Embed Size (px)
Citation preview
Alternating Chemoradiotherapy versus PartlyAccelerated Radiotherapy in Locally AdvancedSquamous Cell Carcinoma of the Head and NeckResults from a Phase III Randomized Trial
Renzo Corvo, M.D.1
Marco Benasso, M.D.2
Giuseppe Sanguineti, M.D.1
Rita Lionetto, M.D.3
Almalina Bacigalupo, M.D.1
Giovanni Margarino, M.D.4
Eugenio Pallestrini, M.D.5
Marco Merlano, M.D.6
Vito Vitale, M.D.1
Riccardo Rosso, M.D.2
1 Oncologia Radioterapica, National Cancer Re-search Institute, Genoa, Italy.
2 Oncologia Medica, National Cancer Research In-stitute, Genoa, Italy.
3 Epidemiologia Clinica e Studi Clinici Controllati,National Cancer Research Institute, Genoa, Italy.
4 Oncologia Chirurgica, National Cancer ResearchInstitute, Genoa, Italy.
5 Divisione Otorinolaringoiatrica San Martino Hos-pital, Genoa, Italy.
6 Oncologia Medica, Santa Croce General Hospital,Cuneo, Italy.
Presented at the 36th Annual Meeting of AmericanSociety of Clinical Oncology, New Orleans, Louisi-ana, May 19–23, 2000.
Supported by the Consiglio Nazionale delleRicerche-Applicazioni Cliniche della Ricerca Onco-logica, Roma, Italy, Grant 96.00687.PF39.
The following oncologists partcipated in this ran-domized study: Paolo Bruzzi, M.D., Isabella Ricci,M.D., Katia Donato, M.D., Franca Foppiano, Ph.D.(Istituto Nazionale per la Ricerca sul Cancro,Genova); Alida Santelli, M.D., Filippo Borasi, M.D.(Divisione of Otorinolaringoiatria–Ospedale SanMartino, Genova); Enzo Mora, M.D., Marco Bar-bieri, M.D. (Clinica Otorinolaringoiatrica-Universita,Genova); Corrado Marziano, M.D., Renato Chiar-lone, M.D., Fulvio Brema, M.D. (Ospedale S. Paolo,Savona); Giovanni Ricci, M.D., Andrea Grimaldi,
M.D., Monica Cavallari, M.D. (Ospedale Galliera,Genova); Giammauro Numico, M.D. (Ospedale S.Croce e Carle, Cuneo, Italy).
Address for reprints: Renzo Corvo, M.D., U.O. On-cologia Radioterapica, Istituto Nazionale per la
Ricerca sul Cancro, Largo Rosanna Benzi, 16132Genoa, Italy; Fax 39-10-5600039; E-mail:[email protected]
Received June 29, 2001; revision received July 9,2001; accepted August 22, 2001.
BACKGROUND. The authors previously have found that in patients with locally
advanced squamous cell carcinoma of the head and neck (SCC-HN), alternating
chemoradiotherapy (ALT) was superior to low-total-dose conventional radiother-
apy alone. The purpose of this randomized trial was to compare the same chemo-
radiotherapy approach with high-total-dose partly accelerated radiotherapy.
METHODS. During 6 years, 136 consecutive patients with previously untreated unfa-
vorable Stage II or Stage III–IV (International Union Against Cancer) SCC of the oral
cavity, pharynx, and larynx were enrolled. They were randomly assigned to chemo-
therapy consisting of 4 cycles of intravenous cisplatin (20 mg/m2 of body surface area
per day for 5 consecutive days) and 5-fluorouracil (200 mg/m2 per day for 5 consec-
utive days; weeks 1, 4, 7, and 10) alternated with three 2-week courses of radiotherapy
(20 grays [Gy] per course, 2 Gy per day, 5 days per week; ALT, 70 patients) or to partly
accelerated radiotherapy with final concomitant boost technique (75 Gy/40 fractions
in 6 weeks; partly accelerated radiotherapy [PA-RT], 66 patients).
RESULTS. At the median follow-up of 60 months (range, 30 –102 months), no
statistical differences were observed in overall survival, progression free survival, or
locoregional control between the 2 treatments. Actuarial 3-year overall survival and
progression free survival were 37% and 35%, respectively, in the ALT group and
29% and 27%, respectively, in PA-RT group. The median overall survival and
progression free survival were 24 and 15 months, respectively, in the ALT arm and
18 and 11 months, respectively, in PA-RT arm. Actuarial 3-year locoregional control
rates were 32% in the ALT group and 27% in the PA-RT group. At multivariate
analysis, tumor classification was the only factor that emerged as a significant
independent variable affecting overall survival. Patients treated in the PA-RT arm
experienced higher Grade 31 (World Health Organization) acute skin and mucosal
reactions than patients in the ALT arm. Moreover, local late mucosal and skin
toxicities occurred more often in patients treated with PA-RT.
CONCLUSIONS. This trial failed to disclose statistically significant differences in the
outcome of patients treated with either ALT or PA-RT. Therefore, definitive con-
clusions could not be made. However, acute skin effects and late mucosal and skin
toxicities above the clavicles appeared to be significantly lower with chemoradio-
therapy. Cancer 2001;92:2856 – 67. © 2001 American Cancer Society.
KEYWORDS: squamous cell carcinoma, head and neck carcinoma, chemoradiother-apy, accelerated radiotherapy, randomized clinical trial.
2856
© 2001 American Cancer SocietyDOI 10.1002/cncr.10132

Conventional radiotherapy, namely, a daily dose of1.8 or 2 grays (Gy), 5 fractions a week for 7 weeks,
has been used for decades as the standard approach totreatment of patients affected by locally advancedsquamous cell carcinoma of the head and neck (SCC-HN).1 Although technologic and radiobiologic ad-vances recently have improved the quality of radio-therapy delivery, approximately 55– 60% of patientswith late diagnosed SCC-HNs who were not eligiblefor radical surgery experienced locoregional failurewithin the first 2 years of definitive radiotherapy.2
Over the past decade, original unconventionalschedules of radiotherapy3 and new strategies exploit-ing different associations of chemotherapy and radio-therapy4 have been investigated increasingly to over-come or minimize the impact of multiple biologicfactors (clonogen number, hypoxia, inherent radiore-sistance, proliferation) that may led to a high risk oflocoregional failure after conventional radiotherapy.5
So far, however, the optimal treatment for the cure ofadvanced SCC-HNs remains controversial.6 Innova-tive therapies should improve locoregional controland survival avoiding heavy acute and late treatment-related toxicities in an attempt to obtain an actualtherapeutic gain.
Concomitant associations of chemoradiotherapyin the synchronous7–9 or alternating10 setting havebeen demonstrated to be superior to conventionalradiotherapy. A recent meta-analysis of randomizedstudies comparing chemoradiotherapy with conven-tional radiotherapy showed that concomitant associ-ations yield an 8% higher 5-year survival benefit;11
however, improved efficacy with concomitant chemo-radiotherapy is accompanied by increased acute tox-icity that may compromise the treatment delivery ofmost programs. Nevertheless, among various con-comitant approaches alternating chemoradiotherapy10
appeared as the treatment that contributed the leastto acute mucosal toxicity; this compelling evidence isrelated to the original alternated timing of chemother-apy and radiotherapy as well as the low-total-radio-therapy dose elapsed.
Since 1982, the National Institute for Cancer Re-search in Genoa, Italy and affiliated centers have beenconducting randomized trials to select which treat-ment modality may be indicated for SCC-HN patientsnot eligible for radical resection. Alternating chemo-radiotherapy has been largely studied in patients withlocally advanced SCC-HN; in the past years, this ap-proach has appeared to be significantly more effectivethan one-a-day fractionation radiotherapy.10
Conversely, accelerated radiotherapy regimenshave provided SCC-HN patients with better results interms of locoregional control,3,12–15 although unequiv-
ocally.16 The rationale for accelerated fractionation isthat reduction in overall treatment time reduces theopportunity for tumor cell regeneration during treat-ment. Among different regimens, acceleration by de-livering six fractions per week17 or using concomitantboost technique14,18 appeared to improve local tumorcontrol rates without increasing late toxicity.
In this context, we have investigated the role thata partly accelerated radiotherapy (PA-RT) regimenwith the concomitant boost technique19 may play inthe control of patients with advanced SCC-HN. Thisregimen, which is similar to that designed at the M. D.Anderson Cancer Center in Houston,18 favored in ourexperience the achievement of promising results es-pecially in locally extended oropharynx tumors.19
Given the high number of patients with high-riskStage IV (International Union Against Cancer [UICC])SCC-HN treated at our institution, this regimen wasintensified, increasing the dose per fraction (1.8 vs. 2Gy), the total subclinical dose (60 vs. 54 Gy), and thetotal dose to clinical disease (75 vs. 72 Gy).19
With this background, the next step was to com-pare alternating chemoradiotherapy (ALT) with PA-RT. Here, we report the results from a randomizedmulticenter trial conducted to compare the two mo-dalities in patients with locally advanced nonmeta-static SCC-HN.
MATERIALS AND METHODSBetween 1992 and 1998, the National Institute forCancer Research in Genoa, Italy and affiliated centersperformed a randomized trial to investigate the effectsof two different treatment modalities in patients withSCC-HN. Patients were examined by a multidisci-plinary team consisting of an otorhinolaryngologistand radiation and medical oncologists. All the patientsunderwent physical examination including endos-copy, chest X-ray, electrocardiogram, a completeblood count, and computed tomography of the headand neck. The tumor was classified according to thecriteria of the International Union Against Cancer byuse of the 4th edition of the TNM classification ofmalignant tumors.20 Patients were included in thestudy if they had a histologically confirmed squamouscell carcinoma; Stage II (tongue base and hypophar-ynx primary only) and Stage III and IV SCC of oralcavity, pharynx (except undifferentiated nasopharyn-geal carcinoma), and larynx, without evidence of dis-tant metastases; age younger than 75 years; a perfor-mance status score of 2 or lower, according to theEastern Cooperative Oncology Group scale;21 ade-quate liver, kidney, bone marrow, lung, and heartfunction; a life expectancy of 6 months or more; anabsence of other neoplasms (with exception of basal
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2857

cell carcinoma of the skin); and geographic accessibil-ity. Other criteria for inclusion were a neutrophilcount greater than 1500 cells/mm3, a platelet countgreater than 120,000 cells/mm3, a serum creatinineconcentration of 1.4 ng/dL or less, and a serum bili-rubin level less than 1.5 mg/dL.
The protocol was approved by the scientific re-view board and by the ethical committee of the Na-tional Institute for Cancer Research in Genoa.
TreatmentPatients randomly assigned to receive the combinedtherapy (ALT arm A) were treated with alternatingchemotherapy (4 courses during weeks 1, 4, 7, and 10)and radiotherapy (3 courses of 20 Gy each, given infractions of 2 Gy per day, 5 times a week, during weeks2–3, 5– 6, and 8 –9) for a total planned radiation dose of60 Gy.10
Patients assigned to receive PA-RT arm B weretreated with a conventional radiotherapy course con-sisting in 30 fractions of 2 Gy per day, 5 times a weekfor 6 weeks, superimposed with a second course of 1.5Gy, once a day, 5 times a week during the last 2 weeks,which encompassed only the macroscopic disease.The interval time between the two daily fractions wasat least 6 hours. The total planned dose of PA-RT was75 Gy in 40 fractions.19
In arm A, chemotherapy consisted of cisplatin(Platinex; Bristol-Myers, Rome, Italy) at a dose of 20mg/m2 per day and fluorouracil (Fluorouracile; Roche,Milan, Italy) at a dose of 200 mg/m2 per day, bothgiven intravenously for 5 consecutive days. Cisplatinwas given during a 2-hour period of forced hydrata-tion with 2 L of saline containing 6 mEq (mmol) ofpotassium chloride per liter and 2 g of magnesiumsulfate. Fluorouracil was administered as an intrave-nous bolus dose at the end of hydration. Metoclopra-mide and/or 5HT3 antagonists were used as anti-emetic agents. Steroids were added in selected cases.
In both groups, radiation therapy was delivered byuse of cobalt-60 gamma rays or 6-MV photons. Pri-mary tumor and the upper cervical lymph nodes weretreated with two coplanar opposed fields. Customizedblocks were systematically used for each individualpatient. The lower part of the neck and the supracla-vicular lymph nodes were treated by use of a singleanterior field with midline block, when indicated. Allfields were treated at each session in both treatmentarms. The total doses planned to the primary tumorand the involved lymph nodes were 60 Gy in arm Aand 75 Gy in arm B. If there were no palpable lymphnodes in the lower part of the neck or in the spinalarea, the dose was limited to 50 Gy in both arms.
The dose to the spinal cord was kept below 50 Gy
in arm A and 46 –50 Gy in arm B. Electron beams wereused to boost the posterior cervical lymph nodes whennecessary. The second daily concomitant boost dosedelivered in arm B in the fifth and sixth weeks oftreatment was planned by two or more coplanar pho-ton beams or by a proper energy-fixed unilateral elec-tron beam. The spinal cord was always excluded fromthe boost field.22
Evaluation CriteriaIn both arms, response to treatment was assessed 6 – 8weeks after the end of therapy.21 A response to treat-ment was defined as complete if all clinically detect-able malignant disease disappeared for at least 4weeks and no new lesions appeared. A response wasdefined as partial if a sustained reduction greater than50% in total tumor size was observed for at least 4weeks with no evidence of new lesions. Stable diseasewas defined as the absence of a marked change in thesize of measurable lesions (a decrease of , 50% or anincrease of , 25%) with no evidence of new lesions.Progressive disease was defined as an increase ofgreater than 25% in the size of one or all lesionspresent at the start of therapy or the appearance ofnew lesion.
Early discontinuation of treatment included pa-tients who did not ultimate the treatment because ofearly death or progression disease during treatment.Early death defined any death that occurred before theend of the treatment.
Locoregional control, i.e., absence of SCC-HN dis-ease above the clavicles, was considered from twodifferent starting points: 1) complete responsesreached only by therapy; and 2) complete responsesreached by therapy plus pathologic complete re-sponses and partial responses converted completelyby a surgical procedure.
Locoregional control was considered as “main-tained” until a tumor and/or lymph node recurrenceappeared in the irradiated field, regardless the devel-opment of distant metastases or a second primarytumor. Using Kaplan–Meier analysis23 of locoregionalcontrol, we considered all cases without a completeresponse as failures the day after randomization. Pa-tients in complete response who failed distantly wereconsidered censored (not failed) the day before theevidence of the progression.
Progression free survival was computed from thetime of treatment randomization. An event was con-sidered evidence of SCC-HN progression at any site,including the occurrence of distant metastases. Pa-tients with second primary tumors were censored.However, given the uncertainty to differentiate secondprimary tumors from distant metastases when histol-
2858 CANCER December 1, 2001 / Volume 92 / Number 11

ogy and site of event were similar, progression freesurvival also was computed including patients whoexperienced second primary tumors. All accrued pa-tients were analyzed for progression free survival. Pa-tients lost to follow-up were censored at the time ofthe last available observation.
Overall survival was computed from the time oftreatment randomization until the time of the latestfollow-up observation or death. All accrued patientswere included in the analysis by the principle of in-tent-to-treat.
Statistical MethodsPatients were subjected to stratification according tothe study participating institution at which they wererecruited, and then they were randomly assigned toreceive either chemotherapy alternated with radio-therapy or PA-RT alone. A posteriori stratification bydisease stage and other clinical features was plannedin Cox regression analysis. Randomization was per-formed by making a telephone call to a central officethat had responsibility over randomization and datamanagement.
The main purpose of this study was to compareoverall survival in the two treatment groups. Second-ary considerations were the assessment of objectiveresponses frequencies, locoregional control, and pro-gression free survival and treatment-associated toxiceffects in the two groups.
It was estimated that 240 patients would havebeen required for the study, based on a projectedimprovement of 20% in the probability of survival at 3years in the PA-RT group with an alpha error of 5%two-sided and a beta error of 20%.
The response rates of the groups were comparedby use of the chi-square test. Toxic reactions weregraded according to the World Health Organization(WHO) scale21 and Radiation Therapy OncologyGroup/European Organization for Research andTreatment of Cancer (RTOG/EORTC) criteria.24,25 Ac-tuarial locoregional control, progression free survival,and overall survival curves were calculated using theKaplan–Meier method, and the log-rank test was usedto compare cure and survival rates between arm A andarm B.
Cox proportional hazards regression analysis wasused26 to explain overall survival and progression freesurvival as a function of a set of independent variables.All the variables were categoric: tumor classification(T2, T3, T4); age (, 60, . 60 years); site of primarydisease (oral cavity, nasopharynx, hypopharynx, oro-pharynx, and larynx); lymph node classification (N0,N1, N2, N3); performance status (0, 1 1 2); and treat-ment (ALT, PA-RT). All analyses were performed using
a BMDP statistical package.27 Reported P values aretwo-sided if not otherwise indicated.
RESULTSBetween March 1992 and April 1998, 136 patients wereregistered from 6 institutions. Seventy patients wereallocated to combined chemoradiotherapy (arm A)and 66 patients to PA-RT (arm B). One hundred two(75%) patients were enrolled from the promoter center(National Institute for Cancer Research), and the re-maining 34 (25%) patients were from affiliated centers.
Enrollment was stopped before the achievementof the planned number of patients because of lowannual accrual. Given the sample size of 136 patients,the statistical power of the study was, at its closure,57% instead of the planned 80%.
On review, three patients (one in arm A and two inarm B) were found to be ineligible. The reasons forinelegibility were prior surgery in arm A and evidenceof distant metastases at diagnosis and histology differ-ent from SCC in arm B. Only one of the three ineligiblepatients received the treatment assigned (arm B). Ma-jor protocol violations were detected in six patients(three in arm A and three in arm B). Causes of majorprotocol deviations were refusal of chemotherapy (2patients), age older than 75 years (1 patient) in arm A,and refusal to receive the second daily dose of radio-therapy (3 patients) in arm B. The two patients as-signed to arm A who refused chemotherapy weretreated with radiotherapy alone. Three patients (twoin arm A and one in arm B) died after randomizationassigment (sepsis in one patient and heart failure intwo patients) and did not receive any treatment.
As shown in Table 1, the two treatment groupswere balanced except for a slightly higher proportionof patients with Stage III (UICC 1992) in arm A and aslightly higher proportion of patients with nasopha-ryngeal tumors in arm B. The numbers of cases evalu-able for different end points are summarized in trialprofile shown in Table 2.
Early Discontinuation of TreatmentTreatment delivery was discontinued in 18 patients: in10 of 70 (14%) in arm A and in 8 of 66 (12%) in arm B.Causes of discontinuation of treatment were the fol-lowing: progressive disease (five patients and threepatients in arm A and B, respectively) and early death(five patients in both arms); causes of early death werecardiovascular failure (two patients), sepsis (two pa-tients), and intracerebral hemorrhage (1 patient) inarm A and intercurrent pneumonitis (1 patient), kid-ney failure (1 patient), sepsis (2 patients), and myo-cardial infarction (1 patient) in arm B.
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2859
Compliance to the TreatmentAs shown in Table 3, the median total dose of radi-ation was 60 and 75 Gy in arm A and arm B, respec-tively. The median overall treatment time of radio-therapy was 56 days (range, 54 –94 days) and 42 days(range, 40 –58 days) in arm A and arm B, respec-tively.
Among the 70 patients treated in arm A, the
median number of chemotherapy cycles was 4(range, 1– 4). In detail, 38 (54%) patients received 4cycles, 17 (24%) patients received 3 cycles, 6 (9%)patients received 2 cycles, and 5 (7%) patients re-ceived 1 cycle. Four (6%) patients did not receivechemotherapy at all (2 patients because of deathafter randomization and 2 for refusal). For 61 pa-tients in arm A who received at least 2 courses ofchemotherapy, we investigated the relative dose in-tensity (RDI). The RDI is the ratio between theplanned dose and the actual delivered intensity. Thedose intensity is expressed as the average dose perweek (mg/m2 per week) in the course of treatment.The analysis showed that the median RDI was 87%:greater than 80% in 43 (70%) patients and less than80% in 18 (30%) patients.
TABLE 1Patients and Tumor Characteristics
Characteristic
No. of patients (%)
Combined therapy(n 5 70) (%)
Radiotherapy(n 5 66) (%)
GenderMale 61 (87) 60 (91)Female 9 (13) 6 (9)
Age (yrs)# 60 38 (54) 36 (54). 60 32 (46) 30 (46)
Performance status (ECOG)0 32 (46) 23 (35)1 38 (54) 40 (61)2 — 3 (4)
Site of primary tumorNasopharynx 4 (6) 8 (12)Oropharynx 28 (40) 24 (36)Oral cavity 14 (20) 12 (18)Larynx 10 (14) 7 (11)Hypopharynx 14 (20) 15 (23)
Clinical stageII 1 (1) 3 (4)III 13 (19) 7 (11)IV 56 (80) 56 (85)
Stage IIT2 N0 1 (1.4) 3 (4)
Stage IIIT2 N1 3 (4.2) —T3 N0 7 (10) 4 (1.5)T3 N1 3 (4.2) 2 (3)
Stage IVT1 N2 1 (1.4) 1 (1.5)T1 N3 2 (3) —T2 N2 6 (8.5) 5 (7.5)T2 N3 1 (1.4) —T3 N1 — 2 (3)T3 N2 5 (7) 9 (13.6)T3 N3 1 (1.4) 3 (4.5)T4 N0 8 (11.4) 12 (18)T4 N1 6 (8.6) 4 (6)T4 N2 20 (28.5) 18 (27.2)T4 N3 6 (8.5) 3 (4.5)
GradingG1 11 (16) 14 (21)G2 25 (36) 20 (31)G3 16 (23) 20 (31)Gx 18 (26) 12 (17)
ECOG: Eastern Cooperative Oncology Group.
TABLE 2Trial Profile for End Points
End point
Randomization (136 patients)
Arm Achemoradiotherapy(70 patients)
Arm Bradiotherapy(66 patients)
Evaluable for response/OS/PFS/LRC 70 66Acute Toxicity
Evaluable 63 64Not evaluableInelegibility 1 1Death before treatment 2 1Death within 2 weeks of treatment 4 0
Long-term toxicityEvaluable 20 12
OS: overall survival; PFS: progression free survival; LRC: locoregional control.
TABLE 3Doses and Overall Treatment Times of Radiotherapya
DoseCombined treatmentALT arm (n 5 58) (%)
Radiotherapy PA-RTarm (n 5 57) (%)
Radiotherapy dose medianGy (range) 60 Gy (58–70) 75 Gy (73–75)
60 Gy 51 patients (88) 75 Gy 52 patients (91). 60 Gy 5 patients (9), 60 Gy 2 patients (3) , 75 Gy 5 patients (9)
Temporary interruptionduring treatment(wks)
None 43 patients (74) 48 patients (84)1 5 patients (9) 7 patients (12)2 6 patients (10) 2 patients (4). 2 4 patients (7) —
a From this analysis 21 patients (12 in arm ALT and 9 in arm PA-RT) were excluded who either never
started treatment (n 5 3) or discontinued the treatment early (n 5 18).
2860 CANCER December 1, 2001 / Volume 92 / Number 11
Response EvaluationAnalysis of patient response showed that the fre-quency of treatment failure was unaffected by the typeof treatment with 27% (19 of 70) of the patients in armA and 24% (16 of 66) of patients in arm B. Conse-quently, the overall response rates were similar: 51 of70 patients (73% with 95% confidence interval [CI],61– 82%) for arm A and 50 of 66 patients (76% with95% CI, 63– 85%) for arm B (Table 4).
Patients treated with the combined treatment ex-perienced a trend for an increased frequency of com-plete response for patients treated with radiotherapyalone: 36 of 70 patients (51% with 95% CI, 39 – 63%) forarm A and 26 of 66 patients (39% with 95% CI, 28 –52%) for arm B (P 5 0.1; see Table 4); in both arms, allpatients with residual disease 6 – 8 weeks after com-pletion of treatment were considered for surgical re-section: 24 partial responders (7 in arm A and 17 inarm B) were not amenable to surgery because of un-resectable residual disease (4 in arm A and 10 in armB), poor clinical condition (3 in arm A and 4 in arm B),or refusal (3 in arm B). Thus, 8 (53%) partial respond-ers in arm A (2 on primary site and 6 on lymph nodesite) and 7 (29%) partial responders in arm B (3 bothon primary and lymph node site and 4 on lymph nodesite only) underwent surgery; major surgery was per-formed on primary tumors in 3 patients, 1 in arm Aand 2 in arm B; neck dissections were performed in 13patients (6 in arm A and 7 in arm B).
After surgery, in arm A 3 (37%) partial responderson tumor site (one patient) or lymph site (2 patients)showed no viable tumor (pathologic complete re-sponse) whereas 4 (50%) became free of tumor (con-verted complete response); in arm B, all the 7 (100%)
partial responders were, instead, converted to com-plete response after surgery.
Therefore, with surgery taken into account, theultimate complete response frequencies were 61% (43of the 70 patients; 95% CI, 48 –71%) in arm A and 50%(33 of the 66 patients; 95% CI, 36 – 61%) in arm B (P5 0.23).
No major treatment-related surgical complicationwas recorded.
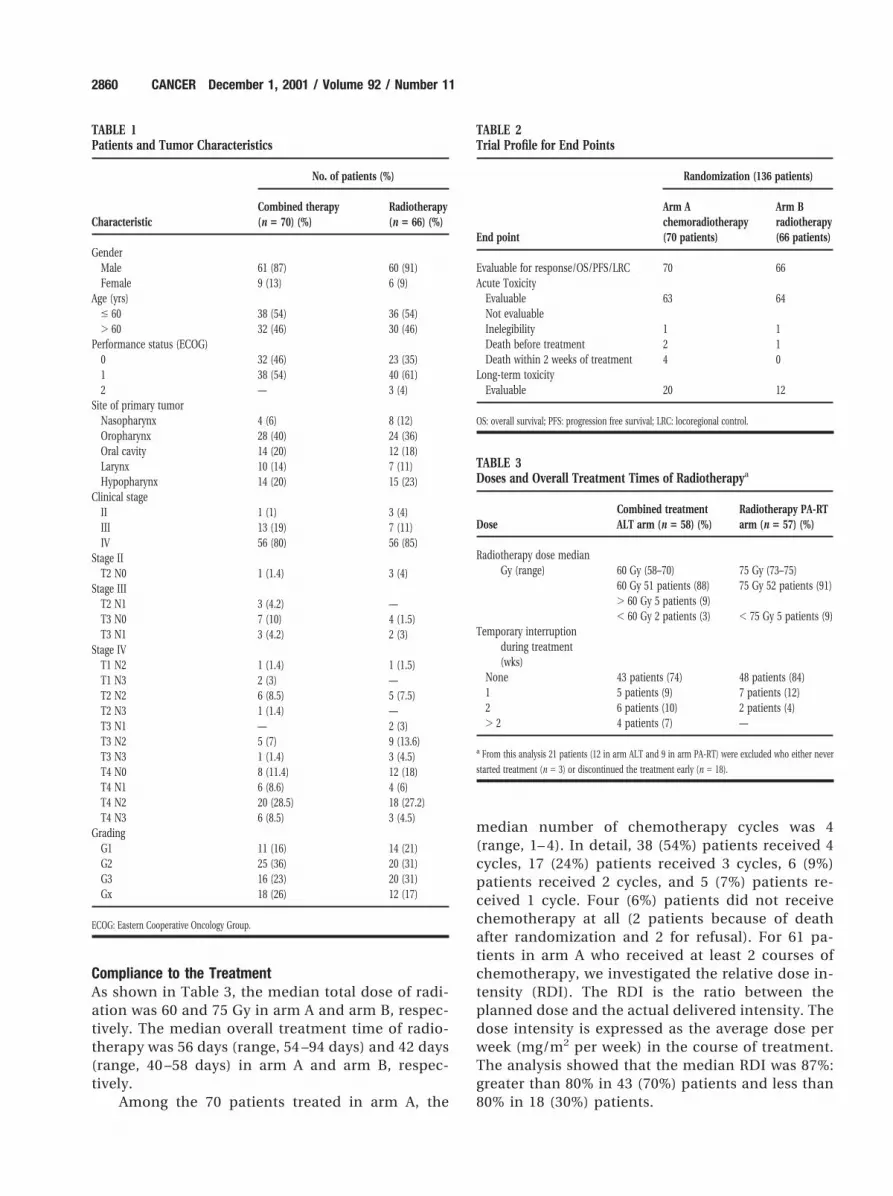
SurvivalAfter a median follow-up of 60 months (range, 30 –102months), 93 patients had died, 43 of 70 (61%) in thecombined treatment arm and 50 of 66 (75%) in theradiotherapy alone arm. Seventy-two (77%) patients(34 in arm A and 38 in arm B) died because of tumorprogression, whereas 21 (23%) patients, 9 in arm A and12 in arm B, died of other causes. The median survivalwas 24 months in the chemoradiotherapy group and19 months in the radiotherapy alone group.
The 3-year overall survival rates were 37% (95%CI, 33– 41%) for the combined treatment group and29% (95% CI, 26 –32%) for the radiotherapy alonegroup (P 5 0.2; Fig. 1).
Progression Free SurvivalSeventy-three (54%) patients, 35 of 70 (50%) in arm Aand 38 of 66 (57%) in arm B, progressed after treat-ment. Among the 35 patients who experienced failureafter chemoradiotherapy, the unique/concomitantsite of progression was locoregional in 28 (80%) pa-tients and distant metastases in 7 (20%) patients.Among the 38 patients who experienced failure afterradiotherapy alone, the unique/concomitant site ofprogression was locoregional in 30 (79%) patients anddistant metastases in 8 (21%) patients.
TABLE 4Response to Treatment
Response
No. of patients (%)
Combined therapy(n 5 70) Radiotherapy (n 5 66)
Complete 36 (51) 26 (39)Partial 15 (21) 24 (36)Overall 51 (73) (95% CI, 61–82) 50 (76) (95% CI, 63–85)Treatment failures 19 (27) 16 (24)
Stable disease 3 (4) 2 (3)Disease progression 5 (7) 3 (5)Never started 2 (3) 1 (1)Early death 5 (7) 5 (8)Inelegibility 1 (1) 2 (3)Major protocol violation 3 (4) 3 (5)
CI: confidence interval.
FIGURE 1. Overall survival among patients with squamous cell carcinoma of
the head and neck treated with chemoradiotherapy (ALT) or partly accelerated
radiotherapy (PA-RT).
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2861
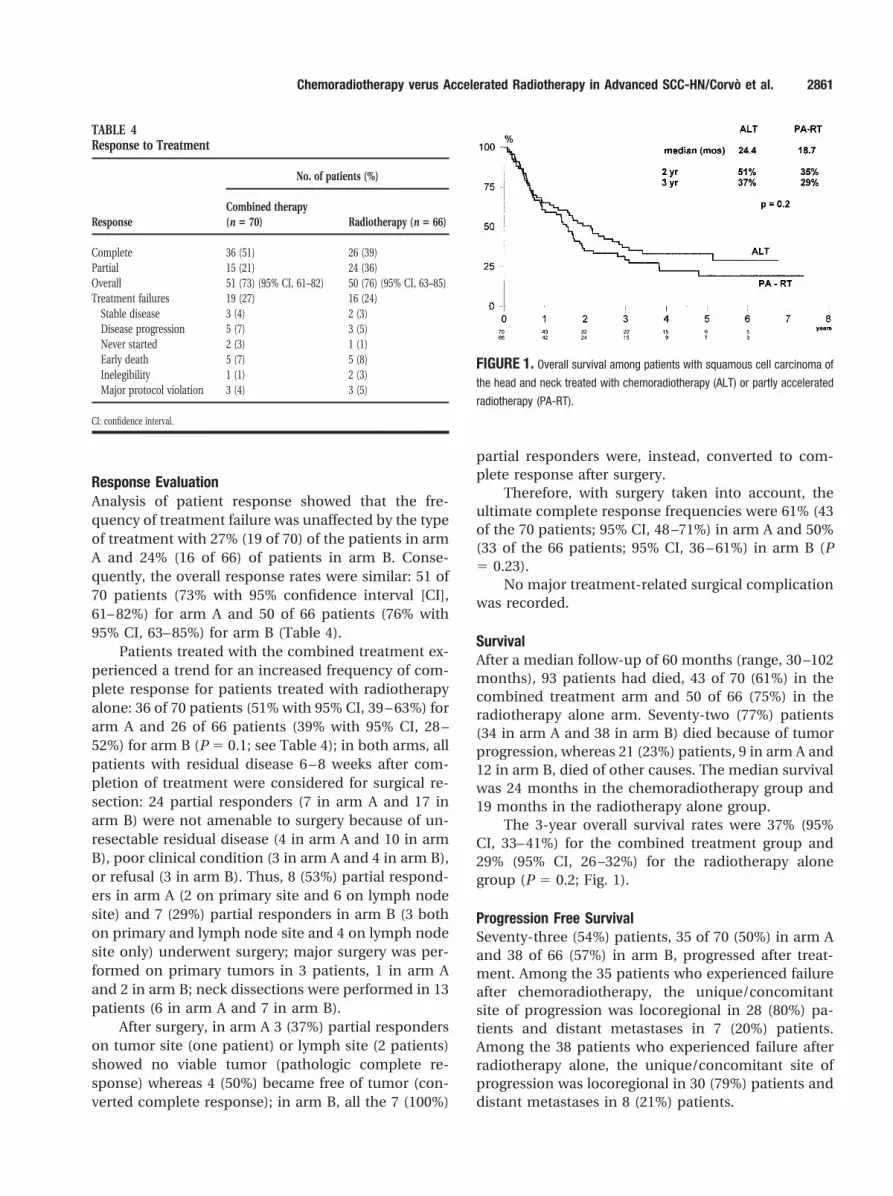
The 3-year progression free survival was esti-mated to be 35% (95% CI, 31–39%) for the patients inarm A and 27% (95% CI, 24 –30%) for patients in arm B(P 5 0.4; Fig. 2). The median progression free survivalwas 15 months in the chemoradiotherapy group and11 months in the radiotherapy group. The 3-year pro-gression free survival computed including patientswho showed second primary tumors was 34% (95% CI,31–38%) for the patients in arm A and 25% (95% CI,22–28%) for those in arm B (P 5 0.2).
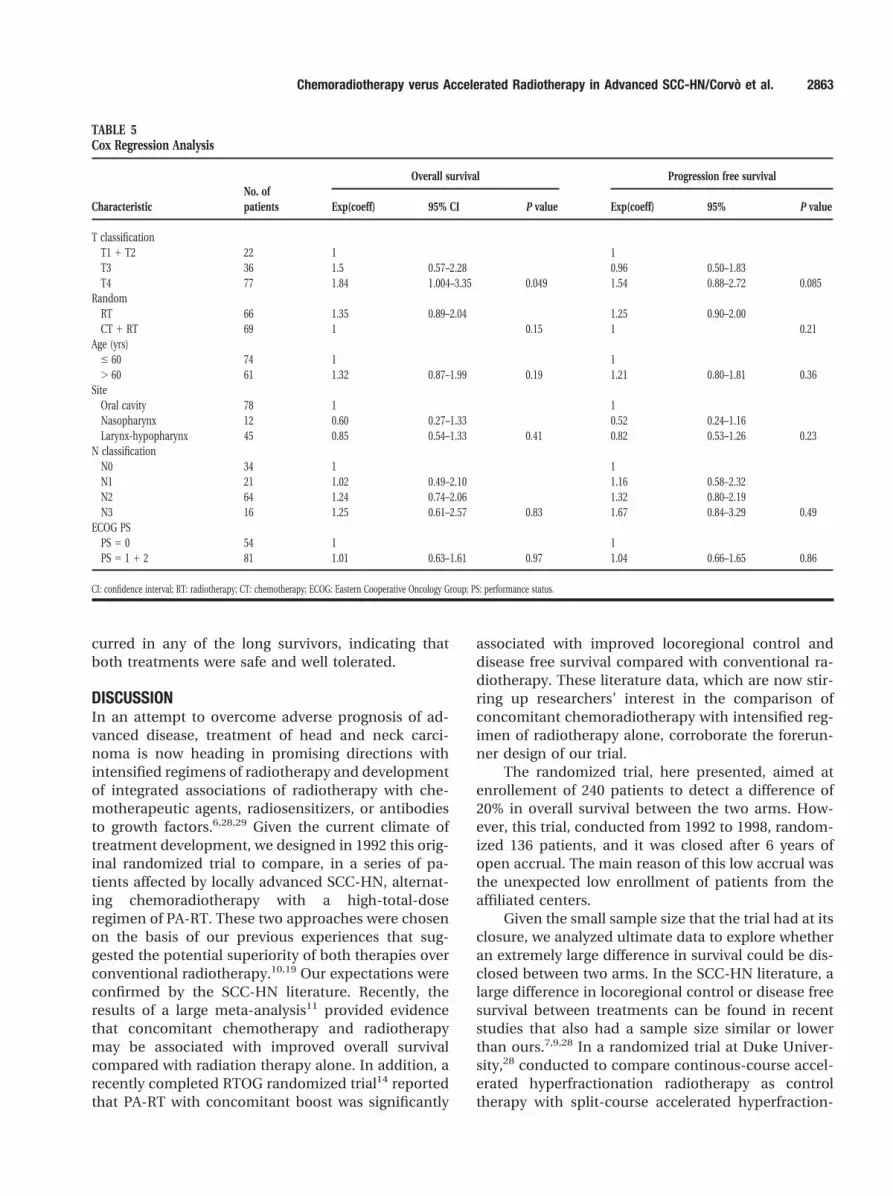
Cox Regression AnalysisAs shown in Table 5, tumor classification was the onlyfactor that emerged as a significantly independentvariable (P 5 0.05) affecting overall survival.
Age older than 60 years and PA-RT showed a trendfor an increased risk of dying whereas tumor classifi-cation marginally affected the risk of having progres-sion disease.
Locoregional ControlAmong the 36 patients in arm A and 26 patients inarm B with complete response at the end of treat-ment, locoregional control was mantained in 42 pa-tients, 22 patients (61%) in arm A and 20 patients(77%) in arm B.
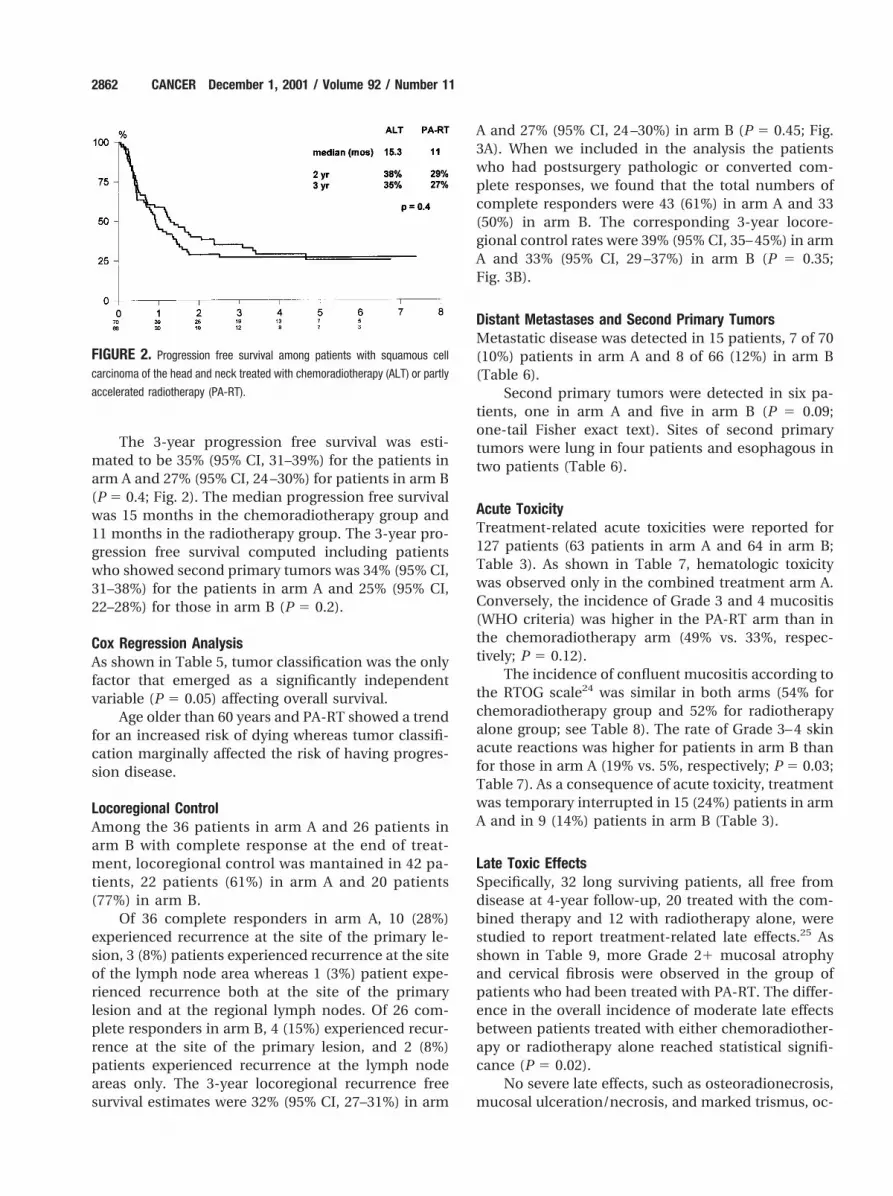
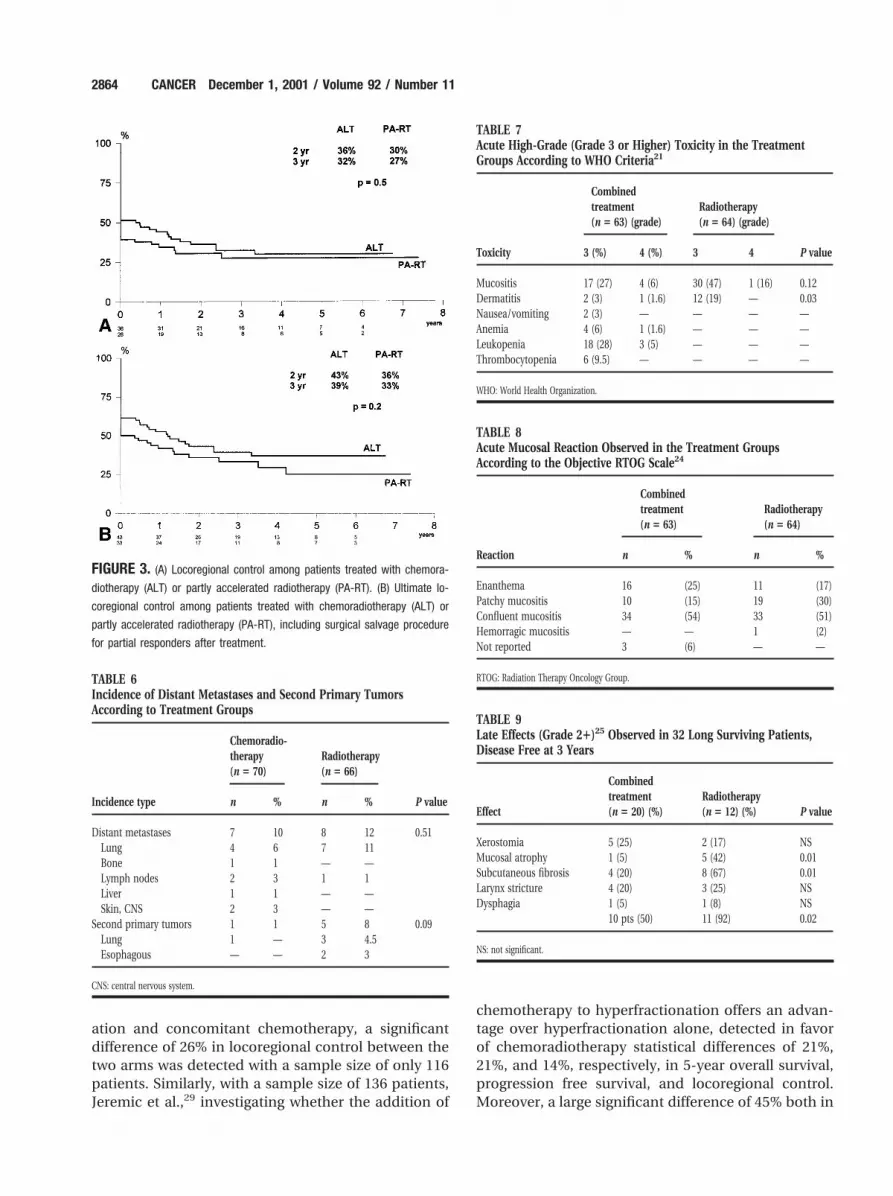
Of 36 complete responders in arm A, 10 (28%)experienced recurrence at the site of the primary le-sion, 3 (8%) patients experienced recurrence at the siteof the lymph node area whereas 1 (3%) patient expe-rienced recurrence both at the site of the primarylesion and at the regional lymph nodes. Of 26 com-plete responders in arm B, 4 (15%) experienced recur-rence at the site of the primary lesion, and 2 (8%)patients experienced recurrence at the lymph nodeareas only. The 3-year locoregional recurrence freesurvival estimates were 32% (95% CI, 27–31%) in arm
A and 27% (95% CI, 24 –30%) in arm B (P 5 0.45; Fig.3A). When we included in the analysis the patientswho had postsurgery pathologic or converted com-plete responses, we found that the total numbers ofcomplete responders were 43 (61%) in arm A and 33(50%) in arm B. The corresponding 3-year locore-gional control rates were 39% (95% CI, 35– 45%) in armA and 33% (95% CI, 29 –37%) in arm B (P 5 0.35;Fig. 3B).
Distant Metastases and Second Primary TumorsMetastatic disease was detected in 15 patients, 7 of 70(10%) patients in arm A and 8 of 66 (12%) in arm B(Table 6).
Second primary tumors were detected in six pa-tients, one in arm A and five in arm B (P 5 0.09;one-tail Fisher exact text). Sites of second primarytumors were lung in four patients and esophagous intwo patients (Table 6).
Acute ToxicityTreatment-related acute toxicities were reported for127 patients (63 patients in arm A and 64 in arm B;Table 3). As shown in Table 7, hematologic toxicitywas observed only in the combined treatment arm A.Conversely, the incidence of Grade 3 and 4 mucositis(WHO criteria) was higher in the PA-RT arm than inthe chemoradiotherapy arm (49% vs. 33%, respec-tively; P 5 0.12).
The incidence of confluent mucositis according tothe RTOG scale24 was similar in both arms (54% forchemoradiotherapy group and 52% for radiotherapyalone group; see Table 8). The rate of Grade 3– 4 skinacute reactions was higher for patients in arm B thanfor those in arm A (19% vs. 5%, respectively; P 5 0.03;Table 7). As a consequence of acute toxicity, treatmentwas temporary interrupted in 15 (24%) patients in armA and in 9 (14%) patients in arm B (Table 3).
Late Toxic EffectsSpecifically, 32 long surviving patients, all free fromdisease at 4-year follow-up, 20 treated with the com-bined therapy and 12 with radiotherapy alone, werestudied to report treatment-related late effects.25 Asshown in Table 9, more Grade 21 mucosal atrophyand cervical fibrosis were observed in the group ofpatients who had been treated with PA-RT. The differ-ence in the overall incidence of moderate late effectsbetween patients treated with either chemoradiother-apy or radiotherapy alone reached statistical signifi-cance (P 5 0.02).
No severe late effects, such as osteoradionecrosis,mucosal ulceration/necrosis, and marked trismus, oc-
FIGURE 2. Progression free survival among patients with squamous cell
carcinoma of the head and neck treated with chemoradiotherapy (ALT) or partly
accelerated radiotherapy (PA-RT).
2862 CANCER December 1, 2001 / Volume 92 / Number 11
curred in any of the long survivors, indicating thatboth treatments were safe and well tolerated.
DISCUSSIONIn an attempt to overcome adverse prognosis of ad-vanced disease, treatment of head and neck carci-noma is now heading in promising directions withintensified regimens of radiotherapy and developmentof integrated associations of radiotherapy with che-motherapeutic agents, radiosensitizers, or antibodiesto growth factors.6,28,29 Given the current climate oftreatment development, we designed in 1992 this orig-inal randomized trial to compare, in a series of pa-tients affected by locally advanced SCC-HN, alternat-ing chemoradiotherapy with a high-total-doseregimen of PA-RT. These two approaches were chosenon the basis of our previous experiences that sug-gested the potential superiority of both therapies overconventional radiotherapy.10,19 Our expectations wereconfirmed by the SCC-HN literature. Recently, theresults of a large meta-analysis11 provided evidencethat concomitant chemotherapy and radiotherapymay be associated with improved overall survivalcompared with radiation therapy alone. In addition, arecently completed RTOG randomized trial14 reportedthat PA-RT with concomitant boost was significantly
associated with improved locoregional control anddisease free survival compared with conventional ra-diotherapy. These literature data, which are now stir-ring up researchers’ interest in the comparison ofconcomitant chemoradiotherapy with intensified reg-imen of radiotherapy alone, corroborate the forerun-ner design of our trial.
The randomized trial, here presented, aimed atenrollement of 240 patients to detect a difference of20% in overall survival between the two arms. How-ever, this trial, conducted from 1992 to 1998, random-ized 136 patients, and it was closed after 6 years ofopen accrual. The main reason of this low accrual wasthe unexpected low enrollment of patients from theaffiliated centers.
Given the small sample size that the trial had at itsclosure, we analyzed ultimate data to explore whetheran extremely large difference in survival could be dis-closed between two arms. In the SCC-HN literature, alarge difference in locoregional control or disease freesurvival between treatments can be found in recentstudies that also had a sample size similar or lowerthan ours.7,9,28 In a randomized trial at Duke Univer-sity,28 conducted to compare continous-course accel-erated hyperfractionation radiotherapy as controltherapy with split-course accelerated hyperfraction-
TABLE 5Cox Regression Analysis
CharacteristicNo. ofpatients
Overall survival Progression free survival
Exp(coeff) 95% CI P value Exp(coeff) 95% P value
T classificationT1 1 T2 22 1 1T3 36 1.5 0.57–2.28 0.96 0.50–1.83T4 77 1.84 1.004–3.35 0.049 1.54 0.88–2.72 0.085
RandomRT 66 1.35 0.89–2.04 1.25 0.90–2.00CT 1 RT 69 1 0.15 1 0.21
Age (yrs)# 60 74 1 1. 60 61 1.32 0.87–1.99 0.19 1.21 0.80–1.81 0.36
SiteOral cavity 78 1 1Nasopharynx 12 0.60 0.27–1.33 0.52 0.24–1.16Larynx-hypopharynx 45 0.85 0.54–1.33 0.41 0.82 0.53–1.26 0.23
N classificationN0 34 1 1N1 21 1.02 0.49–2.10 1.16 0.58–2.32N2 64 1.24 0.74–2.06 1.32 0.80–2.19N3 16 1.25 0.61–2.57 0.83 1.67 0.84–3.29 0.49
ECOG PSPS 5 0 54 1 1PS 5 1 1 2 81 1.01 0.63–1.61 0.97 1.04 0.66–1.65 0.86
CI: confidence interval; RT: radiotherapy; CT: chemotherapy; ECOG: Eastern Cooperative Oncology Group; PS: performance status.
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2863
ation and concomitant chemotherapy, a significantdifference of 26% in locoregional control between thetwo arms was detected with a sample size of only 116patients. Similarly, with a sample size of 136 patients,Jeremic et al.,29 investigating whether the addition of
chemotherapy to hyperfractionation offers an advan-tage over hyperfractionation alone, detected in favorof chemoradiotherapy statistical differences of 21%,21%, and 14%, respectively, in 5-year overall survival,progression free survival, and locoregional control.Moreover, a large significant difference of 45% both in
FIGURE 3. (A) Locoregional control among patients treated with chemora-
diotherapy (ALT) or partly accelerated radiotherapy (PA-RT). (B) Ultimate lo-
coregional control among patients treated with chemoradiotherapy (ALT) or
partly accelerated radiotherapy (PA-RT), including surgical salvage procedure
for partial responders after treatment.
TABLE 6Incidence of Distant Metastases and Second Primary TumorsAccording to Treatment Groups
Incidence type
Chemoradio-therapy(n 5 70)
Radiotherapy(n 5 66)
P valuen % n %
Distant metastases 7 10 8 12 0.51Lung 4 6 7 11Bone 1 1 — —Lymph nodes 2 3 1 1Liver 1 1 — —Skin, CNS 2 3 — —
Second primary tumors 1 1 5 8 0.09Lung 1 — 3 4.5Esophagous — — 2 3
CNS: central nervous system.
TABLE 7Acute High-Grade (Grade 3 or Higher) Toxicity in the TreatmentGroups According to WHO Criteria21
Toxicity
Combinedtreatment(n 5 63) (grade)
Radiotherapy(n 5 64) (grade)
P value3 (%) 4 (%) 3 4
Mucositis 17 (27) 4 (6) 30 (47) 1 (16) 0.12Dermatitis 2 (3) 1 (1.6) 12 (19) — 0.03Nausea/vomiting 2 (3) — — — —Anemia 4 (6) 1 (1.6) — — —Leukopenia 18 (28) 3 (5) — — —Thrombocytopenia 6 (9.5) — — — —
WHO: World Health Organization.
TABLE 8Acute Mucosal Reaction Observed in the Treatment GroupsAccording to the Objective RTOG Scale24
Reaction
Combinedtreatment(n 5 63)
Radiotherapy(n 5 64)
n % n %
Enanthema 16 (25) 11 (17)Patchy mucositis 10 (15) 19 (30)Confluent mucositis 34 (54) 33 (51)Hemorragic mucositis — — 1 (2)Not reported 3 (6) — —
RTOG: Radiation Therapy Oncology Group.
TABLE 9Late Effects (Grade 21)25 Observed in 32 Long Surviving Patients,Disease Free at 3 Years
Effect
Combinedtreatment(n 5 20) (%)
Radiotherapy(n 5 12) (%) P value
Xerostomia 5 (25) 2 (17) NSMucosal atrophy 1 (5) 5 (42) 0.01Subcutaneous fibrosis 4 (20) 8 (67) 0.01Larynx stricture 4 (20) 3 (25) NSDysphagia 1 (5) 1 (8) NS
10 pts (50) 11 (92) 0.02
NS: not significant.
2864 CANCER December 1, 2001 / Volume 92 / Number 11

local control and overall survival was observed from100 patients randomized to receive either a 7-day-per-week continous accelerated irradiation or a conven-tional 5-day-per-week treatment.30
Although the results of these trials seem contra-dictory, with a small sample size of patients it is gen-erally unlikely that a large difference in outcome willbe found, especially when two intensified treatments,such as in our trial, are compared.
In the current trial, a comprehensive analysis, re-ported in detail in “Results”, showed that there was nostatistically significant differences in overall survivaland progression free survival between the two arms.Although the data appeared to evidence a slightlyhigher complete disease clearance after chemoradio-therapy, locoregional control rates for both treatmentswere similar. Importantly, at multivariate analysis,type of treatment modality did not emerge as a signif-icant independent variable affecting overall survival orprogression free survival. One may argue that the re-sults of the PA-RT group observed in our trial arebelow average expectation.14,18 This evidence may bestrictly because of the relatively high number of un-derfed, patients who were heavy smokers and whohad advanced deeply ulcerated head and neck carci-noma who were enrolled in this trial: as shown in“Results” tumors were classified as T4N2-N3 at diag-nosis in more than one-third of patients treated withradiotherapy alone. The unfavorable prognosis of pa-tients who presented with advanced disease at diag-nosis indeed had strong relevance at multivariateanalysis in which among the various variables relatedto patients, tumor, and treatment, T classification wasthe only independent prognostic factor of worse sur-vival.
With regard to locoregional control, the observedrates were similar in both arms because more recur-rences were evident in the chemoradiotherapy armdespite higher initial complete response. Moreover,incidence of distant metastases was similar in botharms whereas second primary tumors occurred con-siderably less often in the chemoradiotherapy group.This difference in second primary tumor occurrencemay have contributed to improve overall survival ratesin the combined arm; that chemotherapy had reducedclinical appearance of second primary tumors is notprovable, though this possibility has been suggestedby others.31
The secondary end point was to assess the differ-ence between the two involved modalities in terms ofside effects. Theoretically, the two approaches wereexpected to have similar acute local toxicity whereas ahigher late toxicity could be expected after PA-RT.
At closure of the study, a pooled formal review
showed that Grade 31 acute skin toxicity was signifi-cantly lower in patients treated with chemoradiother-apy compared with patients treated with radiotherapyalone; also, acute mucositis was lower in the chemo-radiotherapy group, but only a statistical trend wasdetected.
Moreover, the analysis of late mucosal and skintoxicities performed on the subgroup of long-termsurvivors treated with both therapies appeared to ev-idence a lower score of observed effects in patientstreated with chemoradiotherapy. Alhough it is worthnoting that the observed late effects included mainlymucosal atrophy and subcutaneous fibrosis, which areof little consequence to the patient, this clinical evi-dence indicates a different potential of the two treat-ment modalities on normal tissues of the head andneck.
In the chemoradiotherapy arm, one-third of pa-tients experienced acute Grade 31 hematologic toxic-ities; these effects were, however, transient and con-trolled with supportive treatment but prolonged thealternating delivery in 26% of patients.
When we compare overall results obtained in thetwo arms in terms of therapeutic ratio,3 we find thatthe outcomes obtained with ALT were achieved withsignificant evidence of a lower local morbidity forPA-RT. This effect may be in part because of either thelow dose of total radiotherapy elapsed in the com-bined modality or the original alternated timing ofchemotherapy and radiotherapy32 adopted in our ap-proach. Conversely, our intensified PA-RT may haveinduced more local morbidity than that achievable bythe unmodified concomitant boost radiotherapy reg-imen.18
However, comparing the global results of bothtreatment modalities, we may speculate that a prelim-inary trend for an improved therapeutic index ap-peared evident in patients assigned to chemoradio-therapy association. This suggestion is, in our opinion,noteworthy because it may happen that new treat-ment programs that increase efficacy also increasetoxicity and may have a negligible effect in terms ofimproving the therapeutic ratio. In a recent RTOGtrial,14 concomitant boost radiotherapy was acceptedas a significantly better fractionation regimen thanconventional radiotherapy even if it produces an ex-tremely higher mucosal toxicity; similarly, in anotherrandomized trial the improvement of overall survivalby intensified chemoradiotherapy for intensified ra-diotherapy alone was counterbalanced by a signifi-cantly higher rate of Grade 3 and 4 mucositis.29 Theseliterature data indicate that the actual therapeutic ra-tio of new effective strategy in SCC-HN may not besystematically assessed.
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2865
To reduce the risk of systemic morbidity related tochemotherapy, we might obtain an improvement inoverall management of patients with advanced SCC-HN disease if innovative approaches, such as inte-grated chemoradiotherapy, be selected and appliedaccording to individual biologic tumor behavior.5,33,34
Our suggestion, which emerged from a detailed studyof in vivo cell kinetics in a group of patients enrolled inthe current trial, that alternating chemoradiotherapycould be more effective than PA-RT in patients withfast growing SCC-HN needs, nevertheless, to be con-firmed.35 However, although significance of overalltreatment time for radiotherapy in alternating associ-ation is controversial, these findings suggest that theusual time– dose relation may not apply.7,32
In summary, this trial did not disclose statisticallysignificant differences in the outcome of patientstreated either with ALT or PA-RT. Note that acute skineffects and late mucosal and skin toxicities above theclavicles appeared to be lower with chemoradiother-apy. Definitive conclusions cannot be drawn from thistrial, but it does make a substantial contribution tometa-analysis regarding the role of chemoradiother-apy for the cure of advanced SCC-HN.
REFERENCES1. Million RR, Cassisi NJ. Management of head and neck can-
cer: a multidisciplinary approach. Philadelphia: JB Lippin-cott, 1994.
2. Vokes EE, Weichselbaum RR, Lippman SM. Head and neckcancer. N Engl J Med 1993;328:184 –94.
3. Mendenhall W, Amdur RJ, Sieman T, Parson JT. Alteredfractionation in definitive irradiation of squamous cell car-cinoma of the head and neck. Curr Opin Oncol 2000;12:207–14.
4. Tannock IF. Treatment of cancer with radiation and drug.J Clin Oncol 1996;14:3156 –74.
5. Wennerberg J. Predicting response to radiotherapy of squa-mous cell carcinoma of the head and neck [review]. Anti-cancer Res 1996;16:2389 –96.
6. Mc Cann J. Head and neck cancers: making head way intheir treatment? J Natl Cancer Inst 2000;92:12–3.
7. Fu KK, Phillips T, Silverberg IJ, Jacobs C., Goffinet DR, ChunC, et al. Combined radiotherapy and chemotherapy withbleomycin and methotrexate for advanced inoperable headand neck cancer: update of a Northern California OncologyGroup randomized trial. J Clin Oncol 1987;5:1410 – 8.
8. Calais G, Alfonsi M, Bardet E, Sire C, Germain T, Bergerot P,et al. Randomized trial of radiation therapy versus concom-itant chemoradiotherapy for advanced-stage oropharynx tu-mors. J Natl Cancer Inst 1999;9:2081– 6.
9. Adelstein DJ, Lavertu P, Saxton JP, Secic M, Wood BG,Wanahaker JR, et al. Mature results of a phase III random-ized trial comparing concurrent chemoradiotherapy withradiation therapy alone in patients with stage III-IV squa-mous cell carcinoma of the head and neck. Cancer 2000;88:876 – 83.
10. Merlano M, Benasso M, Corvo R, Rosso R, Vitale V, BlengioF, et al. Five-year update of a randomized trial of alternating
radiotherapy and chemotherapy compared with radiother-apy alone in treatment of unresectable squamous cell car-cinoma of the head and neck. J Natl Cancer Inst 1996;88:583–9.
11. Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapyadded to loco-regional treatment for head and neck squa-mous cell carcinoma: three meta-analyses of updated indi-vidual data. Lancet 2000;355:949 –55.
12. Horiot JC, Bontemps P, van den Bogaert W, Le Fur R, van derWeingaert D, Bolla M, et al. Accelerated fractionation (AF)compared to conventional fractionation (CF) improves lo-co-regional control in the radiotherapy of advanced headand neck cancers: results of the EORTC 22851 randomizedtrial. Radiother Oncol 1997;44:111–21.
13. Horiot J-C, La Fur R, Schraub S. Status of the experience ofthe EORTC cooperative group of radiotherapy with hyper-fractionated and accelerated radiotherapy regimen. SeminRadiat Oncol 1992;2:34 –7.
14. Fu KK, Pajak TF, Trotti A, Jones CU, Spencer SA, Phillips TL,et al. A Radiation Therapy Oncology Group (RTOG) phase IIIrandomized study to compare hyperfractionation radiother-apy and two variants of accelerated fractionation to stan-dard fractionation radiotherapy for head and neck squa-mous cell carcinoma: preliminary reports of RTOG 9003. IntJ Radiat Oncol Biol Phys 2000;48::7–16.
15. Bourhis J, Fortin A, Dupuis O. Very accelerated radiationtherapy: preliminary results in locally unresectable headand neck carcinoma. Int J Radiat Oncol Biol Phys 1995;32:747–52.
16. Dische S, Saunders M, Barret A, Harvey A, Gibson D, ParmarM, et al. A randomized multicentre trial of CHART versusconventional radiotherapy in head and neck cancer. Ra-diother Oncol 1997;4:111–21.
17. Overgaard J, Sandhansen H, Overgaard M. Conventionalradiotherapy as primary treatment of squamous cell carci-noma of the head and neck: a randomized study of 5 versus6 fractions per week:report from the Dahanca7 trial. (ab-stract. Int J Radiat Oncol Biol Phys 1997;32:188.
18. Ang KK, Peters LJ, Weber RS, Maor MH, Morrison WH,Wendt CD, et al. Concomitant boost radiotherapy schedulein the treatment of carcinoma of the oropharynx and naso-pharynx. Int J Radiat Oncol Biol Phys 1990;19:1339 – 45.
19. Corvo R, Sanguineti G, Scala M, Garaventa A, Santelli A,Barbieri M, et al. Primary site as predictive factor of localcontrol in advanced head and neck tumors treated by con-comitant boost accelerated radiotherapy. Tumori 1994;80:135– 8.
20. Hermaneck P, Sobin LH, editors. International UnionAgainst Cancer (UICC) TNM classification of malignant tu-mors. 4th ed. Heidelberg, Germany: Springer-Verlag, 1992.
21. Miller AB, Hoorstraten B, Staquet M, Winkler A. Reportingresults of cancer treatment. Cancer 1981;47:207–14.
22. ICRU Report 50. Prescribing, recording and reporting pho-ton beam therapy. Bethesda, MD: International Commis-sion for Radiation Units and Measurements., 1993.
23. Kaplan EL, Meier P. Non parametric estimation of incom-plete observation. J Am Stat Assoc 1985;53:457– 81.
24. Schmidt-Ullrich RK, Johnson CJ, Wazer DE, Masko G, Cha-sin WD, Karmody CS. Accelerated superfractionated irradi-ation for advanced carcinoma of the head and neck: con-comitant boost technique. Int J Radiat Oncol Biol Phys 1991;21:563– 8.
25. LENT SOMA scales for all anatomic sites. Int J Radiat OncolBiol Phys 1995;31:1049 –92.
2866 CANCER December 1, 2001 / Volume 92 / Number 11
26. Cox DR, Dakes D. Analysis of survival data. London: Chap-man and Hall, 1984.
27. Dixon WJ, Brown MB, Engelman L. BMDP statistical soft-ware manual. Berkeley: University of California Press, 1990.
28. Brizel DM, Albers ME, Fisher SR, Scher RL, Richtsmeier WJ,Hars V, et al. Hyperfractionated irradiation with or withoutconcurrent chemotherapy for locally advanced head andneck cancer. N Engl J Med 1998;338:1798 – 804.
29. Jeremic B, Shibamoto Y, Milic B, Nicolic N, Dagovic A,Aleksandrovic J, et al. Hyperfractionated radiation therapywith or without concurrent low-dose daily cisplatin in lo-cally advanced squamous cell carcinoma of the head andneck: a prospective randomized trial. J Clin Oncol 2000;18:1458 – 64.
30. Skladowski K, Maciejewski B, Golen M, Pilecki B, PrzeorekW, Tarnawski R. Randomized clinical trial on 7-day-con-tinous accelerated irradiation (CAIR) of head and neck can-cer -report on 3-year tumor control and normal tissue tox-icity. Radiother Oncol 2000;55:101–10.
31. Paccagnella A, Orlando A, Marchioni C, Zorat P, CaravigliaG, Silemi VC, et al. Phase III trial of initial chemotherapy in
stage III and IV head and neck cancer: a study by theGruppo di Studio sui Tumori della Testa e Collo. J NatlCancer Inst 1994;86:265–72.
32. Sanguineti G, Corvo R, Sormani MP, Benasso M, NumicoGM, Bacigalupo A, et al. Chemotherapy alternated with ra-diotherapy in the treatment of advanced head and neckcarcinomas: predictive factors of outcome. Int J Radiat On-col Biol Phys 1999;44:139 – 47.
33. Ritter MA. Determination of tumor kinetics: strategies forthe delivery of radiotherapy and chemotherapy. Curr OpinOncol 1999;2:177– 82.
34. Corvo R, Giaretti W, Sanguineti G, Geido E, Orecchia R,Guenzi M, et al. In vivo cell kinetics in head and necksquamous cell carcinoma predicts local control and helpsguide radiotherapy regimen. J Clin Oncol 1995;11:1843–50.
35. Corvo R, Paoli G, Giaretti W, Sanguineti G, Geido E, BenassoM, et al. Evidence of cell kinetic as predictive factor ofresponse to radiotherapy alone or chemoradiotherapy inpatients with advanced head and neck cancer. Int J RadiatOncol Biol Phys 2000;47:57– 63.
Chemoradiotherapy verus Accelerated Radiotherapy in Advanced SCC-HN/Corvo et al. 2867





























