Embed Size (px)
Citation preview
Archives of Cardiovascular Disease (2012) 105, 623—630
Available online at
www.sciencedirect.com
CLINICAL RESEARCH
Aldosterone-to-renin ratio for diagnosingaldosterone-producing adenoma: A multicentre study
Le rapport aldostérone/rénine pour diagnostiquer un adénome de Conn : uneétude multicentrique
Michel Duchera, Claire Mounier-Véhierb,Jean-Philippe Baguetc, Jean-Michel Tartièred,Philippe Sosnere, Sylvie Régnier-Le Cozd,Laurence Perezf, Jacques Fourcadeg,Olivier Jabourekb, Sylvain Lejeuned, Arnaud Stolzh,Jean-Pierre Fauvela,∗
a Club des Jeunes Hypertensiologues, Lyon, Franceb Club des Jeunes Hypertensiologues, Lille, Francec Club des Jeunes Hypertensiologues, Grenoble, Franced Club des Jeunes Hypertensiologues, Paris, Francee Club des Jeunes Hypertensiologues, Poitiers, Francef Club des Jeunes Hypertensiologues, Toulouse, Franceg Club des Jeunes Hypertensiologues, Chambéry, Franceh Club des Jeunes Hypertensiologues, Metz, France
Received 2 May 2012; accepted 6 July 2012Available online 2 October 2012
KEYWORDSAldosteronism;Renin;Aldosterone-
SummaryBackground. — Biological diagnostic criteria for diagnosing aldosterone-producing adenoma(APA) are not well-established.Aim. — The aim of the study was to establish the best biological predictors of APA.
producing adenoma;Hypertension;Hypokalaemia;
Methods. — A prospective register was implemented in 17 secondary or tertiary hypertensioncentres. The inclusion criterion was one of the following: onset of hypertension before 40years of age; history of hypokalaemia; drug-resistant hypertension (resistant to three drugs);or spironolactone efficiency on BP.
Abréviations: APA, aldosterone-producing adenoma; ARR, aldosterone-to-renin ratio; AVS, adrenal venous sampling; BP, blood pressure;CT, computed tomography; PA, primary aldosteronism; ROC, receiver operating characteristic.
∗ Corresponding author. Hôpital Édouard-Herriot, club des Jeunes Hypertensiologues, 5, place Arsonval, 69437 Lyon cedex 03, France.E-mail address: [email protected] (J.-P. Fauvel).
1875-2136/$ — see front matter © 2012 Elsevier Masson SAS. All rights reserved.http://dx.doi.org/10.1016/j.acvd.2012.07.006

624 M. Ducher et al.
Aldosterone-to-reninratio
Results. — Among the 338 collected cases, 192 patients had two aldosterone-to-renin ratio(ARR) determinations (after 1 hour supine and at least 1 hour upright) on the same occasion.Twenty-five patients (8.2%) had biological hyperaldosteronism and an adrenal adenoma identi-fied by computed tomography. APA was histologically confirmed in all 12 patients who underwentsurgery. Histologically proven APAs were used as the ‘gold standard’ in receiver operating char-acteristic (ROC) curve analysis. ARRs were computed with a minimum renin value set at 5 ng/Lto avoid misclassification of so-called ‘low-renin hypertension’. To predict an APA, the ARR areaunder the ROC curve was 0.93. A supine ARR cut-off value of 32 ng/ng provided the highest sumof sensitivity (92%) plus specificity (92%). On the basis of an ARR ≥ 32 ng/ng in the supine and/orupright position, sensitivity reached 100%.Conclusion. — The proposed cut-off value of 32 ng/ng for ARR (minimum renin value set at5 ng/L) in one of two determinations had 100% sensitivity and 72% specificity with 20% positiveand 100% negative predictive values for diagnosing APA.© 2012 Elsevier Masson SAS. All rights reserved.
MOTS CLÉSAldosterone ;Rénine ;Adénome de Conn ;Hypertension ;Hypokaliémie ;Rapportaldostérone-rénine
RésuméContexte. — Les critères biologiques pour le diagnostic d’un adénome de Conn ne sont pas bienétabli.Objectif. — L’objectif de cette étude est d’établir les seuils biologiques d’aldostérone et derénine permettant de prédire un adénome de Conn.Méthodes. — Un registre prospectif a été mis en œuvre dans 17 centres de l’hypertension. Lecritère d’inclusion dans le registre était l’un des éléments suivants : apparition de l’hypertensionavant 40 ans, antécédent d’hypokaliémie, hypertension artérielle résistante ou efficacité tropimportante de la spironolactone dans le traitement de l’hypertension.Résultats. — Parmi les 338 cas recueillis, 192 patients ont eu deux déterminations successives derénine et d’aldostérone (une heure en position couchée et au moins une heure debout). Vingt-cinq patients (8,2 %) avaient un hyperaldostéronisme biologique et un adénome surrénalienidentifié par une tomodensitométrie. Une histologie compatible avec un adénome de Conn aété confirmée chez les les 12 patients qui ont été opérés. Un adénome de Conn histologique-ment confirmé a été utilisé comme « gold standard » pour l’établissement des courbes ROC.Les rapports aldostérone/rénine (RAR) ont été calculés avec une valeur minimale de réninefixée à 5 ng/L. Afin de prédire un adénome de Conn, l’aire sous la courbe ROC du RAR était de0,93. Une valeur de RAR couchée supérieure à 32 ng/ng avait les sensibilités (92 %) et spécificité(92 %) les plus élevées. Sur la base d’un RAR supérieur à 32 ng/ng en décubitus dorsal et/ou enorthostatisme, la sensibilité atteint 100 %.Conclusion. — Le seuil de RAR à 32 ng/ng (valeur minimale de rénine à 5 ng/L) lors de l’une desdeux déterminations, soit en décubitus dorsal, soit en orthostatisme a une sensibilité de 100 %,une spécificité de 72 %, une valeur prédictive positive de 20 % et une valeur prédictive négativede 100 % pour le diagnostic d’un adénome de Conn.
. Tou
B
Porittcaaaclptc
tpPtoitTcMt[hh
© 2012 Elsevier Masson SAS
ackground
rimary aldosteronism (PA) is one of the commonest formsf secondary hypertension [1] and diagnosis of PA haseceived much attention in recent years [2—6]. Once PAs confirmed, the subtype must be determined in ordero guide treatment. Almost one-third of PA cases are dueo aldosterone-producing adenoma (APA) and are surgicallyurable. Two-thirds of PA cases are related to idiopathicdrenal primary aldosteronism, frequently with nodulardrenal hyperplasia [7]. APA has been reported to carry
higher risk of left ventricular hypertrophy, stroke andhronic kidney disease [8—13]. A surgical alternative toong-term drug therapy would reduce costs and increase
atients’ quality of life. PA was initially defined as hyper-ension associated with increased aldosterone and low reninoncentrations. High concentrations of aldosterone lead toKit
s droits réservés.
he sodium retention responsible for hypertension and renalotassium loss causing hypokalaemia. However, in half ofA cases, kalaemia is within the normal range and some-imes even blood pressure (BP) is normal. Thus, diagnosisf PA is not easy and screening for possible PA, which wasnitially restricted to hypertension with hypokalaemia, hado be extended to cases of resistant hypertension [14,15].he diagnosis of PA remains biological, associating high con-entrations of aldosterone with low concentrations of renin.any authors have used the aldosterone-to-renin ratio (ARR)
o define PA and several cut-off values have been proposed14,16—22]. Furthermore, to avoid diagnosis of low-reninypertension, minimum values for renin and/or aldosteroneave been advocated for calculating the ARR. As noted by
aplan [23], there are ‘considerable differences in the def-nition of an elevated ARR’. Two strategies have been usedo define the ARR. The first, representing the upper values

ma
TwotwsaabwpTi
S
DMttoutlRt2icpcaitw
R
AlhpApacAsabat(o
pw
Aldosterone-to-renin ratio and aldosterone-producing adeno
obtained in unselected essential hypertensive subjects, ledto a lower cut-off value and a consequently higher percent-age of PA (up to 39% of hypertensives). The second is basedon minimal ARR values in patients with an APA. A moresuitable strategy used by Bernini et al. [24] to assess ARRcut-off values is based on receiver operating characteristic(ROC) analysis. In their single centre study, they proposedan aldosterone-to-plasma renin activity cut-off value andreported a high percentage of APA (8.4%) and IHAP (author todefine at proof stage) (12.7%) in newly diagnosed hyperten-sives. In the PAPY study, Rossi et al. [25] reported that ARRbased on measurement of active renin is a valuable alterna-tive to that based on plasma renin activity. Using a similarstrategy, we conducted a prospective multicentre study todetermine an ARR threshold for detecting an APA.
Methods
A prospective register was implemented in 17 secondary ortertiary hypertensive centres. The inclusion criterion wasone of the following: onset of hypertension before 40 yearsof age; history of hypokalaemia; drug-resistant hypertension(resistant to three drugs); or spironolactone efficiency onBP. The register opened in October 2006 and closed in June2007 when 300 consecutive case reports were recorded asspecified in the study protocol.
For each patient, the following data were col-lected: anthropomorphic variables and lifestyle (weight,height, smoking habits, alcohol consumption, liquorice con-sumption); hypertension history (duration, family history,efficiency of spironolactone if available and potassiumsupplementation; sitting BP [measured three times at 2-minute intervals after a 5-minute rest; the averages ofthe three BP measurements were calculated; validatedautomatic sphygmomanometers were used in all cen-tres]); cardiovascular complications (myocardial infarction,arrhythmia and stroke); biological variables (kalaemia, cre-atininaemia, plasma bicarbonate, 24-hour urinary excretionof creatinine, sodium, potassium, albumin and aldosterone);plasma aldosterone and active renin (both expressed inng/L), determined after 1 hour in a supine position and afterat least 1 hour in an upright position.
A minimum plasma renin value of 5 ng/L was set tocalculate the ARR. Treatments that might interfere withthe renin-angiotensin system were not allowed; however,oral contraceptive and hormonal replacement therapieswere not stopped or modified. A wash-out period priorto ARR screening was 2 weeks for angiotensin-convertingenzyme inhibitors, angiotensin receptor blockers, beta-blockers and diuretics (except for spironolactone) and 4weeks for spironolactone; however, in 22 patients withischaemic myocardial disease, beta-blockers could not beinterrupted. When necessary, authorized treatments werecalcium channel blockers (non-dihydropyridine or long-acting dihydropyridine), central-acting agents (rilmenidine)and alpha-blockers (slow-release prasozin, urapidil). Sodiumdiet and potassium supplementation (if applicable) were not
modified. Cases reports containing unauthorized drugs werediscarded (n = 6).Using complete case report forms, a blind outcome com-mittee (J.-P.F. and J.-P.B.) established the diagnosis of PA.
wsht
625
he ARR cut-off value of 23 ng/ng was used to suspect a PA,ith the minimal renin concentration set at 5 ng/L. This cut-ff value was chosen because it was the lowest reported inhe literature [17]. However, in five case reports, the ARRas greater than 23 ng/ng and computed tomography (CT)
cans were not available; the diagnosis could not be madend these cases were excluded for incomplete data. Actu-lly, in the remaining patients, the minimum ARR value usedy the investigators for high-resolution angiographic CT-scanas 14.5 ng/ng. Thus, a CT-scan was also performed in 99atients (70%) in whom the ARR was lower than 23 ng/ng.wenty-two other case reports were also excluded due toncomplete data.
tatistical analysis
ata were expressed as mean values ± standard deviations.ean values between groups were compared using Student’s
test. Categorical variables were compared using the Chi2
est. ROC analysis was used to evaluate the diagnostic powerf different ARR levels. To estimate classification accuracysing ROC analysis, the disease status of each patient hado be validated without error. Thus, we chose the histo-ogically proven cases of APA as the gold standards for theOC analysis. ARR is a continuous-scale measurement. Oncehe diagnosis of APA for each patient was determined, a
× 2 contingency table was made. Sensitivity (i.e. true pos-tive rate) and specificity (i.e. true negative rate) werealculated for each ARR cut-off value. A ROC curve thatlotted sensitivity against (1—specificity) was drawn. Theloser the area under the ROC curve was to 1, the moreccurate the diagnostic test. The Younden score (sensitiv-ty + specificity—1) provided the optimal ARR cut-off valueo diagnose APA. Data analysis used Medcalc® 11.5.1.0 soft-are.
esults
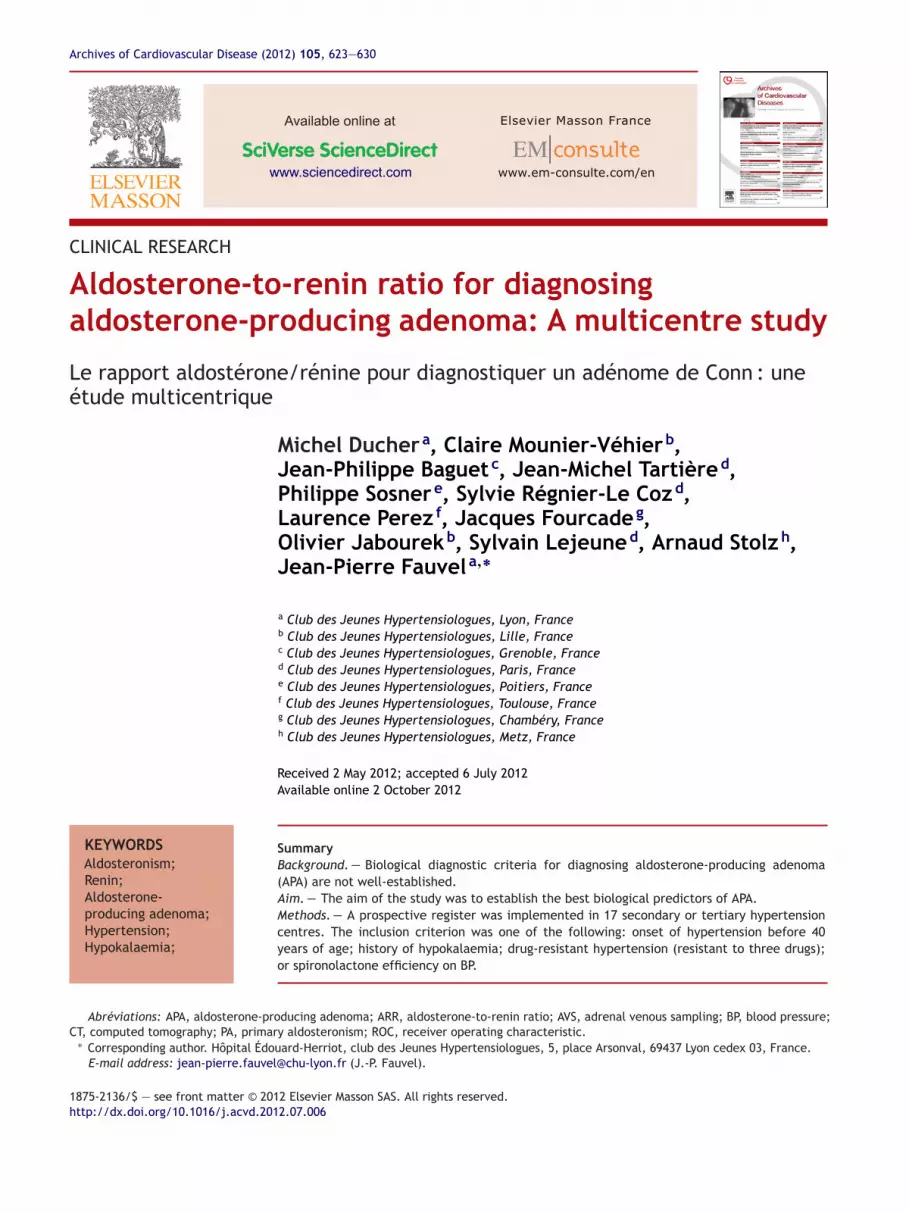
s shown on the flow-chart (Fig. 1), among the 338 col-ected cases, 305 met all the inclusion criteria, 192 patientsad two ARR determinations (supine and upright) and 25atients (8.2%) had biological PA and an adrenal adenoma.mong them, 12 patients chose adrenalectomy and 13referred pharmacological treatments. Five patients (twomong those who chose adrenalectomy) who had biologi-al PA and an adrenal adenoma were taking a beta-blocker.mong the 12 operated patients, only six had adrenal venousampling (AVS); in each case, it confirmed the unilateralldosterone secretion. No technical failure was reportedy the investigators. In all those who underwent unilateraldrenalectomy, an APA was confirmed by histology. Patientsreated by spironolactone achieved either normalizationn = 9) or significant reduction (n = 4) in BP (BP decrease > 20%r use of fewer antihypertensive drugs).
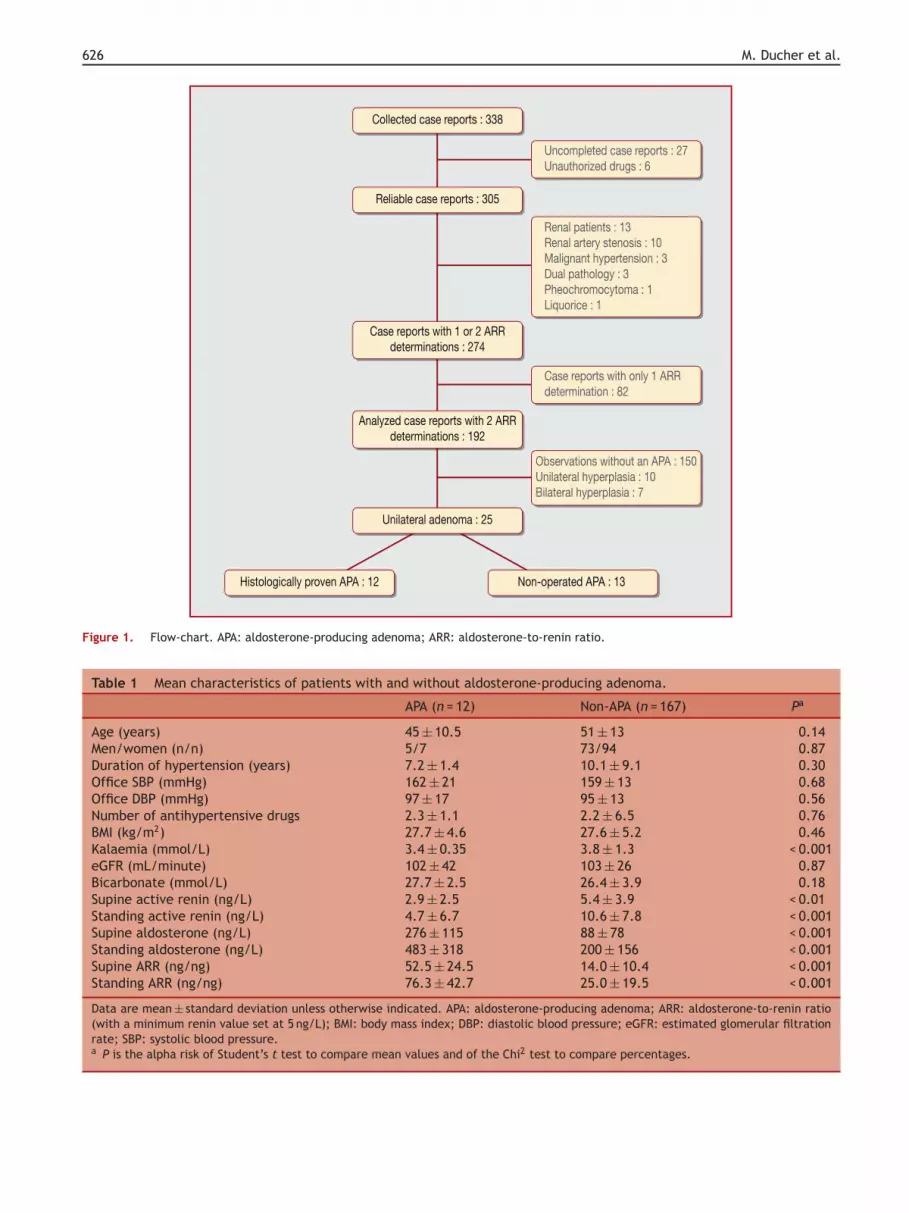
Thus, for our purpose, the 12 patients with histologicallyroven APAs were compared with the 167 remaining patientsho did not have APAs. The mean characteristics of patients
ith histologically proven APAs and those without APAs arehown in Table 1. BP was slightly, but not significantly,igher in APA patients undergoing similar therapy at presen-ation. Four of the 12 (33%) APA patients had normal serum
626 M. Ducher et al.
Collected�case� reports�:�338
Reliable�case�reports�:�305
Unilateral�adenoma�:�25
Histologically�proven�APA�:�12 Non-operated�A PA�:�13
Case�reports�with�1�or�2�ARRdeterminations�:�274
Uncompleted�case�reports�:�27Unauthorized�drugs�:�6
Case�reports�with�only�1�ARRdetermination�:�82
Observations�without�an�A PA�:�150Unilateral�hyperplasia�:�10Bilateral�hyperplasia�:�7
Renal�patients�:�13Renal�artery�stenosis�:�10Malignant�hypertension�:�3Dual�pathology�:�3Pheochromocytoma�:�1Liquorice�:�1
Analyzed�case� reports�with�2�ARRdeterminations�:�192
Figure 1. Flow-chart. APA: aldosterone-producing adenoma; ARR: aldosterone-to-renin ratio.
Table 1 Mean characteristics of patients with and without aldosterone-producing adenoma.
APA (n = 12) Non-APA (n = 167) Pa
Age (years) 45 ± 10.5 51 ± 13 0.14Men/women (n/n) 5/7 73/94 0.87Duration of hypertension (years) 7.2 ± 1.4 10.1 ± 9.1 0.30Office SBP (mmHg) 162 ± 21 159 ± 13 0.68Office DBP (mmHg) 97 ± 17 95 ± 13 0.56Number of antihypertensive drugs 2.3 ± 1.1 2.2 ± 6.5 0.76BMI (kg/m2) 27.7 ± 4.6 27.6 ± 5.2 0.46Kalaemia (mmol/L) 3.4 ± 0.35 3.8 ± 1.3 < 0.001eGFR (mL/minute) 102 ± 42 103 ± 26 0.87Bicarbonate (mmol/L) 27.7 ± 2.5 26.4 ± 3.9 0.18Supine active renin (ng/L) 2.9 ± 2.5 5.4 ± 3.9 < 0.01Standing active renin (ng/L) 4.7 ± 6.7 10.6 ± 7.8 < 0.001Supine aldosterone (ng/L) 276 ± 115 88 ± 78 < 0.001Standing aldosterone (ng/L) 483 ± 318 200 ± 156 < 0.001Supine ARR (ng/ng) 52.5 ± 24.5 14.0 ± 10.4 < 0.001Standing ARR (ng/ng) 76.3 ± 42.7 25.0 ± 19.5 < 0.001
Data are mean ± standard deviation unless otherwise indicated. APA: aldosterone-producing adenoma; ARR: aldosterone-to-renin ratio(with a minimum renin value set at 5 ng/L); BMI: body mass index; DBP: diastolic blood pressure; eGFR: estimated glomerular filtrationrate; SBP: systolic blood pressure.a P is the alpha risk of Student’s t test to compare mean values and of the Chi2 test to compare percentages.

Aldosterone-to-renin ratio and aldosterone-producing adenoma 627
Figure 2. Receiver operating characteristic curve for active renin, aldosterone and aldosterone-to-renin ratio in 12 proven or 25 sus-upine
rwwvo
pected aldosterone-producing adenomas (APAs) determined in the scharacteristic curve; ARR: aldosterone-to-renin ratio.
potassium concentrations (≥ 3.5 mmol/L). Bicarbonate andestimated renal function (Cockcroft and Gault formula) didnot differ between groups. Supine and standing active reninconcentrations were significantly lower and aldosteroneconcentrations were significantly higher in APA patients.
Consequently, supine and standing ARRs were significantlyhigher in APA patients. The area under the ROC curve thatplotted sensitivity versus (1—specificity) for supine activeccF
position for 179 patients. AUC: area under the receiver operating
enin was 0.72 (Fig. 2), while that for supine aldosteroneas 0.92 (Fig. 2). The highest area under the ROC curveas obtained with an ARR calculated with the minimalalue of active renin set at 5 ng/L (data not shown forther renin threshold). The highest area under the ROC
urves provided the highest Younden index and thus the bestompromise between sensitivity and specificity. As shown inig. 2, the AUC for the ROC analysis was 0.93 for supine
628 M. Ducher et al.
Table 2 Diagnostic power of the different biological tests determined in supine position.
Renin Aldosterone ARR
Cut-off values (ng/L) 4.0 167 32AUC 0.72 (0.65—0.79) 0.92 (0.90—0.97) 0.93 (0.89—0.96)Sensitivity (%) 83 (52—98) 92 (61—100) 92 (63—100)Specificity (%) 54 (46—62) 87 (81—92) 92 (87—96)PPV (%) 11 (6—20) 33 (18—52) 46 (25—68)PNV (%) 97 (92—100) 99 (96—100) 99 (97—100)
ed. Acurve
Acgs1p31nvawcs
oha
D
PabchbcrisAo
ptcAfspAOmwtf
chamm
vseiAanppca
awctcls
aaaAtcicficTrttoabt
Data are mean (95% confidence interval) unless otherwise indicatat 5 ng/L); AUC: area under the receiver operating characteristic
RR. The highest Younden coefficients with correspondingut-off values for aldosterone, active renin and ARR areiven in Table 2. The corresponding ARR cut-off value in theupine position was 32 ng/ng. According to this cut-off value,1 APAs were diagnosed. An ARR > 32 ng/ng in the uprightosition revealed the remaining APA. The cut-off value of2 ng/ng for ARR in at least one of two determinations had00% sensitivity, 72% specificity and 20% positive and 100%egative predictive values for diagnosing an APA. Absolutealues of active renin and aldosterone did not provide anydditional information. When applied to the 25 patients, inhom the CT-scan revealed an adrenal adenoma, the ARRut-off value of 32 ng/ng provided a specificity of 92% and aensitivity of 72% (Fig. 2).
According to the CT-scan and the determined thresh-ld of 32 ng/ng, there were five cases of bilateral primaryyperplasia, four cases of unilateral primary hyperplasia (nodenoma) and 34 cases of idiopathic hyperaldosteronism.
iscussion
rimary aldosteronism is defined as inappropriately high andutonomous aldosterone secretion, which is not suppressibley sodium loading. Among PA, diagnosing an APA is of clini-al interest as it is a curable cause of hypertension in aboutalf of the patients [26], adrenalectomy has become simplery coelioscopy and APAs are associated with high cardiovas-ular morbidity and renal impairment [27]. The ARR, whicheflects aldosterone hypersecretion in relation with renin,s currently considered to be the most reliable tool for PAcreening. The aim of our study was to propose a reliableRR threshold that is usable as a first step in the diagnosisf an APA.
The ARR first proposed by Dunn and Espiner [16] in 1976roved to be the best for differentiating PA from essen-ial hypertension. There is marked heterogeneity in theonditions of ARR determination and therefore in proposedRR cut-off values [17,18,22,23,28]. However, although per-ormed in different conditions in a multicentre study (PAPYtudy), ARR determinations showed satisfactory within-atient reproducibility [29]. The population in which theRR cut-off value is determined is of major importance.ur study population is in accordance with current recom-
endations [30]. In our study, the percentage of patientsith an APA was very similar to that reported in the litera-ure. As recommended by Plouin et al. [20], minimum valuesor renin and/or aldosterone must be determined to avoid
c(w[
RR: aldosterone-to-renin ratio (with a minimum renin value set; PPN: negative predictive value; PPV: positive predictive value.
lassifying low-renin hypertension as PA. In our study, theighest area under the ROC curve for ARR was obtained with
minimal value of active renin set at 5 ng/L. To set a mini-al renin concentration at 5 ng/L is equivalent to setting ainimal aldosterone concentration at 160 ng/L.There are considerable differences in definitions of ele-
ated ARR, with most ARR cut-off values set as the mean + 2tandard deviations of values obtained in patients withssential hypertension. A methodology well suited to defin-ng an ARR cut-off is ROC analysis. In our study, diagnosis ofPA was based on the association of biological PA, an adrenaldenoma on CT-scan and a histological proven adrenal ade-oma in operated patients. The proportion of operatedatients was similar to that usually reported [18]. In the 12atients who underwent surgery, histological analysis alwaysonfirmed the APA. For the other cases, spironolactone waslways efficient in normalizing (n = 9) or reducing (n = 4) BP.
In our study, an ARR determination was performed at restnd during an orthostatic stimulation test, as recommendedhen our study was implemented. In 2006, there was nolear consensus on the diagnostic usefulness of confirmatoryests (sodium loading test, fludrocortisone suppression test,aptopril challenge test) [4]. Considering the further pub-ished recommendations [30], the lack of confirmatory testshould be taken into account when interpreting our study.
The population in which the ROC analysis is applied islso of major importance. To our knowledge, ROC curvenalysis has been used mainly in case-control studies. Such
selection of subjects artificially increases the number ofPAs in the tested population and the definition of con-rols is also somewhat arbitrary. Sensitivity and specificityould be artificially increased. Thus, a small bias in select-ng the control population may result in great variations inut-off values, which are based on sensitivity and speci-city. Furthermore, positive and negative predictive valuesannot be calculated accurately in case-control studies.o avoid such sampling bias, we implemented prospectiveegisters in 17 secondary or tertiary hypertension cen-res. Adherence of centres to the register was voluntary;his can be regarded as a limitation of our study. On thether hand, the centres were scattered all over Francend can be considered as representative. To avoid selectionias, investigators were instructed to register consecu-ive case reports from October 2006 to June 2007. We
hecked the possible centre effect by analysis of varianceAnova). The main characteristics of our included patientsere similar to those usually reported in the literature18].

ma
A
TPBp
R
[
[
[
[
[
[
[
[
[
Aldosterone-to-renin ratio and aldosterone-producing adeno
The main limitation in our ‘real-life multicentre study’is that biological variables were determined in each centreand thus were not standardized. However, when a centrallaboratory is used, results are valid only if performed in thatlaboratory. Our approach was more pragmatic and thus theresults, which may be considered as less accurate, can beapplied to different centres.
AVS is the most accurate means of differentiatingbetween uni- and bilateral forms of PA. However, it remainsdifficult and should be undertaken only by trained physi-cians. AVS can lead to false-negative results, especiallyfor right APA [31]. Thus, AVS that was performed onlyin six operated patients over 12 was not taken intoaccount when analysing our results. However, the per-centage of PA patients systematically submitted to AVSranged from 19% to 100% in referral centres for endocrinehypertension worldwide [32]. Even in specialized cen-tres, success rates for AVS were poor [33]. However, AVSremains recommended before surgery [30]. In our study,the absence of AVS should not have interfered with ourresults as only patients with histologically documentedadenoma were used as references in the ROC analy-sis. Usually, surgery efficiency is confirmed by BP andkalaemia determinations. A postsurgery measure of plasmaaldosterone was not performed in our pragmatic clinicalstudy.
One criterion for deciding the cut-off value of a testis to maximize the sum of sensitivity and specificityvalues (Younden coefficient). According to this strategy,the proposed ARR cut-off value is 32 ng/ng. However,a single determination of ARR did not provide suffi-cient sensitivity for clinical practice. A second value ofARR ≥ 32 ng/ng after at least 1-hour standing increasedthe sensitivity to 100%, together with a satisfactory speci-ficity of 72%. However, CT-scans are not sensitive enoughto reveal all the unilateral APAs. Thus, our ARR cut-off value can only be considered for screening for APAsthat can be visualized by CT-scan. What to do if anARR is > 32 ng/ng without any CT-scan adrenal abnormal-ity remains to be explored. Our proposed ARR cut-offvalue of ≥ 32 ng/ng is not far from the one determinedin the PAPY study (27.3 ng/mU corresponding to 38 ng/ng)[25].
Conclusion
In conclusion, our proposed pragmatic approach, basedon an ARR cut-off value ≥ 32 ng/ng in one of twodeterminations, with a minimal active renin valueset at 5 ng/L (or minimal aldosterone at 160 ng/L),diagnosed APA with very good sensitivity and satisfac-tory specificity. Although determined in a prospectivemulticentre study, this cut-off value must be con-firmed.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
[
629
cknowledgements
he authors would like to thank Professor Pierre-Francoislouin for manuscript revision and both Mrs Christianeertheux-Beaufrere and Lynn Richardson for translation sup-ort.
eferences
[1] Rossi GP, Bernini G, Caliumi C, et al. A prospective study ofthe prevalence of primary aldosteronism in 1125 hypertensivepatients. J Am Coll Cardiol 2006;48:2293—300.
[2] Calhoun DA. Is there an unrecognized epidemic of pri-mary aldosteronism? Pro Hypertens 2007;50:447—53, discussion47—53.
[3] Gordon RD, Stowasser M, Tunny TJ, et al. High incidence of pri-mary aldosteronism in 199 patients referred with hypertension.Clin Exp Pharmacol Physiol 1994;21:315—8.
[4] Kaplan NM. Cautions over the current epidemic of primaryaldosteronism. Lancet 2001;357:953—4.
[5] Lim PO, Rodgers P, Cardale K, et al. Potentially high prevalenceof primary aldosteronism in a primary-care population. Lancet1999;353:40.
[6] Mulatero P, Stowasser M, Loh KC, et al. Increased diagno-sis of primary aldosteronism, including surgically correctableforms, in centers from five continents. J Clin Endocrinol Metab2004;89:1045—50.
[7] Stowasser M, Gordon RD, Gunasekera TG, et al. High rate ofdetection of primary aldosteronism, including surgically treat-able forms, after ‘non-selective’ screening of hypertensivepatients. J Hypertens 2003;21:2149—57.
[8] Catena C, Colussi G, Nadalini E, et al. Cardiovascular outcomesin patients with primary aldosteronism after treatment. ArchIntern Med 2008;168:80—5.
[9] Matsumura K, Fujii K, Oniki H, et al. Role of aldosterone inleft ventricular hypertrophy in hypertension. Am J Hypertens2006;19:13—8.
10] Milliez P, Girerd X, Plouin PF, et al. Evidence for an increasedrate of cardiovascular events in patients with primary aldos-teronism. J Am Coll Cardiol 2005;45:1243—8.
11] Ribstein J, Du Cailar G, Fesler P, et al. Relative glomerularhyperfiltration in primary aldosteronism. J Am Soc Nephrol2005;16:1320—5.
12] Rossi GP, Bernini G, Desideri G, et al. Renal damage in pri-mary aldosteronism: results of the PAPY Study. Hypertension2006;48:232—8.
13] Sechi LA, Novello M, Lapenna R, et al. Long-term renaloutcomes in patients with primary aldosteronism. JAMA2006;295:2638—45.
14] Calhoun DA. Aldosteronism and hypertension. Clin J Am SocNephrol 2006;1:1039—45.
15] Mosso L, Carvajal C, Gonzalez A, et al. Primary aldosteronismand hypertensive disease. Hypertension 2003;42:161—5.
16] Dunn PJ, Espiner EA. Outpatient screening tests for primaryaldosteronism. Aust N Z J Med 1976;6:131—5.
17] Giacchetti G, Ronconi V, Lucarelli G, et al. Analysis of screeningand confirmatory tests in the diagnosis of primary aldos-teronism: need for a standardized protocol. J Hypertens2006;24:737—45.
18] Niizuma S, Nakahama H, Kamide K, et al. The cut-off value ofaldosterone-to-renin ratio for the diagnosis of primary aldos-
teronism in patients taking antihypertensive medicine. Clin ExpHypertens 2008;30:640—7.19] Nishizaka MK, Pratt-Ubunama M, Zaman MA, et al. Validity ofplasma aldosterone-to-renin activity ratio in African American

6
[
[
[
[
[
[
[
[
[
[
[
[
[
30
and white subjects with resistant hypertension. Am J Hypertens2005;18:805—12.
20] Plouin PF, Amar L, Chatellier G. Trends in the preva-lence of primary aldosteronism, aldosterone-producingadenomas, and surgically correctable aldosterone-dependent hypertension. Nephrol Dial Transplant 2004;19:774—7.
21] Schwartz GL, Turner ST. Screening for primary aldosteronismin essential hypertension: diagnostic accuracy of the ratio ofplasma aldosterone concentration to plasma renin activity. ClinChem 2005;51:386—94.
22] Tiu SC, Choi CH, Shek CC, et al. The use of aldosterone-reninratio as a diagnostic test for primary hyperaldosteronism and itstest characteristics under different conditions of blood samp-ling. J Clin Endocrinol Metab 2005;90:72—8.
23] Kaplan NM. Primary aldosteronism. In: Kaplan’s Clinical Hyper-tension. 9th ed. Philadelphia: Lippincott Williams & Wilkins;2005. p. 410—33.
24] Bernini G, Moretti A, Orlandini C, et al. Plasma andurine aldosterone to plasma renin activity ratio in thediagnosis of primary aldosteronism. J Hypertens 2008;26:981—8.
25] Rossi GP, Barisa M, Belfiore A, et al. The aldosterone-renin ratiobased on the plasma renin activity and the direct renin assayfor diagnosing aldosterone-producing adenoma. J Hypertens2010;28:1892—9.
[
M. Ducher et al.
26] van der Linden P, Steichen O, Zinzindohoue F, et al. Bloodpressure and medication changes following adrenalectomy forunilateral primary aldosteronism: a follow-up study. J Hyper-tens 2012;30:761—9.
27] Rossi GP. Diagnosis and treatment of primary aldosteronism.Rev Endocr Metab Disord 2011;12:27—36.
28] Kaplan NM. Primary aldosteronism: a contrarian view. RevEndocr Metab Disord 2011;12:49—52.
29] Rossi GP, Seccia TM, Palumbo G, et al. Within-patientreproducibility of the aldosterone: renin ratio in primary aldos-teronism. Hypertension 2010;55:83—9.
30] Funder JW, Carey RM, Fardella C, et al. Case detection, diagno-sis, and treatment of patients with primary aldosteronism: anendocrine society clinical practice guideline. J Clin EndocrinolMetab 2008;93:3266—81.
31] Sarlon-Bartoli G, Michel N, Taieb D, et al. Adrenal venoussampling is crucial before an adrenalectomy whatever theadrenal-nodule size on computed tomography. J Hypertens2011;29:1196—202.
32] Rossi GP, Barisa M, Allolio B, et al. The Adrenal Vein Samp-ling International Study (AVIS) for identifying the majorsubtypes of primary aldosteronism. J Clin Endocrinol Metab
2012;97:1606—14.33] Vonend O, Ockenfels N, Gao X, et al. Adrenal venous samp-ling: evaluation of the German Conn’s registry. Hypertension2011;57:990—5.





























