Embed Size (px)
Citation preview

Journal of Gender, Culture, and Health, Vol. 4, No. 2, 1999
Barriers to Prenatal Care for Mexican andMexican American Women
Ippolytos Kalofonos1 and Lawrence A. Palinkas2,3
Despite the presumed health benefits, Latinas are less likely than womenfrom other ethnic groups to receive adequate prenatal care during theirpregnancy. However, it is unclear whether this trend is the result of politicaleconomic conditions that limit access of many Latinos in the United Statesto adequate health services in general, or of sociocultural conditions thatrestrict the use of such services even when they are made available. Further-more, it is unclear whether these barriers pose a risk for adverse birth out-comes in this population. To address these issues, we conducted a two-phasestudy of the political economic and sociocultural barriers to use of prenatalcare services among Mexican and Mexican American women living in SanDiego, California, and their association with adverse birth outcomes in thispopulation. A quantitative assessment of information abstracted from themedical records of 173 Latinas who had given birth at a university medicalcenter found that absence of Medi-Cal benefits or other forms of healthinsurance was the only significant predictor of inadequate prenatal careduring pregnancy. However, neither lack of insurance nor adequate prenatalcare was associated with any adverse birth outcomes. A qualitative analysisof information obtained from interviews of 30 Latinas receiving prenatalcare services at a medical clinic for the homeless and medically underservedresidents of San Diego identified three major themes underlying the lack ofadequate prenatal care: lack of trust in formal versus informal institutions,wanted versus unwanted pregnancies, and the importance of the socialnetwork.
KEY WORDS: prenatal care; access to care; health services; Hispanics; women.
'University of California, Berkeley-University of California, San Francisco Joint MedicalProgram.
Department of Family and Preventive Medicine, University of California, San Diego.'Correspondence should be addressed to Dr. Lawrence A. Palinkas, Department of Familyand Preventive Medicine, University of California, San Diego, 9500 Oilman Drive, La Jolla,California 92093-0807.
135
1087-3201/99/0600-0135$16.00/0 © 1999 Plenum Publishing Corporation
INTRODUCTION
Prenatal care has long been supported as a cost-effective means toreduce the risks of low birthweight and other pregnancy complications, aswell as a method of providing important medical and nutritional advice topregnant women (Alexander & Korenbrot, 1995; Ross, Sandhu, Bemis,Nessim, Bragonier, & Hobel, 1994; Schramm, 1992). With some variation,prenatal care consists of 10-14 visits to the provider, initiated in the firsttrimester, in which the patient is screened for medical conditions, adminis-tered physical exams, and provided educational and counseling services.In very low income populations, women also are given assistance withenrolling in Medicaid and placement in social services and food supportprograms. However, Latinas are less likely than women from other ethnicgroups in the United States to utilize prenatal care services (Centers forDisease Control and Prevention, 1996; Fullerton, Palinkas, & Cavero, 1991).For instance, a study of 587 Mexican and Mexican American women whodelivered at five hospitals in San Diego County found that only 50% ofthese women entered prenatal care in the first trimester and 18% did notreceive any care (Wallace & Fullerton, 1996). A study by Chavez, Cornelius,and Jones (1986) found that 16.4% of Mexican immigrant women did notreceive prenatal care compared to 1.5% of the non-Latino study partici-pants. When only undocumented immigrants were considered, the percent-age of Mexican women who failed to receive adequate prenatal care waseven higher (20.1%). Those who were uninsured were three times less likelyto seek care than the insured, and in San Diego, only one-fifth of Mexicanimmigrants without insurance sought care within the previous 6 months(Chavez, Flores, & Lopez-Garza, 1992).
In general, Latinos are less likely than other Americans to be coveredby medical insurance (Valdez, Morgenstern, Brown, Wyn, Wang, & Cum-berland, 1993b). While 35-37 million Americans are without health insur-ance, Latinos represent a disproportionate share of this total (Valdez etal, 1993b). In 1989, 7 million Latinos, representing 33% of the Latinopopulation in the United States, were uninsured, compared with 23% ofBlacks and 13% of Whites (Valdez, Giachello, Rodrigueztrias, Gomez, &De La Rocha, 1993a). Health insurance coverage has been found to bethe most important predictor of access to health care (Hubbell, Waitzkin,Mishra, Dombrink, & Chavez, 1991). The effects of restricted access toinsurance are significant, as Valdez et al (1993b) report that Latinos withouthealth insurance received half as much care as those with health insurance.Lack of health insurance is also an important predictor of lack of prenatalcare (Higgins & Burton, 1996).
Access to health insurance, however, does not translate into automatic
Kalofonos and Palinkas136

utilization of services. In California, for instance, the publically fundedMedi-Cal program has provided access to health services to both undocu-mented and legal immigrants since 1988 (Braveman, Bennett, Lewis, Eg-erter, & Showstack, 1993), but studies have indicated that Medi-Cal eligibil-ity does not necessarily translate into adequate prenatal care for recipients(Braveman et al, 1993; Moore & Hepworth, 1994; McDonald & Coburn,1988; Valdez et al., 1993a). Even when financial barriers are lifted, otherobstacles to care still exist. Such obstacles may include the location of fewphysicians in Latino communities (Valdez et al., 1993b) and the lack oftransportation and child care necessary for visiting a physician who doesnot practice within the community (Lia-Hoagberg, Rode, Skovholt, Oberg,Berg, Mullett, & Choi, 1990; Zaid, Fullerton, & Moore, 1996). The lack ofLatino health care providers and poor communication between Latinopatients and non-Latino doctors because of language problems and lackof "cultural competency" also restrict access to health services (Valdez etal, 1991a, p. 536). Zaid et al. (1996) also found that many women wholacked prenatal care did not have information as to where and how it couldbe obtained.
Changing political attitudes toward immigrants in general and undocu-mented immigrants in particular constitutes another important barrier tohealth services access and utilization. In 1986, the passage of the omnibusBudget Reconciliation Act (OBRA) and the Immigration Reform andControl Act (IRCA) permitted states to expand Medicaid coverage toundocumented aliens. In response to these changes, California began stead-ily increasing the medical services provided to undocumented immigrants.By 1989, Medi-Cal coverage had been extended to labor and deliveryservices for all women, including undocumented immigrants and temporaryvisitors with incomes less than 185% of the federal poverty level. In addition,the state provided prenatal care services for undocumented immigrantswho met these income criteria. In 1990, the income eligibility was increasedto 200% of the poverty level.
In recent years, however, prenatal care for undocumented residentshas the subject of intense public debate. In California, former GovernorPete Wilson's efforts to cut Medi-Cal-provided prenatal health care fol-lowed the 1994 passage of Proposition 187, a measure which restrictedaccess to all state-funded programs by noncitizens. Although there is littleevidence to support Wilson's claim that such services constitute a "magnet"for undocumented women seeking public benefits and U.S. citizenship fortheir babies (Scott, 1996), a state appeals court order in January 1998allowed the state to enforce the cutoff, and the state announced it wouldstop accepting applications from illegal immigrants for Medi-Cal-fundedprenatal care on March 1 and cut off current recipients a month later (San
Barriers to Prenatal Care 137

Diego Union-Tribune, 1998). This restriction is believed to affect nearly75,000 undocumented women in the state of California who receive prenatalcare through Medi-Cal-sponsored programs each year, 6,000 in San Diegoalone (Scott, 1996).
Although this mandate has once again been stalled in court, allowingthe prenatal programs to continue, these actions have been bolstered bynew federal reforms which have permitted states to deny immigrants bene-fits, such as the Personal Responsibility and Work Opportunity Reconcilia-tion Act of 1996. One of the effects of this bill is the prohibition of accessto all federal means-tested public benefits for at least 5 years among thoseimmigrants who entered the country after the law's enactment. This includesMedicaid and the Maternal and Child Health Services block grant, whichis commonly used for prenatal care (Minkoff, Bauer, & Joyce, 1997). Thenew federal law has rendered undocumented immigrants ineligible for mostfederal public benefits, unless a state legislates otherwise.
Culturally based attitudes, beliefs, and behaviors regarding prenatalcare are another potential predictor of service utilization. For instance, astudy by Lia-Hoagberg et al. (1990) found a correlation between emotionalresponse and attitude toward the pregnancy and receipt of prenatal care.Eighty-five percent of the women who received inadequate prenatal carehad unplanned pregnancies, compared to 72% of those with adequate care.More significantly, 64% of the adequate cares were happy about the preg-nancy, while only 25% of the inadequate cares expressed this sentiment.This study also found personal support systems to be significant, as 40%of the inadequate cares had significant family problems compared to 15%of the adequate cares.
As Gundelman (1995) observes, the failure of Latinas to seek prenatalhealth care presents us with somewhat of a paradox: despite the dramaticdifference in risk profiles, Mexican American women enjoy pregnancyoutcomes that are comparable to the Anglo women. The paradox is moreaccentuated among foreign-born women, who are poorer than their U.S.-born counterparts. Gundelman's explanation for this paradox is that immi-grants bring with them values, attitudes, and health behaviors that mayprotect them from adverse pregnancy outcomes. Included among theseprotective factors are a very low use of tobacco, alcohol, or illicit drugs;good nutrition; a strong sense of family and social support; and a positiveattitude toward childbearing. These factors may buffer women against thestresses of poverty or directly contribute to positive outcomes by bolsteringthe immune and hormonal systems.
This paradox raises the second major question addressed in this study,which is whether prenatal care is really necessary for this particular groupof women. Several studies have found that participation in a comprehensive
138 Kalofonos and Palinkas

prenatal care program results in significantly reduced rates of lowbirthweight and perinatal mortality, as well as considerable economic sav-ings (Korenbrot, 1985; Moore, Origel, Key, & Resnik, 1986; Wilson, Mun-son, Schubot, Leonardson, & Stevens, 1992). However, Alexander andKorenbrot (1995) point out that despite a nationwide effort to reducefinancial barriers to prenatal health care through the expansion of Medicaidbetween 1981 and 1991, the incidence of low birthweight in the UnitedStates increased, as did the proportion of women getting care in the thirdtrimester. Alexander and Korenbrot cite evidence that prenatal health careis associated with reduced rates of low birthweight only in mature, full-term infants. It has been effective in preventing neither fetal growth retarda-tion nor preterm births. Self-selection bias is a concern in the interpretationof research in this area, as health-conscious women may be more likely toinitiate early prenatal care and maintain the schedule of visits. These womenmay already possess favorable beliefs and health-seeking behaviors suchas a good diet and abstention from the use of alcohol, tobacco, and drugs,and thus already are more likely to have healthier infants. The cost-effec-tiveness may be overemphasized because of the unmeasured differencesin women who do and do not use prenatal care and the ambiguous effective-ness of the preterm prevention programs.
The objective of this study was to examine the political economic andsociocultural barriers to use of prenatal care services among Mexican andMexican American women living in San Diego, California, and to determinewhether the lack of adequate prenatal care was associated with adversebirth outcomes in this population. This investigation was conducted intwo phases: a quantitative assessment of information abstracted from themedical records of 173 Latinas who had given birth at a university medicalcenter, and a qualitative analysis of information obtained from interviewsof 30 Latinas receiving prenatal care services at a medical clinic for thehomeless and medically underserved residents of San Diego.
METHODS
Phase I
The subjects for the first phase of this study were 173 Mexican andMexican American women who had given birth at the UCSD MedicalCenter over a 10-month period (May 1997 through February 1998). Of the113 women who gave birth with two or fewer prenatal care visits at theMedical Center during this period, 89 (78.8%) were Mexican or MexicanAmerican. Eighty-four Latinas who had attended three or more prenatal
Barriers to Prenatal Care 139

care visits (considered by hospital staff as meeting the minimal requirementfor prenatal care) and had given birth at the Medical Center were selectedat random to serve as a control group. The following information wasabstracted from the medical charts of each study participant: age, birthplace,citizenship, marital status, possession of a social security number, healthinsurance status, gravidy, parity, birth weight, APGAR scores at 1 and 5min, and history of tobacco, alcohol, and substance use. Women wereconsidered substance users if they reported using any illegal drugs (mari-juana, heroin, methamphetamines, cocaine), tobacco, or alcohol during thepregnancy regardless of the frequency of the use, or showed positive bloodtest results for drug use during labor and delivery.
Data were analyzed with the assistance of the Statistical Package forthe Social Sciences/PC+ program for IBM PC. Comparisons of social anddemographic characteristics and birth outcomes between women with threeor more prenatal care visits and women with less than three visits were madeusing chi-square tests for categorical variables and independent sample ttests for continuous variables. Multivariate logistic regression was used todetermine the independent odds of receiving prenatal care for each socialand demographic characteristic examined, and the odds of delivering a low-birthweight infant.
Phase II
In order to clarify and expand upon the information gained from thechart review, interviews were also conducted with a sample of pregnantwomen of the same culture and socioeconomic status as the chart reviewcohort. The interviews were conducted at a medical clinic near downtownSan Diego, located on the edge of a low-income, predominantly Latino,neighborhood. The clinic is a part of a comprehensive social services centerthat caters primarily to the homeless, but offers free services to patientswho cannot afford the cost of medical care regardless of residential status,and who do not have any form of health insurance, including Medi-Cal. Itis also affiliated with the UCSD Medical Center, and most of the pregnantwomen who are seen at the clinic give birth at the UCSDMC.
Over 90% of the prenatal care patients who visit the clinic are Mexicanor Mexican American and over 50% of these women are undocumented.Between 70 and 75 patients are seen each week in the prenatal clinic, with15-16 of these new intakes. Thirty Latina women were interviewed whilethey were at the clinic for a prenatal care appointment. After the medicalportion of the visit was completed, women were asked by one of the prenatalcare providers (all bilingual Latinas) if they would be willing to answer
140 Kalofonos and Palinkas

some questions regarding their experiences with prenatal care. The womenwere assured confidentiality and anonymity by the providers as well as theinterviewer, and also were provided with a consent form that explainedthe purpose of the study. Interviews lasted an average of 17 min, with thelongest and shortest lasting 30 and 5 min, respectively. Questions were bothopen-ended and closed. Using the information gleaned from chart reviewdiscussed above as a starting point, women were asked to talk about theirexperiences in trying to get prenatal care and whether they sought Medi-Cal.The interview focused on pregnancy history, attitude toward pregnancy,and experiences in seeking care. Women were not explicitly questionedregarding their legal status, but many women either directly or indirectlyvolunteered this information. The interviews were intended to be conversa-tional rather than question and answer in format, and the informationsought was more qualitative than quantitative. The patients themselvesoften directed the interviews, addressing the issues they believed to bemost important. As a result, all the women did not address the same themes,but a few relevant topics were brought up by most of the patients. All butthree of the interviews were conducted in Spanish.
Interview transcripts were compiled based on notes taken during theinterview. Themes were extracted using a methodology of "Coding Consen-sus, Co-occurrence, and Comparison" outlined by Willms, Best, Taylor,Gilbert, Wilson, Lindsay, and Singer (1990). Individual case studies weredeveloped from the interview transcripts, detailing the account of the inter-viewee using the same language and phrases as those utilized by the speakerwhenever possible. The case studies were then reviewed and cooccurringthemes were noted. In this fashion, the factors associated with inadequateprenatal care could be extracted and cultural idioms and social and culturalmeanings could be identified. The dominant themes were thus identifiedand are discussed below.
RESULTS
Phase I
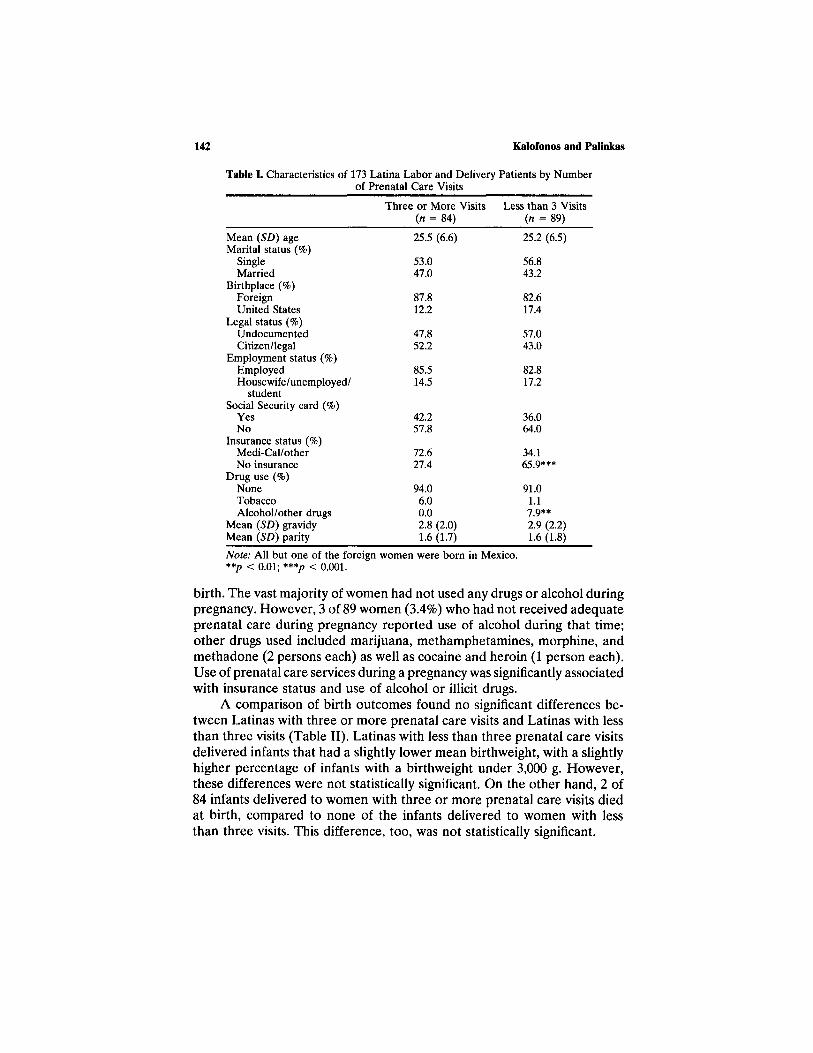
The characteristics of the Latina participants in the Phase I study aresummarized in Table I. The average age of these women was approximately25 years, and most were born in Mexico. For the most part, these womenwere not employed outside the home, and only 40% even had a socialsecurity card. In part, this can be attributed to the fact that more than halfof these women were not legal residents of the United States. A little morethan half of the study sample were married at the time they had given
Barriers to Prenatal Care 141
Kalofonos and Palinkas
birth. The vast majority of women had not used any drugs or alcohol duringpregnancy. However, 3 of 89 women (3.4%) who had not received adequateprenatal care during pregnancy reported use of alcohol during that time;other drugs used included marijuana, methamphetamines, morphine, andmethadone (2 persons each) as well as cocaine and heroin (1 person each).Use of prenatal care services during a pregnancy was significantly associatedwith insurance status and use of alcohol or illicit drugs.
A comparison of birth outcomes found no significant differences be-tween Latinas with three or more prenatal care visits and Latinas with lessthan three visits (Table II). Latinas with less than three prenatal care visitsdelivered infants that had a slightly lower mean birthweight, with a slightlyhigher percentage of infants with a birthweight under 3,000 g. However,these differences were not statistically significant. On the other hand, 2 of84 infants delivered to women with three or more prenatal care visits diedat birth, compared to none of the infants delivered to women with lessthan three visits. This difference, too, was not statistically significant.
142
Table I. Characteristics of 173 Latina Labor and Delivery Patients by Numberof Prenatal Care Visits
Mean (SD) ageMarital status (%)
SingleMarried
Birthplace (%)ForeignUnited States
Legal status (%)UndocumentedCitizen/legal
Employment status (%)EmployedHousewife/unemployed/
studentSocial Security card (%)
YesNo
Insurance status (%)Medi-Cal/otherNo insurance
Drug use (%)NoneTobaccoAlcohol/other drugs
Mean (SD) gravidyMean (SD) parity
Three or More Visits(« = 84)
25.5 (6.6)
53.047.0
87.812.2
47.852.2
85.514.5
42.257.8
72.627.4
94.06.00.02.8 (2.0)1.6 (1.7)
Less than 3 Visits(« = 89)
25.2 (6.5)
56.843.2
82.617.4
57.043.0
82.817.2
36.064.0
34.165.9***
91.01.17.9**2.9 (2.2)1.6 (1.8)
Note: All but one of the foreign women were born in Mexico.**p < 0.01; ***/> < 0.001.
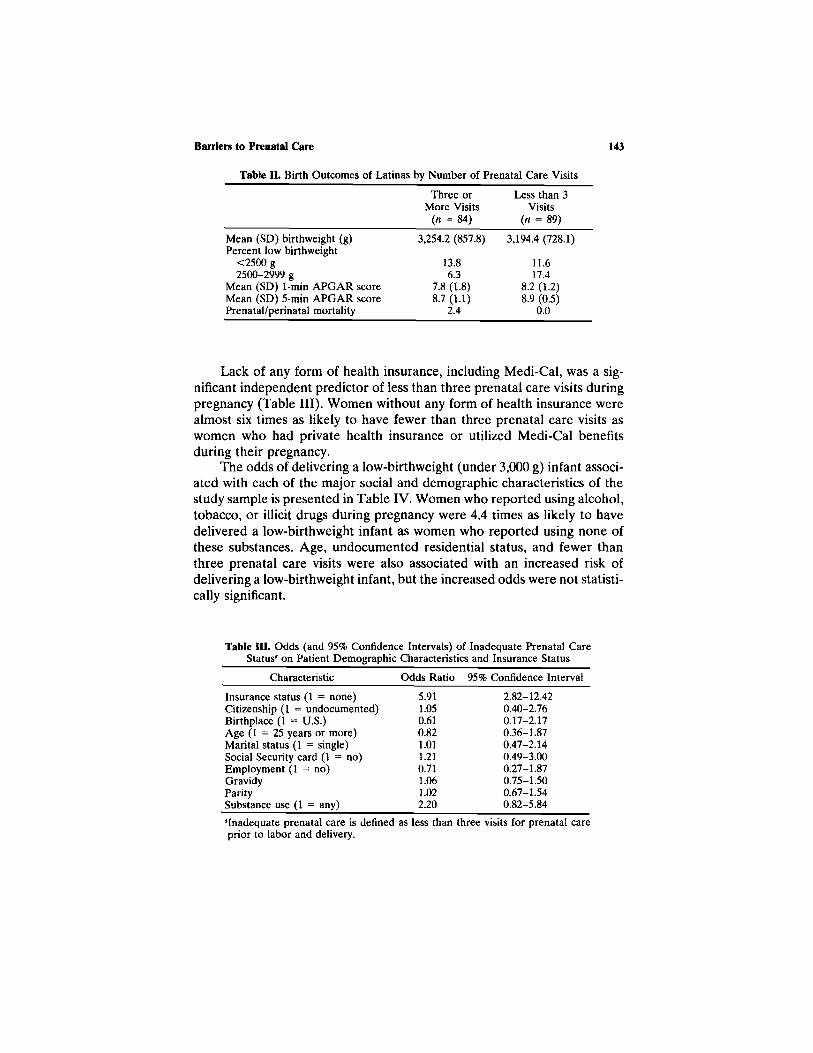
Lack of any form of health insurance, including Medi-Cal, was a sig-nificant independent predictor of less than three prenatal care visits duringpregnancy (Table HI). Women without any form of health insurance werealmost six times as likely to have fewer than three prenatal care visits aswomen who had private health insurance or utilized Medi-Cal benefitsduring their pregnancy.
The odds of delivering a low-birthweight (under 3,000 g) infant associ-ated with each of the major social and demographic characteristics of thestudy sample is presented in Table IV. Women who reported using alcohol,tobacco, or illicit drugs during pregnancy were 4.4 times as likely to havedelivered a low-birthweight infant as women who reported using none ofthese substances. Age, undocumented residential status, and fewer thanthree prenatal care visits were also associated with an increased risk ofdelivering a low-birthweight infant, but the increased odds were not statisti-cally significant.
Table III. Odds (and 95% Confidence Intervals) of Inadequate Prenatal CareStatus" on Patient Demographic Characteristics and Insurance Status
Characteristic
Insurance status (1 = none)Citizenship (1 = undocumented)Birthplace (1 = U.S.)Age (1 = 25 years or more)Marital status (1 = single)Social Security card (1 = no)Employment (1 = no)GravidyParitySubstance use (1 = any)
Odds Ratio
5.911.050.610.821.011.210.711.061.022.20
95% Confidence Interval
2.82-12.420.40-2.760.17-2.170.36-1.870.47-2.140.49-3.000.27-1.870.75-1.500.67-1.540.82-5.84
"Inadequate prenatal care is defined as less than three visits for prenatal careprior to labor and delivery.
Barriers to Prenatal Care 143
Table II. Birth Outcomes of Latinas by Number of Prenatal Care Visits
Mean (SD) birthweight (g)Percent low birthweight
<2500g2500-2999 g
Mean (SD) 1-min APGAR scoreMean (SD) 5-min APGAR scorePrenatal/perinatal mortality
Three orMore Visits
(n = 84)
3,254.2 (857.8)
13.86.3
7.8 (1.8)8.7 (1.1)
2.4
Less than 3Visits
(n = 89)
3,194.4 (728.1)
11.617.4
8.2 (1.2)8.9 (0.5)
0.0

Phase II
Twenty-eight of the 30 women interviewed had been born in Mexicoand all currently reside in San Diego. Three of the women had been livingin the United States for less than 1 year, but 8 had resided north of theborder for over 10 years. The average length of residence in San Diego forthose who were born in Mexico was 7.9 years, with 2 having been in theUnited States as little as 1 year and 4 for over 15 years. The average agewas 26.3 years, and the women had had an average of 1.4 previous children.Twelve of the women initiated prenatal care in the first trimester, 10 inthe second trimester, and 6 in the third trimester (no information on dateof first prenatal care visit was available on the remaining 2 women).
Nearly every woman interviewed had a unique story describing hercircumstances and experiences in seeking prenatal care. However, threemajor themes emerged from the analysis of the interview transcripts. Thefirst theme was the issue of trust or lack of trust in formal versus informalinstitutions. This theme emerged in the context of discussions about Medi-Cal eligibility. Since the chart review established lack of health insuranceas the only statistically significant correlate to inadequate prenatal care, allof the women were asked whether they had health insurance and if theyhad applied for Medi-Cal. Only 4 of the women interviewed at the clinichad any form of health coverage: two had comprehensive Medi-Cal cover-age and 2 had restricted Medi-Cal, to cover prenatal care and the birth.
Nevertheless, every patient interviewed had heard of Medi-Cal andhad at least considered applying. Of the 26 women who did not currentlyhave Medi-Cal, only 1 expressed no interest in obtaining it. One womanhad applied and been turned down, and 3 others were unable to provide
144 Kalofonos and Palinkas
Table IV. Odds (and 95% Confidence Intervals) of Low Birthweight on PatientDemographic Characteristics, Insurance Status, and Prenatal Care Status
Characteristic
Prenatal care status (1 = lessthan 3 visits)
Insurance status (1 = none)Citizenship (1 = undocumented)Birthplace (1 = U.S.)Age (1 = 25 years or more)Marital status (1 = single)Social Security card (1 = no)Employment (1 = no)GravidyParitySubstance use (1 = any)
Odds Ratio 95% Confidence Interval
1.51
0.981.74o:eo1.601.080.400.710.741.034.39
0.62-3.67
0.40-2.420.56-5.410.15-2.470.61-4.220.45-2.580.15-1.110.25-2.000.51-1.070.66-1.591.60-12.05

sufficient documentation that they were permanent residents of California.Four had applied and were awaiting an answer, and 1 had decided not toapply because she was denied services 4 years earlier. Of the remaining 16women, 13 expressed a reluctance to even apply for Medi-Cal because ofthe possible repercussions on their legal status.
Although individual reasons for not applying varied, one theme re-mained constant: these women did not trust the Medi-Cal application pro-cess because of a perceived connection it has with the Immigration andNaturalization Services (INS), endangering those who are not citizens orare undocumented. One woman claimed she was going to apply, but alawyer advised her not to because it could "cause trouble because of mypapers." Another woman frankly expressed her fear, saying, "Me da miedoaplicar," "I am scared to apply because of my papers." She felt her undocu-mented status made her too vulnerable to report information to Medi-Cal.When asked whether she applied to Medi-Cal, a third woman replied,"Queria y no queria," "I wanted to and I didn't want to. I need it to payfor medicine, but I asked if it could affect my chances of getting citizenshipand they told me to ask Immigration [and Naturalization Services]." Sheimmediately withdrew her application because "I don't have papers. I knowpeople who could not become citizens because they had gotten welfareand Medi-Cal." Two other women expressed a desire to apply for Medi-Cal, but did not because their husbands were applying for citizenship andthey did not want to affect their chances. Their fears were based on the beliefthat the INS would have access to the information on their application, andthat as undocumented residents seeking access to public services, theywould endanger the status of their husbands. Indeed, undocumented Medi-Cal recipients who later attempt to legalize their status could be considereda public charge for having once used government-funded health servicesand could thereby be denied legal status, a policy which makes it difficultfor undocumented immigrants to accept such payment programs (Chavezet al, 1992).
The lack of trust in public and governmental institutions may also leadto the choice of this particular clinic, which is affiliated with the CatholicChurch and provides a safe and comfortable aura of security for the women,most of whom are Catholic. In addition, the regular prenatal staff is bilingualand bicultural. The waiting room is often filled with Latino patients as well,and their Spanish conversations add a familiar ambience for a young motherwho is nervous of not only having a baby, but also about being threatenedby deportation. The location of the clinic near one of San Diego's oldestMexican barrios further establishes it as a safe haven.
This lack of trust in public institutions is a common experience amongMexican immigrants and stems from three sources. The first is previous
Barriers to Prenatal Care 145

experience with public institutions in Mexico, often perceived as corruptand outside the bounds of extended kin ties, where trust has traditionallyresided in Mexican society. The second source is experience with publicinstitutions in the United States, often seen as impersonal (hence the lackof accurate information on eligibility) and threatening (as exemplified byaccounts of acquaintances who were caught by the INS or proclaimedineligible for citizenship because they had used Medi-Cal services in thepast). The third source is from perceptions of their own legal (valid or not)and/or moral entitlement to access to these institutions. Many of thesewomen believed they were not morally entitled because they would beaccepting a handout without any structure of reciprocity. The principle ofreciprocity, social exchange based on confianza or fundamental trust, gov-erns the structure of extended kin relations which forms the basis of socialrelationships in Mexico (Alvarez, 1987). These networks of reciprocal rela-tionships of trust have been documented in communities outside MexicoCity (Lomnitz, 1977), in southern Baja California, and in immigrant commu-nities in the San Diego area (Alvarez, 1987). Mexicans immigrate to theUnited States to find work and to make money, not to receive publicbenefits. Evidence indicates that undocumented Mexicans actually under-utilize U.S. health services because of an expressed reluctance to receiving"handouts," as welfare and Medi-Cal are often perceived (Chavez et al,1992).
The issue of trust is also reflected in the sources of information andinfluence that led to the use of this particular clinic for prenatal care. Elevenof the 18 women said they heard about the clinic through informal, word-of-mouth networks, from relatives or friends. Of these 11, 2 began in thefirst trimester, 6 in the second, and 3 in the third. One of the women whobegan in the first trimester reported, "I wanted to go to a clinic when Ifound out I was pregnant, and my uncle told me about this one, so this isthe first one I came to." Another first-trimester initiate explained, "I wasfrightened [of applying for Medi-Cal] . . . but my mother-in-law told meabout the clinic, so I came in." These women feel they can trust the advicegiven by friends and relatives more than a referral from a provider or asocial service worker.
A second theme that emerged from the analysis of interview transcriptswas the attitudes of the women toward their pregnancy. Fourteen of the19 women who were asked whether their pregnancies had been plannedanswered negatively. Of these 14 women, 11 had initiated care after thefirst trimester, including all 6 of those who had initiated care in the thirdtrimester. One woman who began care in the third trimester answered,"None of my pregnancies have been planned. I don't need more kids . . .I don't want to have any more." Her statement reveals feelings of resent-
Kalofonos and Palinkas146

ment and frustration toward the pregnancy. This may have affected herlate initiation of care, but she had not received adequate prenatal care forher previous four pregnancies either. Another late initiate expressed similarfeelings toward her pregnancy: "I feel restricted. I'd like to work but Ican't. I already had three children who have grown up ... with the babycome worries. . .but he [the husband] is happy." Both of these womenseem to perceive their pregnancies as burdens that had been imposed uponthem by circumstances beyond their control.
Other women did not share this view. Although her pregnancy wasunplanned, one patient said it "has brought the family closer together."She appeared very excited and happy about the pregnancy, and initiatedcare in the first week. Another patient who had planned her pregnancyand began care in the first trimester also spoke very positively about herexperience, claiming, "I take better care of myself because the baby isalways on my mind." Another woman who planned the pregnancy begancare late, however, as did a women who initiated care in the second trimesterdespite the fact that she knew about the pregnancy in the first week. Sheaccounted for the delay by saying, "I was very busy because of my work.I did not know free care was available and was not sure if I could afford it."
Although not the rule, unplanned pregnancies appear to be associatedwith inadequate care. A much stronger association, however, appears toexist between inadequate care and undesired pregnancies. Pregnancies that,planned or unplanned, represent something desirable or positive in outcomeare more likely to result in the initiation of prenatal care during the firsttrimester, while pregnancies that represent a burden, a limitation to auton-omy, or more undesired responsibilities for the woman are more likely toresult in delayed initiation of prenatal care to the second or third trimester.The issue of attitude toward pregnancy is important because it reflects thepossibility that there is a trend among Mexican immigrants in the UnitedStates and possibly other Latina immigrants for pregnancies to be unplannedor unwanted. They are unplanned because migration and the accompanyingsocial and cultural transitions bring with them an alteration of expectationsregarding male/female relationships and the rights and responsibilities ofwomen (Vega, 1990). There may also be a lack of understanding of the avail-able methods of contraception or the use of contraceptive methods in thefamily planning decisions of women who are caught in overlapping, coexistingsocial and cultural contexts. The pregnancies are unwanted because of a rec-ognition that large families are not as desirable in a largely urbanized UnitedStates as they are in largely rural Mexico because they limit the opportunitiesfor women in the United States to seek employment (the primary reason forimmigrating to the United States for single women) or because they lack thesocial resources necessary to give birth and raise children that are normally
Barriers to Prenatal Care 147

provided in Mexico by the extended kin group. Some women are, of course,lucky enough to have either their extended family or that of their husband'sclose by, but for many of the patients interviewed here, especially the singlewomen, this was not the case.
A third theme to emerge from the interviews was the role of socialsupport in initiating and maintaining adequate prenatal care. Of the womenwho had initiated care in the first trimester, eight were either married orliving with the father of the child, while one was living with a sister. Fiveof the second-trimester initiates were married or living with the father, andthree were single. Of the third-trimester initiates, one was married and fivewere single. A married patient explained the importance of her family'ssupport: "My husband and family care about me a great deal, even thoughhe works long hours. Eight children already live in the house, and we allspeak as though the ninth is among us. I feel like the baby is already animportant part of us all." This woman initiated care in the first trimester.Another early care initiate whose pregnancy was not planned but nonethe-less was "determined to carry it [the baby] to term" also felt her husband'ssupport was crucial in carrying out her decision. In contrast, a single womanwhose partner left her before she knew of her pregnancy began care in thethird trimester. She reported to be happy having the baby, however, because"it is a good time. I am still young."
The issue of social support is important because it reflects a dilemmafaced by many of these women. Their legal status prevents them fromaccessing the social networks and sources of support left behind in Mexico,because proof of frequent returns to Mexico can cause a woman to beconsidered a "border-crosser," a Mexican who simply comes to the UnitedStates to access public benefits. Their caution and insecurity due to theirundocumented status also hinder the creation of new social networks (Mas-sey, Alarcon, Durand, & Gonzalez, 1987). Vega reports that Mexican Amer-ican immigrants tend to "have smaller social networks available than secondgeneration offspring, and to rely on family more exclusively for emotionalnurturance and problem-solving" (Vega, 1990, p. 1019). This social networkseems to be an important determinant of who gets adequate care and whodoes not. Instead of relying on female relatives as they do in Mexico, manyimmigrant women are forced to rely upon their husbands and the networkof family and friends that is available in the United States. Single womenhave even less access to this network by virtue not only of their maritaland legal status, but also perhaps because of a social stigma that beingsingle and pregnant may carry [although Lewis' famous work in a Mexicanvillage maintains there is no stigma attached to illegitimate children ortheir mothers (Lewis, 1970, p. 290), an assertion shared by findings in morecontemporary work with pregnant Latina teens] (Villarruel, 1998).
Kalofonos and Palinkas148

The presence of strong family ties and an extensive social networkhas been hypothesized as a possible explanation to the "Latina Paradox"discussed above. The hypothesis is that Latinas may have successful birthoutcomes despite inadequate prenatal care because they are so well takencare of by their kin (Gundelman, 1995). The findings presented here, how-ever, indicate that marriage and a stable relationship with the father is alsocorrelated with adequate prenatal care. The women who are likely to havea more extensive social network are also more likely to receive adequatecare, while the single women, who have fewer options for social networking,are also more likely to receive inadequate care. Family support results ingreater assistance that encourages and allows women to visit the clinicmore easily. The presence of a greater network of kin also allows thewoman to take time off work and other responsibilities in order to devotemore time and energy to the pregnancy.
DISCUSSION
Our analysis of the medical records of a cohort of Latinas who gavebirth at the Medical Center found that absence of any form of healthinsurance, including Medi-Cal insurance, during pregnancy was the mostsignificant predictor of the lack of adequate prenatal care. Our interviewswith Latina patients also indicated that that many women who are notcitizens fear coming into contact with any state institutions such as Medi-Cal because they run the risk of being caught by the INS. This fear is fueledby anecdotes of immigration officers conducting raids of clinics in whichall patients who cannot prove legal residence are deported, with American-born children placed in foster homes while their mothers are sent south ofthe border. The anti-immigrant legislation in recent years has also contrib-uted to this insecurity in a very real way, as evidenced by studies demonstra-ting a significant reduction in clinic visits after passage of Proposition 187in California in 1994 (Fenton, Catalano, & Hargreaves, 1996; Moss,Baumeister, & Biewener, 1996). These findings support the political econ-omy of the Latino health model (Chavez et al, 1986, 1992), and suggestthat the utilization of prenatal care services of Mexican immigrants andMexican American women in the United States requires a fundamentalrevision of the political and economic system that restricts access to theseimportant services.
However, this model does not provide a complete explanation as towhy these women are not receiving services. There are also importantcultural components to their access and utilization of health services. Thiscan include traditional health beliefs and practices (Gundelman, 1995) or
Barriers to Prenatal Care 149

assistance from friends and relatives or other social contacts (Lia-Hoagbergetai, 1990). Culture can also affect an individual's attitude toward prenatalhealth care as well as health beliefs and behaviors in general. One of theprimary indicators of the importance of culturally determined attitudestoward pregnancy was the finding that relatively few of these women re-ported any drug, alcohol, or cigarette use during their pregnancy, a patternthat has been observed in other studies (Vega, Kolody, Hwang, & Noble,1993). However, none of the women in our own study who received ade-quate care reported any alcohol or drug use, but approximately 8% ofthe inadequate cares did report use of at least one of these substances.Furthermore, substance abuse was the only significant independent pre-dictor of low birthweight in these women. Substance use has a significanthealth impact because prenatal substance exposure has been linked to manyneonatal and obstetrical complications (Finnegan & Kandall, 1992). Animportant aspect of prenatal care is nutritional and substance-use counsel-ing, and the higher rate of substance use in the inadequate care group maybe an indication that these women would benefit from such counseling.
While population-based surveys that identify general barriers serve asimportant guides in examining the access issue, informant-based reportssuch as the one presented here illustrate the mechanisms with which thebarriers operate. In this particular case, these mechanisms involve a complexrelationship between political and economic barriers to prenatal care, espe-cially for undocumented immigrant women, and a set of cultural factorsrelated to the distrust of public institutions. These cultural factors includethe desirability of the pregnancy and the availability of a social networkthat provides key material and emotional support during this importanttime. The accounts the women provided show how the factors are oftenintegrated and woven together to form the substantial barriers that preventthem from receiving prenatal health care. They also include a set of under-standings and behaviors that result in the delivery of healthy babies withoutthe benefits of prenatal care.
ACKNOWLEDGMENTS
This research was supported by a PHS Health Resources and ServicesAdministration Grant No. Src-w D 32 PE10007-03. The authors wish tothank the staff of the St. Vincent de Paul Center Medical Clinic for theirassistance in the Phase II data collection efforts, especially Drs. PatriciaHolland and Charles Abbott, Lupe Diaz, and Alejandra Limon.
ISO Kalofonos and Palinkas

REFERENCES
Alexander, G. R., & Korenbrot, C. C, (1995). The role of prenatal care in preventing lowbirth weight. The Future of the Children, 5(2), 103-120.
Alvarez, R. J. (1987). Familia: Migration and adaptation in Baja and Alta California, 1800-1975. Berkeley, CA: University of California Press.
Braveman, P., Bennett, T., Lewis, C., Egerter, S., & Showstack, J. (1993). Access to prenatalcare following major Medicaid eligibility expansions. Journal of the American MedicalAssociation, 269, 1285-1289.
Centers for Disease Control and Prevention. (1996). Adequacy of prenatal care utilization—California, 1989-1994. Morbidity and Mortality Weekly Report, 45(30), 653-656.
Chdvez, L. R., Cornelius, W. A., & Jones, O. W. (1986). Utilization of health services byMexican immigrant women in San Diego. Women and Health, 11(2), 3-20.
Chavez, L. R., Flores, E. T., & Lopez-Garza, M. (1992). Undocumented Latin Americanimmigrants and U.S. health services: An approach to a political economy of utilization.Medical Anthropology Quarterly, 6(1), 6-26.
Fenton, J., Catalano, R., & Hargreaves, W. A. (1996). Effect of Proposition 187 on mentalhealth service use in California: A case study. Health Affairs, 15, 182-190.
Finnegan, L. P., & Kandall, S. R. (1992). Maternal and neonatal effects of alcohol and drugs.In J. H. Lowinson, P. Ruiz, R. B. Millman, & J. G. Langrod, (Eds.), Substance abuse: Acomprehensive textbook (2nd ed.). Baltimore: Williams & Wilkins.
Fullerton, J. T., Palinkas, L. A., & Cavero, C. (1991). Nurse-midwifery services in one multi-ethnic, underserved community. Journal of Health Care for the Poor and Underserved,2, 293-306.
Gundelman, S. (1995). Immigrants may hold clues to protecting health during pregnancy:Exploring a paradox. 1995 The California Wellness Foundation and University of Califor-nia Wellness Lectures Program. Wellness Lectures, 3, 45-75.
Higgins, P. G., & Burton, M. (1996). New Mexico women with no prenatal care: Reasons,outcomes, and nursing implications. Health Care for Women International, 17(3), 255-269.
Hubbell, F. A., Waitzkin, H., Mishra, S. I., Dombrink, J., & Chavez, L. R. (1991). Access tomedical care for documented and undocumented Latinos in a southern California county.Western Journal of Medicine, 154, 414-417.
Korenbrot, C. C. (1984). Risk reduction in pregnancies of low-income women. Mobius, 4(3),8-15.
Lewis, O. (1970). Life in a Mexican village: Tepoztldn restudied. Urbana, IL: University ofIllinois Press.
Lia-Hoagberg, B., Rode, P., Skovholt, C., Oberg, C., Berg, C., Mullett, S., & Choi, T. (1990).Barriers and motivators to prenatal care among low-income women. Social Science andMedicine, 30(4), 487-495.
Lomnitz, L. A. (1977). Networks and marginality: Life in a Mexican shantytown. New York:Academic Press.
Massey, D. S., Alarc6n, R., Durand, J., & Gonzalez, H. (1987). Return to Aztlan: The socialprocess of international migration from western Mexico. Berkeley, CA: University ofCalifornia Press.
McDonald, T. P., & Coburn, A. F. (1988). Predictors of prenatal care utilization. Social Scienceand Medicine, 27(2), 167-172.
Minkoff, H., Bauer, T., & Joyce, T. (1997). Welfare reform and the obstetrical care of immi-grants and their newborns. New England Journal of Medicine, 337(10), 705-707.
Moore, P., & Hepworth, J. T. (1994). Use of perinatal and infant health services by Mexican-American Medicaid enrollees. Journal of the American Medical Association, 272(4),297-304.
Moore, T. R., Origel, W., Key, T. C., & Resnik, R. (1986). The perinatal and economic impactof prenatal care in a low socio-economic population. American Journal of Obstetrics andGynecology, 154(1), 29-33.
Barriers to Prenatal Care 151

Moss, N., Baumeister, L., & Biewener, J. (1996). Perspectives of Latina immigrant womenon Proposition 187. Journal of the American Medical Women's Association, 54(4), 161-165.
Ross, M. G., Sandhu, M., Bemis, R., Nessim, S., Bragonier, R., & Hobel, C. (1994). The WestLos Angeles Preterm Birth Prevention Project: II. Cost-effectiveness analysis of high-risk pregnancy interventions. Obstetrics and Gynecology, 83, 506-11.
San Diego Union-Tribune. (1998, January 30). Illegal immigrant prenatal care cutoff set. SanDiego Union-Tribune, A-5.
Scott, M. (1996, November 22). No savings for California taxpayers. San Diego Union-Tribune,B-ll, B-13.
Schramm, W. F. (1992). Weighing costs and benefits of adequate prenatal care for 12,023births in Missouri's Medicaid program, 1988. Public Health Reports, 107(6), 647-652.
Valdez, R. B., Giachello, A. P., Rodrigueztrias, H., Gomez, P., & De La Rocha, C. (1993a).Improving access to health care in Latino communities. Public Health Reports, 108(5),534-539.
Valdez, R. B., Morgenstern, H., Brown, E. R., Wyn, R., Wang, C., & Cumberland, W. (1993b).Insuring Latinos against the cost of illness. Journal of the American Medical Association,269, 889-894.
Vega, W. A. (1990). Hispanic families in the 1980s: A decade of research. Journal of Marriageand the Family, 52(4), 1015-1024.
Vega, W. A., Kolody, B., Hwang, J., & Noble, A. (1993). Prevalence and magnitude ofperinatal substance exposures in California. New England Journal of Medicine, 329(12),850-854.
Villarruel, A. M. (1998). Cultural influences on the sexual attitudes, beliefs and norms ofyoung Latina adolescents. Journal of the Society of Pediatric Nurses, 3, 67-79.
Wallace, H. M., & Fullerton, J. T. (1996). Maternity care for Hispanic women who cross tothe United States side of the Mexico border. Journal of Tropical Pediatrics, 42(6), 335-338.
Willms, D. G., Best, A. J., Taylor, W. T., Gilbert, J. R., Wilson, D. M. C., Lindsay, E.A., &. Singer, J. (1990). A systematic approach for using qualitative methods in primaryprevention research. Medical Anthropology Quarterly, 4(4), 391-409.
Wilson, A. L., Munson, D. P., Schubot, D. B., Leonardson, G., & Stevens, D. C. (1992). Doesprenatal care decrease the incidence and cost of neonatal care intensive care admissions?American Journal of Perinatology, 9(4), 281-284.
Zaid, A., Fullerton, J. T., & Moore, T. (1996). Factors affecting access to prenatal carefor U.S./Mexico border-dwelling Hispanic women. Journal of Nurse-Midwifery, 41(4),277-284.
Kalofonos and Palinkas152





























