Embed Size (px)
Citation preview

1
Effectiveness of Decentralized Program Planning and Management in Improving Age
Appropriate Immunizations in a Rural Area of India
Abstract Objective: To study the effectiveness of planning and management interventions in improving
age appropriate immunization.
Methods: All 4336 children aged <18 month and 5213 children born during July 2005 to
December 2006 were enrolled from Khizrabad Block of Yamunanagar District in India.
Operational bottlenecks were evaluated by review of plans, staffing and stock position, and
condition of cold chain; observations of a sample of immunization sessions, and interview of
parents and health providers. An intervention package was evolved with community-based
volunteers as a pivotal strategy. Mean age at administration of DPT doses served as indicator of
age appropriate immunization. Chi square, t test and ANOVA were used to test statistical
differences before and after the interventions and for comparison with reference population.
Findings: Staff shortage, non-adherence to micro-plans and vaccine stock outs were the major
causes of delayed immunization. After intervention, coverage of third dose of DPT at the age of
6 month was significantly higher among post-intervention cohorts (70%) compared to pre-
intervention (62%). The mean age at administration of 1st, 2nd, and 3rd dose of DPT declined by
17, 21 and 34 days respectively in intervention area whereas no change occurred in hospitalized
children from non-intervention blocks. This corresponds to 21%, 16% and 18% decline over
baseline in mean age at administration of DPT1, 2 and 3 respectively in intervention area.
Conclusions: Better program planning and management can improve immunization
performance. Government of India’s decentralization policy for hiring of contractual staff and
2
community-based volunteers called Accredited Social Health Activists (ASHAs) is likely to
enhance age-appropriate immunization.
Key-words: immunization, age-appropriate, community volunteer, program management
3
Introduction
Communicable diseases kill more than 14 million people annually, predominantly in
developing world1. As of now, measles, pertussis and tetanus are the leading causes of disability
adjusted life years lost among childhood diseases2. Thirty million cases and 888,000 deaths
occur worldwide annually due to measles, of which 85% occur in South East Asia and Africa
regions3. Diphtheria too, has the potential to cause outbreaks especially in countries with low
vaccination coverage 4.
Despite the availability of safe and effective vaccines, the coverage of immunization
against six vaccine preventable diseases has remained variable in different regions of India5.
Beside the emphasis on enhancing the coverage for immunization, there is a need to administer
vaccines at the correct age as per the national immunization schedule to provide protection from
disease at the high risk age6. Numerous studies have documented immunization coverage and
recommended several strategies to enhance the coverage7-12. However, there have been limited
intervention studies to administer vaccines at appropriate age13. Present study was conducted
primarily to identify program interventions that can overcome operational barriers and improve
age-appropriate immunizations.
4
Materials and methods
Study area
This study was conducted in Khizrabad rural Community Development Block of
Yamunanagar district in Haryana state (India) from July 2005 to December 2006. Study district
was purposely chosen as immunization coverage for all currently administered vaccines at one
year of age was 78% 14, which was considered to be adequate coverage for introduction of Hib
vaccine. Out of the four blocks in this district, Khizrabad block was chosen since its geographic
location facilitated better patient access to study hospitals. The study was part of an Indian
Council of Medical Research and Johns Hopkins University Bloomberg School of Public Health
funded pilot project for studying the feasibility of estimating the preventable burden of
haemophilus influenzae type b (Hib) meningitis and pneumonia in India. A written informed
consent was taken from parents of all children who were enrolled in the study. The study was
approved by the Institutional Review Board of the Johns Hopkins University, Baltimore, USA
and the Institute Ethics Committee of Post Graduate Institute of Medical Education and
Research, Chandigarh, India.
In India, Primary Health Care system comprises of a Community Health Center (CHC) to
provide specialist services to 100,000 population while a Primary Health Centre (PHC) provides
preventive, curative, and promotive health care services to 30,000 population. PHC has 5-6
subcentres, each covering a population of 5000, where preventive, promotive and basic medical
care for minor illnesses are provided by multipurpose health workers male [MPHW(M)] and
female [MPHW(F)]. The study block had a network of one CHC, three PHCs and 25 sub centers
to provide health care to a population of 170,000 in 204 villages. Beside the staff of health
services, 155 primary child care workers (anganwadi) of the Integrated Child Development
5
Services Scheme were also available at village level (one for 1000 population) who also mobilize
community for nutritional and health interventions.
Planning, implementation and monitoring of immunization services in Yamunanagar
district is decentralized upto PHC level. The vaccines are stored for a period of three months at
district headquarters from where supplies are sent to CHC and PHCs which have facilities for
storage of vaccines for one month. Outreach sessions are held only once a week (conventionally
on a wednesday) by the subcentres in villages (at anganwadis) where vaccine storage equipment
is not available15. National immunization schedule in India envisages administration of one dose
of BCG at birth to 6 weeks and three doses of DPT and OPV at 6, 10 and 14 weeks respectively,
and measles vaccine is delivered at 9 months of age15.
Situational analysis
Completeness of enrollment of eligible children at subcentre level was ascertained by
comparing the births registered by MPHW(F) during April 2004-March 2005 with children
registered by a trained Community Volunteer (CV) in the corresponding period. This
comparison was done in 13 (52%) subcentres which had the same MPHW(F) working in that
subcentre for 2 consecutive years. Completeness of registration by CVs was validated by field
supervisors in 10% of the randomly selected households.
The study investigators supervised one outreach session in villages at each of the 25
subcentres using standard WHO supervisory checklist to identify problems in planning,
implementation and monitoring of immunization services16. Mothers of 527 children who had
dropped out after the first dose of DPT vaccine, i.e., had not turned up in the next session (one
month after the previous dose) were interviewed to ascertain the reasons for dropout. All the
MPHWs (F) in the block were interviewed to assess the number of sessions held during the
6
preceding month as against the planned number of sessions. Reasons for not holding a session on
the planned date and venue were assessed. Cold chain and vaccine logistics system was also
reviewed.
Intervention package
The results of situational analysis were discussed with district health authorities, CHC
and PHC medical officers and MPHW(F) in separate meetings. A strategy for improving
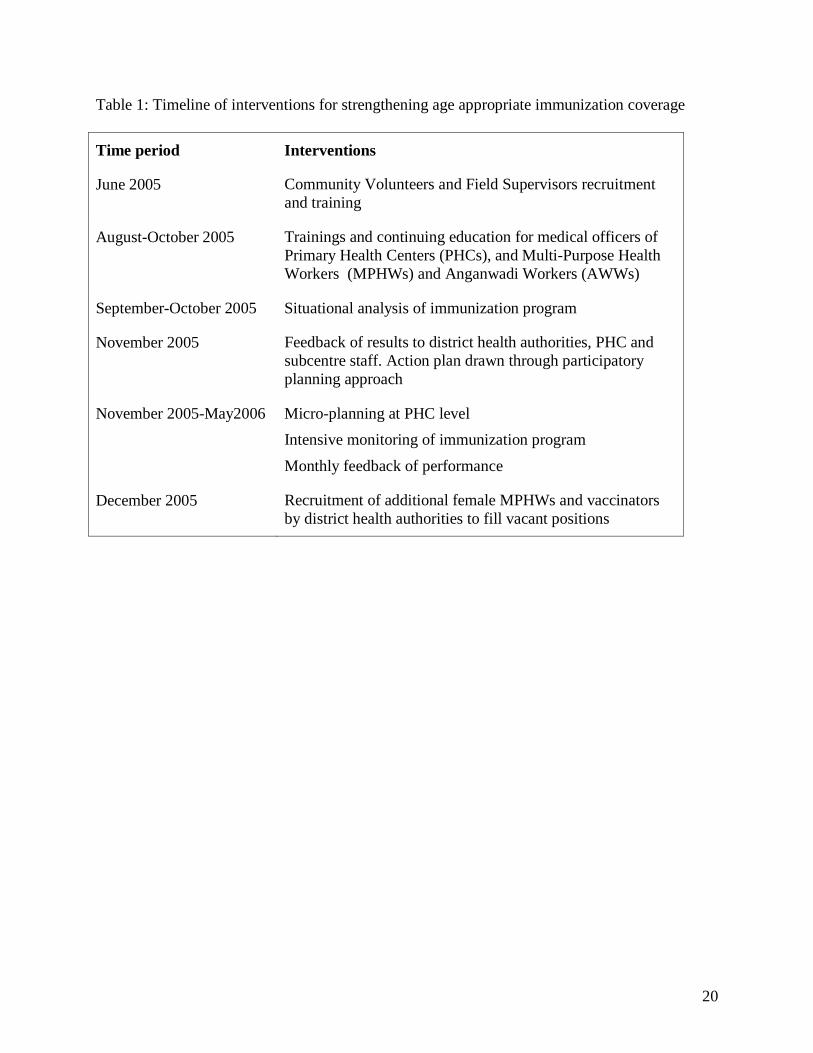
immunization program was jointly worked out (Table 1). Presence of CV as a community
mobilizer was designed as a pivotal part of the overall strategy. Twenty five CVs were recruited
at subcentre level who had minimum tenth grade education and were paid Rs.1000/- (US $25) 17
every month as honorarium for the part-time work. MPHW(F) were recruited on contract for
filling the vacant positions at subcentres. Additionally part-time vaccinators were hired to
supplement immunization activity at subcentre which had a vacancy due to transfer or temporary
absence of the MPHW(F) on a vaccination day. Comprehensive microplans at PHC level were
prepared describing the date, venue, vaccinator, number of clients, vaccine requirement, and
vaccine delivery mechanism for each session. Continuing education sessions were held for
doctors, health workers and anganwadi workers at PHC level highlighting the benefits of age
appropriate immunization. The investigators participated in the monthly review meetings of
program officers and PHC medical officers at district level, where previous month’s
immunization progress was presented and operational problems resolved.
Data collection
Community volunteers enrolled all children who were less than 18 months of age, maintained
log of pregnant women and prospectively enrolled all live births also during the study period
among permanent residents of the block. Past immunization status was recorded for children less
7
than 18 months of age at the time of initial enrolment. Subsequently, CVs recorded
immunization dates prospectively whenever children were vaccinated in the immunization
sessions. These records were submitted as a part of the weekly report. Each child was followed
up till 18 months age and a follow-up form was filled at attainment of the age of 24 months
wherein date for vaccines administered after enrolment were recorded again based on mother’s
recall. Follow-up form was used to test the accuracy of records collected by community
volunteer on a prospective basis. Discordance in data was verified and correct record was then
agreed upon by the field supervisors. Five full time field supervisors were recruited and posted at
PHC level for supervision of CVs. The immunization data of children of less than two years of
age who were admitted to 15 pediatric private and government hospitals from the entire district
was recorded by medical officers as a part of the pneumonia and meningitis surveillance activity.
A total of 4336 children under 18 months were registered at the start of the study and
5213 children were registered prospectively at births during the study period. Majority (99.3%)
of the mothers consented to participate in the study. Overall 1st, 2nd, and 3rd dose of DPT were
administered prospectively to 4810, 4775 and 4730 children during the study. A total of 814
children were admitted in the study hospitals from remaining blocks of Yamunanagar district.
According to their parent’s reports 1st, 2nd, 3rd dose of DPT had been administered to 477, 377
and 294 of them respectively.
Data Analysis
Enrolment and follow-up forms were scanned and converted to electronic format in Epi
Info (version 3.0) statistical software for analysis. Overall effectiveness of interventions was
assessed by comparing immunization coverage of children who had already started or completed
their immunization schedule at the time of enrolment in the study (pre-intervention cohort)
8
reflecting past performance of immunization program versus new births who were enrolled in the
study period before the start of scheduled immunization (post intervention cohort) reflecting the
impact of interventions. Mean of age (days) at the time of administration of different DPT doses
and mean gap (in days) between the DPT doses were compared between the two enrolment
cohorts described above. Similar analysis was done in hospitalized children from all the blocks
except the study block. They were divided into two groups, i.e. children who received
immunization before or after July 2005 (the date of introduction of interventions in the study
block). Chi square test and t-test were used for testing statistical significance of difference
between categorical and continuous variables respectively in the two groups.
The immunization data from weekly reports of CVs were also analyzed for six quarterly
immunization cohorts from July 2005 to December 2006. ANOVA test was used to test the
significance of trend of means over six quarters of the study period. Age-specific coverage of
DPT3 was also calculated in different enrolment cohorts, i.e., children enrolled before and after
receiving 1st dose of DPT.
9
Results
Though nearly 92% children had received third dose of DPT by the age of 12 months, but
only 19% received it by 4 month of age; the age by which every child should have receive it as
per the universal immunization schedule of India. Hence, a situational analysis was conducted to
identify operational barriers that need to be overcome to improve the age-appropriate
immunization coverage.
Operational Problems in the Delivery of Immunization Services
On an average MPHW(F) did not register 7.5% of the births. The percentage of missed
births was less in villages which had an anganwadi centre (0.5%) than those without it (17.2%).
Coverage of birth registration in villages was inversely related to distance from subcentre with
percentage of missed births ranging from 0.02% in subcentre villages or villages within 2 km
from the subcentre village to 9.5% in villages which were 2 to 5 km from subcentre and 8.2% in
villages which were more than 5 km away from the subcentre.
A review of vaccine logistics revealed that ice-lined refrigerators (ILR) and deep freezers
(DF) were not functional in two out of the four PHCs. Only one month requirement of vaccine
could be stocked at the district store due to inadequate storage space. Overall requirement of
ILRs and DFs in the district for storage of three month stock was deficient by 20%. There was
stockout of DPT vaccine during two months in the preceding year (2004-05) at district level.
Updated and comprehensive microplans were not available in PHCs. Sixteen (13.9%)
sessions planned during the preceding month were not held. Major reasons for 16 missed
sessions included monthly staff meeting at PHC scheduled on a day meant for immunization
(50%), vacant post of MPHW(F) (25%), decision taken by MPHW(F) to skip session while
another 12.5% sessions were not held as MPHW(F) was either on leave or away on training and
10
there was no one to replace her. Among sessions held, 23 (23.2%) sessions were not held on the
planned day. Reasons for 527 children who dropped out one month after DPT-1 included: ‘child
not at home on day of immunization’ (47.3%), ‘child not vaccinated due to minor illness’
(27.3%), ‘mother busy and nobody to bring the child to session’ (7%) and ‘session not held’ on
that day (4.6%). Among remaining 14% cases either vaccine was not available in the session or
mother had no information of session being held on that day.
Review of the situation led to the development and implementation of an intervention
package by the district health authorities which addressed the above mentioned operation
barriers. These interventions were found to be effective in improving the age-appropriate in the
study block.
Effectiveness of immunization program management interventions
The coverage of DPT 3rd dose by the age of 4, 6, and 9 month was significantly higher
among post-intervention enrolment cohort (22%, 70%, and 88%) compared to the pre-
intervention cohort (19%, 62%, and 85%) (p<0.001) with insignificant coverage at 12 months.
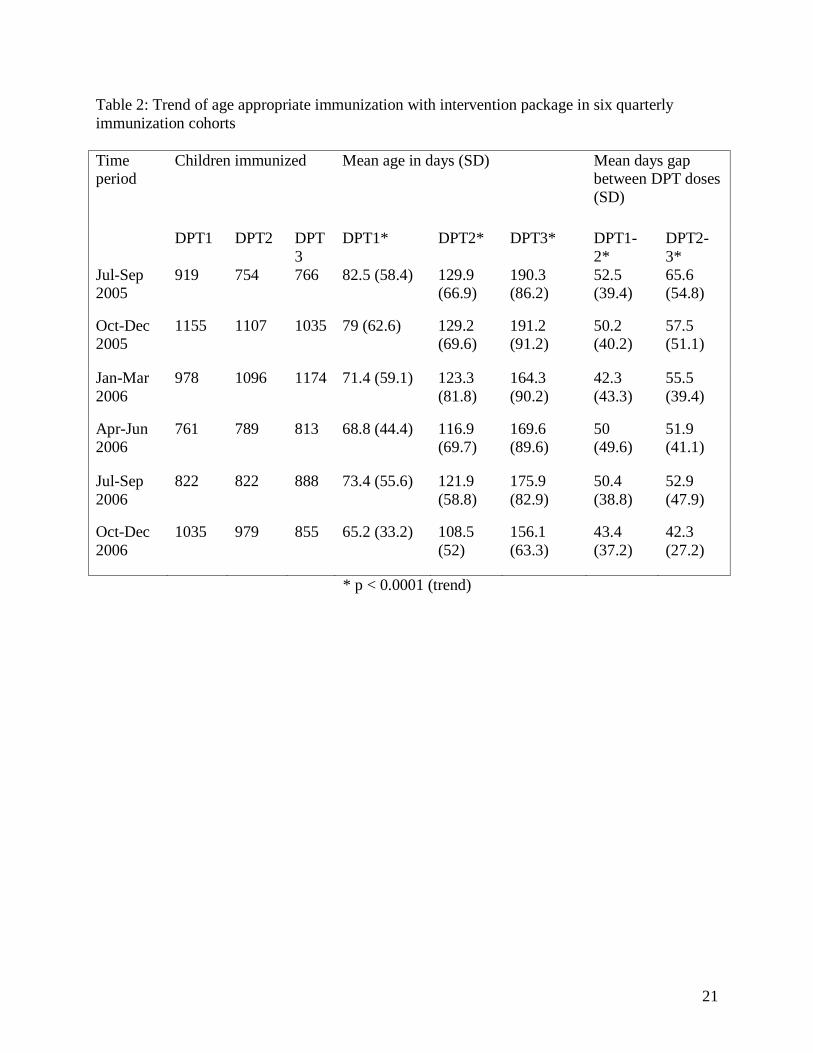
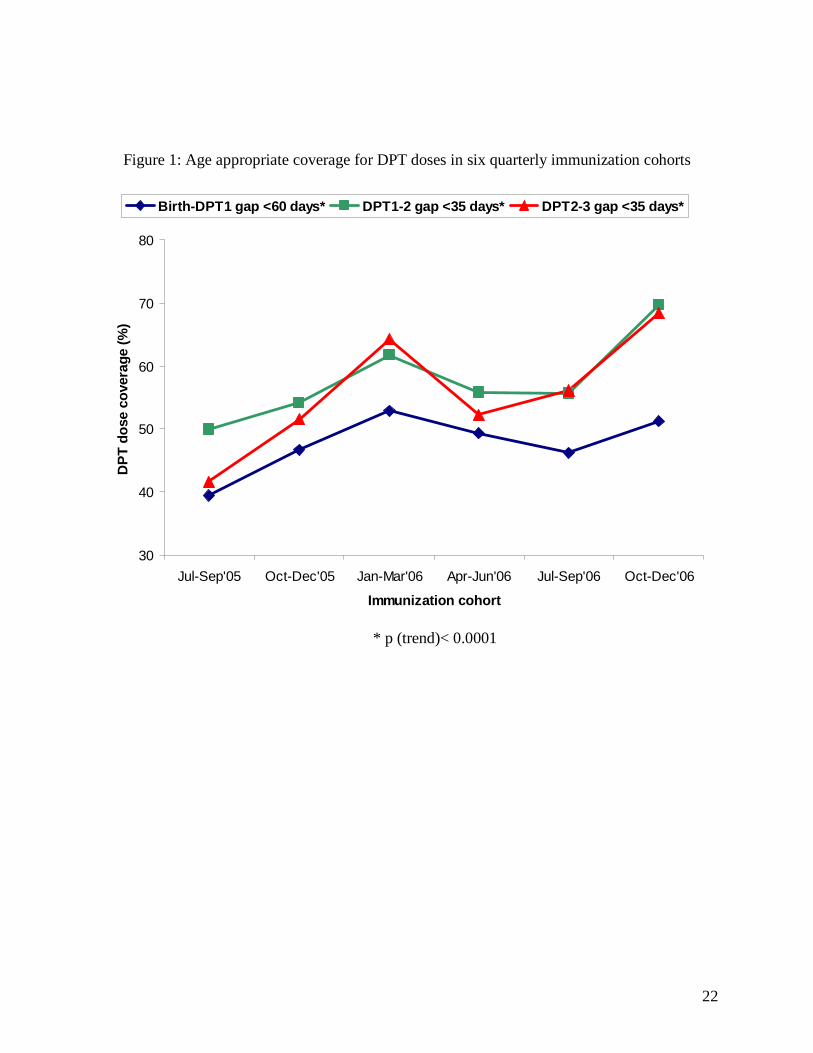
Statistically significant trend was observed in the lowering of the mean age of 1st, 2nd, and
3rd dose of DPT administration from first quarter of the study period (July-September 2005) to
the sixth quarter (October-December 2006) (p< 0.0001) (Table 2, Figure 1). The mean age at
administration of 1st, 2nd, and 3rd dose of DPT declined by 17, 21 and 34 days respectively in
intervention area whereas children admitted to study hospitals from rest of the district did not
show this trend. Mean age for DPT1 in hospitalized controls varied from 65.8 days to 68.9 days
from first to sixth immunization cohort, while it varied from 94.3 days to 129.7 days and 129.4
days to 121.7 days for DPT 2 and DPT3 respectively during the corresponding period.
11
Discussion
Immunization program in the study area was being monitored by assessment of coverage
of fully immunized children at one year of age. Periodic immunization evaluation surveys also
utilize this crude indicator to evaluate the overall performance of routine immunization
program18-20. The emphasis on coverage at one year of age is what drives the work of health
workers and medical officers. This was also evident in the present study area where the coverage
of 3rd dose of DPT was 92% at the age of 12 months but the coverage at 4 month was very low.
Benefits are greater if a child gets immunization at appropriate age especially so for
Haemophilus influenzae ‘b’ (Hib) and Pneumococcal vaccines. Governments are now including
these newer vaccines in their program, therefore, age-appropriate coverage should be made a
benchmark for assessment of the performance of immunization programs.
Major operational lacunae in the immunization programs are related to program
planning and management. The study findings demonstrate that better micro-planning along with
a responsive management information system (MIS) can improve program performance
significantly. Utilizing the data generated from routine MIS, the performance of program was
reviewed in monthly meetings at PHC, CHC and district level for finding solutions that can work
in the local conditions. MIS was used for actions rather than just for data transmission.
Higher than the expected workload also impede program implementation. The average
subcentre in the study area catered to a population of 6800, way above the national norm of
5000, with 12 (48%) subcentres having more than 8000 population. To compound the problem
further, there is shortage of MPHW(F). These findings are in conformity to another local study
21. Hiring of MPHW(F) on contract for subcentres to fill vacant posts, and employment of
additional vaccinators and community volunteers on part-time basis was possible due to the
12
decentralization and delegation of powers of recruitment at district level under the Reproductive
and Child Health II program 22. A related issue which also deserves mention is strengthening of
infrastructure for storage of vaccines and cold chain. This assumes greater importance as
Government of India intends to introduce newer vaccines such as Hib and Hep B.
Under-registration of births appears to be one of the reasons for the gap found in reported
and evaluated coverage of routine immunization services in various studies23-24. Birth registration
can be improved further by universalization of ICDS program in all areas and better intersectoral
coordination with anganwadi workers 25. This was evident in the present study with nearly
complete birth registration by MPHW(F) in villages which had an anganwadi.
Majority of the studies conducted for documenting immunization performance have
focused on overall coverage 7-12. We could not find any published research which estimated age
appropriate immunization coverage except one in grey literature 13. Many authors have however
tried to emphasize the importance of immunizing children for better protection against
pertussis26, measles 27 and haemophilus influenzae type ‘b’ 28.
Substantial drop outs occur after first dose for multi-dose vaccines (like DPT). Another
study from Delhi found similar magnitude of dropout from first to third dose of DPT with the
major reason being lack of information about the session29. This requires a major shift in the
behaviour change communication messages from ‘universal coverage’ to ‘universal timely
coverage’ for clients and in continuing education of health workers.
The study highlights several operational barriers that impede delivery of immunization at
appropriate ages in a developing country setting. However, as evident from the study, effective
tracking by community level workers, improved planning and monitoring of the program can
significantly improve age-appropriate immunization coverage (Table 2).
13
It is often difficult to conduct double blind randomized control trials for finding the
effectiveness of program management interventions. Before and after comparison in an
intervention area and a reference area can provide reasonable assurance about the validity of the
findings. However, it is difficult to find a comparable reference population and even if one finds
a comparable population, ethics committees find it hard to justify spending money only on data
collection in an area where interventions are not planned. Hence, this study utilized
immunization data from hospitalized children as a reference population rather than community
controls from rest of the district. Parents of children admitted in hospitals are likely to be having
better health seeking behaviour. This was reflected in overall better immunization coverage at
baseline in these children than in the children of the study area. However, the age at which
vaccines were administration in study area became lower after the intervention whereas no such
change was observed in the hospitalized children from the reference (non-intervention) area.
There was no difference in the health infrastructure, health indicators, socio-demographic
characteristics of people living in the study area and rest of the district. Absence of any
significant change in timeliness of immunization in the children who were hospitalized from rest
of the district adds strength to the validity of the study findings. The interventions were planned
and implemented within the health infrastructure, therefore, the possibility of replication in
similar settings in other areas is higher. Moreover, there was hardly any chance of selection bias
in this study as only a few parents (0.7%) had refused participation.
Although the mean age for administration of 2nd and 3rd dose of DPT was lowered by
several weeks but the age for 1st DPT dose did not register a significant change among new
births cohort (post-intervention group). The delay in administration of 1st dose is due to a strong
cultural practice in the study area; pregnant women go to their parental house for delivering the
14
first baby and return when the baby is about two month old. Health workers usually administer
vaccine only to the resident population for avoiding the drop out. A policy decision at the state
level is required so that irrespective of place of residence clients can access immunization at
place of migration also. Mothers should also be encouraged to get the child vaccinated wherever
the baby is delivered. It was difficult to administer the vaccine at the age specified in the
immunization schedule because outreach immunization sessions are held only once a month in
each village, which if missed, pushes up the age for initiation and subsequent immunization by
another month. The real impact of program interventions could be seen only in the sixth
immunization cohorts since all interventions could not be administered at a single point of time.
Complete implementation of intervention package was possible only in the third quarter of the
starting year (table 1).
This study was conducted in an area which had overall high rates of immunization
coverage by 12 months of age. Hence, similar results may not be achieved in areas which have
low immunization coverage rates. However, this does not preclude that the planning and
management intervention evolved in this study are not applicable to other areas, we believe that
these interventions would lead to enhanced immunization coverage first, followed by improved
timeliness. This is supported by WHO/UNICEF Global Immunisation and Vision Strategies
(GIVS) which recommend similar interventions 30 in both low and high income settings 31-33
This study demonstrates that decentralized planning and management improves program
performance which has major policy implications for various health programs. The role played
by CVs assumes importance considering the innovative cadre of Accredited Social Health
Activists (ASHA) introduced in India under the National Rural Health Mission (NRHM) 34. The
educational qualification and roles of these village-based volunteers are similar to that of CVs in
15
the present study. There is a renewed interest worldwide in the potential contribution which
community-based health workers can make in programs related to child survival 35. Their role is
especially pertinent where human resources are most lacking. Community-based workers are a
feasible and cost effective option and have the potential of reducing inequity by preferentially
reaching the poorest 36.
This study also has a major bearing on Government of India’s recent health sector
reforms of decentralization and devolution of administrative and financial powers under NRHM;
which provide flexibility at the district level and below for hiring staff on contract including
MPHW(F) and ASHA to meet demand for services. Local village level people can also be hired
to transport vaccine from the place of storage to the venue of outreach immunization session.
These recent initiatives are likely to increase overall and age-appropriate immunization coverage.
16
References
1. Heyman DL, (Ed). Control of Communicable Diseases Manual. 18th edn. Washington
DC. American Public Health Association; 2004: 21.
2. World Health Organization. Statistical Annex. The World Report 2004. WHO, Geneva.
2005: 127.
3. National Institute of Communicable Diseases. CD Alert- Measles continues to remain
major public health problem. New Delhi. 2000; 4(5): 1.
4. National Institute of Communicable Diseases. CD Alert- Diptheria. New Delhi. 1999;
3(4): 1.
5. IIPS (International Institute of Population Sciences) and Ministry of Health and Family
Welfare. India Summary Report Reproductive and Child Health district level household
survey (2002-04) and Facility survey (2003). Mumbai. IIPS.2006.
6. World Health Organization. Global program for vaccines and immunization. Expanded
program on immunizarion: immunization policy. Geneva. WHO GPV/GEN/95.03 Rev.1.
1995.
7. http://www.who.int/ immunization_monitoring/data/ India.pdf. Retrieved on 12-12-2006.
8. Jain SK, Chawla U, Gupta N, Gupta RS, Venketesh S, Lal S. Child survival and safe
motherhood program in Rajasthan. Indian J Pediatr. 2006; 73: 43-7.
9. Bonu S, Rani M, Baker TD. The impact of national polio immunization campaign on
levels of equity in immunization coverage: evidence from rural north India. Soc Sci Med.
2003; 57(10): 1807-19.
17
10. Mavimbe JCT, Muquingue HN, Braa J, Bjune G. Immunization coverage in
Mozambique- From concepts to decision making. Health Policy. 2006; 79(1): 92-100.
11. Robertson SE, Valedez JJ. Global review of health care surveys using lot quality
assurance sampling (LQAS), 1984-2004. Soc Sci and Med. 2006; 63(6): 1648-60.
12. Agarwal S, Bhanot A, Goindi G. Understanding and addressing childhood immunization
coverage in urban slums. Indian Pediatr. 2005; 42: 653-63.
13. Bhanot A, Agarwal S, Srivastava K. Improving age appropriate immunization
immunization among urban poor infants Possible options and approaches. United States
Agency for International Development, Urban Health Resource Centre. New Delhi. 2004.
14. Registrar General of India. Bulletin on Rural Health Statistics in India 2005. New Delhi;
Rural Health Division, Ministry of Health and Family Welfare. 2005.
15. Ministry of Health & Family Welfare. Manual on Community Needs Assessment
Approach (CNAA) in Family Welfare programme. New Delhi; Government of India.
January 1998.
16. Ministry of Health and Family Welfare. Immunization handbook for health workers. New
Delhi. Government of India. 2006.
17. Currency conversion website. http://www.xe.com/ucc/convert.cgi. Accessed on 16-12-
2007.
18. International Institute of Population Sciences and ORC Macro. National Family Health
Survey –1. Mumbai: International Institute of Population Sciences and ORC Macro.
1993.
18
19. International Institute of Population Sciences and ORC Macro. National Family Health
Survey –2. Mumbai: International Institute of Population Sciences and ORC Macro.
1998.
20. National Family Health Survey –3 factsheet. Retrieved from http://www.nfhs.org. on 12-
09-08.
21. Murthy N, Barna A. Integrating reproductive health in health programmes in India. In:
Gender, Population and Development. Eds. Krishnaraj M, Sudarshan RM, Sheriff A.
Oxford. Oxford University Press. 1998. p.291-309.
22. Ministry of Health and Family Welfare. Reproductive and Child Health Program RCH-II.
New Delhi. Government of India. 2002.
23. Singh J, Kumar A, Rai RN, Khare S, Jain DS, Bhatia R et al. Widespread outbreak of
measles in rural Uttar Pradesh, India, 1996: High risk areas and groups. Indian Pediatr.
1999; 36: 249-56.
24. Murray CJL, Shengelia B, Gupta M, Moussavi S, Tandon A, Thiereu M. Validity of
reported immunization coverage in 45 counrties. Lancet. 2003; 362(9389): 1022-7.
25. Lal S. Functioning of subcentres in the system of primary health care. Indian Journal of
Community Medicine. 2001; 26(2): 30-2.
26. Crowcroft NS, Stein C, Duclos P, Birmingham M. How best to estimate the globalburden
of pertussis? Lancet Infectious Diseases 2003; 3: 413-418
27. Dannetun E, Tegnell A, Hermansson G, Torner A, Giesecke J. Timeliness of MMR
vaccination – influence on vaccination coverage. Vaccine 2004; 22: 4228-4232.
28. Von Kries R, Bohm O, Windfuhr A, Haemophilus influenzae b-vaccination: the urgency for
timely vaccination. Eur J Pediatrics 1997; 156: 282-287.
19
29. Sokhey J, Jain DC, Harit AK, Dhariwal AC. Moderate immunization coverage levels in
East Delhi: implications for disease control programmes and introduction of new
vaccines. J Trop Pediatr. 2001; 47(4): 199-203.
30. GIVS Global Immunization Vision and Strategy 2006-2015. http://www.who.int/vaccines-
documents/DocsPDF05/GIVS_Final_EN.pdf (accessed 10 July 2007)
31. Domblowski KJ, Lantz PM, Freed GL. The need for surveillance of delay in age-
appropriate immunization. Am J Prev Med 2002; 23: 36-42.
32. Akmatov MK, Kretzchmar, Kramer A, Mikolajczyk RT, Timeliness of vaccination and
its effect on fraction of vaccinated population. Vaccine 2008; 26:3805-11
33. Hull BP, McIntyre PB. Timeliness of childhood immunisation in Australia. Vaccine 2006;
24:4403-8.
34. Ministry of Health and Family Welfare. National Rural Health Mission (2005-2012)
Mission Document. New Delhi. Government of India.2005.
35. Haines A, Sanders D, Lehmann U, Rowe AK, Lawn JE et al. Achieving child survival
goals: potential contribution of community health workers. Lancet. 2007; 369: 2121-31.
36. Knippenberg R, Lawn JE, Darmstadt GL, Begkoyian G, Fogstad H. Systematic scaling
up of neonatal care in countries. Lancet. 2005; 365: 1087–98.
20
Table 1: Timeline of interventions for strengthening age appropriate immunization coverage
Time period Interventions
June 2005 Community Volunteers and Field Supervisors recruitment and training
August-October 2005 Trainings and continuing education for medical officers of Primary Health Centers (PHCs), and Multi-Purpose Health Workers (MPHWs) and Anganwadi Workers (AWWs)
September-October 2005 Situational analysis of immunization program
November 2005 Feedback of results to district health authorities, PHC and subcentre staff. Action plan drawn through participatory planning approach
November 2005-May2006 Micro-planning at PHC level
Intensive monitoring of immunization program
Monthly feedback of performance
December 2005 Recruitment of additional female MPHWs and vaccinators by district health authorities to fill vacant positions
21
Table 2: Trend of age appropriate immunization with intervention package in six quarterly immunization cohorts Time period
Children immunized Mean age in days (SD) Mean days gap between DPT doses (SD)
DPT1 DPT2 DPT3
DPT1*
DPT2* DPT3* DPT1-2*
DPT2-3*
Jul-Sep 2005
919 754 766 82.5 (58.4) 129.9 (66.9)
190.3 (86.2)
52.5 (39.4)
65.6 (54.8)
Oct-Dec 2005
1155 1107 1035 79 (62.6) 129.2 (69.6)
191.2 (91.2)
50.2 (40.2)
57.5 (51.1)
Jan-Mar 2006
978 1096 1174 71.4 (59.1) 123.3 (81.8)
164.3 (90.2)
42.3 (43.3)
55.5 (39.4)
Apr-Jun 2006
761 789 813 68.8 (44.4) 116.9 (69.7)
169.6 (89.6)
50 (49.6)
51.9 (41.1)
Jul-Sep 2006
822 822 888 73.4 (55.6) 121.9 (58.8)
175.9 (82.9)
50.4 (38.8)
52.9 (47.9)
Oct-Dec 2006
1035 979 855 65.2 (33.2) 108.5 (52)
156.1 (63.3)
43.4 (37.2)
42.3 (27.2)
* p < 0.0001 (trend)
22
Figure 1: Age appropriate coverage for DPT doses in six quarterly immunization cohorts
30
40
50
60
70
80
Jul-Sep'05 Oct-Dec'05 Jan-Mar'06 Apr-Jun'06 Jul-Sep'06 Oct-Dec'06
Immunization cohort
DP
T d
ose
co
vera
ge (
%)
Birth-DPT1 gap <60 days* DPT1-2 gap <35 days* DPT2-3 gap <35 days*
* p (trend)< 0.0001





























