Embed Size (px)
Citation preview
/

t t m~ l1RCf en) ~ ~ lJ}ffi tfitffi i 3tR" ~cf; ~ if <U ~ (1ICfld31 c@ meAT "CflT 3llmr mil ~ om 3p:J Cf'iH air ~ ~ '\it'l"fu ~ ~fClqlHlI3U en) ~ crnr ~ ~ en) ~ ~ ~~il"
'Education is a liberating force, and inour age it is also & democratising force,
"cutting across the barriers of caste andclass, smoothing out inequalities imposedby birth and other circumstances"
- Indira Gandhi
/

1
•l®J ~9~2EU,~ UNIVERSITY
Indira GandhiNational Open UniversitySchool of Health Sciences
BNSL - 034Clinical Nursing Practice in
Critical Care - IT
", #\-.0 Block..
1NURSING INTERVENTION MODALITIESPRACTICAL 1
Nursing Care Plan 5
PRACTICAL 2
• Nursing Case Study I Case Presentation 21~,i PRACTICAL 3
Observation Checklist 53
PRACTICAL 4
Conducting Clinical Teaching 59
PRACTICAL 5
Preparing a Clinical Rotation Plan 69Il
PRACTICAL 6
Patient Care Documentation, Records and Reports 78
PRACTICAL 7
"-Design of a Critical Care Unit 95
: \ PRACTICAL 8
Preparing a Research Proposal and a Term Paper 107
»:./
//
..
Ms. Doli BiswasMission of Mercy Hospital andResearch Centre, 125/1 ParkStreetKolkatta- 700017
Fadty Member, SOHS
EXPERT COMMITTEE
"
Prof. Usha MalikPrincipalLakshmi Bai Batra College ofNursingBatra Hospital and ResearchCenter Tughlakabad, New Delhi
Ms. Sujana ChakrabortyPrincipalCollege of NursingJamia Hamdard University.Hamdard NagarNew Delhi
Ms. Sneh Lata WamanNumbalkarSuperintendent of NursingServicesDirectorate of Health Education& ResearchDental College BuildingMumbai - 400001
Prof. Prasanna KumariPrincipalGovt. College of NursingThiruvananthapuram, Kerala
Prof. Panamma RanadavPrincipalS!. Stephens College of NursingDelhi
Ms. Srinanda GoshPrincipalCollege of NursingWoodland Medical Center Ltd.Kolkata
Ms. Mala GosamiPrincipalState College of Nursing107, Chander NagarDehradun, Utrakhand - 001
Dr. (Mrs.) Kiran BatraPrincipalSilver Oak College of NursingVillage Post OfficeKhizrabad District MohaliAdhipur, Punjab
Prof. Sherly DavidProfessorCollege of NursingCMC Veilore
Ms. Selliama KuruvilaAssociate ProfessorGovt. College of NursingKottyam, Kerala-8
Prof. Bimla KapoorDirector, SOHSIGNOU. New Delhi
Prof. Pity KoulProgramme CoordinatorSOHS,IGNOUNew Delhi
Ms. Neerja SoodLecturerSOl-IS,IGNOUNew Delhi
Ms. Reeta DeviLecturerSOHS,IGNOUNew Delhi
Ms. LaxmiLecturerSOHS,IGNOUNew Delhi
Writers
BLOCK PREPARATION TEAMEditors
Unit 1 - 8Ms. Madhavi VermaFaculty Rufaida College ofNursingJamia HamdardNew Delhi
Ms. Meena AgarwalLecturerFaculty, College of NursingAIIMS, New Delhi
CO-ORDINATION
Block Transformation
Prof. (Dr.) Pity KoulProfessor & ProgrammeCoordinatorSOHS,IGNOUNew Delhi
Director
Prof. T.K. JainaSOHS, IGNOU, New Delhi(From 6'h August 2011)Prof. (Dr.) Bimla KapoorSOHS,IGNOUNew Delhi
Course Coor dlnatur
Prof. (Dr.) Pity KoulProfessor & ProgrammeCoordinatorSOHS,IGNOUNew Delhi
Programme Coordinator
Prof. (Dr.) Pity KoulProfessor & ProgrammeCoordinatorSOHS, IGNOUNew Delhi
PRODUCTIONMr. T.R. ManojAssistant Registrar (P)SOHS, IGNOU, New Delhi
August, 2011© Indira Gandhi National Open University, 2011ISBN: 978-81-266-5585-4All rights reserved. No part of this work may be reproduced in any form, by mimeograpb or any othermeans, without permission in writing from the Tndira Gandhi National Open University.Further information about the School of Health Sciences and the Indira Gandhi National Open Universitycourses may be obtained from the University's office at Maidan Garhi, New Delhi-Ll O 068.Printed and published on behalf of the Indira Gandhi National Open University, New Delhi byDirector, School of Health Sciences.Laser Typeset by : Graphic Printers, 204, Pankaj Tower, Mayur Vihar, Phase-I, Delhi-91.Printed at : Akashdeep Printers, 20-Ansari Road: Darya Ganj, New Delhi-ll0002
/

I
COURSE INTRODUCTION
"
In order to provide needbased and efficient care to the critically ill patients youneed to plan the care based on nursing process. You also need to learn howto develop and use various tools of assessment, make case presentation,prepare lesson plans and rotation plans, In the process of providing care youmay come across such problems which will require evidence based interventionsand evaluations.
.tThis Practical manual will guide you and help you in planning nursing care forcritically ill patients with various disease conditions, assess the problems,implement the care evaluate the care and document the care using appropriateformats. You will also get an understanding of scientific approach in studying
.problems encountered during care and addressing these problems, writing thereport, term paper and developing a project proposal.
For practical 1 to 8 you will be placed in various critical care units for acquiringrequired skills in forming tills skills you may have to under take many activities.These activities are listed at the end of each practical and on the inner page ofback cover of the practical manual. The activities related to research proposalwill help you to develop skills in writing a research proposal conducting thesmall research project and writing a research report or term paper. The clinicalsupervisors and Academic Counsellors will help you in performing all theactivities.
..
The practical manual/course comprises following 3 blocks:
Block 1 Nursing Intervention Modalities
Block 2 Introduction to Computer Basics
Block 3 Application of Computers in Nursing

BLOCK INTRODUCtION
"
In order to provide quality care to the criticall~ ill patients, you need to developknowledge and skills in preparing and using nursing care plan based on nursingprocess and document the care. You-also need to learn various clinical teachingmethods using the lesson plan, prepare the clinical rotation plan and solve theproblems of the patients by using scientific methods. This practical manual willhelp you to gain competency in nursing care planning, clinical teaching, learning,preparing and implementing research projects.
This practical manual book deals with the preparation of nursing care plans,use of nursing process in critical care units, the preparation of nursing carestudy, observation check list, clinical teaching proforma, documentation of patientsrecords, reports; design of critical care unit, development of research proposals/projects, presentation of term paper and critiquing of research studies. Thepractical manual comprises of following eight practicals.
Practical 1 deals with Nursing Care Plan
Practical 2 describes Nursing case study / case presentation
..,rt
Practical 3 deals with Observation Checklist
Practical 4 focuses on Clinical teaching methods
Practical 5 explains preparing a clinical rotation plan
Practical 6 relates to Patient care documentation, records and reports
Practical 7 relates to design of a Critical care unit
Practical 8 deals with preparing a Research proposal and a term paper
i/1
I
,f
PRACTICAL! NURSING CAREPLAN
Structure
"
1.0 Introduction
1.1 Objectives
1.2 Nursing Care Plan and its Importance
1.3 Steps in Developing a Nursing Care Plan
1.4 Format of a Nursing Care Plan Based on Nursing Process
l.5 Let Us Sum Up
1.6 Answers to Check Your Progress
1.7 Activities
1.0 INTRODUCTIONWhile providing nursing care to the patients till now, you must have realized thatthe needs of a patient differ at various phases of illness. You might have alsonoted differences in patients' clinical picture and problems even though they havesame diagnosis.
In order to provide the high standard nursing care it is important that the care isplanned, individualized and reviewed over the period of time so that the nurse andpatient develop professional relationship. The planning should involve the patientthroughout all the phases of nursing process to make individualized plan of care.In this practical, you willleam about preparing and implementing nursing care planbased on nursing process and documentation skills.
1.1 OBJECTIVESAfter completing this practical, you will be able to:
• discuss the need for planning nursing care;
• obtain assessment data from client / patient;
• formulate appropriate nursing diagnoses based on the assessment data;
• formulate appropriate expected outcomes for a patient;
• prepare a nursing care plan using nursing process phases; and
• implement, evaluate and document the planned nursing care.
1.2 NURSING CARE PLAN AND ITS IMPORTANCEA nursing care plan is a plan based on data gathered during patient assessmentthat identifies the patient's care needs, tests the strategy for providing services tomeet those needs, documents treatment goals or objectives, outlines the criteria 5
I

Nursing InterventionModalities
for terminating specified interventions, and documents the individual's progress inmeeting specified goals and objectives.
"
The format of the "plan" in some organizations may be guided by patientspecific policies and procedures, protocols, practice guidelines, clinicalpaths, care maps or a combination of these. The plan of care may includecare, treatment and rehabilitation. Format of nursing care plan is given inSection 1.4.
Importance
• Patient has right to expect that nursing care received will be complete andof high quality. If planning is not done properly, then gaps will exist in thenursing care given and care give will be incomplete, inconsistent, and certainlynot of high quality. '
...tt
Care planning and its documentation provides a means of professionalcommunication. This communication promotes consistency of care for patientand provides a comfort level for the nurse. It also provides a guideline fordocumentation and promotes practicing within legally defined standards.
• Care planning provides legal protection for the nurse. In a legal suit, thenursing care is measured against the idea of what a reasonably prudent nursewould do in some circumstances. The accepted standards of nursing practiceare the accepted definitions of reasonable, prudent nursing care.
•
• The accreditation status of a health care agency depends upon consistentdocumentation of plan of care has been done. All the accrediting and approvalagencies/hospitals have criteria that specifically require documentation ofplanned' care.
• Review of revised nursing standards indicate that the standards require moredetailed care planning and documentation in patient's medical record.
1.3 STEPS IN DEVELOPING A NURSING CAREPLAN
Following steps should be followed while developing a nursing care plan:
• Develop Nursing care plan based on nursing process which includes followingsteps (Fig 1.1).
Assessment
Nursing diagnosis
Planning
Implementation
Evaluation
Assessment
6
• Systematically collect, verify analyze and communicate data about a: patient.
• Collect the data from various sources i.e., Patient, family members including
/

..
, ,
,t.J
'.
friends, Laboratory reports Patient's file, Health team members.
The data can be subjective or objective
Objective data includes factual, measurable and observable informationthat you can see, hear or feel e.g., Pulse, Temperature, Blood pressure,Cyanosis etc.
Subjective data consists of the information expressed by the patient e.g.,Pain, Anorexia, Itching, Nausea, Dizziness etc.
Nu~sing Care Plan
.Implementation'1. Nurse - initiated
treatmentsPhysician-initiatedtreatment
Assessment1. .Subjective
dataObjectivedata
Diagnosis1. Data analysis2. Problem
identificationLabel
F'ig. 1.1: Nursing Process
Formulate Nursing diagnosis
It is the statement of a potential or an altered status of a client, which is derivedfrom nursing assessment and requires interventions from the domain of nursing.
The difference between medical and nursing diagnosis is given in table 1.1.
Table 1.1: Difference between medical and nursing diagnosis
Medical diagnosis Nursing diagnosisDescribes a ' ! Describes an individual response to aspecific disease process disease process or conditioniJriented ~pathophysio}~ Oriented to individualHas well developed No universally accepted classificationclassification system accepted systemby medical professionals -Diagnosis consists of two or Consists of two or three part statementthree words with etiology well known.-
• State the nursing diagnosis based on the assessment : The statementof nursing diagnosis includes, Problem, Etiology, Sign and symptoms.
7
/
, Nursing Intervention: Modalities
"
. .
8
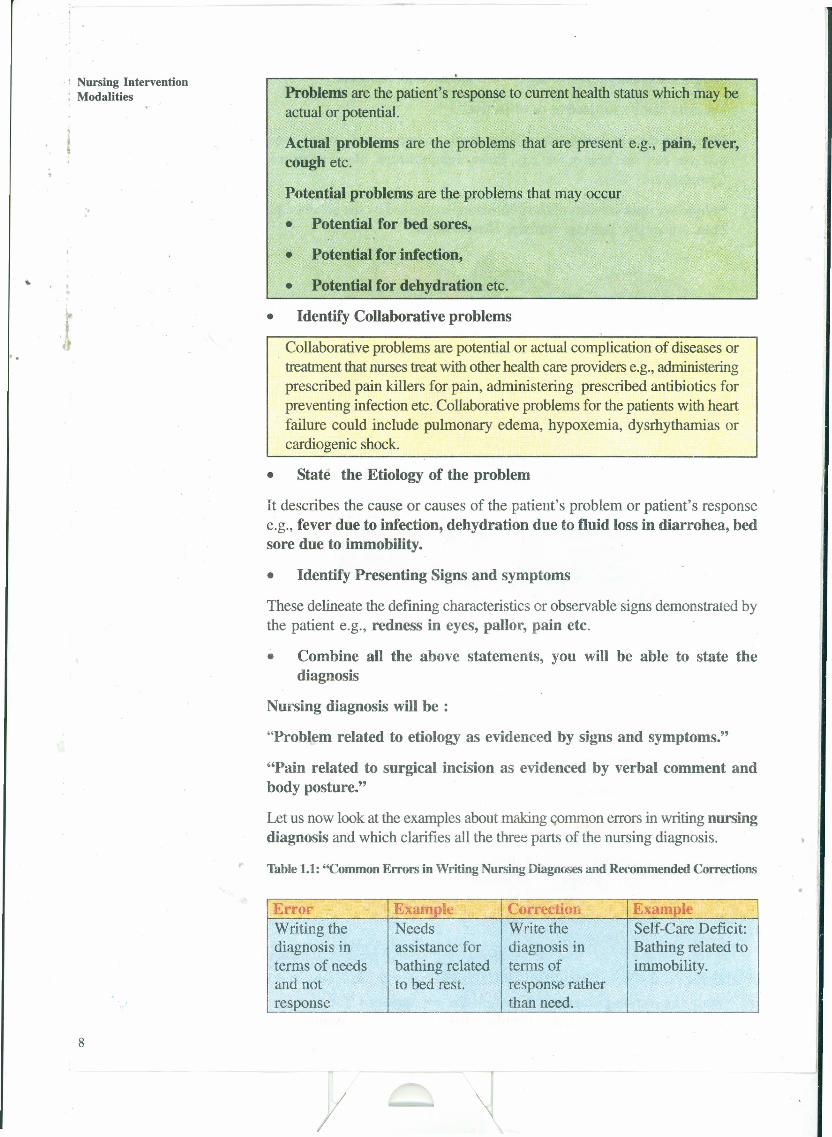
Problems are the patient's response to current health status which may beactual or potential.
Actual problems are the problems that are present e.g., pain, fever,cough etc.
Potential problems are the problems that may occur
• Potential for bed sores,
.• Potential for infection,
• Potential for dehydration etc .
• Identify Collaborative problems
Collaborative problems are potential or actual complication of diseases ortreatment that nurses treat with other health care providers e.g., administeringprescribed pain killers for pain, administering prescribed antibiotics forpreventing infection etc. Collaborative problems for the patients with heartfailure could include pulmonary edema, hypoxemia, dysrhythamias orcardiogenic shock.
• State the Etiology of the problem
It describes the cause or causes of the patient's problem or patient's responsee.g., fever due to infection, dehydration due to fluid loss in diarrohea, bedsore due to immobility.
• Identify Presenting Signs and symptoms
These delineate the defining characteristics or observable signs demonstrated bythe patient e.g., redness in eyes, pallor, pain etc.
• Combine all the above statements, you will be able to state thediagnosis
Nursing diagnosis will be :
"Problem related to etiology as evidenced by signs and symptoms."
"Pain related to surgical incision as evidenced by verbal comment andbody posture."
Let us now look at the examples about making common errors in writing nursingdiagnosis and which clarifies all the three parts of the nursing diagnosis.
Table 1.1: "Common Errors in Writing Nursing Diagnoses and Recommended Corrections
r-r-t-'
Error Example Correction Example --Writing the Needs Write the Self-Care Deficit:diagnosis in assistance for diagnosis in Bathing related toterms of needs bathing related terms of immobility.and not to bed rest. response rather
2:esponse than need.
I

. ;
..
Identifying a Mild anxiety Include in the' No need forpatient's related to problem nursing diagnosis:response that is impending statement of the mild anxietynot necessarily surgery. nursing before surgery isunhealthy. diagnosis only a healthy
patient responses response thatthat are motivates.unhealthy or that preoperative self-the patient wants care behaviour.to change.
Identifying Cough related Avoid including Ineffectivesigns and to long history signs and Airway Clearancesymptoms of of smoking symptoms of related to 20-yearillness as a illness in the history ofproblem problem smoking. ~
statement of thenursingdiagnosis.
Identifying as a Alterations in Express the Self-Care Deficit:patient problem Bowel problem Care ofof etiology what Elimination: statement and Colostomy,cannot be Permanent etiological related to severechanged Colostomy factors in terms anxiety about
related to that can be cancer andcancer of changed; feelings ofbowel. otherwise, powerlessness.. .nursmg energies
are beingdirected to ahopeless task.
Nursing Care Plan
Planning the nursing care
• Prepare Plan for the nursing care
Identifying and specifying the nursing diagnoses leads to the planning phase.
Planning includes following:
Prioritizing the nursing diagnoses
Assigning priorities based on life threatening situations posed by a problem.For example, ineffective airway clearance would pose more of a threatto life than impaired skin integrity
Identifying the goals and expected outcomes (long term and short termgoals)
• State expected outcomes
Expected outcomes are clearly stated in tenus of patient's behaviour orobservable assessment factors. These have to be realistic; achievable, safeand acceptable to the patient. and are written in specific concrete termsdepicting patient's action. These are patient centered and not nurse centered.Establish target dates at the end of the expected outcome. These target datesmay be different for differe,nt patients depending upon their condition. 9
I 1
Nursing InterventionModalities
"
10
.Some of the examples of expected outcomes are:
For a patient on second post-operative day, expected outcome can be:
• Patient will increase oral intake to 1500 ml per 24 hours by 12/02110
For a hypertensive patient getting discharged, expected outcome canbe:
• Patient can, accurately measures own blood pressure by 01/01 /l O.
Once expected outcomes have been written, you are then ready to focus on thenext phase-implementation.
> Implementation Phase
• Implement the nursing care plan which is based on following:
Desired patient outcome
Etiology of nursing diagnosis
Clinical practice guidelines
Scientific principles frame behavioural and biological sciences
Feasibility of successfully implementing the intervention
Acceptance by the patient
Nurses capabilities.
• List the nursing actions to be performed
Nursing actions may include both independent and collaborative activities.
Independent actions are those activities which a nurse performs using his orher own discretionary judgment, e.g., deciding which non-invasive techniqueto be used for pain control.
Collaborative actions are those activities that involve mutual decision makingbetween two or more health care practitioners e.g., Referral to a dieticianor a psychologist or physiotherapist etc.
• Include following five component" while writing Nursing Action
Date: On which the action is written.
,. Action Verb: Specific action that the nurse IS going to do. e.g., Applyspiral bandage.
Content area: Where and what kind of action, e.g., Apply spiralbandage after cleaning the wound with betadine on the left leg.
Time element: How long or how often the nursing action to occur,e.g., Apply spiral bandage after cleaning the wound with betadine onthe left leg every day.
Signature: The nurse who writes the initial action order puts the signature(i.e., Accepting legal and ethical accountability).
/

Properly written nursing actions require you as a nurse to perform the nursingaction and document it appropriately. Further you need to have guidelines ofwhat to do and chart if an untoward reaction occurs at any level of implemen-tation of the action. In the above stated nursing action while cleaning thewound nurse may identify that there is pus draining from the wound or patientis experiencing allergic reaction to betadine.
" > Documentation
• Document nursing action or' nursing care given
Nursing actions are used as the base for documentation
Use flow sheets to highlight significant findings.
Flow sheets are abbreviated progress notes that enable the nurses to recordnursing data quickly and concisely and also provides an easy to read recordof patient's condition over time.
Progress notes made by nurses provide information about the progress aclient is making toward achieving desired outcomes. It also includes informationabout patient's problems and nursing interventions. The format used dependson the documentation system in use in the Institution. Progress notes are con-sidered as evaluation notes. In the example of applying spiral bandageafter cleaning the wound with betadine on the left leg, Progress notescan be made as follows: (Table 1.2)
Table 1.2: Sample Progress notes
Date and time Nursing Evaluation I SignatureActivity Findings
1st Day Wound cleaned • Dischargewith betadine from wound:and spiral Yes/ No I
bandage applied • Colour ofdischarge:PuslBloodStained
• Amount ofdischarge:Dry/ oozing/Minimal!
• SurroundingTissues:Redness/sweeling/painltenderness
2nd day
> Evaluation Phases
• Evaluate the care after providing and documenting the care
/
Nursing Care Plan
11
Nursing InterventionModalities
",
I~I
12
In the evaluation phase' of nursing process, the nurse
• determines if the patient outcomes have been met or not, the process isreviewed from the beginning.
• evaluates whether the sufficient assessment data were obtained to supportidentified nursing diagnosis e.g., was the pain actually related to the woundor because of pressure from light bandaging.
• checks if tpe expected outcomes were realistic, measurable and achievable,If not revision of patient outcome and intervention is necessary
• modify or maintain the plan as a result of evaluation
Document all the activities .•It is used to judge each component of the nursing process it reflects whetherthe patient's problems are resolved or not. This can be done by measuringwhether expected outcomes have been achieved or not. This may lead tofurther evaluation of the process. The cycle is continuous and therefore theprocess is dynamic.
Documentation being the most important of evaluation phase also providesevidence that nursing practice standards of nursing process and its phases havebeen maintained during care of the patient. Assessment, nursing diagnosis,intervention outcomes and evaluation of the patients response to care are criticalparts of the patient's record.
Check Your Progress 1
1) Write the following nursing diagnoses correctly:
a) Impaired skin integrity related to presence of bed sores.
b) Inability to take bath related to that patient looks dirty.
c) Needs counselling related to anxiety.
r .
1.4 FORMAT OF A NURSING CARE PLAN BASEDON NURSING PROCESS
Nursing care plan shown here is developed on the steps or phases of nursingprocess which includes assessment of data identification of nursing diagnosis andselected patient outcomes and nursing intervention, all of which are recorded ina nursing care pian.
I

FORMAT FOR NURSING CAM PLAN Nursing Care Plan
i) Identification data
Name
Age
Sex
" Religion
Marital Status
EducationalBackground
~ Occupation
Date ofAdmission
M.R.D. No.
Diagnosis
Ward
Bed No.
Address
Date ofDischarge
Date of Planning:of care
. ...........................................................
ii) Socio-Economic History:
a) Type of family-Nuclear/Joint
b) Numbers of family members
c) Total family income
d) Housing condition - Own/Rental/WaterlElectricitySupply health facilitiesavailable
Hygiene and groomingill) Personal history -
Any HlO Allergy
Life style habits: smoking, alcohol, tobacco, drugs, exercise, etc.
Dietary habits - vegetarian/non vegetarian
iv) Family Health History - any specific disease in the family,
v) History of past illness
vi) History of present illness - Present complaints
vii) Physical examination at the time of Admission13
/

..
.. \ Nursing InterventionModalities
".
. ,
14
viii) Investigations:Date Name of Findings in patients Normal Value
InvestigationI
.
'f
ix) Doctors Orders:S.No . Dr's Prescriptions Purposes
,
x) Nursing Assessment:
a) Subjective Assessment: Collecting and documented health problems asperceived by the patient e.g., pain, anorexia, restlessness, itching,breathlessness,
b) Objective Assessment: vital signs B.P. pulse, respiration,
Head to foot examination.xi) Nursing Care Plan
Evaluation ~I Implementation
I
I
Nursing PlanningDiagnosis
xii) Progress Notes
,.
Evaluation / Signature,
Date and Nursing Activitytime Findings
1st Day Wound cleaned • Discharge fromwith betadine and ' wound: Yes! Nospiral bandage • Colour ofapplied discharge:
PuslBlood- Stained
• Amount ofdischarge: Dryl
I,' oozing/ Minimal!• Surrounding
Tissues: Redness/swelling/pain/ten-derness
2nd day ';;
xiii) Health Teaching
/

1.5 LET US SUM UPNursing Care Plan
. .
Nursing care plan is plan of care prepared to provide quality nursing care to thepatients. Nursing care plan is to be prepared using different steps of nursingprocess which includes assessment, nursing diagnosis.planning, implementationand evaluation. In this unit, you have learnt about the importance of nursing careplan andhow to prepare nursing care plan using the different steps of nursingprocess.
1.6· ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
I. Impaired skin integrity related to physical immobility / edema
2. Self care deficit: bathing related to immobility
3. Anxiety related to seriousness of the disease.
1.7 ACTIVITIESSelect a patient from medical / surgical critical care unit with any disease/condition.
• Collect objective and subjective data related to the health problems of thepatient based on the guidelines given in the practical.
• Formulate and prioritize nursing diagnoses for this patient
• Plan the desired outcomes.
• Prepare a nursing care plan for this patient using the steps of nursing process.
Supervised Activity
• Select a patient from coronary care unit and collect subjective and objectivedata related to health problem of the patient
• Prepare a nursing care plan
15
/I
Nursing InterventionModalities
Identification data
SAMPLE NURSING CARE PLAN BASED ON NURSING PROCESS
Name
Age
Sex"
Religion
Marital Status :... . • Educational
.1Background
Occupation
Date ofAdmission
M.R.D. No.
Diagnosis
Ward
Bed No.
Address
Date ofDischarge
Date ofPlanning
Mrs Roopa .
27 years , .
Female .
Hindu : : .
Married .
No formal education .
Labourer. .
30/07/03 .
579320 .
TB, chest infection; postnatal case of resp failure,emergency LSCS on 30/07/03.
.. .ICU .
. .. 03 .
Village Tappal, DistAligarh,UP .
...............................................................
........................................... ~ .
25/09/03 .
1) Socio-Economic History
a) Type of family-Nuclear/Joint
b) Number of family members
c) Any specific disease infamily members
d) Total family income
e) Housing condition
16
I
Joint family
She stays with her in laws and has 4members in her family.
Not significant
Her husband works as labourerearning about Rs 200/- per day
They stay in their own pucca house.There is adequate ventilation. Thereis no water supply from the localgovernment. Fetch water fromnearby well. Electricity is availablein the night only.
2) Personal history
Dietary habit
3) Family History
4) History of past illness:
.. . ,
J 5) History of presentillness
6) Physical examinationat the time of Admission
Hygiene and . grooming- patientappears dirty.
No known HlO Allergy to any food or drugs.
No HlO smoking, alcohol, tobacco, drinking etc.
They are vegetarian and are able to arrangemeals for the family members
Not significant.
She has a history of productive cough for 2 years.and taken treatment for TB for 9 months in theyear 2002 before the gestation. No historysuggestive of DM or hypertension.
She was brought to casualty of SJH on 30107103 with term pregnancy and in labor. She is aprimipara with short stature. She was taken upfor emergency LSCS under GA on 30107/07.baby girl was born at 8.30 p.m. with a wt of 2.6kg. lntraoperatively, Sp02 dropped to 92-93%which was maintained at 96% by 50% 02 +50% N20. There were large amount of purulentsecretions in ET tube and Lt sided air entry wasreduced markedly. Postoperatively her Sp02could not be maintained on air. Therefore, shewas not extubated and kept on 100% 02 throughmechanical ventilation. She was then shifted toICU. Emergency tracheostomy was performedunder LA on 22/08/03 with 7.5 cuffed portextube. 2 units of blood were transfused on30107/03.
Nursing Care Plan
Patient was conscious and responding to verbalcommands.
Pulse rate: 128/min
RR: 28/min
BP : 130/80 mm Hg
Chest : Left side air entry decreased. Crepts inupper middle zone.
Pallor: +++ clinically Hb = 7 gm%
17
I
Nursing InterventionModalities
",
18
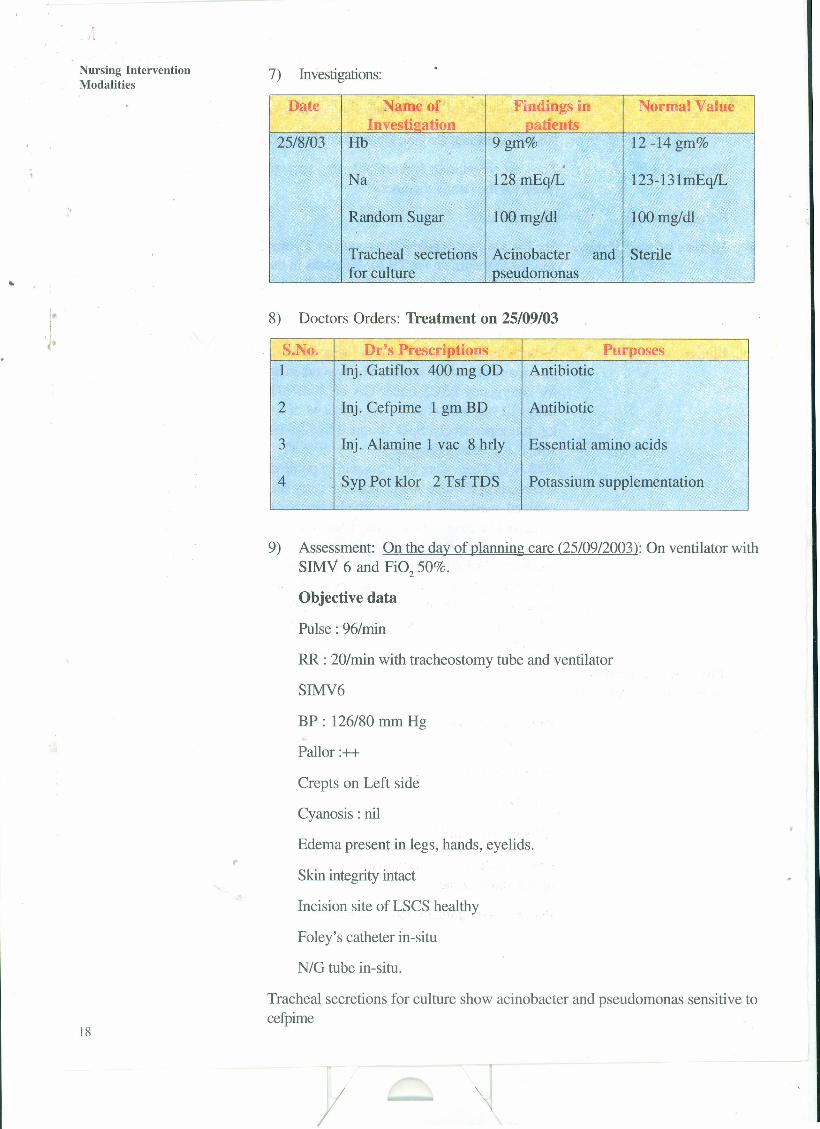
7) Investigations:
Date Name of Findings in Normal ValueInvestiaation ' patients
25/8/03 Hb 9gm% 12 -14 gm%.,
Na 128 mEq/L 123-131mEq/L
Random Sugar 100 mg/dl 100 mg/dl
Tracheal secretions Acinobacter and Sterilefor culture pseudomonas -
8) Doctors Orders: Treatment on 25/09/03
S.No. Dr's Prescriptions Purposes1 Inj. Gatiflox 400 mg OD Antibiotic
2 Inj. Cefpime 1 gm BD , Antibiotic
3 Inj. Alamine 1 vac 8 hrly Essential amino acids
4 Syp Pot klor 2 TsfTDS Potassium supplementation
9) Assessment: On the day of planning care (25/09/2003): On ventilator withSIMV 6 and Fi0250%.
Objective data
Pulse : 96/min
RR : 20/min with tracheostomy tube and ventilator
SIMV6
BP: 126/80 mm Hg
Pallor :++
Crepts on Left side
Cyanosis : nil
Edema present in legs, hands, eyelids.,.Skin integrity intact
Incision site of LSCS healthy
Foley's catheter in-situ
N/G tube in-situ.
Tracheal secretions for culture show acinobacter and pseudomonas sensitive tocefpime
/
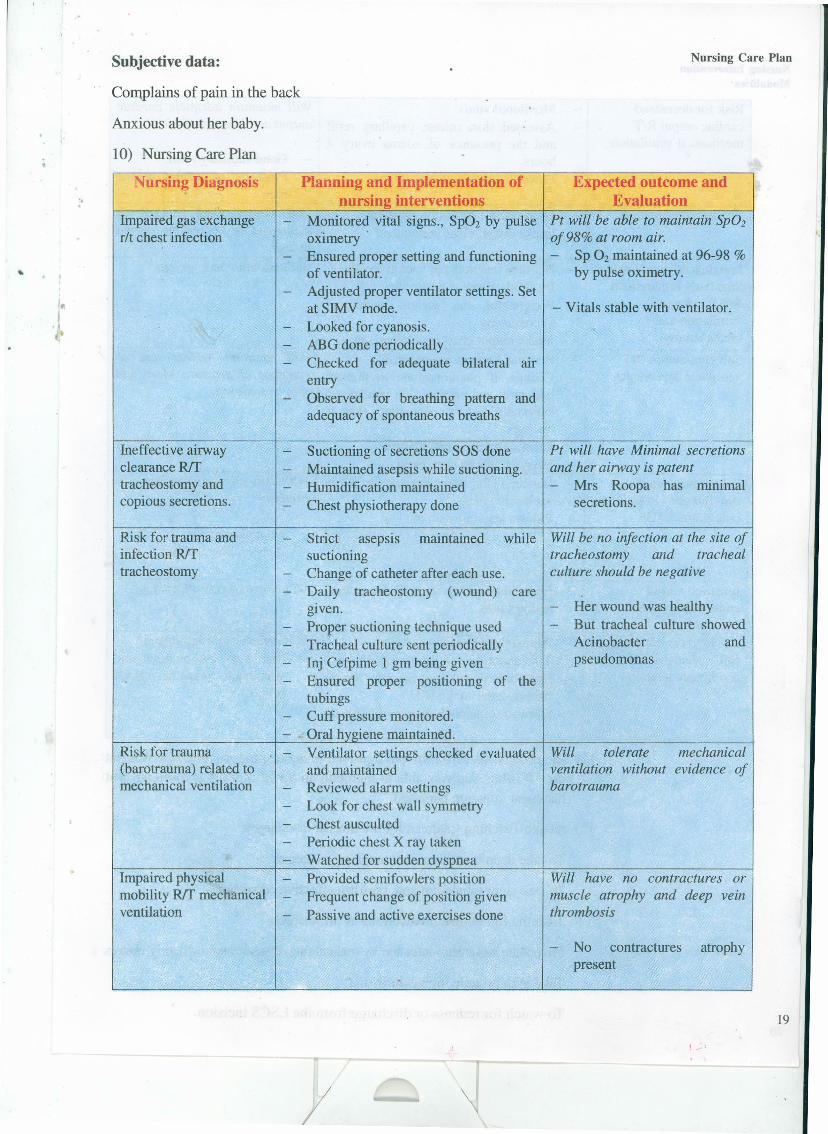
Subjective data:
Complains of pain in the back
Anxious about her baby.
10) Nursing Care Plan
",Nursing Diagnosis Planning and Implementation of
nursing interventions
Nursing Care Plan
Expected outcome andEvaluation
Impaired gas exchange -rlt chest infection
, -
Monitored vital signs., Sp02 by pulseoximetry'Ensured proper setting and functioningof ventilator.Adjusted proper ventilator settings. Setat SIMV mode.Looked for cyanosis.ABG done periodicallyChecked for adequate bilateral airentryObserved for breathing pattern andadequacy of spontaneous breaths
Pt will be able to maintain SpOzof 98% at room air.- Sp O2 maintained at 96-98 %
by pulse oximetry.
- Vitals stable with ventilator.
Ineffective airwayclearance R!Ttracheostomy andcopious secretions.
Suctioning of secretions SOS doneMaintained asepsis while suctioning.Humidification maintainedChest physiotherapy done
Pt will have Minimal secretionsand her airway is patent- Mrs Roopa has minimal
secretions.
Risk for trauma andinfection R!Ttracheostomy
--
Risk for trauma -(barotrauma) related tomechanical ventilation -
----
Impaired physical -mobility R!T mechanical -ventilation -
while Will be no infection at the site oftracheostomy and trachealculture should be negative
Strict asepsis maintainedsuctioningChange of catheter after each use.Daily tracheostomy (wound) caregiven.Proper suctioning technique usedTracheal culture sent periodicallyInj Cefpirne 1 gm being givenEnsured proper positioning of thetubingsCuff pressure monitored.Oral hygiene maintained.Ventilator settings checked evaluatedand maintainedReviewed alarm settingsLook for chest wall symmetryChest auscultedPeriodic chest X ray takenWatched for sudden dyspneaProvided semi fowlers positionFrequent change of position givenPassive and active exercises done
Her wound was healthyBut tracheal culture showedAcinobacter andpseudomonas
Will tolerate mechanicalventilation without evidence ofbarotrauma
Will have no contractures ormuscle atrophy and deep veinthrombosis
No contracturespresent
atrophy
/
19
Nursing InterventionModalities
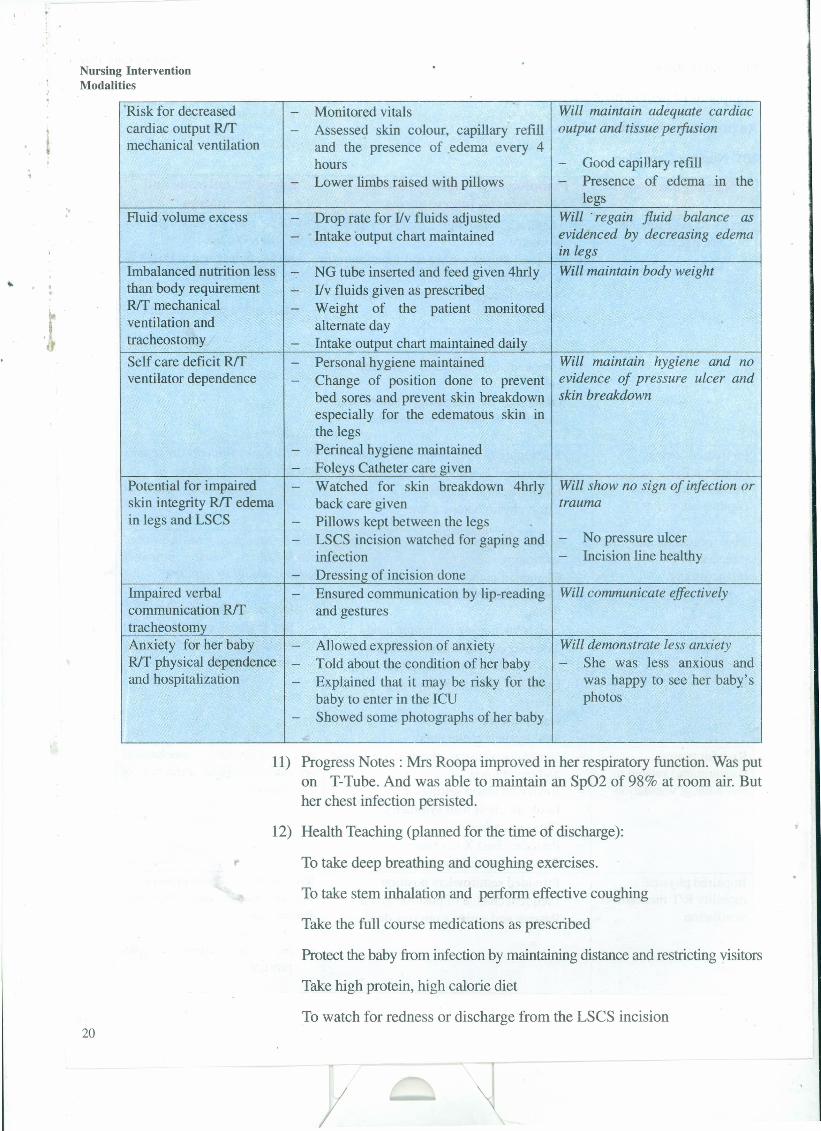
'Risk for decreasedcardiac output Rtfmechanical ventilation
- Monitored vitals- Assessed skin colour, capillary' refill
and the presence of edema every 4hours
- Lower limbs raised with pillows
Will maintain adequate cardiacoutput and tissue perfusion
- Good capillary refill- Presence of edema III the
legs", Fluid volume excess - Drop rate for I/v fluids adjusted
- 'Intake 'output chart maintainedWill 'regain fluid balance asevidenced by decreasing edemain legs
20
- Watched for skin breakdown 4hrly Will show no sign of infection orback care given trauma
- Pillows kept between the legs- LSCS incision watched for gaping and - No pressure ulcer
infection - Incision line healthy- Dressing of incision done
Imbalanced nutrition less - NG tube inserted and feed given 4hrlythan body requirement - I/v fluids given as prescribedR/T mechanical - Weight of the patient monitoredventilation and alternate daytracheostomy - Intake output chart maintained dailySelf care deficit Rtf - Personal hygiene maintainedventilator dependence - Change of position done to prevent
bed sores and prevent skin breakdownespecially for the edematous skin inthe legs
- Perineal hygiene maintained- Foleys Catheter care given
Potential for impairedskin integrity Rtf edemain legs and LSCS
Will maintain body weight
Will maintain hygiene and noevidence of pressure ulcer andskin breakdown
Impaired verbalcommunication Rtftracheostomy
- Ensured communication by lip-reading Will communicate effectivelyand gestures
Anxiety for her baby - Allowed expression of anxietyRff physical dependence - Told about the condition of her babyand hospitalization - Explained that it may be risky for the
baby to enter in the ICD- Showed some photographs of her baby
Will demonstrate less anxiety- She was less anxious and
was happy to see her baby'sphotos
11) Progress Notes: Mrs Roopa improved in her respiratory function. Was puton T-Tube. And was able to maintain an Sp02 of 98% at room air. Buther chest infection persisted.
12) Health Teaching (planned for the time of discharge):
To take deep breathing and coughing exercises.
To take stem inhalation and perform effective coughing
Take the full course medications as prescribed
Protect the baby from infection by maintaining distance and restricting visitors
Take high protein, high calorie diet
To watch for redness or discharge from the LSCS incision
/
PRACTICAL 2 NURSING CASESTUDY/CASEPRESENTATION
"Structure
2.0 Introduction
2.1 Objectives
2.2 Definition and Purposes of Nursing Case Study
2.3 Developing a Nursing Case Study
2.4 Presentation of Nursing Case Study
2.5 Format of Nursing Case Study
2.6 Let Us Sum Up
2.7 Answers to Check Your Progress
2.8 Activities
2.0 INTRODUCTIONIn the previous Practical unit you have learnt about definition and importance ofnursing care plan. You have also learnt how to develop a nursing care plan. Asa student or staff you might have been accountable for complete care of anassigned patient. which include activities like collecting data about his/her problems,disease, medical treatment and identifying needs and planning the nursing care.You also have to take into consideration the patient's health history and all thefactors which affect his health condition Isituation to attain a picture of the patientas well as the facts about his illness and treatment. This whole information canbe documented in the form of case study. In this Practical unit you will learn aboutdeveloping and presenting a nursing case study I case presentation.
2.1 OBJECTIVESAfter completing this practical, you will be able to:
• define nursing case study;
• list the purposes of case study method; and
• prepare and present the nursing case study.
2.2 DEFINITION AND PURPOSES OF NURSINGCASE STUDY
Nursing Case Study is a comprehensive study made of the individual patient tobring about a complete understanding of the required nursing care, to providefactual basis on which to plan and implement his care, to get a prospective andunderstanding of his total care with particular emphasis on continuity of care. 21
/

, Nursing Intervention: Modalities
"
22
By learning about case study a nurse develops the concept or understanding ofa particular disease condition by thoroughly evaluating the management of patientcarried out throughout the patient's stay atthe hospital. It may also include anymanagement during the follow up visit or care at home.
The focus of the nursing care will be based on diagnosis and treatment of healthproblems. The information collected and reported by the doctor is also used bynurses, but within the focus of their care.
The patient's condition at the time of admission is assessed, It is followed byplanning of the management of the patient and by case study you will learncomprehensively case management in terms of clinical presentation, diagnosticevaluation, therapeutic interventions and prevention of complications.
You will accordingly plan the nursing care of the patient as per the nursing processsteps as discussed in the previous unit. The patient's progress is observed andprogress notes are recorded date wise. Discharge and follow up for rehabilitationand health teaching in the ward and at the time of discharge is planned andrecorded.
Purposes of Case Study Method
Case study method will help the nurses to:
• Correlate the theoretical knowledge about the disease as studied in the classroom or from text books with practical management in the clinical setting.
• Apply the knowledge and carry out the nursing care based on steps ofnursmg process.
• Observe the effects of therapeutic interventions on an ongoing basis or dailybasis and if there is need for a change in the therapeutic intervention /programme.
• Learn how to prevent complications and identify initial signs of developmentof any complication.
• Identify and meet patient's health needs by critically thinking and analyzingin relation to your knowledge and experience,
• Realise the importance of functioning of health care members as a team inthe management of a patient.
• Become familiar with professional literature to update your knowledge,
• Contribute towards building up of a specific body of knowledge in nursingscience. If the case studies are filed, they can be useful for future comparisonsand nursing research.
,.
2.3 DEVELOPINGANURSINGCASESTUDY• Initially you have to select a patient and then collect facts and information
related to his disease condition and his social and personal habits.
• List and describe his disease condition, diagnosis, signs and symptoms asfound in the patient.
I

• Compare the clinical picture, signs and symptoms as found in the patient withthose mentioned in text books or learnt in class room.
I
'.
• Compare the treatment or therapeutic intervention as pla~ned or done inyour patient with those studied in theory classes.
• Identify nursing needs and problems of your patient.
• Plan consequent activities, organize them into nursing care plan. Theseshould include supportive and therapeutic care given to the patient, healthteaching needs and how they wete met.
• Record the progress of the patient on daily basis.
• Look for and document the early signs of complications. Relate them andcompare with your previous knowledge acquired in class room learning.
Data assessed for nursing care study must be systematically obtained and organizedin such a manner that can be easily analyzed to make a judgement about thepatients health status and related health problems. The process of obtaining ahealth history and performing a physical examination is a very intimate experiencesfor both the nurse and the patient. A nurse should adhere to cultural codes of thepatient to avoid any culturally based practice while obtaining information for thepurposes of nursing history, total health information of past and present medicalconditions and treatment are included in the nursing history.
2.4 PRESENTATION OF NURSING CASE STUDYThe nursing case study may be written or presented verbally.
• If the study is written, it is generally considered best to record in narrativeform.
• An outline or format may be used as a guide but is not necessarily restricting·your initiative and creative ability in writing.
• A sample format of nursing case study is given in the section 2.5 of thispractical.
• If Nursing care study is presented in the form of verbal report it can bepresented among Peer group, Clinical rounds or Clinical discussions andit may be presented formally or informally.
Advantages of Written Nursing Case Study
• Provides scope for individual differences of the student.
• Provides an opportunity for self expression in writing.
• Provides experience in organizing and writing a paper in a scientific manner.
• Provides a source of material for future reference.
Limitations of Written Nursing Case Study
• Leaves no opportunity, once the study is completed, to branch out andincorporate new ideas.
• Requires a great deal of time to rewrite into an acceptable form.
I
Nursing Case Study/CasePresentation
23
. Nursing InterventionModalities
Advantages of Verbal Nursing Case Presentation
• Provides an opportunity for the supervisor to direct nurse's thinking into newchannels and to correct errors of information,
'.
• Serves as a basis for a better personal understanding and relationship betweenthe supervisor and the staff.
• Is time saving and does not require lengthy recopying of notes into acceptableform,
• Offers an opportunity for public speaking experience.
• Discussion is invited after presentation, the case becomes cooperative andall benefit from the study. This is a source of motivation to the presenter.
• The presenter feels the thrill of achievement in presenting her study to others.
Limitations of verbal Presentation
• Does not offer opportunity for writing and other creative expression.
• It is generally used, it leaves no records which may be kept for futurereference.
Check Your Progress I
i) List any four advantages of case study method.
a)
b)
c)
d)
ii) Fill in,the blanks with appropriate words.
a) Nursing case study can be presented in the form of verbal reportduring discussions/rounds,
b) Case studies can be filed so that they contribute towards building of
2.5 FORMAT OF NURSING CASE STUDYFormat for identification of data for nursing case study is more or less similar asfor nursing care plan, which you have studied in Practical- 1 of block 3 (PracticalCourse 2).
1) Identification data
• Patient's name
• Age
• Sex
24 • Religion and caste
I

/
• Marital statusNursing Case Study/Case
Presentation
• Education
• Occupation
• Ward No.
• Bed No..,
• MRD No.
• Date of admission.. Date of discharge•
• Provisional diagnosis
• Final diagnosis.
Duration of nursing care giveIi by you date from date to History :
1) Medical history & Nursing History
• Present complaints
• History of present illness
Onset of disease
Duration of disease
Any previous treatments and effects
Description of patient on admission
Date and place of admission
Patient's condition on admission
Any treatment given and investigationsdone at the time of admission
Past history of illness, treatment, operation, injuries, allergies andimmunization.
2) Menstrual history, if patient is female
3) Family history of illness
4) Socio-economic status
0 Marital tatus
0 No. of children
0 Total monthly income
0 Nuclear or joint family
0 Housing and sanitation
0 Type of accommodation 25

, .
Nursing InterventionModalitles
"
26
o Type of sanitation'
o Waste disposal
o Water supply
Personal history
o Dietary habits
o . Substance abuse
o Likes and dislikes
o Limitations and restrictions
5) Findings on physical examination: Subjective assessment which the patientwill reveal.
- Objective assessment: head to foot examination
6) Disease related information
• Definition of illness or disease
• Related anatomy and physiology
• Pathophysiology of disease condition
• Etiology / pre-disposing factors of disease
7) Signs and symptoms
Present in Patient under studvS.No. In Literature
8) Investigation
Patient's ValueInvestigation Normal RangeDate
,.9) ~anagement
Given to Patient PurposeS.No. In Literature
N.B.The treatment may include drugs, surgery, diet, physiotherapy, Radiationtherapy etc.
I

10) Management
11) .Nursing care plan (based on steps of Nursing Process)
Nursing Case Study/CasePresentation
Nursing Planning I plementation EvaluationDiagnosis Expected of ursing
outcome interventions
12) Complications..
.t S.No. In Developed Causes Preventive ManagementLiterature in the measures of developed
patient complications
13) Progress notes (these are to be written date wise)
14) Discharge and follow up planning (rehabilitation and health teaching in theward and at the time of discharge)
15) Summary and conclusions
16) Bibliography
2.6 LET US SUM UPIn this unit, you have learnt about the case study method, advantages of casestudy method, how to prepare case study and various forms and presentation ofnursing case study. You have also learnt about the advantages and limitations ofthe verbal presentation and written reports of case study.
2.7 ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
i) a) She is able to correlate the theoretical knowledge about the disease asstudied in the class room or from text books with practical managementin the clinical setting.
b) She is able to apply the knowledge and carry out the nursing carebased on nursing steps of nursing process.
c) She observes the effects of therapeutic interventions on an ongoingbasis or daily basis and if need for a change in the therapeutic intervention!programme is required.
d) She learns how to prevent complications and identify initial signs ofdevelopment of any complication.
ii) a) Clinical
b) Specific body of know ledge in nursing science 27
/

..
Nursing InterventionModalities
'..
28
2.8 ACTIVITIESi) Select a patient from medical / surgical critical care unit or any other critical
care unit of your work area.
• Collect the data and present the case to your peer group in the clinicalsetting.
• Record the activity
ii) Select a patient from medical / surgical ICD.
Prepare a written report of the case as nursing case study based on theguidelines given in the practical .
,.
/
Sample Case Study / Presentation
done on 26/09/10)
. -A CASE PRESENTATION ON - Coronary Artery Disease
Demographic data:
Name of the patent"
Age
I P No
Bed No
Ward
Date of Admission
TIme of Admission
Marital Status
Religion
Spoken Languages
Educational Status
Occupation
Address
Provisional Diagnosis
Final Diagnosis
Surgery Done
Personal History
Height
Weight
Smoking
Alcohol
Substance abuse
Diet
(CABG
Mr, Sunil Mehra
63~rs
32625
2310
IAMS
22/0912010
11:57:29 AM
Married
Hindu
Hindi,English
CA
Director, MNC
C26, Sector 14, NOIDA, UP
Coronary artery disease, BPH
Coronary artery disease (Triple Vessel Disease), BPH
Coronary artery bypass graft done with sephanousvein graft on 26/09/10
5 ft 9 inches
68 kg
8-11 packets a day since the age of 20 years stoppedat 50 yrs of age
Occasional, social drinking
No
Pure Vegetarian, eats all kinds of fruit, vegetables,pulses and grains, Prefers home cooked food preparedin desi ghee, stopped taking ghee and using oil since1999 when he was diagnosed as a hypertensive (BP150/90mm Hg)
Takes water 7-8 glasses per day
/
Nursing Case Study/CasePresentation
29

..
Nursing InterventionModalities
'..
. ,
.ft
30
Hygiene
Elimination
Well kempt, good hygiene measures used, dentalhealth moderate; brushes teeth once a day, bathesevery day.
Urinary frequency adequate. Patient has normal bowelelimination with occasional constipation.
Sleeping pattern A light sleeper, sleeps around 5-6 hrs 124hrs alongwith naps of around 15-20 min, now and then .
Socio economic history:
Mr Sunil is married for 35 yrs and lives in a Posh colony of NOIDA. He has twochildren-2 daughters who are married and settled .
Socio economic Status High Salaried MNC executive.
Own house in posh locality of NOIDA
Urban
Accommodation
Community\
Housing Facility
Type of house \
Ventilation
Own House
Concrete House
Proper
NOIDA water supply
Proper light supply system
Closed drainage system
Water Supply
Light supply
Drainage system
Medical history:
History of past illness:
• Hypertensive since1991 on irregular regimen of antihypertensive
• Suffers frequent UTI.
• Known case of COPD
• No other allergies.
• No other medical complains
Present complaints: Came to the emergency department with severe constrictingchest pain and pain in the left arm for last 2hours. Pain not relieved by rest. Also
,. complained of nausea, excessive perspiration and anxiety.
History of present illness:
• Patient was admitted to emergency room on 22/0912010, 8 pm with severepain in the left arm continued on even taking rest.
• Inj. Morphine was administered to relieve the pain.
• ECG revealed old MI. Cardiologist was summoned ..
• X-ray chest was done which revealed COPD.
I
• Other blood tests like Hb, TLC, DLC, LFf, SGOT, SGPT, PT, INR, BloodSugar, Serological nonreactive Test for HIV, HCV, Hbsag.
• Treated on Budecort+ Asthalin inhalation & Steam inhalation.
• BP was Found to be 170/92 rrunHg. Tab Amifruwas given orally.
• Temperature-99.8F. pulse was 88/min"
Family history:
Father has a history of hypertension
No family history suggestive of:
• • Ischemic heart disease
" • Congenital heart disease
• Stroke
• Diabetes or
• Bleeding
PHYSICAL EXAMINATION on 29/09/10
GE~'ERALAPPEARANCE:
61years 'old male who is awake and alert and who appears healthy and looks hisstated age.
VITALS
Temperature: 98.8°F (oral)
Blood Pressure: (with Normal adult Size Cuff)
• R ArmIPalpation (Systolic) - 120 mmlHg
• R Arm! Auscultation - 126/80 mmHg
• LArmlPalpation (Systolic) - 122 mmIHg
• L Arm! Auscultation - 126/80 mmlHg
Heart Rate by radial pulse palpation: 80 regular ( beats/minute)
Respiration Rate: 18 breaths/minute
HEAD:
• Configuration- nonnocephalic
• Hair- normal texture
• Scalp- No lesions, tenderness
EYES:
• Sclera- white
I
Nursing Case Study/CasePresentation
31

Nursing InterventionModalities
• Conjunctiva- pink
Fundoscopy:
e Pupillary reaction: present
"
• Disc: round, sharp margins, normal color
• Vessels: normal caliber, A!V ratio -1f2
o Background: no abnormal pigmentation, hemorrhages or exudates
• Macula: visualized
EARS:
• External Ear-No lesions, masses, tenderness
•. Auditory Canal- normal
• Eardrum- TM's gray, translucent, with normal light reflex
NOSE:
• Color- pink, no discharge
o Septum- midline
• Inferior and Middle Turbinate - normal
THROAT AND MOUTH:
• Teeth: Present
• Tongue: No lesions
• Gums and Mucosa: No swelling, bleeding, infection
• Pharynx and Tonsillar Fossa: normal
NECK• Active ROM: normal flexion, extension, lateral rotation and tilting
• Trachea: midline, mobile
• Thyroid: non-palpable or palpable, nl size & consistency, no lesions
• Suprasternal Notch: No pulsation
CHEST
Inspection: normal size, symmetrical. Incision on sternum. Healthy, nodrainage
Nipples: nipples symmetrical
• Neck Veins- No JVD at 45°
• Carotid Arteries: Normal32
y

• Palpation (Amplitude and Contour)- normal upstroke & amplitudeI?ilaterally
• Auscultation:murmurs & rub heard
PRECORDIUM:
"
• Inspection - No lifts or heaves - PMI not visible
• Palpation - No parasternal impulses, no thrills, '
• PMI- palpable in 5th ICS, MCL; normal size
AUSCULTATION:
." • Sl- heard best at apex, normal intensity
• S2- heard best at base, normal splitting
• Extra Sounds- S3,
• Murmurs-murmurs present
THORAX & BACK
Observation:symmetrical expansion with respiration
Percussion:no spinal tenderness, no CVA(costovertebral angle) tenderness
LUNGS• Percussion and Palpation of Lung Fields- normal resonant percussion
• Auscultation-hissing sounds heard, diminished vesicular breath soundson left side. COPD present
ABDOMEN
• Observation: scaphoid no scars.
• Auscultation:normal bowel sounds, no bruits
• Palpation: *Superficial - No tenderness, masses, guarding
*Deep - No tenderness, masses
LIVER• Palpation - liver edge not palpable
• Percussion - Size- -10 cm in R midclavicular line
SPLEEN
• Palpation-non palpable
KIDNEYS:
• Left- non palpable
• Right- non palpable
/I
Nursing Case Study/CasePresentation
33
I
Nursing InterventionModalities
FEMORAL PULSES:
• Palpation - 4 / 4 bilateral equal
• Auscultation - no bruits
EXTREMITIES
", Upper:
• Nails-No cyanosis, clubbing
• Palms- normal color, texture
• Muscles- normal size
• Joints (including ROM)
Interphalangeal- normal ROM, no deformities
Wrists - flexion = 900, = extension 70°, radial deviation = 20°,
ulnar deviation = 50°
Elbows - flexion = 160°
Radial pulse - 4 / 4, normal and symmetric
Lower:
• Nails - normal ( no cyanosis, clubbing)
• Muscles - normal size
• Joints (including ROM)
• Ankle - dorsiflex = 200, plantar flexion = 40°, eversion = 20°,
inversion = 20°
• Knee - flexion = 130°
• Hip - flexion = 100°, internal rotation = 40°, external rotation = 40°
• Sephanous graft taken from left leg
o Swelling present, wound healthy
o No discharge
PULSES:
• Posterior Tibial- 4 / 4 bilateral equal
• Dorsalis Pedis- 4 / 4 bilateral equal
SKIN: normal, no lesions
LYMPH NODES
Neck: Submental - not palpable
Submandibular - not palpable
34
/I

",
Anterior and Posterior Cervical - not palpable
Pre and Post Auricular - not palpable
Suboccipital- not palpable Supraclavicular- not palpable
Axillary: Central Axillary - not palpable
Pectoral- not palpable
Subscapular- not palpable
Lateral Axillary- not palpable
Epitrochlear: not palpable
Superficial Inguinal (horizontal and vertical): not palpable
NEUROLOGIC
Mental Status: Awake & Alert; oriented to person, place & time
Cranial Nerves:
• I: Ability to Smell - normal
• IT: Visual Acuity- 20/20 with pocket screener, both eyes
• Visual Fields- intact in all fields
• IT and lIT: Pupillary Reaction to Light- direct & consensual normal
o Accommodation- normal
o ( PERRLA, pupils, equal, round, reactive to light, and accommodationfor both)
• lIT, IV, VI: EOM- intact
• V: Light Touch Face- normal in all 3 divisions of V
• VII: Wrinkle Forehead, Close Eyes, Show Teeth- normal
• VIII: Hearing- normal by rough testing
• X: Cough- normal
• XI: Shrug Shoulders and check sternocleidomastoid muscles - normal
• Xll: Protrude Tongue- midline protrusion
Motor System:
Normal tone5 / 5 strength in all extremities
Sensory: Light Touch- normal
Position Sense- normal
Vibration- normal
Sharp- normal
/I
Nursing Case Study/CasePresentation
35
lNursing InterventionModalities Reflexes:
Deep tendon
• Biceps (C5-6)- 2/4
• Triceps (C6-7)- 2/4
• Brachioradialis-214",
• Knee (L2-4)- 214
• Ankle (S 1)- 2/4
• Plantar Reflex-none (bilateral down going toes)
Coordination:,It • Gait and Balance- normal
• Finger to Nose- normal
• Rapid finger movements- normal
• Tandem Walking- normal
• Romberg- negative
GENITAL EXAM
• Penis: Inspect and Palpate
• Meatus- no discharge
• Glans and Shaft- circumcised male - No lesions, masses or deformities
• Scrotum: Inspect and Palpate
Inspect-hypertrophied
Testes- little enlarged size
Epididymis and Spermatic cord- non tender
RECTAL AND PROSTATE EXAM
• Inspect Anus- no lesions
• Digital Exam of Rectum- normal sphincter tone, no masses
• Digital Exam of Prostate- hypertrophied prostate
• Stool for Occult Blood- negative
Disease related information
CORONARY ARTERY DESEASE
Definition
36
Coronary artery disease is characterized by the presence of atherosclerosis in theepicardial coronary arteries.Atherosclerotic plaques, the hallmark of atherosclerosis,progressively narrow the coronary artery lumen and impair antegrade myocardial
/I

blood flow. The reduction in coronary artery flow may be symptomatic orasymptomatic, occur with exertion or at rest, and culminate in a myocardialinfarction, depending on obstruction severity and the rapidity of development.
Prevalence
.,
Second half of the 20th century has witnessed a global spread of the coronaryartery disease (CAD) epidemic especially in developing countries, including India.Pramingham Heart Study in USA played vital role in defining the risk factors forCHD incidence in general population. The high rates of CAD in urban Indiacompared to rural, despite lower rates of smoking, suggest important roles fornutritional and environmental factors. There is a significant increase in BM! inurban compared to rural (BM! 24 versus 20 in men, 25 versus 20 in women).
There is also a higher rate of abdominal obesity among the urban population, withurban men having a waist to hip ratio (WHR) of 0.99 compared to 0.95 amongrural men, These increases in BM! and WHR result in significant insulin resistanceand dyslipidaemia. Urban-rural differences in prevalence of coronary risk factorsalso provide important information regarding risk factors that need prevention
Related anatomy and physiology
The right and left coronary arteries arise from the right and left coronary sinusesin the root of the aorta just above the aorticvalve orifice. The coronary arteries divideinto large and medium-sized arteries thatrun along the heart's surface (epicardialcoronary arteries) and subsequently sendsmaller arterioles into the myocardiume leftcoronary artery begins as the left mainartery and quickly divides into the leftanterior descending (LAD) and circumflexarteries. The LAD artery usually followsthe anterior interventricular groove and, insome people, continues over the apex.This artery supplies the anterior septum(including the proximal conduction system)and anterior free wall of the left ventricle(LV).The circumflex artery, which is usually smaller than the LAD artery, suppliesthe lateral LV free wall. Most people have right dominance: The right coronaryartery passes along the atrioventricular (AV) groove over the right side of theheart; it supplies the sinus node (in 55%), right ventricle, and usually the AV nodeand inferior myocardial wall. About 10 to 15% of people have left dominance:The circumflex artery is larger and continues along the posterior AV groove tosupply the posterior wall and AV node.
R~tC'OfOMry
_'I'(RCA)_ •.....tMright~ft...•..-.--"tI'I."tII\"tMic.\t&nel1M:t:0f1ht~
.;
CotOfttryVtlnstin bill')~"bOd<lO$hHlthfl'lw.rpr.tlotthtbOCtt
lOftinterior
('n' dn~nd(ng~)O~1I.'Ct •••• .,., (LAO).y •••• ~W0c4
.Nt,O"uMl~rI".••........•• ""fIOO'tOf..-
Pathophysiolm
Coronary atherosclerosis is often irregularly distributed in different vessels buttypically occurs at points of turbulence (e.g., vessel bifurcations). As theatheromatous plaque grows, the arterial lumen progressively narrows, resulting inischemia (often causing angina pectoris). The degree of stenosis required to produceischemia varies with 02 demand.
/
Nursing Case Study/CasePresentation
31

Occasionally, an atheromatous plaque ruptures or splits. Reasons are unclear butprobably relate to plaque morphology, plaque Ca content, and plaque softeningdue to an inflammatory process. Rupture exposes collagen and other thrombogenicmaterial, which activates platelets and the 'coagulation cascade, resulting in anacute thrombus, which interrupts. coronary blood flow and causes some degreeof myocardial ischemia. The consequences of acute ischemia, collectively referredto as acute coronary syndromes (ACS), depend on the location and degree ofobstruction and range from unstable angina to transmural infarction. Markednarrowing.can trigger thrombus formation, causing infarction or life-threateningarrhythmia. Spasm can occur in arteries with or without atheroma.
Nursing InterventionModalities
"
RISK FACTORS
Independent risk factors written Risk factors present in myin the book patient
A family history of CAD Present (Father hadHypertension)
cigarette smoking, Present
diabetes mellitus, Nohypertension, Presenthyperlipidemia, No_.t sedentary lifestyle, Present --
Noobesity.
If!
. "
These risk factors accelerate or modify a complex .and chronic inflammatoryprocess that ultimately manifests as fibrous atherosclerotic plaque.
CLINICAL MANIFESl'A..JIONS
Clinical Manifestations in book
Angina pectoris
Myocardial infarction----
Sensation of heaviness,
Clinical manifestations in thep "ent
~resentpresent
Present
No----.------------------~
Left arm pain present
~
L esent
Presentf--N--a-u-se-a-an-d-v-o-rru--'t-in-g--------- anIy nauseaL- ~I ~
ITightening, squeezing, orconstricting in the chest.
rlPain at rest or with minimalexertion that lasts more than 20
, minutes
Neck or jaw pain
Arm pain
Clammy skin
Shortness of breath
38
/
Present
Present
, .
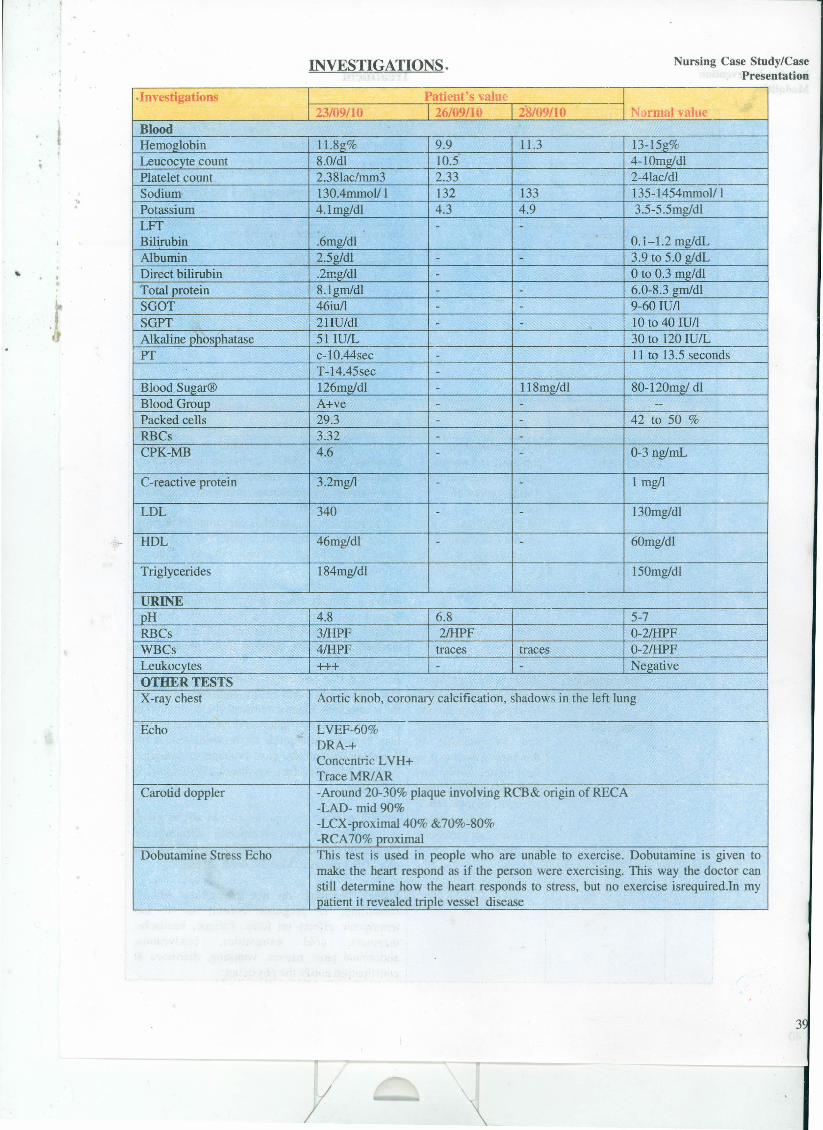
INVESTIGATIONS. Nursing Case Study/CasePresentation
".
.Investigations Patient's value23/09/10 26/09/10 28/09/10 t~irmal value
BloodHernoglobin l1.8g% 9.9 11.3 13-15g%Leucocyte count 8.0/dl 10.5 4-lOmgldlPlatelet count 2.381aclmm3 2.33 2-4Iac/dlSodium 130.4mmol/ I 132 133 135-1454mmoll 1Potassium 4.lmg/dl 4.3 4.9 3.5-5.5mgldlLIT - -Bilirubin .6mg/dl 0.1-1.2 mg/dLAlbumin 2.5g/dl - - 3.9 to 5.0 gldLDirect bilirubin .2mg/dl - o to 0.3 mg/dlTotal protein 8.1gmldl - - 6.0-8.3 gmldlSGOT 46iu/l - - 9-60 lUllSGPT 21IU/dl - - 10 to 40 lUllAlkaline phosphatase 51 lUlL 30 to 120 lUlL --PT c-l0.44sec - 11 to 13.5 seconds
T-14.45sec -
Blood Sugar@ 126mg!dl - 118mg/dl 80-120mg! dlBlood Group A+ve - - --
Packed cells 29.3 - - 42 to 50 %RBCs 3.32 - -
CPK-MB 4.6 - - 0-3 ng/ml,
C-reactive protein 3.2mg/l - - 1 mgll
LDL 340 - - 130mg/dl
HDL 46mgldl - - 60mg/dl
Triglycerides 184mg/dl 150mg/dl
URINEpH 4.8 6.8 5-7RBCs 3IHPF 2IHPF 0-21HPFWBCs 4IHPF traces traces 0-2IHPFLeukocytes +++ - - NegativeOTHER TESTSX-ray chest Aortic knob, coronary calcification, shadows in the left lung
Echo LVEF-60%DRA-+Concentric LVH+TraceMRlAR
Carotid doppler -Around 20-30% plaque involving RCB& origin of RECA-LAD- mid 90%-LCX-proximal40% &70%-80%-RC A70% proximal
Dobutarnine Stress Echo This test is used in people who are unable to exercise. Dobutamine is given tomake the heart respond as if the person were exercising. This way the doctor canstill determine how the heart responds to stress, but no exercise isrequired.In mypatient it revealed triple vessel disease
3
y
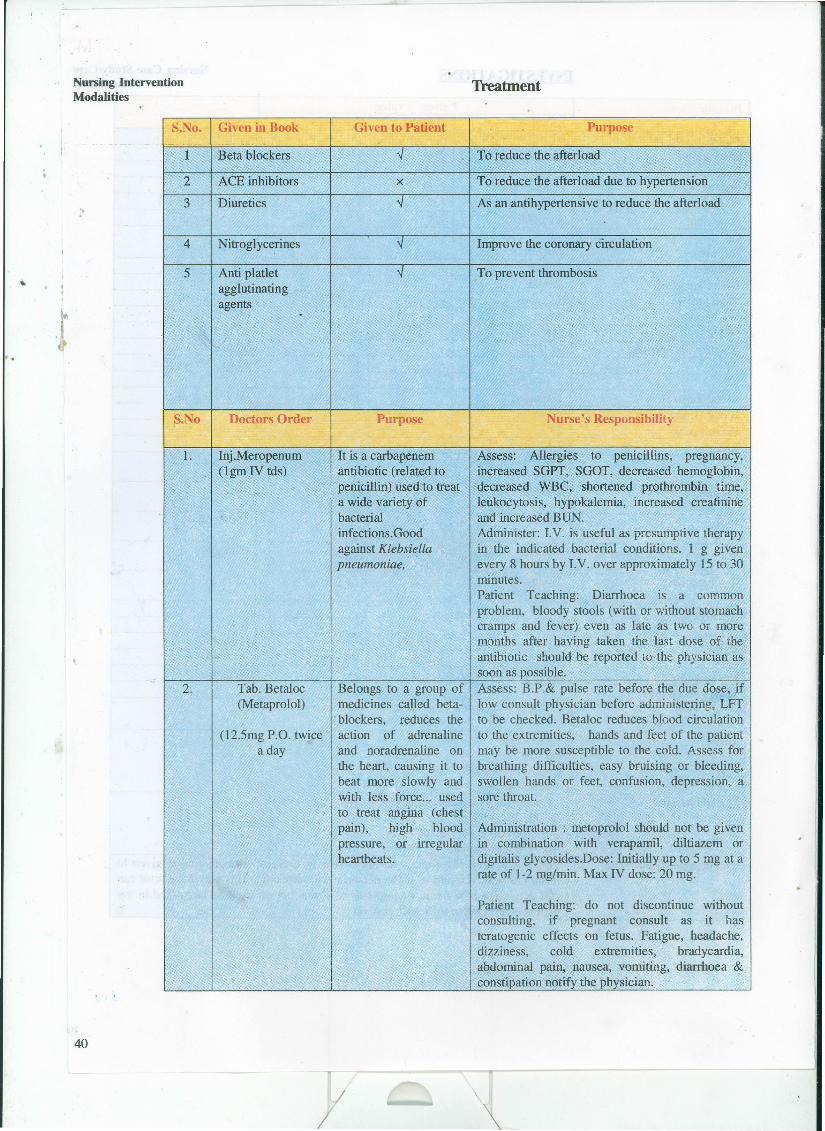
Nursing InterventionModalities
S.No. Given in Book
1 Beta blockers
2 ACE inhibitors
3 Diuretics".
4 Nitroglycerines
5 Anti platletagglutinatingagents .
Treatment
Given to Patient
x
Purpose
To reduce the afterload
To reduce the afterload due to hypertension
As an antihypertensive to reduce the afterload
Improve the coronary circulation
To prevent thrombosis
S.No Doctors Order Purpose Nurse's Responsibility
1. Inj .Meropenum(lgm IV tds)
It is a carbapenemantibiotic (related topenicillin) used to treata wide variety ofbacterialinfections. Goodagainst Klebsiellapneumoniae,
Assess: Allergies to penicillins, pregnancy,increased SGFT, SGOT, decreased hemoglobin,decreased WBC, shortened prothrombin time,leukocytosis, hypokalemia, increased creatinineand increased BUN.Administer: I.V. is useful as presumptive therapyin the indicated bacterial conditions. 1 g givenevery 8 hours by I.V. over approximately 15 to 30minutes.Patient Teaching: Diarrhoea is a commonproblem, bloody stools (with or without stomachcramps and fever) even as late as two or moremonths after having taken the .last dose of theantibiotic should be reported to the physician assoon as possible.
2. Tab. Betaloc(Metaprolol)
(12.Smg P'O. twicea day
Belongs to a group ofmedicines called beta-
.blockers, reduces theaction of adrenalineand noradrenaline onthe heart, causing it tobeat more slowly andwith less force... usedto treat angina (chestpain), high bloodpressure, or irregularheartbeats.
Assess: B.P.& pulse rate before the due dose, jflow consult physician before administering, LFrto be checked. Betaloc reduces blood circulationto the extremities, hands and feet of the patient 'may be more susceptible to the cold. Assess forbreathing difficulties, easy bruising or bleeding,swollen hands or feet, confusion, depression, asore throat.
Administration: metoprolol should not be givenin combination with verapamil, diltiazem ordigitalis glycosides.Dose: Initially up to 5 mg at arate of 1-2 mg/min. Max IV dose: 20 mg.
Patient Teaching: do not discontinue withoutconsulting, if pregnant consult as it hasteratogenic effects on fetus. Fatigue, headache,dizziness, cold extremities, bradycardia,abdominal pain, nausea, vomiting, diarrhoea &constipation notify the physician.
40
. .
F
Nursing Case Study/CasePresentation
and
Patient teaching May decrease oralabsorption of iron salts, don't take with foodscontaining iron.Any one of these symptomsif present inform the physician malaise orlassitude; myalgia; oedema; insomnia;hyperlipidaemia; flatulence, abdominal pain,constipation, eructation, dyspepsia, rectaldisorder; urinary frequency,
".
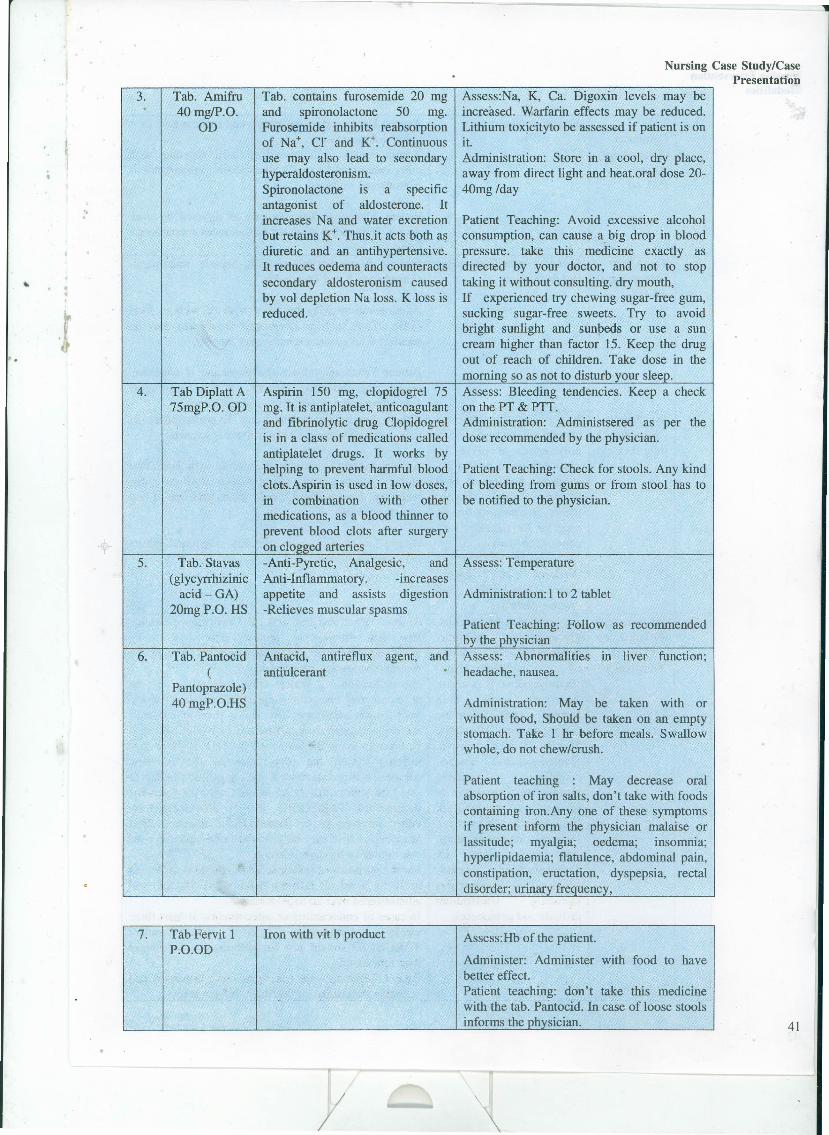
3.
4.
5.
Tab. Pantocid(
Pantoprazole)40mgP.O.HS
Tab. contains furosemide 20 mgand spironolactone 50 mg.Furosemide inhibits reabsorptionof Na+, cr and K+. Continuoususe may also lead to secondaryhyperaldosteronism.Spironolactone is a specificantagonist of aldosterone. Itincreases Na and water excretionbut retains ~+. Thus.it acts both asdiuretic and an antihypertensive.It reduces oedema and counteractssecondary aldosteronism causedby vol depletion Na loss. K loss isreduced.
Aspirin 150 mg, clopidogrel 75mg. It is antiplatelet, anticoagulantand fibrinolytic drug Clopidogrelis in a class of medications calledantiplatelet drugs. It works byhelping to prevent harmful bloodclots.Aspirin is used in low doses,m combination with othermedications, as a blood thinner toprevent blood clots after surgeryon clogged arteries-Anti-Pyretic, Analgesic, andAnti-Inflammatory. -increasesappetite and assists digestion-Relieves muscular spasms
Antacid, antireflux agent,antiulcerant
Assess.Na, K, Ca. Digoxin levels may beincreased. Warfarin effects may be reduced.Lithium toxicityto be assessed if patient is onit.Administration: Store in a cool, dry place,away from direct light and heat.oral dose 20-40mg/day
Patient Teaching: Avoid excessive alcoholconsumption, can cause a big drop in bloodpressure. take this medicine exactly asdirected by your doctor, and not to stoptaking it without consulting. dry mouth,If experienced try chewing sugar-free gum,sucking sugar-free sweets. Try to avoidbright sunlight and sunbeds or use a suncream higher than factor 15. Keep the drugout of reach of children. Take dose in themorning so as not to disturb your sleep.Assess: Bleeding tendencies. Keep a checkon the PT & PTT.Administration: Administsered as per thedose recommended by the physician.
Patient Teaching: Check for stools. Any kindof bleeding from gums or from stool has tobe notified to the physician.
Assess: Temperature
Administration: 1 to 2 tablet
Patient Teaching: Follow as recommendedby the physicianAssess: Abnormalities in liver function;headache, nausea.
Administration: May be taken with orwithout food, Should be taken on an emptystomach. Take 1 hr before meals. Swallowwhole, do not chew!crush.
7. Tab Fervit 1 Iron with vit b product Assess:Hb of the patient.P.O.OD
Administer: Administer with food to havebetter effect.Patient teaching: don't take this medicinewith the tab. Pantocid. In case of loose stoolsinforms the physician.
Tab. Amifru40 mgIP.O.
OD
Tab Diplatt A75mgP.O. OD
Tab. Stavas(glycyrrhizinic
acid-GA)20mgP.O. HS
6.
41

Nursing InterventionModalities
9.
Inj. Targocid400mg(Lyop
hilisedTeicoplanin)
8. Tab. Anti tubercular drugCombutol(Ethambutol)800mgP.O. od
".
"
42
Tab Alprax(Alprazolam).05HS
10. Syp Sparacid(Sucralfate )2OmgP.O. qid
11.
Given to treat the anxietyand depression
It is a basic aluminum saltof sulfated sucrose, whichpolymerizes at pH<4 bycross linking of molecules.Promotes healing of bothduodenal and gastriculcers, is considered to besuperior for patients, whocontinue to smoke.Also given III case ofduodenal and gastriculcers, bile .reflux andchronic gastritisTargocid is a bactericidal,glycopeptide antibiotic,produced by fermentationof Actinoplanesteicomyceticus. It is activein vitro against bothaerobic and anaerobicGram-positive bacteria.Species usually sensitive:Staphylococcus aureus,coagulase negativestaphylococci (sensitive orresistant to methicillin),streptococci, enterococci,Listeria monocytogenes,micrococci, group JKCorynebacteria, Gram-positive anaerobesincluding Clostridiumdifficile and peptococci.
Assess: Decreased visual aquity and make a note of itin the documentation.Administration: Ethambutol is used together withother medicines to treat tuberculosis. Ethambutol isadministerd withfood
Patient education: Take exactly as directed by yourdoctor. If any kind of visual disturbances encountered,inform.Assess: Assess for hypotension, hepatic impairment,slurred speech and Pregnancy.
Administration: May be taken with or without food(Side effects such as sleepiness/ drowsiness may bereduced if taken immediately after meals.).
Patient Teaching: inform the physician if conceive.Never stop this drug abruptly. Watch for fatigue,ataxia/impaired coordination, slurred speech.Assess: For kidney function test. Hypophosphatemiamay occur so a check on electrolytes is required
Administration:A void use of antacids with Sucralfateas they interfere in its action. Given 4 times a daytaken one hour before 3 main meals and one at bedtime for 4-8 wks
Patient Teaching: Constipation, dry mouth and nauseamay occur, inform.
Assess: Renal function test. If Creatinine clearanceless than 40 mL per minute, dose has to beadjusted.assess for agranulocytosis, Eosinophilia,thrombocytopenia or leucopenia.Administration: Water for injection in theaccompanying ampoule is injected slowly into the vialwith the dry substance. The vial is then shaken untilthe dry substance is completely dissolved. Care mustbe taken to avoid the formation of foam. If foam doesdevelop during the preparation of the injectionsolution, it is recommended that the solution be left tostand for approximately 15 minutes until the foam hasdisappeared. TARGOCID may be administered byeither intravenous or intramuscular injection. Theintravenous dose may be given by rapid injection overone minute or by short infusion.For the purposes of infusion, TARGOCID is dissolvedin 20 to 50 mL of infusion solution(NS/5%Dex) andadministered over 20 to 30 minutes.In cases of endocarditis or osteomyelitis at least threeweeks treatment is recommended.TARGOCID should not be administered for longerthan four months.Patient Teaching: rare occasions, lead to nausea andvomiting, headaches or dizziness, inform if so.

"
Nursing Case Study/CasePresentation
Assess; observe-for reversible airway narrowing.Antiasthmatic and COPDpreparationDoxofylline isa theophylline derivative.Similarly, its mechanismof action is related to theinhibition ofphosphodiesteraseactivities, resulting inbronchodilating effects,
12.' Tab.Synasma200mgBD
Asrninistration: May De taken with or without food.(May be taken wl meals to reduce GI discomfort.Some individual prep must be taken w/meals or on anempty stomach)
(doxofylline,Doxilate)
Patient teaching: adverse effects on the fetus, consultthe physician when pregnant and taking this medicine.
13. Budecort +Asthalin
Nebulization
Budecort is an inhaled Administration: This Respirator Solution may be usedglucocorticosteroid with a undiluted for intermittent administration. For this, 2favourable ratio between m1 of Solution is placed in the nebulizer and thetopical anti-inflammatory patient allowed to inhale the nebulized solution untilactivity and systemic bronchodialation is achieved. This usually takes 3-5activity, probably because minutes. Some adult patients may require higher dosesof a combination of high of salbutamol up to 10 mg, in which case, nebulizationlocal anti-inflammatory of the undiluted solution may continue until aerosolactivity, They provide the generation ceases.most potent andconsistently effective long-term control of asthma andhave been recommendedfor asthmatics of allseverities.
Asthalin+ budecortRespirator Solution isindicated for use in theroutine management ofchronic bronchospasmunresponsive toconventional therapy, andin the treatment of acutesevere asthma.
Management of the Patients with Coronary Artery Disease
Aim of the Treatment is to -
1. Reduce cardiac workload,
2. Improve coronary artery blood flow, and
3. Over the long term, halt and reverse the atherosclerotic process.
MEDICAL MANAGEMENT
1. Percutaneous coronary interventionPercutaneous coronary intervention (PCI), commonly known as coronaryangioplasty or simply angioplasty(baloon or stent placement), is one therapeuticprocedure used to treat the stenotic (narrowed) coronary arteries of the heartfound in coronary heart disease.
PCI is usually performed by an interventional cardiologist.
2. Antiplatelet AgentsAspirin is the mainstay of antiplatelet therapy for patients who have known 43
/I

Nursing InterventionModalities
"
44
coronary artery disease or symptoms suggestive of coronary artery disease. Aspirininhibits both cyclooxygenase and-the synthesis of thromboxane A2,
ClopidogreJ (plavix), a thienopyridine derivative, blocks adenosine diphosphate-induced platelet activation. Clopidogrel is indicated as an alternative for patientswho cannot take aspirin.
3. Antianglnal Agents• Betablockers,• calcium channel blockers, and• nitrate
Unless contraindications exist, all 'patients who have a history of angina pectorisshould carry sublingual nitroglycerin. Beta blockers are recommended as first-linetherapy for the management of stable angina in all patients with established coronaryartery disease.
Patients who have a history suggestive of vasospastic angina should be treatedwith a calcium channel blocker or a long-acting nitrate as an initial therapy. Eithertreatment option can also serve as a substitute for a beta blocker in the presenceof traditional angina when intolerable beta blocker effects ensue.
Nitrates improve exercise tolerance and prolong the time to onset of angina inpatients with exertional angina. They are contraindicated in patients who havesevere aortic stenosis or hypertrophic cardiomyopathy because they may adverselyalter hernodynamics and exacerbate symptoms. Ranolazine may be useful fortreating refractory angina pectoris.
• For acute thrombosis, sometimes fibrinolytic drugs
• Plasminogen, a::2-Antiplasmin,Streptokinase, Tissue Plasminogen Activator(t-PA),
• Coronary artery bypass grafting
4. Risk Factor Management
Hypertension
The management of hypertension in patients with coronary artery disease isexceedingly important. Not only does control of blood pressure reduce myocardialoxygen consumption and thereby reduce angina, but it also lowers the incidenceof cardiovascular events.
,. Beta blockers devoid of intrinsic sympathomimetic activity represent first-lineantihypertensive therapy for patients with a history of myocardial infarction orcoronary artery disease with angina.
Angiotensin-converting enzyme (ACE) inhibitors are indicated for all patients withdiabetes meIIitus or a history of myocardial infarction, particularly those withimpaired left ventricular systolic function. In the Heart Outcomes PreventionEvaluation (HOPE) study, high-risk patients without a history of a myocardialinfarction treated with the ACE inhibitor rarnipril experienced a significantreductionin major cardiac events.
/I
".
Calcium channel blockers are useful for patients with hypertension and anginadespite maximum tolerable beta blockade administration. The long-actingdihydropyridines are preferred; short-acting preparations should be avoidedbecause they might increase the risk of cardiac events via precipitous bloodpressure reduction and induction of the coronary steal phenomenon, divertingcoronary arterial blood flow from flow-limited myocardial regions.
Hyperlipidemia
Guidelines of the National Cholesterol Education Program (NCEP) haverecommended an LDL level lower than 70 mg/dl, for all patients with coronaryartery or other atherosclerotic disease. Patients whose LDL levels are higher than100 mg/dl. should start drug therapy. 3-Hydroxy-3-methylglutaryl coenzyme A(HMG-CoA) reductase inhibitors (statins) are the recommended first-line agentsfor patients who have coronary artery disease and elevated total and LDLcholesterol levels.
The NCEP also recommends a target HDL level higher than 45 mg/dl. for menwith coronary artery disease and higher than 55 mg/dl, for women. Patients withmetabolic syndrome (obesity, hypertension, and insulin resistance) often haveHDL levels lower than 35 mg/dL. These patients are at especially high risk forarterial vascular disease. Their recommended lifestyle changes include regularexercise and weight loss, which are two of the most effective ways to raise HDLlevels. If.lifestyle changes fail to increase HDL levels to their target, drug treatmentwith a fibrate or niacin should be considered, particularly in patients whosetriglyceride levels are higher than 200 mgldL.
Diabetes Mellitus
Diabetics with coronary artery disease have a particularly high risk for recurrentcardiovascular events, and they should be targeted for aggressive risk-factormodification. The American Diabetes Association recommends a hemoglobin Aelevel lower than 7%.
5. Lifestyle Modification
Patients with documented coronary artery disease should actively pursue lifestylemodifications that reduce the risk of future cardiovascular events.
Smoking
Tobacco use is one of the most important contributors to recurrent cardiovascularevents. Tobacco use induces endothelial dysfunction, reduces coronaryvasoreactivity, increases circulating carbon monoxide levels, impairs functionalstatus, and raises blood pressure.
Exercise
Functional capacity is a strong predictor of major adverse cardiac events. Functionalcapacity can be improved by following an exercise program that includes at least30 minutes of exercise 3 or 4 days/week; a daily regimen is optimal.
Weight Control
The best weight management strategy is diet and exercise. Ideal benchmarks area body mass index between 19 and 25 kg/m? and a waist circumference of no
/I
\
Nursing Case Study/CasePresentation
45
..
Nursing InterventionModalities
"
46
more than 40 inches for men and 35 inches for women. Weight loss has afavourable metabolic syndrome impact on many cardiac risk factors, includinghypertension, high LDL level, low fIDL level, and glucose intolerance.
SURGICAL MANAGEMENT:
Revascularization
The primary revascularization options are percutaneous coronary intervention andcoronary artery ~ypass grafting surgery. The most common PCI techniques arepercutaneous transluminal coronary angioplasty and coronary stenting. A majorlimitation of PCI is restenosis at the intervention site. This represents the body'sresponse to local injury with an exaggerated neointimal proliferative response. Theuse of stents, aspirin, clopidogrel, and glycoprotein IIblIlla inhibitors lowers therate of restenosis to less than 10% at 6 months in optimal circumstances.
The most common conduits for CABG are the saphenous vein and the internalthoracic (mammary) artery. The long-term patency rates of internal thoracic arterygrafts are superior to those of venous grafts.
CORONARY ARTERY BYPASS GRAFTING (performed in my patient)
Coronary artery disease involves impairment of blood flow through the coronaryarteries,most commonly by atheromas.Clinical presentationsinclude silent ischemia,angina pectoris, acute coronary syndromes (unstable angina, MI), and suddencardiac death. Diagnosis is by symptoms, ECG, stress testing, and sometimescoronary angiography. Prevention consists of modifying reversible risk factors(e.g., hypercholesterolemia, hypertension, physical inactivity,obesity,and smoking).Treatment includes drugs and procedures to reduce ischemia and restore orimprove coronary blood flow.
The number of bypasses• The single vessel bypass• Double vessel bypass [(e.g., the left anterior descending (LAD) coronary
artery and right coronary artery (RCA)]• Triple vessel bypass [(e.g., LAD, ReA, left circumflex artery (LCX)]• Quadruple vessel bypass [(e.g., LAD, RCA, LCX, First diagonal artery
of the LAD)]• Quintuple means five. More than four coronary arteries are uncommon.
THE RISKS AND COMPLICATIONS OF CABG SURGERY
r
Overall mortality related to CABG is 3-4%. During and shortly after CABGsurgery, heart attacks occur in 5 to 10% of patients and are the main cause ofdeath. About 5% of patients require exploration because of bleeding. This secondsurgery increases the risk of chest infection and lung complications. Stroke occursin 1-2%, primarily in elderly patients. Mortality and complications increase with:• age (older than 70 years),• poor heart muscle function,• disease obstructing the left main coronary artery,• diabetes,
/I
• chronic lung disease, and• chronic kidney failure.
Mortality may be higher in women, primarily due to their advanced age at the timeof CABG surgery and smaller coronary arteries. Women develop coronary arterydisease about 10 years later than men because of hormonal "protection" whilethey still regularly menstruate (although in women with risk factors for coronaryartery disease, especially smoking, elevated lipids, and diabetes, the possibility forthe development of coronary artery disease at a young age is very real). Womenare generally of smaller stature than men, with smaller coronary arteries. Thesesmall 'arteriesmake CABG surgery technically more difficult and prolonged. Thesmaller vessels also decrease both short and long-term graft function. J
"
PROGNOSIS
Prognosis following CABG depends on a variety of factors, but successful graftstypically last around 10-15 years.
NURSING MANAGEMENT
PREOPERATIVE ASSESSMENT
• History• Physical examination• Radiographic examination• Electrocardiogram• Laboratory analysis• Assessing patient's functional level• Psychosocial assessment.• Family support systemPHYSICAL EXAMINATION• General appearance and behaviour• Vital signs• Nutritional and fluid status, weight and height• Inspection and palpation of heart• Auscultation of heart
• NP• Peripheral pulses.• Peripheral edema.PSYCHOSOCIAL ASSESSMENT• Meaning of surgery to patient• Coping mechanisms being used.• Support system in effect• Fear regarding present & future• Knowledge & understanding of surgical procedure.
//
Nursing Case Study/CasePresentation
47
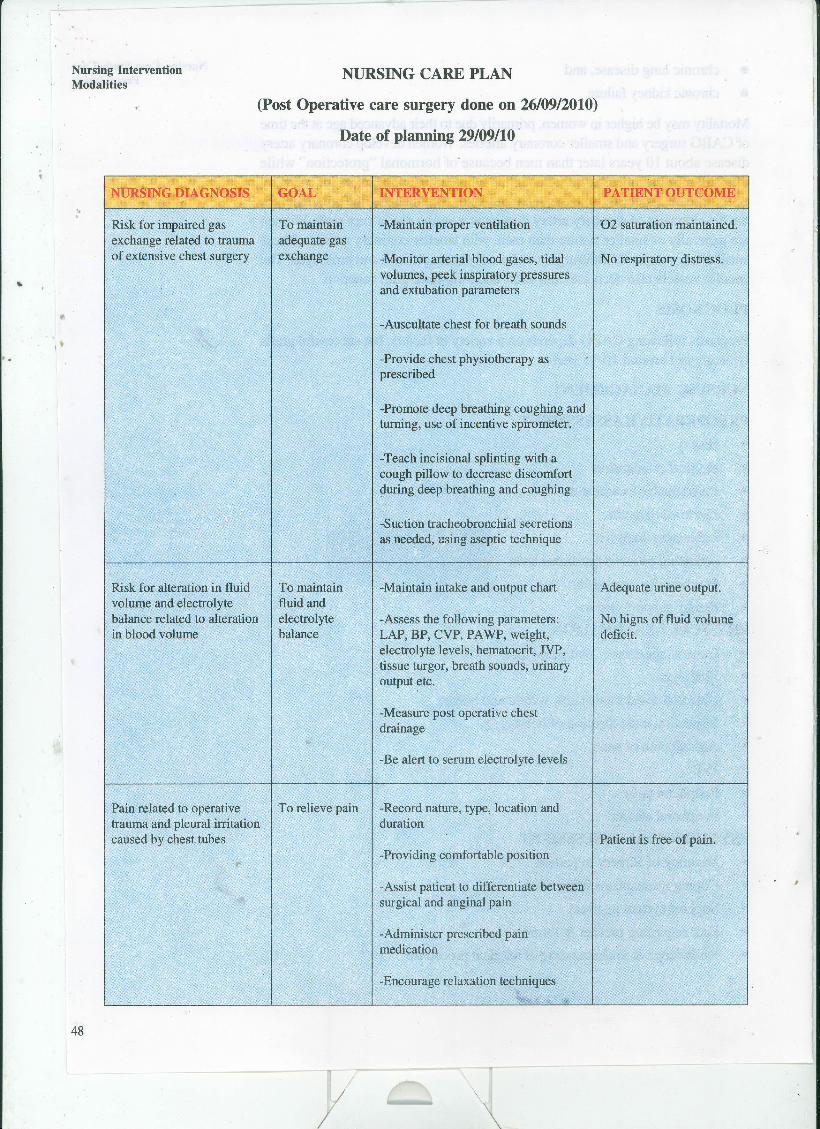
Nursing InterventionModalities
NURSING CARE PLAN
(Post Operative care surgery done on 26/09/2010)
Date of planning 29/09110'
",NURSING DIAGNOSIS GOAL INTERVENTION PATIENT OUTCOME
Risk for impaired gas To maintain -Maintain proper ventilation '02 saturation maintained.exchange related to trauma adequate gasof extensive chest surgery exchange -Monitor arterial blood gases, tidal No respiratory distress.
volumes, peek inspiratory pressuresand extubation parameters
-Auscultate chest for breath sounds
-Provide chest physiotherapy asprescribed
-Promote deep breathing coughing andturning, use of incentive spirometer.
-Teach incisional splinting with acough pillow to decrease discomfortduring deep breathing and coughing
-Suction tracheobronchial secretionsas needed, using aseptic technique
Risk for alteration in fluid To maintain -Maintain intake and output chart Adequate urine output.volume and electrolyte fluid andbalance related to alteration electrolyte -Assess the following parameters: No higns of fluid volumein blood volume balance LAP, BP, CVP, PAWP, weight, deficit.
electrolyte levels, hematocrit, JVP,tissue turgor, breath sounds, urinaryoutput etc.
-Measure post operative chestdrainage
-Be alert to serum electrolyte levels
Pain related to operative To relieve pain -Record nature, type, location andtrauma and pleural irritation durationcaused by chest tubes Patient is free of pain.
-Providing comfortable position
-Assist patient to differentiate betweensurgical and anginal pain
-Administer prescribed painmedication
-Encourage relaxation techniques
I •
48
I

"
Nursing Case Study/CasePresentation
Patient is free of pain.
Fluid intake - outputmaintained.
Adequate urine output.
Maintained the bodytemperature
Dressing of the donor sitedone as per the protocolby the surgeon. No woundinfection
Adequate sleep ensured
·0o
Pain related to operativetrauma and pleural irritationcaused by chest tubes
Risk for decreased renalperfusion related todecreased cardiac output.
Risk forhypothermia/hyperthermiarelated to cardiopulmonarybypass surgery, infectionsetc.
Risk for sensory- perceptualalterations related to sensoryoverload
To relieve pain
To maintainadequate renalperfusion
To maintainnormal bodytemperature
To preventinfection at thedonor site
To preventsensory-perceptualalterations
/I
-Record nature, type, location andduration
-Providing comfortable position
-Assist patient to differentiate betweensurgical and anginal pain
-Administer prescribed painmedication
-Encourage relaxation techniques
-Measure urine output strictly
-Monitor renal function tests
-Report to physician if urine outputless
-Administer medications as prescribed
-Warm the patient gradually withwarm air or warm blankets or heatlamps •
-Assess for dysrythmias due tohypothermia
-Assess for elevated body temperature
-Assess for infection (lungs, urinarytract, incisions and intravascularcatheter)
-Antibiotic therapy as advised by thecardiac surgeon.
-Use the aseptic technique whiledressing and other procedure
-Using propel hand washingtechnique
-Meticulous care to be taken toprevent contamination at the sites ofcatheter and tube insertion.
-Care of the graft donor site.
-Explain all procedures to patient
-Plan nursing care to provide forperiods of uninterrupted sleep withday-night pattern
-Decrease sleep preventingenvironmental stimuli as much aspossible
-Promote continuity of care fromnurse to nurse
-Orient the patient to time, place andperson. Encourage the family to visitat regular times
-Teach relaxation and diversionaltechniques
.
49
. ,
Nursing InterventionModalities
-,
Knowledge deficit about To develop the Develop teaching plan-for patient and Patient is able to list thehome self care patient's family specifically about: self care and rehabilitative
knowledge measuresregarding • Dietcardiac • Activity progression But need to carry outrehabilitation • Exercise themand self care • Deep breathing, coughing
exercises• Medication regimen• Relaxation exercises and de-
stressing measures• Follow up
.It PATIENT'S DAY TO DAY PROGRESS:
.:. Day 1(29/09/10)
This is patient's 3RD post op day
Vital Parameters: Temp; 98.8 F, pulse: 88/ min; Resp; I8/min
Lab Reports: Normal (as shown in the table above)
Cardiac Parameters: ECG normal, 02 saturation 98
Drainage tubes: Removed today.
Mobility: Patient went to the toilet with the help of assistance.
Nutrition: Nourished adequately on soft diet.
Medications: continued as advised
Psychological aspect: Patient shows no signs of anxiety, Wife and Twodaughters are supportive. Patient is cooperative and obeys the commands .
•:. Day 2 (30/09/10)
,.
Vital Parameters: Temp; 98.4 F, pulse: 90/ min; Resp; I8/min
Lab reports: Urine sent for RE & culture.
Cardiac Parameters; ECG normal, 02 saturation 98
Mobility: Patient went to the toilet with the help of assistance; daily activitiesfollowed activities of daily living with the help of his wife.
Nutrition: Nourished adequately on soft diet and IV fluids as advised
Medications: Continued as advised
Psychological aspect: Patient shows no signs of anxiety, Wife and Twodaughters are supportive, is keen to participate in the rehabilitation programme
Wounds at the donor graft site: Healing well, no fever, no other signs ofinfectios at the wound site and systemically.
50
/
.tt
"
Discharge and follow up planning (at the time of discharge)
• To take Diet with low fat and only unsaturated fatty acids like refmed oil
• To perform activities gradually
• To carry Daily Exercises should start with gradual progression
• Deep breathing, coughing exercises to be done 3-4 times daily
• Medication regimen to be strictly followed
• To perform Relaxation exercises and meditations to relieve stress.
• Watch for signs of redness, discharge, and wound gaping at chest wound
• Come for Follow up after one week
Summary and Conclusion.
• The diagnostic and treatment options for coronary artery disease are changingrapidly.
• New pharmaceuticals are being developed and introduced into the treatmentarmamentarium.
• Biologic markers are now used to track coronary artery disease activity atthe vascular level, guiding medication selection and dose titration.
Procedures are less invasive and offer percutaneous treatment optionssuch as drug-eluting stents, previously unavailable.
• Despite these advances, coronary artery disease and its deleteriousmanifestations represent the number one killer in the United States. This islargely caused by poor dietary choices, sedentary lifestyles, and continuanceof tobacco use.
• Efforts at both primary and secondary prevention of obstructive coronaryartery disease among the general public are still lacking.
• Public awareness campaigns are a partial success.
• It is imperative for the physician to allocate time to address the importanceof lifestyle modification efforts.
• Furthermore, the genetic basis of coronary artery disease is slowly beingunraveled.
• In the future, a genetic assessment of an individual's risk for the developmentof atherosclerotic vascular disease may be possible at a young age.
• These findings may guide lifestyle modification prescription and the choiceand dosage of select pharmaceuticals.
• One thing is clear - a preemptive approach is the best way to tackle theenormity of coronary artery disease.We must erase the myth that medications,stenting, and bypass surgery are curative approaches. Instead, the patientmust meet the health care team at least halfway to achieve ;1 successful healthoutcome.
//
Nursing Case Study/CasePresentation
51
I
,.
Nursing InterventionModalities
",
52
BmLIOGRAPHY
• http://www.interscience.wiley.com/joumal/9660/abstract
• http://prf.sagepub.com/cgilcolltentJabstractl23/5/267
• http://www.mayoclinic.com/healthlheart-diseaseIHBOOO16
• http://www.springerlink.com/contentlkrk622453rr07m68/
• http i//www .ctsnet. org/ sections/ c lin icalresources/ adul tcardiac/zenati.html ?cfid=34842500&cftoken=66168423
BOOKS
• Royal & walsh," Watson's Med-Surg Nursing and Related Physiology", 4thEdn. ELBS with Bailliere Tindall
• Thompson et al,"Mosby's Manual of Clinical Nursing." 2nd Edn., MosbyCompany
• Smeltzer et al," Brunner And Suddarth Text Book Of Med. Surg Nursing."9thEdn. Lippincott & company
• Doenges et al," Nursing Care Plans- Guidelines For Individualizing PatientCare." 6thEdn. FA Davis Co ..
• Black & Jacob," Med. -Surg. Nursing- Clinical Management for ContinuityOf Care." yll Edn.,W B Saunders Co., 891-913.
Since nursing personnel are accountable for quality nursing care, they need toestablish values to evaluate the care given. The observations made to evaluatethe nursing care can either be narrated in the log book or an anecdote can be 53
PRACTICAL 3 OBSERVATIONCHECKLIST
Structure
3.0 Introduction
3.1 Objectives
3.2 Concepts, Definitions and' Characteristics of Observation Checklist3.2.1 Definition of observation check list3.2.2 Characteristics of observation check list3.2.3 Phenomena that can be observed
" 3.3 Steps and Prerequisites of Developing Observation Checklist
3.4 Sample Check List
3.5 Let Us Sum Up
3.6 Answers to Check Your Progress
3.7 Activities
3.0 INTRODUCTIONNursing personnel are accountable for quality nursing care. Nurse as health careproviders are expected to observe and record nursing actions to evaluate thequality of nursing care given to a patient in any unit under different conditions. Soit becomes necessary to make specific observations and record those observationsto evaluate the quality of care. There are various techniques which help a nurseto evaluate the nursing care given. One of these measures is observation checklist. In this practical we will discuss how to prepare and use an observation checklist for implementing and evaluating the nursing care of patient.
3.1 OBJECTIVESAfter completing this practical, you will be able to:
• discuss the phenomena that can be observed;
• discuss the characteristics of observation method;
• defme observation check list; and
• prepare observation check list by following appropriate steps.
3.2 CONCEPTS, DEFINITIONS ANDCHARACTERISTICS OF OBSERVATIONCHECKLIST
//
Nursing InterventionModalities
maintained. These nursing actions / interventions can be even rated against a ratingscale. An objective method of evaluating nursing care is by preparing a set ofstatements which ideally should have been done in a particular given situation.The performance of stated actions then can be checked whether performed ornot performed.
3.2.1 Definition of observation check list
" Observation check list is a structured written decument prepared in a formatand used to evaluate the nursing care given to a patient against a presetstandard. .
This includes a pre determined set of statements which should have beenperformed in order to deliver quality nursing care. The observer or evaluatorchecks whether these activities have been performed or tallies the frequencyof a desirable or required behaviour.
It is a tool used for structured observation where phenomenon are recordedby putting a tally against a particular behaviour, event or characteristicdepending upon its presence or absence.
3.2.2 Characteristics of observation check list
I·
• Observation is specific and is not haphazard just looking around for general -impressions.
• Observation of behaviour is systematic and specific to certain activities.
• Observation is quantitative. It means recording the number of instances,certain types of behaviours are noted.
• Observation is recorded immediately - notes are made promptly rathertrusting your memory.
• Observation should be done by someone trained to do such work.
3.2.3 Phenomena that can be observedThere are various phenomena that can be observed in nursing:
• Characteristic and conditions of individuals, such as physiological conditions,vital signs, bowel movements, muscle / moto~ activity etc.
• Verbalcommunication behaviours, such as linguistic behaviour, conversations.
• Non-verbal communication behaviours such as facial expressions, touch,posture, body movements, gestures.
• Activities for example actions that serve as index of health status, performanceactivities of nurses, performance of procedure.
• Environmental characteristics such as noise levels, cleanliness that haveprofound effect on health or individual's behaviour.
3.3 STEPS AND PREREQUISITES OFDEVELOPING OBSERVATION CHECKLIST
54
Now that you have learnt about the definition and characteristic of observationyou will study about the steps and prerequisites of developing observation checklist
/I
..
, .
To develop an observation checklist you need to: .
• Select the aspect of the behaviour to be observed .:
• Mention behaviours in observable terms.
• List behaviours on the left hand column
"• Place check marks on the right hand column.
• Facilitate sufficient opportunities to make observations and check' the.performance accurately.
• Observe the behaviour in real situation.
• Give feedback about the inaccurately perfo!'IIled activities to the concerned, person .
• List the categories of behaviour that mayor may not be manifested by theperformer.
Prerequisites for constructing observation checklist
• Give the definition of behaviour and characteristics to be observed.
• Refer the behaviour based on component of nursing care.
• Develop a system of coding in simplest fashion from simple to complex.
• Do not club together the different aspects of an activity to be observed
• Ensure generalization of system to wide variety of situations.
• Develop, refine and re-test a new category system after trial of the preparedcheck list.
3.4 SAMPLE CHECK LISTPost operative check list to evaluate nursing care following cardiothoracicsurgery
Identification data
Name of the Patient
Age / Sex
Ward / Bed No.
M.R.D. Number
Diagnosis
Operation done
Date of operation
Post-operative day
I
Observation Check List
55

Nursing Intervention- , Modalities
),
",
56
.Post-Operative Check List
S.No. Post-operative Nursing Activities Yes No(Immediate post-operative period for firstfour hours)
l. Kept the AMBU with O2 connection ready atthe bed side.Checked suction, monitors kept ready,ventilator kept ready. .
2. Patient received, IIV lines, and IIV fluidsrestored.
3. Chest drain ages restored.4: Monitors attached.
If required, patient put on to ventilator.Ventilator setting checked.
5. Mediastinal suction attached at low suction.Right and left thoracic suction kept at 0.5mmHg.
6. Chest Drainage recorded at every 15 minutesfor 1 hour.
7. Reported to the surgeon if drainage> 150 ml.8. Head end elevated (30°). . ~9. Checked and recorded pulse, BP,
respiration, temperature, skin colour. IUrine output recorded hourly-
10. ABG recorded every hour.11. Patient not sedated before neurological
examination12. Medications administered as advised:
- Ionotropes- Antibiotics- Heparin/Protamine sulphate- Mannitol- Blood transfusion/plasma
13. ET suction done SOS14. Patient extubated after 4 hours if patient is
stabilized15. NPO status and N / G suction SOS16, Chest physiotherapy performedLATE POST-OPERATIVE PERIODl. Checked and recorded vital signs2. Observed for gag reflex3. Sips of water given after 4 hours of
extubation4. Watched for mediastinal suction tubes,
drainage and recorded.5. Wounddressing and care of other puncture
sites / arterial or venous lines given.
/
.r
".
6. Chest binder applied7. Chest physiotherapy / vibrations performed8'. Steam inhalation given9. Deep breathing and coughing exercises
encouraged10. Position changed 2 hourly .11. Spirometry encouraged12. Removal of urinary catheter13. Ambulation by first post-operative day13. Transfer to post-opetative ward by 2_3raday
as patient improves14. Alternate stitch removal by 7-9 days
Remar~ _
Signature with date
Check Your Progress 1
i) Define check list.
ii) List the phenomena that can be observed?
3.5 LET US SUM UPIn this unit you have learnt definition characteristics and prerequisites ofobservation checklist and its importance in evaluating nursing care. We have alsodiscussed preparation of observation check list as a tool for evaluation. and stepsof preparing observation check list.At the end a sample check list has been givento enable you to develop and use the check list.
3.6 ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
i) It is a tool used for structured observation where phenomenon are recordedby putting a tally against a particular behaviour, event or characteristicdepending upon its presence or absence.
ii) Characteristic and conditions of individuals, such as physiological conditions,vital signs, bowel moments, muscle / motor activity etc.
• Verbal communication behaviours, such as' linguistic behaviour,conversations.
II
Observation Check List
57
I
Nursing InterventionModalities • Non-verbal communication behaviour such as facial expressions, touch,
posture, body movements, gestures.
"
• Activities for example actions that serve as index of health status,performance activities of nurses, performance of procedure.
• Environmental characteristics such as noise levels, cleanliness that haveprofound effect on health or individual's behaviour.
3.7 . ACTIVITIES
"i),
.I ii)
,.
Prepare a check list for discharge of a patient with renal transplant.
Select a patient undergoing coronary by-pass surgery and Prepare a checklist for pre-operative nursing actions for the patient.
,.
58
II I

\
PRACTICAL 4 CONDUCTINGCLINICALTEACIDNG
Structure" 4.0 Introduction
4.1 Objectives
4.2 Clinical Teaching Methods4.2.1 Nursing care plan
4.2.2 Nursing case study4.2.3 Demonstration
4.2.4 Bedside Clinic4.2.5 Nursing Round4.2.6 Clinical conferences
4.2.7 Individual conference
4.3 Proforma for Clinical Teaching
4.4 Let Us Sum Up
4.5 Answers to Check Your Progress
4.6 Activities
4.0 INTRODUCTIONillpractical 3 of this block you have learnt about the preparation of observationcheck list for assessing patient care problems and interventions. In this practicalyou will learn about the preparation of clinical teaching proforma to be usedwhile performing clinical teaching.
You may recall a morning nursing rounds, or demonstration of a new procedure,or use of a new equipment in your ward. These are all examples of clinicalteaching. Clinical teaching is a valuable learning device because it develops theobservational skills and stimulates thought process in the students for providingskilled nursing care of the patients. The students apply their knowledge, skills andattitudes in clinical teaching - learning situations. We shall focus on how to conductclinical teaching and preparing lesson plans for clinical teaching
4.1 OBJECTIVESAfter completing this practical, you will be able to:
• explain various clinical teaching methods used in nursing programmes;
• discuss the teacher's role in conducting clinical teaching in a clinical area; and
• develop various proforma required for conducting clinical teaching in theclinical setting.
59
II
, .
Nursing InterventionModalities 4.2 CLINICAL TEACIllNG METHODS
".
Clinical area is an important teaching-l~arning situation in nursing. It provides thedirect practical real life learning situation where the student directly observes thepatient or the skills performed and practiced on the patient. Students respond tothis method of teaching with enthusiasm. Their interest in learning increases andthey show ability to share ideas and knowledge with others for the benefit ofpatients.
Clinical teaching can be imparted by the nursing faculty, nurse administrator,doctor or any other health team member.
There are various methods used in clinical teaching -
,rt
• Nursing care plan
• Nursing care study
• Demonstration
• Nursing rounds
• Clinical conference
• Bedside clinic
• Group conference
• Individual conference.
4.2.1 Nursing care planYou have already learnt about nursing care plan in practical! nursing case study.
4.2.2 Nursing case studyYou have already learnt about nursing case study in practical 2.
4.2.3 Demonstration
60
Demonstration method is a clinical teaching method in which the teacher exhibitseach step of the process of procedure of a clinical skill in its natural sequence withexplanation of the step. The students learn through observation, thereby developinga mental image of each processes or procedures fortified by verbal commentary.Demonstration method can be used in nursing clinics, conferences or in the patientteaching programmes. It can also be used to teach various ways of establishingrapport with the patient and provide health education.
Purposes
• Provide better learning opportunity by correlating theory with practice.
• Helps in better learning as actions and verbal instruction go side by side
Requisites for a good demonstration
• The demonstrator should be well versed with the procedure to bedemonstrated. She must practice before demonstrating the procedure andshould have the competence in demonstrating the clinical skill.
//
-,
• The articles should be arranged in order of use and tested before, for thegood working condition.
• The students should have knowledge about the topic/procedure or any specialapparatus to be used, in advance to save time and avoid distraction. Amimeographed directions can be given before starting demonstration of aprocedure.
• The patient should be informed about the purpose of the demonstration andpresence of the students. His consent should be taken and patient should bemade comfortable.
Conducting ClinicalTeaching
• The students should have a good view of the actions and procedural steps.
• The steps should accompany the verbal comments and explanation of thestep with the rationale wherever necessary.
• Discussion period should always follow the demonstration for clarification,reemphasizing and surnmarization.
• Arrange for supervised return demonstration for the students as soon aspossible for best retaining and recall.
Conducting demonstration
, Arrange the articles near the bedside of the patient for easy access.
• Explain the procedure to the patient and also how s/he is expected tocooperate during the procedure.
• Demonstrate the procedure step by step explaining the scientific importanceof each step.
• After completing the procedure, make the patient comfortable.
• • Dispose the used articles according to the unit/ward policies.
• Document the procedure and its findings/result.
• Discuss and clear doubts/queries of the students.
4.2.4 Bedside ClinicIt is one of the best methods of teaching and learning situation. The purpose ofthe bed side clinic is to portray the nursing problems and to give vivid picture ofthe related nursing care by associating it with a specific individual.
Purposes
• To provide learning experience for nursing student and to collect informationabout the patient with tact and skill.
• To improve the student's ability to solve nursing problems by detailed studyand analysis of nursing care situation.
• To realize the need for understanding each patient as an individual in orderto appreciate his problems and outlook.
61
y

,.
Nursing InterventionModalities
"
I~
.j,,
62
• To help the student to observe nursing care in an organized and systematicway.
• To be able to work out a nursing care plan to fit in to the needs of individualpatient on the basis of his special problems.
• To be able to recognize opportunities for health teaching in the hospital.
• To understand functioning of certain types of apparatus equipment beingused on patients.
Pre-requisites for conducting bedside clinic
For conducting bedside clinic first of all you should -
• Plan the clinic time, place, patient depending upon the topic and objectives.The students should be aware of the topic beforehand so that they can comeprepared for discussion.
• Obtain the patient's consent for his cooperation.
• Arrange for the comfort and the privacy of the patient.
• Take care that bedside clinic should not disturb other patients or the wardroutine. It should not be held for more than 30 minutes.
\\
Techniques of conducting bedside clinic
• Introduce the patient to the group of students.
• Present the case to the group of students.
e Interact with the patient and lor ask some questions to obtain information.
• Allow the patient to verbalize and express.
• Continue with the planned teaching.
• Make and demonstrate the observations to be made by the students.
• Make the patient comfortable in the bed once the students have madeclinical assessment.
• Hold meeting with the students in a nearby room after the bedside clinic,to discuss the aspects that could not be discussed in front of the patient. Thisperiod is also utilized to evaluate the student in terms of their ability to meetthe objectives.
,.4.2.5 Nursing roundNursing round is the purposeful visit of the nursing team along with the faculty ornursing expert to each patient or selected patients with a view to guide thestudents in obtaining the clinical skills. It can be used to provide information orinstructions to the staff or students. Problem solving rounds help the studentnurses or nursing staff to learn conducting initial interviews, making assessmentof patient's needs and identifying nursing care problems.
Purposes of Nursing Rounds
• To demonstrate important aspects of nursing care.
/I

. ,
• Clarify terminology studied in the class. Conducting ClinicalTeaching
• To compare patient's reaction to disease and study the disease conditions.
• Encourage discussion among students regarding different patients admitted inthe unit.
'..• Helps in assessing the students knowledge and skills about the patient in the
unit
Requisites for conducting Nursing Rounds
Before conducting Nursing Rounds you should-
• Determine students' previous clinical experience to avoid repetition and toadd to earlier experience.
• Keep in mind the probable value and availability of clinical material.
• If some demonstration is done, it should not have a deleterious effect on thepatient.
• Explain the plan to patient and make the patient feel important.
Conducting Nursing Rounds
• Patients are selected with nursing problems to reinforce their theoreticalknowledge.
• Introduce the patient to the group.
• The group observes the sign and symptoms and the behaviour of the patient,at the bedside and makes proper comments. The faculty or the group leadermakes necessary correction in the students remarks or supplements theinformation and gives a direction to the students learning in that particularlearning situation.
• The group observes the equipments and articles under use.
• The students return to the classroom to discuss the nursing diagnoses andrequired nursing care for patients.
• Record the nursing rounds in the ward teaching records with a summary ofnursing care points stressed.
4.2.6 Clinical ConferencesClinical conferences are organized for small group of 6 to 10 students on aparticular topic with different patients having the same problem or on the nursingcare of a patient whose problems are illustrative or different from those usuallyencountered. The students should be familiar with the patients being discussed.The conference can be organized in the ward or in the conference room. Thepermission should be taken from the patient as well as the respective in-charges.The content of the conference will depend on the objectives and the students'level of learning. The participants in the conference should use problem solvingapproach. They should discuss "why, what, and how" of the problem rather thanjust listing the facts or details.
63
/ I
, ,
Nursing InterventionModalities
"
,
64
Purposes of clinical conference
• Group thinking and discussion evokes interest and appreciation.
• Better learning and understanding of the disease and different responses ofthe patients to same health problem can be analysed.
Requisites for clinical conference
For conducting clinical conference you should keep certain things in mind-
• Take the permission from the patient and the ward in-charge.
• Consider the mental and physical comfort and the welfare of the patient.
• The patient should be escorted to the conference room and way back to thebedside.
• There should be informal, permissive atmosphere to encourage questioningfrom the students
Techniques of Conducting clinical conference
• Introduce the patients to the group
• Present Selective aspects of the patient care in the conference
• Discuss the detailed aspects of the selected patient when the patient is sentback to bedside.
Help/direct the students about the specific observations to be made beforethe patient arrives in conferences room. This will enable the student to learnmaximum in the limited time available. The points can then be stressed orfindingshighlighted.
4.2.7 Individual Conference
•
The individual conference is sometimes described as a 'conversation with a purpose',or more simply, as an interview. The two terms 'interview' and 'conference' areused interchangeably. The teacher may introduce the student to new field andstrive to motivate her in the acquisition.
Purposes of Individual Conference
• Provides excellent opportunity for teaching and guidance
• Problems related to individual student can be discussed and resolved
r• Helps to clarify her queries
Requisites for Conducting Individual Conference
For conducting Individual Conference you should-
• Establish good rapport with the students.
• Allow himlher to talk freely.
• Do not show any prejudice, emotional reactions or bias.
/

• Provide sufficient time and be a good listener
• Only specific issues should be discussed.
Conducting Individual conference
• Make the student comfortable
Conducting ClinicalTeaching
• Give sufficient time to verbalize his/her difficulties
• Provide solution according to his/her capabilities.
i) Write the requisites of a good demonstration .
rheck Your Progress 1
..
4.3 PROFORMA FOR CLINICAL TEACHINGProforma can be prepared to suit the specific requirement of the clinical teachingstrategy. It may be prepared for planning, conducting or evaluating the clinicalteaching. Some of these are discussed here.
'.~ Lesson plan
Lesson plan is a blue print of the teaching activity that you will be carrying outwhile teaching. It is the title to the statement of achievements to be realized andthe specific means by which these will be attained. It helps you to plan theteaching in terms of the adequacy, accuracy and relevance of the content. Thelesson plan should be updated timely to incorporate new developments.
Sample Format of Lesson Plan
Identification data For Example
Medical Surgical nursing
Cardiac nursing
Clinical management of a patient with rheumaticheart diseases (RHD)
Subject
Unit
Topic
Group
Date of clinical teaching
Diploma in Critical Care nursing
02/02/10
Duration and time 30 min, 11.30 am
ward 22Venue
AV Aids clinical setting
65
// I
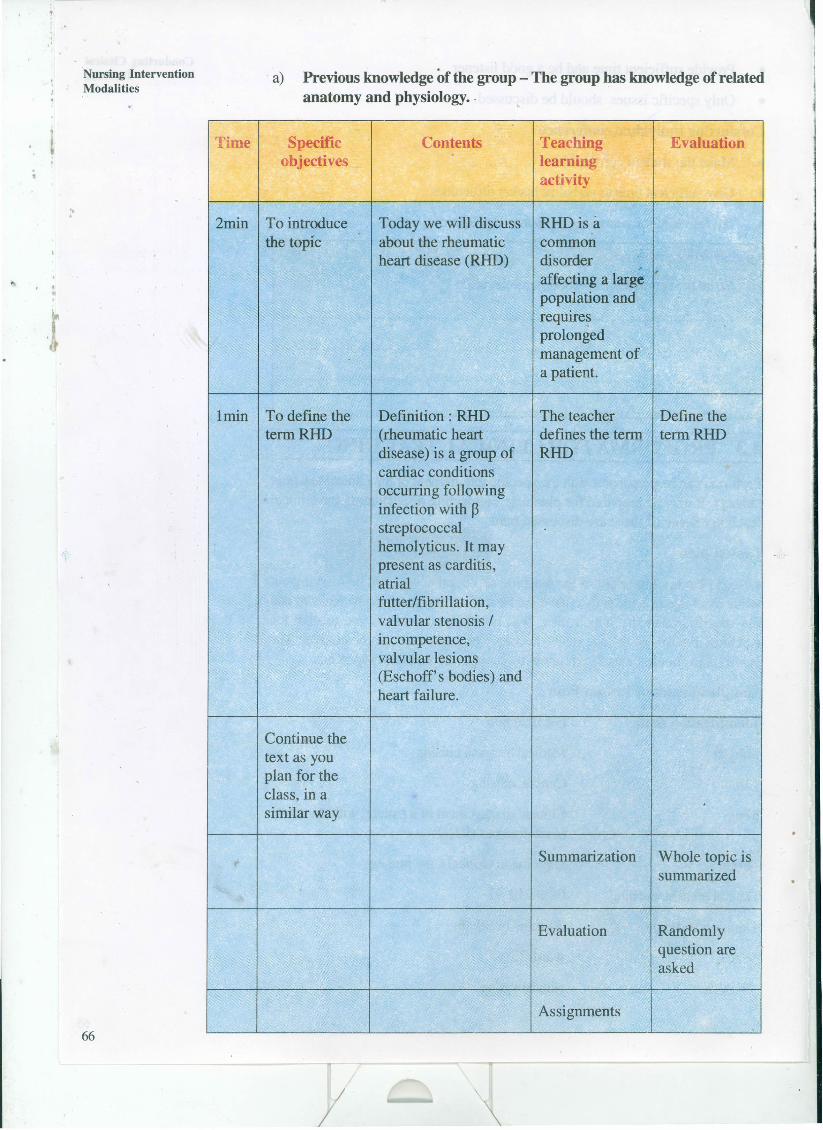
..
Nursing InterventionModalities
".
66
a) Previous knowledge of the group - The group has knowledge of relatedanatomy and physiology. -
Time Specific Contents Teaching Evaluationobjectives
.learningactivity
2min To introduce Today we will discuss RHD is athe topic about the rheumatic common
heart disease (RHD) disorder ,affecting a largepopulation andrequiresprolongedmanagement ofa patient.
lmin To define the Definition: RHD The teacher Define thetermRHD (rheumatic heart defines the term termRHD
disease) is a group of RHDcardiac conditions
I occurring followinginfection with ~streptococcalhemolyticus. It maypresent as carditis,atrialfutter/fibrillation,valvular stenosis /incompetence,valvular lesions(Eschoff's bodies) andheart failure.
Continue thetext as youplan for theclass, in asimilar way
Summarization Whole topic issummarized
Evaluation Randomlyquestion areasked
Assignments

Various proforma can be developed for evaluating student activities in aclinical situation. Some of the examples are as follows:
Rating Scale for evaluating clinical teaching
Conducting ClinicalTeaching
'..
S. No. Behaviour Scores5 4 3 2 1
1 Introduces the patient2 Ensures patient comfort3 Understanding about the case4 Organization of the subject matter5 The clinical skill of observation and
assessment6 Adequacy and relevance of the
matter discussed7 Presentation! communication skills8 Ensures proper viewing by the
,
Group/Group involvement9 Ensures patient's comfort after the
clinical teaching10 .Clarifies doubts of the students
during post clinic sessionTotal score
Checklist for evaluating the return demonstration of surgical dressing.
S.No. Behaviours /Activity YeslNo Remarks1 Explains procedure to the patient2 Collects, necessary equipment and
arranges equipment for convenient use3 Prepares patient & Environment4 Wash hands follows principles of asepsis5 Observes condition of wound ,6 Clean the wound7 Applies dressing8 Replaces equipment after use9 Makes patient comfortable10 Documents findings
Evidences continuity amongpresenters'---+-"-Makes provision for discussions byclass members
3 5
Rating scale for evaluating conduction of nursing conference
1Criteria 1 4S.No. 2
Organizes presentation in clearlogical manner
2 Communicates ideas clearly3
r .4
5 Responds to questions in aknowledgeable manner
6 Shows originality in thepresentation
Total score
II
Nursing InterventionModalities
",
I •
68
4.4 LET US SUM'UPIn this practical you have learnt about various clinical teaching methods and theirsignificance in teaching nursing subjects along with considerations to be madewhile conducting clinicalteaching.Efforts put in conducting clinicalteaching sessionsare very fruitful in achieving expected outcomes of the students in clinical setting.The students are able to develop knowledge, skill and attitude through clinicalteaching methods. Based on the principles of developing evaluation Proforma,more Proformas can be developed according to the need of the situation.
4.5 ANSWERS TO CHECKYOUR PROGRESSCheck Your Progress 1
i) Requisites for a good demonstration
• The demonstrator should be well versed with the procedure and hascompetence of the clinical skills.
• The articles should be arranged and tested before, for the good workingcondition.
• The students should be given knowledge about the topic/procedure or anyspecial apparatus to be used, in advance to save time and avoid distraction.A mimeographed directions can be given before itself.
.• The patient should be informed about the purpose of the demonstration andpresence of the students. His consent should be taken and comfort takencare of.
• The students should have a good view of action
• The steps should accompany the verbal comments and explanation of thestep with the rationale wherever necessary.
• Discussion period should always follow the demonstration for clarification,reemphasizing and summarization.
• Arrange for supervised return demonstration for the students as soon aspossible for best retaining.
4.6 ACTMTIES
,.• Select any topic of your choice for conducting a demonstration for newly
appointed staff in critical care unit.
• Prepare a plan of activities/lesson plan/clinical proforma.
• Conduct a bedside clinic on a critical care patient for the students ofDiploma in critical care nursing programme. Follow the steps given in practicalmanual.
/

PRACTICAL 5 PREPARING ACLINICALROTATION PLAN
Structure"
5.0 Introduction
5.1 Objectives
5.2 Definition and Purposes of Rotation Plan
• 5.3 Factors Affecting Planning of a Clinical Rotation Plan/
5.4 Principles of Planning Clinical Rotation
5.5 Planning a Clinical Rotation
5.6 Sample Rotation Plan
5.7 Let Us Sum Up
5.8 Answer to Check Your Progress
5.9 Activities
5.0 INTRODUCTIONIn practical 4 of this block you have learnt about the various clinical teachingmethods and use of various proformas in clinical teaching setting. Now in this unityou will learn about the preparation of clinical rotation plan and its various aspects.
A student nurse needs to be exposed to a variety of clinical situations in order tomeet her educational objectives. Experience of various specialities is an integralpart of learning wide variety of skills in nursing.While pursuing the basic trainingprograrnme/s you must have been posted for clinical experience in medical surgicalwards, ICU/CCU, paediatric ward, Operation theatre (O'I'), gynecology wardsetc. in different years of your programme. In order to provide adequate, equaland uniform curriculum based clinical experience to all the learners each block ofclinical experience should be carefully planned keeping the objectives in mind. Forthis reason, rotation plans are prepared to guide placement of students for clinicalexperience. In this practical you will learn about clinical rotation plan and howto make a good rotation plan.
5.1 OBJECTIVESAfter completing this practical, you will be able to:
• list the points to be kept in mind while preparing clinical rotation of students;
• plan a clinical rotation of a given group of students effectively; and
• prepare a clinical rotation plan of assigned nursing students.69
/
Nursing InterventionModalities
",
,r!
70
5.2 DEFINITION AND PURPOSES OF ROTATIONPLAN
Rotation refers to regular, successive, and/or recurrent posting of different groupsof nursing students of different c1asses in specified clinical area.
Rotation Plan
His an overall plan of rotation of all students in an educational institution indicatingthe placement of students belonging to various groups of classes in clinical as wellas community nursing fields denoting the duration of such placement.
Types of rotation Plan are:
Master Rotation Plan
It provides placement of other academic schedules like theory blocks, examinationand vacation period, we call it master rotation plan. Master rotation plan givesbroad details of sequence of teaching learning experiences in terms of class roomteaching, clinical areas i.e., medical surgical, Operational Theatre (OT), Paediatric,psychiatric, gynecology, obstetric nursing units, community fields and other academiccalendar events that will follow in a given year of a course programme. RotationPlan for each year can be prepared separately and then exhibited on a single chartfor coordination.
Internal Rotation Plan
The broader areas marked in master rotation plan need further divisions andplanning by the subject teacher inthe form of internal rotation plan to meet theset subject objectives. Internal rotation plan provides information about placementof students in specific departments or clinical areas r~quired in a subject, forexample, master rotation plan can show the period of midwifery posting. But aninternal rotation plan will provide further details of placement in Antenatal Clinic(ANC), labour room, Post natal ward, Operational Theatre (OT), etc.
Purposes of Rotation Plan
• Keep all concerned people informed about the placement of students invarious clinical areas so that coordination is more effective.
• Help in any modifications required in the plan, owing to certain eventualitieswell in time in collaboration with concerned staff (teachers).
,.• Prevent omission, repetition or overlapping of clinical experiences.
• Properly planned rotation plan supplements classroom teaching by systematicexposure to various clinical areas.
• Evaluation of programme is more effective.
• Help in Nursing manpower planning, keeping in mind the number of studentsavailable in each clinical area for their learning experiences.
I

5.3 FACTORS AFFECTING PLANNING OF ACLINICAL ROTATIONPLAN
Preparing a ClinicalRotation Plan
Objectives of the course
"
• The areas of posting of the students will depend upon the course objectives.Critical Care Nursing programme may require placement of students in medicalsurgical and various speciality units. whereas speciaility courses offeringspecialization in a particular stream may require more focused placements inthe speciality area. For example, Students of Diploma in Critical Care Nursingwards may require rotation in cardiology wards, CVTS wards, CCU, Cathlab, cardiac operation theatre intensive care units and critical care units ofdifferent specialities, cardiac out patient department (OPD), Cardiac clinics,pacemaker clinic, cardiac diagnostics and emergency wards.
• Number of students in each class: Since all the students require to beplaced for equal duration in different areas according to Indian NursingCouncil (lNC) guidelines, it is important to decide upon the group, size andnumber of subgroups of students so that all students are exposed to variousspeciality areas equally.
• Number of departments/agencies/areas of experience/ hospitals usedfor clinical posting will decide upon the size of the group and the number ofsubgroups of students.
• Presence of other students of the programmes in the same clinical field.If the clinical field has other students we can not post many students as theymay not get adequate learning situation/experience and it may causeunnecessary confusion and overcrowding.
• Size of the department! agency where posting of students is planned, ifthe hospital is big enough we can make more sub groups to post them atdifferent areas under the same unit! department.
• The agency/ hospital authority concerns and consideration may affect theplanning of clinical rotation.
• Duration of experience in each area as specified by Indian nursingcouncil (INC) will necessitate its incorporation in planning the rotation.
• Indian Nursing Council (INC) specifications regarding description of the -clinical area and duration of posting in the said clinical area will define the
--areato be selected accordingly.
Sequence of classroom instructio~s and its rotation to the clinical experienceareas to facilitate optimum learning.
•
• Vacations, preparatory leave and examination schedule will affect theplanning of the master rotation plan. The plan has to accommodate theseevents appropriately as per the Institute's. calendar events.
71
I

,.
Nursing InterventionModalities 5.4 PRINCIPLES OF PLANNING CLINICAL
ROTATION
".
• Clinical experience must be planned in advance for each student.
• Each student must rotate through each block.
• For planning clinical experience, syllabus of Indian,Nursing Council (INC)should be followed as a guideline for fulfilling minimum requirements.
• Each block should be of same duration. For example, in a "4 week block",rotate students in every week and each student should have been in eachblock for equal amount of time.
• Block may consist of 2 or 3 areas of clinical experience which have beenfitted to make up requisite length of block.
• Student should enter and leave the block as scheduled. For efficient Rotation,dates must be specified or fixed.
• Each block of experience shall be subdivided to rotate students for relatedexperience within the block.
• Simple areas and those considered fundamentals should proceed the morecomplicated ones. The student should be introduced to the clinical areasgradually so that she becomes adjusted to the clinical environment.
• Assignments of students must meet minimum requirements.
• Assignments should not be broken by the service needs of the hospital,except in dire emergencies.
• Rotation must be planned for the complete course and full academic year.
• Continuity of experience is essential. Clinical experience should not be givenin broken blocks.
• All the clinical instructors must be thorough with the Master rotation plan.
• Clinical posting should correlate with the theory in the class.
5.6 PLANNING A CLINICAL ROTATION• Look for the Indian Nursing Council (INC) specifications given in the Indian
Nursing Council (INC) syllabus ( or as per the Institute's syllabus).
Calculate the number of weeks required in a given clinical area. This willdepend upon the prescribed supervised practical hours in the syllabus andnumber of hours per day or number of hours per week which, the Instituteis able to provide.
Example:
•
The prescribed supervised practical hours for B.Sc. Nursing programme, as perINC are as follows:
72
/ \

,
Table 1: Distribution of supervised practical hours for Basic B.Sc. Nursing Preparing a ClinicalRotation Plan
'.
Year I year llyear IIIyear IV year Internship30 hrs per 30 hrs per 30 hrs per 30 hrs per 8 hrs per day
week week week week @.48 hrs per wk
Clinical areas Hrs Wks Hrs Wks Hrs Wks Hrs Wks Hrs Wks
Nursing 450 15foundationMed-surg 720 26 430 9nursing ICommunity 135 4.5health nursing IMed-surg 270 9nursing ITChild health 270 9 145 3nursmgMental health 270 9 95 2nursmgMidwifery and 180 6 180 6 240 5ObstetricalnursingCommunity 135 4.5 195 4health nursingIIResearch 45 1projectTotal hours 450 855 990 315 1150 24
This table clearly indicates the required number of weeks for each clinical areaand the placement of the area in the specified year of the programme.
1. What you have to do now, is to plan the rotation of students year wise.Keep the principles of clinical rotation planning in mind and prepare theblocks accordingly.
2. Start from the date of commencement of the academic session.
3. It is always good if you have initial teaching block of a small period (ifpermissible by the time requirement) in the beginning of the rotation plan,where the students are exposed to the theory classes related to the plannedclinical areas.
4. Specify the dates of the clinical areas. Rotation plan should be made weekwise for the complete academic year.
5. Plan for each year of the programme (i.e., I to IV year) keeping in mindthe limitations of the Institute in terms of availability of the clinical areas andtransport required.
6. Once the clinical rotation of each year is planned and prepared it then canbe depicted on the same graphic chart.
I
73
Nursing InterventionModalities
"
74
Check Your Progress 1
i) Write any four important principles in planning a clinical rotation for a givencourse,
••••• f ••••••••••• ~ ••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••• " •• '" ••
ii) Write the difference between a master rotation plan and an internal rotationplan?
5.6 SAMPLEROTATIONPLANMaster Rotation Plan
We have presented a sample Master rotation plan of B.Sc. Hons. Nursingprogramme for your reference so that you will be able to prepare thesame (See Page No. 75).
r
/I

Year
Wks ???
•
Sample Rotation Plan Name of the College of Nursing
Master Rotation Plan
July
B.Sc. Hons. Nursing (session :2010-2014)
August September October November December January February June
~ '" \ First year\
Teaching Block Nursing Foundation WI Nursing Foundation Teaching Block P
IR E~
NE X
TP A
Second year I Teaching I Medical surgical l~ommunny I IVI~UE Medical surgical T. A M
Block Nursing I 'He~Jth 1)59 surg R Nursing I Block R I
._,~-:--~~ I~~~' n~n!A N
T A
T. Med surg I psychiatric nursing I Paed)atric nurs.i,n~ •• ~~:~_ IVI~U~U'~"V'~"'~ "\Teaching
0 T
Third year I Block Nursing 11 \~ C·~"~\{' . Block
R I
_." r- A ~~:~~'f', 'r." ~.~ y 0
..",»:-. ..,L N
E S
Community r''''~t!~''.(' - f ,-' y. 4i"'I.~~"""""~~' .,
ATeaching I~~r' ·f1'f/_~'·,: :;,.\ :,;~ ,r • N ~~-f:.'~_ :.-.:.j~', .: .t{:(' /1~'( .~.. t~'l~~l;tl~-~-;
Fourth year J: .••.••••«~ ••• ~ ,]Il'~-<_ Health nsg 1I"'~"',IIf' ',,' ' •. ';:-~ :~ ~ L J::!"" ~;Ji)"f .,.r~'ffii~l~'(:~~Block
Legends (key)
oWinter Vacation
-JVi
DTeaching block
DNsgFoundation.. , Examinations
"tl'1r!>'g~ s·Q(/Q
~~= ::"tl e.-I'>~ a
MidwiferyInternship
Med SurgNsg
ComHNlg
I1 ComHNsgIo Psychiatric Nsg
~ PeadNsglL..!!.-J
oo
___ Summer vacationo Preparatory Leave

. ,
Nursing InterventionModalities
Sample Internal Rotation PlanB.Se. Hons Nursing Il year students
at xxx Hospital from 01/03/2010 to 02/04/2010
Subject: Medical Surgical Nursing I
",
Groups 01103/10- 08/03110- 15/03/10- 22/03/10- 29/03/10- 05/04110-
07/03/10 14/03110 21/03110 28/03110 04/04110 12/04/10
Group A Cardiology Cardiac Diagnostics CCU CTVS CTVS
Ward Cath lab ward Ward.
Group B CTVS Cardiology Cardiac Diagnostics CCU CTVS
Ward \Vard Cath lab Ward
Group C CTVS CTVS Cardiology Cardiac Diagnostics CCUWard Ward Ward Cath lab
Group P CCU CTVS CTVS Cardiology Cardiac DiagnosticsWard Ward Ward Cath lab
GroupE Diagnostics CCU CTVS CTVS Cardiology CardiacWard Ward \Vard Cath lab
Group F Cardiac Diagnostics CCU CTVS CTVS Cardiology
Cath lab Ward Ward Ward
Group A* Croup B Group C Group D GrmpE oup F
1 1 1 1 1 12 2 2 2 2 23 3 3
.3 3 3
4 4 4 4 4 45 5 5 5 5 56 6 6 6 6 6
*Six students in each group
Time: From 7.30 am to 1.00 pm
On all working days, except Saturday and Sunday.
Signature of the teacher76
I/

,.
Preparing a ClinicalRotation Plan5.7 LETUSSUMUP
Iri this unit we have learnt about master rotation plan clinical rotation plan, factorsaffecting clinical rotation plan and principles to be kept in mind while planning andpreparing a rotation plan. Clinical rotation is always guided by INC specifications.The minimum requirement for supervised practical hours, as prescribed by INe,has to be met in the clinical rotation of students. A well planned rotation contributes
" towards supplementation of the knowledge, optimum utilization of the learningsituations and smooth completion of programme, It provides better coordinationamongst the faculty members and hospital staff.
.. 5.8 ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
i) Each block should be of same duration
• Simple areas and those considered fundamentals should proceed the morecomplicated ones
• Assignments should not be broken by the service needs of the hospital,except in great emergencies
• Continuity of experience is essential. Clinical experience should not be givenin broken blocks.
ii) Master rotation plan gives broad details of sequence of teaching learningexperiences in terms of class room teaching, clinical areas and other academiccalendar events like examinations and vacation that will follow in a given yearand a given course programme whereas Internal rotation plan providesinformation about placement of students in specific department or clinicalarea required in a subject, for example, master rotation plan can show theperiod of midwifery posting. But an internal rotation plan will further givedetails of placement in ANC, labour room, Post natal ward, OT, etc.
5.9 ACTIVITIES• Prepare clinical rotation for B.Sc. Nursing students (a batch of 50) for the
Medical Surgical Nursing ICU. Follow INC guidelines for reference.
• Prepare a master rotation plan for a batch of 40 diploma in critical carenursing students as per syllabi prescribed by IGNOU for this programme.
77
/

PRACTICAL 6 PATIENT CAREDOCUMENTATION,RECORDS ANDREPORTS
".Structure
6.0 Introduction
6..1 Objectives
6.2 Types of Patient Records6.2.1 Source oriented records6.2.2 Problem oriented records
6.3 Documentation
6.4 Forms of Documenting Systems6.4.1 Traditional narrative charting6.4.2 SOAP charting6.4.3 FOCUS charting6.4.4 PIE charting
6.4.5 Charting-by-exception6.4.6 Computerized charting
6.5 Types of Clinical Records
6.6 Sample Format of Common Clinical Charts
6.7 Let Us Sum Up
6.8 Answers to Check Your Progress
6.9 Activities
6.0 INTRODUCTIONEffective communication among health professionals is vital to the quality of patientcare. The communication occurs through discussion, records and reports and itsappropriate documentation. Nurses often provide quality nursing care but fail todocument it adequately and appropriately so that it can be used as a tool forassessment of the quality or as data for related clinical research. This practical will
,. deal with types of patient records and its adequate and appropriate documentationin terms of forms and formats of documenting systems.
6.1 OBJECTIVES
78
After completing this practical, you will be able to:
• explain various forms of documentation systems used in clinical practice;
• describe documentation by providing complete, concise, relevant and factualinformation;
//

• list various clinical records used for patient care;
• prepare clinical records depending upon the patient'sdisease; and
• elaborate upon the formats of commonly used clinical records.
6.2 TYPESOFPATIENTRECORDS" Patient record is information about the patients in writing or any other permanent
form; documents etc. which reveals his past, present and any remarkable events/history along with treatment modalities and investigations carried out in the hospitalsetting.
There are two types of records;
• Sources oriented records
"
o Problem oriented records.
6.2.1 Sources oriented recordsSource oriented records and its proper documentation provides evidence thatnursing practice standards related to the nursing process have been maintainedduring care of patient. Assessment, diagnosis interventions, outcome and evaluationof the patients response to care are critical part of the patients records, which areof great importance in providing day to day care and for future reference oftreating the patient.
6.2.2 Problem oriented recordsThey focus on specific patient's problems and have five components.
• Database: Subjective and objective data about the patient forms the initialplan of care. (for subjective/objective data, refer unit- 1 related to nursingcare plan).
• Problem list: It is a numbered list of the patient's current problems maintainedaccording to the date and time of identification of the problem. When aproblem is resolved, the date and time is noted or documented.
• Initial plan: This includes expected outcomes and plans for further care ofthe patient.
• Progress notes: You must write a note for each current problem every 24hours or when the patient's condition changes.
Discharge Summary
It covers each problem on the list and notes whether it was resolved. Discuss anyunresolved problem.
Example Problem Oriented Record
Patient received from operation theatre (OT) and has following problems:
Problem -1 nausea vomiting,
Problem-2 pain
(S/he may have more problems. Only two are discussed here)
I
Patient Care Documentation,Records and Reports
79

Nursing InterventionModalities
The patient record as per SOPIER can be written as per following:
11/02/2001 3 PM
".
Problem 1: Nausea related to anaesthetic use
S: Patient states "I feel nauseated"
0: Vomited100 m1of clear fluid at 2.30 pm
A: Patient is nauseated.
P: monitor nausea and give antiemetic drugs as advised
I: informed doctor at 3pm and inj perinorm 2ml ilv given at 3.10 pm
E: Patient states she is no longer nauseated at 3.40 pm
R: Antiemetic not required
Problem 2: Acute pain related to surgical incision
S: patient states "it is hurting"
0: Patient reports pain by tick marking score of 5 on a 10 point rating scale
A: Patient is in pain and needs pain medication
P: Give pain medication as prescribed
I: inj morphine 2mg ilv given at 3.30 pm
E: patient pain is relieved and states pain by marking score 1( as 1/10) on ratingscale
R: Pain medication not required
"
I •
6.3 DOCUMENTATION
80
Document as you know is a piece of paper giving information or evidence whichcould be in the form of written records and or reports for patient care in thehospital. Each institution has its own documentation policies. Policy generallyindicates the type of information that is recorded on each form by the staffresponsible for charting and the frequency of making entries in the records.Consistency in charting is important for patient recovery and legal purposes.
A written report refers to written or a computer based communication intendedto convey information to others. A record is written or is computer based document,and the process of making an entry on a patient's record is called, recording!charting! or documenting.
A clinical record, also called a chart or a case sheet, is a formal, legal documentthat provides evidence of care provided to the patient. Record keeping should betimely, accurate, confidential and patient specific.
The value of clinical record is both scientific and legal. It serves as an evidencethat patient care has been intelligently and competently given. It provides legalprotection to the nurse, health team and the hospital. The data can be used forfuture comparison of interventions or patient's condition. It can also be used asdata for clinical research or auditing.
Purposes of Documentation are as follows:
• Communication amongst the health team member
//

• Planning patient care
• Auditing
• Research
• Education
• Legal protection to the care provider and hospital
• Nurses satisfaction"
• Health care analysis for future reference.
Many institutions have their own documentation systems to record the nursinginterventions,evaluations and patient's response. There are various forms of chartingsystems as mentioned in forms of documenting system. These are discussed in
~ following section 6.4.
,. 6.4 FORMS OF DOCUMENTING SYSTEMSA variety of protocols or charts are used to record information in the patient'srecord, these are listed below :
• Traditional narrative charting,
• Subjective data, objective data,• Assessment and planning (SOAP charting),
• Focus Charting,
• PIE Charting,• Charting by exception and
• Computerized charting.Now we will discuss each one of these briefly:
6.4.1 Traditional narrative chartingsIt is a straight forward chronological account of the patient's status, nursinginterventions performed and the patient's response to interventions. Documentationis usually included in the progress notes and flow sheets. Refer practical 1 forformat of progress reports /flow charts.Guidelines in traditional narrative charting:• Document exactly what you hear, observe, inspect, do or teach.
• Document response of your patient to care, treatment, medication and hisprogress towards the desired outcome.
• Include notification to the doctor for changes, communication with the doctoror other health team members, new orders that are to be followed and thepatient's response. As shown in Example 1.
• Document the condition and progress of patients. You can use the nursingcare plan as a guide.
• Document chronologically and be specific in documenting.• Record data and exact time of documentation along with your signatures.
• Avoid block charting i.e., charting at a single block regarding the interventionscarried out at different time without mentioning the time of execution and
y
Patient Care Documentation,Records and Reports
81
"
Nursing InterventionModalities
"
82
--
response of the patient to each. Correct method is shown in Example 2.
• Never chart nursing activities before they have been performed.
• Making early entries can cause legal problems. Especially if the patient'scondition suddenly changes.
• Follow agency 1hospital policy for the interval between entries. Frequentcharting indicates that the patient has been observed and attended to atreasonable periods of time.
• Draw a line through a mistake rather than scribing the original words.
• Document information clearly and accurately without any subjectiveinterpretation.
Example 1 Importance of specific documentation (Notifying the Doctor)
Consider the nurses role in a patient receiving epidural analgesia. Epidural analgesiais beneficial in pain relief, requiring lesser sedation and allowing for deep breathingexercises. It is also useful in chronic pain. Adverse effects of epidural analgesiainclude sedation, nausea, urinary retention, postural hypotension, itching, respiratorydepression, headache, back-sore, leg weakness, numbness and respiratorydepression. The nurse must monitor the patient for these reactions and notify thedoctor, if they occur.
Charting for such a patient should be as follows:
22/02110 10 am
Patient received from recovery unit with epidural catheter in place. Dressingcovering site is clean, dry and intact. Patient is receiving bupivocaine 0.125% andfentanyl 5 mcg/ml in 250 ml of Normal Satin at 2 mlIhour RR-20/rnin -deep,alert, 02 sat by oximetry = 99% at °22Llmin by cannula. BP 120/80, Pulse 72.Patient reports pain as 2/10 on the pain scale. No nausea, itching, leg weakness,back sore. Patient voided 300ml of pale yellow urine. Bladder scan shows noresidual urine after void. Told patient to report pain greater than 3/10, inability tovoid, numbness oflegs. Epidural infusion label applied to epidural catheter, infusionpump, and tubing.
Signature of Nurse
Suman staff nurse
A patient receiving epidural analgesia is at risk of developing epidural hematomaleading to paralysis of lower limbs, it is your duty to look for the suggestivesymptoms and document the intervention of assessing and reporting them if present.It will include assessing diffuse back pain, paresthesia, bladder and boweldysfunction, inability to move legs. This will prevent the patient from developingparalysis oflower extremities. An example of documentation in such a case wouldbe something like this:
22/02/10 9.15 pm
Called by the patient at 9 pm for lower back discomfort and numbness in rightleg. When asked to point to pain, patient moved hand around general region oflower back. Pedal pulses palpable with brisk capillary refill. Right foot weakerthan Left foot on dorsiflexion and planterflexion against resistance. Unable to
" raise right foot off bed. Patient alert and oriented to time place and person. Nodifficulty in urinating. Voided 350 ml on bedpan at 8.30 pm. Patient told to
/I
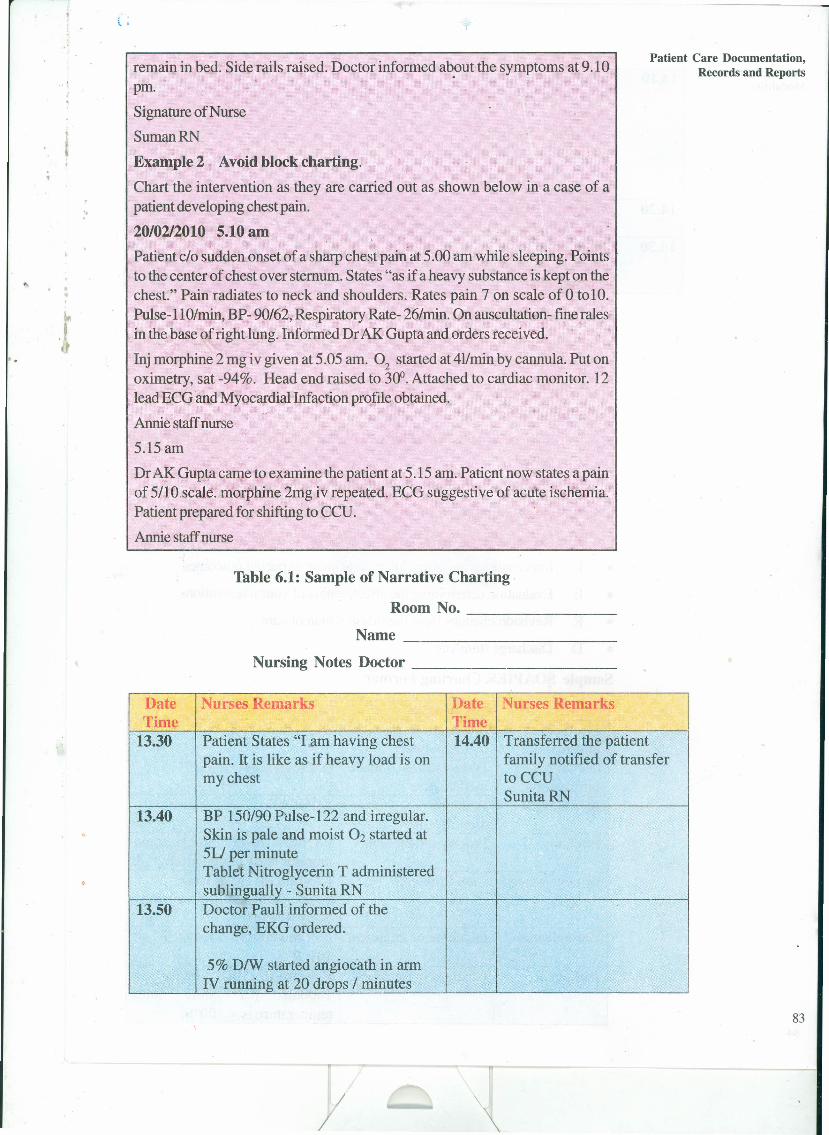
" ,J.
. .
\ .
",
Patient Care Documentation,Records and Reportsremain in bed. Side rails raised. Doctor informed ab,out the symptoms at 9.10
pm.
Signature of Nurse
SumanRN
Example 2 Avoid block charting.
Chart the intervention as they are carried out as shown below in a case of apatient developing chest pain.
20/02/2010 5.10 amPatient clo sudden onset of a sharp chest pain at 5.00 am while sleeping. Pointsto the center of chest over sternum. States "as if a heavy substance is kept on thechest." Pain radiates to neck and shoulders. Rates pain 7 on scale of 0 tolO.Pulse-ll0/min, BP- 90/62, Respiratory Rate- 26/min. On auscultation- fine ralesin the base of right lung. Informed Dr AK Gupta and orders received.
Inj morphine 2 mg iv given at 5.05 am. O2 started at 411minby cannula. Put onoximetry, sat -94%. Head end raised to 300. Attached to cardiac monitor. 12lead ECG and Myocardial Infaction profile obtained.
Annie staffnurse
5.15 am
Dr AK Gupta came to examine the patient at 5.15 am. Patient now states a painof 5/1O,scale. morphine 2mg iv repeated. ECG suggestive of acute ischemia.Patient prepared for shifting to CCU.Annie staffnurse
Table 6.1: Sample of Narrative Charting
Room No. _
Name _
Nursing Notes Doctor _
Date Nurses Remarks Date Nurses RemarksTime Time
13.30 Patient States "I am having chest 14.40 Transferred the patientpain. It is like as if heavy load is on family notified of transfermy chest toCCU
Sunita RN13.40 BP 150/90 Pulse-122 and irregular.
Skin is pale and moist O2 started at5U per minuteTablet Nitroglycerin T administeredsublingually - Sunita RN
13.50 Doctor Paull informed of thechange, EKG ordered.
5% DIW started angiocath in armIV running at 20 drops I minutes
83

,.
Nursing InterventionModalities
",
I '
84
14.10 ECG obtained .BP 142/84 Pulse-ll 0 and stillirregularskin pink but moistno relief from nitroglycerinStates "Its still pretty bad"SunitaRN
14.20 Morphine 10 mg administered forchest pain and anxiety Sunita RN . --
14.30 Transferred to'CCU bed, clothingdentures and eye glassesaccompanied
6.4.2 SOAP chartingYou have learnt formats of soapier charting problem oriented records now wewill focus on use of soapier charting :
SOAPIER approach is used to structure progress notes. The composition ofSOAPIER charting includes following; :
• S Subjective data; reason for seeking care or information, as told by thepatient
• 0 Objective data: observable signs and measurable data.
• A Assessment data: formulated as patients problem and nursing diagnosis.
• P Plan short term and long term strategies to solve patients problems,
• I Interventions measures taken to achieve expected outcomes
• E Evaluation determining the effectiveness of your interventions
• R Revision changes from the original plan of care
• D Discharge summary
Sample SOAPIER Charting Format
Letter Explanation Examples of RecordingS = Subjective Information reported S= " I don't feel well"information by the patients0= Objective Observations made O-Temperature 102.4°PInformation by the nurseAe.Analysis Problem A-Fever
identificationP=Plan Proposed treatment P-Offer extra fluids and
monitor body temperatureI=Implemented Care Provided 1-750ml of fluid intake in 8
hours; temperature assessedevery 4 hours
E=Evaluation Outcome of treatment Ee'Temperature reduced to101°F
R=Revision Changes in treatment R-Increase fluid intake to1000ml per shift untiltemperature is < 100°F.
//

6.4.3 FOCUS chartingThis is modified form of SOAP Charting. It uses the word focus than problems,because word problem carries negative connotations. A focus can be patientscurrent or changed behaviour, significant events in the patient' care for makingentries DAR model is used (D= Data, A = Action, R:::::Response)DAR notationtends to reflect steps in nursing process.
;. Sample DAR Charting Format
30/06/2000 D (Data) - Bladder distended 2 finger above pubis. Has not10.15 am urinated for the past 8 hours, since Catheter was removed
A (Action) - Assisted to toilet. Water turned on at faucet.Instructed to press over bladder with hands.R (Response) - Voided 525 ml of clear urine. Signature ofnurse
6.4.4 PIE chartingPIE charting is composed of problem, intervention, evaluation of care providedto patients.
Sample (PIE) Chart
Date Nursing Remarks SignatureTime4/412010 P - Crackles Heard on inspiration in the bases5.50 am' of right and Left Lungs.
I - Incision splinted with pillow. instructed tobreath deeply, open mouth and caught at theend of expiration SunitaLungs clear with coughing RN
Put in sequence as key :
• P- Problems
• I - Intervention
• E- Evaluation
6.4.5 Charting by exception (CBE)In this only significant or abnormal findings in narrative portions of the record aredocumented.
For this, you have to be well versed with the guidelines for nursing assessmentand document only deviations from the standards. Several types of flow sheetsare involved in this type of documentation. Example of nursing care flow sheet onassessment findings is given below:
/I
\
Patient Care Documentation,Records and Reports
85
I
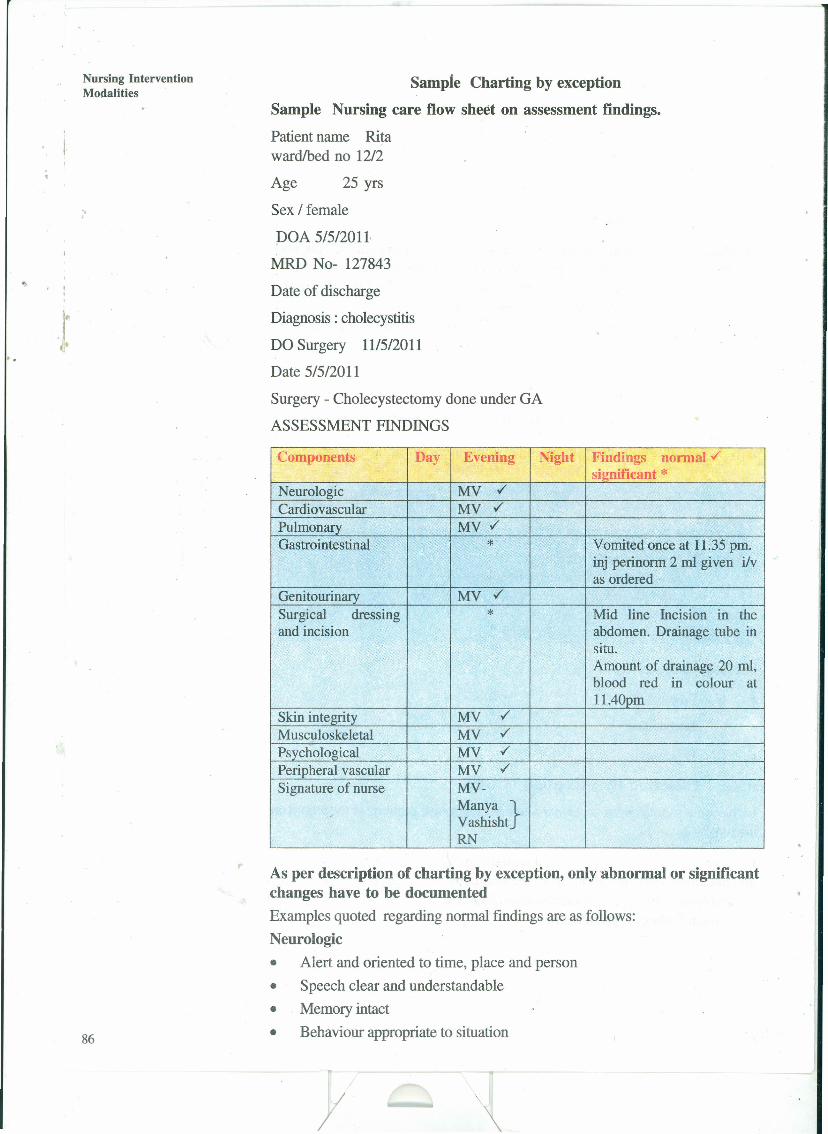
Nursing InterventionModalittes
"
86
Sample Charting by exceptionSample Nursing care flow sheet on assessment findings.Patient name Ritawardlbed no 1212
Age 25 yrs
Sex / female
DOA 5/512011-
MRD No- 127843
Date of discharge
Diagnosis: cholecystitis
DO Surgery 11/512011
Date 5/512011
Surgery - Cholecystectomy done under GA
ASSESSMENT FINDINGS
Components Day Evening Night Findings normal vsignificant *
Neurologic MV ./
Cardiovascular MY ./
Pulmonary MV ./Gastrointestinal * Vomited once at 11.35 pm.
inj perinorm 2 ml given ilvas ordered
Genitourinary MY ./
Surgical--
dressing * Mid line Incision in theand incision abdomen. Drainage tube in
situ.Amount of drainage 20 ml,blood red m colour at11.40pm
Skin integrity MV ./
Musculoskeletal MV ./
Psychological MV ./
Peripheral vascular MV ./
Signature of nurse MV-Manya }VashishtRN
,.As per description of charting by exception, only abnormal or significantchanges have to be documentedExamples quoted regarding normal findings are as follows:Neurologic• Alert and oriented to time, place and person• Speech clear and understandable• Memory intact• Behaviour appropriate to situation
//
• Active range of motion (ROM) in all extremities and symmetric equal strength
• No paresthesiaCardiovascular• Regular apical pulse, 60-80 per minute
• Palpable bilateral peripheral pulses
• No peripheral edema• No calf muscle tenderness• Resting respiration .10-20 per minute, quite and regular
• Clear sputum• Nail beds and mucous membrane pink
Gastrointestinal• Abdomen soft and non distendedo Tolerates normal diet without nausea and vomiting
• No complaints of nausea and vomiting• Bowel movements within one's own normal pattern and consistency
Genitourinary
• No indwelling catheter in use
• Urinates on his own without pain
• Urine clear yellow to amber colour
• Undistended bladder after voiding
Surgical dressing and incision
• Dressing dry and intact• No evidence of redness, increased temperature or tenderness in surrounding
tissues
• Sutures, staples intact• Edges well approximated
• No drainage presentSkin integrity
• Skin colour normal• Skin warm, dry and intact
• Mucous membranes moist
"
Musculoskeletal• ·Normal ROM (Range of motion)
• No swelling or tenderness
• Steady gaitPsychological• Interacts and communicates appropriately
Peripheral vascular• Effected extremity pink, warm and has full range of movement
/I
Patient Care Documentation,Records and Reports
87
Nursing InterventionModalities
• Capillary refill time < 3 seconds
• Peripheral pulses palpable
• Sensation intact without numbness or paresthesia
• No edema
",
..• No pain on passive stretchingNote that, in sample format CBE under 6.4,5, the standard normal findings onassessment are not recorded and only the significant findings that are deviatingfrom normal arerecorded.
, ,6.4.6 Computerized chartingComputerized clinical record systems are being developed to manage the hugevolume of information. Multiple flow sheets are not required in computerizedrecord system. Computers make care planning and documentation relatively easyif one is computer literate. Nowadays most of the hospitals have computerized.Charting system:
Check Your Progress 1i) List the various documentation systems used in patient care documentation.
ii) State the purposes of documentation.
6.5 TYPES OF CLINICAL RECORDS•
These are related to bed side observations and treatment of the patient.
There are various types of records in llse at different clinical settings. These areeither administrative records or patient records. Some of the commonly usedrecords are given below:
Common patient care records
• Admission assessment sheet
• Nursing care plan
• Medicine card! treatment book
• Flowsheets
• Graphic clinical record like temperature pulse respiration charts
• Intake output chart88
/
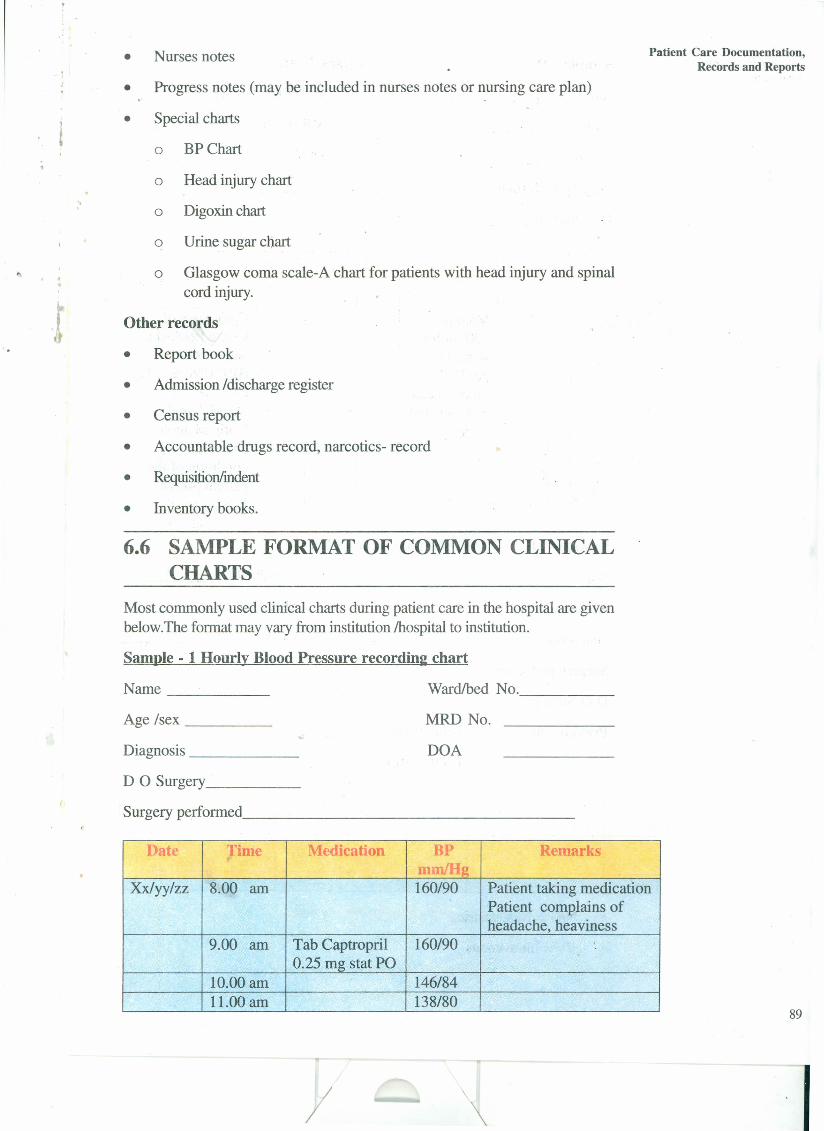
• Nurses notes Patient Care Documentation,Records and Reports
• Progress notes (may be included in nurses notes or nursing care plan)
• Special charts
o BP Chart
"
o Head injury chart
o Digoxin chart
o Urine sugar chart
o Glasgow coma scale-A chart for patients with head injury and spinalcord injury.
Other records
• Report book
• Admission /discharge register
• Census report
• Accountable drugs record, narcotics- record
• Requisition/indent
• Inventory books.
6.6 SAMPLE FORMAT OF COMMON CLINICALCHARTS
Most commonly used clinical charts during patient care in the hospital are givenbelow.The format may vary from institution !hospital to institution.
Sample - 1 Hourly Blood Pressure recordinl: chart
Name _ Ward/bed No. _
Age /sex _ MRD No.
Diagnosis _ DOA
D 0 Surgery _
Surgery performed _
Date :rime Medication BP Remarksf'
Xxlyylzz 8.00 am 160/90 Patient taking medicationPatient complains ofheadache, heaviness
9.00 am Tab Captropril 160/900.25 mg stat PO
10.00 am 146/8411.00 am 138/80
89
y ,I

Nursing InterventionModalities
Sample - 11 Nurses NotesNrone ~ Ward/bed No. _
Age Isex _ MRD No.
Diagnosis _ DOA
"
Surgery performed _
D 0 Surgery _
I •
Date T PR BP Medication Diet urine stool Remarks& I Injection
time11.30 Mannitol Complains of
100 ml IIV severe headachestarted as and vomitingper Dr.'s BP150/90 mm Hgorders, head Pulse.60/minend elevated Dr. Mahapatrato 30° Notified about
change incondition of thepatient SunitaR.N~
Sample - III Intake Output Chart
Name Ward/bed No
Age Isex MRDNo
Diagnosis DOA
Surgery performed
DO Surgery
Previous day's Total Intake
Total Output
Date & Intake OutputTime IIV Oral, N/G Others Urine N/G Drainage Others
Total
* N/G = Nasogastric
* IIV = Intravenous
90
/I
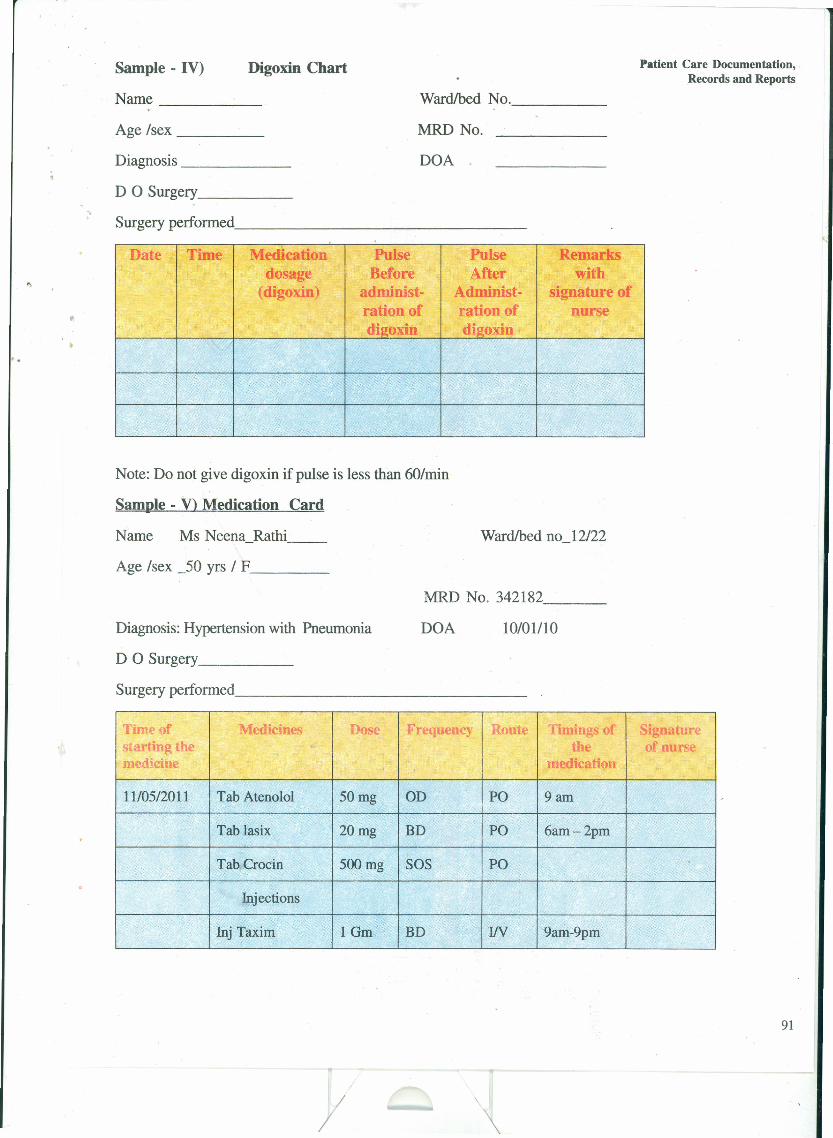
Sample - IV) Digoxin Chart Patient Care Documentation, .Records and Reports
Age Isex _
Wardlbed No. _
MRD No.
Name _
Diagnosis _ DOA .
".D 0 Surgery _
Surgery performed. _
Date, Time Medication Pulse Pulse Remarksdosage Before After with
.' (digoxin) administ- Administ- signature ofration of ration of nursedigoxin digoxin
Note: Do not give digoxin if pulse is less than 60/min
Sample - V) Medication Card
Name Ms Neena_Rathi __ Wardlbed no_12/22
Age Isex _50 yrs 1 F _
MRD No. 342182 _
Diagnosis: Hypertension with Pneumonia DOA 10/01/10
D 0 Surgery _
Surgery performed. _
Time of Medicines OS( requency oute "unings 0 ignaturestarting the the of nursemedicine medication
1110512011 Tab Atenolol 50mg OD PO 9am
Tab lasix 20mg BD PO 6am-2pm
Tab Crocin 500mg SOS POInjections
Inj Taxim IGm BD IfV 9am-9pm
91
y

<,<,
~
\0IV
,
Sample - VI Head Injury ChartName ., _Age Isex _Diagnosis _. _
Surgery performed -----------D 0 Surgery _
Ward/bed No. _MRD No
DOA
Date Time Vitals ENT CSFLeakage Pupil\ary reaction Motor function GCS Remarks and signature of nurse!Bleeding
T P R BP Rt Lt RV LVL RLL LLLL
ll/Ol 6.00 99 90 14. 1001 Patient CSF* No Dilated NS,NR + L .+ t E3 V3M4 Head end elevated to 30 . inj110 AM 78 rnanniroll 00 1111 j(iven.
Placedstrike
"~ .. -"
~ ,.. ~,- , .'-~
• Cerebro Spinal Fluids
• ENT Ear Nose Throat
• GCS .; Glasgow Coma Scale
• CSF - Cerebro Spinal fluid
• Right
• Left
.,
S=ZQ =Q.:;!~ •...::=c-.(JQ~ ...tIl :I
;:;:!~:I..•s·:I
"
if List various patient care records commonly used in clinical practice.
Check Your Progress 2
6.7 LET US SUM UPDocumentation of patient care and maintenance of records and reports is ofutmost importance in a hospital. Documentation is most important form ofcommunication amongst heath care personnel. It provides legal protection to thenurse involved in patient care. The document can be used as data for qualityassessment or for clinical research. In this practical you have learnt about variousdocumentation systems, criteria of good charting and various formats of clinicalrecords specific to patient is diseases condition.
6.8 ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
i) Focus Charting
• Communication among the health team members
• Planning patient care
• Auditing
• Research
• Education
• Legal protection to care provider and hospital
• Nurses satisfaction
• Health care analysis
ii) Traditional narrative charting
• Problem oriented record
• Charting by exception
• Pie charting
• Soap Charting
• Computerized charting
/
Patient Care Documentation,Records and Reports
93:
I

Nursing InterventionModalities
"
,.
94
Check Your Progress 2
Common patient care records:
1. Admission assessment sheet
2. Nursing care plan
3. Medicine card! treatment book
4. Flowsheets .
5. Graphic clinical record like temperature, pulse, respiration chart
6. Intake output chart
7. Nurses notes
8. Progress notes (may be included in nurses notes or nursing care plan)
9. Special charts
a. BP Chart
b. Head injury chart
c. Digoxin chart
d. Urine sugar chart
6.9 ACTIVITIES• Select commonly used clinical records in your medical surgical lCU and
compare them with what you have learned in this practical.
• Select a patient in the CCU of your hospital. Look at the nurses records ofthe patient. Prepare nurses notes and document the care given. Write theprogress notes for the patient over three days.
• Prepare a Glasgow coma scale chart for a patient with head injury.
,.
/

, ,
PRACTICAL 7 DESIGNOFACRITICAL CAREUNIT
".Structure
7.0 Introduction
7.1 .Objectives
7.2 Location of Critical Care Unit
7.3 Determining Bed Strength of a Critical Care Unit
7.4 .Design of Criticai Care Unit7.4.1 Unit Access
7.4.2 Control of Nosocomial Infection7.4.3 Patient Comfort7.4.4 Communications7.4.5 Patient Room Configuration7.4.6 Patient Support Areas
7.4.7 Support Areas for Medical and Paramedical Personnel
7.5 Equipping a Critical Care Area
7.6 Let Us Sum Up
7.7 Answers to Check Your Progress
7.8 Activities
7.0 INTRODUCTIONIn your undergraduate programme you must have visited or worked in a criticalcare unit of the hospital. You may recall that a patient in critical care unit issurrounded by high technological machines, monitors, ventilators etc. All theseequipments are important for the care of patients in critical care unit. Lot ofemphasis is put on planning, organizing and designing of such a unit to meet healthcare needs of critically ill patients. You have to make decisions based on needsand budget of the hospital.
The Physical layout of the critical care unit will vary depending upon the size ofthe hospital, the type of patients to be cared in the unit, architectural design ofbuilding, space and economic restrictions. These special considerations, alongwith wide variety of style of care providers and hospital policies influence thedesign of critical care unit.
Although the same principles apply whether one is building a new hospital or newwing is added to hospital, or remodelling is done in an existing area, but the spaceconstraints and geographical consideration with regard to the rest of the hospitalare much more difficult during remodelling.
In this practical we will discuss about the physical layout of the unit and specialconsiderations, one has to keep in mind while designing a critical care unit. 95
/ I\

..
Nursing InterventionModalities 7.1 OBJECTIVES·
After completing this practical, you will be able to:
• plan and organise a critical care.unit;
'.
• determine the ideal bed strength required for critically ill patients for a unitin a hospital;
• discuss the various aspects important in the design 'of a critical care unit; and
• list down the equipments required in a critical care unit.
. ,7.2 LOCATIONOFACRITICALCAREUNITA critical care unit in a hospital should ideally be located at a place that is nearto laboratories, CT scanner, MRI scanner, nuclear medicine unit, emergencydepartment, step-down units, operation theatre and preferably cafeteria. Since allthe facilities can not be made possible, it is important to identify the most criticalneeds. Satellite laboratories and X-ray facilities may be helpful in meeting theseneeds. There should be spacious elevators near to the critical care unit. It shouldbe located at such a place that it can be easily approached. However, critical careunit should be away from the crowded and noisy areas. Location of Critical Careunit, should ensure the patient as a central focus, so that patients needs andrequired skills of the critical care nurse are utilized to meet the needs of the patientwith accuracy. Location should be aesthetically pleasing with healing environment.The location should be noise free instead therapeutic sounds, ocean waves andrain showers can be introduced.
7.3 DETERMININGBEDSTRENGTHOFACCUThe number of beds to be accommodated is an important issue in today's climateof medical economics. Careful analysis and projection of needs is worth the effortearly in the project. Examining current census needs and reviewing how manydays all beds are full and how many requested admission are denied, will help todetermine the needs. Formulae are available to predict the number of beds dependingupon the percent of time the hospital is willing to be unable to accept admissionsdue to non availability of beds. One such formula
Beds needed = Average census + Z ) Average census
The constant Z is a factor that is determined by the desired probability (p) ofhaving a critical care bed available upon request as below:
r'
P (%) Z
99 2.33
95 1.65
90 1.28
85 1.04
96 80 0.804
I/

..Jt
Another easy calculation is 10% of total hospital bed strength. One to two bedshould be free for routine disinfection.
"
To the above calculated number, the projected community population and economicgrowth should be considered. Future plans of hospital expansion or programmesshould also be considered while determining bed strength of critical care unit.
Structuring the Beds into Units
Critical Care Units larger than 12 to 16 beds are difficult to manage from anadministrative and providing quality care stand point of view. On the other hand,small units with less than 6 beds is not economically efficient. Therefore, it isrecommended that a unit should have 8 to 16 beds. Smaller hospitals may needonly one Critical care unit to meet their demands whereas larger institutes whichrequire more Critical care unit beds will make divisions by either speciality wiseor levels of care. In a hospital where there are large number of patients, aseparate units that can establish specific patient care protocols are desirable.Another way of separating units is by level of care. More critically ill patients maybe placed in a unit with physician coverage round the clock, higher nurse patientratio and increased space for high- technology procedures. Another unit (stepdown unit) would provide care for critically ill patients who require less directphysician care and less high technology machines.
7.4 DESIGN OF CRITICAL CARE UNITOnce the number of beds has been determined and divided into units, spacerequirements can be delineated. Configuration should be such that the beds orindividual rooms are observable from nursing station. In open-bay layout eachbed is allotted 150 to 200 sq feet. In case of individual rooms it should be 225to 250 sq feet. These dimensions are only for patient space. In addition to spacefor patients about 100 sq ft per bed for patient support area should be earmarkedthat would include nurses' station, dirty and clean utility areas, physicians workingarea and storage. Besides space for family waiting area, counselling area, laboratory,nurses' and physicians' rest room also must be considered.
In the space location and over all designing of critical care unit, following pointsshould be kept in mind; which are as follows:
• Unit access
• Control of nosocomial infection
• Patient comfort
• Communication system
• Patient room configuration
• Patient support areas
• Support area for nurses
• Physician support area
/
Design of a Critical CareUnit
97
I
. ,
,.
Nursing InterventionModalities
Let us discuss each one of these as given below:
"
.It
Fig, 7.1 : A Critical Care Unit
7.4.1 Unit Access
Critical Care Unit should be away from the main corridor. Family waiting areaand counselling room should be Located. The main doors of the unit should beas wide as hallway and automatic. The elevators should be nearby and spaciousto accommodate not only occupied bed but also equipment and space for fourto five personneL
7.4.2 Control of Nosocomial Infection
Hand washing facilities should be conveniently located in a critical care unit. Footcontrol of water taps is best. Walls and floors must be of materials that allow.cleaning and decontamination. The critical care unit should have a delineated areaby two levels of cleanliness - clean area I and clean area IT. Clean area I allowsthe entrants to enter only after change of footwear and restricts unnecessary orcasual visitors to the unit. Persons entering in clean area IT will enter only afterchanging clothes and wearing masks. Centralized air conditioning should be witha flow that prevents linear flow from one bed to another and will be ideal. Eachbed should have individual sets of desk, shelf and patient 'care equipments.
7.4.3 Patient Comfort
98
To provide maximum comfort to the patient in a critical care unit. The temperatureshould be maintained between 65 and 85° F and humidity between 30 and 60%.Comfort can be maximized by allowing privacy and noise control. Building materialshould be sound absorbing. Each bed should be separated by thick glass wallswith curtains. In addition each individual room or bed should have a window tothe room !bed view of outside. This will be helpful in differentiating day and night.Wall clocks should be appropriately placed so that patients can easily see fromeach bed. Lighting control to allow dimming for rest periods and brightness forbasic procedures, is of utmost importance. Procedure lights should be ceiling-mounted. Soothing colours and pleasant paintings, views or deeors may be useful.Light shades of blue or beige are soothing.
/ I
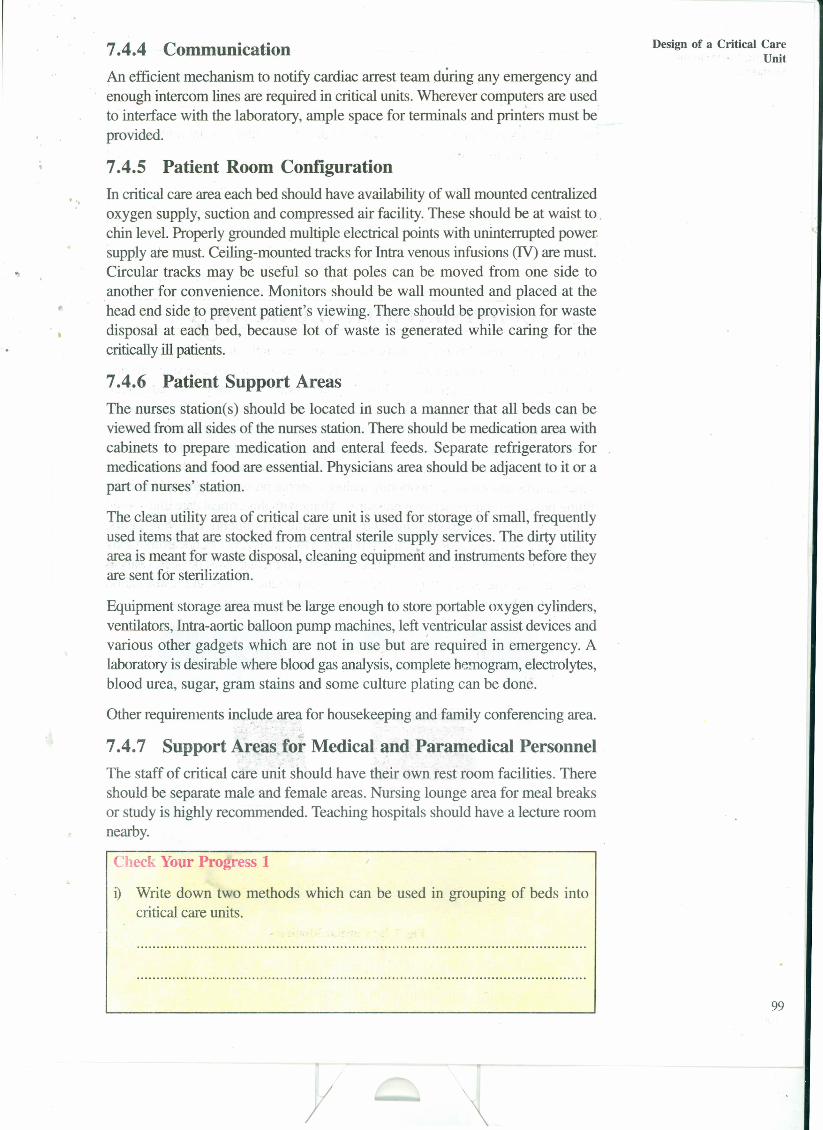
7.4.4 CommunicationAn efficient mechanism to notify cardiac arrest team during any emergency andenough intercom lines are required in critical units. Wherever computers are usedto interface with the laboratory, ample space for terminals and p~ters must beprovided.
. "
7.4.5 Patient Room ConfigurationIn critical care area each bed should have availability of wall mounted centralizedoxygen supply, suction and compressed air facility. These should be at waist to .chin level. Properly grounded multiple electrical points with uninterrupted powersupply ate must. Ceiling-mounted tracks for Intra venous infusions (IV) are must.Circular tracks may be useful so that poles can be moved from one side toanother for convenience. Monitors should be wall mounted and placed at thehead end side to prevent patient's viewing. There should be provision for wastedisposal at each bed, because lot of waste is generated while caring for thecritically ill patients.
7.4.6 Patient Support AreasThe nurses station(s) should be located in such a manner that all beds can beviewed from all sides of the nurses station. There should be medication area withcabinets to prepare medication and enteral feeds. Separate refrigerators formedications and food are essential. Physicians area should be adjacent to it or apart of nurses' station.
The clean utility area of critical care unit is used for storage of small, frequentlyused items that are stocked from central sterile supply services. The dirty utilityarea is meant for waste disposal, cleaning equipment and instruments before theyare sent for sterilization.
Equipment storage area must be large enough to store portable oxygen cylinders,ventilators, Intra-aortic balloon pump machines, left ~entricular assist devices andvarious other gadgets which are not in use but are required in emergency. Alaboratory is desirable where blood gas analysis, complete hemogram, electrolytes,blood urea, sugar, gram stains and some culture plating can be done.
Other requirements include area for housekeeping and family conferencing area.
7.4.7 Support Areas for Medical and Paramedical PersonnelThe staff of critical care unit should have their own rest room facilities. Thereshould be separate male and female areas. Nursing lounge area for meal breaksor study is highly recommended. Teaching hospitals should have a lecture roomnearby.
Check Your Progress 1
D Write down two methods which can be used in grouping of beds intocritical care units.
)I
Design of a Critical CareUnit
99
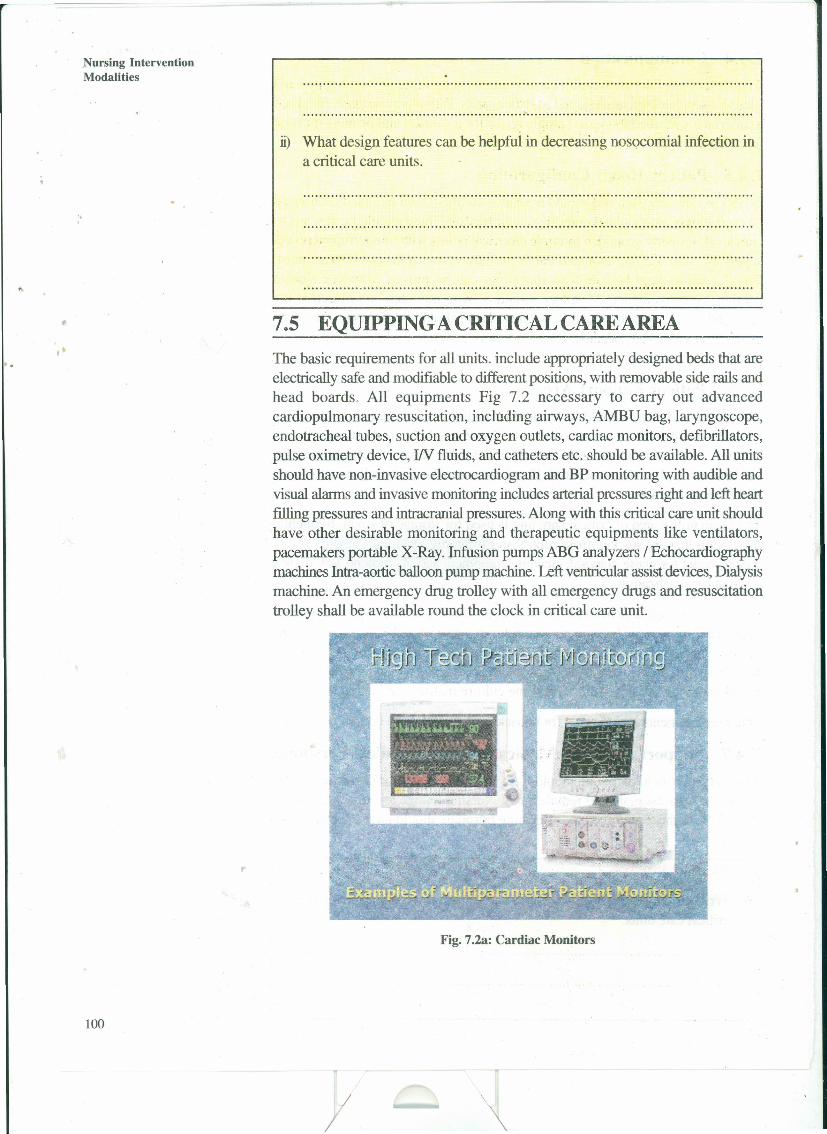
Nursing InterventionModalities
it) What design features can be helpful in decreasing nosocomial infection ina critical care units.
".
7.5 EQUIPPINGACRITICALCAREAREAThe basic requirements for all units. include appropriately designed beds that areelectrically safe and modifiable to different positions, with removable side rails andhead boards. All equipments Fig 7.2 necessary to carry out advancedcardiopulmonary resuscitation, including airways, AMBU bag, laryngoscope,endotracheal tubes, suction and oxygen outlets, cardiac monitors, defibrillators,pulse oximetry device, IIV fluids, and catheters etc. should be available. All unitsshould have non-invasive electrocardiogram and BP monitoring with audible andvisual alarms and invasive monitoring includes arterial pressures right and left heartfilling pressures and intracranial pressures. Along with this critical care unit shouldhave other desirable monitoring and therapeutic equiprnents like ventilators,pacemakers portable X-Ray. infusion pumps ABG analyzers / Echocardiographymachines Intra-aorticballoon pump machine. Left ventricular assist devices, Dialysismachine. An emergency drug trolley with all emergency drugs and resuscitationtrolley shall be available round the clock in critical care unit.
Fig. 7.2a: Cardiac Monitors
100
II

..
"
, .
, Fig, 7.2b: Cardiac Monitors
Fig. 7.2c: Glucometer
Fig. 7.2d: Extra corporeal membrane oxigenator
-+--
//
..
3.. ~'> •
Design of a Critical CareUnit
101
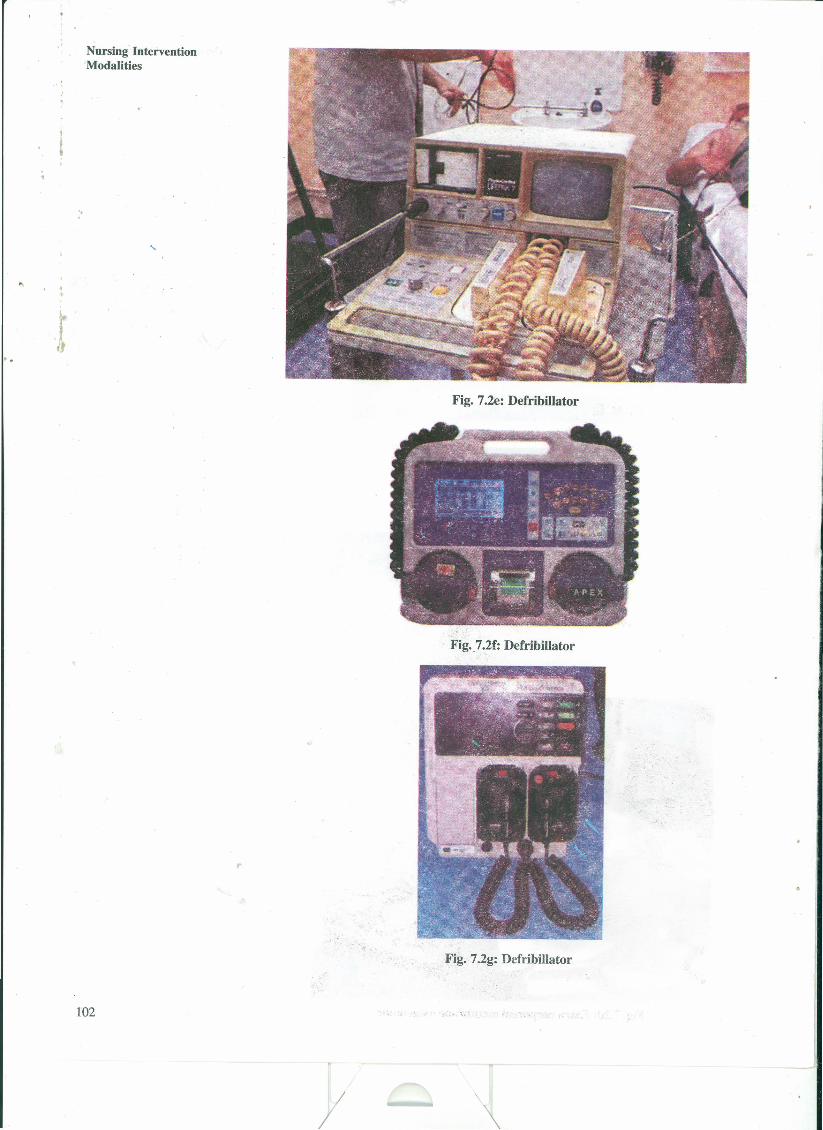
,.
, ,
Nursing InterventionModalities
'..
Jt
102
Fig. 7.2e: Defribillator
Fig.7.2f: Defribillator
,.
Fig. 7.2g: Defribillator
//
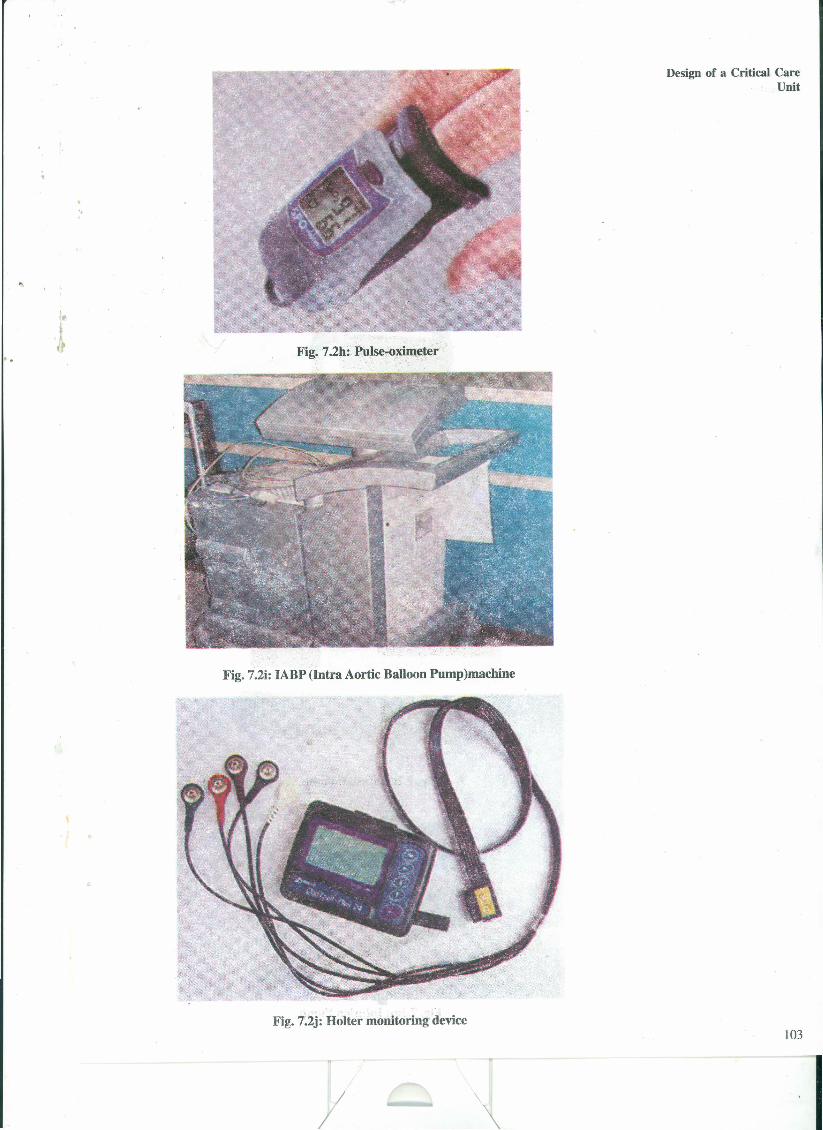
'.
Design of a Critical CareUnit
f!.tFig. 7.2h: Pulse-oximeter
Fig. 7.2i: IABP (Intra Aortic Balloon Pump)machine
Fig. 7.2j: Holter monitoring device103
/I I
, .
Nursing InterventionModalities
'..
104
/
Fig. 7.2k: Ventilator
Fig. 7.21: Infusion Pump
Fig. 7.3m: Infusion Pump
I
, ,
Jt
"
Fig. 7.2n: Airways
Fig. 7.20: EndoTracheal tube
.Fig. 7.2q: AMBU and Mask
Fig. 7.2(a-q): Equipments in critical care unit
Check Your Progress 2
i) List any five essential equipments required for a critical care unit.
..................................................................................................................
I
Design of a Critical CareUnit
105
I
• I
,.
Nursing InterventionModalities
".
Jt
106
ii) What does Invasive pressure monitoring include?
. : .
7.6 LET USSUMUPIn this practical, you have learnt about the physical layout and designing of acritical care unit. We have discussed about the determination of bed strength,configuration of the CCU and the patient's unit, space allocation and designspecifications that can decrease nosocomial infection. We have also focused ourdiscussion on all patient support areas and nurses support areas. The nursesshould be involved in the planning of any critical care unit who can give valuablesuggestions on various supplies and equipments needed.
7.7 ANSWERSTOCHECKYOURPROGRESSCheck Your Progress 1
i) a) depending upon the level of care patients need
b) according to the speciality area.
ii) conveniently located hand washing facilities
delineating clean area I and clean area 11
washable wall and floor materials
separate desk and shelf for each patient
centralized air conditioning
Check Your Progress 2
i) a) AMBU Bag b) oxygen supply c) suction apparatus/outlet
,.
d) noninvasive BP monitoring e) modifiable beds
ii) invasive pressure monitoring may include arterial pressure, right and left heartfilling pressure and intracranial pressures
7.8 ACTIVITIESSelect a high dependency area of your hospital.
(i) Draw a schematic diagram of the physical layout of the unit.
(ii) List down the suggestion you would like to give if there is a remodelling planfor the unit.
/I
PRACTICAL 8 PREPARING ARESEARCHPROPOSAL AND ATERM PAPER
" Structure
8.0 Introduction
8.1 Objectives
8.2 Developing a Nursing Research Proposal8.2.1 Definition
8.2.2 Overview of research proposal8.2.3 Criteria for evaluation of research proposal8.2.4 Steps in understanding a research project
8.3 Term paper8.3.1 Organization of term paper
8.3.2 Presenting your term paper effectively
8.4 Critique8.4.1 Meaning of critiquing
8.4.2 Guidelines for critiquing8.4.3 Checklist for critiquing a study8.4.4 Sample of research critique
8.5 Let Us Sum Up
8.6 Answers to Check Your Progress
8.7 Activities
8.0 INTRODUCTIONThere is a growing consensus that knowledge of nursing research is needed toenhance the professional practice of all nurses. Nursing research is in practiceway back from 1950s. But lot of emphasis on it started from 1970s. Nurses aresince then increasingly studying problems such as health promotion, prevention ofillness, the efficacy of nursing 'interventions and the needs of high risk groups etc.
Recently a renewal of the need for research has gained importance. There isincreased willingness to approach client problems in a systematic way. There aremany funding agencies for furthering research in nursing and the topic is discussedon various platforms. It therefore has become necessary for every nurse to be notonly aware of the process of research but also be able to carry out researchindependently or as a member of research team. In this practical we shall focuson developing a research proposal and term paper.
107
I

'Nursing InterventionModalities
•" •,
".•
~
•4 -
8.2
108
8.1 OBJECTIVESAfter completing this practical, you will be able to:
• develop an understanding of nursing research and research proposal;
• prepare a research proposal;
plan for undertaking a project;
carry out a project independently or as a team member in a research team;
prepare an abstract of the study accomplished by you or in way towardscompletion;
prepare term paper for presentation of the study carried out by you or yourresearch team; and
critically analyze a given study or a proposal.
DEVELOPING A NlTRSING RESEARCHPROPOSAL
Nursing research involves a systematic search for knowledge about issues ofimportance to the nursing profession. It is a systematic and objecti ve process ofanalyzingphenomena of importance to nursing.The domain for nursing thus includesnursing practice, nursing education and nursing administration.
You may recall here that scientific research is the most objective and reliablesource of nursing knowledge. Researcher uses systematic, orderly and objectivemethods of seeking information. Scientific method uses empirical data which isgathered through the sense organs. Information is gained in the form of data orfacts that are obtained in an unbiased manner from some aspects of the real world.
8.2.1 DefinitionIt is a written document specifying what the investigator proposes to study andis therefore written before the project has commenced. It serves to communicatethe research problem, its significance and planned procedure for solving theproblem. Research proposal may be written by the students enrolled for researchproject. It is a prerequisite for the funding agencies or sponsoring authorities.Reviewers of the research proposal may be faculty, people from funding agencyor peer group.
8.2.2 Overview of research proposalYou have learnt about the research process and details of each step of theprocess in your theory of BNS 031 block 6 unit 4. In this practical, you willleamto initiate individual research actvity. The research activity can be small or mayinvolve many competent people, who may work as a research team, towards thecompletion of a research project.
Research proposal helps in the following:
• gives a clear idea of what the researcher plans to do and how and whenvarious tasks are to be accomplished.
• gives an idea of capability of the researcher for following the proposed planof action.
/
"
• provides a brief synopsis of the proposed research that concisely statea theobjectives and methods to be used in the research.
• helps to establish a frame of reference for the reviewers as they begin to readthe research proposal.
• describes the statement of the problem in such a way that its importance isapparent to the reviewers.
• describes how the proposed research will make the contribution to theexisting knowledge or is beneficial on a broader platform like a group ofpeople, community or society.
• indicates generalizing ability of the research proposal, its contribution to thetheory, its potential for improving nursing practice for patient care.
Statement of the problemFor a research proposal, the problem identification should be clearly stated. Itshould be stated in a manner that importance of the problem to be researched isprojected. For example, if you noticed, over the time that the incidence of postoperative infection has increased in a post operative ward. It poses a problemthat needs to be tackled. If you take this as a research problem to be studied,you need to know whether there is presence of occurrence of post operativewound infection. There may be many factors contributing towards post operativeinfection. You need to study them one by one. You may think of whether thestandards for wound care are being followed or not. For this, you need todevelop a standard protocol for wound care to be followed or consider analready existing protocol designed to be followed. Now you need to look for thefollowing:
• whether the protocol is being followed or not
• fmd out the reasons for inability to follow the protocol
• anticipate reasons for not following the protocol
• think and introduce interventions that can tackle the problem
• evaluate the effectiveness of the intervention introduced.
In such a case the statement of problem would be as follows:
"To determine the incidence of post operative infection and practice of woundcare protocol by health professionals in post operative patients of a selectedsurgical unit of a hospital."
You may specify the setting of the research study (the place where you plan toconduct the research study)
Background of the problemIt should clarify and strengthen the arguments for the significance of the researchstudy, and orient the reviewer to what is already known and how the proposedstudy will augment the existing knowledge.
Objectives of the studyThe researcher should provide clearly stated criteria against which proposedresearch study can be assessed. These criteria should be specific and achievable.The objectives of the research study will guide the researcher in selecting the
/I
Preparing a ResearchProposal and a Terni Paper
109
I
Nursing InterventionModalities
approach and planning the methodology for the proposed research study. Forexample, in the problem stated above the objectives would be:
• To determine the incidence of post operative infection in post operativesurgical unit.
• To develop a checklist for evaluating the practice of health professionalsregarding wound care protocol.
• To assess the practice of health professionals in following wound care protocolfor post operative patients.. .
• To determine factors affecting the practice of health care professionals.
Assumptions and delimitations
You will mention the assumptions that are the basis for carrying out the researchstudy. You have to mention the delimitations of the study. Here you have tomention the inclusion and exclusion criteria of the study. For example, will youinclude only the abdominal surgeries or all surgeries? Will it include patients whohave complications like peritonitis which may have direct effect on the incidenceof post operative infection etc.?
Operational definitions
The significant terms are defined operationally.These are specific conditions appliedto a universally accepted term as per the need or objectives of the study.Wheneverthe concerned term is used, it refers to the operational definition of the term astailored for the particular research study. For example, 'Youneed to operationallydefine the terms health professionals here which may include nurses, doctors,physiotherapist depending upon your intention of the study. Post operativeinfection which may be defmed as wound swab for bacterial culture-positive oryou may even define it in terms of presence of signs of wound infection i.e.,redness, discharge, pus and gaping of wound. This will be completely your decisionto define the terms as per need and constraints of your research study.
Conceptual framework
Preparaton of conceptual frame work is mandatory in research study. Identify asuitable conceptual framework depending upon the type of variables under studyor phenomena to be measured in the study. You can discuss with experts who arefamiliar with broad range of theories in nursing. This will enable you to be clearin your mind about your own conceptual perspectives and pick up an appropriateframework for you research study.
Research methodology
You have to explain how research objectives will be addressed. It should describesample plan, research design, instrument /tools, specific procedure for datacollection, analytic strategies to be used. You can also state potential methodologicalproblems and the intended strategies to handle such problems. For example, inthe aforementioned study, the tools would be:
• observation checklist for observing the practice of following the woundcare protocol,
• ' observation checklist for signs of wound infection,
• questionnaire to determine the factors affecting. practicing wound careprotocol.
"
".
110
II
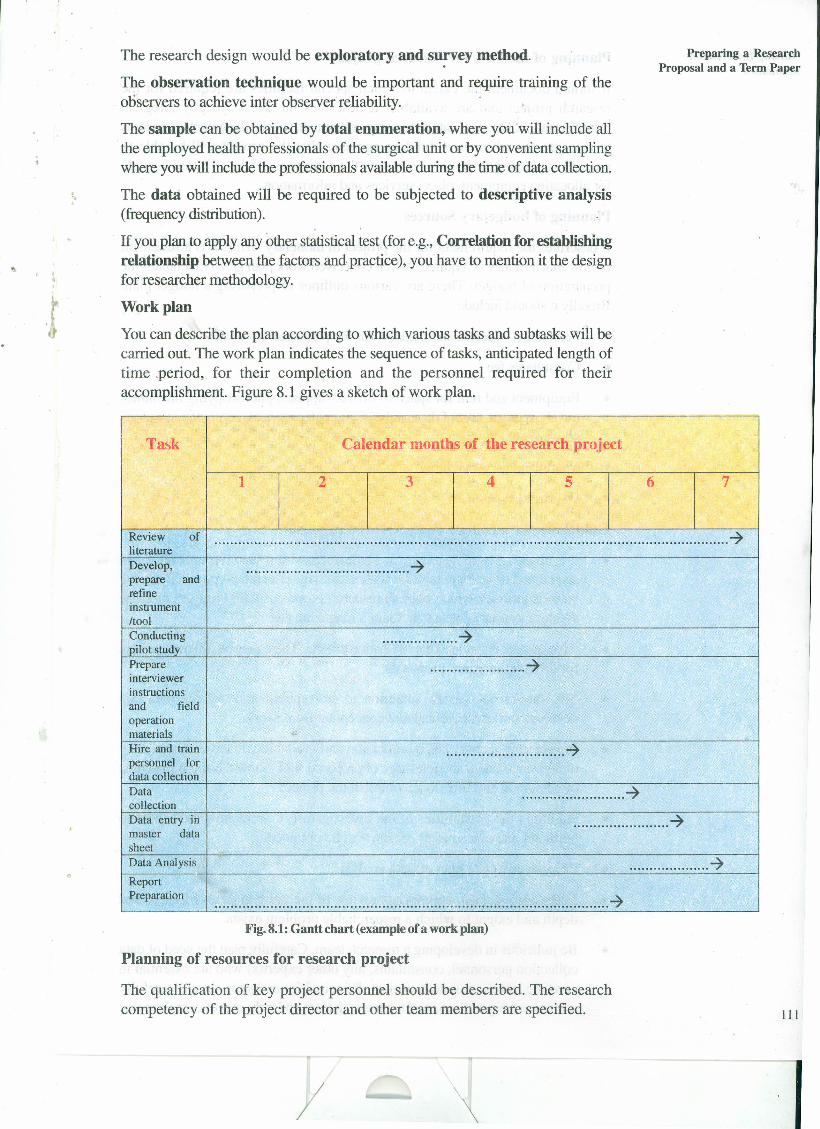
,",
The research design would be exploratory and su~vey method.
The observation technique would be important and require training of theobservers to achieve inter observer reliability.
The sample can be obtained by total enumeration, where you 'will include allthe employed health professionals of the surgical unit or by convenient samplingwhere you will include the professionals available during the time of data collection.
The data obtained will be required to be subjected to descriptive analysis(frequency distribution).
If you plan to apply any other statistical test (for e.g., Correlation for establishingrelationship between the factors and practice), you have to mention it the designfor researcher methodology .
Work plan
You can describe the plan according to which various tasks and subtasks will becarried out. The work plan indicates the sequence of tasks, anticipated length oftime .period, for their completion and the personnel required for theiraccomplishment. Figure 8.1 gives a sketch of work plan.
Preparing a ResearchProposal and a Term Paper
I "
.r
Task Calendar months of the research project
1 2 3 4 5 6 7
Review of ............................................................................................:~...................................-7literatureDevelop, .........................................-7prepare andrefineinstrumentItoolConducting ...................-7pilot studyPrepare ........................-7interviewerinstructionsand fieldoperationmaterials '"Hire and train ..............................-7personnel fordata collectionData ..........................-7collectionData entry in ........................-7master datasheetData Analysis ....................-7Report
IPreparation ...................................................................................................-7
Fig. 8.1: Gantt chart (example of a work plan)
Planning of resources for research project
The qualification of key project personnel should be described. The researchcompetency of the project director and other team members are specified. 111
I/
. .
Nursing 'InterventionModalities
Planning of facilities for research project
It should' document the extent to which special facilities are required for theresearch project and are available. It describes the access to physiologicalinstrumentation, libraries, data processing' equipment, special documents or recordsto reassure the advisors or funding agencies that the project will be able toproceed as planned. It should also specify the willingness of the affiliated Institutefor 'allocating equipment, place, services and information.
Planning of budgetary Sources".
J,
It describes the requirement for the project in monetary terms. It is a statementof how much money is required. A well conceived work plan greatly facilitates thepreparation of budget. There are various outlines of preparing a budget plan .Broadly it should include
• Personnel- salaries and benefits for the personnel involved
• Consultants fee
• Equipment and rent for space of office, supplies, photocopying machines,travel expenses, cost of data analysis, computer services, computation expertsservices etc.
• Miscellaneous expenditure
• Overhead expenses.
Guidelines for writing a good research proposal
• It is always advisable to review some successful research proposals to getacquainted or become familiar with successful research proposal. There arevarious journals which publish research proposals with critiques namely,Western journal ofresearch, Gant's magazine etc.
• Give special attention to the evaluation criteria. There may be different criteriafor different research proposals.
• You should pay careful attention to conceptualization of the idea anddevelopment of theoretical and conceptual framework.
• Project staff quantity and qualification and availability in terms of adequacyof relevant trainees and relevance of proposed staff. Show the appropriatenessof personnel and time to accomplish the project.
• Highlight the capabilities of the investigator(s). Show how the access topertinent relevant sources of data will be obtained.
• Propose adequate plan of data analysis.
112
• Make adequate and appropriate review of literature in terms of scope anddepth and extent to which a researchable problem exists.
• Be judicious in developing a research team. Carefully plan the need of datacollection personnel, consultants, any other expert(s) who are essential incarrying out the research project. Principal investigator should carefullyscrutinize the qualification of the research team and right mix of competencies.
/I
Justify the inclusion of every Staff person and identify the contribution thateach member will make to the successful completion of the research project.Do not keep too many top level professionals who will directly supervise L1.eproject as it may affect the flow of work.
• Before final submission get the draft reviewed and critiqued. If you haveplanned to hire consultants, then include him (her in research proposalpreparation.
" Contents of a research proposal
You as a researcher should know the contents of research proposal. Writtenproposal has a set of instructions that indicate the format to be followed. Thecontent of proposal is organized in a specified format.
Proposals prepared for different reasons vary in the amount of detail but havesimilar outline, which are as follows:
• Introduction
• Background
• Need for the study
• Statement of the problem
• Objectives
• Operational definitions
• Conceptual framework
• Assumption, Delimitations
• Research methodology-variables, research approach, setting, sampling criteriaand technique, data collection procedure, plan of data analysis.
• Finance of the project
• Proposed project timetable
• Outline of the report
• Reference
• Appendices.
8.2.3 Criteria for evaluation of research proposalIn previous sections, you have learnt about the overview of research proposal andin this section you will study about the criteria of research proposal.
Although, the criteria for evaluating research proposal may differ for differentresearch proposals but they generally include as follows:
• Importance of research question
• Its theoretical relevance
• Appropriateness of the research methodology
//
Preparing a ResearchProposal and a Term Paper
j 13
I

Nursing InterventionModalities
".
,.
114
• Availability of appropriate personnel and facilities
• Budgetary requirements,
Theme (problem)
• What is the core idea around for which the investigation is organized?
• Is the central theme stated clearly and explicitly?
• Is the problem clearly stated?
.' Is the central theme stated clearly in the research proposal and then carriedthroughout in the content of the research proposal?
• What is the relationship of the theme with other research findings?
Simplicity, clarity and logical consistency
• Is the proposal written as simply and clearly as possible?
• Does the introduction and justification logical, specifically to the specifiedquestion?
Hypotheses
• Are the questions, hypotheses or objectives researchable?
• Can the questions be answered on empirical basis?
• Are the variables under investigation clearly defined in observable andmeasurable terms ?
• Are the hypotheses relevant and meaningful?
Strategy of investigation
• Has the researcher chosen appropriate research methodology?
• Is the method clear which provides logical extension of the central theme?
Sample
• What is the sample subject? Are the characteristics of the sample clearlystated?
• Has the researcher described the sampling procedure?
• Is the sampling size adequate and clearly stated?
Ethics,.• Is the procedure ethical?
• Are the plans made in such a way to obtain confidentiality and anonymityand to obtain consent from the participants?
Appropriateness of the research design
• Is there a plan to test the feasibility through pilot study?
• Is the treatment variable planned and validated?
//

. ,
".
• Has the investigator selected appropriate and effective design?
Reliability and validity
• How is reliability and validity established and maintained'i
• Are the tools appropriate for the data collection?
Appropriateness of the statistical analysis
• Does the proposal give the plan for statistical analysis?
• Is it appropriate in terms of objectives, importance, size of sample and typeof data?
Personnel and facilities
• Are the personnel adequate in number to perform the assigned tasks?
• Are they qualified to perform the tasks assigned?
• Are the facilities sufficient enough to accomplish the tasks?
Budget
• Is the proposed budget reasonably planned?
• Will the assessment of budegt be able to meet the necessary requisites?
• Is there scope of meeting unexpected expenses?
• Is the demand written in too inflated terms or are not genuinely required?
Check Your Progress 1
D List down the content outline of a research proposal.
8.2.4 Steps in undertaking a research projectWhen you intend to undertake a research project you as a principalinvestigator has to prepare a research proposal on the identified problem as youhave learnt in the previous section of this practical. There are many agencieswhich provide funds for research activities. These include Governmentalorganizations, Ministry of health and family welfare, Ministry of women and childhealth, National Commission of Women, Department of social welfare, Departmentsunder National Programmes or Policies, various professional associations, likeHeart Care Foundation, Sigma Theta Tau International Society for nurses, variouseducational universities and University Grants Commission, National Institute ofHealth and Family Welfare, WHO, UNICEF, UNFDP and many more. Theinformation is also available in "Research Report" section of the journal of NursingResearch. The websites of these can be explored for arranging finances for theproject.
I
Preparing a ResearchProposal and a Term Paper
115
I
Nursing InterventionModalities
a) Identification of funding sourcesThe funding sources are identified and applications are filled. Some of the agencieshave their own application fOlIDS.Proposals may be submitted on these proformas.Most of the proformas require information as given below:
• Title page:
• name and qualification of the principal investigator,
institutionalaffiliation,
amount of money requested,
proposed time of completion of the project and
administrative details
.,
••••
,.• Abstract of research plan: investigator's approach, aim and methods
• Research plan section: approach, methodology, sampling and plan fordata analysis,
• Budget: itemized costs for the project in terms of personnel, resources,equipments, direct and indirect costs etc.
b) Planning
You have to divide the work between the team members of research project.
Make the work plan.
c) Time management
• Keep detailed notes as you progress through your research project
• Be disciplined in your approach
• Be systematic. Do not leave things for the last hour
• Keep in touch with your supervisor
• Divide complex and demanding tasks into more easily programmable subtasks
• Don't overload. Make accurate estimate of time required for explanation ofresearch project.
• Revise your plan regularly.
• Finish your task before writing text or report
d) Supervision of the project
A supervisor is the person who oversees your project. It can be the principalinvestigator or another person appointed to ensure successful completion of thesubtasks by timeliness and coordination of the team members.
Requisites for good supervision of the research project are as follows:
• Give adequate time to meet the members;
• Set the objectives for next meeting and meet the objectives of the plannedmeetings;
• Ensure maintaining proper records;
• Accomplish tasks in small segments as one proceeds from beginning towardsend of research progress.116
"
.- ,J.
8.3 TERM PAPERYou have learnt about the preparation of research proposal and criteria forevaluation of research proposal. Now you will study about the term paper.
Term Paper
"
Term paper is a brief description of the study conducted and is intended forpresentation purposes for general audience with a mix of experts and people whoare not very proficient with research skills. Depending on the intended audience,the r~search report may be detailed like thesis or smaller in the form of a termpaper, while both describe the study. Thesis is generally intended for researchmanagers or experts in the field of nursing, Term paper will include live presentationwith increased attention to headlines, flow diagrams, charts, tables and summariesfor purpose of stressing on major points. A term paper presents up to dateinformation on research in different areas of a discipline. Here you get only ageneral idea of the research design, analysis, and findings.
8.3.1 Organization of term paperAbstract
The first thing that one needs to do before preparing for presentation, is toprepare an abstract and submit it well in advance for acceptance. The informationregarding the date lines are published in journals or personally to the members ofa professional organization generally 6 to 12 months before the event. The requiredlength of abstract varies from 200 to 1000 words. It contains the purposes,researchquestion, design,methodology,major findings and conclusions.The abstractshould report the most important elements of your project in such a way that itgenerates interest. It should be clear, compelling and concise.
Introduction
The introductory section of term paper includes three to four paragraphs. Theareas included are background of the problem, need for the study, problemstatement, statement of objectives, rationale for the study through theoreticalframework, operational definitions of the terms, scope and delimitations of thestudy. It provides the context for the research question.
Literature Study
The related review of literature should be written into a paragraph or two. Onlysalient points of findings, instrument or limitation of the studies are written.
Methodology
This is major area of your term paper. Brief description of research approach,design, setting, sample criteria, sample size, instruments and data collection areincluded in the term paper. The salient features are brought out like samplingtechnique, size of the sample and data collection procedure.
Results
Data analysis and discussion build the main body of your term paper. The essentialtables, figures and graphs are included with interpretation. The power of studyis important to be mentioned.
/I
Preparing a ResearchProposal and a Term Paper
117
Nursing InterventionModalities
"
"
118
Discussions
Includes discussion of the results, including major limitations as well as the mostimportant findings for clinical practice. You have to discuss the clinical relevanceof the findings.
Implication for future research and nursing
Two or three paragraphs are devoted to the conclusion and implications. Youhave to reason out if the hypothesis is found to be not significant. Suggest thevalues of the findings through reflective thinking in terms of possible applicationof the results and contribution of the results to the practice.
8.3.2 Presenting your term paper effectively• To prepare for your term paper presentation, you will need to know the
composition of the audience, the amount of time you have and the objectivesfor presentation. Presentation can vary from informal discussion to highlyformalized address. You can ask for directions from the contact person, if indoubt. Whether the audience is composed of specialists of profession,concerned, will dictate the level of detail you provide. It will also help youto tailor it to their requirement.
• Term paper is planned for 20 to 30 minutes. Therefore, include only the mostimportant points that lead to maximum application of your findings.
• Use simple language with clear expression.
• Design your presenration in such a way that the results are presented logicallyand the flow is continuous.
,.
• Develop an outline as mentioned above, and then add major points undereach heading.
• Do not write a speech. But create a detailed outline for reference and audio-visual aids to support your presentation.
• Diagrams and photographs can be used in describing the intervention ormeasurement of any phenomenon.
• Tables and figures should not duplicate the text. The information presentedin each should be unique, to generate interest of the audience.
• The tables exhibited should be complete in itself.
• Use only easily understandable abbreviations. All tables should have a titleand all columns should have column head and the units or symbols, if any.For example, % or kg etc.
• Group the major elements together with logical transition statements.
• The conclusion should summarize the overall importance of your study, themain concepts and major implications for practice.
• Plan the conclusion with objectivesof maximum retentionof the most importantparts of your term paper.
• Keep time for discussion and queries of the audience. Listen and handle thequestions carefully.
/I
\

,. ,.
Here are details of a study conducted at one o( the hospital in Delhi.The details are cut short to include important content to serve as abase on which you can prepare a term paper. This is followed bywriting of a term paper for the same study. Research study is conductedin a selected Hospital at Delhi and example is stated in this section toenable you to write a term paper and how to present it as term paper.
"A study to evaluate the effectivenessof planned teaching programme on knowledgeregarding self-care following pacemaker implantation and skill to monitor radialpulse in cardiac patients in a selected hospital of Delhi."
Background of StudyCardio vascular diseases are the leading cause of illness and death affecting morethan one in five people in developed countries. About one sixth of those who dieof heart diseases are younger than 65 years of age. Dysrythmias are one of themajor cardiac problems seen in our country. Dysrythmia cause considerablemorbidity and mortality.First degree atrioventricularblock thought to be a relativelybenign arrhythmia, can be associated with severe symptoms that may benefit frompermanent pacing. Some uncontrolled trials have shown a benefit from pacing inpatients with a PR interval greater than 0.3 seconds. Permanent pacing is knownto improve survival in patients with complete heart block, especially if they havehad syncope. Symptoms of A.Y. block generally resolve after insertion of a DDD(dual chamber demand) pacemaker. Patients whose arrhythmia continue to beinducible inspite of antiarrhythmic therapy have a higher mortality rate (43%) thanthose patients whose arrhythmia are no longer inducible (9%).
The pacemaker has emerged as the preferred mode of therapy for most patientswho have life threatening arrhythmia. Today more than 1,50,000 pacemakers areimplanted each year in patients with variety of cardiac arrythmias. According toOvsyshcher lE and Furman S. (2003), despite the established therapeutic efficacyof pacemaker and implantable cardioverter defibrillators (ICDs), markedgeographic and national variations in their implant rates have been documented.
The study revealed as follows:
• The implantation rate of pacemaker and ICDs depends heavily on nationaleconomic status and demographics.
• Economic factors are important determinant of implant rates, though highrate was observed in countries with modest economic resources and highlyeducated physicians and population.
• . Evaluation of pacemaker and ICD implant rates per million of an overallpopulation, unless based on demography, can lead to significant inaccuracywhen comparing different regions and countries. They recommended forfurther studies.
Pacemakers are frequently implanted and complications resulting frompern ianentpacemaker implantations are well known. Early complications of pacinginclude-
• Pneumothorax,
• Lead perforation and Ventricular arrhythmia,
• Complications occurring later can include infection at the implantation site,
I/
Preparing a ResearchProposal and a Term Paper
119
,.
'Iursing Interventionvlodalities
"
120
• Endocarditis,
• Hematoma formation,
• Thrombosis, skin erosion over permanent pulse generator,
• Pacemaker failure,
• Lead dislodgement,
• Twiddler's Syndrome and
• Pacemaker syndrome.
Despite these well known complications, accurate prospective data on implantcomplications are limited. Elderly patients may be at increased risk of implantcomplications and are increasingly being referred for pacemaker implantation.
Pacemaker have become a reliable means of improving a person's quality of lifeand in helping people to live longer. With advanced pacemaker designs, it is theknowledge, skill and activities of the practicing health care professionals thatdetermine the quality of care to the patients.
Need for the Study
Once an individual is operated for Pacemaker implantation s/he becomes a patientfor the rest of his/ her life. These patients require close observation, teaching andregular follow up. They need to know a great deal about post discharge self carein order to derive optimum benefit from the treatment. Lack of preventingprogramme results in increased number of deaths in developing countries than indeveloped countries. Patient education is essential. There are many myths thatshould be addressed before sending patients home with their new pacemaker. Itis imperative that a patient with implantable pacemaker should learn to adopt tohis activities so that he can enjoy better health status.
There is lack of literature on teaching patients with implanted cardiac pacemakersunder conditions existing in developing countries. The studies done in the field ofpatient teaching are not specifically reJated to patients with implanted pacemaker.Hence the researcher felt the need to develop and administer the planned teachingprogramme (PTP) and evaluate its effectiveness. This would equip cardiac patientswith implanted pacemaker with requisite knowledge regarding self care at home.
Statement of the Problem
A study to evaluate the effectiveness of planned teaching programme on knowledgeregarding self care following pacemaker implantation and skill to monitor radialpulse in cardiac patients in a selected hospital of Delhi.
,.Objectives
1. To assess and evaluate the knowledge of cardiac patients about self careafter pacemaker implantation.
2. To assess and evaluate the skill of cardiac patients to monitor their radialpulse.
3. To develop a planned teaching programme for patients with implanted cardiacpacemaker regarding self care and monitoring of radial pulse.
II
" ..
-.
4. To assess the knowledge gained by patients regarding self care afteradministering the planned teaching programme.
5. To assess the skill gained by patients to monitor their radial pulse afteradministering the planned teaching programme.
6. To determine the relationship between knowledge arid skill scores of patientswith implanted pacemakers.
Conceptual framework
The study is based on System's model.
Conceptual Framework
The conceptual model in this study is based on System's Model adopted from aWHO publication (1985). It provides a guide for development, utilization andevaluation of a planned teaching programme. This model consists of three areasinput, process and output. The conceptual frame work of the study is representedin figure 8.2.
Input here refers to
i) Patients with implanted cardiac pacemakers, with their profile i.e., age, sex,education previous knowledge about pacemaker and years of implantation.
ii) Learning Resources i.e., Books, journal, magazines, mass media, and intemet.
iii) Resource person viz., nurses, doctors, clinical teachers.
These variables depict the existing background knowledge and skill of patientsregarding self care following pacemaker implantation.
Process refers to different operational aspects of the development andimplementation of a planned teaching programme. These include:
i) Developing the tools to assess knowledge and skill.
ii) Establishing the validity and reliability of the tool and pretesting the tools.
iii) Developing the planned teaching programmes to impart knowledge regardingself care following pacemaker implantation and demonstrate the skill to monitorradial pulse.
iv) Establishing the validity and reliability of the planned teaching programme.
v) Administering the planned teaching programme.
vi) Determining the effectiveness of planned teaching programme through posttest on knowledge and the skill.
Output refers to the post training evaluation of the performance of the cardiacpatients who were trained in the planned teaching programme, so as to find out,whether there is any evidence of the desired changes in the cognitive area andskills in relation to the set objectives.
If the patients acquire adequate knowledge they will be able to practice self careactivities at home following discharge. Consequently, they will be able to preventcomplications and there will be increase in their health status.
I
Preparing a ResearchProposal and a Term Paper
121
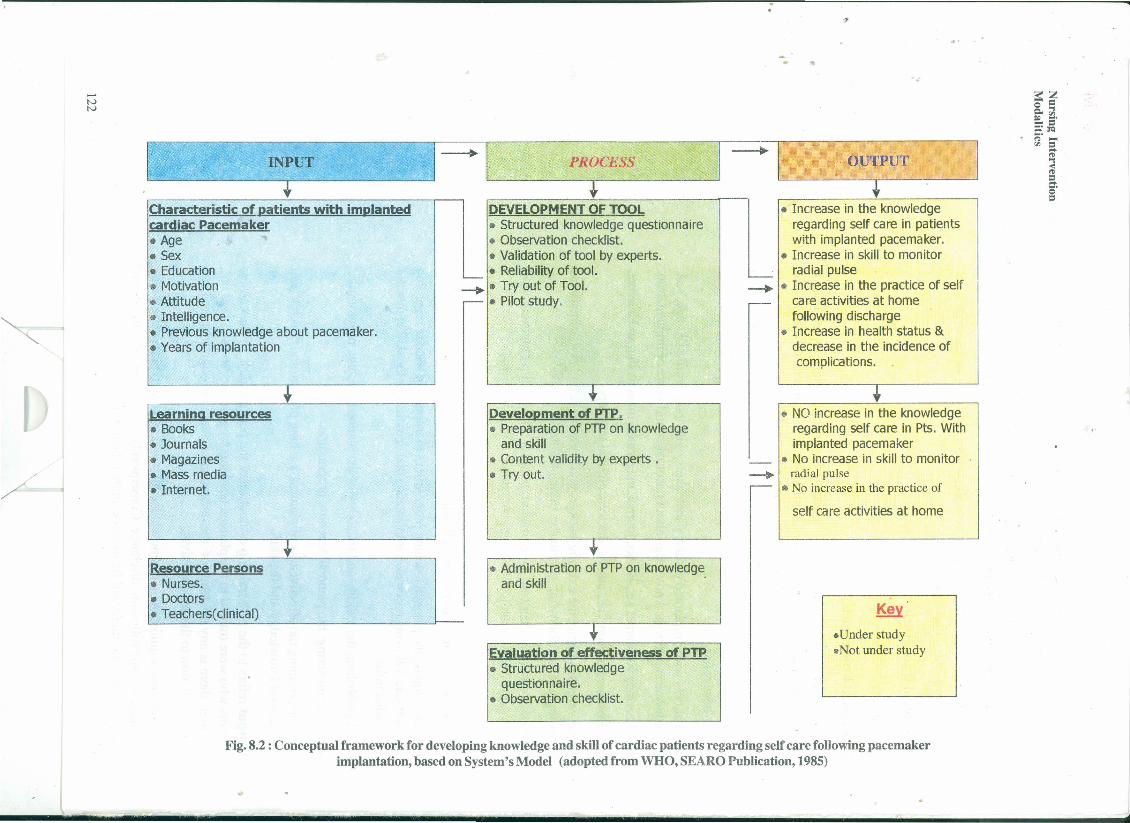
I. .~,INPUT ~I--+ I. ..PROCESS I-==-~I" OUTPUT 1I t t
-~
"<;
Characteristic of patients with implantedcardiac Pacemaker• Age• Sex• Education• Motivation• Attitude• Intelligence.• Previous knowledge about pacemaker.• Years of implantation
Learning resources• Books• Journals• Magazines• Mass media• Internet.
Resource Persons• Nurses.• Doctors• Teacherstcllnical)
l DEVELOPMENT OF TOOL• Structured knowledge questionnaire
L • Observation checklist.• Validation of tool by experts.• Reliability of tool.
--+ • Try out of Tool.- • Pilot study.
••Development of PTP.• Preparation of PTPon knowledge
and skill• Content validity by experts.• Try out.
~••
• Administration of PTPon knowledgeand skill
I
- tEvaluation of effectiveness of PTP• Structured knowledge
questionnaire.• Observation checklist.
~.~
'"
L • Increase in the knowledgeregarding self care in patientswith implanted pacemaker.
• Increase in skill to monitorradial pulse
• Increase in the practice of selfcare activities at homefollowing discharge
• Increase in health status &decrease in the incidence ofcomplications .
•• NO increase in the knowledgeregarding self care in Pts. Withimplanted pacemaker
• No increase in skill to monitorradial pulse
• No increase in the practice of
self care activities at home
~
~
Key
.Under study
.Not under study
Fig. 8.2 : Conceptual framework for developing knowledge and skill of cardiac patients regarding self care following pacemakerimplantation, based on System's Model (adopted from WHO, SEARO Publication, 1985)
.,
.,
:s:zo =Q,'"I= ~.::==:,C1QI'> ••••'" =~
'"I
~..•g'
- ... -- - -. - ~
" ..
Assumptions
• Patient education is one of the methods of changing human behaviour.
• Patient with implanted cardiac pacemaker will have some knowledge aboutself care.
".
• Adequate knowledge regarding self care in patients with implanted pacemakeris essential to improve the health status of the patient.
• Educating patients with implanted pacemaker will help in enhancing theirknowledge regardi~g home care. ,
• Patients will be able to recall the self care knowledge after pacemakerimplantation and practice self care activities after the administration of plannedteaching programme.
• Knowledge of patients can be assessed using structured knowledgequestionnaire.
• Skills of the patients can be assessed using observation check list.
Delimitations: The Study is delimited to:
• Adult patients with implanted cardiac pacemaker in the age group of 20-70years.
• Patients' with implanted cardiac pacemaker attending the follow up clinic ina selected Hospital in Delhi.
• Planned teaching programme will be administered only once after pretestingthe knowledge.
• Assessment of knowledge of cardiac patients will be done once before andonce after the administration of Planned Teaching Programme (PTP) regardingself care following cardiac pacemaker implantation.
• Assessment of skills of cardiac patients will be done once before and onceafter the administration of PTP for developing skill to monitor radial pulse.
The reviewed literature for the present study has been organized & presentedunder two main areas:
1. Follow-up studies of patients with implanted cardiac pacemakers.
2. Literature related to patient teaching strategies.
Klug. D, et al (2004) studied 105patients who were admitted for local inflammatoryfindings, impending pacemaker lead exteriorization or overt infection. Aftersystematic lead extraction, the initial clinical presentation was related to the resultsof lead cultures. The findings of this prospective study were that regardless of theinitial presentation, the intravascular parts of the leads gave positive cultures in79.3% of patients. Additionally, 91.6% of the culture of extravascular lead segmentswere positive. Thus concluding that local complications at the site of pacemakerimplantation are usually associated with the infection of the intravascular part ofthe leads, with a risk of progressing to systemic infection. Such local symptomsshould prompt the extraction of leads even in the absence of other infectiousmanifestations.
/I
Preparing a ResearchProposal and a Term Paper
123
I

. .
Nursing InterventionModalities
Dwevedi SK et al (2001) ,carried out a prospective randontized study of twodurations of antibiotic prophylaxis to determine which one was more effective inpreventing infection following pacemaker implantation. One hundred and seventyeight patients undergoing permanent pacemaker implantation for the first time,were randomized to review short duration or long duration antibiotic prophylaxisfor 2 and 7 days respectively. They concluded that a short course of 48 hrs. ofantibiotic prophylaxis following permanent pacemaker implantation is as effectiveas longer course of 7 days.
"
,r't
Modar:azo (1~90) reported the study of 927 patients of both sexes with multi. programmable pacemaker implantation. Complications accounted were sepsis ofthe pocket, hematoma of the pocket, increased threshold and aseptic neurosis .
Nasker (1981) studied the learning needs of 40 patients with implanted cardiacpacemaker. The data was gathered using a semi-structured interview schedule.The findings indicated that highest percent of patients expressed their learning
. needs in the follow up area. This study showed the gap between the expressedlearning needs of patients with implanted cardiac pacemaker and nurses'participation in meeting those needs. The study also suggested that there wasmuch scope for improving patient teaching activities which should include learningneed to raise the self care status..-..Sheehan et al (1991) explained that educating cardiac patients in how to lead anactive life after a permanent pacemaker implant presents many challenges fornurses involved in their care. She further explained that suitable educational materialdelivered during both the inpatient and the outpatient phases of care, can fostera positive attitude and independence of these patients.
Methodology
Experimental approach is adopted in this study, since the study aims at evaluatingthe effects of a planned teaching programme on knowledge of cardiac patientsregarding self care of patients with implanted pacemaker.
Research Design * Research design selected for the study was a "pretestpost-test control group design".
Symbolic Representation
~ OK] OS] x OK2 OS2
Rc OK! OSl - OK20S2
RE = Experimental group randomly assigned & exposed to PlannedTeaching Programme (PTP)
Rc = Control group randomly assigned & not exposed to Planned TeachingProgramme (PTP)
x = Planned Teaching programme I & Il,
OK! = Knowledge pre test score.
OK2 = Knowledge post test' score.
OS! = Skill pre test score.124 OS2 = Skill post test score.
l
I/I
.rt
*This is only one example of research design. Other designs can alsobe used depending on type of study and the objectives you want toachieve Refer BNS031 BLOCK 6 unit 4 for other methods
"
Variables under study
Independent variable: In the present study independent variable is the plannedteaching programme on self care of patients following pacemaker implantationand Planned Teaching Programme (PTP) on radial pulse monitoring.
Dependent variable.
Dependent variables in the study are:
(a) The knowledge scores of patients on self care following pacemakerimplantation.
(b) Skill scores of patients for monitoring their radial pulse.
Setting of the Study: Investigator conducted the study at G.B.Pant HospitalNew Delhi.
Population: In the study the population comprises of all the patients who haveundergone cardiac pacemaker implantation at G.B.Pant Hospital, New Delhi andattending the pacemaker clinic.
Sample and Sampling technique: Sample is drawn out by using simple randomsampling technique. The names of patients were noted from the OPD registrationbook. These were randomly assigned to control and experimental groups byplacing each odd number to control group and even number to experimentalgroup sample.
Sample Size: A sample of 50 patients were taken. There were 25 subjects incontrol group & 25 subjects in experimental group.
Data collection tools: There were two tools developed for data collection:
• Structured knowledge questionnaire: To assess the knowledge of patientsregarding self care following pacemaker implantation.
• Observation checklist: To assess the skill of patients to monitor their radialpulse.
Content Validity: The initial drafts for the tools were given to nine experts forestablishing content validity. These experts were from the fields of cardiac nursingand cardiology.
Reliability of the tools: Reliability of the structured knowledge questionnairewas computed by using Kuder Richardson Formula -21. It was found to be(r = 0.7). The inter observer reliability of the observation checklist was computedby rank order correlation. It was found to be (p= 0.8).
Data analysis: The finding of the study are presented in three sections.
Section I: Findings on demographic characteristics of subjects.
//
Preparing a ResearchProposal and a Term Paper
125
I

Nursing InterventionModalities
Findings related to pre-test, post test knowledge and skill scoresof control and experimental group.
Section ill: Findings related to correlation between knowledge of patientsregarding self care following implantation and their skill to monitorradial pulse.
Section IT:
'..Table 8.1: Area-wise Mean, Mean Percentage of Pre and Post Test Knowledge Scores
of Subjects in Control and Experimental Group n = 50
"
Mean Percentage Mean Mean
S.No Learning No. Control Group Experimental % gain % gainneed areas of Group III
illItems control expen-
mentalPre Test Post Pre Post groupTest Test Test group
1. General 7 37.7 39.4 41.7 76 1.7 34.3Informationaboutpacemaker
2. Signs of 3 36 36 20 68 0 48batterydepletion andpacemakerfailure
3. Care of 5 24.8 25.6 35.2 74.4 0.8 39.2
IImplantationsite
--4. Precautions 10 26.4 27.6 26 60.8 1.2 34.8
to be .followed ,
..
Table 8.1 shows that the lowest mean pretest score for control group was 24.8in the area of "care of implantation site", followed by 26.4 in the area of "precautionsto be followed," 36 in the area of "signs of battery depletion and pacemakerfailure", and 37.7 in the area of "general information about pacemaker."
In the experimental group, maximum deficit area was related to "signs of batterydepletion & pacemaker failure" i.e. (20%) followed by "precautions to be followedafter implantation," "care of implantation site & general information aboutpacemaker. "
r
126
I
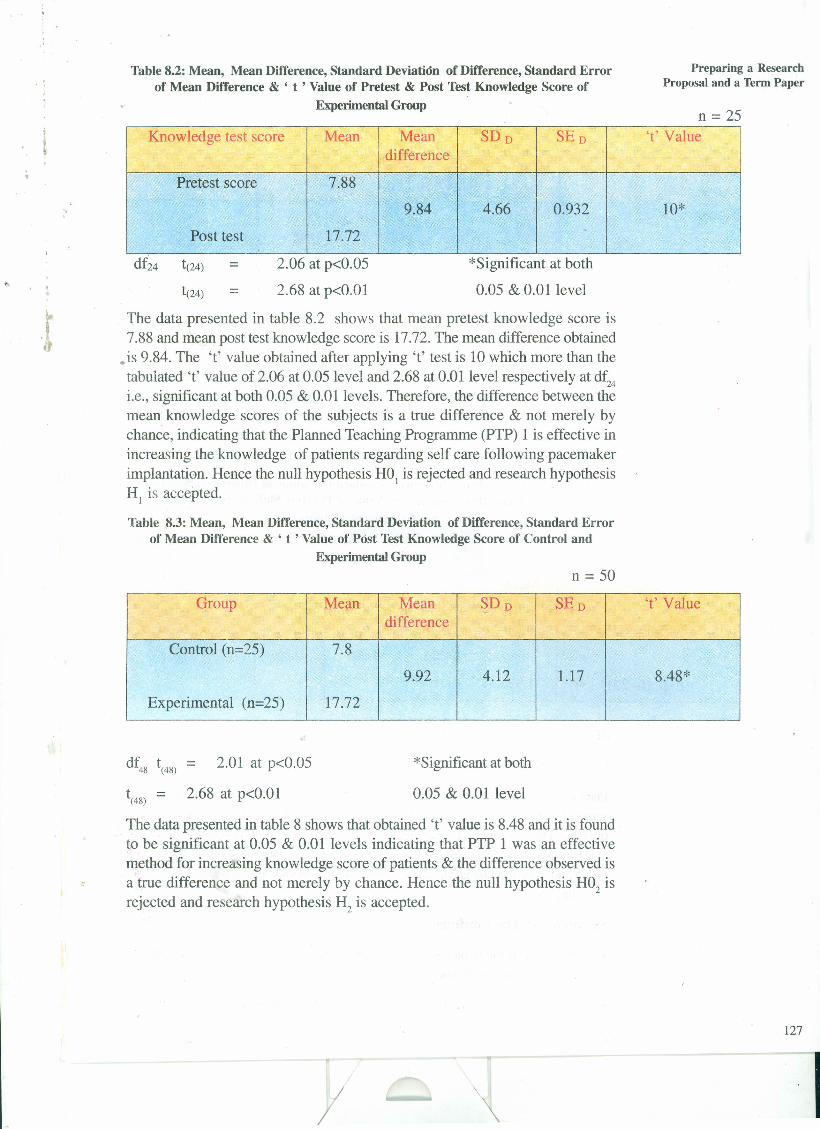
,•
Table 8.2: Mean, Mean Difference, Standard Deviation of Difference, Standard Errorof Mean Difference & ' t ' Value of Pretest & Post Test Knowledge Score of
Experimental Group
Preparing a ResearchProposal and a Term Paper
n = 25
'.
Knowledge test score Mean Mean SDD SED 't'Valuedifference
Pretest score 7.88
9.84 4.66 0.932 10*
Post test 17.72
2.06 at p<0.05
2.68 at p<O.Ol
*Significant at both
0.05 & 0.01 level==
The data presented in table 8.2 shows that mean pretest knowledge score is7.88 and mean post test knowledge score is 17.72. The mean difference obtained
• is 9.84. The '1' value obtained after applying 't' test is 10 which more than thetabulated '1' value of 2.06 at 0.05 level and 2.68 at 0.01 level respectively at df24i.e., significant at both 0.05 & 0.01 levels. Therefore, the difference between themean, knowledge scores of the subjects is a true difference & not merely bychance, indicating that the Planned Teaching Programme (PTP) 1 is effective inincreasing the knowledge of patients regarding self care following pacemakerimplantation. Hence the null hypothesis H01 is rejected and research hypothesisHI is accepted.
Table 8.3: Mean, Mean Difference, Standard Deviation of Difference, Standard Errorof Mean Difference & ' t ' Value of Post Test Knowledge Score of Control and
Experimental Groupn = 50
Group Mean Mean ~DD SED 't'Valuedifference
Control (n=25) 7.8
9.92 4.12 1.17 8.48*
Experimental (n=25) 17.72
df48 t(48)= 2.01 at p<0.05
t(48) = 2.68 at p<O.Ol
*Significant at both
0.05 & 0.01 level
The data presented in table 8 shows that obtained 't' value is 8.48 and it is foundto be significant at 0.05 & 0.01 levels indicating that PTP 1 was an effectivemethod for increasing knowledge score of patients & the difference observed isa true difference and not merely by chance. Hence the null hypothesis H02 isrejected and research hypothesis H2 is accepted.
127
//

Nursing InterventionModalities
Table 8.4: Mean, Mean Difference, Standard Deviation of Difference, StandardError of Mean Difference & ' t ' Value of Pre & Post Test Skill Score of
Experimental Group
n=25
'.Scores Mean Mean SDD SED 't'Value
difference
Pre test 1.92
5.36 2.29 0.46 11.65*
Post test 7.28
df24 t(24)= 2.06 at p<0.05
t(24)= 2.68 at p<O.Ol
*Significant at both
0.05 & 0.01 level
The data presented in table 8.4 shows that obtained 't' value is 11.65 which isfound to be significant at 0.05 & 0.01 levels. Hence the difference observed isa true difference & not merely by chance, indicating that the PTP was effectivein developing the skill of monitoring the radial pulse in the subjects. Hence Nullhypothesis H03 is rejected & research hypothesis ~ is accepted.
Table 8.5: Mean, Mean Difference, Standard Deviation of Difference, StandardError of Mean Difference & ' t ' Value of Pre Test Skill Score of Control
and Experimental Groups.
n=50 .
Groups Mean Mean SDof SED 't'Valuedifference Difference
Control (n=25) 1.88
0.04 1.29 0.36 1.52
Exp. (n:=25) 1.92.df48 t(48)= 2.01 at p<0.05
t(48)= 2.68 at p<O.Ol
Data presented in table 8.5 shows that the control group had a mean pretest skillscore of 1.88 and the experimental group a mean of 1.92, with a mean differenceof 0.04. The 't' value was computed and obtained as 1.52 which is not significant
r at 0.05 level ('t' = 2.01 at df48at p<0.05). Thus it is established that the controlgroup and experimentalgroup did not differinitiallyin their skillregardingmonitoringof radial pulse.
Not significant at 0.05
Summary of The Findings
• Majority of the subjects (48%) in both control and experimental group wereabove 60 years of age.
• As regards to sex distribution, majority of the subjects (66%) were male.
128
//
. "
• Majority ofthe subjects (74%) had undergone implantation of pacemakeronly once.
• Majority of the subjects (42% ) were dependent on their fa~ly.
• Majority of the subjects (44%) had Senior Secondary education and 38%of the subjects were graduates.
• Initially, both the groups i.e., control and experimental group did not differin their level of knowledge regarding self care following pacemakerimplantation with both having inadequate knowledge.
• Initially, both the groups did not differ in their level of skill to monitor theirradial pulse.
• The mean post test knowledge score was significantly higher than the meanpre-test knowledge score of experimental group indicating that PlannedTeaching Programme (PTP) I was effective in increasing their knowledgeregarding self care following pacemaker implantation.
• The mean post test skill score was significantly higher than the mean pretestskill score of Experimental group indicating that Planned Teaching Programme(PTP) IT was effective in developing their skill of monitoring radial pulse.
• The mean post test knowledge score of experimental group was significantlyhigher than the mean post test knowledge score of control group indicatingthat PTP I was effective in increasing their knowledge regarding self carefollowing pacemaker implantation.
• The maximum gain was obtained in the experimental group in the area of"Signs of Battery Depletion and pacemaker failure" followed by the areasof "Care of Implantation", "Precaution to be followed" and the area of"General information about pacemaker".
• There was a positive relationship between knowledge and skill scores.
• There was a significant positive relationship between the post test knowledgeand post test skill.
Conclusions
1. Knowledge deficit existed in all the areas of self care following pacemakerimplantation as evident from the pretest scores.
2. Initially, both the groups i.e., control and experimental group did not differin their level of knowledge regarding self care following pacemakerimplantation with both having inadequate knowledge.
3. Initially, both the groups did not differ in their level of skill to monitor theirradial pulse.
4. The Planned teaching programme I was found to be effective in increasingthe knowledge of cardiac patients regarding self care following pacemakerimplantation.
5. The PTP IT was found to be effective in developing the skill to monitor theirradial pulse.
/
Preparing a ResearchProposal and a Term Paper
129
Nursing InterventionModalities
6. Knowledge regarding' self care following pacemaker implantation hadenhanced the patients' skill to monitor their radial pulse.
,.
Implications
Findings of study revealed that most of the patients had knowledge deficit regardingself care and were unable to monitor their radial pulse which constitutes animportant aspect of self care activity. Therefore, there is a great scope for patientteaching activities in these areas by all categories of nurses. The patients shouldbe provided structured teaching regarding self care and they should be able to
.monitor their radial pulse, before they are discharged .
Since education is one of the powerful tools for developing awareness and healthteaching being an integral part of nursing practice, it should be developedsystematically and scientifically based on the needs of the target audience. Thiswill help to communicate the message appropriately and selectively for them tobe able to enhance their knowledge. The nurses should take interest, plan andconduct teaching programmes, apart from their incidental teaching.
Implication for Nursing Education
It is necessary to examine the existing nursing education in the light of presentneeds of the client and the profession. Specific cardiac nursing contents shouldbecome a component of all basic nursing curriculum as nurses will be dealing withincreased number of cardiac patients and their families. Essential contents neededfor professional management of such patients should be identified and integrated.There should be ongoing updation of contents in all the areas and evaluation.
Nurses who want to practice in cardiac setting and participate actively in care ofcardiac patients in prevention and control of disease must recognize, that therebasic nursing preparation need to be augmented by advanced knowledge oftheoretical and clinical aspects pertaining to cardiac care. Short terms specialitycourses in cardiac nursing should be undertaken by nurses to gain increasedknowledge and clinical expertise to provide specialized care for cardiac patientsand keep abreast of latest developments. There should be continuous updating oftheir knowledge through inservice or continuing education programmes.
Implications for Nursing Administration: The nurse administrators need todevelop ways and means of strengthening knowledge and skills of practicingnurses. Nursing staff should be provided with current knowledge and informationregarding care of patients with pacemaker.
Short term inservice education programme may be conducted which will enablethe nurses to update their knowledge and demonstrate high quality care. Nurseadministratorshould facilitatethe nurses to pursue continuingeducationprogrammes.
A health education cell may be established to take the responsibility of preparinghealth education material and conduct health education programmes pertaining tomajor health problems.
Implications for Nursing Research : There is lack of literature on teachingpatients with implanted cardiac pacemaker under condition existing in developingcountries. More studies can be done on developing different strategies for cardiacpatients education and their effectiveness. Studies can be done to find out the
"
. .
y130
patient satisfaction with the nursing care relating specifically to discharge advicesand patient teaching activities. Further studies can be done to determine theapplication of retained knowledge in the practice of self care and also to measurethe compliance behaviour.
Limitations
"
This study has certain limitations in generalizing its findings.
• The sample of the patients was taken from pacemaker clinic of one specialityhospital only. Therefore, generalization of the finding is limited to the patients-who were attending the pacemaker clinic of the hospital.
• The study was confined to a small number of patients due to limited populationand time limit for data collection.
• No attempt was made to determine the application of retained knowledgein the practice of self care and also to measure compliance behaviour.
Recommendations
On the basis of the findings of the study, it is recommended that:
• The study can be replicated on a large sample to validate the findings andmake generalization.
• A follow up study can be conducted to evaluate effectiveness of PTP inretention of knowledge.
• A study can be done to determine the application of retained knowledge inthe practice of self care and also to measure the compliance behaviour.
• An analysis can be done on nursing care activities related to patient's teachingat selected pacemaker clinic.
• Nurse's knowledge about teaching points for patients wit implanted cardiacpacemaker can be explored to determine their involvement in the productionof teaching material.
• A similar study can be done by using other teaching strategies for example,self-instructional Module etc.
Now you may study example as to how to write a term paper for this studyto be presented in a conference. Complete details of research study aregiven in previous section of this unit."
SAMPLE TERM PAPER
" A study to evaluate the effectiveness of planned teaching programme onknowledge regarding self care following pacemaker implantation and skillto monitor radial pulse in cardiac patients in a selected hospital of Delhi."
ABSTRACT
A study was conducted to evaluate the effectiveness of planned teaching programmeon knowledge regarding self care following pacemaker implantation and their skillto monitor radial pulse in cardiac patients in a selected hospital in Delhi,. TheObjectives of the study were: 1) To assess and evaluate the knowledge ofcardiac patients about selfcare after pacemaker implantation; 2) To assess and
y
Preparing a ResearchProposal and a Term Paper
131
"
,.
Nursing InterventionModalities
"
132
evaluate the skill of cardiac patients to monitor their radial pulse; 3) To developa planned teaching programme for patients with implanted cardiac pacemakerregarding selfcare & monitoring of radial pulse; 4) To assess the knowledgegained by patients after administering the planned teaching programme; 5) Toassess the skill developed by patients to monitor their radial pulse after administeringthe planned teaching programme; 6) To determine the relationship betweenknowledge & skill scores of patients with implanted pacemaker.
The conceptual framework adopted for the study was based on System's Model(from WHO, SEARO Publication,1985). The research approach adopted forthe study was experimental in nature. The research design used was pre-test posttest control group design. The study was carried out on 50 patients in G.B. PantHospital, New Delhi. A simple random sampling technique was used in selectingthe subjects. The data collection was done using two tools (a) Structured
, knowledge questionnaire and (b) Observation checklist. A planned teachingprogramme (intervention) was developed for the study. The data collection wasdone between 26th December, 2004 to 22nd January, 2005.
The findings revealed that after the administration of Planning Teaching Programme(PTP), the subjects belonging to the experimental group gained considerablysignificantly higher knowledge and skill scores than the control group subjects.This indicates that Planned Teaching Programme (PTP) was effective in increasingthe knowledge and skill of cardiac patients in monitoring radial pulse in theexperimental group.
The Major findings are :
• PTP I and II was effective in increasing the knowledge of experimentalgroup regarding self care following pacemaker implantation and in developingtheir skill of monitoring radial pulse.
• The maximum deficit in the pretest knowledge for the experimental groupwas in the area of 'signs & symptoms of Battery depletion and pacemakerfailure'. While in the control group it was in the area of 'Care of implantationsite' .
• The maximum gain was obtained in the experimental group in the area of"Signs of Battery Depletion and pacemaker failure" followed by the areasof "Care of Implantation", "Precaution to be followed" and the area of"General information about pacemaker".
r
• There was a significant positive relationship between the post test knowledgeand post test skill.
The conclusions drawn are (1)The Planned teaching programme was found tobe effective in increasing the knowledge of cardiac patients regarding selfcarefollowing pacemaker implantation and their skill to monitor their radial pulse.(2) Knowledge regarding selfcare following pacemaker implantation had enhancedthe patients' skill to monitor their radial pulse.
The researcher recommends for further studies to determine the application ofretained knowledge in the practice of self care and also to measure the compliancebehaviour, nursing care activities related to patient's teaching at selected pacemakerclinic, nurses' knowledge about teaching points for patients with implanted.
/
..J,
cardiac pacemaker to determine their involvement in the production of teachingmaterial.
Introduction
..
Dysrythmias are one of the major cardiac problems seen in our country and causeconsiderable morbidity and mortality. First degree atrioventricular block thoughtto be a relatively benign arrhythmia, can be associated with severe symptoms thatmay benefit from permanent pacing. Patients whose arrhythmia continue to beinducible inspite of antiarrhythmic therapy have a higher mortality rate (43%) thanthose patients whose arrhythmia are no longer inducible (9%).
The pacemaker has emerged as the preferred mode of therapy for most patientswho have life threatening arrhythmia. Today more than 1,50,000 pacemakers areimplanted each year in patients with variety of cardiac arrythmias.
Early complications of pacing include pneumothorax, lead perforation andventricular arrhythmia. Complications occurring later can include infection at theimplantation site, endocarditis, hematoma formation, thrombosis, skin erosion overpermanent pulse generator, pacemaker failure, lead dislodgement, Twiddler'sSyndrome and pacemaker syndrome. Despite these well known complications,accurate prospective data on implant complications are limited. The patients withpacemakers require close observation and teaching about post discharge selfcare. Lack of preventing programme results in increased number of deaths indeveloping countries.
Statement of the Problem
To evaluate the effectiveness of planned teaching programme on knowledgeregarding self care following pacemaker implantation and skill to monitor radialpulse in cardiac patients in a selected hospital of Delhi.
Objectives
• To assess and evaluate the knowledge of cardiac patients about self careafter pacemaker implantation.
• To assess and evaluate the skill of cardiac patients to monitor their radialpulse.
• To develop a planned teaching programme for patients with implanted cardiacpacemaker regarding self care and monitoring of radial pulse.
• To assess the knowledge gained by patients regarding self care afteradministering the planned teaching programme.
• To assess the skill gained by patients to monitor their radial pulse afteradministering the planned teaching programme.
• To determine the relationship between knowledge and skill scores of patientswith implanted pacemakers.
Delimitations - The Study was delimited to adult patients with implanted cardiacpacemaker in the age group of 20-70 years and Patients with implanted cardiacpacemaker attending the follow up clinic in a selected Hospital in Delhi.
/I
Preparing a ResearchProposal and a Term Paper
133
I

Nursing InterventionModalities
",, I
RE =.., Rc =,
,r X =OK =~ 1
OK =2
OSI =OS =2
,.
Sample & Sampling technique: Sample was drawn out by using simple randomsampling technique: The names of patients were noted from the OPD registrationbook. These were randomly assigned to control and experimental groups byplacing each odd number to control group and even number to experimentalgroup sample.
Sample Size: A sample of 50 patients were taken. There were 25 subjects incontrol group & 25 subjects in experimental group.
Data collection tools : There were two tools developed for data collection:
a) Structured knowledge questionnaire to assess the knowledge of patientsregarding self care following pacemaker implantation.
b) Observation checklist to assess the skill of patients to monitor their radialpulse.
Reliability of the tools: Reliability of the structured knowledge questionnairewas computed by using Kuder Richardson Formula -21. It was found to be134
II I
" ,J,
(r = 0.7). The inter observer reliability of the observation checklist was computedby rank order correlation. It was found to be (p = 0.8~.
Results: The findings of the study are presented in three sections.
Section I: Findings on demographic characteristics of subjects.
Section IT: Findings related to pre-test, post test knowledge and skill scoresof control and experimental group.
Section ill: Findings related to correlation between knowledge of patientsregarding self care following implantation and their skill to monitorradial pulse.
Preparing a ResearchProposal and a Term Paper
"Table 8.1: Area-I wise Mean, Mean Percentage of Pre and Post Test Knowledge
Scores of Subjects in Control and Experimental Group
Mean Percentage Mean Mean
S.No. Learning No. Control Group Experimental % gain % gainneed areas of Group III
IIIItems control experi-
- mentalPre Test Post Pre Post groupTest Test Test group
1. General 7 37.7 39.4 41.7 76 1.7 34.3Informationaboutpacemaker
2. Signs of 3 36 36 20 68 0 48batterydepletionandpacemakerfailure
3. Care of 5 24.8 25.6 35.2 74.4 0.8 39.2Implantationsite
4. Precautions 10 26.4 27.6 26 60.8 1.2 34.8to befollowed
Table 8.1 shows that the experimental group, maximum deficit area was relatedto "signs of battery depletion & pacemaker failure" i.e. (20%) followed by"precautions to be followed after implantation," "care of implantation site & generalinformation about pacemaker."
135
// I

Nursing InterventionModalities
Table 8.2: Mean, Mean Difference, Standard Deviation of Difference, Standard Errorof Mean Difference & ' t ' Value of Pretest & Post Test Knowledge Score of
Experimental Group
n = 25
".Knowledge test score Mean Mean SDD SED 't'Value
difference
Pretest score 7.88
9.84 4.66 0.932 10*
Post test 17.72
df24 t(24)= 2.06 at p<0.05
t(24)= 2.68 at p<O.OI
"Significant at both
0.05 & 0.01 level
The data presented in table 8.2 shows that mean pretest knowledge score is7.88 and mean post test knowledge score is 17.72. The mean difference obtainedis 9.84. The 't' value obtained after applying 't' test is 10 which more than thetabulated 't' value of 2.06 at 0.05 level and 2.68 at 0.01 level respectively at df24i.e. significant at both 0.05 & 0.01 levels. It indicates that the PTP 1 is effectivein increasing the knowledge of patients regarding self care following pacemakerimplantation.
Table 8.3: Mean, Mean Difference, Standard Deviation of Difference, Standard Errorof Mean Difference & ' t ' Value of Post Test Knowledge Score of Control and
Experimental Group
n = 50
Group Mean Mean I SDD SED 't'difference Value
I
Control (n=25) 7.8
9.92 4.12 1.17 8.48*
Experimental (n=25) 17.72I
df48 t(48)= 2.01 at p<0.05
t(48)= 2.68 at p<O.OI
*Significant at both
0.05 & 0.01 level
Thedata presented in table 8.3 shows that obtained 't' value is 8.48 and it isfound to be significant at 0.05 & 0.01 levels indicating that PTP 1 was an effectivemethod for increasing knowledge score of patients.
136
/I
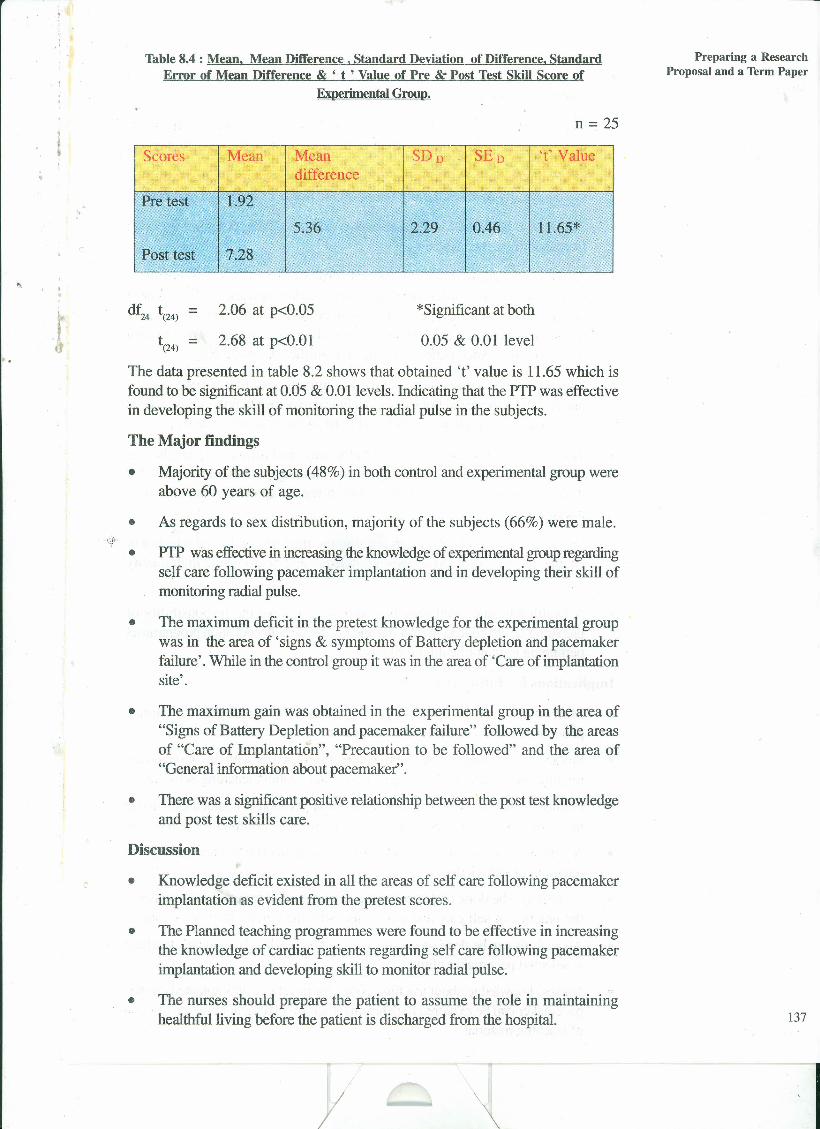
-' ,),
Table 8.4 : Mean. Mean Difference, Standard Deviation of Difference. StandardError of Mean Difference & ' t ' Value of Pre & Post Test Skill Score of
Experimental Group.
n = 25
"
Scores Mean Mean SDD SED 't'Valuedifference
Pre test 1.92
5.36 2.29 0.46 11.65*
Post test 7.28
df24 t(24)= 2.06 at p<0.05
t(24)= 2.68 at p<O.Ol
*Significantatbotll
0.05 & 0.01 level
The data presented in table 8.2 shows that obtained 't' value is 11.65 which isfound to be significant at 0.05 & 0.01 levels. Indicating that the PTP was effectivein developing tlle skill of monitoring the radial pulse in the subjects.
The Major findings
• Majority of the subjects (48%) in both control and experimental group wereabove 60 years of age.
• As regards to sex distribution, majority of the subjects (66%) were male.
PIP was effectivein increasing the knowledge of experimentalgroup regardingself care following pacemaker implantation and in developing their skill ofmonitoring radial pulse.
• The maximum deficit in the pretest knowledge for the experimental groupwas in the area of 'signs & symptoms of Battery depletion and pacemakerfailure'. While in the control group it was in the area of 'Care of implantationsite'.
•
• The maximum gain was obtained in the experimental group in the area of"Signs of Battery Depletion and pacemaker failure" followed by the areasof "Care of Implantation", "Precaution to be followed" and the area of"General information about pacemaker".
• There was a significant positive relationship between the post test knowledgeand post test skills care.
Discussion
• Knowledge deficit existed in all the areas of self care following pacemakerimplantation as evident from the pretest scores.
• The Planned teaching programmes were found to be effective in increasingthe knowledge of cardiac patients regarding self care following pacemakerimplantation and developing skill to monitor radial pulse.
• The nurses should prepare the patient to assume the role in maintaininghealthful living before the patient is discharged from the hospital.
/ \
Preparing a ResearchProposal and a Term Paper
137


. .
8.4 CRITIQUE
"
In the previous section you have learnt as to how to write ~esearch study and itspresentation as a term paper, now you will study critique guidelines and check listfor critiquing a research study.
8.4.1 Meaning of critiquingIt is the examination of all parts of research study to high light the strong and weakpoints of a given research study, with the intention of assigning value to the study.
The use of evidence based practice is undoubtedly justified by professionals.Research evidence is the most critical component of evidence based practice, butit is necessary that one must be able to evaluate this evidence before incorporatingit in practice. Hence you should develop good critiquing skills .
All research articles have strong and weak points. Generally, the best way toconduct a critique review is to read the entire study and make an initial evaluationof the report followed by in-depth evaluation of each part of the study.
Some of the guidelines for evaluating research reports are given below. Manyother guidelines could be used. Many a times there are no right or wrong answerswhen evaluating reports. Even experts may disagree about certain aspects of aparticular study. The guide lines for critique are as follows:
8.4.2 Guidelines for critiquing• Comment on the study's strengths as well as weaknesses.
• Offer a rationale for how a different approach would have solved a problemwhich a researcher has failed to address.
• Be objective. Do not be overly critical.
• Suggest alternatives that the researcher might want to consider. Offer somepractical recommendation or solutions.
• The study should be conducted by a person who is from the same field orprofession. The academic credentials after the name will give educationalbackground and research skins of the researcher.
• The title should contain the critical words or phrases that describe the researchproject. Title should be clear, concise and not loaded with too many words.
• Abstract should briefly describe the essential components of the study-question or the hypotheses, methods, description of subjects and majorfindings.
• The introduction should be interestingly written to catch the attention of thereader. Background information on the problem and significance of nursingneeds must be addressed.
8.4.3 Checklist for critiquing a study• The purpose of the study is stated clearly and explicitly.
• The importance of the study is projected in the introduction through goodliterature review.
II
Preparing a ResearchProposal and a Term Paper
139
,.
..
Nursing InterventionModalities
• The research problem pas significance for clinical practice in nursing.
• The research question is appropriate, refined, and focuses on a single concept.
• The research question includes sufficient detail to identify the population,what will be measured and how and where it will be measured.
• The literature review relies primarily on most recent and relevant studies
" • The review provides support for the importance of the study.
• The review is unbiased and includes both conclusive and inconsistent findings.
• The review is organized so that a logical unfolding of ideas is apparent.
• The design is appropriate for the study.
• It is clearly identified.
• A rationale is provided for the choice of a design, and it is linked to theresearch question
• Data collection instrument and measures are described objectively.
• The measures for reliability and validity of the data collecting instruments areprovided.
• Sampling procedures are likely to produce a representative sample.
• The sample size is adequate.
• Data is subjected to appropriate statistical tests to meet the study objectives.
• Data is appropriately analyzed following statistical inferences and organizedin presentation.
• The findings of the study are presented in a logical order.
• The conclusion, limitations and implications are appropriately deducted.
• The summary includes brief description of the total research study undertaken.It describes tbe statement, objectives, methodology, tools or instruments fordata collection, major findings, conclusion, implications in nursing andrecommendations.
140
ii) What are the broad headings for writing a term paper for a research study?
Check Your Progress 2
i) Discuss the aspects of time management that you should observe inaccomplishment of a project.
/ I

,.
. ' ,),
,r.,
.;. . ~ ;.
..................................................................................................................
iii) Explain the meaning of critiquing.
8.4.4' Sample of research critiquingIn the previous sections of this practical, you have studied about planning andpreparation of project for the research study to be conducted and its presentationin the form of term paper and the critical review of research study along withguidelines and check list for critiquing.
In this section you will learn about the sample of critiquing a research study.Consider the same study as given at 8.4.4 of this Practical. An example ofcritiquing t:m'sstudy is given below:
"A study to evaluate the effectiveness of planned teaching programme onknowledge regarding self care following pacemaker implantation and skillto monitor radial pulse in cardiac patients in a selected hospital of Delhi."
The author provides support for the importance of the study by documenting theseverity of the problem and by presenting evidence that makes a logical linkbetween the background of the problem and need of the study. The literatureserves as an evidence to provide the basis for the hypothesis that intervention ofplanned teaching programme can have effect on the expected outcome of selfcare behaviour in the group. The objectives are clearly stated. They are measurableand concisely formulated. The author is clear in mind, as to what to measure andhow to proceed for the study. The study is based on System's model. Therationale given is the use of an intervention though planned teaching programme.However, Orem's self care deficit theory could be used as the aspect measuredis patients' self care behaviour. The authorclearly defines the inclusion criteria andthe exclusion criteria in the delimitation and sample description.
The author applies experimental design, essentially comparing the interventiongroup to control group. The variables are defined and randornized sampling helpsto control the bias. The subjects were randomly assigned to the groups so thatit can be stated that any variable that can affect the outcome variable is evenlydistributed. These are the strong characteristics of the study. The sample size isjust adequate to apply the inferential statistics. It is not sufficient to drawgeneralization.
The reliability of the tool obtained is appropriately established. the actual reliabilityscore is also mentioned which enables the reviewer to judge the amount of
/ \
Preparing a ResearchProposal and a Term Paper
141
I
..
Nursing InterventionModalities
measurement error. The methods of data collection are described. The interventionis well described. The content of the planned teaching programme is validated.The procedure of intervention introduction is explained.
"
The data analysis is well planned and findings well organized. The data analysisstarts with the comparison of the two groups (control and experimental) in termsof the outcome variable i.e., knowledge score. This establishes that both thegroups were identical or comparable and therefore the effect of the independentvariable Planned Teaching Programme (PTP) is a true effect and not because ofthe group differences. The data presented in the tables show the p values that. .
. show the statistical significance i.e. the differences reported are true and not bychance. This is a proper way of reporting the data. The author has also mentionedthe standard deviation of the group to show the heterogeneity of the group. Therelationship between the knowledge and practice is established by an appropriatetest Product Moment Coefficient of Correlation. The findings are appropriatelyexplained after each table. It would have been further illustrative if the findings arepresented in pictorials, graphs or figures or diagrams to make it more attractive.
The author has done a good job of summarizing the statistical findings so that themost important conclusions of the study are easily drawn. The author hasstraightforwardly mentioned the limitations and has stated that the findings can notbe generalized. The implications for nursing practice, administration, educationand research are well explained.
8.5 I"ETUS SUM UPToday research is an integral part of clinical practice in nursing with well acceptedfact that quality nursing care and nursing research go hand in hand. A betterunderstanding of research paves way for your involvement in collecting empiricalevidence. In the first section of this practical you have learnt how you can writea good proposal and the criteria for a good proposal. In the second section wehave discussed that how should you proceed in carrying out a project. In the thirdsection of the unit we have learnt about writing a term paper and preparing fora paper presentation. The fourth section of this unit deals with skills of critiquing.It will help you to evaluate the quality of a study and thus the clinical evidence.
Nursing research requires a tremendous effort on the part of a practicing nurseresearchers. The knowledge gained through the study should be communicated toa larger audience to bring in valuable changes in nursing practice.
8.6 ANSWERS TO CHECK YOUR PROGRESSCheck Your Progress 1
i) Proposals prepared for different projects vary in the amount of detail buthave similar content outline for research proposals, which are as follows :
• Introduction
• Background
• Need for the study
142 • Statement of the problem
/ II

• Objectives
• Operational definitions
• Conceptual framework
• Assumption, Delimitations
• Research methodology-variables, research approach, setting, samplingcriteria and technique, data collection procedure, plan of data analysis."
• Finance of the project
"- • Proposed project timetable
.1 • Outline of the report
• Reference:.,• Appendices
Check Your Progress 2
i) • Keep detailed notes as you progress through your project
• Be disciplined in your approach
• Be systematic. Do not leave things for the last hour
• Keep in touch with your supervisor
• Divide complex and demanding tasks into more easily programmablesubtasks
• Don't overload. Make accurate estimate of time needed
• Revise your plan regularly
• Finish task before writing text or report
ii) Abstract, introduction, literature review, methods, results, discussion,implications for future research.
iii) It is the examination of all parts of research study to highlight the strong andweak points of a given research study with an intention of assigning a valueto the study.
8.7 ACTIVITIESSelect a problem in any area
Write the Problem Statment
Prepare a brief Proposal
Collect the data and analyse the data
Write a brief report.
ii) Select a research article published in any nursing journal. Critique the studybased on guidelines given in Practical Manual ..
i)
/
Preparing a ResearchProposal and a Term Paper
143
I

,.
".
• I
I~,L
,.
/I
NOTES.
.J.:"
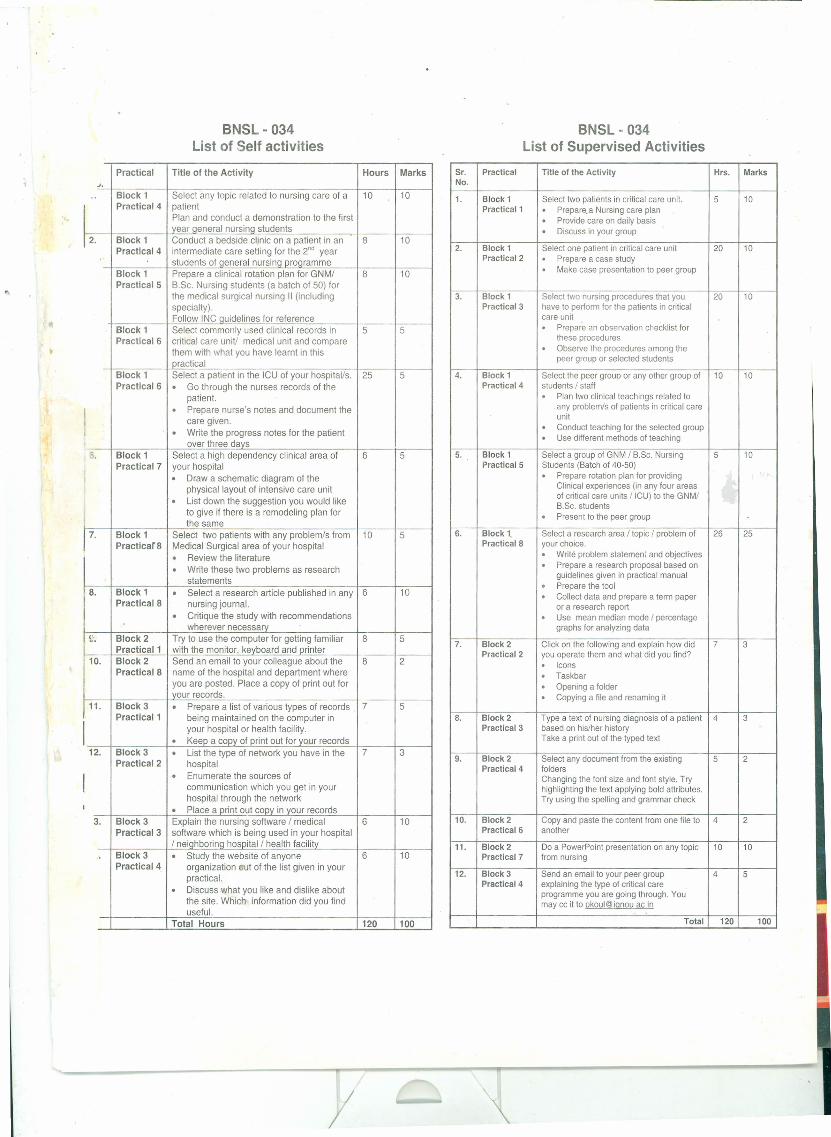
BNSL·034List of Self activities
Practical Title of the Activity Hours MarksJ.
.. Block 1 Select any topic related to nursing care of a 10 10Practical 4 patient
Plan and conduct a demonstration to the firstyear qeneral nursinq students
2. Block 1 Conduct a bedside clinic on a patient in an 8 10Practical 4 intermediate care setting for the 2nd year
students of aeneral nursina proarammeBlock 1 Prepare a clinical rotation plan for GNM/ 8 10Practical 5 B.Sc. Nursing students (a batch of 50) for
the medical surgical nursing 11 (includingspecialty).Follow INC auidelines for reference
Block 1 Select commonly used clinical records in 5 5Practical 6 critical care unit! medical unit and compare
them with what you have learnt in thispractical
Block 1 Select a patient in the ICU of your hospital/s. 25 5Practical 6 · Go through the nurses records of the
patient.· Prepare nurse's notes and document thecare given.· Write the progress notes for the patientover three davs
~. Block 1 Select a high dependency clinical area of 6 5Practical 7 your hospital· Draw a schematic diagram of the
physical layout of intensive care unit· List down the suggestion you would liketo give if there is a remodeling plan forthe same
17.Block 1 Select two patients with any problem/s from 10 5PracticarB Medical Surgical area of your hospital· Review the literature· Write these two problems as research
statementsB. Block 1 · Select a research article published in any 6 10
PracticalB nursing journal.· Critique the study with recommendationswherevernecessa~
£'. Block 2 Try to use the computer for getting familiar 8 5I Practical 1 with the monitor, kevboard and printer
10. Block 2 Send an email to your colleague about the 8 2PracticalB name of the hospital and department where
you are posted. Place a copy of print out foryour records.
11. Block 3 · Prepare a list of various types of records 7 5Practical 1 being maintained on the computer in
I your hospital or health facility.· Keep a copy of print out for your records12. Block 3 · List the type of network you have in the 7 3
Practical 2 hospital
I · Enumerate the sources ofcommunication which you get in yourhospital through the network
I · Place a print out COpy in your records3. Block 3 Explain the nursing software / medical 6 10
Practical 3 software which is being used in your hospital/ neiahborina hosoital / health facilitv
Block 3 · Study the website of anyone 6 10Practical 4 organization eut of the list given in your
practical.· Discuss what you like and dislike aboutthe site. Which information did you finduseful.
Total Hours 120 100
BNSL·034List of Supervised Activities
Sr. Practical Title of the Activity Hrs. MarksNo.
1. Block 1 Select two patients in critical care unit. 5 10Practical 1 · Prepare.a Nursing care plan· Provide care on daily basis· Discuss in your group
2. Block 1 Select one patient in critical care unit 20 10Practical 2 · Prepare a case study· Make case presentation to peer group
3. Block 1 Select two nursing procedures that you 20 10Practical 3 have to pertorm for the patients in critical
care unit· Prepare an observation checklist forthese procedures· Observe the procedures among thepeer group or selected students
4. Block 1 Select the peer group or any other group of 10 10Practical 4 students / staff· Plan two clinical teachings related to
any problem/s of patients in critical careunit· Conduct teaching for the selected group· Use different methods of teaching
5. Block 1 Select a group of GNM / B.Sc. Nursing 5 10Practical 5 Students (Batch of 40-50)· Prepare rotation plan for providing
Clinical experiences (in any four areasof critical care units / ICU) to the GNM/B.Sc. students· Present to the peer group
6. Block 1. Select a research area / topic / problem of 26 25PracticalS your choice.· Write problem statement and objectives· Prepare a research proposal based on
guidelines given in practical manual· Prepare the tool· Collect data and prepare a term paperor a research report· Use mean median mode / percentagegraphs for analyzing data
7. Block 2 Click on the following and explain how did ? 3Practical 2 you operate them and what did you find?· Icons· Taskbar· Opening a folder· Copying a file and renaming it
S. Block 2 Type a text of nursing diagnosis of a patient 4 3Practical 3 based on his/her history
Take a print out of the typed text
9. Block 2 Select any document from the existing 5 2Practical 4 folders
Changing the font size and font style. Tryhighlighting the text applying bold attributes.Try using the spelling and grammar check
10. Block 2 Copy and paste the content from one file to 4 2Practical 6 another
11. Block 2 Do a PowerPoint presentation on any topic 10 10Practical? from nursing
12. Block 3 Send an email to your peer group 4 5Practical 4 explaining the type of critical care
programme you are going through. Youmay cc it to pkoul@ignou ac in
Total 120 100
"
BNSL - 034 Clinical Nursing Practice in Critical Care -nBlock 1 - Nursing Intervention Modalities
Practical- 1 Nursing Care Plan
Practical - 2 Nursing case study / case presentation
Practical - 3 Observation Checklist
Practical - 4 Conducting Clinical Teaching
Practical - 5 Preparing a Clinical Rotation Plan
Practical - 6 Patient Care Documentation, Records and Reports t.
Practical - 7 Design of Critical Care Unit
Practical - 8 Developing a Research Proposal And Term Paper
Block 2 - Introduction to Computer Basics
Practical- 1 Introduction to Computers
Practical - 2 Microsoft Windows
Practical - 3 MS Word : Part I
Practical - 4 MS Word : Part I
Practical - 5 Introduction to Spreadsheets
Practical - 6 MS Excel Toolbars
Practical- 7 MS Power Point
Practical- 8 Internet and E-mailing
Block 3 - Application of Computers in Nursing
Practical - 1 Computerization in Nursing
Practical- 2 Networking for Hospitals and Clinic
Practical - 3 Electronic Patient Records
Practical- 4 Internet and Nursing
y





























