Embed Size (px)
Citation preview

The key actor a qualitative study
of patient participation in the handover
process in Europe
Maria Flink12 Gijs Hesselink3 Loes Pijnenborg4 Hub Wollersheim3
Myrra Vernooij-Dassen356 Ewa Dudzik-Urbaniak7 Carola Orrego8
Giulio Toccafondi9 Lisette Schoonhoven310 Petra J Gademan11 Julie
K Johnson12 Gunnar Oumlhleacuten1314 Helen Hansagi15 Mariann Olsson12
Paul Barach1617 on behalf of the European HANDOVER Research Collaborative
For numbered affiliations seeend of article
Correspondence toMaria Flink Department ofNeurobiology Care Sciencesand Society KarolinskaInstitutet B44 KarolinskaSjukhuset HuddingeStockholm 14186 Swedenmariaflinkkise
Accepted 25 August 2012
ABSTRACTBackground Patient safety experts have postulated thatincreasing patient participation in communications duringpatient handovers will improve the quality of patienttransitions and that this may reduce hospital readmissionsChoosing strategies that enhance patient safety throughimproved handovers requires better understanding ofpatient experiences and preferences for participationObjective The aim of this paper is to explore the patientsrsquoexperiences and perspectives related to the handoversbetween their primary care providers and the inpatienthospitalMethods A qualitative secondary analysis was performedbased on individual and focus group patient interviews with90 patients in five European countriesResults The analysis revealed three themes patientpositioning in the handover process prerequisites forpatient participation and patient preferences for thehandover process Patientsrsquo participation ranged from beingthe key actor to sharing the responsibility with healthcareprofessional(s) to being passive participants For activeparticipation patients required both personal and socialresources as well as prerequisites such as information andrespect Some patients preferred to be the key actor incharge others preferred their healthcare professionals to bethe key actors in the handoverConclusions Patientsrsquo participation is related to thehealthcare system the activity of healthcare professionalsrsquoand patientsrsquo capacity for participation Patients prefer ahandover process where the responsibility is clear andunambiguous Healthcare organisations need a clear andwell-considered system of responsibility for handoverprocesses that takes into account the individual patientrsquosneed of clarity and support in relation to hishers ownrecourses
INTRODUCTION
Each transition of care including the hand-over between the inpatient hospital and thepatientrsquos home and primary care setting is a
potential threat to patient safety1 Severalstudies have found that a suboptimal patienthandover at hospital admission or dischargemay lead to adverse events with this contrib-uting to suboptimal care rehospitalisationand even death1ndash5 Deficits in handover areoften related to inadequate communicationbetween healthcare professionals with insuf-ficient or unclear information exchangedbetween the hospital and primary careprofessionals3
Safe and effective transitions of carebetween care settings require healthcare pro-fessionals that give clear unambiguous andunderstandable information to patients6 7
Some handover communication involves notonly the healthcare professionals transition-ing the patient from one phase of care to thenext but also the patient Improvements inhospital to primary care handovers thatactively include the patient in the exchangeof information between settings and health-care professionals have been associated withreduced rehospitalisation8 9 and faster deliv-ery of information to primary healthcareprofessionals3
While the knowledge about ways toimprove the hospital to primary care hand-over continuum is increasing there are fewstudies that have examined patient participa-tion in handovers The factors behind patientparticipation in the larger domain of health-care decision-making have been studiedPatients differ in their participation indecision-making based on demographicssuch as age10 health literacy10 11 nationalculture12 and expectations for participa-tion13 Improved knowledge about howpatients experience their participation in
OPEN ACCESS
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 1
Original research
BMJ Quality amp Safety Online First published on 30 October 2012 as 101136bmjqs-2012-001171
Copyright Article author (or their employer) 2012 Produced by BMJ Publishing Group Ltd under licence
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
handover processes between community and hospitalcare may help in finding optimal ways of empoweringpatients that will improve the quality and safety of hand-overs This study aims to explore the experiences andperspectives of patients with chronic diseases in regardsto their participation in handover communicationbetween primary and secondary healthcare in fiveEuropean countries
METHODS
Study design and settingsThis study is a secondary analysis of data from a cross-national qualitative study of patient perspectives ontheir handovers conducted at nine hospitals and theirfeeder primary healthcare systems in the NetherlandsSpain Poland Italy and Sweden The settings werechosen to include different regional healthcare systemsand hospitals of different sizes The study was conductedas part of the European HANDOVER Project thatresearched handovers between primary and secondarycare and examined the perspectives of a wide group ofstakeholders in the transition of care between theinpatient hospital and the primary care and communitysetting (FP7-HEALTH-F2ndash2008-223409)14
Primary study populationPatients in the HANDOVER Project encompassed adultswith a chronic disease (diabetes mellitus chronicobstructive pulmonary disease (COPD) heart failure
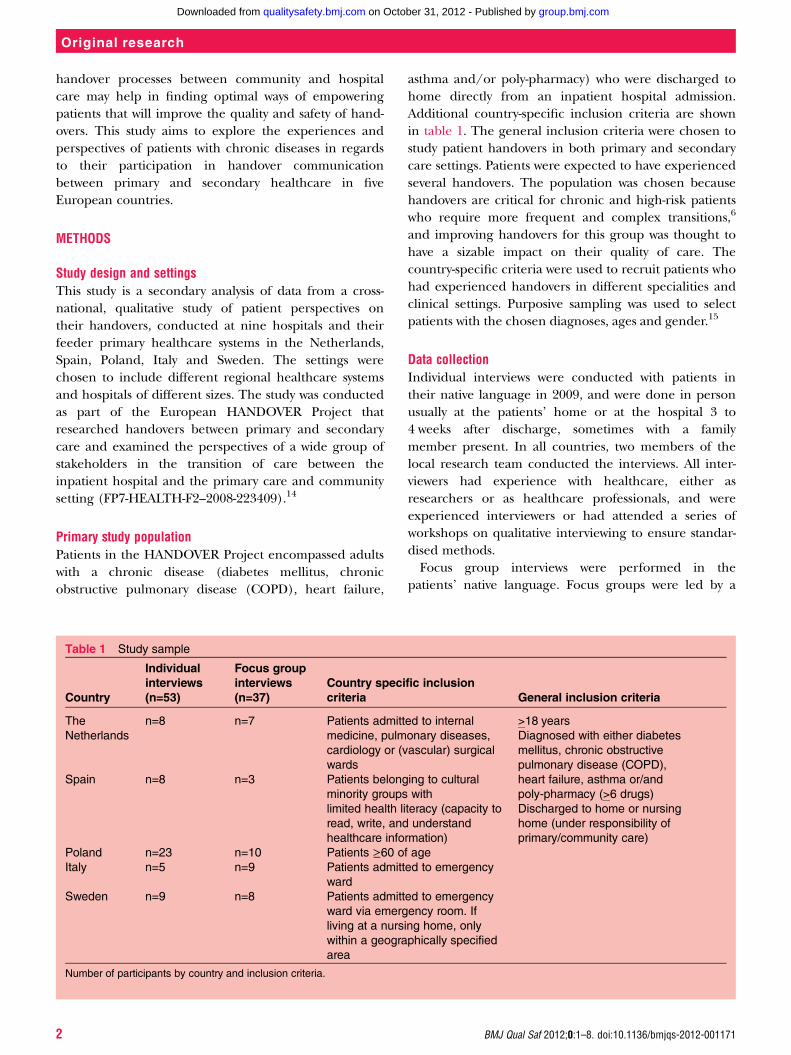
asthma andor poly-pharmacy) who were discharged tohome directly from an inpatient hospital admissionAdditional country-specific inclusion criteria are shownin table 1 The general inclusion criteria were chosen tostudy patient handovers in both primary and secondarycare settings Patients were expected to have experiencedseveral handovers The population was chosen becausehandovers are critical for chronic and high-risk patientswho require more frequent and complex transitions6
and improving handovers for this group was thought tohave a sizable impact on their quality of care Thecountry-specific criteria were used to recruit patients whohad experienced handovers in different specialities andclinical settings Purposive sampling was used to selectpatients with the chosen diagnoses ages and gender15
Data collectionIndividual interviews were conducted with patients intheir native language in 2009 and were done in personusually at the patientsrsquo home or at the hospital 3 to4 weeks after discharge sometimes with a familymember present In all countries two members of thelocal research team conducted the interviews All inter-viewers had experience with healthcare either asresearchers or as healthcare professionals and wereexperienced interviewers or had attended a series ofworkshops on qualitative interviewing to ensure standar-dised methodsFocus group interviews were performed in the
patientsrsquo native language Focus groups were led by a
Table 1 Study sample
Country
Individual
interviews
(n=53)
Focus group
interviews
(n=37)
Country specific inclusion
criteria General inclusion criteria
The
Netherlands
n=8 n=7 Patients admitted to internal
medicine pulmonary diseases
cardiology or (vascular) surgical
wards
gt18 years
Diagnosed with either diabetes
mellitus chronic obstructive
pulmonary disease (COPD)
heart failure asthma orand
poly-pharmacy (gt6 drugs)
Discharged to home or nursing
home (under responsibility of
primarycommunity care)
Spain n=8 n=3 Patients belonging to cultural
minority groups with
limited health literacy (capacity to
read write and understand
healthcare information)
Poland n=23 n=10 Patients ge60 of age
Italy n=5 n=9 Patients admitted to emergency
ward
Sweden n=9 n=8 Patients admitted to emergency
ward via emergency room If
living at a nursing home only
within a geographically specified
area
Number of participants by country and inclusion criteria
2 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
trained moderator and had one or two observers whomade field notes and added question prompts All inter-views were audio-taped and transcribed verbatim in thelocal language according to a jointly decided standar-dised formatBoth individual and focus groups interviews used a
semistructured interview guide developed in English bythe HANDOVER Project researchers and translated intothe local language of the research groups16 The inter-view guide covered these areas of interest Experience with recent handovers (appreciative
problematic situations and consequences) Perceptions about handovers in general (ie experi-
ences attitudes methods tools barriers facilitators) Perceptions about providerpatient tasks roles and
responsibilities Suggestions for improving patient handoversThe guide was piloted in each country and when
necessary adjusted for local conditions and needs (avail-able upon request)A quality assurance protocol17 based on BMJ criteria18
and on criteria presented by Tong et al15 was developed(by MVD and JKJ) and used to ensure trustworthinessthroughout the data collection and data analysesRequirements for informed consent and other ethicaland legal requirements for research using patient infor-mation were fulfilled at all study sites
Sample for secondary analysisFor the secondary analysis data were extracted frompatient interviews in the five countries participating inthe HANDOVER Project The sample consisted of 90patients 53 individually interviewed (55 of the overallsample of patients interviewed individually for the ori-ginal studies conducted as part of the HANDOVERProject) and 37 interviewed in focus groups (100 ofthe overall sample of patients interviewed in groups)
The distribution across countries is shown in table 1Where the gender distribution of the primary samplewas reported it included approximately equal numbersof male and female patients
Data analysisThe analysis consisted of two main parts analysis ofinterviews at the national level and a secondary ana-lysis19 of the cross-national data (see figure 1)
Analysis at national levelTwo interviews from each country were translated intoEnglish and coded inductively using a modifiedgrounded theory approach of Corbin and Strauss20 Aqualitative data analysis software (Atlasti) was used tofacilitate storing coding and indexing of the data21 Theresearchers created a codebook based on codes gener-ated in each country The codebook consisted of thecode and an operational definition both of which wereagreed upon during regularly scheduled conference-calls and face to face meetings and was used for analysisof both individual and focus group interviews Tworesearchers in each country analysed their countryrsquos datain parallel with the data collection and continued tocollect data until conceptual saturation was reached andno new codes or categories were generated20 Localreports were written in English by one or two of theresearchers in each country and used for compiled ana-lyses for the European HANDOVER Project studiesThese studies focused on barriers and facilitators toeffective handovers patient roles and responsibilitiesand patient-centredness and participation culture16 22 23
Secondary analysisThe local reports including quotes from the individualinterviews and focus groups were used for the
Figure 1 Proceduremdashfrom data collection to the current secondary analysis
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 3
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
secondary analysis which focused on patientsrsquo perspec-tive on their own participation in handovers Thus thissecondary analysis seeks to answer a new research ques-tion19 using data that was already collectedLocal reports were analysed using a qualitative induct-
ive content analysis as described by Hsieh andShannon24 Two authors (MF MO) coded the texts inopen coding and three authors (MF MO GH) sortedthe codes into categories and themes Validity checkinginvolved all authors of the local reports who reviewedthe findings to ensure they were consistent with the ori-ginal interview data
RESULTS
The data analysis resulted in eight categories fromwhich three themes were developed (1) patient position-ing in the handover process (2) prerequisites for patient partici-pation and (3) patient preferences for the handover process(see table 2)
Patient positioning in the handover processThree types of patient experiences form the categoriesunder this theme (a) patients as the key actors in thehandover process (b) patients sharing the responsibilityfor the handover with healthcare professionals and (c)healthcare professionals functioning as the key actors inthe handover process
Patients as the key actors in the handover processPatients assumed the responsibility for the handovercommunication including establishing contact with thenext care unit as well as the responsibility for collectingstoring and handing over essential information for man-aging their care such as medication lists or dischargenotes For example when a healthcare professional inthe hospital setting in Italy wrote the discharge note totransition the patient to the primary care settingmdashthisdischarge note was given to the patient for delivery tothe general practitioner The key actor positioning wasmost explicitly stated by the geriatric patients in Polandwho noted they needed to take responsibility in organis-ing the handovers as well as being couriersPatients who functioned as key actors perceived their
active involvement was required for an effective hand-over and to ensure continuity of care These patientshad either learned from past experiences that little orno information was transferred unless they did it them-selves or perceived that healthcare professionalsexpected them to assume the initiative and be activeduring their handovers
Patient Poland ldquoWell we all know by now that it[general practitioner ndash hospital communication] doesnrsquotexist You want a referralmdashthen you get it Then Iarrange my admissionmdashneither my general practitionernor hospital physician care helliprdquo
Being the key actor could cause some patients toblame themselves for not fulfilling the task of facilitatingthe handover when information was lacking betweencare settings
Patient Italy ldquoIt was our fault We forgot to contact thegeneral practitioner during the hospitalisationrdquo
Patients sharing the responsibility for the handoverwith healthcare professionalsExamples of patients sharing responsibility for the hand-over with healthcare professionals were found in Swedenfor patients who were admitted for acute conditionsThese patients participated in sharing essential or spe-cific information for their care transition which comple-mented the handover communication conducted by thehealthcare professional For example during hospitaladmissions the patients informed healthcare profes-sionals about their medications and previous care epi-sodes and at discharge they informed the healthcareprofessionals about the name or address of their generalpractitioner to ensure that the correct primary care pro-fessional received the handover information Healthcareprofessionals actively encouraged patients to share theresponsibility for communication such as ensuring thatproper information was shared between the hospital and
Table 2 Categories and themes
Categories Themes
1 Patients as the key actors
in the handover process
2 Patients sharing the
responsibility for the
handover with healthcare
professionals
3 Healthcare professionals
functioning as the key
actors in the handover
process
A Patient positioning in
the handover process
4 Actions required for patients
to be key actors
5 Resources and discipline
required to be the key actor
6 Facilitators for and barriers
to patient participation
B Prerequisites for
patient participation
7 Patient preferences for
being the key actors
8 Patient preferences
regarding healthcare
professionals serving as the
key actors
C Patient preferences for
the handover process
4 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
communityprimary care settings and asked of thepatients to assume responsibility for their own health
Patient Sweden ldquoThey used to say please call theadvanced home care services just for safety reasons andtell them yoursquore back homerdquo
Healthcare professionals functioning as the key actorsin the handover processSome patients viewed the healthcare professionals as thekey actors in the handover process These patientsassumed that handovers are performed by healthcareprofessionals focusing on verbal andor written commu-nication electronic mail or medical records data sharedbetween the care settings This more passive positioningin the handover was found among the Dutch patientsSome hospitals in the Netherlands had a dedicatedlsquotransfer nursersquo to manage handovers to the primarycare setting after discharge
Patient Netherlands ldquoYes I indeed think that if the hos-pital takes responsibility to discharge patients becausethey think they can manage outside the hospital theyalso have to take that responsibility and arrange an alter-native solution if itrsquos not possiblerdquo
Prerequisites for patient participationThis theme had three categories (a) actions requiredfor patients to be key actors (b) resources and disciplinerequired to be the key actor and (c) facilitators for andbarriers to patient participation
Actions required for patients to be key actorsTo be able to function as key actors patients had toassume the responsibility that is take initiatives and askthe healthcare professionals questions to get the neededinformation
Patient Spain ldquoIn order to have more information it isimportant to ask hellip and sometimes you ask a questionand they answer ldquoWell I donrsquot knowWait please I willask somebodyrdquo hellip and they donrsquot tell you anythingrdquo
In addition patients had to be explicit and sometimesbe assertive in their communication with the healthcareprofessionals to help the handover move forward
Resources and discipline required to be the key actorPatients acknowledged the importance and the potentialof having own resources and noted they investigatedtheir social network to find the best healthcare profes-sional available Patients also used their available familyand contact resources Family members sometimesreplaced the patient in taking responsibility for
conveying handover information and acting as medicalsecretaries or information conduitsPatients with limited personal resources or with low
health literacy had difficulties understanding thereceived information and sharing the information withthe healthcare professionals This limited their participa-tion in the handover communication
Patient Spain ldquoWhat can I say The main thing was thatI could not speak in Spanish so I canrsquot express manythings so that is the problemrdquo
In order to function as the key actors in the handovergeriatric patients in Poland had to be disciplined inorganising and transferring medical documents as theywere the main repository of patient documentation Inthis model lack of discipline and willingness to systemat-ically collect relevant documents were barriers to effect-ive handovers
Patient Poland ldquoIf the patient does not want and would notcomply the best doctor would not (be able to) help himrdquo
Facilitators for and barriers to patient participationPatients reported on several communication facilitators andbarriers related to their participation Patients perceived apositive climate for communication based on mutualrespect in an open atmosphere and on a personal levelbetween them and the healthcare professionals as an enab-ling factor for participation in the handover Accordingly anegative climate for communication involved healthcareprofessionals neglecting patientsrsquo individual needs or beingtoo busy to communicate with patientsLack of information was the main barrier to participa-
tion during the handover process Patients perceived a gapbetween the information they received and the informa-tion they actually needed for continuous care Informationgaps often concerned medication information whenpatients were discharged with unclear or insufficient infor-mation on how best to handle their medications orwithout a new and updated medication list they could notparticipate actively in follow-up Finally the patientsexpressed the need for a dedicated discharge encounterin which they would be given all the information neededthat could help them improve their postdischarge care
Patient Italy ldquoI go back home with a bag of drugs and trustme that this was a mess I could not sort out hellip They didnrsquottell us that there could be a risk of depression I had amedical discharge report they have been really good forGodrsquos sake but they did not explain to us enoughrdquo
Patient preferences for the handover processThere are two categories under this theme (a) patientpreferences for being the key actors and (b) patient
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 5
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
handover processes between community and hospitalcare may help in finding optimal ways of empoweringpatients that will improve the quality and safety of hand-overs This study aims to explore the experiences andperspectives of patients with chronic diseases in regardsto their participation in handover communicationbetween primary and secondary healthcare in fiveEuropean countries
METHODS
Study design and settingsThis study is a secondary analysis of data from a cross-national qualitative study of patient perspectives ontheir handovers conducted at nine hospitals and theirfeeder primary healthcare systems in the NetherlandsSpain Poland Italy and Sweden The settings werechosen to include different regional healthcare systemsand hospitals of different sizes The study was conductedas part of the European HANDOVER Project thatresearched handovers between primary and secondarycare and examined the perspectives of a wide group ofstakeholders in the transition of care between theinpatient hospital and the primary care and communitysetting (FP7-HEALTH-F2ndash2008-223409)14
Primary study populationPatients in the HANDOVER Project encompassed adultswith a chronic disease (diabetes mellitus chronicobstructive pulmonary disease (COPD) heart failure
asthma andor poly-pharmacy) who were discharged tohome directly from an inpatient hospital admissionAdditional country-specific inclusion criteria are shownin table 1 The general inclusion criteria were chosen tostudy patient handovers in both primary and secondarycare settings Patients were expected to have experiencedseveral handovers The population was chosen becausehandovers are critical for chronic and high-risk patientswho require more frequent and complex transitions6
and improving handovers for this group was thought tohave a sizable impact on their quality of care Thecountry-specific criteria were used to recruit patients whohad experienced handovers in different specialities andclinical settings Purposive sampling was used to selectpatients with the chosen diagnoses ages and gender15
Data collectionIndividual interviews were conducted with patients intheir native language in 2009 and were done in personusually at the patientsrsquo home or at the hospital 3 to4 weeks after discharge sometimes with a familymember present In all countries two members of thelocal research team conducted the interviews All inter-viewers had experience with healthcare either asresearchers or as healthcare professionals and wereexperienced interviewers or had attended a series ofworkshops on qualitative interviewing to ensure standar-dised methodsFocus group interviews were performed in the
patientsrsquo native language Focus groups were led by a
Table 1 Study sample
Country
Individual
interviews
(n=53)
Focus group
interviews
(n=37)
Country specific inclusion
criteria General inclusion criteria
The
Netherlands
n=8 n=7 Patients admitted to internal
medicine pulmonary diseases
cardiology or (vascular) surgical
wards
gt18 years
Diagnosed with either diabetes
mellitus chronic obstructive
pulmonary disease (COPD)
heart failure asthma orand
poly-pharmacy (gt6 drugs)
Discharged to home or nursing
home (under responsibility of
primarycommunity care)
Spain n=8 n=3 Patients belonging to cultural
minority groups with
limited health literacy (capacity to
read write and understand
healthcare information)
Poland n=23 n=10 Patients ge60 of age
Italy n=5 n=9 Patients admitted to emergency
ward
Sweden n=9 n=8 Patients admitted to emergency
ward via emergency room If
living at a nursing home only
within a geographically specified
area
Number of participants by country and inclusion criteria
2 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
trained moderator and had one or two observers whomade field notes and added question prompts All inter-views were audio-taped and transcribed verbatim in thelocal language according to a jointly decided standar-dised formatBoth individual and focus groups interviews used a
semistructured interview guide developed in English bythe HANDOVER Project researchers and translated intothe local language of the research groups16 The inter-view guide covered these areas of interest Experience with recent handovers (appreciative
problematic situations and consequences) Perceptions about handovers in general (ie experi-
ences attitudes methods tools barriers facilitators) Perceptions about providerpatient tasks roles and
responsibilities Suggestions for improving patient handoversThe guide was piloted in each country and when
necessary adjusted for local conditions and needs (avail-able upon request)A quality assurance protocol17 based on BMJ criteria18
and on criteria presented by Tong et al15 was developed(by MVD and JKJ) and used to ensure trustworthinessthroughout the data collection and data analysesRequirements for informed consent and other ethicaland legal requirements for research using patient infor-mation were fulfilled at all study sites
Sample for secondary analysisFor the secondary analysis data were extracted frompatient interviews in the five countries participating inthe HANDOVER Project The sample consisted of 90patients 53 individually interviewed (55 of the overallsample of patients interviewed individually for the ori-ginal studies conducted as part of the HANDOVERProject) and 37 interviewed in focus groups (100 ofthe overall sample of patients interviewed in groups)
The distribution across countries is shown in table 1Where the gender distribution of the primary samplewas reported it included approximately equal numbersof male and female patients
Data analysisThe analysis consisted of two main parts analysis ofinterviews at the national level and a secondary ana-lysis19 of the cross-national data (see figure 1)
Analysis at national levelTwo interviews from each country were translated intoEnglish and coded inductively using a modifiedgrounded theory approach of Corbin and Strauss20 Aqualitative data analysis software (Atlasti) was used tofacilitate storing coding and indexing of the data21 Theresearchers created a codebook based on codes gener-ated in each country The codebook consisted of thecode and an operational definition both of which wereagreed upon during regularly scheduled conference-calls and face to face meetings and was used for analysisof both individual and focus group interviews Tworesearchers in each country analysed their countryrsquos datain parallel with the data collection and continued tocollect data until conceptual saturation was reached andno new codes or categories were generated20 Localreports were written in English by one or two of theresearchers in each country and used for compiled ana-lyses for the European HANDOVER Project studiesThese studies focused on barriers and facilitators toeffective handovers patient roles and responsibilitiesand patient-centredness and participation culture16 22 23
Secondary analysisThe local reports including quotes from the individualinterviews and focus groups were used for the
Figure 1 Proceduremdashfrom data collection to the current secondary analysis
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 3
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
secondary analysis which focused on patientsrsquo perspec-tive on their own participation in handovers Thus thissecondary analysis seeks to answer a new research ques-tion19 using data that was already collectedLocal reports were analysed using a qualitative induct-
ive content analysis as described by Hsieh andShannon24 Two authors (MF MO) coded the texts inopen coding and three authors (MF MO GH) sortedthe codes into categories and themes Validity checkinginvolved all authors of the local reports who reviewedthe findings to ensure they were consistent with the ori-ginal interview data
RESULTS
The data analysis resulted in eight categories fromwhich three themes were developed (1) patient position-ing in the handover process (2) prerequisites for patient partici-pation and (3) patient preferences for the handover process(see table 2)
Patient positioning in the handover processThree types of patient experiences form the categoriesunder this theme (a) patients as the key actors in thehandover process (b) patients sharing the responsibilityfor the handover with healthcare professionals and (c)healthcare professionals functioning as the key actors inthe handover process
Patients as the key actors in the handover processPatients assumed the responsibility for the handovercommunication including establishing contact with thenext care unit as well as the responsibility for collectingstoring and handing over essential information for man-aging their care such as medication lists or dischargenotes For example when a healthcare professional inthe hospital setting in Italy wrote the discharge note totransition the patient to the primary care settingmdashthisdischarge note was given to the patient for delivery tothe general practitioner The key actor positioning wasmost explicitly stated by the geriatric patients in Polandwho noted they needed to take responsibility in organis-ing the handovers as well as being couriersPatients who functioned as key actors perceived their
active involvement was required for an effective hand-over and to ensure continuity of care These patientshad either learned from past experiences that little orno information was transferred unless they did it them-selves or perceived that healthcare professionalsexpected them to assume the initiative and be activeduring their handovers
Patient Poland ldquoWell we all know by now that it[general practitioner ndash hospital communication] doesnrsquotexist You want a referralmdashthen you get it Then Iarrange my admissionmdashneither my general practitionernor hospital physician care helliprdquo
Being the key actor could cause some patients toblame themselves for not fulfilling the task of facilitatingthe handover when information was lacking betweencare settings
Patient Italy ldquoIt was our fault We forgot to contact thegeneral practitioner during the hospitalisationrdquo
Patients sharing the responsibility for the handoverwith healthcare professionalsExamples of patients sharing responsibility for the hand-over with healthcare professionals were found in Swedenfor patients who were admitted for acute conditionsThese patients participated in sharing essential or spe-cific information for their care transition which comple-mented the handover communication conducted by thehealthcare professional For example during hospitaladmissions the patients informed healthcare profes-sionals about their medications and previous care epi-sodes and at discharge they informed the healthcareprofessionals about the name or address of their generalpractitioner to ensure that the correct primary care pro-fessional received the handover information Healthcareprofessionals actively encouraged patients to share theresponsibility for communication such as ensuring thatproper information was shared between the hospital and
Table 2 Categories and themes
Categories Themes
1 Patients as the key actors
in the handover process
2 Patients sharing the
responsibility for the
handover with healthcare
professionals
3 Healthcare professionals
functioning as the key
actors in the handover
process
A Patient positioning in
the handover process
4 Actions required for patients
to be key actors
5 Resources and discipline
required to be the key actor
6 Facilitators for and barriers
to patient participation
B Prerequisites for
patient participation
7 Patient preferences for
being the key actors
8 Patient preferences
regarding healthcare
professionals serving as the
key actors
C Patient preferences for
the handover process
4 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
communityprimary care settings and asked of thepatients to assume responsibility for their own health
Patient Sweden ldquoThey used to say please call theadvanced home care services just for safety reasons andtell them yoursquore back homerdquo
Healthcare professionals functioning as the key actorsin the handover processSome patients viewed the healthcare professionals as thekey actors in the handover process These patientsassumed that handovers are performed by healthcareprofessionals focusing on verbal andor written commu-nication electronic mail or medical records data sharedbetween the care settings This more passive positioningin the handover was found among the Dutch patientsSome hospitals in the Netherlands had a dedicatedlsquotransfer nursersquo to manage handovers to the primarycare setting after discharge
Patient Netherlands ldquoYes I indeed think that if the hos-pital takes responsibility to discharge patients becausethey think they can manage outside the hospital theyalso have to take that responsibility and arrange an alter-native solution if itrsquos not possiblerdquo
Prerequisites for patient participationThis theme had three categories (a) actions requiredfor patients to be key actors (b) resources and disciplinerequired to be the key actor and (c) facilitators for andbarriers to patient participation
Actions required for patients to be key actorsTo be able to function as key actors patients had toassume the responsibility that is take initiatives and askthe healthcare professionals questions to get the neededinformation
Patient Spain ldquoIn order to have more information it isimportant to ask hellip and sometimes you ask a questionand they answer ldquoWell I donrsquot knowWait please I willask somebodyrdquo hellip and they donrsquot tell you anythingrdquo
In addition patients had to be explicit and sometimesbe assertive in their communication with the healthcareprofessionals to help the handover move forward
Resources and discipline required to be the key actorPatients acknowledged the importance and the potentialof having own resources and noted they investigatedtheir social network to find the best healthcare profes-sional available Patients also used their available familyand contact resources Family members sometimesreplaced the patient in taking responsibility for
conveying handover information and acting as medicalsecretaries or information conduitsPatients with limited personal resources or with low
health literacy had difficulties understanding thereceived information and sharing the information withthe healthcare professionals This limited their participa-tion in the handover communication
Patient Spain ldquoWhat can I say The main thing was thatI could not speak in Spanish so I canrsquot express manythings so that is the problemrdquo
In order to function as the key actors in the handovergeriatric patients in Poland had to be disciplined inorganising and transferring medical documents as theywere the main repository of patient documentation Inthis model lack of discipline and willingness to systemat-ically collect relevant documents were barriers to effect-ive handovers
Patient Poland ldquoIf the patient does not want and would notcomply the best doctor would not (be able to) help himrdquo
Facilitators for and barriers to patient participationPatients reported on several communication facilitators andbarriers related to their participation Patients perceived apositive climate for communication based on mutualrespect in an open atmosphere and on a personal levelbetween them and the healthcare professionals as an enab-ling factor for participation in the handover Accordingly anegative climate for communication involved healthcareprofessionals neglecting patientsrsquo individual needs or beingtoo busy to communicate with patientsLack of information was the main barrier to participa-
tion during the handover process Patients perceived a gapbetween the information they received and the informa-tion they actually needed for continuous care Informationgaps often concerned medication information whenpatients were discharged with unclear or insufficient infor-mation on how best to handle their medications orwithout a new and updated medication list they could notparticipate actively in follow-up Finally the patientsexpressed the need for a dedicated discharge encounterin which they would be given all the information neededthat could help them improve their postdischarge care
Patient Italy ldquoI go back home with a bag of drugs and trustme that this was a mess I could not sort out hellip They didnrsquottell us that there could be a risk of depression I had amedical discharge report they have been really good forGodrsquos sake but they did not explain to us enoughrdquo
Patient preferences for the handover processThere are two categories under this theme (a) patientpreferences for being the key actors and (b) patient
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 5
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
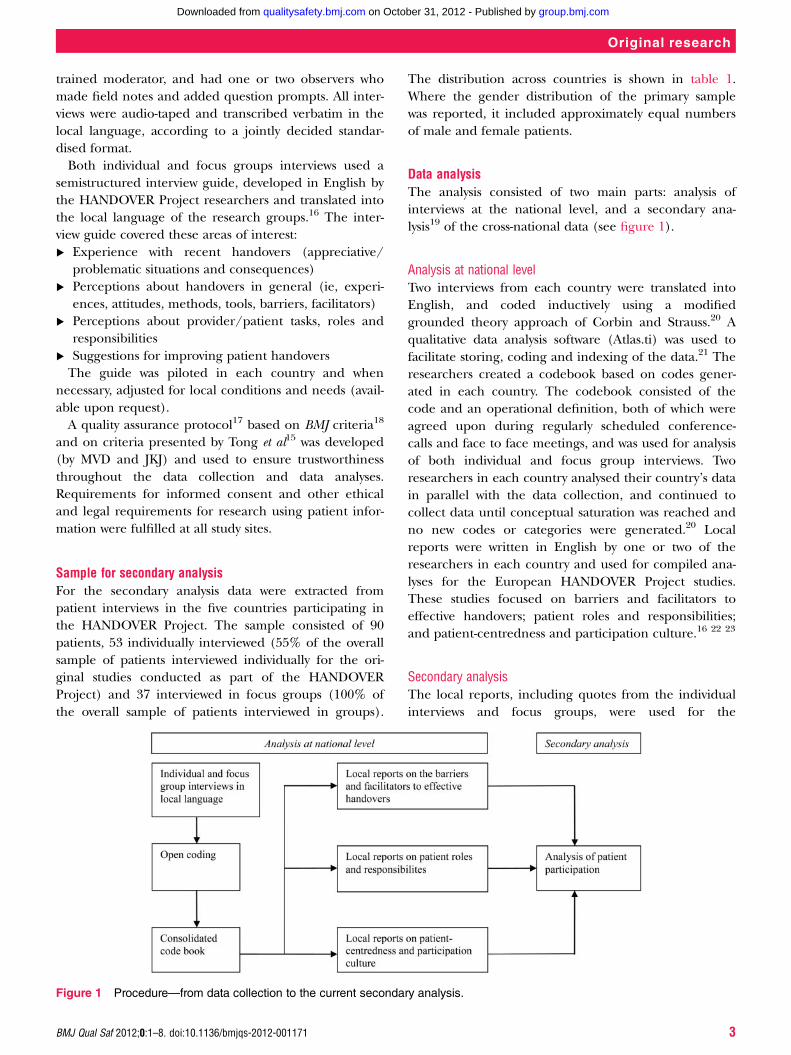
trained moderator and had one or two observers whomade field notes and added question prompts All inter-views were audio-taped and transcribed verbatim in thelocal language according to a jointly decided standar-dised formatBoth individual and focus groups interviews used a
semistructured interview guide developed in English bythe HANDOVER Project researchers and translated intothe local language of the research groups16 The inter-view guide covered these areas of interest Experience with recent handovers (appreciative
problematic situations and consequences) Perceptions about handovers in general (ie experi-
ences attitudes methods tools barriers facilitators) Perceptions about providerpatient tasks roles and
responsibilities Suggestions for improving patient handoversThe guide was piloted in each country and when
necessary adjusted for local conditions and needs (avail-able upon request)A quality assurance protocol17 based on BMJ criteria18
and on criteria presented by Tong et al15 was developed(by MVD and JKJ) and used to ensure trustworthinessthroughout the data collection and data analysesRequirements for informed consent and other ethicaland legal requirements for research using patient infor-mation were fulfilled at all study sites
Sample for secondary analysisFor the secondary analysis data were extracted frompatient interviews in the five countries participating inthe HANDOVER Project The sample consisted of 90patients 53 individually interviewed (55 of the overallsample of patients interviewed individually for the ori-ginal studies conducted as part of the HANDOVERProject) and 37 interviewed in focus groups (100 ofthe overall sample of patients interviewed in groups)
The distribution across countries is shown in table 1Where the gender distribution of the primary samplewas reported it included approximately equal numbersof male and female patients
Data analysisThe analysis consisted of two main parts analysis ofinterviews at the national level and a secondary ana-lysis19 of the cross-national data (see figure 1)
Analysis at national levelTwo interviews from each country were translated intoEnglish and coded inductively using a modifiedgrounded theory approach of Corbin and Strauss20 Aqualitative data analysis software (Atlasti) was used tofacilitate storing coding and indexing of the data21 Theresearchers created a codebook based on codes gener-ated in each country The codebook consisted of thecode and an operational definition both of which wereagreed upon during regularly scheduled conference-calls and face to face meetings and was used for analysisof both individual and focus group interviews Tworesearchers in each country analysed their countryrsquos datain parallel with the data collection and continued tocollect data until conceptual saturation was reached andno new codes or categories were generated20 Localreports were written in English by one or two of theresearchers in each country and used for compiled ana-lyses for the European HANDOVER Project studiesThese studies focused on barriers and facilitators toeffective handovers patient roles and responsibilitiesand patient-centredness and participation culture16 22 23
Secondary analysisThe local reports including quotes from the individualinterviews and focus groups were used for the
Figure 1 Proceduremdashfrom data collection to the current secondary analysis
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 3
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
secondary analysis which focused on patientsrsquo perspec-tive on their own participation in handovers Thus thissecondary analysis seeks to answer a new research ques-tion19 using data that was already collectedLocal reports were analysed using a qualitative induct-
ive content analysis as described by Hsieh andShannon24 Two authors (MF MO) coded the texts inopen coding and three authors (MF MO GH) sortedthe codes into categories and themes Validity checkinginvolved all authors of the local reports who reviewedthe findings to ensure they were consistent with the ori-ginal interview data
RESULTS
The data analysis resulted in eight categories fromwhich three themes were developed (1) patient position-ing in the handover process (2) prerequisites for patient partici-pation and (3) patient preferences for the handover process(see table 2)
Patient positioning in the handover processThree types of patient experiences form the categoriesunder this theme (a) patients as the key actors in thehandover process (b) patients sharing the responsibilityfor the handover with healthcare professionals and (c)healthcare professionals functioning as the key actors inthe handover process
Patients as the key actors in the handover processPatients assumed the responsibility for the handovercommunication including establishing contact with thenext care unit as well as the responsibility for collectingstoring and handing over essential information for man-aging their care such as medication lists or dischargenotes For example when a healthcare professional inthe hospital setting in Italy wrote the discharge note totransition the patient to the primary care settingmdashthisdischarge note was given to the patient for delivery tothe general practitioner The key actor positioning wasmost explicitly stated by the geriatric patients in Polandwho noted they needed to take responsibility in organis-ing the handovers as well as being couriersPatients who functioned as key actors perceived their
active involvement was required for an effective hand-over and to ensure continuity of care These patientshad either learned from past experiences that little orno information was transferred unless they did it them-selves or perceived that healthcare professionalsexpected them to assume the initiative and be activeduring their handovers
Patient Poland ldquoWell we all know by now that it[general practitioner ndash hospital communication] doesnrsquotexist You want a referralmdashthen you get it Then Iarrange my admissionmdashneither my general practitionernor hospital physician care helliprdquo
Being the key actor could cause some patients toblame themselves for not fulfilling the task of facilitatingthe handover when information was lacking betweencare settings
Patient Italy ldquoIt was our fault We forgot to contact thegeneral practitioner during the hospitalisationrdquo
Patients sharing the responsibility for the handoverwith healthcare professionalsExamples of patients sharing responsibility for the hand-over with healthcare professionals were found in Swedenfor patients who were admitted for acute conditionsThese patients participated in sharing essential or spe-cific information for their care transition which comple-mented the handover communication conducted by thehealthcare professional For example during hospitaladmissions the patients informed healthcare profes-sionals about their medications and previous care epi-sodes and at discharge they informed the healthcareprofessionals about the name or address of their generalpractitioner to ensure that the correct primary care pro-fessional received the handover information Healthcareprofessionals actively encouraged patients to share theresponsibility for communication such as ensuring thatproper information was shared between the hospital and
Table 2 Categories and themes
Categories Themes
1 Patients as the key actors
in the handover process
2 Patients sharing the
responsibility for the
handover with healthcare
professionals
3 Healthcare professionals
functioning as the key
actors in the handover
process
A Patient positioning in
the handover process
4 Actions required for patients
to be key actors
5 Resources and discipline
required to be the key actor
6 Facilitators for and barriers
to patient participation
B Prerequisites for
patient participation
7 Patient preferences for
being the key actors
8 Patient preferences
regarding healthcare
professionals serving as the
key actors
C Patient preferences for
the handover process
4 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
communityprimary care settings and asked of thepatients to assume responsibility for their own health
Patient Sweden ldquoThey used to say please call theadvanced home care services just for safety reasons andtell them yoursquore back homerdquo
Healthcare professionals functioning as the key actorsin the handover processSome patients viewed the healthcare professionals as thekey actors in the handover process These patientsassumed that handovers are performed by healthcareprofessionals focusing on verbal andor written commu-nication electronic mail or medical records data sharedbetween the care settings This more passive positioningin the handover was found among the Dutch patientsSome hospitals in the Netherlands had a dedicatedlsquotransfer nursersquo to manage handovers to the primarycare setting after discharge
Patient Netherlands ldquoYes I indeed think that if the hos-pital takes responsibility to discharge patients becausethey think they can manage outside the hospital theyalso have to take that responsibility and arrange an alter-native solution if itrsquos not possiblerdquo
Prerequisites for patient participationThis theme had three categories (a) actions requiredfor patients to be key actors (b) resources and disciplinerequired to be the key actor and (c) facilitators for andbarriers to patient participation
Actions required for patients to be key actorsTo be able to function as key actors patients had toassume the responsibility that is take initiatives and askthe healthcare professionals questions to get the neededinformation
Patient Spain ldquoIn order to have more information it isimportant to ask hellip and sometimes you ask a questionand they answer ldquoWell I donrsquot knowWait please I willask somebodyrdquo hellip and they donrsquot tell you anythingrdquo
In addition patients had to be explicit and sometimesbe assertive in their communication with the healthcareprofessionals to help the handover move forward
Resources and discipline required to be the key actorPatients acknowledged the importance and the potentialof having own resources and noted they investigatedtheir social network to find the best healthcare profes-sional available Patients also used their available familyand contact resources Family members sometimesreplaced the patient in taking responsibility for
conveying handover information and acting as medicalsecretaries or information conduitsPatients with limited personal resources or with low
health literacy had difficulties understanding thereceived information and sharing the information withthe healthcare professionals This limited their participa-tion in the handover communication
Patient Spain ldquoWhat can I say The main thing was thatI could not speak in Spanish so I canrsquot express manythings so that is the problemrdquo
In order to function as the key actors in the handovergeriatric patients in Poland had to be disciplined inorganising and transferring medical documents as theywere the main repository of patient documentation Inthis model lack of discipline and willingness to systemat-ically collect relevant documents were barriers to effect-ive handovers
Patient Poland ldquoIf the patient does not want and would notcomply the best doctor would not (be able to) help himrdquo
Facilitators for and barriers to patient participationPatients reported on several communication facilitators andbarriers related to their participation Patients perceived apositive climate for communication based on mutualrespect in an open atmosphere and on a personal levelbetween them and the healthcare professionals as an enab-ling factor for participation in the handover Accordingly anegative climate for communication involved healthcareprofessionals neglecting patientsrsquo individual needs or beingtoo busy to communicate with patientsLack of information was the main barrier to participa-
tion during the handover process Patients perceived a gapbetween the information they received and the informa-tion they actually needed for continuous care Informationgaps often concerned medication information whenpatients were discharged with unclear or insufficient infor-mation on how best to handle their medications orwithout a new and updated medication list they could notparticipate actively in follow-up Finally the patientsexpressed the need for a dedicated discharge encounterin which they would be given all the information neededthat could help them improve their postdischarge care
Patient Italy ldquoI go back home with a bag of drugs and trustme that this was a mess I could not sort out hellip They didnrsquottell us that there could be a risk of depression I had amedical discharge report they have been really good forGodrsquos sake but they did not explain to us enoughrdquo
Patient preferences for the handover processThere are two categories under this theme (a) patientpreferences for being the key actors and (b) patient
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 5
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
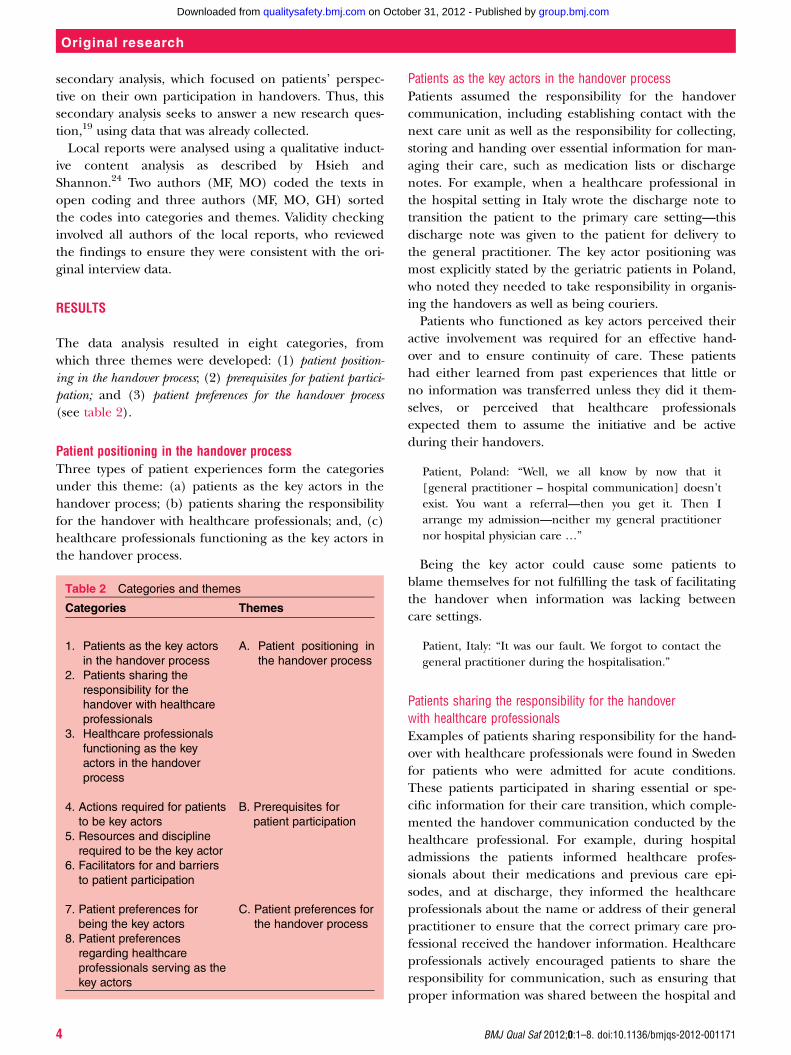
secondary analysis which focused on patientsrsquo perspec-tive on their own participation in handovers Thus thissecondary analysis seeks to answer a new research ques-tion19 using data that was already collectedLocal reports were analysed using a qualitative induct-
ive content analysis as described by Hsieh andShannon24 Two authors (MF MO) coded the texts inopen coding and three authors (MF MO GH) sortedthe codes into categories and themes Validity checkinginvolved all authors of the local reports who reviewedthe findings to ensure they were consistent with the ori-ginal interview data
RESULTS
The data analysis resulted in eight categories fromwhich three themes were developed (1) patient position-ing in the handover process (2) prerequisites for patient partici-pation and (3) patient preferences for the handover process(see table 2)
Patient positioning in the handover processThree types of patient experiences form the categoriesunder this theme (a) patients as the key actors in thehandover process (b) patients sharing the responsibilityfor the handover with healthcare professionals and (c)healthcare professionals functioning as the key actors inthe handover process
Patients as the key actors in the handover processPatients assumed the responsibility for the handovercommunication including establishing contact with thenext care unit as well as the responsibility for collectingstoring and handing over essential information for man-aging their care such as medication lists or dischargenotes For example when a healthcare professional inthe hospital setting in Italy wrote the discharge note totransition the patient to the primary care settingmdashthisdischarge note was given to the patient for delivery tothe general practitioner The key actor positioning wasmost explicitly stated by the geriatric patients in Polandwho noted they needed to take responsibility in organis-ing the handovers as well as being couriersPatients who functioned as key actors perceived their
active involvement was required for an effective hand-over and to ensure continuity of care These patientshad either learned from past experiences that little orno information was transferred unless they did it them-selves or perceived that healthcare professionalsexpected them to assume the initiative and be activeduring their handovers
Patient Poland ldquoWell we all know by now that it[general practitioner ndash hospital communication] doesnrsquotexist You want a referralmdashthen you get it Then Iarrange my admissionmdashneither my general practitionernor hospital physician care helliprdquo
Being the key actor could cause some patients toblame themselves for not fulfilling the task of facilitatingthe handover when information was lacking betweencare settings
Patient Italy ldquoIt was our fault We forgot to contact thegeneral practitioner during the hospitalisationrdquo
Patients sharing the responsibility for the handoverwith healthcare professionalsExamples of patients sharing responsibility for the hand-over with healthcare professionals were found in Swedenfor patients who were admitted for acute conditionsThese patients participated in sharing essential or spe-cific information for their care transition which comple-mented the handover communication conducted by thehealthcare professional For example during hospitaladmissions the patients informed healthcare profes-sionals about their medications and previous care epi-sodes and at discharge they informed the healthcareprofessionals about the name or address of their generalpractitioner to ensure that the correct primary care pro-fessional received the handover information Healthcareprofessionals actively encouraged patients to share theresponsibility for communication such as ensuring thatproper information was shared between the hospital and
Table 2 Categories and themes
Categories Themes
1 Patients as the key actors
in the handover process
2 Patients sharing the
responsibility for the
handover with healthcare
professionals
3 Healthcare professionals
functioning as the key
actors in the handover
process
A Patient positioning in
the handover process
4 Actions required for patients
to be key actors
5 Resources and discipline
required to be the key actor
6 Facilitators for and barriers
to patient participation
B Prerequisites for
patient participation
7 Patient preferences for
being the key actors
8 Patient preferences
regarding healthcare
professionals serving as the
key actors
C Patient preferences for
the handover process
4 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
communityprimary care settings and asked of thepatients to assume responsibility for their own health
Patient Sweden ldquoThey used to say please call theadvanced home care services just for safety reasons andtell them yoursquore back homerdquo
Healthcare professionals functioning as the key actorsin the handover processSome patients viewed the healthcare professionals as thekey actors in the handover process These patientsassumed that handovers are performed by healthcareprofessionals focusing on verbal andor written commu-nication electronic mail or medical records data sharedbetween the care settings This more passive positioningin the handover was found among the Dutch patientsSome hospitals in the Netherlands had a dedicatedlsquotransfer nursersquo to manage handovers to the primarycare setting after discharge
Patient Netherlands ldquoYes I indeed think that if the hos-pital takes responsibility to discharge patients becausethey think they can manage outside the hospital theyalso have to take that responsibility and arrange an alter-native solution if itrsquos not possiblerdquo
Prerequisites for patient participationThis theme had three categories (a) actions requiredfor patients to be key actors (b) resources and disciplinerequired to be the key actor and (c) facilitators for andbarriers to patient participation
Actions required for patients to be key actorsTo be able to function as key actors patients had toassume the responsibility that is take initiatives and askthe healthcare professionals questions to get the neededinformation
Patient Spain ldquoIn order to have more information it isimportant to ask hellip and sometimes you ask a questionand they answer ldquoWell I donrsquot knowWait please I willask somebodyrdquo hellip and they donrsquot tell you anythingrdquo
In addition patients had to be explicit and sometimesbe assertive in their communication with the healthcareprofessionals to help the handover move forward
Resources and discipline required to be the key actorPatients acknowledged the importance and the potentialof having own resources and noted they investigatedtheir social network to find the best healthcare profes-sional available Patients also used their available familyand contact resources Family members sometimesreplaced the patient in taking responsibility for
conveying handover information and acting as medicalsecretaries or information conduitsPatients with limited personal resources or with low
health literacy had difficulties understanding thereceived information and sharing the information withthe healthcare professionals This limited their participa-tion in the handover communication
Patient Spain ldquoWhat can I say The main thing was thatI could not speak in Spanish so I canrsquot express manythings so that is the problemrdquo
In order to function as the key actors in the handovergeriatric patients in Poland had to be disciplined inorganising and transferring medical documents as theywere the main repository of patient documentation Inthis model lack of discipline and willingness to systemat-ically collect relevant documents were barriers to effect-ive handovers
Patient Poland ldquoIf the patient does not want and would notcomply the best doctor would not (be able to) help himrdquo
Facilitators for and barriers to patient participationPatients reported on several communication facilitators andbarriers related to their participation Patients perceived apositive climate for communication based on mutualrespect in an open atmosphere and on a personal levelbetween them and the healthcare professionals as an enab-ling factor for participation in the handover Accordingly anegative climate for communication involved healthcareprofessionals neglecting patientsrsquo individual needs or beingtoo busy to communicate with patientsLack of information was the main barrier to participa-
tion during the handover process Patients perceived a gapbetween the information they received and the informa-tion they actually needed for continuous care Informationgaps often concerned medication information whenpatients were discharged with unclear or insufficient infor-mation on how best to handle their medications orwithout a new and updated medication list they could notparticipate actively in follow-up Finally the patientsexpressed the need for a dedicated discharge encounterin which they would be given all the information neededthat could help them improve their postdischarge care
Patient Italy ldquoI go back home with a bag of drugs and trustme that this was a mess I could not sort out hellip They didnrsquottell us that there could be a risk of depression I had amedical discharge report they have been really good forGodrsquos sake but they did not explain to us enoughrdquo
Patient preferences for the handover processThere are two categories under this theme (a) patientpreferences for being the key actors and (b) patient
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 5
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from

communityprimary care settings and asked of thepatients to assume responsibility for their own health
Patient Sweden ldquoThey used to say please call theadvanced home care services just for safety reasons andtell them yoursquore back homerdquo
Healthcare professionals functioning as the key actorsin the handover processSome patients viewed the healthcare professionals as thekey actors in the handover process These patientsassumed that handovers are performed by healthcareprofessionals focusing on verbal andor written commu-nication electronic mail or medical records data sharedbetween the care settings This more passive positioningin the handover was found among the Dutch patientsSome hospitals in the Netherlands had a dedicatedlsquotransfer nursersquo to manage handovers to the primarycare setting after discharge
Patient Netherlands ldquoYes I indeed think that if the hos-pital takes responsibility to discharge patients becausethey think they can manage outside the hospital theyalso have to take that responsibility and arrange an alter-native solution if itrsquos not possiblerdquo
Prerequisites for patient participationThis theme had three categories (a) actions requiredfor patients to be key actors (b) resources and disciplinerequired to be the key actor and (c) facilitators for andbarriers to patient participation
Actions required for patients to be key actorsTo be able to function as key actors patients had toassume the responsibility that is take initiatives and askthe healthcare professionals questions to get the neededinformation
Patient Spain ldquoIn order to have more information it isimportant to ask hellip and sometimes you ask a questionand they answer ldquoWell I donrsquot knowWait please I willask somebodyrdquo hellip and they donrsquot tell you anythingrdquo
In addition patients had to be explicit and sometimesbe assertive in their communication with the healthcareprofessionals to help the handover move forward
Resources and discipline required to be the key actorPatients acknowledged the importance and the potentialof having own resources and noted they investigatedtheir social network to find the best healthcare profes-sional available Patients also used their available familyand contact resources Family members sometimesreplaced the patient in taking responsibility for
conveying handover information and acting as medicalsecretaries or information conduitsPatients with limited personal resources or with low
health literacy had difficulties understanding thereceived information and sharing the information withthe healthcare professionals This limited their participa-tion in the handover communication
Patient Spain ldquoWhat can I say The main thing was thatI could not speak in Spanish so I canrsquot express manythings so that is the problemrdquo
In order to function as the key actors in the handovergeriatric patients in Poland had to be disciplined inorganising and transferring medical documents as theywere the main repository of patient documentation Inthis model lack of discipline and willingness to systemat-ically collect relevant documents were barriers to effect-ive handovers
Patient Poland ldquoIf the patient does not want and would notcomply the best doctor would not (be able to) help himrdquo
Facilitators for and barriers to patient participationPatients reported on several communication facilitators andbarriers related to their participation Patients perceived apositive climate for communication based on mutualrespect in an open atmosphere and on a personal levelbetween them and the healthcare professionals as an enab-ling factor for participation in the handover Accordingly anegative climate for communication involved healthcareprofessionals neglecting patientsrsquo individual needs or beingtoo busy to communicate with patientsLack of information was the main barrier to participa-
tion during the handover process Patients perceived a gapbetween the information they received and the informa-tion they actually needed for continuous care Informationgaps often concerned medication information whenpatients were discharged with unclear or insufficient infor-mation on how best to handle their medications orwithout a new and updated medication list they could notparticipate actively in follow-up Finally the patientsexpressed the need for a dedicated discharge encounterin which they would be given all the information neededthat could help them improve their postdischarge care
Patient Italy ldquoI go back home with a bag of drugs and trustme that this was a mess I could not sort out hellip They didnrsquottell us that there could be a risk of depression I had amedical discharge report they have been really good forGodrsquos sake but they did not explain to us enoughrdquo
Patient preferences for the handover processThere are two categories under this theme (a) patientpreferences for being the key actors and (b) patient
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 5
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from

preferences regarding healthcare professionals servingas the key actors
Patient preferences for being the key actorsThe preference for being key actors in the handoverprocess was expressed by Swedish patients undergoingacute admissions by geriatric patients in Poland and bypatients in the Netherlands These patients stressed theimportance of patients in contributing to an effectivehandover For example Swedish patients noted thatwhen they assumed responsibility for the handover com-munication worked better It also empowered them andgave them a sense of control over the handover processPatients also found the opportunity to look up andascertain the accuracy of the information being trans-ferred an advantage
Focus group Netherlands
ldquoPatient A You receive the letter and you deliver it to thedoctor and then the general practitioner will visit to seehow you are doing so this is very satisfying for me yes
Interviewer So you are satisfied with this that the infor-mation is routed via you
Patient B I find it an advantage when it is routed via thepatient
Patient A Yes and itrsquos also true that you are certain theinformation is coming acrossrdquo
Patient preferences regarding healthcare professionalsserving as the key actorsPatients who indicated a preference for healthcare pro-fessionals to be the key actors in the handover perceivedhandovers more effective when healthcare professionalswere actively involved These patients felt that profes-sionals should be fully responsible for the handover andreported feeling frustrated when urged to take responsi-bility for the handover and wanted a passive role in theircare Some patients mentioned a transfer nurse as thepreferred key actor for handovers
Relative Sweden ldquoThey should have somebody whoalways gets in touch with the nursing home Someoneresponsible that can take care of all contactsrdquo
One subgroup patients with low health literacy didnot express any preferences regarding participating ornot participating in the handover process
DISCUSSION
Three themes of importance for patient participationwere revealed in the study patient positioning in the
handover process prerequisites for patient participationand patient preferences for the handover processes Thisstudy does not make comparisons across countriesInstead the aim was to study patient participation in hand-over processes with different characteristics in variouscare settings to explore patientsrsquo perspectives moreindepth The findings demonstrate that patientsrsquo position-ing ranged from being the key actor sharing the responsi-bility with healthcare professionals to being passivePatientsrsquo positioning seems to respond to the hand-
over system in an elastic relation and are modulated bytheir perceptions of the healthcare professionals actionsIn systems with less active engagement of healthcare pro-fessionals patients assumed a more active position whilein systems with active engagement particularly by dedi-cated professionals like transfer nurses patients assumeda more passive position Other studies have found thatpatient participation differs depending on the settingspatient and physician attributes10 25 26 and the experi-ences of patient participation in the handover processesmirror these findings Due to the fact that our study wasa secondary analysis of the data we cannot be sure towhich degree the positioning continuum was a result ofthe patient characteristic or reflects the characteristics ofthe participating nationsrsquo healthcare systemsThe passive role of some patients in the handover may
be a consequence of these individuals lacking informationor instructions from healthcare professionals that wouldallow them to actively participate or a lack of personalresources capabilities or discipline To be able to partici-pate actively patients required certain resources and prere-quisites (eg social network health literacy and clearinformationinstructions) as well as being treated withrespect Two recent reviews on patient participation foundpositive outcomes of patient participation include betterinteraction between patients and healthcare professionalsand enhanced patient safety10 27 The findings of this studythus raise the question whether the quality of handovers isreduced when patients are passive participants becausethey may lack the prerequisites for active participationMany patients did not state a preference for shared
responsibility as one might have expected but preferredthat either the healthcare professionals or the patientfunctioned as the key actor We have not found anyearlier studies on patient preferences regarding assum-ing handover responsibility Comparing our findings tostudies on patient participation in decision-making11 28
reveals that patients choose to be passive participantswhen their involvement may have a negative affect onthe outcome of the decision when decisions arecomplex and when patients were severely ill10 11
Patients with cancer preferred a shared or an activerole28 Patientsrsquo preference for healthcare professionalsto be the key actors in our study may be explained by
6 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from

their chronic disease status and the requirement forsharing complex medical information as well as in thepatientsrsquo statements that a handover process with clearresponsibility was most effective Because patients in theprimary interviews were not explicitly asked about theirinterest in shared responsibility we cannot exclude thatsome patientsrsquo desire shared responsibility However ourfindings suggest that patients in our analysis appeared toprefer clarity about who is responsible for the handoverirrespective of whether the patient or the health profes-sionals function as the key actorThe study has several limitations First the initial trans-
lations of the interviews were conducted in the respect-ive countries by the researchers themselves and not byprofessional translators and the secondary analysis wasperformed on the English text by Swedish and Dutchresearchers raising concerns about the potential for lin-guistic misinterpretation This risk was reduced byhaving both the primary researchers and the individualswho conducted the secondary analysis actively involvedin discussions about the study aim and methods byhaving all steps in data collection and analysis monitoredusing a quality assurance programme17 and by ensuringthat the authors of the local reports have read and con-firmed the accuracy of data from the secondary analysisAlso the secondary analysis was not performed directlyon the original data but on data already selected forlocal reports by researchers and it was not possible toconduct a validity check with the original patients inter-viewed Third patient-specific information on age andthe distribution of the chronic conditions is not knownfor the sample for secondary analysis The primary studypopulation in the HANDOVER-study included a repre-sentative distribution by age gender and diagnoses16 22 23
Finally the population was restricted to adult patientswith chronic conditions which may limit the ability totransfer the findings across all handoversThe methodological limitations with secondary analysis
have been well described by Thorne19 A key issue lies inthe distance between the original data sourcemdashthepatientsmdashand the secondary question about patient partici-pation This question was however a natural extension fromthe primary research questions of the HANDOVER-study
CONCLUSIONS
This study despite its limitations increases our knowl-edge of the preferences of patients for participating inthe handover between the inpatient and the primarycare setting Patient participation in handovers betweenprimary and hospital care is related to the healthcaresystem the activity of healthcare professionals and thepatients themselves The ability to participate and take
an active positioning requires patientsrsquo personal andsocial resources prerequisites such as personal and clearinformation and respectful treatment by healthcare pro-fessionals Patients prefer a handover process where theresponsibility for the handover communication is clearand unambiguous that is a system that ensures them intransparent manner there is continuity of their careThis is an important finding for efforts to improvepatient handovers to create and sustain greater reliabil-ity transparency and consistencyFuture improvements of the patient handover will
require the healthcare organisations to develop a clearand well-considered system of assigning responsibility forthis process Regardless of the system chosen the indi-vidual patientrsquos need of clarity and a level of supportthat is tailored to hisher own resources and ability toparticipate in the handover must be taken into accountFuture development and research is needed to find outhow a shared responsibility could look like in practiceand be unambiguous for the patients Such knowledgecan help enhance safe patient transitions between thehospital and the patientrsquos home
Author affiliations1Department of Neurobiology Care Sciences and Society KarolinskaInstitutet Stockholm Sweden2Department of Social Work Karolinska University Hospital StockholmSweden3Scientific Institute for Quality of Healthcare (IQ healthcare) RadboudUniversity Nijmegen Medical Centre Nijmegen The Netherlands4Department on Quality and Safety St Antonius Hospital and Department onQuality and Safety St Antonius Hospital Nieuwegein The Netherlands5Department of Primary Care Radboud University Nijmegen Medical CentreNijmegen The Netherlands6Kalorama Foundation Radboud University Nijmegen Medical CentreNijmegen The Netherlands7National Center for Quality Assessment in Health Care Krakow Poland8Avedis Donabedian Research Institute (FAD) Universitat Autogravenoma deBarcelona and CIBER Epidemiology and Public Health (CIBERESP) BarcelonaSpain9Clinical Risk Management and Patient Safety Centre Tuscany RegionFlorence FI Italy10Faculty of Health Sciences University of Southampton Southampton UK11Primary Health Care Utrecht Area Utrecht The Netherlands12Centre for Clinical Governance Research University of New South WalesSydney Australia13Department of Clinical Science Intervention and Technology KarolinskaInstitutet Stockholm Sweden14Quality and Patient Safety Karolinska University Hospital StockholmSweden15Department of Clinical Neuroscience Karolinska Institutet StockholmSweden16Patient Safety Center University Medical Center Utrecht UtrechtThe Netherlands17Department of Health Studies University of Stavanger Stavanger Norway
Acknowledgements We would like to thank all participating patients forsharing their valuable experiences
Collaborators The European HANDOVER Research Collaborative consists ofVenneri F Albolino S Molisso A Toccafondi G (Azienda Sanitaria FirenzeFlorence Italy) Barach P Gademan P Goumlbel B Johnson J Kalkman CPijnenborg L (Patient Safety Center University Medical Center Utrecht
BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171 7
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from

Utrecht The Netherlands) Wollersheim H Hesselink G Schoonhoven LVernooij-Dassen M Zegers M (Scientific Institute for Quality of HealthcareRadboud University Nijmegen Medical Centre Nijmegen The Netherlands)Boshuizen E Drachsler H Kicken W van der Klink M Stoyanov S (Centre forLearning Sciences and Technologies Open University Heerlen theNetherlands) Kutryba B Dudzik-Urbaniak E Kalinowski M Kutaj-WasikowskaH (National Center for Quality Assessment in Health Care Krakow Poland)Suntildeol R Groene O Orrego C (Avedis Donabedian Institute UniversidadAutoacutenoma de Barcelona Barcelona Spain) Oumlhleacuten G Airosa F Bergenbrant SFlink M Hansagi H Olsson M (Karolinska University Hospital StockholmSweden) Lilford R Chen Y-F Novielli N Manaseki-Holland S (University ofBirmingham Birmingham UK)
Contributors Study conception and design MF LP HW MVD CO LS JKJGO HH MO and PB Acquisition of data MF GH LP HW EDU CO GT PGand MO Analysis at national level- the local reports MF GH LP EDU COGT PG and MO Secondary analysis MF GH MVD MO Drafting andorrevising the article MF GH LP HW MVD EDU CO GT LS PG JKJ GOHH MO and PB
Funding This study was supported by a grant from the European Union theFramework Programme of the European Commission (FP7-HEALTH-F2-2008-223409) The study sponsor had no role in the study design collectionanalysis and interpretation of the data or in the writing of the article anddecision to submit the article for publication
Competing interests None
Ethics approval Ethical review boards in the Netherlands Spain Poland Italyand Sweden
Provenance and peer review Not commissioned externally peer reviewed
Data sharing statement Data are available on request from the correspondingauthor
REFERENCES1 Forster AJ Clark HD Menard A et al Adverse events among
medical patients after discharge from hospital Can Med Assoc J2004170345ndash9
2 Forster AJ Murff HJ Peterson JF et al The incidence and severityof adverse events affecting patients after discharge from thehospital Ann Intern Med 2003138161ndash7
3 Kripalani S LeFevre F Phillips CO et al Deficits in communicationand information transfer between hospital-based and primary carephysiciansmdashImplications for patient safety and continuity of careJAMA 2007297831ndash41
4 Moore C Wisnivesky J Williams S et al Medical errors related todiscontinuity of care from an inpatient to an outpatient setting J GenIntern Med 200318646ndash51
5 Tam VC Knowles SR Cornish PL et al Frequency type andclinical importance of medication history errors at admission tohospital a systematic review Can Med Assoc J 2005173510ndash15
6 Halasyamani L Kripalani S Coleman E et al Transition of care forhospitalized elderly patientsmdashDevelopment of a discharge checklistfor hospitalists J Hosp Med 20061354ndash60
7 Johnson A Sandford J Written and verbal information versus verbalinformation only for patients being discharged from acute hospitalsettings to home systematic review Health Educ Res200520423ndash9
8 Coleman EA Parry C Chalmers S et al The care transitionsinterventionmdashResults of a randomized controlled trial Arch InternMed 20061661822ndash8
9 Jack BW Chetty VK Anthony D et al A reengineered hospitaldischarge program to decrease rehospitalization A randomized trialAnn Intern Med 2009150178ndash88
10 Davis RE Jacklin R Sevdalis N et al Patient involvement in patientsafety what factors influence patient participation and engagementHealth Expect 200710259ndash67
11 Say R Murtagh M Thomson R Patientsrsquo preference for involvementin medical decision making A narrative review Patient Educ Couns200660102ndash14
12 Meeuwesen L van den Brink-Muinen A Hofstede G Candimensions of national culture predict cross-national differences inmedical communication Patient Educ Couns 20097558ndash66
13 Coulter A Jenkinson C European patientsrsquo views on theresponsiveness of health systems and healthcare providers Eur JPublic Health 200515355ndash60
14 Improving the continuity of patient care through identification andimplementation of novel patient handover processes in Europehttpwwwhandovereu (accessed 21 Oct 2011)
15 Tong A Sainsbury P Craig J Consolidated criteria for reportingqualitative research (COREQ) a 32-item checklist for interviews andfocus groups Int J Qual Health Care 200719349ndash57
16 Hansagi H Olsson M Glas S et al Report on the barriers andfacilitators to effective handovers in the social linguistic andtechnological context in which they take place UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
17 Johnson J Barach P Vernooij-Dassen M A standardized approachfor conducting qualitative research across multiple countries BMJQuality and Safety 2012
18 Mays N Pope C Qualitative research in health care Assessingquality in qualitative research BMJ 200032050ndash2
19 Thorne S Ethical and representational issues in qualitativesecondary analysis Qual Health Res 19988547ndash55
20 Corbin J Strauss A Grounded theory research Procedurescanons and evaluative criteria Qual Sociol 1990133ndash21
21 ATLASti Scientific Software Development Company GmbH BerlinGermany httpwwwatlasticom (accessed 21 Mar 2011)
22 Barach P Gademan P Kalkman C et al Report on how variationsin handover processes lead to near misses and adverse outcomesand identifying standardized elements of communication UtrechtThe Netherlands Utrecht Medical Center for the European Union2010
23 Hesselink G Wollersheim H Barach P et al Report on challengesin patient care and the factors that influence change in practiceUtrecht The Netherlands Utrecht Medical Center for the EuropeanUnion 2010
24 Hsieh HF Shannon SE Three approaches to qualitative contentanalysis Qual Health Res 2005151277ndash88
25 Street RL Jr Krupat E Bell RA et al Beliefs about control in thephysician-patient relationship effect on communication in medicalencounters J Gen Intern Med 200318609ndash16
26 Street RL Jr Gordon HS Ward MM et al Patient participation inmedical encounters why some patients are more involved thanothers Med Care 200543960ndash9
27 Longtin Y Sax H Leape LL et al Patient participation currentknowledge and applicability to patient safety Mayo Clin Proc20108553ndash62
28 Tariman JD Berry DL Cochrane B et al Preferred and actualparticipation roles during health care decision making in personswith cancer a systematic review Ann Oncol 2010211145ndash51
8 BMJ Qual Saf 201201ndash8 doi101136bmjqs-2012-001171
Original research
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
doi 101136bmjqs-2012-001171 published online October 30 2012BMJ Qual Saf
Maria Flink Gijs Hesselink Loes Pijnenborg et al Europeparticipation in the handover process in The key actor a qualitative study of patient
httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlUpdated information and services can be found at
These include
References httpqualitysafetybmjcomcontentearly20121029bmjqs-2012-001171fullhtmlref-list-1
This article cites 22 articles 9 of which can be accessed free at
Open Access
httpcreativecommonsorglicensesby-nc30legalcodehttpcreativecommonsorglicensesby-nc30 and compliance with the license Seework is properly cited the use is non commercial and is otherwise in use distribution and reproduction in any medium provided the originalCreative Commons Attribution Non-commercial License which permits This is an open-access article distributed under the terms of the
PltP Published online October 30 2012 in advance of the print journal
serviceEmail alerting
the box at the top right corner of the online articleReceive free email alerts when new articles cite this article Sign up in
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from
CollectionsTopic
(95 articles)Open access Articles on similar topics can be found in the following collections
Notes
(DOIs) and date of initial publication publication Citations to Advance online articles must include the digital object identifier citable and establish publication priority they are indexed by PubMed from initialtypeset but have not not yet appeared in the paper journal Advance online articles are Advance online articles have been peer reviewed accepted for publication edited and
httpgroupbmjcomgrouprights-licensingpermissionsTo request permissions go to
httpjournalsbmjcomcgireprintformTo order reprints go to
httpgroupbmjcomsubscribeTo subscribe to BMJ go to
groupbmjcom on October 31 2012 - Published by qualitysafetybmjcomDownloaded from







![9[1].Handover ta](https://img.dokumen.tips/doc/110x75/631bd2bd3e8acd9977059cca/91handover-ta.jpg)





















