Embed Size (px)
Citation preview
Asymmetric Motion Distribution BetweenComponents of a Mobile-Core Lumbar
Disc ProsthesisAn Explanation of Unequal Wear Distribution in Explanted
CHARITE Polyethylene Cores
Avinash G. Patwardhan, PhD, Robert M. Havey, BS, Nicholas D. Wharton, MS, Parmenion P. Tsitsopoulos, MD, PhD,Patrick Newman, MS, Gerard Carandang, MS, and Leonard I. Voronov, MD, PhD
Investigation performed at the Musculoskeletal Biomechanics Laboratory, Edward Hines Jr. VA Hospital, Hines, Illinois
Background: The biconvex mobile core of the CHARITE lumbar disc prosthesis forms two joints (spherical bearings) withthe metal end plates. We quantified the intra-prosthesis motion to test the hypothesis that the total prosthesis motionwould not be equally distributed between the two bearings of implanted CHARITE discs, which might explain the unequalwear distribution reported in explanted cores.
Methods: The hypothesis was tested by studying the flexion-extension motion responses of (1) twenty-six monosegmentalCHARITE III discs implanted in nineteen human cadaveric lumbar spines, and (2) twenty-one CHARITE III discs (fifteenmonosegmental, six bisegmental) implanted in eighteen patients in other published clinical studies. Intra-prosthesis mo-tions were quantified with use of a radiographic image analysis technique.
Results: Eighty-eight percent of the CHARITE discs implanted in cadaveric specimens exhibited larger motion at thesuperior bearing, with 54% demonstrating more than twice as much motion at the superior bearing as at the inferiorbearing. The ratio of motion at the superior bearing to motion at the inferior bearing averaged 2.68 ± 1.84, which wassignificantly larger than 1.0 (p < 0.001). Ninety percent of prostheses implanted in patients showed larger motion at thesuperior bearing. The motion ratio averaged 2.39 ± 2.47 for monosegmental cases and 2.55 ± 2.66 for all cases; bothratios were significantly larger than 1.0 (p < 0.05).
Conclusions: We found preferentially larger motion at the superior bearing of the CHARITE discs implanted in humancadaveric lumbar spines and in patients, regardless of the implanted level.
Clinical Relevance: The findings regarding unequal motion distribution between the dual bearings of mobile-core discprostheses are relevant to improving in vitro wear testing protocols to better replicate in vivo wear-producing conditions.
Total disc replacement has emerged as a treatment al-ternative for managing pain of discogenic origin1,2. TheCHARITE lumbar disc (DePuy AcroMed, Raynham,
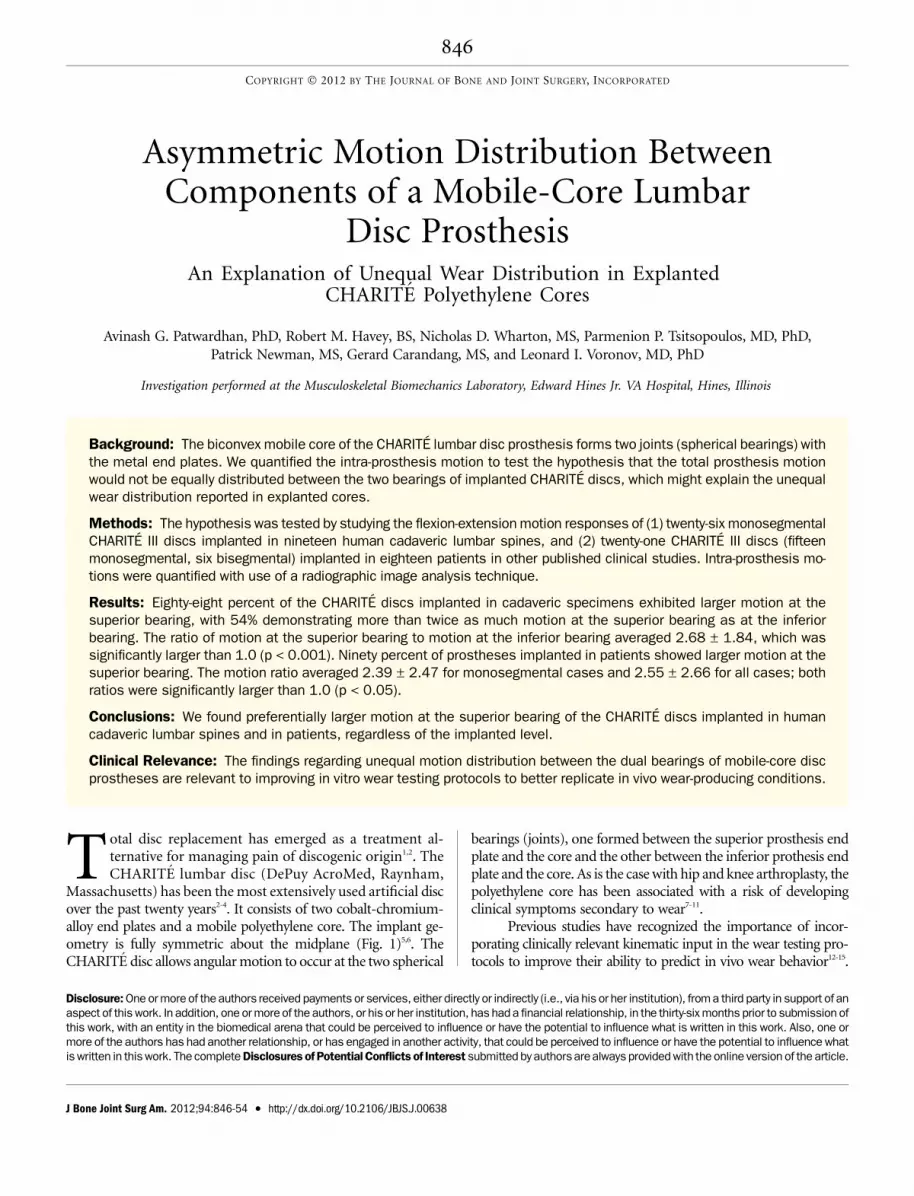
Massachusetts) has been the most extensively used artificial discover the past twenty years2-4. It consists of two cobalt-chromium-alloy end plates and a mobile polyethylene core. The implant ge-ometry is fully symmetric about the midplane (Fig. 1)5,6. TheCHARITE disc allows angular motion to occur at the two spherical
bearings (joints), one formed between the superior prosthesis endplate and the core and the other between the inferior prothesis endplate and the core. As is the case with hip and knee arthroplasty, thepolyethylene core has been associated with a risk of developingclinical symptoms secondary to wear7-11.
Previous studies have recognized the importance of incor-porating clinically relevant kinematic input in the wear testing pro-tocols to improve their ability to predict in vivo wear behavior12-15.
Disclosure: One or more of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of anaspect of this work. In addition, one or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission ofthis work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. Also, one ormore of the authors has had another relationship, or has engaged in another activity, that could be perceived to influence or have the potential to influence whatis written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authorsare always provided with the online version of the article.
846
COPYRIGHT � 2012 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2012;94:846-54 d http://dx.doi.org/10.2106/JBJS.J.00638
The current standards for wear testing of intervertebral disc pros-theses (ISO-18192-116 and ASTM-F2423-0517) specify the cyclicinput profiles of total angular motions between the superiorand inferior end plates of the prosthesis. However, when con-ducting wear tests on prostheses with two spherical bearings,specifying how to distribute the total end-plate-to-end-platemotion between the two bearings becomes problematic becauseof a lack of quantitative data on the intra-prosthesis motiondistribution.
Kurtz et al. performed wear analysis of thirty-eight re-trieved CHARITE artificial lumbar discs18. They measured theheight from the midline to the dome on both sides of theCHARITE core, and the ratio of the two heights was defined asthe symmetry ratio. A symmetry ratio ranging from 0.83 to0.95 was observed in 43% of explanted cores, suggesting anasymmetric distribution of motion between the two bearings ofthe CHARITE disc implanted in patients.
The purpose of the present study was to quantify the mo-tion distribution within CHARITE discs implanted in humanlumbar spinal segments. The primary hypothesis was that the totalprosthesis motion would not be equally distributed between thetwo bearings of a CHARITE disc, which could explain the unequalwear distribution observed in explanted polyethylene cores.
Materials and Methods
The hypothesis was tested by examining the flexion-extension motion re-sponses of (1) twenty-six CHARITE III discs implanted in human ca-
daveric lumbar spines, and (2) twenty-one CHARITE III discs implanted inpatients in previously published clinical studies.
Experimental Study Using Human Cadaveric Lumbar SpinesSpecimensNineteen human cadaveric lumbar spines (L1 to sacrum) were used in the ex-perimental study. The mean donor age was 49.3 ± 10.4 years; eleven donors were
male and eight were female. None of the specimens had radiographic signs ofadvanced degenerative changes. The paravertebral muscles were dissected and thediscs, ligaments, and posterior osseous structures were kept intact. The specimenswere wrapped in saline solution-soaked towels to prevent tissue dehydration.
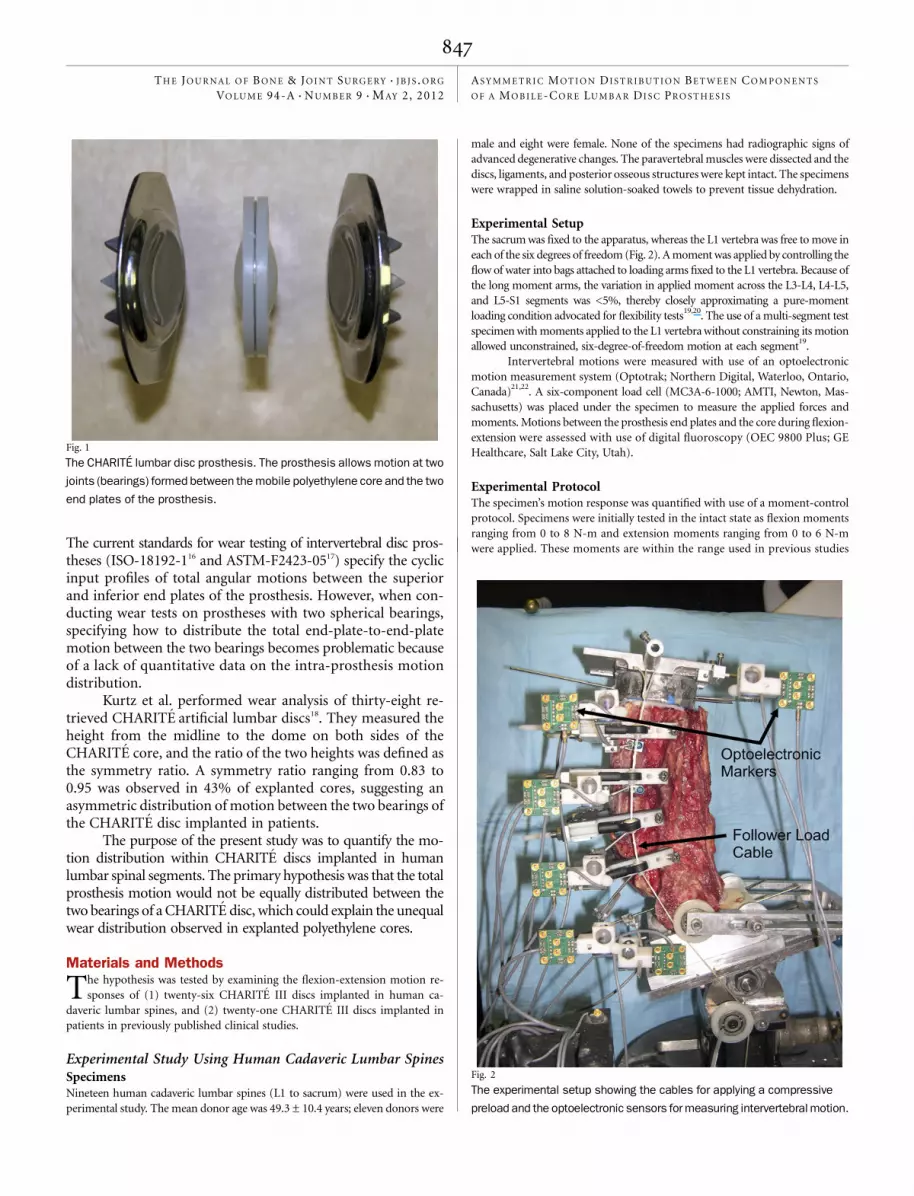
Experimental SetupThe sacrum was fixed to the apparatus, whereas the L1 vertebra was free to move ineach of the six degrees of freedom (Fig. 2). A moment was applied by controlling theflow of water into bags attached to loading arms fixed to the L1 vertebra. Because ofthe long moment arms, the variation in applied moment across the L3-L4, L4-L5,and L5-S1 segments was <5%, thereby closely approximating a pure-momentloading condition advocated for flexibility tests
19,20. The use of a multi-segment test
specimen with moments applied to the L1 vertebra without constraining its motionallowed unconstrained, six-degree-of-freedom motion at each segment
19.
Intervertebral motions were measured with use of an optoelectronicmotion measurement system (Optotrak; Northern Digital, Waterloo, Ontario,Canada)
21,22. A six-component load cell (MC3A-6-1000; AMTI, Newton, Mas-
sachusetts) was placed under the specimen to measure the applied forces andmoments. Motions between the prosthesis end plates and the core during flexion-extension were assessed with use of digital fluoroscopy (OEC 9800 Plus; GEHealthcare, Salt Lake City, Utah).
Experimental ProtocolThe specimen’s motion response was quantified with use of a moment-controlprotocol. Specimens were initially tested in the intact state as flexion momentsranging from 0 to 8 N-m and extension moments ranging from 0 to 6 N-mwere applied. These moments are within the range used in previous studies
Fig. 1
The CHARITE lumbar disc prosthesis. The prosthesis allows motion at two
joints (bearings) formed between the mobile polyethylene core and the two
end plates of the prosthesis.
Fig. 2
The experimental setup showing the cables for applying a compressive
preload and the optoelectronic sensors for measuring intervertebral motion.
847
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

of human lumbar spines18,19,21,23,24
. A compressive follower preload of 400 Nwas applied according to a previously described technique
21,25to simulate
physiologic preloading due to gravity and muscle activity22
.All disc replacement surgical procedures were performed according to
clinical guidelines26
and using the operative technique described in detail in ourprevious cadaveric study
23. The posterior longitudinal ligament was transected
to obtain proper implant positioning23
. Trial implants were used to determineappropriate prosthesis size. The prosthesis midline was centered in the frontalplane and was positioned 1 to 2 mm posterior to the midline of the disc spacein the sagittal plane. Proper placement was confirmed with fluoroscopy. Thespecimens were then tested in flexion-extension.
Twenty-six CHARITE total disc replacements were implanted in nineteenlumbar spines (six at L3-L4, seven at L4-L5, and thirteen at L5-S1) (Table I). Amonosegmental implantation was performed at L3-L4 in six specimens and atL5-S1 in an additional six specimens. In the remaining seven specimens, aCHARITE disc was initially implanted at L5-S1 and motion testing was per-formed. Next, a fusion at L5-S1 was simulated with use of an interbody spacerand pedicle screw instrumentation, and a CHARITE disc was implanted atL4-L5. Motion testing was then repeated as previously described. This allowedassessment of monosegmental total disc replacements at two spinal levels, in acost-effective way, without affecting the motion response of the disc prosthesis.A number of studies
19,20,27have demonstrated that under pure-moment loading
conditions, each motion segment of the specimen is subjected to the same mo-ment; therefore, motion of the L4-L5 total disc replacement will have been un-affected by the adjacent-level fusion.
Data AnalysisFluoroscopic images acquired during flexion-extension were corrected for geo-metric distortion caused by the image intensifier and then analyzed with use of adigital image analysis technique (QMA; Medical Metrics, Houston, Texas). The
ability of the QMA (quantitative motion analysis) technique to produce accuratemeasurements of intervertebral motion from flexion-extension radiographs hasbeen previously validated
28,29. The images were analyzed to calculate (1) motions
occurring between vertebrae before and after prosthesis implantation, (2) totalmotion between the superior and inferior prosthesis end plates, and (3) motiondistribution between the two bearings (Fig. 3).
Statistical AnalysisStatistical analyses were performed with use of SYSTAT software (version 10.2;Chicago, Illinois). Normality of the data for the intervertebral range of motionand for the intra-prosthesis motion distribution was checked with use of theKolmogorov-Smirnov test. All data sets were found to be normally distributed(p > 0.30).
The motions occurring between two vertebrae in cadaveric specimenswere measured by the optoelectronic system and also calculated by QMA ra-diographic analysis of digital fluoroscopic images. The agreement between theradiographic and optoelectronic methods was assessed with use of a Bland-Altman analysis
30. The limits of agreement for the two methods of motion
measurement were ±1.0�.Intra-prosthesis motion distribution was expressed as the motion ratio,
which was defined as the superior-bearing motion divided by the inferior-bearing motion. A one-sample t test was performed to determine whether themotion ratio was significantly different from 1.0, thereby assessing whetherthere was unequal distribution of the prosthesis motion between the twobearings.
An analysis of variance was used to determine whether the preoperativeand postoperative intervertebral motions and the intra-prosthesis motiondistribution were influenced by the level of implantation (segmental level L3-L4, L4-L5, or L5-S1). An a posteriori power analysis was performed to deter-mine the statistical power of the findings in the cadaveric study.
Analysis of Intra-Prosthesis Motion in Clinical CasesThe hypothesis that motion within the mobile-core disc prosthesis is unequallydistributed between the superior and inferior bearings was also tested with useof the motion response of CHARITE discs implanted in patients. A review ofthe scientific literature identified thirty-three clinical studies of CHARITE discs,which were published between 1994 and 2009. Thirteen of the publicationsfeatured flexion-extension radiographs
31-43; however, one of these involved an
earlier prosthesis design (CHARITE II)40
and was therefore excluded fromfurther analysis. Thus, the present study included the clinical cases reported inthe remaining twelve publications (see Appendix). The images were obtainedfrom the original publications in digital (PDF) format at the highest resolutionpossible and stored in an uncompressed file format. Image contrast was
TABLE I Distribution of Twenty-six CHARITE Disc ProsthesesImplanted in Nineteen Human Cadaveric Specimens
SpecimensL3-L4
(N = 6)L4-L5
(N = 7)L5-S1
(N = 13)
1 through 6 CHARITE Intact Intact
7 through 12 Intact Intact CHARITE
13 through 19, initial Intact Intact CHARITE
13 through 19, final Intact CHARITE Fusion
Fig. 3
Radiographic measurement of total prosthesis motion and its distribution between the two bearings. The QMA measurement technique was based on a digital
imagesuperimpositionmethod that tracked themotionofeachdevice componentasan independent object. Total prosthesismotion = (C1 – C2), motionat the
superior bearing = (A1 1 A2), and motion at the inferior bearing = (B1 – B2). In this example of unequal distribution of intra-prosthesis motion in flexion-
extension, total prosthesis motion = 12.3�, motion at the superior bearing = 10.7�, and motion at the inferior bearing = 1.6�, resulting in a motion ratio of 6.7.
848
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

enhanced with use of special filters to optimize implant visualization. One set ofradiographs was eliminated because of inadequate image quality.
Thus, the radiographic analysis was performed on twenty-one im-planted segments in eighteen patients. All of the implants were the CHARITEIII disc prosthesis; ten were implanted at L4-L5 and eleven at L5-S1 (see Ap-pendix)
31-39,41-43. There were fifteen monosegmental disc replacements (seven
at L4-L5 and eight at L5-S1) and six bisegmental disc replacements (three L4-L5and L5-S1 pairs).
To test the reliability of the radiographic measurements, 50% of theimages were randomly selected for reanalysis after an intervening period of atleast eight weeks. The reliability of the measurements was assessed with use ofa Bland-Altman analysis
30, and the limits of agreement for the radiographic
analyses were found to be ±0.5� for angular motion at each bearing of theCHARITE disc. These excellent reliability results are likely due to the ease withwhich the metallic implant components can be tracked with use of the QMAsoftware.
Normality of the motion data was confirmed with use of the Kolmogorov-Smirnov test. The hypothesis that the prosthesis motion was unequally distrib-uted between the superior and inferior joints of the CHARITE disc implantedin patients was tested separately for monosegmental total disc replacements andfor all (monosegmental and bisegmental) total disc replacements. An a poste-riori power analysis was performed to determine the statistical power of thefindings.
Source of FundingResearch funding for this study was received from the U.S. Department ofVeterans Affairs.
ResultsAnalysis of Prosthesis Motion in Cadaveric Specimens
Preoperatively, the flexion-extension range of motion be-tween the vertebrae averaged 8.4� ± 3.2�. After disc re-
placement, the average range of motion for the twenty-siximplanted segments increased to 11.1� ± 2.7� (p < 0.01).
The total prosthesis motion (between the superior andinferior prosthesis end plates) averaged 10.4� ± 2.4� (Table II).The small discrepancy between the total prosthesis motion andthe intervertebral motion can be attributed to a combination ofradiographic measurement accuracy limitations and interfacemotion between the prosthesis and the vertebral end plates.The angular motion at the superior bearing was 7.0� ± 1.9�,representing 67% ± 13% of the total prosthesis motion. Con-versely, the motion at the inferior bearing was 3.4� ± 1.6�,representing 33% ± 13% of the total prosthesis motion.
TABLE II Intra-Prosthesis Motion in CHARITE III Prostheses Implanted in Human Cadaveric Specimens
Index Level No.Total ProsthesisMotion* (deg)
Superior BearingMotion* (deg)
Inferior BearingMotion* (deg)
Superior:InferiorMotion Ratio*
L3-L4 6 10.9 ± 3.7 7.3 ± 2.5 3.6 ± 1.7 2.36 ± 0.99†
L4-L5 7 10.3 ± 2.3 6.9 ± 1.4 3.5 ± 2.2 3.21 ± 2.50†
L5-S1 13 10.2 ± 1.9 6.8 ± 2.1 3.4 ± 1.3 2.55 ± 1.81†
All 26 10.4 ± 2.4 7.0 ± 1.9 3.4 ± 1.6 2.68 ± 1.84†
*Values are given as the mean and the standard deviation. †Significantly larger than 1.0 (one-sample t test; one-tailed p < 0.05).
TABLE III Intra-Prosthesis Motion in CHARITE III Prostheses Implanted in Patients in Previous Clinical Studies*
Implantation Index Level No.Total ProsthesisMotion† (deg)
Superior BearingMotion† (deg)
Inferior BearingMotion† (deg)
Superior:InferiorMotion Ratio†
Monosegmental
L4-L5 7 14.2 ± 4.2 9.7 ± 2.8 4.5 ± 2.4 3.28 ± 3.36‡
L5-S1 7 13.2 ± 4.7 7.9 ± 3.1 5.3 ± 1.9 1.51 ± 0.33‡
All 14 13.7 ± 4.3 8.8 ± 3.0 4.9 ± 2.1 2.39 ± 2.47‡
Bisegmental
L4-L5 3 10.7 ± 1.5 7.8 ± 1.8 3.0 ± 1.9 4.37 ± 4.53
L5-S1 3 8.5 ± 5.3 5.0 ± 3.5 3.5 ± 2.1 1.45 ± 0.47
All 6 9.6 ± 3.7 6.4 ± 2.9 3.2 ± 1.8 2.91 ± 3.29‡
All
L4-L5 10 13.2 ± 3.9 9.1 ± 2.6 4.0 ± 2.2 3.61 ± 3.52‡
L5-S1 10 11.8 ± 5.1 7.0 ± 3.3 4.7 ± 2.0 1.49 ± 0.35‡
All 20 12.5 ± 4.5 8.1 ± 3.1 4.4 ± 2.1 2.55 ± 2.66‡
*L4-L5 data are from references 31-38 and 43. L5-S1 data are from references 32-34, 36, 37, 39, 41, and 42.†Values are given as the mean andthe standard deviation. ‡Significantly larger than 1.0 (one-sample t test; one-tailed p < 0.05).
849
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S
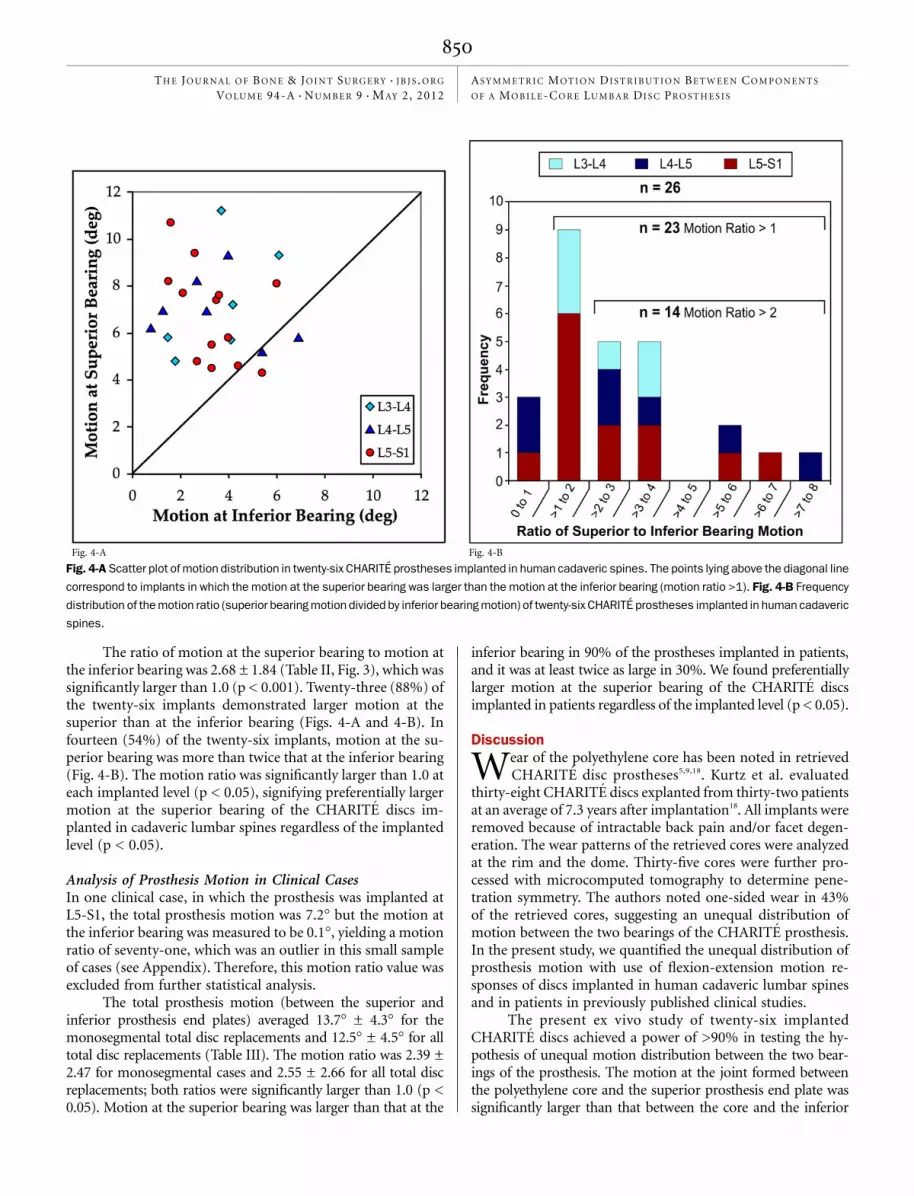
The ratio of motion at the superior bearing to motion atthe inferior bearing was 2.68 ± 1.84 (Table II, Fig. 3), which wassignificantly larger than 1.0 (p < 0.001). Twenty-three (88%) ofthe twenty-six implants demonstrated larger motion at thesuperior than at the inferior bearing (Figs. 4-A and 4-B). Infourteen (54%) of the twenty-six implants, motion at the su-perior bearing was more than twice that at the inferior bearing(Fig. 4-B). The motion ratio was significantly larger than 1.0 ateach implanted level (p < 0.05), signifying preferentially largermotion at the superior bearing of the CHARITE discs im-planted in cadaveric lumbar spines regardless of the implantedlevel (p < 0.05).
Analysis of Prosthesis Motion in Clinical CasesIn one clinical case, in which the prosthesis was implanted atL5-S1, the total prosthesis motion was 7.2� but the motion atthe inferior bearing was measured to be 0.1�, yielding a motionratio of seventy-one, which was an outlier in this small sampleof cases (see Appendix). Therefore, this motion ratio value wasexcluded from further statistical analysis.
The total prosthesis motion (between the superior andinferior prosthesis end plates) averaged 13.7� ± 4.3� for themonosegmental total disc replacements and 12.5� ± 4.5� for alltotal disc replacements (Table III). The motion ratio was 2.39 ±2.47 for monosegmental cases and 2.55 ± 2.66 for all total discreplacements; both ratios were significantly larger than 1.0 (p <0.05). Motion at the superior bearing was larger than that at the
inferior bearing in 90% of the prostheses implanted in patients,and it was at least twice as large in 30%. We found preferentiallylarger motion at the superior bearing of the CHARITE discsimplanted in patients regardless of the implanted level (p < 0.05).
Discussion
Wear of the polyethylene core has been noted in retrievedCHARITE disc prostheses5,9,18. Kurtz et al. evaluated
thirty-eight CHARITE discs explanted from thirty-two patientsat an average of 7.3 years after implantation18. All implants wereremoved because of intractable back pain and/or facet degen-eration. The wear patterns of the retrieved cores were analyzedat the rim and the dome. Thirty-five cores were further pro-cessed with microcomputed tomography to determine pene-tration symmetry. The authors noted one-sided wear in 43%of the retrieved cores, suggesting an unequal distribution ofmotion between the two bearings of the CHARITE prosthesis.In the present study, we quantified the unequal distribution ofprosthesis motion with use of flexion-extension motion re-sponses of discs implanted in human cadaveric lumbar spinesand in patients in previously published clinical studies.
The present ex vivo study of twenty-six implantedCHARITE discs achieved a power of >90% in testing the hy-pothesis of unequal motion distribution between the two bear-ings of the prosthesis. The motion at the joint formed betweenthe polyethylene core and the superior prosthesis end plate wassignificantly larger than that between the core and the inferior
Fig. 4-A Fig. 4-B
Fig. 4-A Scatter plot of motion distribution in twenty-six CHARITE prostheses implanted in human cadaveric spines. The points lying above the diagonal line
correspond to implants in which the motion at the superior bearing was larger than the motion at the inferior bearing (motion ratio >1). Fig. 4-B Frequency
distribution of the motion ratio (superior bearing motion divided by inferior bearing motion) of twenty-six CHARITE prostheses implanted in human cadaveric
spines.
850
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

prosthesis end plate. Eighty-eight percent of the CHARITE discsimplanted in cadaveric specimens exhibited larger motion at thesuperior bearing, with 54% demonstrating more than twice asmuch motion at the superior bearing as at the inferior bearing.
The findings of the ex vivo study must be interpreted inthe context of some limitations. Biomechanical testing at bestmimics the immediate postoperative condition. Therefore, pos-sible postoperative changes in the soft tissues and osseous re-modeling are not incorporated, although anular relaxation maybe accounted for44. A second limitation is the inability to fullyreplicate physiologic loads. Although application of the followerpreload provides a key element of the in vivo loading environ-ment19,25, the complex musculature of the lumbar region rendersmuscle loading nearly impossible to reproduce completely inthe laboratory. More complicated testing setups have beensuggested45, but current recommendations for biomechanicaltesting protocols include the use of pure-moment control withfollower-preload application, reflecting a balance between physi-ologic behavior and experimental limitations19. The experimentalmodel used in the biomechanical study has been well docu-mented21-23,46 and well accepted as a testing standard in the scientificcommunity19,24,45,47,48.
The ultimate validity of a biomechanical model lies inits ability to produce results that are corroborated by clinicalfindings. Therefore, the hypothesis of unequal motion distri-bution was also tested with use of motion data from CHARITEdiscs implanted in patients. The final cohort included fifteensingle-level implantations and six two-level implantations, allutilizing the CHARITE III disc. In one case with a CHARITEdisc implanted at L5-S1, the total prosthesis motion was 7.2�but the motion at the inferior bearing was 0.1�, resulting in amotion ratio of seventy-one, which was an outlier in this smallsample of cases. Excluding this case from statistical analysisdoes not bias our conclusions since the large motion ratio inthis case was consistent with the existence of unequal motiondistribution in the remaining cases.
We recognize that the ‘‘study population’’ used for theradiographic analysis of in vivo prosthesis motion has limitations.First, the sample size for the in vivo study was small. Second, wedid not have firsthand knowledge of the clinical outcomes forindividual patients; this potentially raises a concern that thein vivo motion patterns in some of the patients may have beenassociated with prosthesis-related complications or poor out-comes. In this regard, it should be noted that the implantedprostheses had good postoperative motion and, to the best of ourknowledge, good clinical outcomes and no prosthesis-relatedcomplications according to the available information in thesepublished reports (see Appendix). In light of the limitationsmentioned above, no conclusions were drawn regarding theeffect of the in vivo prosthesis motion patterns on clinical out-comes. The dual methodology of our study has allowed us todemonstrate that the finding of preferentially larger motion at thesuperior bearing of the CHARITE discs implanted in humancadaveric lumbar spines represents a real phenomenon that ispresent in vivo and is not an experimental artifact of the cadavericstudy.
The motion ratio varied over a large range in the ca-daveric specimens and in the patients. In the cadaveric portionof the study, an identical operative technique of disc-spacepreparation and implant positioning, which followed clinicalguidelines, was used in all specimens26,49. Therefore, the vari-ability in the motion ratio may be attributed to variability inspecimen anatomy. Such variability influences the way in whichthe mobile core sits in relation to the prosthesis end plates inthe reconstructed segment, which may in turn influence thefree movement of the core during segmental flexion-extension.In the clinical portion of the study, some variability in thesurgical technique and implant position may be expected sincethe implantations were performed by different surgeons over aperiod of more than fifteen years. However, in spite of thevariability in both portions of the study, we showed that therewas preferentially larger motion at the superior bearing of theCHARITE prosthesis implanted in human cadaveric spines andin patients.
There is no clear consensus in the literature regarding theeffect of implantation level on clinical outcome. Regan foundno statistical difference in the improvements in the visual an-alog scale (VAS) pain score and Oswestry Disability Index(ODI) score of patients with CHARITE prostheses implantedat L4-L5 compared with L5-S1 over twenty-four months50. Theauthors of other studies involving the ProDisc II prosthesis(Synthes Spine, Paoli, Pennsylvania) reported less postopera-tive motion at L5-S1 compared with L4-L551-54, and they sug-gested that this may be attributed to the discrepancy betweenthe center of rotation of the native L5-S1 segment and that of aprosthesis such as the ProDisc that has a fixed center of rota-tion. The present study did not have sufficient statistical powerto assess the effect of implantation level on the motion ratio.However, the motion ratio was significantly larger than 1.0 ateach implanted level (p < 0.05), signifying preferentially largermotion at the superior bearing of the CHARITE disc in humancadaveric lumbar spines and in patients, regardless of the im-planted level.
If all prosthesis motion in the CHARITE disc occurred atthe superior spherical bearing, the center of rotation would belocated at the center of curvature of the superior sphericalbearing, which is caudal to the superior end plate of the inferiorvertebra (Fig. 5-A). If the prosthesis motion was equally dis-tributed between the two spherical bearings (i.e., motionratio = 1.0), the center of rotation would be located at thecenter of the mobile core (Fig. 5-B). Normative reference datasuggest that, within a lumbar level, the center of rotation may befound within a range of up to 8 to 10 mm in the cranial-caudaldirection and that this cranial-caudal location also varies de-pending on the segment level55. Hipp and Wharton measuredthe locations of the center of rotation for flexion-extensionmotion in the lumbar spine of sixty-three asymptomatic in-dividuals with use of the computerized QMA technique55.Using 30 mm as the typical end-plate width, the mean center ofrotation of the L3-L4 and L4-L5 segments would be locatedcaudal to the superior end plate of the inferior vertebra by 2.3 ±1.8 and 3.6 ± 2.1 mm, respectively. This center of rotation
851
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

location is clearly caudal to the midplane of this disc space. Inthe L5-S1 segment, the center of rotation would be cranial tothe S1 superior end plate by 3.3 ± 3.1 mm. Therefore, at L3-L4and L4-L5, unequal distribution of motion between the supe-rior and inferior bearings of the dual-bearing disc prosthesis isneeded to achieve a normal physiologic center of rotation thatis asymmetrically located in relation to the prosthesis midplane(Fig. 5-C). Although the location of the L5-S1 center of rota-tion can coincide with the midplane of the disc, the meanlocation is slightly below the midplane, and the large standarddeviation (3.1 mm) suggests that an asymmetric distribution ofmotion will be needed in a substantial proportion of cases toachieve a normal center of rotation that is below the midplaneof the disc.
It is unclear how closely a prosthesis with a single sphericalbearing can approximate the normal center of rotation locationsat various lumbar levels. Inability to accommodate intra-leveland inter-level variations in the center of rotation may lead toincongruity of the bearing surfaces, as suggested in a previousstudy of L5-S1 segments that had been reconstructed with use ofthe ProDisc-L disc prosthesis56. The impact of such incongruityon the long-term wear or damage to the bearing surfaces remainsunknown.
In contrast, in a dual-bearing prosthesis, the ability of thesuperior and inferior bearings to allow different amounts ofmotion at each interface could, in theory, accommodate vari-ations in the center of rotation between levels and among pa-tients. However, the theoretical existence of this ability of theCHARITE disc is not sufficient to conclude that the motionresponse of the reconstructed spinal segment resembles normalor near-normal motion characteristics. That would first require
determination of the motion ratios needed to support thenormal variation in the center of rotation observed in humanlumbar segments. We found substantial variability in the mo-tion ratios of the CHARITE discs implanted in human ca-daveric specimens and in patients. A motion ratio that is welloutside the normal range would indicate that motion is oc-curring predominantly at only one of the two joints; this sug-gests the presence of a locked-core phenomenon, which mayproduce abnormal motions and stresses at the facet joints of theimplanted segment.
We often observed the core to be locked in extension rel-ative to the inferior end plate, allowing motion predominantly atthe superior bearing for much of the arc of motion from exten-sion to flexion. The core was released only in the final segment ofthe arc of flexion, yielding some motion at the inferior bearing.This is consistent with the findings of O’Leary et al.23, who illus-trated this ‘‘locking phenomenon’’ with use of sequential fluo-roscopic images and load-displacement curves that correspondedto ‘‘stick-slip’’ friction between the polyethylene core and the in-ferior prosthesis end plate. A subsequent study of CHARITE discsimplanted in cadaveric specimens also indicated motion responsethat exhibited a stick-slip phenomenon in the implanted pros-theses27. These phenomena contribute to the degradation of otherquality-of-motion characteristics of the reconstructed segmentsuch as the neutral zone, stiffness, and hysteresis, all of whichshould be considered in assessing the performance of the discprosthesis. Observations from the present study and from thestudy by O’Leary et al. showed impingement, which refers to apinching of the polyethylene core between the two metal endplates of the CHARITE prosthesis, in extension. During im-pingement there is no motion at either bearing of the prosthesis.
Fig. 5
Figs. 5-A, 5-B, and 5-C Illustration showing the effect of intra-prosthesis motion distribution on the location of the center of rotation (COR) in flexion-
extension. Fig. 5-A All of the motion is occurring at the superior bearing. Fig. 5-B Fifty percent of the motion is occurring at the superior bearing and 50%
at the inferior bearing, representing a motion ratio of 1. Fig. 5-C Seventy percent is occurring at the superior bearing and 30% at the inferior bearing,
representing a motion ratio of 2.3.
852
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

The phenomonon of asymmetric motion described in the presentstudy refers to prosthesis motion in the nonimpingement scenario.Although there is ample evidence from retrievals that CHARITEimplants may impinge, it is difficult to say whether there wasimpingement in the clinical cases that we analyzed in the presentstudy since only the flexion and extension radiographs (and notintermediate radiographs) were available.
The findings regarding the distribution of intra-prosthesismotion are relevant to wear testing protocols. The dual-bearingdesign of the CHARITE disc raises an interesting question abouthow to distribute the total end-plate-to-end-plate motion be-tween the two bearings during a wear test so that the results areclinically meaningful and predictive of the long-term wear anddamage of the prosthesis. Previous studies have addressed thisin differing ways. Serhan et al. positioned the CHARITE disc inthe testing machine such that the center of the mobile corewas at the testing machines’s center of rotation, thereby forcingboth end plates to move relative to the polyethylene core14. Arecent finite-element study simulating a wear-test setup of anisolated CHARITE prosthesis indicated that prosthesis articu-lation and wear occurred predominantly at the superior bearingsurface regardless of the imposed center of rotation of the im-plant or the friction coefficient at the inferior bearing57. This isconsistent with the results of the present study, which foundpreferential motion at the superior bearing of the CHARITE discprosthesis implanted in human cadaveric spines and in patients.
A number of factors may influence the in situ motionresponse of the prosthesis implanted in a spine segment. Theseinclude implant position within the disc space, implant height,radii of curvature of the bearing surfaces, disc-space geometry,
facet orientation, and stiffness of the soft-tissue envelope. Theintra-prosthesis motion data in the study describe the responseof a dual-bearing prosthesis when implanted in a human lumbarsegment, thereby taking into account the fact that the discprosthesis is only one component of the three-joint complexand the host anatomy will likely influence the distribution ofprosthesis motion between the two bearings.
AppendixA table summarizing the analyzed clinical cases is avail-able with the online version of this article as a data sup-
plement at jbjs.org. n
Avinash G. Patwardhan, PhDRobert M. Havey, BSParmenion P. Tsitsopoulos, MD, PhDLeonard I. Voronov, MD, PhDDepartment of Orthopaedic Surgery and Rehabilitation,Loyola University Medical Center,2160 South First Avenue, Maywood, IL 60153.Email address for A.G. Patwardhan: [email protected]
Nicholas D. Wharton, MSPatrick Newman, MSMedical Metrics, Inc., 2121 Sage Road, Houston, TX 77056
Gerard Carandang, MSEdward Hines Jr. VA Hospital,5000 South Fifth Avenue, Hines, IL 60141
References
1. McAfee PC. The indications for lumbar and cervical disc replacement. Spine J.2004;4(6 Suppl):177S-181S.2. Blumenthal SL, Ohnmeiss DD, Guyer R, Hochschuler S, McAfee P, Garcia R, Salib R,Yuan H, Lee C, Bertagnoli R, Bryan V, Winter R. Artificial intervertebral discs and beyond:a North American Spine Society Annual Meeting symposium. Spine J. 2002;2:460-3.3. McAfee PC, Geisler FH, Saiedy SS, Moore SV, Regan JJ, Guyer RD, BlumenthalSL, Fedder IL, Tortolani PJ, Cunningham B. Revisability of the CHARITE artificial discreplacement: analysis of 688 patients enrolled in the U.S. IDE study of the CHARITEArtificial Disc. Spine (Phila Pa 1976). 2006;31:1217-26.4. Freeman BJ, Davenport J. Total disc replacement in the lumbar spine: a sys-tematic review of the literature. Eur Spine J. 2006;15 Suppl 3:S439-47.5. Kurtz SM, Peloza J, Siskey R, Villarraga ML. Analysis of a retrieved polyethylenetotal disc replacement component. Spine J. 2005;5:344-50.6. Buttner-Janz K, Hochshuler SS, McAfee PC. The artificial disk. New York:Springer-Verlag; 2003.7. Wright TM. Polyethylene in knee arthroplasty: what is the future? Clin OrthopRelat Res. 2005;440:141-8.8. Cuckler JM. The rationale for metal-on-metal total hip arthroplasty. Clin OrthopRelat Res. 2005;441:132-6.9. Kurtz SM, van Ooij A, Ross R, de Waal Malefijt J, Peloza J, Ciccarelli L, Villarraga ML.Polyethylene wear and rim fracture in total disc arthroplasty. Spine J. 2007;7:12-21.10. Punt IM, Visser VM, van Rhijn LW, Kurtz SM, Antonis J, Schurink GW, van Ooij A.Complications and reoperations of the SB Charite lumbar disc prosthesis: experi-ence in 75 patients. Eur Spine J. 2008;17:36-43.11. Punt IM, Cleutjens JP, de Bruin T, Willems PC, Kurtz SM, van Rhijn LW, SchurinkGW, van Ooij A. Periprosthetic tissue reactions observed at revision of total inter-vertebral disc arthroplasty. Biomaterials. 2009;30:2079-84.12. Bushelow M, Aderman H, Kaddick C. Wear testing of artificial total disc re-placement prostheses: A comparison between two wear simulation methods. Pre-sented at the 5th Global Symposium on Motion Preservation Technology; 2005 May4-7; New York, NY.
13. Nechtow W, Hintner M, Bushelow M, Kaddick C. IVD replacement mechanicalperformance depends strongly on input parameters. Presented at the 52nd AnnualMeeting of the Orthopaedic Research Society; 2006 Mar 19-22; Chicago, IL.14. Serhan HA, Dooris AP, Parsons ML, Ares PJ, Gabriel SM. In vitro wear assess-ment of the Charite Artificial Disc according to ASTM recommendations. Spine (PhilaPa 1976). 2006;31:1900-10.15. Vicars R, Chyuan-Loo F, Goreham-Voss CM, Brown TD, Tipper JL, Fisher J,Ingham E, Hall RM. Experimental motion analysis of a fixed and mobile bearing TDR.Presented at the 56th Annual Meeting of the Orthopaedic Research Society. 2010;New Orleans, LA.16. Implants for surgery -Wear of total intervertebral spinal disc prostheses -Part 1:Loading and displacement parameters for wear testing and corresponding environ-mental conditions for tests (ISO TC 150/SC 5). Geneva: International Organizationfor Standardization; 2005.17. Standard Guide for Functional, Kinematic, and Wear Assessment of Total DiscProstheses (F 2423-05). West Conshohocken, PA: American Society for Testing andMaterials. International. Subcommittee F04.25 of spinal device; 2006.18. Kurtz SM, Patwardhan A, MacDonald D, Ciccarelli L, van Ooij A, Lorenz M, ZindrickM, O’Leary P, Isaza J, Ross R. What is the correlation of in vivo wear and damagepatterns with in vitro TDR motion response? Spine (Phila Pa 1976). 2008;33:481-9.19. Goel VK, Panjabi MM, Patwardhan AG, Dooris AP, Serhan H; American Societyfor Testing and Materials. Test protocols for evaluation of spinal implants. J BoneJoint Surg Am. 2006;88 Suppl. 2:103-9.20. Panjabi MM. Hybrid multidirectional test method to evaluate spinal adjacent-level effects. Clin Biomech (Bristol, Avon). 2007;22:257-65.21. Patwardhan AG, Havey RM, Carandang G, Simonds J, Voronov LI, Ghanayem AJ,Meade KP, Gavin TM, Paxinos O. Effect of compressive follower preload on the flexion-extension response of the human lumbar spine. J Orthop Res. 2003;21:540-6.22. Patwardhan AG, Carandang G, Ghanayem AJ, Havey RM, Cunningham B,Voronov LI, Phillips FM. Compressive preload improves the stability of anteriorlumbar interbody fusion cage constructs. J Bone Joint Surg Am. 2003;85:1749-56.
853
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S

23. O’Leary P, Nicolakis M, Lorenz MA, Voronov LI, Zindrick MR, Ghanayem A, HaveyRM, Carandang G, Sartori M, Gaitanis IN, Fronczak S, Patwardhan AG. Response ofCharite total disc replacement under physiologic loads: prosthesis component mo-tion patterns. Spine J. 2005;5:590-9.24. Demetropoulos CK, Sengupta DK, Knaub MA, Wiater BP, Abjornson C,Truumees E, Herkowitz HN. Biomechanical evaluation of the kinematics of the ca-daver lumbar spine following disc replacement with the ProDisc-L prosthesis. Spine(Phila Pa 1976). 2010;35:26-31.25. Patwardhan AG, Havey RM, Meade KP, Lee B, Dunlap B. A follower load in-creases the load-carrying capacity of the lumbar spine in compression. Spine (PhilaPa 1976). 1999;24:1003-9.26. McAfee PC, Cunningham B, Holsapple G, Adams K, Blumenthal S, Guyer RD,Dmietriev A, Maxwell JH, Regan JJ, Isaza J. A prospective, randomized, multicenterFood and Drug Administration investigational device exemption study of lumbar totaldisc replacement with the CHARITE artificial disc versus lumbar fusion: part II:evaluation of radiographic outcomes and correlation of surgical technique accuracywith clinical outcomes. Spine (Phila Pa 1976). 2005;30:1576-83, E388-90.27. Panjabi M, Malcolmson G, Teng E, Tominaga Y, Henderson G, Serhan H. Hybridtesting of lumbar CHARITE discs versus fusions. Spine (Phila Pa 1976). 2007;32:959-67.28. Reitman CA, Hipp JA, Nguyen L, Esses SI. Changes in segmental intervertebralmotion adjacent to cervical arthrodesis: a prospective study. Spine (Phila Pa 1976).2004;29:E221-6.29. Zhao K, Yang C, Zhao C, An KN. Assessment of non-invasive intervertebralmotion measurements in the lumbar spine. J Biomech. 2005;38:1943-6.30. Bland JM, Altman DG. Statistical methods for assessing agreement betweentwo methods of clinical measurement. Lancet. 1986;1:307-10.31. Blumenthal S, McAfee PC, Guyer RD, Hochschuler SH, Geisler FH, Holt RT,Garcia R Jr, Regan JJ, Ohnmeiss DD. A prospective, randomized, multicenter Foodand Drug Administration investigational device exemptions study of lumbar total discreplacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluationof clinical outcomes. Spine (Phila Pa 1976). 2005;30:1565-75, E387-91.32. Buttner-Janz K, Hahn S, Schikora K, Link HD. [Basic principles of successfulimplantation of the SB Charite model LINK intervertebral disk endoprosthesis]. Or-thopade. 2002;31:441-53. German.33. Cinotti G, David T, Postacchini F. Results of disc prosthesis after a minimumfollow-up period of 2 years. Spine (Phila Pa 1976). 1996;21:995-1000.34. David T. Long-term results of one-level lumbar arthroplasty: minimum 10-yearfollow-up of the CHARITE artificial disc in 106 patients. Spine (Phila Pa 1976).2007;32:661-6.35. Guyer RD, McAfee PC, Hochschuler SH, Blumenthal SL, Fedder IL, OhnmeissDD, Cunningham BW. Prospective randomized study of the Charite artificial disc:data from two investigational centers. Spine J. 2004;4(6 Suppl):252S-259S.36. Lemaire JP, Carrier H, Sariali el-H, Skalli W, Lavaste F. Clinical and radiologicaloutcomes with the Charite artificial disc: a 10-year minimum follow-up. J SpinalDisord Tech. 2005;18:353-9.37. McAfee PC, Fedder IL, Saiedy S, Shucosky EM, Cunningham BW. SB Charitedisc replacement: report of 60 prospective randomized cases in a US center.J Spinal Disord Tech. 2003;16:424-33.38. Tortolani PJ, Cunningham BW, Eng M, McAfee PC, Holsapple GA, Adams KA.Prevalence of heterotopic ossification following total disc replacement. A prospec-tive, randomized study of two hundred and seventy-six patients. J Bone Joint SurgAm. 2007;89:82-8.39. Guyer RD, McAfee PC, Banco RJ, Bitan FD, Cappuccino A, Geisler FH,Hochschuler SH, Holt RT, Jenis LG, Majd ME, Regan JJ, Tromanhauser SG, Wong DC,Blumenthal SL. Prospective, randomized, multicenter Food and Drug Administrationinvestigational device exemption study of lumbar total disc replacement with theCHARITE artificial disc versus lumbar fusion: five-year follow-up. Spine J. 2009;9:374-86.
40. Putzier M, Funk JF, Schneider SV, Gross C, Tohtz SW, Khodadadyan-KlostermannC, Perka C, Kandziora F. Charite total disc replacement—clinical and radiographicalresults after an average follow-up of 17 years. Eur Spine J. 2006;15:183-95.41. Geisler FH, Blumenthal SL, Guyer RD, McAfee PC, Regan JJ, Johnson JP, MullinB. Neurological complications of lumbar artificial disc replacement and comparisonof clinical results with those related to lumbar arthrodesis in the literature: resultsof a multicenter, prospective, randomized investigational device exemption studyof Charite intervertebral disc. Invited submission from the Joint Section Meetingon Disorders of the Spine and Peripheral Nerves, March 2004. J Neurosurg Spine.2004;1:143-54.42. Hochschuler SH, Ohnmeiss DD, Guyer RD, Blumenthal SL. Artificial disc: pre-liminary results of a prospective study in the United States. Eur Spine J. 2002;11Suppl 2:S106-10.43. Sott AH, Harrison DJ. Increasing age does not affect good outcome after lumbardisc replacement. Int Orthop. 2000;24:50-3.44. Havey RM, Voronov LI, Tsitsopoulos PP, Carandang G, Ghanayem AJ, LorenzMA, Zindrick MR, Patwardhan AG. Relaxation response of lumbar segments under-going disc space distraction: implications to the stability of anterior lumbar interbodyimplants. Spine (Phila Pa). 2011 Sep 8; [Epub ahead of print].45. Wilke HJ, Rohlmann A, Neller S, Graichen F, Claes L, Bergmann G. ISSLS prizewinner: a novel approach to determine trunk muscle forces during flexion and ex-tension: a comparison of data from an in vitro experiment and in vivo measurements.Spine (Phila Pa 1976). 2003;28:2585-93.46. Phillips FM, Tzermiadianos MN, Voronov LI, Havey RM, Carandang G, RennerSM, Rosler DM, Ochoa JA, Patwardhan AG. Effect of the Total Facet ArthroplastySystem after complete laminectomy-facetectomy on the biomechanics of implantedand adjacent segments. Spine J. 2009;9:96-102.47. Panjabi M, Henderson G, Abjornson C, Yue J. Multidirectional testing of one- andtwo-level ProDisc-L versus simulated fusions. Spine (Phila Pa 1976). 2007;32:1311-9.48. Sim HB, Murovic JA, Cho BY, Lim TJ, Park J. Biomechanical comparison ofsingle-level posterior versus transforaminal lumbar interbody fusions with bilateralpedicle screw fixation: segmental stability and the effects on adjacent motion seg-ments. J Neurosurg Spine. 2010;12:700-8.49. Geisler FH. Surgical technique of lumbar artificial disc replacement with theCharite artificial disc. Neurosurgery. 2005;56(1 Suppl):46-57.50. Regan JJ. Clinical results of Charite lumbar total disc replacement. Orthop ClinNorth Am. 2005;36:323-40.51. Siepe CJ, Hitzl W, Meschede P, Sharma AK, Khattab MF, Mayer MH. Interde-pendence between disc space height, range of motion and clinical outcome in totallumbar disc replacement. Spine (Phila Pa 1976). 2009;34:904-16.52. Leivseth G, Braaten S, Frobin W, Brinckmann P. Mobility of lumbar segmentsinstrumented with a ProDisc II prosthesis: a two-year follow-up study. Spine (Phila Pa1976). 2006;31:1726-33.53. Shim CS, Lee SH, Shin HD, Kang HS, Choi WC, Jung B, Choi G, Ahn Y, Lee S, LeeHY. CHARITE versus ProDisc: a comparative study of a minimum 3-year follow-up.Spine (Phila Pa 1976). 2007;32:1012-8.54. Kim DH, Ryu KS, Kim MK, Park CK. Factors influencing segmental range ofmotion after lumbar total disc replacement using the ProDisc II prosthesis.J Neurosurg Spine. 2007;7:131-8.55. Hipp JA, Wharton ND. Quantitative motion analysis of motion-preserving andfusion technologies of the spine. In: Yue JJ, Bertagnoli R, McAfee P, An H, editors.Motion preservation surgery of the spine. Philadephia: Saunders Elsevier; 2008.p 85-96.56. Rousseau MA, Bradford DS, Bertagnoli R, Hu SS, Lotz JC. Disc arthroplastydesign influences intervertebral kinematics and facet forces. Spine J. 2006;6:258-66.57. Goreham-Voss CM, Vicars R, Hall RM, Brown TD. Preferential superior surfacemotion in wear simulations of the Charite total disc replacement. Eur Spine J. 2010Jun 26 [Epub ahead of print].
854
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 94-A d NU M B E R 9 d M AY 2, 2012AS Y M M E T R I C MO T I O N DI S T R I B U T I O N BE T W E E N CO M P O N E N T S
O F A MO B I L E -C O R E LU M B A R DI S C PR O S T H E S I S





























