Embed Size (px)
Citation preview
Are personnel in transplant hospitals infavor of cadaveric organ donation?Multivariate attitudinal study in a hospitalwith a solid organ transplant program
Rıos A, Ramırez P, Martınez L, Montoya MJ, Lucas D, Alcaraz J,Rodrıguez MM, Rodrıguez JM, Parrilla P. Are personnel in transplanthospitals in favor of cadaveric organ donation? Multivariate attitudinalstudy in a hospital with a solid organ transplant program.Clin Transplant 2006: 20: 743–754. ª Blackwell Munksgaard, 2006
Abstract: Introduction: A considerable number of professionals who workin a hospital could be against organ donation, which means that when thetime comes, they could act as an obstacle to donation. The objective of thisstudy was to analyze the attitude of hospital professionals toward organdonation and to determine the factors that influence this attitude in aSpanish center with a transplant program.Materials and methods: The study was carried out in a third-level Spanishhospital with a solid organ transplant program. A random sample wastaken (n ¼ 1262) and stratified by job category and type of service. Attitudewas evaluated using a validated questionnaire. Contact was made in eachservice with the person responsible for each of the job categories in order todistribute the survey. The survey was completed anonymously and was self-administered. Student’s t-test, the chi-squared test, and logistic regressionanalysis were applied in the statistical analysis.Results: The survey completion rate was 93% (n ¼ 1168). Most respond-ents were in favor of donation [69% (n ¼ 808)]. Of those who are not infavor, 29% (n ¼ 105) provide fear of apparent death as the reason whilstmost do not give a reason (negative assertion; 57%; n ¼ 206). There aremany factors related to this attitude toward donation, which are evident inthe multivariate analysis: (i) job category, in which physicians are twice aslikely to be in favor of donation than ancillary personnel (OR ¼ 2.02); (ii) arespondent’s knowledge of brain death (OR ¼ 1.64); (iii) having discussedthe matter of organ donation and transplantation within the family(OR ¼ 1.89); (iv) a preference for other options apart from burial(OR ¼ 3.66); (v) being in favor of the performance of autopsy if it werenecessary (OR ¼ 2.76); (vi) not being concerned about mutilation of thecadaver (OR ¼ 2); and (vii) having a partner with a favorable attitudetoward donation (OR ¼ 2.2).Conclusions: Attitude toward cadaveric organ donation among personnelin a transplant hospital is similar to that described in the general public andis determined by many factors. The following factors are most noteworthy:(i) job category; (ii) knowledge of the concept of brain death; (iii) consid-eration of the matter of donation in the family; and (iv) fear of manipula-tion of the cadaver. In view of this attitude, which is similar to that of thegeneral public, it is necessary to carry out promotion activities if we want toincrease cadaveric donation rates.
A. Rıosa,b, P. Ramıreza,b,L. Martınezb, M.J. Montoyac,D. Lucasd, J. Alcaraze,M.M. Rodrıgueza, J.M. Rodrıguezb
and P. Parrillab
aCoordinacion Regional de Trasplantes de la
Comunidad Autonoma de Murcia, Consejerıa de
Sanidad, Murcia, bDepartamento de Cirugıa,
Hospital Universitario Virgen de la Arrixaca, El
Palmar, Servicio Murciano de Salud, Murcia,cServicio de Cirugıa, Hospital Rafael Mendez,
Lorca, Murcia, dCoordinacion Hospitalaria,
Hospital Reina Sofia, Murcia and eServicio de
Hematologıa, Hospital de San Carlos, Murcia,
Espana
Key words: attitude – brain death – hospital
personnel – organ donation
Corresponding author: Dr Antonio Rıos Zambu-
dio, Avenida de la Libertad no 208, Casillas,
30007 Murcia, Espana.
Tel.: 34 968 27 07 57;
e-mail: [email protected]
Accepted for publication 30 June 2006
Clin Transplant 2006: 20: 743–754 DOI: 10.1111/j.1399-0012.2006.00562.xCopyright ª Blackwell Munksgaard 2006
743

The organ deficit is currently the main cause ofdeath in patients who are waiting to receive atransplant organ (1), and it limits the developmentof a therapy that is nowadays the best option for aselect group of patients in which conventionaltreatment does not offer survival or quality of life(2). In Spain, as in all countries, in spite of the highlevels of cadaveric donation, the organ deficitcontinues to be the main limitation of this therapy(3).Currently in Spain, action is being taken on two
fronts in order to alleviate this problem. The first isto encourage living donation, especially of thekidney. The second is to try to achieve completecadaveric donation, which is the reason why �TheNational Strategic Plan for reducing donationrefusal� was established several years ago. It iscoordinated by the National Transplant Organiza-tion, in order to reduce the main factor limitingdonation in Spain, namely family refusal to donate(4).In this strategic plan it has already been estab-
lished that apart from populational factors of apsychosocial nature (5–7), one of the barrierspreventing the procurement of more transplantorgans seems to be located within the hospitalstructure given that a considerable percentage ofthe personnel who work in a hospital seem to beagainst organ donation (8–10), and that at acritical time they could act as an obstacle todonation. After analyzing the current situation interms of attitude toward donation and factorsaffecting such an attitude, it is clear that if we wantto achieve complete cadaveric donation it isnecessary to take action on workers in healthcenters.The objective of this study was to analyze the
attitude of healthcare workers toward the donationof their own organs and to determine the factorsthat influence such an attitude in a health centerwith a solid organ transplant program.
Materials and methods
Study population
The study was carried out in a Spanish third-levelhospital with a cadaveric organ transplant pro-gram (kidney, liver, pancreas, and heart) and aliving donation program (kidney and liver). Arandom sample was taken and stratified accordingto job category (physicians, nurses, healthcareassistants, and ancillary personnel) and service inwhich the worker is based. Workers were selectedrandomly from each job category and service. Atotal of 1262 workers were selected and the study
was carried out between the months of Februaryand December 2003.
Attitudinal survey and study variables
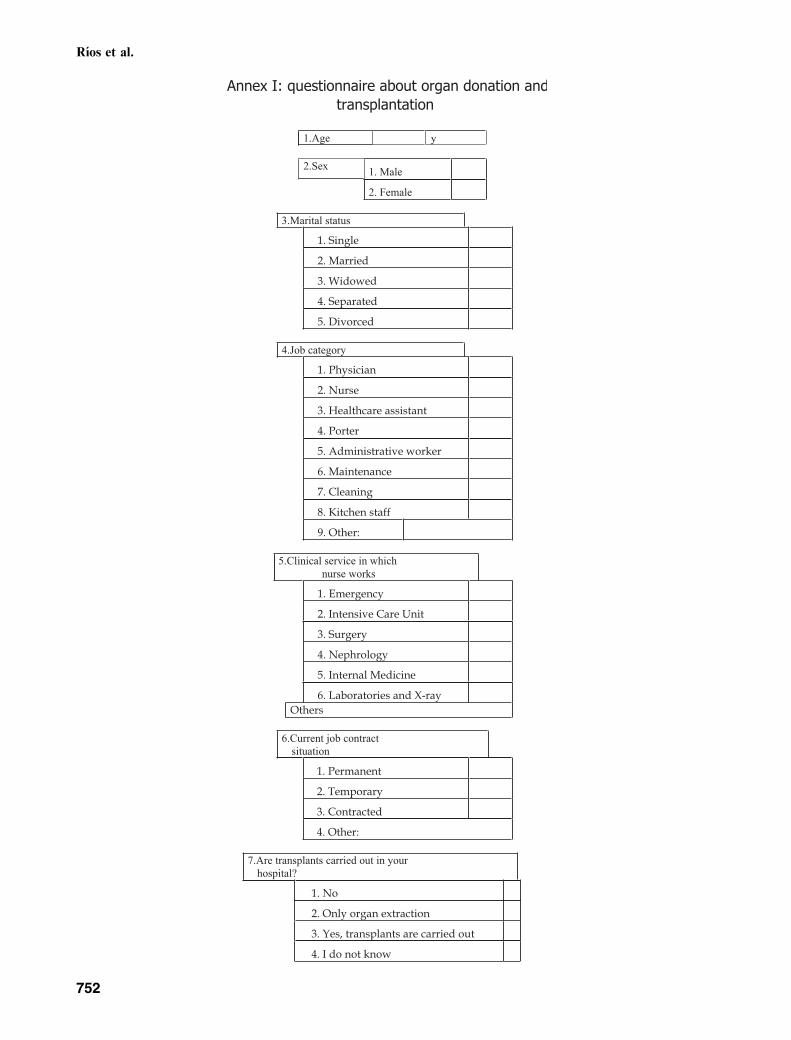
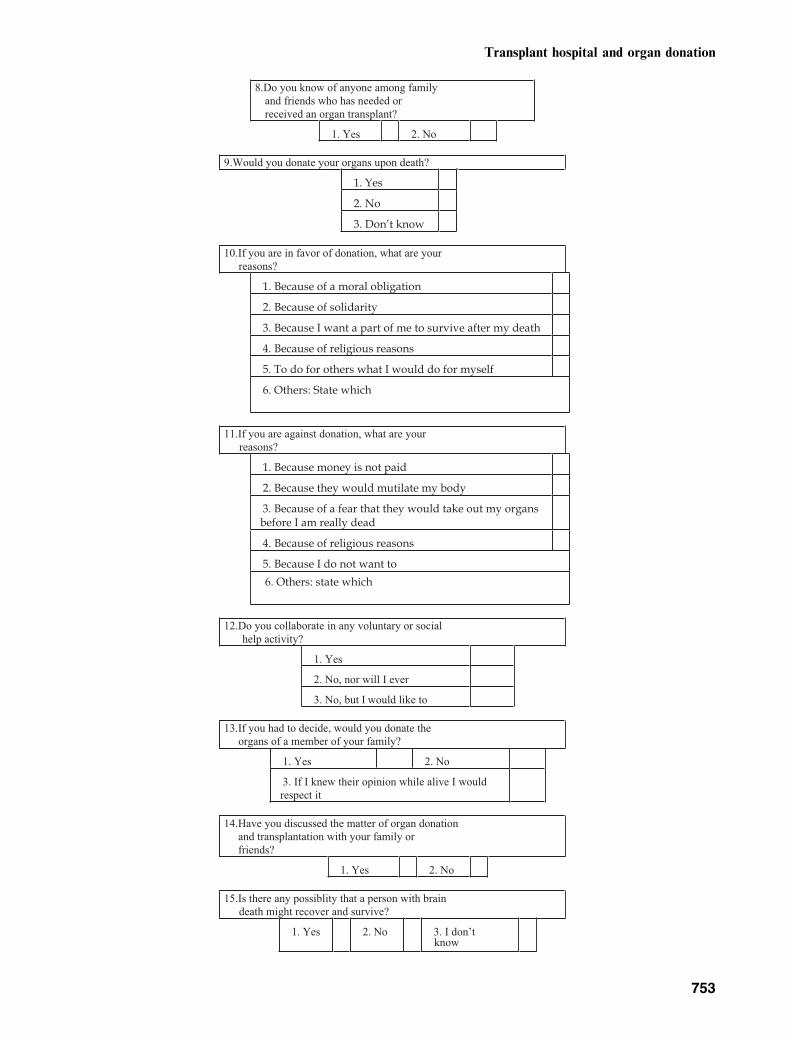
Attitude was evaluated using a survey with 22multiple-choice questions, validated in our geo-graphical area (7, 10–13; Annex I). Contact wasmade in each service with a person responsible foreach of the job categories in order to distribute thesurvey. Accordingly the following were contacted:a physician (generally the head of service) for otherphysicians; the nursing supervisor for nursingpersonnel and healthcare assistants and an admin-istrative officer for ancillary personnel, except inancillary services where contact was made with theperson responsible for the service (head of cleaningfor cleaning personnel, etc.). These representativeswere given an explanation of the project and weremade responsible for the distribution and collec-tion of the questionnaires in randomly selectedwork shifts. The questionnaire was given out at thestart of the working day, given that this offeredsimultaneous access to all the selected workers whocompleted the questionnaire at that moment (threeto five minutes were necessary for its completion).This survey was completed anonymously and wasself-administered and the process was coordinatedby two healthcare collaborators from the RegionalTransplant Coordination Center.
Attitude toward the donation of a respondent’sown organs was used as a dependent variable. Theindependent variables analyzed were: (i) socioper-sonal (age, sex, and marital status); (ii) labor (jobsituation, job category, and type of service inwhich the respondent works); (iii) knowledgeabout organ donation and organ transplantation(previous experience of organ donation and trans-plantation, knowledge of the concept of braindeath, and a respondent’s belief in the possibilityof needing an organ themselves in the future);(iv) social interaction (opinion of a respondent’spartner toward organ donation and transplanta-tion; discussion about organ donation and trans-plantation within the family, and attitude towardthe donation of the organs of a family memberif the decision to donate had to be taken);(v) prosocial voluntary activities (attitude towardvoluntary type prosocial activities); (vi) religion(a respondent’s religion and knowledge of theChurch’s attitude toward organ donation andtransplantation); and (vii) variables of attitudetoward the body (attitude toward cremation of thecadaver; toward burial of the cadaver; towardautopsy; and concern about mutilation of the bodyafter donation).
Rıos et al.
744

Characteristics of the sample
The mean age of the respondents was 39 ± 10 yr,with a slight predominance of females (n ¼ 715;61%), most respondents are married (n ¼ 656;56%). Regarding job category 30% (n ¼ 345) ofrespondents are physicians, 25% (n ¼ 289) arenurses, 13% (n ¼ 157) are healthcare assistants,and 32% (n ¼ 377) are ancillary personnel.
Statistical analysis
The data were stored on a database and analyzedusing the spss 11.0 statistical package. Descriptivestatistics were applied to each of the variables:Student’s t-test and the chi-squared test wereapplied with an analysis of the remainders for thebivariate analysis. Fisher’s exact test was appliedwhen the contingency tables had cells with anexpected frequency of <5. Multiple logistic regres-sion analysis was applied to the variables that werestatistically significant in the bivariate analysis. Inall cases only p-values of <0.05 were considered tobe statistically significant.
Results
Attitude toward cadaveric organ donation
The questionnaire completion rate was 93% (1168respondents out of 1262 selected workers). Atti-tude toward the donation of one’s own solidorgans is favorable in 69% (n ¼ 808) of respond-ents and the main reason given is solidarity (57%;n ¼ 461), and reciprocity, in other words, doingfor others what you would like to be done foryourself (57%; n ¼ 459). The rest of the respond-ents (31%; n ¼ 360) are against donation or areundecided and the most frequent reason offeredwas fear of apparent death (29%; n ¼ 105). Mostdo not give a reason (a negative assertion; 57%;n ¼ 206).
The vast majority of respondents (96%;n ¼ 1121) know that transplants are carried outin their hospital.
Social–personal variables
An analysis of the socio-personal variables that canbe related to attitude toward organ donation showsthat age is related to attitude (p ¼ 0.000). Thus,the respondents who are in favor tend to beyounger than the rest of the respondents (38 vs.41 yr old).
Regarding sex, attitude is significantly morefavorable among males than among females
(74% vs. 67%; p ¼ 0.010; Table 1). With respectto marital status, single respondents tend to have amore positive attitude than those who are married(78% vs. 64%; p ¼ 0.000).
Labor variables
An analysis of job category shows that attitude ismore favorable among physicians than nurses,healthcare assistants, and ancillary personnel (88%vs. 63%, 54% and 63%; p ¼ 0.000). However, norelationship has been found between attitude andwhether a worker is based in a service that isdirectly related to transplantation or not(p ¼ 0.859).Regarding job contract situation, attitude is
more favorable among contracted personnel thanpersonnel who have a permanent position (75% vs.63%; p ¼ 0.000; Table 1).
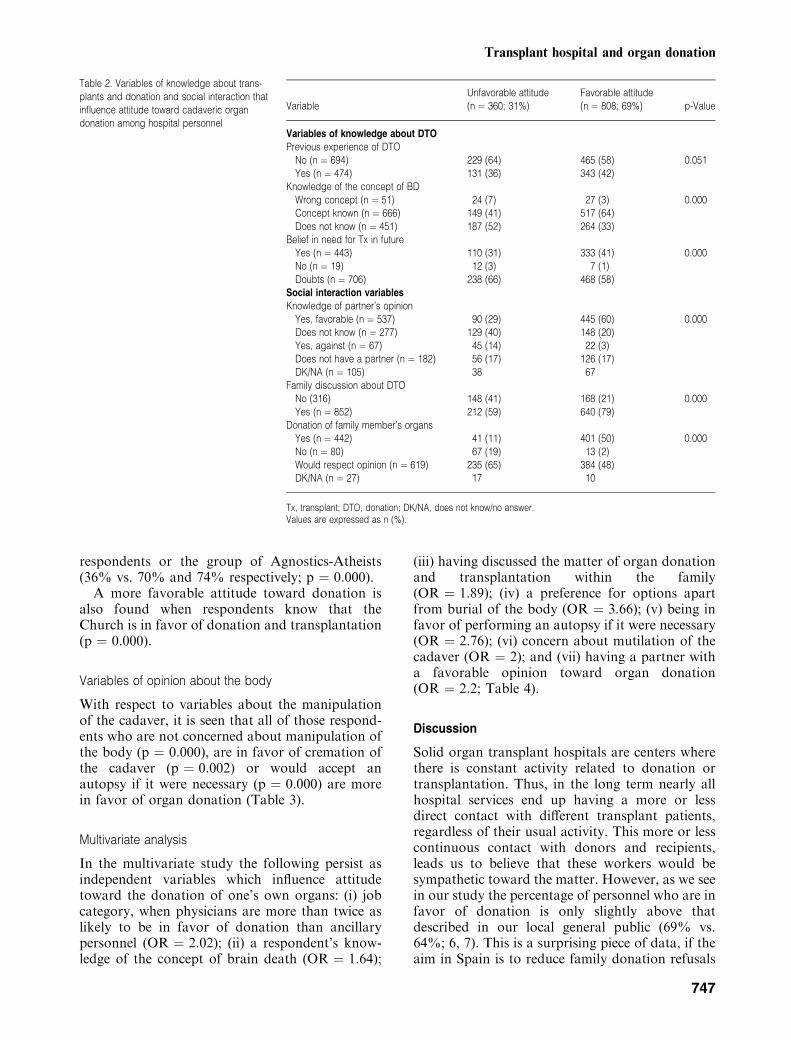
Variables of knowledge about organ donation
Respondents who have had previous personalexperience of organ donation and transplantationhave a more favorable attitude than those whohave not had such experience although this rela-tionship is not statistically significant (p ¼ 0.051).Thus, those who have known a transplant patientor a donor have a more favorable attitude thanthose who have not (72% vs. 67%).It is noteworthy that only 57% (n ¼ 666) of
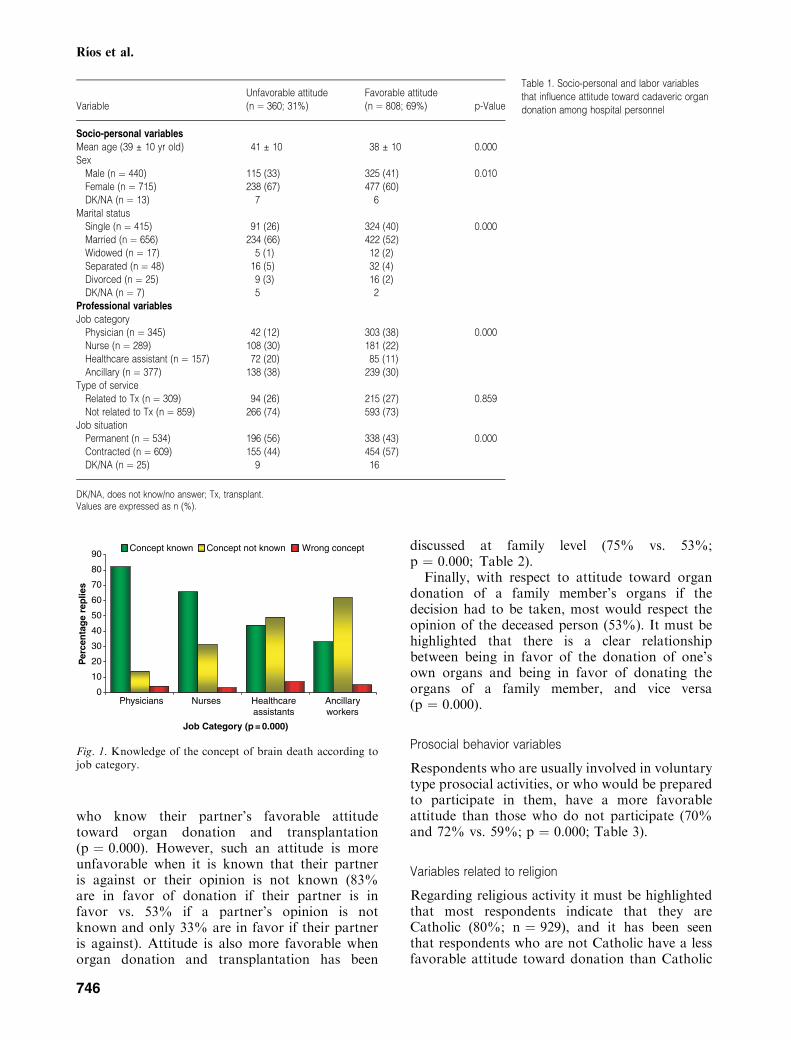
respondents understand the concept of brain deathand such understanding is significantly related toattitude toward donation (p ¼ 0.000). Accord-ingly, 78% of those who understand this conceptare in favor whilst of those who do not considerbrain death to be the death of a person only 53%are in favor and among those who claim not toknow the concept 59% are in favor. In addition, aclose relationship has been found between know-ledge of the concept of brain death and jobcategory as illustrated in Fig. 1. In this way, whilst82% (n ¼ 283) of physicians understand the con-cept, the percentage decreases to 66% amongnurses, 44% among healthcare assistants, and33% among ancillary personnel.On the other hand, those respondents who
believe that they might need a transplant in thefuture are more in favor of donation than thosewho do not believe this or who have doubts aboutthe matter (p ¼ 0.000).
Social interaction variables
Among social interaction variables we find thatthere is a more favorable attitude among those
Transplant hospital and organ donation
745
who know their partner’s favorable attitudetoward organ donation and transplantation(p ¼ 0.000). However, such an attitude is moreunfavorable when it is known that their partneris against or their opinion is not known (83%are in favor of donation if their partner is infavor vs. 53% if a partner’s opinion is notknown and only 33% are in favor if their partneris against). Attitude is also more favorable whenorgan donation and transplantation has been
discussed at family level (75% vs. 53%;p ¼ 0.000; Table 2).
Finally, with respect to attitude toward organdonation of a family member’s organs if thedecision had to be taken, most would respect theopinion of the deceased person (53%). It must behighlighted that there is a clear relationshipbetween being in favor of the donation of one’sown organs and being in favor of donating theorgans of a family member, and vice versa(p ¼ 0.000).
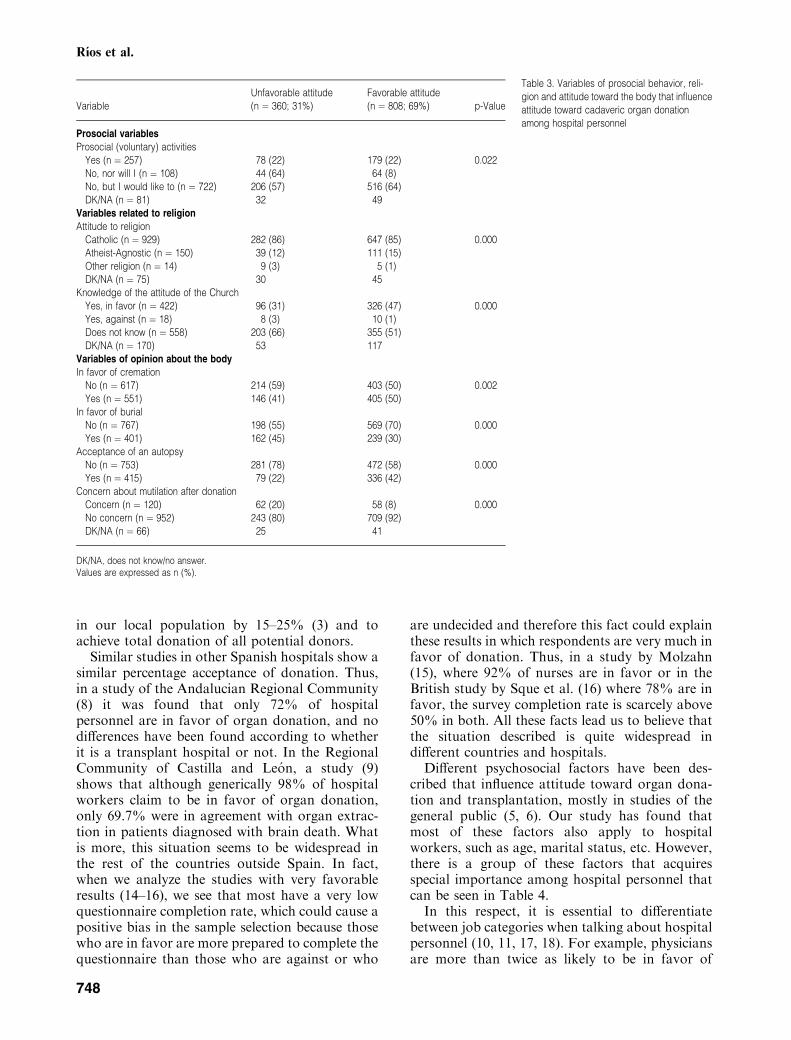
Prosocial behavior variables
Respondents who are usually involved in voluntarytype prosocial activities, or who would be preparedto participate in them, have a more favorableattitude than those who do not participate (70%and 72% vs. 59%; p ¼ 0.000; Table 3).
Variables related to religion
Regarding religious activity it must be highlightedthat most respondents indicate that they areCatholic (80%; n ¼ 929), and it has been seenthat respondents who are not Catholic have a lessfavorable attitude toward donation than Catholic
0
10
20
30
40
50
60
70
80
90
Per
cen
tag
e re
plie
s
Physicians Nurses Healthcareassistants
Ancillaryworkers
Job Category (p = 0.000)
Concept known Concept not known Wrong concept
Fig. 1. Knowledge of the concept of brain death according tojob category.
Table 1. Socio-personal and labor variablesthat influence attitude toward cadaveric organdonation among hospital personnelVariable
Unfavorable attitude(n ¼ 360; 31%)
Favorable attitude(n ¼ 808; 69%) p-Value
Socio-personal variables
Mean age (39 ± 10 yr old) 41 ± 10 38 ± 10 0.000Sex
Male (n ¼ 440) 115 (33) 325 (41) 0.010Female (n ¼ 715) 238 (67) 477 (60)DK/NA (n ¼ 13) 7 6
Marital statusSingle (n ¼ 415) 91 (26) 324 (40) 0.000Married (n ¼ 656) 234 (66) 422 (52)Widowed (n ¼ 17) 5 (1) 12 (2)Separated (n ¼ 48) 16 (5) 32 (4)Divorced (n ¼ 25) 9 (3) 16 (2)DK/NA (n ¼ 7) 5 2
Professional variables
Job categoryPhysician (n ¼ 345) 42 (12) 303 (38) 0.000Nurse (n ¼ 289) 108 (30) 181 (22)Healthcare assistant (n ¼ 157) 72 (20) 85 (11)Ancillary (n ¼ 377) 138 (38) 239 (30)
Type of serviceRelated to Tx (n ¼ 309) 94 (26) 215 (27) 0.859Not related to Tx (n ¼ 859) 266 (74) 593 (73)
Job situationPermanent (n ¼ 534) 196 (56) 338 (43) 0.000Contracted (n ¼ 609) 155 (44) 454 (57)DK/NA (n ¼ 25) 9 16
DK/NA, does not know/no answer; Tx, transplant.Values are expressed as n (%).
Rıos et al.
746
respondents or the group of Agnostics-Atheists(36% vs. 70% and 74% respectively; p ¼ 0.000).
A more favorable attitude toward donation isalso found when respondents know that theChurch is in favor of donation and transplantation(p ¼ 0.000).
Variables of opinion about the body
With respect to variables about the manipulationof the cadaver, it is seen that all of those respond-ents who are not concerned about manipulation ofthe body (p ¼ 0.000), are in favor of cremation ofthe cadaver (p ¼ 0.002) or would accept anautopsy if it were necessary (p ¼ 0.000) are morein favor of organ donation (Table 3).
Multivariate analysis
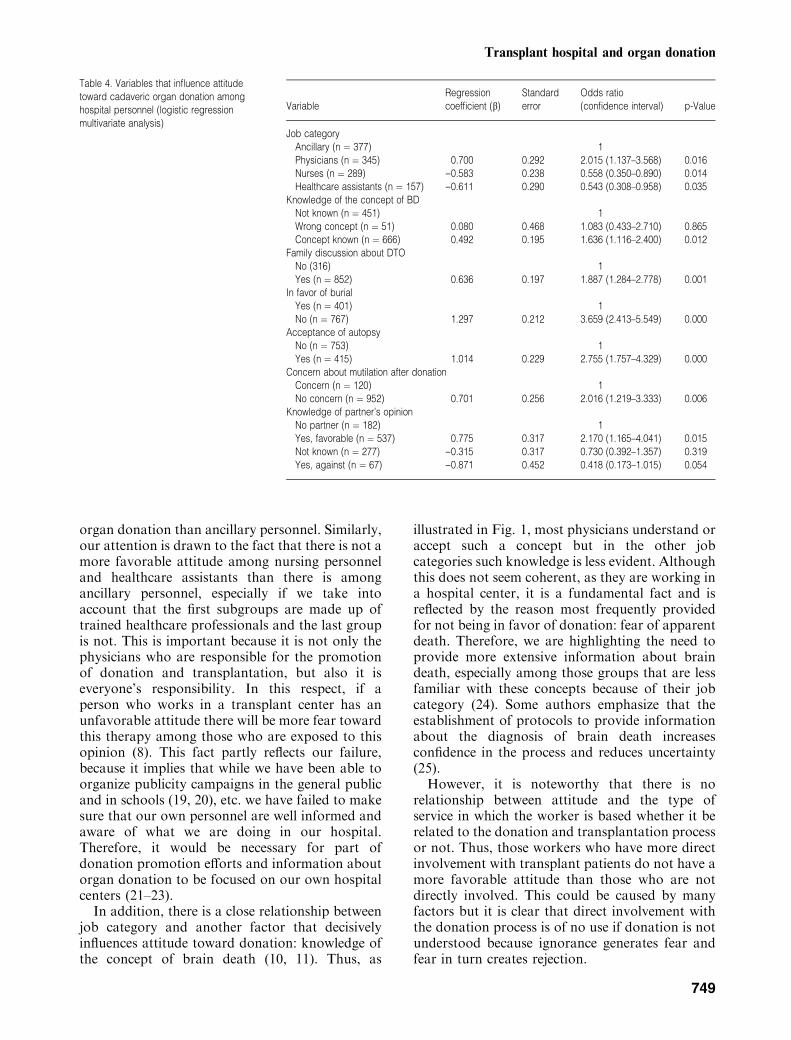
In the multivariate study the following persist asindependent variables which influence attitudetoward the donation of one’s own organs: (i) jobcategory, when physicians are more than twice aslikely to be in favor of donation than ancillarypersonnel (OR ¼ 2.02); (ii) a respondent’s know-ledge of the concept of brain death (OR ¼ 1.64);
(iii) having discussed the matter of organ donationand transplantation within the family(OR ¼ 1.89); (iv) a preference for options apartfrom burial of the body (OR ¼ 3.66); (v) being infavor of performing an autopsy if it were necessary(OR ¼ 2.76); (vi) concern about mutilation of thecadaver (OR ¼ 2); and (vii) having a partner witha favorable opinion toward organ donation(OR ¼ 2.2; Table 4).
Discussion
Solid organ transplant hospitals are centers wherethere is constant activity related to donation ortransplantation. Thus, in the long term nearly allhospital services end up having a more or lessdirect contact with different transplant patients,regardless of their usual activity. This more or lesscontinuous contact with donors and recipients,leads us to believe that these workers would besympathetic toward the matter. However, as we seein our study the percentage of personnel who are infavor of donation is only slightly above thatdescribed in our local general public (69% vs.64%; 6, 7). This is a surprising piece of data, if theaim in Spain is to reduce family donation refusals
Table 2. Variables of knowledge about trans-plants and donation and social interaction thatinfluence attitude toward cadaveric organdonation among hospital personnel
VariableUnfavorable attitude(n ¼ 360; 31%)
Favorable attitude(n ¼ 808; 69%) p-Value
Variables of knowledge about DTO
Previous experience of DTONo (n ¼ 694) 229 (64) 465 (58) 0.051Yes (n ¼ 474) 131 (36) 343 (42)
Knowledge of the concept of BDWrong concept (n ¼ 51) 24 (7) 27 (3) 0.000Concept known (n ¼ 666) 149 (41) 517 (64)Does not know (n ¼ 451) 187 (52) 264 (33)
Belief in need for Tx in futureYes (n ¼ 443) 110 (31) 333 (41) 0.000No (n ¼ 19) 12 (3) 7 (1)Doubts (n ¼ 706) 238 (66) 468 (58)
Social interaction variables
Knowledge of partner’s opinionYes, favorable (n ¼ 537) 90 (29) 445 (60) 0.000Does not know (n ¼ 277) 129 (40) 148 (20)Yes, against (n ¼ 67) 45 (14) 22 (3)Does not have a partner (n ¼ 182) 56 (17) 126 (17)DK/NA (n ¼ 105) 38 67
Family discussion about DTONo (316) 148 (41) 168 (21) 0.000Yes (n ¼ 852) 212 (59) 640 (79)
Donation of family member’s organsYes (n ¼ 442) 41 (11) 401 (50) 0.000No (n ¼ 80) 67 (19) 13 (2)Would respect opinion (n ¼ 619) 235 (65) 384 (48)DK/NA (n ¼ 27) 17 10
Tx, transplant; DTO, donation; DK/NA, does not know/no answer.Values are expressed as n (%).
Transplant hospital and organ donation
747
in our local population by 15–25% (3) and toachieve total donation of all potential donors.Similar studies in other Spanish hospitals show a
similar percentage acceptance of donation. Thus,in a study of the Andalucian Regional Community(8) it was found that only 72% of hospitalpersonnel are in favor of organ donation, and nodifferences have been found according to whetherit is a transplant hospital or not. In the RegionalCommunity of Castilla and Leon, a study (9)shows that although generically 98% of hospitalworkers claim to be in favor of organ donation,only 69.7% were in agreement with organ extrac-tion in patients diagnosed with brain death. Whatis more, this situation seems to be widespread inthe rest of the countries outside Spain. In fact,when we analyze the studies with very favorableresults (14–16), we see that most have a very lowquestionnaire completion rate, which could cause apositive bias in the sample selection because thosewho are in favor are more prepared to complete thequestionnaire than those who are against or who
are undecided and therefore this fact could explainthese results in which respondents are very much infavor of donation. Thus, in a study by Molzahn(15), where 92% of nurses are in favor or in theBritish study by Sque et al. (16) where 78% are infavor, the survey completion rate is scarcely above50% in both. All these facts lead us to believe thatthe situation described is quite widespread indifferent countries and hospitals.
Different psychosocial factors have been des-cribed that influence attitude toward organ dona-tion and transplantation, mostly in studies of thegeneral public (5, 6). Our study has found thatmost of these factors also apply to hospitalworkers, such as age, marital status, etc. However,there is a group of these factors that acquiresspecial importance among hospital personnel thatcan be seen in Table 4.
In this respect, it is essential to differentiatebetween job categories when talking about hospitalpersonnel (10, 11, 17, 18). For example, physiciansare more than twice as likely to be in favor of
Table 3. Variables of prosocial behavior, reli-gion and attitude toward the body that influenceattitude toward cadaveric organ donationamong hospital personnel
VariableUnfavorable attitude(n ¼ 360; 31%)
Favorable attitude(n ¼ 808; 69%) p-Value
Prosocial variables
Prosocial (voluntary) activitiesYes (n ¼ 257) 78 (22) 179 (22) 0.022No, nor will I (n ¼ 108) 44 (64) 64 (8)No, but I would like to (n ¼ 722) 206 (57) 516 (64)DK/NA (n ¼ 81) 32 49
Variables related to religion
Attitude to religionCatholic (n ¼ 929) 282 (86) 647 (85) 0.000Atheist-Agnostic (n ¼ 150) 39 (12) 111 (15)Other religion (n ¼ 14) 9 (3) 5 (1)DK/NA (n ¼ 75) 30 45
Knowledge of the attitude of the ChurchYes, in favor (n ¼ 422) 96 (31) 326 (47) 0.000Yes, against (n ¼ 18) 8 (3) 10 (1)Does not know (n ¼ 558) 203 (66) 355 (51)DK/NA (n ¼ 170) 53 117
Variables of opinion about the body
In favor of cremationNo (n ¼ 617) 214 (59) 403 (50) 0.002Yes (n ¼ 551) 146 (41) 405 (50)
In favor of burialNo (n ¼ 767) 198 (55) 569 (70) 0.000Yes (n ¼ 401) 162 (45) 239 (30)
Acceptance of an autopsyNo (n ¼ 753) 281 (78) 472 (58) 0.000Yes (n ¼ 415) 79 (22) 336 (42)
Concern about mutilation after donationConcern (n ¼ 120) 62 (20) 58 (8) 0.000No concern (n ¼ 952) 243 (80) 709 (92)DK/NA (n ¼ 66) 25 41
DK/NA, does not know/no answer.Values are expressed as n (%).
Rıos et al.
748
organ donation than ancillary personnel. Similarly,our attention is drawn to the fact that there is not amore favorable attitude among nursing personneland healthcare assistants than there is amongancillary personnel, especially if we take intoaccount that the first subgroups are made up oftrained healthcare professionals and the last groupis not. This is important because it is not only thephysicians who are responsible for the promotionof donation and transplantation, but also it iseveryone’s responsibility. In this respect, if aperson who works in a transplant center has anunfavorable attitude there will be more fear towardthis therapy among those who are exposed to thisopinion (8). This fact partly reflects our failure,because it implies that while we have been able toorganize publicity campaigns in the general publicand in schools (19, 20), etc. we have failed to makesure that our own personnel are well informed andaware of what we are doing in our hospital.Therefore, it would be necessary for part ofdonation promotion efforts and information aboutorgan donation to be focused on our own hospitalcenters (21–23).
In addition, there is a close relationship betweenjob category and another factor that decisivelyinfluences attitude toward donation: knowledge ofthe concept of brain death (10, 11). Thus, as
illustrated in Fig. 1, most physicians understand oraccept such a concept but in the other jobcategories such knowledge is less evident. Althoughthis does not seem coherent, as they are working ina hospital center, it is a fundamental fact and isreflected by the reason most frequently providedfor not being in favor of donation: fear of apparentdeath. Therefore, we are highlighting the need toprovide more extensive information about braindeath, especially among those groups that are lessfamiliar with these concepts because of their jobcategory (24). Some authors emphasize that theestablishment of protocols to provide informationabout the diagnosis of brain death increasesconfidence in the process and reduces uncertainty(25).However, it is noteworthy that there is no
relationship between attitude and the type ofservice in which the worker is based whether it berelated to the donation and transplantation processor not. Thus, those workers who have more directinvolvement with transplant patients do not have amore favorable attitude than those who are notdirectly involved. This could be caused by manyfactors but it is clear that direct involvement withthe donation process is of no use if donation is notunderstood because ignorance generates fear andfear in turn creates rejection.
Table 4. Variables that influence attitudetoward cadaveric organ donation amonghospital personnel (logistic regressionmultivariate analysis)
VariableRegressioncoefficient (b)
Standarderror
Odds ratio(confidence interval) p-Value
Job categoryAncillary (n ¼ 377) 1Physicians (n ¼ 345) 0.700 0.292 2.015 (1.137–3.568) 0.016Nurses (n ¼ 289) )0.583 0.238 0.558 (0.350–0.890) 0.014Healthcare assistants (n ¼ 157) )0.611 0.290 0.543 (0.308–0.958) 0.035
Knowledge of the concept of BDNot known (n ¼ 451) 1Wrong concept (n ¼ 51) 0.080 0.468 1.083 (0.433–2.710) 0.865Concept known (n ¼ 666) 0.492 0.195 1.636 (1.116–2.400) 0.012
Family discussion about DTONo (316) 1Yes (n ¼ 852) 0.636 0.197 1.887 (1.284–2.778) 0.001
In favor of burialYes (n ¼ 401) 1No (n ¼ 767) 1.297 0.212 3.659 (2.413–5.549) 0.000
Acceptance of autopsyNo (n ¼ 753) 1Yes (n ¼ 415) 1.014 0.229 2.755 (1.757–4.329) 0.000
Concern about mutilation after donationConcern (n ¼ 120) 1No concern (n ¼ 952) 0.701 0.256 2.016 (1.219–3.333) 0.006
Knowledge of partner’s opinionNo partner (n ¼ 182) 1Yes, favorable (n ¼ 537) 0.775 0.317 2.170 (1.165–4.041) 0.015Not known (n ¼ 277) )0.315 0.317 0.730 (0.392–1.357) 0.319Yes, against (n ¼ 67) )0.871 0.452 0.418 (0.173–1.015) 0.054
Transplant hospital and organ donation
749

In addition to the two factors mentioned earlier,another two are of particular relevance in health-care personnel: the role of the family unit andattitude toward manipulation of the cadaver. Withrespect to the first, we can see that having spokenabout or discussed the matter of organ donationand transplantation within the family is an inde-pendent factor related to attitude toward donation,so that those who have discussed the matter arenearly twice as likely to be in favor than those whohave not (OR ¼ 1.9). In the same way, thepartner’s attitude toward donation is of greatimportance (10, 11). Thus, we find that a favorableattitude is related to a partner’s favorable opinionand vice versa, being against is related to apartner’s negative opinion toward donation. Con-sequently, as in the general public, discussing thematter of donation among family and friends tendsto have a positive effect on attitude towarddonation (8, 26).With respect to a negative attitude toward
manipulation of the cadaver, this is a fundamentalfactor that makes donation difficult (7, 27). In thisrespect we have found that all the variables relatedto manipulation of the cadaver are negativelyrelated to attitude toward organ donation andmany of these persist as independent factors.Healthcare workers are no less sensitive than thegeneral public regarding the feelings that arisebecause of manipulation of the body and it hasbeen found that they have great difficulty inallowing action to be carried out on the cadaver,even with such well-accepted aims such as trans-plantation (8).The difference between Spain and other coun-
tries is that the professionalism of the hospitalTransplant Coordinator who is integrated in thehospital structure has improved the detection ofdonors and the search for a positive response whenorgans are requested (28, 29). This model is whatdifferentiates our country from the rest and due tothis, in spite of less positive than expected attitudestoward donation, we have achieved high levels ofcadaveric organ donation. However, if we want toachieve total donation, which is make use of alldetected donors, then we will have to make theattitude of hospital workers more favorable.To conclude, we could say that a positive
attitude toward donation among hospital person-nel is no more than 70%, and is determined bymany psychosocial factors, most importantly: jobcategory, knowledge of brain death, attitude in thefamily unit, and attitude toward manipulation ofthe cadaver. Therefore, it is essential for there to bepromotion activities in the hospital if we want toincrease cadaveric donation rates, given the
important effect that a negative attitude of thisgroup can have on populational attitude (30).Raising the awareness of hospital workers is afundamental aspect in the organ donation andtransplantation process (24), and they should beaware that when a patient is brain dead, the vitalexpectations of this patient come to an end andconsequently there is a hopeful opportunity forother patients and families who are waiting for atransplantation as the ultimate solution to aserious health problem.
References
1. Cantarovich F. Improvement in organ shortage througheducation. Transplantation 2002: 73: 1844.
2. Ramırez P, Mejıas D, Miras M et al. Valoracion delestado de salud y calidad de vida de pacientes sometidos atrasplante de hıgado. Cir Esp 1999: 66: 203.
3. Organizacion Nacional de Trasplantes. Memoria deactividadesONT2004(1aparte).RevEspTraspl2005:14:45.
4. Martınez JM, Lopez JS, Martın A, Martın MJ,Scandroglio B, Martın JM. Organ donation and familydecision-taking within the Spanish donation system. SocSci Med 2001: 53: 405.
5. Martınez JM, Martın A, Lopez Jorge S. La opinionpublica espanola ante la donacion y el trasplante de org-anos. Med Clin 1995: 105: 401.
6. Conesa C, Rıos A, Ramırez P et al. Psycho-social profilein favour of organ donation. Transplant Proc 2003: 35:1276.
7. Conesa C, Rıos A, Ramırez P, Canteras M, Rodrıguez
MM, Parrilla P. Estudio multivariante de los factorespsicosociales que influyen en la actitud poblacional haciala donacion deorganos. Nefrologia 2005: 25: 684.
8. Frutos MA, Blanca MJ, Rosel J, Ruiz P, Elosegui E.Opiniones de profesionales sanitarios de Malaga sobredonacion y trasplante de organos: actitudes en hospitalescon y sin actividad trasplantadora. Rev Esp Traspl 1992: 1:221.
9. Trasplantes del Hospital General de Segovia. Opiniones yactitudes del personal del Hospital General de Segoviaacerca de la extraccion de organos para trasplante. Nefr-ologia 1991: 11(Suppl. 1): 57.
10. Rıos A, Conesa C, Ramırez P et al. Attitude towarddeceased organ donation and transplantation among theworkers in the surgical services in a hospital with atransplant program. Transplant Proc 2005: 37: 3603.
11. Rıos A, Conesa C, Ramırez P et al. Ancillary hospitalpersonnel faced with organ donation and transplantation.Transplant Proc 2006: 38: 858.
12. Conesa C, Rıos A, Ramırez P, Canteras M, Rodrıguez
MM, Parrilla P. Socio-Personal profile of teenagersopposed to organ donation. Nephrol Dial Transplant2004: 19: 1269.
13. Conesa C, Rıos A, Ramırez P et al. Rural primary carecentres as a source of information about organ donation.Transplant Proc 2005: 37: 3609.
14. Ozdag N. The nurses knowledge, awareness and accept-ance of tissue-organ donation. EDTNA ERCA J 2001: 27:201.
15. Molzahn AE. Knowledge and attitudes of critical carenurses regarding organ donation. Can J Cardiovasc Nurs1997: 8: 13.
Rıos et al.
750
16. Sque M, Payne S, Vlachonikolis I. Cadaveric dono-transplantation: nurses� attitudes, knowledge and beha-viour. Soc Sci Med 2000: 50: 541.
17. Johnson CM, Miller SL, Kurek SJ, Lagares-Garcia
JA, Broznick BA, Nathan H. Organ donation: a state-wide survey of trauma surgeons. J Trauma 2001: 51: 110.
18. Bogh L, Madsen M. Attitudes, knowledge, and profi-ciency in relation to organ donation: a questionnaire-basedanalysis in donor hospitals in northern Denmark. Trans-plant Proc 2005: 37: 3256.
19. Rıos A, Conesa C, Munuera C, Pascual FJ, Fajardo
D. Campana informativa sobre la donacion y trasplante deorganos en escolares. Aten Primaria 1998: 21: 623.
20. Conesa C, Rıos A, Ramırez P, Rodrıguez MM, Cant-
eras M, Parrilla P. Importancia de los profesionales deAtencion Primaria en la educacion sanitaria de la donaciondeorganos. Aten Primaria 2004: 34: 528.
21. Chernenko SM, Jensen L, Newburn-Cook C, Bigam
DL. Organ donation and transplantation: a survey ofcritical care health professionals in nontransplant hospi-tals. Prog Transplant 2005: 15: 69.
22. Tebourski F, Jaouadi N, Ben Alaya D, Benamar-
Elgaaied A, Ayed M. Attitude of health personnel toorgan donation and transplantation [article in French].Tunis Med 2003: 81: 482.
23. Gross T, Marguccio I, Martinoli S. Attitudes of hos-pital staff involved in organ donation to the procedure.Transpl Int 2000: 13: 351.
24. Frutos MA. Concienciacion para la donacion. Nefrologia1999: 19: 288.
25. Dodd-McCue D, Tartaglia A, Myer K, Kuthy S,Faulkner K. Unintended consequences: the impact ofprotocol change on critical care nurses� perceptions ofstress. Prog Transplant 2004: 14: 61.
26. Caballer Miedes A, Martınez Sancho M. Variablesinfluyentes en la actitud hacia la donacion de organos.Psicothema 2000: 12(Suppl. 2): 100.
27. Sanner M. A comparison of public attitudes towardautopsy, organ donation, and anatomic dissection. ASwedish survey. JAMA 1994: 271: 284.
28. Wight C, Cohen B, Miranda B, Fernandez M, Beas-
ley C. Hospital attitudes: preliminary findings from donoraction pilot projects. Transpl Int 1998: 11(Suppl. 1): S397.
29. Miranda B, Fernandez M, de Felipe C, Naya M,Gonzalez JM, Matesanz R. Organ donation in Spain.Nephrol Dial Transplant 1999: 14(Suppl. 3): 15.
30. Williams MA, Lipsett PA, Rushton CH et al. Thephysician’s role in discussing organ donation with families.Crit Care Med 2003: 31: 1568.
Transplant hospital and organ donation
751
Rıos et al.
752
Transplant hospital and organ donation
753
Rıos et al.
754





























