Embed Size (px)
Citation preview

For Peer Review
Medication adherence in Palestinian Arabs with
schizophrenia
Journal: Journal of Clinical Pharmacy and Therapeutics
Manuscript ID: JCPT-2011-1338
Manuscript Type: Original Article
Date Submitted by the
Author: 14-Apr-2011
Complete List of Authors: Sweileh, Waleed Ihbesheh, MAnal Jarar, Ikhlas sawalha, ansam; an-najah national university, pharamcy Abu-Taha, Adham zyoud, Sa'ed Morisky, Donald
Keywords: Schizophrenia, Ethnic Differences, Clinical Pharmacy
Journal of Clinical Pharmacy and Therapeutics

For Peer Review
1
Medication adherence in Palestinian Arabs with schizophrenia
Authors
1. Waleed M. Sweileh, Associate Professor of Clinical Pharmacology, Department of
Pharmacology and Toxicology, School of Pharmacy, An-Najah National University,
Nablus, Palestine.
2. Manal S. Ihbesheh, MS. Biochemistry, School of Pharmacy, Department of
Biochemistry, An-Najah National University, Nablus, Palestine.
3. Ikhlas S. Jarar, MS. Pharmacology, Department of Pharmacology and Toxicology,
School of Pharmacy, An-Najah National University, Nablus, Palestine.
4. Ansam F. Sawalha, Associate Professor of Clinical Toxicology, Department of
Pharmacology and Toxicology, School of Pharmacy, An-Najah National University,
Nablus, Palestine.
5. Adham S. Abu Taha, Assistant Professor of Clinical Pharmacology, Department of
Pharmacology and Toxicology, School of Pharmacy, An-Najah National University,
Nablus, Palestine.
6. Sa’ed H. Zyoud, MS Clinical Pharmacy, WHO Collaborating Centre for Drug
Information, National Poison Centre, Universiti Sains Malaysia (USM), 11800 Penang,
Malaysia.
7. Donald E. Morisky, Sc.D., M.S.P.H., Sc.M. Professor and Program Director, Doctoral
Training in the Social and Behavioral Determinants of Infectious and Chronic Disease
Prevention Department of Community Health Sciences UCLA School of Public Health,
650 Charles E. Young Drive South, Los Angeles, CA 90095-1772, USA
Corresponding author
Waleed M. Sweileh,
Associate Professor, Clinical Pharmacology,
Department of Pharmacology and Toxicology,
School of Pharmacy,
An-Najah National University,
P.O. Box: 7,
Nablus, Palestine
Short running title: Medication adherence and treatment satisfaction
Page 1 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
2
Medication adherence in Palestinian Arabs with schizophrenia
Abstract
Background and Objective: Arab world have complex societal and unique cultural beliefs about
mental illness. No studies have been carried out to assess medication adherence, treatment
satisfaction and clinical symptoms among schizophrenic patients in the Arab world. Therefore, the
objectives of this study were to assess medication adherence and to investigate relationships of
medication adherence with treatment satisfaction and clinical symptoms in a sample of Palestinian
Arab patients with schizophrenia.
Methodology: Medication adherence was measured using the 8-item Morisky Medication
Adherence Scale (MMAS) while treatment satisfaction was measured using the Treatment
Satisfaction Questionnaire for Medication (TSQM 1.4). Psychiatric symptoms were measured
using the expanded Brief Psychiatric Rating Scale (BPRS-E). Data were entered and analyzed
using SPSS 16 for windows.
Results: A convenience sample of 131 schizophrenic patients was studied. Based on MMAS, 44
patients (33.6%) had a low rate, 58 (44.3%) had a medium rate & 29 (22.1%) had a high rate of
adherence. The means of satisfaction with regard to effectiveness, side effects, convenience and
global satisfaction were 72.6 ± 20.5, 67.9 ± 31.47, 63.2 ± 14.3 & 63.1 ± 18.8 respectively. There
was a significant difference in the means of effectiveness (P<0.01), convenience (P<0.01), global
satisfaction (P<0.01), but not side effects domains (P=0.1) among patients with different levels of
adherence. Furthermore, there was a significant difference in the mean of positive symptom score
(P<0.01) but negative symptom score (P=0.4) among patients with different levels of adherence.
Conclusions: Medication non-adherence was common among Palestinian Arab patients and was
associated with low treatment satisfaction scores and poor positive symptom scores.
Key words: Schizophrenia, medication adherence, treatment satisfaction
Page 2 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
3
Introduction
Schizophrenia is a chronic psychiatric disorder that impairs the quality of
patients’ life (Palmer et al., 2002; Pinikahana et al., 2002; Sharma and Antonova
2003). Antipsychotic drug therapy has been reported to successfully minimize the
frequency of acute schizophrenic episodes and hospitalization and that adherence is
a necessary element to achieve such success (Awad and Voruganti 2004; Campbell
et al., 1999). Furthermore, adherence has been reported to lead to considerable cost
savings for the health system (Damen et al., 2008). However, non-adherence to
antipsychotic medications is common and is considered as an integral barrier to the
successful treatment of schizophrenia (Byrne et al., 2008; Dolder et al., 2002; Kim
et al., 2006).
Several factors can contribute to medication non adherence in patients with
schizophrenia (Misdrahi et al., 2002; Svestka and Bitter 2007; Lowry 1998). Such
factors include race, culture and religion. For example, a review article about
psychotropic medications found that rates of non-adherence were higher among
Latinos than Euro-Americans and clinical and research interventions to improve
adherence should be culturally appropriate and incorporate identified factors
(Lanouette et al., 2009). Another study examined how religious beliefs and practices
can affect medication and illness representations in chronic schizophrenia. The
authors concluded that religion and spirituality contribute to shaping representations
of disease and attitudes toward medical treatment in patients with schizophrenia and
that this dimension should be on the agenda of psychiatrists working with patients
with schizophrenia (Borras et al., 2007). In the Arab world, families of patients with
schizophrenia suffer from stigmatization (Kadri et al., 2004). Actually, the common
belief in the Arab society is that mental illnesses have a devilish and sinful
component. Unfortunately, Pubmed search showed no studies about medication
adherence and treatment satisfaction among schizophrenic Arab patients. Therefore,
the objectives of this study were to assess medication adherence and to investigate
Page 3 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
4
relationships of medication adherence with treatment satisfaction and clinical
symptoms in a sample of Palestinian Arab patients with schizophrenia.
Methodology
Study Design and Patient selection:
This cross sectional study was conducted between July 2010 and September
2010 at Al-Makhfya psychiatric Health Center in Nablus, Palestine. Approval to
perform the study was obtained from the Palestinian ministry of health and
Institutional Review Board at An-Najah National University. Patients who met the
following criteria were invited to participate in this study: 1) their age was between
20 and 65 years, 2) they were diagnosed with schizophrenia as defined by DSM-IV
and confirmed in their medical files and 3) they had not been suffering from an
acute attack of illness during the past year. A convenience sample of 150 patients
met the inclusion criteria during the study period.
Assessment and measures
The instrument used in this study consisted of four parts: part one collected
socio-demographic and medication data obtained directly from the patient and his
medical files; part two was medication adherence test, part three was the treatment
satisfaction test and the final part was the psychiatric assessment.
Medication adherence was tested using Arabic version of the validated eight-
item Morisky Medication Adherence Scale (MMAS) (Morisky et al., 2008; Morisky
et al., 1986). English version of the MMAS was translated into Arabic and was
approved by professor Morisky through e-mail communication. The translation
process was carried out according to the following procedure: 1) A forward
translation of the original questionnaire was carried out from English to Arabic
language by two qualified independent, native linguistic expert translators (2) A
back translation from Arabic language to English was carried out by two different
Page 4 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
5
translators. (3) The back translated questionnaire was tested and approved by the
developer through e-mail. The Arabic version of MMAS is an 8-item questionnaire
with 7 yes/no questions while the last question was a 5-point Likert scale. Based on
the scoring system of MMAS, adherence was rated as follows: high adherence (=
8), medium adherence (6 - <8) and low adherence (< 6).
Treatment satisfaction was tested using the Arabic version of Treatment
Satisfaction Questionnaire for Medication (TSQM 1.4) which the researchers
obtained from Quintiles Strategic Research Services. The TSQM 1.4 is a 14-item
psychometrically robust and validated instrument consisting of four scales (Bharmal
et al., 2009). The four scales of the TSQM 1.4 include the effectiveness scale
(questions 1 to 3), the side effects scale (questions 4 to 8), the convenience scale
(questions 9 to 11) and the global satisfaction scale (questions 12 to 14). The TSQM
1.4 domain scores were calculated as recommended by the instrument’s authors,
which is described in detail elsewhere (Atkinson et al., 2005; Atkinson et al., 2004).
The TSQM 1.4 domain scores range from 0 to 100 with higher scores representing
higher satisfaction on that domain.
Psychiatric symptoms, positive and negative schizophrenic symptoms were
evaluated by a psychiatrist and well trained psychologists using the expanded Brief
Psychiatric Rating Scale (BPRS-E) (Lukoff et al., 1986; Overall and Gorham 1962;
Overall and Gorham 1988; Ventura et al., 1993) at the same visit. The BPRS–E
consists of 24 items measuring psychiatric symptoms. Each item in BPRS-E is rated
from 0 – 7 based on the severity of the symptom where the highest score indicate
the highest severity. BPRS-E measures four different dimensions: manic
excitement/ disorganization, positive symptoms, negative symptoms, and
depression/ anxiety (Ruggeri et al., 2005). Positive symptom score (PSS) was based
on the sum of scores of the followings: grandiosity, suspiciousness, hallucinations,
unusual thought content and conceptual disorganization. Negative symptom score
(NSS) was based on the sum of scores of the following symptoms: disorientation,
Page 5 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
6
blunted affect, emotional withdrawal, motor retardation, and mannerism and
posturing.
Data analysis
Continuous variables like the Morisky score, satisfaction domain scores,
BPRS, PSS and NSS were expressed as mean ± SD. Correlation between
continuous variables was carried out using Pearson correlation test. Difference in
means among groups was carried out using one-way ANOVA test with the Tukey
post-hoc test. All statistical analyses were conducted using Statistical Package for
Social Sciences (SPSS; version 16.0) for Windows. The conventional 5 percent
significance level was used throughout the study.
Results
1. Demographic and clinical characteristics
One hundred and fifty patients out of 267 registered schizophrenic patients met
the inclusion criteria. One hundred and thirty one (131) patients agreed to
participate giving a response rate of 87.3%. Of the 131 patients, 40 (30.5%) were
female and 91 (69.5%) were male. The mean age of the patients was 42.9 ± 10.3
years (range = 20 – 65 years). The mean duration of illness was 16.23 ± 9.59 years.
Eighteen patients (13.7%) had other non-psychiatric diseases mainly diabetes
mellitus (10 patients; 7.6%). Smoker schizophrenic patients represented 55% (72
patients) of the sample. None of the patients were reported to have any type of drug
abuse. Details regarding demographic and clinical characteristics of the studied
patients are shown in Table 1.
2. Assessment of adherence, treatment satisfaction and psychiatric symptoms
Based on MMAS, 44 (33.6%) of patients had a low adherence, 58 (44.3%) had a
medium adherence & 29 (22.1%) had a high medication adherence. The average
Page 6 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
7
adherence score (6.1 ± 1.7) for the patients generally indicates medium rate of
adherence. There was a significant positive correlation between age and adherence
(P = 0.028; r = 0.19). However, no such correlation was observed with the duration
of illness (P = 0.13). Furthermore, no significant difference in the means of
adherence was found between male and female (P = 0.76). Patients having other
chronic diseases have significantly higher adherence score compared to those who
do not, but the significance was at the borderline (P = 0.049).
The average scores of satisfaction with regard to effectiveness, side effects,
convenience & global satisfaction were 72.6 ±20.5; 67.9 ± 31.5; 63.2 ± 14.3; & 63.1
± 18.8 respectively. The mean BPRS score of the patients was 68.4 ± 24.5 with 14.4
± 6.7 & 13.7 ± 6.1 means for PSS and NSS respectively. Analysis of satisfaction and
psychiatric scores based on adherence levels (low, medium and high) is shown in
table 2. There was a significant difference in means of effectiveness (P <0.01, F =
8), convenience (P < 0.01; F = 12.5) and global satisfaction domain (P< 0.01, F = 9)
but not in side effects domain (P = 0.1; F = 2) among the three levels of adherence.
Patients in the high adherence category had the highest satisfaction score compared
to those in low and medium adherence categories. Results of post hoc analysis are
also shown in Table 2.
Significant difference was found in the means of BPRS (P < 0.01; F = 4.9),
PSS (P < 0.01, F = 5.7) but not in NSS (P = 0.3; F = 1) among the three levels of
adherence. Patients in the high adherence category had the greatest improvement in
psychiatric symptoms and positive symptoms but not in negative symptoms. Post
hoc analysis of psychiatric symptoms versus adherence levels is shown in table 2.
Discussion
This study is the first of its type in Palestine and Arab world to assess medication
adherence among patients with schizophrenia and the first study that used an Arabic
version for MMAS. Results of our study showed that the majority of schizophrenic
Page 7 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
8
Palestinian Arab patients were non-adherent and that younger patients had
significantly lower adherence scores than elderly ones. Our findings regarding
impact of age on medication adherence is in agreement with finding reported by
other researchers (Hui et al., 2006; Sajatovic et al., 2007). However, other
researchers reported equal non adherence among middle aged and elderly patients
(Jeste et al., 1999a). Several studies have shown that up to 80% of all schizophrenic
patients discontinue antipsychotic medications and that non-adherence rates ranging
from 20% to 89%, with an average rate of approximately 50%, have been reported
(Fenton et al., 1997; Lacro et al., 2002; Young et al., 1986). In a study of
schizophrenia psychopathology carried out in Kuwait, the authors concluded that
the persistence of psychotic symptoms despite freely available antipsychotic
treatment call for attention to the need for continued interaction with family
members in order to address the impact of symptoms (Zahid and Ohaeri, 2010).
There is a wide range of reported rates of adherence among schizophrenic patients.
Differences in methodology used to assess adherence as well as social and cultural
differences among different countries might be responsible for different results
obtained regarding rate of adherence (Breen et al., 2007). A study carried out in
Malaysia among people with different religious background has concluded that lay
beliefs about schizophrenia may serve different functions for different ethno-
cultural groups, which have an influence on help-seeking behaviour (Swami et al.,
2008). Similar results were obtained by Sheikh and Furnham (Sheikh and Furnham,
2000). Psychiatrists and health professionals tend to underestimate the importance
of this issue possibly due to the low rates of religious affiliation of psychiatrists, or a
lack of knowledge of religions (Shafranske 1996; Neeleman and King 1993; Lukoff
et al; 1995).
Although patient’s satisfaction with treatment regimen is crucial for
medication adherence (Atkinson et al., 2004; Taira et al., 2006), few studies had
examined the relationship between adherence, treatment satisfaction and therapeutic
outcome in patients with schizophrenia (Freudenreich et al., 2004; Fujikawa et al.,
Page 8 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
9
2008; Watanabe et al., 2004). Our findings endorse previous reports that treatment
satisfaction is positively associated with antipsychotic medication adherence and
improved clinical outcomes (Gharabawi et al., 2006; Hofer et al., 2004; Masand and
Narasimhan 2006). Other researchers also had similar conclusions. A study by
Maneesakorn and colleagues indicated that antipsychotic medication adherence has
positive impact on psychiatric symptoms and satisfaction with medication
(Maneesakorn et al., 2007; Mohamed et al., 2009). On the other hand, medication
non-adherence had negative impact on treatment response, highlighting the
importance of adherence to achieve satisfactory treatment outcome (Lindenmayer et
al., 2009). A study by Liu-Seifert et al 2005 has found that discontinuing of
treatment may lead to exacerbation of psychiatric symptoms and undermining
therapeutic progress (Liu-Seifert et al., 2005). In these studies, poor response to
treatment and worsening of underlying psychiatric symptoms, and to a lesser extent,
intolerability to medication were the primary contributors to treatment being
discontinued.
The conclusions of our study can be summarized as follows: First, the
majority of the patients had low to medium rate of adherence. Second, treatment
satisfaction and psychiatric symptoms are better in patients with higher adherence
rate. Our study has few limitations. First, sample size used in the study might be
relatively small to draw conclusions for assessing adherence, satisfaction and
psychiatric symptoms. Furthermore, the convenience sampling might create a bias
problem in assessing adherence and satisfaction. Second, instruments that we used
to assess adherence, satisfaction and BPRS might not be the gold standard for this
purpose. A third potential limitation of our study is that the patients who participated
in the study were homogenous in that all of them had governmental insurance and
tends to use similar medications and treated by the same psychiatric team. Non-
adherence among schizophrenic patients might be inherent in the context of the
disease itself. Despite these limitations, results of this study were useful in
Page 9 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
10
understanding adherence, satisfaction and psychiatric symptoms among Arab
culture in which publication in this field is scarce.
Acknowledgement: The authors would like to acknowledge and thank the
Palestinian ministry of health and the team at the Al-Makhfya psychiatric center/
Nablus/ Palestine.
Funding: None
Conflict of Interest: None
Page 10 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
11
References
Atkinson MJ, Kumar R, Cappelleri JC, Hass SL. 2005. Hierarchical construct validity of the
treatment satisfaction questionnaire for medication (TSQM version II) among outpatient
pharmacy consumers. Value Health 8 Suppl 1: S9-S24.
Atkinson MJ, Sinha A, Hass SL, et al. 2004. Validation of a general measure of treatment
satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a
national panel study of chronic disease. Health Qual Life Outcomes 2: 12.
Awad AG, Voruganti LN. 2004. Impact of atypical antipsychotics on quality of life in patients
with schizophrenia. CNS Drugs 18: 877-893.
Bharmal M, Payne K, Atkinson MJ, Desrosiers MP, Morisky DE, Gemmen E. 2009. Validation of
an abbreviated Treatment Satisfaction Questionnaire for Medication (TSQM-9) among
patients on antihypertensive medications. Health Qual Life Outcomes 7: 36.
Borras L, Mohr S, Brandt PY, Gillieron C, Eytan A, Huguelet P. 2007. Religious beliefs in
schizophrenia: their relevance for adherence to treatment. Schizophr Bull 33: 1238-1246.
Breen A, Swartz L, Joska J, Flisher AJ, Corrigall J. 2007. Adherence to treatment in poorer
countries: a new research direction? Psychiatr Serv 58: 567-568.
Byrne MK, Deane FP, Caputi P. 2008. Mental health clinicians' beliefs about medicines, attitudes,
and expectations of improved medication adherence in patients. Eval Health Prof 31: 390-
403.
Campbell M, Young PI, Bateman DN, Smith JM, Thomas SH. 1999. The use of atypical
antipsychotics in the management of schizophrenia. Br J Clin Pharmacol 47: 13-22.
Damen J, Thuresson PO, Heeg B, Lothgren M. 2008. A pharmacoeconomic analysis of
compliance gains on antipsychotic medications. Appl Health Econ Health Policy 6: 189-
197.
Dolder CR, Lacro JP, Dunn LB, Jeste DV. 2002. Antipsychotic medication adherence: is there a
difference between typical and atypical agents? Am J Psychiatry 159: 103-108.
Fenton WS, Blyler CR, Heinssen RK. 1997. Determinants of medication compliance in
schizophrenia: empirical and clinical findings. Schizophr Bull 23: 637-651.
Freudenreich O, Cather C, Evins AE, Henderson DC, Goff DC. 2004. Attitudes of schizophrenia
outpatients toward psychiatric medications: relationship to clinical variables and insight. J
Clin Psychiatry 65: 1372-1376.
Fujikawa M, Togo T, Yoshimi A, et al. 2008. Evaluation of subjective treatment satisfaction with
antipsychotics in schizophrenia patients. Prog Neuropsychopharmacol Biol Psychiatry 32:
755-760.
Gharabawi GM, Greenspan A, Rupnow MF, et al. 2006. Reduction in psychotic symptoms as a
predictor of patient satisfaction with antipsychotic medication in schizophrenia: data from
a randomized double-blind trial. BMC Psychiatry 6: 45.
Hofer A, Kemmler G, Eder U, Edlinger M, Hummer M, Fleischhacker WW. 2004. Quality of life
in schizophrenia: the impact of psychopathology, attitude toward medication, and side
effects. J Clin Psychiatry 65: 932-939.
Hui CL, Chen EY, Kan C, Yip K, Law C, Chiu CP. 2006. Anti-psychotics adherence among out-
patients with schizophrenia in Hong Kong. Keio J Med 55: 9-14.
Jeste DV, Lacro JP, Bailey A, Rockwell E, Harris MJ, Caligiuri MP. 1999. Lower incidence of
tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am
Geriatr Soc 47: 716-719.
Kadri N, Manoudi F, Berrada S, Moussaoui D. 2004. Stigma impact on Moroccan families of
patients with schizophrenia. Can J Psychiatry49(9):625-9.
Kim SW, Yoon JS, Choi SK. 2006. Survey of medication adherence in patients with
Page 11 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
12
schizophrenia--Korean ADHES data. Hum Psychopharmacol 21: 533-537.
Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. 2002. Prevalence of and risk factors for
medication nonadherence in patients with schizophrenia: a comprehensive review of
recent literature. J Clin Psychiatry 63: 892-909.
Lanouette NM, Folsom DP, Sciolla A, Jeste DV. 2009. Psychotropic medication nonadherence
among United States Latinos: a comprehensive literature review. Psychiatr Serv 60: 157-
174.
Lindenmayer JP, Liu-Seifert H, Kulkarni PM, et al. 2009. Medication nonadherence and treatment
outcome in patients with schizophrenia or schizoaffective disorder with suboptimal prior
response. J Clin Psychiatry 70: 990-996.
Liu-Seifert H, Adams DH, Kinon BJ. 2005. Discontinuation of treatment of schizophrenic patients
is driven by poor symptom response: a pooled post-hoc analysis of four atypical
antipsychotic drugs. BMC Med 3: 21.
Lowry DA. 1998. Issues of non-compliance in mental health. J Adv Nurs 28: 280-287.
Lukoff D, Liberman RP, Nuechterlein KH. 1986. Symptom monitoring in the rehabilitation of
schizophrenic patients. Schizophr Bull 12: 578-602. Lukoff D, Lu FG, Turner R. 1995. Cultural considerations in the assessment and treatment of
religious and spiritual problems. Psychiatr Clin North Am.18:467–485.
Maneesakorn S, Robson D, Gournay K, Gray R. 2007. An RCT of adherence therapy for people
with schizophrenia in Chiang Mai, Thailand. J Clin Nurs 16: 1302-1312.
Masand PS, Narasimhan M. 2006. Improving adherence to antipsychotic pharmacotherapy. Curr
Clin Pharmacol 1: 47-56.
Misdrahi D, Llorca PM, Lancon C, Bayle FJ. 2002. [Compliance in schizophrenia: predictive
factors, therapeutical considerations and research implications]. Encephale 28: 266-272.
Mohamed S, Rosenheck R, McEvoy J, Swartz M, Stroup S, Lieberman JA. 2009. Cross-sectional
and longitudinal relationships between insight and attitudes toward medication and clinical
outcomes in chronic schizophrenia. Schizophr Bull 35: 336-346.
Morisky DE, Ang A, Krousel-Wood M, Ward HJ. 2008. Predictive validity of a medication
adherence measure in an outpatient setting. J Clin Hypertens (Greenwich) 10: 348-354.
Morisky DE, Green LW, Levine DM. 1986. Concurrent and predictive validity of a self-reported
measure of medication adherence. Med Care 24: 67-74. Neeleman J, King MB. 1993. Psychiatrists’ religious attitudes in relation to their clinical practice:
a survey of 231 psychiatrists. Acta Psychiatr Scand. 88:420–424.
Overall J, Gorham D. 1962. The brief psychiatric rating scale. Psychol Rep 10: 799-812.
Overall JE, Gorham DR. 1988. The Brief Psychiatric Rating Scale (BPRS): recent developments
in ascertainment and scaling. Psychopharmacol Bull 21: 97-99.
Palmer BW, Heaton RK, Gladsjo JA, et al. 2002. Heterogeneity in functional status among older
outpatients with schizophrenia: employment history, living situation, and driving.
Schizophr Res 55: 205-215.
Pinikahana J, Happell B, Hope J, Keks NA. 2002. Quality of life in schizophrenia: a review of the
literature from 1995 to 2000. Int J Ment Health Nurs 11: 103-111.
Ruggeri M, Koeter M, Schene A, et al. 2005. Factor solution of the BPRS-expanded version in
schizophrenic outpatients living in five European countries. Schizophr Res 75: 107-117.
Sajatovic M, Blow FC, Kales HC, Valenstein M, Ganoczy D, Ignacio RV. 2007. Age comparison
of treatment adherence with antipsychotic medications among individuals with bipolar
disorder. Int J Geriatr Psychiatry 22: 992-998. Shafranske E. 1996. Religion and the Clinical Practice of Psychology. Washington, DC:
American Psychological Association.
Sharma T, Antonova L. 2003. Cognitive function in schizophrenia. Deficits, functional
consequences, and future treatment. Psychiatr Clin North Am 26: 25-40.
Page 12 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
13
Sheikh S, Furnham A. 2000. A cross-cultural study of mental health beliefs and attitudes towards
seeking professional help. Soc Psychiatry Psychiatr Epidemiol. 35(7):326-34.
Svestka J, Bitter I. 2007. Nonadherence to antipsychotic treatment in patients with schizophrenic
disorders. Neuro Endocrinol Lett 28 Suppl 1: 95-116.
Swami V, Furnham A, Kannan K, Sinniah D. 2008. Beliefs about schizophrenia and its treatment
in Kota Kinabalu, Malaysia. Int J Soc Psychiatry 54(2):164-79.
Taira M, Hashimoto T, Takamatsu T, Maeda K. 2006. Subjective response to neuroleptics: the
effect of a questionnaire about neuroleptic side effects. Prog Neuropsychopharmacol Biol
Psychiatry 30: 1139-1142.
Watanabe A, Shibata I, Kato T. 2004. Differences of satisfaction with medication between
patients with schizophrenia treated with typical antipsychotics and atypical antipsychotics.
Psychiatry Clin Neurosci 58: 268-273.
Young JL, Zonana HV, Shepler L. 1986. Medication noncompliance in schizophrenia:
codification and update. Bull Am Acad Psychiatry Law 14: 105-122.
Zahid MA, Ohaeri JU. 2010. Schizophrenia psychopathology in a Kuwaiti Arab sample.
Psychopathology 43(6):345-356. 2010.
Page 13 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
14
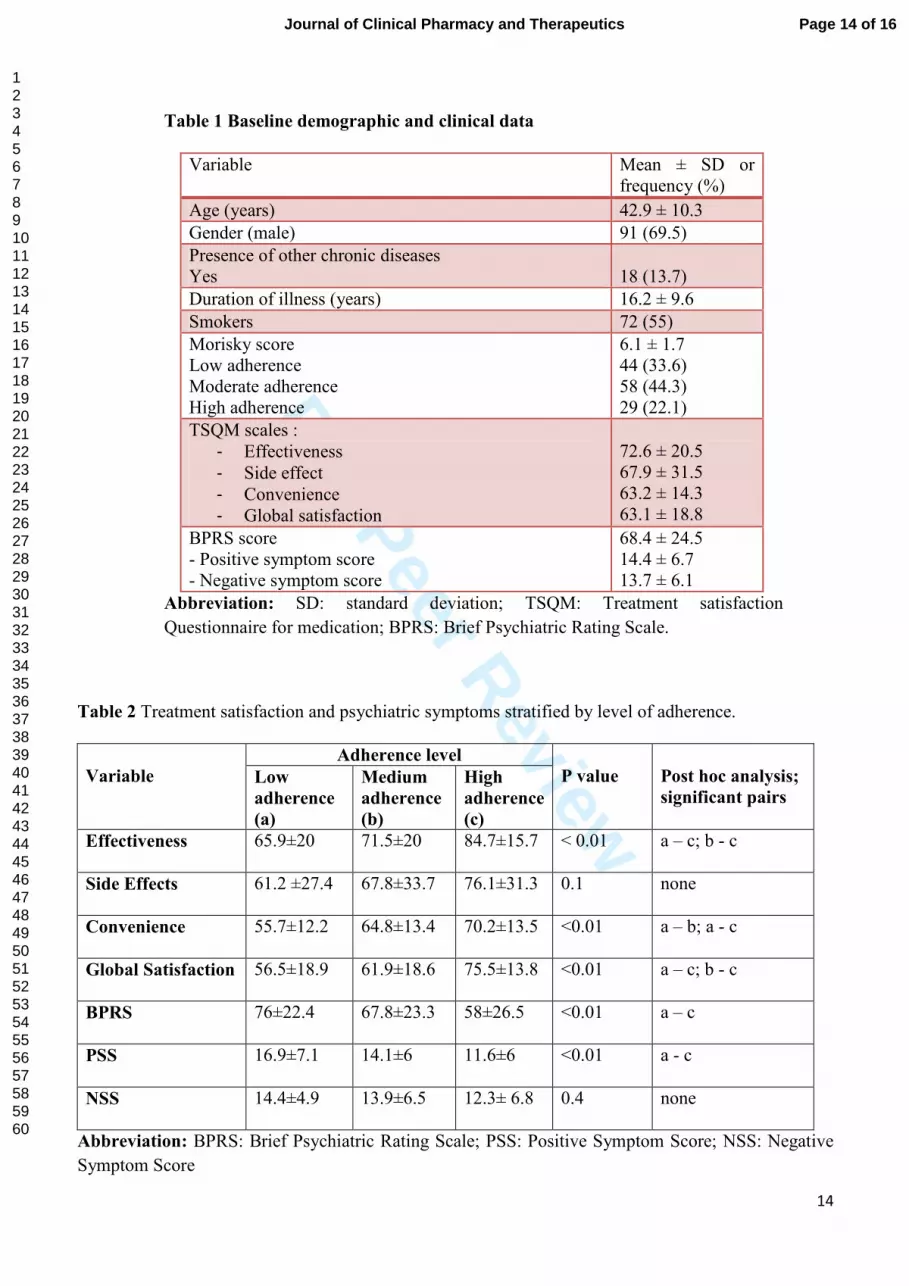
Table 1 Baseline demographic and clinical data
Variable Mean ± SD or
frequency (%)
Age (years) 42.9 ± 10.3
Gender (male) 91 (69.5)
Presence of other chronic diseases
Yes
18 (13.7)
Duration of illness (years) 16.2 ± 9.6
Smokers 72 (55)
Morisky score
Low adherence
Moderate adherence
High adherence
6.1 ± 1.7
44 (33.6)
58 (44.3)
29 (22.1)
TSQM scales :
- Effectiveness
- Side effect
- Convenience
- Global satisfaction
72.6 ± 20.5
67.9 ± 31.5
63.2 ± 14.3
63.1 ± 18.8
BPRS score
- Positive symptom score
- Negative symptom score
68.4 ± 24.5
14.4 ± 6.7
13.7 ± 6.1
Abbreviation: SD: standard deviation; TSQM: Treatment satisfaction
Questionnaire for medication; BPRS: Brief Psychiatric Rating Scale.
Table 2 Treatment satisfaction and psychiatric symptoms stratified by level of adherence.
Adherence level
Variable Low
adherence
(a)
Medium
adherence
(b)
High
adherence
(c)
P value
Post hoc analysis;
significant pairs
Effectiveness
65.9±20 71.5±20 84.7±15.7 < 0.01 a – c; b - c
Side Effects
61.2 ±27.4 67.8±33.7 76.1±31.3 0.1 none
Convenience
55.7±12.2 64.8±13.4 70.2±13.5 <0.01 a – b; a - c
Global Satisfaction
56.5±18.9 61.9±18.6 75.5±13.8 <0.01 a – c; b - c
BPRS
76±22.4 67.8±23.3 58±26.5 <0.01 a – c
PSS
16.9±7.1 14.1±6 11.6±6 <0.01 a - c
NSS
14.4±4.9 13.9±6.5 12.3± 6.8 0.4 none
Abbreviation: BPRS: Brief Psychiatric Rating Scale; PSS: Positive Symptom Score; NSS: Negative
Symptom Score
Page 14 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
15
Page 15 of 16 Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
16
Page 16 of 16Journal of Clinical Pharmacy and Therapeutics
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960





























