Embed Size (px)
Citation preview
Antibodies and Human Transplant Rejection
G. M. WILLIAMS, M.D., B. DEPLANQUE, M.D.,R. LOWER, M.D., D. HUME, M.D.
From the Department of Surgery, Medical College of Virginia, Richmond, Virginia
RECENT studies in "hyperacute rejection"have stimulated interest in the role of anti-body in human allograft rejection. Thisdramatic form of graft rejection was re-ported to occur in recipients who prior totransplantation had serum antibodies reac-tive to the histocompatibility antigens ofthe donor.4' 14,19 Experience has shown thatnot all recipients having cytotoxic anti-bodies to the donor's lymphocytes haveviolent rejections,9 and further some recipi-ents having early intravascular coagulationin the allograft did not have detectableantibodies to the donor's lymphocytes.'2"'These observations have raised clinically sig-nificant questions. First, is the cross-matchbetween the recipient's serum and the do-nor's lymphocytes a reliable means for ex-cluding the presence of antibodies havingpathogenic effects upon the graft? If not,what technics are available for the per-formance of a valid cross-match? Second,if high levels of circulating antibody wereacutely toxic to the graft, what is the ef-fect of lower levels of the same antibodyor of antibodies reacting with less acces-sible antigens? Finally, what is the extentof the clinical problem posed by patients
Presented at the Annual Meeting of the Ameri-can Surgical Association, April 30-May 2, 1969,Cincinnati, Ohio.
Supported by grants (HE-10551, HE-08203,T-5646, MO-IFR 65-07, Atomic Energy Commis-sion Grant AT 40-1-2459, and Contract PH-43-68-659.
rejecting multiple transplants? The studiesto be reported here represent attempts toanswer these questions based on correla-tions between the clinical course and sero-logical findings accompanying 21 humanallografts.
Material and Methods
The patients reported in this study werehospitalized at the Clinical TransplantationCenter at the Medical College of Virginiawith one exception, patient D. L. PatientD. L. received a kidney from a cadaver inRichmond and underwent transplantationin Washington, D. C. by the Transplanta-tion Service at Georgetown University.The patients reported are those whoseserological response to the transplant couldbe monitored by reactions with culturedkidney cells from the organ donor. Thegroup includes all those patients who re-jected a kidney transplant that could besuccessfully cultured, and all who receiveda cadaveric organ where one kidney fromthe cadaver was not transplanted but placedinto tissue culture. The technics of trans-plantation and of immunosuppression thatwere used were the same as those reportedpreviously.3 A small group of the patientsreceived intramuscular injections of horseantilymphocytic globulin prepared byMonaco.6 The serological and tissue cul-ture technics used are identical to thosedescribed previously."'- 16, 18
603
604 WILLIAMS, DEPLANE
TABLE 1. The Time Distribution of the Numbers andof Types of Renal Allografts Performed at
the Medical College of Virginia
No. of Transplants
FunctionalAll Secondary Secondary
Period Primary Cadaver Cadaver
1963-66 102 11 111967 1 1 7 31968 11 5 11969 (Jan-May) 4 4 2
Results
The Clinical ProblemDuring the first 4 years of the renal
transplantation program at the MedicalCollege of Virginia 102 primary and 11secondary kidney allografts were done(Table 1). Ninety-seven of the 102 pri-mary and all of the secondary transplantsfunctioned. This rate of patient turnoverstopped in 1967. Only 11 new patients re-ceived kidney grafts in 1967 and 1968.Twelve secondary transplants were done ofwhich only four had any significant periodof function.The time, effort and expense of caring
for patients with allograft rejection wasconsiderable (Table 2). Seven patients hadgood renal function one year followingsecondary transplantation out of a total of19 patients who could have had success-ful function at 1 year. This group of 19patients undergoing secondary transplanta-tion required a sum total of 142 patient-months of hospitalization. Six patients ac-cumulated 102 patient-months of hospitali-zation during which time they receivednine kidney grafts which never functioned.Only one of these patients is still alive.The mean number of patient-months ofhospitalization expended to produce onegraft successful at one year was 20.3. Bedspace on the Transplantation Unit waspre-empted by patients whose grafts had
QUE, LOVWER AND HUME Annals of SurgeryOctober 1969
TABLE 2. Hospital Time and Success Rate ofSecondary Renal Allografts
Total number of patientsTotal patient-months of hospitalization to dateNumber of patients with currently functioning
allograftsNumber of patients whose allografts have func-
tioned more than 1 yearNumber of patients whose allografts could have
functioned more than 1 yearMean patient-months of hospitalization required
per successful secondary allograft at 1 year
23
154
20.3
failed and who continued to reject addi-tional grafts.
In order to define the reason for thehigh failure rate of secondary transplantsoccurring after 1966, a search was firstmade for possible changes in technic. Ananalysis of the success rate of primary andsecondary transplants from cadaveric do-nors revealed that there was no comparabledecline in the success rate for primarygrafts. Functional grafts were obtained in39 of 43 primary transplants, but in only 17of 27 secondary transplants. Technicalfactors complicating transplantation wereclearly present in three of four primarytransplants that failed. However, no ap-parent technical faults contributed to thefailure of the ten secondary grafts. Earlybiopsies taken from nine secondary trans-plants revealed large numbers of polymor-phonuclear leukocytes in the renal capil-laries on eight occasions. Thus other thanthe small sample size, there was no obviousexplanation why secondary transplantsfunctioned uniformly well prior to 1967but failed to have any period of functionin over one half of the transplants carriedout after 1967. Paradoxically, prior to 1967the recipients of second transplants werematched with their donors for ABO com-patibility only.
Rejection and Preformed AntibodiesEarly in our experience five kidney grafts
were placed into recipients whose serum
Volume 170 ANTIBODIES AND HUMA]Number 4
showed cytotoxicity to the donor's lympho-cytes. Three of the five kidneys were re-
moved at the time of insertion on the basisof extreme cyanosis and dramatic reduc-tions in blood flow. The two kidneys whichwere not removed at transplantation never
functioned (Table 4).A negative cytotoxicity reaction between
the recipient's serum drawn within 2 weeksof transplantation and the donor's lympho-cytes formed the basis for the selection ofdonors for 11 transplants. Despite this pre-
caution, six kidney grafts failed to func-tion, although none of these reactions were
sufficiently violent to require resection ofthe graft at the time of transplantation.One liver recipient and one heart trans-plant recipient experienced transient func-tion of their grafts, but both died from re-
jection 7 days after transplantation. All ofthe recipients were found to have antibodydetectable in reactions with the culturedkidney cells of the donor (Table 4).The serum from three recipients failed
to react with either the lymphocytes or the
N TRANSPLANT REJECTION 605TABLE 3. The Frequency of Non-functional Renal
Allografis in Primary and SecondaryCadaveric Donor Grafts
Function of CadavericKidneys
Category Present Absent
1st transplants 39 4*2nd transplants 17 10**
* Three known technical failures.** No known technical failures.Two additional secondary transplants were rejected
on A-V shunts.
kidney cells of the donor and their graftsfunctioned normally (Table 4). Two ofthese patients had previously rejected onekidney transplant and had demonstrablecytotoxic antibodies to other potential do-nors. Three other patients are enjoying nor-mal renal function 12, 5, and 2 months fol-lowing transplantation despite the presenceof pre-existing serum antibodies reactiveagainst donor kidney cells. The antibodytiters were low in two of these recipients
TABLE 4. Correlations between Preformed Antibody Actizity and the Clinical Outcome of Human Allografts
Technic for Detecting Pre-existingAntibody against Antigens Clinical Outcome
AntibodyAntibody Titer
Titer Imm. GraftMixed Adher Removed Tran-
Lympho- Agglut. vs. at Non- sientPatient & Cyto- vs. Kidney Kidney Transpl. Func- Func- Func-
Organ # Transplant toxicity Cells Cells Oper. tional tion tional
Kidney S. S. #3 + 1/90 1/64 +W. J. #2 + 1/90 1/32 +M. D. #2 + 1/810 +M.D. #3 + +S. G. #2 + 1/810 +
S. S. #2 - 1/90 +P. S. #3 - 1/90 +H. F. #1 - 1/30 +
E. R. #3 - 1/30 +P. S. #4 - 1/200 1/8 +C. R. #2 - 1/30 +D. P. #1 - 1/2 +D. P. #2 - 1/30 +D.L. #1 - 1/2 +
Heart P. J. - 1/16 +
Liver A. H. - 1/30 +
Totals 3 8 2 3
WILLIAMS, DEPLANQUE, LOWER AND HUME
3 44
- 21mgBS21mg%
> Eluate90 9SO
Annals of SurgeryOctober 1969
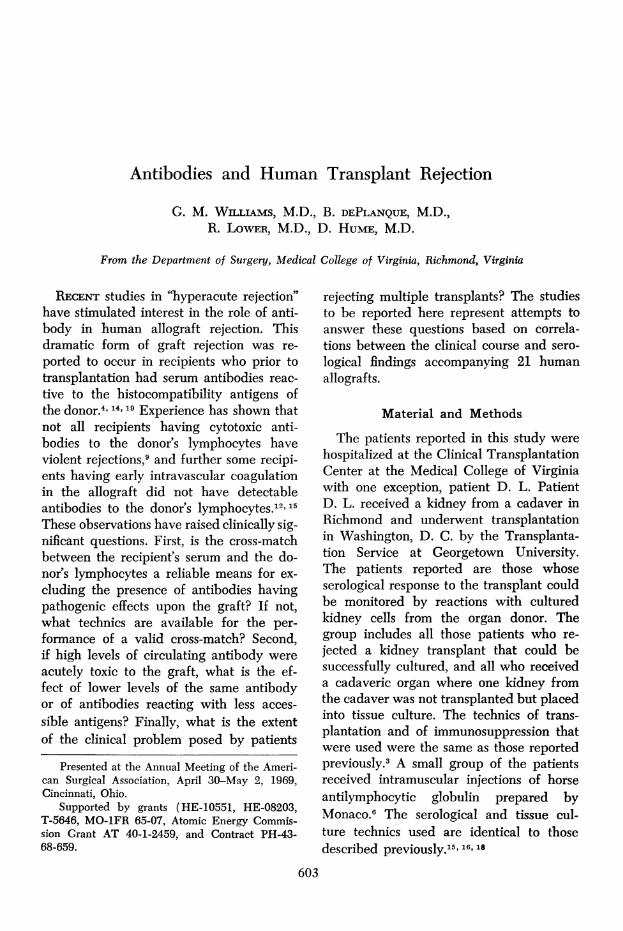
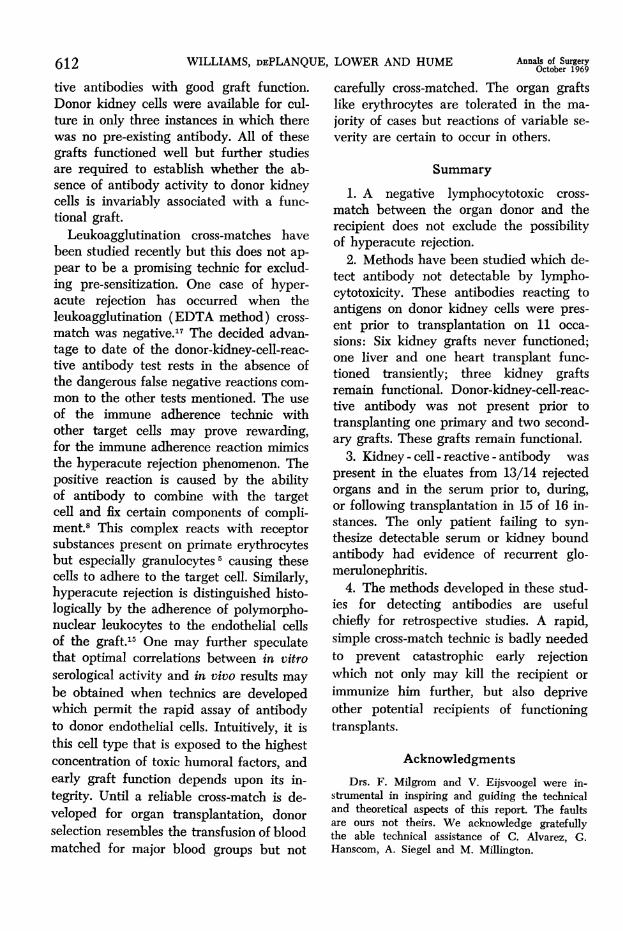
Fic. 1. The postop-erative course of A. H.,recipient of a liver trans-plant. Despite daily ex-
Ai7/ change transfusions the',te' prothrombin concentra-
tion remained low andantibody reappeared inthe circulation.
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140 150 ro0 170
TIME (hrs )
(H. F., D. L.) but the third patients (D. P.#2) had a relatively high titer of antibodyto donor kidney cells by the immune ad-herence test (Table 4).
In addition to the 16 grafts listed inTable 4, two kidneys developed extensiveaccumulations of polymorphonuclear leu-kocytes in the renal capillaries while be-ing perfused through the recipient's A.V.shunt. Cytotoxic antibodies were presentagainst donor lymphocytes in one instance.In the other, cytotoxic antibodies were notpresent, but antibodies were detected byimmune adherence in reactions with donorkidney cells. Including these latter twokidneys, serum antibody detected in reac-
tions with donor cells was present prior totransplantation on 18 occasions. Thirteenkidney grafts never functioned; three func-tioned well, and one liver and one hearttransplant were rejected at one week. Nocase of early dramatic failure occurred inwhich pre-existing antibodies to donor an-
tigens were not detected. Systemic hepa-rinization and massive steroid treatmentwere ineffective in reversing these fulmi-nating rejections.The two patients who rejected non-renal
transplants acutely are of particular inter-
est. Both recipients were Negroes and bothreceived Negro organs. Neither of the pa-
tients had any history of blood transfusionsor pregnancies. The course following hearttransplantation in P. J. has been describedin greater detail elsewhere."8 The heartfunctioned well for 41/2 days, but at thattime uncontrollable rejection occurred. Theheart at autopsy was edematous and hem-orrhagic. The cellular infiltrate was a mix-ture of mononuclear and polymorphonu-clear leukocytes. The clinical course of theliver transplant recipient was characterizedby more rapid graft failure.
Case ReportA. H., a 2-year-old Negro boy with biliary
atresia was admitted to the Pediatric Service ofthe Medical College of Virginia because of de-terioration of liver function and ascites.
Eight potential donors were screened over a
2-month period, and, in three instances, the pa-
tient's serum produced cytotoxic activity againstthe potential donor's lymphocytes. The eventualdonor of the liver transplant was a 3-year-oldchild who was accidently shot in the head. Leuko-cyte typing revealed donor-recipient incompati-bilities at HLA-1 and HLA-3. A freshly drawnserum sample from the patient failed to react withthe lymphocytes of the donor by cytotoxicity. Thedecision to transplant the liver from this donor
606
Volume 170Number 4
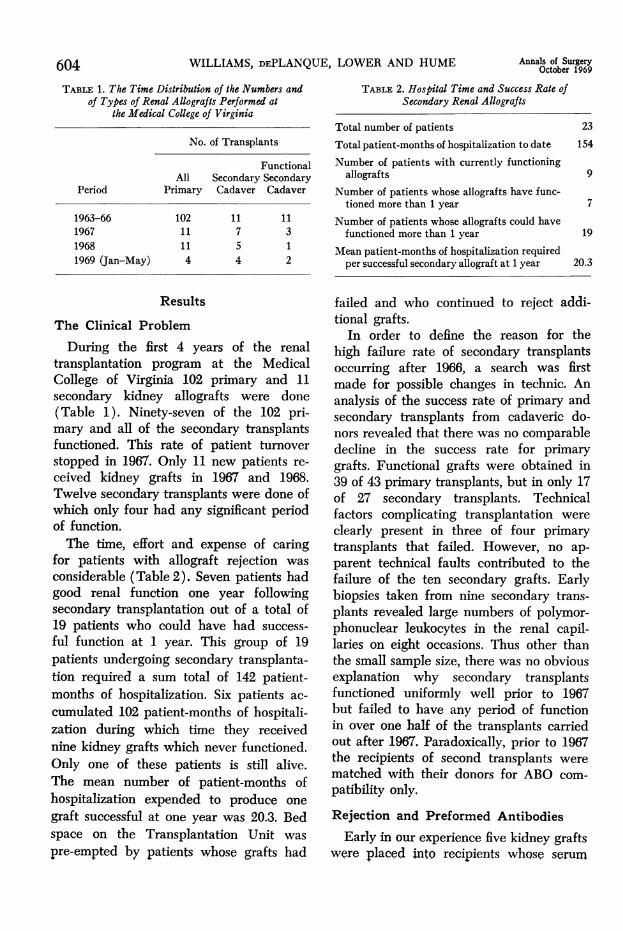
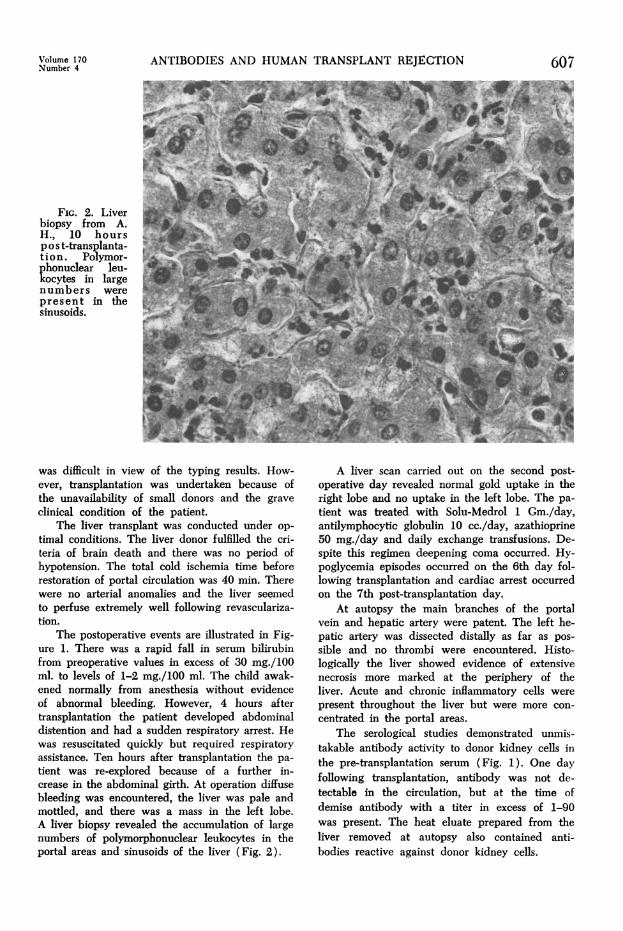
FIG. 2. Liverbiopsy from A.H., 10 hoursp o s t-transplanta-tion . Polymor-phonuclear leu-kocytes in largenumbers werepresent in thesinusoids.
ANTIBODIES AND HUMAN TRANSPLANT REJECTION
was difficult in view of the typing results. How-ever, transplantation was undertaken because ofthe unavailability of small donors and the graveclinical condition of the patient.
The liver transplant was conducted under op-timal conditions. The liver donor fulfilled the cri-teria of brain death and there was no period ofhypotension. The total cold ischemia time beforerestoration of portal circulation was 40 min. Therewere no arterial anomalies and the liver seemedto perfuse extremely well following revasculariza-tion.
The postoperative events are illustrated in Fig-ure 1. There was a rapid fall in serum bilirubinfrom preoperative values in excess of 30 mg./100ml. to levels of 1-2 mg./100 ml. The child awak-ened normally from anesthesia without evidenceof abnormal bleeding. However, 4 hours aftertransplantation the patient developed abdominaldistention and had a sudden respiratory arrest. Hewas resuscitated quickly but required respiratoryassistance. Ten hours after transplantation the pa-tient was re-explored because of a further in-crease in the abdominal girth. At operation diffusebleeding was encountered, the liver was pale andmottled, and there was a mass in the left lobe.A liver biopsy revealed the accumulation of largenumbers of polymorphonuclear leukocytes in theportal areas and sinusoids of the liver (Fig. 2).
607
A liver scan carried out on the second post-operative day revealed normal gold uptake in theright lobe and no uptake in the left lobe. The pa-tient was treated with Solu-Medrol 1 Gm./day,antilymphocytic globulin 10 cc./day, azathioprine50 mg./day and daily exchange transfusions. De-spite this regimen deepening coma occurred. Hy-poglycemia episodes occurred on the 6th day fol-lowing transplantation and cardiac arrest occurredon the 7th post-transplantation day.
At autopsy the main branches of the portalvein and hepatic artery were patent. The left he-patic artery was dissected distally as far as pos-sible and no thrombi were encountered. Histo-logically the liver showed evidence of extensivenecrosis more marked at the periphery of theliver. Acute and chronic inflammatory cells werepresent throughout the liver but were more con-centrated in the portal areas.
The serological studies demonstrated unmis-takable antibody activity to donor kidney cells inthe pre-transplantation serum (Fig. 1). One dayfollowing transplantation, antibody was not de-tectable in the circulation, but at the time ofdemise antibody with a titer in excess of 1-90was present. The heat eluate prepared from theliver removed at autopsy also contained anti-bodies reactive against donor kidney cells.
WILLIAMS, DEPLANQUE, LOWER AND HUME
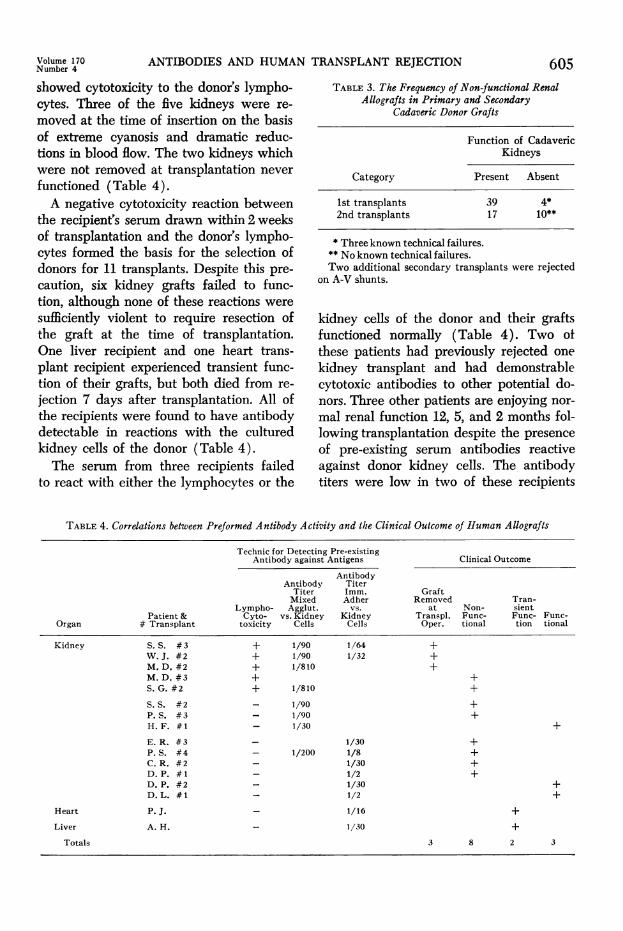
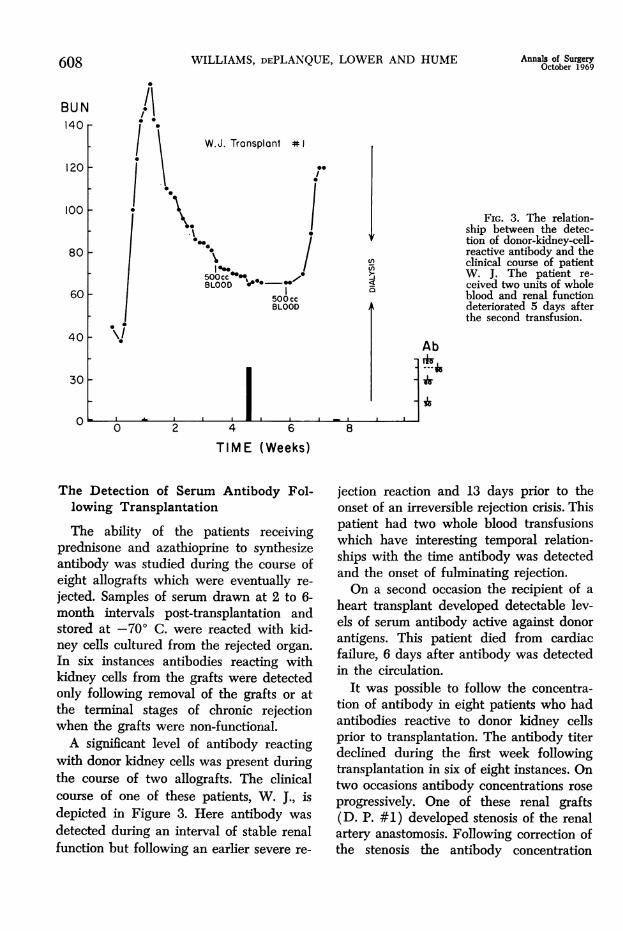
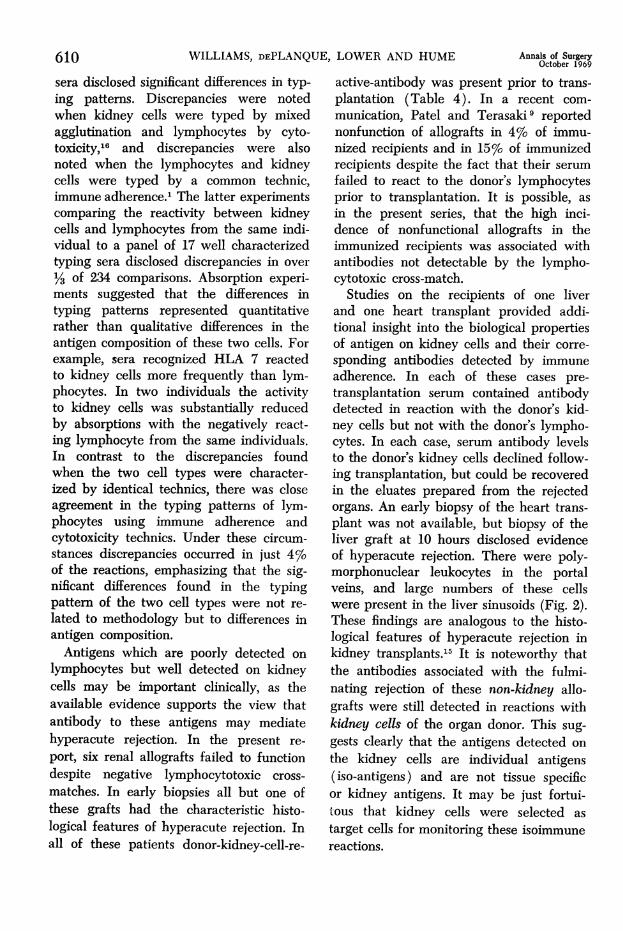
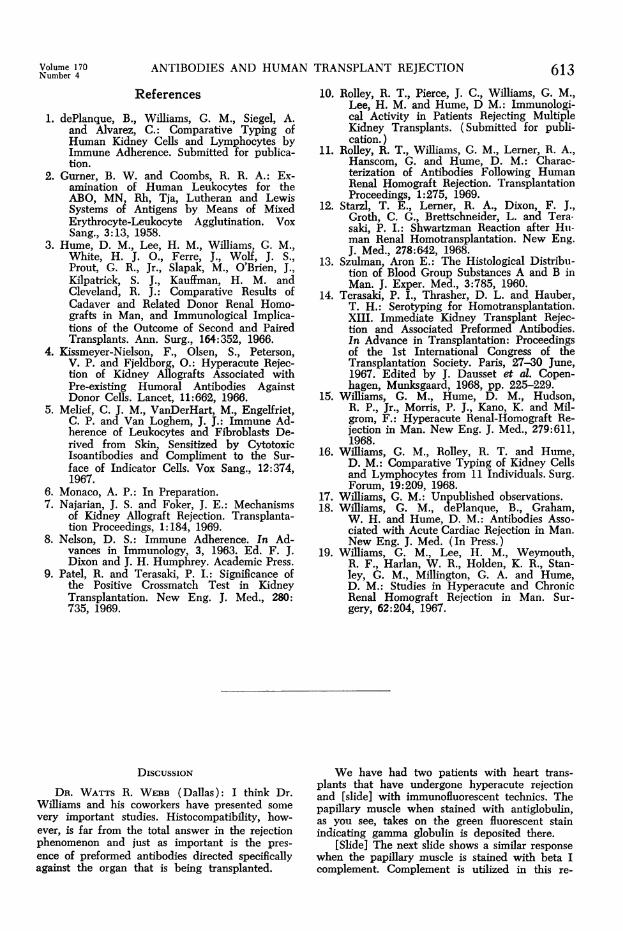
Fic. 3. The relation-ship between the detec-tion of donor-kidney-cell-reactive antibody and theclinical course of patientW. J. The patient re-ceived two units of wholeblood and renal functiondeteriorated 5 days afterthe second transfusion.
AbiT,
TIME (Weeks)
The Detection of Serum Antibody Fol-lowing Transplantation
The ability of the patients receivingprednisone and azathioprine to synthesizeantibody was studied during the course ofeight allografts which were eventually re-
jected. Samples of serum drawn at 2 to 6-month intervals post-transplantation andstored at -700 C. were reacted with kid-ney cells cultured from the rejected organ.
In six instances antibodies reacting withkidney cells from the grafts were detectedonly following removal of the grafts or atthe terminal stages of chronic rejectionwhen the grafts were non-functional.A significant level of antibody reacting
with donor kidney cells was present duringthe course of two allografts. The clinicalcourse of one of these patients, W. J., isdepicted in Figure 3. Here antibody was
detected during an interval of stable renalfunction but following an earlier severe re-
jection reaction and 13 days prior to theonset of an irreversible rejection crisis. Thispatient had two whole blood transfusionswhich have interesting temporal relation-ships with the time antibody was detectedand the onset of fulminating rejection.On a second occasion the recipient of a
heart transplant developed detectable lev-els of serum antibody active against donorantigens. This patient died from cardiacfailure, 6 days after antibody was detectedin the circulation.
It was possible to follow the concentra-tion of antibody in eight patients who hadantibodies reactive to donor kidney cellsprior to transplantation. The antibody titerdeclined during the first week followingtransplantation in six of eight instances. Ontwo occasions antibody concentrations rose
progressively. One of these renal grafts(D. P. #1) developed stenosis of the renalartery anastomosis. Following correction ofthe stenosis the antibody concentration
Annals of SurgeryOctober 1969608
BUN140
120
100
80
60
40
30
0
Volume 170 ANTIBODIES AND HUMA:Number 4
continued to increase. A second patient(P. S. #4) received a graft which neverfunctioned and which was necrotic on re-moval 13 days following transplantation.Serum antibody reacting with cultured
donor kidney cells was never demonstratedin one case of graft failure. (E. R. #2).This patient developed proteinuria, and thetransplant had linear deposits of IgG andBIC globulin along the glomerular base-ment membrane. Serum drawn prior to thistransplant produced significant proteinuriain squirrel monkeys."1
The Detection of Antibody in Heat Elu-ates Prepared from Rejected Allografts
Heating homogenized rejected allograftsto 56° C. released antibodies reactive tocultured cells from donor kidneys in 13 of14 instances (Table 5). Antibody was notrecovered from the graft of E. R. #2, nor,as mentioned above could isoantibody bedetected following removal of this trans-plant.Donor reactive antibody was detected in
eluates prepared from organs rejected byhyperacute, acute, or chronic mechanisms.Antibody was recovered from two kidneysremoved for hyperacute rejection 2 hoursafter the initiation of blood flow to thegraft. Antibodies were also present in allof the eluates prepared from five kidneysundergoing fulminating early rejection butremoved at 1 to 9 weeks following trans-plantation. The eluates prepared from threechronically rejected kidneys removed at 2,2 and 3 years were also positive. In eachinstance the titer of antibody relative tothe concentration of IgG present in theeluate was higher than the correspondingvalues in the serum, suggesting that ourpositive results could not have been dueto contamination of the hemogenates byantibody in the serum.
DiscussionDuring the past 2% years, 10 of 16 sec-
ondary renal allografts performed at the
LN TRANSPLANT REJECTION 609TABLE 5. The Detection of Donor-kidney-cell-reactive
Antibody in Eluates of Rejected Organs
Clinical Type of No. withOrgan Rejection No. Antibody
Kidney Chronic 4 3Acute 1 1Hyperacute 6 6
Heart Acute 2 2
Liver Hyperacute 1 1
14 13
Medical College of Virginia did not func-tion. This experience has been disconcert-ing particularly since 11 of the secondarygrafts carried out prior to 1967 functioned(Table 1). During the past 2 years bedspace and medical attention has shiftedfrom the care of postoperative patients tothe care of dibilitated "rejectors." In thissetting of clinical concern and frustrationmethods were developed and applied inthe hope of distinguishing the critical fac-tors related to the success and failure ofsecondary allografts.An early case of "hyperacute rejection"
influenced the direction for our studies. Inthis case, studies carried out in collabora-tion with Milgrom and Kano15 demon-strated that, while the recipient's pre-trans-plantation serum failed to react with thelymphocytes of the donor, there was aclear reaction with the donor's kidney cells.That cells from different tissues containedimportant differences in antigen concentra-tion was also suggested by the distributionof A and B blood group antigens of recog-nized importance in human transplanta-tion. These antigens known to be in highconcentration on erythrocytes and endo-thelial cells13 are demonstrated to be onlymphocytes by extremely sensitive tech-nics 2 and not by lymphocytotoxicity.
Systematic studies comparing the spec-trum of activity of an individual's lympho-cytes and kidney cells to characterized
610 WILLIAMS, DEPLANQUE, LOWER AND HUME
sera disclosed significant differences in typ-ing patterns. Discrepancies were notedwhen kidney cells were typed by mixedagglutination and lymphocytes by cyto-toxicity,16 and discrepancies were alsonoted when the lymphocytes and kidneycells were typed by a common technic,immune adherence.1 The latter experimentscomparing the reactivity between kidneycells and lymphocytes from the same indi-vidual to a panel of 17 well characterizedtyping sera disclosed discrepancies in over1/3 of 234 comparisons. Absorption experi-ments suggested that the differences intyping patterns represented quantitativerather than qualitative differences in theantigen composition of these two cells. Forexample, sera recognized HLA 7 reactedto kidney cells more frequently than lym-phocytes. In two individuals the activityto kidney cells was substantially reducedby absorptions with the negatively react-ing lymphocyte from the same individuals.In contrast to the discrepancies foundwhen the two cell types were character-ized by identical technics, there was closeagreement in the typing patterns of lym-phocytes using immune adherence andcytotoxicity technics. Under these circum-stances discrepancies occurred in just 4%of the reactions, emphasizing that the sig-nificant differences found in the typingpattern of the two cell types were not re-lated to methodology but to differences inantigen composition.
Antigens which are poorly detected onlymphocytes but well detected on kidneycells may be important clinically, as theavailable evidence supports the view thatantibody to these antigens may mediatehyperacute rejection. In the present re-port, six renal allografts failed to functiondespite negative lymphocytotoxic cross-matches. In early biopsies all but one ofthese grafts had the characteristic histo-logical features of hyperacute rejection. Inall of these patients donor-kidney-cell-re-
Annals of SurgeryOctober 1969
active-antibody was present prior to trans-plantation (Table 4). In a recent com-munication, Patel and Terasaki9 reportednonfunction of allografts in 4% of immu-nized recipients and in 15% of immunizedrecipients despite the fact that their serumfailed to react to the donor's lymphocytesprior to transplantation. It is possible, asin the present series, that the high inci-dence of nonfunctional allografts in theimmunized recipients was associated withantibodies not detectable by the lympho-cytotoxic cross-match.
Studies on the recipients of one liverand one heart transplant provided addi-tional insight into the biological propertiesof antigen on kidney cells and their corre-sponding antibodies detected by immuneadherence. In each of these cases pre-transplantation serum contained antibodydetected in reaction with the donor's kid-ney cells but not with the donor's lympho-cytes. In each case, serum antibody levelsto the donor's kidney cells declined follow-ing transplantation, but could be recoveredin the eluates prepared from the rejectedorgans. An early biopsy of the heart trans-plant was not available, but biopsy of theliver graft at 10 hours disclosed evidenceof hyperacute rejection. There were poly-morphonuclear leukocytes in the portalveins, and large numbers of these cellswere present in the liver sinusoids (Fig. 2).These findings are analogous to the histo-logical features of hyperacute rejection inkidney transplants.15 It is noteworthy thatthe antibodies associated with the fulmi-nating rejection of these non-kidney allo-grafts were still detected in reactions withkidney cells of the organ donor. This sug-gests clearly that the antigens detected onthe kidney cells are individual antigens(iso-antigens) and are not tissue specificor kidney antigens. It may be just fortui-tous that kidney cells were selected astarget cells for monitoring these isoimmunereactions.
Volume 170 ANTIBODIES AND HUMANumber 4
The grafts placed into sensitized recipi-ents displayed different degrees of func-tion. Three out of the total of 16 graftsstudied were clearly non-viable at onehour; eight others had sufficient perfusionto risk leaving the graft in place, and fivegrafts appeared to be functioning well atthe conclusion of the operative procedure.Three of these five grafts continue to func-tion well. Quantitative considerations mightexplain why two of these three grafts func-tioned despite the presence of antibody(Table 4), but the third patient had titersof antibody to donor kidney cells associ-ated with violent rejections in other pa-tients. It is evident that antibody is justone of several factors important in immedi-ate graft failure. The co-existence of "block-ing" or "enhancing" antibodies, and defectsin the compliment and coagulaiton systemmight explain why these three grafts func-tioned well despite evidence of pre-exist-ing immunity. This situation appears analo-gous to the success of some transplantsmismatched for major blood group anti-gens.
It is likely that antibody synthesized aftertransplantation also produces variable ef-fects on the graft. There is increasingexperimental evidence recently reviewedby Najarian 7 that antibodies can be toxicto allografts, and the present studiesleave little doubt about the ability ofeven immunosuppressed human recipientsto synthesize antibody to their grafts. Atsome time following transplantation donor-kidney-cell-reactive-antibodies were de-tected in the circulation of 15 of 16 pa-tients and antibodies were recovered ineluates from 13 of 14 rejected grafts. Thesingle patient (E. R. #2) not demonstrat-ing antibody in either the serum or eluateprobably lost the function of her graft onthe basis of recurrent glomerulonephritis.Attempts to monitor the rejection processby measuring the serum levels of the donor-kidney-reactive-antibody are hampered by
LN TRANSPLANT REJECTION 611the absorption of this antibody by thegraft. Donor-kidney-cell-antibody was de-tected in most instances at times whenthe graft was clearly functioning poorly.Only two patients had detectable levelsof serum antibody during intervals ofclinically stable graft function. However,here the detection of antibody precededfulminating graft rejections unresponsiveto steriods. These findings support theview advanced previously that antibodiesare important mediators of allograft re-jection, and further, that detection ofdonor-reactive antibody in the circulationrepresents a situation where the rate ofantibody synthesis exceeds the rate ofabsorption by the graft. For this to occureither antibody synthesis must be veryrapid or circulation to the graft must bepoor, or both. Under any of these circum-stances the prognosis is gloomy for thecontinued function of the graft.
In the future it seems evident that, inaddition to means for better donor organprocurement and better immunosuppres-sion, better methods are required for per-forming a prospective donor-recipient cross-match to exclude pre-sensitization. Currentimmunosuppressive technics have been ap-plied extensively to our immunized pro-spective recipients without affecting thetiters of circulating isoantibodies.10 At pres-ent it appears most likely that the problemof pre-immunization must be solved byproper donor selection rather than relyingon more potent immunosuppressive agents.Our experience using donor kidney cells astargets for detecting pre-immunization hasbeen rewarding, but these technics are cer-tainly not ideal. A prospective cross-matchusing donor kidney cells is not possiblewith mixed agglutination and is imprac-ticable with immune adherence especiallyin living donors. This defect was mani-fested in our present studies where welacked the opportunity to correlate the ab-sence of preformed donor-kidney-cell reac-
612 WILLIAMS, DEPLANQUE, LOWER AND HUME
tive antibodies with good graft function.Donor kidney cells were available for cul-ture in only three instances in which therewas no pre-existing antibody. All of thesegrafts functioned well but further studiesare required to establish whether the ab-sence of antibody activity to donor kidneycells is invariably associated with a func-tional graft.
Leukoagglutination cross-matches havebeen studied recently but this does not ap-pear to be a promising technic for exclud-ing pre-sensitization. One case of hyper-acute rejection has occurred when theleukoagglutination (EDTA method) cross-match was negative.17 The decided advan-tage to date of the donor-kidney-cell-reac-tive antibody test rests in the absence ofthe dangerous false negative reactions com-mon to the other tests mentioned. The useof the immune adherence technic withother target cells may prove rewarding,for the immune adherence reaction mimicsthe hyperacute rejection phenomenon. Thepositive reaction is caused by the abilityof antibody to combine with the targetcell and fix certain components of compli-ment.8 This complex reacts with receptorsubstances present on primate erythrocytesbut especially granulocytes 5 causing thesecells to adhere to the target cell. Similarly,hyperacute rejection is distinguished histo-logically by the adherence of polymorpho-nuclear leukocytes to the endothelial cellsof the graft.15 One may further speculatethat optimal correlations between in vitroserological activity and in vivo results maybe obtained when technics are developedwhich permit the rapid assay of antibodyto donor endothelial cells. Intuitively, it isthis cell type that is exposed to the highestconcentration of toxic humoral factors, andearly graft function depends upon its in-tegrity. Until a reliable cross-match is de-veloped for organ transplantation, donorselection resembles the transfusion of bloodmatched for major blood groups but not
Annals of SurgeryOctober 1969
carefully cross-matched. The organ graftslike erythrocytes are tolerated in the ma-jority of cases but reactions of variable se-verity are certain to occur in others.
Summary1. A negative lymphocytotoxic cross-
match between the organ donor and therecipient does not exclude the possibilityof hyperacute rejection.
2. Methods have been studied which de-tect antibody not detectable by lympho-cytotoxicity. These antibodies reacting toantigens on donor kidney cells were pres-ent prior to transplantation on 11 occa-sions: Six kidney grafts never functioned;one liver and one heart transplant func-tioned transiently; three kidney graftsremain functional. Donor-kidney-cell-reac-tive antibody was not present prior totransplanting one primary and two second-ary grafts. These grafts remain functional.
3. Kidney - cell - reactive - antibody waspresent in the eluates from 13/14 rejectedorgans and in the serum prior to, during,or following transplantation in 15 of 16 in-stances. The only patient failing to syn-thesize detectable serum or kidney boundantibody had evidence of recurrent glo-merulonephritis.
4. The methods developed in these stud-ies for detecting antibodies are usefulchiefly for retrospective studies. A rapid,simple cross-match technic is badly neededto prevent catastrophic early rejectionwhich not only may kill the recipient orimmunize him further, but also depriveother potential recipients of functioningtransplants.
AcknowledgmentsDrs. F. Milgrom and V. Eiisvoogel were in-
strumental in inspiring and guiding the technicaland theoretical aspects of this report. The faultsare ours not theirs. We acknowledge gratefullythe able technical assistance of C. Alvarez, G.Hanscom, A. Siegel and M. Millington.
Volume 170 ANTIBODIES AND HUMAN TRANSPLANT REJECTION 613Number 461References
1. dePlanque, B., Williams, G. M., Siegel, A.and Alvarez, C.: Comparative Typing ofHuman Kidney Cells and Lymphocytes byImmune Adherence. Submitted for publica-tion.
2. Gurner, B. W. and Coombs, R. R. A.: Ex-amination of Human Leukocytes for theABO, MN, Rh, Tja, Lutheran and LewisSystems of Antigens by Means of MixedErythrocyte-Leukocyte Agglutination. VoxSang., 3:13, 1958.
3. Hume, D. M., Lee, H. M., Williams, G. M.,White, H. J. O., Ferre, J., Wolf, J. S.,Prout, G. R., Jr., Slapak, M., O'Brien, J.,Kilpatrick, S. J., Kauffman, H. M. andCleveland, R. J.: Comparative Results ofCadaver and Related Donor Renal Homo-grafts in Man, and Immunological Implica-tions of the Outcome of Second and PairedTransplants. Ann. Surg., 164:352, 1966.
4. Kissmeyer-Nielson, F., Olsen, S., Peterson,V. P. and Fjeldborg, O.: Hyperacute Rejec-tion of Kidney Allografts Associated withPre-existing Humoral Antibodies AgainstDonor Cells. Lancet, 11:662, 1966.
5. Melief, C. J. M., VanDerHart, M., Engelfriet,C. P. and Van Loghem, J. J.: Immune Ad-herence of Leukocytes and Fibroblasts De-rived from Skin, Sensitized by CytotoxicIsoantibodies and Compliment to the Sur-face of Indicator Cells. Vox Sang., 12:374,1967.
6. Monaco, A. P.: In Preparation.7. Najarian, J. S. and Foker, J. E.: Mechanisms
of Kidney Allograft Rejection. Transplanta-tion Proceedings, 1:184, 1969.
8. Nelson, D. S.: Immune Adherence. In Ad-vances in Immunology, 3, 1963. Ed. F. J.Dixon and J. H. Humphrey. Academic Press.
9. Patel, R. and Terasaki, P. I.: Significance ofthe Positive Crossmatch Test in KidneyTransplantation. New Eng. J. Med., 280:735, 1969.
10. Rolley, R. T., Pierce, J. C., Williams, G. M.,Lee, H. M. and Hume, D M.: Immunologi-cal Activity in Patients Rejecting MultipleKidney Transplants. (Submitted for publi-cation.)
11. Rolley, R. T., Williams, G. M., Lerner, R. A.,Hanscom, G. and Hume, D. M.: Charac-terization of Antibodies Following HumanRenal Homograft Rejection. TransplantationProceedings, 1:275, 1969.
12. Starzl, T. E., Lerner, R. A., Dixon, F. J.,Groth, C. G., Brettschneider, L. and Tera-saki, P. I.: Shwartzman Reaction after Hii-man Renal Homotransplantation. New Eng.J. Med., 278:642, 1968.
13. Szulman, Aron E.: The Histological Distribu-tion of Blood Group Substances A and B inMan. J. Exper. Med., 3:785, 1960.
14. Terasaki, P. I., Thrasher, D. L. and Hauber,T. H.: Serotyping for Homotransplantation.XIII. Immediate Kidney Transplant Rejec-tion and Associated Preformed Antibodies.In Advance in Transplantation: Proceedingsof the 1st Intemational Congress of theTransplantation Society. Paris, 27-30 June,1967. Edited by J. Dausset et al. Copen-hagen, Munksgaard, 1968, pp. 225-229.
15. Williams, G. M., Hume, D. M., Hudson,R. P., Jr., Morris, P. J., Kano, K. and Mil-grom, F.: Hyperacute Renal-Homograft Re-jection in Man. New Eng. J. Med., 279:611,1968.
16. Williams, G. M., Rolley, R. T. and Hume,D. M.: Comparative Typing of Kidney Cellsand Lymphocytes from 11 Individuals. Surg.Forum, 19:209, 1968.
17. Williams, G. M.: Unpublished observations.18. Williams, G. M., dePlanque, B., Graham,
W. H. and Hume, D. M.: Antibodies Asso-ciated with Acute Cardiac Rejection in Man.New Eng. J. Med. (In Press.)
19. Williams, G. M., Lee, H. M., Weymouth,R. F., Harlan, W. R., Holden, K. R., Stan-ley, G. M., Millington, G. A. and Hume,D. M.: Studies in Hyperacute and ChronicRenal Homograft Rejection in Man. Sur-gery, 62:204, 1967.
DIscussION
DR. WATTS R. WEBB (Dallas): I think Dr.Williams and his coworkers have presented somevery important studies. Histocompatibility, how-ever, is far from the total answer in the rejectionphenomenon and just as important is the pres-ence of preformed antibodies directed specificallyagainst the organ that is being transplanted.
We have had two patients with heart trans-plants that have undergone hyperacute rejectionand [slide] with immunofluorescent technics. Thepapillary muscle when stained with antiglobulin,as you see, takes on the green fluorescent stainindicating gamma globulin is deposited there.
[Slide] The next slide shows a similar responsewhen the papillary muscle is stained with beta Icomplement. Complement is utilized in this re-





























