in
du
ct a
nd
su
pe
rvis
e r
ed
ep
loye
es e
sp
ecia
lly a
s s
om
e w
ere
an
xio
us a
nd
re
qu
ire
d a
lo
t o
f su
pp
ort
. T
he
y w
ou
ld h
ave
lik
ed
ad
ditio
nal m
an
agem
ent ca
pa
city a
t th
e s
tart
an
d a
gre
ate
r
un
de
rsta
ndin
g o
f th
e s
kill
s s
et
of th
ose
jo
inin
g th
em
. M
an
age
rs w
ho
se
sta
ff h
ad
be
en
re
de
plo
ye
d f
elt u
na
ble
to
co
nn
ect w
ith
the
ir te
am
me
mb
ers
an
d fe
lt p
ow
erle
ss to
he
lp.
05 IP
R_2
021_
M06
_fin
al
Page 57 of 300
On
th
e o
the
r h
an
d m
ana
ge
rs r
efle
cte
d it
wa
s a
n e
me
rgin
g s
itu
atio
n a
nd
th
ere
we
re p
ositiv
e o
utc
om
es s
uch a
s r
ede
plo
ye
es
co
ntin
uin
g to
wo
rk in
th
e s
erv
ice
on
th
e B
ank (
a fe
w e
ve
n c
han
ge
d r
ole
s to
jo
in th
em
), th
ere
wa
s a
positiv
e im
pa
ct o
n th
e r
ece
ivin
g
team
of h
avin
g a
dd
itio
na
l ca
pa
city a
nd
skill
s s
et a
nd
on p
atie
nt ca
re. T
he fe
elin
g o
f w
ork
ing
to
ge
the
r a
nd
le
arn
ing
fro
m e
ach
oth
er
we
re a
lso
th
em
es.
Feed
back f
rom
ta
cti
cal te
am
Th
e ta
ctical te
am
wo
rke
d w
ell
bring
ing
a b
ala
nce
of skill
s
su
ch a
s p
roje
ct m
ana
ge
me
nt, H
R, tr
ain
ing
, and c
linic
al, h
ow
eve
r
fin
din
g a
co
mm
on w
ay t
o m
ana
ge
th
e p
roce
ss a
t p
ace
wh
en
se
ttin
g u
p f
rom
scra
tch
wa
s c
halle
ng
ing
. C
om
mu
nic
ation
with
are
a
team
s to a
gre
e r
edeplo
ym
ent sta
rt d
ate
s a
nd d
eta
ils w
as d
ifficult a
t tim
es a
s p
eople
were
not sure
of th
eir r
ole
s a
nd
respo
nsib
ilitie
s a
nd
th
e ta
ctical te
am
had
lim
ite
d in
form
atio
n a
bo
ut sta
ff s
kill
s, h
ou
rs a
nd
wo
rkin
g p
att
ern
s w
hic
h m
ean
t so
me
se
rvic
es s
tru
gg
led w
here
wo
rkin
g h
ou
rs d
id n
ot fit w
ith
usua
l sh
ifts
, le
avin
g s
taff
fe
elin
g li
ke
th
ey w
ere
not re
qu
ire
d o
r h
avin
g t
o b
e
mo
ve
d to
ano
the
r p
lacem
ent.
A n
um
ber
of sta
ff w
ere
to
ld th
ey w
ere
bein
g r
ede
plo
ye
d b
ut d
id n
ot g
o a
nyw
here
as th
e n
ee
ds
ch
an
ge
d. A
cce
ssin
g tra
inin
g a
nd
IT
eq
uip
me
nt so
me
tim
es s
low
ed t
he p
roce
ss d
ow
n e
spe
cia
lly in
th
e b
eg
innin
g.
Co
nc
lus
ion
an
d r
eco
mm
en
da
tio
ns
Th
e la
rge
sca
le r
ede
plo
ym
ent o
f sta
ff w
as f
ast p
ace
d w
ith
th
e ta
ctical te
am
co
ord
inatin
g th
e m
ove
me
nt o
f sta
ff c
entr
ally
oft
en
with
ou
t th
e fu
ll p
ictu
re le
ad
ing
to
so
me
mis
ma
tch
es o
f skill
s o
r re
qu
ire
me
nts
. R
eceiv
ing
te
am
s a
nd
re
de
plo
ye
d s
taff
had
little
tim
e
to p
repare
and m
anag
ers
found s
upport
ing
sta
ff in
itia
lly c
halle
ng
ing
. T
here
was s
till
an o
vera
ll positiv
e im
pact on indiv
idua
ls a
nd
team
s a
nd
on p
atie
nt ca
re.
Re
de
plo
ym
ent
at sca
le w
ill n
ot ta
ke
pla
ce a
ga
in a
nd
so
ma
ny o
f th
e c
halle
ng
es w
ould
not su
rfa
ce a
ga
in h
ow
eve
r th
ere
are
so
me
org
anis
ation
al le
arn
ing
s th
at ca
n b
e a
pp
lied s
hou
ld s
ma
ller
sca
le r
ede
plo
ym
ent e
ve
r b
e n
ee
de
d in
clu
din
g:
•A
re
de
plo
ym
ent p
ack fo
r sta
ff, r
eceiv
ing
ma
na
ge
rs, su
bsta
ntive
ma
na
ge
rs s
hou
ld b
e d
eve
lope
d t
o s
et o
ut ro
les a
nd
respo
nsib
ilitie
s
•E
arly in
du
ction
an
d a
perio
d o
f fa
mili
arisatio
n w
ith
th
e n
ew
te
am
wo
uld
be r
eq
uire
d
•A
dditio
na
l su
pp
ort
sh
ou
ld b
e id
en
tifie
d f
or
team
s r
eceiv
ing
re
de
plo
ye
es t
o p
rovid
e s
upe
rvis
ion a
nd
we
llbein
g s
upp
ort
•A
ce
ntr
al te
am
wo
rkin
g w
ith
are
a-b
ase
d r
ede
plo
ym
ent co
ord
inato
rs a
nd
adm
inis
tra
tors
to
arr
ang
e r
ede
plo
ym
ents
acro
ss
are
as o
r se
rvic
es w
ould
be r
eq
uire
d to
re
du
ce th
e im
pact o
n m
ana
ge
rs
•P
repa
ring
fo
r b
usin
ess c
ontin
uity s
itu
atio
ns s
hou
ld inclu
de
sta
ff r
ede
plo
ym
ent to
ensu
re te
am
s a
re m
ore
pre
pa
red
•S
taff
wh
o h
ad
a p
ositiv
e e
xp
erie
nce
sh
ou
ld b
e s
upp
ort
ed to
ke
ep
lin
ks w
ith
se
rvic
es to
ensu
re s
kill
s a
re m
ain
tain
ed
•W
here
sta
ff h
ave
ind
ica
ted
th
ey w
ould
be h
ap
py t
o b
e r
ede
plo
ye
d a
ga
in, th
ey s
hou
ld b
e in
clu
de
d in
th
e p
rim
ary
gro
up
if
furt
her
rede
plo
ym
ent w
as r
eq
uire
d
18
Wo
rkfo
rce
Sp
otl
igh
t R
ep
ort
co
nti
nu
ed
Page 58 of 300
Fin
ance
Re
po
rt
19
05 IP
R_2
021_
M06
_fin
al
Page 59 of 300
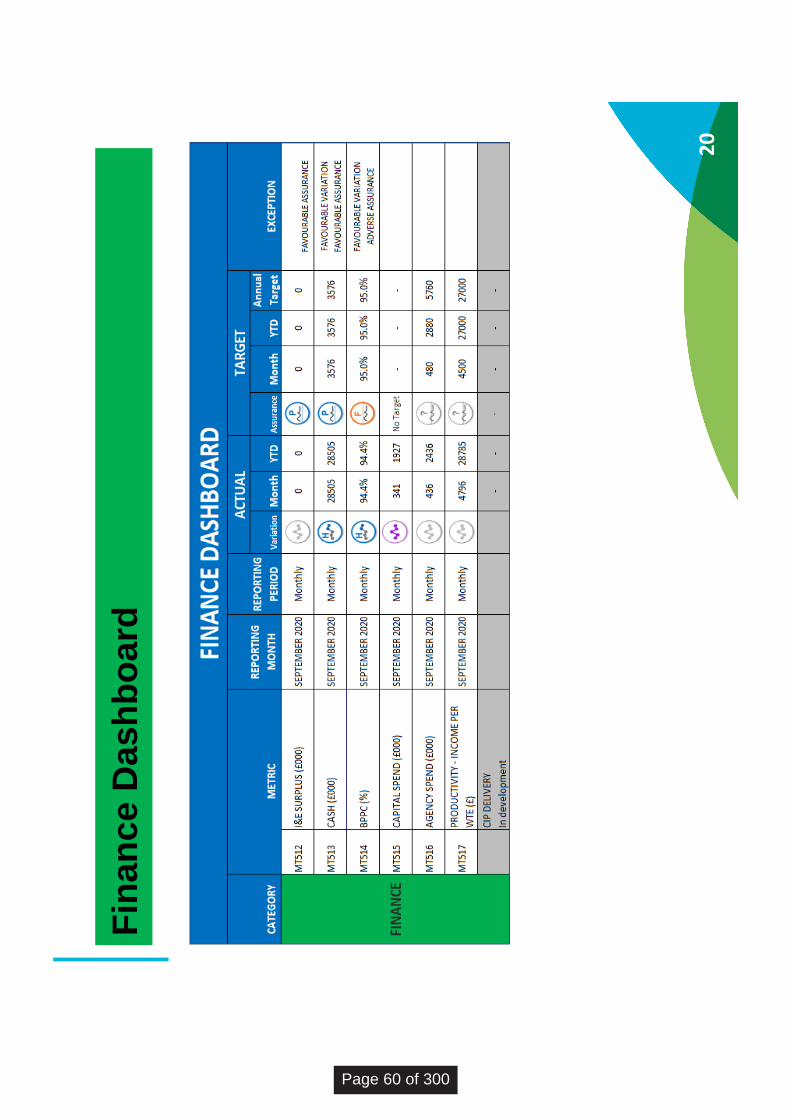
20
Fin
an
ce D
ash
bo
ard
Page 60 of 300
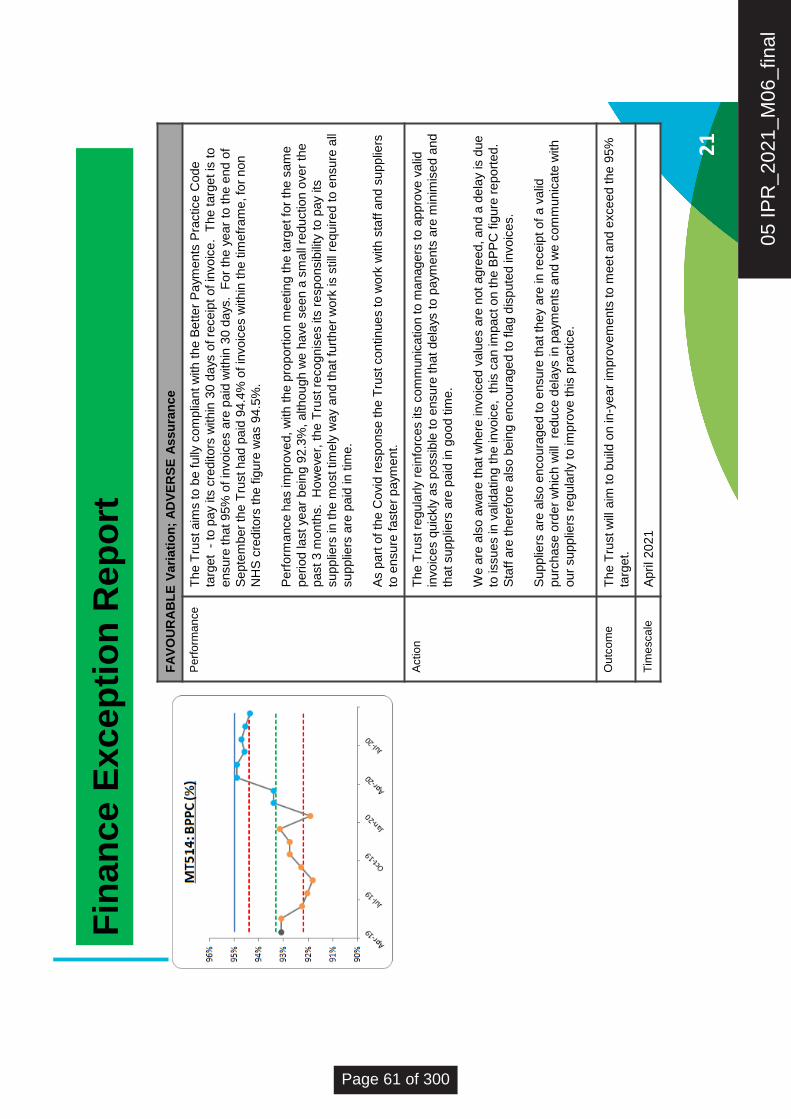
FA
VO
UR
AB
LE
Va
ria
tio
n;
AD
VE
RS
E A
ssu
ran
ce
Pe
rfo
rma
nce
Th
e T
rust a
ims to
be fu
lly c
om
plia
nt w
ith
th
e B
ette
r P
aym
ents
Pra
ctice
Cod
e
targ
et
-to
pay
its c
reditors
within
30 d
ays
of re
ceip
t of in
voic
e.
The targ
et is
to
ensu
re th
at 9
5%
of in
vo
ice
s a
re p
aid
with
in 3
0 d
ays.
Fo
r th
e y
ear
to th
e e
nd
of
Se
pte
mb
er
the T
rust h
ad
pa
id 9
4.4
% o
f in
vo
ice
s w
ith
in t
he t
ime
fra
me
, fo
r n
on
NH
S c
redito
rs t
he
fig
ure
wa
s 9
4.5
%.
Pe
rfo
rma
nce
has im
pro
ve
d,
with
th
e p
rop
ort
ion m
eetin
g th
e ta
rge
t fo
r th
e s
am
e
perio
d la
st
year
bein
g 9
2.3
%, a
lth
ou
gh
we
have
se
en
a s
ma
ll re
du
ctio
n o
ve
r th
e
past 3
mo
nth
s. H
ow
eve
r, t
he T
rust re
co
gn
ise
s its
re
sp
on
sib
ility
to
pay its
su
pp
liers
in
th
e m
ost tim
ely
wa
y a
nd
th
at
furt
he
r w
ork
is s
till
requ
ire
d t
o e
nsu
re a
ll
su
pp
liers
are
paid
in
tim
e.
As p
art
of th
e C
ovid
re
sp
on
se
th
e T
rust co
ntin
ue
s to
wo
rk w
ith
sta
ff a
nd
su
pp
liers
to e
nsu
re fa
ste
r p
aym
ent.
Actio
nT
he T
rust re
gu
larly
rein
forc
es its
co
mm
un
ica
tio
n to
ma
na
ge
rsto
app
rove
va
lid
invo
ice
s q
uic
kly
as p
ossib
le t
o e
nsu
re th
at
de
lays
to
paym
ents
are
min
imis
ed a
nd
that su
pp
liers
are
paid
in
goo
d tim
e.
We
are
als
o a
wa
re t
hat w
here
in
vo
ice
d v
alu
es a
re n
ot
ag
ree
d, a
nd
a d
ela
y is
due
to issu
es in
va
lidatin
g t
he in
vo
ice
, t
his
ca
n im
pact o
n t
he
BP
PC
fig
ure
re
po
rte
d.
Sta
ff a
re th
ere
fore
als
o b
ein
g e
nco
ura
ge
d to
fla
g d
isp
ute
d in
vo
ice
s.
Su
pp
liers
are
als
o e
nco
ura
ge
d to
ensu
re th
at th
ey a
re in
re
ce
ipt o
f a
va
lid
purc
hase
ord
er
wh
ich
will
re
du
ce
dela
ys in
pa
yme
nts
and
we
co
mm
unic
ate
with
our
su
pp
liers
re
gu
larly
to im
pro
ve
th
is p
ractice
.
Ou
tco
me
Th
e T
rust w
illa
im to
build
on in
-ye
ar
imp
rove
me
nts
to
me
et a
nd
exce
ed
th
e 9
5%
targ
et.
Tim
esca
leA
pril2021
21
Fin
an
ce E
xcep
tio
n R
ep
ort
05 IP
R_2
021_
M06
_fin
al
Page 61 of 300

22
Fin
an
ce S
po
tlig
ht
Rep
ort
•F
ina
ncia
l R
egim
e a
nd
M7
-12
Pla
ns: F
or
the
six
mo
nth
pe
rio
d to
th
e e
nd
of
Se
pte
mber
20
20, N
HS
pro
vid
ers
we
re f
un
ded
thro
ugh
a n
atio
nally
agre
ed
blo
ck c
on
tra
ct,
with
no
pro
vid
er
exp
ecte
d to
be
op
era
ting a
fin
ancia
l d
eficit a
s a
re
su
lt o
f th
e
CO
VID
re
sp
on
se. I
t w
as a
gre
ed
th
at re
aso
na
ble
co
sts
re
latin
g to
ou
r o
pe
ratio
ns d
urin
g th
is p
erio
d w
ere
re
imb
urs
ed
thro
ugh a
“to
p u
p”
arr
an
gem
ent if o
ur
incom
e s
tream
s a
re u
nab
le to
cover
them
. A
s a
resu
lt th
e T
rust ha
s r
ep
ort
ed a
bre
ake
ve
n p
ositio
n f
or
this
pe
rio
d.
•F
rom
Octo
be
r 2
02
0, fo
r th
e fin
al six
mo
nth
s o
f th
e f
ina
ncia
l ye
ar
the
NH
S f
ina
ncia
l re
gim
e h
as c
ha
nge
d. F
or
this
pe
rio
d
the
Tru
st h
as s
ub
mitte
d a
pla
n th
at fo
reca
sts
a d
eficit o
f £
4.0
m. T
he
de
ficit is a
s a
re
su
lt o
f tw
o issu
es:
i.N
HS
E’s
pla
nn
ing a
ssu
mp
tio
n th
at P
rovid
ers
’ no
n-N
HS
in
co
me
str
ea
ms w
ill r
etu
rn t
o le
ve
ls r
ep
ort
ed in
th
e 2
01
9/2
0
fin
an
cia
l ye
ar,
wh
ich
th
e T
rust
ha
s h
igh
ligh
ted
is n
ot a
ch
ieva
ble
in
th
is tim
efr
am
e (
£3
.5m
).
ii.T
he
Tru
st’s f
ore
ca
st th
at th
ere
is a
lik
ely
ris
k t
ha
t th
e v
alu
e o
f a
nn
ual le
ave
ca
rrie
d fo
rwa
rd b
y s
taff
will
in
cre
ase
by
the
en
d o
f th
e f
ina
ncia
l ye
ar
as a
re
su
lt o
f th
e r
esp
on
se to
th
e p
an
dem
ic. T
he
Tru
st
will
ne
ed t
o m
ake
a p
rovis
ion
to
co
ve
r th
is in
its
acco
unts
. B
oth
of
the
se
issu
es a
re “
allo
wa
ble
” re
aso
ns fo
r th
e T
rust
in te
rms o
f its r
ep
ort
ed p
ositio
n
an
d th
ere
fore
do
no
t re
fle
ct a
n u
nd
erlyin
g issu
e r
ela
ted
to
its
fin
an
cia
l su
sta
ina
bili
ty.
•T
he
pla
ns in
clu
de £
7.7
m o
f a
dd
itio
nal sp
en
d a
nd
in
co
me
assu
mp
tions r
ela
tin
g to
se
rvic
e d
eve
lop
ments
in
clu
ded
inclu
din
g:
i.E
xte
nd
ing im
mu
nis
ations s
erv
ice
s
ii.W
idenin
g a
cce
ss to
Psych
olo
gic
al T
he
rap
ies
iii.
Ad
ditio
na
l in
patient b
ed
s in
Brigh
ton
an
d H
ove
an
d W
est S
usse
x
iv.
Incre
asin
g c
ap
acity in th
e T
rust’s U
rgen
t C
om
munity R
esp
on
se s
erv
ices (
“Hom
e F
irst”
)
v.
En
ha
ncin
g th
e le
ve
l o
f clin
ica
l in
pu
t in
to C
are
Ho
me
s
•In
a c
ha
nge
fro
m p
revio
us p
lan
nin
g r
ou
nd
s, th
e p
lan
s h
ave
be
en
de
ve
lop
ed p
rim
arily
th
rou
gh
a s
yste
m b
ase
d a
pp
roa
ch,
via
th
e S
usse
x H
ea
lth
an
d C
are
In
tegra
ted
Ca
re S
yste
m (
ICS
). T
his
ha
s m
ea
nt th
at a
ll N
HS
bo
die
s in
Su
sse
x h
ave
de
ve
lop
ed th
eir a
pp
roa
ch to
pla
nnin
g a
nd
th
e f
ina
ncia
l p
lan
s th
em
se
lve
s a
s p
art
of a
syste
m w
ide
co
llab
ora
tive
, w
ith
ris
ks
an
d o
pp
ort
unitie
s in
in
div
idu
al o
rga
nis
ations b
ein
g m
itig
ate
d o
r im
ple
mente
d th
rou
gh
a c
olle
ctive
ap
pro
ach to
ma
na
gin
g
risk.
Th
is a
pp
roa
ch is lik
ely
to
be
on
e in
cre
asin
gly
fo
llow
ed
as w
e h
ea
d in
to 2
02
1/2
2.
Page 62 of 300
Tru
stw
ide
Ris
ks
23
05 IP
R_2
021_
M06
_fin
al
Page 63 of 300
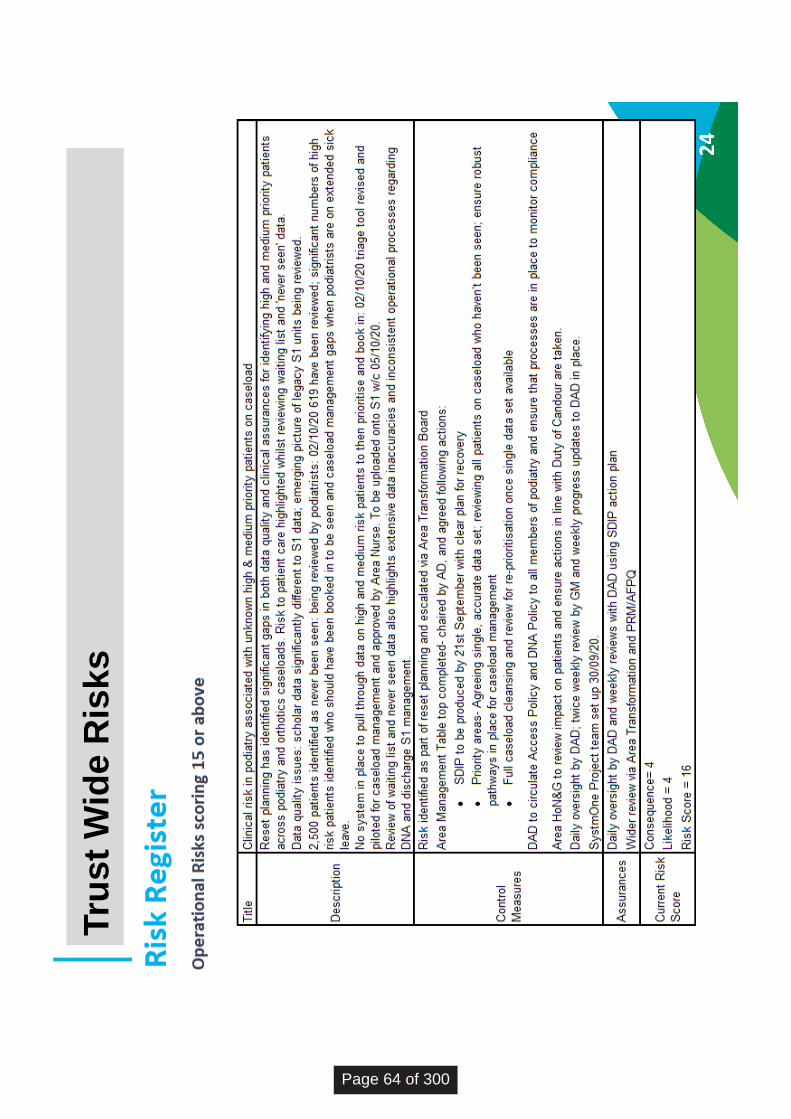
24
Tru
st
Wid
e R
isks
Page 64 of 300

25
Tru
st
Wid
e R
isks
IT R
isks
IT
Ris
ks s
corin
g 15
or a
bove
Th
ere
were
no
IT ri
sks
scor
ing
15 o
r abo
ve
05 IP
R_2
021_
M06
_fin
al
Page 65 of 300

BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number: 6
Report Title: Infection Prevention and Control Assurance
Purpose:
Approval Assurance X Discussion Briefing X
Summary: The Board is provided with the first summary report of key Infection Prevention and Control (IPC) issues. The report will ensure the Board has regular oversight of IPC issues and risk management. The IPC Board Assurance Framework (BAF) is attached at Appendix 1; future reports will highlight changes and exceptions to this framework.
Recommendation: The Board are asked to note this paper and in particular:
Take assurance from the IPC BAF that the trust has robust systems and processes in place to prevent healthcare acquired infection.
Appropriate actions and decisions are taken to manage risk but that this is within the context of a national pandemic.
Previously reviewed by: Nil
Relevance to Trust’s Strategic Goals: Population Health; Quality Improvement; Patient Experience; Thriving Staff; Value and Sustainability
Relevance to CQC Domains: Safe; Caring; Responsive; Effective; Well Led
Equality and Diversity: No formal assessment undertaken; equality and diversity is part of the clinical risk assessment for patients and staff.
Report author: Donna Lamb, Chief Nurse
Report owner: Donna Lamb, Chief Nurse
06 C
S In
fect
ion
Pre
vent
ion
and
Con
trol
Boa
rd A
ssur
ance
Page 66 of 300
Infection Prevention and Control – summary of key issues and risks 1.0 IPC Board Assurance Framework The IPC BAF was introduced earlier this year to provide a framework for trusts to assess themselves against IPC standards. This was first presented to the Trust Board in May 2020. The framework has since been revised and a third version was submitted to the Care Quality Commission (CQC) and discussed in an engagement meeting on 14 August 2020. The CQC found that the trust had undertaken a thorough assessment of infection prevention and control across all services, since the pandemic of Covid 19 was declared, which had regularly reviewed. They noted that appropriate systems were in place including the prevention of healthcare associated infections. The full BAF (v3 as shared with the CQC) is attached at appendix 1 for your information; future reports will report exceptions against this framework. A new version (v4) has now been released and we will be required to report against this from January 2021. 2.0 Key IPC risks and issues 2.1 Outbreak management Outbreak management for Covid-19 is more complex than flu or norovirus because of the ability for people to be infectious and asymptomatic, the level of community transmission and the challenges in providing Covid-19 secure environments in inpatient settings. The trust currently has three outbreaks in Horizon (Horsham), Crowborough and Don Baines (Bognor). There are currently 25 affected patients and 10 staff. Patients are cohorted in two units and Crowborough is currently closed to admissions. 2.2 Learning from outbreaks Learning includes:
PPE breaches due to human factors and meeting individual patient’s needs
Attending work when unwell
Maintaining social distancing in shared areas 2.3 IPC team capacity The IPC team has an establishment of 4.29 wte clinical staff; because of resignations (post-retirement and promotion) the capacity from 1 January 2021 will be 2.6 wte, all at a band 7 (specialist nurse) level. The team model has been reviewed and a revised model shared with the Executive team which increases the strategic and clinical leadership, provides for professional development and which will enable a more comprehensive service to be delivered now and for the future. Whilst this is being discussed, we have started recruitment to the 8C senior post. Recruitment is challenging as there is significant demand for qualified IPC nurses and demand is high. Management and leadership to the team is
Page 67 of 300

being provided by the deputy chief nurse and one of the band 7 nurses is taking on a clinical lead role. The team will also be going in to Business Continuity to enable them to provide the required level of support, advice and guidance to our inpatient settings. 2.4 Estates It is important to note that we have to manage IPC precautions in the estate that we have. Socially distancing staff and fully cohorting Covid-19 positive patients or those self-isolating can be difficult; not all of our single rooms or bays are ensuite for instance. Decisions are made with the advice of the IPC team and consider all risks. Recommendation The Board is asked to take assurance from the IPC BAF that the trust has robust systems and processes in place to prevent healthcare acquired infection. The Board is also asked to note however that our systems, processes and decision-making enables us to manage risk but not to eradicate it within the current pandemic. 06
CS
Infe
ctio
n P
reve
ntio
nan
d C
ontr
ol B
oard
Ass
uran
ce
Page 68 of 300

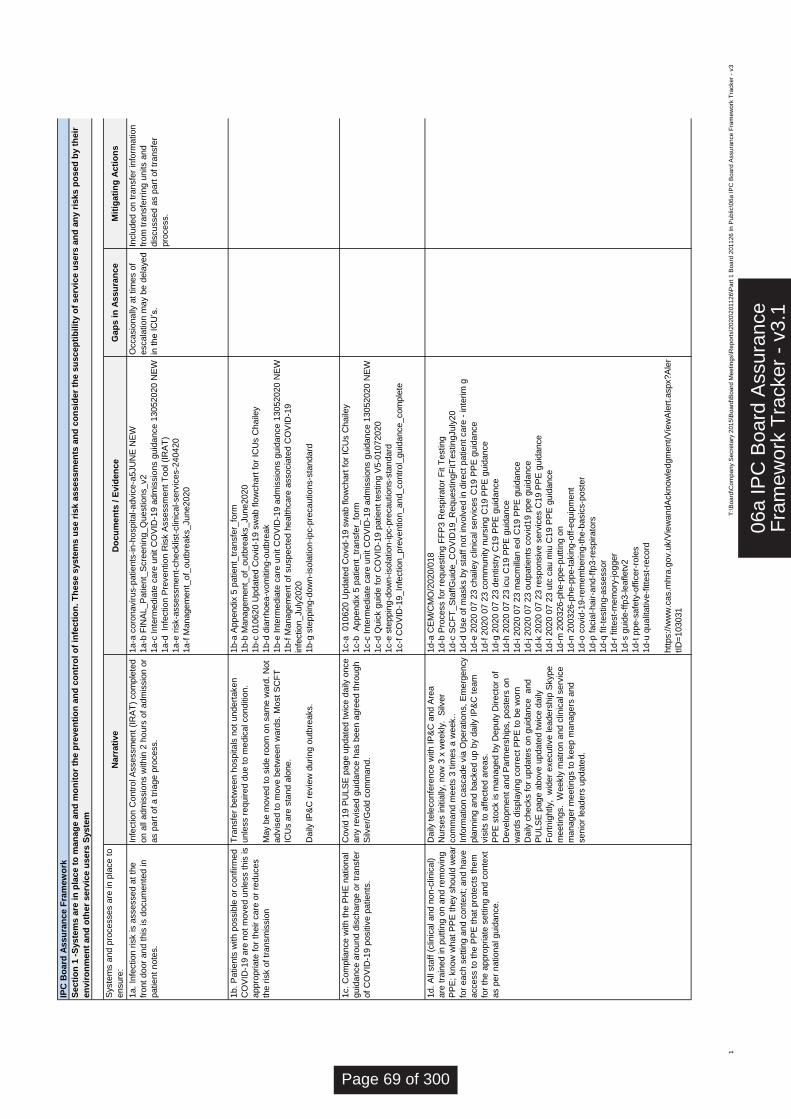
Syste
ms a
nd p
rocesses a
re in p
lace t
o
ensure
:D
ocu
men
ts /
Evid
en
ce
1a.
Infe
ction r
isk is a
ssessed a
t th
e
front
door
and t
his
is d
ocum
ente
d in
patient
note
s.
1a-a
coro
navirus-p
atients
-in-h
ospital-advic
e-a
5JU
NE
NE
W
1a-b
FIN
AL_P
atient_
Scre
enin
g_Q
uestions_v2
1a-c
Inte
rmedia
te c
are
unit C
OV
ID-1
9 a
dm
issio
ns g
uid
ance 1
3052020 N
EW
1a-d
In
fection P
revention R
isk A
ssessm
ent
Tool (I
RA
T)
1a-e
ris
k-a
ssessm
ent-
checklis
t-clin
ical-serv
ices-2
40420
1a-f
Managem
ent_
of_
outb
reaks_June2020
1b.
Patients
with p
ossib
le o
r confirm
ed
CO
VID
-19 a
re n
ot
moved u
nle
ss t
his
is
appro
priate
for
their c
are
or
reduces
the r
isk o
f tr
ansm
issio
n
1b-a
Appendix
5 p
atient_
transfe
r_fo
rm
1b-b
Managem
ent_
of_
outb
reaks_June2020
1b-c
010620 U
pdate
d C
ovid
-19 s
wab f
low
chart
for
ICU
s C
haile
y
1b-d
dia
rrhoea-v
om
itin
g-o
utb
reak
1b-e
Inte
rmedia
te c
are
unit C
OV
ID-1
9 a
dm
issio
ns g
uid
ance 1
3052020 N
EW
1b-f
Managem
ent
of
suspecte
d h
ealthcare
associa
ted C
OV
ID-1
9
infe
ction_July
2020
1b-g
ste
ppin
g-d
ow
n-isola
tion-ipc-p
recautions-s
tandard
1c.
Com
plia
nce w
ith t
he P
HE
national
guid
ance a
round d
ischarg
e o
r tr
ansfe
r
of
CO
VID
-19 p
ositiv
e p
atients
.
1c-a
010620 U
pdate
d C
ovid
-19 s
wab f
low
chart
for
ICU
s C
haile
y
1c-b
A
ppendix
5 p
atient_
transfe
r_fo
rm
1c-c
Inte
rmedia
te c
are
unit C
OV
ID-1
9 a
dm
issio
ns g
uid
ance 1
3052020 N
EW
1c-d
Quic
k g
uid
e f
or
CO
VID
-19 p
atient
testing V
5-0
1072020
1c-e
ste
ppin
g-d
ow
n-isola
tion-ipc-p
recautions-s
tandard
1c-f
CO
VID
-19_In
fection_pre
vention_and_contr
ol_
guid
ance_com
ple
te
1d.
All
sta
ff (
clin
ical and n
on-c
linic
al)
are
tra
ined in p
utt
ing o
n a
nd r
em
ovin
g
PP
E;
know
what
PP
E t
hey s
hould
wear
for
each s
ett
ing a
nd c
onte
xt;
and h
ave
access t
o t
he P
PE
that
pro
tects
them
for
the a
ppro
priate
sett
ing a
nd c
onte
xt
as p
er
national guid
ance.
1d-a
CE
M/C
MO
/2020/0
18
1d-b
Pro
cess f
or
requesting F
FP
3 R
espirato
r F
it T
esting
1d-c
SC
FT
_S
taff
Guid
e_C
OV
ID19_R
equestingF
itT
estingJuly
20
1d-d
Use o
f m
asks b
y s
taff
not
involv
ed in d
irect
patient
care
- inte
rim
g
1d-e
2020 0
7 2
3 c
haile
y c
linic
al serv
ices C
19 P
PE
guid
ance
1d-f
2020 0
7 2
3 c
om
munity n
urs
ing C
19 P
PE
guid
ance
1d-g
2020 0
7 2
3 d
entistr
y C
19 P
PE
guid
ance
1d-h
2020 0
7 2
3 icu C
19 P
PE
guid
ance
1d-i 2
020 0
7 2
3 m
acm
illan e
ol C
19 P
PE
guid
ance
1d-j 2
020 0
7 2
3 o
utp
atients
covid
19 p
pe g
uid
ance
1d-k
2020 0
7 2
3 r
esponsiv
e s
erv
ices C
19 P
PE
guid
ance
1d-l 2
020 0
7 2
3 u
tc c
au m
iu C
19 P
PE
guid
ance
1d-m
200326-p
he-p
pe-p
utt
ing o
n
1d-n
200326-p
he-p
pe-t
akin
g-o
ff-e
quip
ment
1d-o
covid
-19-r
em
em
bering-t
he-b
asic
s-p
oste
r
1d-p
facia
l-hair-a
nd-f
fp3-r
espirato
rs
1d-q
fit-t
esting-a
ssessor
1d-r
fitte
st-
mem
ory
-jogger
1d-s
guid
e-f
fp3-leafletv
2
1d-t
ppe-s
afe
ty-o
ffic
er-
role
s
1d-u
qualit
ative-f
itte
st-
record
htt
ps:/
/ww
w.c
as.m
hra
.gov.u
k/V
iew
andA
cknow
ledgm
ent/
Vie
wA
lert
.aspx?A
ler
tID
=103031
Occasio
nally
at
tim
es o
f
escala
tion m
ay b
e d
ela
yed
in t
he IC
U’s
.
Covid
19 P
ULS
E p
age u
pdate
d t
wic
e d
aily
once
any r
evis
ed g
uid
ance h
as b
een a
gre
ed t
hro
ugh
Silv
er/
Gold
com
mand.
Secti
on
1 -
Syste
ms a
re i
n p
lace t
o m
an
ag
e a
nd
mo
nit
or
the p
reven
tio
n a
nd
co
ntr
ol
of
infe
cti
on
. T
hese s
yste
ms u
se r
isk a
ssessm
en
ts a
nd
co
nsid
er
the s
uscep
tib
ilit
y o
f serv
ice u
sers
an
d a
ny r
isks p
osed
by t
heir
en
vir
on
men
t an
d o
ther
serv
ice u
sers
Syste
m
IPC
Bo
ard
Assu
ran
ce F
ram
ew
ork
Inclu
ded o
n t
ransfe
r in
form
ation
from
tra
nsfe
rrin
g u
nits a
nd
dis
cussed a
s p
art
of
transfe
r
pro
cess.
Mit
igati
ng
Acti
on
s
Tra
nsfe
r betw
een h
ospitals
not
undert
aken
unle
ss r
equired d
ue t
o m
edic
al conditio
n.
May b
e m
oved t
o s
ide r
oom
on s
am
e w
ard
. N
ot
advis
ed t
o m
ove b
etw
een w
ard
s.
Most
SC
FT
ICU
s a
re s
tand a
lone.
Daily
IP
&C
revie
w d
uring o
utb
reaks.
Narr
ati
ve
Daily
tele
confe
rence w
ith IP
&C
and A
rea
Nurs
es initia
lly,
now
3 x
weekly
. S
ilver
com
mand m
eets
3 t
imes a
week..
Info
rmation c
ascade v
ia O
pera
tions,
Em
erg
ency
pla
nnin
g a
nd b
acked u
p b
y d
aily
IP
&C
team
vis
its t
o a
ffecte
d a
reas.
PP
E s
tock is m
anaged b
y D
eputy
Directo
r of
Develo
pm
ent
and P
art
ners
hip
s,
poste
rs o
n
ward
s d
ispla
yin
g c
orr
ect
PP
E t
o b
e w
orn
Daily
checks f
or
update
s o
n g
uid
ance
and
PU
LS
E p
age a
bove u
pdate
d t
wic
e d
aily
Fort
nig
htly,
wid
er
executive leaders
hip
Skype
meetings.
Weekly
matr
on a
nd c
linic
al serv
ice
manager
meetings t
o k
eep m
anagers
and
senio
r le
aders
update
d.
Infe
ction C
ontr
ol A
ssessm
ent
(IR
AT
) com
ple
ted
on a
ll adm
issio
ns w
ithin
2 h
ours
of
adm
issio
n o
r
as p
art
of
a t
riage p
rocess.
Gap
s i
n A
ssu
ran
ce
1T
:\B
oa
rd\C
om
pa
ny S
ecre
tary
201
5\B
oa
rd\B
oa
rd M
ee
ting
s\R
ep
ort
s\2
02
0\2
011
26
\Part
1 B
oa
rd 2
011
26
In
Pub
lic\0
6a
IP
C B
oa
rd A
ssura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 69 of 300
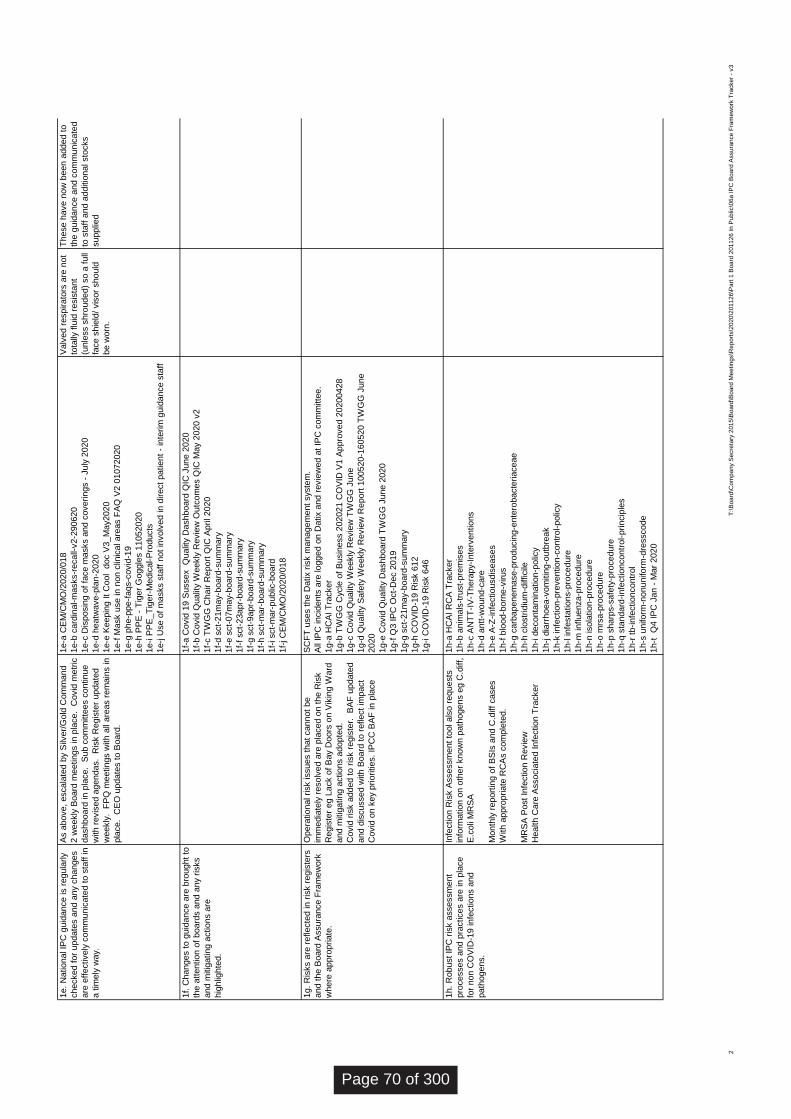
1e.
National IP
C g
uid
ance is r
egula
rly
checked f
or
update
s a
nd a
ny c
hanges
are
eff
ectively
com
munic
ate
d t
o s
taff
in
a t
imely
way.
1e-a
CE
M/C
MO
/2020/0
18
1e-b
card
inal-m
asks-r
ecall-
v2-2
90620
1e-c
Dis
posin
g o
f fa
ce m
asks a
nd c
overings -
July
2020
1e-d
heatw
ave-p
lan-2
020
1e-e
Keepin
g It
Cool d
oc V
3_M
ay2020
1e-f
Mask u
se in n
on c
linic
al are
as F
AQ
V2 0
1072020
1e-g
phe-p
pe-f
aqs-c
ovid
-19
1e-h
PP
E -
Tig
er
Goggle
s 1
1052020
1e-i P
PE
_T
iger-
Medic
al-P
roducts
1e-j U
se o
f m
asks s
taff
not
involv
ed in d
irect
patient
- in
terim
guid
ance s
taff
1f.
Changes t
o g
uid
ance a
re b
rought
to
the a
ttention o
f board
s a
nd a
ny r
isks
and m
itig
ating a
ctions a
re
hig
hlig
hte
d.
1f-
a C
ovid
19 S
ussex
Qualit
y D
ashboard
QIC
June 2
020
1f-
b C
ovid
Qualit
y W
eekly
Revie
w O
utc
om
es Q
IC M
ay 2
020 v
2
1f-
c T
WG
G C
hair R
eport
QIC
April 2020
1f-
d s
ct-
21m
ay-b
oard
-sum
mary
1f-
e s
ct-
07m
ay-b
oard
-sum
mary
1f-
f sct-
23apr-
board
-sum
mary
1f-
g s
ct-
9apr-
board
-sum
mary
1f-
h s
ct-
mar-
board
-sum
mary
1f-
i sct-
mar-
public
-board
1f-
j C
EM
/CM
O/2
020/0
18
1g.
Ris
ks a
re r
eflecte
d in r
isk r
egis
ters
and t
he B
oard
Assura
nce F
ram
ew
ork
where
appro
priate
.
SC
FT
uses t
he D
atix r
isk m
anagem
ent
syste
m.
All
IPC
incid
ents
are
logged o
n D
atix a
nd r
evie
wed a
t IP
C c
om
mitte
e.
1g-a
HC
AI T
racker
1g-b
TW
GG
Cycle
of
Busin
ess 2
02021 C
OV
ID V
1 A
ppro
ved 2
0200428
1g-c
Covid
Qualit
y W
eekly
Revie
w T
WG
G J
une
1g-d
Qualit
y S
afe
ty W
eekly
Revie
w R
eport
100520-1
60520 T
WG
G J
une
2020
1g-e
Covid
Qualit
y D
ashboard
TW
GG
June 2
020
1g-f
Q3 IP
C O
ct-
Dec 2
019
1g-g
sct-
21m
ay-b
oard
-sum
mary
1g-h
CO
VID
-19 R
isk 6
12
1g-i C
OV
ID-1
9 R
isk 6
46
1h.
Robust
IPC
ris
k a
ssessm
ent
pro
cesses a
nd p
ractices a
re in p
lace
for
non C
OV
ID-1
9 infe
ctions a
nd
path
ogens.
1h-a
HC
AI R
CA
Tra
cker
1h-b
anim
als
-tru
st-
pre
mis
es
1h-c
AN
TT
-IV
-Thera
py-I
nte
rventions
1h-d
antt
-wound-c
are
1h-e
A-Z
-infe
ctiousdis
eases
1h-f
blo
od-b
orn
e-v
irus
1h-g
carb
apenem
ase-p
roducin
g-e
nte
robacte
riaceae
1h-h
clo
str
idiu
m-d
ifficile
1h-i d
econta
min
ation-p
olic
y
1h-j d
iarr
hoea-v
om
itin
g-o
utb
reak
1h-k
infe
ction-p
revention-c
ontr
ol-polic
y
1h-l infe
sta
tions-p
rocedure
1h-m
influenza-p
rocedure
1h-n
isola
tion-p
rocedure
1h-o
mrs
a-p
rocedure
1h-p
sharp
s-s
afe
ty-p
rocedure
1h-q
sta
ndard
-infe
ctioncontr
ol-princip
les
1h-r
tb-infe
ctioncontr
ol
1h-s
uniform
-nonuniform
-dre
sscode
1h-t
Q
4 IP
C J
an -
Mar
2020
Opera
tional risk issues t
hat
cannot
be
imm
edia
tely
resolv
ed a
re p
laced o
n t
he R
isk
Regis
ter
eg L
ack o
f B
ay D
oors
on V
ikin
g W
ard
and m
itig
ating a
ctions a
dopte
d.
Covid
ris
k a
dded t
o r
isk r
egis
ter.
B
AF
update
d
and d
iscussed w
ith B
oard
to r
eflect
impact
Covid
on k
ey p
riorities.
IPC
C B
AF
in p
lace
Infe
ction R
isk A
ssessm
ent
tool als
o r
equests
info
rmation o
n o
ther
know
n p
ath
ogens e
g C
.diff,
E.c
oli
MR
SA
Month
ly r
eport
ing o
f B
SIs
and C
.diff
cases
With a
ppro
priate
RC
As c
om
ple
ted.
MR
SA
Post
Infe
ction R
evie
w
Health C
are
Associa
ted Infe
ction T
racker
As a
bove,
escala
ted b
y S
ilver/
Gold
Com
mand
2 w
eekly
Board
meetings in p
lace.
Covid
metr
ic
dashboard
in p
lace.
Sub c
om
mitte
es c
ontinue
with r
evis
ed a
gendas.
Ris
k R
egis
ter
update
d
weekly
. F
PQ
meetings w
ith a
ll are
as r
em
ain
s in
pla
ce.
CE
O u
pdate
s t
o B
oard
.
Valv
ed r
espirato
rs a
re n
ot
tota
lly f
luid
resis
tant
(unle
ss s
hro
uded)
so a
full
face s
hie
ld/
vis
or
should
be w
orn
.
These h
ave n
ow
been a
dded t
o
the g
uid
ance a
nd c
om
munic
ate
d
to s
taff
and a
dditio
nal sto
cks
supplie
d
2T
:\B
oa
rd\C
om
pa
ny S
ecre
tary
201
5\B
oa
rd\B
oa
rd M
ee
ting
s\R
ep
ort
s\2
02
0\2
011
26
\Part
1 B
oa
rd 2
011
26
In
Pub
lic\0
6a
IP
C B
oa
rd A
ssura
nce F
ram
ew
ork
Tra
cker
- v3
Page 70 of 300
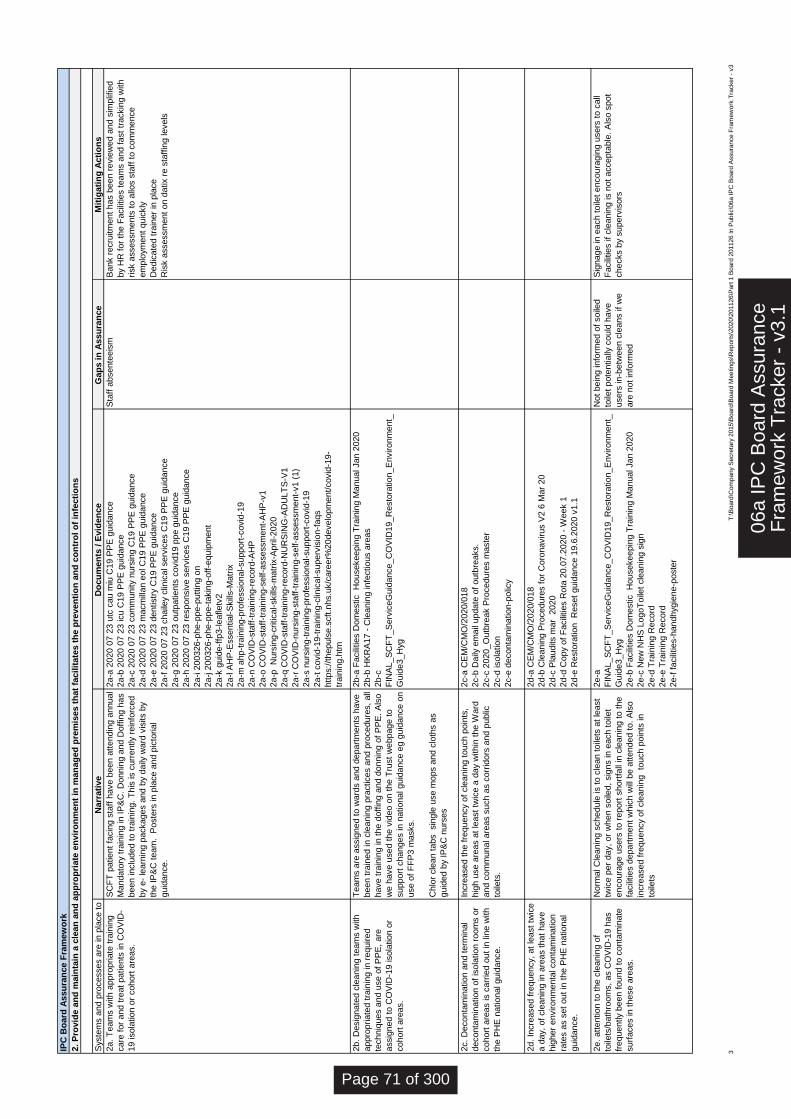
Syste
ms a
nd p
rocesses a
re in p
lace t
o
ensure
:
Do
cu
men
ts /
Evid
en
ce
Gap
s i
n A
ssu
ran
ce
2a.
Team
s w
ith a
ppro
priate
tra
inin
g
care
for
and t
reat
patients
in C
OV
ID-
19 isola
tion o
r cohort
are
as.
2a-a
2020 0
7 2
3 u
tc c
au m
iu C
19 P
PE
guid
ance
2a-b
2020 0
7 2
3 icu C
19 P
PE
guid
ance
2a-c
2020 0
7 2
3 c
om
munity n
urs
ing C
19 P
PE
guid
ance
2a-d
2020 0
7 2
3 m
acm
illan e
ol C
19 P
PE
guid
ance
2a-e
2020 0
7 2
3 d
entistr
y C
19 P
PE
guid
ance
2a-f
2020 0
7 2
3 c
haile
y c
linic
al serv
ices C
19 P
PE
guid
ance
2a-g
2020 0
7 2
3 o
utp
atients
covid
19 p
pe g
uid
ance
2a-h
2020 0
7 2
3 r
esponsiv
e s
erv
ices C
19 P
PE
guid
ance
2a-i 2
00326-p
he-p
pe-p
utt
ing o
n
2a-j 2
00326-p
he-p
pe-t
akin
g-o
ff-e
quip
ment
2a-k
guid
e-f
fp3-leafletv
2
2a-l A
HP
-Essential-S
kill
s-M
atr
ix
2a-m
ahp-t
rain
ing-p
rofe
ssio
nal-support
-covid
-19
2a-n
CO
VID
-sta
ff-t
rain
ing-r
ecord
-AH
P
2a-o
CO
VID
-sta
ff-t
rain
ing-s
elf-a
ssessm
ent-
AH
P-v
1
2a-p
N
urs
ing-c
ritical-skill
s-m
atr
ix-A
pril-2020
2a-q
CO
VID
-sta
ff-t
rain
ing-r
ecord
-NU
RS
ING
-AD
ULT
S-V
1
2a-r
CO
VID
-nurs
ing-s
taff
-tra
inin
g-s
elf-a
ssessm
ent-
v1 (
1)
2a-s
nurs
ing-t
rain
ing-p
rofe
ssio
nal-support
-covid
-19
2a-t
covid
-19-t
rain
ing-c
linic
al-superv
isio
n-f
aqs
htt
ps:/
/thepuls
e.s
cft
.nhs.u
k/c
are
er%
20develo
pm
ent/
covid
-19-
train
ing.h
tm
Sta
ff a
bsente
eis
m
2b.
Desig
nate
d c
leanin
g t
eam
s w
ith
appro
priate
d t
rain
ing in r
equired
techniq
ues a
nd u
se o
f P
PE
, are
assig
ned t
o C
OV
ID-1
9 isola
tion o
r
cohort
are
as.
2b-a
Facili
ties D
om
estic
Housekeepin
g T
rain
ing M
anual Jan 2
020
2b-b
HK
RA
17 -
Cle
anin
g infe
ctious a
reas
2b-c
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e3_H
yg
2c.
Deconta
min
ation a
nd t
erm
inal
deconta
min
ation o
f is
ola
tion r
oom
s o
r
cohort
are
as is c
arr
ied o
ut
in lin
e w
ith
the P
HE
national guid
ance.
2c-a
CE
M/C
MO
/2020/0
18
2c-b
Daily
em
ail
update
of
outb
reaks.
2c-c
2020_O
utb
reak P
rocedure
s m
aste
r
2c-d
isola
tion
2c-e
deconta
min
ation-p
olic
y
2d.
Incre
ased f
requency,
at
least
twic
e
a d
ay,
of
cle
anin
g in a
reas t
hat
have
hig
her
environm
enta
l conta
min
ation
rate
s a
s s
et
out
in t
he P
HE
national
guid
ance.
2d-a
CE
M/C
MO
/2020/0
18
2d-b
Cle
anin
g P
rocedure
s f
or
Coro
navirus V
2 6
Mar
20
2d-c
Pla
udits m
ar
2020
2d-d
Copy o
f F
acili
ties R
ota
20.0
7.2
020 -
Week 1
2d-e
Resto
ration
Reset
guid
ance 1
9.6
.2020 v
1.1
2e.
att
ention t
o t
he c
leanin
g o
f
toile
ts/b
ath
room
s,
as C
OV
ID-1
9 h
as
frequently b
een f
ound t
o c
onta
min
ate
surf
aces in t
hese a
reas.
2e-a
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e3_H
yg
2e-b
Facili
ties D
om
estic
Housekeepin
g T
rain
ing M
anual Jan 2
020
2e-c
New
NH
S L
ogoT
oile
t cle
anin
g s
ign
2e-d
Tra
inin
g R
ecord
2e-e
Tra
inin
g R
ecord
2e-f
facili
ties-h
andhygie
ne-p
oste
r
Not
bein
g info
rmed o
f soile
d
toile
t pote
ntially
could
have
users
in-b
etw
een c
leans if
we
are
not
info
rmed
Sig
nage in e
ach t
oile
t encoura
gin
g u
sers
to c
all
Facili
ties if
cle
anin
g is n
ot
accepta
ble
. A
lso s
pot
checks b
y s
uperv
isors
Norm
al C
leanin
g s
chedule
is t
o c
lean t
oile
ts a
t le
ast
twic
e p
er
day,
or
when s
oile
d,
sig
ns in e
ach t
oile
t
encoura
ge u
sers
to r
eport
short
fall
in c
leanin
g t
o t
he
facili
ties d
epart
ment
whic
h w
ill b
e a
ttended t
o.
Als
o
incre
ased f
requency o
f cle
anin
g
touch p
oin
ts in
toile
ts
Incre
ased t
he f
requency o
f cle
anin
g t
ouch p
oin
ts,
hig
h u
se a
reas a
t le
ast
twic
e a
day w
ithin
the W
ard
and c
om
munal are
as s
uch a
s c
orr
idors
and p
ublic
toile
ts.
SC
FT
patient
facin
g s
taff
have b
een a
ttendin
g a
nnual
Mandato
ry t
rain
ing in IP
&C
. D
onnin
g a
nd D
off
ing h
as
been inclu
ded t
o t
rain
ing.
This
is c
urr
ently r
ein
forc
ed
by e
- le
arn
ing p
ackages a
nd b
y d
aily
ward
vis
its b
y
the IP
&C
team
. P
oste
rs in p
lace a
nd p
icto
rial
guid
ance.
Bank r
ecru
itm
ent
has b
een r
evie
wed a
nd s
implif
ied
by H
R f
or
the F
acili
ties t
eam
s a
nd f
ast
trackin
g w
ith
risk a
ssessm
ents
to a
llos s
taff
to c
om
mence
em
plo
ym
ent
quic
kly
Dedic
ate
d t
rain
er
in p
lace
Ris
k a
ssessm
ent
on d
atix r
e s
taff
ing levels
Team
s a
re a
ssig
ned t
o w
ard
s a
nd d
epart
ments
have
been t
rain
ed in c
leanin
g p
ractices a
nd p
rocedure
s,
all
have t
rain
ing in t
he d
off
ing a
nd d
onnin
g o
f P
PE
. A
lso
we h
ave u
sed t
he v
ideo o
n t
he T
rust
webpage t
o
support
changes in n
ational guid
ance e
g g
uid
ance o
n
use o
f F
FP
3 m
asks.
Chlo
r cle
an t
abs
sin
gle
use m
ops a
nd c
loth
s a
s
guid
ed b
y IP
&C
nurs
es
IPC
Bo
ard
Assu
ran
ce F
ram
ew
ork
2.
Pro
vid
e a
nd
main
tain
a c
lean
an
d a
pp
rop
riate
en
vir
on
men
t in
man
ag
ed
pre
mis
es t
hat
facil
itate
s t
he p
reven
tio
n a
nd
co
ntr
ol
of
infe
cti
on
s
Narr
ati
ve
Mit
igati
ng
Acti
on
s
3T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
ep
ort
s\2
020\2
01126\P
art
1 B
oard
201126 In P
ub
lic\0
6a IP
C B
oard
Assura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 71 of 300
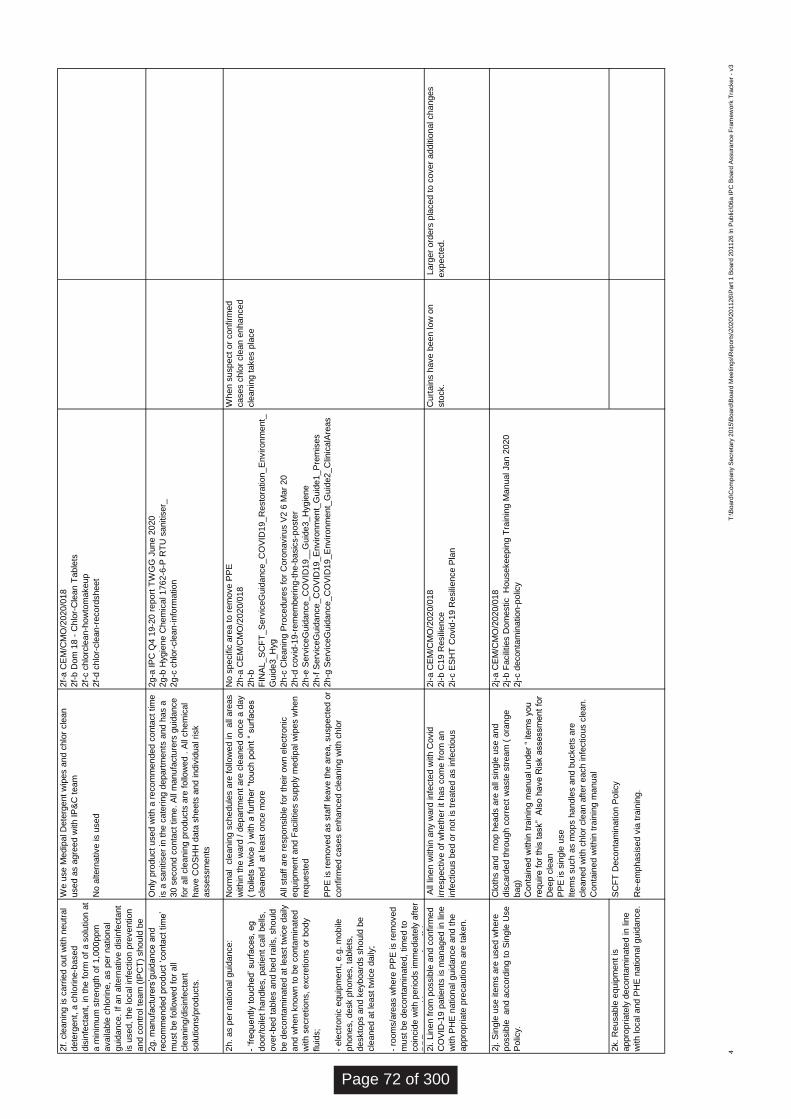
2f.
cle
anin
g is c
arr
ied o
ut
with n
eutr
al
dete
rgent,
a c
hlo
rine-b
ased
dis
infe
cta
nt,
in t
he f
orm
of
a s
olu
tion a
t
a m
inim
um
str
ength
of
1,0
00ppm
availa
ble
chlo
rine,
as p
er
national
guid
ance.
If a
n a
ltern
ative d
isin
fecta
nt
is u
sed,
the local in
fection p
revention
and c
ontr
ol te
am
(IP
CT
) should
be
consulted o
n t
his
to e
nsure
that
this
is
2f-
a C
EM
/CM
O/2
020/0
18
2f-
b D
om
18 -
Chlo
r-C
lean T
able
ts
2f-
c c
hlo
rcle
an-h
ow
tom
akeup
2f-
d c
hlo
r-cle
an-r
ecord
sheet
2g.
manufa
ctu
rers
’guid
ance a
nd
recom
mended p
roduct
‘conta
ct
tim
e’
must
be f
ollo
wed f
or
all
cle
anin
g/d
isin
fecta
nt
solu
tions/p
roducts
.
2g-a
IP
C Q
4 1
9-2
0 r
eport
TW
GG
June 2
020
2g-b
Hygie
ne C
hem
ical 1762-6
-P R
TU
sanitis
er_
2g-c
chlo
r-cle
an-info
rmation
2h.
as p
er
national guid
ance:
- ‘fre
quently t
ouched’ surf
aces,
eg
door/
toile
t handle
s,
patient
call
bells
,
over-
bed t
able
s a
nd b
ed r
ails
, should
be d
econta
min
ate
d a
t le
ast
twic
e d
aily
and w
hen k
now
n t
o b
e c
onta
min
ate
d
with s
ecre
tions,
excre
tions o
r body
fluid
s;
- ele
ctr
onic
equip
ment,
e.g
. m
obile
phones,
desk p
hones,
table
ts,
deskto
ps a
nd k
eyboard
s s
hould
be
cle
aned a
t le
ast
twic
e d
aily
;
- ro
om
s/a
reas w
here
PP
E is r
em
oved
must
be d
econta
min
ate
d,
tim
ed t
o
coin
cid
e w
ith p
eriods im
media
tely
aft
er
PP
E r
em
oval by g
roups o
f sta
ff (
at
No s
pecific
are
a t
o r
em
ove P
PE
2h-a
CE
M/C
MO
/2020/0
18
2h-b
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e3_H
yg
2h-c
Cle
anin
g P
rocedure
s f
or
Coro
navirus V
2 6
Mar
20
2h-d
covid
-19-r
em
em
bering-t
he-b
asic
s-p
oste
r
2h-e
Serv
iceG
uid
ance_C
OV
ID19__G
uid
e3_H
ygie
ne
2h-f
Serv
iceG
uid
ance_C
OV
ID19_E
nvironm
ent_
Guid
e1_P
rem
ises
2h-g
Serv
iceG
uid
ance_C
OV
ID19_E
nvironm
ent_
Guid
e2_C
linic
alA
reas
When s
uspect
or
confirm
ed
cases c
hlo
r cle
an e
nhanced
cle
anin
g t
akes p
lace
2i. L
inen f
rom
possib
le a
nd c
onfirm
ed
CO
VID
-19 p
atients
is m
anaged in lin
e
with P
HE
national guid
ance a
nd t
he
appro
priate
pre
cautions a
re t
aken.
2i-a C
EM
/CM
O/2
020/0
18
2i-b C
19 R
esili
ence
2i-c E
SH
T C
ovid
-19 R
esili
ence P
lan
Curt
ain
s h
ave b
een low
on
sto
ck.
2j. S
ingle
use ite
ms a
re u
sed w
here
possib
le
and a
ccord
ing t
o S
ingle
Use
Polic
y.
2k.
Reusable
equip
ment
is
appro
priate
ly d
econta
min
ate
d in lin
e
with local and P
HE
national guid
ance.
We u
se M
edip
al D
ete
rgent
wip
es a
nd c
hlo
r cle
an
used a
s a
gre
ed w
ith IP
&C
team
No a
ltern
ative is u
sed
All
linen w
ithin
any w
ard
infe
cte
d w
ith C
ovid
irre
spective o
f w
heth
er
it h
as c
om
e f
rom
an
infe
ctious b
ed o
r not
is t
reate
d a
s infe
ctious
Larg
er
ord
ers
pla
ced t
o c
over
additio
nal changes
expecte
d.
Only
pro
duct
used w
ith a
recom
mended c
onta
ct
tim
e
is a
sanitis
er
in t
he c
ate
ring d
epart
ments
and h
as a
30 s
econd c
onta
ct
tim
e.
All
manufa
ctu
rers
guid
ance
for
all
cle
anin
g p
roducts
are
follo
wed .
All
chem
ical
have C
OS
HH
data
sheets
and indiv
idual risk
assessm
ents
Clo
ths a
nd
mop h
eads a
re a
ll sin
gle
use a
nd
dis
card
ed t
hro
ugh c
orr
ect
waste
str
eam
( o
range
bag)
Conta
ined w
ithin
tra
inin
g m
anual under
“ item
s y
ou
require f
or
this
task”
Als
o h
ave R
isk a
ssessm
ent
for
Deep c
lean
PP
E is s
ingle
use
Item
s s
uch a
s m
ops h
andle
s a
nd b
uckets
are
cle
aned w
ith c
hlo
r cle
an a
fter
each infe
ctious c
lean.
Conta
ined w
ithin
tra
inin
g m
anual
SC
FT
Deconta
min
ation P
olic
y
Re-e
mphasis
ed v
ia t
rain
ing.
2j-a C
EM
/CM
O/2
020/0
18
2j-b F
acili
ties D
om
estic
Housekeepin
g T
rain
ing M
anual Jan 2
020
2j-c d
econta
min
ation-p
olic
y
Norm
al c
leanin
g s
chedule
s a
re f
ollo
wed in
all
are
as
within
the w
ard
/ d
epart
ment
are
cle
aned o
nce a
day
( to
ilets
tw
ice )
with a
furt
her
“touch p
oin
t “
surf
aces
cle
aned
at
least
once m
ore
All
sta
ff a
re r
esponsib
le f
or
their o
wn e
lectr
onic
equip
ment
and F
acili
ties s
upply
medip
al w
ipes w
hen
requeste
d
PP
E is r
em
oved a
s s
taff
leave t
he a
rea,
suspecte
d o
r
confirm
ed c
ases e
nhanced c
leanin
g w
ith c
hlo
r
4T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
ep
ort
s\2
020\2
01126\P
art
1 B
oard
201126 In P
ub
lic\0
6a IP
C B
oard
Assura
nce F
ram
ew
ork
Tra
cker
- v3
Page 72 of 300
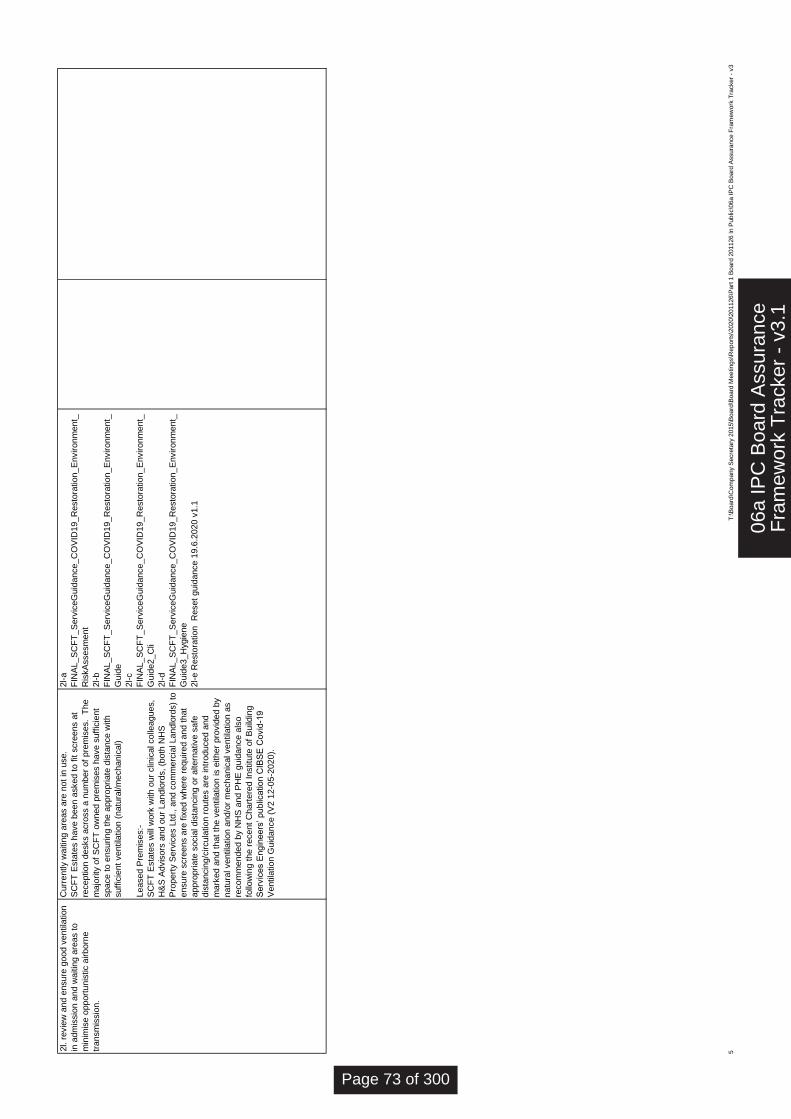
2l. r
evie
w a
nd e
nsure
good v
entila
tion
in a
dm
issio
n a
nd w
aitin
g a
reas t
o
min
imis
e o
pport
unis
tic a
irborn
e
transm
issio
n.
2l-a
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Ris
kA
ssesm
ent
2l-b
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e
2l-c
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e2_C
li
2l-d
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e3_H
ygie
ne
2l-e R
esto
ration
Reset
guid
ance 1
9.6
.2020 v
1.1
Curr
ently w
aitin
g a
reas a
re n
ot
in u
se.
SC
FT
Esta
tes h
ave b
een a
sked t
o f
it s
cre
ens a
t
reception d
esks a
cro
ss a
num
ber
of
pre
mis
es.
The
majo
rity
of
SC
FT
ow
ned p
rem
ises h
ave s
uff
icie
nt
space t
o e
nsuring t
he a
ppro
priate
dis
tance w
ith
suff
icie
nt
ventila
tion (
natu
ral/m
echanic
al)
Leased P
rem
ises:-
SC
FT
Esta
tes w
ill w
ork
with o
ur
clin
ical colle
agues,
H&
S A
dvis
ors
and o
ur
Landlo
rds,
(both
NH
S
Pro
pert
y S
erv
ices L
td.,
and c
om
merc
ial Landlo
rds)
to
ensure
scre
ens a
re f
ixed w
here
required a
nd t
hat
appro
priate
socia
l dis
tancin
g o
r altern
ative s
afe
dis
tancin
g/c
ircula
tion r
oute
s a
re intr
oduced a
nd
mark
ed a
nd t
hat
the v
entila
tion is e
ither
pro
vid
ed b
y
natu
ral ventila
tion a
nd/o
r m
echanic
al ventila
tion a
s
recom
mended b
y N
HS
and P
HE
guid
ance a
lso
follo
win
g t
he r
ecent
Chart
ere
d Institu
te o
f B
uild
ing
Serv
ices E
ngin
eers
’ public
ation C
IBS
E C
ovid
-19
Ventila
tion G
uid
ance (
V2 1
2-0
5-2
020).
5T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
ep
ort
s\2
020\2
01126\P
art
1 B
oard
201126 In P
ub
lic\0
6a IP
C B
oard
Assura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 73 of 300
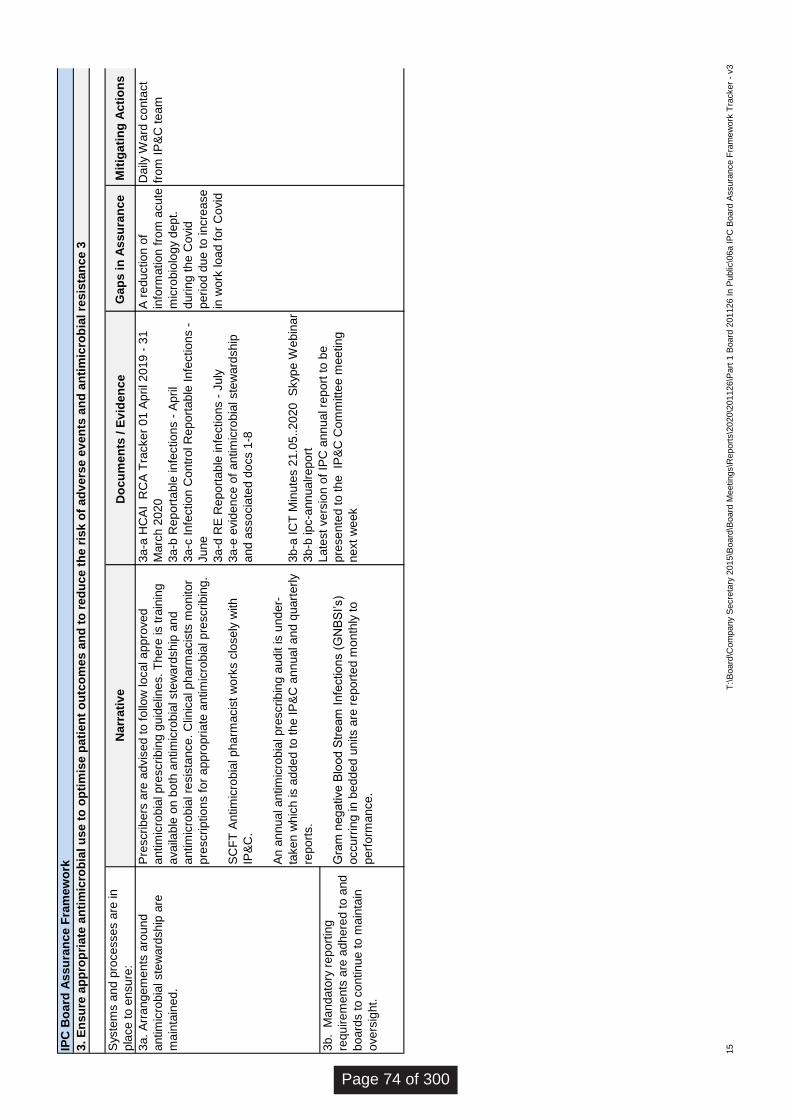
Syste
ms a
nd p
rocesses a
re in
pla
ce to e
nsure
:D
ocu
men
ts / E
vid
en
ce
3a. A
rrangem
ents
aro
und
antim
icro
bia
l ste
ward
ship
are
main
tain
ed.
3b. M
andato
ry r
eport
ing
requirem
ents
are
adhere
d to a
nd
board
s to c
ontinue to m
ain
tain
overs
ight.
Pre
scribers
are
advis
ed to f
ollo
w local appro
ved
antim
icro
bia
l pre
scribin
g g
uid
elin
es.
There
is t
rain
ing
availa
ble
on b
oth
antim
icro
bia
l ste
ward
ship
and
antim
icro
bia
l re
sis
tance. C
linic
al pharm
acis
ts m
onitor
pre
scriptions f
or
appro
priate
antim
icro
bia
l pre
scribin
g.
SC
FT
Antim
icro
bia
l pharm
acis
t w
ork
s c
losely
with
IP&
C.
An
annual antim
icro
bia
l pre
scribin
g a
udit is u
nder-
taken w
hic
h is a
dded to the IP
&C
annual and q
uart
erly
report
s.
Gra
m n
egative B
lood S
tream
Infe
ctions (
GN
BS
I’s)
occurr
ing in b
edded u
nits a
re r
eport
ed m
onth
ly to
perf
orm
ance.
3a-a
HC
AI
RC
A T
racke
r 0
1 A
pril 201
9 -
31
Marc
h 2
020
3a-b
Report
able
infe
ctions -
Ap
ril
3a-c
Infe
ction C
ontr
ol R
eport
ab
le In
fectio
ns -
June
3a-d
RE
Report
able
in
fectio
ns -
Ju
ly
3a-e
evid
ence o
f antim
icro
bia
l ste
wa
rdsh
ip
and a
ssocia
ted d
ocs 1
-8
3b-a
IC
T M
inute
s 2
1.0
5..20
20
S
kyp
e W
ebin
ar
3b-b
ipc-a
nnualreport
Late
st vers
ion o
f IP
C a
nn
ua
l re
po
rt to
be
pre
sente
d to t
he IP
&C
Com
mitte
e m
eeting
next
week
A r
edu
ction o
f
info
rma
tion f
rom
acute
mic
robio
logy d
ep
t.
durin
g the
Covid
perio
d d
ue to in
cre
ase
in w
ork
lo
ad
fo
r C
ovid
Da
ily W
ard
conta
ct
fro
m IP
&C
te
am
IPC
Bo
ard
Assu
ran
ce F
ram
ew
ork
3. E
nsu
re a
pp
rop
riate
an
tim
icro
bia
l u
se t
o o
pti
mis
e p
ati
en
t o
utc
om
es a
nd
to
red
uce t
he r
isk o
f ad
vers
e e
ve
nts
an
d a
nti
mic
rob
ial re
sis
tan
ce 3
Narr
ati
ve
Ga
ps
in
As
su
ran
ce
Mit
igati
ng
Ac
tio
ns
15
T:\
Board
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meetings\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 In P
ublic
\06a IP
C B
oard
Assura
nce F
ram
ew
ork
Tra
cker
- v3
Page 74 of 300
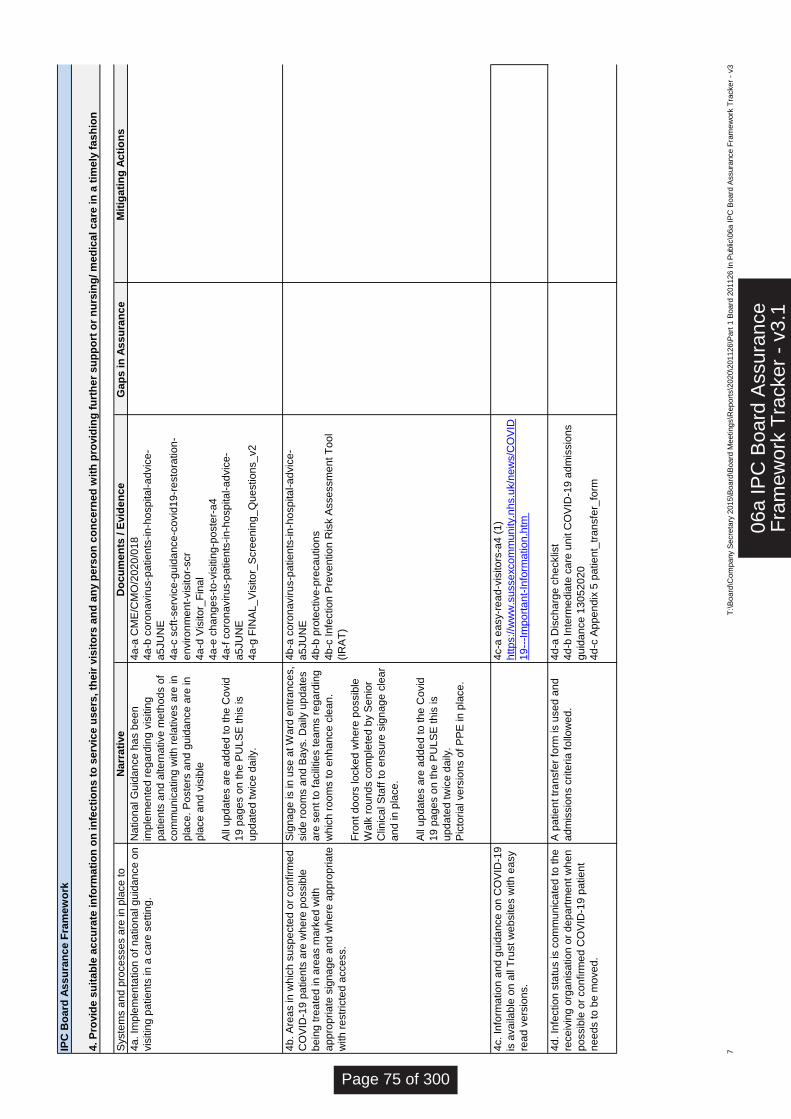
Syste
ms a
nd
pro
ce
sse
s a
re in
pla
ce
to
en
su
re:
Do
cu
me
nts
/ E
vid
en
ce
G
ap
s in
As
su
ran
ce
4a
. Im
ple
me
nta
tio
n o
f n
atio
na
l g
uid
an
ce
on
vis
itin
g p
atie
nts
in
a c
are
se
ttin
g.
4a
-a C
ME
/CM
O/2
02
0/0
18
4a
-b c
oro
na
viru
s-p
atie
nts
-in
-ho
sp
ita
l-a
dvic
e-
a5
JU
NE
4a
-c s
cft
-se
rvic
e-g
uid
an
ce
-co
vid
19
-re
sto
ratio
n-
en
viro
nm
en
t-vis
ito
r-scr
4a
-d V
isito
r_F
ina
l
4a
-e c
ha
ng
es-t
o-v
isitin
g-p
oste
r-a
4
4a
-f c
oro
na
viru
s-p
atie
nts
-in
-ho
sp
ita
l-a
dvic
e-
a5
JU
NE
4a
-g F
INA
L_
Vis
ito
r_S
cre
en
ing
_Q
ue
stio
ns_
v2
4b
. A
rea
s in
wh
ich
su
sp
ecte
d o
r co
nfirm
ed
CO
VID
-19
pa
tie
nts
are
wh
ere
po
ssib
le
be
ing
tre
ate
d in
are
as m
ark
ed
with
ap
pro
pria
te s
ign
ag
e a
nd
wh
ere
ap
pro
pria
te
with
re
str
icte
d a
cce
ss.
4b
-a c
oro
na
viru
s-p
atie
nts
-in
-ho
sp
ita
l-a
dvic
e-
a5
JU
NE
4b
-b p
rote
ctive
-pre
ca
utio
ns
4b
-c In
fectio
n P
reve
ntio
n R
isk A
sse
ssm
en
t T
oo
l
(IR
AT
)
4c. In
form
atio
n a
nd
gu
ida
nce
on
CO
VID
-19
is a
va
ilab
le o
n a
ll T
rust w
eb
site
s w
ith
ea
sy
rea
d v
ers
ion
s.
4c-a
ea
sy-r
ea
d-v
isito
rs-a
4 (
1)
http
s://w
ww
.su
sse
xco
mm
un
ity.n
hs.u
k/n
ew
s/C
OV
ID
19
---I
mp
ort
an
t-In
form
atio
n.h
tm
4d
. In
fectio
n s
tatu
s is c
om
mu
nic
ate
d to
th
e
rece
ivin
g o
rga
nis
atio
n o
r d
ep
art
me
nt w
he
n
po
ssib
le o
r co
nfirm
ed
CO
VID
-19
pa
tie
nt
ne
ed
s to
be
mo
ve
d.
4d
-a D
isch
arg
e c
he
cklis
t
4d
-b In
term
ed
iate
ca
re u
nit C
OV
ID-1
9 a
dm
issio
ns
gu
ida
nce
13
05
20
20
4d
-c A
pp
en
dix
5 p
atie
nt_
tra
nsfe
r_fo
rm
Sig
na
ge
is in
use
at W
ard
en
tra
nce
s,
sid
e r
oo
ms a
nd
Ba
ys. D
aily
up
da
tes
are
se
nt to
fa
cili
tie
s te
am
s r
eg
ard
ing
wh
ich
ro
om
s to
en
ha
nce
cle
an
.
Fro
nt d
oo
rs lo
cke
d w
he
re p
ossib
le
Wa
lk r
ou
nd
s c
om
ple
ted
by S
en
ior
Clin
ica
l S
taff
to
en
su
re s
ign
ag
e c
lea
r
an
d in
pla
ce
.
All
up
da
tes a
re a
dd
ed
to
th
e C
ovid
19
pa
ge
s o
n th
e P
UL
SE
th
is is
up
da
ted
tw
ice
da
ily.
Pic
toria
l ve
rsio
ns o
f P
PE
in
pla
ce
.
A p
atie
nt tr
an
sfe
r fo
rm is u
se
d a
nd
ad
mis
sio
ns c
rite
ria
fo
llow
ed
.
Na
tio
na
l G
uid
an
ce
ha
s b
ee
n
imp
lem
en
ted
re
ga
rdin
g v
isitin
g
pa
tie
nts
an
d a
lte
rna
tive
me
tho
ds o
f
co
mm
un
ica
tin
g w
ith
re
lative
s a
re in
pla
ce
. P
oste
rs a
nd
gu
ida
nce
are
in
pla
ce
an
d v
isib
le
All
up
da
tes a
re a
dd
ed
to
th
e C
ovid
19
pa
ge
s o
n th
e P
UL
SE
th
is is
up
da
ted
tw
ice
da
ily.
IPC
Bo
ard
As
su
ran
ce
Fra
me
wo
rk
4. P
rovid
e s
uit
ab
le a
cc
ura
te in
form
ati
on
on
in
fec
tio
ns
to
se
rvic
e u
se
rs, th
eir
vis
ito
rs a
nd
an
y p
ers
on
co
nc
ern
ed
wit
h p
rovid
ing
fu
rth
er
su
pp
ort
or
nu
rsin
g/ m
ed
ica
l c
are
in
a t
ime
ly f
as
hio
n
Na
rra
tive
M
itig
ati
ng
Ac
tio
ns
7T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 75 of 300
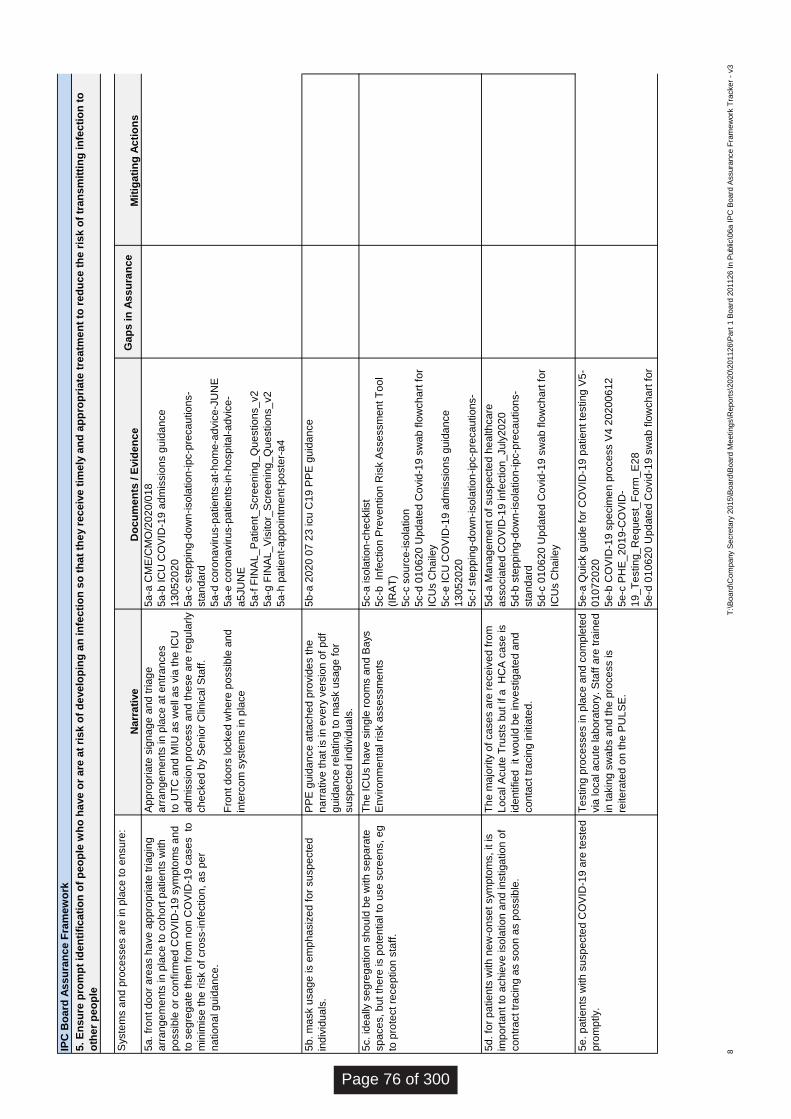
Syste
ms a
nd
pro
ce
sse
s a
re in
pla
ce
to
en
su
re:
Do
cu
me
nts
/ E
vid
en
ce
G
ap
s in
As
su
ran
ce
5a
. fr
on
t d
oo
r a
rea
s h
ave
ap
pro
pria
te tria
gin
g
arr
an
ge
me
nts
in
pla
ce
to
co
ho
rt p
atie
nts
with
po
ssib
le o
r co
nfirm
ed
CO
VID
-19
sym
pto
ms a
nd
to s
eg
reg
ate
th
em
fro
m n
on
CO
VID
-19
ca
se
s to
min
imis
e th
e r
isk o
f cro
ss-in
fectio
n, a
s p
er
na
tio
na
l g
uid
an
ce
.
5a
-a C
ME
/CM
O/2
02
0/0
18
5a
-b IC
U C
OV
ID-1
9 a
dm
issio
ns g
uid
an
ce
13
05
20
20
5a
-c s
tep
pin
g-d
ow
n-iso
latio
n-ip
c-p
reca
utio
ns-
sta
nd
ard
5a
-d c
oro
na
viru
s-p
atie
nts
-at-
ho
me
-ad
vic
e-J
UN
E
5a
-e c
oro
na
viru
s-p
atie
nts
-in
-ho
sp
ita
l-a
dvic
e-
a5
JU
NE
5a
-f F
INA
L_
Pa
tie
nt_
Scre
en
ing
_Q
ue
stio
ns_
v2
5a
-g F
INA
L_
Vis
ito
r_S
cre
en
ing
_Q
ue
stio
ns_
v2
5a
-h p
atie
nt-
ap
po
intm
en
t-p
oste
r-a
4
5b
. m
ask u
sa
ge
is e
mp
ha
siz
ed
fo
r su
sp
ecte
d
ind
ivid
ua
ls.
5b
-a 2
02
0 0
7 2
3 icu
C1
9 P
PE
gu
ida
nce
5c. id
ea
lly s
eg
reg
atio
n s
ho
uld
be
with
se
pa
rate
sp
ace
s, b
ut th
ere
is p
ote
ntia
l to
use
scre
en
s, e
g
to p
rote
ct re
ce
ptio
n s
taff
.
5c-a
iso
latio
n-c
he
cklis
t
5c-b
In
fectio
n P
reve
ntio
n R
isk A
sse
ssm
en
t T
oo
l
(IR
AT
)
5c-c
so
urc
e-iso
latio
n
5c-d
01
06
20
Up
da
ted
Co
vid
-19
sw
ab
flo
wch
art
fo
r
ICU
s C
ha
iley
5c-e
IC
U C
OV
ID-1
9 a
dm
issio
ns g
uid
an
ce
13
05
20
20
5c-f
ste
pp
ing
-do
wn
-iso
latio
n-ip
c-p
reca
utio
ns-
sta
nd
ard
5d
. fo
r p
atie
nts
with
ne
w-o
nse
t sym
pto
ms, it is
imp
ort
an
t to
ach
ieve
iso
latio
n a
nd
in
stig
atio
n o
f
co
ntr
act tr
acin
g a
s s
oo
n a
s p
ossib
le.
5d
-a M
an
ag
em
en
t o
f su
sp
ecte
d h
ea
lth
ca
re
asso
cia
ted
CO
VID
-19
in
fectio
n_
Ju
ly2
02
0
5d
-b s
tep
pin
g-d
ow
n-iso
latio
n-ip
c-p
reca
utio
ns-
sta
nd
ard
5d
-c 0
10
62
0 U
pd
ate
d C
ovid
-19
sw
ab
flo
wch
art
fo
r
ICU
s C
ha
iley
5e
. p
atie
nts
with
su
sp
ecte
d C
OV
ID-1
9 a
re te
ste
d
pro
mp
tly.
5e
-a Q
uic
k g
uid
e f
or
CO
VID
-19
pa
tie
nt te
stin
g V
5-
01
07
20
20
5e
-b C
OV
ID-1
9 s
pe
cim
en
pro
ce
ss V
4 2
02
00
61
2
5e
-c P
HE
_2
01
9-C
OV
ID-
19
_T
estin
g_
Re
qu
est_
Fo
rm_
E2
8
5e
-d 0
10
62
0 U
pd
ate
d C
ovid
-19
sw
ab
flo
wch
art
fo
r
ICU
s C
ha
iley
Th
e m
ajo
rity
of
ca
se
s a
re r
ece
ive
d f
rom
Lo
ca
l A
cu
te T
rusts
bu
t if a
H
CA
ca
se
is
ide
ntifie
d it w
ou
ld b
e in
ve
stig
ate
d a
nd
co
nta
ct tr
acin
g in
itia
ted
.
Ap
pro
pria
te s
ign
ag
e a
nd
tria
ge
arr
an
ge
me
nts
in
pla
ce
at e
ntr
an
ce
s
to U
TC
an
d M
IU a
s w
ell
as v
ia th
e IC
U
ad
mis
sio
n p
roce
ss a
nd
th
ese
are
re
gu
larly
ch
ecke
d b
y S
en
ior
Clin
ica
l S
taff
.
Fro
nt d
oo
rs lo
cke
d w
he
re p
ossib
le a
nd
inte
rco
m s
yste
ms in
pla
ce
Te
stin
g p
roce
sse
s in
pla
ce
an
d c
om
ple
ted
via
lo
ca
l a
cu
te la
bo
rato
ry. S
taff
are
tra
ine
d
in ta
kin
g s
wa
bs a
nd
th
e p
roce
ss is
reite
rate
d o
n th
e P
UL
SE
.
PP
E g
uid
an
ce
atta
ch
ed
pro
vid
es th
e
na
rra
tive
th
at is
in
eve
ry v
ers
ion
of
pd
f
gu
ida
nce
re
latin
g to
ma
sk u
sa
ge
fo
r
su
sp
ecte
d in
div
idu
als
.
Th
e IC
Us h
ave
sin
gle
ro
om
s a
nd
Ba
ys
En
viro
nm
en
tal risk a
sse
ssm
en
ts
IPC
Bo
ard
As
su
ran
ce
Fra
me
wo
rk
5. E
ns
ure
pro
mp
t id
en
tifi
ca
tio
n o
f p
eo
ple
wh
o h
ave
or
are
at
ris
k o
f d
eve
lop
ing
an
in
fec
tio
n s
o t
ha
t th
ey r
ec
eiv
e t
ime
ly a
nd
ap
pro
pri
ate
tre
atm
en
t to
re
du
ce
th
e r
isk
of
tra
ns
mit
tin
g in
fec
tio
n t
o
oth
er
pe
op
le
Na
rra
tive
Mit
iga
tin
g A
cti
on
s
8T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
Page 76 of 300
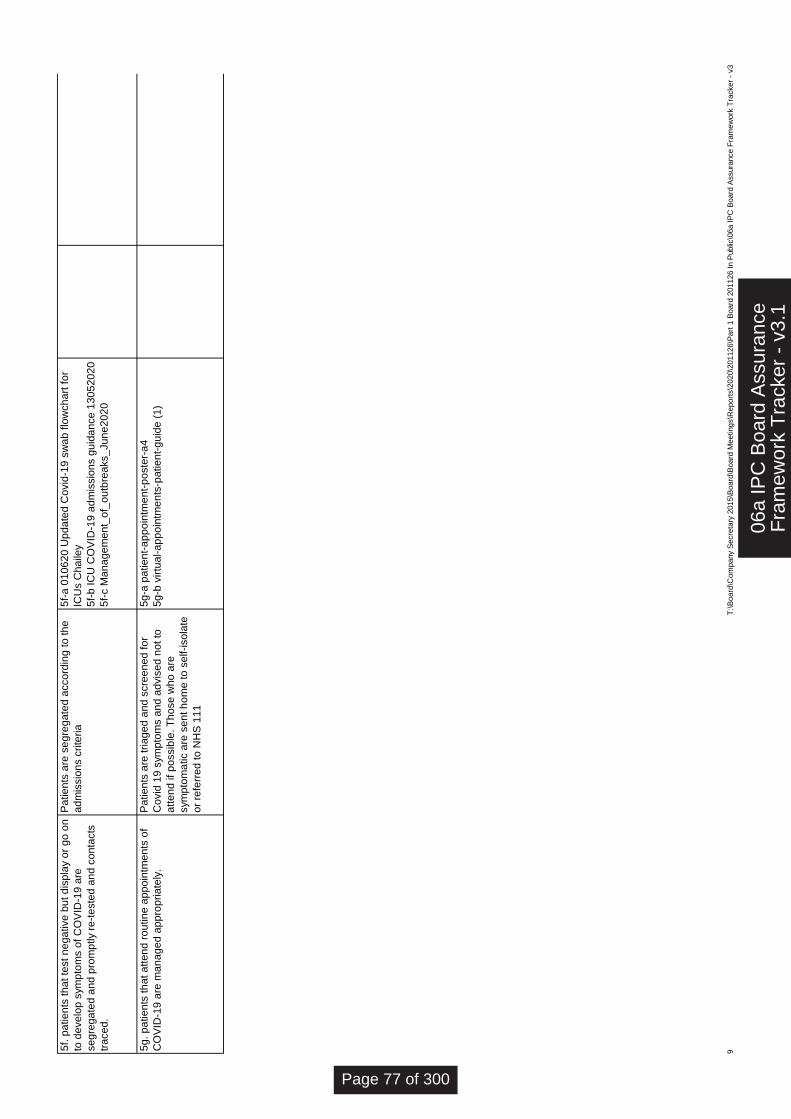
5f.
pa
tie
nts
th
at te
st n
eg
ative
bu
t d
isp
lay o
r g
o o
n
to d
eve
lop
sym
pto
ms o
f C
OV
ID-1
9 a
re
se
gre
ga
ted
an
d p
rom
ptly r
e-t
este
d a
nd
co
nta
cts
tra
ce
d.
5f-
a 0
10
62
0 U
pd
ate
d C
ovid
-19
sw
ab
flo
wch
art
fo
r
ICU
s C
ha
iley
5f-
b IC
U C
OV
ID-1
9 a
dm
issio
ns g
uid
an
ce
13
05
20
20
5f-
c M
an
ag
em
en
t_o
f_o
utb
rea
ks_
Ju
ne
20
20
5g
. p
atie
nts
th
at a
tte
nd
ro
utin
e a
pp
oin
tme
nts
of
CO
VID
-19
are
ma
na
ge
d a
pp
rop
ria
tely
.
5g
-a p
atie
nt-
ap
po
intm
en
t-p
oste
r-a
4
5g
-b v
irtu
al-a
pp
oin
tme
nts
-pa
tie
nt-
gu
ide
(1
)
Pa
tie
nts
are
tria
ge
d a
nd
scre
en
ed
fo
r
Co
vid
19
sym
pto
ms a
nd
ad
vis
ed
no
t to
atte
nd
if
po
ssib
le. T
ho
se
wh
o a
re
sym
pto
ma
tic a
re s
en
t h
om
e to
se
lf-iso
late
or
refe
rre
d to
NH
S 1
11
Pa
tie
nts
are
se
gre
ga
ted
acco
rdin
g to
th
e
ad
mis
sio
ns c
rite
ria
9T
:\B
oard
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meeting
s\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 77 of 300
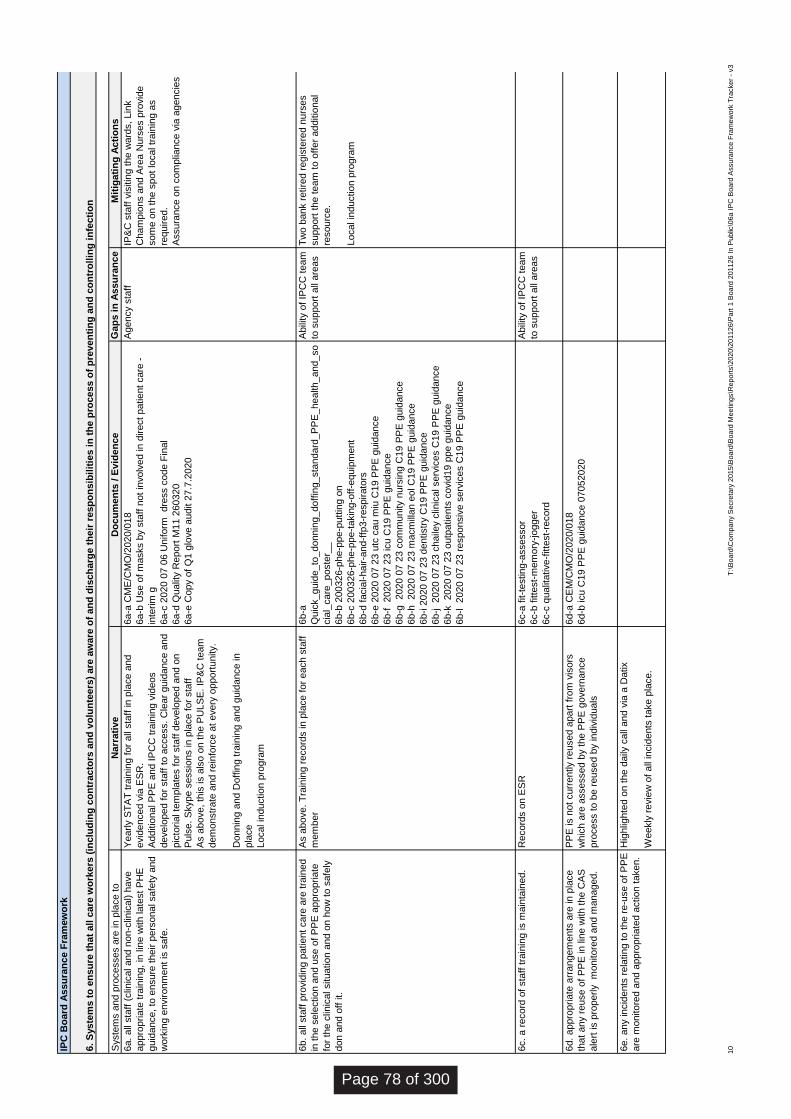
Syste
ms a
nd p
rocesses a
re in
pla
ce t
o
ensure
:
Do
cu
men
ts /
Evid
en
ce
6a.
all
sta
ff (
clin
ical and n
on-c
linic
al) h
ave
appro
priate
tra
inin
g,
in lin
e w
ith late
st
PH
E
guid
ance,
to e
nsure
their p
ers
onal safe
ty a
nd
work
ing e
nvironm
ent
is s
afe
.
6a-a
CM
E/C
MO
/2020/0
18
6a-b
Use o
f m
asks b
y s
taff
not
involv
ed in
direct
patie
nt
care
-
inte
rim
g
6a-c
2020 0
7 0
6 U
niform
dre
ss c
ode F
inal
6a-d
Qualit
y R
eport
M11 2
60320
6a-e
Copy o
f Q
1 g
love a
udit 2
7.7
.2020
6b.
all
sta
ff p
rovid
ing p
atie
nt
care
are
tra
ined
in t
he s
ele
ctio
n a
nd u
se o
f P
PE
appro
pria
te
for
the c
linic
al situatio
n a
nd o
n h
ow
to s
afe
ly
don a
nd o
ff it.
6b-a
Quic
k_guid
e_to
_donnin
g_doff
ing_sta
ndard
_P
PE
_health_and_so
cia
l_care
_poste
r__
6b-b
200326-p
he-p
pe-p
utt
ing o
n
6b-c
200326-p
he-p
pe-t
akin
g-o
ff-e
quip
ment
6b-d
facia
l-hair-a
nd-f
fp3-r
espirato
rs
6b-e
2020 0
7 2
3 u
tc c
au m
iu C
19 P
PE
guid
ance
6b-f
2020 0
7 2
3 icu C
19 P
PE
guid
ance
6b-g
2020 0
7 2
3 c
om
munity n
urs
ing C
19 P
PE
guid
ance
6b-h
2020 0
7 2
3 m
acm
illa
n e
ol C
19 P
PE
guid
ance
6b-i 2
020 0
7 2
3 d
entistr
y C
19 P
PE
guid
ance
6b-j
2020 0
7 2
3 c
haile
y c
linic
al serv
ices C
19 P
PE
guid
ance
6b-k
2020 0
7 2
3 o
utp
atie
nts
covid
19 p
pe g
uid
ance
6b-l
2020 0
7 2
3 r
esponsiv
e s
erv
ices C
19 P
PE
guid
ance
6c.
a r
ecord
of
sta
ff t
rain
ing is m
ain
tain
ed.
6c-a
fit-t
estin
g-a
ssessor
6c-b
fitte
st-
mem
ory
-jo
gger
6c-c
qualit
ative-f
itte
st-
record
6d.
appro
pria
te a
rrangem
ents
are
in
pla
ce
that
any r
euse o
f P
PE
in
lin
e w
ith t
he C
AS
ale
rt is p
roperly
monitore
d a
nd m
anaged.
6d-a
CE
M/C
MO
/2020/0
18
6d-b
icu C
19 P
PE
guid
ance 0
7052020
6e.
any in
cid
ents
rela
tin
g t
o t
he r
e-u
se o
f P
PE
are
monitore
d a
nd a
ppro
pria
ted a
ctio
n t
aken.
Hig
hlig
hte
d o
n t
he d
aily
call
and v
ia a
Datix
Weekly
revie
w o
f all
incid
ents
take p
lace.
Record
s o
n E
SR
Abili
ty o
f IP
CC
team
to s
upport
all
are
as
PP
E is n
ot
curr
ently r
eused a
part
fro
m v
isors
whic
h a
re a
ssessed b
y t
he P
PE
govern
ance
pro
cess t
o b
e r
eused b
y in
div
iduals
Yearly S
TA
T t
rain
ing f
or
all
sta
ff in
pla
ce a
nd
evid
enced v
ia E
SR
.
Additio
nal P
PE
and I
PC
C t
rain
ing v
ideos
develo
ped f
or
sta
ff t
o a
ccess.
Cle
ar
guid
ance a
nd
pic
toria
l te
mpla
tes f
or
sta
ff d
evelo
ped a
nd o
n
Puls
e.
Skype s
essio
ns in
pla
ce f
or
sta
ff
As a
bove,
this
is a
lso o
n t
he P
ULS
E.
IP&
C t
eam
dem
onstr
ate
and r
ein
forc
e a
t every
opport
unity.
Donnin
g a
nd D
off
ing t
rain
ing a
nd g
uid
ance in
pla
ce
Local in
ductio
n p
rogra
m
Agency s
taff
IP&
C s
taff
vis
itin
g t
he w
ard
s,
Lin
k
Cham
pio
ns a
nd A
rea N
urs
es p
rovid
e
som
e o
n t
he s
pot
local tr
ain
ing a
s
required.
Assura
nce o
n c
om
plia
nce v
ia a
gencie
s
As a
bove.
Tra
inin
g r
ecord
s in
pla
ce f
or
each s
taff
mem
ber
Abili
ty o
f IP
CC
team
to s
upport
all
are
as
Tw
o b
ank r
etire
d r
egis
tere
d n
urs
es
support
the t
eam
to o
ffer
additio
nal
resourc
e.
Local in
ductio
n p
rogra
m
IPC
Bo
ard
Assu
ran
ce F
ram
ew
ork
6.
Syste
ms t
o e
ns
ure
th
at
all
care
wo
rkers
(in
clu
din
g c
on
tracto
rs a
nd
vo
lun
teers
) are
aw
are
of
an
d d
isch
arg
e t
heir
resp
on
sib
ilit
ies i
n t
he
pro
cess o
f p
reven
tin
g a
nd
co
ntr
oll
ing
in
fecti
on
Narr
ati
ve
Gap
s i
n A
ssu
ran
ce
Mit
iga
tin
g A
cti
on
s
10
T:\
Board
\Com
pany
Secre
tary
2015\B
oard
\Board
Meetings\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
Page 78 of 300
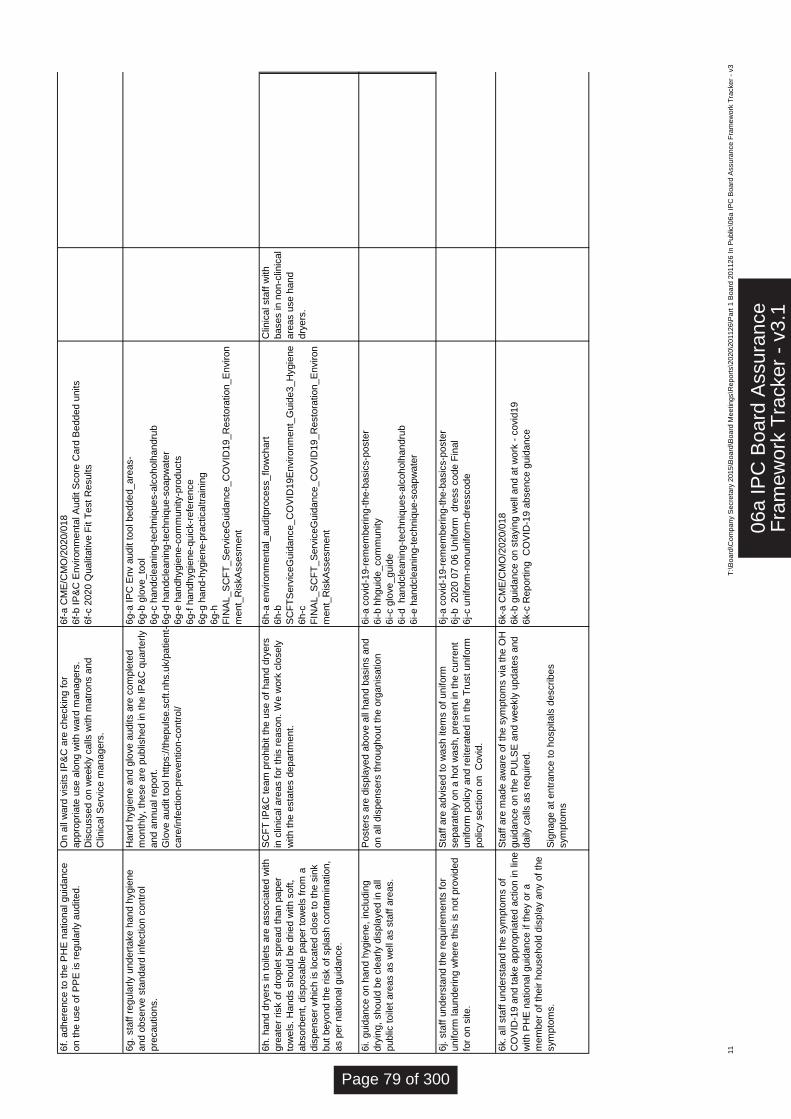
6f.
adhere
nce t
o t
he P
HE
natio
nal guid
ance
on t
he u
se o
f P
PE
is r
egula
rly a
udited.
6f-
a C
ME
/CM
O/2
020/0
18
6f-
b I
P&
C E
nvironm
enta
l A
udit S
core
Card
Bedded u
nits
6f-
c 2
020 Q
ualit
ative F
it T
est
Results
6g.
sta
ff r
egula
rly u
ndert
ake h
and h
ygie
ne
and o
bserv
e s
tandard
in
fectio
n c
ontr
ol
pre
cautio
ns.
6g-a
IP
C E
nv a
udit t
ool bedded_are
as-
6g-b
glo
ve_to
ol
6g-c
handcle
anin
g-t
echniq
ues-a
lcoholh
andru
b
6g-d
handcle
anin
g-t
echniq
ue-s
oapw
ate
r
6g-e
handhygie
ne-c
om
munity-p
roducts
6g-f
handhygie
ne-q
uic
k-r
efe
rence
6g-g
hand-h
ygie
ne-p
racticaltra
inin
g
6g-h
FIN
AL_S
CF
T_
Se
rvic
eG
uid
ance_C
OV
ID19_R
esto
ratio
n_E
nviron
ment_
Ris
kA
ssesm
ent
6h.
hand d
ryers
in
toile
ts a
re a
ssocia
ted w
ith
gre
ate
r risk o
f dro
ple
t spre
ad t
han p
aper
tow
els
. H
ands s
hould
be d
rie
d w
ith s
oft
,
absorb
ent,
dis
posable
paper
tow
els
fro
m a
dis
penser
whic
h is lo
cate
d c
lose t
o t
he s
ink
but
beyond t
he r
isk o
f spla
sh c
onta
min
atio
n,
as p
er
natio
nal guid
ance.
6h-a
environm
enta
l_auditpro
cess_flo
wchart
6h-b
SC
FT
Serv
iceG
uid
ance_C
OV
ID19E
nvironm
ent_
Guid
e3_H
ygie
ne
6h-c
FIN
AL_S
CF
T_
Se
rvic
eG
uid
ance_C
OV
ID19_R
esto
ratio
n_E
nviron
ment_
Ris
kA
ssesm
ent
Clin
ical sta
ff w
ith
bases in
non-c
linic
al
are
as u
se h
and
dry
ers
.
6i. g
uid
ance o
n h
and h
ygie
ne,
inclu
din
g
dry
ing,
should
be c
learly d
ispla
yed in
all
public
toile
t are
as a
s w
ell
as s
taff
are
as.
6i-a c
ovid
-19-r
em
em
berin
g-t
he-b
asic
s-p
oste
r
6i-b h
hguid
e_com
munity
6i-c g
love_guid
e
6i-d
handcle
anin
g-t
echniq
ues-a
lcoholh
andru
b
6i-e h
andcle
anin
g-t
echniq
ue-s
oapw
ate
r
6j. s
taff
unders
tand t
he r
equirem
ents
for
uniform
la
underin
g w
here
this
is n
ot
pro
vid
ed
for
on s
ite.
6j-a c
ovid
-19-r
em
em
berin
g-t
he-b
asic
s-p
oste
r
6j-b
2020 0
7 0
6 U
niform
dre
ss c
ode F
inal
6j-c u
niform
-nonuniform
-dre
sscode
6k.
all
sta
ff u
nders
tand t
he s
ym
pto
ms o
f
CO
VID
-19 a
nd t
ake a
ppro
pria
ted a
ctio
n in
lin
e
with P
HE
natio
nal guid
ance if
they o
r a
mem
ber
of
their h
ousehold
dis
pla
y a
ny o
f th
e
sym
pto
ms.
6k-a
CM
E/C
MO
/2020/0
18
6k-b
guid
ance o
n s
tayin
g w
ell
and a
t w
ork
- c
ovid
19
6k-c
Report
ing
CO
VID
-19 a
bsence g
uid
ance
Sta
ff a
re m
ade a
ware
of
the s
ym
pto
ms v
ia t
he O
H
guid
ance o
n t
he P
ULS
E a
nd w
eekly
update
s a
nd
daily
calls
as r
equired.
Sig
nage a
t entr
ance t
o h
ospitals
describ
es
sym
pto
ms
Hand h
ygie
ne a
nd g
love a
udits a
re c
om
ple
ted
month
ly,
these a
re p
ublis
hed in
the I
P&
C q
uart
erly
and a
nnual re
port
.
Glo
ve a
udit t
ool htt
ps:/
/thepuls
e.s
cft
.nhs.u
k/p
atie
nt-
care
/in
fectio
n-p
reventio
n-c
ontr
ol/
Sta
ff a
re a
dvis
ed t
o w
ash ite
ms o
f uniform
separa
tely
on a
hot
wash,
pre
sent
in t
he c
urr
ent
uniform
polic
y a
nd r
eitera
ted in
the T
rust
uniform
polic
y s
ectio
n o
n
Covid
.
SC
FT
IP
&C
team
pro
hib
it t
he u
se o
f hand d
ryers
in c
linic
al are
as f
or
this
reason.
We w
ork
clo
sely
with t
he e
sta
tes d
epart
ment.
Poste
rs a
re d
ispla
yed a
bove a
ll hand b
asin
s a
nd
on a
ll dis
pensers
thro
ughout
the o
rganis
atio
n
On a
ll w
ard
vis
its I
P&
C a
re c
heckin
g f
or
appro
priate
use a
long w
ith w
ard
managers
.
Dis
cussed o
n w
eekly
calls
with m
atr
ons a
nd
Clin
ical S
erv
ice m
anagers
.
11
T:\
Board
\Com
pany
Secre
tary
2015\B
oard
\Board
Meetings\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 79 of 300
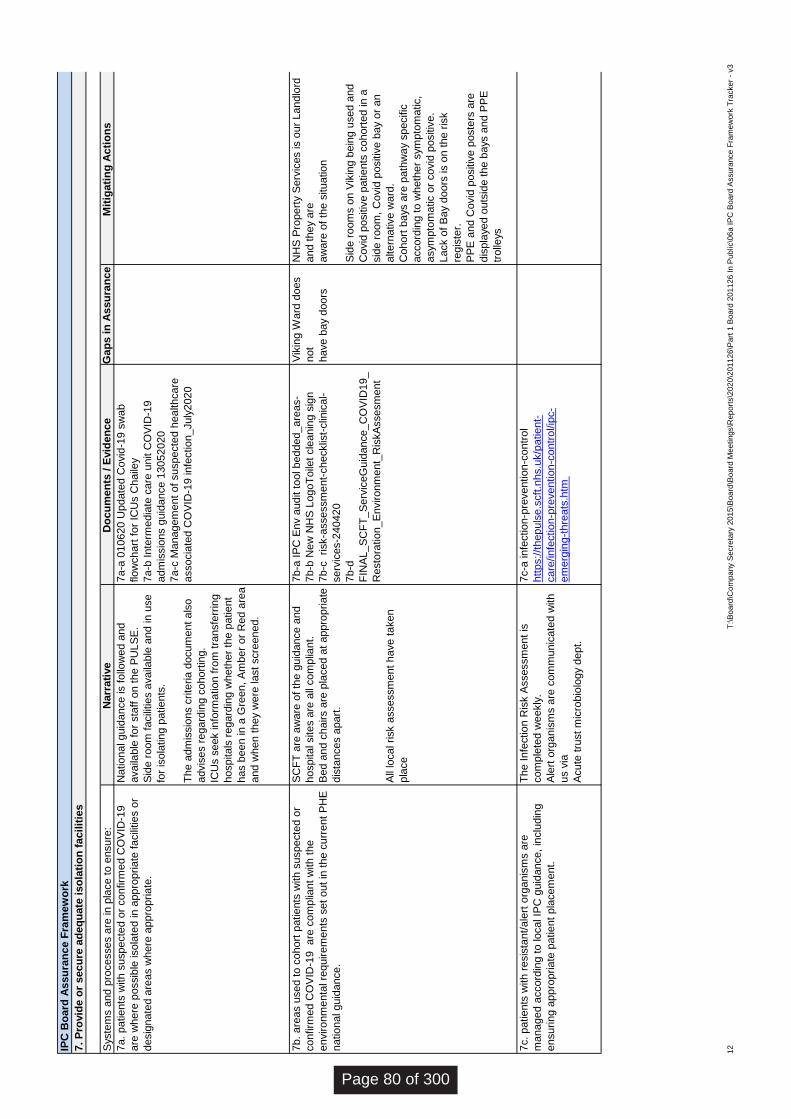
Syste
ms a
nd
pro
ce
sse
s a
re in
pla
ce t
o e
nsu
re:
Do
cu
me
nts
/ E
vid
en
ce
7a.
patie
nts
with
su
spe
cte
d o
r co
nfirm
ed C
OV
ID-1
9
are
wh
ere
possib
le iso
late
d in
app
rop
ria
te f
acili
tie
s o
r
desig
na
ted a
rea
s w
here
app
rop
ria
te.
7a-a
010
62
0 U
pda
ted C
ovid
-19
sw
ab
flo
wch
art
fo
r IC
Us C
haile
y
7a-b
In
term
edia
te c
are
unit C
OV
ID-1
9
adm
issio
ns g
uid
an
ce 1
30
52
02
0
7a-c
Ma
na
ge
me
nt
of
su
spe
cte
d h
ea
lth
care
associa
ted C
OV
ID-1
9 in
fectio
n_
July
202
0
7b.
are
as u
sed
to
co
ho
rt p
atie
nts
with
su
spe
cte
d o
r
co
nfirm
ed C
OV
ID-1
9
are
co
mp
liant
with
th
e
enviro
nm
enta
l re
qu
ire
me
nts
se
t o
ut
in t
he c
urr
ent
PH
E
natio
na
l g
uid
an
ce.
7b-a
IP
C E
nv a
ud
it t
ool b
ed
de
d_
are
as-
7b-b
Ne
w N
HS
Log
oT
oile
t cle
an
ing s
ign
7b-c
risk-a
ssessm
ent-
ch
ecklis
t-clin
ica
l-
se
rvic
es-2
40
42
0
7b-d
FIN
AL
_S
CF
T_
Se
rvic
eG
uid
an
ce_
CO
VID
19_
Re
sto
ratio
n_
En
viro
nm
ent_
Ris
kA
sse
sm
ent
7c.
patie
nts
with
re
sis
tant/
ale
rt o
rga
nis
ms a
re
ma
na
ge
d a
ccord
ing t
o lo
cal IP
C g
uid
an
ce,
inclu
din
g
ensu
ring
app
rop
ria
te p
atie
nt
pla
cem
ent.
7c-a
in
fectio
n-p
reve
ntion
-co
ntr
ol
htt
ps:/
/th
ep
uls
e.s
cft
.nhs.u
k/p
atie
nt-
ca
re/in
fectio
n-p
reve
ntion
-co
ntr
ol/ip
c-
em
erg
ing-t
hre
ats
.htm
The
In
fectio
n R
isk A
sse
ssm
ent
is
co
mp
lete
d w
eekly
.
Ale
rt o
rga
nis
ms a
re c
om
mu
nic
ate
d w
ith
us v
ia
Acu
te t
rust
mic
robio
logy d
ep
t.
Na
tio
na
l g
uid
an
ce is f
ollo
we
d a
nd
availa
ble
fo
r sta
ff o
n t
he P
UL
SE
.
Sid
e r
oom
fa
cili
tie
s a
vaila
ble
and
in
use
for
iso
latin
g p
atie
nts
.
The
adm
issio
ns c
rite
ria d
ocu
me
nt
als
o
advis
es r
ega
rdin
g c
oho
rtin
g.
ICU
s s
eek in
form
atio
n f
rom
tra
nsfe
rrin
g
hosp
ita
ls r
ega
rdin
g w
heth
er
the p
atie
nt
has b
ee
n in
a G
reen
, A
mb
er
or
Re
d a
rea
and
wh
en
th
ey w
ere
la
st
scre
en
ed
.
SC
FT
are
aw
are
of
the g
uid
an
ce a
nd
hosp
ita
l site
s a
re a
ll co
mp
liant.
Be
d a
nd
ch
airs a
re p
laced
at
app
rop
ria
te
dis
tance
s a
pa
rt.
All
local risk a
ssessm
ent
have
ta
ke
n
pla
ce
Vik
ing W
ard
doe
s
not
have
bay d
oo
rs
NH
S P
rope
rty S
erv
ices is o
ur
Lan
dlo
rd
and
th
ey a
re
aw
are
of
the s
itu
atio
n
Sid
e r
oom
s o
n V
ikin
g b
ein
g u
sed
and
Co
vid
positiv
e p
atie
nts
co
ho
rte
d in
a
sid
e r
oom
, C
ovid
positiv
e b
ay o
r a
n
alte
rna
tive
wa
rd.
Co
ho
rt b
ays a
re p
ath
wa
y s
pecific
accord
ing t
o w
heth
er
sym
pto
ma
tic,
asym
pto
ma
tic o
r co
vid
positiv
e.
Lack o
f B
ay d
oo
rs is o
n t
he r
isk
regis
ter.
PP
E a
nd
Co
vid
positiv
e p
oste
rs a
re
dis
pla
ye
d o
uts
ide t
he b
ays a
nd
PP
E
tro
lleys
IPC
Bo
ard
As
su
ran
ce F
ram
ew
ork
7.
Pro
vid
e o
r s
ec
ure
ad
eq
uate
is
ola
tio
n f
acil
itie
s
Na
rra
tive
G
ap
s i
n A
ssu
ran
ce
Mit
igati
ng
Ac
tio
ns
12
T:\
Bo
ard
\Com
pa
ny S
ecre
tary
20
15
\Boa
rd\B
oa
rd M
ee
ting
s\R
ep
ort
s\2
02
0\2
01
12
6\P
art
1 B
oa
rd 2
01
12
6 I
n P
ub
lic\0
6a
IP
C B
oa
rd A
ssura
nce
Fra
me
wo
rk T
racker
- v3
Page 80 of 300
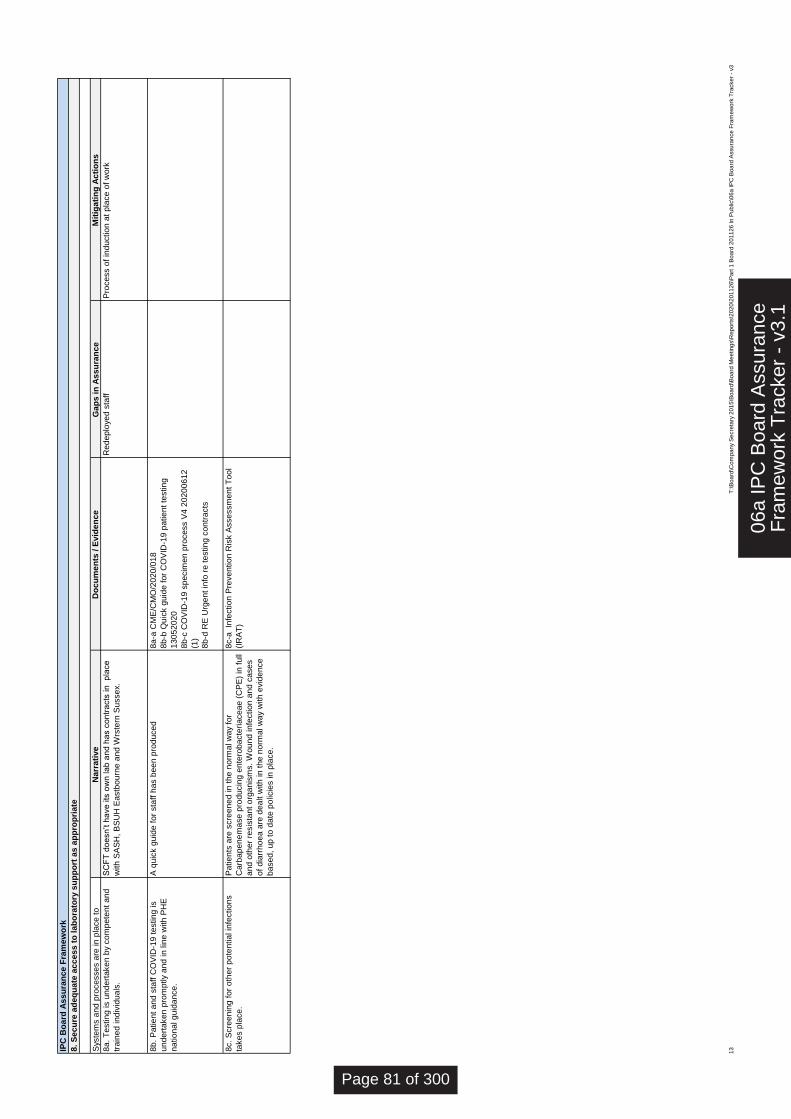
Syste
ms a
nd
pro
ce
sse
s a
re in
pla
ce
to
en
su
re:
Do
cu
me
nts
/ E
vid
en
ce
G
ap
s i
n A
ss
ura
nc
e
8a
. T
estin
g is u
nd
ert
ake
n b
y c
om
pe
ten
t a
nd
tra
ine
d in
div
idu
als
.
Red
ep
loye
d s
taff
8b
. P
atie
nt
an
d s
taff
CO
VID
-19
te
stin
g is
un
de
rta
ke
n p
rom
ptly a
nd
in
lin
e w
ith
PH
E
na
tio
na
l g
uid
an
ce
.
8a
-a C
ME
/CM
O/2
02
0/0
18
8b
-b Q
uic
k g
uid
e f
or
CO
VID
-19
pa
tie
nt
testin
g
13
05
20
20
8b
-c C
OV
ID-1
9 s
pe
cim
en
pro
ce
ss V
4 2
02
00
61
2
(1)
8b
-d R
E U
rge
nt
info
re
te
stin
g c
on
tra
cts
8c.
Scre
en
ing
fo
r o
the
r p
ote
ntia
l in
fectio
ns
take
s p
lace
.
8c-a
In
fectio
n P
reve
ntio
n R
isk A
sse
ssm
en
t T
oo
l
(IR
AT
)
Pa
tie
nts
are
scre
en
ed
in
th
e n
orm
al w
ay f
or
Carb
ap
en
em
ase
pro
du
cin
g e
nte
rob
acte
ria
ce
ae
(C
PE
) in
fu
ll
an
d o
the
r re
sis
tan
t o
rga
nis
ms.
Wo
un
d in
fectio
n a
nd
ca
se
s
of
dia
rrh
oe
a a
re d
ea
lt w
ith
in
th
e n
orm
al w
ay w
ith
evid
en
ce
ba
se
d,
up
to
da
te p
olic
ies in
pla
ce
.
A q
uic
k g
uid
e f
or
sta
ff h
as b
ee
n p
rod
uce
d
SC
FT
do
esn
’t h
ave
its
ow
n la
b a
nd
ha
s c
on
tra
cts
in
p
lace
with
SA
SH
, B
SU
H E
astb
ou
rne
an
d W
rste
rn S
usse
x.
Pro
ce
ss o
f in
du
ctio
n a
t p
lace
of
work
IPC
Bo
ard
As
su
ran
ce
Fra
me
wo
rk
8.
Se
cu
re a
de
qu
ate
ac
ce
ss
to
la
bo
rato
ry s
up
po
rt a
s a
pp
rop
ria
te
Narr
ati
ve
M
itig
ati
ng
Ac
tio
ns
13
T:\B
oa
rd\C
om
pa
ny
Se
cre
tary
20
15
\Bo
ard
\Bo
ard
Me
etin
gs\R
ep
ort
s\2
02
0\2
01
12
6\P
art
1 B
oa
rd 2
01
12
6 In
Pu
blic
\06
a IP
C B
oa
rd A
ssu
ran
ce
Fra
me
wo
rk T
racke
r -
v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 81 of 300
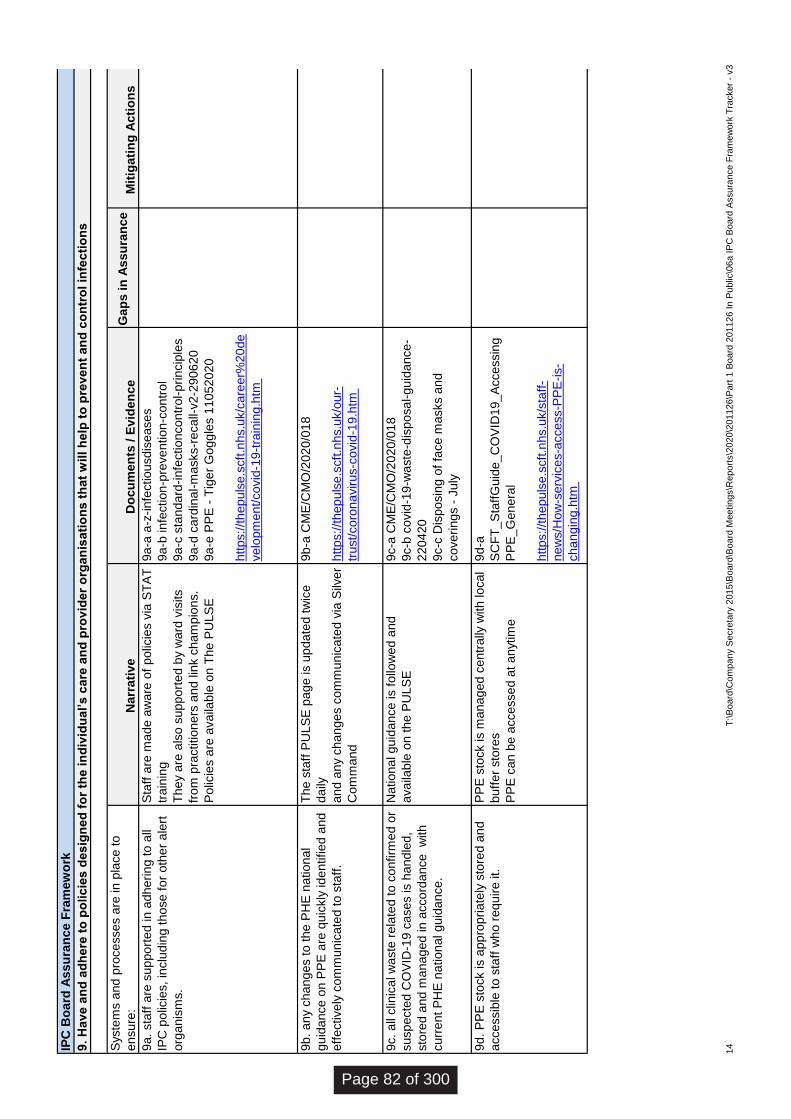
Syste
ms a
nd
pro
ce
sses a
re in p
lace
to
en
sure
:D
ocu
men
ts /
Evid
en
ce
9a
. sta
ff a
re s
up
po
rte
d in a
dh
eri
ng
to
all
IPC
po
licie
s,
inclu
din
g t
hose
for
oth
er
ale
rt
org
anis
ms.
9a
-a a
-z-i
nfe
ctiou
sdis
ease
s
9a
-b infe
ction
-pre
ve
ntion
-con
trol
9a
-c s
tand
ard
-infe
ction
con
trol-
pri
ncip
les
9a
-d c
ard
inal-
masks-r
eca
ll-v2
-29
06
20
9a
-e P
PE
- T
ige
r G
ogg
les 1
10
52
02
0
htt
ps://t
hep
uls
e.s
cft
.nhs.u
k/c
are
er%
20
de
velo
pm
en
t/co
vid
-19
-tra
inin
g.h
tm
9b
. a
ny c
han
ge
s to
th
e P
HE
nation
al
gu
ida
nce
on P
PE
are
qu
ickly
ide
ntified
and
eff
ectively
co
mm
un
icate
d t
o s
taff
.
9b
-a C
ME
/CM
O/2
02
0/0
18
htt
ps://t
hep
uls
e.s
cft
.nhs.u
k/o
ur-
trust/
co
ron
avir
us-c
ovid
-19
.htm
9c.
all
clin
ica
l w
aste
rela
ted t
o c
onfirm
ed
or
susp
ecte
d C
OV
ID-1
9 c
ases is h
and
led
,
sto
red
and
man
ag
ed
in a
cco
rda
nce
w
ith
curr
en
t P
HE
nation
al g
uid
an
ce.
9c-a
CM
E/C
MO
/202
0/0
18
9c-b
covid
-19
-waste
-dis
posa
l-gu
ida
nce
-
22
04
20
9c-c
Dis
po
sin
g o
f fa
ce
masks a
nd
cove
ring
s -
Ju
ly
9d
. P
PE
sto
ck is a
pp
rop
riate
ly s
tore
d a
nd
acce
ssib
le t
o s
taff
who
req
uir
e it.
9d
-a
SC
FT
_S
taff
Gu
ide
_C
OV
ID19_
Accessin
g
PP
E_G
en
era
l
htt
ps://t
hep
uls
e.s
cft
.nhs.u
k/s
taff
-
ne
ws/H
ow
-serv
ices-a
cce
ss-P
PE
-is-
cha
ng
ing
.htm
Natio
na
l gu
ida
nce
is f
ollo
wed
and
ava
ilable
on t
he P
ULS
E
PP
E s
tock is m
an
ag
ed
ce
ntr
ally
with loca
l
bu
ffer
sto
res
PP
E c
an b
e a
ccesse
d a
t a
nytim
e
Sta
ff a
re m
ad
e a
ware
of
polic
ies v
ia S
TA
T
train
ing
The
y a
re a
lso
su
pp
ort
ed b
y w
ard
vis
its
from
pra
ctition
ers
and
lin
k c
ham
pio
ns.
Polic
ies a
re a
va
ilable
on T
he
PU
LS
E
The
sta
ff P
ULS
E p
ag
e is u
pda
ted t
wic
e
da
ily
an
d a
ny c
han
ge
s c
om
mun
icate
d v
ia S
ilver
Com
man
d
IPC
Bo
ard
Ass
ura
nce
Fra
mew
ork
9.
Hav
e a
nd
ad
here
to
po
lic
ies d
es
ign
ed
fo
r th
e i
nd
ivid
ual’
s c
are
an
d p
rovid
er
org
an
isati
on
s t
hat
will
help
to
pre
ven
t a
nd
co
ntr
ol in
fec
tio
ns
Narr
ati
ve
Ga
ps i
n A
ss
ura
nce
M
itig
ati
ng
Acti
on
s
14
T:\
Board
\Com
pany S
ecre
tary
2015\B
oard
\Board
Meetings\R
eport
s\2
020\2
01126\P
art
1 B
oard
201126 I
n P
ublic
\06a I
PC
Board
Assura
nce F
ram
ew
ork
Tra
cker
- v3
Page 82 of 300
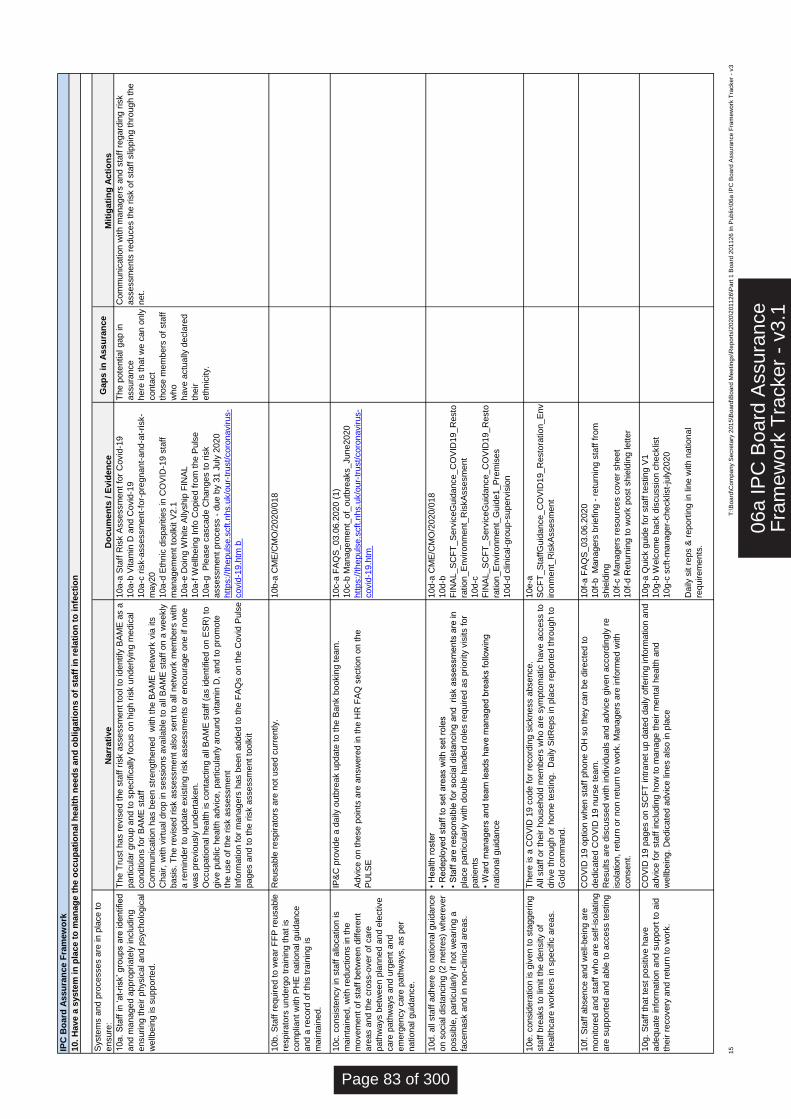
Syste
ms a
nd p
rocesses a
re in p
lace t
o
ensure
:D
ocu
men
ts /
Evid
en
ce
Gap
s i
n A
ssu
ran
ce
10a.
Sta
ff in ‘at-
risk’ gro
ups a
re identified
and m
anaged a
ppro
priate
ly inclu
din
g
ensuring t
heir p
hysic
al and p
sycholo
gic
al
wellb
ein
g is s
upport
ed.
10a-a
Sta
ff R
isk A
ssessm
ent
for
Covid
-19
10a-b
Vitam
in D
and C
ovid
-19
10a-c
ris
k-a
ssessm
ent-
for-
pre
gnant-
and-a
t-risk-
may20
10a-d
Eth
nic
dis
parities in C
OV
ID-1
9 s
taff
managem
ent
toolk
it V
2.1
10a-e
Doin
g W
hite A
llyship
FIN
AL
10a-f
Wellb
ein
g Info
Copie
d f
rom
the P
uls
e
10a-g
P
lease c
ascade C
hanges t
o r
isk
assessm
ent
pro
cess -
due b
y 3
1 J
uly
2020
htt
ps:/
/thepuls
e.s
cft
.nhs.u
k/o
ur-
trust/
coro
navirus-
covid
-19.h
tm b
The p
ote
ntial gap in
assura
nce
here
is t
hat
we c
an o
nly
conta
ct
those m
em
bers
of
sta
ff
who
have a
ctu
ally
decla
red
their
eth
nic
ity.
10b.
Sta
ff r
equired t
o w
ear
FF
P r
eusable
respirato
rs u
nderg
o t
rain
ing t
hat
is
com
plia
nt
with P
HE
national guid
ance
and a
record
of
this
tra
inin
g is
main
tain
ed.
10b-a
CM
E/C
MO
/2020/0
18
10c.
consis
tency in s
taff
allo
cation is
main
tain
ed,
with r
eductions in t
he
movem
ent
of
sta
ff b
etw
een d
iffe
rent
are
as a
nd t
he c
ross-o
ver
of
care
path
ways b
etw
een p
lanned a
nd e
lective
care
path
ways a
nd u
rgent
and
em
erg
ency c
are
path
ways,
as p
er
national guid
ance.
10c-a
FA
QS
_03.0
6.2
020 (
1)
10c-b
Managem
ent_
of_
outb
reaks_June2020
htt
ps:/
/thepuls
e.s
cft
.nhs.u
k/o
ur-
trust/
coro
navirus-
covid
-19.h
tm
10d.
all
sta
ff a
dhere
to n
ational guid
ance
on s
ocia
l dis
tancin
g (
2 m
etr
es)
where
ver
possib
le,
part
icula
rly if
not
wearing a
facem
ask a
nd in n
on-c
linic
al are
as.
10d-a
CM
E/C
MO
/2020/0
18
10d-b
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Ris
kA
ssesm
ent
10d-c
FIN
AL_S
CF
T_S
erv
iceG
uid
ance_C
OV
ID19_R
esto
ration_E
nvironm
ent_
Guid
e1_P
rem
ises
10d-d
clin
ical-gro
up-s
uperv
isio
n
10e.
consid
era
tion is g
iven t
o s
taggering
sta
ff b
reaks t
o lim
it t
he d
ensity o
f
healthcare
work
ers
in s
pecific
are
as.
10e-a
SC
FT
_S
taff
Guid
ance_C
OV
ID19_R
esto
ration_E
nv
ironm
ent_
Ris
kA
ssesm
ent
10f.
Sta
ff a
bsence a
nd w
ell-
bein
g a
re
monitore
d a
nd s
taff
who a
re s
elf-isola
ting
are
support
ed a
nd a
ble
to a
ccess t
esting
10f-
a F
AQ
S_03.0
6.2
020
10f-
b
Managers
briefing -
retu
rnin
g s
taff
fro
m
shie
ldin
g
10f-
c M
anagers
resourc
es c
over
sheet
10f-
d R
etu
rnin
g t
o w
ork
post
shie
ldin
g lett
er
10g.
Sta
ff t
hat
test
positiv
e h
ave
adequate
info
rmation a
nd s
upport
to a
id
their r
ecovery
and r
etu
rn t
o w
ork
.
10g-a
Quic
k g
uid
e f
or
sta
ff t
esting V
1
10g-b
Welc
om
e b
ack d
iscussio
n c
hecklis
t
10g-c
scft
-manager-
checklis
t-ju
ly2020
Daily
sit r
eps &
report
ing in lin
e w
ith n
ational
requirem
ents
.
• H
ealth r
oste
r
• R
edeplo
yed s
taff
to s
et
are
as w
ith s
et
role
s
• S
taff
are
responsib
le f
or
socia
l dis
tancin
g a
nd
risk a
ssessm
ents
are
in
pla
ce p
art
icula
rly w
ith d
ouble
handed r
ole
s r
equired a
s p
riority
vis
its f
or
patients
• W
ard
managers
and t
eam
leads h
ave m
anaged b
reaks f
ollo
win
g
national guid
ance
CO
VID
19 p
ages o
n S
CF
T intr
anet
up d
ate
d d
aily
off
ering info
rmation a
nd
advic
e f
or
sta
ff inclu
din
g h
ow
to m
anage t
heir m
enta
l health a
nd
wellb
ein
g.
Dedic
ate
d a
dvic
e lin
es a
lso in p
lace
IP&
C p
rovid
e a
daily
outb
reak u
pdate
to t
he B
ank b
ookin
g t
eam
.
Advic
e o
n t
hese p
oin
ts a
re a
nsw
ere
d in t
he H
R F
AQ
section o
n t
he
PU
LS
E
CO
VID
19 o
ption w
hen s
taff
phone O
H s
o t
hey c
an b
e d
irecte
d t
o
dedic
ate
d C
OV
ID 1
9 n
urs
e t
eam
.
Results a
re d
iscussed w
ith indiv
iduals
and a
dvic
e g
iven a
ccord
ingly
re
isola
tion,
retu
rn o
r non r
etu
rn t
o w
ork
. M
anagers
are
info
rmed w
ith
consent.
There
is a
CO
VID
19 c
ode f
or
record
ing s
ickness a
bsence.
All
sta
ff o
r th
eir h
ousehold
mem
bers
who a
re s
ym
pto
matic h
ave a
ccess t
o
drive t
hro
ugh o
r hom
e t
esting.
Daily
SitR
eps in p
lace r
eport
ed t
hro
ugh t
o
Gold
com
mand.
The T
rust
has r
evis
ed t
he s
taff
ris
k a
ssessm
ent
tool to
identify
BA
ME
as a
part
icula
r gro
up a
nd t
o s
pecific
ally
focus o
n h
igh r
isk u
nderlyin
g m
edic
al
conditio
ns f
or
BA
ME
sta
ff
Com
munic
ation h
as b
een s
trength
ened
with t
he B
AM
E n
etw
ork
via
its
Chair,
with v
irtu
al dro
p in s
essio
ns a
vaila
ble
to a
ll B
AM
E s
taff
on a
weekly
basis
. T
he r
evis
ed r
isk a
ssessm
ent
als
o s
ent
to a
ll netw
ork
mem
bers
with
a r
em
inder
to u
pdate
exis
ting r
isk a
ssessm
ents
or
encoura
ge o
ne if
none
was p
revio
usly
undert
aken.
Occupational health is c
onta
cting a
ll B
AM
E s
taff
(as identified o
n E
SR
) to
giv
e p
ublic
health a
dvic
e,
part
icula
rly a
round v
itam
in D
, and t
o p
rom
ote
the u
se o
f th
e r
isk a
ssessm
ent
Info
rmation f
or
managers
has b
een a
dded t
o t
he F
AQ
s o
n t
he C
ovid
Puls
e
pages a
nd t
o t
he r
isk a
ssessm
ent
toolk
it
Com
munic
ation w
ith m
anagers
and s
taff
regard
ing r
isk
assessm
ents
reduces t
he r
isk o
f sta
ff s
lippin
g t
hro
ugh t
he
net.
Reusable
respirato
rs a
re n
ot
used c
urr
ently.
IPC
Bo
ard
Assu
ran
ce F
ram
ew
ork
10.
Have a
syste
m i
n p
lace t
o m
an
ag
e t
he o
ccu
pati
on
al
healt
h n
eed
s a
nd
ob
lig
ati
on
s o
f sta
ff i
n r
ela
tio
n t
o i
nfe
cti
on
Narr
ati
ve
Mit
igati
ng
Acti
on
s
15
T:\B
oa
rd\C
om
pa
ny S
ecre
tary
201
5\B
oa
rd\B
oa
rd M
ee
ting
s\R
ep
ort
s\2
02
0\2
011
26
\Part
1 B
oa
rd 2
011
26
In
Pub
lic\0
6a
IP
C B
oa
rd A
ssura
nce F
ram
ew
ork
Tra
cker
- v3
06a
IPC
Boa
rd A
ssur
ance
Fra
mew
ork
Tra
cker
- v
3.1
Page 83 of 300

BOARD OF DIRECTORS – PUBLIC MEETING
26 November 2020
Agenda Item Number: 07
Report Title: Quality Account 2019/20
Purpose:
Approval X Assurance Discussion Briefing
Summary: Providers of NHS healthcare are required to publish a quality account each year. These are required by the Health Act 2009, and in the terms set out in the National Health Service (Quality Accounts) Regulations 2010 as amended1 (‘the quality accounts regulations’). Compliance is assured when the document is uploaded to the NHS Choices website. Normally the deadline for publication is 30 June; however this year the publication date was postponed due to COVID-19, with a revised publication date of on or before 15 December 2020 given.
Recommendation: The Board is asked to approve the attached Quality Account 2019/20 for publication by the given deadline. Please note, due to the pandemic and to the subsequent delay in publication the Trust’s external auditors were not required this year to produce a substantial assurance report on the contents of the Quality Account.
Previously reviewed by: Quality Improvement Committee
Relevance to Trust’s Strategic Goals: Relevant to all SCFT’s strategic goals: Population Health; Quality Improvement; Patient Experience; Thriving Staff; Value and Sustainability
Relevance to CQC Domains: Relevant to all CQC domains: Safe; Caring; Responsive; Effective; Well Led
Equality and Diversity: The report has been reviewed and there were no equality and diversity issues identified for action or escalation.
Report author: Janet Parfitt, Quality Development Lead (Assurance)
Report owner: Donna Lamb, Chief Nurse
1 SI 2010/279; as amended by the NHS (Quality Accounts) Amendment Regulations 2011 (SI 2011/269, the NHS (Quality Accounts) Amendment Regulations 2012 (SI 2012/3081) and the NHS (Quality Accounts) Amendment Regulations 2017 (SI 2017/744).
07 C
S Q
ualit
y A
ccou
nt 2
0192
0
Page 84 of 300

Quality Account
2019/2020
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 85 of 300

Quality Account 2019/20 Page 2 of 64
Summary Welcome to Sussex Community NHS Foundation Trust’s (SCFT) annual Quality Account, which outlines the quality of our services and priorities for improvement that we will focus on during 2020/21 and reviews our progress against the quality improvement areas that we set ourselves during 2019/20. Despite challenging conditions for the NHS locally and nationally, including responding to COVID-19, SCFT has made good progress on all its priorities for improvement as set out in part 2b.
As the largest community health and care provider in Sussex, our mission is to provide excellent care at the heart of the community. The Trust strives to achieve this mission through a set of five strategic goals:
Quality Improvement Patient Experience Thriving Staff Value and Sustainability Population Health
We provide a wide range of medical, nursing therapeutic and specialist care to over 9,000 children and adults a day. We work to help people plan, manage and adapt to changes in their health, to prevent avoidable admission to hospital and to minimise hospital stay. We care for most people in their own homes or as close to home as possible, such as in our Intermediate Care Units, clinics and other centres. The people we care for are at the centre of everything we do and we work closely with GPs, acute hospitals, local authority social care partners, mental health trusts, charities and voluntary organisations to ensure care is coordinated to meet individual needs.
Every General Practice in England is a member of a Clinical Commissioning Group (CCG). CCGs commission (plan and buy) the majority of health services, including emergency care, elective hospital care, maternity services, and community and mental health services for patients. The CCGs that cover Sussex and Brighton & Hove commission care from SCFT.
SCFT is proud to have staff who continuously strive to improve the care they deliver, thankful to our patients for taking the time to tell us when we got it right, but also where we could do better, and appreciative of our colleagues across the local health economy for working with us to provide a comprehensive and highly effective local health service.
Page 86 of 300

Quality Account 2019/20 Page 3 of 64
Contents
Summary 2 Introduction 4 Part 1 Statement on Quality from the Chief Executive 5 Part 2 Priorities for Improvement and Statements of Assurance from the Board 7 Part 2.1 Priorities for Improvement 7 A Review of our Priorities for Improvement from 2019/20 12 Part 2.2 Statements of Assurance from the Board 19 Clinical Audit 19 Research 25 Commissioning for Quality and Improvement (CQUIN) 26 Care Quality Commission (CQC) 28 NHS Number and General Medical Practice Code Validity 29 Data Security and Protection Report 30 Data Quality 30 Review of Current Data Quality 30 Payment by Results 30 Assurance Processes to Monitor Data Quality and Validity 31 Learning from Deaths 32 Avoidable Deaths 33 Part 2.3 Reporting against Core Indicators 34 Hospital Readmissions (Core Indicator 19) 34 Friends and Family Test (FFT) Staff (Core Indicator 21) 34 Friends and Family Test (FFT) Patient (Core Indicator 21.1) 35 VTE Assessments (Core Indicator 23) 37 Clostridium difficile (Core Indicator 24) 37 Patient Safety Incidents (Core Indicator 25) 38 Incident Reporting 40 Serious Incidents 40 Part 3 Other Information 42 Incomplete pathways within 18 weeks (Mandatory Indicator) 42 Percentage of patients with a total time in Minor Injury Units and Urgent Treatment
Centres (Mandatory Indicator) 43
Medication incidents (Local Indicator) 44 Safe Care 45 Falls 45 Healthcare Associated Infections (HCAIs) 46 Never Events 47 Effective Care 48 Freedom to Speak Up 48 National Institute for Health and Care Excellence (NICE) 49 Guardian of Safe Working 49 Central Alert System 50 Effective Care 51 Complaints 51 Duty of Candour 51 Staff Survey 52 Improving Access to Psychological Therapies (IAPT) 53 Annual Organisational Audit (AOA) on Medical Appraisal and Validation 54 Annex 1 Statements form External Stakeholders 55 Annex 2 Statement of Directors’ Responsibilities for the Quality Account 59 Conclusion 60 Feedback 61 Appendix 1 Glossary of Terms 62
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 87 of 300
Quality Account 2019/20 Page 4 of 64
Introduction NHS Trusts must publish a Quality Account each year, as required by the Health Act 2009, and in the terms set out in the National Health Service (Quality Accounts) Regulations 2010 as amended (‘the quality accounts regulations’). Publication in 2020 has been delayed due to COVID-19 from the usual date at end of June 2020 to15th December 2020.
The Quality Account helps the Trust to improve public accountability for the quality of care we provide using data sources and narrative to explain what that data shows; it also looks back on the priorities for improvement we set ourselves in 2019/20 reporting on the progress we made; and looks forward to the priorities for improvement we have set ourselves to achieve in 2020/21.
Further information on quality accounts can be found on the NHS website https://www.nhs.uk/
1 SI 2010/279; as amended by the NHS (Quality Accounts) Amendments Regulations 2011 (SI 2011/269 and the NHS (Quality Accounts) Amendments Regulations 2012 (SI 2012/3081)
Page 88 of 300
Quality Account 2019/20 Page 5 of 64
Part 1
Statement on Quality from the Chief Executive
I am happy to introduce the Quality Account 2019/20 for Sussex Community NHS Foundation Trust (SCFT). The report gives us an opportunity to reflect on our many quality achievements and successes over the last year. It also enables us to identify areas where we want to focus attention on the agreed priorities for improvement for the coming year, 2020/21. The last year has seen many new challenges for us all, and SCFT has adapted and responded to COVID-19, maintaining a focus on protecting our patients and our staff, whilst supporting the wider system. I am fortunate to be part of an organisation, which has worked tirelessly to care for some of our most vulnerable, whilst also caring for each other.
The high quality care our staff deliver is driven by an organisational culture that embraces the Trust’s values - compassionate care, working together, achieving ambitions, and delivering excellence - all of which are embedded within the Trust’s Performance Development Review (PDR) system for staff. These values have been essential over the last year and I have seen them displayed in abundance.
This year has also reminded us of the importance of valuing difference, and ensuring that everyone should have equity of access to services based on need. As a Trust, we are committed to reducing inequality and driving out any discrimination our patients and families might experience. We will place the voice of both our communities and patients at the heart of our organisation and how we develop services.
We could not have responded to the new challenges this year without our health and social care partners, third sector organisations, SCFT volunteers and other external stakeholders. The focus we place on improving quality will continue to ensure we are able to deliver improvements across organisational boundaries so that patients and their families have joined up care, and they are central to any decisions.
When the Care Quality Commission (CQC) (the independent regulator of health and social care in England) last inspected us at the end of 2017, we achieved an improved ‘Good’ rating with ‘Outstanding’ features. Ratings across all CQC domains for the areas inspected were ‘Good’ and we were rated as ‘Outstanding’ for ‘Caring’ in our community inpatient services and ‘Responsive’ for our community end of life care. Although the inspection planned for March 2020 was cancelled due to COVID-19, the Trust participated in the CQC’s Interim
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 89 of 300

Quality Account 2019/20 Page 6 of 64
Emergency Support Framework during August 2020, which was based on the Trust’s Infection, Prevention and Control Board Assurance Framework. The CQC reported that they took full assurance from this.
In line with national and locally identified areas where improvements to quality could be made, the Trust’s Board of Directors and Council of Governors agreed five new priorities for improvement for 2020/21 and these are detailed in Part 2.1. We developed our priorities for improvement in line with our long-term Trust ambitions and strategies, which are based on patient safety, patient experience and clinical effectiveness, together with discussions with staff and external stakeholders, including patient representatives following a range of engagement events. I am confident that we will rise to the challenges we have set ourselves to improve the patient-centred, safety and effectiveness of the care we deliver to our local population.
On the basis of the process the Trust has in place for the production of the Quality Account, I can confirm that to the best of my knowledge that the information contained within this document is accurate.
Siobhan Melia Chief Executive November 2020
Page 90 of 300

Quality Account 2019/20 Page 7 of 64
Part 2
Priorities for Improvement and Statements of Assurance from the Board
Part 2.1
Priorities for Improvement 2020/21
This section of the Quality Account outlines the annual key priorities for improvement.
Safe Care Violence and Aggression towards NHS staff To further increase our knowledge and understanding of the incidents of physical and verbal abuse SCFT staff experience whilst working so we can keep our staff safe.
Why have we chosen this? How will we achieve this? How will we measure this?
Physical and verbal abuse was the most common type of incident reported by SCFT staff in 2018/19. This reflects the national picture in the NHS and is consistent with benchmarking against other community organisations but staff need to know they are SCFT’s most valuable resource and we want them to be safe at work.
This issue is included as a workforce priority in the Sustainability and Transformation Plan (STP) – with physical and verbal abuse often cited as the reason staff leave the Trust’s employ. It also links with SCFT’s Strategic Goal - Thriving Staff included in the Trust’s Strategy.
A Task & Finish Group (reporting into the Workforce Committee) has been set up to examine such reported incidents to increase our understanding of their causes and effects.
The Trust has included closer monitoring of violence and aggression incidents in quality reports to Board committees and further in-depth analysis of incidents at the Trust’s Health & Safety Committee.
The number of incidents of staff who leave the Trust citing physical and verbal abuse as their reason for leaving will be reduced. Staff will feel safer knowing the Trust is investigating such incidents further.
Specialist Lead: Deputy Director of Human Resources and Occupational Development/Violence and Aggression Task Force Chair
Governance Group:
Health & Safety Committee
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 91 of 300
Quality Account 2019/20 Page 8 of 64
Effective Care Translating research evidence into improved care
Translating research evidence into improved care, specifically the development, implementation and evaluation of a frailty pathway to improve outcomes of care for older people with continued collaborative working with other providers.
This priority for Improvement is a continuation of the five year priority introduced in last year’s Quality Account
Why have we chosen this? How will we achieve this? How will we measure this?
Frailty is associated typically with increasing age. Re-aligning healthcare services to the needs of an ageing population is a national priority. SCFT provides care and services to an increasingly older population across all the geographical areas served. Areas such as Coastal West Sussex have a higher than national average population aged over 80 years. A frailty pathway is a priority area for our ageing population to improve the detection, assessment, case management and outcomes of care; the right care right place right time.
This priority links with SCFT’s Strategic Goal – Quality Improvement included in the Trust’s Strategy
We will work as a multi-disciplinary group of clinical and medical professionals, acute care providers and the CCGs, to enhance continuity of care on frailty assessment and management across healthcare settings.
The development and implementation of the frailty pathway will be informed by national guidance on best practice and research evidence, which will be integrated into clinical practice.
We will work with primary care to support the identification and management of care for people living with frailty and across care settings.
Evaluation will be an ongoing process from development through to implementation.
2020/2021 priorities:
By implementation of and subsequent evaluation of the frailty pathway using the clinical frailty scale and by conducting a staff survey.
Patients will be assured that research undertaken by the Trust focusing on frailty assessment and management will help improve healthcare for our aging population.
Specialist Lead: Honorary Nurse Consultant and Health Education England (HEE)/National Institute for Health Research (NIHR) Senior Clinical Lecturer in Palliative Care
Governance Group:
Frailty Steering Group
Page 92 of 300
Quality Account 2019/20 Page 9 of 64
National Institute for Health and Care Excellence (NICE) Guidance
Revise how the outputs on NICE Guidance are reported, in order to accurately reflect the timescales for the Trust’s NICE processes in a real time manner. Why have we chosen this? How will we achieve this? How will we measure
this?
The current SCFT timescale for implementing NICE guidance is 3 years. Where guidance is relevant to SCFT we will aim to implement within the shortest time practicable.
This will lead to an increase in assurance that patients are receiving the most effective care as soon as possible increasing their confidence that they are receiving excellent care in line with NICE guidance.
This priority links with SCFT’s Strategic Goal – Quality Improvement included in the Trust’s Strategy.
The Quality Development team will review all guidance issued by NICE on a monthly basis for its relevance and where relevant will assign a timescale for implementation within the Trust.
We will assign a graded, rag rated system to guidance; with guidance allocated Red as urgently in need of implementation and to be reviewed within 2 months of issue, Amber to be reviewed within 4 months and Green to be reviewed within 6 months of issue.
All NICE guidance issued throughout the year will be reviewed and assessed for relevance and assigned a timescale for implementation on this merit. The updated performance metric reporting will be reported monthly on SCFT applicability and compliance with NICE guidance.
Patients will be confident that their care is based on best practice.
Specialist Lead: Quality Development Lead (Effectiveness)
Governance Group:
Clinical Effectiveness Group (CEG)
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 93 of 300
Quality Account 2019/20 Page 10 of 64
Patient Centred Care Implementing a system to identify patients with a Learning
Disability who access SCFT services Why have we chosen this? How will we achieve this? How will we measure this?
All teams should be able to make reasonable adjustments to their services so that patients with a learning disability can access the service in an easy way. After a comprehensive benchmarking process, it was noted that SCFT did not have a mechanism to capture, monitor and report how many patients with a Learning Disability accessed our services at any given time.
This priority links with SCFT’s Strategic Goals – Population Health and Patient Experience, both included in the Trust’s Strategy.
The planned SystmOne (SCFT’s electronic patient administration system) roll out across all Trust services is due to be completed at the end of 2020. One of the positive outcomes from the planned roll out of SystmOne will be the ability to identify all patients with a learning disability. This means we are able to capture, monitor and report on the data collected from the system so services are able to make reasonable adjustments
To facilitate this aim, we will also develop link champions in each area and train them to raise awareness so we can meet our patients’ needs appropriately.
We will be able to demonstrate how many patients with a learning disability were seen by Trust services. Each area will have access to a minimum of one link champion.
This will enable the Trust to identify services used by patients with a learning disability and ensure access is enhanced by making reasonable adjustments.
Specialist Lead: Deputy Medical Director
Governance Group:
Trust wide Governance Group (TWGG)
Page 94 of 300
Quality Account 2019/20 Page 11 of 64
To record the protected characteristics of service users who makea complaint about one of SCFT’s services.
Why have we chosen this? How will we achieve this? How will we measure this?
It is important the Trust can accurately evidence the demographics of the patient feedback we receive through the complaints and Patient Advice and Liaison Service (PALS) process to ensure our procedures are equitable and accessible to all. All patients, their families and carers must have confidence that Trust processes are applied equitably to all those for whom we seek to provide excellent patient care.
This priority links with SCFT’s Strategic Goal – Patient Experience included in the Trust’s Strategy.
By reviewing the demographics of people who make a complaint or who contact PALS, we will be able to identify and address any gaps or areas of concerns.
Improvements will be necessary to the way we collect and record data through our existing incident reporting systems (Datix), and on system upgrades (SystmOne) and we will work closely with SCFT’s Datix Lead and SystmOne colleagues to ensure cross system working by the end of the current financial year 2020-21, which will enable accurate reporting.
Once cross system working has been established, we will produce monthly reports from Datix, which will include patient/complainant demographics that will be reviewed at local level through Area Team meetings and at Trust wide level through the Patient Experience Group (PEG) and Trust Wide Governance Group (TWGG).
This will lead to the Trust being able to identify seldom-engaged groups of patients and ensure any barriers experienced are overcome leading to care that is more equitable.
Specialist Lead: Quality Development Manager
Governance Group:
Patient Experience Group (PEG)
We will document progress against these priorities in our Quality Account for 2020/21.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 95 of 300
Quality Account 2019/20 Page 12 of 64
A Review of our Priorities for Improvement from 2019/20 The table below summarises progress against priorities for improvement set for 2019/20 in the 2018/19 Quality Account. Each priority is described and then reviewed on the implementation. Progress summary against 2019/20 priorities for improvement Safe Care Review Of Serious Incidents. We will promote shared learning to patients, relatives, staff and external partners by reviewing the process of recording, monitoring and sharing recommendations for learning following a Serious Incident (SI) investigation. This will reflect the Trust’s culture of ongoing quality improvement and continuous journey to reduce unintended and unexpected patient harm. Why did we choose this? How did we do? Patients, their families and carers want to be assured that when any incident or SI causes them harm, lessons are identified and acted upon and shared with all staff trust-wide.
SCFT is committed to creating a ‘Just Culture’ by listening to staff, learning lessons and so improving patient care as a direct result. Identifying learning from staff who share concerns under the raising concerns process could enable prevention of greater numbers of patient safety events. Just Culture is about creating a culture of fairness, openness and learning in the NHS by making colleagues feel confident to speak up when things go wrong, rather than fearing blame.
Achieved
A Standard Operating Procedure was created; ensuring all tabletop exercises held to review and learn from serious incidents with all the staff involved follow an agreed framework, ensuring all expectations are met. This remains under review, as it has not been possible to devise a tool that fits all cases. This work stream will be progressed to a set of guidelines. In the meantime, guides have been developed to support staff through the SI process and table top exercise.
A staff survey will be developed in 2020/21 as we progress the patient safety strategy post-COVID-19 restoration and a Duty of Candour tracker is being progressed for monthly review at the Serious Incident and Root Cause Analysis Review Group (SIRCAG).
Learning from SIs had been shared via a monthly shared learning document at Area Governance Meetings. This has now progressed to the information being captured in a monthly Patient Safety Newsletter, which is published on the Pulse and cascaded via the Area Nurses, giving a much wider audience for lessons learned.
The numbers of staff raising concerns via the ‘Freedom to Speak Up’ (FTSU) route has increased significantly during 2019/20 (from 55 cases in 2018/19 to 150 cases in 2019/20). This clearly demonstrates an increase in staff awareness of this route to raise concerns.
The recently published National FTSU Index uses 4 questions from the NHS staff survey relating to how staff feel they are treated when involved in errors or incidents and reporting unsafe practice. SCFT was ranked 15th out of all trusts in the country. This confirms SCFT has a positive reporting culture.
Page 96 of 300
Quality Account 2019/20 Page 13 of 64
Children and Young People’s (CYP) Services Safety Thermometer Why did we choose this? How did we do? The CYP Safety Thermometer is a national tool that had been designed to measure commonly occurring harms in people that engage with children and young people's services. The tool focusses on Deterioration, Extravasation, Pain and Skin Integrity. SCFT provides children’s services across a range of areas including community services; bed based and Urgent Treatment Centres/ Minor injury Units and Dentistry; the new CYP Safety Thermometer will enable oversight of safety across all services that children and young people access.
Achieved
CYP Safety Thermometer is a national tool that was designed to measure commonly occurring harms in people that engage with children and young people's services. However, data submitted was never reported on fully and use of the tool (and data collection) ceased nationally in March 2020, with no alternative offered. As the CYP Safety Thermometer was acute focussed and not a direct fit with Children’s Community Nursing (CCN), we continue to monitor elements of it via Datix (SCFT’s on-line incident reporting system).
Deterioration – via Datix report and investigation. Extravasation – via Datix report and investigation.
Highly unusual in a community setting as we do not usually have intravenous fluids running, but rather administer mostly bolus intravenous anti-biotics.
Skin Integrity - Datix report and investigation. Pain – the service plans to develop an appropriate
pain audit for CCN and this is in progress via Standards, Quality Improvement and Development Group (SQuID).
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 97 of 300
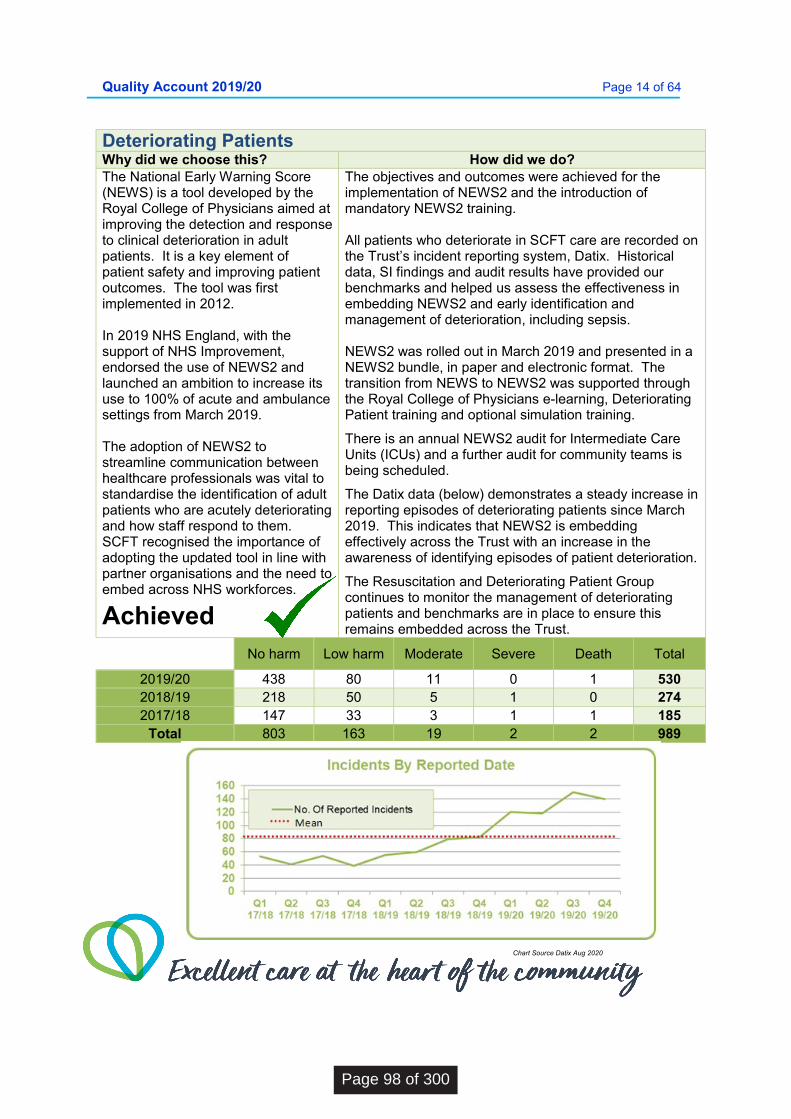
Quality Account 2019/20 Page 14 of 64
Chart Source Datix Aug 2020
Deteriorating Patients Why did we choose this? How did we do? The National Early Warning Score (NEWS) is a tool developed by the Royal College of Physicians aimed at improving the detection and response to clinical deterioration in adult patients. It is a key element of patient safety and improving patient outcomes. The tool was first implemented in 2012. In 2019 NHS England, with the support of NHS Improvement, endorsed the use of NEWS2 and launched an ambition to increase its use to 100% of acute and ambulance settings from March 2019. The adoption of NEWS2 to streamline communication between healthcare professionals was vital to standardise the identification of adult patients who are acutely deteriorating and how staff respond to them. SCFT recognised the importance of adopting the updated tool in line with partner organisations and the need to embed across NHS workforces.
Achieved
The objectives and outcomes were achieved for the implementation of NEWS2 and the introduction of mandatory NEWS2 training. All patients who deteriorate in SCFT care are recorded on the Trust’s incident reporting system, Datix. Historical data, SI findings and audit results have provided our benchmarks and helped us assess the effectiveness in embedding NEWS2 and early identification and management of deterioration, including sepsis. NEWS2 was rolled out in March 2019 and presented in a NEWS2 bundle, in paper and electronic format. The transition from NEWS to NEWS2 was supported through the Royal College of Physicians e-learning, Deteriorating Patient training and optional simulation training.
There is an annual NEWS2 audit for Intermediate Care Units (ICUs) and a further audit for community teams is being scheduled.
The Datix data (below) demonstrates a steady increase in reporting episodes of deteriorating patients since March 2019. This indicates that NEWS2 is embedding effectively across the Trust with an increase in the awareness of identifying episodes of patient deterioration.
The Resuscitation and Deteriorating Patient Group continues to monitor the management of deteriorating patients and benchmarks are in place to ensure this remains embedded across the Trust.
No harm Low harm Moderate Severe Death Total
2019/20 438 80 11 0 1 530 2018/19 218 50 5 1 0 274 2017/18 147 33 3 1 1 185
Total 803 163 19 2 2 989
Page 98 of 300
Quality Account 2019/20 Page 15 of 64
Effective Care
Translating research evidence into improved care Translating research evidence into improved care specifically the development, implementation and evaluation of a frailty pathway to improve outcomes of care for older people with continued collaborative working with other providers.
Why did we choose this? How did we do?
Frailty is associated typically with increasing age. Re-aligning healthcare services to the needs of an ageing population is a national priority. The trust provides care and services to an increasingly older population across all the geographical areas served. Areas such as Coastal West Sussex have a higher than national average population aged over 80 years. A frailty pathway is a priority area for our ageing population to improve the detection, assessment, case management and outcomes of care; the right care right place right time.
Achieved
We have introduced a number of developments including:
1. Development and incorporation of training on frailty for clinical staff in adult services. Our training on frailty used three approaches:
I. Identification of frailty clinical competencies II. Mapping the national frailty capabilities onto
the SCFT core skills frameworks for nurses, advanced nurse practitioners and AHPs respectively.
2. ELearning resources were identified, piloted and promoted by the NHS Acute Frailty Network.
3. A mapping exercise on clinical practice to identify, assess and manage frailty in and across services identified the Rockwood Clinical Frailty Scale (CFS) as the frailty assessment tool available across our adult services. An audit was conducted to assess use and clinical competencies and its findings have informed the frailty clinical competencies and training needs analysis, forming a baseline for the evaluation of our training programme and frailty pathway.
4. The Multi-disciplinary Frailty Steering Group was established with representation from across disciplines, settings and areas. The Steering Group oversees the delivery of the Frailty Pathway and collaboration with our partner organisations.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 99 of 300
Quality Account 2019/20 Page 16 of 64
Best Practice NICE Guidance Why did we choose this? How did we do? We want to ensure that once our patients/service users physical, mental health and social needs are holistically assessed, their care, treatment and support is delivered in line with legislation, standards and evidence-based guidance, including NICE and other expert professional bodies, to achieve effective outcomes. This particular priority is about further testing our response to NICE guidance and to look at sustainable changes made in practice.
Achieved
Following liaison with two other NHS Trusts, potential processes for gaining assurance of compliance with NICE guidance were shared with the Clinical Effectiveness Group (CEG). Following discussion it was agreed to implement a change of time frames for assessing applicability of guidance issued.
An audit of historical NICE Guidance was carried out, with a report of findings shared with CEG in October 2019. It was found that SCFT’s services continue to be compliant with guidance that was still applicable, as well as highlighting several instances where guidance was no longer directly applicable.
A re-audit began in February 2020, but was suspended until February 2021, and an additional audit planned for 2020/21, with specialist groups reviewing compliant NICE guidance, has been postponed until early 2021/22. Delays for both are due to SCFT’s response to the COVID-19 pandemic.
Substantial levels of assurance of SCFT’s compliance with NICE Guidance were demonstrated through applicability to services always assessed within nominated timeframe, outstanding benchmarking addressed and scrutinized by CEG, and continued compliance, with NICE guidance, achieved within the time frame given.
The above provides assurance to the Public and to the Trust that continued reviewing of processes and annual auditing ensures SCFT are meeting the standards set through NICE guidance.
Bank Staff recruitment People who use our services need to have confidence that there are sufficient staff employed through our bank to help supplement core staffing in areas, and therefore feel safe when accessing care. Why did we choose this? How did we do?
A focus on recruitment to the SCFT Bank will increase the numbers and types of staff accessible in a variety of locations, who are available to fill shifts, resulting in a reduction in the amount the Trust spends on agency staff. Achieved
In 2015/16, the Trust had 1,414 bank staff, including 459 registered nurses and 290 other clinicians. By the end of 2019/20, this had increased to 2,106 bank staff; including 758 registered nurses and 650 additional clinicians. The figures in the bank staff recruitment table, for each staff group in 2019/20 show that the use of taster days, geographical specific recruitment and booking systems with timeframes, have all led to an increase in the number of staff recruited to the bank. The time to hire has also been consistently reduced to below 45 days over quarter four. The time taken for substantive staff to join the bank, as well as the time for bank staff to be made substantive (made permanent), has also been reduced.
Page 100 of 300

Quality Account 2019/20 Page 17 of 64
Bank Staff Recruitment
Add Prof Scientific & Technic
Additional Clinical
Services
Admin & Clerical
Allied Health
Professionals
Estates & Ancillary
Medical & Dental
Nursing & Midwifery
Registered Totals
Mar 20
7 3 1 1
8 20 Feb 20
9 3 5
1 12 30
Jan 20
15 5 3 1
12 36 Dec 19
13 14 1 3 1 14 46
Nov 19 1 20 13 4 8
14 60 Oct 19 1 22 9 3 5 2 10 52 Sep 19 1 25 16 10 3 1 17 73 Aug 19
19 9 7 4 2 17 58
Jul 19 1 24 9 4 2 1 6 47 Jun19
15 10 6 10 3 15 59
May19 1 22 12 3 11 8 14 71 Apr19
19 5 7 5 2 4 42
Totals 5 210 108 54 53 21 143 594
Person Centred Care Friends & Family Test
Improve how people feel about the care they receive by improving our analysis of patient feedback. We will specifically focus on increasing the FFT response rates at Minor Injury Units and Urgent Treatment Centres in the Trust’s four areas; Central, Children’s & Well-Being, East and West. Why did we choose this? How did we do?
FFT gives the public an opportunity to provide feedback to the Trust regarding our services. Currently the numbers of FFT responses are not reaching the expected 15% response rate.
Achieved
An ambitious trajectory was proposed to incrementally increase FFT response rates throughout the year. At the start of the year MIU/UTC’s had a 4.36% response rate overall and whilst there were some peeks and falls throughout the year the average response rate at the close of the year was 8.38%. Looking ahead, we are reviewing how we are capturing patient feedback as part of our work on the Patient Experience and Involvement Strategy.
Throughout the COVID-19 pandemic, we have increased our bank workforce considerably, with 120 new starters joining the organisation/going through the recruitment process. This is across the main staffing groups.
We have also restarted our online recruitment events, reaching out to bank staff for conversion to substantive, with a variety of contracts available and have commenced a new online statutory and clinical training package for HCAs.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 101 of 300
Quality Account 2019/20 Page 18 of 64
Recommended Summary Plan for Emergency Care and Treatment (ReSPECT)
People need to feel that they are involved in decisions about their care, particularly in emergency situations, or at the end of their lives. We will prepare our Clinical workforce for the implementation of Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) through a comprehensive education and training programme. Why did we choose this? How did we do? ReSPECT is a process that creates personalised recommendations for a person’s clinical care in a future emergency in which they are unable to make or express choices. It provides health and care professionals responding to that emergency with a summary of recommendations to help them to make immediate decisions about that person’s care and treatment. ReSPECT can be complementary to a wider process of advance/anticipatory care planning. The ReSPECT process aligns with SCFT’s End of Life (EOL) Care Strategy and represents a quality improvement initiative that focusses on SCFT’s person-centred approach to care. It gives us an opportunity to upskill many more staff members to undertake the conversations that are crucial to patients reaching the end of their lives.
Achieved
Since April 2019, SCFT has undertaken a comprehensive training programme; ReSPECT Level 1 Awareness training has been delivered to 1,518 staff members in 131 hour long sessions.
ReSPECT Level 2 Training has been delivered to 674 nurses, doctors, physiotherapists and occupational therapists; this comprised 296 hours of highly specialised structured blended learning designed to prepare staff with the skills and tools to undertake ReSPECT conversations with patients.
An initial ReSPECT clinical audit has been carried out to assess the application of the ReSPECT Level 2 training process to the use of the ReSPECT documentation. The audit was conducted in both the Community and Intermediate Care Unit settings and demonstrated good application of the skills delivered within the ReSPECT Level 2 training programme. The audit showed that staff have been engaging in ReSPECT conversations with patients and subsequently recording that information correctly on the ReSPECT form.
Areas of outstanding practice included the documentation standards, recording of capacity, recording of active involvement of the patient in the process and the use of clear and easily understood language.
Further audits are planned over 2020, including aspects such as staff and patient engagement.
Page 102 of 300
Quality Account 2019/20 Page 19 of 64
Part 2.2
Statements of Assurance from the Board During 2019/20, Sussex Community NHS Foundation Trust provided and/or sub-contracted over 100 relevant health services.
SCFT has reviewed all the data available on the quality of care in these relevant health services.
The income generated by the relevant health services reviewed in 2019/20 represents 85.1% of the total income generated from the provision of relevant health services by SCFT for 2019/20.
Clinical Audit (National and Local) and National Enquiries
Clinical audit measures the quality of care and services against agreed standards, and suggests or makes improvements where necessary. During 2019/20, thirteen national clinical audits covered relevant health services that SCFT provides and one National Confidential Enquiry (NCEPOD) over this period.
National Audit for Care at End of Life (NACEL)
Sentinel Stroke National Audit Programme (SSNAP)
National Audit of Inpatient Falls (NAIF) National Diabetes Audit – Adults Pulmonary Rehabilitation audit
(NACAP) Parkinson’s UK audit Learning Disability Improvement
Standards Epilepsy 12 Audit (RCPCH)
Learning Disabilities Mortality Review Programme (LeDeR)
National Clinical Audit for Specialist Rehabilitation following major Injury (NCASRI)
National Audit of facing the future: Standards for Children in Emergency Care Settings
Community Hospitals Project (Replacing NAIC)
Community Services Project (Replacing NAIC)
Confidential Enquiry During 2019/20 SCFT participated in one national confidential enquiry into patient outcomes and deaths (NCEPOD) project which was ‘Long Term Ventilation study’ This was a review of the quality of care provided to children and young people aged 0-24 years who were receiving long-term ventilation.
During 2019/20, SCFT participated in all 13 (100%) of the national clinical audits for which it was eligible and relevant to participate in. Data collection was completed for the audits listed below:
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 103 of 300
Quality Account 2019/20 Page 20 of 64
National Clinical Audits & National Enquiries 2019/20
Participation (% cases submitted)
National Audit for Care at End of Life (NACEL)
Case note review - 16 (Arundel & District Hospital- 58.8%) (Bognor Regis War Memorial Hospital- 70.6%) (Crawley Hospital- 70.6%) (Crowborough War Memorial Hospital- 19.6%) (Horsham Hospital- 45.1%) (Lewes Victoria Hospital- 19.6%) (The Kleinwort Centre - 68.6%) (Uckfield Community Hospital - 19.6%) (Zachary Merton Hospital - 70.6%)
Epilepsy 12 Audit (RCPCH) 8 (N/A- Part of South East Thames Paediatric Epilepsy Group (SETPEG))
Long Term Ventilation study 4 (<1%) Pulmonary Rehabilitation Audit (NACAP)
Crawley Horsham and Mid Sussex COPD Adult Community Services – 43 (<1%)
Respiratory Service Brighton and Hove – 23 (1.5%) High Weald Lewis and Haven Community Respiratory
Service – 20 (<1%) COPD Coastal Service - <5 (<1%)
Parkinson’s UK audit Neuro-Rehab- Brighton – 20 (<1%) OT Horsham – 10 (1%) CNRT Physio Coastal West Sussex – 10 Physio Horsham – 10 (<1%) SaLT Hove – 25 (2%) SaLT Uckfield – 10 (<1%) SaLT Horsham – 10 (<1%)
Learning Disabilities Mortality Review Programme (LeDeR)
Continuous review and submission - Over 1000 deaths nationwide
National Clinical Audit for Specialist Rehabilitation following major Injury (NCASRI)
Continuous submission of overnight, rehabilitation patient data (N/A)
National Audit of facing the future: Standards for Children in Emergency Care Settings
N/A (N/A)
Community Hospitals Project (Replacing NAIC)
Intermediate Care Unit patient survey – 50 (N/A)
Community Services Project (Replacing NAIC)
N/A (N/A)
Completed Clinical Audits and NCEPOD Study Data These national clinical audits and NCEPOD study in which SCFT participated, and for which data collection was completed during 2019/20, are tabled below, alongside the number of cases submitted to each audit or enquiry as a percentage of the number of registered cases required by the terms of that audit or enquiry.
Page 104 of 300
Quality Account 2019/20 Page 21 of 64
National Clinical Audits & National Enquiries 2019/20
Participation (% cases submitted)
Learning Disability Improvement Standards
Learning disability service user survey - up to 100 Staff survey - 50 (N/A)
Sentinel Stroke National Audit Programme (SSNAP)
Horsham, Crawley and Mid-Sussex area - approx. 250 per annum (N/A)
Community Neuro Rehab Team (CNRT) Chichester – 33 (N/A)
CNRT Worthing – 76 (N/A) CNRT Newhaven – 17 (N/A)
National Audit of Inpatient Falls (NAIF)
Case note review – 1 (N/A)
National Diabetes Audit – Adults 1482 patients - Type 1 diabetes (N/A) 2516 patients - Type 2 diabetes (N/A)
Actions to Improve Quality of Healthcare The reports of 2 national clinical audits were reviewed by SCFT in 2019/20 and the Trust intends to take the following actions to improve the quality of healthcare provided.
Learning Disabilities Mortality Review Programme (LeDeR) Actions to Improve The need for accurate recording of causes of death as part of the process of learning is one of the ways to reduce premature mortality for people with a learning disability was shared at SCFT’s Mortality Review Group on which the Trust’s Deputy Medical Director and Clinical Service Manager for Learning Disability sit.
Sentinel Stroke National Audit Programme (SSNAP) Actions to Improve 2019 SSNAP findings identified standards not met in the stroke pathways in SCFT teams in West Sussex Worthing Community Neuro Rehab Team (CNRT). One issue raised was that the area was not commissioned or funded to provide an Early Supported Discharge service (ESD). This was a long-standing issue, but the SSNAP findings added weight for the service to be commissioned. Recruitment to an ESD service in SCFT began in March 2020, but was suspended due to the COVID-19 pandemic. This work stream will recommence in August 2020.
National Audits Scheduled for 2020/21 SCFT has identified eight national audits scheduled to occur in 2020/21 in which the Trust is eligible and appropriate to participate. These were confirmed by TWGG in July 2020, with registration and participation ongoing, or anticipated to begin from September 2020.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 105 of 300
Quality Account 2019/20 Page 22 of 64
National Audits Scheduled for 2020/21
Audit Description
Outcomes and recommendations
Audit of use of Malnutrition Universal Scoring Tool (MUST) tool
Audit findings provided reasonable assurance that the majority of patients’ MUST tools had been completed, however the following actions were not always up to standard and the Nutrition & Hydration Group will be taking them forward to ensure this learning is shared and acted upon.
Record ward details for every patient. Patient’s height to be recorded, to enable staff to calculate BMI
accurately. Patients to be asked about their weight loss and for this to be recorded. Patients’ weight loss in previous 3-6 months to be recorded in all relevant
sections. Date of admission and date of completion of MUST tool to be completed
every time. MUST tool to be completed within 24 hours of admission, where
possible. Ensure the overall scores are calculated for each entry and that the
corresponding action is undertaken within the specified time frame. Ensure documentation is standardised across units.
Audit of standards of mealtimes within Intermediate Care Units
Audit findings provided reasonable assurance that staff were supporting patients at mealtimes in line with SCFT policy, with several actions underway to provide 100% assurance: Patients to be supported to wash/wipe their hands before each meal. 100% of patients to be offered support to eat and drink if required. The availability of extra portions of food to be offered to all patients.
Pulmonary Rehabilitation Audit (NACAP) National Audit of Inpatient Falls (NAIF) National Clinical Audit for Specialist
Rehabilitation following major Injury (NCASRI)
Community Services Project
Learning Disabilities Mortality Review Programme (LeDeR)
Survey of Rehabilitation Need for Post COVID-19 Patients
National Diabetes Audit – Adults Sentinel Stroke National Audit
Programme (SSNAP)
Local Clinical Audits 2019/20 and Actions SCFT develops an annual schedule of Trust-wide (Local) clinical audits driven by national best practice guidance, monitoring effectiveness of changes introduced associated with quality improvements, lessons identified from investigations and audit, and assurance review outcomes. The schedule is agreed via SCFT’s governance committee structure. There were 20 Trust-wide (Local) audits and 10 Trust-Priority (Local) – 30 audits in total undertaken during 2019/20, which were approved by the Quality Improvement Committee in April 2019. The reports of the 30 Trust-wide (Local) clinical audits undertaken in 2019/20 were reviewed by SCFT and below are listed a selection of actions the Trust intends to take to improve the quality of healthcare provided.
Page 106 of 300
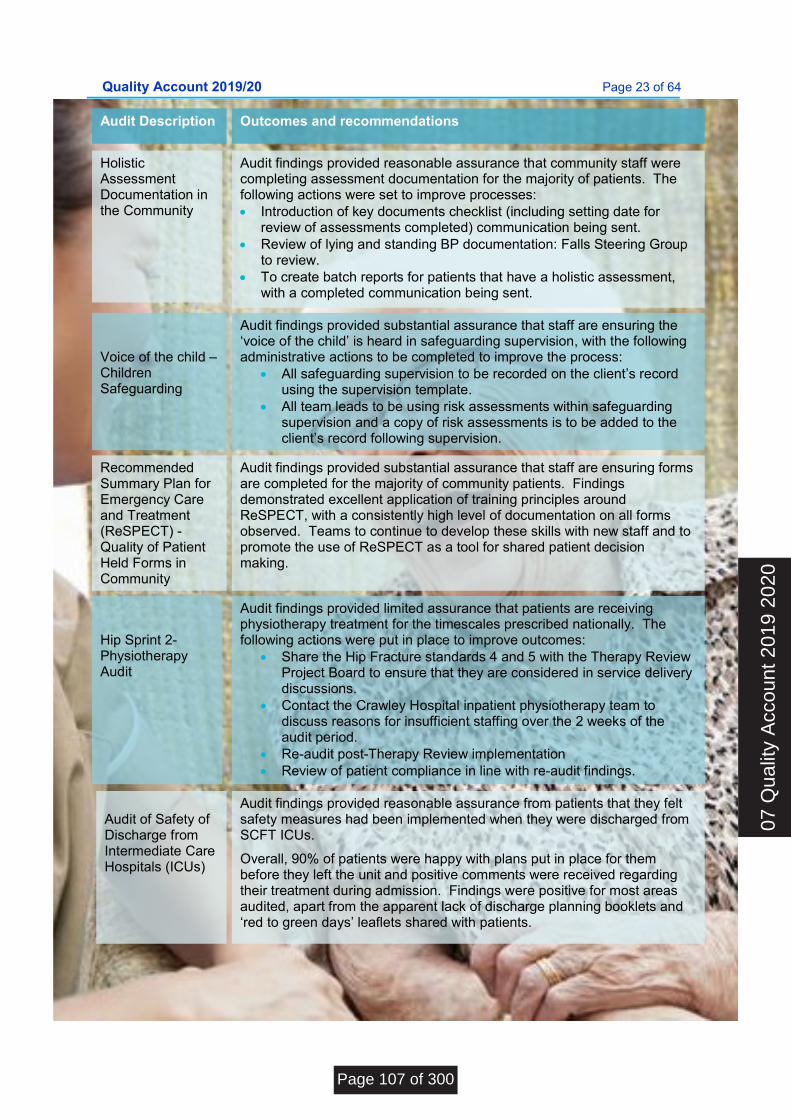
Quality Account 2019/20 Page 23 of 64
Voice of the child – Children Safeguardi
Audit Description Outcomes and recommendations
Holistic Assessment Documentation in the Community
Audit findings provided reasonable assurance that community staff were completing assessment documentation for the majority of patients. The following actions were set to improve processes: Introduction of key documents checklist (including setting date for
review of assessments completed) communication being sent. Review of lying and standing BP documentation: Falls Steering Group
to review. To create batch reports for patients that have a holistic assessment,
with a completed communication being sent.
Audit findings provided substantial assurance that staff are ensuring the ‘voice of the child’ is heard in safeguarding supervision, with the following administrative actions to be completed to improve the process:
All safeguarding supervision to be recorded on the client’s record using the supervision template.
All team leads to be using risk assessments within safeguarding supervision and a copy of risk assessments is to be added to the client’s record following supervision.
Voice of the child – Children Safeguarding
Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) - Quality of Patient Held Forms in Community
Audit findings provided substantial assurance that staff are ensuring forms are completed for the majority of community patients. Findings demonstrated excellent application of training principles around ReSPECT, with a consistently high level of documentation on all forms observed. Teams to continue to develop these skills with new staff and to promote the use of ReSPECT as a tool for shared patient decision making.
Hip Sprint 2- Physiotherapy Audit
Audit findings provided limited assurance that patients are receiving physiotherapy treatment for the timescales prescribed nationally. The following actions were put in place to improve outcomes:
Share the Hip Fracture standards 4 and 5 with the Therapy Review Project Board to ensure that they are considered in service delivery discussions.
Contact the Crawley Hospital inpatient physiotherapy team to discuss reasons for insufficient staffing over the 2 weeks of the audit period.
Re-audit post-Therapy Review implementation Review of patient compliance in line with re-audit findings.
Audit of Safety of Discharge from Intermediate Care Hospitals (ICUs)
Audit findings provided reasonable assurance from patients that they felt safety measures had been implemented when they were discharged from SCFT ICUs.
Overall, 90% of patients were happy with plans put in place for them before they left the unit and positive comments were received regarding their treatment during admission. Findings were positive for most areas audited, apart from the apparent lack of discharge planning booklets and ‘red to green days’ leaflets shared with patients.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 107 of 300
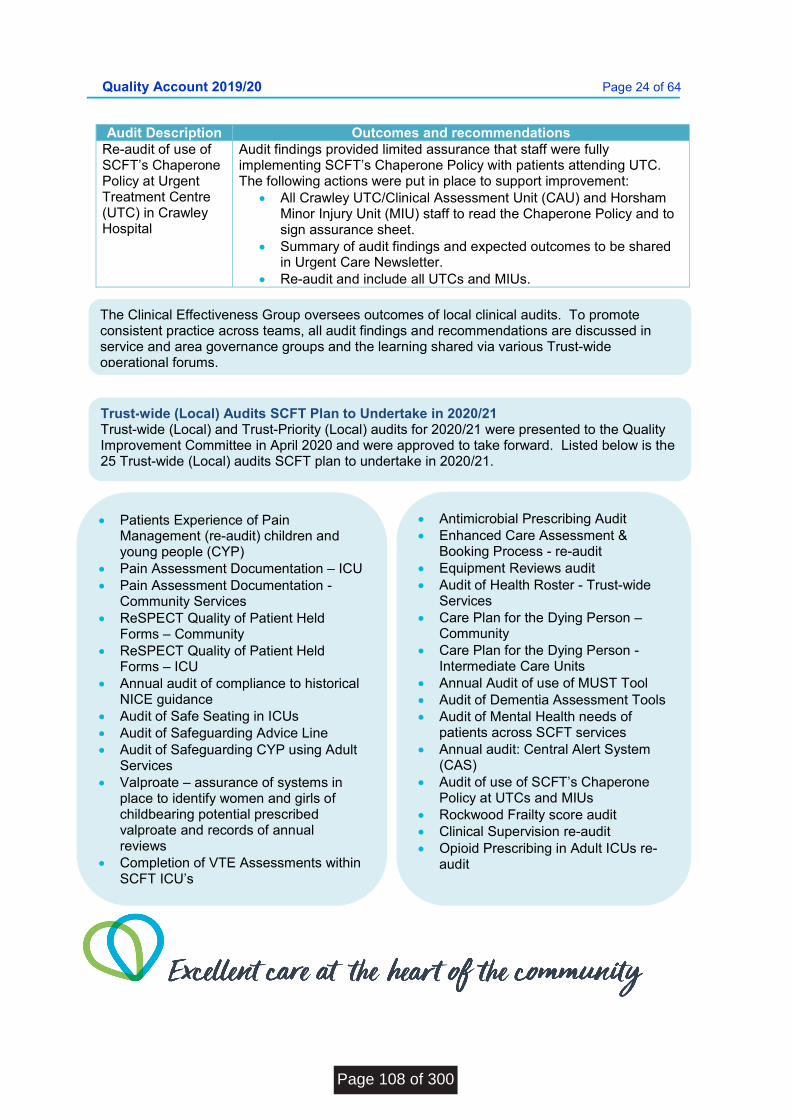
Quality Account 2019/20 Page 24 of 64
Audit Description Outcomes and recommendations Re-audit of use of SCFT’s Chaperone Policy at Urgent Treatment Centre (UTC) in Crawley Hospital
Audit findings provided limited assurance that staff were fully implementing SCFT’s Chaperone Policy with patients attending UTC. The following actions were put in place to support improvement:
All Crawley UTC/Clinical Assessment Unit (CAU) and Horsham Minor Injury Unit (MIU) staff to read the Chaperone Policy and to sign assurance sheet.
Summary of audit findings and expected outcomes to be shared in Urgent Care Newsletter.
Re-audit and include all UTCs and MIUs.
The Clinical Effectiveness Group oversees outcomes of local clinical audits. To promote consistent practice across teams, all audit findings and recommendations are discussed in service and area governance groups and the learning shared via various Trust-wide operational forums.
Trust-wide (Local) Audits SCFT Plan to Undertake in 2020/21 Trust-wide (Local) and Trust-Priority (Local) audits for 2020/21 were presented to the Quality Improvement Committee in April 2020 and were approved to take forward. Listed below is the 25 Trust-wide (Local) audits SCFT plan to undertake in 2020/21.
Patients Experience of Pain Management (re-audit) children and young people (CYP)
Pain Assessment Documentation – ICU Pain Assessment Documentation -
Community Services ReSPECT Quality of Patient Held
Forms – Community ReSPECT Quality of Patient Held
Forms – ICU Annual audit of compliance to historical
NICE guidance Audit of Safe Seating in ICUs Audit of Safeguarding Advice Line Audit of Safeguarding CYP using Adult
Services Valproate – assurance of systems in
place to identify women and girls of childbearing potential prescribed valproate and records of annual reviews
Completion of VTE Assessments within SCFT ICU’s
Antimicrobial Prescribing Audit Enhanced Care Assessment &
Booking Process - re-audit Equipment Reviews audit Audit of Health Roster - Trust-wide
Services Care Plan for the Dying Person –
Community Care Plan for the Dying Person -
Intermediate Care Units Annual Audit of use of MUST Tool Audit of Dementia Assessment Tools Audit of Mental Health needs of
patients across SCFT services Annual audit: Central Alert System
(CAS) Audit of use of SCFT’s Chaperone
Policy at UTCs and MIUs Rockwood Frailty score audit Clinical Supervision re-audit Opioid Prescribing in Adult ICUs re-
audit
Page 108 of 300
Quality Account 2019/20 Page 25 of 64
Research
Research Capacity and
Capability The Trust continues to build research capacity and capability with a growing number of staff leading the design of research studies as Chief Investigators, named as Co-applicants on research grants and leading the delivery of research studies as site Principal Investigators. Our research activity in 2019/20 includes:
19 studies opened. 17 published articles.
Activity in 2020/21
SCFT recognises that clinical research is central to the NHS. It is through research that the NHS is able to offer the ‘best’ treatments and services and improve people’s health. Organisations that take part in clinical research are actively working to improve treatments, interventions and services offered to patients. Participation in clinical research in SCFT gives patients access to the latest treatments in development and improves clinical effectiveness. The number of patients receiving relevant health services provided, or sub-contracted, by SCFT in 2019/20 that were recruited during that period to participate in research approved by a research ethics committee was 737. In addition, 137 clinical staff and health professionals were recruited to studies approved by the Health Research Authority, making a total of 874 participants to 19 studies. This year the SCFT delivery team supported 19 research projects. Each research project, whether from the National Institute for Health Research (NIHR) portfolio, or devised by SCFT researchers is designed to improve outcomes for patients. SCFT were ranked sixth out of 35 Community Trusts nationally in 2019/20 for volume of studies and ranked 6th for our recruitment numbers. This is not an insubstantial record given that many of the national studies are aimed at acute services, not community services.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 109 of 300
Quality Account 2019/20 Page 26 of 64
Commissioning for Quality and Improvement (CQUIN)
National CQUIN 2019/20 outcomes
National CQUIN 2019/20
Success Measures How Did We Do?
Staff Flu Vaccinations
Achieving an 80% uptake of flu vaccinations by frontline clinical staff
82% of frontline staff received flu vaccination
Use of anxiety disorder specific measures in Improving Access to Psychological Therapies (IAPT)
Achieving 65% of referrals with a specific anxiety disorder problem descriptor finishing a course of treatment having paired scores recorded on the specified Anxiety Disorder Specific Measure (ADSM)
Achieved 70 % of referrals with a specific anxiety disorder problem descriptor finishing a course of treatment having paired scores recorded on the specified Anxiety Disorder Specific Measure.
CQUIN CQUIN was introduced in 2009 to make a proportion of healthcare providers’ income conditional on demonstrating improvements in quality and innovation in specified areas of care. This means that a proportion of Sussex Community NHS Foundation Trust’s income in 2019/20 was conditional on achieving quality improvement and innovation goals agreed between the Trust and any person or body they entered into a contract, agreement or arrangement with for the provision of relevant health services, through the Commissioning
SCFT has completed the following CQUIN indicators, which represented 1.25% of the overall contract value and achieved the predetermined quality improvement targets and goals.
CCG2: Staff Flu Vaccinations CCG3: Alcohol and Tobacco CCG6: Use of anxiety disorder
specific measures in IAPT (Improving Access to Psychological Therapies)
CCG7 Three High Impact Actions to prevent falls
The value achieved for the financial year 2019/20 is £1.9 million.
In addition, NHS England has set five separate CQUINs for Children and Wellbeing Services valued at £100k bringing the CQUIN total value to £2m. Children Health Information System School Aged Immunisation
Programme Abdominal Aortic Aneurysm
Screening Programme Augmentive and Alternative
Communications Prosthetic
Page 110 of 300
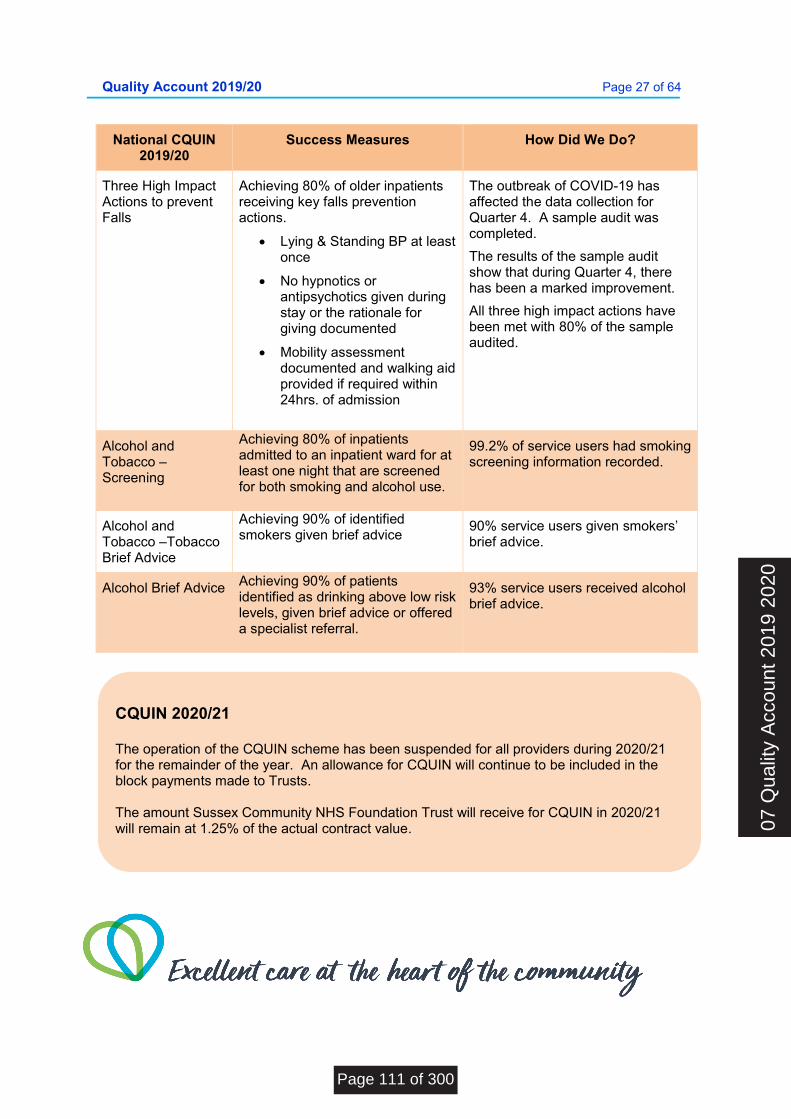
Quality Account 2019/20 Page 27 of 64
National CQUIN 2019/20
Success Measures How Did We Do?
Three High Impact Actions to prevent Falls
Achieving 80% of older inpatients receiving key falls prevention actions.
Lying & Standing BP at least once
No hypnotics or antipsychotics given during stay or the rationale for giving documented
Mobility assessment documented and walking aid provided if required within 24hrs. of admission
The outbreak of COVID-19 has affected the data collection for Quarter 4. A sample audit was completed.
The results of the sample audit show that during Quarter 4, there has been a marked improvement.
All three high impact actions have been met with 80% of the sample audited.
Alcohol and Tobacco –Screening
Achieving 80% of inpatients admitted to an inpatient ward for at least one night that are screened for both smoking and alcohol use.
99.2% of service users had smoking screening information recorded.
Alcohol and Tobacco –Tobacco Brief Advice
Achieving 90% of identified smokers given brief advice
90% service users given smokers’ brief advice.
Alcohol Brief Advice Achieving 90% of patients identified as drinking above low risk levels, given brief advice or offered a specialist referral.
93% service users received alcohol brief advice.
CQUIN 2020/21 The operation of the CQUIN scheme has been suspended for all providers during 2020/21 for the remainder of the year. An allowance for CQUIN will continue to be included in the block payments made to Trusts. The amount Sussex Community NHS Foundation Trust will receive for CQUIN in 2020/21 will remain at 1.25% of the actual contract value. 07
Qua
lity
Acc
ount
201
9 20
20
Page 111 of 300

Quality Account 2019/20 Page 28 of 64
Care Quality Commission (CQC)
Safe Effective Caring Responsive Well-led Overall
(Last rated) Community health Services For Adults
Good
Good
Good
Good
Good
Good (Mar 2015)
Community health Services For CYP
Good
Good
Good
Good
Good
Good (Mar 2015)
Community Inpatient Services
Good
Good
Outstanding
Good
Good
Good (Sept 2017)
End of life Care Good
Good
Good
Outstanding
Good
Good (Mar 2015)
Sexual Health services
Good
Good
Good
Good
Good
Good (Oct 2017)
The Trust was inspected between September and October 2017 under the Chief Inspector of Hospitals regime. Three groups of services were inspected, community inpatient services: community dental services and sexual health services. The inspection focused on five key questions:
Are services safe? Are services effective? Are services caring? Are services responsive? Are services well led?
In January 2018, England’s Chief Inspector of Hospitals rated the Trust as “Good” for each domain and we achieved an overall rating of ‘Good’. The ‘caring’ domain for our community inpatient services and the ‘responsive’ domain for our community end of life care were both rated Outstanding by the CQC.
Sussex Community NHS Foundation Trust is required to register with the Care Quality Commission and its current registration status is GOOD with Outstanding features. Ratings across all CQC domains for the areas inspected were Good, with the exception of the ‘caring’ domain for our community inpatient services and the ‘responsive’ domain for our community end of life care, which were both rated Outstanding.
SCFT has no conditions on its registration and the CQC has not taken any enforcement action against SCFT during 2019/20. SCFT has not participated in any special reviews or investigations by the Care Quality Commission during 2019/20.
SCFT is required to register with the Care Quality Commission. The Trust has 13 registered locations and is registered to carry out the following regulated activities: Nursing care Family planning services Treatment of disease, disorder or
injury Surgical procedures Diagnostic and screening procedures
Page 112 of 300
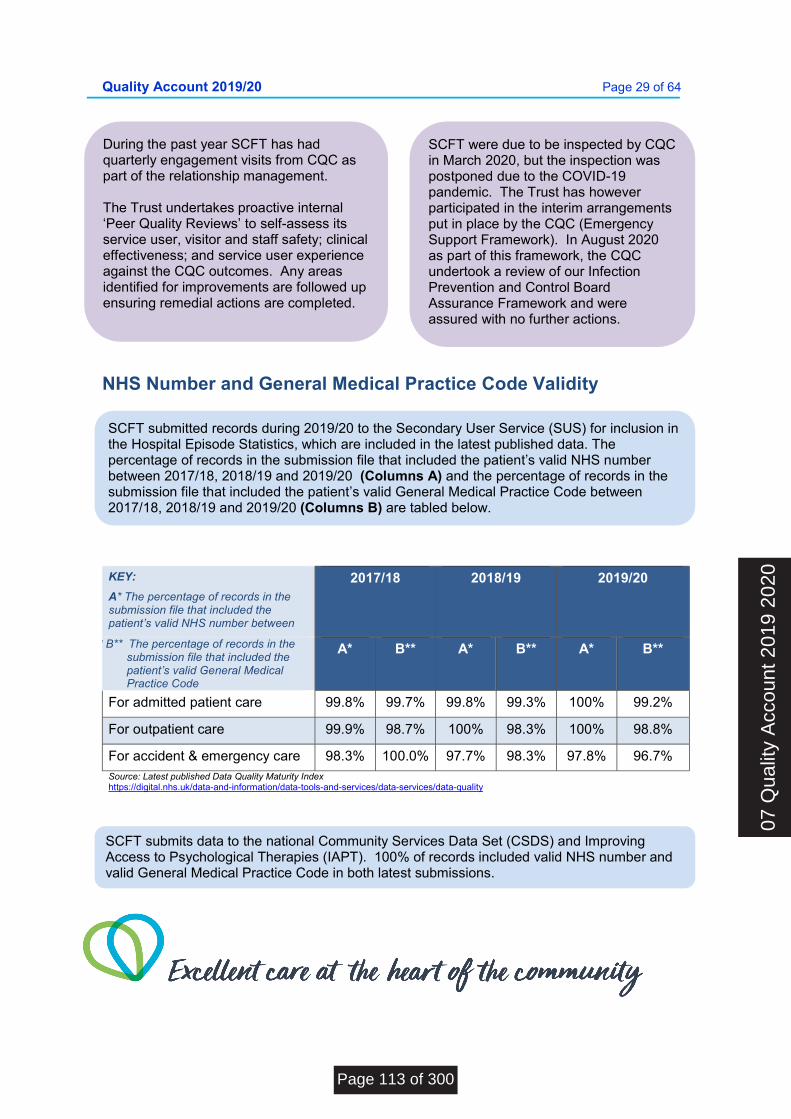
Quality Account 2019/20 Page 29 of 64
NHS Number and General Medical Practice Code Validity
KEY:
A* The percentage of records in the submission file that included the patient’s valid NHS number between
2017/18 2018/19 2019/20
** B** The percentage of records in the submission file that included the patient’s valid General Medical Practice Code
A* B** A* B** A* B**
For admitted patient care 99.8% 99.7% 99.8% 99.3% 100% 99.2%
For outpatient care 99.9% 98.7% 100% 98.3% 100% 98.8%
For accident & emergency care 98.3% 100.0% 97.7% 98.3% 97.8% 96.7% Source: Latest published Data Quality Maturity Index https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/data-quality
During the past year SCFT has had quarterly engagement visits from CQC as part of the relationship management. The Trust undertakes proactive internal ‘Peer Quality Reviews’ to self-assess its service user, visitor and staff safety; clinical effectiveness; and service user experience against the CQC outcomes. Any areas identified for improvements are followed up ensuring remedial actions are completed.
SCFT were due to be inspected by CQC in March 2020, but the inspection was postponed due to the COVID-19 pandemic. The Trust has however participated in the interim arrangements put in place by the CQC (Emergency Support Framework). In August 2020 as part of this framework, the CQC undertook a review of our Infection Prevention and Control Board Assurance Framework and were assured with no further actions.
SCFT submitted records during 2019/20 to the Secondary User Service (SUS) for inclusion in the Hospital Episode Statistics, which are included in the latest published data. The percentage of records in the submission file that included the patient’s valid NHS number between 2017/18, 2018/19 and 2019/20 (Columns A) and the percentage of records in the submission file that included the patient’s valid General Medical Practice Code between 2017/18, 2018/19 and 2019/20 (Columns B) are tabled below.
SCFT submits data to the national Community Services Data Set (CSDS) and Improving Access to Psychological Therapies (IAPT). 100% of records included valid NHS number and valid General Medical Practice Code in both latest submissions.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 113 of 300
Quality Account 2019/20 Page 30 of 64
Data Quality Investment in information systems to monitor and improve the quality of care The Trust has invested significant sums over the last 5 years on IT Infrastructure and Information Systems. The most significant investment has been the roll out of SystmOne, the Trust’s electronic patient record. The movement of the vast majority of the Trust’s clinical services onto a single, consistent system is transforming the way the Trust monitors and reports its activity in order to improve patient care. The system has been rolled out to almost all services across the Trust according to an agreed and prioritised plan. Local services are instrumental in customising the system for their service-based needs. This allows them to ensure that the system is set up around the key reporting requirements for their patients. The Trust has recognised that there is a need for ongoing support for the reporting requirements. A series of business cases have been approved to ensure ongoing support in the development in the way that data is captured and reported. The 2019/20 capital investment in systems and hardware is more than 50% of the total capital programme and significantly higher than the sums in previous years.
Payment by Results SCFT was not subject to the Payment by Results clinical coding audit during 2019/20 by NHS Improvement.
Data Security and Protection Assessment Report SCFT’s Data Security and Protection Toolkit Assessment Report (formerly the Information Governance Toolkit) reports all requirements have been met for 2019/20. The Trust has a robust programme of information governance improvements and awareness and a governance framework to monitor and assure via the Information Governance and Security Group.
Review of current data quality The Trust surveyed its staff in 2019/20 specifically on current data quality as it related to their teams. Teams were asked to give a level of confidence in their own data quality. Based on a range of scores between 1, not at all confident and 10, extremely confident, the median score was 7, and the majority of responses between 6 and 9. This shows reasonable confidence from staff in their own data quality, but the survey highlighted the need for further training and education for staff to improve the position. A new training package is currently being designed.
The Trust’s annual internal audit programme included a number of data quality audits, agreed by the Trust’s Executive and Audit Committee. The audits covered areas where the Trust requires assurance on data quality for internally or externally reported data. For 2019/20, this included an audit on safe staffing data, which reported substantial assurance. Further data quality audits relating to the use of rostering systems and SystmOne are also in progress.
SCFT’s Quality Account includes a number of key performance reports that are usually subject to external review by SCFT’s external auditors as part of the annual audit process. This requirement has been cancelled this year due to the COVID-19 pandemic.
Information is reviewed monthly through Finance, Performance and Quality meetings, at Area and Trust levels. Data is reported and variances to plan and exceptions reported and remedial actions agreed. This includes actions to improve data quality.
Page 114 of 300

Quality Account 2019/20 Page 31 of 64
Assurance Processes to Monitor Data Quality and Validity
There are a range of processes in place to monitor data quality and check the validity of data. Firstly, there are checks that are undertaken through the design and deployment of SystmOne. Post go live, services receive monthly standard data quality measures to review the data going into the system and remedial action is taken to address any data quality gaps that become apparent once the system has gone live.
Externally reported information is routed through the Performance team, with extensive validation processes in place to gain assurance on the quality of the data particularly for Statutory and Contractual Returns. A Finance and Information Group monitors the quality of Contractual data and reporting for our Clinical Services, with progress monitored via a Data Quality Improvement Plan (DQIP) reviewed on a quarterly basis.
Internally, there is a monthly process for the scrutiny, review and challenge of data by services in advance of monthly Executive led Finance, Performance and Quality (FPQ) meetings with each operational area. A Performance data analyst business partner model has been introduced in the last 12 months to help operational teams with the challenge of data quality and as a result of the FPQ and business partner model, data quality is improving.
Trust reporting is delivered largely through Scholar, the Trust’s self-service performance reporting system. Scholar holds dashboards across a range of quality, performance, workforce and finance metrics. These are generally available at Trust, Operational, Area and individual Service levels, giving managers and clinicians access to their quality and performance data in a way that demonstrates how it contributes to overall performance of the Trust.
Good access to regularly updated data has enabled better detection of data quality issues. Services are supported by Performance and Quality Improvement (QI) business partners, who work alongside the Digital team to make iterative changes to their processes in order to improve data quality. Better data, in turn leads to better decision-making.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 115 of 300
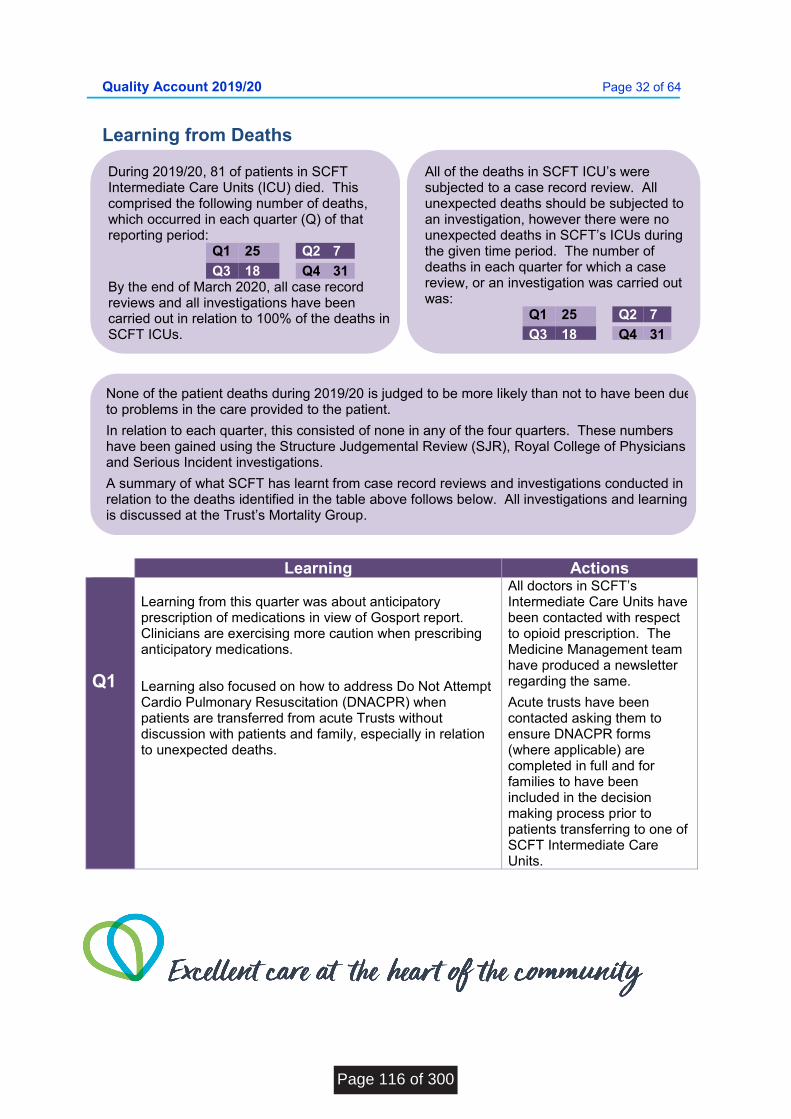
Quality Account 2019/20 Page 32 of 64
Learning from Deaths
Learning Actions Q1
Learning from this quarter was about anticipatory prescription of medications in view of Gosport report. Clinicians are exercising more caution when prescribing anticipatory medications.
Learning also focused on how to address Do Not Attempt Cardio Pulmonary Resuscitation (DNACPR) when patients are transferred from acute Trusts without discussion with patients and family, especially in relation to unexpected deaths.
All doctors in SCFT’s Intermediate Care Units have been contacted with respect to opioid prescription. The Medicine Management team have produced a newsletter regarding the same.
Acute trusts have been contacted asking them to ensure DNACPR forms (where applicable) are completed in full and for families to have been included in the decision making process prior to patients transferring to one of SCFT Intermediate Care Units.
During 2019/20, 81 of patients in SCFT Intermediate Care Units (ICU) died. This comprised the following number of deaths, which occurred in each quarter (Q) of that reporting period:
Q1 25 Q2 7
Q3 18 Q4 31 By the end of March 2020, all case record reviews and all investigations have been carried out in relation to 100% of the deaths in SCFT ICUs.
All of the deaths in SCFT ICU’s were subjected to a case record review. All unexpected deaths should be subjected to an investigation, however there were no unexpected deaths in SCFT’s ICUs during the given time period. The number of deaths in each quarter for which a case review, or an investigation was carried out was:
Q1 25 Q2 7
Q3 18 Q4 31
None of the patient deaths during 2019/20 is judged to be more likely than not to have been due to problems in the care provided to the patient.
In relation to each quarter, this consisted of none in any of the four quarters. These numbers have been gained using the Structure Judgemental Review (SJR), Royal College of Physicians and Serious Incident investigations.
A summary of what SCFT has learnt from case record reviews and investigations conducted in relation to the deaths identified in the table above follows below. All investigations and learning is discussed at the Trust’s Mortality Group.
Page 116 of 300
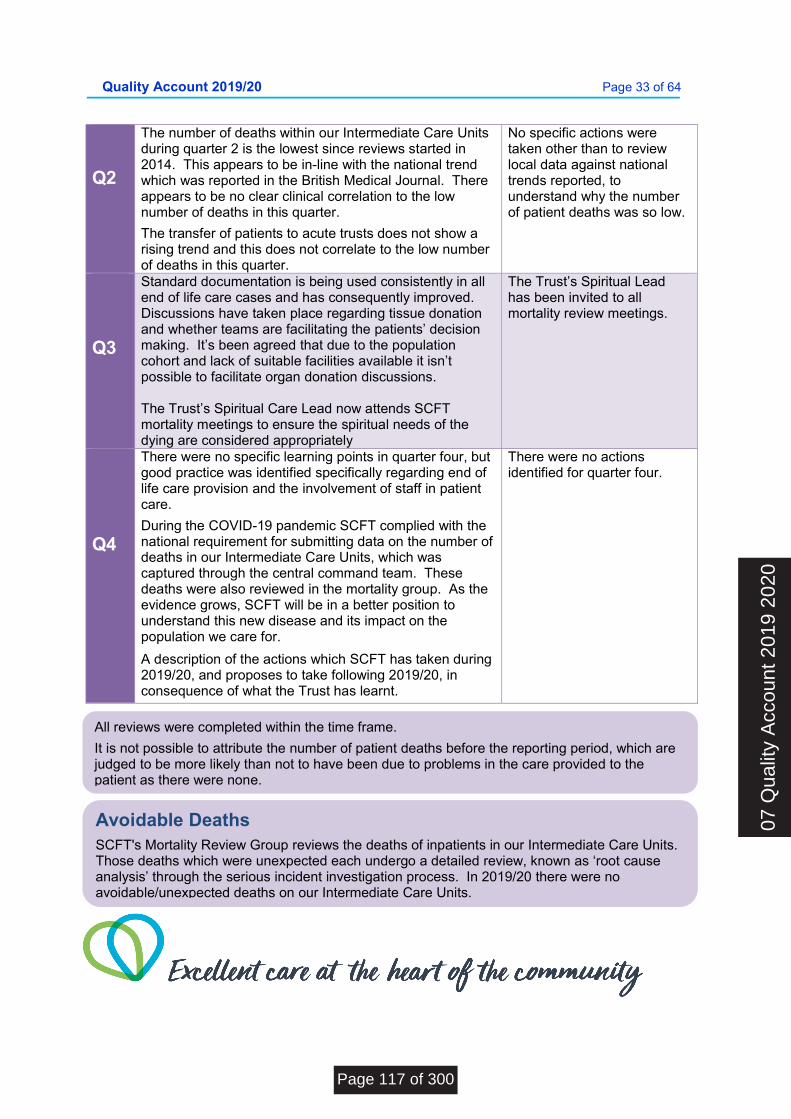
Quality Account 2019/20 Page 33 of 64
Q2
The number of deaths within our Intermediate Care Units during quarter 2 is the lowest since reviews started in 2014. This appears to be in-line with the national trend which was reported in the British Medical Journal. There appears to be no clear clinical correlation to the low number of deaths in this quarter.
The transfer of patients to acute trusts does not show a rising trend and this does not correlate to the low number of deaths in this quarter.
No specific actions were taken other than to review local data against national trends reported, to understand why the number of patient deaths was so low.
Q3
Standard documentation is being used consistently in all end of life care cases and has consequently improved. Discussions have taken place regarding tissue donation and whether teams are facilitating the patients’ decision making. It’s been agreed that due to the population cohort and lack of suitable facilities available it isn’t possible to facilitate organ donation discussions. The Trust’s Spiritual Care Lead now attends SCFT mortality meetings to ensure the spiritual needs of the dying are considered appropriately
The Trust’s Spiritual Lead has been invited to all mortality review meetings.
Q4
There were no specific learning points in quarter four, but good practice was identified specifically regarding end of life care provision and the involvement of staff in patient care.
During the COVID-19 pandemic SCFT complied with the national requirement for submitting data on the number of deaths in our Intermediate Care Units, which was captured through the central command team. These deaths were also reviewed in the mortality group. As the evidence grows, SCFT will be in a better position to understand this new disease and its impact on the population we care for.
A description of the actions which SCFT has taken during 2019/20, and proposes to take following 2019/20, in consequence of what the Trust has learnt.
There were no actions identified for quarter four.
All reviews were completed within the time frame.
It is not possible to attribute the number of patient deaths before the reporting period, which are judged to be more likely than not to have been due to problems in the care provided to the patient as there were none.
Avoidable Deaths
SCFT's Mortality Review Group reviews the deaths of inpatients in our Intermediate Care Units. Those deaths which were unexpected each undergo a detailed review, known as ‘root cause analysis’ through the serious incident investigation process. In 2019/20 there were no avoidable/unexpected deaths on our Intermediate Care Units.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 117 of 300
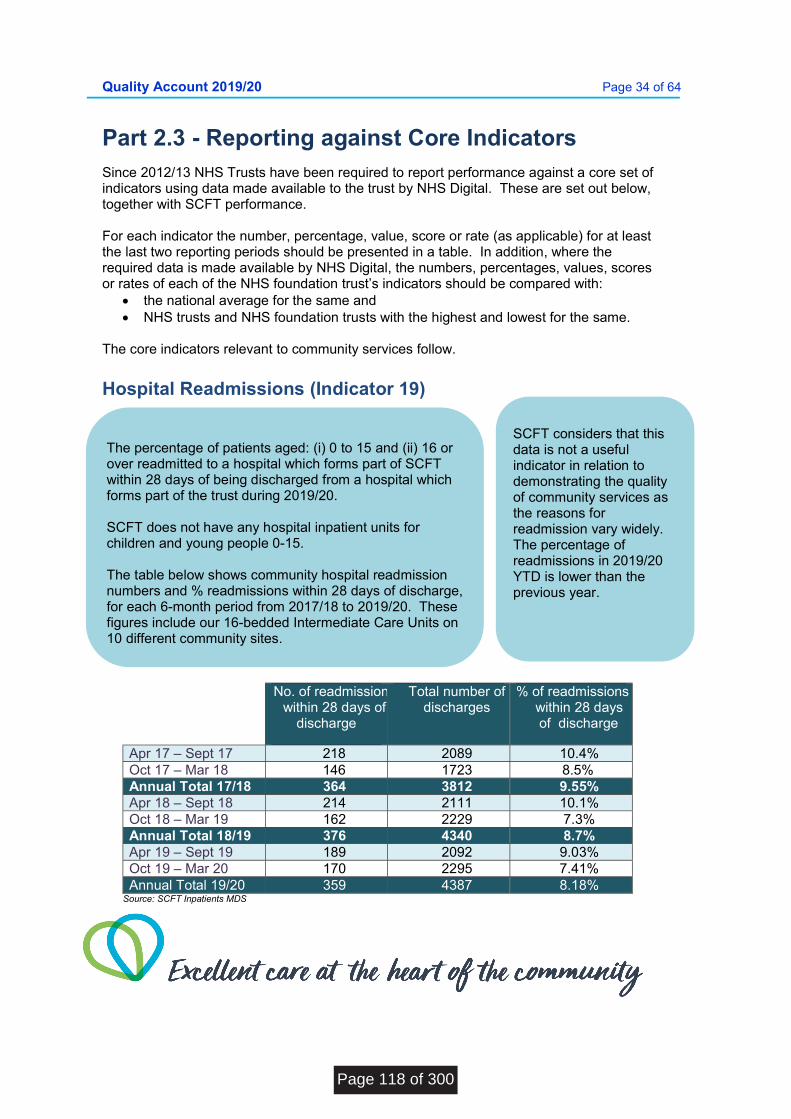
Quality Account 2019/20 Page 34 of 64
Part 2.3 - Reporting against Core Indicators Since 2012/13 NHS Trusts have been required to report performance against a core set of indicators using data made available to the trust by NHS Digital. These are set out below, together with SCFT performance. For each indicator the number, percentage, value, score or rate (as applicable) for at least the last two reporting periods should be presented in a table. In addition, where the required data is made available by NHS Digital, the numbers, percentages, values, scores or rates of each of the NHS foundation trust’s indicators should be compared with:
the national average for the same and NHS trusts and NHS foundation trusts with the highest and lowest for the same.
The core indicators relevant to community services follow.
Hospital Readmissions (Indicator 19)
No. of readmissionswithin 28 days of
discharge
Total number of discharges
% of readmissions within 28 days
of discharge
Apr 17 – Sept 17 218 2089 10.4% Oct 17 – Mar 18 146 1723 8.5% Annual Total 17/18 364 3812 9.55% Apr 18 – Sept 18 214 2111 10.1% Oct 18 – Mar 19 162 2229 7.3% Annual Total 18/19 376 4340 8.7% Apr 19 – Sept 19 189 2092 9.03% Oct 19 – Mar 20 170 2295 7.41% Annual Total 19/20 359 4387 8.18%
Source: SCFT Inpatients MDS
The percentage of patients aged: (i) 0 to 15 and (ii) 16 or over readmitted to a hospital which forms part of SCFT within 28 days of being discharged from a hospital which forms part of the trust during 2019/20. SCFT does not have any hospital inpatient units for children and young people 0-15. The table below shows community hospital readmission numbers and % readmissions within 28 days of discharge, for each 6-month period from 2017/18 to 2019/20. These figures include our 16-bedded Intermediate Care Units on 10 different community sites.
SCFT considers that this data is not a useful indicator in relation to demonstrating the quality of community services as the reasons for readmission vary widely. The percentage of readmissions in 2019/20 YTD is lower than the previous year.
Page 118 of 300
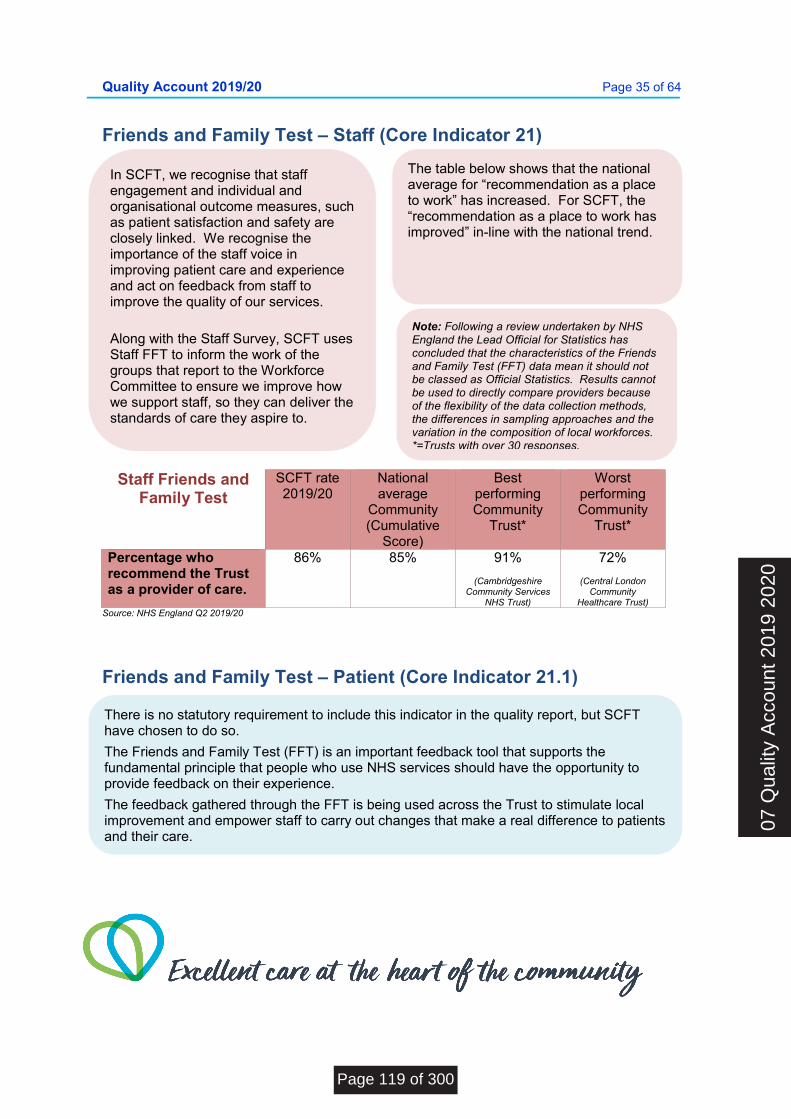
Quality Account 2019/20 Page 35 of 64
Friends and Family Test – Staff (Core Indicator 21)
Staff Friends and Family Test
SCFT rate 2019/20
National average
Community (Cumulative
Score)
Best performing Community
Trust*
Worst performing Community
Trust*
Percentage who recommend the Trust as a provider of care.
86% 85% 91%
(Cambridgeshire Community Services
NHS Trust)
72%
(Central London Community
Healthcare Trust) Source: NHS England Q2 2019/20
Friends and Family Test – Patient (Core Indicator 21.1)
The table below shows that the national average for “recommendation as a place to work” has increased. For SCFT, the “recommendation as a place to work has improved” in-line with the national trend.
Note: Following a review undertaken by NHS England the Lead Official for Statistics has concluded that the characteristics of the Friends and Family Test (FFT) data mean it should not be classed as Official Statistics. Results cannot be used to directly compare providers because of the flexibility of the data collection methods, the differences in sampling approaches and the variation in the composition of local workforces. *=Trusts with over 30 responses.
There is no statutory requirement to include this indicator in the quality report, but SCFT have chosen to do so.
The Friends and Family Test (FFT) is an important feedback tool that supports the fundamental principle that people who use NHS services should have the opportunity to provide feedback on their experience.
The feedback gathered through the FFT is being used across the Trust to stimulate local improvement and empower staff to carry out changes that make a real difference to patients and their care.
In SCFT, we recognise that staff engagement and individual and organisational outcome measures, such as patient satisfaction and safety are closely linked. We recognise the importance of the staff voice in improving patient care and experience and act on feedback from staff to improve the quality of our services.
Along with the Staff Survey, SCFT uses Staff FFT to inform the work of the groups that report to the Workforce Committee to ensure we improve how we support staff, so they can deliver the standards of care they aspire to.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 119 of 300
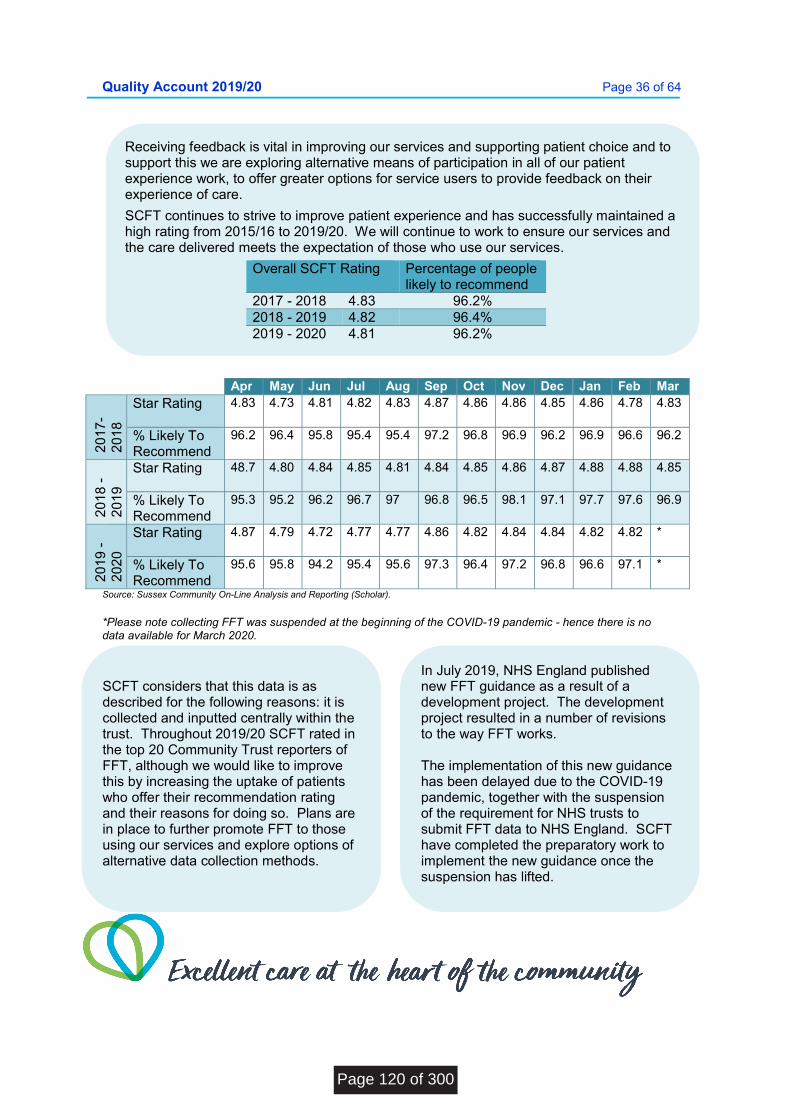
Quality Account 2019/20 Page 36 of 64
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
20
17-
20
18
Star Rating
4.83 4.73 4.81 4.82 4.83 4.87 4.86 4.86 4.85 4.86 4.78 4.83
% Likely To Recommend
96.2 96.4 95.8 95.4 95.4 97.2 96.8 96.9 96.2 96.9 96.6 96.2
20
18 -
20
19
Star Rating
48.7 4.80 4.84 4.85 4.81 4.84 4.85 4.86 4.87 4.88 4.88 4.85
% Likely To Recommend
95.3 95.2 96.2 96.7 97 96.8 96.5 98.1 97.1 97.7 97.6 96.9
20
19 -
20
20
Star Rating
4.87 4.79 4.72 4.77 4.77 4.86 4.82 4.84 4.84 4.82 4.82 *
% Likely To Recommend
95.6 95.8 94.2 95.4 95.6 97.3 96.4 97.2 96.8 96.6 97.1 *
Source: Sussex Community On-Line Analysis and Reporting (Scholar).
*Please note collecting FFT was suspended at the beginning of the COVID-19 pandemic - hence there is no data available for March 2020.
Receiving feedback is vital in improving our services and supporting patient choice and to support this we are exploring alternative means of participation in all of our patient experience work, to offer greater options for service users to provide feedback on their experience of care.
SCFT continues to strive to improve patient experience and has successfully maintained a high rating from 2015/16 to 2019/20. We will continue to work to ensure our services and the care delivered meets the expectation of those who use our services.
Overall SCFT Rating Percentage of people likely to recommend
2017 - 2018 4.83 96.2% 2018 - 2019 4.82 96.4% 2019 - 2020 4.81 96.2%
SCFT considers that this data is as described for the following reasons: it is collected and inputted centrally within the trust. Throughout 2019/20 SCFT rated in the top 20 Community Trust reporters of FFT, although we would like to improve this by increasing the uptake of patients who offer their recommendation rating and their reasons for doing so. Plans are in place to further promote FFT to those using our services and explore options of alternative data collection methods.
In July 2019, NHS England published new FFT guidance as a result of a development project. The development project resulted in a number of revisions to the way FFT works. The implementation of this new guidance has been delayed due to the COVID-19 pandemic, together with the suspension of the requirement for NHS trusts to submit FFT data to NHS England. SCFT have completed the preparatory work to implement the new guidance once the suspension has lifted.
Page 120 of 300
Quality Account 2019/20 Page 37 of 64
VTE Assessments (Core Indicator 23)
Clostridium difficile (Core Indicator 24)
The percentage of patients who were admitted to one of our Intermediate Care Units and who were risk assessed for venous thromboembolism during the reporting period. Reporting Period
The percentage of patients who were admitted to hospital and who were risk assessed for venous thromboembolism
2017 - 2018 94% 2018 - 2019 96% 2019 - 2020 96% Source: Scholar Trust Metrics 20.5.2020
SCFT has identified an issue within the data collection process. However, spot checks have identified 100% compliance. Going forward, the roll out of SystmOne to all Intermediate Care Units is due to be completed by December 2020 and this will improve data collection.
Clostridium difficile, also known as C. difficile (or C. diff), is a bacterium that can infect the bowel and cause diarrhoea. The bacteria often live harmlessly because the other bacteria normally found in the bowel keep it under control. However, some antibiotics can interfere with the balance of bacteria in the bowel, which can cause the C.diff bacteria to multiply and produce toxins that make a person ill. This occurs mainly in elderly and other vulnerable patient groups especially those who have been exposed to antibiotic treatment, but it can spread easily to others.
In order to continually improve, each C.diff case is investigated and the results reviewed to determine whether the case was linked with a lapse in the quality of care provided to patients.
SCFT considers that this data is as described for the following reasons - all our Intermediate Care Units submit data on the percentage of patients who were admitted to hospital and who were risk assessed for venous thromboembolism to our on-line analysis and reporting system (Scholar).
The table overleaf shows the rate per 100,000 occupied bed days (OBDs) of cases of C.diff infection reported within the Trust amongst patients aged 2 or over from 2017/18 to 2018/19.
2019/20 During 2019/20, there were no cases of C. diff attributed to SCFT. The Infection Prevention and Control Team continue to reinforce the important messages for preventing C.diff infection and work together with SCFT’s Antimicrobial Pharmacist reinforcing the messages regarding good prescribing and avoiding unnecessary antimicrobial reduction.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 121 of 300
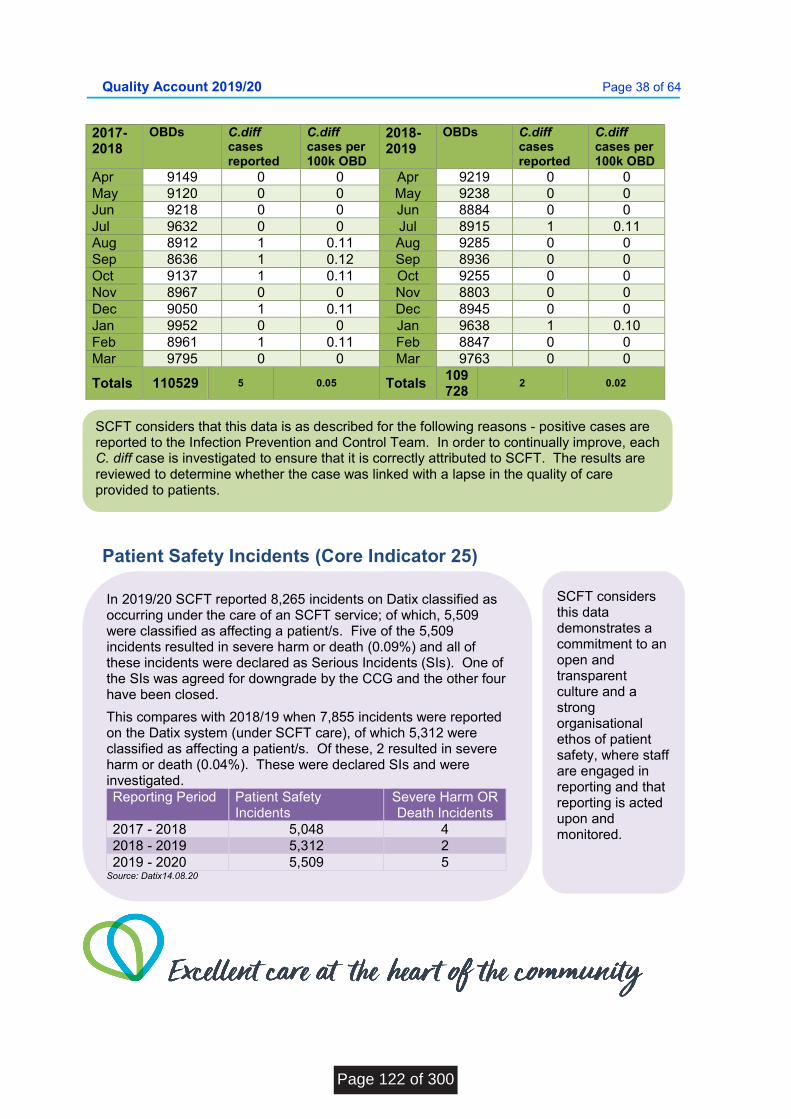
Quality Account 2019/20 Page 38 of 64
2017-2018
OBDs C.diff cases reported
C.diff cases per 100k OBD
2018-2019
OBDs C.diff cases reported
C.diff cases per 100k OBD
Apr 9149 0 0 Apr 9219 0 0 May 9120 0 0 May 9238 0 0 Jun 9218 0 0 Jun 8884 0 0 Jul 9632 0 0 Jul 8915 1 0.11 Aug 8912 1 0.11 Aug 9285 0 0 Sep 8636 1 0.12 Sep 8936 0 0 Oct 9137 1 0.11 Oct 9255 0 0 Nov 8967 0 0 Nov 8803 0 0 Dec 9050 1 0.11 Dec 8945 0 0 Jan 9952 0 0 Jan 9638 1 0.10 Feb 8961 1 0.11 Feb 8847 0 0 Mar 9795 0 0 Mar 9763 0 0
Totals 110529 5 0.05 Totals 109728
2 0.02
Patient Safety Incidents (Core Indicator 25)
SCFT considers that this data is as described for the following reasons - positive cases are reported to the Infection Prevention and Control Team. In order to continually improve, each C. diff case is investigated to ensure that it is correctly attributed to SCFT. The results are reviewed to determine whether the case was linked with a lapse in the quality of care provided to patients.
In 2019/20 SCFT reported 8,265 incidents on Datix classified as occurring under the care of an SCFT service; of which, 5,509 were classified as affecting a patient/s. Five of the 5,509 incidents resulted in severe harm or death (0.09%) and all of these incidents were declared as Serious Incidents (SIs). One of the SIs was agreed for downgrade by the CCG and the other four have been closed.
This compares with 2018/19 when 7,855 incidents were reported on the Datix system (under SCFT care), of which 5,312 were classified as affecting a patient/s. Of these, 2 resulted in severe harm or death (0.04%). These were declared SIs and were investigated. Reporting Period Patient Safety
Incidents Severe Harm OR Death Incidents
2017 - 2018 5,048 4 2018 - 2019 5,312 2 2019 - 2020 5,509 5
Source: Datix14.08.20
SCFT considers this data demonstrates a commitment to an open and transparent culture and a strong organisational ethos of patient safety, where staff are engaged in reporting and that reporting is acted upon and monitored.
Page 122 of 300
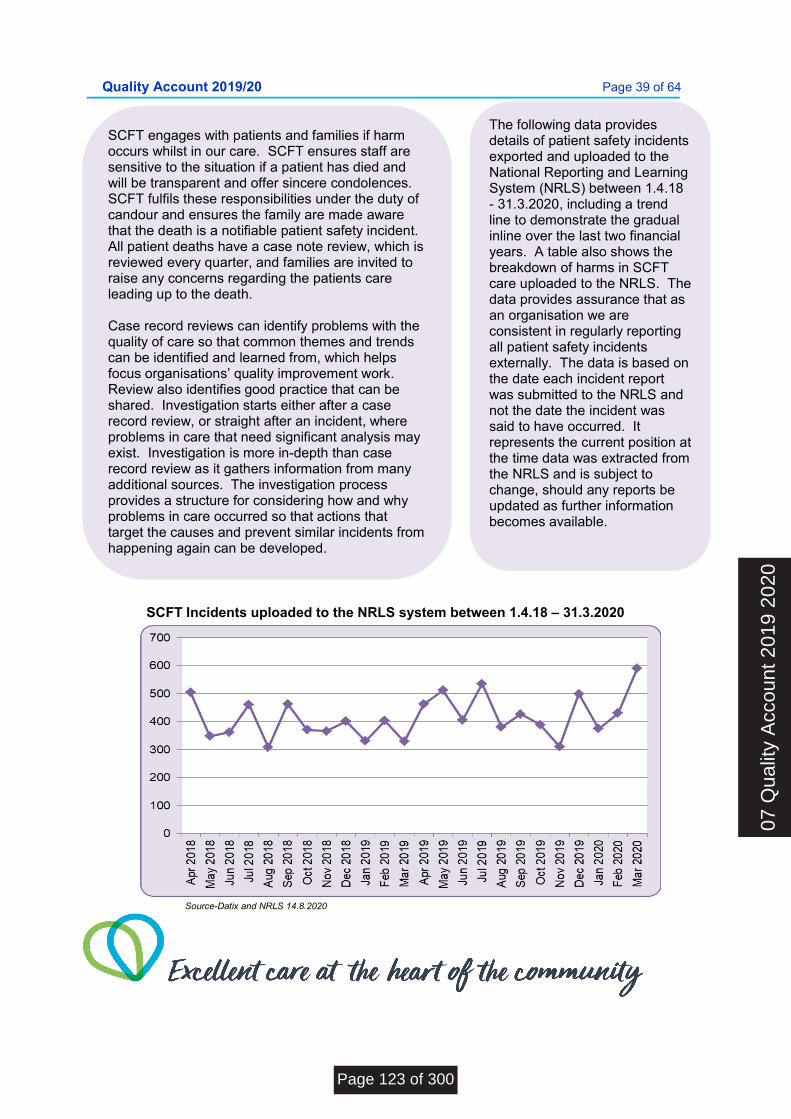
Quality Account 2019/20 Page 39 of 64
SCFT Incidents uploaded to the NRLS system between 1.4.18 – 31.3.2020
Source-Datix and NRLS 14.8.2020
SCFT engages with patients and families if harm occurs whilst in our care. SCFT ensures staff are sensitive to the situation if a patient has died and will be transparent and offer sincere condolences. SCFT fulfils these responsibilities under the duty of candour and ensures the family are made aware that the death is a notifiable patient safety incident. All patient deaths have a case note review, which is reviewed every quarter, and families are invited to raise any concerns regarding the patients care leading up to the death. Case record reviews can identify problems with the quality of care so that common themes and trends can be identified and learned from, which helps focus organisations’ quality improvement work. Review also identifies good practice that can be shared. Investigation starts either after a case record review, or straight after an incident, where problems in care that need significant analysis may exist. Investigation is more in-depth than case record review as it gathers information from many additional sources. The investigation process provides a structure for considering how and why problems in care occurred so that actions that target the causes and prevent similar incidents from happening again can be developed.
The following data provides details of patient safety incidents exported and uploaded to the National Reporting and Learning System (NRLS) between 1.4.18 - 31.3.2020, including a trend line to demonstrate the gradual inline over the last two financial years. A table also shows the breakdown of harms in SCFT care uploaded to the NRLS. The data provides assurance that as an organisation we are consistent in regularly reporting all patient safety incidents externally. The data is based on the date each incident report was submitted to the NRLS and not the date the incident was said to have occurred. It represents the current position at the time data was extracted from the NRLS and is subject to change, should any reports be updated as further information becomes available.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 123 of 300
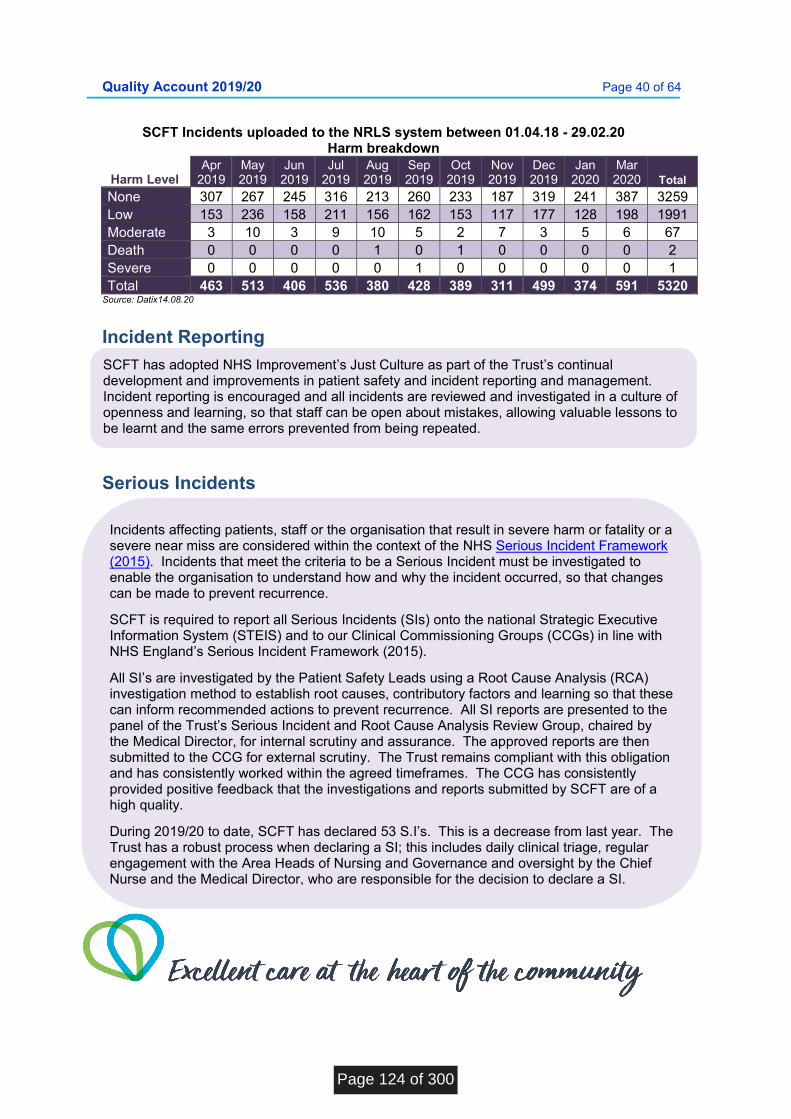
Quality Account 2019/20 Page 40 of 64
SCFT Incidents uploaded to the NRLS system between 01.04.18 - 29.02.20 Harm breakdown
Harm Level Apr
2019 May 2019
Jun 2019
Jul 2019
Aug 2019
Sep 2019
Oct 2019
Nov 2019
Dec 2019
Jan 2020
Mar 2020 Total
None 307 267 245 316 213 260 233 187 319 241 387 3259 Low 153 236 158 211 156 162 153 117 177 128 198 1991 Moderate 3 10 3 9 10 5 2 7 3 5 6 67 Death 0 0 0 0 1 0 1 0 0 0 0 2 Severe 0 0 0 0 0 1 0 0 0 0 0 1 Total 463 513 406 536 380 428 389 311 499 374 591 5320
Source: Datix14.08.20
Incident Reporting
Serious Incidents
Incidents affecting patients, staff or the organisation that result in severe harm or fatality or a severe near miss are considered within the context of the NHS Serious Incident Framework (2015). Incidents that meet the criteria to be a Serious Incident must be investigated to enable the organisation to understand how and why the incident occurred, so that changes can be made to prevent recurrence.
SCFT is required to report all Serious Incidents (SIs) onto the national Strategic Executive Information System (STEIS) and to our Clinical Commissioning Groups (CCGs) in line with NHS England’s Serious Incident Framework (2015).
All SI’s are investigated by the Patient Safety Leads using a Root Cause Analysis (RCA) investigation method to establish root causes, contributory factors and learning so that these can inform recommended actions to prevent recurrence. All SI reports are presented to the panel of the Trust’s Serious Incident and Root Cause Analysis Review Group, chaired by the Medical Director, for internal scrutiny and assurance. The approved reports are then submitted to the CCG for external scrutiny. The Trust remains compliant with this obligation and has consistently worked within the agreed timeframes. The CCG has consistently provided positive feedback that the investigations and reports submitted by SCFT are of a high quality.
During 2019/20 to date, SCFT has declared 53 S.I’s. This is a decrease from last year. The Trust has a robust process when declaring a SI; this includes daily clinical triage, regular engagement with the Area Heads of Nursing and Governance and oversight by the Chief Nurse and the Medical Director, who are responsible for the decision to declare a SI.
SCFT has adopted NHS Improvement’s Just Culture as part of the Trust’s continual development and improvements in patient safety and incident reporting and management. Incident reporting is encouraged and all incidents are reviewed and investigated in a culture of openness and learning, so that staff can be open about mistakes, allowing valuable lessons to be learnt and the same errors prevented from being repeated.
Page 124 of 300
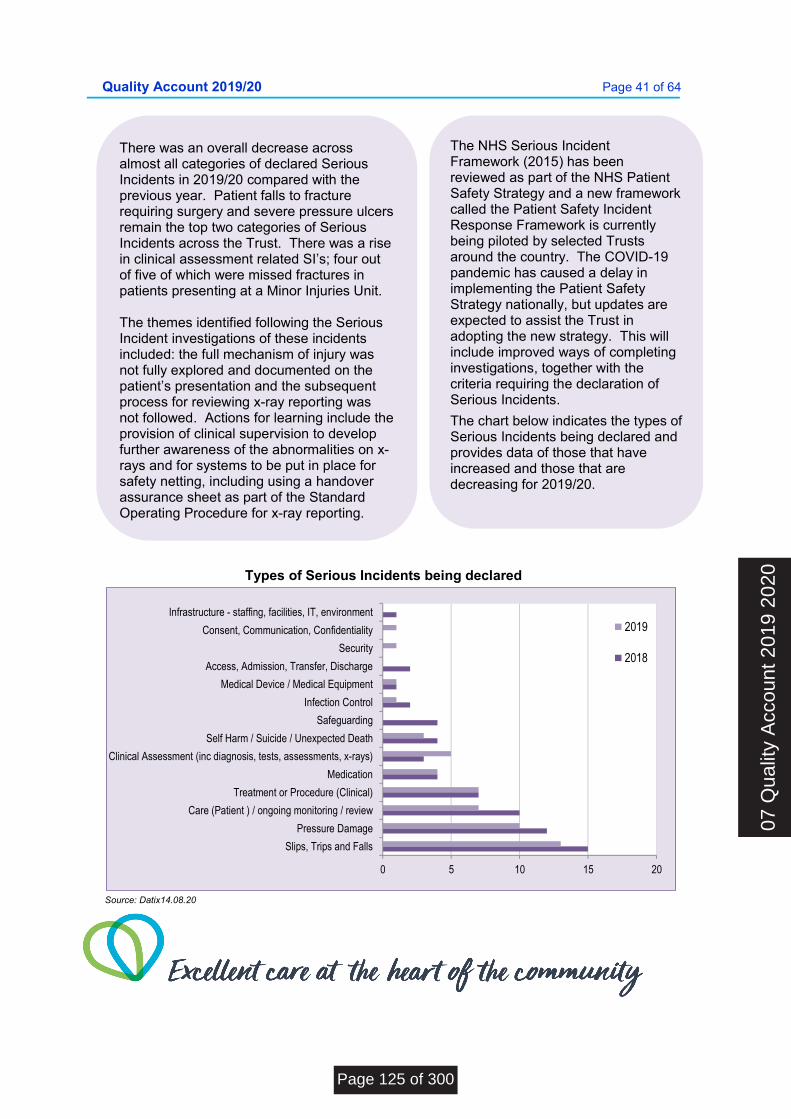
Quality Account 2019/20 Page 41 of 64
Types of Serious Incidents being declared
0 5 10 15 20
Slips, Trips and Falls
Pressure Damage
Care (Patient ) / ongoing monitoring / review
Treatment or Procedure (Clinical)
Medication
Clinical Assessment (inc diagnosis, tests, assessments, x-rays)
Self Harm / Suicide / Unexpected Death
Safeguarding
Infection Control
Medical Device / Medical Equipment
Access, Admission, Transfer, Discharge
Security
Consent, Communication, Confidentiality
Infrastructure - staffing, facilities, IT, environment2019
2018
Source: Datix14.08.20
The NHS Serious Incident Framework (2015) has been reviewed as part of the NHS Patient Safety Strategy and a new framework called the Patient Safety Incident Response Framework is currently being piloted by selected Trusts around the country. The COVID-19 pandemic has caused a delay in implementing the Patient Safety Strategy nationally, but updates are expected to assist the Trust in adopting the new strategy. This will include improved ways of completing investigations, together with the criteria requiring the declaration of Serious Incidents.
The chart below indicates the types of Serious Incidents being declared and provides data of those that have increased and those that are decreasing for 2019/20.
There was an overall decrease across almost all categories of declared Serious Incidents in 2019/20 compared with the previous year. Patient falls to fracture requiring surgery and severe pressure ulcers remain the top two categories of Serious Incidents across the Trust. There was a rise in clinical assessment related SI’s; four out of five of which were missed fractures in patients presenting at a Minor Injuries Unit. The themes identified following the Serious Incident investigations of these incidents included: the full mechanism of injury was not fully explored and documented on the patient’s presentation and the subsequent process for reviewing x-ray reporting was not followed. Actions for learning include the provision of clinical supervision to develop further awareness of the abnormalities on x-rays and for systems to be put in place for safety netting, including using a handover assurance sheet as part of the Standard Operating Procedure for x-ray reporting.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 125 of 300

Quality Account 2019/20 Page 42 of 64
Why did we choose this measure? The Trust continues to perform significantly better than the national average. The total number of people waiting has increased since last year. The table below shows the numbers of patients waiting from referral to start their elective treatment (incomplete patient pathways) up to M12/ Mar 2020 for our consultant-led services. SCFT continues to carefully monitor all incomplete pathways to assure exact reporting. The Performance Team works closely with all Services to reduce reporting errors and ensure that all electronic records are up to date and accurate. Breach reasons are recorded and retained as evidence and to promote understanding.
Mandatory Indicator (Effectiveness) Incomplete pathways within 18 weeks
Part 3 - Other Information This section documents the quality of services SCFT provides by reviewing progress against indicators for quality improvement, and feedback from sources such as incident reporting, service user and staff feedback.
The three key measures are from the quality domains: patient safety, patient experience and clinical effectiveness, some of which reflect the priorities for improvement.
As set out in national guidance, usually the Trust’s external auditors, Grant Thornton, would have tested two mandatory indicators relevant to the Trust and one local indicator selected by Trust Governors. This requirement was removed for this year due to COVID-19.
The data for all indicators selected in Part 3 – Other Information - is governed by standard national definitions.
Page 126 of 300
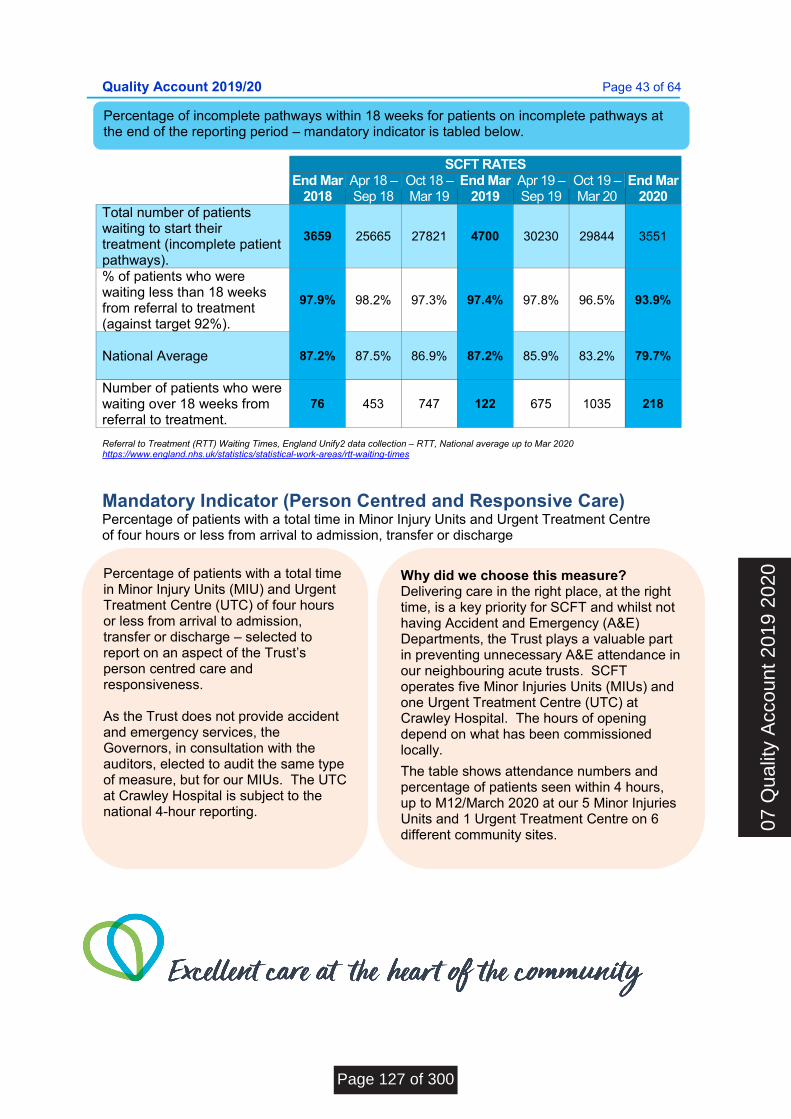
Quality Account 2019/20 Page 43 of 64
SCFT RATES
End Mar
2018 Apr 18 – Sep 18
Oct 18 – Mar 19
End Mar 2019
Apr 19 – Sep 19
Oct 19 – Mar 20
End Mar 2020
Total number of patients waiting to start their treatment (incomplete patient pathways).
3659 25665 27821 4700 30230 29844 3551
% of patients who were waiting less than 18 weeks from referral to treatment (against target 92%).
97.9% 98.2% 97.3% 97.4%
97.8%
96.5% 93.9%
National Average
87.2% 87.5% 86.9% 87.2% 85.9% 83.2% 79.7%
Number of patients who were waiting over 18 weeks from referral to treatment.
76 453 747 122 675 1035 218
Referral to Treatment (RTT) Waiting Times, England Unify2 data collection – RTT, National average up to Mar 2020 https://www.england.nhs.uk/statistics/statistical-work-areas/rtt-waiting-times
Mandatory Indicator (Person Centred and Responsive Care) Percentage of patients with a total time in Minor Injury Units and Urgent Treatment Centre of four hours or less from arrival to admission, transfer or discharge
Percentage of patients with a total time in Minor Injury Units (MIU) and Urgent Treatment Centre (UTC) of four hours or less from arrival to admission, transfer or discharge – selected to report on an aspect of the Trust’s person centred care and responsiveness.
As the Trust does not provide accident and emergency services, the Governors, in consultation with the auditors, elected to audit the same type of measure, but for our MIUs. The UTC at Crawley Hospital is subject to the national 4-hour reporting.
Why did we choose this measure? Delivering care in the right place, at the right time, is a key priority for SCFT and whilst not having Accident and Emergency (A&E) Departments, the Trust plays a valuable part in preventing unnecessary A&E attendance in our neighbouring acute trusts. SCFT operates five Minor Injuries Units (MIUs) and one Urgent Treatment Centre (UTC) at Crawley Hospital. The hours of opening depend on what has been commissioned locally.
The table shows attendance numbers and percentage of patients seen within 4 hours, up to M12/March 2020 at our 5 Minor Injuries Units and 1 Urgent Treatment Centre on 6 different community sites. .
Percentage of incomplete pathways within 18 weeks for patients on incomplete pathways at the end of the reporting period – mandatory indicator is tabled below.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 127 of 300
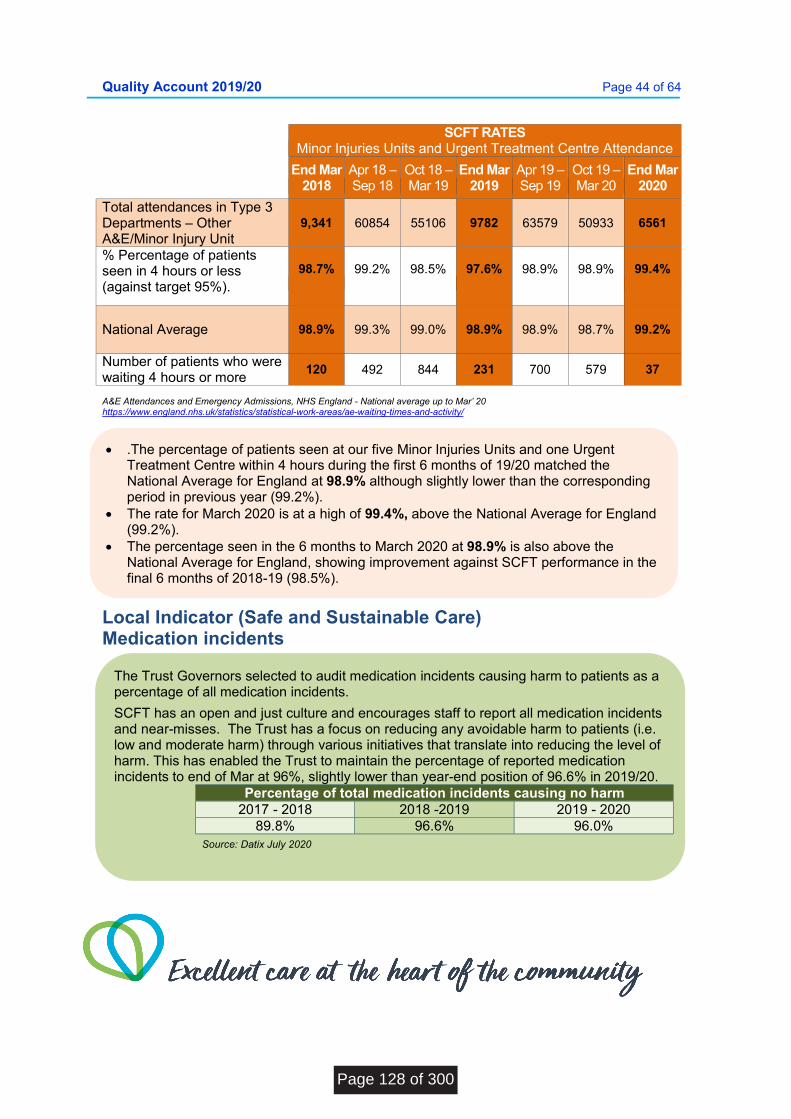
Quality Account 2019/20 Page 44 of 64
SCFT RATES
Minor Injuries Units and Urgent Treatment Centre Attendance
End Mar 2018
Apr 18 – Sep 18
Oct 18 – Mar 19
End Mar 2019
Apr 19 – Sep 19
Oct 19 – Mar 20
End Mar 2020
Total attendances in Type 3 Departments – Other A&E/Minor Injury Unit
9,341 60854 55106 9782 63579 50933 6561
% Percentage of patients seen in 4 hours or less (against target 95%).
98.7%
99.2%
98.5%
97.6%
98.9%
98.9%
99.4%
National Average
98.9% 99.3% 99.0% 98.9% 98.9% 98.7% 99.2%
Number of patients who were waiting 4 hours or more
120 492 844 231 700 579 37
A&E Attendances and Emergency Admissions, NHS England - National average up to Mar’ 20 https://www.england.nhs.uk/statistics/statistical-work-areas/ae-waiting-times-and-activity/
Local Indicator (Safe and Sustainable Care) Medication incidents
.The percentage of patients seen at our five Minor Injuries Units and one Urgent Treatment Centre within 4 hours during the first 6 months of 19/20 matched the National Average for England at 98.9% although slightly lower than the corresponding period in previous year (99.2%).
The rate for March 2020 is at a high of 99.4%, above the National Average for England (99.2%).
The percentage seen in the 6 months to March 2020 at 98.9% is also above the National Average for England, showing improvement against SCFT performance in the final 6 months of 2018-19 (98.5%).
The Trust Governors selected to audit medication incidents causing harm to patients as a percentage of all medication incidents.
SCFT has an open and just culture and encourages staff to report all medication incidents and near-misses. The Trust has a focus on reducing any avoidable harm to patients (i.e. low and moderate harm) through various initiatives that translate into reducing the level of harm. This has enabled the Trust to maintain the percentage of reported medication incidents to end of Mar at 96%, slightly lower than year-end position of 96.6% in 2019/20.
Percentage of total medication incidents causing no harm 2017 - 2018 2018 -2019 2019 - 2020
89.8% 96.6% 96.0%
Source: Datix July 2020
Page 128 of 300
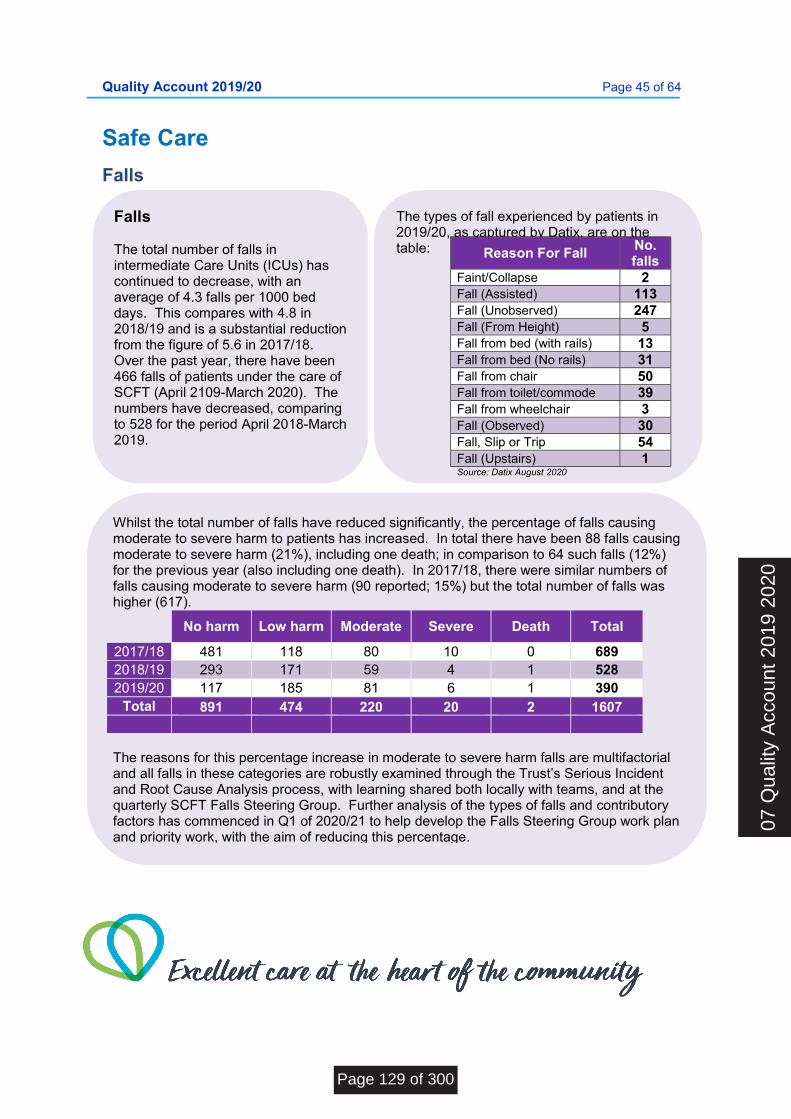
Quality Account 2019/20 Page 45 of 64
The types of fall experienced by patients in 2019/20, as captured by Datix, are on the table:
Safe Care
Falls
Reason For Fall No. falls
Faint/Collapse 2 Fall (Assisted) 113 Fall (Unobserved) 247 Fall (From Height) 5 Fall from bed (with rails) 13 Fall from bed (No rails) 31 Fall from chair 50 Fall from toilet/commode 39 Fall from wheelchair 3 Fall (Observed) 30 Fall, Slip or Trip 54 Fall (Upstairs) 1 Source: Datix August 2020
Falls The total number of falls in intermediate Care Units (ICUs) has continued to decrease, with an average of 4.3 falls per 1000 bed days. This compares with 4.8 in 2018/19 and is a substantial reduction from the figure of 5.6 in 2017/18. Over the past year, there have been 466 falls of patients under the care of SCFT (April 2109-March 2020). The numbers have decreased, comparing to 528 for the period April 2018-March 2019.
Whilst the total number of falls have reduced significantly, the percentage of falls causing moderate to severe harm to patients has increased. In total there have been 88 falls causing moderate to severe harm (21%), including one death; in comparison to 64 such falls (12%) for the previous year (also including one death). In 2017/18, there were similar numbers of falls causing moderate to severe harm (90 reported; 15%) but the total number of falls was higher (617).
No harm Low harm Moderate Severe Death Total
2017/18 481 118 80 10 0 689 2018/19 293 171 59 4 1 528 2019/20 117 185 81 6 1 390
Total 891 474 220 20 2 1607
The reasons for this percentage increase in moderate to severe harm falls are multifactorial and all falls in these categories are robustly examined through the Trust’s Serious Incident and Root Cause Analysis process, with learning shared both locally with teams, and at the quarterly SCFT Falls Steering Group. Further analysis of the types of falls and contributory factors has commenced in Q1 of 2020/21 to help develop the Falls Steering Group work plan and priority work, with the aim of reducing this percentage.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 129 of 300
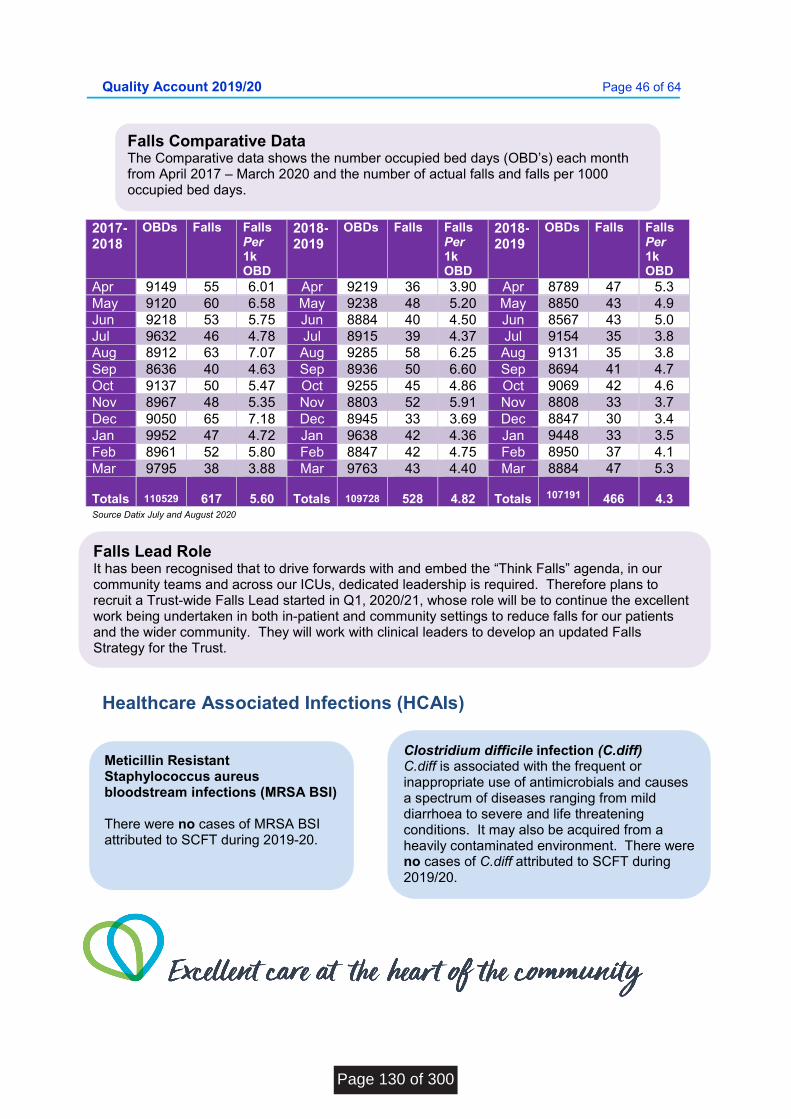
Quality Account 2019/20 Page 46 of 64
2017-2018
OBDs Falls Falls Per 1k OBD
2018-2019
OBDs Falls Falls Per 1k OBD
2018-2019
OBDs Falls Falls Per 1k OBD
Apr 9149 55 6.01 Apr 9219 36 3.90 Apr 8789 47 5.3 May 9120 60 6.58 May 9238 48 5.20 May 8850 43 4.9 Jun 9218 53 5.75 Jun 8884 40 4.50 Jun 8567 43 5.0 Jul 9632 46 4.78 Jul 8915 39 4.37 Jul 9154 35 3.8 Aug 8912 63 7.07 Aug 9285 58 6.25 Aug 9131 35 3.8 Sep 8636 40 4.63 Sep 8936 50 6.60 Sep 8694 41 4.7 Oct 9137 50 5.47 Oct 9255 45 4.86 Oct 9069 42 4.6 Nov 8967 48 5.35 Nov 8803 52 5.91 Nov 8808 33 3.7 Dec 9050 65 7.18 Dec 8945 33 3.69 Dec 8847 30 3.4 Jan 9952 47 4.72 Jan 9638 42 4.36 Jan 9448 33 3.5 Feb 8961 52 5.80 Feb 8847 42 4.75 Feb 8950 37 4.1 Mar 9795 38 3.88 Mar 9763 43 4.40 Mar 8884 47 5.3 Totals
110529
617
5.60
Totals
109728
528
4.82
Totals
107191
466
4.3
Source Datix July and August 2020
Healthcare Associated Infections (HCAIs)
Falls Comparative Data The Comparative data shows the number occupied bed days (OBD’s) each month from April 2017 – March 2020 and the number of actual falls and falls per 1000 occupied bed days.
Falls Lead Role It has been recognised that to drive forwards with and embed the “Think Falls” agenda, in our community teams and across our ICUs, dedicated leadership is required. Therefore plans to recruit a Trust-wide Falls Lead started in Q1, 2020/21, whose role will be to continue the excellent work being undertaken in both in-patient and community settings to reduce falls for our patients and the wider community. They will work with clinical leaders to develop an updated Falls Strategy for the Trust.
Meticillin Resistant Staphylococcus aureus bloodstream infections (MRSA BSI) There were no cases of MRSA BSI attributed to SCFT during 2019-20.
Clostridium difficile infection (C.diff) C.diff is associated with the frequent or inappropriate use of antimicrobials and causes a spectrum of diseases ranging from mild diarrhoea to severe and life threatening conditions. It may also be acquired from a heavily contaminated environment. There were no cases of C.diff attributed to SCFT during 2019/20.
Page 130 of 300

Quality Account 2019/20 Page 47 of 64
Never Events
Gram Negative Blood Stream Infections (GNBSI) (Most commonly E.coli, Pseudomonas or Klebsiella)
From April 2017, a new DH target to reduce gram-negative blood stream infections was introduced. A 50% reduction of Gram Negative Bloodstream Infections (GNBSIs) is expected by 2023 (E.coli bloodstream infection is the largest most prevalent group of GNBSI). SCFT continues to track and monitor GNBSI whenever we receive information from our acute providers.
There were 5 cases of GNBSI in Intermediate Care Units (ICUs) during 2019/20. This is a reduction of 1 from last year.
Our IP&C team led on the Root Cause Analysis (RCA) for four cases of E.coli blood stream infection and one case of Pseudomonas aeruginosa infection in intermediate care units. Two of the patients had urinary catheters and some learning was identified regarding sampling which has been incorporated into our work regarding care of urinary catheters and the daily catheter record (DCR).
Never Events are serious, principally preventable patient safety incidents that should not occur in healthcare. In 2019/20 there were no Never Events reported by SCFT.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 131 of 300
Quality Account 2019/20 Page 48 of 64
Effective Care
Freedom to Speak Up
Key activities during 2019/20 included:
The publication of Sir Robert Francis’s Freedom to Speak Up review was published in February 2015 and highlighted the need for organisational culture change across the NHS.
The role of the Freedom to Speak Up (FTSU) Guardian is to enable and support staff to raise concerns and ensure their voice is heard clearly at a senior level within the organisation. The FTSU Guardian is an alternative route for issues of concern to be raised at the highest level and the post holder has a clear remit from the Chief Executive and the Trust Board to act candidly, with complete autonomy from the management team where necessary. A FTSU Guardian has been in post for just over 3.5 years at SCFT. It is clear that the visibility of the role has increased and this has resulted in increasing numbers of staff accessing the FTSU Guardian support.
The SCFT Guardian delivered training to University of Brighton student nurses as part of their new patient safety module.
The Guardian delivered team talks (both operational and corporate) during the year and led a session for Area Management Teams in each of the four areas of the Trust.
In January, a session was specifically held for middle managers who attend the Wider Executive Leadership Team meeting. This provided an opportunity for some feedback from managers on FTSU in SCFT and will be incorporated into the FTSU strategy.
For the first time in October 2019, the National Guardian Office (NGO) published a FTSU Index to monitor speaking up culture in the NHS. NHS England commissioned the NGO to develop the index based on four questions from the annual NHS staff survey. It was published again in July 2020 based on the most recent NHS staff survey data.
In quarter 3 of 2019, SCFT’s FTSU ambassadors were launched. Eight ambassadors have been appointed, with a rolling training programme and quarterly group supervision facilitated by the Guardian.
October is assigned by the National Guardian Office as National Speak Up month. The FTSU Guardian used this opportunity to visit many areas in the trust visiting 17 sites in eight days.
The Guardian was interviewed for a podcast by The Business of Healthcare with Tara Humphrey: Episode 16: Influencing a Culture to Speak Up and this was launched during the month on social media.
The Guardian regularly engages with the four staff networks (BAME, Disability, LGBT+ and Religion and Belief) to ensure the voices of those potentially vulnerable groups can be heard.
Links have been established with the Volunteer Team and Practice Education Team to ensure the induction they provide to our students and volunteers includes FTSU as a core component.
Page 132 of 300
Quality Account 2019/20 Page 49 of 64
NICE (National Institute for Health and Care Excellence) Guidance
Guardian of Safe Working
SCFT scored 84% in the 2020 index. This was a percentage improvement from the previous year (83%) and is a testament to the work of many in the organisation to create a culture that places the principles of FTSU at the heart of what we do.
SCFT was ranked joint 14th nationally out of all NHS trusts and 6th out of Community Trusts.
During 2020/21 a FTSU strategy and board self-assessment against national FTSU standards plans will be developed, thus ensuring a clear vision and direction for Speaking Up.
SCFT has a systematic process in place for the dissemination, review, implementation and monitoring of applicable NICE guidance and use of the guidance to assess practice. Clinical Governance and Harm Free Groups and Area Management Teams are responsible for monitoring progress and implementation of NICE Guidance, overseen by the Clinical Effectiveness Group and the Trust wide Governance Group.
The current SCFT timescale for implementing NICE guidance is 3 years. One of SCFT’s priorities for improvement 2020/21 will be to ensure where guidance is relevant to SCFT we will aim to implement within the shortest time practicable. This will lead to an increase in assurance that patients are receiving the most effective care as soon as possible increasing their confidence that they are receiving excellent care in line with NICE guidance.
The Guardian of Safe Working reports quarterly to the Board on matters relating to the work of the Guardian. The Board also receive a consolidated annual report. The Trust has 5 (5.0 WTE) established training posts and the total vacancy (average WTE) in 2019/20 was 1.05. The consolidated annual report to the Board details the reasons for the vacancy and the actions taken to reduce vacancy.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 133 of 300

Quality Account 2019/20 Page 50 of 64
Central Alert System
The Department of Health (DH) Central Alert System (CAS) is designed to rapidly disseminate important safety and device alerts to nominated leads in NHS Trusts in a consistent and streamlined way for onward transmission to those who need to take action. Trusts are required to acknowledge receipt of each alert and respond as relevant within specified timescales. Summary of SCFT responses to CAS Alerts received annually since 2015/16. 2015/16 2016/17 2017/18 2018/19 2019/20
Total number of alerts received
132 139 125 110 137
Acknowledged within 2 working days
132
(100%)
132
(95%)
123
(98%)
107
(97%)
137
(100%) Found to be applicable to SCFT for action
19
(14%)
14
(10%)
11
(9%)
25
(23%)
23
(18%) Applicable alert responses within prescribed timescales
18
(95%)
14
(100%)
11
(100%)
23
(92%)
23
(100%)
Source: SCFT Safety Alert System Datix/Safeguard system 2019/20 data 7.8.2020.
All alerts received within 2019/20 were acknowledged within the prescribed timeframe. All alerts that were applicable to SCFT for action were closed within the deadline given, with satisfactory levels of assurance. One alert originally passed its deadline date due to organisations being given one working day to action the alert and alerts being issued on a Friday. However, this alert was then superseded by an updated version and therefore it does not go down as a breach, either internally or externally. Where responses are not fully completed within the prescribed timescales, remedial works/improvements are commenced and the details of work undertaken by SCFT loaded onto the CAS system to evidence the mitigation and assurance measures, and when compliance is anticipated.
Page 134 of 300
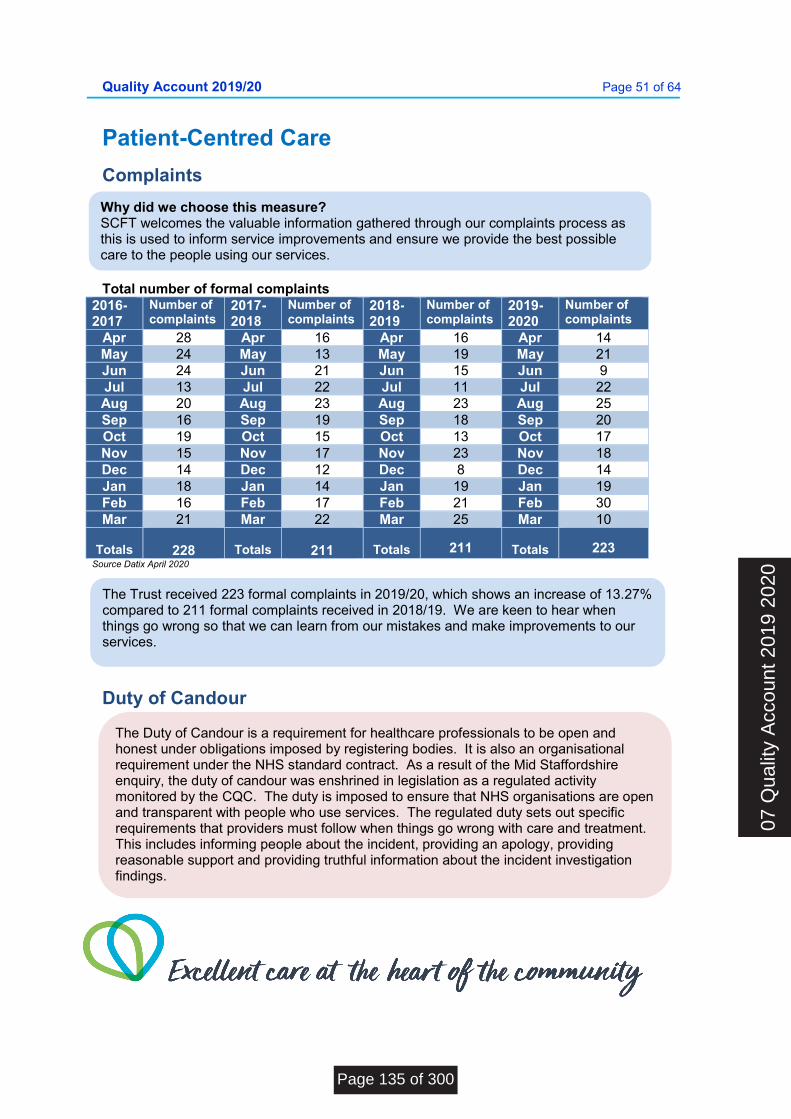
Quality Account 2019/20 Page 51 of 64
Patient-Centred Care
Complaints Total number of formal complaints
2016-2017
Number of complaints
2017-2018
Number of complaints
2018-2019
Number of complaints
2019-2020
Number of complaints
Apr 28 Apr 16 Apr 16 Apr 14 May 24 May 13 May 19 May 21 Jun 24 Jun 21 Jun 15 Jun 9 Jul 13 Jul 22 Jul 11 Jul 22 Aug 20 Aug 23 Aug 23 Aug 25 Sep 16 Sep 19 Sep 18 Sep 20 Oct 19 Oct 15 Oct 13 Oct 17 Nov 15 Nov 17 Nov 23 Nov 18 Dec 14 Dec 12 Dec 8 Dec 14 Jan 18 Jan 14 Jan 19 Jan 19 Feb 16 Feb 17 Feb 21 Feb 30 Mar 21 Mar 22 Mar 25 Mar 10
Totals
228
Totals
211
Totals
211
Totals
223 Source Datix April 2020
Duty of Candour
Why did we choose this measure? SCFT welcomes the valuable information gathered through our complaints process as this is used to inform service improvements and ensure we provide the best possible care to the people using our services.
The Trust received 223 formal complaints in 2019/20, which shows an increase of 13.27% compared to 211 formal complaints received in 2018/19. We are keen to hear when things go wrong so that we can learn from our mistakes and make improvements to our services.
The Duty of Candour is a requirement for healthcare professionals to be open and honest under obligations imposed by registering bodies. It is also an organisational requirement under the NHS standard contract. As a result of the Mid Staffordshire enquiry, the duty of candour was enshrined in legislation as a regulated activity monitored by the CQC. The duty is imposed to ensure that NHS organisations are open and transparent with people who use services. The regulated duty sets out specific requirements that providers must follow when things go wrong with care and treatment. This includes informing people about the incident, providing an apology, providing reasonable support and providing truthful information about the incident investigation findings.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 135 of 300
Quality Account 2019/20 Page 52 of 64
Staff Survey
The application of the legal duty of candour is now monitored through the Datix incident management system, enabling the patient safety team to audit that the duty of candour procedure is being followed. A duty of candour tracker has also been developed to be scrutinised at Serious Incident and Root Cause Analysis Review Group (SIRCARG).
A review of the process for Q4 2019/20 and Q1 2020/21 has identified that the duty of candour was required for 32 incidents causing significant harm. 19 of those have had the duty completed and 13 have been initiated and remain in progress to enable the sharing of investigation findings to complete the process.
During 2018, training for staff was provided by the Patient Safety Leads, to help staff understand the regulation and to empower them to say sorry when an incident occurs.
The plan was to continue this training in 2019, but capacity within the patient safety team prevented this being continued. The team is currently working with the Professional Head of Nursing and Education to develop a course accessible for staff on-line. To further support staff to follow the duty of candour process, senior managers are prompted at the time of the incident, of the need to follow the duty of candour procedure.
The NHS staff survey is conducted annually. From 2018 onwards, the results from questions are grouped to give scores in ten indicators. The indicator scores are based on a score out of 10 for certain questions, with the indicator score being the average of those.
The response rate to the 2019 survey among trust staff was 66% (2018: 57%). Scores for each indicator together with that of the survey-benchmarking group (Community Trusts) are presented overleaf.
In 2019, the results showed that: 71% would recommend the Trust as
an employer. 77% describe themselves as
enthusiastic about their jobs 79% would recommend our services
to friends and relatives These positive results are a continuation of a trend of improvement in recent years. The percentage of people that recommend the Trust as a place to work rose from 66% in 2017 to 69% in 2018 and last year reached 71%.
Areas where we want to do better in 2020/21 include: Reduce aggression, violence and
abuse experienced by our staff from patients and their families, our own staff and colleagues from partner organisations we work with and this links with one of our priorities for improvement.
Reduce experienced discrimination relating to disability and ethnicity.
Do more to share patient and service user feedback to drive improvements
The improvements above will be delivered through established communication and engagement channels at the Trust, including the use of social media.
Page 136 of 300
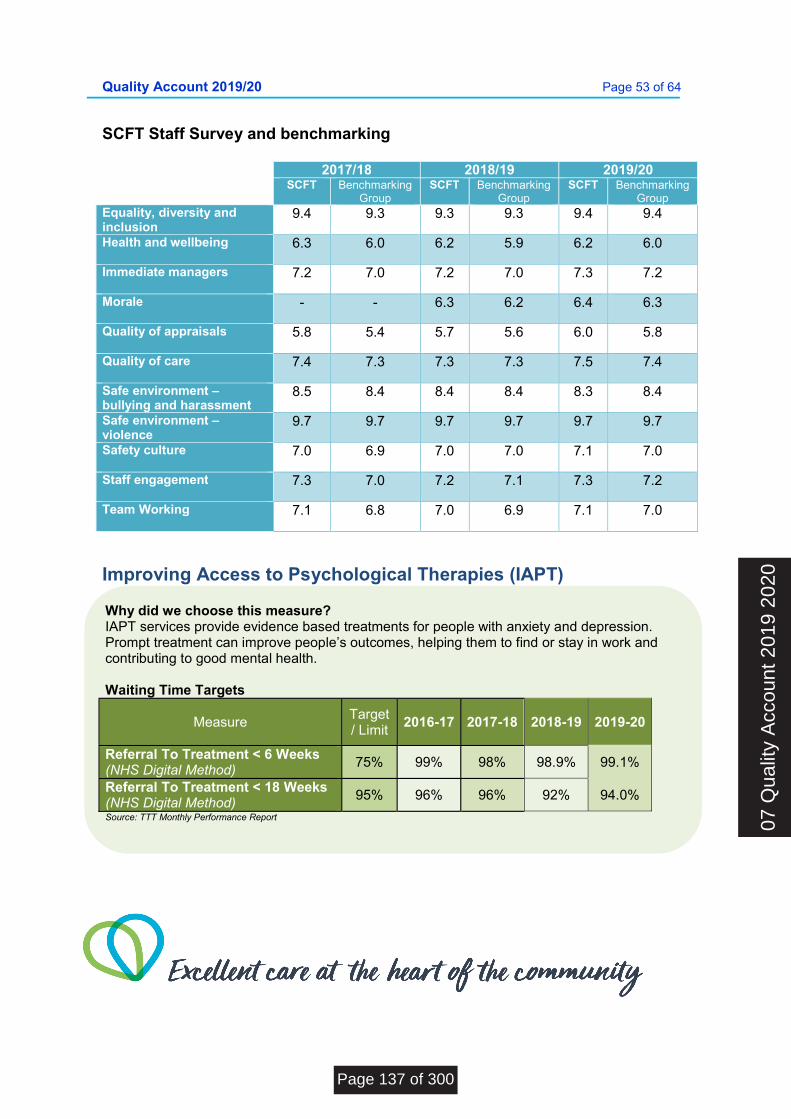
Quality Account 2019/20 Page 53 of 64
SCFT Staff Survey and benchmarking
2017/18 2018/19 2019/20 SCFT Benchmarking
Group SCFT Benchmarking
Group SCFT Benchmarking
Group Equality, diversity and inclusion
9.4 9.3 9.3 9.3 9.4 9.4
Health and wellbeing
6.3 6.0 6.2 5.9 6.2 6.0
Immediate managers
7.2 7.0 7.2 7.0 7.3 7.2
Morale
- - 6.3 6.2 6.4 6.3
Quality of appraisals
5.8 5.4 5.7 5.6 6.0 5.8
Quality of care
7.4 7.3 7.3 7.3 7.5 7.4
Safe environment – bullying and harassment
8.5 8.4 8.4 8.4 8.3 8.4
Safe environment – violence
9.7 9.7 9.7 9.7 9.7 9.7
Safety culture
7.0 6.9 7.0 7.0 7.1 7.0
Staff engagement
7.3 7.0 7.2 7.1 7.3 7.2
Team Working
7.1 6.8 7.0 6.9 7.1 7.0
Improving Access to Psychological Therapies (IAPT)
Why did we choose this measure? IAPT services provide evidence based treatments for people with anxiety and depression. Prompt treatment can improve people’s outcomes, helping them to find or stay in work and contributing to good mental health. Waiting Time Targets
Measure Target / Limit
2016-17 2017-18 2018-19 2019-20
Referral To Treatment < 6 Weeks (NHS Digital Method)
75% 99% 98% 98.9% 99.1%
Referral To Treatment < 18 Weeks (NHS Digital Method)
95% 96% 96% 92% 94.0%
Source: TTT Monthly Performance Report 07
Qua
lity
Acc
ount
201
9 20
20
Page 137 of 300

Quality Account 2019/20 Page 54 of 64
Annual Organisational Audit (AOA) on Medical Appraisal and Revalidation
Medical Revalidation was launched in 2012 to strengthen the way that doctors are regulated, with the aim of improving the quality of care provided to patients, improving patient safety and increasing public trust and confidence in the medical system. Provider organisations have a statutory duty to support their Responsible Officers in discharging their duties under the Responsible Officer Regulations and it is expected that provider boards will oversee compliance by: Monitoring the frequency and quality
of medical appraisals in their organisations;
Checking there are effective systems in place for monitoring the conduct and performance of their doctors;
Confirming that feedback from
patients is sought periodically so that their views can inform the appraisal and revalidation process for their doctors; and
Ensuring that appropriate pre-
employment background checks (including pre-engagement for locums) are carried out to ensure that medical practitioners have qualifications and experience appropriate to the work performed.
As at 31 March 2019, there were 57 doctors with a prescribed connection to Sussex Community NHS Foundation Trust and all doctors were allocated a trained appraiser. On 19 March 2020, NHS England announced an immediate suspension of annual appraisals for doctors working in the NHS in light of Government advice on managing the COVID-19 pandemic. Fifty-three appraisals were completed up until the suspension date, a 93% compliance rate for the 2019/20 appraisal year. Revalidation recommendations to the General Medical Council (GMC) were all carried out in a timely manner within year.
Page 138 of 300
Quality Account 2019/20 Page 55 of 64
Annex 1 - Statements from External Stakeholders
Where 50% or more of the relevant health services that the NHS foundation trust directly provides or sub-contracts during the reporting period are provided under contracts, agreements or arrangements with NHS England, the trust must provide a draft copy of its quality account to NHS England for comment prior to publication and should include any comments made in its published report. This does not apply to SCFT. Where the above does not apply, SCFT must provide a copy of the draft quality account to the clinical commissioning group, which has responsibility for the largest number of people to whom the trust has provided relevant health services during the reporting period for comment prior to publication and should include any comments made in its published report. NHS Foundation Trusts must also send draft copies of their quality account to their local Healthwatch organisation and overview and scrutiny committee (OSC) for comment prior to publication, and should include any comments made in their final published report.
The commissioners have a legal obligation to review and comment, while local Healthwatch organisations and OSCs will be offered the opportunity to comment on a voluntary basis. The organisations invited to review and comment on SCFT’s Quality Account were: Healthwatch Brighton & Hove
Healthwatch West Sussex
West Sussex County Council HASC
Brighton & Hove City Council’s Health and Wellbeing Overview and Scrutiny Committee (HWOSC)
East Sussex County Council’s Health Overview and Scrutiny Committee (HOSC)
NHS Brighton & Hove Clinical Commissioning Group
NHS Coastal Clinical Commissioning Group
NHS Crawley Clinical Commissioning Group
NHS High Weald Lewes Havens Clinical Commissioning Group
NHS Horsham and Mid Sussex Clinical Commissioning Group
Comments were received from Sussex NHS Commissioners, which can be read in the following pages.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 139 of 300
Quality Account 2019/20 Page 56 of 64
Comments from NHS Brighton and Hove CCG, NHS East Sussex CCG & NHS West Sussex CCG Working together as Sussex NHS Commissioners
Page 140 of 300
Quality Account 2019/20 Page 57 of 64
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 141 of 300
Quality Account 2019/20 Page 58 of 64
Sent on behalf of Cllr Colin Belsey, Chair of East Sussex HOSC
Dear Janet Parfitt
Thank you for providing the East Sussex Health Overview and Scrutiny Committee (HOSC) with the opportunity to comment on your Trust’s draft Quality Report 2019/20.
On this occasion the Committee has not provided a statement as we do not have any specific evidence to submit to you. However, we look forward to an ongoing involvement in the development of future Trust Quality Reports. Please contact Harvey Winder, Democratic Services Officer on 01273 481796 should you have any queries. Councillor Colin Belsey Chair Health Overview and Scrutiny Committee
Comments EMAIL
Page 142 of 300
Quality Account 2019/20 Page 59 of 64
Annex 2 - Statement of Directors’ Responsibilities for the Quality Account The Directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year. NHS Improvement has issued guidance to NHS foundation trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS foundation trust boards should put in place to support the data quality for the preparation of the quality report. In preparing the quality report, directors are required to take steps to satisfy themselves that:
the content of the quality report meets the requirements set out in the NHS foundation trust annual reporting manual 2019/20 and supporting guidance;
the content of the quality report is not inconsistent with internal and external sources of information including:
o board minutes and papers for the period April 2019 to May 2020; o papers relating to quality reported to the board over the period April 2019 to May
2020; o feedback from commissioners dated 27 October 2020; o feedback from Governors, dated March 2020; o the trust’s complaints report published under regulation 18 of the Local Authority
Social Services and NHS Complaints Regulations 2009, dated March 2020; o the latest national patient survey published March 2020; o the 2019 national staff survey, published March 2020; o the Head of Internal Audit’s annual opinion of the Trust’s control environment dated
May 2020; the quality report presents a balanced picture of the NHS foundation trust’s performance
over the period covered; the performance information reported in the quality report is reliable and accurate; there are proper internal controls over the collection and reporting of the measures of
performance included in the quality report, and these controls are subject to review to confirm that they are working effectively in practice;
the data underpinning the measures of performance reported in the quality report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review; and
the quality report has been prepared in accordance with NHS Improvement’s annual reporting manual and supporting guidance (which incorporates the Quality Accounts regulations) as well as the standards to support data quality for the preparation of the quality report.
The Directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the quality report. By order of the board. Peter Horn, Chairman
Siobhan Melia, Chief Executive
November 2020 November 2020
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 143 of 300
Quality Account 2019/20 Page 60 of 64
Conclusion This Quality Report 2019/20 reports on SCFT’s progress and performance against a wide range of priorities for improvement and indicators over the last year. These achievements have been made as a result of the commitment from our staff to deliver excellent care. Continuous improvement is a collective responsibility and we will continue to nurture and develop this culture as the Trust progresses in its quality improvement journey. Our ambition is for more and more of our services to be rated as ‘Outstanding’ against Care Quality Commission (CQC) standards and requirements. Achievement of the priorities for improvement for 2020/21 will contribute toward this aim. We will continue to monitor progress against these and look forward to reporting on our progress in the 2020/21 Quality Account. This Quality Account has been prepared in accordance with the Department of Health’s Quality Account Toolkit, first published in December 2010 and available electronically at www.dh.gov.uk/publications and NHS Improvement’s Detailed requirements for Quality Accounts for Foundation Trusts 2016/17, available electronically at https://improvement.nhs.uk/resources/nhs-foundation-Trust-quality-reports-201617-requirements/
Page 144 of 300
Quality Account 2019/20 Page 61 of 64
Feedback We would very much like to know what you think about our Quality Account. Please use this form to let us know what you think and what you would like us to include in next year’s.
1. Who are you?
Patient, family member or carer
Member Of Staff
Other (Please Specify)
2. What did you like about this report?
3. What could we improve?
4. What would you like us to include in next year’s report?
5. Are there any other comments you would like to make?
Thank you for taking the time to read this report and give us your comments. Please post this form to:
Siobhan Melia Chief Executive Sussex Community NHS Foundation Trust J Block, Brighton General Hospital Elm Grove, Brighton East Sussex BN2 3EW
You can also contact us via social media using:
twitter.com/nhs_sct facebook.com/sussexcommunitynhs
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 145 of 300
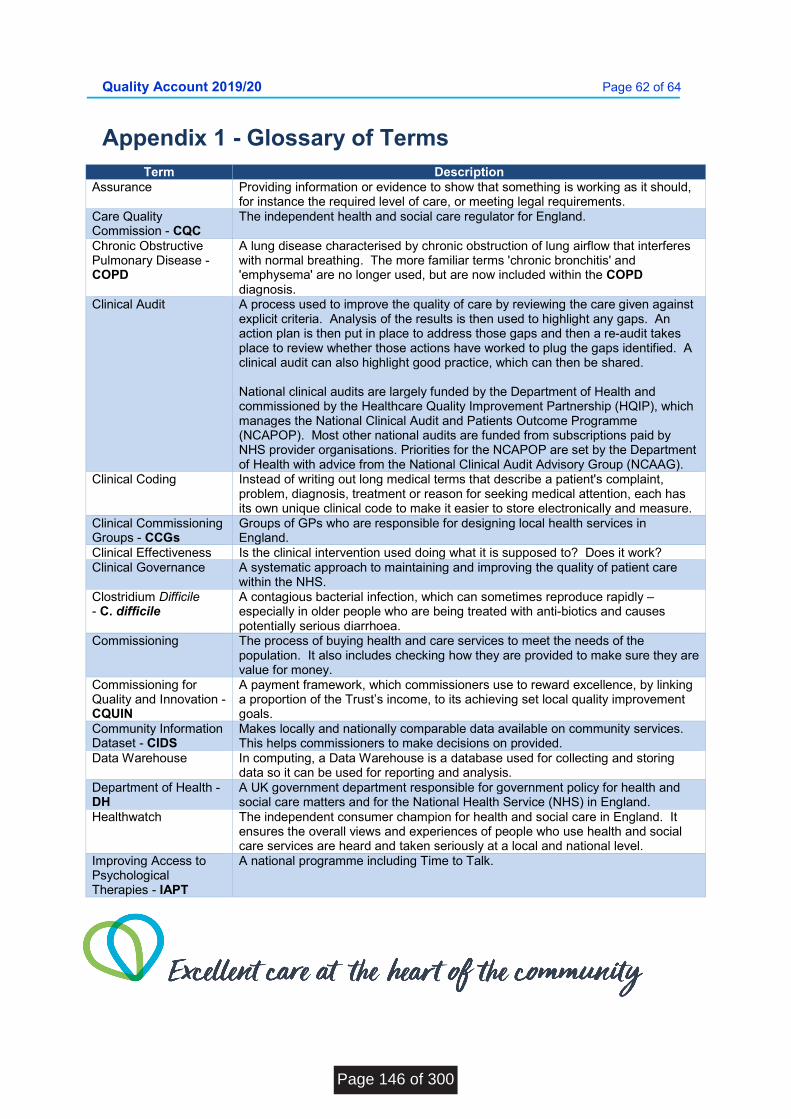
Quality Account 2019/20 Page 62 of 64
Appendix 1 - Glossary of Terms Term Description
Assurance Providing information or evidence to show that something is working as it should, for instance the required level of care, or meeting legal requirements.
Care Quality Commission - CQC
The independent health and social care regulator for England.
Chronic Obstructive Pulmonary Disease - COPD
A lung disease characterised by chronic obstruction of lung airflow that interferes with normal breathing. The more familiar terms 'chronic bronchitis' and 'emphysema' are no longer used, but are now included within the COPD diagnosis.
Clinical Audit A process used to improve the quality of care by reviewing the care given against explicit criteria. Analysis of the results is then used to highlight any gaps. An action plan is then put in place to address those gaps and then a re-audit takes place to review whether those actions have worked to plug the gaps identified. A clinical audit can also highlight good practice, which can then be shared. National clinical audits are largely funded by the Department of Health and commissioned by the Healthcare Quality Improvement Partnership (HQIP), which manages the National Clinical Audit and Patients Outcome Programme (NCAPOP). Most other national audits are funded from subscriptions paid by NHS provider organisations. Priorities for the NCAPOP are set by the Department of Health with advice from the National Clinical Audit Advisory Group (NCAAG).
Clinical Coding Instead of writing out long medical terms that describe a patient's complaint, problem, diagnosis, treatment or reason for seeking medical attention, each has its own unique clinical code to make it easier to store electronically and measure.
Clinical Commissioning Groups - CCGs
Groups of GPs who are responsible for designing local health services in England.
Clinical Effectiveness Is the clinical intervention used doing what it is supposed to? Does it work? Clinical Governance A systematic approach to maintaining and improving the quality of patient care
within the NHS. Clostridium Difficile - C. difficile
A contagious bacterial infection, which can sometimes reproduce rapidly – especially in older people who are being treated with anti-biotics and causes potentially serious diarrhoea.
Commissioning The process of buying health and care services to meet the needs of the population. It also includes checking how they are provided to make sure they are value for money.
Commissioning for Quality and Innovation - CQUIN
A payment framework, which commissioners use to reward excellence, by linking a proportion of the Trust’s income, to its achieving set local quality improvement goals.
Community Information Dataset - CIDS
Makes locally and nationally comparable data available on community services. This helps commissioners to make decisions on provided.
Data Warehouse In computing, a Data Warehouse is a database used for collecting and storing data so it can be used for reporting and analysis.
Department of Health - DH
A UK government department responsible for government policy for health and social care matters and for the National Health Service (NHS) in England.
Healthwatch The independent consumer champion for health and social care in England. It ensures the overall views and experiences of people who use health and social care services are heard and taken seriously at a local and national level.
Improving Access to Psychological Therapies - IAPT
A national programme including Time to Talk.
Page 146 of 300
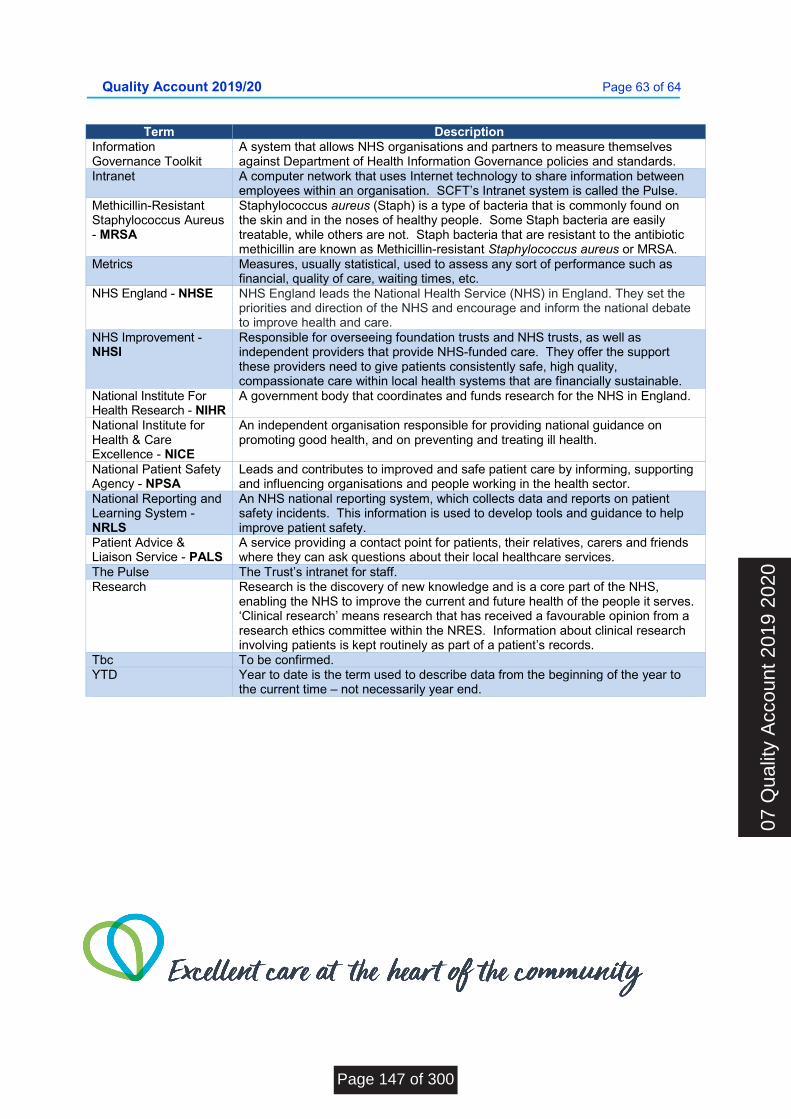
Quality Account 2019/20 Page 63 of 64
Term Description Information Governance Toolkit
A system that allows NHS organisations and partners to measure themselves against Department of Health Information Governance policies and standards.
Intranet A computer network that uses Internet technology to share information between employees within an organisation. SCFT’s Intranet system is called the Pulse.
Methicillin-Resistant Staphylococcus Aureus - MRSA
Staphylococcus aureus (Staph) is a type of bacteria that is commonly found on the skin and in the noses of healthy people. Some Staph bacteria are easily treatable, while others are not. Staph bacteria that are resistant to the antibiotic methicillin are known as Methicillin-resistant Staphylococcus aureus or MRSA.
Metrics Measures, usually statistical, used to assess any sort of performance such as financial, quality of care, waiting times, etc.
NHS England - NHSE NHS England leads the National Health Service (NHS) in England. They set the priorities and direction of the NHS and encourage and inform the national debate to improve health and care.
NHS Improvement - NHSI
Responsible for overseeing foundation trusts and NHS trusts, as well as independent providers that provide NHS-funded care. They offer the support these providers need to give patients consistently safe, high quality, compassionate care within local health systems that are financially sustainable.
National Institute For Health Research - NIHR
A government body that coordinates and funds research for the NHS in England.
National Institute for Health & Care Excellence - NICE
An independent organisation responsible for providing national guidance on promoting good health, and on preventing and treating ill health.
National Patient Safety Agency - NPSA
Leads and contributes to improved and safe patient care by informing, supporting and influencing organisations and people working in the health sector.
National Reporting and Learning System - NRLS
An NHS national reporting system, which collects data and reports on patient safety incidents. This information is used to develop tools and guidance to help improve patient safety.
Patient Advice & Liaison Service - PALS
A service providing a contact point for patients, their relatives, carers and friends where they can ask questions about their local healthcare services.
The Pulse The Trust’s intranet for staff. Research Research is the discovery of new knowledge and is a core part of the NHS,
enabling the NHS to improve the current and future health of the people it serves. ‘Clinical research’ means research that has received a favourable opinion from a research ethics committee within the NRES. Information about clinical research involving patients is kept routinely as part of a patient’s records.
Tbc To be confirmed. YTD
Year to date is the term used to describe data from the beginning of the year to the current time – not necessarily year end.
07 Q
ualit
y A
ccou
nt 2
019
2020
Page 147 of 300

Quality Account 2019/20 Page 64 of 64
Page 148 of 300
BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number: 8
Report Title: Serious Incident Report Q2 2020/21
Purpose: Approval Assurance X Discussion Briefing
Summary: This is a quarterly assurance report which has been reviewed by the Trust Wide Governance Group and provides an overview of SCFT Serious Incident management and patient safety processes. Quarter 2 has seen a slight increase in the declaration of serious incidents following the decrease that occurred during the initial months of the COVID-19 pandemic. The Trust has robust processes in place with good incident reporting rates and daily triage of all patient safety incidents. The report also provides some of the Community Indicators National Benchmarking Network data which resumed in August 2020. There is limited information available and this is provided in a new format, however, the data provided does not raise any areas of concern for SCFT. This is further evident through an analysis of the monthly and twice yearly data set published by the National Reporting and Learning System and the report provides an overview of this data analysis. This provides evidence that the Trust has a continuously improving safety awareness and culture and compares favourably with other similar NHS community Trusts. The report also includes a statement to confirm that there were no incidents reported to the Health & Safety Executive (HSE) under the Reporting of Injuries Diseases and Dangerous Occurrences Regulations (RIDDOR) or to the Care Quality Commission (CQC) under the Ionising Radiation (Medical Exposure) Regulations (IRMER).
Recommendation:
The Board is asked to note the contents of this report.
Previously reviewed by: Trust Wide Governance Group was assured by the report on the 3.11.2020
Relevance to Trust’s Strategic Goals: Population Health; Quality Improvement; Patient Experience; Thriving Staff;
Relevance to CQC Domains: Safe; Caring; Responsive; Effective; Well Led
Equality and Diversity: There are no equality and diversity implications from this report or content.
Report author: Debbie Johnson, Patient Safety Manager
Report owner: Sara Lightowlers, Medical Director
08 C
S S
erio
us In
cide
nts
Q2
Page 149 of 300

2020-2021 Q2 Report: Serious Incidents, Patient Safety and RIDDOR Deborah Johnson, Patient Safety Manager
Mark Plows, Safety and Risk Manager
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 150 of 300
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 2
Description 2020-2021 Q2 Report: Serious Incidents
Date published 23/10/2020
Executive Lead Medical Director
Author Deborah Johnson, Patient Safety Manager
Contact details [email protected]
Primary audience
Secondary audience(s)
Trust Wide Governance Group Trust Board
Notes
Table of Contents Introduction ...................................................................................................................... 3
1. Serious Incidents: National Benchmarking ................................................................ 3
2. Serious Incidents Quarter 2 2020/21 .............................................................................. 4 3. Serious Incident Themes from Quarter 2 2020/21. ...................................................................... 5 4. Patient Safety Incidents reported to the National Reporting and Learning System (NRLS) .......................................................................................................................................................................... 6
5. Quarter 2 Serious Incident Investigation Vignette .......................................................... 9
6. Incidents reported under RIDDOR ................................................................................ 10 7. Conclusion and Recommendations ...................................................................................................... 10
Page 151 of 300
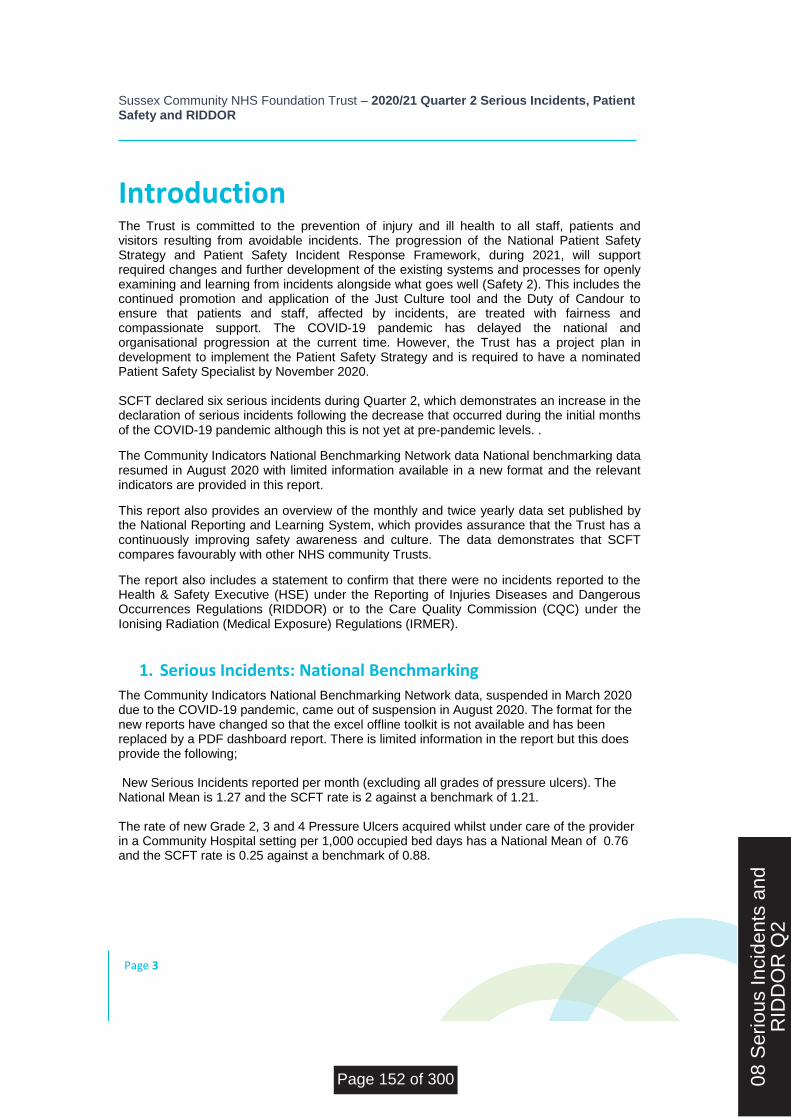
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 3
Introduction The Trust is committed to the prevention of injury and ill health to all staff, patients and visitors resulting from avoidable incidents. The progression of the National Patient Safety Strategy and Patient Safety Incident Response Framework, during 2021, will support required changes and further development of the existing systems and processes for openly examining and learning from incidents alongside what goes well (Safety 2). This includes the continued promotion and application of the Just Culture tool and the Duty of Candour to ensure that patients and staff, affected by incidents, are treated with fairness and compassionate support. The COVID-19 pandemic has delayed the national and organisational progression at the current time. However, the Trust has a project plan in development to implement the Patient Safety Strategy and is required to have a nominated Patient Safety Specialist by November 2020. SCFT declared six serious incidents during Quarter 2, which demonstrates an increase in the declaration of serious incidents following the decrease that occurred during the initial months of the COVID-19 pandemic although this is not yet at pre-pandemic levels. .
The Community Indicators National Benchmarking Network data National benchmarking data resumed in August 2020 with limited information available in a new format and the relevant indicators are provided in this report.
This report also provides an overview of the monthly and twice yearly data set published by the National Reporting and Learning System, which provides assurance that the Trust has a continuously improving safety awareness and culture. The data demonstrates that SCFT compares favourably with other NHS community Trusts.
The report also includes a statement to confirm that there were no incidents reported to the Health & Safety Executive (HSE) under the Reporting of Injuries Diseases and Dangerous Occurrences Regulations (RIDDOR) or to the Care Quality Commission (CQC) under the Ionising Radiation (Medical Exposure) Regulations (IRMER).
1. Serious Incidents: National Benchmarking
The Community Indicators National Benchmarking Network data, suspended in March 2020 due to the COVID-19 pandemic, came out of suspension in August 2020. The format for the new reports have changed so that the excel offline toolkit is not available and has been replaced by a PDF dashboard report. There is limited information in the report but this does provide the following; New Serious Incidents reported per month (excluding all grades of pressure ulcers). The National Mean is 1.27 and the SCFT rate is 2 against a benchmark of 1.21. The rate of new Grade 2, 3 and 4 Pressure Ulcers acquired whilst under care of the provider in a Community Hospital setting per 1,000 occupied bed days has a National Mean of 0.76 and the SCFT rate is 0.25 against a benchmark of 0.88.
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 152 of 300
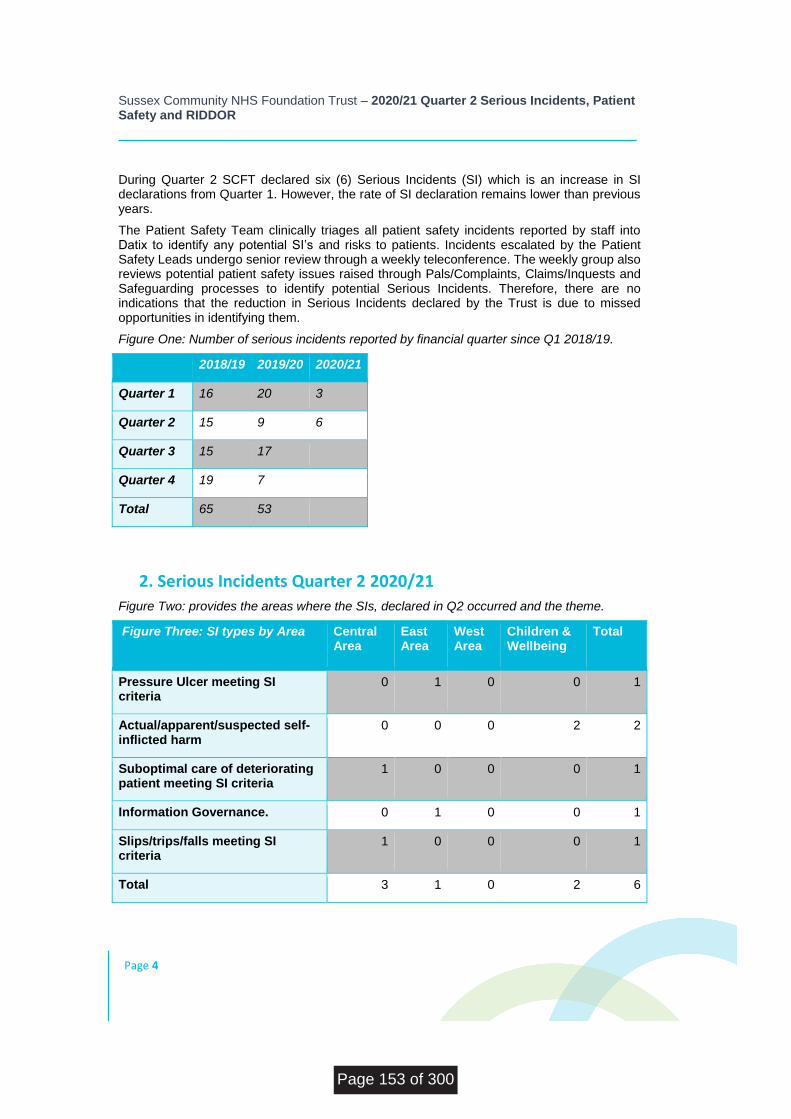
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 4
During Quarter 2 SCFT declared six (6) Serious Incidents (SI) which is an increase in SI declarations from Quarter 1. However, the rate of SI declaration remains lower than previous years.
The Patient Safety Team clinically triages all patient safety incidents reported by staff into Datix to identify any potential SI’s and risks to patients. Incidents escalated by the Patient Safety Leads undergo senior review through a weekly teleconference. The weekly group also reviews potential patient safety issues raised through Pals/Complaints, Claims/Inquests and Safeguarding processes to identify potential Serious Incidents. Therefore, there are no indications that the reduction in Serious Incidents declared by the Trust is due to missed opportunities in identifying them.
Figure One: Number of serious incidents reported by financial quarter since Q1 2018/19.
2018/19 2019/20 2020/21
Quarter 1 16 20 3
Quarter 2 15 9 6
Quarter 3 15 17
Quarter 4 19 7
Total 65 53
2. Serious Incidents Quarter 2 2020/21
Figure Two: provides the areas where the SIs, declared in Q2 occurred and the theme.
Figure Three: SI types by Area
Central Area
East Area
West Area
Children & Wellbeing
Total
Pressure Ulcer meeting SI criteria
0 1 0 0 1
Actual/apparent/suspected self-inflicted harm
0 0 0 2 2
Suboptimal care of deteriorating patient meeting SI criteria
1 0 0 0 1
Information Governance. 0 1 0 0 1
Slips/trips/falls meeting SI criteria
1 0 0 0 1
Total 3 1 0 2 6
Page 153 of 300
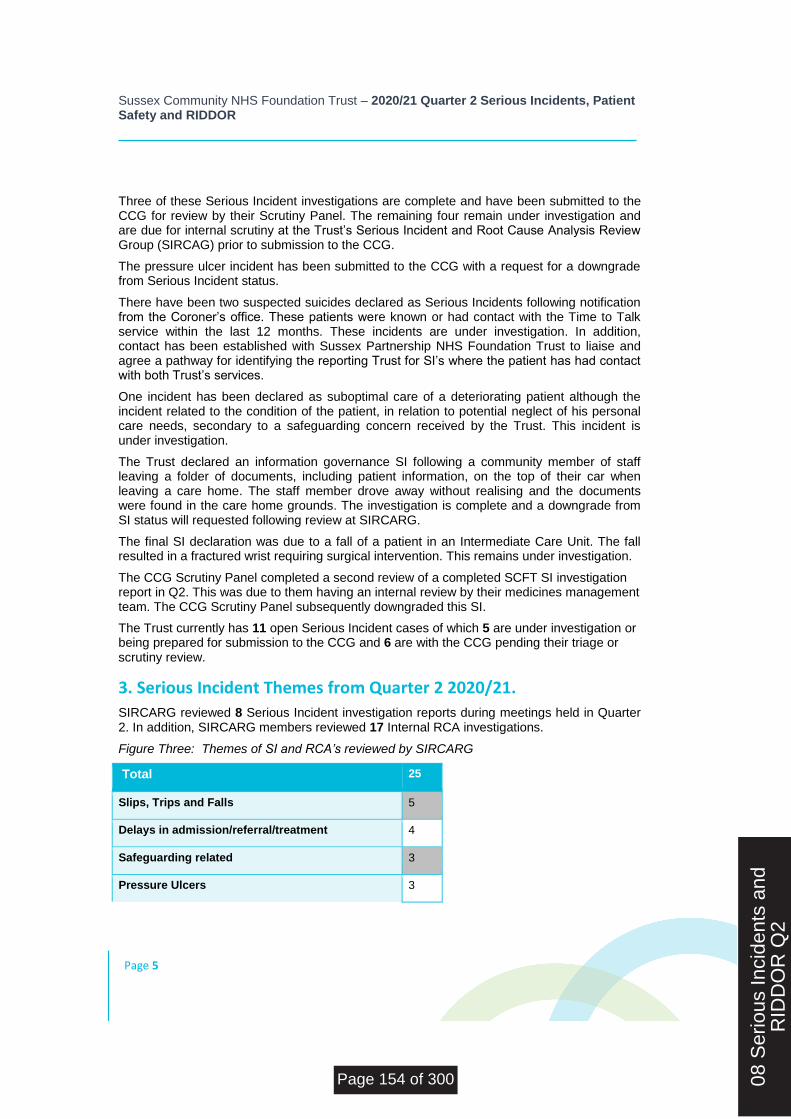
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 5
Three of these Serious Incident investigations are complete and have been submitted to the CCG for review by their Scrutiny Panel. The remaining four remain under investigation and are due for internal scrutiny at the Trust’s Serious Incident and Root Cause Analysis Review Group (SIRCAG) prior to submission to the CCG.
The pressure ulcer incident has been submitted to the CCG with a request for a downgrade from Serious Incident status.
There have been two suspected suicides declared as Serious Incidents following notification from the Coroner’s office. These patients were known or had contact with the Time to Talk service within the last 12 months. These incidents are under investigation. In addition, contact has been established with Sussex Partnership NHS Foundation Trust to liaise and agree a pathway for identifying the reporting Trust for SI’s where the patient has had contact with both Trust’s services.
One incident has been declared as suboptimal care of a deteriorating patient although the incident related to the condition of the patient, in relation to potential neglect of his personal care needs, secondary to a safeguarding concern received by the Trust. This incident is under investigation.
The Trust declared an information governance SI following a community member of staff leaving a folder of documents, including patient information, on the top of their car when leaving a care home. The staff member drove away without realising and the documents were found in the care home grounds. The investigation is complete and a downgrade from SI status will requested following review at SIRCARG.
The final SI declaration was due to a fall of a patient in an Intermediate Care Unit. The fall resulted in a fractured wrist requiring surgical intervention. This remains under investigation.
The CCG Scrutiny Panel completed a second review of a completed SCFT SI investigation report in Q2. This was due to them having an internal review by their medicines management team. The CCG Scrutiny Panel subsequently downgraded this SI.
The Trust currently has 11 open Serious Incident cases of which 5 are under investigation or being prepared for submission to the CCG and 6 are with the CCG pending their triage or scrutiny review.
3. Serious Incident Themes from Quarter 2 2020/21.
SIRCARG reviewed 8 Serious Incident investigation reports during meetings held in Quarter 2. In addition, SIRCARG members reviewed 17 Internal RCA investigations.
Figure Three: Themes of SI and RCA’s reviewed by SIRCARG
Total 25
Slips, Trips and Falls 5
Delays in admission/referral/treatment 4
Safeguarding related 3
Pressure Ulcers 3
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 154 of 300
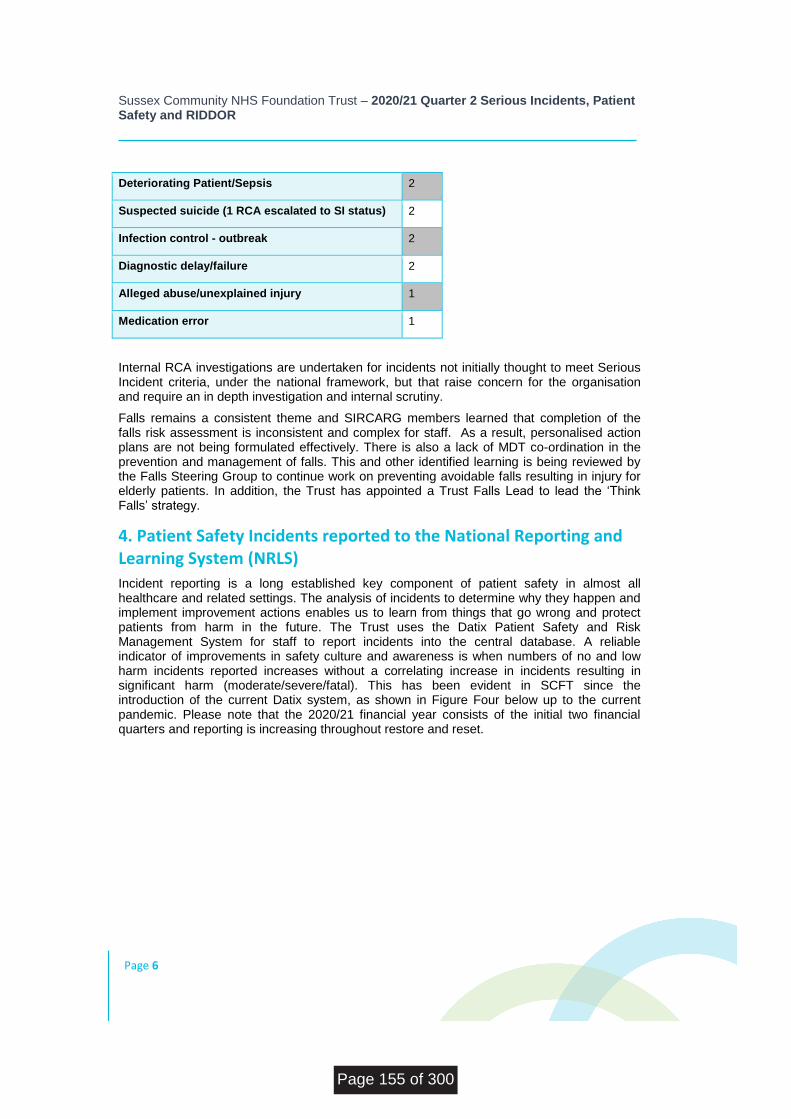
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 6
Deteriorating Patient/Sepsis 2
Suspected suicide (1 RCA escalated to SI status) 2
Infection control - outbreak 2
Diagnostic delay/failure 2
Alleged abuse/unexplained injury 1
Medication error 1
Internal RCA investigations are undertaken for incidents not initially thought to meet Serious Incident criteria, under the national framework, but that raise concern for the organisation and require an in depth investigation and internal scrutiny.
Falls remains a consistent theme and SIRCARG members learned that completion of the falls risk assessment is inconsistent and complex for staff. As a result, personalised action plans are not being formulated effectively. There is also a lack of MDT co-ordination in the prevention and management of falls. This and other identified learning is being reviewed by the Falls Steering Group to continue work on preventing avoidable falls resulting in injury for elderly patients. In addition, the Trust has appointed a Trust Falls Lead to lead the ‘Think Falls’ strategy.
4. Patient Safety Incidents reported to the National Reporting and Learning System (NRLS)
Incident reporting is a long established key component of patient safety in almost all healthcare and related settings. The analysis of incidents to determine why they happen and implement improvement actions enables us to learn from things that go wrong and protect patients from harm in the future. The Trust uses the Datix Patient Safety and Risk Management System for staff to report incidents into the central database. A reliable indicator of improvements in safety culture and awareness is when numbers of no and low harm incidents reported increases without a correlating increase in incidents resulting in significant harm (moderate/severe/fatal). This has been evident in SCFT since the introduction of the current Datix system, as shown in Figure Four below up to the current pandemic. Please note that the 2020/21 financial year consists of the initial two financial quarters and reporting is increasing throughout restore and reset.
Page 155 of 300
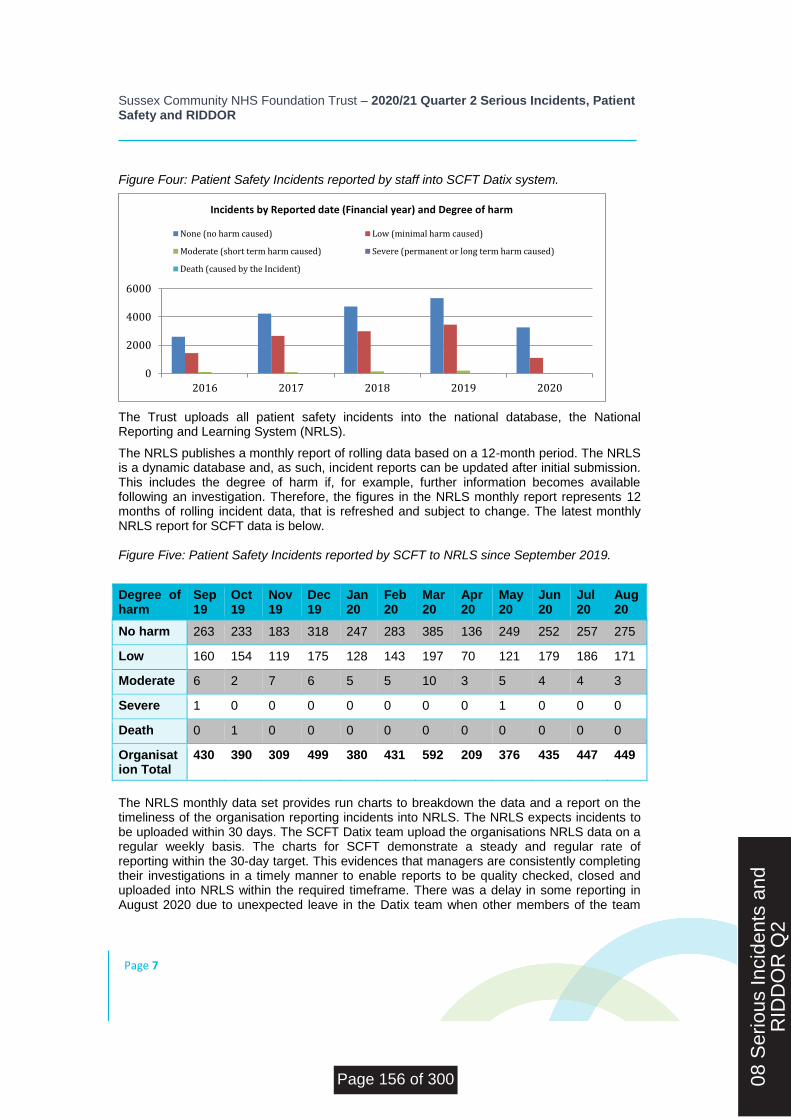
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 7
Figure Four: Patient Safety Incidents reported by staff into SCFT Datix system.
The Trust uploads all patient safety incidents into the national database, the National Reporting and Learning System (NRLS).
The NRLS publishes a monthly report of rolling data based on a 12-month period. The NRLS is a dynamic database and, as such, incident reports can be updated after initial submission. This includes the degree of harm if, for example, further information becomes available following an investigation. Therefore, the figures in the NRLS monthly report represents 12 months of rolling incident data, that is refreshed and subject to change. The latest monthly NRLS report for SCFT data is below. Figure Five: Patient Safety Incidents reported by SCFT to NRLS since September 2019.
Degree of harm
Sep19
Oct19
Nov19
Dec19
Jan20
Feb 20
Mar20
Apr20
May20
Jun20
Jul20
Aug20
No harm 263 233 183 318 247 283 385 136 249 252 257 275
Low 160 154 119 175 128 143 197 70 121 179 186 171
Moderate 6 2 7 6 5 5 10 3 5 4 4 3
Severe 1 0 0 0 0 0 0 0 1 0 0 0
Death 0 1 0 0 0 0 0 0 0 0 0 0
Organisation Total
430 390 309 499 380 431 592 209 376 435 447 449
The NRLS monthly data set provides run charts to breakdown the data and a report on the timeliness of the organisation reporting incidents into NRLS. The NRLS expects incidents to be uploaded within 30 days. The SCFT Datix team upload the organisations NRLS data on a regular weekly basis. The charts for SCFT demonstrate a steady and regular rate of reporting within the 30-day target. This evidences that managers are consistently completing their investigations in a timely manner to enable reports to be quality checked, closed and uploaded into NRLS within the required timeframe. There was a delay in some reporting in August 2020 due to unexpected leave in the Datix team when other members of the team
0
2000
4000
6000
2016 2017 2018 2019 2020
Incidents by Reported date (Financial year) and Degree of harm
None (no harm caused) Low (minimal harm caused)
Moderate (short term harm caused) Severe (permanent or long term harm caused)
Death (caused by the Incident)
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 156 of 300
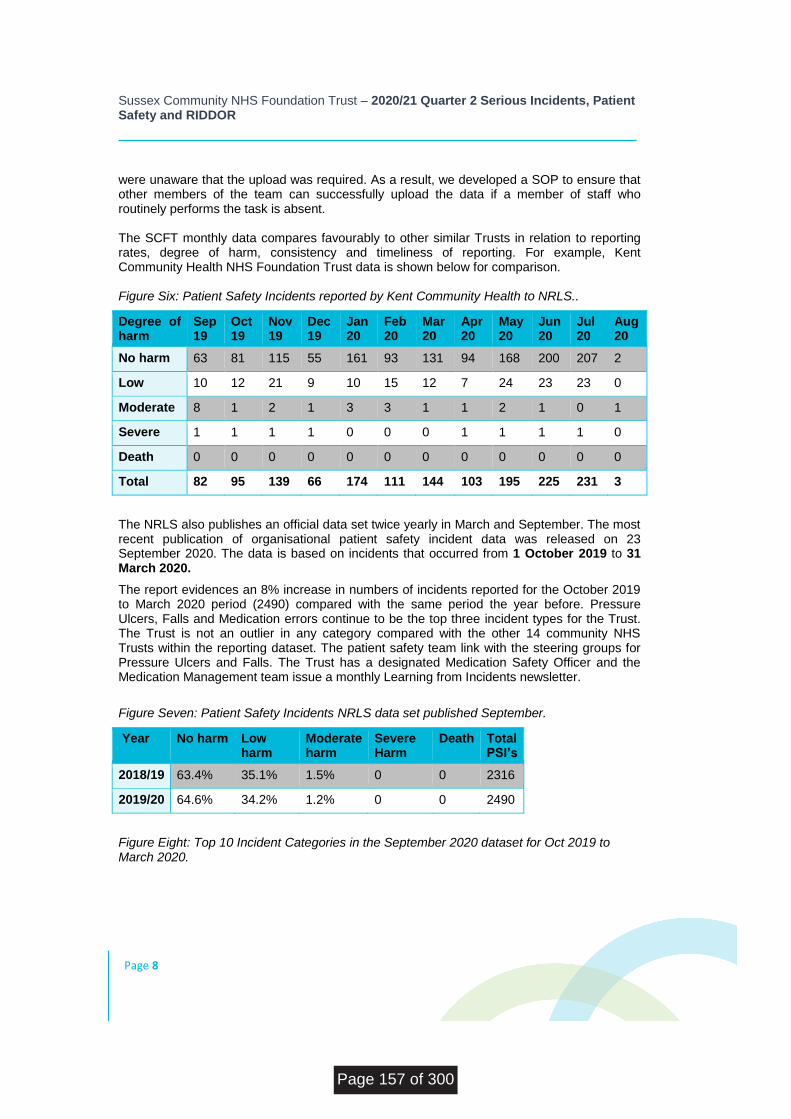
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 8
were unaware that the upload was required. As a result, we developed a SOP to ensure that other members of the team can successfully upload the data if a member of staff who routinely performs the task is absent. The SCFT monthly data compares favourably to other similar Trusts in relation to reporting rates, degree of harm, consistency and timeliness of reporting. For example, Kent Community Health NHS Foundation Trust data is shown below for comparison. Figure Six: Patient Safety Incidents reported by Kent Community Health to NRLS..
Degree of harm
Sep19
Oct19
Nov19
Dec19
Jan20
Feb20
Mar20
Apr20
May20
Jun20
Jul20
Aug20
No harm 63 81 115 55 161 93 131 94 168 200 207 2
Low 10 12 21 9 10 15 12 7 24 23 23 0
Moderate 8 1 2 1 3 3 1 1 2 1 0 1
Severe 1 1 1 1 0 0 0 1 1 1 1 0
Death 0 0 0 0 0 0 0 0 0 0 0 0
Total 82 95 139 66 174 111 144 103 195 225 231 3
The NRLS also publishes an official data set twice yearly in March and September. The most recent publication of organisational patient safety incident data was released on 23 September 2020. The data is based on incidents that occurred from 1 October 2019 to 31 March 2020.
The report evidences an 8% increase in numbers of incidents reported for the October 2019 to March 2020 period (2490) compared with the same period the year before. Pressure Ulcers, Falls and Medication errors continue to be the top three incident types for the Trust. The Trust is not an outlier in any category compared with the other 14 community NHS Trusts within the reporting dataset. The patient safety team link with the steering groups for Pressure Ulcers and Falls. The Trust has a designated Medication Safety Officer and the Medication Management team issue a monthly Learning from Incidents newsletter.
Figure Seven: Patient Safety Incidents NRLS data set published September.
Year No harm Low harm
Moderate harm
Severe Harm
Death Total PSI’s
2018/19 63.4% 35.1% 1.5% 0 0 2316
2019/20 64.6% 34.2% 1.2% 0 0 2490
Figure Eight: Top 10 Incident Categories in the September 2020 dataset for Oct 2019 to March 2020.
Page 157 of 300
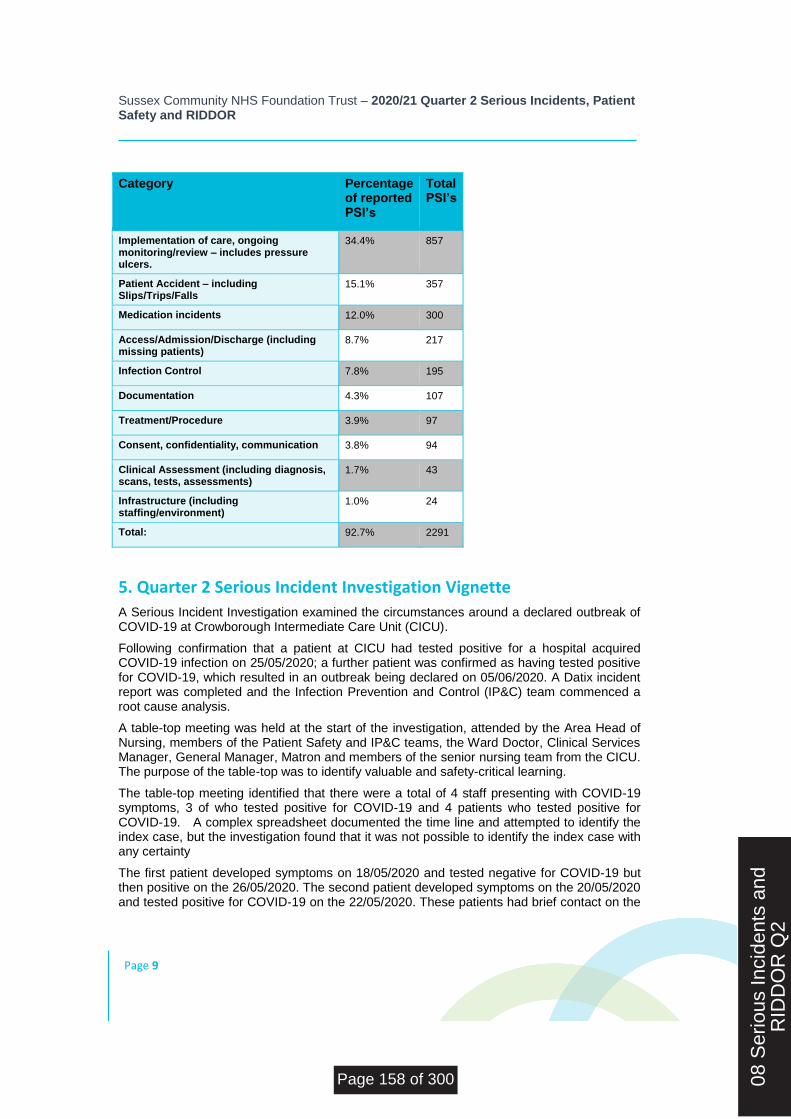
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 9
Category Percentage of reported PSI’s
Total PSI’s
Implementation of care, ongoing monitoring/review – includes pressure ulcers.
34.4% 857
Patient Accident – including Slips/Trips/Falls
15.1% 357
Medication incidents 12.0% 300
Access/Admission/Discharge (including missing patients)
8.7% 217
Infection Control 7.8% 195
Documentation 4.3% 107
Treatment/Procedure 3.9% 97
Consent, confidentiality, communication 3.8% 94
Clinical Assessment (including diagnosis, scans, tests, assessments)
1.7% 43
Infrastructure (including staffing/environment)
1.0% 24
Total: 92.7% 2291
5. Quarter 2 Serious Incident Investigation Vignette
A Serious Incident Investigation examined the circumstances around a declared outbreak of COVID-19 at Crowborough Intermediate Care Unit (CICU).
Following confirmation that a patient at CICU had tested positive for a hospital acquired COVID-19 infection on 25/05/2020; a further patient was confirmed as having tested positive for COVID-19, which resulted in an outbreak being declared on 05/06/2020. A Datix incident report was completed and the Infection Prevention and Control (IP&C) team commenced a root cause analysis.
A table-top meeting was held at the start of the investigation, attended by the Area Head of Nursing, members of the Patient Safety and IP&C teams, the Ward Doctor, Clinical Services Manager, General Manager, Matron and members of the senior nursing team from the CICU. The purpose of the table-top was to identify valuable and safety-critical learning.
The table-top meeting identified that there were a total of 4 staff presenting with COVID-19 symptoms, 3 of who tested positive for COVID-19 and 4 patients who tested positive for COVID-19. A complex spreadsheet documented the time line and attempted to identify the index case, but the investigation found that it was not possible to identify the index case with any certainty
The first patient developed symptoms on 18/05/2020 and tested negative for COVID-19 but then positive on the 26/05/2020. The second patient developed symptoms on the 20/05/2020 and tested positive for COVID-19 on the 22/05/2020. These patients had brief contact on the
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 158 of 300

Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 10
17/05/2020. It was established that a member of staff who was moved from another ICU to work at CICU between 16/05/2020 and 18/05/2020, became unwell on 23/05/2020 and tested positive for COVID-19.
The incubation period for COVID-19 is considered to be 1-14 days before the symptoms to become apparent and some people do not display symptoms. Therefore, both patients could have been incubating the virus prior to their transfer to CICU and the staff member could have been incubating symptoms from contact with COVID-19 positive patients at the other ICU prior to being relocated to work at CICU.
This investigation found that the staff at the CICU acted promptly and efficiently to ensure that patients who were displaying symptoms were immediately isolated and swabbed. CICU staff followed IP&C guidelines and outbreak measures whilst delivering care to patients in a global pandemic.
Guidelines on the wearing of PPE were shared with SCFT staff as soon as Public Health England (PHE) updated these. The investigation found that the staff were not wearing PPE at the nurse’s station. The nurse’s station is classed as a clinical area, however the staff at the CICU had classed this area as a clerical area, but had not taken into consideration that at the time they were providing enhanced care to a patient who was sitting at the nurse’s station and therefore they should have been wearing PPE. It has now been confirmed with all staff that all areas within the ICU’s are classified as clinical areas.
Learning was identified around risk assessing staff moving between units and the movement of patients around an ICU. Whilst bed moves can be necessary they do generate more movement of furniture and patient belongings, increasing the chance of spreading the virus. Bed moves are to be risk assessed and documented to ensure they are also easier to time line.
A screening assessment tool was introduced at the start of the pandemic for all admissions into SCFT ICU’s to ask about risk of exposure to COVID-19, to fully inform mapping of patient admissions to the ICU. The referring acute Trusts were not providing Information on whether patients were transferring from a negative or positive COVID-19 on the ICU’s referral document. As a result, the ICU updated this document to ensure this information is captured prior to admission.
6. Incidents reported under RIDDOR
During Quarter 2 there have been no incidents meeting the RIDDOR requirement to report significant health and safety incidents to the HSE. Whenever notifiable incidents are identified, the Health and Safety team reviews the incident, notifies the applicable Executive Directors, and reports the incident to the HSE. The Health and Safety Committee reviews the notifiable incidents in further detail and provides assurance to the Executive Committee. The Health and Safety Committee, via the Radiation Protection (sub) Group, provides assurance of incidents reported under IRMER to the CQC. There have been no IRMER reportable incidents in Quarter 2.
7. Conclusion and Recommendations
This report provides assurance that the organisation has robust safety systems and processes in place. The Trust continues to promote an effective safety culture that strives to
Page 159 of 300
Sussex Community NHS Foundation Trust – 2020/21 Quarter 2 Serious Incidents, Patient Safety and RIDDOR
Page 11
report all patient safety incidents in a transparent manner. The Patient Safety Team closely monitored the reduction in incident reporting during the COVID-19 outbreak and it is noted that incident reporting increased during reset and restoration and continues to be monitored.
The team awaits further updates from the national patient safety team with regards to progressing the National Patient Safety Agenda.
08 S
erio
us In
cide
nts
and
RID
DO
R Q
2
Page 160 of 300

BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number: 9
Report Title: Mortality Report Q2
Purpose:
Approval Assurance x Discussion Briefing
Summary: Sussex Community NHS Foundation Trust has been using structured judgmental forms to review the period before a patient has died. Reviewing deaths in this way would enable us to identify any trends that would indicate that a particular service has higher deaths than average which would lead to a more in-depth review of the care provided within that service. In Quarter 2 there were 13 deaths across our intermediate care units. The analysis of deaths is detailed in the report. The numbers of deaths are low but this is in keeping with national trend. From the review there are no avoidable deaths. All deaths are explainable and there is no evidence of suboptimal care or different care provision that would have made a difference.
Recommendation:
Members are asked to note the content of report
Previously reviewed by: Mortality Review Group held on 6/10/2020 Trust Wide Governance Group on 3/11/2020
Relevance to Trust’s Strategic Goals: Population Health; Quality Improvement; Patient Experience; Thriving Staff; Value and Sustainability
Relevance to CQC Domains: Safe; Caring; Responsive; Effective; Well Led
Equality and Diversity: Not applicable
Report author: Dr Vivek Patil, Deputy Medical Director
Report owner: Dr Sara Lightowlers, Medical Director.
09 C
S M
orta
lity
Rep
ort Q
2
Page 161 of 300

Mortality Review Report Q2 2020 Dr Vivek Patil Deputy Medical Director
09 M
orta
lity
Rep
ort
Q2
Page 162 of 300
Sussex Community NHS Foundation Trust – Name of report title
Page 2
Reader Box
Description This is the summary of all the structured judgmental review of deaths in our intermediate care units. Any learning from how we cared for the patient pre and post death is shared across trust through mortality review meetings.
Date published 28/10/2020
Date due for review None
Executive Lead Dr Sara Lightowlers Medical Director
Author Dr Vivek Patil Deputy Medical Director
Contact details [email protected]
Primary audience Mortality Review Group & Trust Wide Governance Group.
Secondary audience(s)
Executive Team, Trust Board, Quality Committee and others.
Notes This is the summary of mortality reviews done in our intermediate care units using structured judgmental forms. The aim is to identify if the trust could have improved the quality of care leading up to the death, identify any trends that would indicate that poor care had led to the death and to identify if there are any particular services where mortality is higher than expected and to take the necessary actions as need be.
Table of Contents 1 Introduction ………………………………………….3 2 Results of Q 2 and analysis………………………….Error! Bookmark not defined. 3 Lessons learnt………………………………………………5
Page 163 of 300
Sussex Community NHS Foundation Trust – Name of report title
Page 3
1. Introduction Sussex Community NHS Foundation Trust (SCFT) has been using structured judgmental forms to review the period before a patient has died. This has been in practice since 2014. Reviewing deaths in this way has led to identify any trends that would indicate that a particular service has higher deaths than average which would lead to a more in-depth review of the care provided within that service. We have also introduced a buddy system where by neighboring inpatient units undertake the review for one another. This is in line with recommendation by NHSI
2. Results for Q2 and analysis.
2.1 Overall deaths during reporting period.
From 1st July to 30th Sept 2020 there were 13 reported deaths in our intermediate care units. All deaths have been reviewed using the structured judgmental review (SJR) forms. We aim to undertake the review of all deaths in intermediate care units in a defined time line. This is not always possible due to a combination of heightened case load activity and the availability of senior staff to undertake the review. The breakdown of number of deaths in each area and units are as follows. East Area 7 deaths - Uckfield intermediate care unit - 3 Lewes intermediate care unit - 2 Crowborough intermediate care unit - 1 Kleinwort intermediate care unit- 1 Central Area 4 deaths – Crawley intermediate care units – 3 Horizon intermediate care unit -1 West Area 2 deaths – Bognor intermediate care unit -1 Zackery Merton unit – 1 It is to be noted that the overall number of deaths reported across UK is lower during Q2 and this is explained by the excess number of deaths seen in Q1 due to the COVID- 19 pandemic.
2.2 Deaths that have been reviewed using SJR process.
Age range is from 78 to 96 with mean age range of 87.5 for all the deaths reviewed using structured judgmental forms (SJR) forms.
SJR forms were completed by ward doctors, advanced nurse practitioners and ward sisters.
All admissions were before 20:00. The time of admission did not have any relation to outcome of death.
Length of stay varied from 2 days to 40 days.
Main causes of death were pneumonia, cardiovascular disease, advanced dementia and cancer.
From the review of cases it is noted that 3 had malignancy and 1 had distal metastases.
09 M
orta
lity
Rep
ort
Q2
Page 164 of 300

Sussex Community NHS Foundation Trust – Name of report title
Page 4
Increasing comorbidity is seen in the form of cardiovascular, respiratory and metabolic (diabetes) pathology.
2.3 Involvement of Coroner
There were no hospital post mortems but the Coroner was consulted in 2 of the deaths. This demonstrates that clinicians are actively reporting to Coroner and seeking advice in cases where diagnosis may not be clear.
2.4 Medical oversight of patients who have died.
First clinical review of patients took place within an hour to one working day in line with the standard operating procedure for our intermediate care units.
It has been recorded that in all reviews there was evidence of clear management plans within one working day and there were no omissions in the initial management plans.
2.5 Transfer between wards and hospitals.
All patients were admitted to the appropriate ward in the first instance. There were no patient transfers between our intermediate care units themselves. There were no patient transfer to the acute trusts for terminally ill patients.
2.6 Medical staff reviews.
It has been documented that patients were seen on regular basis in accordance with the standard operating procedure and documentation was noted to be of good medical standards. It is worth noting that some of our units are Nurse led units and if there is a sudden change in patients clinical condition, doctor input is sought accordingly.
2.7 Care preceding death.
There were no documented falls in any patients who died.
None of the patients who died developed pressure ulcers in our care
Fluid balance has been documented as adequate in all cases. Nutrition assessment was addressed appropriately for those nearing end of life and dietician input was requested in two cases.
National Early Warning Score (NEWS) was recorded as appropriate in all cases and in majority of cases this was discontinued as patients approached end of life.
None of the patients had raised troponin (indicating a heart attack), abrupt drop in haemoglobin ( indicating blood loss ), hypoglycaemia ( low blood sugar level) or raised international normalized ratio (INR) ( indicating a likelihood of bleeding).
4 patients had urinary catheter in situ and reviews suggest that these were inserted for appropriate clinical reasons i.e. acute urinary retention and end of life care. It is to be noted that none of them developed any post insertion infection. This demonstrates good catheter care provided in our units.
Page 165 of 300
Sussex Community NHS Foundation Trust – Name of report title
Page 5
Reviews of structured judgmental review (SJR) forms suggest that 3 people had respiratory tract infection. They were all treated appropriately where needed with oral or intravenous antibiotics.
There is no documentation of never events in patients who have died under our care. In one case patient was noted to have Acute Kidney Injury secondary to cardiorenal syndrome. This patient did have a clear management in place with appropriate input from secondary care physician.
In all cases a decision to limit the treatment was made. Resuscitation status was documented in all cases apart from two. All patients were seen before the death by a clinician.
The Palliative care team was involved in two cases. From the review it is felt that patients received optimal care in the patient’s preferred place. All patients’ relatives and carers were involved in discussion about preferred place of death using technology.
In overall review it is felt that there was no delay in making a diagnosis and there was good communication between teams. There was no delay in delivering care and no recorded suboptimal care provision. It is felt from the review that a different care would have made no difference to the outcome of patients. All deaths were explainable. From the review it is felt that there were no avoidable deaths. There was no evidence of poor communication, organisational failure or delivery of suboptimal care provided.
2.8 Evidence of Good Standard of Care
Highlights of good care were communication between teams, documentation, keeping families and carers involved using technology and the care given by the staff themselves.
The standard of documentation is noted to be excellent in 4, good in 6 and average in rest.
3. Learnings Two unexpected deaths were also discussed in the meeting. After initial investigation by the Area Nurses it was noted that these were reported to Coroner and cause of death was discussed in detail. It was agreed that these two deaths were not avoidable and were explainable. It was noted both patients should have had, review of their resuscitation status. It was highlighted and noted that it is important to have these discussion at the initial admission process if not already done by Acute Trusts. Discussion was also centered on management of COVID 19 patients at their terminal stage. The latest guidelines were discussed in the meeting too and a slide deck containing the information has been shared with all doctors and ANP’s. It is to be noted that the Coroner for East Sussex Area has praised the care given by the staff at end of life care. This was in relation to one of the patient who has had an unexpected death.
09 M
orta
lity
Rep
ort
Q2
Page 166 of 300


BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number: 10
Report Title: Emergency Preparedness, Resilience and Response (EPRR) Annual Report
Purpose:
Approval Assurance X Discussion Briefing
Summary: This report provides an account of Sussex Community NHS Foundation Trust’s emergency preparedness and response activities undertaken throughout 2019/20. It details the emergency planning processes followed by the Trust to ensure the effective and timely response to the Coronavirus pandemic (COVID-19). The document also outlines the planning process followed by the Trust to ensure the successful management of concurrent major, critical or business continuity incidents. This report provides assurance to the Board of the Trust’s continued effective resilience programme and recommends the programme of EPPR work priorities for 2020/21.
Recommendation:
The Board is asked to note the content of the report and agree the associated work priorities to maintain full compliance against the EPRR Core Standards over the next 12 months.
Previously reviewed by: Executive Committee
Relevance to Trust’s Strategic Goals: Quality Improvement; Value and Sustainability
Relevance to CQC Domains: Safe; Well Led
Equality and Diversity: Not applicable
Report author: Rebecca Allsopp, Emergency Planning Lead Hannah Shorten, Emergency Planning Officer
Report owner: Kate Pilcher, Chief Operating Officer
10 C
S E
PR
R A
nnua
l Rep
ort
2020
Page 167 of 300

Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 1
Emergency Preparedness,
Resilience and Response
(EPRR) Annual Report
2020
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 168 of 300
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 2
Contents Introduction ............................................................................................................................ 3
Background .......................................................................................................................... 3
Governance Arrangements ................................................................................................... 3
Overview and Summary of EPRR Activity ............................................................................ 4
EPRR Risk ............................................................................................................................ 4
NHS England EPRR Annual Assurance Process .................................................................. 6
Business Continuity Management ......................................................................................... 6
Training and Exercising ........................................................................................................ 7
Live Incidents ........................................................................................................................ 9
Plans .................................................................................................................................. 10
EU Exit End of Transition Period Preparations .................................................................... 10
Management of concurrent incidents .................................................................................. 11
Conclusion ............................................................................................................................ 12
Page 169 of 300
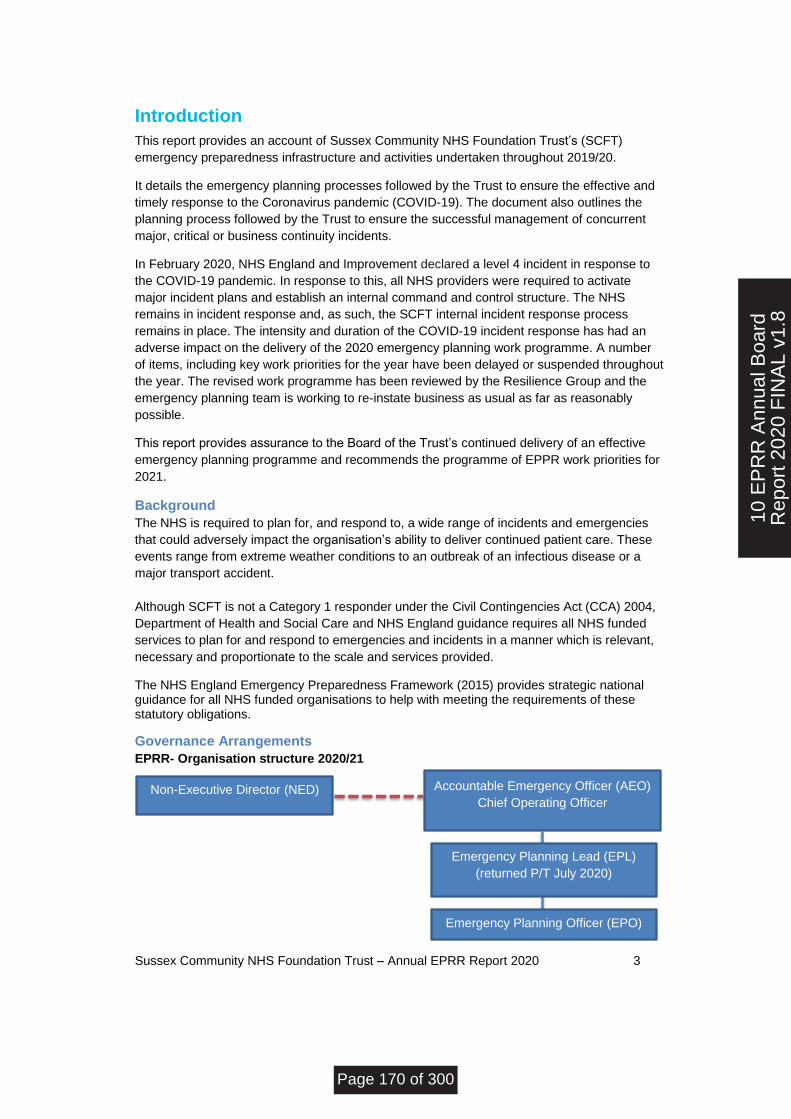
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 3
Introduction
This report provides an account of Sussex Community NHS Foundation Trust’s (SCFT)
emergency preparedness infrastructure and activities undertaken throughout 2019/20.
It details the emergency planning processes followed by the Trust to ensure the effective and
timely response to the Coronavirus pandemic (COVID-19). The document also outlines the
planning process followed by the Trust to ensure the successful management of concurrent
major, critical or business continuity incidents.
In February 2020, NHS England and Improvement declared a level 4 incident in response to
the COVID-19 pandemic. In response to this, all NHS providers were required to activate
major incident plans and establish an internal command and control structure. The NHS
remains in incident response and, as such, the SCFT internal incident response process
remains in place. The intensity and duration of the COVID-19 incident response has had an
adverse impact on the delivery of the 2020 emergency planning work programme. A number
of items, including key work priorities for the year have been delayed or suspended throughout
the year. The revised work programme has been reviewed by the Resilience Group and the
emergency planning team is working to re-instate business as usual as far as reasonably
possible.
This report provides assurance to the Board of the Trust’s continued delivery of an effective
emergency planning programme and recommends the programme of EPPR work priorities for
2021.
Background
The NHS is required to plan for, and respond to, a wide range of incidents and emergencies
that could adversely impact the organisation’s ability to deliver continued patient care. These
events range from extreme weather conditions to an outbreak of an infectious disease or a
major transport accident.
Although SCFT is not a Category 1 responder under the Civil Contingencies Act (CCA) 2004,
Department of Health and Social Care and NHS England guidance requires all NHS funded
services to plan for and respond to emergencies and incidents in a manner which is relevant,
necessary and proportionate to the scale and services provided.
The NHS England Emergency Preparedness Framework (2015) provides strategic national guidance for all NHS funded organisations to help with meeting the requirements of these statutory obligations.
Governance Arrangements
EPRR- Organisation structure 2020/21
Non-Executive Director (NED) Accountable Emergency Officer (AEO)
Chief Operating Officer
Emergency Planning Officer (EPO)
Emergency Planning Lead (EPL)
(returned P/T July 2020)
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 170 of 300
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 4
NHS England requires all NHS funded organisations to have an Accountable Emergency
Officer (AEO) for EPRR. The AEO for the Trust is the Chief Operating Officer, supported by an
Emergency Planning Lead and Emergency Planning Officer to ensure Trust obligations under
the EPRR core standards are met. There is also an appointed Non-Executive Director.
The Trust Resilience Group is responsible for overseeing the Trust’s emergency planning programme of work. The Resilience Group meets quarterly and has a role in the triangulation of outputs from key governance work streams which help to proactively identify potential gaps in the Trust’s resilience plans and structures. The outcomes of the Resilience Group are summarised and presented to the Executive Committee quarterly, with the assurance position reported to Trust Board annually. The Trust EPRR work is linked into national structures through the Local Health Resilience
Partnership (LHRP), which provides a strategic forum for joint EPRR planning across a
geographic area and supports the health sector’s contribution to multi agency planning. The
Trust’s Accountable Emergency Officer and Emergency Planning Lead/Officer attend the
Sussex LHRP Executive Group, and the Sussex Health Responder Group (SHRG)
respectively.
Overview and Summary of EPRR Activity
This report outlines EPRR activity over the past year from November 2019- 2020.
EPRR Risk
There are currently five EPRR risks on the Trust risk register. Throughout the year, six risks
have been closed, three of which are currently sitting on the accepted risk register (see
below).
EPRR risks for the period November 2019-2020
The majority of EPRR risks score between 6 –12. Due to the nature of the risk area, the
impacts of specific risks are often scored at a major (4) or catastrophic (5). The emergency
planning team take actions to ensure that robust mitigating plans are in place; however, there
are some risks that can never be entirely mitigated and are, therefore, accepted by the
organisation. The following risks have been accepted at their current score over the past year:
362-There is a risk that services will be unable to continue critical services following a
significant fire / flood or other incident at multi occupancy sites
552- Adverse weather affecting the Trust's ability to provide critical services.
146-Lack of back-up generator at Kleinwort
This brings the total of accepted risks on the EPRR register to seven. These risks will continue
to be monitored annually, and in line with national or regional direction.
Page 171 of 300
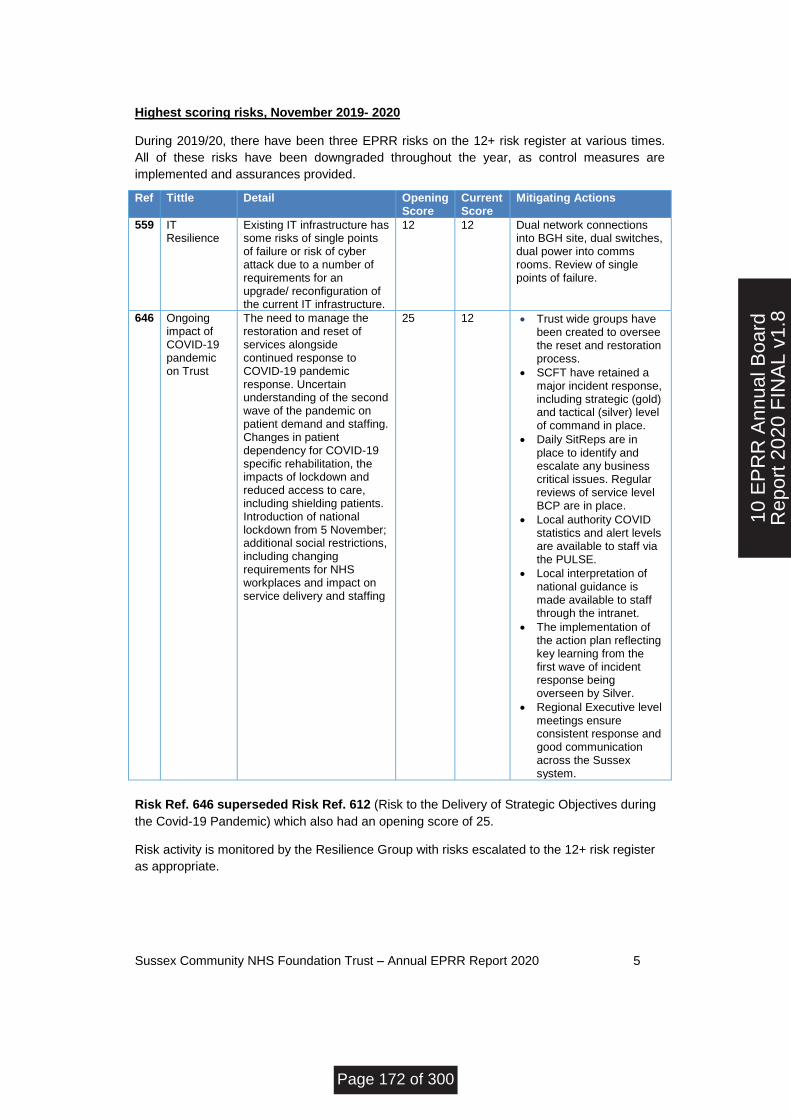
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 5
Highest scoring risks, November 2019- 2020
During 2019/20, there have been three EPRR risks on the 12+ risk register at various times.
All of these risks have been downgraded throughout the year, as control measures are
implemented and assurances provided.
Ref Tittle Detail Opening Score
Current Score
Mitigating Actions
559 IT Resilience
Existing IT infrastructure has some risks of single points of failure or risk of cyber attack due to a number of requirements for an upgrade/ reconfiguration of the current IT infrastructure.
12 12 Dual network connections into BGH site, dual switches, dual power into comms rooms. Review of single points of failure.
646
Ongoing impact of COVID-19 pandemic on Trust
The need to manage the restoration and reset of services alongside continued response to COVID-19 pandemic response. Uncertain understanding of the second wave of the pandemic on patient demand and staffing. Changes in patient dependency for COVID-19 specific rehabilitation, the impacts of lockdown and reduced access to care, including shielding patients. Introduction of national lockdown from 5 November; additional social restrictions, including changing requirements for NHS workplaces and impact on service delivery and staffing
25
12
Trust wide groups have been created to oversee the reset and restoration process.
SCFT have retained a major incident response, including strategic (gold) and tactical (silver) level of command in place.
Daily SitReps are in place to identify and escalate any business critical issues. Regular reviews of service level BCP are in place.
Local authority COVID statistics and alert levels are available to staff via the PULSE.
Local interpretation of national guidance is made available to staff through the intranet.
The implementation of the action plan reflecting key learning from the first wave of incident response being overseen by Silver.
Regional Executive level meetings ensure consistent response and good communication across the Sussex system.
Risk Ref. 646 superseded Risk Ref. 612 (Risk to the Delivery of Strategic Objectives during
the Covid-19 Pandemic) which also had an opening score of 25.
Risk activity is monitored by the Resilience Group with risks escalated to the 12+ risk register
as appropriate.
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 172 of 300
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 6
NHS England EPRR Annual Assurance Process
Core Standards
The minimum requirements which commissioners and providers of NHS funded services must
meet are set out in the current NHS England Core Standards for EPRR. These standards are
in accordance with the Civil Contingencies Act 2004 and the NHS Act 2006. Compliance
against these standards is assessed each year via the NHS England annual EPPR assurance
framework. The outcome of the Trust 2019 assurance process was an overall rating of fully
compliant.
Due to the ongoing COVID 19 incident response, the 2020 annual assurance process has
been amended to focus on the following three areas only:
1. Progress made by organisations that were reported as partially or non-compliant in the
2019/20 process
2. The process of capturing and embedding learning from the first wave of the COVID-19
pandemic
3. Inclusion of progress and learning in winter planning preparations.
The Trusts 2020 statement of assurance reports that the organisation has maintained its
status of fully compliant throughout the year, and outlines how organisational learning from the
first wave of the COVID 19 incident response has been captured and embedded into practice.
The statement also outlines the SCFT cold weather and winter plans, accounting for effects of
winter, seasonal flu and a second wave of COVID-19.
2020 Annual Assurance Process Deadlines:
31.10.20 Statements of assurance are made to regional EPRR teams by CCGs
31.12.20 Regional EPRR teams submit their statement of assurance to the national EPRR team
28.02.21 National EPRR team to have completed conversations with regional teams
31.03.21 National EPRR assurance reported to the NHS England and NHS Improvement board and DHSC.
Business Continuity Management
Business Continuity Plans
As part of the level 4 national incident response to COVID-19 the entire NHS was put into
business continuity, with providers required to release capacity to support the COVID-19
preparedness and response. A number of services were suspended across the system,
including a number of SCFT services to ensure the system could cope with the anticipated
large numbers of COVID-19 patients.
In addition to this, there has been a significant change to service delivery across the Trust,
with teams switching to remote working where appropriate or necessary (telephone/video
conferences). This has been implemented throughout clinical and corporate teams.
As part of the COVID-19 incident response, all services were requested to review their
Business Continuity Plans with particular focus on mitigating plans to manage staffing
reduction (up to 50%). Services have been asked to regularly review these plans throughout
Page 173 of 300
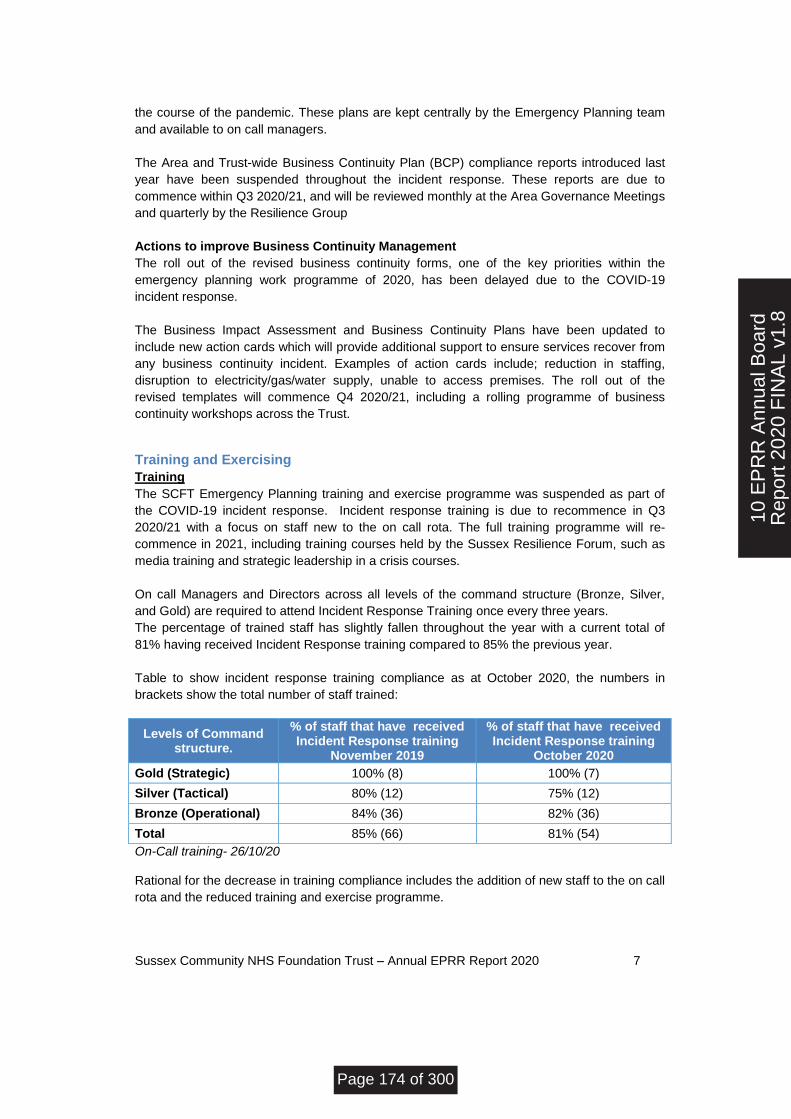
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 7
the course of the pandemic. These plans are kept centrally by the Emergency Planning team
and available to on call managers.
The Area and Trust-wide Business Continuity Plan (BCP) compliance reports introduced last
year have been suspended throughout the incident response. These reports are due to
commence within Q3 2020/21, and will be reviewed monthly at the Area Governance Meetings
and quarterly by the Resilience Group
Actions to improve Business Continuity Management
The roll out of the revised business continuity forms, one of the key priorities within the
emergency planning work programme of 2020, has been delayed due to the COVID-19
incident response.
The Business Impact Assessment and Business Continuity Plans have been updated to
include new action cards which will provide additional support to ensure services recover from
any business continuity incident. Examples of action cards include; reduction in staffing,
disruption to electricity/gas/water supply, unable to access premises. The roll out of the
revised templates will commence Q4 2020/21, including a rolling programme of business
continuity workshops across the Trust.
Training and Exercising
Training
The SCFT Emergency Planning training and exercise programme was suspended as part of
the COVID-19 incident response. Incident response training is due to recommence in Q3
2020/21 with a focus on staff new to the on call rota. The full training programme will re-
commence in 2021, including training courses held by the Sussex Resilience Forum, such as
media training and strategic leadership in a crisis courses.
On call Managers and Directors across all levels of the command structure (Bronze, Silver,
and Gold) are required to attend Incident Response Training once every three years.
The percentage of trained staff has slightly fallen throughout the year with a current total of
81% having received Incident Response training compared to 85% the previous year.
Table to show incident response training compliance as at October 2020, the numbers in
brackets show the total number of staff trained:
Levels of Command structure.
% of staff that have received Incident Response training
November 2019
% of staff that have received Incident Response training
October 2020
Gold (Strategic) 100% (8) 100% (7)
Silver (Tactical) 80% (12) 75% (12)
Bronze (Operational) 84% (36) 82% (36)
Total 85% (66) 81% (54)
On-Call training- 26/10/20 Rational for the decrease in training compliance includes the addition of new staff to the on call
rota and the reduced training and exercise programme.
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 174 of 300
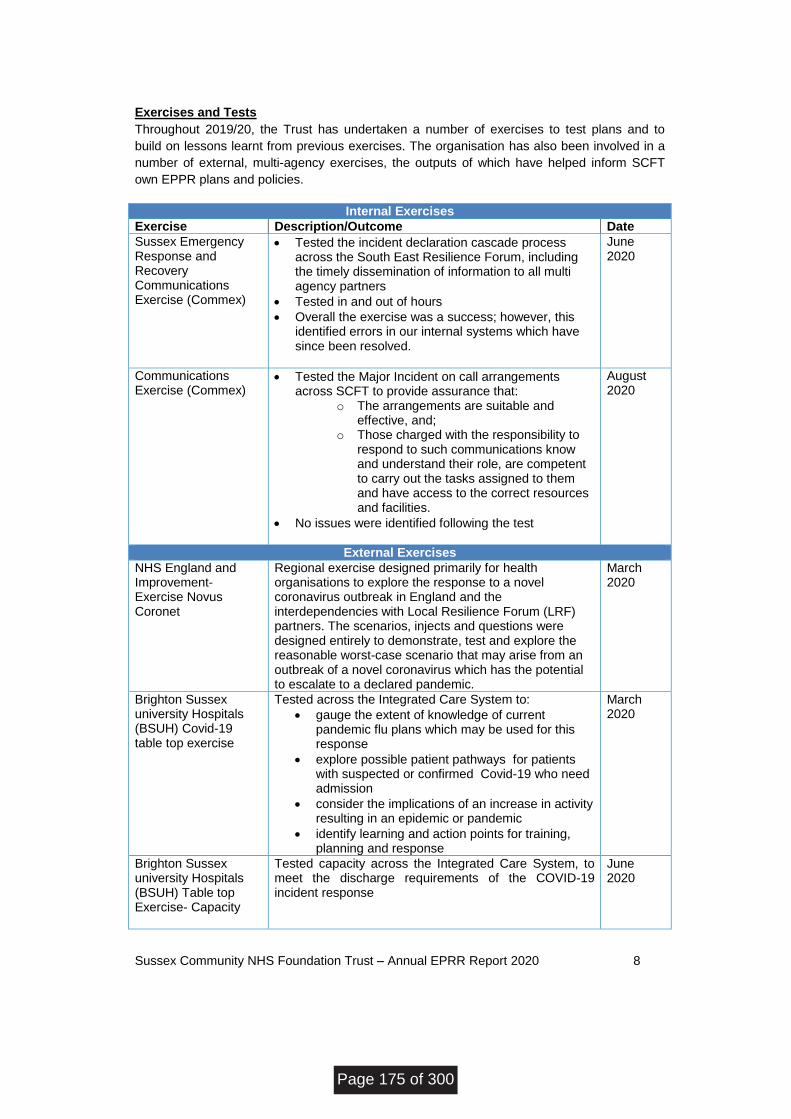
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 8
Exercises and Tests
Throughout 2019/20, the Trust has undertaken a number of exercises to test plans and to
build on lessons learnt from previous exercises. The organisation has also been involved in a
number of external, multi-agency exercises, the outputs of which have helped inform SCFT
own EPPR plans and policies.
Internal Exercises
Exercise Description/Outcome Date
Sussex Emergency Response and Recovery Communications Exercise (Commex)
Tested the incident declaration cascade process across the South East Resilience Forum, including the timely dissemination of information to all multi agency partners
Tested in and out of hours
Overall the exercise was a success; however, this identified errors in our internal systems which have since been resolved.
June 2020
Communications Exercise (Commex)
Tested the Major Incident on call arrangements across SCFT to provide assurance that:
o The arrangements are suitable and effective, and;
o Those charged with the responsibility to respond to such communications know and understand their role, are competent to carry out the tasks assigned to them and have access to the correct resources and facilities.
No issues were identified following the test
August 2020
External Exercises
NHS England and Improvement- Exercise Novus Coronet
Regional exercise designed primarily for health organisations to explore the response to a novel coronavirus outbreak in England and the interdependencies with Local Resilience Forum (LRF) partners. The scenarios, injects and questions were designed entirely to demonstrate, test and explore the reasonable worst-case scenario that may arise from an outbreak of a novel coronavirus which has the potential to escalate to a declared pandemic.
March 2020
Brighton Sussex university Hospitals (BSUH) Covid-19 table top exercise
Tested across the Integrated Care System to:
gauge the extent of knowledge of current pandemic flu plans which may be used for this response
explore possible patient pathways for patients with suspected or confirmed Covid-19 who need admission
consider the implications of an increase in activity resulting in an epidemic or pandemic
identify learning and action points for training, planning and response
March 2020
Brighton Sussex university Hospitals (BSUH) Table top Exercise- Capacity
Tested capacity across the Integrated Care System, to meet the discharge requirements of the COVID-19 incident response
June 2020
Page 175 of 300
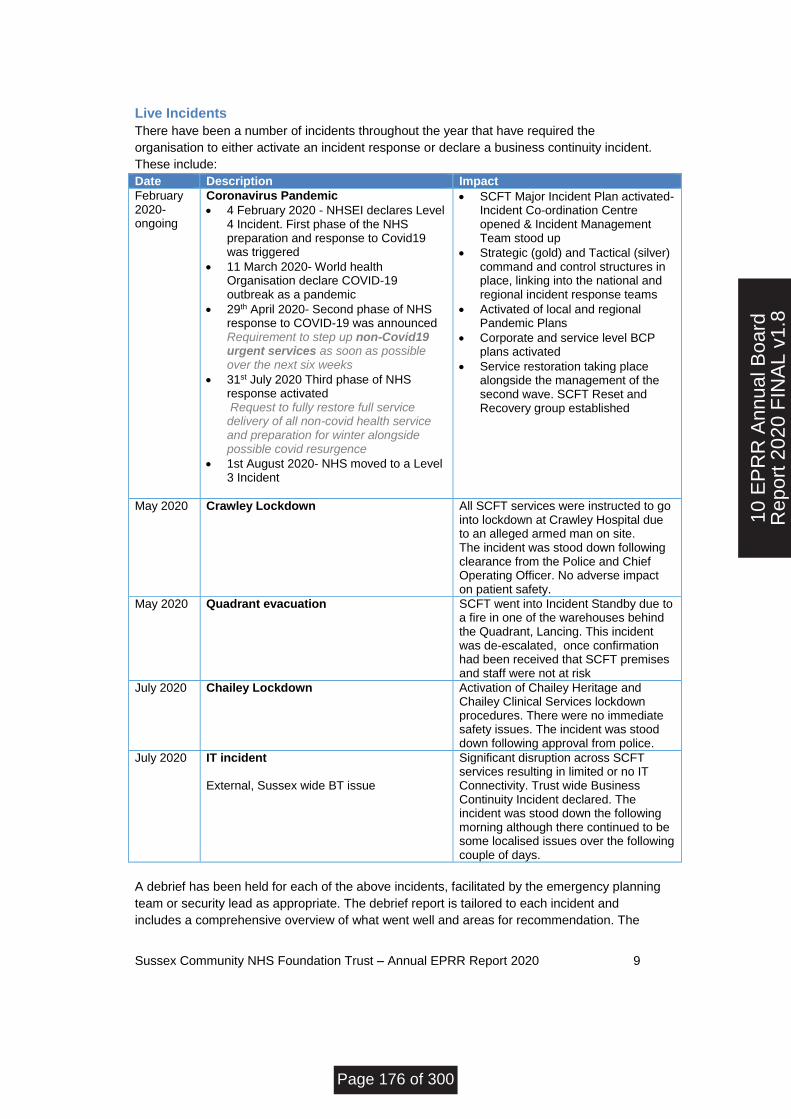
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 9
Live Incidents
There have been a number of incidents throughout the year that have required the
organisation to either activate an incident response or declare a business continuity incident.
These include:
Date Description Impact
February 2020-ongoing
Coronavirus Pandemic
4 February 2020 - NHSEI declares Level 4 Incident. First phase of the NHS preparation and response to Covid19 was triggered
11 March 2020- World health Organisation declare COVID-19 outbreak as a pandemic
29th April 2020- Second phase of NHS response to COVID-19 was announced Requirement to step up non-Covid19 urgent services as soon as possible over the next six weeks
31st July 2020 Third phase of NHS response activated Request to fully restore full service delivery of all non-covid health service and preparation for winter alongside possible covid resurgence
1st August 2020- NHS moved to a Level 3 Incident
SCFT Major Incident Plan activated- Incident Co-ordination Centre opened & Incident Management Team stood up
Strategic (gold) and Tactical (silver) command and control structures in place, linking into the national and regional incident response teams
Activated of local and regional Pandemic Plans
Corporate and service level BCP plans activated
Service restoration taking place alongside the management of the second wave. SCFT Reset and Recovery group established
May 2020 Crawley Lockdown All SCFT services were instructed to go into lockdown at Crawley Hospital due to an alleged armed man on site. The incident was stood down following clearance from the Police and Chief Operating Officer. No adverse impact on patient safety.
May 2020 Quadrant evacuation SCFT went into Incident Standby due to a fire in one of the warehouses behind the Quadrant, Lancing. This incident was de-escalated, once confirmation had been received that SCFT premises and staff were not at risk
July 2020 Chailey Lockdown
Activation of Chailey Heritage and Chailey Clinical Services lockdown procedures. There were no immediate safety issues. The incident was stood down following approval from police.
July 2020 IT incident External, Sussex wide BT issue
Significant disruption across SCFT services resulting in limited or no IT Connectivity. Trust wide Business Continuity Incident declared. The incident was stood down the following morning although there continued to be some localised issues over the following couple of days.
A debrief has been held for each of the above incidents, facilitated by the emergency planning
team or security lead as appropriate. The debrief report is tailored to each incident and
includes a comprehensive overview of what went well and areas for recommendation. The
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 176 of 300
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 10
individual debrief reports, including the accompanying action plans, are held by the emergency
planning team, and overseen by the Resilience Group. The emergency planning team work
with respective action owners to ensure that key organisational learning is captured and
embedded into practice.
As the status of the COVID 19 incident response is still ongoing, SCFT has carried out a
formal and comprehensive debrief of phase one COVID 19 response for the incident
management team. Separate debriefs were held for Strategic Command and Tactical
Command. A combined debrief report has been collated and provides a summary of what
went well, areas of improvement and outlines key learning points. This report has been signed
off by Tactical and Strategic Command. A robust action plan has been developed and
approved and lessons are being embedded into practice and into the organisation’s processes
in preparation for a second wave. Progress against the action plan is overseen by Silver
Command.
SCFT has also contributed to the ICS structured debrief report for phase one of the COVID 19
response. All work stream leads were asked to feedback on their respective area, identifying
lessons learnt and areas for recommendation at a system level. The outcomes of this report
have been cross checked to the Trusts internal debrief report. A second debrief will be held
once the incident is formally stood down.
Throughout the year there have also been a number of smaller IT incidents which has resulted
in the activation of service level business continuity plans. These include the national
disruption to NHS Net and more local IT disruption affecting teams’ ability to connect to the
Trust’s server.
On 6th August 2020, the Met Office issued a warning of high temperatures for the South East
England over the forthcoming week. Public Health England raised the Heat Health Watch to
level 3, requiring all services to activate their Heatwave Plan. There were no reported incidents
as a result of the heatwave period, with no noted impact on service delivery across the Trust.
A number of supporting documents including keeping cool quick tips, uniform and PPE
guidance was produced to support teams throughout this period.
Plans
A series of plans have been reviewed and updated throughout 2020, these include:
Fuel Shortage Plan
Lockdown Policy
Heatwave Plan
Cold Weather Plan
Winter Plan
On call incident specific response plans and guidance
EU Exit End of Transition Period Preparations
The UK exited the EU on 31 January 2020 and is now in a transition period that ends on 31
December 2020. The Department of Health & Social Care (DHSC) are asking the NHS to take
steps now to prepare for the possibility of a default outcome, whilst remaining agile to respond
should a free trade agreement be agreed.
In the coming weeks guidance will be issued on what national plans and what further
mitigations need to be put in place for the following:
Page 177 of 300

Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 11
Continuity of supply
Improved trader readiness
Winter pressures
Increased complexity for reciprocal and cost recovery
Staffing resilience
Data
Ongoing review of government planning assumptions
DHSC will set out an assurance of system preparedness that will take place late November.
EU exit issues will be managed through NHS incident response structures and battle rhythm in
place for COVID-19 (local, regional and national level) and winter operations will be an aligned
function. Transition to incident response and daily sit rep reporting will be established in
December. There will be a single commercial and procurement cell (national) across COVID
and EU exit.
Trust Actions
Ensure Senior Responsible Officer (SRO) and associated team in place
Make board aware of issues
Prepare communication plans / key messages to front line colleagues
Revisit operational guidance from each work-stream and ensure plans are up to date
Revisit assurance exercises and address outstanding actions
Test and communicate escalation routes
Engage across system to identify any further concerns interdependencies and
vulnerabilities around supply chain
With partners ensure integrated system based approach to plans
Consider differences – implications of winter, assumption about port access, vulnerable
populations
Ensure local risk assessments are up to date.
Trust Preparations to date
The SCFT EU Exit Task and Finish Group was stood down in January 2020. In preparation for
the end of the transition period, the group was re-activated in September 2020. The group
currently holds a minimum position awaiting further guidance from DHSC regarding the NHS
preparations and response.
In order to ensure local preparedness the EU exit group have met to:
Review and agree terms of reference and membership
Review SCFT previous position and established processes, and agree next steps
Review risk assessment against reasonable worst case scenario
Agree UK end of transition SRO
Arrange meeting timetable.
Management of concurrent incidents
The emergency planning team have developed a plan for the management of concurrent
incidents, in the event the Trust has to respond to multiple incidents at the same time.
The principle of this framework is that multiple incidents would continue to be managed
through the established command and control structure, with separate cells feeding into the
10 E
PR
R A
nnua
l Boa
rdR
epor
t 202
0 F
INA
L v1
.8
Page 178 of 300
Sussex Community NHS Foundation Trust – Annual EPRR Report 2020 12
Tactical Lead as required. Each cell will have its own emergency planning support and
allocated admin resource. The management of this event will be dynamically assessed, with
the flexibility to cross over and link cells where required.
The model reflects the national and regional operational structure.
Conclusion
Throughout 2020, the emergency planning team have been at the core of the Trust Incident
Response. Whilst this has disrupted the team’s programme of work, there is a sense of
achievement within the team regarding the organisations response to Covid-19 in what is
deemed an unprecedented incident.
The team currently compromises of an Emergency Planning Lead (WTE 0.8) and an
Emergency Planning Officer (1 WTE). This additional resource (from 1.0 WTE in previous
years) has meant that business as usual activities have been restored as far as reasonably
possible following the first wave of the Pandemic. The expansion of the team also means that
there is adequate resource and actions in place to support the organisation to sustain its
EPPR assurance rating of fully compliant.
Priorities for 2021 include:
Roll out of the new Business Continuity Management processes, which will include
workshops delivered throughout the Trust over the course of the year.
Improvement in the quality of service level BCPs and routine review and testing by
services.
Continued focus on the training and exercise programme.
The interface between emergency planning and other subject areas (Fire, Estates and IT) is
an area of continuous improvement, and over the forthcoming months, the emergency
planning team will continue to work dynamically with other subject leads to assess the
completeness of plans and complete oversight of EPRR requirements.
Throughout 2021, the Resilience Group will continue to monitor EPRR activity and to review
the implementation of recommended actions resulting from EPRR Risks, new national
guidance and learning from incidents.
Page 179 of 300
Page 1 of 3
BOARD OF DIRECTORS - PUBLIC MEETING
26 November 2020
Agenda Item Number:
Report Title 2020 Local Clinical Excellence Awards Annual Report
Purpose
Approval Assurance X Discussion Briefing
Summary A report to the Board on the 2020 local consultant clinical excellence awards round and the national changes made to this years’ round in light of the COVID-19 pandemic. The report is provided in accordance with the Local Clinical Excellence Awards Guidance 2018-21 (England).
Previously reviewed by: Dr Sara Lightowlers, Medical Director
Recommendation: The Board is asked to review the content of this report.
CQC Domains (Safe; Caring; Responsive; Effective; Well Led) indicate which are relevant below:
Well Led
Relevance to Trust’s Strategic Goals:
Quality Improvement and Thriving staff
Equality and Diversity The clinical excellence awards scheme is subject to equality impact assessment. No adverse impact on equality and diversity has been identified.
Report authors: Dr Sara Lightowlers – Medical Director Richenda Tite – Medical and Dental HR Manager
Report owner: Dr Sara Lightowlers – Medical Director
12 L
ocal
Clin
ical
Exc
elle
nce
Aw
ards
Ann
ual R
epor
t 202
0
Page 180 of 300
Page 2 of 3
1.0 Executive Summary a) Clinical Excellence Awards are annual awards to recognise and reward NHS
consultants who perform ‘over and above’ the standard expected of their role. Awards are given for quality and excellence, acknowledging exceptional personal contributions.
b) In 2018, NHS Employers and the British Medical Association (BMA) agreed
an amendment to the Terms and Conditions – Consultants (England) 2003. The agreement details the new provisions that will apply to new local CEAs awarded from 1 April 2018 to 31 March 2021 and future awards from 1 April 2021.
c) Under the new three-year arrangement, awards are time limited for the
duration of the three year period and non-consolidated, allowing for reinvestment of the released funds when the award ends. The lump-sum value of the award is £3,092 per annum.
d) Local CEAs made prior to 1 April 2018 will be retained by award holders,
subject to a nationally agreed review process from 2021 onwards.
2.0 2020 Local Clinical Excellence Awards a) In March 2020, the Department of Health and the British Medical Association
agreed to halt the 2020/21 local CEA rounds as a result of the COVID-19 pandemic, with the award money to be distributed equally among eligible consultants instead. This was to enable clinicians, administrators and the executive to focus on immediate priorities.
b) The national agreement, which was discussed and endorsed at the Trust’s
Joint Local Negotiating Committee, meant the 2020 local CEA funding, as well as the money rolled over from the last two years of the scheme, would be distributed equally among eligible consultants as a one-off, non-consolidated payment in place of the normal local CEA round.
d) 2020 Summary:
Number of consultants as at 1 April 2020 26
Number of eligible consultants as at 1 April 2020 23
2020 investment and carry forward from 2018/19 and 20/21 rounds £73,685.00
2020 value of one-off, non-consolidated payment per eligible consultant £3,203.69
The non-consolidated payment will be made to eligible consultants in the November payroll.
Page 181 of 300
Page 3 of 3
3.0 Conclusion a) Given the current circumstances with COVID-19, the temporary three year
arrangement for local CEAs is being extended for another year (to 31 March 2022) to enable the Department of Health to complete negotiations on future arrangements with the Unions, to be implanted from 1 April 2022.
b) The Board is asked to note the contents of the report.
12 L
ocal
Clin
ical
Exc
elle
nce
Aw
ards
Ann
ual R
epor
t 202
0
Page 182 of 300

BOARD OF DIRECTORS – PUBLIC MEETING
26 November 2020
Agenda Item Number: 13
Report Title: Standing Financial Instructions, Standing Orders , Reservation and Delegation of Powers and Detailed Scheme of Delegation
Purpose: Approval x Assurance x Discussion Briefing
Summary: The Board is asked to ratify the following four documents:
Standing Financial Instructions and Scheme of Delegation.
Standing Orders for the Board of Board of Directors.
Reservation and Delegation of Powers.
Detailed Scheme of Delegation. For ease these documents have been incorporated into one document. The updated full document and the individual four documents will be made available on the intranet (Pulse). These documents support the effective and efficient business of the Board including items for delegation.
Recommendation:
The Board is asked to ratify these documents.
Previously reviewed:
All four documents at the October Audit Committee with minor amends incorporated.
Standing Orders of the Board of Directors – Virtually.
Standing Financial Instruction – Executive Committee 15 September.
Reservation and Delegation of Powers – Virtually.
Detailed Scheme of Delegation – Executive Committee 15 September.
Relevance to Trust’s Strategic Goals: To support the effective and efficient business of the Board.
Relevance to CQC Domains: This paper relates to the CQC well-led domain.
Equality and Diversity: An Equality and Human Rights Analysis (EHRA) is not applicable to these documents. There are no negative impacts on any specific groups or protected characteristics.
Report author: Paul Somerville, Deputy Trust Secretary
Report owner: Mike Jennings, Chief Financial Officer and Zoe Smith, Trust Secretary
13 C
S S
tand
ing
Fin
anci
alIn
stru
ctio
ns a
nd S
tand
ing
Page 183 of 300
STANDING FINANCIAL INSTRUCTIONS AND SCHEME OF DELEGATION
Author(s)
Head of Financial Accounts
Version
2020: v1
Version Date
July 2020
Implementation/approval Date
October 2020
Review Date
October 2022 (or sooner if legislative and/or regulatory/best practice governance changes require this)
Review Body
Audit Committee (but requiring Board approval)
Policy Reference Number
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 184 of 300
2
CONTENTS
CONTENTS 2
1. INTRODUCTION 5 1.1 General 5 1.2 Responsibilities and delegation 5
2. AUDIT 7 2.1 Audit Committee 7 2.2 Chief Financial Officer 7 2.3 Role of Internal Audit 8 2.4 External Audit 9 2.5 Fraud and Corruption 9 2.6 Security Management 9
3. RESOURCE LIMIT CONTROL 10
4. ALLOCATIONS, PLANNING, BUDGETS, BUDGETARY CONTROL, AND MONITORING 10 4.1 Preparation and Approval of Plans and Budgets 10 4.2 Budgetary Delegation 10 4.3 Budgetary Control and Reporting 11 4.4 Capital Expenditure 12 4.5 Monitoring Returns 12
5. ANNUAL ACCOUNTS AND REPORTS 12 5.1 The Chief Financial Officer 12 The Chief Financial Officer, on behalf of the Trust, will: 12 5.2 Annual Report 12
6. BANK ACCOUNTS 12 6.1 General 12 6.2 Bank Accounts 12 6.3 Banking Procedures 13 6.4 Tendering and Review 13
7. INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS 13
7.1 Income Systems 13 7.2 Fees and Charges 13 7.3 Debt Recovery 13 7.4 Security of Cash, Cheques and other Negotiable Instruments 13
8. TENDERING AND CONTRACTING PROCEDURE 14 8.1 Duty to comply with Standing Orders and Standing Financial Instructions 14 8.2 EU Directives Governing Public Procurement 14 8.3 Reverse eAuctions 14 8.4 Department of Health and Social Care Guidance 14 8.5 Formal Competitive Tendering 14 8.6 Contracting/Tendering Procedure 16 8.7 Quotations: Competitive and non-competitive 20 8.8 Authorisation of Tenders and Competitive Quotations 20 8.9 Instances where formal competitive tendering or competitive quotation is not required 21 8.10 Private Finance for capital procurement (see overlap with Standing Financial Instruction 24) 21 8.11 Compliance requirements for all contracts 21 8.12 Personnel and Agency or Temporary Staff Contracts 22 8.13 Healthcare Services Agreements (see overlap with Standing Financial Instruction 18) 22 8.14 Disposals (See overlap with Standing Financial Instruction 26) 22
Page 185 of 300
3
8.15 In-house Services 22 8.16 Applicability of Standing Financial Instructions on Tendering and Contracting to funds held in trust (see overlap with Standing Financial Instruction 29) 23
9. NHS CONTRACTS FOR PROVISION OF SERVICES (see overlap with Standing Financial Instruction 17.13) 23
9.1 Contracts 23 9.2 Involving Partners and jointly managing risk 23 9.3 Department of Health and Social Care Policies and Guidelines 23 9.4 Reports to Board on commissioner contracts 23
10. COMMISSIONING 24
11. TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE TRUST BOARD AND EXECUTIVE COMMITTEE AND EMPLOYEES 24
11.1 Funded Establishment 24 11.2 Staff Appointments 24 11.3 Processing Payroll 24 11.4 Contracts of Employment 25
12. NON-PAY EXPENDITURE 25 12.1 Delegation of Authority 25 12.2 Choice, Requisitioning, Ordering, Receipt and Payment for Goods and Services (see overlap
with Standing Financial Instruction No. 8). 26 12.3 Joint Finance Arrangements with Local Authorities and Voluntary Bodies (see overlap with Standing Order 9.1) 28
13. EXTERNAL BORROWING 28 13.2 INVESTMENTS 29
14. FINANCIAL FRAMEWORK 29
15. CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND SECURITY OF ASSETS 29 15.1 Capital Investment 29 15.2 Private Finance (see overlap with Standing Financial Instruction 17.10) 30 15.3 Asset Registers 31 15.4 Security of Assets 31
16. STORES AND RECEIPT OF GOODS 32 16.1 General position 32 16.2 Control of Stores, Stocktaking, condemnations and disposal 32 16.3 Goods supplied by NHS Supply Chain 33
17. DISPOSALS AND CONDEMNATIONS, LOSSES AND SPECIAL PAYMENTS 33 17.1 Disposals and Condemnations 33 17.2 Losses and Special Payments 33
18. INFORMATION TECHNOLOGY 34 18.1 Responsibilities and duties of the Chief Financial Officer 34 18.2 Responsibilities and duties of other Directors and Officers in relation to computer systems of a general application 35 18.3 Contracts for Computer Services with other health bodies or outside agencies 35 18.4 Risk Assessment 35 18.5 Requirements for Computer Systems which have an impact on corporate financial systems 35
19. PATIENTS' PROPERTY 35 19.1 Safe Custody 36 The Trust has a responsibility to provide safe custody for money and other personal property (hereafter referred to as "property") handed in by patients, in the possession of unconscious or
confused patients, or found in the possession of patients dying in hospital or dead on arrival. 36 19.2 Informed Before or at Admission 36 The Chief Executive is responsible for ensuring that patients or their guardians, as appropriate, are
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 186 of 300

4
informed before or at admission by: 36 19.3 Written Instructions 36 19.4 Opening of Separate Accounts for Patients' Moneys 36 19.5 When Probate or Letters of Administration are Required 36 19.6 Staff Responsibilities and Duties 36 19.7 Safekeeping for Specific Purposes 36
20. FUNDS HELD ON TRUST 36 20.1 Corporate Trustee 36 20.2 Accountability to Charity Commission and Secretary of State for Health and Social Care 37 20.3 Applicability of Standing Financial Instructions to funds held on Trust 37
21. Acceptance Of Gifts By Staff And Link To Standards Of Business Conduct 37
22. PAYMENTS TO INDEPENDENT CONTRACTORS 37
23. RETENTION OF RECORDS 37
24. RISK MANAGEMENT AND INSURANCE 37 24.1 Programme of Risk Management 37 24.2 Insurance arrangements with commercial insurers 38
APPENDICES
25. Appendix 1 - Standing Orders for the Board of Directors 39
26. Appendix 2 - Reservation and Delegation of Powers 83
27. Appendix 3 - Detailed Scheme of Delegation 105
Page 187 of 300
5
1. INTRODUCTION
1.1 General
1.1.1 These Standing Financial Instructions (SFIs) are issued to ensure that the Trust’s
financial affairs are managed in accordance with the law and Government policy in
order to achieve probity, accuracy, economy, efficiency and effectiveness. They are issued, for the regulation of the conduct of its members and officers in relation to all financial matters with which they are concerned. They shall have effect as if
incorporated in the Standing Orders (SOs).
1.1.2 These Standing Financial Instructions detail the financial responsibilities, policies and procedures adopted by the Trust. They are designed to ensure that the Trust's
financial transactions are carried out in accordance with the law and with Government policy in order to achieve probity, accuracy, economy, efficiency and effectiveness. They should be used in conjunction with the Schedule of Decisions
Reserved to the Board and the Scheme of Delegation adopted by the Trust.
1.1.3 These Standing Financial Instructions identify the financial responsibilities which apply to everyone working for the Trust and its constituent organisations including
Trading Units, except where those Trading units have adopted different SFIs specific to their circumstances... They do not provide detailed procedural advice
and should be read in conjunction with the detailed departmental and financial procedure notes. All financial procedures must be approved by the Chief Financial Officer.
1.1.4 Should any difficulties arise regarding the interpretation or application of any of the
Standing Financial Instructions then the advice of the Chief Financial Officer must be sought before acting. The user of these Standing Financial Instructions should
also be familiar with and comply with the provisions of the Trust’s Standing Orders.
1.1.5 The failure to comply with Standing Financial Instructions and Standing Orders can in certain circumstances be regarded as a disciplinary matter that could result
in dismissal.
1.1.6 Overriding Standing Financial Instructions – If for any reason these Standing
Financial Instructions are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the
noncompliance shall be reported to the next formal meeting of the Audit Committee for referring action or ratification. All members of the Board and staff have a duty to
disclose any non-compliance with these Standing Financial Instructions to the Chief Executive as soon as possible.
1.2 Responsibilities and delegation
1.2.1 The Trust Board
The Board exercises financial supervision and control by:
i) formulating the financial strategy
ii) requiring the submission and approval of budgets within approved allocations/overall income
iii) Defining and approving essential features in respect of important procedures and
financial systems (including the need to obtain value for money) and
iv) defining and approving essential features in respect of important procedures and financial systems (including the need to obtain value for money); and
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 188 of 300
6
v) defining specific responsibilities placed on members of the Board and employees as indicated in the Scheme of Delegation document.
1.2.2 The Board has resolved that certain powers and decisions may only be exercised
by the Board in formal session. These are set out in the Reservation of Matters Reserved to the Board document. All other powers have been delegated to such other committees as the Trust has established.
1.2.3 The Chief Executive and the Chief Financial Officer
The Chief Executive and the Chief Financial Officer will, as far as possible, delegate their detailed responsibilities, but they remain accountable for financial control.
Within the Standing Financial Instructions, it is acknowledged that the Chief
Executive is ultimately accountable to the Board, and as Accounting Officer, to the Secretary of State, for ensuring that the Board meets its obligation to perform its functions within the available financial resources. The Chief Executive has overall
executive responsibility for the Trust’s activities; is responsible to the Chair and the Board for ensuring that its financial obligations and targets are met and has overall
responsibility for the Trust’s system of internal control.
1.2.4 It is a duty of the Chief Executive to ensure that Members of the Board and,
employees and all new appointees are notified of, and put in a position to understand their responsibilities within these Instructions.
1.2.5 The Chief Financial Officer The Chief Financial Officers responsible for:
i) implementing the Trust’s financial policies and for coordinating any corrective action
necessary to further these policies;
ii) maintaining an effective system of internal financial control including ensuring that detailed financial procedures and systems incorporating the principles of separation
of duties and internal checks are prepared, documented and maintained to supplement these instructions;
(iii) ensuring that sufficient records are maintained to show and explain the Trust’s
transactions, in order to disclose, with reasonable accuracy, the financial position of the Trust at any time;
and, without prejudice to any other functions of the Trust, and employees of the Trust, the duties of the Chief Financial Officer include;
(iv) the provision of financial advice to other members of the Board and employees;
(v) the design, implementation and supervision of systems of internal financial control;
(vi) the preparation and maintenance of such accounts, certificates, estimates, records
and reports as the Trust may require for the purpose of carrying out its statutory duties.
1.2.6 Board Members and Employees
All members of the Board and employees, severally and collectively, are responsible
for:
(i) the security of the property of the Trust;
(ii) avoiding loss;
iii) exercising economy and efficiency in the use of resources;
Page 189 of 300
7
iv) conforming with the requirements of Standing Orders, Standing Financial Instructions, Financial Procedures, Scheme of Delegation, constitution and terms of
authorisation
1.2.7 Contractors and their employees
Any contractor or employee of a contractor who is empowered by the Trust to commit the Trust to expenditure or who is authorised to obtain income shall be
covered by these instructions. It is the responsibility of the Chief Executive to ensure that such persons are made aware of this.
1.2.8 For all members of the Board and any employees who carry out a financial
function, the form in which financial records are kept and the manner in which members of the Board and employees discharge their duties must be acceptable
in the professional opinion of the Chief Financial Officer.
2. AUDIT
2.1 Audit Committee
2.1.1 In accordance with Standing Orders, the Board shall formally establish a Committee, with clearly defined terms of reference and following guidance from the
NHS Audit Committee Handbook (2005 and any subsequent versions), which will provide an independent and objective view of internal control by:
i) overseeing internal and external audit services;
ii) reviewing financial and information systems and significant financial reporting judgments;
iii) review the establishment and maintenance of an effective system of internal control,
across the whole of the organisation’s activities (both clinical and non-clinical), that supports the achievement of the organisation’s objectives;
iv) monitoring compliance with Standing Orders and Standing Financial Instructions;
v) reviewing schedules of losses and compensations and making recommendations to
the Board;
vi) reviewing the arrangements in place to support the Assurance Framework process
prepared on behalf of the Board and advising the Board accordingly.
2.1.2 It is the responsibility of the Audit Committee to ensure an adequate Internal Audit
service is provided and the Chief Financial Officer shall be involved in the selection process when/if an Internal Audit service provider is changed.
2.1.3 The Audit Committee has delegated powers to approve the Trust’s annual report
and accounts.
2.2 Chief Financial Officer
2.2.1 The Chief Financial Officers responsible for:
i) ensuring there are arrangements to review, evaluate and report on the effectiveness
of internal financial control including the establishment of an effective Internal Audit function;
ii) ensuring that the Internal Audit is adequate and meets the NHS mandatory audit standards;
iii) deciding at what stage to involve the police in cases of misappropriation and other
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 190 of 300
8
irregularities not involving fraud or corruption;
iv) ensuring that an annual internal audit report is prepared for the consideration of the
Audit Committee which should allow the Chair to give assurance to the Board. The report must cover:
a) a clear opinion on the effectiveness of internal control in accordance with current
assurance framework guidance issued by the Department of Health and Social Care including for example compliance with control criteria and standards;
b) major internal financial control weaknesses discovered;
c) progress on the implementation of internal audit recommendations;
d) progress against plan over the previous year;
e) strategic audit plan covering the coming three years;
f) a detailed plan for the coming year.
2.2.2 The Chief Financial Officer or designated auditors are entitled without necessarily
giving prior notice to require and receive:
i) access to all records, documents and correspondence relating to any financial or
other relevant transactions, including documents of a confidential nature;
ii) access at all reasonable times to any land, premises or members of the Board or employee of the Trust;
iii) the production of any cash, stores or other property of the Trust under a member of
the Board and/or an employee's control; and
iv) explanations concerning any matter under investigation.
2.3 Role of Internal Audit
2.3.1 Internal Audit will review, appraise and report upon:
i) the extent of compliance with, and the financial effect of, relevant established
policies, plans and procedures;
ii) the adequacy and application of financial and other related management controls;
iii) the suitability of financial and other related management data;
iv) the extent to which the Trust’s assets and interests are accounted for and safeguarded from loss of any kind, arising from:
a) fraud and other offences;
b) waste, extravagance, inefficient administration;
c) poor value for money or other causes.
v) Internal Audit shall also independently verify the Assurance Statements in
accordance with guidance from the Department of Health and Social Care.
2.3.2 Whenever any matter arises which involves, or is thought to involve, irregularities
concerning cash, stores, or other property or any suspected irregularity in the
Page 191 of 300
9
exercise of any function of a pecuniary nature, the Chief Financial Officer must be notified immediately.
2.3.3 The Chief Internal Auditor will normally attend Audit Committee meetings and has a right of access to all Audit Committee members, the Chair and Chief Executive of
the Trust.
2.3.4 The Chief Internal Auditor shall be accountable to the Chair of the Audit Committee. The reporting system for internal audit shall be agreed between the
Chief Financial Officer, the Audit Committee and the Chief Internal Auditor. The agreement shall be in writing and shall comply with the guidance on reporting
contained in the NHS Internal Audit Standards. The reporting system shall be reviewed at least every three years.
2.4 External Audit
The External Auditor is appointed by the Council of Governors and paid for by the
Trust. The Audit Committee must ensure a cost-efficient service. If there are any problems relating to the service provided by the External Auditor, then this should
be raised with the External Auditor and reported to the Audit Committee and the Council of Governors if the issue cannot be resolved.
2.5 Fraud and Corruption
2.5.1 Fraud: any person who dishonestly makes a false representation to make a gain
for themselves or another, or who dishonesty fails to disclose to person information
which they are under a legal duty to disclose, or commits fraud by abuse of position including any offence as defined in the Fraud Act 2006.
2.5.2 Bribery: Where the trust is engaged in commercial activity it could be considered
guilty of a corporate bribery offence if an employee, agent, subsidiary or any other person acting on its behalf bribes another person, intending to obtain or retain
business or an advantage in the conduct of business for the Trust and it cannot demonstrate that it has adequate procedures in place to prevent such. The Trust does not tolerate any bribery on its behalf, even if this might result in a loss of
business for it. Criminal liability must be prevented at all times.
2.5.3 In line with their responsibilities, the Trust Chief Executive and Chief Financial Officer shall monitor and ensure compliance with Directions issued by the
Secretary of State for Health and Social Care on fraud and corruption, primarily using a local risk based approach to fraud, in conjunction with its Counter Fraud
Specialist (CFS)
2.5.4 The Trust shall nominate a suitable person to carry out the duties of the Local
Counter Fraud Specialist as specified by the Department of Health and Social Care Counter Fraud and Corruption Manual and guidance
2.5.5 The Counter Fraud Specialist shall report to the Chief Financial Officer and shall
work with staff in the NHS Counter Fraud Authority (NHSCFA) in accordance with the Department of Health and Social Care Counter Fraud and Corruption Manual.
2.5.6 The Counter Fraud Specialist will provide a written report, at least annually, on
counter fraud work within the Trust.
2.6 Security Management
2.6.1 In line with their responsibilities, the Trust Chief Executive will monitor and ensure
compliance with Directions issued by the Secretary of State for Health and Social Care on NHS security management.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 192 of 300
10
2.6.2 The Trust shall nominate a suitable person to carry out the duties of the Local
Security Management Specialist (LSMS) as specified by the Secretary of State for Health and Social Care guidance on NHS security management.
2.6.3 The Trust shall nominate a Non-Executive Director to be responsible to the Board for NHS security management.
2.6.4 The Chief Executive has overall responsibility for controlling and coordinating
security. However, key tasks are delegated to the Security Management Director (SMD) and the appointed Local Security Management Specialist (LSMS).
3. RESOURCE LIMIT CONTROL
Not applicable to NHS Foundation Trusts, for which the only control is through a Prudential Borrowing Limit (PBL).
4. ALLOCATIONS, PLANNING, BUDGETS, BUDGETARY CONTROL, AND MONITORING
4.1 Preparation and Approval of Plans and Budgets
4.1.1 The Chief Executive will compile and submit to the Board an Annual Operating Plan which takes into account financial targets and forecast income, efficiencies and service developments. The Trust will give information as to its forward planning in respect of each financial year to the Independent Regulator. This information will be prepared by the Directors who must have regard to the views of the Council of Governors
4.1.2 Prior to the start of the financial year the Chief Financial Officer will, on behalf of the Chief Executive, prepare and submit budgets for approval by the Board. Such
budgets will:
i) be in accordance with the aims and objectives set out in the Annual Operating Plan;
ii) accord with activity and workforce plans;
iii) be produced following discussion with appropriate budget holders;
iv) be prepared within the limits of available funds and with regard to the prudential borrowing limit;
v) identify potential risks.
4.1.3 The Chief Financial Officer shall monitor financial performance against budget and
plan, periodically review them, and report to the Board.
4.1.4 All budget holders must provide information as required by the Chief Financial
Officer to enable budgets to be compiled.
4.1.5 All budget holders will participate in the development of their budgets and will sign up to them before the start of the financial year to which the budget relates.
4.1.6 The Chief Financial Officer has a responsibility to ensure that adequate training is
delivered on an on-going basis to budget holders to help them manage successfully.
4.2 Budgetary Delegation
4.2.1 The Chief Executive may delegate the management of budgets for defined services to the officers responsible for the management of those services. Control
Page 193 of 300
11
of budgets shall be exercised in accordance with these Standing Financial Instructions and supplementary guidance issued by the Chief Financial Officer.
4.2.2 The Chief Executive and delegated budget holders must not exceed the budgetary total or virement limits set by the Board.
4.2.3 Budgets shall be used only for the purpose for which they were provided and any
budgeted funds not required for their designated purpose shall revert to the immediate control of the Chief Executive, unless covered by delegated powers of
virement.
4.2.4 Non-recurring budgets should not be used to finance recurring expenditure without the authority in writing of the Chief Executive, as advised by the Chief
Financial Officer.
4.3 Budgetary Control and Reporting
4.3.1 The Chief Financial Officer will devise and maintain systems of budgetary control. These will include:
i) monthly financial reports to the Board in a form approved by the Board containing:
a) income and expenditure to date showing trends and forecast year-end position;
b) movements in working capital;
c) movements in cash and capital;
d) capital project spend and projected outturn against plan;
e) explanations of any material variances from plan;
f) details of any corrective action where necessary and the Chief Executive's and/or
Chief Financial Officer’s view of whether such actions are sufficient to correct the situation.
ii) the issue of timely, accurate and comprehensible advice and financial reports to
each budget holder, covering the areas for which they are responsible.
iii) investigation and reporting of variances from financial, workload and manpower budgets.
iv) monitoring of management action to correct variances.
v) arrangements for the authorisation of budget transfers.
4.3.2 Each Budget Holder is responsible for ensuring that:
i) any likely overspending or reduction of income which cannot be met by virement in
accordance with the Trust’s Virement Policy (where applicable) is not incurred without the prior consent of the Board;
ii) the amount provided in the approved budget is not used in whole or in part for any purpose other than that specifically authorised subject to the rules of virement;
iii) no permanent or temporary employees are appointed without the approval of the
Chief Executive other than those provided for within the available resources and manpower establishment as approved by the Board.
4.3.3 The Chief Executive is responsible for identifying and implementing cost savings
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 194 of 300
12
and income generation initiatives in accordance with the requirements of the Annual Operating Plan and a balanced budget.
4.4 Capital Expenditure
The general rules applying to delegation and reporting shall also apply to capital
expenditure. (The particular applications relating to capital are contained in Standing Financial Instruction 15).
4.5 Monitoring Returns
The Chief Executive is responsible for ensuring that the appropriate monitoring forms are submitted to the requisite monitoring organisation.
5. ANNUAL ACCOUNTS AND REPORTS
5.1 The Chief Financial Officer
The Chief Financial Officer, on behalf of the Trust, will:
i) prepare financial returns in accordance with the accounting policies and guidance given by the Department of Health and Social Care and the Treasury, the Trust’s
accounting policies, and generally accepted accounting practice;
ii) prepare and submit annual financial reports to the Independent Regulator certified
in accordance with current guidelines;
iii) submit financial returns to the Independent Regulator for each financial year in accordance with the timetable prescribed by the Department of Health and Social
Care;
5.2 Annual Report
The Trust’s annual report including the audited annual accounts must be presented to a public meeting and made available to the public. A copy of the annual report and accounts and any report of the external auditor are laid before Parliament and following this, copies of these documents are sent to the Independent Regulator. The Trust’s annual report including the audited annual accounts must be presented to the Board of Directors for approval and received by the Council of Governors at a public meeting.
6. BANK ACCOUNTS
6.1 General
6.1.1 The Chief Financial Officer is responsible for managing the Trust’s banking
arrangements and for advising the Trust on the provision of banking services and operation of accounts. This advice will take into account guidance/ directions
issued from time to time by the Department of Health and Social Care.
6.1.2 The Board shall approve the banking arrangements.
6.2 Bank Accounts
The Chief Financial Officer is responsible for:
i) bank accounts;
ii) establishing separate bank accounts for the Trust’s non-exchequer funds;
iii) ensuring payments made from bank accounts do not exceed the amount credited to the account except where arrangements have been made;
iv) reporting to the Board all arrangements made with the Trust’s bankers for accounts
to be overdrawn;
v) monitoring compliance with Department of Health and Social Care guidance on the
Page 195 of 300
13
level of cleared funds.
6.3 Banking Procedures
6.3.1 The Chief Financial Officer will prepare detailed instructions on the operation of
bank accounts which must include:
i) the conditions under which each bank account is to be operated;
ii) those authorised to sign cheques or other orders drawn on the Trust’s accounts.
6.3.2 The Chief Financial Officer must advise the Trust’s bankers in writing of the
conditions under which each account will be operated.
6.4 Tendering and Review
6.4.1 The Chief Financial Officer will review the commercial banking arrangements of
the Trust at regular intervals to ensure they reflect best practice and represent best value for money by periodically seeking competitive tenders for the Trust’s
commercial banking business.
6.4.2 Competitive tenders should be sought periodically, and ideally, at least every five years. The results of the tendering exercise should be reported to the Board.
7. INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS
7.1 Income Systems
7.1.1 The Chief Financial Officer is responsible for designing, maintaining and ensuring
compliance with systems for the proper recording, invoicing, collection and coding of all monies due.
7.1.2 The Chief Financial Officer is also responsible for the prompt banking of all monies
received.
7.2 Fees and Charges
7.2.1 The Chief Financial Officer is responsible for approving and regularly reviewing the level of all fees and charges other than those determined by the Department of
Health and Social Care or by Statute. Independent professional advice on matters of valuation shall be taken as necessary. Where sponsorship income (including items in kind such as subsidised goods or loans of equipment) is considered the
guidance in the Department of Health and Social Care’s Commercial Sponsorship – Ethical standards in the NHS shall be followed.
7.2.2 All employees must inform the Chief Financial Officer promptly of money due
arising from transactions which they initiate/deal with, including all contracts, leases, tenancy agreements, private patient undertakings and other transactions.
7.3 Debt Recovery
7.3.1 The Chief Financial Officer is responsible for the appropriate recovery action on all outstanding debts.
7.3.2 Income not received should be dealt with in accordance with losses procedures.
7.3.3 Overpayments should be detected (or preferably prevented) and recovery initiated.
7.4 Security of Cash, Cheques and other Negotiable Instruments
7.4.1 The Chief Financial Officer is responsible for:
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 196 of 300
14
i) approving the form of all receipt books, agreement forms, or other means of officially acknowledging or recording monies received or receivable;
ii) ordering and securely controlling any such stationery;
iii) the provision of adequate facilities and systems for employees whose duties include
collecting and holding cash, including the provision of safes or lockable cash boxes, the procedures for keys, and for coin operated machines;
iv) prescribing systems and procedures for handling cash and negotiable securities on behalf of the Trust.
7.4.2 Official money shall not under any circumstances be used for the encashment of
private cheques or IOUs.
7.4.3 All cheques, cash etc., shall be banked intact. Disbursements shall not be made from cash received, except under arrangements approved by the Chief Financial
Officer.
7.4.4 The holders of safe keys shall not accept unofficial funds for depositing in their
safes unless such deposits are in special sealed envelopes or locked containers. It shall be made clear to the depositors that the Trust is not to be held liable for any
loss, and written indemnities must be obtained from the organisation or individuals absolving the Trust from responsibility for any loss.
8. TENDERING AND CONTRACTING PROCEDURE
8.1 Duty to comply with Standing Orders and Standing Financial Instructions
The procedure for making all contracts by or on behalf of the Trust shall comply with
these Standing Orders and Standing Financial Instructions (except where Suspension of Standing Orders is applied).
8.2 EU Directives Governing Public Procurement
Directives by the Council of the European Union promulgated by the Department of Health and Social Care prescribing procedures for awarding all forms of contracts shall have effect as if incorporated in these Standing Orders and Standing Financial
Instructions.
8.3 Reverse eAuctions
The Trust must have policies and procedures in place for the control of all tendering
activity carried out through Reverse eAuctions should the Trust choose to use this mechanism.
8.4 Department of Health and Social Care Guidance
The Trust shall comply as far as is practicable with the requirements of the Department of Health and Social Care “Estate code” and any other relevant guidance in respect of capital investment and estate and property transactions. In the case of
management consultancy contracts the Trust shall comply as far as is practicable with Department of Health and Social Care guidance "The Procurement and
Management of Consultants within the NHS".
8.5 Formal Competitive Tendering
8.5.1 General Applicability
The Trust shall ensure that competitive tenders are invited for:
i) the supply of goods, materials and manufactured articles;
ii) the rendering of services including all forms of management consultancy services
(other than specialised services sought from or provided by the Department of Health
Page 197 of 300
15
and Social Care);
iii) For the design, construction and maintenance of building and engineering works
(including construction and maintenance of grounds and gardens); and for disposals.
8.5.2 Health Care Services Where the Trust elects to invite tenders for the supply of healthcare services these
Standing Orders and Standing Financial Instructions shall apply as far as they are applicable to the tendering procedure and need to be read in conjunction with
Standing Financial Instructions 18 and 19.
8.5.3 Exceptions and instances where formal tendering need not be applied:
i) Formal tendering procedures need not be applied where:
a) the estimated expenditure or income does not, or is not reasonably expected to, exceed £30,000
b) where the supply is proposed under special arrangements negotiated by the Department of Health and Social Care, in which event the said special arrangements
must be complied with;
c) regarding disposals as set out in Standing Financial Instruction 25.
ii) Formal tendering procedures may be waived in the following circumstances:
a) in very exceptional circumstances where the Chief Executive decides that formal tendering procedures would not be practicable or the estimated expenditure or
income would not warrant formal tendering procedures, and the circumstances are detailed in an appropriate Trust record;
b) where the requirement is covered by an existing contract;
c) where Government Procurement Service and NHS Supply Chain agreements are in
place and have been approved by the Board. The Trust is expected to utilise regional or national frameworks where they are available;
d) where a consortium arrangement is in place and a lead organisation has been appointed to carry out tendering activity on behalf of the consortium members;
e) where the timescale genuinely precludes competitive tendering but failure to plan
the work properly would not be regarded as a justification for a single tender;
f) where specialist expertise is required and is available from only one source;
g) when the task is essential to complete the project, and arises as a consequence of a recently completed assignment and engaging different consultants for the new task
would be inappropriate;
h) there is a clear benefit to be gained from maintaining continuity with an earlier
project. However in such cases the benefits of such continuity must outweigh any potential financial advantage to be gained by competitive tendering;
i) for the provision of legal advice and services providing that any legal firm or
partnership commissioned by the Trust is regulated by the Law Society for England and Wales for the conduct of their business (or by the Bar Council for England and
Wales in relation to the obtaining of Counsel’s opinion) and are generally recognised as having sufficient expertise in the area of work for which they are commissioned.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 198 of 300
16
The Chief Financial Officer will ensure that any fees paid are reasonable and within commonly accepted rates for the costing of such work;
i) The waiving of competitive tendering procedures should not be used to avoid competition or for administrative convenience or to award further work to a
consultant originally appointed through a competitive procedure;
ii) Where it is decided that competitive tendering is not applicable and should be waived, the fact of the waiver and the reasons should be documented and recorded in an appropriate Trust record and reported to the Audit Committee at each meeting.
8.5.4 Fair and Adequate Competition
Where the exceptions set out in Standing Financial Instructions 17.1 and 17.5.3 apply, the Trust shall ensure that invitations to tender are sent to a sufficient number
of firms/individuals to provide fair and adequate competition as appropriate, and in no case less than two firms/individuals, having regard to their capacity to supply the goods or materials or to undertake the services or works required. To ensure
transparency, advertising should be considered for all procurements exceeding £10,000.
8.5.5 List of Approved Firms
The Trust shall ensure that the firms/individuals invited to tender (and where appropriate, quote) are among those on approved framework lists. Where a
framework does not exist refer to 8.5.1 and 8.5.3. Where in the opinion of the Chief Financial Officer it is desirable to seek tenders from firms not on the approved lists, the reason shall be recorded in writing to the Chief Executive (see Standing
Financial Instruction 8.6.8 List of Approved Firms).
8.5.6 Building and Engineering Construction Works It is not anticipated that the reasons for waiving formal tendering processes will apply
for building and engineering construction works and maintenance and so competitive tenders should be sought in every instance. Where the process has been waived for
such a project a specific report will be made to the Trust’s Audit Committee by the Chief Financial Officer detailing the reason for the waiver and providing assurance on compliance with EU and other procurement law.
8.5.7 Items which subsequently breach thresholds after original approval
Items estimated to be below the limits set in this Standing Financial Instruction for which formal tendering procedures are not used which subsequently prove to have a
value above such limits shall be reported to the Chief Executive, and be recorded in an appropriate Trust record.
8.6 Contracting/Tendering Procedure
8.6.1 Invitation to tender
i) All invitations to tender shall state the date and time as being the latest time for the receipt of tenders.
) All invitations to tender shall state that no tender will be accepted unless
Submitted via a secure electronic tendering system
iii) Every tender for goods, materials, services or disposals shall embody such of the NHS Standard Contract Conditions as are applicable.
iv) Every tender for building or engineering works (except for maintenance work, when
Estate Code guidance shall be followed) shall embody or be in the terms of the current edition of one of the Joint Contracts Tribunal Standard Forms of Building Contract or Department of the Environment (GC/Wks) Standard forms of contract
amended to comply with concode; or, when the content of the work is primarily
Page 199 of 300
17
engineering, the General Conditions of Contract recommended by the Institution of Mechanical and Electrical Engineers and the Association of Consulting Engineers (Form A), or (in the case of civil engineering work) the General Conditions of
Contract recommended by the Institute of Civil Engineers, the Association of Consulting Engineers and the Federation of Civil Engineering Contractors. These
documents shall be modified and/or amplified to accord with Department of Health and Social Care guidance and, in minor respects, to cover special features of
individual projects.
8.6.2 Receipt and safe custody of tenders
The Chief Executive or their nominated representative will be responsible for the receipt, endorsement and safe custody of tenders received until the time appointed
for their opening.
8.6.3 Opening tenders and Register of tenders
E-Tenders: Access to the E-Tender system is restricted to appropriate Trust
approved officers with password controlled access in accordance with Opening tenders and Register of tenders 8.6.3i.
Tender documents are uploaded into the secure portal, and a time and date for submitting documents is set which enables tenders to be submitted electronically at
the specified time.
It is not possible to access tender details prior to the system set specified date and time of opening. This preserves the security of unopened tenders.
A nominated officer from Procurement is selected to release documents on the specified return date or as soon as practical. Access is provided through secure
password access.
Once the tender submission closing date and time has elapsed access to the tender box is closed to suppliers. Suppliers cannot upload or alter documents after the closing time.
An audit report detailing the names and details of all documents is electronically
available upon request
In the event that both electronic and conventional tenders are returned at the designated time and of opening then the procedures set out above must be adhered to dependent on the return format. Tenders will be annotated on the opening record
to identify the tender return method.
Conventional tenders: as soon as practicable after the date and time stated as being the latest time for the receipt of tenders, they shall be opened by two senior officers/managers designated by the Chief Executive and not from the originating
department.
The rules relating to the opening of tenders will need to be read in conjunction with any delegated authority set out in the Trust’s Scheme of Delegation.
The ‘originating’ Department will be taken to mean the Department sponsoring or commissioning the tender.
The involvement of Finance Directorate staff in the preparation of a tender proposal
will not preclude the Chief Financial Officer or any approved Senior Manager from the Finance Directorate from serving as senior managers to open tenders.
All Executive Director “Members” of the Trust Board will be authorised to open tenders regardless of whether they are from the originating department provided that
the other authorised person opening the tenders with them is not from the originating
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 200 of 300
18
department. The Trust’s Company Secretary will count as a Director for the purposes of opening
tenders.
Every tender received shall be marked with the date of opening and initiated by those present at the opening.
An electronic activity log is maintained within the tendering system that provides information on:
a) the name of all firms individuals invited;
b) the names of firms individuals from which tenders have been received;
c) the date the tenders were opened;
d) the persons present at the opening;
e) the price shown on each tender;
f) Incomplete tenders, i.e. those from which information necessary for the adjudication
of the tender is missing, and amended tenders i.e., those amended by the tenderer upon their own initiative either orally or in writing after the due time for receipt, but
prior to the opening of other tenders, will only be considered in exceptional circumstances
8.6.4 Admissibility
i) If for any reason the designated officers are of the opinion that the tenders
received are not strictly competitive (for example, because their numbers are insufficient or any are amended, incomplete or qualified) no contract shall be
awarded without the approval of the Chief Executive.
ii) Where only one tender is sought and/or received, the Chief Executive and Chief Financial Officer shall, as far practicable, ensure that the price to be paid is fair and reasonable and will ensure value for money for the Trust.
8.6.5 Late tenders
The electronic tendering system does not permit the submission of late tenders
8.6.6 Acceptance of formal tenders (See overlap with Standing Financial Instruction 8.7)
i) Any discussions with a tenderer which are deemed necessary to clarify technical aspects of the tender before the award of a contract will not disqualify the tender.
ii) Tenders shall be awarded to the supplier that best meets the pre agreed evaluation
criteria and provides the most economically advantageous tender to the Trust. Such reasons shall be set out in either the contract file, or other appropriate record.
It is accepted that the lowest price does not always represent the best value for money. Other factors affecting the success of a project include:
a) experience and qualifications of team members;
b) understanding of client’s needs;
c) feasibility and credibility of proposed approach;
Page 201 of 300
19
d) ability to complete the project on time.
iii) Where other factors are taken into account in selecting a tenderer, these must be clearly recorded and documented in the contract file, and the reason(s) for not
accepting the lowest tender clearly stated.
iv) No tender shall be accepted which will commit expenditure in excess of that which
has been allocated by the Trust and which is not in accordance with these Instructions except with the authorisation of the Chief Executive.
v) The use of these procedures must demonstrate that the award of the contract was:
a) not in excess of the going market rate / price current at the time the contract was
awarded;
b) that best value for money was achieved.
vi) All tenders should be treated as confidential and should be retained for inspection.
8.6.7 Tender reports to the Trust Board
Reports to the Trust Board will be made on an exceptional circumstance basis only.
8.6.8 List of approved firms (see Standing Financial Instruction 8.5.5)
a) Firms included on the approved list of tenderers shall ensure that when engaging,
training, promoting or dismissing employees or in any conditions of employment, shall not discriminate against any person because of colour, race, ethnic or national origins, religion or sex, and will comply with the provisions of the Equal Pay Act
1970, the Sex Discrimination Act 1975, the Race Relations Act 1976, and the Disabled Persons (Employment) Act 1944 and any amending and/or related
legislation.
b) Firms shall conform at least with the requirements of the Health and Safety at Work Act and any amending and/or other related legislation concerned with the health,
safety and welfare of workers and other persons, and to any relevant British Standard Code of Practice issued by the British Standard Institution. Firms must provide to the appropriate manager a copy of its safety policy and evidence of the
safety of plant and equipment, when requested.
iii) Financial Standing and Technical Competence of Contractors
The Chief Financial Officer may make or institute any enquiries he/she deems appropriate concerning the financial standing and financial suitability of approved contractors. The Director with lead responsibility for clinical governance will similarly
make such enquiries as is felt appropriate to be satisfied as to their technical / medical competence.
8.6.9 Exceptions to using approved contractors
If in the opinion of the Chief Executive and the Chief Financial Officer or the Director with lead responsibility for clinical governance it is impractical to use a potential contractor from the framework list of approved firms/individuals (for example where
specialist services or skills are required and there are insufficient suitable potential contractors on the list), or where a list for whatever reason has not been prepared,
the Chief Executive should ensure that appropriate checks are carried out as to the technical and financial capability of those firms that are invited to tender or quote.
An appropriate record in the contract file should be made of the reasons for inviting a tender or quote other than from an approved list.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 202 of 300
20
8.7 Quotations: Competitive and non-competitive
8.7.1 General Position on quotations
Quotations are required where formal tendering procedures are not adopted and where the intended expenditure or income exceeds, or is reasonably expected to
exceed £10,000 but not exceed £29,999.1
8.7.2 Competitive Quotations
i) Quotations should be obtained from at least 3 firms/individuals based on specifications or terms of reference prepared by, or on behalf of, the Trust.
ii) Quotations should be in writing unless the Chief Executive or their nominated officer
determines that it is impractical to do so in which case quotations may be obtained by telephone. Confirmation of telephone quotations should be obtained as soon as possible and the reasons why the telephone quotation was obtained should be set
out in a permanent record.
iii) All quotations should be treated as confidential and should be retained for inspection.
iv) The Chief Executive or their nominated officer should evaluate the quotation and select the quote which gives the best value for money. If this is not the lowest
quotation if payment is to be made by the Trust, or the highest if payment is to be received by the Trust, then the choice made and the reasons why should be recorded in a permanent record.
8.7.3 Non-Competitive Quotations
Non-competitive quotations in writing may be obtained in the following circumstances:
i) The supply of proprietary or other goods of a special character and the rendering of services of a special character, for which it is not, in the opinion of the responsible
officer, possible or desirable to obtain competitive quotations;
ii) The supply of goods or manufactured articles of any kind which are required quickly and are not obtainable under existing contracts;
iii) Miscellaneous services, supplies and disposals;
iv) Where the goods or services are for building and engineering maintenance the
responsible works manager must certify that the first two conditions of this Standing Financial Instruction (i.e. (i) and (ii) apply).
8.7.4 Quotations to be within Financial Limits
No quotation shall be accepted which will commit expenditure in excess of that
which has been allocated by the Trust and which is not in accordance with Standing Financial Instructions except with the authorisation of either the Chief Executive or
Chief Financial Officer.
8.8 Authorisation of Tenders and Competitive Quotations
Providing all the conditions and circumstances set out in these Standing Financial Instructions have been fully complied with, formal authorisation and awarding of a
contract may be decided by the following staff to the values set out in the Trust’s Scheme of Delegation.
Formal authorisation must be put in writing. In the case of authorisation by the Trust
Board this shall be recorded in their minutes.
1 Limits changed, with effect from 1-Apr-13, at a board meeting held on 21-Mar-13
Page 203 of 300
21
8.9 Instances where formal competitive tendering or competitive quotation is not required
Where competitive tendering or a competitive quotation is not required the Trust should adopt one of the following alternatives:
i) where suitable products are available the Trust shall use either NHS Supply Chain,
Government Procurement Service or NHS Commercial Solutions for procurement of all goods and services unless the Chief Executive or nominated officers deem it
inappropriate. The decision to use alternative sources must be documented;
ii) If the Trust does not use the approved collaborative bodies - where tenders or
quotations are not required, because expenditure is below £10,0002, the Trust shall
procure goods and services in accordance with procurement procedures approved
by the Chief Financial Officer.
8.10 Private Finance for capital procurement (see overlap with Standing Financial Instruction 24)
The Trust should normally market-test for PFI (Private Finance Initiative funding) when considering a capital procurement. When the Board proposes, or is required, to use finance provided by the private sector the following should apply:
i) The Chief Executive shall demonstrate that the use of private finance represents
value for money and genuinely transfers risk to the private sector;
ii) Where the sum exceeds delegated limits, a business case must be referred to the appropriate Department of Health and Social Care for approval or treated as per current
guidelines;
iii) The proposal must be specifically agreed by the Board of the Trust;
iv) The selection of a contractor/finance company must be on the basis of competitive tendering or quotations.
8.11 Compliance requirements for all contracts
The Board may only enter into contracts on behalf of the Trust within the statutory powers delegated to it by the Secretary of State and shall comply with:
i) The Trust’s Standing Orders and Standing Financial Instructions;
ii) EU Directives, Public Contract Regulations 2015 and other statutory provisions;
iii) Any relevant directions including the Estate code and guidance on the Procurement and Management of Consultants;
iv) Such of the NHS Standard Contract Conditions as are applicable;
v) Contracts with Foundation Trusts must be in a form compliant with appropriate NHS
guidance;
vi) Where appropriate contracts shall be in or embody the same terms and conditions of contract as was the basis on which tenders or quotations were invited;
vii) In all contracts made by the Trust, the Board shall endeavour to obtain best value
for money by use of all systems in place. The Chief Executive shall nominate an
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 204 of 300

22
officer who shall oversee and manage each contract on behalf of the Trust.
8.12 Personnel and Agency or Temporary Staff Contracts
The Chief Executive shall nominate officers with delegated authority to enter into contracts of employment, regarding staff, agency staff or temporary staff service
contracts.
8.13 Healthcare Services Agreements (see overlap with Standing Financial Instruction 9 )
As a Foundation Trust and being a Public Benefit Corporation (PBC) Contracts with NHS providers for the supply of healthcare services Contracts are legal documents
and are enforceable in law. The Chief Executive shall nominate officers to commission Contracts with providers
of healthcare in line with a commissioning plan approved by the Board.
8.14 Disposals (See overlap with Standing Financial Instruction 17)
Competitive Tendering or Quotation procedures shall not apply to the disposal of:
i) any matter in respect of which a fair price can be obtained only by negotiation or
sale by auction as determined (or pre-determined in a reserve) by the Chief Executive or their nominated officer;
ii) obsolete or condemned articles and stores, which may be disposed of in accordance with the supplies policy of the Trust;
iii) items to be disposed of with an estimated sale value of less than £5,000, this figure to
be reviewed on a periodic basis;
iv) items arising from works of construction, demolition or site clearance, which should be dealt with in accordance with the relevant contract;
v) land or buildings concerning which Department of Health and Social Care guidance has
been issued but subject to compliance with such guidance.
8.15 In-house Services
8.15.1 The Chief Executive shall be responsible for ensuring that best value for money
can be demonstrated for all services provided on an in-house basis. The Trust may also determine from time to time that in- house services should be market tested by
competitive tendering.
8.15.2 In all cases where the Board determines that in-house services should be subject
to competitive tendering the following groups shall be set up:
i) Specification group, comprising the Chief Executive or nominated officer/s and specialist;
ii) In-house tender group, comprising a nominee of the Chief Executive and technical
support;
iii) Evaluation team, comprising normally a specialist officer, a supplies officer and a Chief Financial Officer representative. For services having a likely annual
expenditure exceeding £250,000, a Non-Executive Director should be a member of the evaluation team.
8.15.3 All groups should work independently of each other and individual officers may be a member of more than one group but no member of the in-house tender group may
participate in the evaluation of tenders.
Page 205 of 300
23
8.15.4 The evaluation team shall make recommendations to the Board in the form of a contract award recommendation report.
8.15.5 The Chief Executive shall nominate an officer to oversee and manage the contract
on behalf of the Trust.
8.16 Applicability of Standing Financial Instructions on Tendering and
Contracting to funds held in trust (see overlap with Standing Financial Instruction 29)
These Instructions shall not only apply to expenditure from Exchequer funds but
also to works, services and goods purchased from the Trust’s trust funds and private resources.
9. NHS CONTRACTS FOR PROVISION OF SERVICES (SEE OVERLAP WITH STANDING FINANCIAL INSTRUCTION 8.13)
9.1 Contracts
The Chief Executive, as the Accounting Officer, is responsible for ensuring the Trust
enters into suitable contracts with service commissioners for the provision of NHS services.
All contracts should aim to implement the agreed priorities contained within the Annual Operating Plan and wherever possible, be based upon integrated care
pathways to reflect expected patient experience. In discharging this responsibility, the Chief Executive should take into account:
i) the standards of service quality expected;
ii) the relevant national service framework (if any);
iii) the provision of reliable information on cost and volume of services;
iv) the NHS National Performance Assessment Framework;
v) that contracts build where appropriate on existing Joint Investment Plans;
vi) that contracts are based on integrated care pathways.
9.2 Involving Partners and jointly managing risk
A good contract will result from a dialogue of clinicians, users, carers, public health professionals and managers. it will reflect knowledge of local needs and inequalities. This will require the chief executive to ensure that the trust works with all partner
agencies involved in both the delivery and the commissioning of the service required. The contract will apportion responsibility for handling a particular risk to the
party or parties in the best position to influence the event and financial arrangements should reflect this. In this way the trust can jointly manage risk with all
interested parties.
9.3 Department of Health and Social Care Policies and Guidelines
The trust will need to ensure that contracts agreed with partner organisations reflect evolving NHS policies and guidance.
9.4 Reports to Board on commissioner contracts
The Chief Executive, as the Accounting Officer, will need to ensure that regular reports are provided to the board detailing actual and forecast income from the
commissioner contract. This will include information on costing arrangements, which increasingly should be based upon healthcare resource groups (HRGs). Where HRGs are unavailable for specific services, all parties should agree a common
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 206 of 300
24
currency for application across the range of contracts.
10. COMMISSIONING (Currently not applicable, however, this subject will be reviewed periodically).
11. PAY EXPENDITURE
11.1 Funded Establishment
11.1.1 The manpower plans incorporated within the annual budget will form the funded
establishment.
11.1.2 The funded establishment of any department may not be varied without the approval of the Chief Executive or nominated officers.
11.2 Staff Appointments
11.2.1 No officer or Member of the Trust Board or employee may engage, re-engage, or re-grade employees, either on a permanent or temporary nature, or hire agency
staff, or agree to changes in any aspect of remuneration:
i) unless authorised to do so by the Chief Executive;
ii) within the limit of their approved budget and funded establishment.
11.2.2 The Board will approve procedures presented by the Chief Executive for the determination of commencing pay rates, condition of service, etc., for employees.
11.3 Processing Payroll
11.3.1 The Chief Financial Officer Is responsible for:
i) specifying timetables for submission of properly authorised time records and other
notifications;
ii) the final determination of pay and allowances;
iii) making payment on agreed dates;
iv) agreeing method of payment.
11.3.2 The Chief Financial Officer will issue instructions regarding:
i) verification and documentation of data;
ii) the timetable for receipt and preparation of payroll data and the payment of
employees and allowances;
iii) maintenance of subsidiary records for superannuation, income tax, social security and other authorised deductions from pay;
iv) security and confidentiality of payroll information;
v) checks to be applied to completed payroll before and after payment;
vi) authority to release payroll data under the provisions of the Data Protection Act;
vii) methods of payment available to various categories of employee and officers;
Page 207 of 300
25
viii) procedures for payment by cheque, bank credit, or cash to employees and officers;
ix) procedures for the recall of cheques and bank credits;
x) pay advances and their recovery, including for any approved salary finance loan
schemes ;
xi) maintenance of regular and independent reconciliation of pay control accounts;
xii) separation of duties of preparing records and handling cash;
xiii) a system to ensure the recovery from those leaving the employment of the Trust of
sums of money and property due by them to the Trust.
11.3.3 Appropriately nominated managers have delegated responsibility for:
i) submitting time records, and other notifications in accordance with agreed timetables;
ii) completing time records and other notifications in accordance with the Chief
Financial Officer’s instructions and in the form prescribed by the Chief Financial Officer;
iii) submitting termination forms in the prescribed form immediately upon knowing the effective date of an employee's or officer’s resignation, termination or retirement.
Where an employee fails to report for duty or to fulfill obligations in circumstances that suggest they have left without notice, the Chief Financial Officer must be informed immediately.
11.3.4 Regardless of the arrangements for providing the payroll service, the Chief Financial Officer shall ensure that the chosen method is supported by appropriate
(contracted) terms and conditions, adequate internal controls and audit review procedures and that suitable arrangements are made for the collection of payroll
deductions and payment of these to appropriate bodies.
11.4 Contracts of Employment
The Board shall delegate responsibility to an officer for:
i) ensuring that all employees are issued with a Contract of Employment in a form approved by the Board and which complies with employment legislation;
ii) dealing with variations to, or termination of, contracts of employment.
12. NON-PAY EXPENDITURE
12.1 Delegation of Authority
12.1.1 The Board will approve the level of non-pay expenditure on an annual basis and
the Chief Executive will determine the level of delegation to budget managers.
12.1.2 The Chief Executive will set out:
i) the list of managers who are authorised to place requisitions for the supply of goods
and services;
ii) the maximum level of each requisition and the system for authorisation above that level.
12.1.3 The Chief Executive shall set out procedures on the seeking of professional
advice regarding the supply of goods and services.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 208 of 300
26
12.2 Choice, Requisitioning, Ordering, Receipt and Payment for Goods and
Services (see overlap with Standing Financial Instruction No. 8).
12.2.1 Requisitioning
The requisitioner, in choosing the item to be supplied (or the service to be performed) shall always obtain the best value for money for the Trust. In so doing,
the advice of the Trust’s adviser on supply shall be sought. Where this advice is not acceptable to the requisitioner, the Chief Financial Officer (and/or the Chief
Executive) shall be consulted.
12.2.2 System of Payment and Payment Verification The Chief Financial Officer shall be responsible for the prompt payment of accounts
and claims. Payment of contract invoices shall be in accordance with contract terms, or otherwise, in accordance with national guidance.
12.2.3 The Chief Financial Officer will:
i) advise the Board regarding the setting of thresholds above which quotations (competitive or otherwise) or formal tenders must be obtained; and, once approved,
the thresholds should be incorporated in Standing Orders and Standing Financial Instructions and regularly reviewed;
ii) prepare procedural instructions or guidance within the Scheme of Delegation on the
obtaining of goods, works and services incorporating the thresholds;
iii) be responsible for the prompt payment of all properly authorised accounts and
claims;
iv) Be responsible for designing and maintaining a system of verification, recording and payment of all amounts payable. The system shall provide for a:
a) list of Trust employees (including specimens of their signatures) authorised to
certify invoices;
b) certification that:
- goods have been duly received, examined and are in accordance with specification and the prices are correct;
- work done or services rendered have been satisfactorily carried out in accordance
with the order, and, where applicable, the materials used are of the requisite standard and the charges are correct;
- in the case of contracts based on the measurement of time, materials or expenses,
the time charged is in accordance with the time sheets, the rates of labour are in accordance with the appropriate rates, the materials have been checked as regards quantity, quality, and price and the charges for the use of vehicles, plant and
machinery have been examined;
- where appropriate, the expenditure is in accordance with regulations and all necessary authorisations have been obtained;
- the account is arithmetically correct;
- the account is in order for payment.
c) a timetable and system for submission to the Chief Financial Officer of accounts for
payment; provision shall be made for the early submission of accounts subject to
Page 209 of 300
27
cash discounts or otherwise requiring early payment;
d) instructions to employees regarding the handling and payment of accounts within
the Finance Department.
v) be responsible for ensuring that payment for goods and services is only made once the goods and services are received. The only exceptions are set out in Standing
Financial Instruction 21.2.4 below.
12.2.4 Prepayments Prepayments are only permitted where exceptional circumstances apply. In such
instances:
i) prepayments are only permitted where the financial advantages outweigh the disadvantages (i.e. cash flows must be discounted to NPV using the National Loans
Fund (NLF) rate plus 2%);
ii) the appropriate officer must provide, in the form of a written report, a case setting
out all relevant circumstances of the purchase. The report must set out the effects on the Trust if the supplier is at some time during the course of the prepayment
agreement unable to meet their commitments;
iii) the Chief Financial Officer will need to be satisfied with the proposed arrangements before contractual arrangements proceed (taking into account the EU public
procurement rules where the contract is above a stipulated financial threshold);
iv) the budget holder is responsible for ensuring that all items due under a prepayment
contract are received and they must immediately inform the appropriate Director or Chief Executive if problems are encountered.
12.2.5 Official orders
Official Orders must:
i) be consecutively numbered;
ii) be in a form approved by the Chief Financial Officer;
iii) state the Trust’s terms and conditions of trade;
iv) only be issued to, and used by, those duly authorised by the Chief Executive.
12.2.6 Duties of Managers and Officers Managers and officers must ensure that they comply fully with the guidance and
limits specified by the Chief Financial Officer and that:
i) all contracts (except as otherwise provided for in the Scheme of Delegation), leases,
tenancy agreements and other commitments which may result in a liability are notified to the Chief Financial Officer in advance of any commitment being made;
ii) contracts above specified thresholds are advertised and awarded in accordance
with EU rules on public procurement;
iii) where consultancy advice is being obtained, the procurement of such advice must be in accordance with guidance issued by the Department of Health and Social Care;
iv) no order shall be issued for any item or items to any firm which has made an offer of
gifts, reward or benefit to directors or employees, other than:
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 210 of 300
28
a) isolated gifts of a trivial character or inexpensive seasonal gifts, such as calendars;
and
b) conventional hospitality, such as lunches in the course of working visits.
(This provision needs to be read in conjunction with Standing Order No. 6 and
the principles outlined in the national guidance contained in HSG 93(5) “Standards of Business Conduct for NHS Staff”)
v) no requisition/order is placed for any item or items for which there is no budget
provision unless authorised by the Chief Financial Officer on behalf of the Chief Executive;
vi) all goods, services, or works are ordered on an official order except works and
services executed in accordance with a contract and purchases from petty cash;
vii) verbal orders must only be issued very exceptionally - by an employee designated
by the Chief Executive and only in cases of emergency or urgent necessity. These must be confirmed by an official order and clearly marked "Confirmation Order";
viii) orders are not split or otherwise placed in a manner devised so as to avoid the
financial thresholds;
ix) goods are not taken on trial or loan in circumstances that could commit the Trust to a future uncompetitive purchase;
x) changes to the list of employees and officers authorised to certify invoices are
notified to the Chief Financial Officer;
xi) purchases from petty cash are restricted in value and by type of purchase in
accordance with instructions issued by the Chief Financial Officer;
xii) petty cash records are maintained in a form as determined by the Chief Financial Officer.
12.2.7 The Chief Executive and Chief Financial Officer shall ensure that the arrangements
for financial control and financial audit of building and engineering contracts and property transactions comply with the guidance contained within CONCODE and
ESTATECODE. The technical audit of these contracts shall be the responsibility of the relevant Director.
12.3 Joint Finance Arrangements with Local Authorities and Voluntary Bodies
(see overlap with Standing Order 9.1) Payments to local authorities and voluntary organisations made under the powers of
section 28A of the NHS Act shall comply with procedures laid down by the Chief Financial Officer which shall be in accordance with these Acts. (See overlap with
Standing Order No. 9.1)
13. EXTERNAL BORROWING 13.1.1 The Chief Financial Officer shall prepare procedural instructions on the operation of
all Commercial Bank accounts, Investments accounts and the Office of the
Paymaster General account for the approval by the Executive Committee.
13.1.2 The Chief Financial Officer is responsible for managing the Trust’s banking
arrangements and for advising the Trust on the provision of banking services and operation of accounts. This advice will take into account guidance/directions
issued by the Regulator.
Page 211 of 300
29
13.1.3 The Board will agree the list of employees (including specimens of their
signatures) who are authorised to make short term borrowings on behalf of the Trust. This must contain the Chief Executive and the Chief Financial Officer.
13.1.4 The Chief Financial Officer must prepare detailed procedural instructions concerning applications for loans and overdrafts.
13.1.5 All short-term borrowings should be kept to the minimum period of time possible,
consistent with the overall cash flow position, represent good value for money, and comply with the Trust’s Treasury Management Policy.
13.1.6 Any short-term borrowing must be with the authority of two members of an
authorised panel, one of which must be the Chief Executive or the Chief Financial Officer. The Board must be made aware of all short term borrowings at the next
Board meeting.
13.1.7 All long-term borrowing must be consistent with the plans outlined in the current
Annual Operating Plan and be approved by the Trust Board.
13.1.8 Assets protected under the Terms of Authorisation shall not be used or allocated for borrowing non-protected assets will be eligible as security for loans.
13.1.9 The Board shall approve the Trust’s overdraft facility provider, if applicable..
13.1.10 All short term borrowings must be kept to the minimum period of time consistent
with the overall cash flow position, represent good value for money, comply with the Trust’s Treasury Management Policy and all guidance issued by NHSI.
13.1.11 The Trust’s overdraft facility may only be used with the pre-approval of the Chief
Financial Officer and approval of the Board.
13.1.12 Long term borrowings will only be used to finance longer term Capital or
Investment Programmes
13.1.13 Long term borrowings in respect of strategic Capital Projects shall be formally approved by the Board.
13.2 INVESTMENTS
13.2.1 Temporary cash surpluses must be held only in such public or private sector investments as notified by the Secretary of State and authorised by the Board.
13.2.2 The Chief Financial Officers responsible for advising the Board on investments
and shall report periodically to the Board concerning the performance of investments held.
13.2.3 The Chief Financial Officer will prepare detailed procedural instructions on the
operation of investment accounts and on the records to be maintained.
14. FINANCIAL FRAMEWORK [Not Applicable but section from model SFIs left in form completeness.]
15. CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET
REGISTERS AND SECURITY OF ASSETS
15.1 Capital Investment
15.1.1 The Chief Executive:
i) shall ensure that there is an adequate appraisal and approval process in place for
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 212 of 300
30
determining capital expenditure priorities and the effect of each proposal upon business plans;
ii) is responsible for the management of all stages of capital schemes and for ensuring that schemes are delivered on time and to cost;
iii) shall ensure that the capital investment is not undertaken without confirmation of
purchaser(s) support and the availability of resources to finance all revenue consequences, including capital charges.
15.1.2 For every capital expenditure proposal the Chief Executive shall ensure:
i) that a business case is produced setting out:
a) an option appraisal of potential benefits compared with known costs to determine
the option with the highest ratio of benefits to costs;
b) the involvement of appropriate Trust personnel and external agencies;
c) appropriate project management and control arrangements.
ii) that the Chief Financial Officer has certified professionally to the costs and revenue
consequences detailed in the business case.
15.1.3 For capital schemes where the contracts stipulate stage payments, the Chief Executive will issue procedures for their management, incorporating the
recommendations of “Estate code”.
15.1.4 The Chief Financial Officer shall assess on an annual basis the requirement for the operation of the construction industry tax deduction scheme in accordance with
Inland Revenue guidance.
15.1.5 The Chief Financial Officer shall issue procedures for the regular reporting of expenditure and commitment against authorised expenditure.
15.1.6 The approval of a capital programme shall not constitute approval for expenditure
on any scheme. The Chief Executive shall issue to the manager responsible for any scheme:
i) specific authority to commit expenditure;
ii) authority to proceed to tender (see overlap with Standing Financial Instruction 8.6);
iii) approval to accept a successful tender (see overlap with Standing Financial
Instruction 17.6).
The Chief Executive will issue a scheme of delegation for capital investment management in accordance with "Estate code" guidance and the Trust’s Standing
Orders.
15.1.7 The Chief Financial Officer shall issue procedures governing the financial
management, including variations to contract, of capital investment projects and valuation for accounting purposes. These procedures shall fully take into account
the delegated limits for capital schemes included in Annex C of HSC (1999) 246.
15.2 Private Finance (see overlap with Standing Financial Instruction 8.10)
The Trust should normally test for Private Finance Initiative when considering
capital procurement. When the Trust proposes to use finance which is to be provided other than through its Allocations, the following procedures shall apply:
Page 213 of 300

31
i) the Chief Financial Officer shall demonstrate that the use of private finance represents value for money and genuinely transfers significant risk to the private
sector;
ii) where the sum involved exceeds delegated limits, the business case must be referred
to the Department of Health and Social Care or in line with any current guidelines;
iii) the proposal must be specifically agreed by the Board.
15.3 Asset Registers
15.3.1 The Chief Executive is responsible for the maintenance of registers of assets,
taking account of the advice of the Chief Financial Officer concerning the form of any register and the method of updating, and arranging for a physical check of
assets against the asset register to be conducted once a year.
15.3.2 The Trust shall maintain an asset register recording fixed assets. The minimum data set to be held within these registers shall be as specified in the Manual for
Accounts as issued by the Department of Health and Social Care.
15.3.3 Additions to the fixed asset register must be clearly identified to an appropriate
budget holder and be validated by reference to:
i) properly authorised and approved agreements, architect's certificates, supplier's invoices and other documentary evidence in respect of purchases from third parties;
ii) stores, requisitions and wages records for own materials and labour including
appropriate overheads;
iii) lease agreements in respect of assets held under a finance lease and capitalised.
15.3.4 Where fixed assets are sold, scrapped, lost or otherwise disposed of, their value must be removed from the accounting records and each disposal must be
validated by reference to authorisation documents and invoices (where appropriate).
15.3.5 The Chief Financial Officer shall approve procedures for reconciling balances on
fixed assets accounts in ledgers against balances on fixed asset registers.
15.3.6 The value of each asset shall be indexed or revalued to current values in
accordance with methods specified in the Group Accounting Manual issued by the Department of Health and Social Care.
15.3.7 The value of each asset shall be depreciated using methods and rates as
specified in the Group Accounting Manual issued by the Department of Health and Social Care.
15.3.8 The Chief Financial Officer of the Trust shall calculate and pay PDC dividend
charges as specified in the Group Accounting Manual issued by the Department of Health and Social Care.
15.4 Security of Assets
15.4.1 The overall control of fixed assets is the responsibility of the Chief Executive.
15.4.2 Asset control procedures (including fixed assets, cash, cheques and negotiable
instruments, and also including donated assets) must be approved by the Chief Financial Officer. This procedure shall make provision for:
i) recording managerial responsibility for each asset;
ii) identification of additions and disposals;
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 214 of 300

32
iii) identification of all repairs and maintenance expenses;
iv) physical security of assets;
v) periodic verification of the existence of, condition of, and title to, assets recorded;
vi) identification and reporting of all costs associated with the retention of an asset;
vii) reporting, recording and safekeeping of cash, cheques, and negotiable instruments.
15.4.3 All discrepancies revealed by verification of physical assets to fixed asset register
shall be notified to the Chief Financial Officer.
15.4.4 Whilst each employee and officer has a responsibility for the security of property
of the Trust, it is the responsibility of Board members and senior employees in all disciplines to apply such appropriate routine security practices in relation to NHS
property as may be determined by the Board. Any breach of agreed security practices must be reported in accordance with agreed procedures.
15.4.5 Any damage to the Trust’s premises, vehicles and equipment, or any loss of
equipment, stores or supplies must be reported by Board members and employees in accordance with the procedure for reporting losses.
15.4.6 Where practical, assets should be marked as Trust property.
16. STORES AND RECEIPT OF GOODS
16.1 General position
Stores, defined in terms of controlled stores and departmental stores (for immediate use) should be:
i) kept to a minimum;
ii) subjected to annual stock take;
iii) valued in accordance with the Trust’s agreed accounting policies.
16.2 Control of Stores, Stocktaking, condemnations and disposal
16.2.1 Subject to the responsibility of the Chief Financial Officer for the systems of control, overall responsibility for the control of stores shall be delegated to an employee by
the Chief Executive. The day-to-day responsibility may be delegated by them to departmental employees and stores managers/keepers, subject to such delegation
being entered in a record available to the Chief Financial Officer. The control of any Pharmaceutical stocks shall be the responsibility of a designated Pharmaceutical
Officer; the control of any fuel oil and coal of a designated estates manager.
16.2.2 The responsibility for security arrangements and the custody of keys for any
stores and locations shall be clearly defined in writing by the designated manager/Pharmaceutical Officer. Wherever practicable, stocks should be marked
as health service property.
16.2.3 The Chief Financial Officer shall set out procedures and systems to regulate the stores including records for receipt of goods, issues, and returns to stores, and
losses.
16.2.4 Stocktaking arrangements shall be agreed with the Chief Financial Officer and
there shall be a physical check covering all items in store at least once a year.
Page 215 of 300
33
16.2.5 Where a complete system of stores control is not justified, alternative arrangements shall require the approval of the Chief Financial Officer.
16.2.6 The designated Manager/Pharmaceutical Officer shall be responsible for a system
approved by the Chief Financial Officer for a review of slow moving and obsolete items and for condemnation, disposal, and replacement of all unserviceable articles. The designated Officer shall report to the Chief Financial Officer any
evidence of significant overstocking and of any negligence or malpractice (see also overlap with SFI No. 17 Disposals and Condemnations, Losses and Special
Payments. Procedures for the disposal of obsolete stock shall follow the procedures set out for disposal of all surplus and obsolete goods.
16.3 Goods supplied by NHS Supply Chain
For goods supplied via the NHS Supply Chain central warehouses, the Chief Executive shall identify those authorised to requisition and accept goods from the
store. The authorised person shall check receipt against the delivery note before forwarding this to the Chief Financial Officer who shall satisfy themselves that the
goods have been received before accepting the recharge.
17. DISPOSALS AND CONDEMNATIONS, LOSSES AND SPECIAL
PAYMENTS
17.1 Disposals and Condemnations
17.1.1 Procedures
The Chief Financial Officer must prepare detailed procedures for the disposal of
assets including condemnations, and ensure that these are notified to managers.
17.1.2 When it is decided to dispose of a Trust asset, the Head of Department or authorised deputy will determine and advise the Chief Financial Officer of the
estimated market value of the item, taking account of professional advice where appropriate.
17.1.3 All unserviceable articles shall be: i) condemned or otherwise disposed of by an employee authorised for that purpose by
the Chief Financial Officer;
ii) recorded by the Condemning Officer in a form approved by the Chief Financial Officer which will indicate whether the articles are to be converted, destroyed or
otherwise disposed of. All entries shall be confirmed by the countersignature of a second employee authorised for the purpose by the Chief Financial Officer.
17.1.4 The Condemning Officer shall satisfy themselves as to whether or not there is evidence of negligence in use and shall report any such evidence to the Chief
Financial Officer who will take the appropriate action.
17.2 Losses and Special Payments
17.2.1 Procedures
The Chief Financial Officer must prepare procedural instructions on the recording of and accounting for condemnations, losses, and special payments.
17.2.2 Any employee or officer discovering or suspecting a loss of any kind must either immediately inform their head of department, who must immediately inform the
Chief Executive and the Chief Financial Officer or inform an officer charged with responsibility for responding to concerns involving loss. This officer will then
appropriately inform the Chief Financial Officer and/or Chief Executive. Where a criminal offence is suspected, the Chief Financial Officer must immediately inform
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 216 of 300
34
the police if theft or arson is involved. In cases of fraud and corruption or of anomalies which may indicate fraud or corruption, the Chief Financial Officer must inform the relevant Counter Fraud Specialist in accordance with Secretary of State
for Health and Social Care’s Directions.
The Chief Financial Officer must notify the Counter Fraud Specialist of all frauds.
17.2.3 For losses apparently caused by theft, arson, neglect of duty or gross carelessness, except if trivial, the Chief Financial Officer Chief Financial Officer
must immediately notify:
i) the Board;
ii) the External Auditor.
iii) the LCFS.
17.2.4 The Resources Committee shall approve the writing-off of any losses which are
above the thresholds set out in the detailed scheme of delegation.
17.2.5 The Chief Financial Officer shall be authorised to take any necessary steps to safeguard the Trust’s interests in bankruptcies and company liquidations.
17.2.6 For any loss, the Chief Financial Officer should consider whether any insurance
claim can be made.
17.2.7 The Chief Financial Officer shall maintain a Losses and Special Payments Register in which write-off action is recorded.
17.2.8 All losses and special payments must be reported to the Audit Committee.
18. INFORMATION TECHNOLOGY
18.1 Responsibilities and duties of the Chief Digital and Technology Officer
18.1.1 The Chief Digital and Technology Officer, who is responsible for the accuracy and security of the computerised financial data of the Trust, shall:
i) devise and implement any necessary procedures to ensure adequate (reasonable)
protection of the Trust’s data, programs and computer hardware for which the Director is responsible from accidental or intentional disclosure to unauthorised
persons, deletion or modification, theft or damage, having due regard for the Data Protection Act 1998;
ii) ensure that adequate (reasonable) controls exist over data entry, processing,
storage, transmission and output to ensure security, privacy, accuracy, completeness, and timeliness of the data, as well as the efficient and effective operation of the system;
iii) ensure that adequate controls exist such that the computer operation is separated
from development, maintenance and amendment;
iv) ensure that an adequate management (audit) trail exists through the computerised system and that such computer audit reviews as the Director may consider
necessary are being carried out.
Page 217 of 300
35
18.1.2 The Chief Digital and Technology Officer shall need to ensure that new financial systems and amendments to current financial systems are developed in a
controlled manner and thoroughly tested prior to implementation. Where this is undertaken by another organisation, assurances of adequacy must be obtained from them prior to implementation.
18.1.3 The Trust shall publish and maintain a Freedom of Information (FOI) Publication
Scheme, or adopt a model Publication Scheme approved by the Information Commissioner. A Publication Scheme is a complete guide to the information
routinely published by a public authority. It describes the classes or types of information about our Trust that we make publicly available.
18.2 Responsibilities and duties of other Directors and Officers in relation to
computer systems of a general application
In the case of computer systems which are proposed General Applications (i.e. normally those applications which the majority of Trust’s in the Region wish to
sponsor jointly) all responsible directors and employees will send to the Chief Digital and Technology Officer:
i) details of the outline design of the system;
ii) in the case of packages acquired either from a commercial organisation, from the
NHS, or from another public sector organisation, the operational requirement.
18.3 Contracts for Computer Services with other health bodies or outside
agencies
The Chief Digital and Technology Officer shall ensure that contracts for computer
services for financial applications with another health organisation or any other agency shall clearly define the responsibility of all parties for the security, privacy,
accuracy completeness, and timeliness of data during processing, transmission and storage. The contract should also ensure rights of access for audit purposes.
Where another health organisation or any other agency provides a computer service for financial applications, the Chief Digital and Technology Officer shall
periodically seek assurances that adequate controls are in operation.
18.4 Risk Assessment
The Chief Digital and Technology Officer shall ensure that risks to the Trust arising
from the use of IT are effectively identified and considered and appropriate action taken to mitigate or control risk. This shall include the preparation and testing of
appropriate disaster recovery plans.
18.5 Requirements for Computer Systems which have an impact on corporate
financial systems
Where computer systems have an impact on corporate financial systems the Chief
Financial Officer shall need to be satisfied that:
i) systems acquisition, development and maintenance are in line with corporate policies such as an Information Technology Strategy;
ii) data produced for use with financial systems is adequate, accurate, complete and
timely, and that a management (audit) trail exists;
iii) Chief Financial Officer staff have access to such data;
iv) Such computer audit reviews as are considered necessary are being carried out.
19. PATIENTS' PROPERTY
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 218 of 300
36
19.1 Safe Custody
The Trust has a responsibility to provide safe custody for money and other
personal property (hereafter referred to as "property") handed in by patients, in the possession of unconscious or confused patients, or found in the possession of patients dying in hospital or dead on arrival.
19.2 Informed Before or at Admission
The Chief Executive is responsible for ensuring that patients or their guardians, as appropriate, are informed before or at admission by:
i) notices and information booklets; (notices are subject to sensitivity guidance);
ii) hospital admission documentation and property records;
iii) The oral advice of administrative and nursing staff responsible for admissions, that
the Trust will not accept responsibility or liability for patients' property brought into Health Service premises, unless it is handed in for safe custody and a copy of an official patients' property record is obtained as a receipt.
19.3 Written Instructions
The Chief Financial Officer must provide detailed written instructions on the collection, custody, investment, recording, safekeeping, and disposal of
patients' property (including instructions on the disposal of the property of deceased patients and of patients transferred to other premises) for all staff
whose duty is to administer, in any way, the property of patients. Due care should be exercised in the management of a patient's money in order to maximise the benefits to the patient.
19.4 Opening of Separate Accounts for Patients' Moneys
Where Department of Health and Social Care instructions require the opening of separate accounts for patients' moneys, these shall be opened and operated
under arrangements agreed by the Chief Financial Officer.
19.5 When Probate or Letters of Administration are required
In all cases where property of a deceased patient is of a total value in excess of
£5,000 (or such other amount as may be prescribed by any amendment to the Administration of Estates, Small Payments, Act 1965), the production of Probate or Letters of Administration shall be required before any of the property
is released. Where the total value of property is £5,000 or less, forms of indemnity shall be obtained.
19.6 Staff Responsibilities and Duties
Staff should be informed, on appointment, by the appropriate service or senior manager of their responsibilities and duties for the administration of the property of patients.
19.7 Safekeeping for Specific Purposes
Where patients' property or income is received for specific purposes and held for safekeeping the property or income shall be used only for that purpose,
unless any variation is approved by the donor or patient in writing.
20. FUNDS HELD ON TRUST
20.1 Corporate Trustee
20.1.1 Standing Orders outline the Board’s responsibilities as a corporate trustee for the management of funds it holds on trust, along with Standing Financial Instruction
20.2 that defines the need for compliance with Charities Commission latest guidance and best practice.
Page 219 of 300
37
20.1.2 The discharge of the Board’s corporate trustee responsibilities are distinct from its responsibilities for exchequer funds and may not necessarily be discharged in
the same manner, but there must still be adherence to the overriding general principles of financial regularity, prudence and propriety. Trustee responsibilities cover both charitable and non-charitable purposes.
20.1.3 The Chief Financial Officer shall ensure that each trust fund which the Trust is
responsible for managing is managed appropriately with regard to its purpose and to its requirements.
20.2 Accountability to Charity Commission and Secretary of State for Health
and Social Care
20.2.1 The trustee responsibilities must be discharged separately and full recognition
given to the Board’s dual accountabilities to the Charity Commission for charitable funds held on trust and to the Secretary of State for all funds held on trust.
20.2.2 The Schedule of Matters Reserved to the Board and the Scheme of Delegation make clear where decisions regarding the exercise of discretion regarding the
disposal and use of the funds are to be taken and by whom. All Trust Board members and Trust officers must take account of that guidance before taking
action.
20.3 Applicability of Standing Financial Instructions to funds held on Trust
20.3.1 In so far as it is possible to do so, most of the sections of these Standing Financial
Instructions will apply to the management of funds held on trust. (See overlap with Standing Financial Instruction 17.16).
20.3.2 The over-riding principle is that the integrity of each Trust must be maintained and
statutory and Trust obligations met. Materiality must be assessed separately from Exchequer activities and funds.
21. ACCEPTANCE OF GIFTS BY STAFF AND LINK TO STANDARDS OF BUSINESS CONDUCT
21.1.1 The Chief Financial Officer shall ensure that all staff are made aware of the Trust
policy on acceptance of gifts and other benefits in kind by staff. This policy follows the guidance contained in the Department of Health and Social Care circular HSG
(93) 5 ‘Standards of Business Conduct for NHS Staff’ and is also deemed to be an integral part of these Standing Orders and Standing Financial Instructions (see overlap with Standing Order 6).
22. PAYMENTS TO INDEPENDENT CONTRACTORS Not applicable to NHS Trusts.
23. RETENTION OF RECORDS 23.1 The Chief Executive shall be responsible for maintaining archives for all
records required to be retained in accordance with Department of Health and Social Care guidelines.
23.2 The records held in archives shall be capable of retrieval by authorised
persons.
23.3 Records held in accordance with latest Department of Health and Social Care guidance shall only be destroyed at the express instigation of the Chief
Executive. Detail shall be maintained of records so destroyed.
24. RISK MANAGEMENT AND INSURANCE
24.1 Programme of Risk Management
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 220 of 300
38
The Chief Executive shall ensure that the Trust has a programme of risk management, in accordance with current Department of Health and Social Care assurance framework requirements, which must be approved and monitored by the
Board.
The programme of risk management shall include:
i) a process for identifying and quantifying risks and potential liabilities;
ii) engendering among all levels of staff a positive attitude towards the control of risk;
iii) management processes to ensure all significant risks and potential liabilities are addressed including effective systems of internal control, cost effective insurance
cover, and decisions on the acceptable level of retained risk;
iv) contingency plans to offset the impact of adverse events;
v) audit arrangements including; internal audit, clinical audit, health and safety review;
vi) a clear indication of which risks shall be insured;
vii) arrangements to review the Risk Management programme.
The existence, integration and evaluation of the above elements will assist in
providing a basis to make an Annual Governance Statement within the Annual Report and Accounts as required by current Department of Health and Social Care
guidance. The Board shall decide if the Trust will insure through the risk pooling schemes
administered by NHS Resolution or self-insure for some or all of the risks covered by the risk pooling schemes. If the Board decides not to use the risk pooling schemes
for any of the risk areas (clinical, property and employers/third party liability) covered by the scheme this decision shall be reviewed annually.
24.2 Insurance arrangements with commercial insurers
The Chief Financial Officer shall ensure that other insurance arrangements exist as appropriate.
Page 221 of 300
39
STANDING ORDERS FOR THE BOARD OF DIRECTORS
Author(s)
Trust Secretary
Version
2020
Version Date
October 2020
Implementation/approval Date
Review Date
October 2022 (or sooner if legislative and/or regulatory/best practice governance changes require this)
Review Body
Audit Committee (but requiring Board approval)
APPENDIX 1
1
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 222 of 300
40
i. INTRODUCTION
1. The Trust’s Standing Orders have been compiled in accordance with the requirements and provisions of the NHS and Community Care Act 1990, Health and Social Care (Community Health and Standard) Act 2003, the National Health Service Act 2006 (the 2006 Act), the Health and Social Care Act 2008 (the 2008 Act), the Health Act 2009 (the 2009 Act), and the Health and Social Care Act 2012 (the 2012 Act).
2. Failure to comply with Standing Orders and Standing Financial Instructions is a disciplinary matter which could result in dismissal.
ii. STANDING ORDERS
1. Standing Orders set out the composition and responsibilities of the Board of Directors and the code of conduct to which its members must comply. They also set out how Board business should be conducted and contain the Trust’s rules in relation to procurement.
2. A number of decisions in relation to the operation and management of the Trust
are reserved for the Board of Directors (the Board), and the Scheme of Delegation (as referred to in Standing Orders) sets out what these are. It is important that all staff are aware of and comply with Standing Orders, Standing Financial Instructions and the Scheme of Delegation at all times.
3. The Trust shall deal with its regulator, NHS Improvement, in an open and co-operative manner and shall promptly notify NHS Improvement of anything relating to the Trust of which NHS Improvement would reasonably expect prompt notice, including, without prejudice to the foregoing generality, any anticipated failure or anticipated prospect of failure on the part of the Trust to meet its obligations under its Licence, or any financial, performance, governance and/or quality thresholds which NHS Improvement may specify from time to time.
4. The Chair, Chief Executive, or any other authorised person giving information to the public on behalf of the Trust, shall ensure that they follow the principles set out by the Committee on Standards in Public Life and that they adhere to the principles set out within the Independent Commission’s Good Governance Standard for Public Service. They must also ensure that they adhere to the current version of the NHS Foundation Trust Code of Governance as revised and issued by NHS Improvement from time to time.
2
Page 223 of 300
41
CONTENTS
SECTION A – INTERPRETATION AND DEFINITIONS FOR STANDING ORDERS AND STANDING FINANCIAL INSTRUCTIONS
SECTION B – STANDING ORDERS
Page 6
8
1.
1.1 1.2 1.3
INTRODUCTION
Statutory Framework NHS Regulatory Framework Delegation of Powers
6 6 9
2.
2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8
THE BOARD OF DIRECTORS: COMPOSITION OF
MEMBERSHIP, TENURE AND ROLE OF MEMBERS Composition of the Board of Directors Tenure of Office Disqualification as a Director Executive Directors Corporate Role of the Board and Responsibilities Schedule of Matters Reserved to the Board and Scheme of Delegation Lead Roles for Board Members Senior Independent Director
9
9 11 12 13 13 14 14 14
3.
3.1 3.2 3.3 3.4 3.5 3.6 3.7 3.8
MEETINGS OF THE BOARD OF DIRECTORS Calling Meetings Notice of Meetings and the business to be transacted Agenda and Supporting Papers Admissibility of Papers Petitions Notice of Motion Emergency Motions Motions: Procedure at and during a meeting
14
14 15 15 15 16 16 16 16
3.9 3.10 3.11
3.12 3.13 3.14 3.15 3.16 3.17 3.18 3.19 3.20 3.21
Motion to Rescind a Resolution Chair of meeting Chair’s ruling
Quorum Voting Suspension of Standing Orders Variation and amendment of Standing Orders Record of Attendance Minutes Interest of Directors in Contracts and Other Matters on account of pecuniary interests Failure to Declare an Interest Admission of Public and Press Observers at Trust meetings
18 18 19
19 19 20 20 20 21 21
21 22 23
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 224 of 300
42
4.
4.1 4.2 4.3 4.4 4.5 4.6 4.7 4.8
APPOINTMENT OF COMMITTEES AND SUB-COMMITTEES Appointment of Committees Confidential Proceedings Applicability of Standing Orders and Standing Financial Instructions to Committees Terms of Reference Delegation of Powers by Committees to Sub-Committees Approval of Appointments to Committees Appointments for Statutory functions Committees to be established by the Board:
Audit Committee Nominations and Remuneration Committee Charitable Funds Committee Other Committees
23
23 24 24 24 24 24 25 25 25
25 26 26
5.
5.1 5.2 5.3 5.4 5.5 5.6 5.7
ARRANGEMENTS FOR THE EXERCISE OF FUNCTIONS BY DELEGATION Delegation of functions to Committees, Officers or other bodies Emergency powers and urgent decisions Delegation of Committees Delegation to Officers Reservation of Powers and Scheme of Delegation Duty to report non-compliance with Standing Orders and Standing Financial Instructions Overriding Standing Orders
26
26 26 26 27 27 27 27
6.
6.1 6.2 6.3 6.4 6.5
OVERLAP WITH OTHER TRUST POLICY STATEMENTS/ PROCEDURES, REGULATIONS AND STANDING FINANCIAL INSTRUCTIONS Policy statements: general principles Specific Policy statements Standing Financial Instructions Specific guidance Provider Licence/Health Legislation
28
28 28 28 28 29
7.
7.1
DUTIES AND OBLIGATIONS OF BOARD MEMBERS/ DIRECTORS AND SENIOR MANAGERS UNDER THE STANDING ORDERS Declaration of Interests Requirements for Declaring Interests and applicability to Board Interests which are relevant and material Advice on Interests Record of Interests in Board of Directors’ minutes Publication of declared interests in Annual Report
29
29 29
29 30 30 30
Page 225 of 300
43
7.2 7.3
7.4
Conflicts of interest which arise during the course of a meeting Register of Interests Exclusion of Chair and Members in Proceedings on Account of Pecuniary Interest Definition of terms used in interpreting ‘Pecuniary’ interest Exclusion in proceedings of the Board of Directors Waiver of Standing Orders made by the Secretary of State for Health Standards of Business Conduct Policy - Trust Policy and National Guidance - Interest of Officers in Contracts - Canvassing of, and Recommendations by, Members in
relation to appointments Relatives of Members or Officers Acceptance of Gifts
30
31 31
31 32 33 35 35 35 35
36 36
8.
8.1 8.2 8.3 8.4
CUSTODY OF SEAL, SEALING OF DOCUMENTS AND SIGNATURE OF DOCUMENTS Custody of Seal Sealing of Documents Register of Sealing Signature of Documents
37
37 37 37 37
9. DISPOSALS 38
10. IN HOUSE SERVICES 38
11. SIGNATURE OF DOCUMENTS 38
12. MISCELLANEOUS 39
13. RELATIONSHIP BETWEEN THE BOARD OF DIRECTORS AND THE COUNCIL OF GOVERNORS
39
14. TENDERING AND CONTRACT PROCEDURE 40
5
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 226 of 300
44
SECTION A – INTERPRETATION AND DEFINITIONS FOR STANDING ORDERS AND STANDING FINANCIAL INSTRUCTIONS
1.1 Save as otherwise permitted by law, at any meeting, the Chair of the NHS Foundation Trust (NHSFT) shall be the final authority on the interpretation of Standing Orders (on which they should be advised by the Chief Executive and/or Trust Secretary).
1.2 Any expression to which a meaning is given in the National Health Service Act 2006 shall have the same meaning in these Standing Orders and Standing Financial Instructions and in addition:
a. "Accounting Officer" means the NHS Officer responsible and
accountable for funds entrusted to the Trust. The officer shall be responsible for ensuring the proper stewardship of public funds and assets. For this Trust the Accounting Officer shall be the Chief Executive.
b. "Trust" means Sussex Community NHS Foundation Trust.
c. "Board of Directors” or “Board” means the Chair, Executive and Non-
Executive Directors of the Trust collectively as a body.
d. "Budget" means a resource, expressed in financial terms, proposed by the Board for the purpose of carrying out, for a specific period, any or all of the functions of the Trust.
e. “Budget holder” means the director or employee with delegated
authority to manage finances (Income and Expenditure) for a specific area of the organisation.
f. "Chair of the Board", “Chair of the Council” or “Chair of the Trust”
is the person appointed by the Council of Governors to lead the Board of Directors and to ensure that it successfully discharges its overall responsibility for the Trust as a whole. The expression “the Chair of the Trust” shall be deemed to include the Deputy Chair of the Trust if the Chair is absent from the meeting or is otherwise unavailable.
g. "Chief Executive" means the chief officer and the accounting officer of
the Trust.
h. “Council of Governors” means the Council of Governors of the Trust as described by the Trust’s Constitution.
i. "Commissioning" means the process for determining the need for and
for obtaining the supply of healthcare and related services by the Trust within available resources.
6
Page 227 of 300
45
j. "Committee" means a committee or sub-committee created and
appointed by the Board of Directors or Council of Governors.
k. "Committee members" means persons formally appointed by the Board or Council to sit on or to chair specific committees.
l. "Trust Secretary" means a person who may be appointed to act
independently of the Board to provide advice on corporate governance issues.
m. “Constitution” means the Trust’s Constitution as approved by the
Board of Directors and Council of Governors.
n. "Contracting and procuring" means the systems for obtaining the supply of goods, materials, manufactured items, services, building and engineering services, works of construction and maintenance and for disposal of surplus and obsolete assets.
o. "Deputy Chair" means the non-officer member appointed by the
Council of Governors to take on the Chair’s duties if the Chair is absent for any reason.
p. "Chief Financial Officer" means the Chief Financial Officer of the Trust.
q. "Executive Director" means a Member of the Board of Directors who
holds an executive office of the Trust. r. “Funds held on trust” shall mean those funds which the Trust holds on
date of incorporation, receives on distribution by statutory instrument or chooses subsequently to accept under powers derived under S.90 of the NHS Act 1977, as amended. Such funds may or may not be charitable.
s. “NHS Improvement” means the body responsible for overseeing
foundation trusts and NHS trusts, as well as independent providers that provide NHS-funded care in England (and any successor body or bodies from time to time)
t. "Nominated officer" means an officer charged with the responsibility for discharging specific tasks within Standing Orders and Standing Financial Instructions.
u. "Non-Executive Director" means a Member of the Board of Directors
who does not hold an executive office of the Trust and is appointed by the Council of Governors.
v. "Officer" means employee of the Trust or any other person holding a paid appointment or office with the Trust.
w. "SFIs" means Standing Financial Instructions.
7
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 228 of 300
46
x. "SOs" means Standing Orders for the Board of Directors.
Wherever possible, references to gender incorporate both male and female. Any references to one gender alone are made for ease of reference only and should be read to apply to either male or female persons.
SECTION B – STANDING ORDERS 1. INTRODUCTION
1.1 Statutory Framework
a. Sussex Community NHS Foundation Trust (the Trust) is a statutory body which became a public benefit corporation on 1 April 2016 following its authorisation as a NHS Foundation Trust by NHS Improvement pursuant to the National Health Service Act 2006 (the 2006 Act).
b. The principal place of business of the Trust is Brighton General Hospital, Elm Grove, Brighton BN2 3EW.
c. The Trust is governed by the 2006 and 2012 Acts, its Constitution and its
Licence. The Board of Directors is required to adopt Standing Orders for the regulation of its proceedings and business.
d. As a body corporate, the Trust has specific powers to contract in its own
name and to act as a corporate trustee. In the latter role, it is accountable to the Charity Commission for those funds deemed to be charitable. The Trust also has a common law duty as a bailee for patients' property held by the Trust on behalf of patients.
e. These Standing Orders bring together all the relevant information for the
Board of Directors included in the Constitution and supporting annexes and can be amended from time to time under Section 26 and Annex 7 Section 6 of the Constitution.
f. The Trust will also be bound by such other statutes and legal provisions
which govern the conduct of its affairs.
1.2 NHS Regulatory Framework
a. In addition to the statutory requirements, NHS Improvement, the Care Quality Commission and other healthcare regulatory bodies as may exist may issue further requirements to which the Trust must adhere.
b. The Constitution provides for the Trust to draw up a Schedule of Decisions Reserved to the Board and a Scheme of Delegation to enable responsibility to be clearly delegated to Committees of the Board and individual Directors. The Constitution also provides for the establishment
8
Page 229 of 300
47
of an Audit Committee and Nominations and Remuneration Committee(s) and sets out arrangements for dealing with possible conflicts of interests of Board Directors. The Codes of Conduct makes various requirements concerning possible conflicts of interest of Board members.
c. The Code of Practice on Openness in the NHS sets out the requirements
for public access to information on the NHS. This is also subject to the Freedom of Information Act 2000.
1.3 Delegation of Powers
The Board has powers to delegate and make arrangements for
delegation. The Standing Orders set out the detail of these arrangements. Under the Standing Order relating to the Arrangements for the Exercise of Functions (SO 5) the Board is given powers to "make arrangements for the exercise, on behalf of the Board, of any of their functions by a committee, sub-committee or joint committee appointed by virtue of Standing Order 4, or by an officer of the Trust, in each case subject to such restrictions and conditions as the Board thinks fit or as the Secretary of State may direct". Delegated Powers are covered in a separate document (‘Reservation of Powers and Scheme of Delegation’). This document has effect as if incorporated into the Standing Orders.
2. THE BOARD OF DIRECTORS: COMPOSITION OF MEMBERSHIP,
TENURE AND ROLE OF MEMBERS
All business shall be conducted in the name of the Trust. The business of the Trust is to be managed by the Board of Directors who, subject to the Constitution, shall exercise all the powers of the Trust. A third party dealing in good faith with the Trust shall not be affected by any defect in the process by which Directors are appointed or any vacancy on the Board of Directors.
All funds received in trust shall be held in the name of the Trust as corporate trustee.
The powers of the Trust established under statute shall be exercised by
the Board meeting in public session except as otherwise provided for in Standing Order 4.
The Trust will be subject to the general duty to consult and involve patients and the public, and to seek assurance that the appropriate consultation process has been adhered to in line with national guidance.
2.1 Composition of the Membership of the Board
The Board shall consist of Executive Directors, Non-Executive Directors and a Chair. The Chair and Non-Executive Directors of the Trust are appointed by the Council of Governors at a General Meeting. The Council
9
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 230 of 300
48
of Governors is also required to give its approval to the Chair and Non-Executive’s appointment of the Chief Executive. a. The role of the Chair is to:- o Provide leadership to the Board and promote the highest standards of
integrity, probity and corporate governance throughout the organisation and particularly at the level of the Board;
o Lead the Board in establishing effective decision-making processes and acting as the guardian of due process;
o Ensure that constructive relationships based on candour, trust and mutual respect exist between Executive and Non-Executive Directors, elected and appointed members of the Council of Governors and between the Board of Directors and Council of Governors;
o Provide general leadership of the Board of Directors and the Council of Governors, ensuring that the Board and Council work together effectively;
o Enable all Board members to make a full contribution to the Board's affairs and ensure that the Board acts collectively;
o Set a Board agenda that is focused on strategy and risk, performance, quality and accountability;
o Ensure the Board has adequate support and is provided efficiently with all the necessary data on which to base informed decisions;
o Lead Non-Executive Board members, through a formally constituted Nominations and Remuneration Committee, on the appointment, appraisal and remuneration of the Chief Executive and (with the latter) other Executive Board members;
o Appoint effective and suitable Non-Executive Board members to Committees of the Board; and,
o Advise the Governors on the performance of Non-Executive Board members.
o Conduct annual appraisals of the Non-Executive Directors. o Ensure that the Council of Governors receives training and development
to enable them to effectively carry out their role. o Set an agenda for the Council of Governors that is focused on strategy,
quality, Trust and Board performance, set out in such a way that it facilitates the Councils’ contribution to strategy and to holding the Non-Executive Directors (including the Chair) to account for the performance of the Board.
b. The role of a Non-Executive is to: o Support the Chair, Chief Executive and Executive Directors in promoting
the Trust’s values; o Constructively challenge the proposed decisions of the Board and ensure
that appropriate challenge is made in all circumstances; o Contribute to the development of strategy; o Support a positive culture throughout the Trust and adopt behaviours in
the boardroom and elsewhere that exemplify the corporate culture; o Scrutinise the performance of the Executive management in meeting
agreed goals and objectives;
10
Page 231 of 300
49
o Appoint and determine appropriate levels of remuneration for the Chief Executive (whose appointment is subject to the approval of the Council of Governors) and Executive Directors;
o Develop an ongoing dialogue with the Council of Governors on the progress made in delivering the Trust’s strategic objectives, the high level financial and operational performance of the Trust.
c. A Chief Executive (who is the accounting officer), who is appointed (and
removed) by the Chair and Non-Executive Directors, and whose appointment is subject to the approval of a majority of the members of the Council of Governors present and voting at a meeting.
d. Four other Executive Directors appointed (and removed) by a
Committee consisting of the Chief Executive, Chair, and the other Non-Executive Directors. These must include a Finance Director, a registered medical practitioner or registered dentist (within the meaning of the Dentists Act 1984) and a Registered Nurse or Midwife.
e. All Board members shall subscribe to the Code of Conduct and
Accountability for NHS Boards 2004 f. The Board of Directors shall elect one of the Non-Executive Directors to
be Deputy Chair of the Board. If the Chair is unable to discharge his/her office as Chair of the Trust, the Deputy Chair of the Board shall be acting Chair of the Trust. The Board, in consultation with the Governors, may appoint one of the Non-Executive Directors to act as the Senior Independent Director (SID). The SID may be the same person as the Deputy Chair but need not be.
g. The Trust shall have a Trust Secretary who may be an employee. The
Secretary may not be a Council Member, or the Chief Executive, or the Finance Director. The Secretary shall be accountable to the Chief Executive and their functions shall be as listed in the Constitution.
2.2 Tenure of Office
a. The tenure of office for Directors shall be:-
Chair – as determined by the Council of Governors.
Non-Executive Directors – as determined by the Council of Governors.
Chief Executive and Chief Financial Officer – for the period of their employment in those posts.
Other Executive Directors – for the period of their employment in those posts.
11
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 232 of 300
50
b. Any re-appointment of a Non-Executive Director by the Council of Governors shall be subject to a satisfactory appraisal carried out in accordance with procedures approved by the Board.
c. The Chair or a Non-Executive Director may resign his/her office at any
time during the period for which they were appointed by giving notice in writing to the Council of Governors.
d. Where a Non-Executive Director is appointed to be the Chair of the Trust,
his/her tenure of office as a Non-Executive Director shall terminate when his/her appointment as Chair takes effect and time served as a Non-Executive Director shall not count towards time served as Chair.
2.3 Disqualification as a Director A person may not become or continue as a Director of the Trust if:- a. He/she is not deemed a “fit and proper person” in accordance with NHS
Improvement’s provider licence and/or the requirements of the Care Quality Commission;
b. He/she is a member of the Council of Governors;
c. He/she has been adjudged bankrupt or his/her estate has been sequestrated and in either case he/she has not been discharged;
d. He/she has made a composition or arrangement with, or granted a Trust
deed for, his/her creditors and has not been discharged in respect of it;
e. He/she has within the preceding five years been convicted in the British Isles of any offence, and a sentence of imprisonment (whether suspended or not) for a period of three months or more (without the option of a fine) was imposed;
f. He/she is the subject of a disqualification order made under the Company
Directors Disqualification Act 1986;
g. In the case of a Non-Executive Director, he/she is no longer a member of one of the public constituencies;
h. He/she is a person whose tenure of office as a Chair or as a member or
Director of a health service body has been terminated on the grounds that his/her appointment is not in the interests of the health service, for non-attendance at meetings, or for non-disclosure of a pecuniary interest;
i. He/she has had his/her name removed, by a direction under section 46 of
the 1977 Act, from any list prepared under Part II of that Act, and has not subsequently had his/her name included on such a list;
12
Page 233 of 300
51
j. He/she has within the preceding two years been dismissed, otherwise than by reason of redundancy, from any paid employment with a health service body;
k. In the case of a Non-Executive Director, he/she has refused to fulfil any
training or appraisal requirement established by the Board; or
l. He/she has failed to sign and deliver to the Trust Secretary a statement in the form required by the Board confirming acceptance of the Code of Conduct for NHS Managers.
2.4 Executive Directors a. Executive Directors are usually employees of the Trust. However a
person holding a post in a university or a person seconded to work for the Trust may also be appointed as an Executive Director.
b. Executive Directors, including the Chief Executive, may be removed from the Board in line with due process if, in the view of the appointing body, it is not in the interests of the Trust for them to continue as a Director. If any Executive Director is suspended from his/her post with the Trust he/she will also be suspended from being a Director for the period of his/her suspension.
c. Two people who job-share may be appointed as Executive Directors of
the Trust but shall count as one Director for the purpose of SO 1. Both may attend meetings of the Trust but they have one vote between them and count as one person for the purpose of a quorum, whether either or both attend. In the event of disagreement between the two Directors no vote may be cast.
2.5 Corporate Role of the Board and Responsibilities
a. The Board is held accountable by NHS Improvement on behalf of the
Secretary of State for the following key functions:- o To formulate strategy; o To ensure accountability by holding the organisation to account for the
delivery of the strategy and through seeking assurance that systems of control are robust and reliable;
o Shaping a positive culture for the Board and the organisation; o To, individually and collectively, act with a view to promoting the success
of the Trust so as to maximise the benefits for the members of the corporation as a whole and for the public;
o To maintain and improve quality of care; o To ensure compliance with all applicable laws, regulation and statutory
guidance.
13
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 234 of 300
52
o To work in partnership with patients, carers, local health organisations, local government authorities and others to provide safe, effective, accessible, and well-governed services for patients.
b. All business shall be conducted in the name of the Trust. c. All funds received in trust shall be held in the name of the Trust as
corporate trustee. d. The powers of the Trust established under statute shall be exercised by
the Board meeting in public session except as otherwise provided for in Standing Order No. 3.
e. The Board shall define and regularly review the functions it exercises on behalf of the Secretary of State.
2.6 Reservation of Powers and Scheme of Delegation
The Board has resolved that certain powers and decisions may only be exercised by the Board in formal session. These powers and decisions are set out in the document entitled ‘Reservation of Powers and Scheme of Delegation’ and shall have effect as if incorporated into the Standing Orders. Those powers which it has delegated to officers and other bodies are contained in the Scheme of Delegation.
2.7 Lead Roles for Board Members The Chair will ensure that the designation of Lead Roles or appointments of Board members as required by the Department of Health and Social Care or as set out in any statutory or other guidance will be made in accordance with that guidance or statutory requirement (e.g. appointing a Lead Board Member with responsibilities for Infection Control, Medical Revalidation, Information Risk, the Caldicott Guardian function, etc.).
2.8 Senior Independent Director
The Senior Independent Director shall perform the role set out in “The NHS Foundation Trust Code of Governance” (2010, revised 2013 and
2014) issued by NHS Improvement. The Senior Independent Director shall be available to members and Governors who have concerns that they do not feel they can raise with the Chair or any Executive Director of the Trust. Recourse to the Senior Independent Director shall not replace the right to instigate the dispute resolution procedure as set out in the Constitution.
3. MEETINGS OF THE BOARD OF DIRECTORS
3.1. Calling meetings
14
Page 235 of 300
53
a. Ordinary meetings of the Board shall be held at regular intervals at such times and places as the Chair may determine.
b. The Chair of the Trust may call a meeting of the Board at any time.
c. One third or more members of the Board may requisition a meeting in writing. If the Chair refuses, or fails, to call a meeting within seven days of a requisition being presented, the members signing the requisition may forthwith call a meeting.
3.2. Notice of Meetings and the Business to be transacted
a. Before each meeting of the Board a written notice specifying the
business proposed to be transacted shall be delivered to every member, or sent by post to the usual place of residence of each member, or sent by email, so as to be available to members at least 3 clear days before the meeting. Want of service of such a notice on any member shall not affect the validity of a meeting.
b. In the case of a meeting called by members in default of the Chair calling the meeting, the notice shall be signed by those members.
c. No business shall be transacted at the meeting other than that specified
on the agenda, or emergency motions allowed under Standing Order 3.6.
d. A member desiring a matter to be included on an agenda shall make his/her request to the Chair at least 15 clear days before the meeting. The request should state whether the item of business is proposed to be transacted in the presence of the public and should include appropriate supporting information. Requests made less than 15 days before a meeting may be included on the agenda at the discretion of the Chair.
e. Before each meeting of the Board a public notice of the time and place of
the meeting, and the public part of the agenda, shall be displayed at the Trust’s principal offices and/or on the Trust’s website at least 3 clear days before the meeting, (required by the Public Bodies (Admission to Meetings) Act 1960 Section 1 (4) (a)).
3.3. Agenda and Supporting Papers
The Agenda will be sent to members a minimum of 5 days (including
Saturdays and Sundays) before the meeting and supporting papers, whenever possible, shall accompany the agenda, but will certainly be dispatched (electronically or in hard copy) no later than 3 clear (working) days before the meeting, save in emergency.
3.4. Admissibility of papers
Board papers must:-
15
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 236 of 300
54
a. be written using the appropriate template and contain clear recommendations for consideration by the Board; and
b. be submitted to the Trust Secretary (or his/her nominee) for dispatch a minimum of 5 clear days before the date of the Board meeting, to facilitate the timely distribution of papers.
The Trust Secretary has the delegated authority of the Board to remove an item from the agenda if it is not received in time or to a suitable standard or is not on the agenda for the meeting and does not have Chair’s approval for late inclusion on the agenda (SO 3.2 c and d).
3.5. Petitions For the purposes of these Standing Orders, a petition is defined as "a document embodying a formal written request for some form of action or the consideration of some matter by the Board". Where a petition has been received by the Trust the Chair shall include the petition as an item for the agenda of the next meeting.
3.6. Notice of Motion a. Subject to the provision of Standing Orders 3.8 ‘Motions: Procedure at
and during a meeting’ and 3.9 ‘Motions to rescind a resolution’, a member of the Board wishing to move a motion shall send a written notice to the Chief Executive who will ensure that it is brought to the immediate attention of the Chair.
b. The notice shall be delivered at least 15 clear days before the meeting. The Chief Executive shall include in the agenda for the meeting all notices so received that are in order and permissible under governing regulations. This Standing Order shall not prevent any motion being withdrawn or moved without notice on any business mentioned on the agenda for the meeting.
3.7. Emergency Motions
Subject to the agreement of the Chair, and subject also to the provision of
Standing Order 3.8 ‘Motions: Procedure at and during a meeting’, a member of the Board may give written notice of an emergency motion after the issue of the notice of meeting and agenda, up to one hour before the time fixed for the meeting. The notice shall state the grounds of urgency. If in order, it shall be declared to the Board at the commencement of the business of the meeting as an additional item included in the agenda. The Chair's decision to include the item shall be final.
3.8. Motions: Procedure at and during a meeting
a. Who may propose?
16
Page 237 of 300
55
A motion may be proposed by the Chair of the meeting or any member
present. It must also be seconded by another member.
b. Contents of motions The Chair may exclude from the debate at his/her discretion any such
motion of which notice was not given on the notice summoning the meeting other than a motion relating to:
o the receipt of a report; o consideration of any item of business before the Board; o the accuracy of minutes; o that the Board proceed to next business; o that the Board adjourn; o that the question be now put.
c. Amendments to motions
i. A motion for amendment shall not be discussed unless it has been
proposed and seconded. ii. Amendments to motions shall be moved relevant to the motion, and
shall not have the effect of negating the motion before the Board.
iii. If there are a number of amendments, they shall be considered one at a time. When a motion has been amended, the amended motion shall become the substantive motion before the meeting, upon which any further amendment may be moved.
d. Rights of reply to motions
i.Amendments
The mover of an amendment may reply to the debate on their amendment immediately prior to the mover of the original motion, who shall have the right of reply at the close of debate on the amendment, but may not otherwise speak on it.
ii.Substantive/original motion
The member who proposed the substantive motion shall have a right of reply at the close of any debate on the motion.
e. Withdrawing a motion
A motion, or an amendment to a motion, may be withdrawn.
f. Motions once under debate
17
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 238 of 300
56
i. When a motion is under debate, no motion may be moved other than:- o an amendment to the motion; o the adjournment of the discussion, or the meeting; o that the meeting proceed to the next business; o that the question should be now put; o the appointment of an 'ad hoc' committee to deal with a specific
item of business; o that a member/director be not further heard; o a motion under Section l (2) or Section l (8) of the Public Bodies
(Admissions to Meetings) Act l960 resolving to exclude the public, including the press (see Standing Order 3.20).
ii. In those cases where the motion is either that the meeting proceeds to the ‘next business’ or ‘that the question be now put’ in the interests of objectivity these should only be put forward by a member of the Board who has not taken part in the debate and who is eligible to vote.
iii. If a motion to proceed to the next business or that the question be now put, is carried, the Chair should give the mover of the substantive motion under debate a right of reply, if not already exercised. The matter should then be put to the vote.
3.9. Motion to Rescind a Resolution
a. Notice of motion to rescind any resolution (or the general substance of any
resolution) which has been passed within the preceding six calendar months shall bear the signature of the member who gives it and also the signature of three other members, and before considering any such motion of which notice shall have been given, the Board may refer the matter to any appropriate Committee or the Chief Executive for recommendation.
b. When any such motion has been dealt with by the Board it shall not be competent for any director/member other than the Chair to propose a motion to the same effect within six months. This Standing Order shall not apply to motions moved in pursuance of a report or recommendations of a Committee or the Chief Executive.
3.10. Chair of meeting
a. At any meeting of the Board the Chair, if present, shall preside. If the
Chair is absent from the meeting, the Deputy Chair, if present, shall preside.
b. If the Chair and Deputy Chair are absent, such member (who is not also an Officer Member of the Trust) as the members present shall choose shall preside.
18
Page 239 of 300
57
3.11. Chair's ruling The decision of the Chair of the meeting on questions of order, relevancy and regularity (including procedure on handling motions) and their interpretation of the Standing Orders and Standing Financial Instructions, at the meeting, shall be final.
3.12. Quorum
a. No business shall be transacted at a meeting unless at least one-half of the whole number of the Chair and members (including at least one member who is also an Officer Member of the Trust and one member who is not) is present.
b. An Officer in attendance for an Executive Director (Officer Member) but without formal acting up status may not count towards the quorum.
c. If the Chair or member has been disqualified from participating in the
discussion on any matter and/or from voting on any resolution by reason of a declaration of a conflict of interest (see SO No.7) that person shall no longer count towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business.
3.13. Voting
a. Save as provided in Standing Orders 3.l4 – Suspension of Standing
Orders and 3.l5 – Variation and Amendment of Standing Orders, every question put to a vote at a meeting shall be determined by a majority of the votes of members present and voting on the question. In the case of an equal vote, the person presiding (i.e. the Chair of the meeting, shall have a second, and casting vote.
b. At the discretion of the Chair, all questions put to the vote shall be determined by oral expression or by a show of hands, unless the Chair directs otherwise, or it is proposed, seconded and carried that a vote be taken by paper ballot.
c. If at least one third of the members present so request, the voting on any
question may be recorded so as to show how each member present voted or did not vote (except when conducted by paper ballot).
d. If a member so requests, their vote shall be recorded by name.
e. In no circumstances may an absent member vote by proxy. Absence is
defined as being absent at the time of the vote.
19
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 240 of 300
58
f. A manager who has been formally appointed to act up for an Officer Member during a period of incapacity or temporarily to fill an Executive Director vacancy shall be entitled to exercise the voting rights of the Officer Member.
g. A manager attending the Board meeting to represent an Officer Member
during a period of incapacity or temporary absence without formal acting up status may not exercise the voting rights of the Officer Member. An Officer’s status when attending a meeting shall be recorded in the minutes.
h. For the voting rules relating to joint members see Standing Order 2.4.
3.14. Suspension of Standing Orders
a. Except where this would contravene any statutory provision or any direction made by the Secretary of State or the rules relating to the Quorum (SO 3.12), any one or more of the Standing Orders may be suspended at any meeting, provided that at least two-thirds of the whole number of the members of the Board are present (including at least one member who is an Officer Member of the Trust and one member who is not) and that at least two-thirds of those members present signify their agreement to such suspension. The reason for the suspension shall be recorded in the Board's minutes.
b. A separate record of matters discussed during the suspension of Standing Orders shall be made and shall be available to the Chair and members of the Board.
c. No formal business may be transacted while Standing Orders are
suspended.
d. The Audit Committee shall review every decision to suspend Standing Orders.
3.15. Variation and amendment of Standing Orders
These Standing Orders shall not be varied except in the following circumstances:
o upon a notice of motion under Standing Order 3.6; o upon a recommendation of the Chair or Chief Executive included on
the agenda for the meeting; o that two thirds of the Board members are present at the meeting
where the variation or amendment is being discussed, and that at least half of the Board’s Non-Officer members vote in favour of the amendment;
o providing that any variation or amendment does not contravene a statutory provision or direction made by the Secretary of State.
3.16. Record of Attendance
20
Page 241 of 300
59
The names of the Chair and Directors/members/officers present at the meeting shall be recorded in the minutes of the meeting.
3.17. Minutes
a. The minutes of the proceedings of a meeting shall be drawn up and submitted for agreement at the next ensuing meeting.
b. No discussion shall take place upon the minutes except upon their accuracy or where the Chair considers discussion appropriate.
3.18. Interest of Directors in Contracts and Other Matters on account of
pecuniary interests
a. Any Director who has a material interest in a matter as defined below shall declare such interest to the Board of Directors and:
i. shall not be present except with the permission of the Board of
Directors in any discussion of the matter, and
ii. shall not vote on the issue (and if by inadvertence they do remain and vote, their vote shall not be counted).
b. Any Director who fails to disclose any interest required to be disclosed
under the preceding paragraph must permanently vacate their office if required to do so by a majority of the remaining Directors.
c. A material interest is:
i. any directorship of a company;
ii. any interest (excluding a holding of shares in a company whose
shares are listed on any public exchange where the holding is less than 2% of the total shares in issue) held by a Director in any firm or company or business which, in connection with the matter, is trading with the Trust, or is likely to be considered as a potential trading partner with the Trust;
iii. any interest in an organisation providing health and social care
services to the National Health Service;
iv. a position of authority in a charity or voluntary organisation in the field of health and social care; any affiliation to a special interest group campaigning on health or social care issues
3.19. Failure to Declare an Interest
If a Director of the Board fails to declare an interest, or is found to have used their position or knowledge for private advantage, disciplinary action
21
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 242 of 300
60
will be taken by the Board, which could lead to removal.
3.20. Admission of public and the press a. Admission and exclusion on grounds of confidentiality of business
to be transacted
Members of the Council of Governors, the public and representatives of the press may attend all meetings of the Trust, but shall be required to withdraw upon the Board agreeing the following resolution:
o 'that representatives of the Council of Governors, the press and
other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest', Section 1 (2), Public Bodies (Admission to Meetings) Act l960
o Guidance should be sought from the Trust Secretary and/or the
Trust’s Freedom of Information Lead to ensure correct procedure is followed on matters to be included in the exclusion.
b. General disturbances
The Chair (or Deputy Chair if one has been appointed) or the person presiding over the meeting shall give such directions as he/she thinks fit with regard to the arrangements for meetings and accommodation of the public and representatives of the press such as to ensure that the Trust’s business shall be conducted without interruption and disruption and, without prejudice to the power to exclude on grounds of the confidential nature of the business to be transacted, the public will be required to withdraw upon the Board agreeing the following resolution:
o That in the interests of public order, the meeting adjourn for (the
period to be specified) to enable the Board to complete its business without the presence of the public'. Section 1(8) Public Bodies (Admissions to Meetings) Act l960.
c. Business proposed to be transacted when the press and public
have been excluded from a meeting
Matters to be dealt with by the Board following the exclusion of representatives of the press, and other members of the public, as provided in (a) and (b) above, shall be confidential to the members of the Board. Members and Officers or any employee or Governor of the Trust in attendance shall not reveal or disclose the contents of papers or
22
Page 243 of 300
61
minutes marked 'Commercial in Confidence' outside of the Trust without the express permission of the Board. This prohibition shall apply equally to the content of any discussion during the Board meeting which may take place on such reports or papers.
d. Use of Mechanical or Electrical Equipment for Recording or
Transmission of Meetings
Nothing in these Standing Orders shall be construed as permitting the introduction by the public, or press representatives, of recording, transmitting, video or similar apparatus, into meetings of the Board or Committee thereof. Such permission shall be granted only upon resolution of the Board.
3.21. Observers at Board meetings
The Board will decide what arrangements and terms and conditions it feels are appropriate to offer in extending an invitation to observers to attend and address any of the Board's meetings and may change, alter or vary these terms and conditions as it deems fit.
4. APPOINTMENT OF COMMITTEES AND SUB-COMMITTEES
4.1. Appointment of Committees
i. The National Health Service Act 2006 states that the Board will establish
a Nominations and Remuneration Committee and Audit Committee. Membership of these Committees will consist of a minimum of three Non-Executive Directors. The Nominations and Remuneration Committee and Audit Committee are formal Committees of the Board and will have a Non-Executive Director as Chair. Executive Directors and other staff may be invited to attend these committees.
ii. The Board may appoint further committees (including a committee of the whole Board) to exercise functions on its behalf. Such committees may consist wholly or partly of Directors or wholly of persons who are not Directors. Where functions are being carried out by committees or sub-committees, their members, including those who are not Directors, are acting on behalf of and with delegated authority from the Board, and this should be reflected in the Committee’s Terms of Reference.
iii. A Committee appointed under SO 4.1 may appoint sub-committees
consisting wholly or partly of members of the Committee.
iv. Each such committee or sub-committee shall have such terms of reference or powers as approved by the Board. Such terms of reference shall have effect as if incorporated into Standing Orders.
v. Committees may not delegate their powers to a sub-committee unless
expressly authorised by the Board.
23
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 244 of 300
62
vi. The appointment of Directors to committees and sub-committees of the
Board comes to an end on the termination of their terms of office as Directors.
vii. Standing Order 3.18 relating to pecuniary interests, applies to members
of committees and sub-committees of the Trust whether or not they are Directors of the Trust itself.
viii. Executive Directors may not be appointed to any committee or sub-
committee set up to carry out the functions of "managers" under the Mental Health Act 1983. Most important of these is the hearing of appeals by detained patients under section 23 (3) (c) Schedule 9 of the 1990 Act.
4.2. Confidential Proceedings
A Director or Officer or Governor of the Trust shall not disclose a matter considered by the Board or a Committee in confidence without permission until the Board or Committee has considered the matter in public or has resolved to make the matter public.
4.3. Applicability of Standing Orders and Standing Financial Instructions to Committees The Standing Orders and Standing Financial Instructions of the Trust, as far as they are applicable, shall as appropriate apply to meetings and any committees established by the Trust. In which case the term “Chair” is to be read as a reference to the Chair of other committees as the context permits, and the term “member” is to be read as a reference to a member of other committees also as the context permits. (There is no requirement to hold meetings of committees established by the Board in public.)
4.4. Terms of Reference Each committee shall have such terms of reference and powers and be subject to such conditions (as to reporting back to the Board) as the Board shall decide and shall be in accordance with any legislation and
regulation or direction issued by the Secretary of State. Such terms of reference shall have effect as if incorporated into the Standing Orders.
4.5. Delegation of powers by Committees to Sub-Committees Where committees are authorised to establish sub-committees they may
not delegate executive powers to the sub-committee unless expressly authorised by the Board.
4.6. Approval of Appointments to Committees The Board shall approve the appointments to each of the committees
24
Page 245 of 300
63
which it has formally constituted. Where the Board determines, and regulations permit, that persons, who are neither members nor officers, shall be appointed to a committee, the terms of such appointment shall be within the powers of the Board as defined by the Secretary of State. The Board shall define the powers of such appointees and shall agree allowances, including reimbursement for loss of earnings, and/or expenses in accordance where appropriate with national guidance.
4.7. Appointments for Statutory functions Where the Board is required to appoint persons to a committee and/or to
undertake statutory functions as required by the Secretary of State, and where such appointments are to operate independently of the Board, such appointment shall be made in accordance with the regulations and directions made by the Secretary of State.
4.8. Committees established by the Board
The committees established by the Board are:
a. Audit Committee
In line with the requirements of the NHS Audit Committee Handbook,
NHS Codes of Conduct and Accountability, the Higgs report, and NHS Improvement’s Code of Governance, an Audit Committee will be established and constituted to provide the Board with an independent and objective review on its financial systems, financial information, clinical audit programme, systems and processes for clinical and quality governance, and compliance with laws, governance practice, and regulations governing the NHS. The Terms of Reference will be approved by the Board and reviewed on a periodic basis.
b. Board of Directors’ Nominations and Remuneration Committee
In line with the requirements of the NHS Codes of Conduct and
Accountability, the Higgs report, and NHS Improvement’s Code of Governance, a Nominations and Remuneration Committee will be established and constituted.
The committee will be comprised exclusively of Non-Executive Directors,
a minimum of three, who are independent of management. The principal purpose of the Committee will be to, on behalf of the Board,
set appropriate remuneration and terms of service for the Chief Executive and other Executive Directors including:
i. all aspects of salary (including any performance-related elements/bonuses);
ii. provisions for other benefits, including pensions and cars;
25
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 246 of 300
64
iii. arrangements for termination of employment and other contractual terms.
c. Charitable Funds Committee
In line with its role as a corporate trustee for any funds held in trust, either
as charitable or non charitable funds, the Board will establish a Charitable Funds Committee to administer those funds in accordance with any statutory or other legal requirements or best practice required by the Charity Commission.
The provisions of this Standing Order must be read in conjunction with
Standing Financial Instructions 17.
d. Other Committees
The Board may also establish such other committees as required to
discharge the Trust's responsibilities. 5. ARRANGEMENTS FOR THE EXERCISE OF TRUST FUNCTIONS BY
DELEGATION
5.1. Delegation of Functions to Committees, Officers or other bodies
a. Subject to such directions as may be given by the Secretary of State, the Board may make arrangements for the exercise, on behalf of the Board, of any of its functions by a committee, sub-committee appointed by virtue of Standing Order 4, or by an officer of the Trust, or by another body as defined in Standing Order 5.2 below, in each case subject to such restrictions and conditions as the Trust thinks fit.
b. Where a function is delegated by these Regulations to another Trust, then that Trust or health service body exercises the function in its own right; the receiving Trust has responsibility to ensure that the proper delegation of the function is in place. In other situations, i.e. delegation to committees, sub-committees or officers, the Trust delegating the function retains full responsibility.
5.2. Emergency Powers and Urgent Decisions The powers which the Board has reserved to itself within these Standing
Orders (see Standing Order 2.6) may in emergency or for an urgent decision be exercised jointly by the Chief Executive and the Chair after having consulted at least two non-officer members. The exercise of such powers by the Chief Executive and Chair shall be reported to the next formal meeting of the Board in public session for formal ratification.
5.3. Delegation to Committees
26
Page 247 of 300
65
a. The Board shall agree from time to time to the delegation of executive powers to be exercised by other committees, or sub-committees, or joint-committees, which it has formally constituted in accordance with directions issued by the Secretary of State. The constitution and terms of reference of these committees, or sub-committees, or joint committees, and their specific executive powers shall be approved by the Board in respect of its sub-committees.
5.4. Delegation to Officers
a. Those functions of the Trust which have not been retained as reserved by the Board or delegated to other committee or sub-committee or joint-committee shall be exercised on behalf of the Trust by the Chief Executive. The Chief Executive shall determine which functions he/she will perform personally and shall nominate officers to undertake the remaining functions for which he/she will still retain accountability to the Trust.
b. The Chief Executive shall prepare a Scheme of Delegation identifying his/her proposals which shall be considered and approved by the Board. The Chief Executive may periodically propose amendment to the Scheme of Delegation which shall be considered and approved by the Board.
c. Nothing in the Scheme of Delegation shall impair the discharge of the
direct accountability to the Board of the Chief Financial Officer to provide information and advise the Board in accordance with statutory or Department of Health and Social Care requirements. Outside these statutory requirements, the Chief Financial Officer shall be accountable to the Chief Executive for operational matters.
5.5. Reservation of Powers and Scheme of Delegation
The arrangements made by the Board as set out in the "Reservation of Powers and Scheme of Delegation” shall have effect as if incorporated in these Standing Orders.
5.6. Duty to report non-compliance with Standing Orders and Standing
Financial Instructions
If for any reason these Standing Orders are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the non-compliance, shall be reported to the next formal meeting of the Board for action or ratification. All members of the Board and staff have a duty to disclose any non-compliance with these Standing Orders to the Chief Executive as soon as possible.
5.7. Over-riding Standing Orders
Should there be a need to over-ride these Standing Orders, the
27
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 248 of 300
66
permission of the Chief Executive will be sought, who will in turn consult with the Chair wherever possible. Full details and any justification for this non-compliance together with the circumstances around the non-compliance, shall be reported by the relevant Executive Director to the next formal meeting of the Board of Directors. All staff have a duty to disclose any potential or impending non-compliance to their Executive Director, who has a duty to report to the Chief Executive as soon as possible.
6. OVERLAP WITH OTHER TRUST POLICY STATEMENTS/
PROCEDURES, REGULATIONS AND THE STANDING FINANCIAL INSTRUCTIONS
6.1. Policy statements: general principles The Board or one of its Committees will from time to time approve Policy
statements/ procedures which will apply to all or specific groups of staff employed by the Trust. The decisions to approve such policies and procedures will be recorded in an appropriate Board or Committee minute and will be deemed where appropriate to be an integral part of the Trust's Standing Orders and Standing Financial Instructions.
6.2. Specific Policy statements
Notwithstanding the application of SO 6.1 above, these Standing Orders
and Standing Financial Instructions must be read in conjunction with the following Policy statements:
a. the Trust’s Standards of Business Conduct Policy (including gifts and
hospitality); b. the Staff Disciplinary Policy and Appeals Procedures adopted by the
Trust, both of which shall have effect as if incorporated in these Standing Orders.
c. Anti-fraud, Bribery and Corruption Policy
6.3. Standing Financial Instructions
Standing Financial Instructions adopted by the Board in accordance with all financial regulations, directions and guidance issued by NHS Improvement and any other relevant body shall have effect as if incorporated in these Standing Orders.
6.4. Specific guidance
Notwithstanding the application of SO 6.1 above, these Standing Orders and the Standing Financial Instructions must be read in conjunction with any directions and guidance issued by NHS Improvement and any other relevant body and in accordance with the following:
28
Page 249 of 300
67
o Data Protection Act 2018 o DH Caldicott Guardian Manual 2010 o Human Rights Act 1998; o Freedom of Information Act 2000; o Equality Act 2010; o Information Governance Toolkit o Bribery Act 2010 o Fit and proper persons regulations o Fraud Act 2006
6.5. Provider Licence/ Health Legislation
In the event of and to the extent of any conflict or inconsistency between
these SOs and the Provider Licence, the Provider Licence shall prevail. In the event of and to the extent of any conflict or inconsistency between these SOs and the provisions of the National Health Service Act 2006 and/or Health and Social Care Act 2012, the provisions of the National Health Service Act 2006 and/or Health and Social Care Act 2012 shall prevail.
7. DUTIES AND OBLIGATIONS OF BOARD MEMBERS/DIRECTORS AND
SENIOR MANAGERS UNDER THESE STANDING ORDERS
7.1. Declaration of Interests
a. Requirements for Declaring Interests and applicability to Board Members
THE NHS CODE OF ACCOUNTABILITY REQUIRES BOARD MEMBERS TO DECLARE INTERESTS WHICH ARE RELEVANT AND MATERIAL TO THE NHS BOARD OF WHICH THEY ARE A MEMBER. ALL EXISTING BOARD MEMBERS SHOULD DECLARE SUCH INTERESTS. ANY BOARD MEMBERS APPOINTED SUBSEQUENTLY SHOULD DO SO ON APPOINTMENT.
b. Interests which are relevant and material
INTERESTS WHICH SHOULD BE REGARDED AS "RELEVANT AND MATERIAL" ARE:
i. Directorships, including Non-Executive Directorships held in
private companies or PLCs (with the exception of those of dormant companies);
ii. Ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the NHS;
iii. Majority or controlling shareholdings in organisations likely or possibly seeking to do business with the NHS;
29
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 250 of 300
68
iv. A position of authority in a charity or voluntary organisation in the field of health and social care;
v. Any connection with a voluntary or other organisation contracting for NHS services;
vi. Research funding/grants that may be received by an individual or their department;
vii. Interests in pooled funds that are under separate management.
ANY MEMBER OF THE BOARD WHO COMES TO KNOW THAT THE TRUST HAS ENTERED INTO OR PROPOSES TO ENTER INTO A CONTRACT IN WHICH HE/SHE OR ANY
PERSON CONNECTED WITH HIM/HER (AS DEFINED IN STANDING ORDER 7.3 BELOW AND ELSEWHERE) HAS ANY PECUNIARY INTEREST, DIRECT OR INDIRECT, THE BOARD MEMBER SHALL DECLARE HIS/HER INTEREST BY GIVING NOTICE IN WRITING OF SUCH FACT TO THE TRUST AS SOON AS PRACTICABLE.
c. Advice on Interests
If Board members have any doubt about the relevance of an interest, this
should be discussed with the Chair of the Trust or with the Trust Secretary.
International Accounting Standard No 24 (issued by the International
Accounting Standards Board) specifies that influence rather than the immediacy of the relationship is more important in assessing the relevance of an interest. The interests of partners in professional partnerships including general practitioners should also be considered.
d. Recording of Interests in Board minutes
At the time Board members' interests are declared, they should be
recorded in the Board minutes. Any changes in interests should be declared at the next Board meeting
following the change occurring and recorded in the minutes of that meeting.
e. Publication of declared interests in Annual Report
Board members' directorships of companies likely or possibly seeking to
do business with the NHS should be published in the Trust's annual report. The information should be kept up to date for inclusion in succeeding annual reports.
f. Conflicts of interest which arise during the course of a meeting
30
Page 251 of 300
69
During the course of a Board meeting, if a conflict of interest is established, the Board member concerned should withdraw from the meeting and play no part in the relevant discussion or decision. (See overlap with SO 7.3)
7.2. Register of Interests
A. THE CHIEF EXECUTIVE (OR HIS/HER NOMINEE) WILL ENSURE
THAT A REGISTER OF INTERESTS IS ESTABLISHED TO RECORD FORMALLY DECLARATIONS OF INTERESTS OF BOARD OR COMMITTEE MEMBERS. IN PARTICULAR THE REGISTER WILL INCLUDE DETAILS OF ALL DIRECTORSHIPS AND OTHER RELEVANT AND MATERIAL INTERESTS (AS DEFINED IN SO 7.1.2) WHICH HAVE BEEN DECLARED BY BOTH EXECUTIVE AND NON-EXECUTIVE BOARD MEMBERS.
25. B. THESE DETAILS WILL BE KEPT UP TO DATE BY MEANS OF AN
ANNUAL REVIEW OF THE REGISTER IN WHICH ANY CHANGES TO INTERESTS DECLARED DURING THE PRECEDING TWELVE MONTHS WILL BE INCORPORATED.
26. C. THE REGISTER WILL BE AVAILABLE TO THE PUBLIC AND THE
CHIEF EXECUTIVE (OR HIS/HER NOMINEE) WILL TAKE REASONABLE STEPS TO BRING THE EXISTENCE OF THE REGISTER TO THE ATTENTION OF LOCAL RESIDENTS AND TO PUBLICISE ARRANGEMENTS FOR VIEWING IT.
7.3. Exclusion of Chair and Members in proceedings on account of
pecuniary interest
a. Definition of terms used in interpreting ‘Pecuniary’ interest
For the sake of clarity, the following definition of terms is to be used in interpreting this Standing Order:
i. "spouse" shall include any person who lives with another person in the
same household (and any pecuniary interest of one spouse shall, if known to the other spouse, be deemed to be an interest of that other spouse);
ii. "contract" shall include any proposed contract or other course of dealing.
iii. “Pecuniary interest”
Subject to the exceptions set out in this Standing Order, a person
shall be treated as having an indirect pecuniary interest in a contract if:-
31
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 252 of 300
70
o he/she, or a nominee of his/her, is a member of a company or other body (not being a public body), with which the contract is made, or to be made or which has a direct pecuniary interest in the same, or
o he/she is a partner, associate or employee of any person with whom the contract is made or to be made or who has a direct pecuniary interest in the same.
iv. Exception to Pecuniary interests
A person shall not be regarded as having a pecuniary interest in any contract if:-
o neither he/she or any person connected with him/her has any beneficial interest in the securities of a company of which he/she or such person appears as a member, or
o any interest that he/she or any person connected with him/her
may have in the contract is so remote or insignificant that it cannot reasonably be regarded as likely to influence him/her in relation to considering or voting on that contract, or
o those securities of any company in which he/she (or any person
connected with him/her) has a beneficial interest do not exceed £10,000 in nominal value or one per cent of the total issued share capital of the company or of the relevant class of such capital, whichever is the less. Provided however, that where this applies, the person shall nevertheless be obliged to disclose/declare their interest in accordance with Standing Order 7.1.
b. Exclusion in proceedings of the Board
i. Subject to the following provisions of this Standing Order, if the Chair
or a member of the Board has any pecuniary interest, direct or indirect, in any contract, proposed contract or other matter and is present at a meeting of the Board at which the contract or other matter is the subject of consideration, they shall at the meeting and as soon as practicable after its commencement disclose the fact and shall not take part in the consideration or discussion of the contract or other matter or vote on any question with respect to it.
ii. The Secretary of State may, subject to such conditions as he/she may think fit to impose, remove any disability imposed by this Standing Order in any case in which it appears to him/her in the interests of the National Health Service that the disability should be removed. (See SO 7.3.c on the ‘Waiver’ which has been approved by the Secretary of State for Health).
32
Page 253 of 300
71
iii. The Board may exclude the Chair or a member of the Board from a meeting of the Board while any contract, proposed contract or other matter in which he/she has a pecuniary interest is under consideration.
iv. Any remuneration, compensation or allowance payable to the Chair or
a Member by virtue of paragraph 11 of Schedule 5A to the National Health Service Act 1977 (pay and allowances) shall not be treated as a pecuniary interest for the purpose of this Standing Order.
v. This Standing Order applies to a committee or sub-committee and to a
joint committee or sub-committee as it applies to the Trust and applies to a member of any such committee or sub-committee (whether or not he/she is also a member of the Trust) as it applies to a member of the Trust.
c. Waiver of Standing Orders made by the Secretary of State for Health
i. Power of the Secretary of State to make waivers
Under regulation 11(2) of the NHS (Membership and Procedure
Regulations SI 1999/2024 (“the Regulations”), there is a power for the Secretary of State to issue waivers if it appears to the Secretary of State in the interests of the health service that the disability in regulation 11 (which prevents a Chair or a member from taking part in the consideration or discussion of, or voting on any question with respect to, a matter in which he/she has a pecuniary interest) is removed. A waiver has been agreed in line with sub-sections (2) to (4) below.
ii. Definition of ‘Chair’ for the purpose of interpreting this waiver
For the purposes of paragraph 7.3.iii. (below), the “relevant Chair” is:
o at a meeting of the Board, the Chair of that Trust;
o at a meeting of a Committee:-
- in a case where the member in question is the Chair of that Committee, the Chair of the Trust;
- in the case of any other member, the Chair of that Committee.
iii. Application of waiver
A waiver will apply in relation to the disability to participate in the proceedings of the Trust on account of a pecuniary interest. It will apply to:-
A member of the Sussex Community NHS Foundation Trust
33
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 254 of 300
72
(“the Trust”), who is a healthcare professional, within the meaning of regulation 5(5) of the Regulations, and who is providing or performing, or assisting in the provision or performance, of –
o services under the National Health Service Act 1977; or o services in connection with a pilot scheme under the National
Health Service Act 1997; for the benefit of persons for whom the Trust is responsible.
Where the ‘pecuniary interest’ of the member in the matter
which is the subject of consideration at a meeting at which
he/she is present:-
o arises by reason only of the member’s role as such a professional providing or performing, or assisting in the provision or performance of, those services to those persons;
o has been declared by the relevant Chair as an interest which
cannot reasonably be regarded as an interest more substantial than that of the majority of other persons who:–
are members of the same profession as the member in question,
are providing or performing, or assisting in the provision or performance of, such of those services as he/she provides or performs, or assists in the provision or performance of, for the benefit of persons for whom the Trust is responsible.
iv. Conditions which apply to the waiver and the removal of having a
pecuniary interest
The removal is subject to the following conditions:
o the member must disclose his/her interest as soon as practicable after the commencement of the meeting and this must be recorded in the minutes;
o the relevant Chair must consult the Chief Executive before
making a declaration in relation to the member in question pursuant to paragraph 7.3.iii above, except where that member is the Chief Executive;
o in the case of a meeting of the Board; the member may take part
in the consideration or discussion of the matter which must be subjected to a vote and the outcome recorded; but may not vote on any question with respect to it.
34
Page 255 of 300
73
o in the case of a meeting of the Committee; the member may take part in the consideration or discussion of the matter which must be subjected to a vote and the outcome recorded; may vote on any question with respect to it; but the resolution which is subject to the vote must comprise a recommendation to, and be referred for approval by, the Board.
7.4. Standards of Business Conduct
a. Trust Policy and National Guidance
i. Directors and Officers should comply with the NHS Foundation Trust
Code of Governance 2010 (revised 2013 and 2014) and/or subsequent iterations of the same document, the Code of Conduct for NHS Managers and any guidance and directions issued by NHS Improvement. This section of these Standing Orders should be read in conjunction with these documents.
ii. All Trust staff and members of must comply with the Trust’s Standards of Business Conduct Policy.
b. Interest of Officers in Contracts
i. Any officer or employee of the Trust who comes to know that the Trust
has entered into or proposes to enter into a contract in which he/she or any person connected with him/her (as defined in SO 7.3) has any pecuniary interest, direct or indirect, the Officer shall declare their interest by giving notice in writing of such fact to the Chief Executive or Trust Secretary as soon as practicable.
ii. An Officer should also declare to the Chief Executive any other employment or business or other relationship of his/her, or of a cohabiting spouse, that conflicts, or might reasonably be predicted could conflict with the interests of the Trust.
iii. The Trust will require interests, employment or relationships so
declared to be entered in a register of interests of staff.
c. Canvassing of and Recommendations by Members in Relation to Appointments
i. Canvassing of members of the Trust or of any Committee of the Trust
directly or indirectly for any appointment under the Trust shall disqualify the candidate for such appointment. The contents of this paragraph of the Standing Order shall be included in application forms or otherwise brought to the attention of candidates.
ii. Members of the Trust shall not solicit for any person any appointment under the Trust or recommend any person for such appointment; but this paragraph of this Standing Order shall not preclude a member from
35
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 256 of 300
74
giving written testimonial of a candidate’s ability, experience or character for submission to the Trust.
d. Relatives of Members or Officers
i. Candidates for any staff appointment under the Trust shall, when
making an application, disclose in writing to the Trust whether they are related to any member or the holder of any office under the Trust. Failure to disclose such a relationship shall disqualify a candidate and, if appointed, render him/her liable to instant dismissal.
ii. The Chair and every member and officer of the Trust shall disclose to the Board any relationship between themself and a candidate of whose candidature that member or officer is aware. It shall be the duty of the Chief Executive to report to the Board any such disclosure made.
iii. On appointment, members (and prior to acceptance of an appointment
in the case of Executive Directors) should disclose to the Trust whether they are related to any other member or holder of any office under the Trust.
iv. Where the relationship to a member of the Trust is disclosed, the
Standing Order headed ‘Disability of Chair and members in proceedings on account of pecuniary interest’ (SO 7) shall apply.
e. Acceptance of Gifts (see Standards of Business Conduct Policy)
Staff (including Non-Executive Directors and bank and agency staff) should not accept gifts in any form, whether from patients, patients' relatives or from potential suppliers, other than as provided below.
i. Gifts from suppliers or contractors Sussex Community NHS Foundation
Trust does business (or is likely to do business) with, or customers, should be declined, whatever the value. Subject to this, low cost branded promotional aids (such as calendars, diaries or other small gifts) may be accepted where they are valued at under £6 in total. Team or directorate gifts of low value, such as confectionary (up to approximately £20) intended to be shared by the team may also be accepted. Gifts accepted from suppliers in accordance with this provision must be declared to the Trust Secretary. A clear reason should be recorded as to why it was considered permissible to accept the gift, alongside the actual or estimated value and include line manager approval.
ii. Modest gifts from other sources (e.g. patients, families, service users,
foreign dignitaries) may be accepted up to a value of £50 and do need not be declared. Multiple gifts from the same source over a 12 month period should be declared where the cumulative value exceeds £50.
iii. Under no circumstances should staff solicit gifts of any kind.
36
Page 257 of 300
75
iv. Money should never be accepted as a personal gift and should be
refused. If, however, an individual offers to make a gift of money to the Trust, he/she should be referred to the Trust Secretary.
v. Any charitable donations of sums of money, cheques or gift vouchers
given to a member of staff must be passed to the Service Unit's Operations Manager for onward transmission to the Special Trustees. A receipt should be issued and letter of thanks sent.
vi. Where the donor specifies how the money is to be spent, his/her
wishes must be followed.
8. CUSTODY OF SEAL, SEALING OF DOCUMENTS AND SIGNATURE OF DOCUMENTS
8.1 Custody of Seal
The common seal of the Trust shall be kept by the Chief Executive or a
nominated Manager by him/her in a secure place.
8.2 Sealing of Documents Where it is necessary that a document shall be sealed, the seal shall be
affixed in the presence of two senior managers duly authorised by the Chief Executive, and not also from the originating department, and shall be attested by them.
8.3 Register of Sealing
The Chief Executive shall keep a register in which he/she, or another
manager of the Authority authorised by him/her, shall enter a record of the sealing of every document.
8.4 Signature of documents
a. Where any document will be a necessary step in legal proceedings on
behalf of the Trust, it shall, unless any enactment otherwise requires or authorises, be signed by the Chief Executive and/or any Executive Director(s).
b. In land transactions, the signing of certain supporting documents will be delegated to Managers and set out clearly in the Scheme of Delegation but will not include the main or principal documents effecting the transfer (e.g. sale/purchase agreement, lease, contracts for construction works and main warranty agreements or any document which is required to be executed as a deed).
c. The Chief Executive or nominated officers shall be authorised by the
Board, to sign on behalf of the Trust any agreement or other document
37
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 258 of 300
76
(not required to be executed as a deed) the subject matter of which has been approved by the Board or committee or sub-committee to which the Board has delegated appropriate authority.
d. For clinical negligence claims the authorised signatory for the claim is the
Chief Nurse, acting on behalf of the Trust’s solicitors. 9. DISPOSALS
Competitive tendering or quotation procedures shall not apply to the disposal of: a. any matter in respect of which a fair price can be obtained only by
negotiation or sale by auction as determined (or pre-determined in a reserve) by the Chief Executive or his nominated officer;
b. obsolete or condemned articles and stores, which may be disposed of in accordance with the supplies policy of the Trust;
c. items to be disposed of with an estimated sale value of less than £5,000; d. items arising from works of construction, demolition or site clearance,
which should be dealt with in accordance with the relevant contract; e. land or buildings concerning which Department of Health and Social
Care or other statutory body guidance has been issued but subject to compliance with such guidance.
10. IN-HOUSE SERVICES
10.1 In all cases where the Board of Directors determines that in-house services should be subject to competitive tendering the following groups shall be set up:
a. Specification group, comprising the Chief Executive or nominated officer/s and specialist.
b. In-house tender group, comprising a nominee of the Chief Executive and technical support.
c. Evaluation team, comprising normally a specialist officer, a supplies officer and the Chief Financial Officer or his nominated representative. For services having a likely annual expenditure exceeding £100,000, a non-officer member should be a member of the evaluation team.
10.2 All groups should work independently of each other. No officer is able to sit on both the in-house tender group and the evaluation group.
10.3 The evaluation team shall make recommendations to the Executive Leadership Team Meeting and / or the Board of Directors, in accordance with the Trust’s detailed scheme of delegation.
11. SIGNATURE OF DOCUMENTS
11.1 Where the signature of any document will be a necessary step in legal proceedings involving the Trust, it shall be signed by the Chief Executive, unless any enactment otherwise requires or authorises, or the Board of
38
Page 259 of 300
77
Directors shall have given the necessary authority to some other person for the purpose of such proceedings.
11.2 The Chief Executive or nominated officers shall be authorised, by resolution of the Board of Directors, to sign on behalf of the Trust any agreement or other document not requested to be executed as a deed, the subject matter of which has been approved by the Board of Directors or any committee or sub-committee with delegated authority.
12. MISCELLANEOUS
12.1 Standing Orders to be given to Board Members and Officers – It is the duty of the Chief Executive to ensure that existing Board Members and officers and all new appointees are notified of and understand their responsibilities within Standing Orders and Standing Financial Instructions. The current versions of Standing Orders, Standing Financial Instructions and the Scheme of Delegation will be available to staff at all times via the Trust’s intranet.
12.2 Documents having the standing of Standing Orders – Standing Financial Instructions and Reservation of Powers and Scheme of Delegation shall have effect as if incorporated into Standing Orders.
12.3 Review of Standing Orders – Standing Orders shall be reviewed as
required by the Audit Committee and Board of Directors. The requirement for review extends to all documents having the effect as if incorporated in Standing Orders.
12.4 Dispute Resolution – Where there is a dispute between the Board of
Directors and the Council of Governors, the procedure set out in the Constitution as at the date of the dispute should be referred to and followed.
12.5 Corporate Documents – Specific to the setting up of the Trust shall be
held in a secure place by the Chief Executive.
12.6 Indemnity Insurance – Members of the Board of Directors who act honestly and in good faith will not have to meet out of their personal resources any personal civil liability which is incurred in the execution or purported execution of their Board functions, save where they have acted recklessly. Any costs arising in this way will be met by the Trust and the Trust shall have the power to purchase suitable insurance to cover such costs.
13. RELATIONSHIP BETWEEN THE BOARD OF DIRECTORS AND THE
COUNCIL OF GOVERNORS
13.1 The Council of Governors will hold the Non-Executive Directors individually and collectively to account for the performance of the Board. The Council of Governors will work closely with the Board of Directors in
39
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 260 of 300
78
order to comply with the requirements of the National Health Service Act 2006, the Health and Social Care Act 2012 and the Provider Licence in all respects and in particular in relation to matters set out in the Constitution including those referred to in SOs 13.2 and 13.3 below.
13.2 The members of the Board of Directors, having regard to the views of the Council of Governors, are to prepare the information as to the Trust’s forward planning in respect of each financial year to be given to NHS Improvement.
13.3 The members of the Board of Directors are to present to the Council of
Governors at a general meeting, the Annual Accounts, any report of the auditor on them, the Annual Report and the Quality Report.
13.4 The annual reports are to give:
o information on any steps taken by the Trust to secure that (taken as a whole) the actual membership of its Public Constituency is representative of those eligible for such membership; and
o any other information NHS Improvement requires as specified in the Annual Reporting Manual published by NHS Improvement each year.
13.5 The Council of Governors may request that a matter which relates to the
annual accounts or forward planning for the Trust is included on the agenda for a meeting of the Board of Directors.
13.6 If the Council of Governors so desires such a matter as described within SO 13.5 to be included on an agenda, they shall make their request in writing to the Chair at least 10 clear days before the meeting of the Board and provide the information stipulated at SO 3.4. The Chair shall decide whether the matter is appropriate to be included on the agenda. Requests made less than 10 days before a meeting may be included on the agenda at the discretion of the Chair.
14. TENDERING AND CONTRACT PROCEDURE 14.1 All goods and services obtained by the Trust should be subject to either competitive quotations or competitive tendering subject to the financial limits specified in the Scheme of Delegation.
14.2 The procedure for entering into contracts by or on behalf of the Trust shall comply with these Standing Orders, and where appropriate European Union Directives on public sector purchasing promulgated by the Department of Health and Social Care (under HSG(95)38) prescribing procedures for awarding all forms of contracts, shall have effect as if incorporated in these Standing Orders. 14.3 The Trust shall comply as far as is practicable with the requirements of the Department of Health and Social Care "Capital Investment Manual" and “Estatecode” in respect of capital investment and estate and property transactions until such time as guidance is issued by NHS Improvement. In relation to investment decisions, the Trust will follow NHS Improvement’s
40
Page 261 of 300
79
guidance on ‘Risk Evaluation for Investment Decisions’ (REID), and reporting limits set out in the Compliance Framework. In the case of management consultancy contracts the Trust shall comply as far as is practicable with Department of Health and Social Care guidance "The Procurement and Management of Consultants within the NHS”. 14.4 Formal Competitive Tendering – The Trust shall ensure that competitive tenders are invited for the supply of goods, materials and manufactured articles and for the rendering of services including all forms of management consultancy services (other than specialised services sought from or provided by the Department of Health and Social Care); for the design, construction and maintenance of building and engineering works (including construction and maintenance of grounds and gardens); and for disposals. 14.5 Competitive quotations should be sought for all expenditure in excess of the limit specified in the Detailed Scheme of Delegation, and where 14.6 c applies. 14.6 Formal tendering and quotation procedures may be waived by officers to whom powers have been delegated by the Chief Executive without reference to the Chief Executive (except in (b) to (g) below) where: a. The estimated expenditure or income does not, or is not reasonably expected to, exceed the specified amount, (this figure to be reviewed annually); or b. where the supply is proposed under special arrangements negotiated by the Department of Health and Social Care in which event the said special arrangements must be complied with; c. the timescale genuinely precludes competitive tendering. Failure to plan the work properly is not a justification for single tender; d. specialist expertise is required and is available from only one source; e. the task is essential to complete the project, and arises as a consequence of a recently completed assignment and engaging different consultants for the new task would be inappropriate;
f. there is a clear benefit to be gained from maintaining continuity with an earlier project. However in such cases the benefits of such continuity must outweigh any potential financial advantage to be gained by competitive tendering; g. Where provided for in the Capital Investment Manual; h. Where the supply of goods or services is covered by an NHS Framework Agreement and the price is certain (i.e. quoted). 14.7 Unless one of the above applies, the limited application of the single tender rules should not be used to avoid competition or for administrative convenience or to award further work to a consultant originally appointed through a competitive
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 262 of 300
80
procedure. 14.8 Where it is decided that competitive tendering is not applicable and should be waived by virtue of (b) to (g) above the fact of the waiver and the reasons should be documented on a Single Tender or Quotation Action form (STA/SQA) and reported by the Chief Executive to the Executive Leadership Team. All such waivers (STA/SQA’s) should also be reported at the next available meeting of the Audit Committee. 14.9 The Trust shall use NHS SupplyChain or contracts or frameworks let by other collaborative organisations for procurement of all goods and services unless the Chief Executive or nominated officers deem it inappropriate. 14.10 There are a number of instances when formal tenders or quotes need not be sought as follows:- a. Agency/Consultancy Staff – where the good/service purchased are staffing expertise or agency staff or expenditure in relation to training or training courses. b. Part order or call-off order from tendered contract c. Specialist training course d. Specialist research 14.11 The Trust shall ensure that invitations to tender are sent to a sufficient number of firms/individuals to provide fair and adequate competition as appropriate, and in no case less than three firms/individuals, having regard to their capacity to supply the goods or materials or to undertake the services or works required. 14.12 The Trust shall ensure that normally the firms/individuals invited to tender (and where appropriate, quote) are among those on approved lists compiled. As an alternative to maintaining its own list the Trust may, where appropriate approve a list prepared by or for another body. Where in the opinion of the Chief Finance Officer it is desirable to seek tenders from firms not on the approved lists, the reason shall be recorded in writing to the Chief Executive for approval.
14.13 Where quotations are required under Standing Order 14.5 they should be obtained from at least three firms/individuals based on specifications or terms of reference prepared by, or on behalf of, the Trust. 14.14 Both tenders and quotations should be requested electronically using the Trust’s e-tendering system 14.15 All tenders and quotations should be treated as confidential and should be retained for inspection. 14.16 The Chief Executive or the nominated officer (via the scheme of delegation) should select the tender or quotation which gives the best quality and
Page 263 of 300
81
value for money. If this is not the lowest then this fact and the reasons why the lowest offer was not chosen should be stated in a permanent record. 14.17 Non-competitive quotations in writing may be obtained for the following purposes: a. the supply of goods/services of a special character for which it is not, in the opinion of the Chief Executive or the nominated officer, b. possible or desirable to obtain competitive quotations; the goods/services are required urgently. 14.18 The Chief Executive shall be responsible for ensuring that best value for money can be demonstrated for all services provided under contract or in-house. The Trust may also determine from time to time that in-house services should be market tested by competitive tendering (Standing Order 10). 14.19 Private Finance/Procure 21 The Trust may consider using PFI/Procure 21 when considering a capital procurement. When the Board proposes that PFI/Procure 21 be considered: a. The Chief Executive shall demonstrate that the scheme represents value for money and genuinely transfers risk to the private sector. b. The proposal must be specifically agreed by the Board. c. Trust competitive tendering/quotations procedures should apply where necessary. 14.20 Contracts – The Board of Directors may only enter into contracts on behalf of the Trust within the statutory powers delegated to it and shall comply with: a. these Standing Orders; b. the Trust’s Standing Financial Instructions; c. any relevant statutory provisions; d. any relevant and mandatory directions including NHS Improvement’s guidance on Risk Evaluation for Investment Decisions, the Department of Health and Social Care’s Capital Investment Manual, Estate Code and guidance on the
Procurement and Management of Consultants; e. such of the NHS Standard Contract Conditions as are applicable. Where appropriate, contracts shall be in or embody the same terms and conditions of contract as was the basis on which tenders or quotations were invited. 14.21 In all contracts made by the Trust, the Board of Directors shall endeavour to obtain best value for money. The Chief Executive shall nominate an officer who shall oversee and manage each contract on behalf of the Trust. 14.22 Personnel and Agency or Temporary Staff Contracts – The Chief Executive shall nominate officers with delegated authority to enter into contracts of employment, regarding staff, agency staff or temporary staff service contracts.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 264 of 300
82
14.23 Legally Binding Contracts (LBC) for the provision of Healthcare – Legally binding contracts for the supply of healthcare services shall be drawn up in accordance with Legal Advice, best practice and where possible use the model contract for Acute NHSFTs. These legally binding contracts will be administered by the Trust. 14.24 Cancellation of Contracts – Except where specific provision is made in model Forms of Contracts or standard Schedules of Conditions approved for use within the NHS, there shall be inserted in every written contract a clause empowering the Trust to cancel the contract and to recover from the contractor the amount of any loss resulting from such cancellation, if the contractor shall have offered, or given or agreed to give, any person any gift or consideration of any kind as an inducement or reward for doing or forbearing to do or for having done or forborne to do any action in relation to the obtaining or execution of the contract or any other contract with the Trust, or for showing or forbearing to show favour or disfavour to any person in relation to the contracts or any other contract with the Trust, or if the like acts shall have been done by any person employed by them or acting on their behalf (whether with or without the knowledge of the contractor), or if in relation to any contract with the Trust the contractor or any person employed by them or acting on their behalf shall have committed any offence under the Prevention of Corruption Acts 1889 and 1916 an other appropriate legislation. 14.25 Determination of Contracts for Failure to Deliver Goods or Materials – There shall be inserted in every written contract for the supply of goods or materials a clause to secure that, should the contractor fail to deliver the goods or materials or any portion thereof within the time or times specified in the contract, the Trust may without prejudice determine the contract either wholly or to the extent of such default and purchase other goods, or material of similar description to make good (a) such default, or (b) in the event of the contract being wholly determined the goods or materials remaining to be delivered. The clause shall further secure that the amount by which the cost of so purchasing other goods or materials exceeds the amount which would have been payable to the contractor in respect of the goods or materials shall be recoverable from the contractor. 14.26 Contracts involving Funds Held on Trust – shall do so individually to a specific named fund. Such contracts involving charitable funds shall comply with
the requirements of the Charities Act.
Page 265 of 300
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
3 o
f 117
RE
SE
RV
AT
ION
AN
D D
EL
EG
AT
ION
OF
PO
WE
RS
S
CH
EM
E O
F R
ES
ER
VA
TIO
N A
ND
DE
LE
GA
TIO
N (
DE
CIS
ION
S R
ES
ER
VE
D T
O T
HE
BO
AR
D)
RE
F
TH
E B
OA
RD
D
EC
ISIO
NS
RE
SE
RV
ED
TO
TH
E B
OA
RD
N/A
T
HE
BO
AR
D
Ge
ne
ral E
nab
lin
g P
rov
isio
ns
Th
e T
rust
Bo
ard
ma
y d
ete
rmin
e a
ny m
att
er,
fo
r w
hic
h it
ha
s d
ele
ga
ted
or
sta
tuto
ry a
uth
ori
ty,
it
wis
he
s in
full
se
ssio
n w
ith
in its
sta
tuto
ry p
ow
ers
.
AP
PE
ND
IX 2
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 266 of 300

ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
4 o
f 117
RE
F
TH
E B
OA
RD
D
EC
ISIO
NS
RE
SE
RV
ED
TO
TH
E B
OA
RD
N/A
T
HE
BO
AR
D
Re
gu
lati
on
s a
nd
Co
ntr
ol
Ap
pro
ve
Sta
nd
ing
Ord
ers
(S
Os),
a s
ch
ed
ule
of m
att
ers
re
se
rve
d to
th
e B
oa
rd a
nd
Sta
nd
ing
Fin
an
cia
l In
str
uctio
ns f
or
the
re
gu
latio
n o
f its p
roce
ed
ing
s a
nd
bu
sin
ess.
Su
sp
en
d S
tan
din
g O
rde
rs.
Va
ry o
r a
me
nd
th
e S
tan
din
g O
rde
rs.
Ra
tify
an
y u
rge
nt
de
cis
ion
s t
ake
n b
y t
he
Ch
air
an
d C
hie
f E
xe
cu
tive
in
pu
blic s
essio
n in
acco
rda
nce
with
SO
.
Ap
pro
ve
a s
ch
em
e o
f d
ele
ga
tio
n o
f p
ow
ers
fro
m t
he
Bo
ard
to
co
mm
itte
es.
Re
qu
ire
an
d r
ece
ive
th
e d
ecla
ratio
n o
f B
oa
rd m
em
be
rs’ i
nte
rests
th
at m
ay c
on
flic
t w
ith
th
ose
of
Tru
st
an
d d
ete
rmin
ing
th
e e
xte
nt
to w
hic
h t
ha
t m
em
be
r m
ay r
em
ain
in
vo
lve
d w
ith
th
e m
att
er
un
de
r co
nsid
era
tio
n.
Re
qu
ire
an
d r
ece
ive
th
e d
ecla
ratio
n o
f o
ffic
ers
’ in
tere
sts
th
at
ma
y c
on
flic
t w
ith
th
ose
of
the
Tru
st.
Ap
pro
ve
arr
an
ge
me
nts
fo
r d
ea
lin
g w
ith
co
mp
lain
ts.
Ad
op
t th
e o
rga
nis
atio
n s
tru
ctu
res, p
roce
sse
s a
nd
pro
ce
du
res to
fa
cili
tate
th
e d
isch
arg
e o
f b
usin
ess
by th
e T
rust
an
d t
o a
gre
e m
odific
ations th
ere
to.
Re
ce
ive
re
po
rts fro
m c
om
mitte
es in
clu
din
g th
ose
th
at th
e T
rust is
re
qu
ire
d b
y th
e S
ecre
tary
of S
tate
or
oth
er
reg
ula
tio
n to
esta
blis
h a
nd
to
ta
ke
ap
pro
pri
ate
actio
n o
n.
Co
nfirm
th
e re
co
mm
en
da
tio
ns o
f th
e T
rust’s c
om
mitte
es w
he
re th
e c
om
mitte
es d
o n
ot h
ave
exe
cu
tive
pow
ers
.
Ap
pro
ve
arr
an
ge
me
nts
re
latin
g t
o t
he
dis
ch
arg
e o
f th
e B
oa
rd’s
re
sp
on
sib
ilitie
s a
s a
co
rpo
rate
tr
uste
e f
or f
un
ds h
eld
on
tru
st.
Esta
blis
h t
erm
s o
f re
fere
nce
an
d r
ep
ort
ing
arr
an
ge
me
nts
of
all
co
mm
itte
es a
nd
su
b-c
om
mitte
es
tha
t are
esta
blis
hed b
y the B
oard
.
Ap
pro
ve
arr
an
ge
me
nts
re
latin
g t
o t
he
dis
ch
arg
e o
f th
e T
rust’s r
esp
on
sib
ilitie
s a
s a
ba
iler
for
pa
tie
nts
’ pro
pe
rty.
Au
tho
rise
use
of
the
se
al.
Ra
tify
or
oth
erw
ise
of
failu
re t
o c
om
ply
with
Sta
nd
ing
Ord
ers
bro
ug
ht
to t
he
Ch
ief
Exe
cu
tive
’s
att
en
tio
n in
acco
rda
nce
with
SO
s.
Dis
cip
lin
e m
em
be
rs o
f th
e B
oa
rd o
r e
mp
loye
es w
ho
are
in
bre
ach
of
sta
tuto
ry r
eq
uir
em
en
ts o
r
SO
s.
Page 267 of 300

ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
5 o
f 117
RE
F
TH
E B
OA
RD
D
EC
ISIO
NS
RE
SE
RV
ED
TO
TH
E B
OA
RD
N/A
T
HE
BO
AR
D
Ap
po
intm
en
ts / D
ism
iss
al
Ap
po
int
an
d d
ism
iss c
om
mitte
es (
an
d in
div
idu
al m
em
be
rs)
tha
t a
re d
ire
ctly a
cco
un
tab
le t
o t
he
Bo
ard
.
Dis
mis
s E
xe
cu
tive
Dir
ecto
rs
Co
nfirm
ap
po
intm
en
t o
f m
em
be
rs o
f a
ny c
om
mitte
e o
f th
e T
rust
as r
ep
rese
nta
tive
s o
n o
uts
ide
b
od
ies.
Dis
mis
s th
e T
rust
Se
cre
tary
(if th
e a
pp
oin
tme
nt o
f a
Tru
st S
ecre
tary
is r
eq
uir
ed
un
de
r S
tan
din
g
Ord
ers
).
N/A
T
HE
BO
AR
D
Str
ate
gy
, P
lan
s a
nd
Bu
dg
ets
De
fin
e t
he
str
ate
gic
aim
s a
nd
ob
jective
s o
f th
e T
rust.
Ap
pro
ve
pro
po
sa
ls f
or
en
su
rin
g q
ua
lity a
nd
de
ve
lop
ing
clin
ica
l g
ove
rna
nce
in
se
rvic
es p
rovid
ed
by
the
Tru
st,
ha
vin
g r
eg
ard
to
an
y g
uid
an
ce
issu
ed
by t
he
Se
cre
tary
of
Sta
te.
Ap
pro
ve
th
e T
rust’s p
olicie
s a
nd
pro
ce
du
res f
or
the
ma
na
ge
me
nt
of
risk.
Ap
pro
ve
Ou
tlin
e a
nd
Fin
al B
usin
ess C
ase
s f
or
Ca
pita
l In
ve
stm
en
t.
Ap
pro
ve
Tru
st’s b
ud
ge
t.
Ap
pro
ve
an
nu
ally T
rust’s p
rop
ose
d o
rga
nis
atio
na
l d
eve
lop
me
nt
pro
po
sa
ls.
Ra
tify
pro
po
sa
ls f
or
acq
uis
itio
n,
dis
po
sa
l o
r ch
an
ge
of
use
of
lan
d a
nd
/or
bu
ild
ing
s.
Ap
pro
ve
PF
I p
rop
osa
ls.
Ap
pro
ve
th
e o
pe
nin
g o
f b
an
k a
cco
un
ts.
Ap
pro
ve
pro
po
sa
ls o
n in
div
idu
al co
ntr
acts
(o
the
r th
an
NH
S c
on
tra
cts
) o
f a
ca
pita
l o
r re
ve
nu
e
na
ture
am
ou
ntin
g t
o,
or
like
ly t
o a
mo
un
t to
ove
r £
1.5
millio
n o
ve
r a
3 y
ea
r p
eri
od
.
Ap
pro
ve
pro
po
sa
ls in
in
div
idu
al ca
se
s f
or
the
wri
te o
ff o
f lo
sse
s o
r m
akin
g o
f sp
ecia
l p
aym
en
ts
ab
ove
th
e lim
its o
f d
ele
ga
tio
n t
o t
he
Ch
ief
Exe
cu
tive
an
d C
hie
f F
ina
ncia
l O
ffic
er
(fo
r lo
sse
s a
nd
sp
ecia
l p
aym
en
ts)
pre
vio
usly
ap
pro
ve
d b
y t
he
Bo
ard
.
Ap
pro
ve
in
div
idu
al co
mp
en
sa
tio
n p
aym
en
ts (
Re
mu
ne
ratio
n C
om
mitte
e f
or
red
un
da
ncy
co
mp
en
sa
tio
n).
Ap
pro
ve
pro
po
sa
ls f
or
actio
n in
litig
atio
n a
ga
inst
or
on
be
ha
lf o
f th
e T
rust.
N/A
T
HE
CO
UN
CIL
OF
GO
VE
RN
OR
S
Au
dit
Ap
pro
ve
th
e a
pp
oin
tme
nt
(an
d w
he
re n
ece
ssa
ry d
ism
issa
l) o
f E
xte
rna
l A
ud
ito
rs.
De
pu
ty C
ha
ir
Ap
po
int
on
e o
f th
e N
ED
s (
oth
er
tha
n t
he
Ch
air
) a
s t
he
De
pu
ty C
ha
ir o
f th
e B
oa
rd.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 268 of 300
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
6 o
f 117
RE
F
TH
E B
OA
RD
D
EC
ISIO
NS
RE
SE
RV
ED
TO
TH
E B
OA
RD
N/A
T
HE
BO
AR
D
Au
dit
Ap
pro
va
l o
f e
xte
rna
l a
ud
ito
rs’ a
rra
ng
em
en
ts f
or
the
se
pa
rate
in
de
pe
nd
en
t e
xa
min
atio
n o
f fu
nd
s
he
ld o
n t
rust,
an
d t
he
su
bm
issio
n o
f re
po
rts t
o t
he
Au
dit C
om
mitte
e m
ee
tin
gs w
ho
will
ta
ke
ap
pro
pri
ate
actio
n.
Re
ce
ipt
of
the
an
nu
al m
an
ag
em
en
t le
tte
r re
ce
ive
d f
rom
th
e e
xte
rna
l a
ud
ito
r a
nd
ag
ree
me
nt
of
pro
po
se
d a
ctio
n,
takin
g a
cco
un
t o
f th
e a
dvic
e,
wh
ere
ap
pro
pri
ate
, o
f th
e A
ud
it C
om
mitte
e.
Re
ce
ive
an
an
nu
al re
po
rt f
rom
th
e I
nte
rna
l A
ud
ito
r (H
ea
d o
f In
tern
al A
ud
it O
pin
ion
) a
nd
ag
ree
actio
n o
n r
eco
mm
en
da
tio
ns w
he
re a
pp
rop
ria
te o
f th
e A
ud
it C
om
mitte
e
N/A
T
HE
BO
AR
D
An
nu
al R
ep
ort
s a
nd
Ac
co
un
ts
Re
ce
ipt
an
d a
pp
rova
l o
f th
e A
nn
ua
l R
ep
ort
an
d A
cco
un
ts f
or
fun
ds h
eld
on
tru
st.
N/A
T
HE
BO
AR
D
Mo
nit
ori
ng
Re
ce
ive
of su
ch
re
po
rts a
s th
e B
oa
rd s
ee
s fit fro
m c
om
mitte
es in
re
sp
ect o
f th
eir
exe
rcis
e o
f p
ow
ers
dele
gate
d.
Co
ntin
uo
us a
pp
rais
al
of
the
aff
air
s o
f th
e T
rust
by m
ea
ns o
f th
e p
rovis
ion
to
th
e B
oa
rd a
s t
he
Bo
ard
ma
y r
eq
uir
e f
rom
dir
ecto
rs,
co
mm
itte
es,
an
d o
ffic
ers
of
the
Tru
st
as s
et
ou
t in
ma
na
ge
me
nt
po
licy s
tate
me
nts
. A
ll m
on
ito
rin
g r
etu
rns r
eq
uir
ed
by t
he
De
pa
rtm
en
t o
f H
ea
lth
an
d t
he
Ch
ari
ty
Co
mm
issio
n s
ha
ll b
e r
ep
ort
ed
, a
t le
ast
in s
um
ma
ry,
to t
he
Bo
ard
.
Re
ce
ive
re
po
rts f
rom
th
e C
hie
f F
ina
ncia
l O
ffic
er
on
fin
an
cia
l p
erf
orm
an
ce
ag
ain
st
bu
dg
et
an
d
Lo
ca
l D
elive
ry P
lan
an
d a
lso
on
actu
al a
nd
fo
reca
st
inco
me
fro
m S
LA
.
DE
CIS
ION
S/D
UT
IES
DE
LE
GA
TE
D B
Y T
HE
BO
AR
D T
O C
OM
MIT
TE
ES
RE
F
CO
MM
ITT
EE
D
EC
ISIO
NS
/DU
TIE
S D
EL
EG
AT
ED
BY
TH
E B
OA
RD
TO
CO
MM
ITT
EE
S
SF
I A
UD
IT C
OM
MIT
TE
E
Th
e C
om
mitte
e w
ill:
Exa
min
e a
nd
re
po
rt o
n t
he
in
teg
rity
of
the
fin
an
cia
l sta
tem
en
t o
f th
e T
rust.
Exa
min
e a
nd
re
po
rt o
n t
he
eff
ective
ne
ss o
f in
tern
al co
ntr
ols
.
Exa
min
e a
nd
re
po
rt o
n t
he
in
tern
al a
nd
exte
rna
l a
ud
it f
un
ctio
ns.
Ap
pro
ve
th
e T
rust’s a
nn
ua
l re
po
rt a
nd
acco
un
ts a
nd
Qu
ality
Acco
un
ts.
Pro
vid
e a
ssura
nce
on th
e e
ffectiveness o
f th
e T
rust’s g
overn
ance
str
uctu
res, assu
rance
pro
cesses a
nd r
isk m
anage
ment acro
ss th
e w
ho
le o
f th
e T
rust’s a
ctivitie
s, in
clu
din
g Info
rmation
Go
vern
ance.
Page 269 of 300
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
7 o
f 117
SF
I B
OA
RD
NO
MIN
AT
ION
S
AN
D R
EM
UN
ER
AT
ION
C
OM
MIT
TE
E
Th
e C
om
mitte
e w
ill, a
ctin
g w
ith
th
e B
oa
rd’s
de
leg
ate
d a
uth
ori
ty:
Se
t a
pp
rop
ria
te r
em
un
era
tio
n a
nd
te
rms o
f se
rvic
e f
or
the
Ch
ief
Exe
cu
tive
, o
the
r E
xe
cu
tive
Dir
ecto
rs a
nd
oth
er
se
nio
r e
mp
loye
es in
clu
din
g;
all a
sp
ects
of
sa
lary
(in
clu
din
g
an
y p
erf
orm
an
ce
re
late
d e
lem
en
ts/b
on
use
s);
Ma
ke
pro
vis
ion
s f
or
oth
er
be
ne
fits
, in
clu
din
g p
en
sio
ns a
nd
ca
rs;
Ma
ke
arr
an
ge
me
nts
fo
r te
rmin
atio
n o
f e
mp
loym
en
t a
nd
oth
er
co
ntr
actu
al te
rms.
SC
HE
ME
OF
DE
LE
GA
TIO
N D
ER
IVE
D F
RO
M T
HE
AC
CO
UN
TIN
G O
FF
ICE
R M
EM
OR
AN
DU
M
RE
F
DE
LE
GA
TE
D T
O
DU
TIE
S D
EL
EG
AT
ED
7
CH
IEF
EX
EC
UT
IVE
A
cco
un
tab
le t
hro
ug
h N
HS
Acco
un
tin
g O
ffic
er
to P
arl
iam
en
t fo
r ste
wa
rdsh
ip o
f T
rust
reso
urc
es.
9
CH
IEF
EX
EC
UT
IVE
&
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
En
su
re t
he
acco
un
ts o
f th
e T
rust
are
pre
pa
red
un
de
r p
rin
cip
les a
nd
in
a f
orm
at
dir
ecte
d b
y t
he
S
ecre
tary
of
Sta
te.
Acco
un
ts m
ust
dis
clo
se
a t
rue
an
d f
air
vie
w o
f th
e T
rust’s in
co
me
an
d e
xp
en
ditu
re a
nd
its
sta
te o
f
aff
air
s.
Sig
n t
he
acco
un
ts o
n b
eh
alf o
f th
e B
oa
rd.
10
CH
IEF
EX
EC
UT
IVE
S
ign
a s
tate
me
nt
in t
he
an
nu
al re
po
rt a
nd
acco
un
ts o
utlin
ing
re
sp
on
sib
ilitie
s a
s t
he
Acco
un
tin
g
Off
ice
r.
Sig
n a
sta
tem
en
t in
th
e a
nn
ua
l re
po
rt a
nd
acco
un
ts o
utlin
ing
re
sp
on
sib
ilitie
s in
re
sp
ect
of
Inte
rna
l
Co
ntr
ol.
Sig
n t
he
qu
ality
re
po
rt
12
C
HIE
F E
XE
CU
TIV
E
En
su
re e
ffe
ctive
ma
na
ge
me
nt
syste
ms t
ha
t sa
feg
ua
rd p
ub
lic f
un
ds a
nd
assis
t th
e T
rust
Ch
air
to
imp
lem
en
t re
qu
ire
me
nts
of
co
rpo
rate
go
ve
rna
nce
in
clu
din
g e
nsu
rin
g m
an
ag
ers
:
Ha
ve
a c
lea
r vie
w o
f th
eir
ob
jective
s a
nd
th
e m
ea
ns t
o a
sse
ss a
ch
ieve
me
nts
in
re
latio
n t
o
tho
se
ob
jective
s;
Be
assig
ne
d w
ell
de
fin
ed
re
sp
on
sib
ilitie
s f
or
ma
kin
g b
est
use
of
reso
urc
es;
Ha
ve
th
e in
form
atio
n,
tra
inin
g a
nd
acce
ss t
o t
he
exp
ert
ad
vic
e t
he
y n
ee
d t
o e
xe
rcis
e t
he
ir
resp
on
sib
ilitie
s e
ffe
ctive
ly.
12
CH
AIR
Im
ple
me
nt
req
uir
em
en
ts o
f co
rpo
rate
go
ve
rna
nce
.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 270 of 300
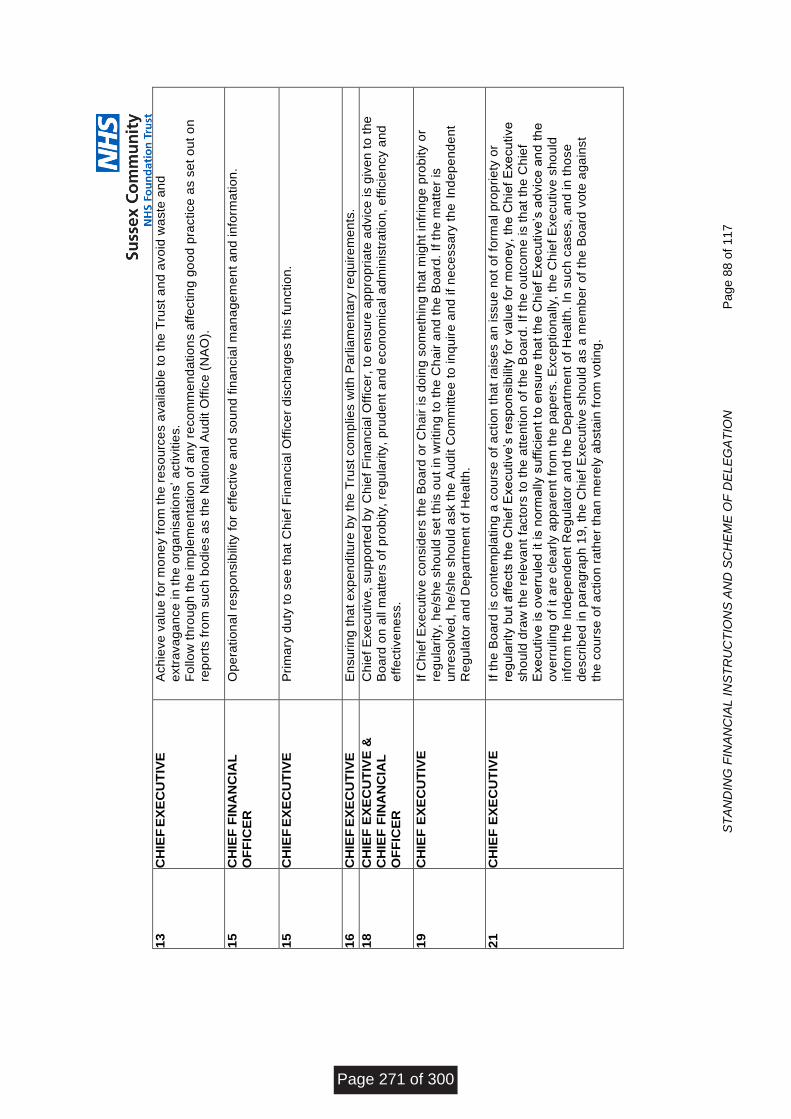
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
8 o
f 117
13
CH
IEF
EX
EC
UT
IVE
A
ch
ieve
va
lue
fo
r m
on
ey f
rom
th
e r
eso
urc
es a
va
ila
ble
to
th
e T
rust
an
d a
vo
id w
aste
an
d
extr
ava
ga
nce
in
th
e o
rga
nis
atio
ns’ a
ctivitie
s.
Fo
llo
w t
hro
ug
h t
he
im
ple
me
nta
tio
n o
f a
ny r
eco
mm
en
da
tio
ns a
ffe
ctin
g g
oo
d p
ractice
as s
et
ou
t o
n
rep
ort
s f
rom
su
ch
bo
die
s a
s t
he
Na
tio
na
l A
ud
it O
ffic
e (
NA
O).
15
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
O
pe
ratio
na
l re
sp
on
sib
ility
fo
r e
ffe
ctive
an
d s
ou
nd
fin
an
cia
l m
an
ag
em
en
t a
nd
in
form
atio
n.
15
CH
IEF
EX
EC
UT
IVE
P
rim
ary
du
ty t
o s
ee
th
at
Ch
ief
Fin
an
cia
l O
ffic
er
dis
ch
arg
es t
his
fu
nctio
n.
16
CH
IEF
EX
EC
UT
IVE
E
nsu
rin
g t
ha
t e
xp
en
ditu
re b
y t
he
Tru
st
co
mp
lie
s w
ith
Pa
rlia
me
nta
ry r
eq
uir
em
en
ts.
18
CH
IEF
EX
EC
UT
IVE
&
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
Ch
ief
Exe
cu
tive
, su
pp
ort
ed
by C
hie
f F
ina
ncia
l O
ffic
er,
to
en
su
re a
pp
rop
ria
te a
dvic
e is g
ive
n t
o t
he
B
oa
rd o
n a
ll m
att
ers
of
pro
bity,
reg
ula
rity
, p
rud
en
t a
nd
eco
no
mic
al a
dm
inis
tra
tio
n,
eff
icie
ncy a
nd
eff
ective
ne
ss.
19
CH
IEF
EX
EC
UT
IVE
If
Ch
ief
Exe
cu
tive
co
nsid
ers
th
e B
oa
rd o
r C
ha
ir is d
oin
g s
om
eth
ing
th
at
mig
ht
infr
ing
e p
rob
ity o
r
reg
ula
rity
, h
e/s
he
sh
ou
ld s
et
this
ou
t in
wri
tin
g t
o t
he
Ch
air
an
d t
he
Bo
ard
. If
th
e m
att
er
is
un
reso
lve
d,
he
/sh
e s
ho
uld
ask t
he
Au
dit C
om
mitte
e t
o in
qu
ire
an
d if
ne
ce
ssa
ry t
he
In
de
pe
nd
en
t
Re
gu
lato
r a
nd
De
pa
rtm
en
t o
f H
ea
lth
.
21
CH
IEF
EX
EC
UT
IVE
If
th
e B
oa
rd is c
on
tem
pla
tin
g a
co
urs
e o
f a
ctio
n t
ha
t ra
ise
s a
n issu
e n
ot
of
form
al p
rop
rie
ty o
r
reg
ula
rity
bu
t a
ffe
cts
th
e C
hie
f E
xe
cu
tive
’s r
esp
on
sib
ility
fo
r va
lue
fo
r m
on
ey,
the
Ch
ief
Exe
cu
tive
sh
ou
ld d
raw
th
e r
ele
va
nt
facto
rs t
o t
he
att
en
tio
n o
f th
e B
oa
rd.
If t
he
ou
tco
me
is t
ha
t th
e C
hie
f
Exe
cu
tive
is o
ve
rru
led
it
is n
orm
ally s
uff
icie
nt
to e
nsu
re t
ha
t th
e C
hie
f E
xe
cu
tive
’s a
dvic
e a
nd
th
e
ove
rru
lin
g o
f it a
re c
lea
rly a
pp
are
nt
fro
m t
he
pa
pe
rs.
Exce
ptio
na
lly,
the
Ch
ief
Exe
cu
tive
sh
ou
ld
info
rm t
he
In
de
pe
nd
en
t R
eg
ula
tor
an
d t
he
De
pa
rtm
en
t o
f H
ea
lth
. In
su
ch
ca
se
s,
an
d in
th
ose
de
scri
be
d in
pa
rag
rap
h 1
9,
the
Ch
ief
Exe
cu
tive
sh
ou
ld a
s a
me
mb
er
of
the
Bo
ard
vo
te a
ga
inst
the
co
urs
e o
f a
ctio
n r
ath
er
tha
n m
ere
ly a
bsta
in f
rom
vo
tin
g.
Page 271 of 300
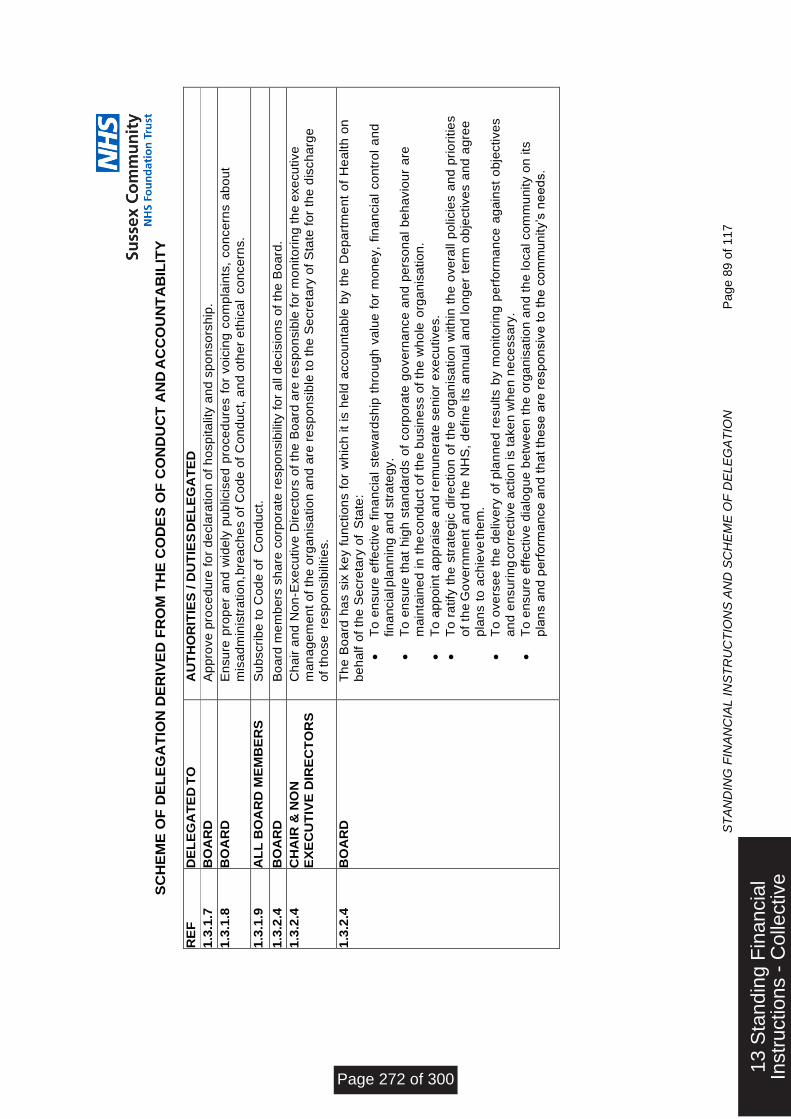
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 8
9 o
f 117
SC
HE
ME
OF
DE
LE
GA
TIO
N D
ER
IVE
D F
RO
M T
HE
CO
DE
S O
F C
ON
DU
CT
AN
D A
CC
OU
NT
AB
ILIT
Y
RE
F
DE
LE
GA
TE
D T
O
AU
TH
OR
ITIE
S / D
UT
IES
DE
LE
GA
TE
D
1.3
.1.7
B
OA
RD
A
pp
rove
pro
ce
du
re f
or
de
cla
ratio
n o
f h
osp
ita
lity
an
d s
po
nso
rsh
ip.
1.3
.1.8
B
OA
RD
E
nsu
re p
rop
er
an
d w
ide
ly p
ub
licis
ed
pro
ce
du
res f
or
vo
icin
g c
om
pla
ints
, co
nce
rns a
bo
ut
mis
ad
min
istr
atio
n, b
rea
ch
es o
f C
od
e o
f C
on
du
ct,
an
d o
the
r e
thic
al
co
nce
rns.
1.3
.1.9
A
LL
BO
AR
D M
EM
BE
RS
S
ub
scri
be
to
Co
de
of
Co
nd
uct.
1.3
.2.4
B
OA
RD
B
oa
rd m
em
be
rs s
ha
re c
orp
ora
te r
esp
on
sib
ility
fo
r a
ll d
ecis
ion
s o
f th
e B
oa
rd.
1.3
.2.4
C
HA
IR &
NO
N
EX
EC
UT
IVE
DIR
EC
TO
RS
C
ha
ir a
nd
No
n-E
xe
cu
tive
Dir
ecto
rs o
f th
e B
oa
rd a
re r
esp
on
sib
le f
or
mo
nito
rin
g t
he
exe
cu
tive
m
an
ag
em
en
t o
f th
e o
rga
nis
atio
n a
nd
are
re
sp
on
sib
le t
o t
he
Se
cre
tary
of
Sta
te f
or
the
dis
ch
arg
e
of
tho
se
re
sp
on
sib
ilitie
s.
1.3
.2.4
B
OA
RD
T
he
Bo
ard
ha
s s
ix k
ey f
un
ctio
ns f
or
wh
ich
it
is h
eld
acco
un
tab
le b
y t
he
De
pa
rtm
en
t o
f H
ea
lth
on
be
ha
lf o
f th
e S
ecre
tary
of
Sta
te:
To
en
su
re e
ffe
ctive
fin
an
cia
l ste
wa
rdsh
ip t
hro
ug
h v
alu
e f
or
mo
ne
y,
fin
an
cia
l co
ntr
ol
an
d
fin
an
cia
l pla
nn
ing
an
d s
tra
teg
y.
To
en
su
re t
ha
t h
igh
sta
nd
ard
s o
f co
rpo
rate
go
ve
rna
nce
an
d p
ers
on
al
be
ha
vio
ur
are
ma
inta
ine
d in
th
e c
on
du
ct
of
the
bu
sin
ess o
f th
e w
ho
le o
rga
nis
atio
n.
To
ap
po
int
ap
pra
ise
an
d r
em
un
era
te s
en
ior
exe
cu
tive
s.
To
ra
tify
th
e s
tra
teg
ic d
ire
ctio
n o
f th
e o
rga
nis
atio
n w
ith
in t
he
ove
rall p
olicie
s a
nd
pri
ori
tie
s
of
the
Go
ve
rnm
en
t a
nd
th
e N
HS
, d
efin
e its
an
nu
al
an
d lo
ng
er
term
ob
jective
s a
nd
ag
ree
pla
ns t
o a
ch
ieve
the
m.
To
ove
rse
e t
he
de
live
ry o
f p
lan
ne
d r
esu
lts b
y m
on
ito
rin
g p
erf
orm
an
ce
ag
ain
st
ob
jective
s
an
d e
nsu
rin
g c
orr
ective
actio
n is t
ake
n w
he
n n
ece
ssa
ry.
To
en
su
re e
ffe
ctive
dia
log
ue
be
twe
en
th
e o
rga
nis
atio
n a
nd
th
e lo
ca
l co
mm
un
ity o
n its
pla
ns a
nd
pe
rfo
rma
nce
an
d t
ha
t th
ese
are
re
sp
on
siv
e t
o t
he
co
mm
un
ity’s
ne
ed
s.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 272 of 300
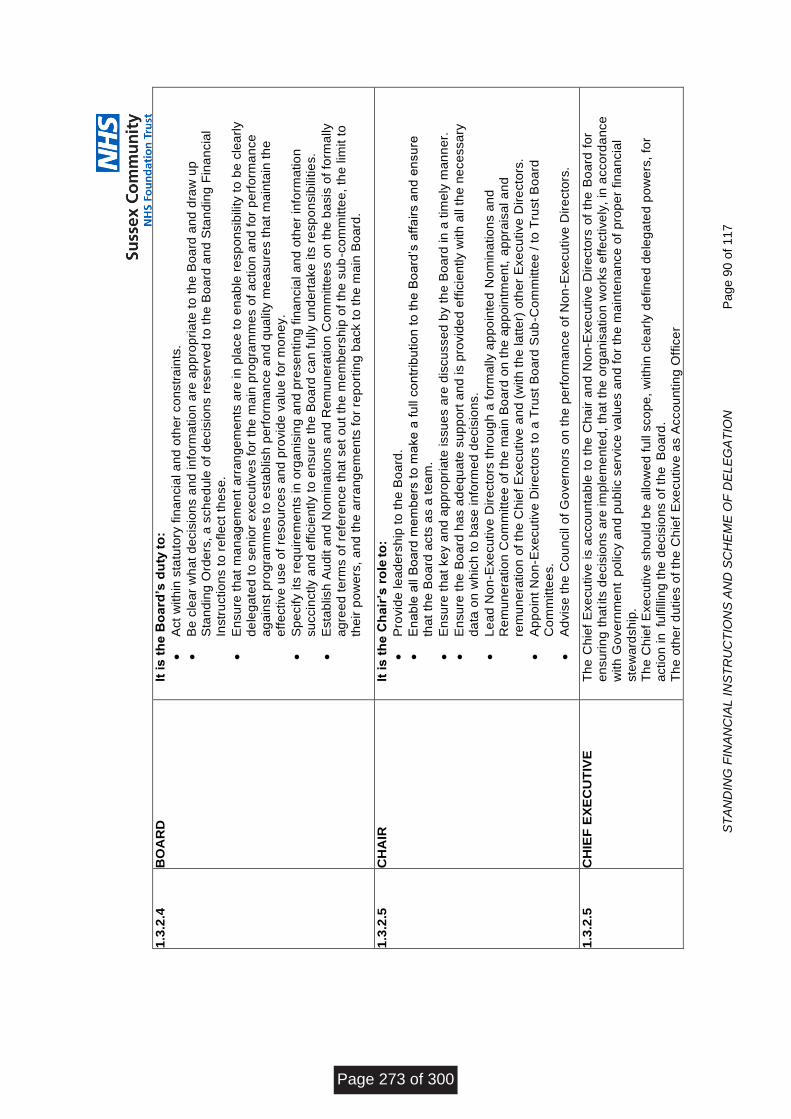
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
0 o
f 117
1.3
.2.4
B
OA
RD
It
is
th
e B
oa
rd’s
du
ty to
:
Act
with
in s
tatu
tory
fin
an
cia
l a
nd
oth
er
co
nstr
ain
ts.
Be
cle
ar
wh
at
de
cis
ion
s a
nd
in
form
atio
n a
re a
pp
rop
ria
te t
o t
he
Bo
ard
an
d d
raw
up
S
tan
din
g O
rde
rs,
a s
ch
ed
ule
of
de
cis
ion
s r
ese
rve
d t
o t
he
Bo
ard
an
d S
tan
din
g F
ina
ncia
l
Instr
uctio
ns t
o r
efle
ct
the
se
.
En
su
re t
ha
t m
an
ag
em
en
t a
rra
ng
em
en
ts a
re in
pla
ce
to
en
ab
le r
esp
on
sib
ility
to
be
cle
arl
y
de
leg
ate
d t
o s
en
ior
exe
cu
tive
s f
or
the
ma
in p
rog
ram
me
s o
f a
ctio
n a
nd
fo
r p
erf
orm
an
ce
a
ga
inst
pro
gra
mm
es t
o e
sta
blis
h p
erf
orm
an
ce
an
d q
ua
lity
me
asu
res t
ha
t m
ain
tain
th
e
eff
ective
use
of
reso
urc
es a
nd
pro
vid
e v
alu
e f
or
mo
ne
y.
Sp
ecify its
re
qu
ire
me
nts
in
org
an
isin
g a
nd
pre
se
ntin
g f
ina
ncia
l a
nd
oth
er
info
rma
tio
n
su
ccin
ctly a
nd
eff
icie
ntly t
o e
nsu
re t
he
Bo
ard
ca
n f
ully u
nd
ert
ake
its
re
sp
on
sib
ilitie
s.
Esta
blis
h A
ud
it a
nd
No
min
atio
ns a
nd
Re
mu
ne
ratio
n C
om
mitte
es o
n t
he
ba
sis
of
form
ally
ag
ree
d t
erm
s o
f re
fere
nce
th
at
se
t o
ut
the
me
mb
ers
hip
of
the
su
b-c
om
mitte
e,
the
lim
it t
o
the
ir p
ow
ers
, a
nd
th
e a
rra
ng
em
en
ts f
or
rep
ort
ing
ba
ck t
o t
he
ma
in B
oa
rd.
1.3
.2.5
C
HA
IR
It is
th
e C
ha
ir’s
ro
le to
:
Pro
vid
e le
ad
ers
hip
to
th
e B
oa
rd.
En
ab
le a
ll B
oa
rd m
em
be
rs t
o m
ake
a f
ull c
on
trib
utio
n t
o t
he
Bo
ard
’s a
ffa
irs a
nd
en
su
re
tha
t th
e B
oa
rd a
cts
as a
te
am
.
En
su
re t
ha
t ke
y a
nd
ap
pro
pri
ate
issu
es a
re d
iscu
sse
d b
y t
he
Bo
ard
in
a t
ime
ly m
an
ne
r.
En
su
re t
he
Bo
ard
ha
s a
de
qu
ate
su
pp
ort
an
d is p
rovid
ed
eff
icie
ntly w
ith
all
the
ne
ce
ssa
ry
da
ta o
n w
hic
h t
o b
ase
in
form
ed
de
cis
ion
s.
Le
ad
No
n-E
xe
cu
tive
Dir
ecto
rs t
hro
ug
h a
fo
rma
lly a
pp
oin
ted
No
min
atio
ns a
nd
R
em
un
era
tio
n C
om
mitte
e o
f th
e m
ain
Bo
ard
on
th
e a
pp
oin
tme
nt,
ap
pra
isa
l a
nd
rem
un
era
tio
n o
f th
e C
hie
f E
xe
cu
tive
an
d (
with
th
e la
tte
r) o
the
r E
xe
cu
tive
Dir
ecto
rs.
Ap
po
int
No
n-E
xe
cu
tive
Dir
ecto
rs t
o a
Tru
st
Bo
ard
Su
b-C
om
mitte
e /
to
Tru
st
Bo
ard
C
om
mitte
es.
Ad
vis
e t
he
Co
un
cil
of
Go
ve
rno
rs o
n t
he
pe
rfo
rma
nce
of
No
n-E
xe
cu
tive
Dir
ecto
rs.
1.3
.2.5
C
HIE
F E
XE
CU
TIV
E
Th
e C
hie
f E
xe
cu
tive
is a
cco
un
tab
le t
o t
he
Ch
air
an
d N
on
-Exe
cu
tive
Dir
ecto
rs o
f th
e B
oa
rd f
or
en
su
rin
g t
ha
t its
de
cis
ion
s a
re im
ple
me
nte
d,
tha
t th
e o
rga
nis
atio
n w
ork
s e
ffe
ctive
ly,
in a
cco
rda
nce
with
Go
ve
rnm
en
t p
olic
y a
nd
pu
blic
se
rvic
e v
alu
es a
nd
fo
r th
e m
ain
ten
an
ce
of
pro
pe
r fin
an
cia
l
ste
wa
rdsh
ip.
Th
e C
hie
f E
xe
cu
tive
sh
ou
ld b
e a
llo
we
d f
ull
sco
pe
, w
ith
in c
lea
rly d
efin
ed
de
leg
ate
d p
ow
ers
, fo
r
actio
n in
fu
lfill
ing
th
e d
ecis
ion
s o
f th
e B
oa
rd.
Th
e o
the
r d
utie
s o
f th
e C
hie
f E
xe
cu
tive
as A
cco
un
tin
g O
ffic
er
Page 273 of 300
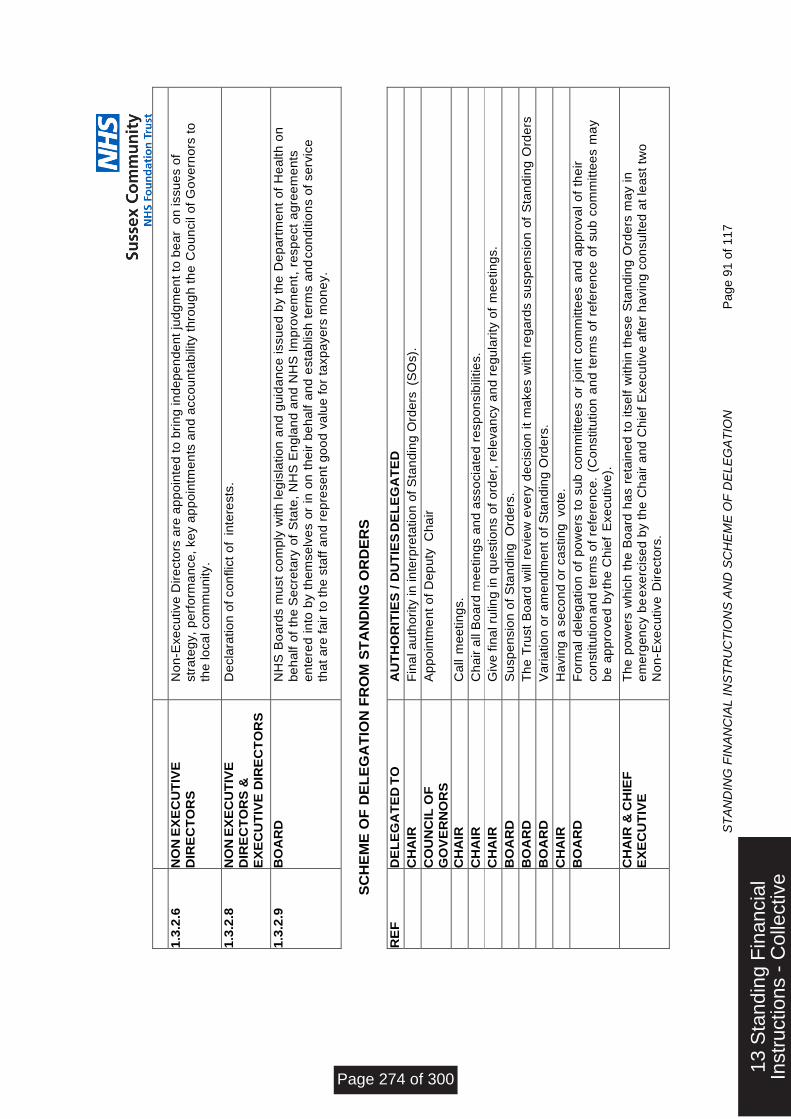
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
1 o
f 117
1.3
.2.6
N
ON
EX
EC
UT
IVE
DIR
EC
TO
RS
N
on
-Exe
cu
tive
Dir
ecto
rs a
re a
pp
oin
ted
to
bri
ng
in
de
pe
nd
en
t ju
dg
me
nt
to b
ea
r o
n issu
es o
f
str
ate
gy,
pe
rfo
rma
nce
, ke
y a
pp
oin
tme
nts
an
d a
cco
un
tab
ility t
hro
ug
h t
he
Co
un
cil
of
Go
ve
rno
rs t
o
the
lo
ca
l co
mm
un
ity.
1.3
.2.8
N
ON
EX
EC
UT
IVE
DIR
EC
TO
RS
&
EX
EC
UT
IVE
DIR
EC
TO
RS
De
cla
ratio
n o
f co
nflic
t o
f in
tere
sts
.
1.3
.2.9
B
OA
RD
N
HS
Bo
ard
s m
ust
co
mp
ly w
ith
le
gis
latio
n a
nd
gu
ida
nce
issu
ed
by t
he
De
pa
rtm
en
t o
f H
ea
lth
on
be
ha
lf o
f th
e S
ecre
tary
of
Sta
te,
NH
S E
ng
lan
d a
nd
NH
S I
mp
rove
me
nt,
re
sp
ect
ag
ree
me
nts
en
tere
d in
to b
y t
he
mse
lve
s o
r in
on
th
eir
be
ha
lf a
nd
esta
blish
te
rms a
nd
co
nd
itio
ns o
f se
rvic
e
tha
t a
re f
air
to
th
e s
taff
an
d r
ep
rese
nt
go
od
va
lue
fo
r ta
xp
aye
rs m
on
ey.
SC
HE
ME
OF
DE
LE
GA
TIO
N F
RO
M S
TA
ND
ING
OR
DE
RS
RE
F
DE
LE
GA
TE
D T
O
AU
TH
OR
ITIE
S / D
UT
IES
DE
LE
GA
TE
D
C
HA
IR
Fin
al a
uth
ori
ty in
in
terp
reta
tio
n o
f S
tan
din
g O
rde
rs (
SO
s).
C
OU
NC
IL O
F
GO
VE
RN
OR
S
Ap
po
intm
en
t o
f D
ep
uty
C
ha
ir
C
HA
IR
Ca
ll m
ee
tin
gs.
C
HA
IR
Ch
air
all
Bo
ard
me
etin
gs a
nd
asso
cia
ted
re
sp
on
sib
ilitie
s.
C
HA
IR
Giv
e f
ina
l ru
ling
in
qu
estio
ns o
f o
rde
r, r
ele
va
ncy a
nd
re
gu
lari
ty o
f m
ee
tin
gs.
B
OA
RD
S
usp
en
sio
n o
f S
tan
din
g O
rde
rs.
B
OA
RD
T
he
Tru
st
Bo
ard
will
re
vie
w e
ve
ry d
ecis
ion
it
ma
ke
s w
ith
re
ga
rds s
usp
en
sio
n o
f S
tan
din
g O
rde
rs
with
in 3
0 d
ays o
f su
sp
en
sio
n.
B
OA
RD
V
ari
atio
n o
r a
me
nd
me
nt
of
Sta
nd
ing
Ord
ers
.
C
HA
IR
Ha
vin
g a
se
co
nd
or
ca
stin
g vo
te.
B
OA
RD
F
orm
al
de
leg
atio
n o
f p
ow
ers
to
su
b c
om
mitte
es o
r jo
int
co
mm
itte
es a
nd
ap
pro
va
l o
f th
eir
co
nstitu
tio
n a
nd
te
rms o
f re
fere
nce
. (C
on
stitu
tio
n a
nd
te
rms o
f re
fere
nce
of
su
b c
om
mitte
es m
ay
be
ap
pro
ve
d b
y th
e C
hie
f E
xe
cu
tive
).
C
HA
IR &
CH
IEF
E
XE
CU
TIV
E
Th
e p
ow
ers
wh
ich
th
e B
oa
rd h
as r
eta
ine
d t
o its
elf w
ith
in t
he
se
Sta
nd
ing
Ord
ers
ma
y in
e
me
rge
ncy b
e e
xe
rcis
ed
by t
he
Ch
air
an
d C
hie
f E
xe
cu
tive
aft
er
ha
vin
g c
on
su
lte
d a
t le
ast
two
No
n-E
xe
cu
tive
Dir
ecto
rs.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 274 of 300
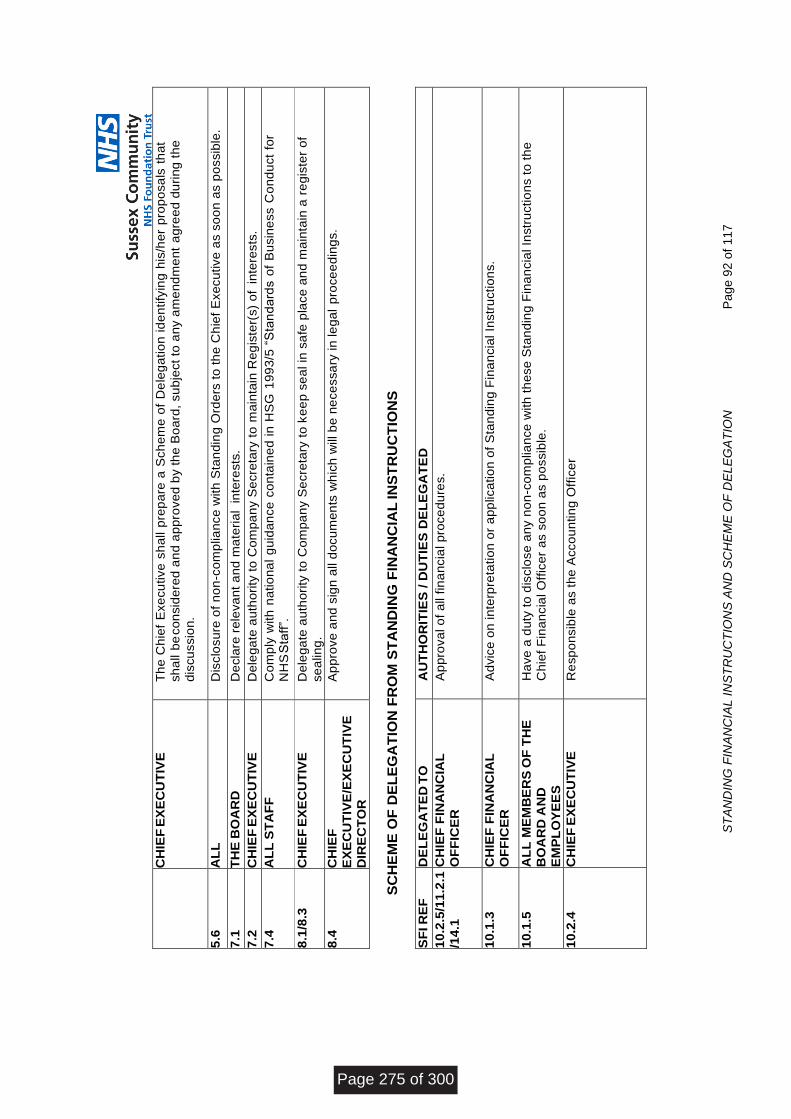
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
2 o
f 117
C
HIE
F E
XE
CU
TIV
E
Th
e C
hie
f E
xe
cu
tive
sh
all p
rep
are
a S
ch
em
e o
f D
ele
ga
tio
n id
en
tify
ing
his
/he
r p
rop
osa
ls t
ha
t
sh
all
be
co
nsid
ere
d a
nd
ap
pro
ve
d b
y t
he
Bo
ard
, su
bje
ct
to a
ny a
me
nd
me
nt
ag
ree
d d
uri
ng
th
e
dis
cu
ssio
n.
5.6
A
LL
D
isclo
su
re o
f n
on
-co
mp
lia
nce
with
Sta
nd
ing
Ord
ers
to
th
e C
hie
f E
xe
cu
tive
as s
oo
n a
s p
ossib
le.
7.1
T
HE
BO
AR
D
De
cla
re r
ele
va
nt
an
d m
ate
ria
l in
tere
sts
.
7.2
C
HIE
F E
XE
CU
TIV
E
De
leg
ate
au
tho
rity
to
Co
mp
an
y S
ecre
tary
to
ma
inta
in R
eg
iste
r(s)
of
inte
rests
.
7.4
A
LL
ST
AF
F
Co
mp
ly w
ith
na
tio
na
l g
uid
an
ce
co
nta
ine
d in
HS
G 1
99
3/5
“S
tan
da
rds o
f B
usin
ess C
on
du
ct
for
NH
S S
taff
”.
8.1
/8.3
C
HIE
F E
XE
CU
TIV
E
De
leg
ate
au
tho
rity
to
Co
mp
an
y S
ecre
tary
to
ke
ep
se
al in
sa
fe p
lace
an
d m
ain
tain
a r
eg
iste
r o
f
se
alin
g.
8.4
C
HIE
F
EX
EC
UT
IVE
/EX
EC
UT
IVE
D
IRE
CT
OR
Ap
pro
ve
an
d s
ign
all
do
cu
me
nts
wh
ich
will
be
ne
ce
ssa
ry in
le
ga
l p
roce
ed
ing
s.
SC
HE
ME
OF
DE
LE
GA
TIO
N F
RO
M S
TA
ND
ING
FIN
AN
CIA
L IN
ST
RU
CT
ION
S
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
10
.2.5
/11
.2.1
/14
.1
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
A
pp
rova
l o
f a
ll f
ina
ncia
l p
roce
du
res.
10
.1.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
dvic
e o
n in
terp
reta
tio
n o
r a
pp
lica
tio
n o
f S
tan
din
g F
ina
ncia
l In
str
uctio
ns.
10
.1.5
A
LL
ME
MB
ER
S O
F T
HE
BO
AR
D A
ND
EM
PL
OY
EE
S
Ha
ve
a d
uty
to
dis
clo
se
an
y n
on
-co
mp
lian
ce
with
th
ese
Sta
nd
ing
Fin
an
cia
l In
str
uctio
ns t
o t
he
Ch
ief
Fin
an
cia
l O
ffic
er
as s
oo
n a
s p
ossib
le.
10
.2.4
C
HIE
F E
XE
CU
TIV
E
Re
sp
on
sib
le a
s t
he
Acco
un
tin
g O
ffic
er
Page 275 of 300
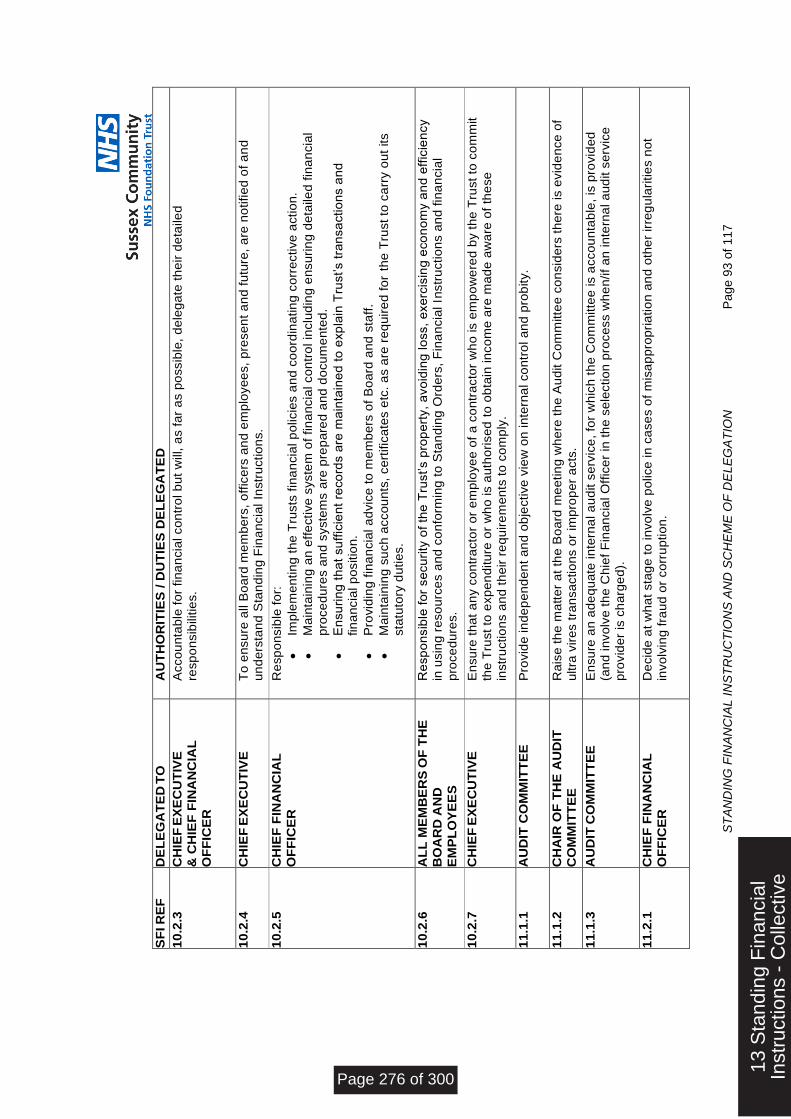
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
3 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
10
.2.3
C
HIE
F E
XE
CU
TIV
E
& C
HIE
F F
INA
NC
IAL
OF
FIC
ER
Acco
un
tab
le f
or
fin
an
cia
l co
ntr
ol b
ut
will, a
s f
ar
as p
ossib
le,
de
leg
ate
th
eir
de
taile
d
resp
on
sib
ilitie
s.
10
.2.4
C
HIE
F E
XE
CU
TIV
E
To
en
su
re a
ll B
oa
rd m
em
be
rs,
off
ice
rs a
nd
em
plo
ye
es,
pre
se
nt
an
d f
utu
re,
are
no
tifie
d o
f a
nd
u
nd
ers
tan
d S
tan
din
g F
ina
ncia
l In
str
uctio
ns.
10
.2.5
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
R
esp
on
sib
le f
or:
Imp
lem
en
tin
g t
he
Tru
sts
fin
an
cia
l p
olicie
s a
nd
co
ord
ina
tin
g c
orr
ective
actio
n.
Ma
inta
inin
g a
n e
ffe
ctive
syste
m o
f fin
an
cia
l co
ntr
ol in
clu
din
g e
nsu
rin
g d
eta
ile
d f
ina
ncia
l
pro
ce
du
res a
nd
syste
ms a
re p
rep
are
d a
nd
do
cu
me
nte
d.
En
su
rin
g t
ha
t su
ffic
ien
t re
co
rds a
re m
ain
tain
ed
to
exp
lain
Tru
st’s t
ran
sa
ctio
ns a
nd
fin
an
cia
l p
ositio
n.
Pro
vid
ing
fin
an
cia
l a
dvic
e t
o m
em
be
rs o
f B
oa
rd a
nd
sta
ff.
Ma
inta
inin
g s
uch
acco
un
ts,
ce
rtific
ate
s e
tc.
as a
re r
eq
uir
ed
fo
r th
e T
rust
to c
arr
y o
ut
its
sta
tuto
ry d
utie
s.
10
.2.6
A
LL
ME
MB
ER
S O
F T
HE
BO
AR
D A
ND
EM
PL
OY
EE
S
Re
sp
on
sib
le f
or
se
cu
rity
of
the
Tru
st’s p
rop
ert
y,
avo
idin
g lo
ss,
exe
rcis
ing
eco
no
my a
nd
eff
icie
ncy
in u
sin
g r
eso
urc
es a
nd
co
nfo
rmin
g t
o S
tan
din
g O
rde
rs,
Fin
an
cia
l In
str
uctio
ns a
nd
fin
an
cia
l
pro
ce
du
res.
10
.2.7
C
HIE
F E
XE
CU
TIV
E
En
su
re t
ha
t a
ny c
on
tra
cto
r o
r e
mp
loye
e o
f a
co
ntr
acto
r w
ho
is e
mp
ow
ere
d b
y t
he
Tru
st
to c
om
mit
the
Tru
st
to e
xp
en
ditu
re o
r w
ho
is a
uth
ori
se
d t
o o
bta
in in
co
me
are
ma
de
aw
are
of
the
se
instr
uctio
ns a
nd
th
eir
re
qu
ire
me
nts
to
co
mp
ly.
11
.1.1
A
UD
IT C
OM
MIT
TE
E
Pro
vid
e in
de
pe
nd
en
t a
nd
ob
jective
vie
w o
n in
tern
al co
ntr
ol a
nd
pro
bity.
11
.1.2
C
HA
IR O
F T
HE
AU
DIT
C
OM
MIT
TE
E
Ra
ise
th
e m
att
er
at
the
Bo
ard
me
etin
g w
he
re t
he
Au
dit C
om
mitte
e c
on
sid
ers
th
ere
is e
vid
en
ce
of
ultra
vir
es t
ran
sa
ctio
ns o
r im
pro
pe
r a
cts
.
11
.1.3
A
UD
IT C
OM
MIT
TE
E
En
su
re a
n a
de
qu
ate
in
tern
al a
ud
it s
erv
ice
, fo
r w
hic
h t
he
Co
mm
itte
e is a
cco
un
tab
le,
is p
rovid
ed
(a
nd
in
vo
lve
th
e C
hie
f F
ina
ncia
l O
ffic
er
in t
he
se
lectio
n p
roce
ss w
he
n/if
an
in
tern
al a
ud
it s
erv
ice
pro
vid
er
is c
ha
rge
d).
11
.2.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
D
ecid
e a
t w
ha
t sta
ge
to
in
vo
lve
po
lice
in
ca
se
s o
f m
isa
pp
rop
ria
tio
n a
nd
oth
er
irre
gu
lari
tie
s n
ot
invo
lvin
g f
rau
d o
r co
rru
ptio
n.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 276 of 300
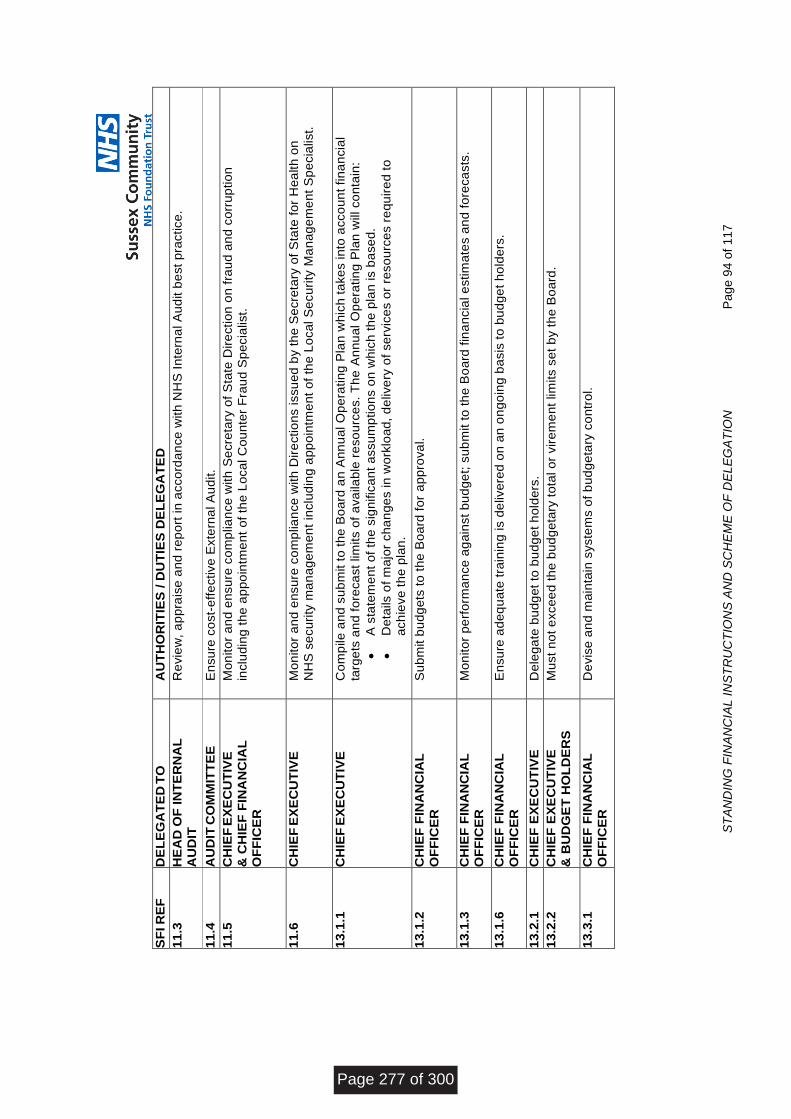
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
4 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
11
.3
HE
AD
OF
IN
TE
RN
AL
A
UD
IT
Re
vie
w,
ap
pra
ise
an
d r
ep
ort
in
acco
rda
nce
with
NH
S I
nte
rna
l A
ud
it b
est
pra
ctice
.
11
.4
AU
DIT
CO
MM
ITT
EE
E
nsu
re c
ost-
eff
ective
Exte
rna
l A
ud
it.
11
.5
CH
IEF
EX
EC
UT
IVE
& C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Mo
nito
r a
nd
en
su
re c
om
plia
nce
with
Se
cre
tary
of
Sta
te D
ire
ctio
n o
n f
rau
d a
nd
co
rru
ptio
n
inclu
din
g t
he
ap
po
intm
en
t o
f th
e L
oca
l C
ou
nte
r F
rau
d S
pe
cia
list.
11
.6
CH
IEF
EX
EC
UT
IVE
M
on
ito
r a
nd
en
su
re c
om
plia
nce
with
Dir
ectio
ns issu
ed
by t
he
Se
cre
tary
of
Sta
te f
or
He
alth
on
NH
S s
ecu
rity
ma
na
ge
me
nt
inclu
din
g a
pp
oin
tme
nt
of
the
Lo
ca
l S
ecu
rity
Ma
na
ge
me
nt
Sp
ecia
list.
13
.1.1
C
HIE
F E
XE
CU
TIV
E
Co
mp
ile
an
d s
ub
mit t
o t
he
Bo
ard
an
An
nu
al O
pe
ratin
g P
lan
wh
ich
ta
ke
s in
to a
cco
un
t fin
an
cia
l
targ
ets
an
d f
ore
ca
st
lim
its o
f a
va
ila
ble
re
so
urc
es.
Th
e A
nn
ua
l O
pe
ratin
g P
lan
will co
nta
in:
A s
tate
me
nt
of
the
sig
nific
an
t a
ssu
mp
tio
ns o
n w
hic
h t
he
pla
n is b
ase
d.
De
tails
of
ma
jor
ch
an
ge
s in
wo
rklo
ad
, d
elive
ry o
f se
rvic
es o
r re
so
urc
es r
eq
uir
ed
to
a
ch
ieve
th
e p
lan
.
13
.1.2
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
S
ub
mit b
ud
ge
ts t
o t
he
Bo
ard
fo
r a
pp
rova
l.
13
.1.3
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Mo
nito
r p
erf
orm
an
ce
ag
ain
st
bu
dg
et;
su
bm
it t
o t
he
Bo
ard
fin
an
cia
l e
stim
ate
s a
nd
fo
reca
sts
.
13
.1.6
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
E
nsu
re a
de
qu
ate
tra
inin
g is d
elive
red
on
an
on
go
ing
ba
sis
to
bu
dg
et
ho
lde
rs.
13
.2.1
C
HIE
F E
XE
CU
TIV
E
De
leg
ate
bu
dg
et
to b
ud
ge
t h
old
ers
.
13
.2.2
C
HIE
F E
XE
CU
TIV
E
& B
UD
GE
T H
OL
DE
RS
M
ust
no
t e
xce
ed
th
e b
ud
ge
tary
to
tal o
r vir
em
en
t lim
its s
et
by t
he
Bo
ard
.
13
.3.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
D
evis
e a
nd
ma
inta
in s
yste
ms o
f b
ud
ge
tary
co
ntr
ol.
Page 277 of 300
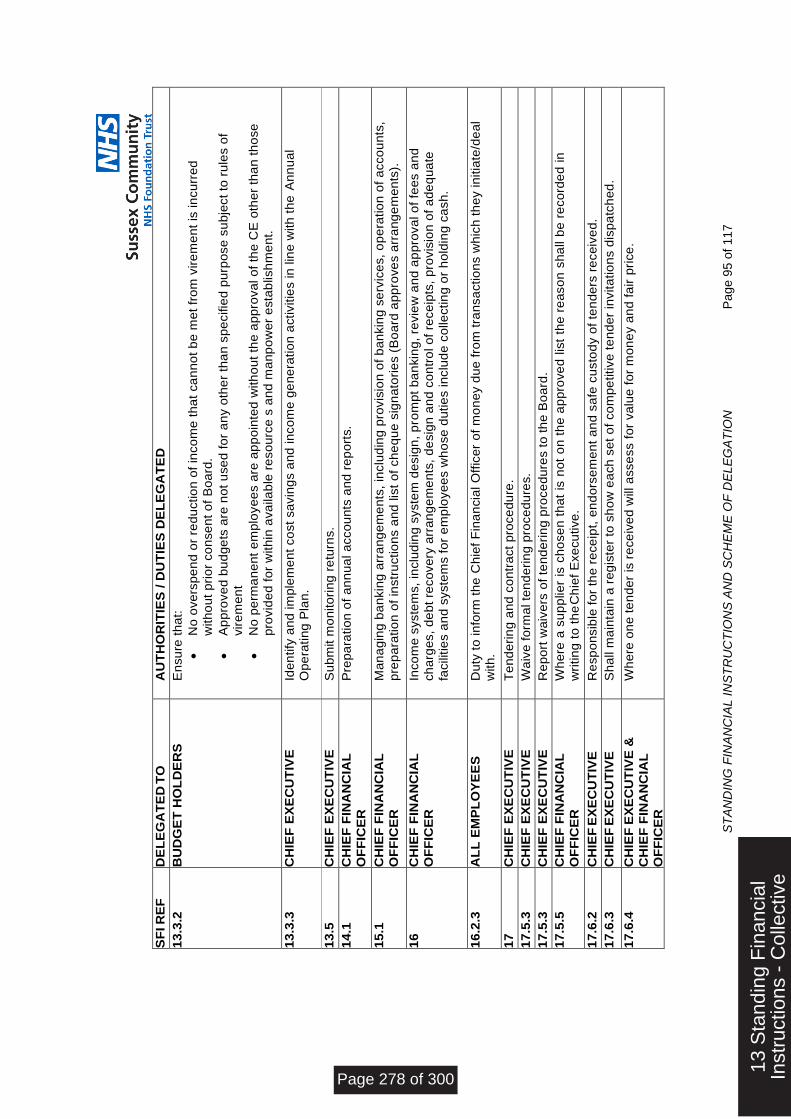
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
5 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
13
.3.2
B
UD
GE
T H
OL
DE
RS
E
nsu
re t
ha
t:
No
ove
rsp
en
d o
r re
du
ctio
n o
f in
co
me
th
at
ca
nn
ot
be
me
t fr
om
vir
em
en
t is
in
cu
rre
d
with
ou
t p
rio
r co
nse
nt
of
Bo
ard
.
Ap
pro
ve
d b
ud
ge
ts a
re n
ot
use
d f
or
an
y o
the
r th
an
sp
ecifie
d p
urp
ose
su
bje
ct
to r
ule
s o
f vir
em
en
t
No
pe
rma
ne
nt
em
plo
ye
es a
re a
pp
oin
ted
with
ou
t th
e a
pp
rova
l o
f th
e C
E o
the
r th
an
th
ose
p
rovid
ed
fo
r w
ith
in a
va
ila
ble
re
so
urc
e s
an
d m
an
po
we
r e
sta
blish
me
nt.
13
.3.3
C
HIE
F E
XE
CU
TIV
E
Ide
ntify
an
d im
ple
me
nt
co
st
sa
vin
gs a
nd
in
co
me
ge
ne
ratio
n a
ctivitie
s in
lin
e w
ith
th
e A
nn
ua
l O
pe
ratin
g P
lan
.
13
.5
CH
IEF
EX
EC
UT
IVE
S
ub
mit m
on
ito
rin
g r
etu
rns.
14
.1
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
P
rep
ara
tio
n o
f a
nn
ua
l a
cco
un
ts a
nd
re
po
rts.
15
.1
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
M
an
ag
ing
ba
nkin
g a
rra
ng
em
en
ts,
inclu
din
g p
rovis
ion
of
ba
nkin
g s
erv
ice
s,
op
era
tio
n o
f a
cco
un
ts,
pre
pa
ratio
n o
f in
str
uctio
ns a
nd
lis
t o
f ch
eq
ue
sig
na
tori
es (
Bo
ard
ap
pro
ve
s a
rra
ng
em
en
ts).
16
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
In
co
me
syste
ms,
inclu
din
g s
yste
m d
esig
n,
pro
mp
t b
an
kin
g,
revie
w a
nd
ap
pro
va
l o
f fe
es a
nd
ch
arg
es,
de
bt
reco
ve
ry a
rra
ng
em
en
ts,
de
sig
n a
nd
co
ntr
ol o
f re
ce
ipts
, p
rovis
ion
of
ad
eq
ua
te
facili
tie
s a
nd
syste
ms f
or
em
plo
ye
es w
ho
se
du
tie
s in
clu
de
co
lle
ctin
g o
r h
old
ing
ca
sh
.
16
.2.3
A
LL
EM
PL
OY
EE
S
Du
ty t
o in
form
th
e C
hie
f F
ina
ncia
l O
ffic
er
of
mo
ne
y d
ue
fro
m t
ran
sa
ctio
ns w
hic
h t
he
y in
itia
te/d
ea
l w
ith
.
17
CH
IEF
EX
EC
UT
IVE
T
en
de
rin
g a
nd
co
ntr
act
pro
ce
du
re.
17
.5.3
C
HIE
F E
XE
CU
TIV
E
Wa
ive
fo
rma
l te
nd
eri
ng
pro
ce
du
res.
17
.5.3
C
HIE
F E
XE
CU
TIV
E
Re
po
rt w
aiv
ers
of
ten
de
rin
g p
roce
du
res t
o t
he
Bo
ard
.
17
.5.5
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
W
he
re a
su
pp
lie
r is
ch
ose
n t
ha
t is
no
t o
n t
he
ap
pro
ve
d lis
t th
e r
ea
so
n s
ha
ll b
e r
eco
rde
d in
wri
tin
g t
o t
he
Ch
ief
Exe
cu
tive
.
17
.6.2
C
HIE
F E
XE
CU
TIV
E
Re
sp
on
sib
le f
or
the
re
ce
ipt,
en
do
rse
me
nt
an
d s
afe
cu
sto
dy o
f te
nd
ers
re
ce
ive
d.
17
.6.3
C
HIE
F E
XE
CU
TIV
E
Sh
all
ma
inta
in a
re
gis
ter
to s
ho
w e
ach
se
t o
f co
mp
etitive
te
nd
er
invita
tio
ns d
isp
atc
he
d.
17
.6.4
C
HIE
F E
XE
CU
TIV
E &
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
Wh
ere
on
e t
en
de
r is
re
ce
ive
d w
ill a
sse
ss f
or
va
lue
fo
r m
on
ey a
nd
fa
ir p
rice
.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 278 of 300
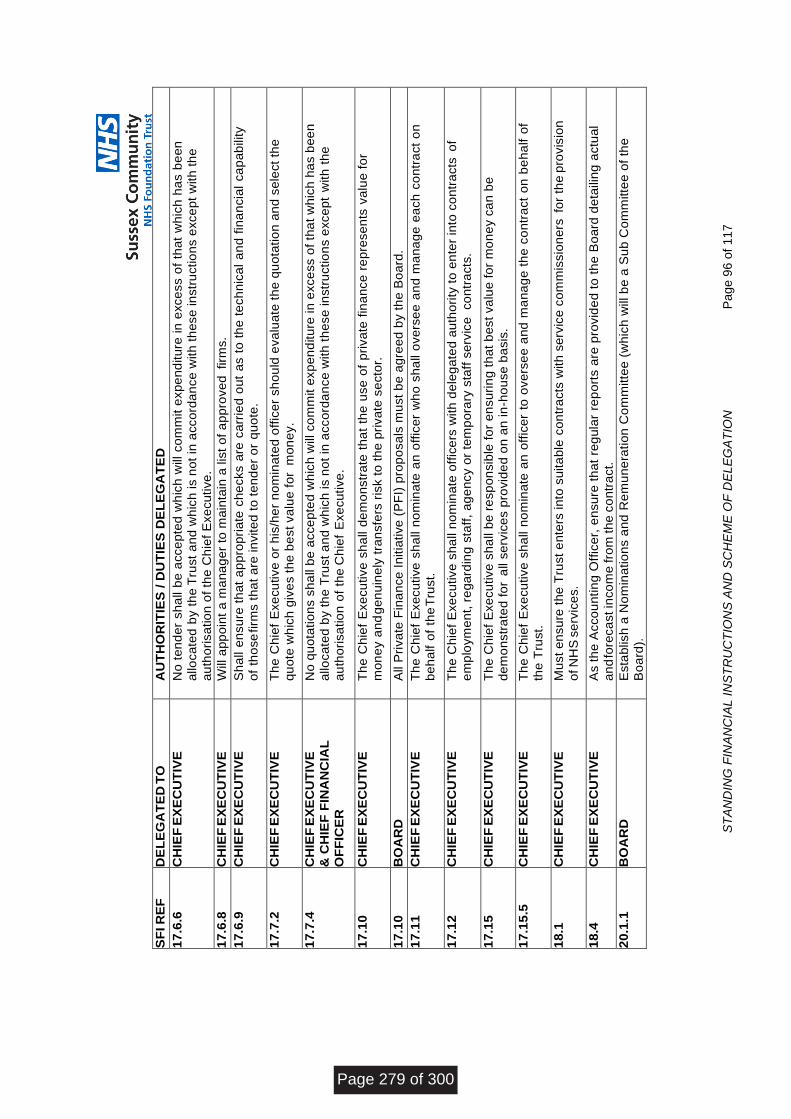
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
6 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
17
.6.6
C
HIE
F E
XE
CU
TIV
E
No
te
nd
er
sh
all
be
acce
pte
d w
hic
h w
ill co
mm
it e
xp
en
ditu
re in
exce
ss o
f th
at
wh
ich
ha
s b
ee
n
allo
ca
ted
by t
he
Tru
st
an
d w
hic
h is n
ot
in a
cco
rda
nce
with
th
ese
in
str
uctio
ns e
xce
pt
with
th
e
au
tho
risa
tio
n o
f th
e C
hie
f E
xe
cu
tive
.
17
.6.8
C
HIE
F E
XE
CU
TIV
E
Will a
pp
oin
t a
ma
na
ge
r to
ma
inta
in a
lis
t o
f a
pp
rove
d f
irm
s.
17
.6.9
C
HIE
F E
XE
CU
TIV
E
Sh
all e
nsu
re t
ha
t a
pp
rop
ria
te c
he
cks a
re c
arr
ied
ou
t a
s t
o t
he
te
ch
nic
al
an
d f
ina
ncia
l ca
pa
bility
of
tho
se
firm
s t
ha
t a
re in
vite
d t
o t
en
de
r o
r q
uo
te.
17
.7.2
C
HIE
F E
XE
CU
TIV
E
Th
e C
hie
f E
xe
cu
tive
or
his
/he
r n
om
ina
ted
off
ice
r sh
ou
ld e
va
lua
te t
he
qu
ota
tio
n a
nd
se
lect
the
qu
ote
wh
ich
giv
es t
he
be
st
va
lue
fo
r m
on
ey.
17
.7.4
C
HIE
F E
XE
CU
TIV
E
& C
HIE
F F
INA
NC
IAL
OF
FIC
ER
No
qu
ota
tio
ns s
ha
ll b
e a
cce
pte
d w
hic
h w
ill co
mm
it e
xp
en
ditu
re in
exce
ss o
f th
at
wh
ich
ha
s b
ee
n
allo
ca
ted
by t
he
Tru
st
an
d w
hic
h is n
ot
in a
cco
rda
nce
with
th
ese
in
str
uctio
ns e
xce
pt
with
th
e
au
tho
risa
tio
n o
f th
e C
hie
f E
xe
cu
tive
.
17
.10
CH
IEF
EX
EC
UT
IVE
T
he
Ch
ief
Exe
cu
tive
sh
all d
em
on
str
ate
th
at
the
use
of
pri
va
te f
ina
nce
re
pre
se
nts
va
lue
fo
r
mo
ne
y a
nd
ge
nu
ine
ly t
ran
sfe
rs r
isk t
o t
he
pri
va
te s
ecto
r.
17
.10
BO
AR
D
All P
riva
te F
ina
nce
In
itia
tive
(P
FI)
pro
po
sa
ls m
ust
be
ag
ree
d b
y t
he
Bo
ard
.
17
.11
CH
IEF
EX
EC
UT
IVE
T
he
Ch
ief
Exe
cu
tive
sh
all n
om
ina
te a
n o
ffic
er
wh
o s
ha
ll o
ve
rse
e a
nd
ma
na
ge
ea
ch
co
ntr
act
on
be
ha
lf o
f th
e T
rust.
17
.12
CH
IEF
EX
EC
UT
IVE
T
he
Ch
ief
Exe
cu
tive
sh
all n
om
ina
te o
ffic
ers
with
de
leg
ate
d a
uth
ori
ty t
o e
nte
r in
to c
on
tra
cts
of
em
plo
ym
en
t, r
eg
ard
ing
sta
ff,
ag
en
cy o
r te
mp
ora
ry s
taff
se
rvic
e co
ntr
acts
.
17
.15
CH
IEF
EX
EC
UT
IVE
T
he
Ch
ief
Exe
cu
tive
sh
all b
e r
esp
on
sib
le f
or
en
su
rin
g t
ha
t b
est
va
lue
fo
r m
on
ey c
an
be
d
em
on
str
ate
d f
or
all
se
rvic
es p
rovid
ed
on
an
in
-ho
use
ba
sis
.
17
.15
.5
CH
IEF
EX
EC
UT
IVE
T
he
Ch
ief
Exe
cu
tive
sh
all n
om
ina
te a
n o
ffic
er
to o
ve
rse
e a
nd
ma
na
ge
th
e c
on
tra
ct
on
be
ha
lf o
f
the
Tru
st.
18
.1
CH
IEF
EX
EC
UT
IVE
M
ust
en
su
re t
he
Tru
st
en
ters
in
to s
uita
ble
co
ntr
acts
with
se
rvic
e c
om
mis
sio
ne
rs f
or
the
pro
vis
ion
of N
HS
se
rvic
es.
18
.4
CH
IEF
EX
EC
UT
IVE
A
s t
he
Acco
un
tin
g O
ffic
er,
en
su
re t
ha
t re
gu
lar
rep
ort
s a
re p
rovid
ed
to
th
e B
oa
rd d
eta
ilin
g a
ctu
al
an
d fo
reca
st in
co
me
fro
m th
e c
on
tra
ct.
20
.1.1
B
OA
RD
E
sta
blis
h a
No
min
atio
ns a
nd
Re
mu
ne
ratio
n C
om
mitte
e (
wh
ich
will
be
a S
ub
Co
mm
itte
e o
f th
e
Bo
ard
).
Page 279 of 300
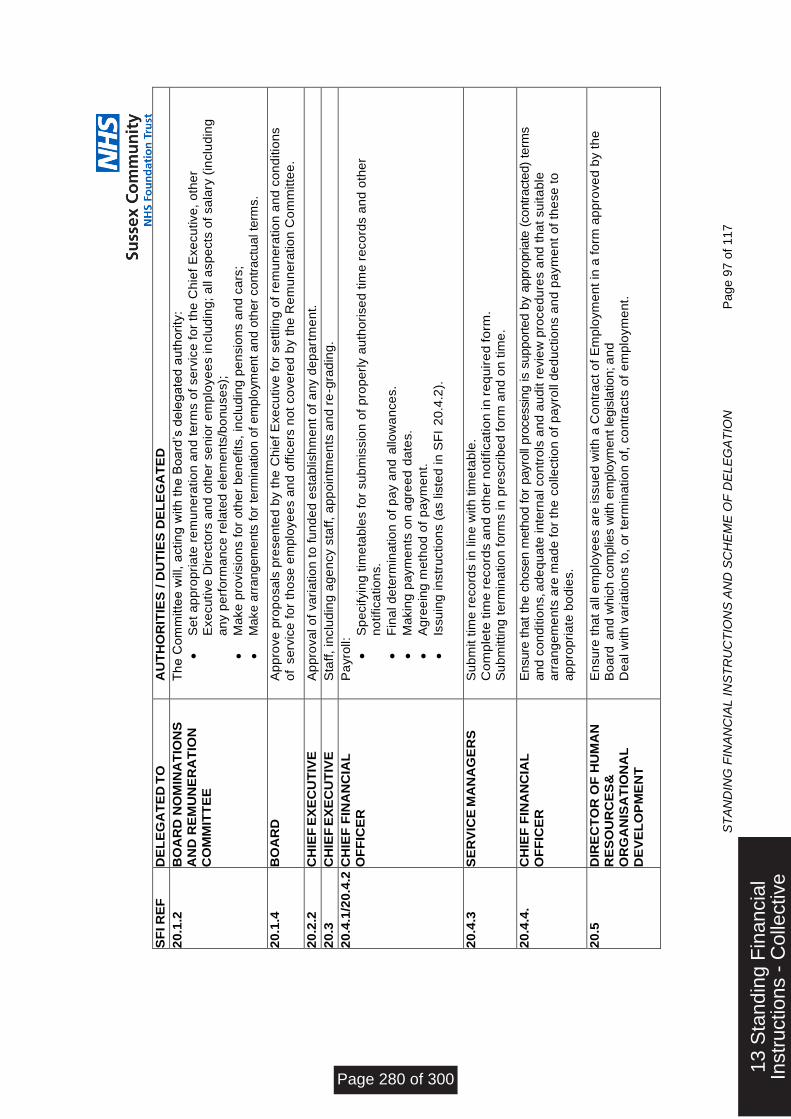
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
7 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
20
.1.2
B
OA
RD
NO
MIN
AT
ION
S
AN
D R
EM
UN
ER
AT
ION
CO
MM
ITT
EE
Th
e C
om
mitte
e w
ill, a
ctin
g w
ith
th
e B
oa
rd’s
de
leg
ate
d a
uth
ori
ty:
Se
t a
pp
rop
ria
te r
em
un
era
tio
n a
nd
te
rms o
f se
rvic
e f
or
the
Ch
ief
Exe
cu
tive
, o
the
r
Exe
cu
tive
Dir
ecto
rs a
nd
oth
er
se
nio
r e
mp
loye
es in
clu
din
g;
all a
sp
ects
of
sa
lary
(in
clu
din
g
an
y p
erf
orm
an
ce
re
late
d e
lem
en
ts/b
on
use
s);
Ma
ke
pro
vis
ion
s f
or
oth
er
be
ne
fits
, in
clu
din
g p
en
sio
ns a
nd
ca
rs;
Make a
rrangem
ents
for
term
ination o
f em
plo
ym
ent a
nd o
ther
contr
actu
al te
rms.
2
0.1
.4
BO
AR
D
Ap
pro
ve
pro
po
sa
ls p
rese
nte
d b
y t
he
Ch
ief
Exe
cu
tive
fo
r se
ttlin
g o
f re
mu
ne
ratio
n a
nd
co
nd
itio
ns
of
se
rvic
e f
or
tho
se
em
plo
ye
es a
nd
off
ice
rs n
ot
co
ve
red
by t
he
Re
mu
ne
ratio
n C
om
mitte
e.
20
.2.2
C
HIE
F E
XE
CU
TIV
E
Ap
pro
va
l o
f va
ria
tio
n t
o f
un
de
d e
sta
blish
me
nt
of
an
y d
ep
art
me
nt.
20
.3
CH
IEF
EX
EC
UT
IVE
S
taff
, in
clu
din
g a
ge
ncy s
taff
, a
pp
oin
tme
nts
an
d r
e-g
rad
ing
.
20
.4.1
/20
.4.2
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
P
ayro
ll:
Sp
ecifyin
g t
ime
tab
les f
or
su
bm
issio
n o
f p
rop
erl
y a
uth
ori
se
d t
ime
re
co
rds a
nd
oth
er
no
tifica
tio
ns.
Fin
al d
ete
rmin
atio
n o
f p
ay a
nd
allo
wa
nce
s.
Ma
kin
g p
aym
en
ts o
n a
gre
ed
da
tes.
Ag
ree
ing
me
tho
d o
f p
aym
en
t.
Issu
ing
in
str
uctio
ns (
as lis
ted
in
SF
I 2
0.4
.2).
20
.4.3
S
ER
VIC
E M
AN
AG
ER
S
Su
bm
it t
ime
re
co
rds in
lin
e w
ith
tim
eta
ble
.
Co
mp
lete
tim
e r
eco
rds a
nd
oth
er
no
tifica
tio
n in
re
qu
ire
d fo
rm.
Su
bm
ittin
g t
erm
ina
tio
n f
orm
s in
pre
scri
be
d f
orm
an
d o
n t
ime
.
20
.4.4
. C
HIE
F F
INA
NC
IAL
OF
FIC
ER
E
nsure
that
the c
hosen m
eth
od for
payro
ll pro
cessin
g is s
upport
ed b
y a
ppro
priate
(contr
acte
d)
term
s
and c
on
ditio
ns, a
de
qu
ate
in
tern
al co
ntr
ols
an
d a
ud
it r
evie
w p
roce
du
res a
nd
th
at
su
ita
ble
a
rra
ng
em
en
ts a
re m
ad
e f
or
the
co
lle
ctio
n o
f p
ayro
ll d
ed
uctio
ns a
nd
pa
ym
en
t o
f th
ese
to
ap
pro
pri
ate
bo
die
s.
20
.5
DIR
EC
TO
R O
F H
UM
AN
R
ES
OU
RC
ES
&
OR
GA
NIS
AT
ION
AL
DE
VE
LO
PM
EN
T
En
su
re t
ha
t a
ll e
mp
loye
es a
re issu
ed
with
a C
on
tra
ct
of
Em
plo
ym
en
t in
a f
orm
ap
pro
ve
d b
y t
he
B
oa
rd a
nd
whic
h c
om
plie
s w
ith e
mplo
ym
ent le
gis
lation; a
nd
De
al w
ith
va
ria
tio
ns t
o,
or
term
ina
tio
n o
f, c
on
tra
cts
of
em
plo
ym
en
t.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 280 of 300
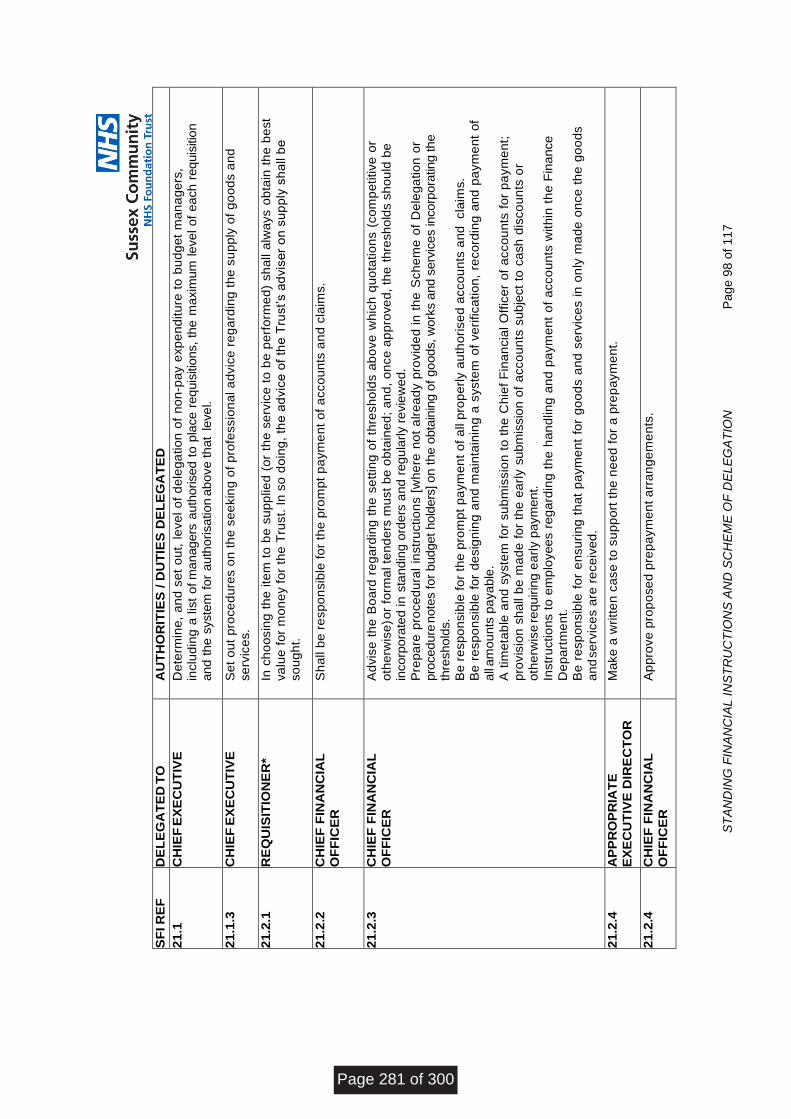
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
8 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
21
.1
CH
IEF
EX
EC
UT
IVE
D
ete
rmin
e,
an
d s
et
ou
t, le
ve
l o
f d
ele
ga
tio
n o
f n
on
-pa
y e
xp
en
ditu
re t
o b
ud
ge
t m
an
ag
ers
, in
clu
din
g a
lis
t o
f m
anagers
auth
orised t
o p
lace r
equis
itio
ns,
the
maxim
um
level of
each r
equis
itio
n
and t
he s
yste
m f
or
auth
orisation
ab
ove th
at
leve
l.
21
.1.3
C
HIE
F E
XE
CU
TIV
E
Se
t o
ut
pro
ce
du
res o
n t
he
se
ekin
g o
f p
rofe
ssio
na
l a
dvic
e r
eg
ard
ing
th
e s
up
ply
of
go
od
s a
nd
se
rvic
es.
21
.2.1
R
EQ
UIS
ITIO
NE
R*
In c
ho
osin
g t
he
ite
m t
o b
e s
up
plie
d (
or
the
se
rvic
e t
o b
e p
erf
orm
ed
) sh
all a
lwa
ys o
bta
in t
he
be
st
va
lue
fo
r m
on
ey f
or
the
Tru
st.
In
so
do
ing
, th
e a
dvic
e o
f th
e T
rust’s a
dvis
er
on
su
pp
ly s
ha
ll b
e
so
ug
ht.
21
.2.2
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Sh
all
be
re
sp
on
sib
le f
or
the
pro
mp
t p
aym
en
t o
f a
cco
un
ts a
nd
cla
ims.
21
.2.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
dvis
e t
he
Bo
ard
re
ga
rdin
g t
he
se
ttin
g o
f th
resh
old
s a
bo
ve
wh
ich
qu
ota
tio
ns (
co
mp
etitive
or
oth
erw
ise
) or
form
al te
nd
ers
mu
st
be
ob
tain
ed
; a
nd
, o
nce
ap
pro
ve
d,
the
thre
sh
old
s s
ho
uld
be
incorp
ora
ted
in
sta
ndin
g o
rders
an
d r
eg
ula
rly r
evie
we
d.
Pre
pa
re p
roce
du
ral
instr
uctio
ns [
wh
ere
no
t a
lre
ad
y p
rovid
ed
in
th
e S
ch
em
e o
f D
ele
ga
tio
n o
r
pro
cedure
note
s for
budget hold
ers
] on the o
bta
inin
g o
f goods, w
ork
s a
nd s
erv
ices incorp
ora
ting the
thre
shold
s.
Be
re
sp
on
sib
le f
or
the
pro
mp
t p
aym
en
t o
f a
ll p
rop
erl
y a
uth
ori
se
d a
cco
un
ts a
nd
cla
ims.
Be r
esp
on
sib
le f
or
de
sig
nin
g a
nd
ma
inta
inin
g a
syste
m o
f ve
rifica
tio
n,
reco
rdin
g a
nd p
aym
en
t of
all
am
ou
nts
pa
ya
ble
.
A t
ime
tab
le a
nd
syste
m f
or
su
bm
issio
n t
o t
he C
hie
f F
ina
ncia
l O
ffic
er
of
acco
un
ts f
or
pa
ym
en
t;
pro
vis
ion
sh
all
be
ma
de
fo
r th
e e
arl
y s
ub
mis
sio
n o
f a
cco
un
ts s
ubje
ct
to c
ash d
isco
un
ts o
r
oth
erw
ise
re
quirin
g e
arl
y p
aym
ent.
Instr
uctio
ns t
o e
mp
loyee
s r
eg
ard
ing
th
e h
an
dlin
g a
nd
pa
ym
en
t o
f a
cco
un
ts w
ith
in t
he
Fin
ance
De
pa
rtm
en
t.
Be
re
sp
on
sib
le f
or
en
su
rin
g t
ha
t p
aym
en
t fo
r g
oo
ds a
nd
se
rvic
es in
on
ly m
ad
e o
nce
th
e g
oo
ds
an
d s
erv
ice
s a
re r
ece
ive
d.
21
.2.4
A
PP
RO
PR
IAT
E
EX
EC
UT
IVE
DIR
EC
TO
R
Ma
ke
a w
ritt
en
ca
se
to
su
pp
ort
th
e n
ee
d f
or
a p
rep
aym
en
t.
21
.2.4
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
pp
rove
pro
po
se
d p
rep
aym
en
t a
rra
ng
em
en
ts.
Page 281 of 300
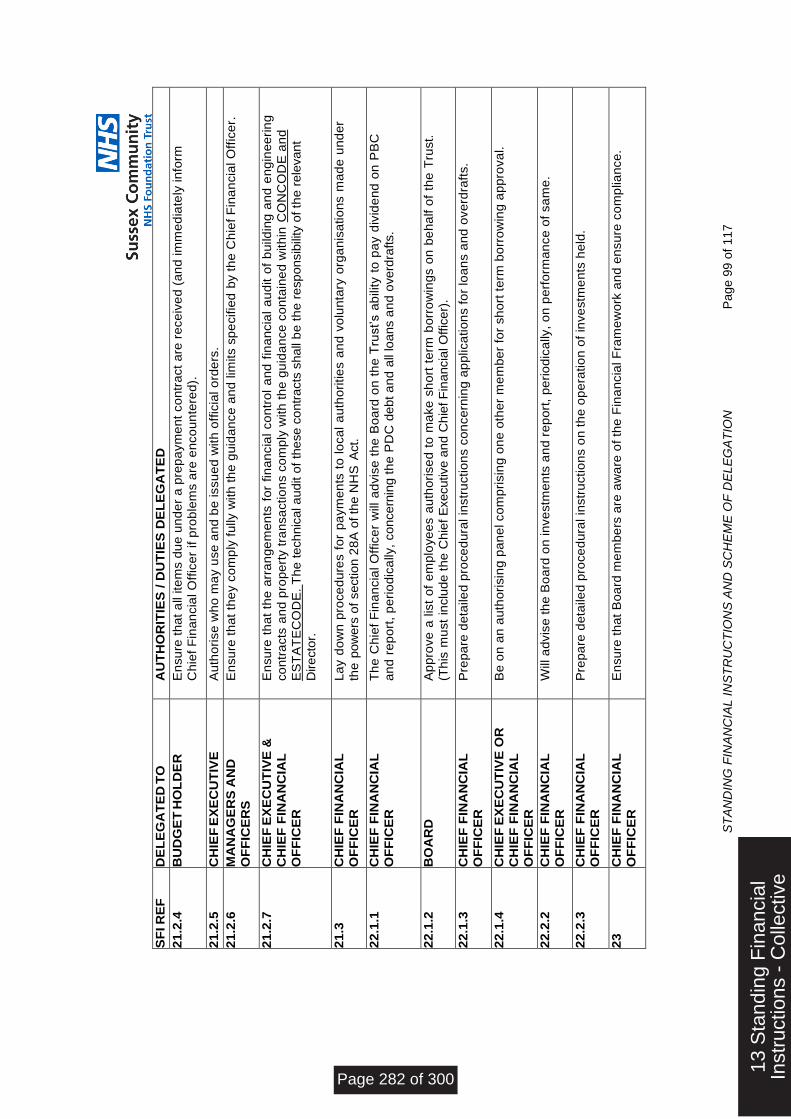
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 9
9 o
f 117
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
21
.2.4
B
UD
GE
T H
OL
DE
R
En
su
re t
ha
t a
ll ite
ms d
ue
un
de
r a
pre
pa
ym
en
t co
ntr
act
are
re
ce
ive
d (
an
d im
me
dia
tely
in
form
C
hie
f F
ina
ncia
l O
ffic
er
if p
rob
lem
s a
re e
nco
un
tere
d).
21
.2.5
C
HIE
F E
XE
CU
TIV
E
Au
tho
rise
wh
o m
ay u
se
an
d b
e issu
ed
with
off
icia
l o
rde
rs.
21
.2.6
M
AN
AG
ER
S A
ND
OF
FIC
ER
S
En
su
re t
ha
t th
ey c
om
ply
fu
lly w
ith
th
e g
uid
an
ce
an
d lim
its s
pe
cifie
d b
y t
he
Ch
ief
Fin
an
cia
l O
ffic
er.
21
.2.7
C
HIE
F E
XE
CU
TIV
E &
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
En
su
re t
ha
t th
e a
rra
ng
em
en
ts f
or
fin
an
cia
l co
ntr
ol
an
d f
ina
ncia
l a
ud
it o
f b
uild
ing
an
d e
ng
ine
eri
ng
co
ntr
acts
an
d p
rop
ert
y t
ran
sa
ctio
ns c
om
ply
with
th
e g
uid
an
ce
co
nta
ine
d w
ith
in C
ON
CO
DE
an
d
ES
TA
TE
CO
DE
. T
he
te
ch
nic
al a
udit o
f th
ese c
ontr
acts
shall
be
th
e r
esp
onsib
ility
of th
e r
ele
vant
Dire
cto
r.
21
.3
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
L
ay d
ow
n p
roce
du
res f
or
pa
ym
en
ts t
o lo
ca
l a
uth
ori
tie
s a
nd
vo
lun
tary
org
an
isa
tio
ns m
ad
e u
nd
er
the
pow
ers
of
section 2
8A
of th
e N
HS
Act.
22
.1.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
T
he
Ch
ief
Fin
an
cia
l O
ffic
er
will
ad
vis
e t
he
Bo
ard
on
th
e T
rust’s a
bility t
o p
ay d
ivid
en
d o
n P
BC
an
d r
ep
ort
, p
eri
od
ica
lly,
concern
ing t
he
PD
C d
ebt a
nd
all
loans a
nd
overd
rafts.
22
.1.2
B
OA
RD
A
pp
rove
a lis
t o
f e
mp
loye
es a
uth
ori
se
d t
o m
ake
sh
ort
te
rm b
orr
ow
ing
s o
n b
eh
alf o
f th
e T
rust.
(Th
is m
ust
inclu
de
th
e C
hie
f E
xecutive a
nd C
hie
f F
inancia
l O
ffic
er)
.
22
.1.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
P
rep
are
de
taile
d p
roce
du
ral in
str
uctio
ns c
on
ce
rnin
g a
pp
lica
tio
ns f
or
loa
ns a
nd
ove
rdra
fts.
22
.1.4
C
HIE
F E
XE
CU
TIV
E O
R
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
Be
on
an
au
tho
risin
g p
an
el co
mp
risin
g o
ne
oth
er
me
mb
er
for
sh
ort
te
rm b
orr
ow
ing
ap
pro
va
l.
22
.2.2
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
W
ill a
dvis
e t
he
Bo
ard
on
in
ve
stm
en
ts a
nd
re
po
rt,
pe
rio
dic
ally
, o
n p
erf
orm
an
ce
of
sa
me
.
22
.2.3
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Pre
pa
re d
eta
iled
pro
ce
du
ral in
str
uctio
ns o
n t
he
op
era
tio
n o
f in
ve
stm
en
ts h
eld
.
23
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
E
nsu
re t
ha
t B
oa
rd m
em
be
rs a
re a
wa
re o
f th
e F
ina
ncia
l F
ram
ew
ork
an
d e
nsu
re c
om
plia
nce
.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 282 of 300
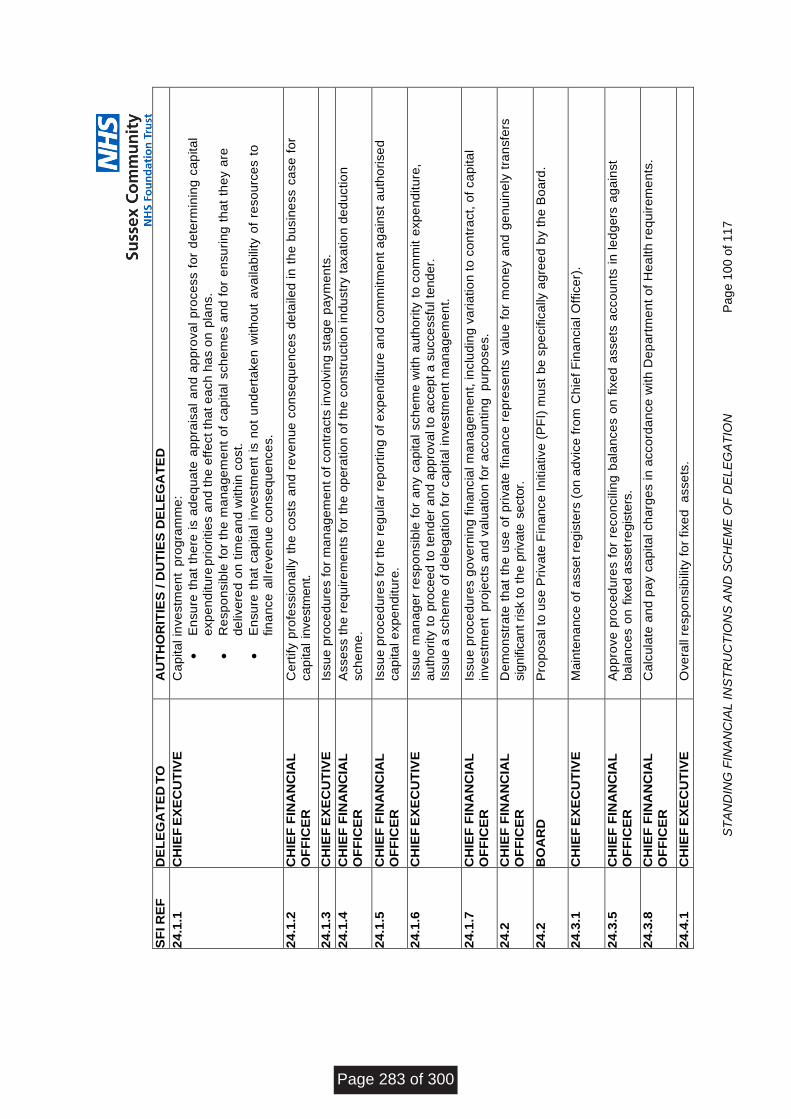
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
00
of
11
7
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
24
.1.1
C
HIE
F E
XE
CU
TIV
E
Ca
pita
l in
ve
stm
en
t p
rog
ram
me
:
En
su
re t
ha
t th
ere
is a
de
qu
ate
ap
pra
isa
l a
nd
ap
pro
va
l p
roce
ss f
or
de
term
inin
g c
ap
ita
l
exp
en
ditu
re p
rio
ritie
s a
nd
th
e e
ffe
ct
tha
t e
ach
ha
s o
n p
lan
s.
Re
sp
on
sib
le f
or
the
ma
na
ge
me
nt
of
ca
pita
l sch
em
es a
nd
fo
r e
nsu
rin
g t
ha
t th
ey a
re
de
live
red
on
tim
e a
nd
with
in c
ost.
En
su
re t
ha
t ca
pita
l in
ve
stm
en
t is
no
t u
nd
ert
ake
n w
ith
ou
t a
va
ilab
ility
of
reso
urc
es t
o
fin
an
ce
all re
ve
nu
e c
on
se
qu
en
ce
s.
2
4.1
.2
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
C
ert
ify p
rofe
ssio
na
lly t
he
co
sts
an
d r
eve
nu
e c
on
se
qu
en
ce
s d
eta
ile
d in
th
e b
usin
ess c
ase
fo
r
ca
pita
l in
vestm
ent.
24
.1.3
C
HIE
F E
XE
CU
TIV
E
Issu
e p
roce
du
res f
or
ma
na
ge
me
nt
of
co
ntr
acts
in
vo
lvin
g s
tag
e p
aym
en
ts.
24
.1.4
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
sse
ss t
he
re
qu
ire
me
nts
fo
r th
e o
pe
ratio
n o
f th
e c
on
str
uctio
n in
du
str
y t
axa
tio
n d
ed
uctio
n
sch
em
e.
24
.1.5
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Issu
e p
roce
du
res f
or
the
re
gu
lar
rep
ort
ing
of
exp
en
ditu
re a
nd
co
mm
itm
en
t a
ga
inst
au
tho
rise
d
ca
pita
l e
xp
en
ditu
re.
24
.1.6
C
HIE
F E
XE
CU
TIV
E
Issu
e m
an
ag
er
resp
on
sib
le f
or
an
y c
ap
ita
l sch
em
e w
ith
au
tho
rity
to
co
mm
it e
xp
en
ditu
re,
au
tho
rity
to
pro
cee
d t
o t
en
de
r a
nd
appro
val to
accept a
succe
ssfu
l te
nd
er.
Issu
e a
sch
em
e o
f d
ele
ga
tio
n f
or
ca
pita
l in
ve
stm
en
t m
an
ag
em
en
t.
24
.1.7
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
Is
su
e p
roce
du
res g
ove
rnin
g f
ina
ncia
l m
an
ag
em
en
t, in
clu
din
g v
ari
atio
n t
o c
on
tra
ct,
of
ca
pita
l
inve
stm
en
t p
roje
cts
an
d v
alu
atio
n f
or
acco
un
tin
g p
urp
ose
s.
24
.2
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
D
em
on
str
ate
th
at
the
use
of
pri
va
te f
ina
nce
re
pre
se
nts
va
lue
fo
r m
on
ey a
nd
ge
nu
ine
ly t
ran
sfe
rs
sig
nific
ant risk t
o t
he
private
secto
r.
24
.2
BO
AR
D
Pro
po
sa
l to
use
Pri
va
te F
ina
nce
In
itia
tive
(P
FI)
mu
st
be s
pe
cific
ally
ag
ree
d b
y t
he
Bo
ard
.
24
.3.1
C
HIE
F E
XE
CU
TIV
E
Ma
inte
na
nce
of
asse
t re
gis
ters
(o
n a
dvic
e f
rom
Ch
ief
Fin
an
cia
l O
ffic
er)
.
24
.3.5
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
pp
rove
pro
ce
du
res f
or
reco
ncilin
g b
ala
nce
s o
n f
ixe
d a
sse
ts a
cco
un
ts i
n le
dg
ers
ag
ain
st
ba
lan
ce
s o
n f
ixed
asset r
egis
ters
.
24
.3.8
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
C
alc
ula
te a
nd
pa
y c
ap
ita
l ch
arg
es in
acco
rda
nce
with
De
pa
rtm
en
t o
f H
ea
lth
re
qu
ire
me
nts
.
24
.4.1
C
HIE
F E
XE
CU
TIV
E
Ove
rall
resp
on
sib
ility
fo
r fixe
d a
sse
ts.
Page 283 of 300
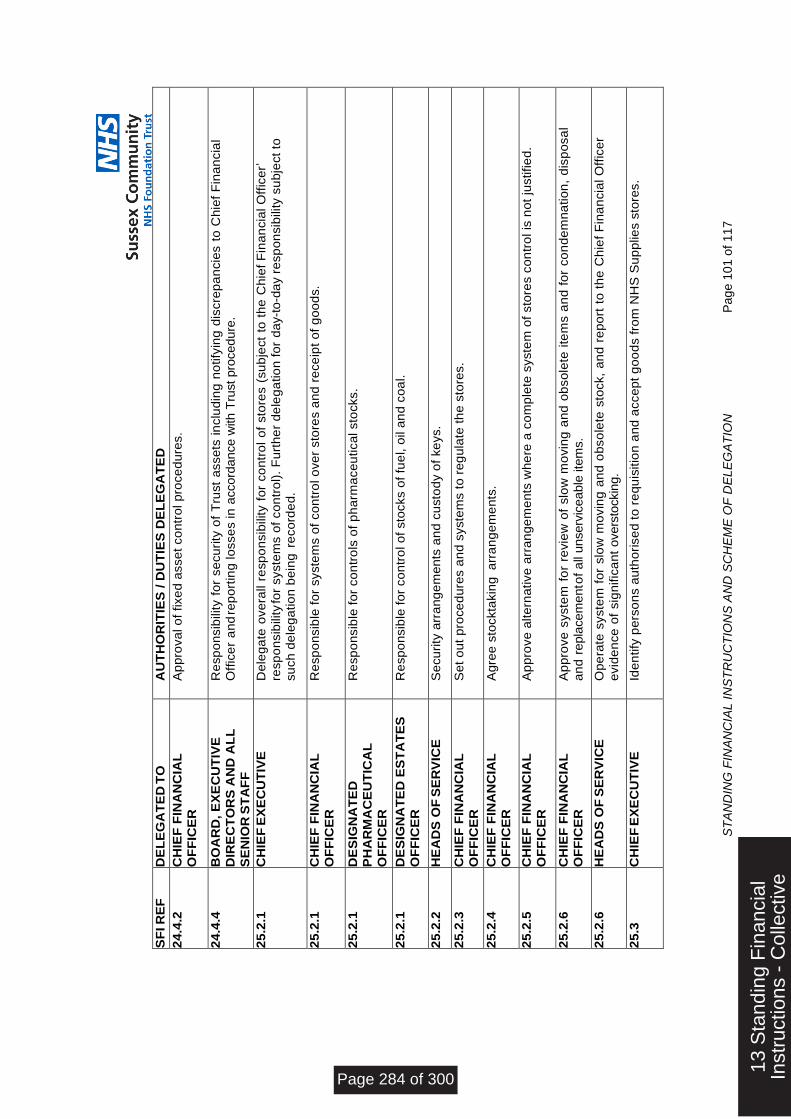
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
01
of
11
7
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
24
.4.2
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Ap
pro
va
l o
f fixe
d a
sse
t co
ntr
ol p
roce
du
res.
24
.4.4
B
OA
RD
, E
XE
CU
TIV
E
DIR
EC
TO
RS
AN
D A
LL
SE
NIO
R S
TA
FF
Re
sp
on
sib
ility f
or
se
cu
rity
of
Tru
st
asse
ts in
clu
din
g n
otify
ing
dis
cre
pa
ncie
s t
o C
hie
f F
ina
ncia
l
Off
ice
r a
nd
rep
ort
ing
lo
sse
s in
accord
ance w
ith T
rust pro
cedure
.
25
.2.1
C
HIE
F E
XE
CU
TIV
E
De
leg
ate
ove
rall r
esp
on
sib
ility
fo
r co
ntr
ol
of
sto
res (
su
bje
ct
to t
he
Ch
ief
Fin
an
cia
l O
ffic
er’
resp
on
sib
ility fo
r syste
ms o
f co
ntr
ol)
. F
urt
he
r d
ele
ga
tio
n f
or
day-t
o-d
ay r
esp
on
sib
ility
su
bje
ct
to
su
ch
de
leg
atio
n b
ein
g r
eco
rde
d.
25
.2.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
R
esp
on
sib
le f
or
syste
ms o
f co
ntr
ol o
ve
r sto
res a
nd
re
ce
ipt
of
go
od
s.
25
.2.1
D
ES
IGN
AT
ED
P
HA
RM
AC
EU
TIC
AL
OF
FIC
ER
Re
sp
on
sib
le f
or
co
ntr
ols
of
ph
arm
ace
utica
l sto
cks.
25
.2.1
D
ES
IGN
AT
ED
ES
TA
TE
S
OF
FIC
ER
R
esp
on
sib
le f
or
co
ntr
ol o
f sto
cks o
f fu
el, o
il a
nd
co
al.
25
.2.2
H
EA
DS
OF
SE
RV
ICE
S
ecu
rity
arr
an
ge
me
nts
an
d c
usto
dy o
f ke
ys.
25
.2.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
S
et
ou
t p
roce
du
res a
nd
syste
ms t
o r
eg
ula
te t
he
sto
res.
25
.2.4
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
gre
e s
tockta
kin
g a
rra
ng
em
en
ts.
25
.2.5
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
pp
rove
alte
rna
tive
arr
an
ge
me
nts
wh
ere
a c
om
ple
te s
yste
m o
f sto
res c
on
tro
l is
no
t ju
stifie
d.
25
.2.6
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
A
pp
rove
syste
m f
or
revie
w o
f slo
w m
ovin
g a
nd
ob
so
lete
ite
ms a
nd
fo
r co
nd
em
na
tio
n,
dis
po
sa
l
an
d r
epla
cem
ent o
f a
ll unserv
iceable
ite
ms.
25
.2.6
H
EA
DS
OF
SE
RV
ICE
O
pe
rate
syste
m f
or
slo
w m
ovin
g a
nd
ob
so
lete
sto
ck,
an
d r
ep
ort
to
th
e C
hie
f F
ina
ncia
l O
ffic
er
evid
en
ce
of
sig
nific
an
t o
vers
tockin
g.
25
.3
CH
IEF
EX
EC
UT
IVE
Id
en
tify
pe
rso
ns a
uth
ori
se
d t
o r
eq
uis
itio
n a
nd
acce
pt
go
od
s f
rom
NH
S S
up
plie
s s
tore
s.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 284 of 300
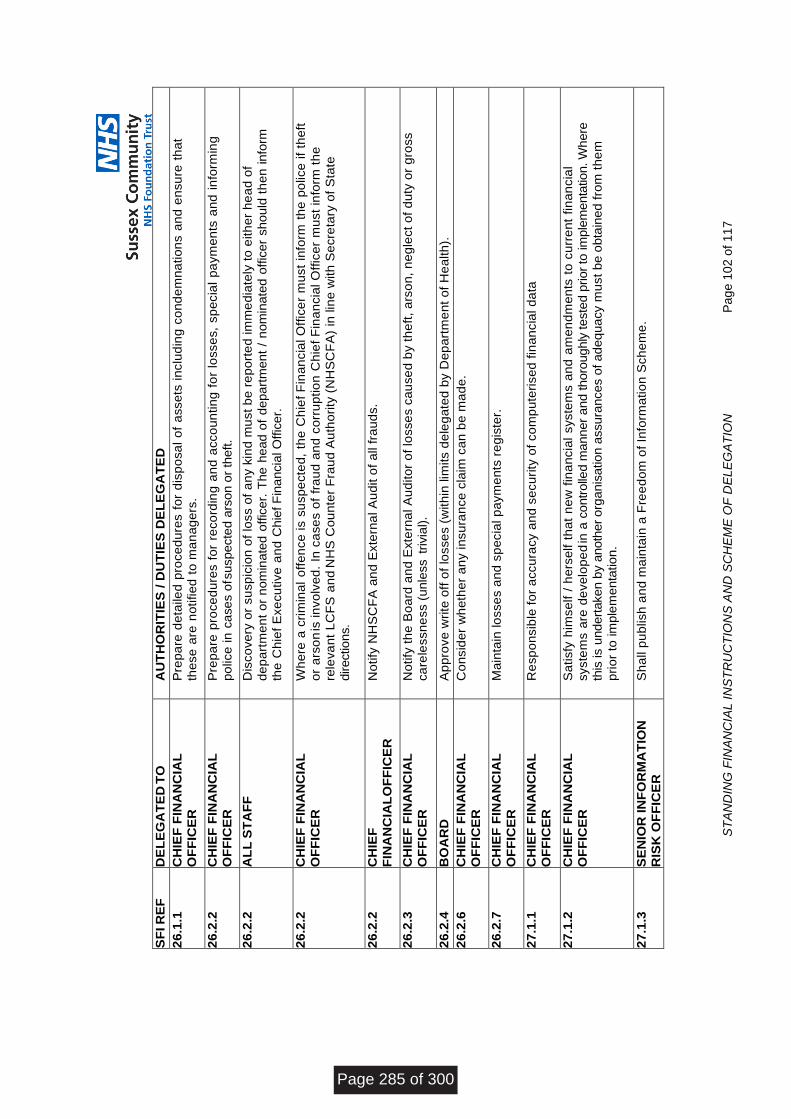
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
02
of
11
7
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
26
.1.1
C
HIE
F F
INA
NC
IAL
O
FF
ICE
R
Pre
pa
re d
eta
iled
pro
ce
du
res f
or
dis
po
sa
l o
f a
sse
ts in
clu
din
g c
on
de
mn
atio
ns a
nd
en
su
re t
ha
t th
ese
are
no
tifie
d t
o m
an
ag
ers
.
26
.2.2
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
P
rep
are
pro
ce
du
res f
or
reco
rdin
g a
nd
acco
un
tin
g f
or
losse
s,
sp
ecia
l p
aym
en
ts a
nd
in
form
ing
po
lice
in
ca
se
s o
f suspecte
d a
rson o
r th
eft.
26
.2.2
A
LL
ST
AF
F
Dis
co
ve
ry o
r su
sp
icio
n o
f lo
ss o
f a
ny k
ind
mu
st
be
re
po
rte
d im
me
dia
tely
to
eith
er
he
ad
of
de
pa
rtm
en
t o
r n
om
inate
d o
ffic
er.
The
head o
f d
epart
men
t /
nom
inate
d o
ffic
er
should
th
en
info
rm
the
Ch
ief
Exe
cu
tive
an
d C
hie
f F
ina
ncia
l O
ffic
er.
26
.2.2
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
W
he
re a
cri
min
al
off
en
ce
is s
usp
ecte
d,
the
Ch
ief
Fin
an
cia
l O
ffic
er
mu
st
info
rm t
he
po
lice
if
the
ft
or
ars
on
is in
vo
lve
d.
In c
ase
s o
f fr
au
d a
nd
co
rru
ptio
n C
hie
f F
ina
ncia
l O
ffic
er
mu
st
info
rm t
he
rele
va
nt
LC
FS
an
d N
HS
Co
un
ter
Fra
ud
Au
tho
rity
(N
HS
CF
A)
in lin
e w
ith
Se
cre
tary
of
Sta
te
directions.
26
.2.2
C
HIE
F
FIN
AN
CIA
LO
FF
ICE
R
No
tify
NH
SC
FA
an
d E
xte
rna
l A
ud
it o
f a
ll fr
au
ds.
26
.2.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
N
otify
th
e B
oa
rd a
nd
Exte
rna
l A
ud
ito
r o
f lo
sse
s c
au
se
d b
y t
he
ft,
ars
on
, n
eg
lect
of
du
ty o
r g
ross
ca
rele
ssn
ess (
unle
ss tr
ivia
l).
26
.2.4
B
OA
RD
A
pp
rove
wri
te o
ff o
f lo
sse
s (
with
in lim
its d
ele
ga
ted
by D
ep
art
me
nt
of
He
alth
).
26
.2.6
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
C
on
sid
er
wh
eth
er
an
y in
su
ran
ce
cla
im c
an
be
ma
de
.
26
.2.7
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
M
ain
tain
lo
sse
s a
nd
sp
ecia
l p
aym
en
ts r
eg
iste
r.
27
.1.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
R
esp
on
sib
le f
or
accu
racy a
nd
se
cu
rity
of
co
mp
ute
rise
d f
ina
ncia
l d
ata
27
.1.2
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
S
atisfy
him
se
lf /
he
rse
lf t
ha
t n
ew
fin
an
cia
l syste
ms a
nd
am
en
dm
en
ts t
o c
urr
en
t fin
an
cia
l
syste
ms a
re d
eve
lop
ed
in a
contr
olle
d m
anner
and thoro
ughly
teste
d p
rior
to im
ple
menta
tion. W
here
this
is u
ndert
aken b
y a
noth
er
org
anis
ation a
ssura
nces o
f ad
eq
ua
cy m
ust
be o
bta
ined
fro
m t
he
m
pri
or
to im
ple
menta
tio
n.
27
.1.3
S
EN
IOR
IN
FO
RM
AT
ION
R
ISK
OF
FIC
ER
S
ha
ll p
ub
lish
an
d m
ain
tain
a F
ree
do
m o
f In
form
atio
n S
ch
em
e.
Page 285 of 300

ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
03
of
11
7
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
27
.2
RE
LE
VA
NT
OF
FIC
ER
S
Se
nd
pro
po
sa
ls f
or
ge
ne
ral co
mp
ute
r syste
ms t
o C
hie
f D
igita
l a
nd
Te
ch
no
log
y O
ffic
er
27
.3
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
E
nsu
re t
ha
t co
ntr
acts
with
oth
er
bo
die
s f
or
the
pro
vis
ion
of
co
mp
ute
r se
rvic
es f
or
fin
an
cia
l a
pp
lica
tio
ns c
lea
rly d
efin
e r
esp
on
sib
ility o
f a
ll p
art
ies f
or
se
cu
rity
, p
riva
cy,
accu
racy,
co
mp
lete
ne
ss a
nd
tim
elin
ess o
f data
during p
rocessin
g, tr
ansm
issio
n a
nd s
tora
ge, an
d a
llow
for
audit revie
w.
Se
ek p
eri
od
ic a
ssu
ran
ce
s f
rom
th
e p
rovid
er
tha
t a
de
qu
ate
co
ntr
ols
are
in
op
era
tio
n.
27
.4
CH
IEF
DIG
ITA
L A
ND
TE
CH
NO
LO
GY
OF
FIC
ER
E
nsu
re t
ha
t ri
sks t
o t
he
Tru
st
fro
m u
se
of
IT a
re id
en
tifie
d a
nd
co
nsid
ere
d a
nd
th
at
dis
aste
r
reco
ve
ry p
lan
s a
re in
pla
ce
.
27
.5
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
W
he
re c
om
pu
ter
syste
ms h
ave
an
im
pa
ct
on
co
rpo
rate
fin
an
cia
l syste
ms s
atisfy
him
se
lf /
he
rse
lf
tha
t:
Syste
m a
cq
uis
itio
n,
de
ve
lop
me
nt
an
d m
ain
ten
an
ce
are
in
lin
e w
ith
co
rpo
rate
po
licie
s.
Da
ta a
sse
mb
led
fo
r p
roce
ssin
g b
y f
ina
ncia
l syste
ms is a
de
qu
ate
, a
ccu
rate
, co
mp
lete
an
d t
ime
ly,
an
d t
ha
t a m
an
ag
em
en
t ra
il e
xis
ts.
Th
e C
hie
f F
ina
ncia
l O
ffic
er
an
d s
taff
ha
ve
acce
ss t
o s
uch
da
ta.
Su
ch
co
mp
ute
r a
ud
it r
evie
ws a
re b
ein
g c
arr
ied
ou
t a
s a
re c
on
sid
ere
d n
ece
ssa
ry.
28
.2
CH
IEF
EX
EC
UT
IVE
R
esp
on
sib
le f
or
en
su
rin
g p
atie
nts
an
d g
ua
rdia
ns a
re i
nfo
rme
d a
bo
ut
pa
tie
nts
’ m
on
ey a
nd
p
rop
ert
y p
roce
du
res o
n a
dm
issio
n.
28
.3
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
P
rovid
e d
eta
iled
wri
tte
n in
str
uctio
ns o
n t
he
co
lle
ctio
n,
cu
sto
dy,
inve
stm
en
t, r
eco
rdin
g,
sa
feke
ep
ing
an
d d
isp
osa
l of
pa
tie
nts
’ p
rop
ert
y (
inclu
din
g in
str
uctio
ns o
n t
he
dis
po
sa
l o
f th
e
pro
pe
rty o
f d
ece
ase
d p
atie
nts
an
d o
f p
atie
nts
tra
nsfe
rre
d t
o o
the
r p
rem
ise
s)
for
all
sta
ff w
ho
se
du
ty is t
o a
dm
inis
ter,
in
an
y w
ay,
the
pro
pe
rty o
f.
28
.6
SE
RV
ICE
MA
NG
ER
S
Info
rm s
taff
of
the
ir r
esp
on
sib
ilitie
s a
nd
du
tie
s f
or
the
ad
min
istr
atio
n o
f th
e p
rop
ert
y o
f p
atie
nts
.
29
.1.3
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
S
ha
ll e
nsu
re t
ha
t e
ach
tru
st
fun
d w
hic
h t
he
Tru
st
is r
esp
on
sib
le f
or
ma
na
gin
g is m
an
ag
ed
ap
pro
pri
ate
ly.
30
.1.1
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
E
nsu
re a
ll s
taff
are
ma
de
aw
are
of
the
Tru
st
po
licy o
n t
he
acce
pta
nce
of
gifts
an
d o
the
r b
en
efits
in k
ind
by s
taff
.
32
CH
IEF
EX
EC
UT
IVE
R
ete
ntio
n o
f d
ocu
me
nt
pro
ce
du
res in
acco
rda
nce
with
HS
C 1
99
9/0
53
. (H
SC
19
99
/05
3 h
as b
ee
n
rep
lace
d b
y t
he
NH
S c
od
e o
f p
ractice
: P
art
s 1
an
d 2
(A
pri
l 2
00
6)
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 286 of 300
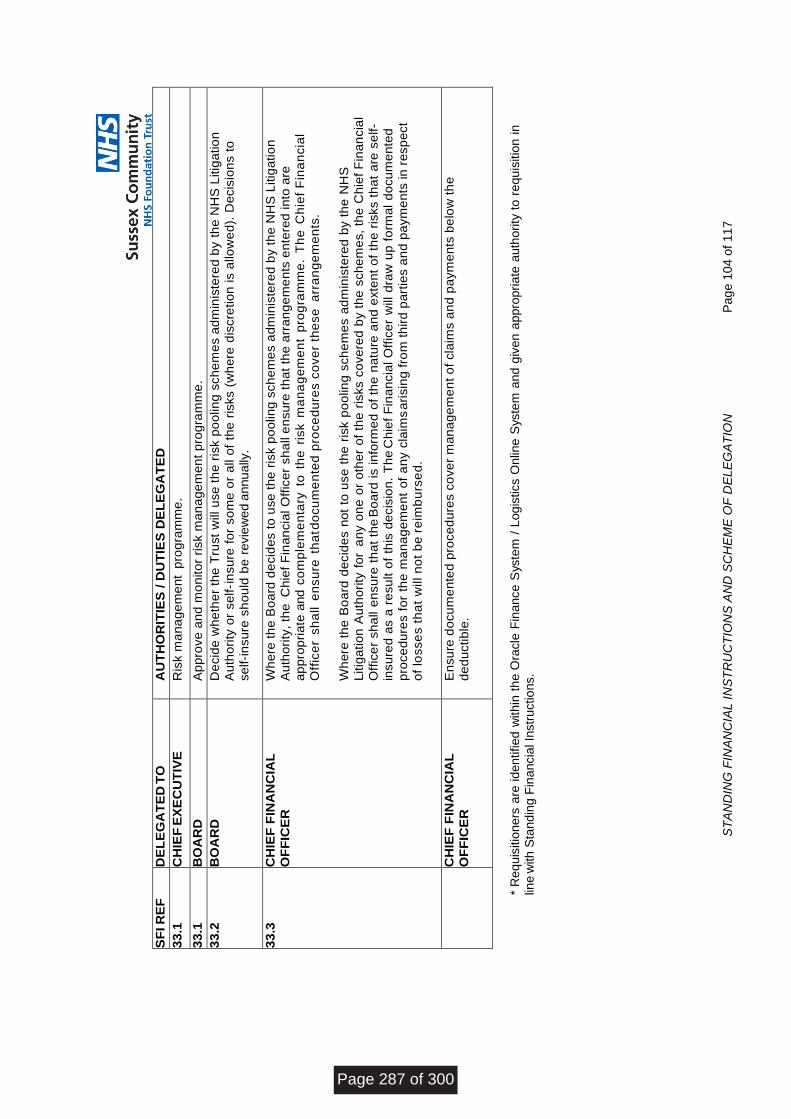
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
04
of
11
7
SF
I R
EF
D
EL
EG
AT
ED
TO
A
UT
HO
RIT
IES
/ D
UT
IES
DE
LE
GA
TE
D
33
.1
CH
IEF
EX
EC
UT
IVE
R
isk m
an
ag
em
en
t p
rog
ram
me
.
33
.1
BO
AR
D
Ap
pro
ve
an
d m
on
ito
r ri
sk m
an
ag
em
en
t p
rog
ram
me
.
33
.2
BO
AR
D
De
cid
e w
he
the
r th
e T
rust
will u
se
th
e r
isk p
oo
lin
g s
ch
em
es a
dm
inis
tere
d b
y t
he
NH
S L
itig
atio
n
Au
tho
rity
or
se
lf- i
nsu
re f
or
so
me
or
all o
f th
e r
isks (
wh
ere
dis
cre
tio
n is a
llow
ed
). D
ecis
ion
s t
o
se
lf-i
nsu
re s
ho
uld
be
revie
we
d a
nnu
ally
.
33
.3
CH
IEF
FIN
AN
CIA
L
OF
FIC
ER
W
he
re t
he
Bo
ard
de
cid
es t
o u
se
th
e r
isk p
oo
lin
g s
ch
em
es a
dm
inis
tere
d b
y t
he
NH
S L
itig
atio
n
Au
tho
rity
, th
e C
hie
f F
ina
ncia
l O
ffic
er
sh
all
en
su
re t
ha
t th
e a
rra
ng
em
en
ts e
nte
red
in
to a
re
ap
pro
pri
ate
and c
om
ple
me
nta
ry t
o th
e r
isk m
an
ag
em
en
t p
rog
ram
me
. T
he
C
hie
f F
ina
ncia
l
Off
ice
r sh
all e
nsu
re t
ha
t do
cu
me
nte
d p
roce
du
res c
ove
r th
ese
a
rra
ng
em
en
ts.
Wh
ere
th
e B
oa
rd d
ecid
es n
ot
to u
se
th
e r
isk p
oo
ling
sch
em
es a
dm
inis
tere
d b
y t
he
NH
S
Litig
atio
n A
uth
ori
ty f
or
an
y o
ne
or
oth
er
of
the
ris
ks c
ove
red
by t
he
sch
em
es,
the
Ch
ief
Fin
an
cia
l
Off
ice
r sh
all
en
su
re t
ha
t th
e B
oa
rd is in
form
ed
of
the
na
ture
an
d e
xte
nt
of
the
ris
ks t
ha
t a
re s
elf-
insu
red
as a
re
su
lt o
f th
is d
ecis
ion
. T
he
Ch
ief
Fin
an
cia
l O
ffic
er
will
dra
w u
p f
orm
al
do
cu
me
nte
d
pro
ce
du
res f
or
the
ma
na
ge
me
nt
of
an
y c
laim
s a
risin
g f
rom
th
ird
pa
rtie
s a
nd
pa
ym
en
ts in
re
sp
ect
of
losse
s t
ha
t w
ill n
ot
be
re
imb
urs
ed
.
C
HIE
F F
INA
NC
IAL
OF
FIC
ER
E
nsu
re d
ocu
me
nte
d p
roce
du
res c
ove
r m
an
ag
em
en
t o
f cla
ims a
nd
pa
ym
en
ts b
elo
w t
he
de
du
ctib
le.
* R
eq
uis
itio
ners
are
identified
within
th
e O
racle
Fin
ance
Syste
m /
Logis
tics O
nlin
e S
yste
m a
nd
giv
en a
ppro
pri
ate
auth
ority
to
requ
isitio
n in
line w
ith S
tand
ing
Fin
ancia
l In
str
uctio
ns.
Page 287 of 300
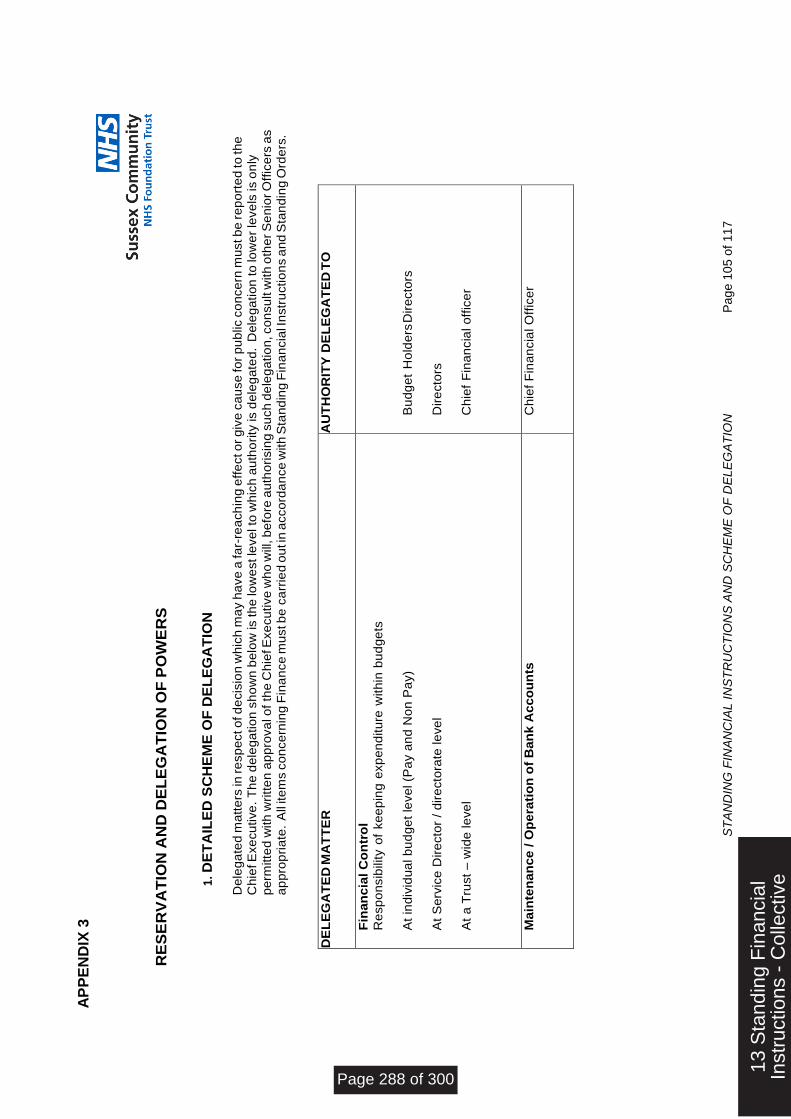
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
05
of
11
7
RE
SE
RV
AT
ION
AN
D D
EL
EG
AT
ION
OF
PO
WE
RS
1. D
ET
AIL
ED
SC
HE
ME
OF
DE
LE
GA
TIO
N
De
leg
ate
d m
att
ers
in re
sp
ect o
f d
ecis
ion
wh
ich
ma
y h
ave
a fa
r-re
ach
ing
eff
ect o
r g
ive
ca
use
fo
r p
ub
lic c
on
ce
rn m
ust b
e re
po
rte
d to
th
e
Ch
ief E
xe
cu
tive
. T
he
de
leg
atio
n s
ho
wn
be
low
is th
e lo
we
st le
ve
l to
wh
ich
au
tho
rity
is d
ele
ga
ted
. D
ele
ga
tio
n to
low
er
leve
ls is o
nly
pe
rmitte
d w
ith
wri
tte
n a
pp
rova
l o
f th
e C
hie
f E
xe
cu
tive
wh
o w
ill, b
efo
re a
uth
ori
sin
g s
uch
de
leg
atio
n, co
nsu
lt w
ith
oth
er S
en
ior O
ffic
ers
as
ap
pro
pri
ate
. A
ll ite
ms c
on
ce
rnin
g F
ina
nce
mu
st b
e c
arr
ied
ou
t in
acco
rda
nce
with
Sta
nd
ing
Fin
an
cia
l In
str
uctio
ns a
nd
Sta
nd
ing
Ord
ers
.
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Fin
an
cia
l C
on
tro
l
Re
sp
on
sib
ility o
f ke
ep
ing
exp
en
ditu
re w
ith
in b
ud
ge
ts
At
ind
ivid
ua
l b
ud
ge
t le
ve
l (P
ay a
nd
No
n P
ay)
At
Se
rvic
e D
ire
cto
r /
dir
ecto
rate
le
ve
l
At
a T
rust
– w
ide
le
ve
l
Bu
dg
et
Ho
lde
rs D
ire
cto
rs
Dir
ecto
rs
Ch
ief
Fin
an
cia
l o
ffic
er
Ma
inte
na
nc
e / O
pe
rati
on
of
Ba
nk
Ac
co
un
ts
Ch
ief
Fin
an
cia
l O
ffic
er
AP
PE
ND
IX 3
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 288 of 300
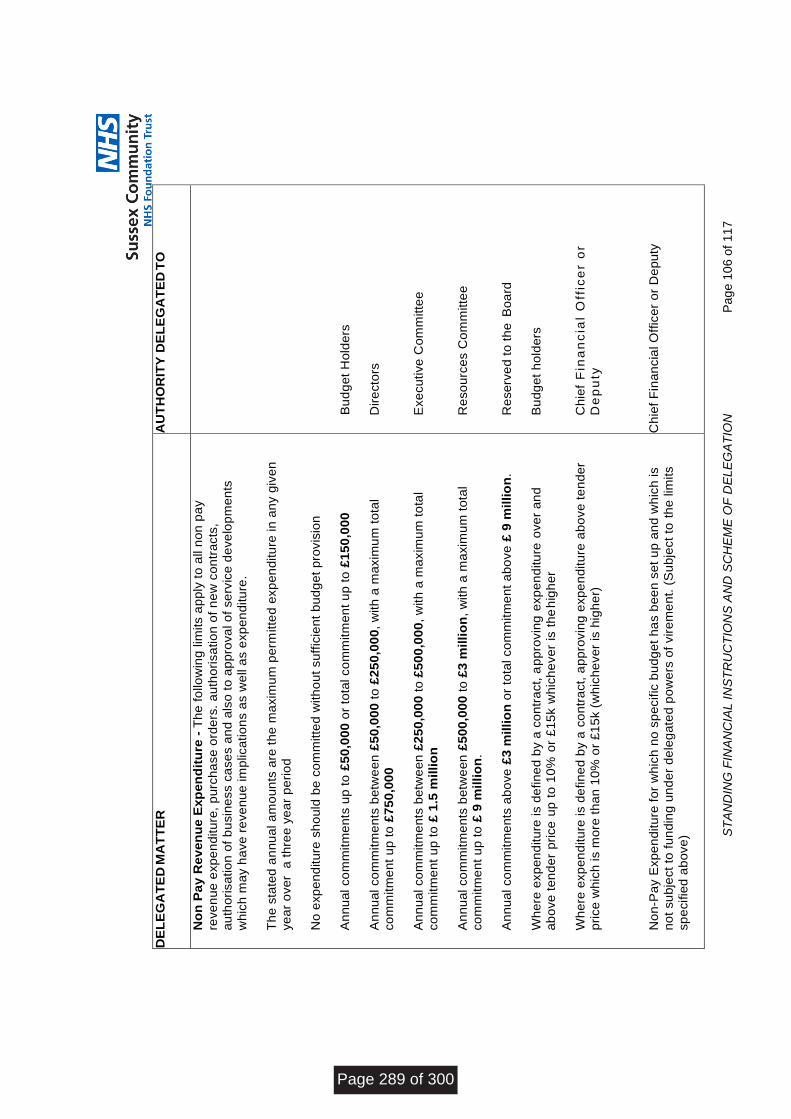
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
06
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
No
n P
ay
Re
ven
ue
Exp
en
dit
ure
- T
he
fo
llo
win
g lim
its a
pp
ly t
o a
ll n
on
pa
y
reve
nu
e e
xp
en
ditu
re,
pu
rch
ase
ord
ers
. a
uth
ori
sa
tio
n o
f n
ew
co
ntr
acts
, a
uth
ori
sa
tio
n o
f b
usin
ess c
ase
s a
nd
als
o t
o a
pp
rova
l o
f se
rvic
e d
eve
lop
me
nts
wh
ich
ma
y h
ave
re
ve
nu
e im
plica
tio
ns a
s w
ell a
s e
xp
en
ditu
re.
Th
e s
tate
d a
nn
ua
l a
mo
un
ts a
re t
he
ma
xim
um
pe
rmitte
d e
xp
en
ditu
re in
an
y g
ive
n
ye
ar
ove
r a
th
ree
ye
ar
pe
rio
d
N
o e
xp
en
ditu
re s
ho
uld
be
co
mm
itte
d w
ith
ou
t su
ffic
ien
t b
ud
ge
t p
rovis
ion
An
nu
al co
mm
itm
en
ts u
p t
o £
50
,00
0 o
r to
tal co
mm
itm
en
t u
p t
o £
15
0,0
00
A
nn
ua
l co
mm
itm
en
ts b
etw
ee
n £
50
,00
0 t
o £
25
0,0
00
, w
ith
a m
axim
um
to
tal
co
mm
itm
en
t u
p t
o £
75
0,0
00
An
nu
al co
mm
itm
en
ts b
etw
ee
n £
25
0,0
00
to
£5
00
,00
0,
with
a m
axim
um
to
tal
co
mm
itm
en
t u
p t
o £
1.5
millio
n
An
nu
al co
mm
itm
en
ts b
etw
ee
n £
50
0,0
00
to
£3
milli
on
, w
ith
a m
axim
um
to
tal
co
mm
itm
en
t u
p t
o £
9 m
illi
on
.
An
nu
al co
mm
itm
en
ts a
bo
ve
£3
millio
n o
r to
tal co
mm
itm
en
t a
bo
ve
£ 9
mil
lio
n.
Wh
ere
exp
en
ditu
re is d
efin
ed
by a
co
ntr
act,
ap
pro
vin
g e
xp
en
ditu
re o
ve
r a
nd
a
bo
ve
te
nd
er
pri
ce
up
to
10
% o
r £
15
k w
hic
he
ve
r is
th
e h
igh
er
Wh
ere
exp
en
ditu
re is d
efin
ed
by a
co
ntr
act,
ap
pro
vin
g e
xp
en
ditu
re a
bo
ve
te
nd
er
pri
ce
wh
ich
is m
ore
th
an
10
% o
r £
15
k (
wh
ich
eve
r is
hig
he
r)
No
n-P
ay E
xp
en
ditu
re f
or
wh
ich
no
sp
ecific
bu
dg
et
ha
s b
ee
n s
et
up
an
d w
hic
h is
no
t su
bje
ct
to f
un
din
g u
nd
er
de
leg
ate
d p
ow
ers
of
vir
em
en
t. (
Su
bje
ct
to t
he
lim
its
sp
ecifie
d a
bo
ve
)
Bu
dg
et
Ho
lde
rs
Dir
ecto
rs
Exe
cu
tive
Co
mm
itte
e
Re
so
urc
es C
om
mitte
e
Re
se
rve
d t
o t
he
B
oa
rd
Bu
dg
et
ho
lde
rs
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Page 289 of 300
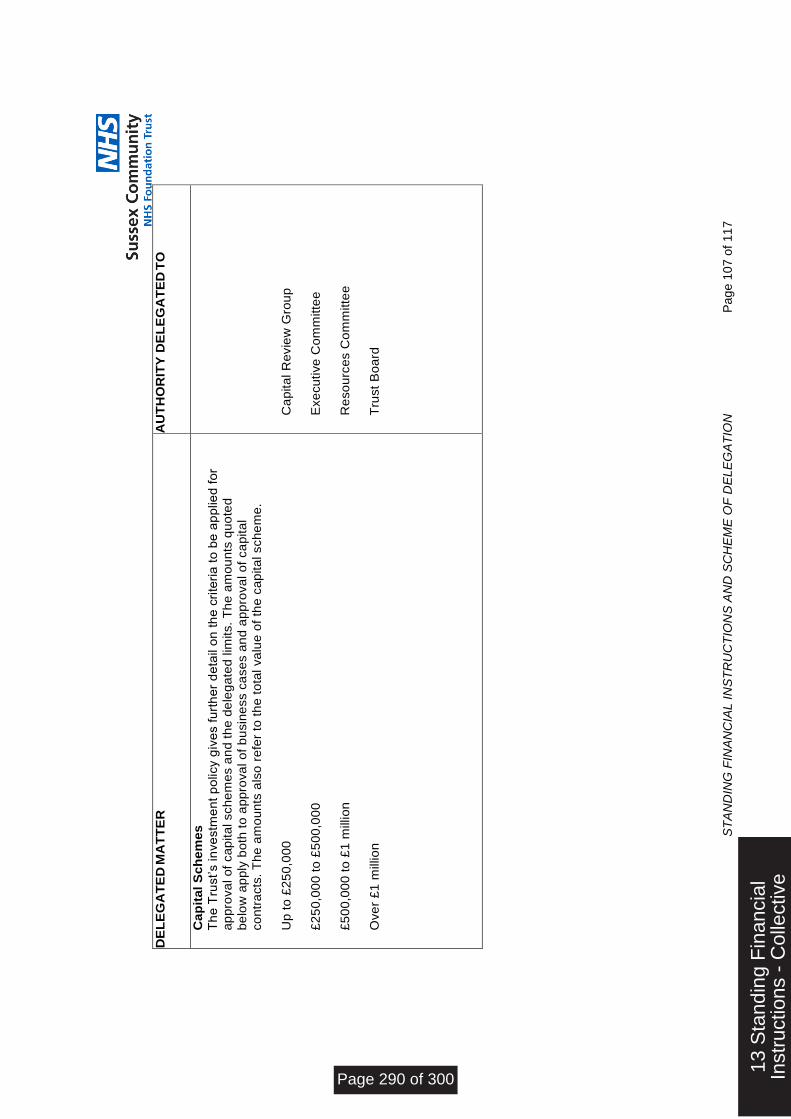
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
07
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Ca
pit
al S
ch
em
es
Th
e T
rust’s in
ve
stm
en
t p
olicy g
ive
s f
urt
he
r d
eta
il o
n t
he
cri
teri
a t
o b
e a
pp
lied
fo
r a
pp
rova
l o
f ca
pita
l sch
em
es a
nd
th
e d
ele
ga
ted
lim
its.
Th
e a
mo
un
ts q
uo
ted
be
low
ap
ply
bo
th t
o a
pp
rova
l o
f b
usin
ess c
ase
s a
nd
ap
pro
va
l o
f ca
pita
l
co
ntr
acts
. T
he
am
ou
nts
als
o r
efe
r to
th
e t
ota
l va
lue
of
the
ca
pita
l sch
em
e.
Up
to
£2
50
,00
0
£
25
0,0
00
to
£5
00
,00
0
£5
00
,00
0 t
o £
1 m
illio
n
Ove
r £
1 m
illio
n
Ca
pita
l R
evie
w G
rou
p
Exe
cu
tive
Co
mm
itte
e
Re
so
urc
es C
om
mitte
e
Tru
st
Bo
ard
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 290 of 300
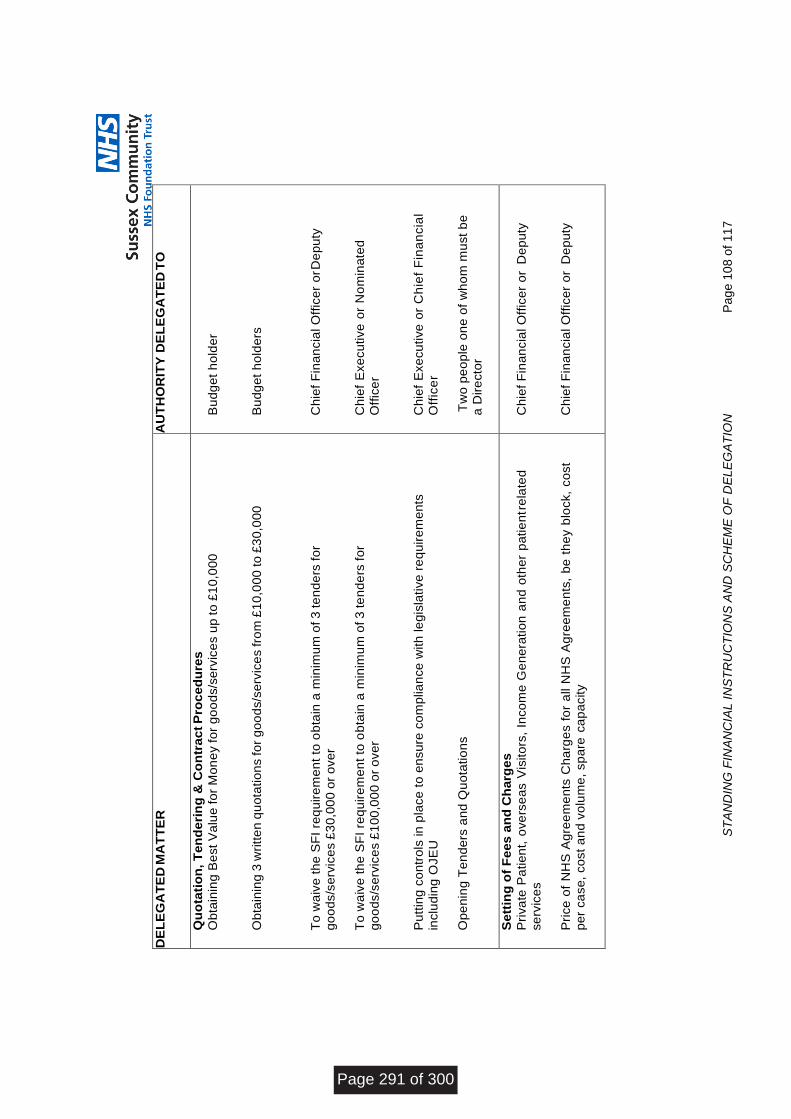
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
08
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Qu
ota
tio
n, T
en
de
rin
g &
Co
ntr
ac
t P
roc
ed
ure
s
Ob
tain
ing
Be
st V
alu
e fo
r M
on
ey fo
r g
oo
ds/s
erv
ice
s u
p to
£1
0,0
00
O
bta
inin
g 3
wri
tte
n q
uo
tatio
ns fo
r g
oo
ds/s
erv
ice
s fro
m £
10
,00
0 to
£3
0,0
00
To
wa
ive
th
e S
FI
req
uir
em
en
t to
ob
tain
a m
inim
um
of 3
te
nd
ers
fo
r
go
od
s/s
erv
ice
s £
30
,00
0 o
r o
ve
r
To
wa
ive
th
e S
FI
req
uir
em
en
t to
ob
tain
a m
inim
um
of 3
te
nd
ers
fo
r
go
od
s/s
erv
ice
s £
10
0,0
00
or
ove
r P
utt
ing
co
ntr
ols
in
pla
ce
to
en
su
re c
om
plia
nce
with
le
gis
lative
re
qu
ire
me
nts
inclu
din
g O
JE
U
Op
en
ing
Te
nd
ers
an
d Q
uo
tatio
ns
Bu
dg
et
ho
lde
r
Bu
dg
et
ho
lde
rs
Ch
ief
Fin
an
cia
l O
ffic
er
or D
ep
uty
Ch
ief
Exe
cu
tive
or
No
min
ate
d
Off
ice
r C
hie
f E
xe
cu
tive
or
Ch
ief
Fin
an
cia
l
Off
ice
r
Tw
o p
eo
ple
on
e o
f w
ho
m m
ust
be
a
Dir
ecto
r
Ch
ief
Exe
cu
tive
or
No
min
ate
d
Off
ice
r/s
Se
ttin
g o
f F
ees
an
d C
harg
es
Pri
va
te P
atie
nt,
ove
rse
as V
isito
rs,
Inco
me
Ge
ne
ratio
n a
nd
oth
er
pa
tie
nt r
ela
ted
se
rvic
es
Pri
ce
of
NH
S A
gre
em
en
ts C
ha
rge
s f
or
all N
HS
Ag
ree
me
nts
, b
e t
he
y b
lock,
co
st
pe
r ca
se
, co
st
an
d v
olu
me
, sp
are
ca
pa
city
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Page 291 of 300
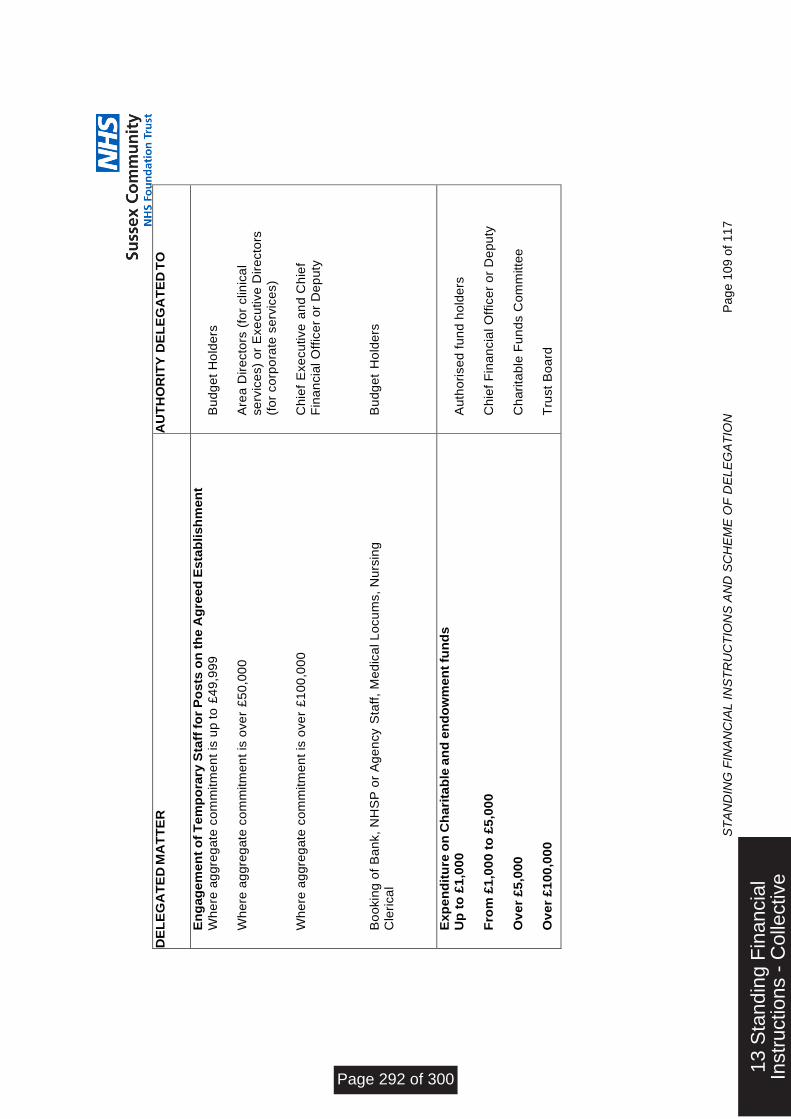
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
09
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
En
gag
em
en
t o
f T
em
po
rary
Sta
ff f
or
Po
sts
on
th
e A
gre
ed
Es
tab
lish
men
t
Wh
ere
ag
gre
ga
te c
om
mitm
en
t is
up
to
£4
9,9
99
W
he
re a
gg
reg
ate
co
mm
itm
en
t is
ove
r £
50
,00
0
Wh
ere
ag
gre
ga
te c
om
mitm
en
t is
ove
r £
10
0,0
00
Bo
okin
g o
f B
an
k,
NH
SP
or
Ag
en
cy S
taff
, M
ed
ica
l L
ocu
ms,
Nu
rsin
g
Cle
rica
l
Bu
dg
et
Ho
lde
rs
Are
a D
ire
cto
rs (
for
clin
ica
l
se
rvic
es)
or
Exe
cu
tive
Dir
ecto
rs
(fo
r co
rpo
rate
se
rvic
es)
Ch
ief
Exe
cu
tive
an
d C
hie
f
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Bu
dg
et
Ho
lde
rs
Exp
en
dit
ure
on
Ch
ari
tab
le a
nd
en
do
wm
en
t fu
nd
s
Up
to
£1
,00
0
Fro
m £
1,0
00
to
£5
,00
0
Ov
er
£5
,000
Ov
er
£1
00
,00
0
Au
tho
rise
d f
un
d h
old
ers
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Ch
ari
tab
le F
un
ds C
om
mitte
e
Tru
st
Bo
ard
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 292 of 300
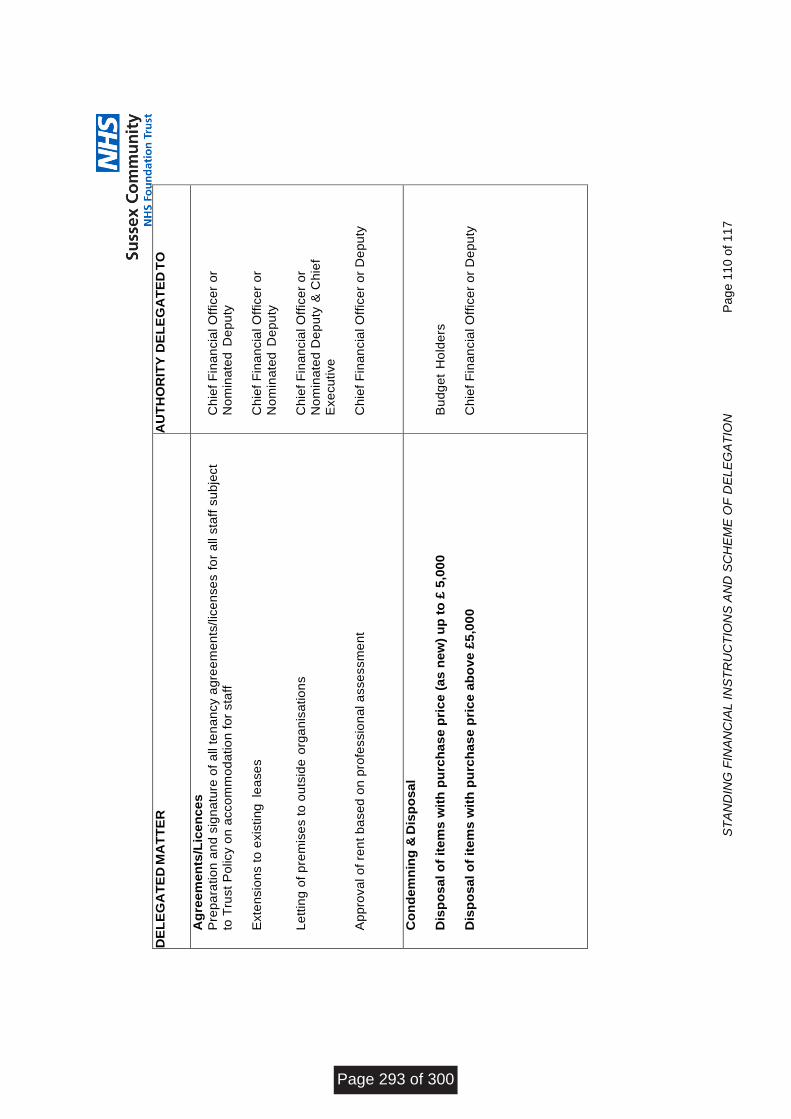
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
10
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Ag
ree
men
ts/L
ice
nc
es
Pre
pa
ratio
n a
nd
sig
na
ture
of
all
ten
an
cy a
gre
em
en
ts/lic
en
se
s f
or
all s
taff
su
bje
ct
to T
rust
Po
licy o
n a
cco
mm
od
atio
n f
or
sta
ff
Exte
nsio
ns t
o e
xis
tin
g le
ase
s
Le
ttin
g o
f p
rem
ise
s t
o o
uts
ide
org
an
isa
tio
ns
Ap
pro
va
l o
f re
nt
ba
se
d o
n p
rofe
ssio
na
l a
sse
ssm
en
t
Ch
ief
Fin
an
cia
l O
ffic
er
or
No
min
ate
d D
ep
uty
Ch
ief
Fin
an
cia
l O
ffic
er
or
No
min
ate
d D
ep
uty
Ch
ief
Fin
an
cia
l O
ffic
er
or
No
min
ate
d D
ep
uty
& C
hie
f
Exe
cu
tive
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Co
nd
em
nin
g &
Dis
po
sa
l
Dis
po
sa
l o
f it
em
s w
ith
pu
rch
as
e p
ric
e (
as
ne
w)
up
to
£ 5
,00
0
Dis
po
sa
l o
f it
em
s w
ith
pu
rch
as
e p
ric
e a
bo
ve
£5
,00
0
Bu
dg
et
Ho
lde
rs
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Page 293 of 300
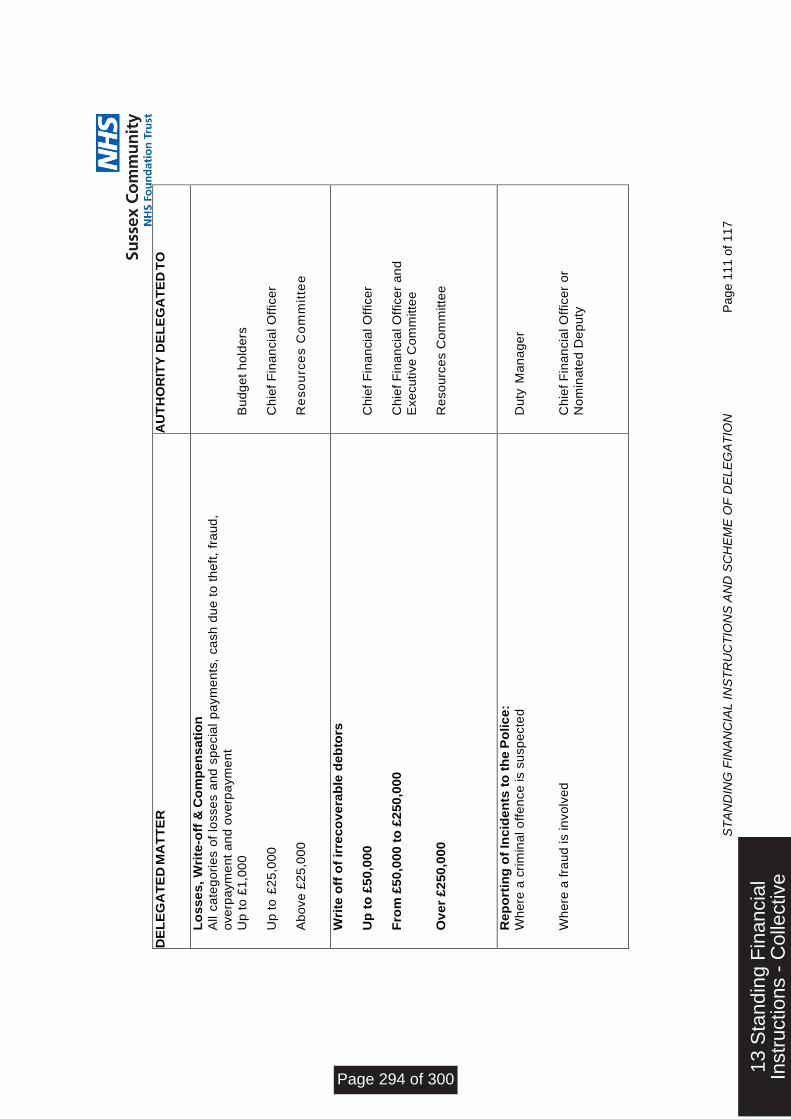
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
11
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Lo
ss
es
, W
rite
-off
& C
om
pe
ns
ati
on
All
ca
teg
ori
es o
f lo
sse
s a
nd
sp
ecia
l p
aym
en
ts,
ca
sh
du
e t
o t
he
ft,
fra
ud
, o
ve
rpa
ym
en
t a
nd
ove
rpa
ym
en
t
Up
to
£1
,00
0
Up
to
£2
5,0
00
Ab
ove
£2
5,0
00
Bu
dg
et
ho
lde
rs
Ch
ief
Fin
an
cia
l O
ffic
er
Re
so
urc
es C
om
mit
tee
Wri
te o
ff o
f ir
rec
ov
era
ble
de
bto
rs
Up
to
£5
0,0
00
Fro
m £
50
,000
to
£2
50
,000
Ov
er
£2
50
,00
0
Ch
ief
Fin
an
cia
l O
ffic
er
Ch
ief
Fin
an
cia
l O
ffic
er
an
d
Exe
cu
tive
Co
mm
itte
e
Re
so
urc
es C
om
mitte
e
Re
po
rtin
g o
f In
cid
en
ts t
o t
he
Po
lic
e:
Wh
ere
a c
rim
ina
l o
ffe
nce
is s
usp
ecte
d
Wh
ere
a f
rau
d is in
vo
lve
d
Du
ty M
an
ag
er
Ch
ief
Fin
an
cia
l O
ffic
er
or
No
min
ate
d D
ep
uty
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 294 of 300
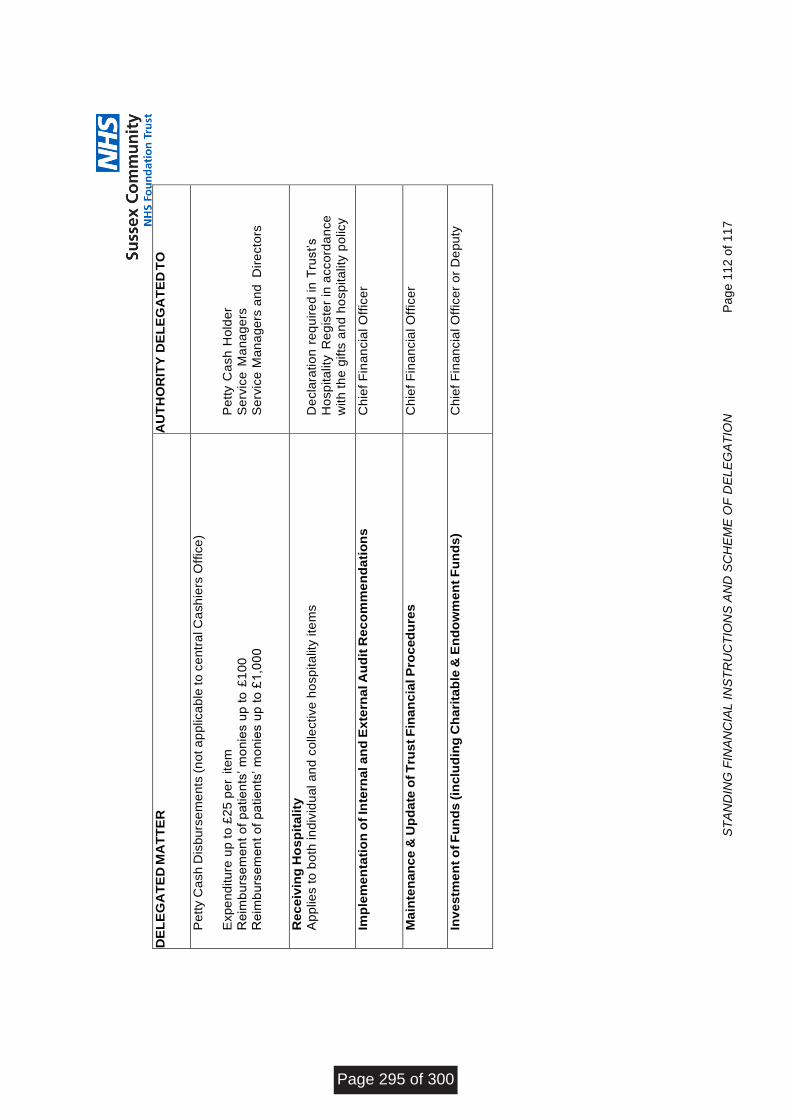
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
12
of
11
7
DE
LE
GA
TE
D M
AT
TE
R
AU
TH
OR
ITY
DE
LE
GA
TE
D T
O
Pe
tty C
ash
Dis
bu
rse
me
nts
(n
ot a
pp
lica
ble
to
ce
ntr
al C
ash
iers
Off
ice
)
Exp
en
ditu
re u
p t
o £
25
pe
r ite
m
Re
imb
urs
em
en
t o
f p
atie
nts
’ m
on
ies u
p t
o £
10
0
Re
imb
urs
em
en
t o
f p
atie
nts
’ m
on
ies u
p t
o £
1,0
00
Pe
tty C
ash
Ho
lde
r
Se
rvic
e M
an
ag
ers
Se
rvic
e M
an
ag
ers
an
d D
ire
cto
rs
Re
ce
ivin
g H
os
pit
ality
Ap
plie
s t
o b
oth
in
div
idu
al a
nd
co
llective
ho
sp
ita
lity ite
ms
De
cla
ratio
n r
eq
uir
ed
in
Tru
st’s
Ho
sp
ita
lity R
eg
iste
r in
acco
rda
nce
with
th
e g
ifts
an
d h
osp
ita
lity
po
licy
Imp
lem
en
tati
on
of
Inte
rna
l a
nd
Ex
tern
al A
ud
it R
ec
om
me
nd
ati
on
s
Ch
ief
Fin
an
cia
l O
ffic
er
Ma
inte
na
nc
e &
Up
da
te o
f T
rus
t F
ina
nc
ial P
roc
ed
ure
s
Ch
ief
Fin
an
cia
l O
ffic
er
Inv
es
tme
nt
of F
un
ds
(in
clu
din
g C
ha
rita
ble
& E
nd
ow
men
t F
un
ds
) C
hie
f F
ina
ncia
l O
ffic
er
or
De
pu
ty
Page 295 of 300
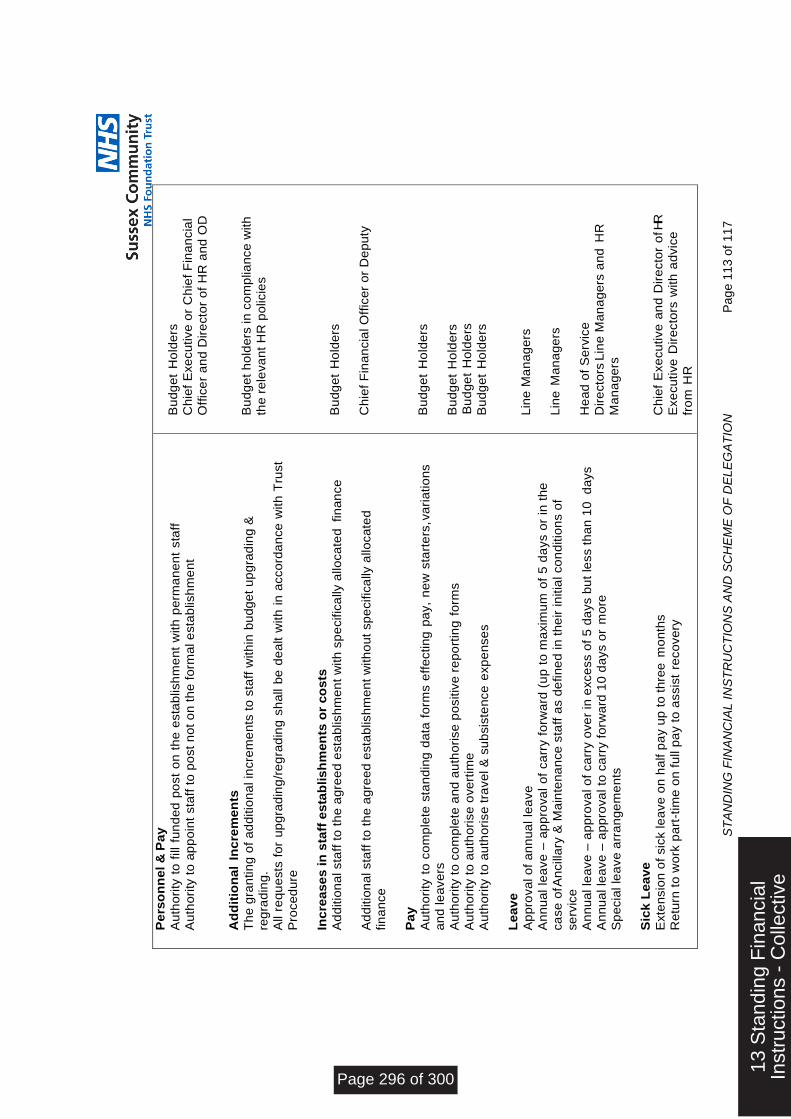
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
13
of
11
7
Pe
rso
nn
el &
Pay
Au
tho
rity
to
fill
fu
nd
ed
po
st
on
th
e e
sta
blish
me
nt
with
pe
rma
ne
nt
sta
ff
Au
tho
rity
to
ap
po
int
sta
ff t
o p
ost
no
t o
n t
he
fo
rma
l e
sta
blish
me
nt
Ad
dit
ion
al
Inc
rem
en
ts
Th
e g
ran
tin
g o
f a
dd
itio
na
l in
cre
me
nts
to
sta
ff w
ith
in b
udg
et
up
gra
din
g &
re
gra
din
g.
All
req
ue
sts
fo
r u
pg
rad
ing
/re
gra
din
g s
ha
ll be d
ea
lt w
ith
in
acco
rda
nce
with
Tru
st
Pro
ce
du
re
Inc
rea
se
s in
sta
ff e
sta
blis
hm
en
ts o
r co
sts
Ad
ditio
na
l sta
ff t
o t
he
ag
ree
d e
sta
blis
hm
en
t w
ith
sp
ecific
ally a
llo
ca
ted
fin
an
ce
A
dd
itio
na
l sta
ff t
o t
he
ag
ree
d e
sta
blis
hm
en
t w
ith
ou
t sp
ecific
ally a
llo
ca
ted
fin
an
ce
Pa
y
Au
tho
rity
to
co
mp
lete
sta
nd
ing
da
ta f
orm
s e
ffe
ctin
g p
ay,
ne
w s
tart
ers
, va
ria
tio
ns
an
d le
ave
rs
Au
tho
rity
to
co
mp
lete
an
d a
uth
ori
se
po
sitiv
e r
ep
ort
ing
fo
rms
Au
tho
rity
to
au
tho
rise
ove
rtim
e
Au
tho
rity
to
au
tho
rise
tra
ve
l &
su
bsis
ten
ce
exp
en
se
s
Le
av
e
Ap
pro
va
l o
f a
nn
ua
l le
ave
An
nu
al
lea
ve
– a
pp
rova
l o
f ca
rry f
orw
ard
(u
p t
o m
axim
um
of
5 d
ays o
r in
th
e
ca
se
of A
ncill
ary
& M
ain
ten
an
ce
sta
ff a
s d
efin
ed
in
th
eir
in
itia
l co
nd
itio
ns o
f
se
rvic
e
An
nu
al le
ave
– a
pp
rova
l o
f ca
rry o
ve
r in
exce
ss o
f 5
da
ys b
ut
less t
ha
n 1
0 d
ays
An
nu
al le
ave
– a
pp
rova
l to
ca
rry f
orw
ard
10
da
ys o
r m
ore
Sp
ecia
l le
ave
arr
an
ge
me
nts
Sic
k L
ea
ve
Exte
nsio
n o
f sic
k le
ave
on
ha
lf p
ay u
p t
o t
hre
e m
on
ths
Re
turn
to
wo
rk p
art
-tim
e o
n f
ull
pa
y t
o a
ssis
t re
co
ve
ry
Bu
dg
et
Ho
lde
rs
Ch
ief
Exe
cu
tive
or
Ch
ief
Fin
an
cia
l
Off
ice
r a
nd
Dir
ecto
r o
f H
R a
nd
OD
B
ud
ge
t h
old
ers
in
co
mp
lia
nce
with
the
re
leva
nt
HR
po
licie
s
Bu
dg
et
Ho
lde
rs
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
B
ud
ge
t H
old
ers
Bu
dg
et
Ho
lde
rs
Bu
dg
et
Ho
lde
rs
Bu
dg
et
Ho
lde
rs
Lin
e M
an
ag
ers
L
ine
Ma
na
ge
rs
He
ad
of
Se
rvic
e
Dir
ecto
rs L
ine
Ma
na
ge
rs a
nd
HR
Ma
na
ge
rs
Ch
ief
Exe
cu
tive
an
d D
ire
cto
r o
f HR
Exe
cu
tive
Dir
ecto
rs w
ith
ad
vic
e
fro
m H
R
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 296 of 300

ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
14
of
11
7
Exte
nsio
n o
f sic
k l
ea
ve
on
fu
ll p
ay (
Dir
ecto
r o
f P
eo
ple
an
d S
tra
teg
y o
r C
hie
f
Exe
cu
tive
) S
tud
y L
eav
e
stu
dy le
ave
ou
tsid
e t
he
UK
me
dic
al sta
ff s
tud
y le
ave
(U
K)
all
oth
er
stu
dy le
ave
(U
K)
Re
mo
va
l E
xp
en
se
s, e
xce
ss
re
nt
an
d h
ou
se
pu
rch
ase
s
Au
tho
risa
tio
n o
f p
aym
en
t o
f re
mo
va
l e
xp
en
se
s in
cu
rre
d b
y o
ffic
ers
ta
kin
g u
p
ne
w a
pp
oin
tme
nts
(p
rovid
ing
co
nsid
era
tio
n w
as p
rom
ise
d a
t in
terv
iew
)
Up
to
£ 5
,00
0
Ab
ove
£5
,00
0
Gri
ev
an
ce
Pro
ced
ure
All g
rie
va
nce
s c
ase
s m
ust
be
de
alt w
ith
str
ictly in
acco
rda
nce
with
th
e G
rie
va
nce
P
roce
du
re a
nd
th
e a
dvic
e o
f a
Hu
ma
n R
eso
urc
es O
ffic
er
mu
st
be
so
ug
ht
wh
en
the
gri
eva
nce
re
ach
es t
he
le
ve
l o
f G
en
era
l M
an
ag
er.
Au
tho
rise
d C
ar
& M
ob
ile P
ho
ne
Use
rs R
eq
ue
sts
fo
r n
ew
po
sts
to
be
au
tho
rise
d
as c
ar
use
rs
Re
qu
ests
fo
r n
ew
po
sts
to
be
au
tho
rise
d a
s m
ob
ile t
ele
ph
on
e u
se
rs
Re
ne
wa
l o
f F
ixe
d T
erm
Co
ntr
act
Re
du
nd
an
cy –
Dis
mis
sin
g O
ffic
ers
Ill H
ea
lth
Re
tire
me
nt
De
cis
ion
to
pu
rsu
e r
etire
me
nt
on
th
e g
rou
nd
s o
f ill-
he
alth
Dis
mis
sa
l
Ch
ief
Exe
cu
tive
Me
dic
al
Dir
ecto
r/D
ep
uty
CO
Os
Ch
ief
Exe
cu
tive
B
ud
ge
t H
old
ers
Dir
ecto
r o
f H
R a
nd
OD
Exe
cu
tive
Dir
ecto
rs
Exe
cu
tive
Dir
ecto
rs
Ch
ief
Exe
cu
tive
or
Exe
cu
tive
D
ire
cto
rs o
r N
om
ina
ted
De
pu
ty
De
sig
na
ted
Exe
cu
tive
Dir
ecto
r
actin
g o
n b
eh
alf o
f th
e T
rust
Bo
ard
(as d
efin
ed
in
th
e R
ed
un
da
ncy
Po
licy)
Dis
mis
sin
g O
ffic
ers
D
ism
issin
g O
ffic
ers
Page 297 of 300
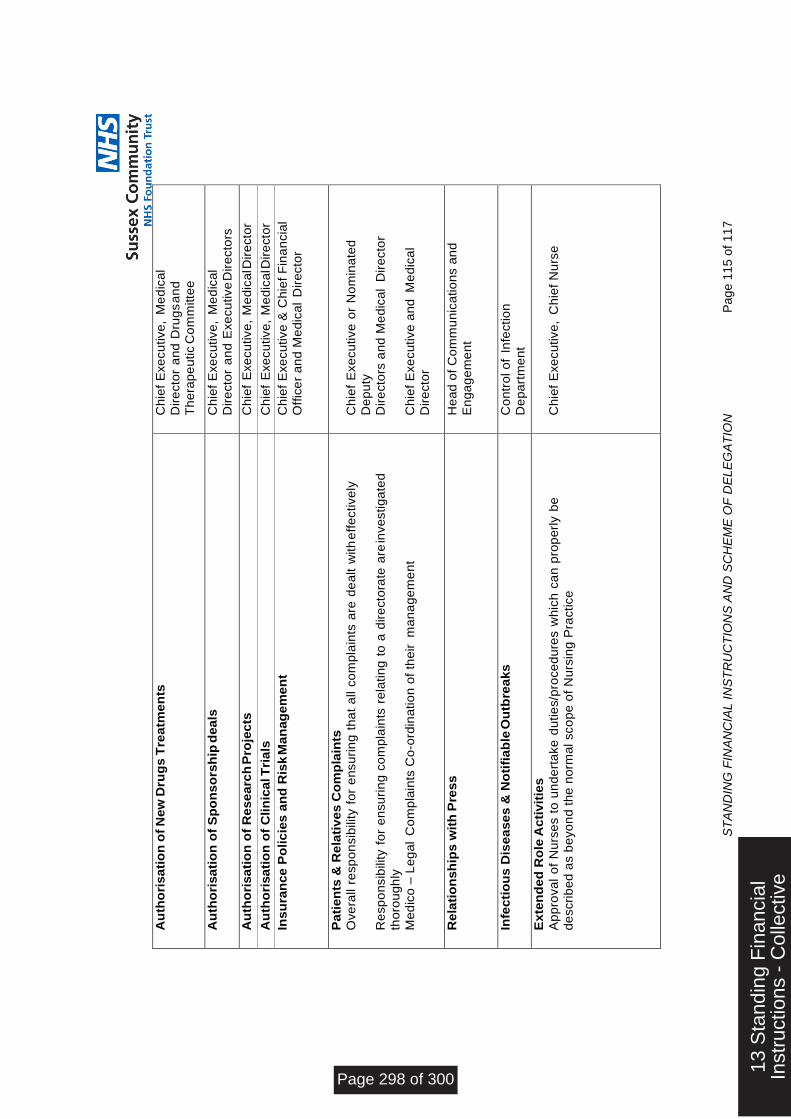
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
15
of
11
7
Au
tho
risa
tio
n o
f N
ew
Dru
gs
Tre
atm
en
ts
Ch
ief
Exe
cu
tive
, M
ed
ica
l
Dir
ecto
r a
nd
Dru
gs a
nd
T
he
rap
eu
tic C
om
mitte
e
Au
tho
risa
tio
n o
f S
po
ns
ors
hip
dea
ls
Ch
ief
Exe
cu
tive
, M
ed
ica
l
Dir
ecto
r a
nd
Exe
cu
tive
Dir
ecto
rs
Au
tho
risa
tio
n o
f R
ese
arc
h P
roje
cts
C
hie
f E
xe
cu
tive
, M
ed
ica
l Dir
ecto
r
Au
tho
risa
tio
n o
f C
lin
ica
l T
ria
ls
Ch
ief
Exe
cu
tive
, M
ed
ica
l Dir
ecto
r
Ins
ura
nce
Po
lic
ies
an
d R
isk
Ma
nag
em
en
t C
hie
f E
xe
cu
tive
& C
hie
f F
ina
ncia
l
Off
ice
r a
nd
Me
dic
al
Dir
ecto
r
Pa
tie
nts
& R
ela
tiv
es
Co
mp
lain
ts
Ove
rall
resp
on
sib
ility
fo
r e
nsu
rin
g t
ha
t a
ll c
om
pla
ints
are
de
alt w
ith
eff
ective
ly
Re
sp
on
sib
ility f
or
en
su
rin
g c
om
pla
ints
re
latin
g t
o a
dir
ecto
rate
are
inve
stig
ate
d
tho
rou
gh
ly
Me
dic
o –
Le
ga
l C
om
pla
ints
Co
-ord
ina
tio
n o
f th
eir
m
an
ag
em
en
t
Ch
ief
Exe
cu
tive
or
No
min
ate
d
De
pu
ty
Dir
ecto
rs a
nd
Me
dic
al
Dir
ecto
r
Ch
ief
Exe
cu
tive
an
d M
ed
ica
l
Dir
ecto
r
Re
lati
on
sh
ips
wit
h P
ress
H
ea
d o
f C
om
mu
nic
atio
ns a
nd
En
ga
ge
me
nt
Infe
cti
ou
s D
ise
ase
s &
No
tifi
ab
le O
utb
rea
ks
C
on
tro
l o
f In
fectio
n
De
pa
rtm
en
t
Ex
ten
de
d R
ole
Ac
tiv
itie
s
Ap
pro
va
l o
f N
urs
es t
o u
nd
ert
ake
du
tie
s/p
roce
du
res w
hic
h c
an
pro
pe
rly b
e
de
scri
be
d a
s b
eyo
nd
th
e n
orm
al sco
pe
of
Nu
rsin
g P
ractice
Ch
ief
Exe
cu
tive
, C
hie
f N
urs
e
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 298 of 300
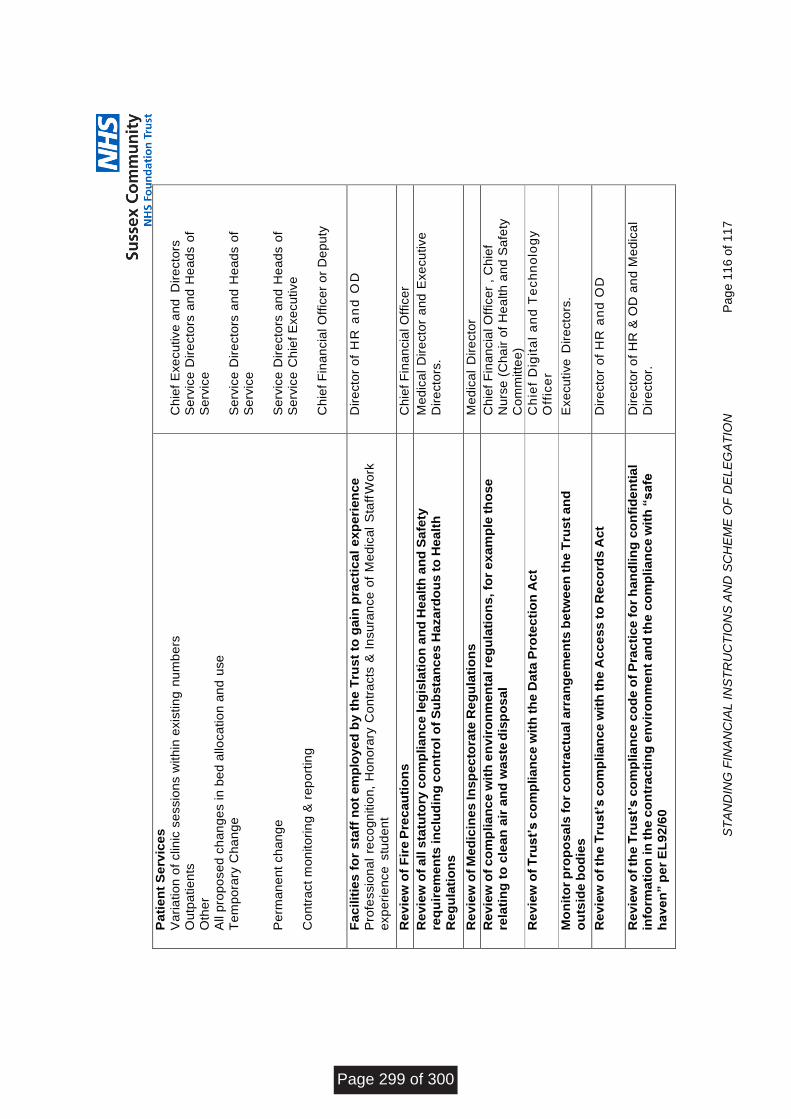
ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
16
of
11
7
Pa
tie
nt
Se
rvic
es
Va
ria
tio
n o
f clin
ic s
essio
ns w
ith
in e
xis
tin
g n
um
be
rs
Ou
tpa
tie
nts
Oth
er
All p
rop
ose
d c
ha
ng
es in
be
d a
lloca
tio
n a
nd
use
Te
mp
ora
ry C
ha
ng
e
Pe
rma
ne
nt
ch
an
ge
Co
ntr
act
mo
nito
rin
g &
re
po
rtin
g
Ch
ief
Exe
cu
tive
an
d D
ire
cto
rs
Se
rvic
e D
ire
cto
rs a
nd
He
ad
s o
f
Se
rvic
e
Se
rvic
e D
ire
cto
rs a
nd
He
ad
s o
f
Se
rvic
e
Se
rvic
e D
ire
cto
rs a
nd
He
ad
s o
f
Se
rvic
e C
hie
f E
xe
cu
tive
Ch
ief
Fin
an
cia
l O
ffic
er
or
De
pu
ty
Fa
cilit
ies
fo
r s
taff
no
t em
plo
yed
by
th
e T
rus
t to
ga
in p
rac
tic
al
exp
eri
en
ce
Pro
fessio
na
l re
co
gn
itio
n,
Ho
no
rary
Co
ntr
acts
& I
nsu
ran
ce
of
Me
dic
al
Sta
ff W
ork
exp
eri
en
ce
stu
de
nt
Dir
ecto
r o
f H
R a
nd
OD
Re
vie
w o
f F
ire
Pre
cau
tio
ns
Ch
ief
Fin
an
cia
l O
ffic
er
R
ev
iew
of
all s
tatu
tory
co
mp
lian
ce
leg
isla
tio
n a
nd
He
alt
h a
nd
Sa
fety
req
uir
em
en
ts in
clu
din
g c
on
tro
l o
f S
ub
sta
nc
es
Ha
za
rdo
us
to
He
alt
h
Re
gu
lati
on
s
Me
dic
al
Dir
ecto
r a
nd
Exe
cu
tive
Dir
ecto
rs.
Re
vie
w o
f M
ed
icin
es
In
sp
ec
tora
te R
eg
ula
tio
ns
Me
dic
al
Dir
ecto
r
R
ev
iew
of
co
mp
lia
nce
wit
h e
nv
iro
nm
en
tal re
gu
lati
on
s, fo
r e
xa
mp
le th
ose
rela
tin
g t
o c
lean
air
an
d w
as
te d
isp
os
al
Ch
ief
Fin
an
cia
l O
ffic
er
, C
hie
f
Nu
rse
(C
ha
ir o
f H
ea
lth
an
d S
afe
ty
Co
mm
itte
e)
Re
vie
w o
f T
rus
t’s
co
mp
lia
nc
e w
ith
th
e D
ata
Pro
tec
tio
n A
ct
Ch
ief
Dig
ita
l a
nd
Te
ch
no
log
y
Off
ice
r
Mo
nit
or
pro
po
sa
ls f
or
co
ntr
ac
tua
l a
rra
ng
em
en
ts b
etw
een
th
e T
rus
t a
nd
ou
tsid
e b
od
ies
Exe
cu
tive
Dir
ecto
rs.
Re
vie
w o
f th
e T
rus
t’s
co
mp
lia
nce
wit
h t
he
Ac
ce
ss
to
Re
co
rds
Ac
t D
ire
cto
r o
f H
R a
nd
OD
Re
vie
w o
f th
e T
rus
t’s
co
mp
lia
nce
co
de
of
Pra
cti
ce
fo
r h
an
dlin
g c
on
fid
en
tia
l
info
rma
tio
n in
th
e c
on
trac
tin
g e
nv
iro
nm
en
t an
d t
he
co
mp
lia
nce
wit
h “
sa
fe
ha
ve
n” p
er
EL
92
/60
Dir
ecto
r o
f H
R &
OD
an
d M
ed
ica
l
Dir
ecto
r.
Page 299 of 300

ST
AN
DIN
G F
INA
NC
IAL I
NS
TR
UC
TIO
NS
AN
D S
CH
EM
E O
F D
EL
EG
AT
ION
P
ag
e 1
17
of
11
7
Th
e k
eep
ing
of
a D
ec
lara
tio
n o
f In
tere
sts
Re
gis
ter
Co
mp
an
y S
ecre
tary
Att
es
tati
on
of
Sea
lin
gs
in
acc
ord
an
ce
wit
h S
tan
din
g O
rde
rs
Ch
air
/Ch
ief
Exe
cu
tive
.
Th
e k
eep
ing
of
a r
eg
iste
r o
f S
ea
lin
gs
Co
mp
an
y S
ecre
tary
Th
e k
eep
ing
of
the
Ho
sp
ita
lity
Re
gis
ter
Co
mp
an
y S
ecre
tary
Re
ten
tio
n o
f R
ec
ord
s
Ch
ief
Exe
cu
tive
.
Clin
ica
l A
ud
it
Me
dic
al D
ire
cto
r, C
hie
f N
urs
e,
Se
rvic
e D
ire
cto
rs &
Qu
alit
y
Co
mm
itte
e.
13 S
tand
ing
Fin
anci
alIn
stru
ctio
ns -
Col
lect
ive
Page 300 of 300






























