Embed Size (px)
Citation preview
4/8/19
1
ANA Testing: HEp-2 IFA versus Solid-Phase Assays
Kathleen A. Hoag, PhD, MLS(ASCP)cm
Associate Professor, Biomedical Laboratory Diagnostics ProgramMichigan State University
Speaker conflict of interest/disclosure
• Dr. Hoag is an employee of Michigan State University, but her opinions and interpretations are hers alone• Dr. Hoag has no commercial/vendor sponsorship nor financial interest• Dr. Hoag is a member of the scientific advisory board for American
Proficiency Institute, Traverse City, MI
Learning Objectives
At the conclusion of the presentation, the attendees should be able to:• Describe the basic HEp-2 IFA procedure for ANA screening• Identify several solid-phase ANA assays and list the target antigens• List pros and cons of both the HEp-2 IFA and solid-phase ANA
Definitions:
• Antinuclear antibody (ANA) = autoantibody which targets nuclear components of self cells• Fluorescent Antinuclear Antibody (FANA) = HEp-2 Indirect
Immunofluorescence Assay (IIFA) = Gold standard for screening detection of antinuclear antibody• Extractable nuclear antigen (ENA) = testing designed to identify the
specific cellular antigen targeted by ANA• Anti-dsDNA• Anti-Ro• Anti-SS-A or SS-B• etcetera
Utility of Antinuclear Antibody Testing
• ANA assays are screening tests for systemic autoimmune rheumatologic diseases (SLE, Sjogren’s syndrome, Systemic sclerosis/Scleroderma, RA)• Numerous studies (over 4 decades) determined that ANA positivity is
higher in females than males, and incidence increases with age• Apparently healthy individuals may have positive ANA tests, so follow-
up testing is always indicated and must be correlated with patient history and symptoms
Learning Objectives
At the conclusion of the presentation, the attendees should be able to:• Describe the basic HEp-2 IFA procedure for ANA screening• Identify several solid-phase ANA assays and list the target antigens• List pros and cons of both the HEp-2 IFA and solid-phase ANA
4/8/19
2
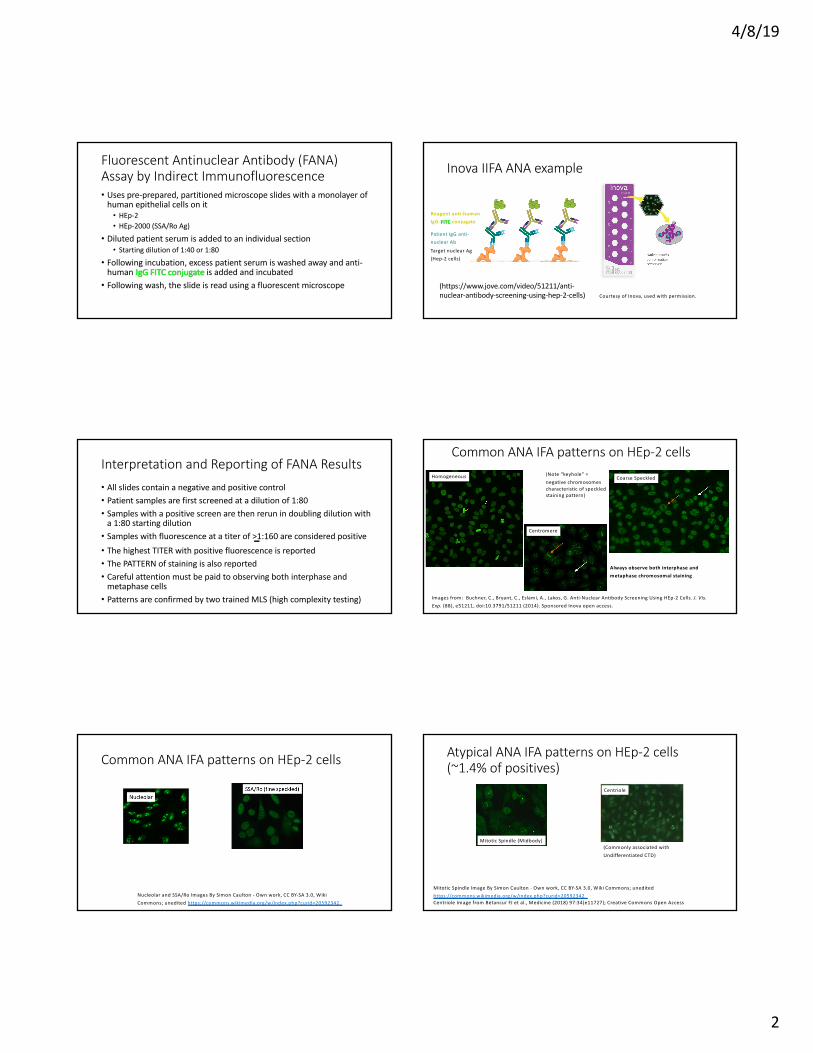
Fluorescent Antinuclear Antibody (FANA) Assay by Indirect Immunofluorescence• Uses pre-prepared, partitioned microscope slides with a monolayer of
human epithelial cells on it• HEp-2• HEp-2000 (SSA/Ro Ag)
• Diluted patient serum is added to an individual section• Starting dilution of 1:40 or 1:80
• Following incubation, excess patient serum is washed away and anti-human IgG FITC conjugate is added and incubated• Following wash, the slide is read using a fluorescent microscope
Inova IIFA ANA example
Courtesy of Inova, used with permission.
Target nuclear Ag(Hep-2 cells)
Patient IgG anti-nuclear Ab
Reagent anti-human IgG-FITC conjugate
(https://www.jove.com/video/51211/anti-nuclear-antibody-screening-using-hep-2-cells)
Interpretation and Reporting of FANA Results• All slides contain a negative and positive control• Patient samples are first screened at a dilution of 1:80• Samples with a positive screen are then rerun in doubling dilution with
a 1:80 starting dilution• Samples with fluorescence at a titer of >1:160 are considered positive• The highest TITER with positive fluorescence is reported• The PATTERN of staining is also reported• Careful attention must be paid to observing both interphase and
metaphase cells• Patterns are confirmed by two trained MLS (high complexity testing)
Common ANA IFA patterns on HEp-2 cells
Images from: Buchner, C., Bryant, C., Eslami, A., Lakos, G. Anti-Nuclear Antibody Screening Using HEp-2 Cells. J. Vis. Exp. (88), e51211, doi:10.3791/51211 (2014). Sponsored Inova open access.
Centromere
(Note “keyhole” = negative chromosomes characteristic of speckled staining pattern)
Homogeneous Coarse Speckled
Always observe both interphase and metaphase chromosomal staining
Common ANA IFA patterns on HEp-2 cells
Nucleolar and SSA/Ro Images By Simon Caulton - Own work, CC BY-SA 3.0, Wiki Commons; unedited https://commons.wikimedia.org/w/index.php?curid=20592342
Atypical ANA IFA patterns on HEp-2 cells (~1.4% of positives)
Mitotic Spindle (Midbody)
Mitotic Spindle Image By Simon Caulton - Own work, CC BY-SA 3.0, Wiki Commons; unedited https://commons.wikimedia.org/w/index.php?curid=20592342Centriole Image from Betancur FJ et al., Medicine (2018) 97:34(e11727); Creative Commons Open Access
Centriole
(Commonly associated with Undifferentiated CTD)
4/8/19
3
Patients with a positive FANA need further testing• FANA testing for most systemic autoimmune rheumatic diseases is quite
sensitive [Arch Pathol Lab Med 2000;124:71]• SLE: 95-100% ANA positive• Scleroderma: 60-80% ANA positive• Drug-induced lupus: ~100%• Autoimmune hepatic disease: ~100%• Mixed connective tissue disease: ~100%
• But, not specific• Italy = 6.1% of population is *positive (ages 43+/-13) [Autoimmunity Rev
2016;15:162]• United States = 5% of “normal persons” are *positive [Arch Pathol Lab Med
2000;124:71]
*>1:160 titer
Patients with a positive FANA need further testing• ANA may be positive in patients with the following autoimmune
inflammatory diseases, but it is not considered useful in diagnosis • Rheumatoid arthritis 30-50%• Multiple sclerosis 25%• ITP 10-30%• Thyroid disease 30-50%• Fibromyalgia 15-25%
[Arch Pathol Lab Med 2000;124:71]
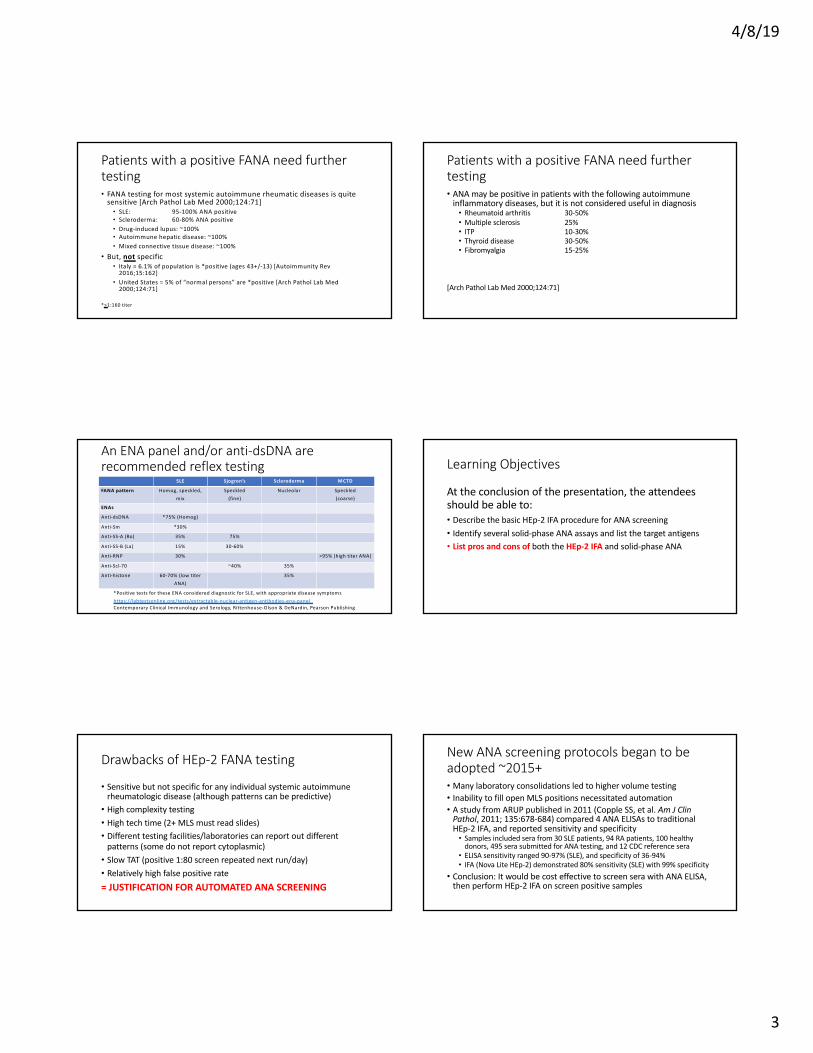
An ENA panel and/or anti-dsDNA are recommended reflex testing
SLE Sjogren’s Scleroderma MCTD
FANA pattern Homog, speckled,
mix
Speckled
(fine)
Nucleolar Speckled
(coarse)
ENAs
Anti-dsDNA *75% (Homog)
Anti-Sm *30%
Anti-SS-A (Ro) 35% 75%
Anti-SS-B (La) 15% 30-60%
Anti-RNP 30% >95% (high titer ANA)
Anti-Scl-70 ~40% 35%
Anti-histone 60-70% (low titer
ANA)
35%
*Positive tests for these ENA considered diagnostic for SLE, with appropriate disease symptoms
https://labtestsonline.org/tests/extractable-nuclear-antigen-antibodies-ena-panelContemporary Clinical Immunology and Serology, Rittenhouse-Olson & DeNardin, Pearson Publishing
Learning Objectives
At the conclusion of the presentation, the attendees should be able to:• Describe the basic HEp-2 IFA procedure for ANA screening• Identify several solid-phase ANA assays and list the target antigens• List pros and cons of both the HEp-2 IFA and solid-phase ANA
Drawbacks of HEp-2 FANA testing
• Sensitive but not specific for any individual systemic autoimmune rheumatologic disease (although patterns can be predictive)• High complexity testing• High tech time (2+ MLS must read slides)• Different testing facilities/laboratories can report out different
patterns (some do not report cytoplasmic)• Slow TAT (positive 1:80 screen repeated next run/day)• Relatively high false positive rate= JUSTIFICATION FOR AUTOMATED ANA SCREENING
New ANA screening protocols began to be adopted ~2015+• Many laboratory consolidations led to higher volume testing• Inability to fill open MLS positions necessitated automation• A study from ARUP published in 2011 (Copple SS, et al. Am J Clin
Pathol, 2011; 135:678-684) compared 4 ANA ELISAs to traditional HEp-2 IFA, and reported sensitivity and specificity• Samples included sera from 30 SLE patients, 94 RA patients, 100 healthy
donors, 495 sera submitted for ANA testing, and 12 CDC reference sera• ELISA sensitivity ranged 90-97% (SLE), and specificity of 36-94%• IFA (Nova Lite HEp-2) demonstrated 80% sensitivity (SLE) with 99% specificity
• Conclusion: It would be cost effective to screen sera with ANA ELISA, then perform HEp-2 IFA on screen positive samples
4/8/19
4
Learning Objectives
At the conclusion of the presentation, the attendees should be able to:• Describe the basic Hep-2 IFA procedure for ANA screening• Identify several solid-phase ANA assays and list the target antigens• List pros and cons of both the Hep-2 IFA and solid-phase ANA
Introduction to Solid-Phase ANA screens
• Solid-phase assays for ANA have employed a variety of test antigens, from lysates of HEp-2 cells to mixtures of multiple extracted and/or recombinant nuclear antigen targets• Solid-phase assays utilize a variety of formats:• Enzyme immunoassay (EIA/ELISA)• Chemiluminescent immunoassay (CIA)• Fluoroenzyme immunoassay (FEIA)• Dot-blot immunoassay• Line immunoassay (LIA; ~Western blot)• Multiplex bead assay
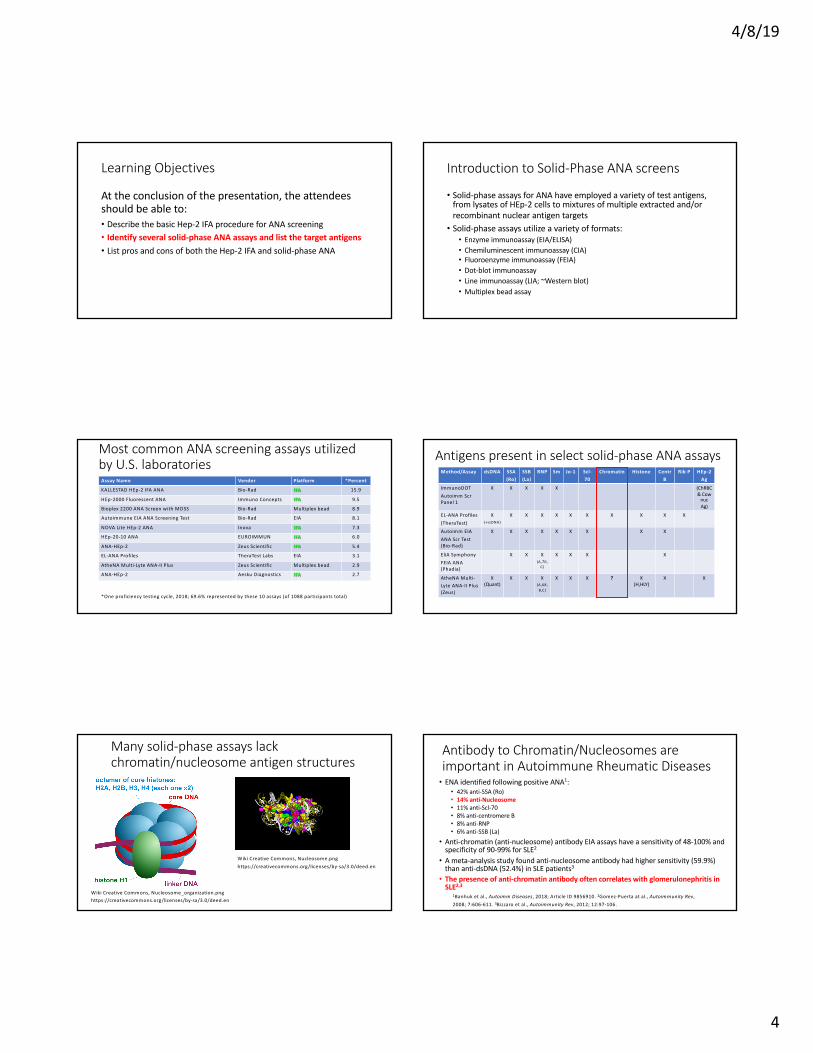
Most common ANA screening assays utilized by U.S. laboratories
Assay Name Vendor Platform *Percent
KALLESTAD HEp-2 IFA ANA Bio-Rad IFA 15.9
HEp-2000 Fluorescent ANA Immuno Concepts IFA 9.5
Bioplex 2200 ANA Screen with MDSS Bio-Rad Multiplex bead 8.9
Autoimmune EIA ANA Screening Test Bio-Rad EIA 8.1
NOVA Lite HEp-2 ANA Inova IFA 7.3
HEp-20-10 ANA EUROIMMUN IFA 6.0
ANA-HEp-2 Zeus Scientific IFA 5.4
EL-ANA Profiles TheraTest Labs EIA 3.1
AtheNA Multi-Lyte ANA-II Plus Zeus Scientific Multiplex bead 2.9
ANA-HEp-2 Aesku Diagnostics IFA 2.7
*One proficiency testing cycle, 2018; 69.6% represented by these 10 assays (of 1088 participants total)
Antigens present in select solid-phase ANA assaysMethod/Assay dsDNA SSA
(Ro)SSB(La)
RNP Sm Jo-1 Scl-70
Chromatin Histone CentrB
Rib P HEp-2 Ag
ImmunoDOT
Autoimm ScrPanel 1
X X X X X (ChRBC& Cow
nucAg)
EL-ANA Profiles
(TheraTest)
X (+ssDNA)
X X X X X X X X X X
Autoimm EIA
ANA Scr Test(Bio-Rad)
X X X X X X X X X
EliA Symphony
FEIA ANA(Phadia)
X X X (A,70,
C)
X X X X
AtheNA Multi-
Lyte ANA-II Plus(Zeus)
X (Quant)
X X X(A,68,
B,C)
X X X ? X(H,HLY)
X X
Many solid-phase assays lack chromatin/nucleosome antigen structures
Wiki Creative Commons, Nucleosome.png https://creativecommons.org/licenses/by-sa/3.0/deed.en
Wiki Creative Commons, Nucleosome_organization.png https://creativecommons.org/licenses/by-sa/3.0/deed.en
Antibody to Chromatin/Nucleosomes are important in Autoimmune Rheumatic Diseases• ENA identified following positive ANA1:
• 42% anti-SSA (Ro)• 14% anti-Nucleosome• 11% anti-Scl-70• 8% anti-centromere B• 8% anti-RNP• 6% anti-SSB (La)
• Anti-chromatin (anti-nucleosome) antibody EIA assays have a sensitivity of 48-100% and specificity of 90-99% for SLE2
• A meta-analysis study found anti-nucleosome antibody had higher sensitivity (59.9%) than anti-dsDNA (52.4%) in SLE patients3
• The presence of anti-chromatin antibody often correlates with glomerulonephritis in SLE2,3
1Banhuk et al., Autoimm Diseases, 2018; Article ID 9856910. 2Gomez-Puerta at al., Autoimmunity Rev,
2008; 7:606-611. 3Bizzaro et al., Autoimmunity Rev, 2012; 12:97-106.
4/8/19
5
Even the form of chromatin/nucleosome utilized in ANA testing matters• The meta-analysis also compared anti-nucleosome assays which used
either native nucleosomes or nucleosomes with histone H1 removed1
• They found comparable sensitivity of 59% and 61%, respectively for SLE• H1-stripped nucleosomes had much better specificity (95.7%) than whole
nucleosomes (87.5%) for SLE
• In a comparison of line-immunoassays for ANA, investigators also found no correlation in positive vs negative results for two assays detecting anti-nucleosome and anti-histone antibody, again suggesting that the preparation method used for antigen is critical2
1Bizzaro et al., Autoimmunity Rev, 2012; 12:97-106. 2Yi, A et al., Clin Biochem , 2018; 55:75-79.
Comparison studies between FANA (IIFA) and solid-phase assays for ANA testing• Claessen et al. found differences in sensitivity & specificity between
HEp-2 IFA, FEIA, and CIA (Autoimmun Rev 2018; 17:533-540)
• Sensitivity was disease specific as well, since both the FEIA and CIA were more sensitive than IIFA in the case of Sjogren’s syndrome (HEp-2 are insensitive for anti-SSA/Ro)
Assay/Manufacturer Sensitivity Specificity
Nova Lite HEp-2, Inova Diagnostics 95% 61%
EliA CTD Screen, FEIA, Thermo Fisher 80.5% 97.5%
QUANTA Flash CTD Screen Plus, CIA, Inova Diagnostics 86% 88%
Comparison studies between FANA (IIFA) and solid-phase assays for ANA testing
• One study followed 411 subjects with a positive BioPlex ANA (multiplex) screen who were negative by IIFA HEp-2 assay (Perez et al., Clin Chem Lab Med 2018; 56:1771-1777)• At 3 years follow-up, 76% were positive by IIFA and 87% had an autoimmune
diagnosis, suggesting the multiplex assay had greater sensitivity and earlier detection of autoimmunity
• Perez et al. also noted that ELISA, FEIA and LIA had only moderate sensitivity for ANA detection compared to IIFA, while they had high specificity compared to the low specificity of IIFA (Autoimmun Rev 2018; 17:548-552)
Comparison studies between FANA (IIFA) and solid-phase assays for ANA testing• These three previous articles came to the same general conclusion:
The best practice for the greatest sensitivity of autoimmune disease would be to perform BOTH HEp-2 IFA and a solid-phase assay for ANA screening
2018 Annals of Rheumatic DiseasesDavid Pisetsky and colleague published a concise report detailing variability in ANA assay results when three IFA assays,
an ELISA and a multiplex microbead assay were used for testing
sera from SLE patients
- especially noting that ~10 % were negative in each assay
Let the Controversy Begin! Pisetsky et al. concern was on clinical trial inclusion, which requires a positive ANA• They found 10% of established SLE patients had a NEGATIVE ANA,
which would exclude them from SLE clinical trials• But, what does this mean for screening/diagnosis of SLE and other
systemic autoimmune rheumatic diseases???• If a patient tests negative in an ANA screening test, autoimmune
disease, especially SLE, is generally ruled OUT
4/8/19
6
The eight letters to the editor in reply to Pisetskyet al. exposed somewhat of an ANA dirty secret• All agreed that there was great variability in ANA assays, not only
between platforms, but also within platforms (including HEp-2 IFA)• One demonstrated none, minimal or weak agreement in 3 ANA Line
Immunoassays compared to IFA in detection of dsDNA, SSA/Ro, SSB/La, Sm and RNP (Ann Rheum Dis 2018; article 214693)• Two questioned pattern reporting of HEp-2 IFA, especially the lack of
consensus on reporting cytoplasmic staining (Ann Rheum Dis 2018; articles 213374 & 214615)• Another provided data on automated IFA reader systems,
demonstrating unacceptable light intensity variability within and between instruments used to test the same sample in 21 different laboratory facilities (Ann Rheum Dis 2018; article 213543)
The eight letters to the editor in reply to Pisetskyet al. exposed somewhat of an ANA dirty secret• Four of the eight concluded that the BEST PRACTICE for ANA
screening would be to perform BOTH HEp-2 IFA and a solid-phase assay (Ann Rheum Dis 2018; articles 213440,213516,213821,214805)
Learning Objectives
At the conclusion of the presentation, the attendees should be able to:• Describe the basic HEp-2 IFA procedure for ANA screening• Identify several solid-phase ANA assays and list the target antigens• List pros and cons of both the HEp-2 IFA and solid-phase ANA
Conclusions: Pros and Cons of HEp-2 IFA and ANA solid phase assays• HEp-2 IFA has higher sensitivity (80-90%) for all systemic autoimmune
rheumatic diseases (up to 100 target Ag), but virtually zero specificity• HEp-2 IFA has low sensitivity for Sjogren’s syndrome (SSA in HEp-2000
corrects this problem)• Solid phase ANA assays have a limited number of target antigens, and
miss complex antigens such as nucleosomes/chromatin• Problematic for SLE patients with low titer ANA, anti-chromatin antibody and
nephropathy• Solid phase ANA assays will likely never detect rare targets• There is no consensus on solid phase ANA target antigen preparation
Conclusions: Best practices recommendation
• If your lab uses solid phase ANA screen followed by HEp-2 IFA if positive, consider:• Running BOTH HEp-2 IFA and solid phase assay in parallel, or• Add an anti-chromatin EIA assay to the solid phase ANA screen
Questions?



![arXiv:2010.04386v1 [hep-ph] 9 Oct 2020](https://img.dokumen.tips/doc/110x75/63289409e491bcb36c0bd402/arxiv201004386v1-hep-ph-9-oct-2020.jpg)






![arXiv:1203.1488v2 [hep-ph] 20 Apr 2012](https://img.dokumen.tips/doc/110x75/633880c3c5ddac3e970cf87b/arxiv12031488v2-hep-ph-20-apr-2012.jpg)
![arXiv:2203.09099v1 [hep-th] 17 Mar 2022](https://img.dokumen.tips/doc/110x75/633170e05696ca447302c095/arxiv220309099v1-hep-th-17-mar-2022.jpg)

![arXiv:2104.07634v1 [hep-ex] 15 Apr 2021](https://img.dokumen.tips/doc/110x75/63389ed1c8bee53b0e04d055/arxiv210407634v1-hep-ex-15-apr-2021.jpg)
![arXiv:1506.01399v4 [hep-ph] 6 Jun 2017](https://img.dokumen.tips/doc/110x75/63295916bfbc0e6324091208/arxiv150601399v4-hep-ph-6-jun-2017.jpg)


![arXiv:2206.11881v1 [hep-ph] 23 Jun 2022](https://img.dokumen.tips/doc/110x75/633525043108fad7760fd68e/arxiv220611881v1-hep-ph-23-jun-2022.jpg)
![arXiv:1802.05857v1 [hep-ph] 16 Feb 2018](https://img.dokumen.tips/doc/110x75/6328acc1051fac18490ed78d/arxiv180205857v1-hep-ph-16-feb-2018.jpg)
![arXiv:1705.10620v2 [hep-ph] 4 Feb 2019](https://img.dokumen.tips/doc/110x75/633c8f3d585a97cd4b07a348/arxiv170510620v2-hep-ph-4-feb-2019.jpg)
![arXiv:1602.03560v2 [hep-lat] 19 May 2016](https://img.dokumen.tips/doc/110x75/63294038eedc98f54f011b01/arxiv160203560v2-hep-lat-19-may-2016.jpg)

![arXiv:2203.01246v2 [hep-ph] 18 Jun 2022](https://img.dokumen.tips/doc/110x75/633dc4a08bbded2b20035e60/arxiv220301246v2-hep-ph-18-jun-2022.jpg)

![arXiv:1112.4538v1 [hep-th] 20 Dec 2011](https://img.dokumen.tips/doc/110x75/63286d285c2c3bbfa804a6bb/arxiv11124538v1-hep-th-20-dec-2011.jpg)
![arXiv:2102.12943v2 [hep-th] 24 Mar 2021](https://img.dokumen.tips/doc/110x75/6323718fb104cba27a08b1e9/arxiv210212943v2-hep-th-24-mar-2021.jpg)

![arXiv:2006.04822v2 [hep-ph] 13 Nov 2020](https://img.dokumen.tips/doc/110x75/6328f02acedd78c2b50e4d71/arxiv200604822v2-hep-ph-13-nov-2020.jpg)
![arXiv:1907.08002v5 [hep-ex] 28 Jan 2020](https://img.dokumen.tips/doc/110x75/6328a9ed051fac18490ed620/arxiv190708002v5-hep-ex-28-jan-2020.jpg)
