Embed Size (px)
Citation preview

Vol. XXXVII, no. 4, 2010 ISSN: 0390-6663
CLINICAL AND EXPERIMENTALOBSTETRICS & GYNECOLOGY
an International Journal
Editors-in-ChiefM. Marchetti J.H. CheckMontréal (CND) Camden, NJ (USA)
Assistant EditorJ. Wilson
San Diego - CA (USA)
Editorial Board
Publishing Organization (M. Morsani):I.R.O.G. CANADA, Inc. - 4900 Côte St-Luc - Apt # 212 - Montréal, Qué. H3W 2H3 (Canada)Tel. +514-4893242 - Fax +514-4854513 - E-mail: [email protected] - www.irog.net
Editorial Office (M. Critelli):Galleria Storione, 2/A - 35123 Padua (Italy) - Tel. (39) 049 8756900 - Fax (39) 049 8752018
CLINICAL AND EXPERIMENTAL OBSTETRICS AND GYNECOLOGY (ISSN 0390-6663) publishes original work, preferablybrief reports, in the fields of Gynecology, Obstetrics, Fetal Medicine, Gynecological Endocrinology and related subjects. (Fertilityand Sterility, Menopause, Uro-gynecology, Ultrasound in Obstetrics and Gynecology, Sexually Transmitted Diseases, ReproductiveBiological Section). The Journal is covered by INDEX MEDICUS, MEDLINE, EMBASE/Excerpta Medica.
CLINICAL AND EXPERIMENTAL OBSTETRICS AND GYNECOLOGY is issued every three months in onevolume per year by IROG CANADA Inc. Montréal. Printed in Italy by “La Garangola”, Tipografia Editrice - Via E. Dalla Costa, 6 -35129 Padova (Italy).
Audet-Lapointe P., Montréal (Canada)
Axt-Fliedner R., Lübeck (Germany)
Basta A., Krakow (Poland)
Bender H.J., Dusseldorf (Germany)
Bhattacharya N., Calcutta (India)
Bonilla Musoles F., Valencia (Spain)
Charkviani T., Tbilisi (Georgia)
Dexeus S., Barcelona (Spain)
Di Paola G., Buenos Aires (Argentina)
Eskes T.K.A.B.,Nijmegen (The Netherlands)
Franchi M., Verona (Italy)
Friedrich M., Homburg (Germany)
Gomel V., Vancouver (Canada)
Gorins A., Paris (France)
Grella P.V., Padua (Italy)
Holub Z., Kladno (Czech Republic)
Jordan J.A., Birmingham, England (UK)
Kaplan B., Petach Tikva (Israel)
Kralj B., Ljubljana (Slovenia)
Markowska J., Poznan (Poland)
Marth C., Innsbruck (Austria)
Meden-Vrtovec H., Ljubljana (Slovenia)
Ohara N., Kobe (Japan)
Papadopoulos N., Alexandroupolis (Greece)
Rakar S., Ljubljana (Slovenia)
Sciarra J.J., Chicago, IL (USA)
Stelmachow J., Warsaw (Poland)
Varras M.N., Athens (Greece)
Vîrtej P., Bucharest (Romania)
Winter R., Graz (Austria)
Founding EditorA. Onnis
Montréal (CND)

The multiple uses of ethinyl estradiol for treating infertilityJ.H. Check - Camden, NJ (USA)Ethinyl estradiol, a higher dosage estrogen preparation that does not contribute to serum estradiol, is useful for treating infertility.
A practical approach to the prevention of miscarriage: Part 4 - role of infectionJ.H. Check - Camden, NJ (USA)Evidence exists that both pathogenic and non-pathogenic bacteria can be the cause of pregnancy loss (more sporadic thanhabitual) and antibiotic therapy before and during pregnancy can improve outcome.
Acute intermittent porphyria in pregnancy: A common misdiagnosisA. Farfaras, F. Zagouri, G. Zografos, A. Kostopoulou, T.N. Sergentanis, S. Antoniou - Athens, GREECEPregnancy in women with AIP is associated with higher rates of spontaneous abortion and considerable mortality. Until clini-cal improvement is achieved, symptomatic treatment with hemin is recommended.
Reproductive Biology SectionPregnancy following calcium ionophore oocyte activation in an oligozoospermia patient with repeatedfailure of fertilization after ICSI
S. Sugaya - Joetsu City, JAPANA successful pregnancy outcome after calcium ionophore oocyte activation was achieved in an infertile couple that demonstrat-ed repeated failed fertilization after ICSI.
Artificial oocyte activation with calcium ionophore allowed fertilization and pregnancy in a couple withlong-term unexplained infertility where the female partner had diminished EGG reserve and failure tofertilize oocytes despite intracytoplasmic sperm injection
J.H. Check, D. Summers-Chase, R. Cohen, D. Brasile - Camden, NJ (USA)Fertilization of oocytes and pregnancy is possible in women with diminished egg reserve and previous history of failed fertil-ization by intracyoplasmic sperm injection by artificial oocyte activation with calcium ionophore.
General SectionImmediate and perioperative outcomes of polypropylene mesh in pelvic floor repair in a predominantlyobese population
T.O. Adedipe, S.J. Vine - Merthyr Tydfil, UKThe immediate perioperative outcomes of GPS use in transvaginal repairs of genital prolapse in a predominantly obese popula-tion are identified.
Relation between Doppler findings and perinatal outcomes in fetuses with intrauterine growthrestriction
M. Kazandi, C. Guven, F. Akercan, B. Zeybek, T. Cirpan, M. Ergenoglu, O. Yeniel, A. Akdemir, S. Ozsener -Izmir, TURKEYThe relationship between perinatal outcomes and fetal Doppler findings was investigated.
Impact of the medicalization of labor on mode of deliveryU. Indraccolo, S. Calabrese, R. Di Iorio, L. Corosu, E. Marinoni, S.R. Indraccolo - Rome, ITALYMedical interventions during labor cause a rise in operative delivery. The exception is epidural analgesia because it reducescesarean section.
EDITORIAL ARTICLES
ORIGINAL ARTICLES
REVIEW ARTICLE
249
252
256
261
263
266
269
273
Contents Clinical and Experimental Obstetrics & Gynecology - Vol. XXXVII, no. 4, 2010

247Contents
Maximizing the benefits of screening mammography for women 40-49 years oldK. Bastardis-Zakas, G. Iatrakis, I. Navrozoglou, P. Peitsidis, N. Salakos, P. Malakassis, S. Zervoudis -Athens, GREECEMeta-analysis indicating that the beneficial results of mammography screening on younger women depend greatly on the timeinterval between mammograms.
Multidisciplinary approach during menopausal transition and postmenopause in Brazilian womenI.C.E. Sorpreso, L.H.L. Vieira, M.A. Haidar, M.G. Nunes, E.C. Baracat, J.M. Soares Júnior - São Paulo,BRAZILMultidisciplinary management of menopause identifying clinical characteristics, nutritional habits, functional capacity andquality of life in Brazilian women.
Reproductive outcomes after hysteroscopic metroplasty for uterine septumF. Sendag, T. Mermer, S. Yucebilgın, K. Oztekin, O. Bilgin - Izmir, TURKEYHysteroscopic metroplasty for uterine septum improves pregnancy outcome in patients who have a desire to conceive.
Fertility sparing in young women with ovarian tumorsF. Ghaemmaghami, M. Karimi Zarchi, A. Naseri, A.S. Mousavi, M. Modarres Gilani, F. Ramezanzadeh, E.Rezaiof - Tehran, IRANConservative surgical management can be applied to young patients with a Stage I (grade 1, 2) epithelial ovarian tumor, a sexcord-stromal tumor and to patients with borderline and germ cell ovarian tumors.
Laparoscopic sacral colpopexy for uterine prolapse with prolene meshL. Hong, X. Xu, L. Chen, Q. Fu - Wuhan, CHINALaparoscopic sacral colpopexy with prolene mesh can effectively restore optimal vaginal function, anatomy and prevent pro-lapse recurrence.
Development of secondary ovarian lesions after hysterectomy without oophorectomy versus unilateraloophorectomy for benign conditions: A retrospective analysis of patients during a nine-year period ofobservation
A. Baloglu, I. Bezircioglu, B. Cetinkaya, L. Karcı, M. Bicer - Izmir, TURKEYWhen unilateral oophorectomy was performed at hysterectomy, the incidence of de novo ovarian pathology occurred moreoften than in hysterectomies performed without oophorectomy.
Unwanted pregnancy and induced abortion among young women 16-22 years old in Greece: a retrospective study of the risk factors
N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. Iavazzo - Athens, GREECEFactors like education and contraception among others, must be taken into strong consideration in order for unwanted pregnan-cies and induced abortions to be successfully confronted.
Conservative and surgical treatment of abnormal placentation: Report of five cases and review of theliterature
M. Kazandi - Izmir, TURKEYInvestigation of diagnostic tools, risk factors and treatment of placental adhesive disorders.
Abuse Assessment Screen (AAS) questionnaire: the Greek validationE. Antoniou, E. Ioannidi-Kapolou, M. Daglas, V. Vivilaki, D. Karamitros, V. Dafermos, G. Iatrakis - Athens,GREECEThe Greek version of the AAS questionnaire seems to be a reliable and valid tool for the diagnosis of violence during pregnancy.
Twin pregnancy after in vitro fertilization in a woman with a unicornuate uterusS. Sugaya - Joetsu City, JAPANThe successful outcome of a twin pregnancy after in vitro fertilization in a patient with unicornuate uterus was achieved withintensive obstetric management.
Clinical significance of procalcitonin in cervico-vaginal secretions of women with preterm rupture ofmembranes
U. Kuyumcuoglu, K. Kangal, A.I. Guzel, Y. Celik - Diyarbakir, TURKEYThe value of vaginal fluid procalcitonin determinations can be useful for diagnostics of PPROM with or without amnionitis.
278
283
287
290
295
299
303
310
313
317
319

Placental growth factor: a putative screening test for gestational diabetes mellitus in first trimester M. Kazandi, P.S. Hasdemir, B. Zeybek, A. Akcay - Izmir, TURKEYPlacental growth factor as a screening test for gestational diabetes was evaluated.
Haemophilus parainfluenzae infective endocarditis associated with pelvic abscess: an uncommoncomplication of endometriosis
T. Miquel-Goulenok, A. Le Tohic, J.J Laurichesse, B. Iung, C. Leport, P. Longuet - Paris, FRANCEThe case of a woman with a native mitral valve endocarditis due to Haemophilus parainfluenzae (HPI) associated with a pelvicabscess and endometriosis is reported.
A rare case of congenital pulmonary lymphangiectasia, hydrothorax and ascites in a male embryoaborted at 20 weeks of gestation
D. Hassiakos, K. Bakalianou, C. Iavazzo, A. Liapis, C. Dastamani, A. Kondi-Pafiti - Athens, GREECEA case of congenital pulmonary lymphangiectasia caracterized by hydrothorax and ascites was diagnosed by ultrasound.
Successful pregnancy after radiotherapy with 131I for differentiated thyroid cancer. A case report andreview of the literature
I. Grammatikakis, E. Trakakis, N. Evangelinakis, E. Hintipas, G. Salamalekis, D. Kassanos - Athens,GREECESuccessful pregnancy can follow an operative and complementary treatment of thyroid cancer.
Sequential methotrexate treatment with and estrogen and progestin in a retained adhesive placentaT. Mizuno, H. Takagi, K. Matsunami, A. Imai - Gifu, JAPANA successful case of conservative treatment with the use of estrogen and progestogen and of methotrexate in combination is pre-sented.
Contents index vol. XXXVII, 2010
Authors index vol. XXXVII, 2010
322
324
326
328
331
335
339
248 Contents
ERRATA - CORRIGEWhat kind of care and support do infertile women undergoing fertility treatment in Greece expect? A question-naire survey
K. Lykeridou, K. Gourounti, A. Sarantaki, Z. Roupa, G. Iatrakis, S. Zervoudis, G. Vaslamatzis - Athens, TURKEYProvision of information regarding medical and psychosocial aspects of infertility should be part of the routine care in fertility clinics.
Vol. XXXVII, n. 3, 2010, page 167
Errata: Athens, TURKEY
Corrige: Athens, GREECE
CASE REPORTS

249
Revised manuscript accepted for publication August 6, 2009
The multiple uses of ethinyl estradiol for treating infertility
J.H. CheckThe University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School at Camden,
Cooper Hospital/University Medical Center, Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology & Infertility, Camden, NJ (USA)
[1061/29]
Introduction
Ethinyl estradiol is one of the most consumed estrogen products in the world since it is the estrogen part of almostall oral contraceptives. Ethinyl estradiol without the progestin was distributed worldwide but eventually commercialproduction ceased by most pharmaceutical companies. Today it is only available as a commercial product in Germanyfrom Schering. The reason why production stopped was because of lack of use. However, it can still be compoundedby pharmacies if ordered.
I have been using ethinyl estradiol for 35 years and find it a very useful tool in treating infertility and use it fre-quently. This editorial will expound the various clinical uses for this drug when treating an infertile couple.
Cervical factor
A meta-analysis by Griffith and Grimes concluded that the postcoital test has poor validity as a diagnostic test forinfertility and encouraged physicians to abandon the test [1]. If the definition of a poor postcoital test is considered asthe absence of sperm with progressive forward motion in the cervical mucus, we found only 10% of patients conceivedover six months vs 74% who did demonstrate sperm with progressive forward motion in the mucus [2]. Similarly innatural cycles there was only a 3.4% pregnancy rate per cycle when there was no motile sperm in the mucus vs 21.2%with properly timed intrauterine insemination (IUI) [2]. Thus, I strongly believe that this simple inexpensive test shouldstill be performed even though today the frequency of abnormalities in women not taking clomiphene citrate is low(approximately 3%) [3].
The most common cause of a poor postcoital test today is the use of clomiphene citrate. Clomiphene citrate acts pre-dominantly like an anti-estrogen drug by binding to and eventually depleting nuclear estrogen receptor. The blockingof estrogen effect results in a lack of estrogen suppression of follicle stimulating hormone (FSH) leading to a rise inserum FSH which in turn causes ovulation. However, it also blocks the estrogen effect on cervical mucus. Sometimesthis negative effect on mucus can be negated by adding estrogen after clomiphene is stopped for the following five tonine days until ovulation is achieved. The reason for using ethinyl estradiol over other estrogen preparations is that itdoes not measure in the serum assay for 17 beta-E2 and thus the effect of clomiphene citrate on follicular maturationcan be better determined. Our group found in the first cycle of clomiphene citrate therapy that 69% (40/58) of thewomen failed to show any sperm in the cervical mucus with intercourse at least eight hours before in an appropriatelytimed postcoital test (based on ultrasound and serum E2 and progesterone criteria) [4].
In cycle 2, all 16 of the group of 18 who had a normal postcoital test in cycle 1 and did not conceive still had spermwith progressive motion in the cervical mucus, though half had ethinyl estradiol added as follicular maturationapproached because of an obvious decrease in amount and quality of the mucus [4].
SummaryPurpose: To demonstrate the usefulness of ethinyl estradiol, a drug no longer commercially produced in most countries, in treating
various fertility related issues. Methods: Twenty to 40 micrograms of ethinyl estradiol can be started on day 2 or 3 of the cycle andcombined with exogenous gonadotropin can be useful in improving hostile cervical mucus or inducing ovulation in women with hyper-gonadotropic amenorrhea. It can be used from the day after stopping clomiphene citrate to help negate the adverse effect of this drugon cervical mucus. Results: Successful pregnancies have been achieved saving the couple the expense of intrauterine insemination (IUI)or using donor oocytes. Conclusions: This drug can be very helpful for those physicians who treat each infertile woman on an individ-ual basis and carefully ascertain the couple’s input as to their preferences rather than a “herd” type of medicine.
Key words: Ethinyl estradiol; Postcoital test; Clomiphene citrate; Premature ovarian failure; Premature luteinization.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Editorial Articles

J.H. Check 250
Of the 40 patients with poor postcoital tests, 34 were given ethinyl estradiol after the clomiphene was stopped in adosage of either .02 or .05 mg until ovulation [4]. Only one of the six (16.7%) who did not have added supplementalestrogen showed sperm with linear progressive motion in the mucus vs 43.7% (7/16) taking .02 mg ethinyl estradioland 55.5% (10/18) using .05 mg ethinyl estradiol [4]. There were no pregnancies achieved in cycle 1 in the 40 womenwho had poor postcoital tests (IUI was not performed) vs 11.1% (2/18) who demonstrated sperm with linear progres-sive motion.
Of course one might argue why worry about whether the cervical mucus kills the sperm or not and just do intrauter-ine insemination (IUI). In fact a common practice among infertility specialists is to perform an IUI each month withouteven checking a postcoital test. Some of these infertility specialists quote the aforementioned meta-analysis stating thatthe postcoital test has no validity [1], with the assumption that the test has no validity. Others, including our group, donot agree and believe that the postcoital test is a valuable fertility tool [3, 5].
Rather than “waste” such a high amount of money, as mentioned, many physicians treating infertility automaticallydo an IUI. If we assume that a postcoital test costs $100 and it usually needs to be performed only one to two timesper patient, consider the immense costs of performing an IUI every month with prices ranging from $250 to $1,000each month, not just per patient. Even if the IUI is paid for by insurance carriers, performing this procedure monthly(especially since the majority will not need it) increases the cost of the healthcare. As mentioned above, adding ethinylestradiol after stopping clomiphene citrate until ovulation can improve cervical mucus in a significant percentage ofwomen taking clomiphene citrate without interfering with the measurement of estradiol. This is important in determin-ing if the use of clomiphene citrate has allowed the development of a mature follicle.
Clomiphene citrate is frequently prescribed by general gynecologists who do not have the facilities to perform anIUI. Adding ethinyl estradiol to the clomiphene citrate is even more important for these physicians since they could becreating iatrogenic infertility by inhibiting sperm getting to the uterine cavity. It is imperative that any doctor prescrib-ing clomiphene citrate should perform an appropriately timed postcoital test. If poor, and IUI is an option, this proce-dure can be performed in this cycle. However, the woman should be given the option of continuing with clomiphenecitrate and IUI or switching to gonadotropin injections which do not create poor quality mucus.
A woman may for various reasons have less sensitivity to estradiol so that poor quality mucus exists despite attain-ing an adequate mid-cycle serum estradiol. Of course the mucus glands are being exposed over a two-week course witha gradually rising serum estradiol. Ethinyl estradiol, as mentioned, is the component of the oral contraceptive that helpssuppress ovulation by inhibiting the release from the pituitary of follicle stimulating hormone (FSH). If ethinyl estra-diol is started from the early follicular phase in dosages of 20 to 40 μg the mucus glands will be exposed to a pharma-cologic dosage of estrogen. This can sometimes improve the quality of the mucus. However, the follicular maturationwould be thwarted by the ethinyl estradiol, but this could be counteracted by the concomitant use of gonadotropin stim-ulation [6]. Sometimes, the ethinyl estradiol can be added later in the follicular phase which may be too late to sup-press follicular maturation but could still improve mucus so exogenous FSH is not needed [7]. Alternatively a shortcourse of low-dose FSH could be added concomitant to the use of ethinyl estratiol which if the mucus abnormality iscorrected allows a better chance of monofollicular recruitment [8, 9].
Inducing ovulation in women with ovarian failure
In 1984 our group demonstrated that the use of higher dosage estrogen of any kind can help to recruit follicular mat-uration in women in apparent premature menopause [10]. The mechanism is related to restoring down-regulated FSHreceptors in the granulosa-theca cells by the chronic elevation of serum FSH. A reasonable pregnancy rate has beenachieved [10-14]. Though all estrogens can restore sensitivity of gonadotropin-resistant follicles to either endogenousor exogenous gonadotropins, the advantage of using ethinyl estradiol is that it allows proper measurement of estradiolwhich aids tremendously in determining if a mature follicle has been attained.
Extending the length of the follicular phase
Sometimes for religious reasons, e.g., Orthodox Jewish women, intercourse is not allowed until one week after thecessation of menses, after a ceremonial bath referred to as a mikvah. Some of these women are very fertile but fail toachieve a pregnancy because they are ovulating before they can have intercourse. Sometimes they are actually ovulat-ing on the day of the mikvah or even shortly thereafter, however the mucus may have receded several hours after theluteinizing hormone (LH) surge but before oocyte release.
There is evidence that a short follicular phase is associated with infertility even if a mature dominant follicle isattained [15, 16]. This seems to apply both to women whose short follicular maturation time may be related to dimin-ished oocyte reserve and thus higher early follicular phase FSH driving follicular maturation quicker, and to womenwho appear to have adequate oocyte reserves [16]. This may be related to inadequate time exposure to estradiol withfailure to generate sufficient endometrial progesterone receptors [16]. Lengthening the follicular phase with ethinylestradiol has resulted in improvement of pregnancy rates [16].
Sometimes ethinyl estradiol can be used from day 2 to day 8 or so, then stopped, and follicular maturation ensuesnaturally or sometimes a low dose of gonadotropins is needed to stimulate the follicles.

The multiple uses of ethinyl estradiol for treating infertility 251
Premature luteinization
A rise of LH before full maturation of the dominant follicle (i.e., 18-24 mm in size with a serum estradiol > 200pg/ml) leading to a rise in serum progesterone above 2 ng/ml is referred to as premature luteinization [17]. In thenormal ovulatory cycle in the late follicular phase estradiol has a positive feedback effect on LH release from the pitu-itary gland causing this hormone to rise. However, in pharmacologic dosages, estrogen will suppress LH. Thus fre-quently a condition, e.g., polycystic ovarian syndrome is treated with oral contraceptives to allow the pharmacologicdosage of ethinyl estradiol to lower the chronically elevated LH so as to reduce the production by the ovaries of excessandrogens. Ethinyl estradiol can be used in cases of premature luteinization to keep the gonadotropins suppressed andthen the follicle can be matured by using exogenous gonadotropins [18].
One could of course try to treat premature luteinization with GnRH agonists or antagonists. These agents are 100times as expensive as ethinyl estradiol.
Final comments
Ethinyl estradiol has many uses in treating infertile couples. However, it is unlikely that any pharmaceutical companywill rekindle an interest in commercial production because it is the common practice for most physicians to simply doIUI and not worry about postcoital tests. Furthermore, most physicians are not aware that apparent menopause can betemporarily reversed and will simply recommend donor oocytes. Nevertheless, for those treating physicians who haveinterests in these areas compounding pharmacies can easily make the ethinyl estradiol. I am not aware of another estro-gen product that does not measure in the assay for estradiol.
References[1] Griffith C.S., Grimes D.A.: “The validity of the postcoital test”. Am. J. Obstet. Gynecol., 1990, 162, 615.[2] Check J.H., Chase J.S., Spirito P.: “Efficacy of intrauterine insemination versus sexual relations versus intracervical insemination for treatment
of cervical factor infertility”. Am. J. Gynecol. Health., 1991, 5, 12.[3] Check J.H.: “The importance of the postcoital test”. Am. J. Obstet. Gynecol., 1991, 164, 932.[4] Check J.H., Adelson H.G., Davies E.: “Effect of clomiphene citrate therapy on postcoital tests in successive treatment cycles including response
to supplemental estrogen therapy”. Arch. Androl., 1994, 32, 69.[5] Hull M.G.R., Savage P.E., Bromham D.R.: “Prognostic value of the postcoital test: prospective study based on time-specific rates”. Br. J. Obstet.
Gynaecol., 1982, 89, 299.[6] Check J.H., Adelson H.G.: “Improvement of cervical factor by high dose estrogen and human menopausal gonadotropin therapy with ultra-
sound monitoring”. Obstet. Gynecol., 1984, 63, 179.[7] Check J.H., Chase J.S., Adelson H.G., Dietterich C.: “Diagnosis and treatment of the cervical factor. I. Improvement with a short course treat-
ment of high dose estrogen”. Int. J. Fertil., 1986, 31, 360.[8] Check J.H., Wu C.H., Dietterich C., Lauer C., Liss J.: “The treatment of cervical factor with ethinyl estradiol and human menopausal
gonadotropins”. Int. J. Fertil., 1986, 31, 148.[9] Check J.H., Dietterich C., Lauer C., Liss J.: “Ovulation inducing drugs versus specific mucus therapy for cervical factor”. Int. J. Fertil., 1991,
36, 108.[10] Check J.H., Chase J.S.: “Ovulation induction in hypergonadotropic amenorrhea with estrogen and human menopausal gonadotropin therapy”.
Fertil. Steril., 1984, 42, 919.[11] Check J.H., Nowroozi K., Chase J.S., Nazari A., Shapse D., Vaze M.: “Ovulation induction and pregnancies in 100 consecutive women with
hypergonadotropic amenorrhea”. Fertil. Steril., 1990, 53, 811.[12] Check J.H., Chase J.S., Wu C.H., Adelson H.G.: “Ovulation induction and pregnancy with an estrogen-gonadotropin stimulation technique in
a menopausal woman with marked hypoplastic ovaries”. Am. J. Obstet. Gynecol., 1989, 160, 405.[13] Check M.L., Check J.H., Kaplan H.: “Pregnancy despite imminent ovarian failure and extremely high endogenous gonadotropins and thera-
peutic strategies: Case report and review”. Clin. Exp. Obstet. Gynecol., 2004, 31, 299.[14] Check J.H., Katsoff B.: “Successful pregnancy with spontaneous ovulation in a woman with apparent premature ovarian failure who failed to
conceive despite four transfers of embryos derived from donated oocytes”. Clin. Exp. Obstet. Gynecol., 2006, 33, 13.[15] Check J.H., Adelson H., Lurie D., Jamison T.: “Effect of the short follicular phase on subsequent conception”. Gynecol. Obstet. Invest., 1992,
34, 180.[16] Check J.H., Liss J.R., Shucolski K., Check M.L.: “Effect of short follicular phase with follicular maturity on conception outcome”. Clin. Exp.
Obstet. Gynecol., 2003, 30, 195.[17] Check J.H., Chase J.S., Nowroozi K., Dietterich C.J.: “Premature luteinization Treatment and incidence in natural cycles”. Hum. Reprod.,
1991, 6, 190.[18] Check J.H., Wu C.H., Goldberg B.B., Kurtz A., Adelson H.G.: “High-dose estrogen to prevent premature spontaneous ovulation during hMG
therapy: Two case reports”. Infertility, 1984, 7, 45.
Address reprint requests to:J.H. CHECK, M.D., Ph.D.7447 Old York RoadMelrose Park, PA 19027 (USA)e-mail: [email protected]

252
[789/27]
Revised manuscript accepted for publication November 2, 2009
A practical approach to the prevention of miscarriagePart 4 - role of infection
J.H. CheckThe University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School at Camden,
Cooper Hospital/University Medical Center, Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology & Infertility, Camden, NJ (USA)
[1056/29]
Introduction
In our large population of women who have conceivedfollowing in vitro fertilization-embryo transfer (IVF-ET)aged 39.9 and under, irrespective of their previous infer-tility or miscarriage history or their status of ovarianoocyte reserve, there is approximately a 10% chance thata woman showing ultrasound evidence of pregnancy at 6-8 weeks will have a miscarriage. Accidental aneuploidyis the most common cause of a given miscarriage [1]. Itis debatable if a predisposition to aneuploidy exists or notbut if it does it is uncommon [2-4].
Nevertheless by chance alone a younger woman couldhave had two consecutive first trimester spontaneousabortions or miscarried in two of three pregnanciesrelated to two accidental aneuploidal fetuses. Theoreti-cally one in 100 women could lose two in a row from afactor that can not be controlled or prevented.
Prior editorials have discussed certain causes of spon-taneous abortion that are remediable, e.g., progesteronedeficiency. A woman presenting with frequent miscar-riages could have been unlucky and have had several dif-ferent etiologies to the various first trimester pregnancylosses. The frantic primary, secondary, or tertiary aborterwants to not only eradicate any of the causes of miscar-riage that she may be prone to have, e.g., need of extraprogesterone, but would like to prevent another loss fromany new etiology, especially if it is remediable.
Recurrent miscarriage is defined as three or more con-secutive miscarriages. It has been estimated to occur in0.5% to 3% of women [5]. There is little evidence thatpelvic infections are a cause of recurrent miscarriages.However, there are data suggesting that a first trimester
miscarriage or a loss later in the pregnancy can be relatedto an infectious etiology. This editorial will present someof the data suggesting that certain infections could resultin a loss of a pregnancy. As in most areas of medicinethere will be studies not finding an association. Neverthe-less after weighing the evidence I hope to present a strat-egy to cover the possibility of an infection leading to amiscarriage.
Microorganisms considered as possible causes of somemiscarriages or pregnancy loss
There are studies suggesting that the followingmicroorganisms may on some occasions lead to fetalloss: ureaplasma urealyticum, mycoplasma hominis,chlamydia trachomatis, a group of microorganismsresponsible for causing bacterial vaginosis, streptococ-cus, several bacteria in the clostridiales order, genitaltuberculosis, trichomonas vaginalis, neisseria gonor-rhoeae, listeria monocytogenes, cytomegalovirus (CMV),herpes simplex virus and toxoplasmosis [6].
Any one of these could cause a miscarriage but someare more likely candidates in any given miscarriage. Themore likely microorganisms will be discussed becausethey are the ones that lead to my final suggested strategy.I will emphasize that infection and miscarriage is a highlycontroversial area and there is no one strategy that can besaid to be the correct one. I will provide the studies thathave led me to my particular strategy but it should beemphasized that it is personal. Perhaps after presentingthe data and evidence the reader will decide on their ownstrategy different than mine.
Evaluation for infections
In all women coming to our practice for either infertil-ity or history of miscarriage we culture the cervix for
SummaryPurpose: To evaluate the role of infection as a cause of pregnancy loss. Methods: Studies concerning the risk factor of certain
microorganisms for first trimester miscarriage and premature rupture of membranes are reviewed. The microorganisms especiallyconsidered were ureaplasma/mycoplasma, the potpourri of organisms causing bacterial vaginosis and chlamydia trachomatis. Results:The consensus is that all these microorganisms can on occasion lead to first trimester spontaneous abortion and second trimester lossespecially related to premature rupture of membranes. Conclusions: Reactivation during pregnancy is possible so the best strategiesinvolve giving a course of appropriate antibiotics prior to pregnancy but giving antibiotics at least intermittently during the first trimester.Similar antibiotic therapy could be considered for unexplained recurrent miscarriage where negative cultures exist.
Key words: Spontaneous abortion; Bacteria; Premature rupture of membrane; Antibiotics.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

A practical approach to the prevention of miscarriage Part 4 - role of infection 253
mycoplasma, ureaplasma, gonorrhea, and chlamydia.Moreover vaginal cytology for bacterial vaginosis is eval-uated. For the subgroup of women who have a history ofmiscarriages, we also do a deep vaginal culture for GroupB streptococcus.
Culture positive for mycoplasma or ureaplasma
Not only do we culture the cervical fluid but we alsoculture the semen specimen. If either the female or malepartner tests positive we generally treat both partnerswith doxycycline 100 mg twice daily for two weeks.
We do not repeat the culture but instead with a positivepregnancy test begin treatment with either erythromycin500 mg four times a day or azithromycin 250 mg a dayfor a week then skip a week then resume on an alternateweek basis throughout the first trimester. I do not recul-ture after the initial two-week course of doxycyclinebecause it is hard to eradicate, thus giving a more pro-longed antibiotic course of therapy could lead to compli-cations, e.g., toxic bacterial enterocolitis or thrush.
I do not reculture necessarily when pregnancy occursbecause based on one positive culture I will nonethelessadd a macrolide drug to keep the infection in check. If therepeat culture of the cervix was negative I could not besure that it was still not present at the endometrial level.Also even if the cultures were negative at the moment inthe pregnancy they were obtained one can never tell whenthe concentration will become high enough again to dodamage. It is not practical to keep getting cultures on aweekly basis plus it may take ten days to growmycoplasma/ureaplasma. The male partner is only treatedonce but is advised to use condoms during the firsttrimester.
One study found that in pregnant women with avaginal discharge 49% cultured positive for U. ure-alyticum and an additional 14% were positive for M.hominis [7]. It is unlikely that all or even most womenthat culture positive for these organisms will lose apregnancy. However there are data suggesting thatwomen with enough concentration of these microorgan-isms to demonstrate a positive culture will have agreater pregnancy loss rate than those who are negative.Cervical colonization ureaplasma was found in 43% ofnormal pregnant women (n = 310), 42% of womenundergoing voluntary termination (n = 89), 41.5% ofnormal fertile women (n = 65), 53% of women withspontaneous abortion (n = 122), and 69.5% of womenwith recurrent miscarriage (n = 76) [8]. Another studyfound U. urealyticum and M. hominis in 74.1% and27.6% of 58 women with spontaneous abortion vs 48%and 10% of 50 women who had live deliveries [9].
Thus studies by Naessens et al. would suggest thattreating women with antibiotics who culture positive formycoplasma could reduce the risk of miscarriage [8].
One study did find an extremely high percentage (90%)of pregnancy loss in women whose cervical cultures werepositive for mycoplasma [10]. Using doxycycline onlyprior to conception reduced the miscarriage rate to 48%whereas using erythromycin in addition during preg-
nancy reduced the miscarriage rate to 15% and pretreat-ing with doxycycline then using erythromycin duringpregnancy resulted in a loss rate of 16% [10]. This was aprospective study though it is hard to believe thatuntreated controls could have a 90% loss rate. Neverthe-less, it is this study that has guided my decision to giveonly a two-week course of doxycycline rather than a pro-longed course prior to pregnancy and not to re-culture forthe microorganisms but always treat with a macrolide,eg., erythromycin or azithromycin at least during the timethat our practice is responsible for patient care, i.e., thefirst trimester.
Bacterial vaginosis (BV)
Bacterial vaginosis is an interesting condition in whichthe normal predominant type of bacteria that populatesthe vagina, i.e., lactobacilli, which reduces the vaginalpH by metabolizing squamous cell glycogen to lacticacid, is replaced by predominantly anerobic bacteria.Bacterial vaginosis is probably the most common causeof vaginal discharge; for some reason colonization withthese microorganisms does not cause an inflammatoryreaction so that is why it is given the name vaginosisrather than vaginitis. Actually sometimes mycoplasmaand ureaplasma can be the cause of BV but othercommon bacteria include Gardnerella vaginales, variousmobiluncus species, prevotella, porphyromonas, bac-teroides and peptostreptococcus.
Most commonly I identify BV by observing a fishyvaginal odor and confirm it by a wet smear of cells takenfrom the lateral vaginal wall demonstrating the adherenceof bacteria by a phase contrast microscope showing“shaggy” epithelial cells (so called clue-cells). Occasion-ally for borderline cases the diagnosis will be confirmedby the demonstration of a vaginal pH > 4.5 or eliciting afishy odor from the vaginal fluid by adding potassiumhydroxide.
Interesting, though the actual cause of BV is unknown,one study of infertile women undergoing IVF-ET foundthat BV was three times more likely to be present inwomen with tubal factor than women having IVF-ET forendometriosis, unexplained infertility or male factor [11].When lactobacilli are the predominant vaginal microor-ganism of the vagina the acidic pH helps provide protec-tion against infection. By replacing the flora with organ-isms associated with BV and raising the pH, the womanis at greater risk of infection whether BV vaginalmicroorganisms ascend and now inhabit the endometrialcavity (but since not evoking a host inflammatoryresponse so-called endometriosis) and directly in somemanner creates an adverse mileu leading to pregnancycomplications, or merely allows a more serious pathogento cause the problem, remains to be determined [12, 13].For example women may have colonization with chlamy-dia from previous exposure but host defenses are keepingit in check. The presence of BV could activate thechlamydia which in turn leads to pregnancy loss. Onestudy found that women with endometrial cultures that

J.H. Check 254
grow out chlamydia had a 59% miscarriage rate whereastreatment with antibiotics reduced the miscarriage rate tozero [14, 15]. Normally the uterine cavity is consideredrelatively sterile. However, studies performing endome-trial cultures have demonstrated the presence of patho-genic bacteria even in the presence of normal cervicalcultures [16].
Intravaginal or oral clindamycin treatment will help toeradicate BV [17, 18]. Metronidazole therapy was foundto be about as effective as clindamycin [19]. Metronida-zole therapy vs placebo showed marked reduction inpreterm labor and preterm births and also prematurerupture of membranes [19, 20]. Not all studies concurthat treating BV prevents pre-term deliveries. A Cochranemeta-analysis concluded that antibiotic treatment (betterwith oral than intravaginal) resulted in a trend for fewerbirths before 37 weeks gestation especially in thosewomen with a previous history of preterm births [21].
As far as miscarriages related to BV a large study of867 consecutive women undergoing IVF-ET found thatthere was no difference in the conception rate of the25% demonstrating BV vs the 75% without BV [22].However, the group with BV had a significantly highermiscarriage rate (32% vs 18.5%) with no obvious con-founding variables. Another study found that the presenceof BV significantly increased the risk of first trimesterbleeding [23].
Chlamydiae
One study reported a 60% miscarriage rate withchlamydiae cultured during pregnancy yet antibiotictreatment resulted in 100% full-term deliveries [14]. Inthat same study 42% of 163 women with recurrent mis-carriages cultured positive for chlamydiae [14]. Of coursethis prevalence will depend on the study population. Wepredominantly see private patients in our practice and weculture all women for chlamydia and rarely obtain a pos-itive culture.
The relationship of high titer IgG antibodies to C. tra-chomatis and miscarriage is controversial. One studyfound a three to four fold increased miscarriage rate inwomen with three or four previous miscarriages com-pared to controls with no history of miscarriage [24]. Theauthor suggested that the pregnancy could reactivatedormant chlamydial infection, thus causing the miscar-riage [24]. However other studies found no correlation[25-27].
History of miscarriage with negative cervical cultures
Supposing a woman presents with three consecutivemiscarriages with the karyotype of two of the abortusesfinding normal males. Suppose these last two miscar-riages occurred despite aggressive progesterone supportstarted in the luteal phase and continued throughout thefirst trimester. The women seeks your help to try toprevent another one. Furthermore, her uterine cavity wasdemonstrated to be normal by sonohysterogram and hys-teroscopy. Coagulation studies are normal.
Theoretically, the reason for the losses could beimmunological in nature or infectious. Immune issues arevery controversial. Nevertheless even if one does believethat immune therapy can be effective (I am one of thosereproductive endocrinologists who think some cases willbenefit from such therapy), the treatment is problematic.In the United States the Food and Drug Administrationrequires that investigational new drug approval (IND) beobtained prior to using lymphocyte immunotherapy (LIT)and the cost for this IND is about one million dollars.Thus no or few American centers perform this procedureand couples must go to Mexico for therapy. Intravenousimmunoglobulin is extremely expensive and for mostwomen cost-prohibitive.
If culture of the sperm or cervix demonstrates ure-aplasma/mycoplasma or clue-cells are seen in the wetsmear then one can hope that the pregnancy losses wererelated to an infectious etiology and the woman can betreated both before conception and during her firsttrimester.
However, what should the treating physician suggest ifall cervical and vaginal cultures are negative? Can aphysician and patient be sure that the endometrial cavitywas not overgrown with these microorganisms? Theanswer is no. Some of these microorganisms are fastidi-ous and may be present in the cervix but not grow out onculture explaining a negative culture. There is also thepossibility that they have colonized the endometrialcavity but are not present in the cervix. As mentioned,molecular genetics has allowed the detection of manyother types of bacteria in the vaginal flora and with cer-vical cultures for which there has not been developed asyet growth media [6].
Under these circumstances I will frequently empiri-cally prescribe erythromycin or azithromycin intermit-tently during the first trimester. Since some studies havefound ureaplasma and mycoplasma in about three-fourthsof women with miscarriages and it can develop at anytime I use the macrolides because they will cover themycoplasma and Group B streptococcus and they are safein pregnancy and generally well tolerated [9].
We previously found that when performing a fetalultrasound during the first trimester there was a high mis-carriage rate if the sac size was found to be more than oneweek earlier for gestational age than the crown-rumplength [28]. We considered the possibility that this phe-nomenon could be related to leakage of amniotic fluid byan infection. Our policy is to add a macrolide when wesee this occurrence even if repeat cultures for ureaplasmaand mycoplasma are negative. The exception would be ifwe find clue-cells on vaginal cytology when metronida-zole or tinidazole would be used instead. These agentswould be given intermittently. Since instituting thispolicy we have found a marked reduction in miscarriageswhen a crown-rump length/sac size discrepancy is found.These data are unpublished because our ethics committeerejected a proposal for a placebo control or no-treatmentcontrol.

A practical approach to the prevention of miscarriage Part 4 - role of infection 255
References[1] Rubio C., Simon C., Vidal F., Rodrigo L., Pehlivan T., Remohi J.,
Pellicer A.: “Chromosomal abnormalities and embryo develop-ment in recurrent miscarriage couples”. Hum. Reprod., 2003, 18,182.
[2] Sullivan A.E., Silver R.M., LaCoursiere D.Y., Porter T.F., BranchD.W.: “Recurrent fetal aneuploidy and recurrent miscarriage”.Obstet. Gynecol., 2004, 104, 784.
[3] Carp H.J.A., Dirnfeld M., Dor J., Grudzinskas J.G.: “ART inrecurrent miscarriage preimplantation genetic diagnosis/screeningor surrogacy?”. Hum. Reprod., 2004, 19, 1502.
[4] Cohen R., Check J.H.: “Recurrent aneuploidy - fact or fiction”.Clin. Exp. Obstet. Gynecol., in press
[5] Li T.C., Makris M., Tomsu M., Tuckerman E., Laird S.: “Recur-rent miscarriage: actiology, management and prognosis”. Hum.Reprod. Update, 2002, 8, 463.
[6] Fredricks D.N., Marrazzo J.M.: “Molecular methodology in deter-mining vaginal flora in health and disease: its time has come”.Curr. Infect. Dis. Rep., 2005, 7, 463.
[7] Di Bartolomeo S., Rodriquez M., Sauka D., Alberto De Torres R.:“Microbiologic profile in symptomatic pregnant women’s genitalsecretions in Gran Buenos Aires, Argentina”. Enform Infec. Micro-biol. Clin., 2001, 19, 99.
[8] Naessens A., Foulon W., Cammu H., Goossens A., Lauwers S.:“Epidemiology and pathogenesis of U. urealyticum in sponta-neous abortion and early preterm labor”. Acta Obstet. Gynecol.Scand., 1987, 66, 513.
[9] Ye L.L., Zhang B.Y., Cao W.L.: “Relationship between the endo-cervical mycoplasma infection and spontaneous abortion due toearly embryonic death”. Zhonghua Fu Chan Ke Za Zhi, 2004, 39,83.
[10] Quinn P.A., Shewchuk A.B., Shuber J., Lie K.I., Ryan E.,Chipman M.L., Nocilla D.M.: “Efficacy of antibiotic therapy inpreventing spontaneous pregnancy loss among couples colonizedwith genital mycoplasmas”. Am. J. Obstet. Gynecol., 1983, 145,239.
[11] Wilson J.D., Ralph S.G., Rutherford A.J.: “Rates of BV in womenundergoing in vitro fertilization for different types of infertility”.BJOG, 2002, 109, 714.
[12] Toth A., Lesser M.I., Brooks-Toth C.W., Feiner C.: “Outcome ofsubsequent pregnancies following antibiotic therapy after primaryor multiple spontaneous abortion”. Surg. Gynecol. Obstet., 1986,163, 243.
[13] Finiker D.A.: “Hypothesis on the role of sub-clinical bacteria ofthe endometrium (bacteria endometrialis) in gynecological andobstetric enigmas”. Hum. Reprod. Update, 1995, 373.
[14] Mezinova N.N., Chuchupalov P.D., Evdokimova N.S., FokhridinaL.I.: “Effect of antichlamydial drugs on the effectiveness of thetreatment of habitual abortion”. Akush. Ginekol. (Mosk), 1991, 7,30.
[15] Mezinova N.N., Chuchupalov P.D.: “Endometrial Chlamydiainfection in women with habitual abortion”. Akush. Ginekol.(Mosk), 1992, 2, 25.
[16] Lucisano A., Morandotti G., Marana R., Leone F., Branca G., Del-l’Acqua S., Sanna A.: “Chlamydial genital infections and laparo-scopic findings in infertile women”. Eur. J. Epidemiol., 1992, 8,645.
[17] Borisov I., Dimitrova V., Mazneikova V., Shopova E.: “Therapeu-tic regimens for treating bacterial vaginosis in pregnant women”.Akush. Ginekol. (Sofiia), 1999, 38, 14.
[18] Ugwumadu A., Reid F., Hay P., Manyonda I.: “Natural history ofbacterial vaginosis and intermediate flora in pregnancy and effectof oral clindamycin”. Obstet. Gynecol., 2004, 104, 114.
[19] Morales W.J., Schorr S., Albritton J.: “Effect of metronidazole inpatients with preterm birth in preceding pregnancy and bacterialvaginosis: a placebo-controlled, double blind study”. Am. J.Obstet. Gynecol., 1994, 171, 345.
[20] Camargo R.P., Simoes J.A., Cecatti J.G., Alves V.M., Faro S.:“Impact of treatment for bacterial vaginosis on prematurity amongBrazilian pregnant women: a retrospective cohort study”. SaoPaulo Med. J., 2005, 123, 108.
[21] Brocklehurst P., Hanna M., McDonald H.: “Intervention for treat-ing bacterial vaginosis in pregnancy”. Cochrane Database Syst.Rev., 2000, (2), CD00026.
[22] Ralph S.G., Rutherford A.J., Wilson J.D.: “Influence of bacterialvaginosis on conception and miscarriage in the first trimester:cohort study”. Br. Med. J., 1999, 319, 220.
[23] French J.I., McGregor J.A., Draper D., Parker R., McFee J.: “Ges-tational bleeding, bacterial vaginosis and common reproductivetract infections: risk for preterm birth and benefit of treatment”.Obstet. Gynecol., 1999, 93, 715.
[24] Witkin S.S., Ledger W.J.: “Antibodies to Chlamydia trachomaticin sera of women with recurrent spontaneous abortions”. Am. J.Obstet. Gynecol., 1992, 167, 135.
[25] Olliaro P., Regazzetti A., Gorini G., Milano F., Marchetti A., Ron-danelli E.G.: “Chlamydia trachomatis infection in ‘sine causa’recurrent abortion”. Boll. Ist. Sieroter Milan, 1991, 70, 467.
[26] Rae R., Smith I.W., Liston W.A., Kilpatrick D.C.: “Chlamydialserologic studies and recurrent spontaneous abortion”. Am. J.Obstet. Gynecol., 1994, 170, 782.
[27] Paukku M., Tulppala M., Puolakkainen M., Anttila T., PaavonenJ.: “Lack of association between serum antibodies to Chlamydiatrachomatis and a history of recurrent pregnancy loss”. Fertil.Steril., 199?, 72, 427.
[28] Nazari A., Check J.H., Epstein R., Dietterich C., Farzanfar S.:“Relationship of small for dates sac size to crown rump length andspontaneous abortion in patients with a known date of ovulation”.Obstet. Gynecol., 1991, 78, 369.
Address reprint requests to:J.H. CHECK, M.D., Ph.D.7447 Old York RoadMelrose Park, PA 19027 (USA)e-mail: [email protected]

256
[789/27]
Revised manuscript accepted for publication November 4, 2009
Acute intermittent porphyria in pregnancy:A common misdiagnosis
A. Farfaras1, F. Zagouri2, G. Zografos3, A. Kostopoulou3, T.N. Sergentanis3, S. Antoniou4
1Department of Gynecology, General Hospital of Athens, G. Gennimatas2Department of Clinical Therapeutics, Alexandra Hospital, Athens
3Department of Surgery, General Hospital of Athens, G. Gennimatas4Department of Cytology, General Hospital of Athens, Sotiria (Greece)
[1748/29]
Introduction
Acute intermittent porphyria (AIP) is a rare metabolicdisorder, inherited in an autosomal dominant fashion.Pregnancy represents an essential risk factor in patientssuffering from AIP. There are only limited reports dealingwith the incidence, the clinical presentation, the diagno-sis, the differential diagnosis and the treatment of patientswith AIP in pregnancy. It is this rarity that has resulted inthe increasing number of misdiagnoses of AIP.
This review article tries to disentangle different modal-ities concerning the management of patients with AIP inpregnancy and to keep physicians alert.
Classification of porphyria
The term porphyria refers to a group of rare, heteroge-neous, metabolic disorders arising from the reducedactivity of any of the enzymes in the heme biosyntheticpathway. Porphyrias can be classified as hepatic or ery-throid depending on the main site of the defect. They canalso be classified as either clinically acute: acute intermit-tent porphyria (AIP), hereditary coproporphyria (HCP),variegate porphyria (VP), ALA-dehydratase deficientporphyria (ADP), or cutaneous: porphyria cutanea tarda(PCT), hepatoerythropoietic porphyria (HEP), erythro-poietic protoporphyria (EPP), congenital erythropoieticporphyria (CEP) according to their major clinical mani-
festations [1-3]. With the exception of porphyria cutaneatarda, all porphyrias are attributed to inherited enzymedeficiencies and all hepatic porphyrias are acute. Someacute porphyrias may also display cutaneous manifesta-tions; however, cutaneous porphyrias never present acuteneurologic manifestations, with the exception of erythro-poietic protoporphyria in crisis [4].
Inheritance of AIP
AIP is inherited in an autosomal dominant fashion,caused by a deficiency in the enzyme uroporphyrinogenI synthetase, often called porphinobillinogen deaminase(PBG). The gene responsible for encoding this enzyme islocated on chromosome 11q24, and the coding sequencesare spread over 15 exons. So far, 301 mutations in thePBGD gene have been described [5]. The mutationsreported include single base substitutions, splicingdefects, insertions, and deletions that lead to structuralimpairment or loss of function of PBGD. As a conse-quence, the defect is unable to convert PBG to uropor-phyrinogen I [6-10].
The outcome of a mutation is a 50% decrease inenzyme activity. This explains the rarity of homozygotes,as a failure to produce hemin in this condition is incom-patible with life [1-11]. The remaining activity of theenzyme is usually sufficient. This could possibly justifywhy only 10% to 15% of the gene carriers have the clin-ical syndrome. Moreover, almost 33% of patients arereported with a family history of the disorder [12, 13].
SummaryAcute intermittent porphyria (AIP) is inherited in an autosomal dominant fashion. Only 10% to 15% of the gene carriers have the
clinical syndrome. The prevalence of AIP in Europe is 1/20,000. Pregnancy represents an essential risk factor in patients suffering fromAIP. The clinical syndrome in AIP presents mainly with acute attacks, especially during the first trimester. Misdiagnosis of AIP unfor-tunately is very common. Pregnancy in women with AIP is associated with higher rates of spontaneous abortion, hypertension, lowbirth weight infants and considerable mortality (2-42%). Pregnancy, despite the major hormonal alterations it causes, is seldom asso-ciated with porphyric symptoms. There are only limited reports supporting the use of hemin during pregnancy, but experience indicatesthat it can be safely administered in pregnant women. Until clinical improvement is achieved, symptomatic treatment is recommended.Despite the fact that pregnancy in women suffering from AIP is related to higher rates of morbidity and complications, close manage-ment throughout the pregnancy could ensure a good outcome.
Key words: Acute intermittent porphyria; Pregnancy; Hemin; Treatment; Acute attacks.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Review Article

Acute intermittent porphyria in pregnancy: A common misdiagnosis 257
Incidence of AIP
The prevalence of AIP in Europe is estimated to be onein 20,000 people. However, the frequency rates betweendifferent populations, ranging from 1.5 per 100,000Swedish people living in the USA and 3 per 100,000people in Finland and Western Australia, to 1 per 1,000people in Lapland Sweden, with clinical disease mani-festing in approximately 10% of these carriers. Peak ageof presentation is in the third decade [14-19]. Pregnancyrepresents an essential risk factor in patients sufferingfrom AIP. Acute attacks have been reported as being morecommon during pregnancy (24-95%), especially duringthe first trimester [20, 21].
Clinical presentation of AIP in pregnancy
The clinical syndrome in AIP presents mainly withacute attacks. Acute attacks are expected in cases wherethere is an increased demand for hepatic heme; com-monly when a precipitating factor occurs. In response,there is an induced synthesis of -aminolaevulinic acid(ALA) and overproduction of porphyrin precursors fol-lowing the synthetic pathway to the point at which thepartial enzyme deficiency becomes restrictive. Intermedi-ates, which have no known useful physiologic function,accumulate in the body. Precipitating factors that caninduce symptoms can be categorized as drugs, starvation,infection, and hormonal factors.
Endogenous hormones have been described as a vitalfactor in the induction and severity of acute attacks inpatients with AIP [22]. During pregnancy, there is amajor increase in sex hormone levels and on that basis,pregnancy has been thought to represent an essential riskfactor in patients suffering from AIP.
In fact, acute attacks have been reported as being morecommon during pregnancy (24-95%), especially during thefirst trimester, but pregnancy is generally well tolerated.However, pregnancy in women with AIP is associated withhigher rates of spontaneous abortion, hypertension and lowbirth weight infants [20, 21]. Furthermore, it is associatedwith considerable mortality (2-42%) [20]. Additionally, ithas been reported that smoking may be related to a worseoutcome of pregnancy in women with AIP. Smoking,which increases hepatic cytochrome P450 enzymes andpresumably heme synthesis, has also been shown to beassociated with a higher frequency of attacks [23].
On the other hand, it has been reported that pregnancy,despite the major hormonal alterations it causes, isseldom associated with porphyric symptoms and thatwith appropriate and close management, a good outcomecould be achieved [24-27].
At the hormonal level, progesterone variability maypartially explain why attacks are more common inwomen and during the luteal phase of the menstrual cycle[28, 29]. Moreover, oral estrogen intake is linked with ahigher incidence of acute attacks in women with AIP[30]. In addition, despite the fact that there is no differ-ence in AIP prevalence between genders, women seem to
suffer more often than men. The onset of menses is cor-related with a 10% to 20% higher incidence of acuteattacks in women with AIP [31, 32]. Furthermore, attacksare more frequent during childbearing years, with only afew cases having been described in women beforepuberty. Similarly, attacks are limited after menopause[33, 34]. The use of gonadotropin-releasing hormoneanalogue (GnRH) has been shown to protect women withAIP from cyclical attacks. GnRH use, after an initialperiod of stimulating gonadotrophin secretion, leads todown-regulation of pituitary function, reduced secretionof gonadotropins and, as a consequence, a drop in theendogenous sex-hormone levels [32, 33, 35, 36].
AIP is characterized by acute attacks of abdominalpain, which is present in 85% to 95% of patients. Abdom-inal pain is severe, diffuse and unremitting but typicallypresents without rebound tenderness or guarding.However, pain is frequently accompanied by nausea/vom-iting (43%-88%), constipation (48%-84%), tachycardia(80%) and occasionally by diarrhea (5%-12%). Lessoften, fever or leukocytosis may present, raising suspi-cion of acute surgical abdomen. However, despite theseverity of symptoms, clinical examination of theabdomen is normal in most cases, probably because thereis no peritonism [37]. Pain in the abdomen is believed tobe related to autonomic neuropathy, as is pain in theextremities, back, chest, neck or head that present in 50%to 70% of cases. Extremity pain indicates involvement ofthe sensory nerves, with objective sensory loss beingreported in 10% to 40% of patients [38-43].
Peripheral, motor neuropathy manifests early during anacute attack as muscle weakness (42%-68%). This weak-ness is usually symmetric, affecting the upper extremitiesmore often than lower and involving the proximalmuscles of the extremities. Fasciculation is absent anddeep tendon reflexes are lost in severe attacks. Weaknessmay progress to respiratory paralysis (8%-20%) More-over, seldom, the cranial nerves may be involved resem-bling Guillain Barre’ syndrome. Mental symptoms occurin 40% to 58% of patients, ranging from minor changesin behavior to agitation, confusion, hallucinations,depression, or even psychosis and schizophrenia [44-46].Psychiatric symptoms may present as the only manifesta-tion of AIP [47] and this is probably the explanation forthe higher prevalence of AIP in patients with psychiatricillness than in the general population [48-50].
Electrolyte disturbances are commonly found in AIP;hypokalemia, hyponatremia, hypomagnesemia,hypochloremia, azotemia and dehydration may becomesevere [51]. Seizures may present in up to 15% ofpatients, due to hyponatremia, which is often the result ofa syndrome of inappropriate antidiuretic hormone secre-tion (SIADH) or sodium depletion [52].
AIP is also related to chronic hypertension (36%-55%),despite the fact that hypotension may occur during acuteattacks. Renal impairment has also been described as along- term complication [53]. Furthermore, patients suf-fering from AIP are at higher risk of developing hepato-cellular carcinoma [54-60].

A. Farfaras, F. Zagouri, G. Zografos, A. Kostopoulou, T.N. Sergentanis, S. Antoniou 258
Risk factors of acute attacks
An acute attack of AIP may be precipitated by manyfactors during surgery and anesthesia, including fasting,dehydration, stress, infection, and drugs. Drugs used inanesthesia, many of which have high lipid solubility, andcytochrome metabolism have been implicated in thedevelopment of severe reactions in patients with AIP. Inemergency cases, without knowledge of the problem andfull biochemical examinations, the situation could wellbecome serious. Knowledge of the situation poses a hard-to-solve puzzle, in selection of the appropriate drugs andoperating management. Summaries of anesthetic drugs,known for their safety, have been published; however,there are also numerous conflicting reports [32]. Further-more, other factors such as stress or infections may pre-cipitate a porphyric crisis. On the other hand, availabilityof very short-acting anesthetic agents has led to theincreased safety of anesthetic techniques. However, itwould be fair to say that most analgesic agents may beused safely, despite the fact that some isolated casereports have implicated these drugs in porphyric attacks.Provided that reasonable precautions are adopted andsensible guidelines are followed, anesthesia may be con-sidered safe. Postoperative close monitoring should con-tinue for five days, to delay the onset of a porphyric crisis[61-74].
Diagnosis - differential diagnosis
Misdiagnosis of AIP unfortunately is very common,probably because of the rarity of the disease. When anacute attack of AIP is suspected, increased urinary por-phobilinogen levels are expected. However, due to thelow sensivity (40%-69%) and speciality (28%-53%) ofthe method, measurement of the 24-hour urinary excre-tion of porphobilinogen has become the first-line exami-nation. However, further evaluation is needed, in order todifferentiate between AIP, variegate porphyria and hered-itary coproporphyria. Erythrocyte porphobilinogen deam-inase activity is decreased up to 50% in almost 90% ofpatients. Additionally, urine porphyrin levels aremarkedly increased, while plasma and fecal porphyrinlevels remain normal or slightly elevated [75-81].
Due to its dominant mode of inheritance, it is prudentto screen relatives for acute porphyrins and to offerproper genetic counselling to family members at risk.When possible, diagnosis should be confirmed in child-hood to avoid the precipitating factors which may induceacute attacks after puberty. However, given the fact thatapproximately 50% of patients remain symptom-freethroughout their lives, 30-40% experience mild symp-toms and that the measuring of porphyrins and porphyrinprecursors in these individuals may give variable results,DNA analysis is the only reliable means to screensymptom-free patients. Despite the large number of pos-sible mutations, those reported are usually family spe-cific. Those members who are unaffected experiencegreat psychological relief as it is unnecessary for them to
follow the restrictions required to prevent attacks. More-over, screening of future generations of that particularfamily branch is not necessary [10, 13, 82].
Treatment of acute attacks of AIP
Hospitalization is required for treatment of acuteattacks of AIP. The primary objective is to identify andlimit any potential precipitating factors. Careful examina-tion for underlying infections must be performed. Initialtreatment comprises high glucose or intravenous heminintake. Glucose is clearly less effective and is recom-mended only for attacks with mild pain and without signsof paresis. Hemin acts by repressing hepatic ALA syn-thase activity, thus reducing the overproduction of ALAand porphobilinogen [83-90]. A response to hemetherapy is usually observed within one to four days afterthe start of infusion, but early initiation of intravenoushemin is associated with an earlier response andimproved outcome [91-94]. There are only limitedreports supporting the use of hemin during pregnancy, butexperience indicates that it can be safely administered inpregnant women [35].
Until clinical improvement is achieved, symptomatictreatment is recommended. One of the main objectivesshould be that of pain control. However, careful selectionof drugs allowed in pregnancy is paramount. Oral contra-ceptives have been shown to act as precipitating factors[34]. It is recommended that the use of sex hormones inwomen suffering from AIP is restricted. Notwithstanding,contraception is encouraged when adopting barriermethods.
Prevention of future attacks
Prevention of future attacks requires identification andavoidance of precipitating factors, preferably followed bychanges in habits. Prevention comprises adequate carbo-hydrate and high calorie diets, avoidance of exacerbatingdrugs, alcohol consumption, smoking, dehydration, psy-chological stress, sex hormone treatment and sensitivityto treatment of any infection. Moreover, the patientshould be forewarned that high estrogen concentrationsmay provoke attacks during pregnancy. Despite the factthat pregnancy in women suffering from AIP is related tohigher rates of morbidity and complications, close man-agement throughout the pregnancy could ensure a goodoutcome.
References[1] James M.F., Hift R.J.: “Porphyrias”. Br. J. Anaesth., 2000, 85, 143.[2] Gonzalez-Arriaza H.L., Bostwick J.M.: “Acute porphyrias: a case
report and review”. Am. J. Psych., 2003, 160, 450.[3] Anderson K.E., Bloomer J.R., Bonkovsky H.L., Kushner J.P.,
Pierach C.A., Pimstone N.R. et al.: “Recommendations for thediagnosis and treatment of the acute porphyrias”. Ann. Intern.Med., 2005, 142, 439.
[4] Rank J.M., Carithers R., Bloomer J.: “Evidence for neurologicaldysfunction in end-stage protoporphyric liver disease”. Hepatol-ogy, 1993, 18, 1404.

Acute intermittent porphyria in pregnancy: A common misdiagnosis 259
[5] Hrdinka M., Puy H., Martasek P.: “May 2006 update in porpho-bilinogen deaminase gene polymorphisms and mutations causingacute intermittent porphyria: comparison with the situation inSlavic population”. Physiol. Res., 2006, 55 (suppl. 2), S119.
[6] Di P.E., Besana V., Moriondo V., Brancaleoni V., Cappellini M.D.:“Gene symbol: HMBS. Disease: porphyria, acute intermittent”.Hum. Genet., 2006, 119, 364.
[7] Gouya L., Puy H., Robreau A.M., Lyoumi S., Lamoril J., Da S.V.et al.: “Modulation of penetrance by the wild-type allele in domi-nantly inherited erythropoietic protoporphyria and acute hepaticporphyrias”. Hum. Genet., 2004, 114, 256.
[8] Pischik E., Mehtala S., Kauppinen R.: “Nine mutations includingthree novel mutations among Russian patients with acute intermit-tent porphyria”. Hum. Mutat., 2005, 26, 496.
[9] Lam C.W., Poon P.M., Tong S.F., Lo A.W., Lai C.K., Choi K.L. etal.: “Novel mutation and polymorphisms of the HMBS genedetected by denaturing HPLC”. Clin. Chem., 2001, 47, 343.
[10] Kauppinen R., von und zu Fraunberg M.: “Molecular and bio-chemical studies of acute intermittent porphyria in 196 patientsand their families”. Clin. Chem., 2002, 48, 1891.
[11] Kappas A., Sassa S., Galbraith R.A., Nordmann Y.: “The por-phyrias”. In: Scriver C.R., Beaudet A.L., Sly W.S., Valle D.,Childs B., Kinzler K.W., Vogelstein B. (eds.). The Metabolic andMolecular Bases of Inherited Disease. 8th ed., McGraw-Hill, NewYork, 2001, 7012.
[12] Thadani H., Deacon A., Peters T.: “Diagnosis and management ofporphyria”. Br. Med. J., 2000, 320, 1647.
[13] Mattern S.E., Tefferi A.: “Acute porphyria: the cost of suspicion”.Am. J. Med., 1999, 107, 621.
[14] Goldberg A., Rimingron C.: “Diseases of porphyrin metabolism”.Springfield (IL): Charles C. Thomas, 1962.
[15] Thunell S., Floderus Y., Henrichson A., Harper P.: “Porphyria inSweden”. Physiol. Res., 2006, 55 (suppl. 2), S109.
[16] Scarlett Y.V., Brenner D.A.: “Porphyrias”. J. Clin. Gastroenterol.,1998, 27, 192.
[17] Sassa S., Kappas A.: “Molecular aspects of the inherited porphyr-ias”. J. Intern. Med., 2000, 247, 169.
[18] Burgovne K., Swartz R., Ananth J.: “Porphyria: reexamination ofpsychiatric implications”. Psychother. Psychosom., 1995, 64, 121.
[19] Regan L., Gonsalves L., Tesar G.: “Acute intermittent porphyria”.Psychosomatics, 1999, 40, 521.
[20] Kanaan C., Veille J.C., Lakin M.: “Pregnancy and acute intermit-tent porphyria”. Obstet. Gynecol. Surv., 1989, 44, 244.
[21] Kantor G., Rolbin S.H.: “Acute intermittent porphyria and cae-sarean delivery”. Can J. Anaesth., 1992, 39, 282.
[22] Dombeck T.A., Satonik R.C.: “The porphyrias”. Emerg. Med.Clin. North Am., 2005, 23, 885.
[23] Lip G.Y., McColl K.E., Goldberg A., Moore M.R.: “Smoking andrecurrent attacks of acute intermittent porphyria”. Br. Med. J.,1991, 302, 507.
[24] Wenger S., Meisinger V., Brucke T., Deecke L.: “Acute porphyricneuropathy during pregnancy-effect of haematin therapy”. Eur.Neurol., 1998, 39, 187.
[25] Pischik E., Kauppinen R.: “Can pregnancy stop cyclical attacks ofporphyria?”. Am. J. Med., 2006, 119, 88.
[26] Stickelmann P., Diedrich K., Pless V., Schlebusch H., Krebs D.:“Pregnancy and labor in acute intermittent porphyria”. GeburtshilfeFrauenheilkd, 1989, 49, 755.
[27] Milo R., Neuman M., Klein C., Caspi E., Arlazoroff A.: “Acute inter-mittent porphyria in pregnancy”. Obstet. Gynecol., 1989, 73, 450.
[28] Anderson K.E., Spitz I.M., Bardin C.W., Kappas A.: “Agonadotropin releasing hormone analogue prevents cyclicalattacks of porphyria”. Arch. Intern. Med., 1990, 15, 1469.
[29] De Block C.E., Leeuw I.H., Gaal L.F.: “Premenstrual attacks ofacute intermittent porphyria: hormonal and metabolic aspects - acase report”. Eur. J. Endocrinol., 1999, 141, 50.
[30] Andersson C., Innala E., Backstrom T.: “Acute intermittent por-phyria in women: clinical expression, use and experience ofexogenous sex hormones. A population-based study in northernSweden”. J. Intern. Med., 2003, 254, 176.
[31] Zimmerman T.S., McMillin J.M., Watson C.J.: “Onset of manifes-tations of hepatic porphyria in relation to the influence of femalesex hormones”. Arch. Intern. Med., 1966, 118, 229.
[32] Welland F.H., Hellman E.S., Collins A., Hunter G.W., TschudyD.P.: “Factors affecting the excretion of porphyrin precursors bypatients with acute intermittent porphyria. The effect of ethinylestradiol”. Metabolism, 1964, 13, 251.
[33] Jensen N.F., Fiddler D.S., Striepe V.: “Anesthetic considerations inporphyrias”. Anesth. Analg., 1995, 80, 591.
[34] Kauppinen R.: “Porphyrias”. Lancet, 2005, 365, 241.[35] Anderson K.E., Spitz I.M., Sassa S., Bardin C.W., Kappas A.:
“Prevention of cyclical attacks of acute intermittent porphyria witha long-acting agonist of luteinizing hormone-releasing hormone”.N. Engl. J. Med., 1984, 311, 643.
[36] McNulty S.J., Hardy K.J.: “Two patients with acute intermittentporphyria treated with nafarelin to prevent menstrual exacerba-tions”. J.R. Soc. Med., 2000, 93, 429.
[37] Eales L., Day R.S., Blekkenhorst G.H.: “The clinical and bio-chemical features of variegate porphyria: an analysis of 300 casesstudied at Groote Schuur Hospital, Cape Town”. Int. J. Biochem.,1980, 12, 837.
[38] Nordmann Y., Puy H.: “Human hereditary hepatic porphyrias”.Clin. Chim. Acta, 2002, 325, 17.
[39] Hardarson A., Rolfsson H.: “Severe abdominal pain and hypona-tremia was acute intermittent porphyria”. Lakartidningen, 2007,104, 1483.
[40] Palmer K.M.: “Abdominal pain due to acute intermittent por-phyria: when is the sound of hoof-beats not horses, but zebras? Acase report”. Dimens Crit Care Nurs., 2006, 25, 103.
[41] Mossner J.: “Acute abdomen”. Internist. (Berl.), 2005, 46, 974.[42] Mogos D., Guran M., Marinescu S., Firescu M., Teodorescu M.,
Marinescu A.G. et al.: “False surgical acute abdomen with inter-mittent acute porphyria”. Chirurgia (Bucur), 2004, 99, 247.
[43] Rosland J.H.: “Recurrent abdominal pain caused by acute inter-mittent porphyria”. Tidsskr Nor Laegeforen, 2001, 121, 2818.
[44] Elder G.H., Hift R.J., Meissner P.N.: “The acute porphyrias”.Lancet, 1997, 349, 1613.
[45] Gonzalez-Arriaza H.L., Bostwick J.M.: “Acute porphyrias: a casereport and review”. Am. J.. Psychiatry, 2003, 160, 450.
[46] Burgovne K., Swartz R., Ananth J.: “Porphyria: reexamination ofpsychiatric implications”. Psychother. Psychosom., 1995, 64, 121.
[47] Ellencweig N., Schoenfeld N., Zemishlany Z.: “Acute intermittentporphyria: psychosis as the only clinical manifestation”. Isr. J.Psychiatry Relat. Sci., 2006, 43, 52.
[48] Tishler P.V., Woodward B., O’Connor J., Holbrook D.A., SeidmanL.J., Hallett M. et al.: “High prevalence of intermittent acute por-phyria in a psychiatric patient population”. Am. J. Psychiatry,1985, 142, 1430.
[49] Santosh P.J., Malhotra S.: “Varied psychiatric manifestations ofacute intermittent porphyria”. Biol. Psychiatry, 1994, 36, 744.
[50] McEwin R., Lawn J., Jonas C.T.: “A survey of porphyria amongpsychiatric patients”. Med. J. Aust., 1972, 5, 303.
[51] Disler P.B., Eales L.: “The acute attack of porphyria”. S. Afr. Med.J., 1982, 16, 82.
[52] Bonkowsky H.L., Schady W.: “Neurologic manifestations of acuteporphyria”. Semin. Liver Dis., 1982, 2, 108.
[53] Church S.E., McColl K.E., Moore M.R., Youngs G.R.: “Hyperten-sion and renal impairment as complications of acute porphyria”.Nephrol. Dial Transplant, 1992, 7, 986.
[54] Ostrowski J., Kostrzewska E., Michalak T., Zawirska B., Medrze-jewski W., Gregor A.: “Abnormalities in liver function and mor-phology and impaired aminopyrine metabolism in hereditaryhepatic porphyrias”. Gastroenterology, 1983, 85, 1131.
[55] Lithner F., Wetterberg L.: “Hepatocellular carcinoma in patientswith acute intermittent porphyria”. Acta Med. Scand., 1984, 215,271.
[56] Kauppinen R., Mustajoki P.: “Acute hepatic porphyria and hepato-cellular carcinoma”. Br. J. Cancer, 1988, 57, 117.
[57] Andersson C., Bjersing L., Lithner F.: “The epidemiology of hepa-tocellular carcinoma in patients with acute intermittent porphyria”.J. Intern. Med., 1996, 240, 195.
[58] Bjersing L., Andersson C., Lithner F.: “Hepatocellular carcinomain patients from northern Sweden with acute intermittent por-phyria: morphology and mutations”. Cancer Epidemiol. Biomark-ers Prev., 1996, 5, 393.
[59] Andant C., Puy H., Faivre J., Deybach J.C.: “Acute hepatic porphyr-ias and primary liver cancer”. N. Engl. J. Med., 1998, 338, 1853.

A. Farfaras, F. Zagouri, G. Zografos, A. Kostopoulou, T.N. Sergentanis, S. Antoniou 260
[60] Linet M.S., Gridley G., Nyren O., Mellemkjaer L., Olsen J.H.,Keehn S. et al.: “Primary liver cancer, other malignancies, andmortality risks following porphyria: a cohort study in Denmarkand Sweden”. Am. J. Epidemiol., 1999, 149, 1010.
[61] Harrison G.G., Meissner P.N., Hift R.J.: “Anaesthesia for the por-phyric patient”. Anaesthesia, 1993, 48, 417.
[62] Ashley E.M.: “Anaesthesia for porphyria”. Br. J. Hosp. Med.,1996, 56, 37.
[63] Bohrer H., Schmidt H.: “Regional anesthesia as anesthetic tech-nique of choice in acute hepatic porphyria”. J. Clin. Anesth., 1992,4, 259.
[64] Elcock D., Norris A.: “Elevated porphyrins following propofolanaesthesia in acute intermittent porphyria”. Anaesthesia, 1994,49, 957.
[65] Hughes P.J.: “Propofol in acute porphyrias”. Anaesthesia, 1990,45, 415.
[66] Jensen N.F., Fiddler D.S., Striepe V.: “Anesthetic considerations inporphyrias”. Anesth. Analg., 1995, 80, 591.
[67] Rushman G.B., Jooste C.A.: “Anaesthesia for the porphyricpatient”. Anaesthesia, 1993, 48, 1009.
[68] Hsieh C.H., Hung P.C., Chien C.T., Shih Y.R., Peng S.K., LukH.N. et al.: “The use of rocuronium and sevoflurane in acute inter-mittent porphyria-a case report”. Acta Anaesthesiol. Taiwan,2006, 44, 169.
[69] Aragones N., Costa A., Pardina B., Metje M.T., Estanyol N., Vil-lalonga A.: “Anesthesia in a woman with acute abdomen and inter-mittent acute porphyria”. Rev. Esp. Anestesiol. Reanim., 2005, 52,118.
[70] Kunitz O., Frank J.: “Anesthesiologic management of patientswith acute porphyria”. Anaesthesist., 2001, 50, 957.
[71] Campos J.H., Stein D.K., Michel M.K., Moyers J.R.: “Anesthesiafor aortic valve replacement in a patient with acute intermittentporphyria”. J. Cardiothorac. Vasc. Anesth., 1991, 5, 258.
[72] Deybach J.C., Da S.V., Phung L.N., Levy J.C., Nordmann Y.:“Drug risk of hepatic porphyria. Development of an animal exper-iment model”. Presse Med., 1987, 16, 68.
[73] Sneyd J.R., Kreimer-Birnbaum M., Lust M.R., Heflin J.: “Use ofsufentanil and atracurium anesthesia in a patient with acute por-phyria undergoing coronary artery bypass surgery”. J. Cardiotho-rac Vasc. Anesth., 1995, 9, 75.
[74] Stevens J.J., Kneeshaw J.D.: “Mitral valve replacement in a patientwith acute intermittent porphyria”. Anesth. Analg., 1996, 82, 416.
[75] Bonkovsky H.L., Barnard G.F.: “Diagnosis of porphyric syn-dromes: a practical approach in the era of molecular biology”.Semin Liver Dis., 1998, 18, 57.
[76] Deacon A.C., Peters T.J.: “Identification of acute porphyria: eval-uation of a commercial screening test for urinary porphobilino-gen”. Ann. Clin. Biochem., 1998, 35, 726.
[77] Tefferi A., Colgan J.P., Solberg L.A. Jr.: “Acute porphyrias: diag-nosis and management”. Mayo Clin. Proc., 1994, 69, 991.
[78] Hindmarsh J.T.: “The porphyrias, appropriate test selection”. Clin.Chim. Acta, 2003, 333, 203.
[79] Hindmarsh J.T., Oliveras L., Greenway D.C.: “Biochemical differ-entiation of the porphyrias”. Clin. Biochem., 1999, 32, 609.
[80] Herrick A.L., McColl K.E.: “Lack of certainty on the diagnosis ofacute intermittent porphyria: comment on the concise communica-tion by Cohen et al.”. Arthritis Rheum., 1998, 41, 188.
[81] Buttery J.E., Carrera A.M., Pannall P.R.: “Reliability of the por-phobilinogen screening assay”. Pathology, 1990, 22, 197.
[82] Kauppinen R., Mustajoki P.: “Prognosis of acute porphyria: occur-rence of acute attacks, precipitating factors, and associated dis-eases”. Medicine (Baltimore), 1992, 71, 1.
[83] Watson C.J., Pierach C.A., Bossenmaier I., Cardinal R.: “Postu-lated deficiency of hepatic heme and repair by hematin infusionsin the "inducible" hepatic porphyrias”. Proc. Natl. Acad. Sci USA,1977, 74, 2118.
[84] Watson C.J., Pierach C.A., Bossenmaier I., Cardinal R.: “Use ofhematin in the acute attack of the "inducible" hepatic prophyrias”.Adv. Intern. Med., 1978, 23, 265.
[85] Pierach C.A., Bossenmaier I., Cardinal R., Weimer M., WatsonC.J.: “Hematin therapy in porphyric attacks”. Klin. Wochenschr.,1980, 58, 829.
[86] Kostrzewska E., Gregor A., Tarczynska-Nosal S.: “Heme arginate(Normosang) in the treatment of attacks of acute hepatic porphyr-ias”. Mater. Med. Pol., 1991, 23, 259.
[87] Herrick A.L., McColl K.E., Moore M.R., Cook A., Goldberg A.:“Controlled trial of haem arginate in acute hepatic porphyria”.Lancet, 1989, 1, 1295.
[88] Kostrzewska E., Gregor A.: “Acute hepatic porphyrias. Detection,prophylaxis and treatment”. Mater Med. Pol., 1996, 28, 5.
[89] McColl K.E., Moore M.R., Thompson G.G., Goldberg A.: “Treat-ment with haematin in acute hepatic porphyria”. Q.J. Med., 1981,50, 161.
[90] Mustajoki P., Tenhunen R., Tokola O., Gothoni G.: “Haemarginate in the treatment of acute hepatic porphyrias”. Br. Med. J.(Clin Res Ed), 1986, 293, 538.
[91] Mustajoki P., Nordmann Y.: “Early administration of hemearginate for acute porphyric attacks”. Arch. Intern. Med., 1993,153, 2004.
[92] Nordmann Y., Deybach J.C.: “Acute attacks of hepatic porphyria:specific treatment with heme arginate”. Ann. Med. Interne (Paris),1993, 144, 165.
[93] Pierach C.A.: “Hematin therapy for the porphyric attack”. SeminLiver Dis., 1982, 2, 125.
[94] Elder G.H., Hift R.J., Meissner P.N.: “The acute porphyrias”.Lancet, 1997, 349, 1613.
Address reprint requests to:F. ZAGOURI, M.D., Ph.D.23 Irakleous str., 17671Athens (Greece)e-mail: [email protected]

261
Revised manuscript accepted for publication February 11, 2010
Pregnancy following calcium ionophore oocyte activation in an oligozoospermia patient with repeated failure of
fertilization after ICSI
S. SugayaDepartment of Obstetrics and Gynecology, Niigata Workmen’s Accident Hospital, Joetsu City (Japan)
[1082/30]
Introduction
Intracytoplasmic sperm injection (ICSI) is an extreme-ly useful method of treating patients who have anextremely low sperm count, and it has been reported thatthe fertilization rate after ICSI is 64% to 71% [1, 2].Conversely, it has been reported that 3% of all cycles areobserved to result in no fertilized oocyte, despite the per-formance of ICSI [3, 4].
One cause of fertilization failure after ICSI is believedto be oocyte activation failure attributable to the sperm.Correspondingly, it has recently been reported that fertil-ization can be achieved by using calcium ionophore toactivate the oocyte, thereby obtaining favorable results [5-8]. A case of secondary infertility is reported in which fer-tilization had not been achieved despite the performanceof ICSI but wherein fertilization was achieved by usingcalcium ionophore to activate the oocyte after ICSI.
Case ReportA 40-year-old female and her 47-year-old husband presented
at the Niigata Workmen’s Accident Hospital for secondaryinfertility of two years duration. The patient had previously con-ceived in intrauterine insemination and delivered a normalmature infant. Her menstrual cycles were regular and her hor-monal testing was normal. The semen analyses revealed oligo-zoospermia (motile sperm: 0.5-1.5 x 106/ml). Thereafter thepatient elected to undergo ICSI.
The patient underwent ovarian stimulation with 100 mgclomiphene citrate on days 4-8 of her menstrual cycle and 150 IUof HMG (HMG Nikken; Nikken Chemicals Co., LTD., Japan)injection on day 8 and day 10. Two mature oocytes wereretrieved. Motile sperm with no obvious abnormal morphology
were injected into two metaphase II (MII) oocytes using theroutine ICSI procedure. However, none of the oocytes becamefertilized.
In the second attempt, the patient underwent ovarian stimula-tion with 100 mg clomiphene citrate on days 4-8 and 150 IU ofHMG injection on day 8, day 10 and day 12 of her menstrualcycle. As a result three oocytes were retrieved. Motile spermwere injected into two MII oocytes. However, none of theoocytes became fertilized.
In the third attempt, the patient underwent ovarian stimula-tion with 100 mg clomiphene citrate on days 4-8 and 150 IU ofHMG injection on day 8 and day 10 of her menstrual cycle. Asa result, three mature oocytes were retrieved. We performedcalcium ionophore oocyte activation after obtaining informedconsent. Motile sperm were injected into three MII oocytes.After 30 min of the ICSI procedure, three oocytes were exposedto 5 μmol/l of calcium ionophore A23187 (Sigma, St. Louis,MO) in HFF99 (Fuso Pharmaceutical Industries, Ltd., Japan)medium with 10% SSS (Irvine, Santa Ana, CA) for 5 min at37°C in 5% CO2/5% O2. The oocytes were then washed in freshmedia and incubated overnight at 37°C in 5% CO2/5% O2 inHFF99 medium with 10% SSS. This time, two of three oocytesbecame normally fertilized (two pronuclei). One oocyte hadthree pronuclei. One embryo transfer was performed on day 3of culture. The patient thereafter conceived and delivered a2,520 g healthy baby without any congenital abnormalities at 36weeks of gestation.
Discussion
For a case of secondary infertility in which fertilizationcould not be achieved despite the performance of ICSI,calcium ionophore was used to activate the oocyte afterICSI. Thereby, fertilization was achieved, thus leading topregnancy and a successful delivery. Recently, it has beenreported that in cases in which fertilization could not beachieved via ICSI, oocyte activation has been performed
SummaryA successful pregnancy outcome after calcium ionophore A23187 oocyte activation in an infertile couple with a repeated failure of
achieving fertilization after ICSI is reported. The secondary infertility couple with oligozoospermia underwent ICSI two times.However, none of the oocytes were fertilized. In the third ICSI attempt, three oocytes after ICSI were activated using calcium ionophorefor five minutes. Two of three oocytes thus became fertilized. A successful pregnancy outcome was thereafter achieved with the deliv-ery of a healthy infant without congenital abnormalities. Oocyte activation using calcium ionophore was thus found to be a usefulmethod in a case of repeated failure of fertilization after ICSI.
Key words: Repeated fertilization failure; ICSI; Oocyte activation; Calcium ionophore.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Original Articles
Reproductive Biology Section

S. Sugaya 262
using calcium ionophore, and subsequent fertilization hasbeen achieved leading to pregnancy and successful deliv-ery [5-8]. In round-head spermatozoa (globozoospermia)with an abnormal shaped sperm head, fertilization rateafter ICSI is low, and there has been the report of a casein which oocyte activation was performed using calciumionophore [8]. There has also been the report of a case inwhich fertilization was not achieved via the usual ICSIdespite a normal motility rate and shape of the sperm, butoocyte activation using calcium ionophore was per-formed, thus leading to pregnancy [6]. It is believed thatthis case is one in which the condition of sperm previous-ly having a fertilizing capacity changes over time there-after, thus resulting in the loss of oocyte activation capac-ity. To the extent of our search of the pertinent medical lit-erature, there have not been any reports of cases in whichoocyte activation has been performed for such cases, andthereby resulting in a live birth, so the present case con-stitutes the first such report.
When considering whether the cause of oocyte activa-tion failure after ICSI is attributable to the sperm, it isnecessary to examine mainly whether there is any abnor-mality in the oocyte activation factor within the sperm.Recently, as for the oocyte activation factor within thesperm, phospholipase Cζ (PLCζ) has been reported as apotential candidate, which has been attracting attention[9]. This refers to the fact that fertilization is achieved byoocyte activation due to PLCζ which is brought into theoocyte cytoplasm after ICSI.
In the present case, since the first fetus was conceivedvia intrauterine insemination and a live birth wasachieved, it is believed the sperm had a normal fertilizingcapacity. Thereafter, the sperm count decreased, leadingto an indication for ICSI, after which it was determined toadminister the treatment. The first and second ICSI bothconstituted ICSI using normal shaped sperm having satis-factory mobility, but no fertilization was observed. It iscommonly believed that the cause of fertilization failuremay be an abnormality in the quality of the oocyte or anoocyte activation failure attributable to the sperm, but theoocyte that was used in the first and second ICSI had amorphologically favorable condition. Therefore, oocyteactivation failure attributable to the sperm might havebeen the cause of the fertilization failure. One method forproving oocyte activation failure attributable to the spermis to verify the presence or absence of oocyte activationby performing ICSI for the provided oocyte, but this wasnot ethically possible. Even though it was not clinicallypossible to prove oocyte activation failure attributable tothe sperm, it was determined that artificial oocyte activa-tion was necessary, and a course of using calciumionophore to activate the oocyte was taken. After per-forming ICSI for three mature oocytes and then using cal-
cium ionophore to activate the oocytes, normal fertiliza-tion was thus observed in two oocytes. Pregnancy wasachieved via implantation, thereafter leading to a success-ful live birth.
Conclusion
In this study, calcium ionophore was used to activatethe oocytes for a case demonstrating secondary infertilityof fertilization failure after ICSI and thus a live birth wasachieved. The present method is therefore believed to beextremely useful for cases of fertilization failure afterICSI.
References[1] Tarlatzis B.C., Bili H.: “Intracytoplasmic sperm injection. Survey of
world results”. Ann. NY. Acad. Sci., 2000, 900, 336. [2] Van Steirteghem A., Nagy P., Joris H., Janssenswillen C., Staessen
C., Verheyen G., Camus M., Tournaye H., Devroey P.: “Results ofintracytoplasmic sperm injection with ejaculated, fresh and frozen-thawed epididymal and testicular spermatozoa”. Hum. Reprod.,1998, 13 (suppl. 1), 134.
[3] Liu J., Nagy Z., Joris H., Tournaye H., Devroey P., Van SteirteghemA.: “Successful fertilization and establishment of pregnancies afterintracytoplasmic sperm injection in patients with globozoosper-mia”. Hum. Reprod., 1995, 10, 626.
[4] Flaherty S.P., Payne D., Matthews C.D.: “Fertilization failures andabnormal fertilization after intracytoplasmic sperm injection”.Hum. Reprod., 1998, 13 (suppl. 1), 155.
[5] Nakagawa K., Yamano S., Moride N., Yamashita M., YoshizawaM., Aono T.: “Effect of activation with Ca ionophore A23187 andpuromycin on the development of human oocytes that failed to fer-tilize after intracytoplasmic sperm injection”. Fertil. Steril., 2001,76, 148.
[6] Eldar-Geva T., Brooks B., Margalioth E.J., Zylber-Haran E., GalM., Silber S.J.: “Successful pregnancy and delivery after calciumionophore oocyte activation in a normozoospermic patient with pre-vious repeated failed fertilization after intracytoplasmic sperminjection”. Fertil. Steril., 2003, 79 (suppl. 3), 1656.
[7] Murase Y., Araki Y., Mizuno S., Kawaguchi C., Naito M.,Yoshizawa M., Araki Y.: “Pregnancy following chemical activationof oocytes in a couple with repeated failure of fertilization usingICSI: case report”. Hum. Reprod., 2004, 19, 1604.
[8] Kim S.T., Cha Y.B., Park J.M., Gye M.C.: “Successful pregnancyand delivery from frozen-thawed embryos after intracytoplasmicsperm injection using round-headed spermatozoa and assistedoocyte activation in a globozoospermic patient with mosaic Downsyndrome”. Fertil. Steril., 2001, 75, 445.
[9] Saunders C.M., Larman M.G., Parrington J., Cox L.J., Royse J.,Blayney L.M., Swann K., Lai F.A.: “PLC zeta: a sperm-specifictrigger of Ca(2+) oscillations in eggs and embryo development”.Development, 2002, 129, 3533.
Address reprint requests to:S. SUGAYA, M.D.Department of Obstetrics and GynecologyJoetsu General Hospital148-1, Daidofukuda, 9438507, Joetsu City (Japan)e-mail:[email protected]

263
Revised manuscript accepted for publication August 31, 2009
Artificial oocyte activation with calcium ionophore allowedfertilization and pregnancy in a couple with long-termunexplained infertility where the female partner had
diminished EGG reserve and failure to fertilize oocytesdespite intracytoplasmic sperm injection
J.H. Check, D. Summers-Chase, R. Cohen, D. BrasileThe University of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School at Camden,
Cooper Hospital/University Medical Center, Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology & Infertility, Camden, NJ (USA)
[1041/29]
Introduction
Oocyte activation is characterized by a two-step patternof rises in intracellular calcium (Ca++) concentrations. Afirst Ca++ rise, referred to as the trigger, originates fromthe oocyte after sperm-oocyte membrane interaction.This initial Ca++ rise that is released from internal Ca++
stores of the oocyte membrane is dependent on a recep-tor-mediated interaction between the sperm and theoocyte plasma membrane [1].
With intracytoplasmic sperm injection (ICSI) thesperm oocyte plasma membrane interaction is eliminated.However, the mechanical injection procedure itself(which can occur by merely the injection without sperm)also causes a massive influx of calcium into the oocyteand is referred to as a pseudotrigger [1].
The second step of oocyte activation is referred to as theoscillator related to the characteristic of a series of shortercalcium transients of high amplitude that begins 30minutes after the trigger (step one) and continues for threeto four hours [1]. The oscillator function is dependent onthe release of a sperm associated activating factor. Thisfactor has been named oscillogen or oscillin [2]. Thissperm oocyte activating factor can control the frequencyof oscillations (thus the name oscillin). It is not species-specific and thus a deficiency of oscillin in human spermcan be detected by failure to activate mouse oocytes [3].This test is referred to as the mouse oocyte activation test
or MOAT. Sperm demembranization is necessary to allowthe release of the cytosolic sperm factor responsible forthe oscillator function and its sustained activity [4, 5].
ICSI has enabled fertilization of oocytes fromextremely low concentrations of viable sperm, spermcoated with a high concentration of antisperm antibodies,and immature testicular sperm even when taken manyhours after the death of a man not on life support [6-8].In 3% or less of cases in women who make an adequatenumber of follicles there will be complete failure to fer-tilize the oocytes despite ICSI [9-11].
Fertilization failure despite ICSI can be related to thepartial or complete inability of the sperm to activateoocytes [12]. Another reason for fertilization failuredespite ICSI is the inability of the oocytes to decondensethe sperm [13]. Sometimes the problem is obviouslyrelated to the sperm lacking oscillin, e.g., with globo-zoospermia where the fertilization rate varies from 0-37% [9, 14, 15]. Fertilization has occurred with globo-zoospermia following ICSI when the eggs were activatedartificially by calcium ionophore [15, 16]. A case wasdescribed where calcium ionophore allowed activationand fertilization of an oocyte and a successful pregnancyin a couple with fertilization failure despite normo-zoospermic motile sperm [17].
The case described here reports another situation wherethere was complete fertilization failure despite normalsperm and ICSI where oocyte activation with calciumionophore was performed followed by fertilization withICSI leading to a pregnancy only this time in a womanwith diminished egg reserve.
SummaryPurpose: To determine if fertilization and embryo development and pregnancy was possible following in vitro fertilization (IVF)
in a couple with long-term unexplained infertility where the female partner had diminished egg reserve and where fertilization failureoccurred despite conventional oocyte insemination and intracyoplasmic sperm injection (ICSI). Methods: In vitro fertilization wasperformed using a low-dose follicle stimulating hormone (FSH) stimulation protocol. Prior to ICSI, artificial oocyte activation withcalcium ionophore was used. Results: Only one mature oocyte was retrieved but it fertilized and cleaved to a good quality 8-cellembryo on day 3. A pregnancy with fetal viability was achieved but she subsequently miscarried. A second attempt successful. Con-clusions: Fertilization and pregnancy is possible even in women with diminished egg reserve with previous failed fertilization withICSI by performing artificial oocyte activation with calcium ionophore. It is not clear if the sperm lacked oscillin or if the eggs werenot responsive to oscillin.
Key words: Artificial oocyte activation; Calcium ionophore; Normal sperm; Diminished egg reserve; Minimal stimulation.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

J.H. Check, D. Summers-Chase, R. Cohen, D. Brasile 264
Case Report
A 34-year-old female married for 14 years and having unpro-tected sex for 12 years presented with primary infertility. Shelived in another state and was found to be “approachingmenopause” with a serum FSH of 64 mIU/ml. A second serumFSH was 37 mIU/ml with a serum estradiol (E2) of 56 pg/ml. Shestill had spontaneous menses but had oligomenorrhea. The onlyinterruption to her attempts at fertility was a one and a half respitewhile she was evaluated and treated for an ocular pseudotumor.
The couple had insurance coverage for in vitro fertilization(IVF) but not for donor egg coverage. The reproductive centerthat they had consulted presented data from one of the leadingIVF centers in the world claiming no live pregnancies despitethe transfer of normal appearing embryos in women of any ageif the serum FSH was > 15 mIU/ml [18]. They refused to tryany treatment other than the use of donor oocytes which thecouple could not afford.
The couple was aware of the data from our IVF center thatfound quite reasonable pregnancy rates with IVF-ET in womenwhose mean day 3 serum FSH was much higher than 15mIU/ml as long as a lower dosage of FSH was used for follic-ular maturation [19]. Though there did not appear to be anyproblem in the semen analysis or fallopian tubes, because of thelength of their infertility and their insurance coverage for IVF-ET we recommended IVF-ET.
The initial semen analysis at our facility showed a normalsemen concentration of 32.7 million per ml with 70.6% motil-ity with 18% with rapid linear motion. The hypo-osmoticswelling test was normal at 68% and there were no antispermantibodies. The one “abnormality” was that the percentage ofsperm with normal morphology using strict criteria was only4% [20]. The couple was advised that for many years some cli-nicians believed (and some still believe this concept today) thatwhen the sperm morphology was � 4% that neither intercourse,intrauterine insemination or conventional oocyte inseminationwill result in adequate pregnancy rates [20]. In fact they hadconcluded the pregnancy rates approached zero [21-24].However, they were also advised that our own data failed to cor-roborate these previous studies and in fact found no predictivevalue of strict morphology � 4% [25-27]. In fact in anotherstudy we actually found that there was no greater risk of failedfertilization with conventional oocyte insemination with terato-zoospermia sperm compared to ICSI but the former resulted insignificantly higher pregnancy rates per transfer [11].
For cycle 1 a protocol was used that used a little more FSHthan the usual minimal stimulation used for diminished eggreserve based on a more optimistic baseline blood with a serumE2 of 87.9 pg/ml and a serum FSH of 11 mIU/ml [28]. The peakserum E2 reached 331 pg/ml and two mature oocytes wereinseminated by conventional insemination. The couple chosethis fertilization option because of the data showing higher preg-nancy rates with conventional oocyte insemination and to deter-mine if their long-term infertility failure could be related tofailed fertilization [11]. Indeed these oocytes failed to fertilize.
For cycle 2 a lower dose FSH protocol was used and wasstarted on day 5 when the serum E2 was 54.2 pg/ml and theserum FSH was 14.3 mIU/ml. For both cycles the serum FSHwas lowered with ethinyl estradiol [30, 31]. Three mature folli-cles were retrieved but none fertilized despite ICSI. Semenparameters were completely normal.
For her third and final insurance covered cycle we suggestedartificial oocyte activation with calcium ionophore. For cycle 3her day 2 serum E2 was 38.6 and the serum FSH was 12.6mIU/ml while taking ethinyl estradiol (20 μg) daily. With aminimum stimulation protocol her peak serum E2 reached 200
pg/ml. A single metaphase II egg was retrieved. Artificial oocyteactivation was performed using calcium ionophore as previouslydescribed [15-17]. An 8-cell embryo on day 3 with 25% fragmen-tation was transferred and she conceived. She showed fetal via-bility six weeks from egg retrieval with properly rising serumbeta human chorionic gonadotropin levels. However, unfortu-nately she subsequently had a miscarriage. Knowing now what isneeded to achieve a pregnancy the couple tried again using a low-dose FSH protocol because of diminished egg reserve and artifi-cial oocyte activation with calcium ionophore. Two oocytes fer-tilized and two embryos (a 5-cell and 8-cell) were transferred andshe has completed the first trimester.
Discussion
It is clear that women with markedly elevated FSHlevels, even over 100 mIU/ml, and even those in apparentmenopause, can achieve successful pregnancies [29-35].Those who believe that an elevated serum FSH results inembryos that do not implant still recognize that there isgenerally no problem with fertilization [18]. Though it isclear that the probable cause of the couple’s long-terminfertility was the inability of the sperm to fertilize theegg, it is not clear whether the problem was a sperm oroocyte factor.
The problem of failed fertilization should not havebeen related to the first step of fertilization, i.e., thetrigger rise of Ca++ that occurs with contact of the spermwith the oocyte membrane since the first cycle using con-ventional insemination demonstrated no problem withsperm binding. Furthermore, even if for some reasonbinding of sperm did not cause the trigger, then the defectshould have been obviated by the mechanical injection ofthe oocyte membrane by ICSI (pseudotrigger) in cycle 2.
Most of the data suggests that Ca++ ionophore treatmentof oocytes has a reasonable chance of allowing fertiliza-tion and normal embryo development and even pregnan-cies when the sperm are deficient in oscillin. However,there are some data suggesting that Ca++ ionophore treat-ment can also allow fertilization when the problem withfailed fertilization is related to oocyte rather than spermdefects [36].
If calcium ionophore proves less efficient for oocyte vssperm-related defects leading to failed fertilization thereis another technique that has been shown to enable fertil-ization when the egg does not respond to proper spermsignals [37]. Fertilization and embryo development andpregnancies have been reported using a modified ICSItechnique using vigorous aspiration of oocyte cytoplasmwhen failed fertilization has been related to a defectiveoocyte factor that is involved in the activation of theoscillator mechanism [37]. Comparative studies in alarger series which would require a cooperative studybetween many IVF centers could help to determine whichtechnique is more efficacious for sperm or oocyte relateddefects in the oscillator mechanism of fertilization andwhether one technique is safer than the other. Whencalcium ionophore is used the patient should be advisedthat there is limited information of its potential toxiceffect on oocytes and embryos.

Artificial oocyte activation with calcium ionophore allowed fertilization and pregnancy in a couple with long-term unexplained etc. 265
Acknowledgment
We would like to thank Ascend Specialty Rx for providingpartial grant support.
References[1] Tesarik J., Mendoza C., Greco E.: “The activity (calcium oscilla-
tor?) responsible for human oocyte activation after injection withround spermatids is associated with spermatid nuclei”. Fertil.Steril., 2000, 74, 1245.
[2] Parrington J., Swann K., Shevchenko V.I., Sesay A.K., Lai F.A.:“Calcium oscillations in mammalian eggs triggered by a solublesperm protein”. Nature, 1996, 379, 364.
[3] Rybouchkin A., Dozortsev D., Pelinck M.J., De Sutter P., DhontM.: “Analysis of the oocyte activation capacity and chromosomalcomplement of round-headed human spermatozoa by their injec-tion into mouse oocytes”. Hum. Reprod., 1996, 11, 2170.
[4] Dozortsev D., Qian C., Ermilov A., Rybouchkin A., De Sutter P.,Dhont M.: “Sperm-associated oocyte-activating factor is releasedfrom the spermatozoon within 30 minutes after injection as a resultof the sperm-oocyte interaction”. Hum. Reprod., 1997, 12, 2792.
[5] Yanagida K., Katayose H., Hirata S., Yazawa H., Hayashi S., SatoA.: “Influence of sperm immobilization on onset of Ca(2 +) oscil-lations after ICSI”. Hum. Reprod., 2001, 16, 148.
[6] Van Steirteghem A.C., Nagy Z., Joris H., Liu H., Liu J., StaessenC. et al.: “High fertilization and implantation rates after intracyto-plasmic sperm injection”. Hum. Reprod., 1993, 8, 1061.
[7] Check M.L., Check J.H., Summers-Chase D., Choe J.K., CheckD.J., Nazari A.: “Live birth after posthumous testicular sperm aspi-ration and intracytoplasmic sperm injection with cryopreservedsperm: Case report”. Clin. Exp. Obstet. Gynecol., 2002, 24, 95.
[8] Check M.L., Check J.H., Katoff D., Summers-Chase D.: “ICSI asan effective therapy for male factor with antisperm antibodies”.Arch. Androl., 2000, 45, 125.
[9] Liu J., Nagy Z., Joris H., Tournay H., Devroey P., Van SteirteghemA.: “Successful fertilization and establishment of pregnancies afterintracytoplasmic sperm injection in patients with globozoosper-mia”. Hum. Reprod., 1995, 10, 626.
[10] Flaherty S.P., Payne D., Matthews C.D.: “Fertilization failures andabnormal fertilization after intracytoplasmic sperm injection”.Hum. Reprod., 1998, 13 (suppl. 1), 155.
[11] Check J.H., Bollendorf A., Wilson C., Summers-Chase D.,Horwath D., Yuan W.: “A retrospective comparison of pregnancyoutcome following conventional oocyte insemination vs. intracy-toplasmic sperm injection for isolated abnormalities in sperm mor-phology using strict criteria”. J. Androl., 2007, 28, 607.
[12] Sakkas D., Urner F., Bianchi P.G., Bizzaro D., Wagner I., Jaque-noud N., Minicardi G., Campana A.: “Sperm chromatin anomaliescan influence decondensation after intracytoplasmic sperm inec-tion”. Hum. Reprod., 1996, 11, 837.
[13] Schmiady H., Tandler-Schneider A., Kentenich H.: “Prematurechromosome condensation of the sperm nucleus after intracyto-plasmic sperm injection”. Hum. Reprod., 1996, 11, 2239.
[14] Battaglia D.E., Koehler J.K., Klein N.A., Tucker M.J.: “Failure ofoocyte activation after intracytoplasmic sperm injection usinground-headed sperm”. Fertil. Steril., 1997, 68, 118.
[15] Rybouchkin A.V., Van der Straeten F., Quatacker J., De Sutter P.,Dhont M.: “Fertilization and pregnancy after assisted oocyte acti-vation and intracytoplasmic sperm injection in a case of round-headed sperm associated with deficient oocyte activation capac-ity”. Fertil. Steril., 1997, 68, 1144.
[16] Tesarik J., Sousa M.: “More than 90% fertilization rates afterintracytoplasmic sperm injection and artificial induction of oocyteactivation with calcium ionophore”. Fertil. Steril., 1995, 63, 343.
[17] Eldar-Geva T., Brooks B., Margalioth E.J., Zylber-Haran E., GalM., Silber S.J.: “Successful pregnancy and delivery after calciumionophore oocyte activation in a normozoospermic patient withprevious repeated failed fertilization after intracytoplasmic sperminjection”. Fertil. Steril., 2003, 79, 1656.
[18] Roberts J., Spandorfer S., Fasouliotis S.J., Kashyap S., RosenwaksZ.: “Taking a basal follicle-stimulating hormone history is essentialbefore initiating in vitro fertilization”. Fertil. Steril., 2005, 83, 37.
[19] Check J.H., Summers-Chase D., Yuan W., Horwath D., Wilson C.:“Effect of embryo quality on pregnancy outcome following singleembryo transfer in women with a diminished egg reserve”. Fertil.Steril., 2007, 87, 749.
[20] Kruger T.F., Acosta A.A., Simmons K.F., Swanson R.J., Matta J.F.,Veeck L.L. et al.: “A new method of evaluating sperm morphol-ogy with predictive value for in vitro fertilization”. Urology, 1987,30, 248.
[21] Grow D., Oehninger S., Seltman H., Toner J., Swanson R.J., DrgerT., Muasher S.J.: “Sperm morphology as diagnosed by strict crite-ria probing the impact of teratozoospermia on fertilization rate andpregnancy outcome in a large in vitro fertilization population”.Fertil. Steril., 1994, 62, 559.
[22] Hammitt D.G., Walker D.L., Syrop C.H., Miller T.M., BennettM.R.: “Treatment of severe male factor infertility with high concen-trations of motile sperm by microinsemination in embryo cryop-reservation straws”. J. In Vitro Fertil. Embryo Transf., 1991, 8, 101.
[23] Oehninger S., Acosta A.A., Morshedi M., Veeck L., Swanson R.I.,Simmons K., Rosenwaks Z.: “Corrective measures and pregnancyoutcome in in vitro fertilization in patients with severe sperm mor-phology abnormalities”. Fertil. Steril., 1988, 50, 283.
[24] Ord T., Patrizio P., Balmaceda J.P., Asch R.H.: “Can severe malefactor infertility be treated without micromanipulation?”. Fertil.Steril., 1993, 60, 110.
[25] Check J.H., Adelson H.G., Schubert B.R., Bollendorf A.: “Evalu-ation of sperm morphology using Kruger’s strict criteria”. Arch.Androl., 1992, 28, 15.
[26] Kiefer D., Check J.H., Katsoff D.: “The value of motile density,strict morphology, and the hypoosmotic swelling test in in vitrofertilization embryo transfer”. Arch. Androl., 1996, 37, 57.
[27] Check M.L., Bollendorf A., Check J.H., Katsoff D.: “Reevaluationof the clinical importance of evaluating sperm morphology usingstrict criteria”. Arch. Androl., 2002, 48, 1.
[28] Check J.H.: “Mild ovarian stimulation”. J. Assist. Reprod. Genet.,2007, 24, 621.
[29] Check J.H., Chase J.S.: “Ovulation induction in hyperg-onadotropic amenorrhea with estrogen and human menopausalgonadotropin therapy”. Fertil. Steril., 1984, 42, 919.
[30] Check J.H., Nowroozi K., Chase J.S., Nazari A., Shapse D., VazeM.: “Ovulation induction and pregnancies in 100 consecutivewomen with hypergonadotropic amenorrhea”. Fertil. Steril., 1990,53, 811.
[31] Check M.L., Check J.H., Kaplan H.: “Pregnancy despite imminentovarian failure and extremely high endogenous gonadotropins andtherapeutic strategies: Case report and review”. Clin. Exp. Obstet.Gynecol., 2004, 31, 299.
[32] Check J.H., Chase J.S., Wu C.H., Adelson H.G.: “Ovulationinduction and pregnancy with an estrogen-gonadotropin stimula-tion technique in a menopausal woman with marked hypoplasticovaries”. Am. J. Obstet. Gynecol., 1989, 160, 405.
[33] Check J.H., Check M.L., Katsoff D.: “Three pregnancies despite ele-vated serum FSH and advanced age”. Hum. Reprod., 2000, 15, 1709.
[34] Check J.H., Katsoff B.: “Successful pregnancy with spontaneousovulation in a woman with apparent premature ovarian failure whofailed to conceive despite four transfers of embryos derived fromdonated oocytes”. Clin. Exp. Obstet. Gynecol., 2006, 33, 13.
[35] Check M.L., Check J.H., Choe J.K., Berger G.S.: “Successfulpregnancy in a 42-year-old woman with imminent ovarian failurefollowing ovulation induction with ethinyl estradiol withoutgonadotropins and in vitro fertilization”. Clin. Exp. Obstet.Gynecol., 2002, 29, 11.
[36] Heindryckx B., Van der Elst J., De Sutter P., Dhont M.: “Treatmentoption for sperm- or oocyte-related fertilization failure: assistedoocyte activation following diagnostic heterologous ICSI”. Hum.Reprod., 2005, 20, 2237.
[37] Tesarik J., Rienzi L., Ubaldi F., Mendoza C., Greco E.: “Use of amodified intracytoplasmic sperm injection technique to overcomesperm-borne oocyte activation failures”. Fertil. Steril., 2002, 78, 619.
Address reprint requests to:J.H. CHECK, M.D., Ph.D.7447 Old York RoadMelrose Park, PA 19027 (USA)e-mail: [email protected]

Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
[789/27]
Revised manuscript accepted for publication February 23, 2010
Immediate and perioperative outcomes of polypropylenemesh in pelvic floor repair in a predominantly obese
population
T.O. Adedipe, S.J. Vine Department of Obstetrics and Gynecology, Prince Charles Hospital, Merthyr Tydfil (UK)
[1088/30]
Introduction
The first commercially available ‘system’ for transvagi-nal delivery of polypropylene mesh into the vesicovagi-nal and or rectovaginal plane to repair uterine and orvaginal prolapse was approved in 2004 by the Food andDrug Adminstration in the US. The system has been usedin France for some time with data on follow-up beingcompiled.
This system has been shown to be able to providesimilar results to abdominal sacral colpoplexy while pre-cluding morbidities associated with laparotomy or pro-longed laparoscopy. The system used is one of severalcommercially available kits which through the use ofpolypropylene mesh, combines apical support with rein-forcement of either or both the anterior and posteriorvagina.
The use of polypropylene mesh has been buttressed bythe fact that the scarring and sclerosis produced by clas-sical pelvic reconstructive surgery restores only 50% ofthe preoperative tissue strength [1-3].
There have been several studies examining the immedi-ate postoperative sequelae. Further studies are compilingdata on the long-term sequelae. However this study lookedat outcomes in a predominantly obese cohort population.
Materials and Methods
This retrospective study was to identify perioperative andpostoperative (3 months and 12 months) complications associ-ated with use of polypropylene mesh for prolapse repair in pre-dominantly obese patients in a UK district general hospital. Thesample size included a total of 27 women between November
2006 and December 2008 and both practitioners were proficientin performing stress incontinence surgeries.
All patients had preoperative evaluation including history,physical examination and urine culture. Pelvic organ prolapsequantitative examination was a tool used in identifying degreeof prolapse. The type of prolapse was identified based on defi-nitions adopted by the International Continence Society [4].Urodynamic evaluation was performed when indicated byurinary symptoms.
The polypropylene mesh repair procedures were carried outusing the manufacturer’s instructions [5]. A course of preoper-ative vaginal estrogen was offered on a need-to basis. All thewomen underwent general anaesthesia as this was the local pro-tocol. This was also the case for excisions of persistent erodedmesh. Prophylactic antibiotics were given intraoperativelywhile a transurethral Foley catheter and gauze packing in thevagina were performed at the end of the procedure. The catheterand packing were left in for a period of 24 hrs. The women weredischarged home without catheters on the second or third day.They were reviewed 8-12 weeks and 6 and 12 months later.
The primary outcome was deviation from a normal operativeand postoperative course within 8-12 weeks of surgery. Compli-cations seen during surveillance at 6 and 12 months in some ofthe women have also been included.
Complications were based on the Dindo scale of 0-5 based ontherapeutic consequences of a complication. Grade I includesminor risk events not requiring therapy other than analgesics,antipyretics, antiemetics and antidiarrheal drugs while grade IIincludes events which require pharmacological treatment withdrugs other than the ones listed for grade I complications. Inter-ventions within grade III included the use of blood transfusionsand total parenteral nutrition. This grade is subdivided intograde IIIa and IIIb. Grade IIIb required the need of generalanesthesia.
Grade IV included life-threatening complications while gradeV complications resulted in death [6].
Data was obtained from the review of patients’ records.Results are presented as mean (range) for continuous variablesand as percentages for categorical variables.
Summary
This retrospective study was to identify perioperative and postoperative complications associated with use of polypropylene meshfor pelvic floor repair in a UK district general hospital in a predominantly obese population. The sample size was 27 women withdata retrieved from records. Total mesh was used in 37.1%, isolated anterior mesh in 44.4%, and an isolated posterior mesh in 18.5%.There was a high incidence of obese (BMI kg/m2 � 30.0) women (66.67%). The highest recorded thus far. A high proportion of thewomen (44.4%) were also over the age of 65 years with attendant comorbidities. The age range was 45-77 years. Complicationsincluded mesh exposure (7.4%), catheterization at discharge (7.4%), bladder injury during dissection (3.7%) and recurrent prolapse(7.4%). In the carefully selected individuals, polypropylene mesh for prolapse repair appears to be a safe technique to correct pelvicorgan prolapse. However, long-term follow-up is needed with further research.
Key words: Vaginal mesh; Pelvic organ prolapse; Predominant obesity; Immediate and perioperative morbidity.
266
General Section

Immediate and perioperative outcomes of polypropylene mesh in pelvic floor repair in a predominantly obese population 267
Results
Another focus of this study was to examine if there wasa difference in results in overweight and obese patients.The incidence of overweight and obese women in thispopulation was 92.59%. There was a predominant per-centage of obesity (BMI � 30) in this group (66.67%).
Most of the subjects were postmenopausal (88.88%)with a good percentage (51.85%) having had no previoushormonal replacement therapy. A good number of thewomen had previous pelvic organ prolapse repair(37.04%). Most women had grade II prolapse (66.67%).General anesthesia was utilized in all the cases.
Demographic and clinical details are in displayed inTable 1.
Concomitant procedures, carried out in four of thecases included anterior vaginal wall repair, posteriorvaginal wall repair, bladder neck buttressing and tension-free vaginal tape insertion (TVT). Total mesh was used inten cases, anterior mesh in 12 cases while five womenhad posterior mesh insertion.
Mean age was 61 years with average hospital stayabout three days and the average BMI being 29.8. Meanoperative time was 87.48 minutes with average blood lossbeing 105.56 ml. The above figures were comparativewith other studies examined [7, 8].
Mesh exposure was seen in 7.4% of cases at 12 weeksfollow-up in our study. This was managed by excisionunder general anesthesia due to personal requests andreluctance to continue with topical estrogen; 7.4% wenthome catheterized as a result of urinary retention follow-ing a urinary tract infection; 7.4% presented with a recur-rent prolapse within the 12-week postoperative period.There was also another case of recurrent prolapse follow-ing a bout of respiratory problems three months postop-eratively. There was resolution of a case of mesh erosionwhich presented 12 months later with the use of topicalestrogen cream.
A case of a promptly repaired bladder injury duringdissection was seen. There was no bladder perforationwith trocar insertion.
There was also no incidence of hematoma or rectalinjury. No hemorrhage of more than 250 ml wasrecorded.
Table 2 reflects type of complication in relation to typeof repair done.
Discussion
Polyprolene mesh is the most commonly used syntheticgraft material used in prolapse repair surgery. Mesh expo-sures, erosions, infections and sinus tract formation arethe most often encountered complications described [9].
In a predominantly obese population, surgical compli-cations are bound to be on the increase. It was interestingto observe different types of morbidities seen in this sub-group of women. All the complications were found inoverweight and obese women. The complications seen inthe overweight group included two cases of urinary tractinfection, one of intraoperative bladder injury, one ofrecurrent prolapse and one of mesh erosion. The obeseand very obese group had two cases of mesh exposure,one case of recurrent prolapse, and one case of recurrentprolapse following respiratory infection.
The Dindo morbidity scale grades complications basedon invasiveness of the successful treatment module. Thecommon complications were recurrent prolapse (7.4%)and urinary tract infection (7.4%).
A significant number of the recurrent prolapses werefrom the group with a history of recurrent prolapse(37.04%). One had a conservation of cervix following aprevious laparoscopic subtotal hysterectomy while theother had conservation of the uterus due to personalrequests despite contrary counselling and advice. Therewas one presentation of a rectocele following an anteriormesh insertion three months later following a bout of res-piratory infections.
Reasons for prolapse recurrences are varied andinclude:
1) Changes in stability of the pelvic floor after surgery.This has been identified by the study done by Clark et al.[10] which revealed a 40% incidence of recurrence post-operatively at another site.
2) A greater likelihood of recurrent prolapse has alsobeen associated with age < 60 yrs and preoperative pelvicorgan prolopse quantification stage 3 or 4 [3].These char-acteristics were evident in this group of recurrent pro-lapse.
Table 1. — Demographic and clinical details of the studypopulation.
Clinical characteristics
Mean age (range) 61.78 (45-77)Mean body mass index kg/m2 (range) 29.8 (22-37)Mean hospital stay (range) 3.07 (2 -5)Mean estimated blood loss (range) 105.56 (50-250)Menopausal status (%)Premenopausal 11.11Postmenopausal 51.85Postmenopausal + HRT 37.04Preoperative stage of prolapse (%)Stage II 66.67Stage III 29.62Stage IV 4.71Previous hysterectomy 62.96Previous surgery for POP 37.04POP: pelvic organ prolapse.
Table 2. — Type of complication in relation to type of repairdone.
Complications Total Anterior Posterior Freq Morbidity(10) (12) (5) (%) grade
UTI 1 1 0 7.4 IIIntraoperative injury 1 0 0 3.7 IRecurrent POP 1 1 0 7.4 IIIbRec POP+Resp Infection 0 1 0 3.7 IIIbMesh exposure 0 1 1 7.4 IIIMesh erosion
(12 months later) 0 1 0 3.7 IIPOP: pelvic organ prolapse.

T.O. Adedipe, S.J. Vine 268
3) Inherent weak native tissues, the use of which haveled to treatment failures [7]. As there was a significantnumber of repeat procedures for recurrence (37.04%),this may be a contributing factor.
Of the patients, 7.4% went home catheterized as aresult of retention from urinary tract infection. This figurewas well below the median rate of 10.9% reported afterabdominal sacral colpopexy [11].
The visceral injury made during dissection waspromptly repaired and a catheter was left in for a periodof ten days under antibiotic cover. She was a 77-year-oldwoman with no previous history of hormone replacementtherapy resulting in atrophic vaginal tissues. A cystogramcarried out thereafter was normal.
There was no bladder perforation with trocar insertion.The rate of visceral injuries is comparative to a previ-ously published rate of 4.0% during Prolift insertion [12]although it is higher than the 0.2% rate reported for tran-sobturator techniques of midurethral sling placement[13]. There was also no incidence of haematoma or rectalinjury. No hemorrhage of more than 250 ml wasrecorded. These results were better or comparative toother studies [7, 8].
Mesh exposure rate (7.4%) was relatively high in thisstudy as compared to 4% in a post mesh insertion studyinvolving the use of Prolift [7] or 3.7% in an abdominalsacral colpoplexy study [14]. However a recent reviewhas shown rates to be between 4.6-10.7% [15]. Theoverall surgical intervention to correct mesh exposurewas 7.4% and this was due to hospital protocol and per-sonal requests. The case of mesh erosion occurred 12months later in a postmenopausal woman and was possi-bly due to estrogen deficiency as this erosion resolvedwith the use of vaginal estrogen therapy. The rates ofmesh exposure and erosion could be due to the high meanage in our cohort (61.78 yrs) and the present hospital pro-tocol of intermittent use of preoperative vaginal estrogenon a need-to basis as opposed to a mandatory preopera-tive course.
Limitations of this study included the relatively smallsample size and a retrospective design encouraging bias.This was reduced by data analysis from consecutive con-sultation notes identified on the computer records. Ourfindings are particular for women who are overweight orobese with a significant percentage of recurrent prolapse,adding more data regarding safety and complications ofmesh pelvic floor repair systems. There appeared to be ahigh incidence of certain complications. Alterations inpractice have been made to reduce these complications,i.e., use of preoperative vaginal estrogen therapy. Wehope also to build on our areas of success via an on-goingassessment of these women with the aim of followingthem up to 24 months postoperatively.
Conclusion
In carefully selected individuals, polypropylene meshfor prolapse repair appears to be a safe technique to
correct pelvic organ prolapse. However, long-termfollow-up is needed. Further research should be directedtowards well-conducted and adequately powered ran-domized controlled trials.
References[1] Whiteside J.L., Weber A.M., Meyn L.A., Walters M.D.: “Risk
factors for prolapse recurrence after vaginal repair”. Am. J. Obstet.Gynecol., 2004, 191, 1533.
[2] Cosson M., Boukerrou M., Lambaudie E., Lobry P., Crepin G.,Ego A.: “Biomechanics of stress distribution and resistance of bio-logical tissues: why use prostheses for the cure of genital pro-lapse?”. J. Gynecol. Obstet. Biol. Reprod. (Paris), 2003, 32, 329.
[3] Brenner J.: “Mesh materials in hernia repair”. In: Schumpelick V.,Wantz G.E. (eds.): “Inguinal Hernia Repair. Expert Meeting onHernia Surgery”. St Moritz, 1994, Karger, Basel, 1995, 172.
[4] Bump R.C., Mattiasson A., Bo K., Brubaker L.P., Delancey J.O.,Klarksov P. et al.: “The standardization of terminology of femalepelvic organ prolapse and pelvic floor dysfunction”. Am. J. Obstet.Gynecol., 1996, 175, 10.
[5] Manufacture’s Instructions for Use guide: Gynecare Prolift PelvicFloor Repair System: Surgical technique. Gynecare/Ethicon,Somerville, NJ, 2004.
[6] Dindo D., Demartines N., Clavien P.A.: “Classification of surgicalcomplications: a new proposal with evaluation in a cohort of 6336patients and results of a survey”. Am. Surg., 2004, 240, 205.
[7] Fatton B., Amblard J., Debodinance P., Cosson M., Jacquetin B.:“Transvaginal reapir of genital prolapse: preliminary results of anew tension-free vaginal mesh (Prolift technique)-a case seriesmulticentric study”. Int. Urogynecol. J., 2006, 18, 743.
[8] Alperin M., Sutkin G., Ellison R., Meyn L., Moalli P., Zyczynski H.:“Perioperative outcomes of the Prolift pelvic floor repair systemsfollowing introduction to a urogynaecology teaching service”. Int.Urogynecol. J. Pelvic Floor Dysfunct., 2008, 19, 1617.
[9] Lo T.-S., Wang A.C.: “Abdominal colposacropexy andsacrospinous ligament suspension for severe uterovaginal pro-lapse: a comparison”. J. Gynecol. Surg., 1998, 14, 59.
[10] Clark A.L., Gregory T., Smith V.J., Edwards R.: “Epidemiologicevaluation of reoperation for surgically treated pelvic organ pro-lapse and urinary incontinence”. Am. J. Obstet. Gynecol., 2003,189, 1261.
[11] Nygaard I.E., McCreery R., Brubaker L., Connolly A., Cundiff G.,Weber A.M. et al.: “Abdominal sacrocolpoplexy: A comprehen-sive (review)”. Obstet. Gynecol., 2004, 104, 805.
[12] Altman D., Falconer C.: “Perioperative morbidity using transvagi-nal mesh in pelvic organ prolapse repair”. Obstet. Gynecol., 2007,109 (2 pt 1), 303.
[13] Sung V.W., Schleinitz M.D., Rardin C.R., Ward R., Myers D.L.:“Comparison of retropubic vs transobturator approach tomidurethral slings: a systematic review and meta-analysis”. Am. J.Obstet. Gynecol., 2007, 197, 3.
[14] Culligan P.J., Blackwell L., Goldsmith L.J., Graham C.A., RogersA., Heit M.H.: “A randomized controlled trial comparing thefascia lata and the synthetic mesh for sacral colpopexy”. Obstet.Gynecol., 2005, 106, 29.
[15] Feiner B., Jelovsek J.E., Maher C.: “Efficacy and safety of trans-vaginal mesh kits in the treatment of prolapse of the vaginal apex:a systematic review”. BJOG, 2009, 119, 1.
Address reprint requests to:T.O. ADEDIPE, M.D.Department of Obstetrics and GynecologyPrince Charles HospitalMerthyr Tydfil (UK)e-mail: [email protected]

269
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication January 18, 2010
Relation between Doppler findings and perinatal outcomesin fetuses with intrauterine growth restriction
M. Kazandi, C. Guven, F. Akercan, B. Zeybek, T. Cirpan, M. Ergenoglu, O. Yeniel, A. Akdemir, S. Ozsener
Department of Obstetrics and Gynecology, Ege University School of Medicine, Bornova, Izmir (Turkey)
[1079/29]
Introduction
Normal fetal growth depends on genetic growth poten-tial, along with maternal, fetal, placental and externalfactors. Defects in one or a combination of these factorsaffect fetal growth [1].
Intrauterine growth restriction (IUGR) is commonlycharacterized by birth weight below the 10th percentile.The American College of Obstetricians and Gynecolo-gists (ACOG) describes IUGR as estimated fetal gesta-tional age below the 10th percentile [2]. IUGR stands asone of the significant causes of perinatal mortality andmorbidity in modern obstetric practice. Cooperation of anobstetrician and neonatologist in the management offetuses with IUGR is essential. Mortality and morbidityrates can be decreased with correct diagnosis, suitablecare and timely intervention. Timing of birth is veryessential in antenatal management as there is no currentlyavailable successful intrauterine therapy. Maximum ges-tational age and minimum risk for intrauterine life shouldbe aimed in timing of birth [3]. Neonatal consequences ofIUGR comprise perinatal asphyxia and neonatal adaptiveproblems, and short- and long-term sequelae. Perinatalmortality rate increases by 10-20 times in infants withIUGR compared to normal fetuses [4].
Presence and severity of fetal hypoxemia and its prena-tal consequences can be correctly determined by Dopplerultrasound (US). Doppler US can noninvasively detectblood flow in uteroplacental circulation. It has been morecommonly used in recent years due to its noninvasive and
easy to use nature, and the fact that it provides repro-ducible results. Doppler US provides correct antenataldetection of IUGR, on-time intervention, and decrease inmortality and morbidity rates [5].
The relation between fetal venous and arterial Dopplerfindings and perinatal outcomes were correlated in acohort of IUGR fetuses.
Materials and Methods
Eighty-two cases hospitalized in Ege University Faculty ofMedicine, Obstetrics and Gynecology Clinic with a prediagno-sis of IUGR between November 2008 and July 2009 wereincluded in this study prospectively. The study was conductedin accordance with the guidelines, and approval was given bythe Ethical Committee of the Ege University Hospital. Demo-graphic and US data and Doppler parameters of all the patientsand fetuses were recorded and prospectively evaluated. Patientswere grouped according to Doppler parameters: those withnormal Doppler findings (n = 43), and those with impaired arte-rial (n = 27) and venous systems (n = 12). Fetal or chromoso-mal anomalies, fetal infections, multiple pregnancies, prema-ture membrane rupture and birth weight above the 10th
percentile were criteria for exclusion from the study.Gestational weeks were determined according to the date of
last menstrual period, and confirmed by early US measure-ments. In patients who were not sure of the date of the lastmenstrual cycle, gestational weeks were calculated by firsttrimester crown-rump length (CRL) measurement. CRL wastaken as a reference when a difference more than five days waspresent between the calculation based on the last menstrualdate and CRL.
Fetal weight was calculated in all the cases by US measure-ments of biparietal diameter, head circumference, femur length,
Summary
Purpose of Investigation: To find the relationship between fetal Doppler findings and perinatal outcomes in intrauterine growthrestriction. Methods: Eighty-two cases with a prenatal diagnosis of intrauterine growth restriction between November 2008 and July2009 were included in this prospective study at Ege University School of Medicine. Fetuses were grouped according to Dopplerparameters: those with normal Doppler findings (n = 43), and those with impaired arterial (n = 27) and venous systems (n = 12).Results: Out of 82 growth restricted cases, 43 (52.4%) had normal Doppler findings, while 27 (32.9%) displayed impaired arterialparameters and 12 (14.6%) had impaired venous parameters. The mean first minute Apgar scores were 7.57 ± 1.53 for the groupwith normal Doppler flows, 6.8 ± 2 for the group with an impaired arterial system, and 4 ± 1.94 for the group with an impairedvenous system. Two cases from the normal Doppler flow group (n = 42), four cases from the impaired arterial flow group (n = 27),and 11 cases from the impaired venous flow group (n = 11) had fifth minute Apgar scores under 6. Evaluation of the umbilical arteryblood gas revealed acidosis in two cases from the normal Doppler flow group (n = 42), three cases from the impaired arterial systemgroup (n = 27), and five cases from the impaired venous system group (n = 11). Conclusion: A Doppler spectrum from normal tovenous system impairment correlated with poor fetal outcomes including fetal acidosis, fetal mortality and morbidity, decreasedApgar scores at 1 and 5 min, and neonatal morbidity.
Key words: Fetal Doppler; IUGR, Perinatal morbidity.

M. Kazandi, C. Guven, F. Akercan, B. Zeybek, T. Cirpan, M. Ergenoglu, O. Yeniel, A. Akdemir, S. Ozsener 270
humerus length, and abdominal circumference. Intrauterinegrowth restriction diagnosis was confirmed when the birthweight was under the 10th percentile.
All US examinations and measurements were performed bya single operator with Voluson 730 Expert Ultrasound ColorDoppler equipment. A 4-MHz convex probe was used in theseprocedures. The umbilical artery, bilateral uterine arteries,middle cerebral arteries, umbilical vein and ductus venosusparameters were assessed.
Umbilical artery Doppler measurements were performed atthe free segment of the umbilical cord, distant from the fetusand the placenta. Following the observation that the acquiredwaveforms stayed stable for at least five cardiac cycles, meas-urements were performed on three different cycles and theresults were averaged.
In the fetal middle cerebral artery (MCA) measurements, fol-lowing detection of the vascular structures of the Willis polygonby color mode, Doppler indexes were measured at 0 degreeangle from the MCA closest to the probe.
Absent diastolic flow or reverse flow in the umbilical artery,or an MCA PI less than the 5th percentile was evaluated as asign of an impaired arterial system. The venous system wasconsidered impaired in case of pulsation in the umbilical vein,and A wave absence or reversal in ductus venosus.
Birth was performed in at most 24 hours following DopplerUS measurement. Right after the infant was born, the cord wasclamped before the first respiration, and 2 to 3 cc blood was col-lected with a heparin-coated needle from the umbilical arteryprior to placenta separation. The blood was examined within atmost 10 min with a Nova Biomedical blood gas analyzer.Umbilical artery pH values under 7.20 were considered as aci-dosis.
The clinical parameters compared were maternal age, gesta-tional week, birth weight, Apgar score at 1 and 5 min, umbili-cal artery blood gas, intrauterine death, neonatal death, andneonatal morbidity.
To evaluate the findings of the study, SPSS 13.0 (StatisticalPackage for Social Sciences) software was used for statisticalanalysis. Comparison of the significance of quantitative databetween the groups was performed by the variance analysis test,while the chi-square test was used to assess the significance ofthe differences between the qualitative data obtained. Relationsbetween the parameters were examined by the Pearson correla-tion test. The results were evaluated in mean ± standard devia-tion, 95% confidence interval, and p < 0.05 significance level.
Results
Out of 82 IUGR cases, 43 (52.4%) had normal Dopplerfindings, while 27 (32.9%) displayed impaired arterialparameters and 12 (14.6%) had impaired venous param-eters.
Mean age was 29.04 ± 5.49 years in the group withnormal Doppler flows, 30.5 ± 5.7 years in the group withimpaired arterial system, and 28.5 ± 4.94 in the groupwith impaired venous system. There was no statisticallysignificant difference between the groups in terms ofmaternal age.
In the group with normal Doppler flow, mean gesta-tional age was 258.6 ± 19.1 days and mean birth weightwas 1968.8 ± 471 g; while mean gestational age was231.2 ± 17 days and mean birth weight was 1233.7 ± 381g in the group with an impaired arterial system; and these
figures were 222.7 ± 23.7 days and 991.2 ± 564 g,respectively, for the group with an impaired venoussystem. While there were no statistically significant dif-ferences in terms of gestational age between the groupswith impaired arterial and venous systems, a statisticallysignificant difference was apparent between the groupwith normal Doppler flows and the other two groups (p <0.05). No significant difference was detected in terms ofbirth weights between the group with an impaired arterialsystem and that with an impaired venous system, yet asignificant difference was found between the groups withimpaired arterial and venous systems and the group withnormal Doppler flows (p < 0.05).
Mean first minute Apgar scores were 7.57 ± 1.53 forthe group with normal Doppler flows, 6.8 ± 2 for thegroup with an impaired arterial system, and 4 ± 1.94 forthe group with an impaired venous system. While therewas no statistically significant difference between groupswith normal Doppler flows and impaired arterial systemin terms of the first minute Apgar scores, the differencedetected between the group with an impaired venoussystem and the other two groups was statistically signifi-cant (p < 0.05).
Two cases from the normal Doppler flow group (n = 42),four cases from the impaired arterial flow group (n = 27),and 11 cases from impaired venous flow group (n = 11)had fifth minute Apgar scores under 6. In terms of the fifthminute Apgar scores, there was no statistically significantdifference between groups with normal Doppler flows andimpaired arterial systems, and the difference detectedbetween the group with impaired venous systems and theother two groups was significant (p < 0.05).
Evaluation of the umbilical artery blood gas revealedacidosis in two cases from the normal Doppler flow group(n = 42), three cases from the impaired arterial systemgroup (n = 27), and five cases from the impaired venoussystem group (n = 11). While the group with normalDoppler findings and that with an impaired arterial systemhad no significant difference between them in terms ofumbilical artery blood gas values, a significant differencewas observed between the group with an impaired venoussystem and the other two groups (p < 0.05).
Two postnatal death cases occurred in the group withnormal Doppler flows (n = 43), while this rate was fourfor the group with an impaired arterial system (n = 27),and five for the group with an impaired venous system (n= 12). There was one fetal death case in utero in each oneof the groups with normal Doppler findings and impairedvenous systems. The groups with impaired arterialsystems and normal Doppler flow had no statistically sig-nificant difference between them in terms of mortalityrates, while there was a significant difference between theimpaired venous system group and the other two groups(p < 0.05).
There was a significant difference between the threegroups in terms of intubation status and respiratory dis-tress syndrome (RDS) (p < 0.05), however there was nosignificant difference in terms of intraventricular hemor-rhage (IVH) (Table 1).

Relation between Doppler findings and perinatal outcomes in fetuses with intrauterine growth restriction 271
Discussion
Fetuses with IUGR are at higher risk for poor perinataland long-term consequences compared to the fetuses withnormal growth patterns. Perinatal mortality increases 8-fold when fetal weight is under the 10th percentile, and by20-fold when the fetal weight is under the 3rd percentile [6].Combined use of fetal biometry, biophysics profile (BPP),NST, and arterial and venous Doppler US provides the bestresults in the management of these fetuses. When usedalone, these tests have a limited value in IUGR manage-ment. Timing of birth is very critical in preterm fetuseswith IUGR, and gestational age is the factor that con-tributes the most to poor outcomes [7, 8]. Bilardo et al. [9]found poor perinatal outcomes to be 45% and perinatalmortality rate to be 36% under 30 weeks gestation in aseverely premature IUGR group (n = 33).
Birth weight is one of the most significant findingsaffecting perinatal morbidity and mortality. Risk for poorperinatal consequences increases by 5-30 times forinfants born with a birth weight of 1500-2500 g (< 10th
percentile) at term compared to infants born at 10th-90th
percentile, while this risk is increased by 70-100 timesfor infants with a birth weight of 1500 g or less (3rd per-centile) [10]. In our study, mean birth weight was 991 ±564 g in the group with an impaired venous system, 1,233± 381 g in the impaired arterial system group, and 1,968± 471 g in the normal Doppler flow group.
The relation between venous Doppler anomalies andperinatal consequences is very significant for clinicalmanagement. A progressive rise in venous Dopplerindexes reflects impairment in cardiac function. Thisimpairment indicates progress from fetal hypoxemia toacidosis and intrauterine death if birth does not occur. Incase of increase or abnormality in venous system Dopplerindexes, sensitivity for fetal acidemia is 70-90%, andspecificity is 70-80% [11]. In our study, we detectedacidemia (umbilical artery pH < 7.2) in 45% (5/11) of thegroup with an impaired venous system, in 11% (3/27) ofthe group with an impaired arterial system, and in 4.7%(2/42) of the normal Doppler flow group. As a result,Doppler US is useful in the evaluation of fetal oxygena-tion and acid-base status.
Fetuses with IUGR are also prone to multiorganfailure, RDS, IVH, NEC, bronchopulmonary dysplasia,and hemorrhage disorders [12,13]. In a study whichincluded 300 fetuses with IUGR, cases were separatedinto 2 groups [14]. Group 1 (n = 137) consisted of fetuseswith end-diastolic flow in the umbilical artery, whilegroup two (n = 163) consisted of those with absence of
diastolic flow or reverse flow in umbilical artery. Rate ofRDS, sepsis, perinatal mortality and morbidity, and needfor a neonatal unit was higher in Group 2. Also in a studywhere 404 pregnant women with IUGR fetuses wereexamined, 39 (9.7%) of the fetuses developed NEC [15].NEC incidence has been observed to increase in particu-lar with change in the venous parameters from normal toabnormal in Doppler ultrasound.
Conclusion
IUGR stands as one of the significant causes of perina-tal mortality and morbidity in modern obstetric practice.Mortality and morbidity rates can be decreased with acorrect diagnosis, suitable care and on-time intervention.Time of birth is very essential in antenatal management,as there is no currently available successful intrauterinetherapy. In our study, gestational age at delivery and birthweight decreased, acidosis in umbilical artery blood gasand mortality increased, first and fifth minute apgarscores decreased, and the neonatal morbidity rate waselevated from normal to impaired venous system findingsin Doppler.
References[1] Gardosi J., Chang A., Kalyan B., Sahota D., Symonds E.M.: “Cus-
tomised antenatal growth charts”. Lancet, 1992, 339, 283.[2] American College of Obstetricians and Gynecologists. Intrauter-
ine growth restriction. ACOG Practice Bulletin no. 12, Washing-ton DC, 2000.
[3] Baschat A.A., Hecher K.: “Fetal growth restriction due to placen-tal disease”. Semin. Perinatol., 2004, 28, 67.
[4] Regev R.H., Lusky A., Dolfin T., Litmanovitz I., Arnon S., Reich-man B., Israel Neonatal Network: “Excess mortality and morbid-ity among small- for- gestational- age premature infants: a popu-lation based study”. J. Pediatr., 2003, 143, 186.
[5] Alfirevic Z., Neilson J.P.: “Doppler ultrasonography in high preg-nancies: systematic review with meta-analysis”. Am. J. Obstet.Gynecol., 1995, 172, 1379.
[6] Scott K.E., Usher R.: “Fetal malnutrition: its incidence, causes andeffects”. Am. J. Obstet. Gynecol., 1966, 94, 951.
[7] Vergani P., Roncaglia N., Locatelli A., Andreotti C., Crippa I., Pez-zullo J.C., Ghidini A.: “Antenatal predictors of neonatal outcomein fetal growth restriction with absent end diastolic flow in theumbilical artery”. Am. J. Obstet. Gynecol., 2005, 193, 1213.
[8] Baschat A.A.: “Arterial and venous Doppler in the diagnosis andmanagement of early onset fetal growth restriction”. Early Hum.Dev., 2005, 81, 877.
[9] Bilardo C.M., Wolf H., Stigter R.H., Ville Y., Baez E., Visser G.H.,Hecher K.: “Relationship between monitoring parameters andperinatal outcome in severe, early intrauterine growth restriction”.Ultrasound Obstet. Gynecol., 2004, 23, 119.
[10] Williams R.L., Creasy R.K., Cunningham G.C., Hawes W.E.,Norris F.D., Tashiro M.: “Fetal growth and perinatal viability inCalifornia”. Obstet. Gynecol., 1982, 59, 624.
[11] Baschat A.A., Güclü S., Kush M.L., Gembruch U., Weiner C.P.,Harman C.R.: “Venous Doppler in the prediction of acid-basestatus of growth restricted fetuses with elevated placental bloodflow resistance”. Am. J. Obstet. Gynecol., 2004, 191, 277.
[12] Fang S.: “Management of preterm infants with intrauterine growthrestriction”. Earl. Hum. Dev., 2005, 81, 889.
[13] Tommiska V., Heinonen K., Lehtonen L., Renlund M., Saarela T.,Tammela O., Virtanen M., Fellman V.: “No improvement inoutcome of nationwide extremely low birthweight infant popula-tions between 1996-1997 and 1999-2000”. Pediatrics, 2007, 119,29.
Table 1. — Neonatal morbidity status.
Normal Doppler Abnormal Arterial Abnormal Venous(n = 42) (n = 27) (n = 11)
RDS 4 (%9) 9 (%33) 10 (%91) p < 0.05IVH 1 (%2) 1 (%3.7) 1 (%9) n.s.Intubation 3 (%7) 9 (%33) 10 (%91) p < 0.05RDS: Respiratory distress syndrome; IVH: Intraventricular hemorrhage; ns: nonsignificant; p < 0.05: statistically significant.

M. Kazandi, C. Guven, F. Akercan, B. Zeybek, T. Cirpan, M. Ergenoglu, O. Yeniel, A. Akdemir, S. Ozsener 272
[14] Yildirim G., Turhan E.: “Perinatal and neonatal outcomes ofgrowth restricted fetuses with positive end diastolic and absent orreversed umbilical artery Doppler waveforms”. Saudi Med. J.,2008, 29, 403.
[15] Manogura A.C., Turan O., Kush M.L., Berg C., Bhide A., TuranS. et al.: “Predictors of necrotizing enterocolitis in pretermgrowth-restricted neonates”. Am. J. Obstet. Gynecol., 2008, 198,638.
Address reprint requests to:M. KAZANDI, M.D.Department of Obstetrics and GynecologyEge University School of MedicineBornova, Izmir35100 (Turkey)e-mail: [email protected]

273
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication July 19, 2010
Impact of the medicalization of labor on mode of delivery
U. Indraccolo1, S. Calabrese2, R. Di Iorio2, L. Corosu2, E. Marinoni3, S.R. Indraccolo2
1Department of Surgical Sciences, University of Foggia, Foggia, Italy2Department of Woman’s Health, “La Sapienza” University, Rome, Italy
3Center for Scientific Research, San Pietro Hospital, “Fatebenefratelli” Rome (Italy)
[1142/30]
Introduction.
It has been reported [1] so far that the term “normallabor” does not have a clearly definable, practical defini-tion and, consequently, in clinical practice it may happenthat inappropriate medical interventions could be imple-mented in some cases in which labor does not seemnormal according to a subjective judgement. Such med-icalization is not functional to the “normal” progressionof delivery [2]. We also believe that physicians may inter-vene more in high-risk pregnancies, in order to reducelabor time. This may be due to a categorical attribution ofobstetric risk resulting in an excessive number of medicalinterventions, thereby obstructing “normal labor” even incases where labor could take place without consequencesdespite the pregnancy being “at risk”.
The goal of this study was to evaluate whether routinemedical interventions on labor (oxytocin augmentation,amniotomy, epidural analgesia, induction) condition deliv-ery outcome independently of each other and independ-ently of obstetric risk. In addition, the study evaluateswhether there is an ideal window during labor in which toinitiate such medical interventions as safely as possible.
Materials and Methods
The study was conducted prospectively on pregnant womenadmitted to the Operative Unit of the Gynecology and Obstet-rics of San Pietro Hospital Fatebenefratelli, Rome betweenJanuary 2008 and August 2008. This hospital is a tertiary facil-ity in which epidural analgesis is offered “on demand”. The
study encompassed 1,047 women with singleton gestations withcefalic presentation, during labor or needing induction of labor(planned cesarean section was excluded). Data regarding labor(cervical dilation and station) in relationship to the initiation ofoxytocin augmentation, epidural analgesia, and amniotomywere gathered for each patient. Data concerning labor induc-tion, birth method and all personal and anamnestic data of theparturients were collected after birth by analyzing patientrecords relative to the admission. On the basis of this informa-tion, obstetric risk was determined using a point systemreported by Pescetto et al. [3]. This system objectively attrib-utes a score of global risk by considering multiple pregesta-tional and gestational factors (i.e., hereditary diseases, mater-nal age, social behavior, parity, previous obstetric history,diseases or nutritional disorders during pregnancy, endocrino-logical disorders, abnormality or diseases of the genital tract,others), to which a point is assigned (0, 5, 10, 15, 20, 30). Suchscoring system does not consider all the situations that can bedefined as “conferring an obstetric risk” but allows for theintroduction of possible missing factors by leaving some fieldsopen. The sum of scores indicates a global risk, subdivided intothree categories: low risk (from 0 to 15), intermediate risk(from 20 to 25) and high risk (equal to or over 30). Althoughthis system may be debatable, to our knowledge there is not yetan internationally validated scoring system for evaluatingobstetric risk.
Despite the existence of the Pescetto risk scoring instrument[3], in Italy obstetric risk is not usually quantified in clinicalpractice. Therefore, in this study the clinical decisions weremade only on the basis of presence/absence of obstetric riskdefined in a subjective manner by the physician caring for theparturient on the basis of his or her own professional expertise.The variable “obstetric risk” was included in the multivariatelogistic analysis as an independent variable with three levels ofexpression (low risk, intermediate risk, high risk). Such variablewas used to check if the medical interventions were higher inpatients truly at high risk.
Summary
Aims: To evaluate whether routine medical interventions during labor (oxytocin augmentation, induction, amniotomy, epiduralanalgesia) condition the outcome of delivery independently of each other and of obstetric risk (calculated in an objective manner).Moreover, to evaluate whether there is an ideal window for initiating such interventions. Methods: Prospective, observational studywith 1,047 patients enrolled. Results: Medical interventions were high, whether in low-, medium- or high-risk pregnancies. Oxy-tocin augmentation (odds ratio 4.678) labour induction (odds ratio 1.717) amniotomy (odds ratio 1.403) and obstetric risk (interme-diate-risk odds ratio 1.889, high-risk odds ratio 2.008) increase the probability of an operative delivery. Oxytocin augmentationincreases both the probability of a Cesarean delivery and vacuum extraction. Epidural analgesia reduces the probability of cesareandelivery and increases the probability of vacuum extraction. The greater the cervical dilation when oxytocin infusion is initiated, thelower the probability of an operative delivery. The more advanced the cervical dilation and the lower the station when amniotomyor epidural analgesia are carried out, the lower the probability of an operative delivery. Obstetric risk and oxytocin augmentationappear to increase the probability of operative delivery in patients who have undergone amniotomy or epidural analgesia. In addi-tion, labor induction in patients who undergo epidural analgesia increases the risk of operative delivery. Conclusions: Medical inter-ventions during labor are high and cause a rise in operative delivery. Therefore, practitioners should defer it as much as possible.The exception is epidural analgesia because it seems to reduce the number of cesarean sections.
Key words: Labor; Oxytocin augmentation; Amniotomy; Epidural analgesia.
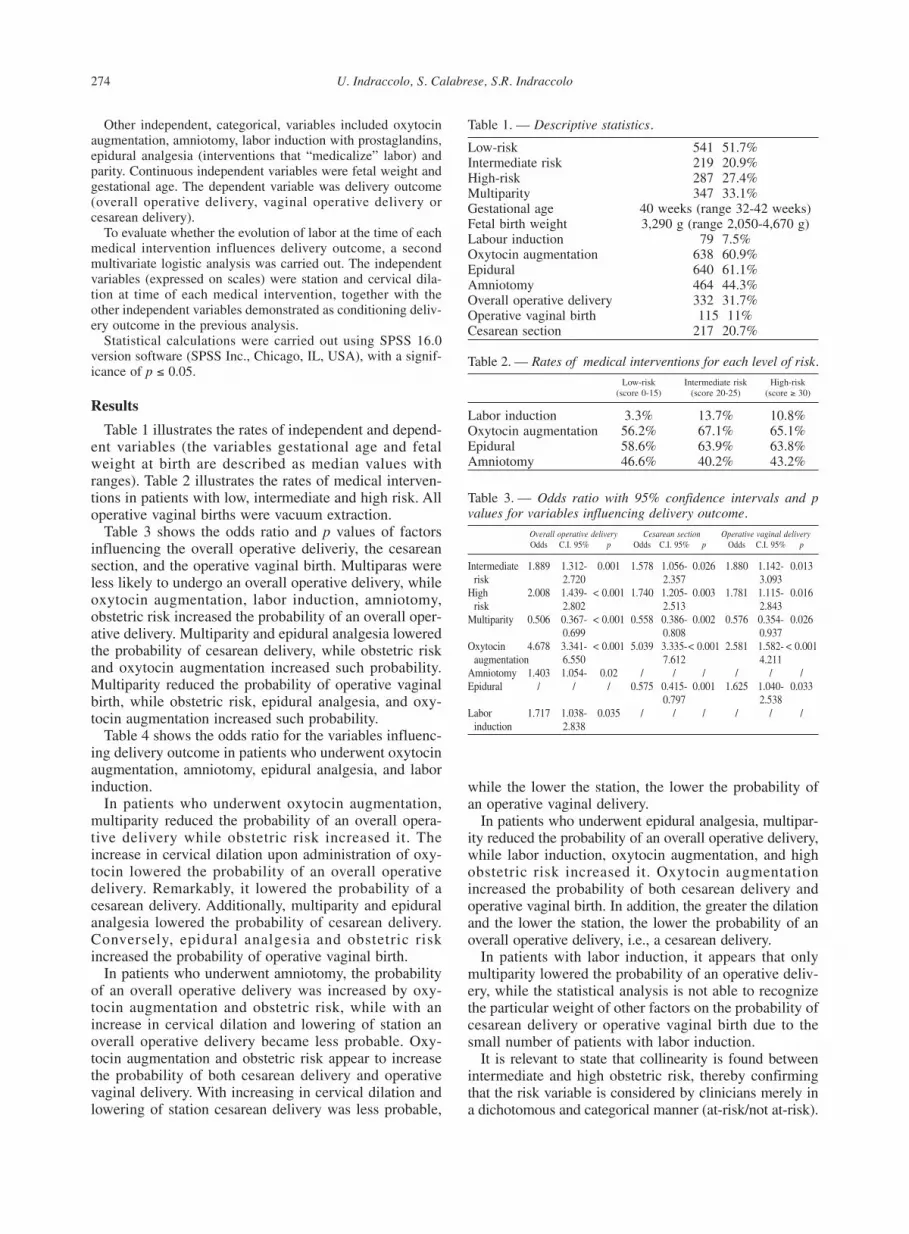
U. Indraccolo, S. Calabrese, S.R. Indraccolo 274
Other independent, categorical, variables included oxytocinaugmentation, amniotomy, labor induction with prostaglandins,epidural analgesia (interventions that “medicalize” labor) andparity. Continuous independent variables were fetal weight andgestational age. The dependent variable was delivery outcome(overall operative delivery, vaginal operative delivery orcesarean delivery).
To evaluate whether the evolution of labor at the time of eachmedical intervention influences delivery outcome, a secondmultivariate logistic analysis was carried out. The independentvariables (expressed on scales) were station and cervical dila-tion at time of each medical intervention, together with theother independent variables demonstrated as conditioning deliv-ery outcome in the previous analysis.
Statistical calculations were carried out using SPSS 16.0version software (SPSS Inc., Chicago, IL, USA), with a signif-icance of p � 0.05.
Results
Table 1 illustrates the rates of independent and depend-ent variables (the variables gestational age and fetalweight at birth are described as median values withranges). Table 2 illustrates the rates of medical interven-tions in patients with low, intermediate and high risk. Alloperative vaginal births were vacuum extraction.
Table 3 shows the odds ratio and p values of factorsinfluencing the overall operative deliveriy, the cesareansection, and the operative vaginal birth. Multiparas wereless likely to undergo an overall operative delivery, whileoxytocin augmentation, labor induction, amniotomy,obstetric risk increased the probability of an overall oper-ative delivery. Multiparity and epidural analgesia loweredthe probability of cesarean delivery, while obstetric riskand oxytocin augmentation increased such probability.Multiparity reduced the probability of operative vaginalbirth, while obstetric risk, epidural analgesia, and oxy-tocin augmentation increased such probability.
Table 4 shows the odds ratio for the variables influenc-ing delivery outcome in patients who underwent oxytocinaugmentation, amniotomy, epidural analgesia, and laborinduction.
In patients who underwent oxytocin augmentation,multiparity reduced the probability of an overall opera-tive delivery while obstetric risk increased it. Theincrease in cervical dilation upon administration of oxy-tocin lowered the probability of an overall operativedelivery. Remarkably, it lowered the probability of acesarean delivery. Additionally, multiparity and epiduralanalgesia lowered the probability of cesarean delivery.Conversely, epidural analgesia and obstetric riskincreased the probability of operative vaginal birth.
In patients who underwent amniotomy, the probabilityof an overall operative delivery was increased by oxy-tocin augmentation and obstetric risk, while with anincrease in cervical dilation and lowering of station anoverall operative delivery became less probable. Oxy-tocin augmentation and obstetric risk appear to increasethe probability of both cesarean delivery and operativevaginal delivery. With increasing in cervical dilation andlowering of station cesarean delivery was less probable,
while the lower the station, the lower the probability ofan operative vaginal delivery.
In patients who underwent epidural analgesia, multipar-ity reduced the probability of an overall operative delivery,while labor induction, oxytocin augmentation, and highobstetric risk increased it. Oxytocin augmentationincreased the probability of both cesarean delivery andoperative vaginal birth. In addition, the greater the dilationand the lower the station, the lower the probability of anoverall operative delivery, i.e., a cesarean delivery.
In patients with labor induction, it appears that onlymultiparity lowered the probability of an operative deliv-ery, while the statistical analysis is not able to recognizethe particular weight of other factors on the probability ofcesarean delivery or operative vaginal birth due to thesmall number of patients with labor induction.
It is relevant to state that collinearity is found betweenintermediate and high obstetric risk, thereby confirmingthat the risk variable is considered by clinicians merely ina dichotomous and categorical manner (at-risk/not at-risk).
Table 1. — Descriptive statistics.
Low-risk 541 51.7%Intermediate risk 219 20.9%High-risk 287 27.4%Multiparity 347 33.1%Gestational age 40 weeks (range 32-42 weeks)Fetal birth weight 3,290 g (range 2,050-4,670 g)Labour induction 79 7.5%Oxytocin augmentation 638 60.9%Epidural 640 61.1%Amniotomy 464 44.3%Overall operative delivery 332 31.7%Operative vaginal birth 115 11%Cesarean section 217 20.7%
Table 2. — Rates of medical interventions for each level of risk.
Low-risk Intermediate risk High-risk(score 0-15) (score 20-25) (score � 30)
Labor induction 3.3% 13.7% 10.8%Oxytocin augmentation 56.2% 67.1% 65.1%Epidural 58.6% 63.9% 63.8%Amniotomy 46.6% 40.2% 43.2%
Table 3. — Odds ratio with 95% confidence intervals and pvalues for variables influencing delivery outcome.
Overall operative delivery Cesarean section Operative vaginal deliveryOdds C.I. 95% p Odds C.I. 95% p Odds C.I. 95% p
Intermediate 1.889 1.312- 0.001 1.578 1.056- 0.026 1.880 1.142- 0.013risk 2.720 2.357 3.093
High 2.008 1.439- < 0.001 1.740 1.205- 0.003 1.781 1.115- 0.016risk 2.802 2.513 2.843
Multiparity 0.506 0.367- < 0.001 0.558 0.386- 0.002 0.576 0.354- 0.0260.699 0.808 0.937
Oxytocin 4.678 3.341- < 0.001 5.039 3.335-< 0.001 2.581 1.582- < 0.001augmentation 6.550 7.612 4.211
Amniotomy 1.403 1.054- 0.02 / / / / / /Epidural / / / 0.575 0.415- 0.001 1.625 1.040- 0.033
0.797 2.538Labor 1.717 1.038- 0.035 / / / / / /
induction 2.838

Impact of the medicalization of labor on mode of delivery 275
Discussion
The present study is one of the few to evaluate theeffects of combined routine obstetric interventions ondelivery outcome. In addition, it also appears to be theonly one to control both obstetric risk and the timingduring labor in which oxytocin augmentation, epiduralanalgesia or amniotomy were carried out.
Obstetric risk greatly influences delivery outcome. Anoperative delivery is performed twice as often in parturi-ents labelled as “at-risk”. In addition, these patients seemdestined to be submitted to a greater number of medicalinterventions during labor, resulting in a greater numberof operative deliveries. In clinical practice, obstetric riskis not quantified and is determined subjectively. Suchpolicy seems to overestimate the obstetric risk, since themedical interventions are high even in low-risk patients.Therefore, an objective system for assessing risk could beuseful for grading the type of interventions, in order toavoid unnecessary medicalization. However, on the basisof the data illustrated in Table 2, it can be noted that therate of medical interventions is remarkably high. Gould[1] notes that this type of behavior is more likely in largebirth centers routinely accustomed to managing patholog-ical pregnancies.
There are other reports about the excessive number ofmedical interventions in low-risk patients [4, 5] particu-larly concerning oxytocin administration. The presentstudy highlights a rise in risk of an overall operativedelivery of about 4.7. Oxytocin augmentation in clinicalpractice appears to pose many dangers [6-8]. Concerningthe delivery outcome, observational studies report thatoxytocin administration seems to reduce labor time innulliparas and to increase cesarean delivery both in nul-liparas and in multiparas [6, 7]. On the contrary, in ran-domized studies, it is reported that oxytocin augmenta-tion reduces the labor times of nulliparas without causingan increase in the number of cesareans or other unfavor-able outcomes [9-12]. We believe that in randomizedstudies cited, the procedure for oxytocin administrationwas strictly adhered to. On the contrary, observationalstudies (among which the present one) do not verifywhether oxytocin augmentation follows a precise proto-col, with a higher number of operative deliveries. Thispossibility is indirectly supported by Clark et al. [13].Said authors have demonstrated that a strict adherence toa check-list for oxytocin augmentation (that takes intoconsideration, among other factors, the frequency andquality of contractions and electronic fetal monitoring)annuls the dangers associated with the use of this drug.We are not able to assess which kind of protocol was fol-lowed during oxytocyn augmentation in the presentstudy, however it appears that oxytocin augmentationoverall causes an increase in the number of cesareandeliveries when it is administered at onset of cervicaldilation, independently of other variables and in particu-lar, independently of station. Because the first phases ofcervical dilation do not only depend on the effect of oxy-tocin, as illustrated in relation to the physiology of labor[14, 15], it may be dangerous to increase uterine contrac-
Table 4. — Odds ratio with 95% confidence intervals for thevariables influencing delivery outcome in patients whounderwent oxytocin augmentation, amniotomy, epiduralanalgesia, labor induction.
Patients with oxytocin augmentationOverall operative delivery Cesarean section Operative vaginal delivery
Multiparity 0.504 0.539C.I. 95% 0.335-0.759 C.I. 95% 0.340-0.854 /
p = 0.001 p = 0.009Intermediate risk 2.006 2.135
C.I. 95% 1.276-3.153 / C.I. 95% 1.228-3.711p = 0.003 p = 0.007
High risk 2.109 1.891C.I. 95% 1.379-3.224 / C.I. 95% 1.112-3.216
p = 0.001 p = 0.019Epidural 0.597 1.894
/ C.I. 95% 0.397-0.899 C.I. 95% 1.126-3.185p = 0.013 p = 0.016
Dilatation 0.493 0.409(increasing) C.I. 95% 0.428-0.567 C.I. 95% 0.344-0.487
p < 0.001 p < 0.001Patients with amniotomy
Overall operative delivery Cesarean section Operative vaginal delivery
Intermediate risk 3.047 1.992 2.319C.I. 95% 1.708-5.437 C.I. 95% 1.079-3.679 C.I. 95% 1.176-4.573
p < 0.001 p = 0.028 p = 0.015High risk 2.518 2.218 1.385
C.I. 95% 1.467-4.322 C.I. 95% 1.249-3.940 C.I. 95% 0.704-2.726p = 0.001 p = 0.007 N.S.
Oxytocin 3.492 2.698 2.434augmentation C.I. 95% 2.008-6.071 C.I. 95% 1.426-5.104 C.I. 95% 1.145-5.177
p < 0.001 p = 0.002 p = 0.021Dilatation 0.695 0.637
(increasing) C.I. 95% 0.577-0.838 C.I. 95% 0,521-0,780 /p < 0.001 p < 0.001
Station (lowering) 0.388 0.513 0.611C.I. 95% 0.247-0.608 C.I. 95% 0.324-0.813 C.I. 95% 0.408-0.916
p < 0.001 p = 0.005 p = 0.017Patients with epidural
Overall operative delivery Cesarean section Operative vaginal delivery
Multiparity 0.577 0.483C.I. 95% 0.355-0.939 / C.I. 95% 0.263-0.887
p = 0.027 p = 0.019Intermediate risk 1.605
C.I.95% 0.956-2.695 / /N.S.
High risk 1.650C.I. 95% 1.015-2.681 / /
p = 0.043Oxytocin 3.476 2.534 3.128
augmentation C.I. 95% 2.115-5.712 C.I. 95% 1.309-4.905 C.I. 95% 1.687-5.801p < 0.001 p = 0.006 p < 0.001
Labor induction 2.016C.I. 95% 1.009-4.029 / /
p = 0.047Dilatation 0.381 0.198
(increasing) C.I. 95% 0.302-0.480 C.I. 95% 0.141-0.279 /p < 0.001 p < 0.001
Station (lowering) 0.435 0.372C.I. 95% 0.321-0.589 C.I. 95% 0.256-0.540 /
p < 0.001 p < 0.001Patients with labor induction
Overall operative delivery Cesarean section Operative vaginal delivery
Multiparity 0.338C.I. 95% 0.114-1.000 / /
p = 0.05
Oxytocin / / 6.651augmentation C.I.95% 0.816-54.197
N.S.
Odds ratio with 95% confidence intervals for the variables influencing delivery outcome inpatients who underwent oxytocin augmentation, amniotomy, epidural analgesia, laborinduction.

U. Indraccolo, S. Calabrese, S.R. Indraccolo 276
tions during the latent phase of labor. Moreover, oxytocinaugmentation increases the number of operative vaginalbirths. It may be that administering oxytocin in increas-ing doses for too long a time could cause uterine inertiaand therefore call for vacuum extraction. This fact justi-fies the data supporting successful spontaneous deliveryoutcomes when oxytocin augmentation is initiated uponadvanced cervical dilation, so that the drug is infused fora shorter amount of time. Therefore we feel it is justifiedto defer the use of the oxytocin as much as possible ratherthan administer it from the first stage of labor. This canalso be inferred by the results of Daniel-Spiegel et al.[16] which, after labor induction using oxytocin, does notreveal any benefits when it is continued to be used afterlabor has begun.
It is reported that amniotomy slightly increases thenumber of cesarean deliveries without clear implicationson cervical dilation at the time it is carried out [17]. Someauthors [18-20] have reported that amniotomy beyond a3 cm dilation could prevent dysfunctional labor. Addi-tionally, Barrett et al [20] confirm that amniotomy tendsto increase the rate of early deceleration revealed by car-diotocography. Johnson et al. and Sheiner et al. [21, 22]report that routine amniotomy may shorten the first phaseof labor only in nulliparas, increasing the overall cesareandeliveries. Cesareans should be due to the anomalies ofthe cardiotochographic pattern induced by the amniotomyitself [21]. However, the present study suggests thatamniotomy may also cause dystocia. In fact, if station islow when amniotomy is carried out, the probability of anoperative delivery is reduced. In addition, it does notappear that the procedure particularly increases cesareanbirths or operative vaginal births, demonstrating that thechoice of intervention depends on the evolution of labor.
Some reviews [23-25] have analyzed the effects ofepidural analgesia on delivery outcomes, revealing that itdoes not increase the number of cesareans but doesappear to increase the number of operative vaginal births,without there being a clear reason. In fact, the clinicalsignificance of longer labor times due to the epidural isnot yet understood [25] but does not appear to confer anyneonatal risk [23]. A study by Wong et al. [26] compar-ing epidural analgesia with systemic analgesia in nulli-paras has demonstrated that the former can shorten thetime required for cervical dilation, thereby shorteninglabor time, without increasing the number of cesareans oroperative vaginal births. That study suggests therapeuticuse of epidural analgesia during labor and the data pre-sented in our own study support this possibility. Epiduralanalgesia does not appear to cause increased risk of oper-ative deliveries because on one hand it reduces the prob-ability of cesareans and on the other it increases the prob-ability of operative vaginal birth. It is not possible toexplain the reason for this effect using the data here pre-sented. However, the decrease in number of cesareansseems to indicate that epidural analgesia facilitates themechanisms of cervical dilation. This effect appears toincrease with increased cervical dilation and station,while it seems annulled in patients induced with
prostaglandins or those who receive oxytocin augmenta-tion. A possible explanation could be connected withneurological involvement for cervical dilation [27],which, however, is not decisive if the mechanisms thatmodify the cervix are not triggered. Such mechanisms areset off by the prostaglandin analogues used for inducinglabor.
Concerning labor induction, the data are insufficient toallow for a sufficiently powerful multivariate analysis. Itappears to be confirmed that induced parturients can bemore susceptible to an operative delivery, as is alreadyknown [28, 29].
Some limitations in interpreting the data may appear. Inthe clinical setting the decisions for managing labor coulddiffer according to a subjective opinion of the obstetricrisk and of the need for intervention. For example, somemay attempt to prevent dysfunctional labor or to reducelabor time by intervening as soon as possible, whilesomeone else may try to limit any interventions alto-gether. Additionally, the protocol for oxytocin infusion,epidural analgesia, labor induction were not homoge-neous, as it may happen in routine care. Therefore, theindications and the modes of medical intervention vary.We have controlled the effect of each medical interven-tion assessing when it was performed, in relationship tostation and cervical dilatation. However, we are not ableto state which kind of protocol is better for each kind ofintervention.
Conclusion
When medical interventions during labor are usedexcessively, they bring about an excessive number ofoperative deliveries, both in high-risk pregnancies andabove all, in those not at risk. Since we are not able toassess which is the best protocol for each medical inter-vention, each intervention should be limited or deferredas much as possible to favor the “normal” evolution oflabor [1]. The only exception: it is considered very usefulto supply “on demand” epidural analgesia in light of thedemonstrated reduction of cesarean deliveries.
References[1] Gould D.: “Normal labor: a concept analysis”. J. Adv. Nurs., 2000,
31, 418.[2] Romano A.M., Lothian J.A.: “Promoting, protecting, and support-
ing normal birth: a look at the evidence”. J. Obstet. Gynecol.Neonatal. Nurs., 2008, 37, 94.
[3] “Diagnosi di gravidanza ed igiene della gravidanza”. In: PescettoG., De Cecco L., Pecorari D., Ragni N. (eds.). Ginecologia e Oste-tricia. Rome, Società Editrice Universo, 2001, 2, 1109.
[4] Moen M.S., Holmen M., Tollefsrud S., Rolland R.: “Low-riskpregnant women in an obstetric department-how do they givebirth?”. Tidsskr Nor Laegeforen, 2005, 125, 2635.
[5] Oliveira M.I., Dias M.A., Cunha C., Leal Mdo C.: “Quality assess-ment of labor care provided in the Unified Health System in Riode Janeiro, Southeastern Brazil, 1999-2001”. Rev. Saude Publica,2008, 42, 895.
[6] Svärdby K., Nordström L., Sellström E.: “Primiparas with orwithout oxytocin augmentation: a prospective descriptive study”.J. Clin. Nurs., 2007, 16, 179.

Impact of the medicalization of labor on mode of delivery 277
[7] Battista L., Chung J.H., Lagrew D.C., Wing D.A.: “Complicationsof labor induction among multiparous women in a community-based hospital system”. Am. J. Obstet. Gynecol., 2007, 197, 241.e.
[8] Oscarsson M.E., Amer-Wåhlin I., Rydhstroem H., Källén K.:“Outcome in obstetric care related to oxytocin use. A population-based study”. Acta Obstet. Gynecol. Scand., 2006, 85, 1094.
[9] Cammu H., Van Eeckhout E.: “A randomised controlled trial ofearly versus delayed use of amniotomy and oxytocin infusion innulliparous labor”. Br. J. Obstet. Gynaecol., 1996, 103, 313.
[10] Sadler L.C., Davison T., McCowan L.M.: “A randomised con-trolled trial and meta-analysis of active management of labor”.BJOG, 2000, 107, 909.
[11] Hinshaw K., Simpson S., Cummings S., Hildreth A., Thornton J.:“A randomized controlled trial of early versus delayed oxytocinaugmentation to treat primary dysfunctional labor in nulliparouswomen”. BJOG, 2008, 115, 1289.
[12] Dencker A., Berg M., Bergqvist L., Ladfors L., Thorsén L.S., LiljaH.: “Early versus delayed oxytocin augmentation in nulliparouswomen with prolonged labor-a randomised controlled trial”.BJOG, 2009, 116, 530.
[13] Clark S., Belfort M., Saade G., Hankins G., Miller D., Frye D. etal.: “Implementation of a conservative checklist-based protocolfor oxytocin administration: maternal and newborns outcomes”.Am. J. Obstet. Gynecol., 2007, 197, 480.e.
[14] Kelly R.W.: “Inflammatory mediators and cervical ripening”. J.Reprod. Immunol., 2002, 57, 217.
[15] Smith R.: “Parturition”. N. Engl. J. Med., 2007, 356, 271.[16] Daniel-Spiegel E., Weiner Z., Ben-Shlomo I., Shalev E.: “For how
long should oxytocin be continued during induction of labor?”.BJOG, 2004, 111, 331.
[17] Smyth R.M., Alldred S.K., Markham C.: “Amniotomy for short-ening spontaneous labor”. Cochrane Database Syst. Rev., 2007,17, CD006167.
[18] Fraser W.D., Sauve R., Parboosingh I.J., Fung T., Sokol R.,Persaud D.: “A randomized controlled trial of early amniotomy”.Br. J. Obstet. Gynaecol., 1991, 98, 84.
[19] Fraser W.D., Marcoux S., Moutquin J.M., Christen A.: “Effect ofearly amniotomy on the risk of dystocia in nulliparous women.The Canadian Early Amniotomy Study Group”. N. Engl. J. Med.,1993, 328, 1145.
[20] Barrett J.F., Savage J., Phillips K., Lilford R.J.: “Randomized trialof amniotomy in labor versus the intention to leave membranesintact until the second stage”. Br. J. Obstet. Gynaecol., 1992, 99, 5.
[21] Johnson N., Lilford R., Guthrie K., Thornton J., Barker M., KellyM.: “Randomised trial comparing a policy of early with selectiveamniotomy in uncomplicated labor at term”. Br. J. Obstet.Gynaecol., 1997, 104, 340.
[22] Sheiner E., Segal D., Shoham-Vardi I., Ben-Tov J., Katz M.,Mazor M.: “The impact of early amniotomy on mode of deliveryand pregnancy outcome”. Arch. Gynecol. Obstet., 2000, 264, 63.
[23] Liu E.H., Sia A.T.: “Rates of caesarean section and instrumentalvaginal delivery in nulliparous women after low concentrationepidural infusions or opioid analgesia: systematic review”. BMJ,2004, 328, 1410.
[24] Anim-Somuah M., Smyth R., Howell C.: “Epidural versus non-epidural or no analgesia in labor”. Cochrane Database Syst. Rev.,2005, 19, CD000311.
[25] Gaiser R.R.: “Labor epidurals and outcome”. Best. Pract. Res.Clin. Anaesthesiol., 2005, 19, 1.
[26] Wong C.A., Scavone B.M., Peaceman A.M., McCarthy R.J., Sul-livan J.T., Diaz N.T. et al.: “The risk of cesarean delivery with neu-raxial analgesia given early versus late in labor”. N. Engl. J. Med.,2005, 352, 655.
[27] Hollingsworth M., Isherwood C.N.: “Mechanical responses of theisolated cervix and uterine horn of pregnant rats near term todrugs”. Br. J. Pharmacol., 1978, 63, 513.
[28] Lin M.G., Rouse D.J.: “What is a failed labor induction?”. Clin.Obstet. Gynecol., 2006, 49, 585.
[29] Grobman W.A.: “Elective induction: When? Ever?”. Clin. Obstet.Gynecol., 2007, 50, 537.
Address reprint requests to:U. INDRACCOLO, M.D.Via Montagnano, 1662032 Camerino (MC) Italye.mail: [email protected]

278
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
[789/27]
Revised manuscript accepted for publication August 31, 2009
Maximizing the benefits of screening mammography forwomen 40-49 years old
K. Bastardis-Zakas1, G. Iatrakis2, I. Navrozoglou3, P. Peitsidis2, N. Salakos4, P. Malakassis2, S. Zervoudis2, 3
1Technological Institute of Athens, School of Healthcare Sciences, Faculty of Obstetrics, Athens2Lito Hospital Department of Mastology. Athens
3Ioannina University, Gynecology Department, Breast Unit, Ioannina4Aretaieio University Hospital, Gynecology Department, Athens (Greece)
[1078/29]
Introduction
The unequivocal belief in mammography as a benefi-cial factor when applied to women aged 50 years andolder is the result of several randomized controlled trialswhich indicate a mortality risk reduction of about 25%[1] in those women who underwent screening proce-dures. What has been less certain, is whether or notscreening mammography is of a similarly advantageousnature on younger age groups, namely on women aged40-49 years of age. Several randomized controlled trials(RCTs) [1-8] have been conducted to elucidate on thematter, beginning with the HIP trial of Greater New York[4] up to the NBSS Canadian study [7] and the greatlyanticipated British Age Trial [8].
The results of most of the trials were consistent withthe approach of conducting screening mammography onyounger women, albeit, statistically those results did notreach significance – with two possible reasons beingeither that indeed mammography does not constitute aneffective screening method on those specific age groups,or simply because the RCTs themselves were of a limited
statistical power to detect any actual difference betweenthe control and study groups. This latter possibility standsas such, primarily because the number of participants wasindeed small in relation to the issue at hand, which alsoposes an issue in accordance with the relatively low inci-dence of breast cancer in that age group when comparedto older age groups [9-11].
The answer to the statistical weakness of several sepa-rate studies came in the form of meta-analyses whichcombined different RCTs, adjusting their different modelapproach in accordance to the studies’ heterogeneity. Atleast seven meta-analyses [1, 12-17] have been conductedso far, at least three of which [1, 2, 5, 18, 19] have beenrevised and updated some years after the initial publica-tion. Only three of those meta-analyses [11, 15, 16]reached a statistical significance regarding the relativemortality risk reduction.
With the majority of studies showing a non-significanttrend towards the effectiveness of screening mammo-grams in younger women, and only a handful demon-strating statistical significance, the question arose: whywas mammographic sensitivity in younger age groupslagging behind that of older women? Certain studies [20,21] indicated that mammographic sensitivity was greatly
Summary
Background: While women aged 50 and older are broadly considered to benefit from screening mammograms, the evidence ofany similar advantages for younger women are still considered insufficient to form any substantial conclusions on the matter. Theprimary goal of this study was to examine whether or not the mortality rate of younger women is benefited by mammography, andif so, how can this beneficial effect be maximized. Methods: The authors have taken into account all available randomized controltrials (RCTs) and have conducted a meta-analysis based on those RCTs to study the effect of mammography on the mortality rateof women younger than age 50. Further interpretation on various aspects of the results has also led to separate meta-analyses, withthe RCTs included grouped in accordance to the mean time interval between screening mammograms employed by each study. Thefindings and conclusions of the comparison were used to calculate the number of mammograms necessary to reduce the absolutedeath risk, depending on the time interval between screening mammograms. Results: The meta-analysis indicated a reduction inbreast-cancer mortality in the intervention group, which reached statistical significance (relative risk (RR) 0.81 [95% CI 0.71-0.93]p < 0.01). Furthermore, when the RCTs included were grouped according to their mean time interval between mammograms, therewas a definite increase of statistical significance in favor of those RCTs with shorter interval times (RR 0.76 [95% CI 0.64-0.89] p< 0.01). Conclusions: The significant mortality rate reduction demonstrated by the meta-analytical results is a key indicator of thebeneficial effect of mammography on the age group of women younger than 50. Additionally, the increase in the aforesaid signifi-cance when combining RCTs with short time intervals between mammograms, as opposed to those RCTs with longer intervals, sug-gests that the optimal use of mammographic screening lies with the former. This is better demonstrated when taking in account ourapproach to answering the practical question of “how many screening mammograms will take to save one life?” in correlation withthe mean time interval involved.
Key words: Mammography before 50 years old; Screening mammography; Mammography in young women.

Maximizing the benefits of screening mammography for women 40-49 years old 279
affected by the density of breast tissue, which is greaterin younger women, whereas rapid tumor growth sharedan equally important role in decreased sensitivity whenthe time-interval between mammograms was lengthened.
With the aforementioned issues in mind, we facilitatedthe first data of the ten-year follow-up results made avail-able by the British Age Trial. We used these data toconduct our own meta-analysis combining the majorityof previous RCTs and we furthermore explored and inter-preted different meta-analytical plots in an attempt toshed some light on the importance of interval timesbetween mammograms and the level on which they influ-ence the ultimate effectiveness of mammography onyounger women.
Materials & Methods
The results of the analyses of all available RCTs [1, 3-8] weregathered in order to form the statistical pool needed to conductthe meta-analysis. The relative risks (RRs) and confidenceintervals (CIs) were used as presented without re-conductingseparate analyses of individual data for each RCT and re-eval-uated data were used in cases where that approach was applica-ble [1, 2, 5, 18, 19]. The data were analyzed using MIX v1. 7[22, 23]. All meta-analyses conducted utilized the inverse vari-ance method with a fixed-effects model, although a random-effects model and homogeneity check were also used for cross-check purposes. All RCTs mentioned in this paper were usedfor the final meta-analysis, excluding the Canadian NBSS Trial.An all inclusive meta-analysis has nevertheless been conductedto study whether the exclusion of this study significantly alteredthe outcome, and a sensitivity analysis was also used to studythe same matter.
Once the results of the meta-analysis were obtained, thestudies included were sorted by the mean interval time theyused between screening mammograms. The statistical trend wasexamined and two new meta-analyses, consisting of thosestudies with a mean interval time shorter than 24 months andthose consisting of studies with a mean interval time longer than24 months, respectively, were conducted. The relative riskreduction (RRR) was calculated for all groups of studies thatwere used to examine if and when that reduction was more sig-nificant and to draw a comparison where applicable.
Finally, we calculated the absolute death risk reduction forthe two groups consisting of studies using different time inter-vals to answer the practical question of “how many screeningmammograms are needed in order to save a life?” and explicateits correlation to the time interval between screening mammo-grams.
Results
The meta-analysis resulted in statistical significance(RR 0.81 [95% CI 0.71 - 0.93] p = 0.0025) (Figure 1).Although homogeneity among the included samples jus-tified the use of a fixed-effects model (Q = 8.0431, pvalue = 0.4293), we also conducted a meta-analysis usinga random-effects model and the results of each approachwere shown to be identical. All studies were included,with the exception of the Canadian NBSS Trial and toascertain that this study’s exclusion did not affect the sta-tistical significance of the results, we used as reference
both a sensitivity analysis plot (Figure 2) as well asanother meta-analysis (Figure 3), this time including theNBSS Trial. The results of this all-including meta-analy-sis were also significant (RR 0.84 [95% CI 0.74 - 0.95] p= 0.0049).
Once statistical significance was ascertained, wemoved on to examine possible trends in our results andtheir respective interpretations. During that procedure,we examined the cumulative forest plot of our meta-analysis with the RCTs arranged by decreasing meantime interval between mammograms. A cumulative plotgraphically exhibits the meta-analytical outcome result-ing by adding studies up to that point and it was thusdemonstrated that with each addition of a study of ashorter mean interval time, the overall RR decreasedwhile the RRR increased (Figure 4). To better examinethe importance of time interval between mammograms,we divided the included RCTs in two groups, one con-sisting of RCTs with a mean time interval between mam-mograms over 24 months and a second group withstudies of a mean time interval less than 24 months. Wethen conducted a separate meta-analysis for each group(Figure 5) and calculated the relative risk reduction (= 1- RR) for both of these groups to present a viable com-parison of the effect of time intervals between screeningmammograms. For the group of studies with a mean timeinterval shorter than 24 months, the RRR was shown tobe 24% (RR 0.76 [95% CI 0.64 - 0.89] p = 0.0007) whilefor the group of studies with mean interval times longerthan 24 months, the results were not significant (RR 0.96[95% CI 0.74-1.25] p = 0.7856).
We then moved on to calculate the RRR for all RCTsincluded in the meta-analysis and it was found to be 19%(RR 0.81 [95% CI 0.71-0.93] p = 0.0025). We comparedthis result with that of the meta-analysis consisting onlyof RCTs with interval times shorter than 24 months andalthough in both cases the p value was well below 0.01,the significance of the results when considering only theshort interval time RCTs, increases 3-fold.
With that in mind, we went ahead to calculate thereduction of absolute death risk (RADR) for both cases.The RADR is equal to the RRR, multiplied by theabsolute death risk (ADR). Keen & Keen [24] have esti-mated that the ADR at age 40 is 0.475% and that riskmore than doubles between the starting ages of 45 and55. We have chosen the modest approach of using thelowest percentage, that of 0.475%. Using the aforemen-tioned formula (RADR = RRR * ADR) we calculated theRADR to be 0.0906% and 0.1155% for all RCTs of themeta-analysis and for the shorter mean time intervalRCTs, respectively. Because the ADR acts as a constant,the 22% difference between the two results remainsfixed, regardless of the actual value of the ADR.
Discussion
Our aim was to attempt a conclusive analysis of theprevious RCTs, facilitated by the relatively new resultsfrom the British Age Trial to statistically ascertain

K. Bastardis-Zakas, G. Iatrakis, I. Navrozoglou, P. Peitsidis, N. Salakos, P. Malakassis, S. Zervoudis 280
whether or not, screening mammography’s beneficialeffects transcends the 50-year-old limit and positivelyaffects younger women as well.
The study selection was based on the up to standardmethodology from a statistical and academic point ofview. As such, all studies were included with the excep-tion of the NBSS trial which was found lacking the nec-essary credibility for adding to the statistical conclusionsfacilitated by the rest of the RCTs. The reasons for thislack of credibility, as have been explicitly described by anumber of publications [25-27], include the nature of theselection of the participants for this specific trial, as theNBSS study invited volunteers which were afterwardsrandomized in study or control groups and thus, a selec-
tion bias may have been generated. Additionally, theNBSS study prescreened all participants with a clinicalbreast examination, something which could have weak-ened the findings of the trial by distributing women withclinical findings to the control and study groups. Thisprescreening procedure also leaves room for selectionbias within the study, a possibility all the more strikingwhen considering the noteworthy difference of advancedcancer occurrences between the control and the studygroup: the rate of advanced cancers of the latter was 3.8times higher compared to that of the control group, a dif-ference that would constitute reason enough to excludethis study from a meta-analysis regardless of the reasonsthat caused it. Furthermore, a rough 26% of the control
Figure 1. — Forest plot of the meta-analysis excluding theNBSS Study.Figure 2. — Sensitivity plot of the meta-analysis. A sensitivityanalysis shows to what extent each study influences the com-bined result. Each diamond represents the outcome whichresults by excluding the corresponding study.Figure 3. — Forest plot of the meta-analysis including theNBSS study for cross-check.Figure 4. — Cumulative plot of the meta-analysis sorted bymean-time interval between screening mammograms. Each dotrepresents the meta-analytic outcome as a result of includingthe studies up to that point.Figure 5. — Comparative figure of meta-analyses includingshort-time interval RCTs and long-time interval RCTs, respec-tively.
Short interval (> 24 mo) studies Long interval (> 24 mo) studies

Maximizing the benefits of screening mammography for women 40-49 years old 281
group underwent mammography screening during thestudy. Criticism has also been addressed towards thequality of the mammography conducted, which may haveresulted in false-negative results and unfounded encour-agement to the study group as well as to the short-followup period of the study. For those reasons, we chose not toinclude the findings of this study in our meta-analysis.
Although the NBSS study was not included, we wantedto make sure that the significant results of our meta-analysis did not occur due to the exclusion of this trialalone. We thus conducted a separate, all-including meta-analysis and a sensitivity analysis. The all-inclusive meta-analysis turned out significant results while the exclusionof the study was adequately supported by the sensitivityanalysis as well.
During examination of the cumulative plot of the meta-analysis, it was observed that a tendency of increasingsignificance occurred simultaneously with a decrease ofthe mean interval time between screening mammograms.Further examination using two separate meta-analyses,one for short-interval time mammograms and one forlong-interval time ones, provided us with statistical evi-dence that more frequent screening mammogramsprovide more significant results in terms of mortalityreduction. This statistically apparent indication is consis-tent with previous suggestions [28-33] that due to the dif-ferences of mastic density between younger and olderwomen as well as to the more aggressive nature of tumorsaffecting the former, a more frequent approach of mam-mographic screening should be implemented.
In particular, while the RRR for the short-interval timemammograms was a promising 24%, the respective resultfor long-interval time mammograms was not significantstatistically. When the RR of the short-interval timemammograms was compared to the RR of all studiesincluded (short and long interval time alike) the signifi-cance factor was found to increase 3-fold in favor of theformer. This pointed us in a direction of turning numbersto more practical functions, and we attempted to seek ananswer to the question of “how many mammograms doesit take to save a life?”.
The results were naturally in favor of the short-timeinterval approach when compared to all time intervalsincluded, with 865 mammograms with a short-time inter-val between them, as opposed to 1,103 mammogramswith a longer intervening time-span. What is noteworthyis that although the actual numbers may vary, the differ-ence between them remains a fixed 22% in favor of theshort-interval time mammograms. The idea that fewermammograms are needed to save a life while at the sametime they should be more frequent, may seem hard tograsp initially, but considering a fixed time-span ofscreening might ease the concept: in a 4-year period ofscreening, four lives will be respectively saved if an ade-quate number (in our case, 865) of women attend eachyear. If the screening examination was biannual, only twolives would have been saved if an adequate number ofwomen (1,103 in our case) did attend every two years. Inour simplified example, this means that out of 3,460
women, four will be saved in four years if annual screen-ing is implemented, while out of 4,412 women, only twowill be saved in the same period of time, if implementingbiannual screening.
Conclusions
The statistical significance of the meta-analysis, is anexplicit indicator of the beneficial results of screeningmammography in women younger than 50 years. TheRRR of 19% can be considered as a designating factor inthe approach of screening mammography where theminimum age for regular screening mammograms isabove the 50-year-old “barrier”.
Moreover, the considerable difference between theRRR of those studies comprising short-interval timesbetween mammograms and their long-interval time coun-terparts, represents the rather obvious advantage of theformer in terms of mortality reduction. In a more practi-cal aspect of the results, the obtained values from themeta-analyses of the above-mentioned groups of long-interval and short-interval studies can be used to calculatethe number of screening mammograms needed to avertan event of RADR, or, put simply, to save a life. Havingthe RADR calculated, the number of mammogramsneeded to save a life when taking into account all studies,long-time and short-time intervals alike, is 1/0.0906% =1103 while when using the short-interval studies alone,the number of necessary screening mammograms dropsto 1/0, 1.155% = 865.
References[1] Nystrom L., Andersson I., Bjurstam N., Frisell J., Nordenskjold B.:
“Long-term effects of mammography screening: updated overviewof the Swedish randomised trials”. Lancet, 2002, 359, 909.
[2] Andersson I., Janzon L.: “Reduced breast cancer mortality inwomen under age 50: updated results from the Malmo Mammo-graphic Screening Program”. J. Natl. Cancer Inst. Monogr., 1997,22, 63.
[3] Bjurstam N., Bjorneld L., Warwick J., Sala E., Duffy S.W.,Nyström L. et al.: “The Gothenburg Breast Screening Trial”. Am.Can. Soc., 2003, 97, 2387.
[4] Shapiro S., Venet W., Strax P., Venet L.: “Periodic Screening forBreast Cancer”. Baltimore, Johns Hopkins University Press, 1988.
[5] Tabar L., Vitak B., Chen H.H., Duffy S.W., Yen M.F., Chiang C.F.et al.: “The Swedish two-county trial twenty years later: updatedmortality results and new insights from long-term follow-up”.Radiol. Clin. North Am., 2000, 38, 625.
[6] Alexander F.E., Anderson T.J., Brown H.K., Forrest A.P., HepburnW., Kirkpatrick A.E. et al.: “14-years of follow-up from the Edin-burgh randomised trial of breast-cancer screening”. Lancet, 1999,353, 1903.
[7] Miller A.B., To T., Baines C.J., Wall C.: “The Canadian NationalBreast Screening Study 1: breast cancer mortality after 11 to 16years of follow-up”. Ann. Intern. Med., 2002, 137, E305.
[8] Moss S.M., Cuckle H., Evans A., Johns L., Waller M., Bobrow L.:“Effect of mammographic screening from age 40 years on breastcancer mortality at 10 years’ follow-up: a randomized controlledtrial”. Lancet, 2006, 368, 2053.
[9] Horner M.J., Ries L.A.G., Krapcho M., Neyman N., Aminou R.,Howlader N. et al. (eds). SEER Cancer Statistics Review, 1975-2006, National Cancer Institute, 2006.
[10] Office for National Statistics, Cancer Statistics registrations: Reg-istrations of cancer diagnosed in 2006, England. Series MB1 no.37. 2009, National Statistics, London.

K. Bastardis-Zakas, G. Iatrakis, I. Navrozoglou, P. Peitsidis, N. Salakos, P. Malakassis, S. Zervoudis 282
[11] American Cancer Society Breast Cancer Facts & Figures, 2005-2006.
[12] Anonymous. Breast-cancer screening with mammography inwomen aged 40-49 years. Swedish Cancer Society and theSwedish National Board of Health and Welfare. Int. J. Cancer,1996, 68, 693.
[13] Demissie K., Mills O.F., Rhoads G.G.: “Empirical comparison ofthe results of RCTs and case-control studies in evaluating theeffectiveness of screening mammography”. J. Clin. Epidemiol.,1998, 51, 81.
[14] Glasziou P.P., Woodward A.J., Mahon C.M.: “Mammographicscreening trials for women aged under 50: a quality assessmentand meta-analysis”. Med. J. Australia, 1995, 162, 625.
[15] Hendrick R.E., Smith R.A., Rutledge J.H. 3rd, Smart C.R.: “Benefitof screening mammography in women aged 40-49: a new meta-analysis of RCTs”. J. Nat. Cancer Inst. Monogr., 1997, 22, 87.
[16] Kerlikowske K., Grady D., Rubin S.M., Sandrock C., Ernster V.L.:“Efficacy of screening mammography”. JAMA, 1995, 273, 149.
[17] Nystrom L., Rutqvist L.E., Wall S., Lindgren A., Lindqvist M.,Rydén S. et al.: “Breast cancer screening with mammography:overview of Swedish randomised trials”. Lancet, 1993, 341, 974.
[18] Glasziou P., Irwig L.: “The quality and interpretation of mammo-graphic screening trials for women ages 40-49”. J. Nat. CancerInstit. Monographs, 1997, 22, 73.
[19] Kerlikowske K.: “Efficacy of screening mammography amongwomen aged 40 to 49 years and 50 to 69 years: comparison of rel-ative and absolute benefit”. J. Nat. Cancer Instit. Monographs,1997, 22, 79.
[20] Buist D.S.M., Porter P.L., Lehman C., Taplin S.H., White E.:“Factors contributing to mammography failure in women aged 40-49 years”. J. Natl. Cancer Inst., 2004, 96, 1432.
[21] Organizing Committee and Collaborators, Falun Meeting:“Breast-cancer screening with mammography in women aged 40-49 years”. Int. J. Cancer, 1996, 68, 693.
[22] Bax L., Yu L.M., Ikeda N., Tsuruta H., Moons K.G.M.: “Develop-ment and validation of MIX: comprehensive free software formeta-analysis of causal research data”. BMC Med. Res. Methodol.,2006, 6, 50.
[23] Bax L., Yu L.M., Ikeda N., Tsuruta H., Moons K.G.M.: “MIX:comprehensive free software for meta-analysis of causal researchdata”. Version 1.7. http://mix-for-meta-analysis.info, 2008.
[24] Keen J.D., Keen J.E.: “What is the point: will screening mam-mography save my life?”. BMC Med. Inform. Decis. Making,2009, 9, 18.
[25] Leitch M.: “Controversies in breast cancer screening”. The Amer-ican Cancer Society National Conference on GynecologicCancers, Washington, DC, April 6-8, 1995.
[26] Kopans D.B.: “Screening mammography for women age 40 to 49years”. Ann. Int. Med., 2007, 147.
[27] Green B., Taplin S.: “Breast cancer screening controversies”.JABFP, 2003, 16, 233.
[28] Feig S.A.: “Estimation of currently attainable benefit from mam-mographic screening of women aged 40-49 years”. Cancer, 1995,75, 2412.
[29] Feig S.A.: “Increased benefit from shorter screening mammographyintervals for women ages 40-49 years”. Cancer, 1997, 80, 2035.
[30] Feig S.A.: “Determination of mammographic screening intervals with surrogate measures for women aged 40-49 years”. Radiology,
1994, 93, 311.[31] Tabar L., Fagerberg G., Day N.E., Holmberg L.: “What is the
optimum interval between screening examinations? An analysisbased on the latest results of the Swedish Two-County breastcancer screening trial”. Br. J. Cancer, 1987, 55, 547.
[32] Feig S.A.: “Factors contributing to mammography failure inwomen aged 40-49 years: expert perspective”. Breast Diseases: AYear Book”. Quarterly, 2006, 16, 323.
[33] Moskowitz M.: “Breast cancer. Age-specific growth rates andscreening strategies”. Radiology, 1986, 161, 37.
Address reprint requests to:S. ZERVOUDIS, M.D., Ph.D.Lito Maternity HospitalDepartment of Mastology 7-13. Mouson street11524 Athens (Greece)e-mail: [email protected]

283
Revised manuscript accepted for publication November 26, 2009
Multidisciplinary approach during menopausal transitionand postmenopause in Brazilian women
I.C.E. Sorpreso, L.H.L. Vieira, M.A. Haidar, M.G. Nunes, E.C. Baracat, J.M. Soares Júnior1Department of Gynecology, Discipline of Gynecological Endocrinology, Federal University of São Paulo (UNIFESP) and Escola Paulista
de Medicina (Paulista Medical School) (EPM), São Paulo (Brazil)
[1063/29]
Introduction
Population ageing occurs in many developed and devel-oping countries. Life expectancy for Brazilian women is75.6 years [1]. More and more women experience hor-monal alterations related to menopausal transition andpost-menopause. Not only in developed countries but alsoin developing ones there is an increasing tendency in lifeexpectancy for women who live with diseases during theageing years [2]. Health care and adequate treatment areessential to maintain life quality.
Women’s menopausal transition and postmenopausalperiod is the passage from the reproductive phase (men-acme) to senescence that generally occurs between 40and 65 years [3]. In Brazilian women, natural menopauseoccurs between 48 and 50 years. It is considered prema-ture menopause when it occurs before 40 years and latemenopause after 52 years [4, 5].
Menopausal transition begins with the variation ofmenstrual cycle duration with high follicle stimulatinghormone (FSH) and ends with the last menstruation(menopause). After this phase, postmenopause takesplace [3]. Generally, in the first phase, women may pres-ent menstrual dysfunction and vasomotor symptoms,while in the second phase the effects of low levels ofestrogens may be stronger, resulting in hot flashes, uro-genital symptoms and cognitive alterations that mayaffect a woman’s life [4, 6].
The view of multiprofessional health care teamsfocused on menopause involves clinical and educationalaspects. Activities should be established and integrated,aiming at the success of methodology and development ofeach project. The knowledge about specific characteris-tics of each group to be studied is fundamental [7-9].
This study aims at identifying the clinical characteris-tics, the nutritional habits, the functional capacity and thequality of life of women during transitional menopauseand postmenopause.
Materials and Methods
This study is part of the Integral Program of Women HealthCare during Climaterium (PIAC). It is a comprehensive healthcare program and multidisciplinary project that gives orienta-tion to women in the transition to menopause and post-menopause. This project has been approved by the Ethics Com-mittee of the Federal University of São Paulo, São PauloMedical School (UNIFESP – EPM). Clinical, physical, nutri-tional and quality of life aspects that may interfere in women’shealth during menopause were analyzed. Voluntary patientswere examined at the Ambulatory Medical Center formenopausal transition and postmenopause, Discipline of Gyne-cological Endocrinology, Department of Gynecology, UNIFESP– EPM. The participants’ age varied between 40 and 70 yearsand they were nominally invited between June and August2006. After they were informed about the project, 115 womensigned a consent form to participate in the study. Exclusion cri-teria were: the use of any specific hormonal drugs to minimizemenopausal symptoms in the previous 12 months to the inter-view; ingestion of soy and its derivatives or herbal substances;acknowledged or suspicious neoplasia; kidney, thyroid or liverchronic diseases; cerebral vascular disease and myocardialinfarction; tabacco use (> 10 cigarettes a day) , hyperprolactine-mia; thromboembolic disturbances; diabetes mellitus; systemicarterial hypertension uncontrolled and age below 40. The vol-untary patients were divided into two groups: GI - transition tomenopause (n = 48); GII – postmenopause (n = 67) with nomenstruation for more than a year. The Kuppermann-BlattMenopausal Index (IMK), Women’s Health Questionnaire(WHQ), the Modified Stanford Health Assessment Question-naire – simplified, modified and validated version in Brazil(MHAQ-Brazil) and food frequency questionnaire were applied
SummaryObjective: To identify clinical, physical, life quality and nutritional aspects of Brazilian women during menopausal transition and
postmenopausal periods. Methods: 115 women agreed to participate in the study. They were divided into two groups: GI – menopausaltransition (n = 48) and GII - postmenopause (n = 67). The Kupperman-Blatt Menopausal Index (IMK) and Women’s Health Question-naire (WHQ), Food Frequency Questionnaire and functional capacity were used. All patients were examined and underwent clinicaland gynecological examination. Results: There was no significant difference in IMK, WHQ and functional capacity in either group.There was a higher caloric intake, especially in sugars, in postmenopause women than in menopausal transition women. Both groupspresented reduced parameters in life quality and functional capacity. Conclusion: Our data suggests that there is no significant differ-ence between women in menopausal transition and postmenopause, except in relation to the nutritional parameter. In both groups, thewomen presented low quality of life and reduced functional capacity.
Key words: Premenopause; Postmenopause; Diet; Comprehensive healthcare.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

I.C.E. Sorpreso, L.H.L. Vieira, M.A. Haidar, M.G. Nunes, E.C. Baracat, J.M. Soares Júnior 284
in all volunteers in this study. Participants underwent clinicaland gynecologic examination. Epidemiologic data was col-lected such as age, marital status, and economic status(employed or not employed). The IMK was developed in 1953and it has been used in many studies to evaluate the gravity ofmenopausal symptoms [10]. The index includes 11 symptoms.Each category is calculated in a four point scale in which zeroequals asymptomatic and four, severely symptomatic. Totalpoints for each item evaluates the gravity of menopausal symp-toms that may vary from 0 to 51 points, the higher the punctu-ation the more severe the complaint. The WHQ was the firstquestionnaire to be included in the International Health RelatedQuality of Life Outcomes Database [11]. It was validated inBrazil [12] to evaluate health status, because it is easy to under-stand and to apply. It has 36 items, divided into nine dimen-sions: depressive mood (six items); somatic symptoms (sevenitems); anxiety/fears (4 items); vasomotor symptoms (twoitems); sleep problems (three items); sexual functioning (threeitems); menstrual problems (four items); cognitive difficulties(three items) and attraction (three items). The scale varies fromzero to four points, the higher the score the more pronouncedthe suffering and dysfunctions. The MHAQ – Brazil [13, 14]allows for the evaluation of measured parameters in therapeuticassay and was used to check functional capacity. It has eightsub-scales which evaluate different aspects of the patient’s dailylife. Each one of these sub-scales presents two or three ques-tions related to physical activities. The patient was asked thedegree of difficulty he found in realizing a determined activityone week previous to the interview and assign a grade from zero(no difficulty) to three (impossibility to realize the activity). Thesub-scale grade is equivalent to the higher grade attributed inone of the two or three questions. The instrument’s final scoreis obtained by the arithmetical average of the grades of the eightsub-scales and it varied from zero to three. The questionnairerelated to food frequency [15] is based on the individual. It reg-isters or describes the patient’s usual food ingestion based on alist of different foods. The quantity and kind of food on the listvaried according to the aim of the evaluation. The food fre-quency questionnaire offers qualitative information on foodingestion. This study established the number of women whoingested specific food during the week previous to the inter-view. In the statistical analysis data was processed, and esti-mates were made about the distribution center and of the vari-ability of the results for numerical variables: average, standarddeviation and standard error for the average. The unpairedStudent’s t-test or chi-square test were use to compare dataobtained from the studied groups. The significance level wasfixed at 0.05 for both tests; 90% confidence limit was calculatedwith 40 patients per group.
Results
Clinical characteristics included age, body mass index(BMI), marital status, and economic status (Table 1). Theaverage age of women on transition menopause (48. 22 ±2.30) was lower than that of postmenopause women(55.10 ± 3.4, p < 0.05). There was no statistical differencebetween the groups as to BMI and marital status. In bothgroups BMI was above 26. Unemployment rate was sig-nificantly higher among postmenopause women.Table 2indicates IMK, WHQ and MHAQ - Brazil. There was nosignificant statistical difference between either group.Nutritional characteristics indicated that postmenopause
women presented higher daily consumption of carbohy-drates, especially of sugars (p < 0.05). The other itemsconsidered showed no significant difference (Table 3).
Discussion
This study aimed at identifying clinical, nutritionalhabits, functional capacity and life quality of womenduring the menopausal transition and postmenopause.These are important aspects to be considered when plan-ning multiprofessional care for the prevention of diseasesand quality of life of women. Our studies suggest that, in
Table 1. — Clinical characteristics of the participants of thestudy (average ± standard deviation).
Characteristics Menopausal transition Postmenopause p(n = 48) (n = 67)
Age* 48.22 ± 2.30 55.10 ± 3.4 < 0.01BMI* 26.66 ± 5.29 28.2 ± 6.02 0.15Marital Status** 0.63Single-Widow 18 28Married-Stable Union 20 30Divorced-Separated 10 9Economic Status** 0.02Unemployed 10 53Employed 38 44*Unpaired Student’s t-test was used. ** χ2 test was used to compare marital status andeconomic status.
Table 2. — Characteristics of the participants of the study(average ± standard deviation) in relation to IMK, functionalcapacity and WHQ.
Menopausal transition Postmenopause p(n = 48) (n = 67)
IMK* 20.83 ± 24.89 21.32 ± 21.96 0.86MHAQ-BR* 2.88 ± 1.45 2.8 ± 1.98 0.87WHQ*Depressive Mood 17.51 ± 8.45 17.92 ± 7.99 0.92Somatic Symptoms 17.55 ± 4.43 16.63 ± 5.12 0.78Cognitive difficulties 7.03 ± 2.33 6.88 ± 3.21 0.83Vasomotor Symptoms 4.71 ±1.95 4.91 ± 2.06 0.86Anxiety/Fears 8.41 ± 2.45 8.15 ± 2.07 0.79Sexual Functioning 5.51 ± 3.45 5.18 ± 3.99 0.98Sleep Problems 8.03 ± 2.77 7.98 ± 2.65 0.94Menstrual Symptoms 8.44 ± 1.45 _ _Attraction 7.50 ± 4.45 7.42 ± 2.67 0.77*Student’s t-test was used for data analysis.
Table 3. — - Characteristics of the participants of the studyconcerning nutrition.
Weekly food ingestion Menopausal transition Postmenopause p(n = 48) (n = 67)
Milk and Derivatives 40 61 0.71Vegetables/Fruit/Juice 32 39 0.13Sugars 24 66 0.002Rice, Pasta, Bread 44 63 0.67Eggs 18 25 0.88Canned Food/
Fried Food/Salted Food 11 21 0.28Coffee 35 57 0.70Red Meat 23 31 0.11χ2 test was used for data analysis.

Multidisciplinary approach during menopausal transition and postmenopause in Brazilian women 285
spite of age and hormonal differences in the menopausaltransition and postmenopausal women, additional fac-tors were not identified in relation to IMK, functionalcapacity and WHQ. IMK is an instrument used to eval-uate climacteric symptoms that may influence life qual-ity [16, 17].
The most important symptom is vasomotor-related andit might appear in transition menopause and in the firstyears of postmenopause [18]. It must be emphasized thatduring menopausal transition hot flashes appear whenthere is a decrease in estrogen concentration. It is knownthat during this period estrogen fluctuation occurs and thesymptoms may appear or disappear spontaneously [19]. Itshould be expected that menopausal transition womenpresented a lower IMK than that of postmenopausalwomen [16, 20]. Our work did not detect any significantdifference between either study group. However, climac-teric symptoms have a great impact on women’s qualityof life [21] and both groups presented moderate climac-teric symptoms. The WHQ evaluation for both groupswas not significant. However, depressive mood andsomatic symptoms were those mostly mentioned.
Functional capacity evaluated in this study did not pres-ent any statistical difference in either group. However, itwas noted that the functional capacity of women in bothgroups was reduced. The studied women are predisposedto limitations in their daily activities which may favor dis-eases that worsen their life quality during the ageingprocess [16]. The decrease in life quality may be shownin the WHQ and it is in accordance with this study.
Associations between weight gain in relation to agepoint to postmenopause as a cause [22]. Some otherauthors consider weight gain similar in postmenopausecompared to transition menopause [23]. We observed nosignificant differences in relation to BMI in either group.Some studies also did not find any correlation betweenBMI and climacteric symptoms [24].
An increase was noted in carbohydrate ingestion, espe-cially sugars in postmenopause women which may pre-dispose them to obesity, insulin resistance and diabetesmellitus [25]. The BMI in our study presented overweightthat may impair life quality and favor cardiovascular dis-eases [26, 27] as well as limit functional capacity [28].The highest sugar ingestion was observed in women inthe postmenopause study group which had a great num-ber of unemployed women. The decrease in income maycontribute not only to lower protein and vegetable inges-tion but also to the increase in daily consumption of car-bohydrates.
Conclusion
Both groups presented health conditions, life quality,functional capacity and nutritional habits inadequate forthe ageing process. A multidisciplinary approach shouldalert physicians about patients’ profiles and the focusshould be on the prevention of diseases and improvementin healthcare.
References[1] Carvalho J.A.M., Rodríguez-Wong L.L.: “A transição da estrutura
etária do Brasil da primeira metade do século XXI”. Cad. SaúdePública, 2008, 24, 597.
[2] Mathers C.D., Sadana R., Salomon J.A., Murray C.J.L., LopezA.D.: “Healthy life expectancy in 191 countries, 1999”. Lancet,2001, 357, 1685.
[3] Soules M.R., Sherman S., Parrott E., Rebar R., Santoro N., UtianW. et al.: “Executive summary: Stages of Reprodutive AgingWorkshop (STRAW)”. Climateric, 2001, 4, 267.
[4] De Lorenzi D.R.S., Baracat E.C., Saciloto B., Padilha I. Jr.:“Factors related to quality of life in post-menopause”. Rev. Assoc.Med. Bras, .2006, 52, 312.
[5] Marinho R.M., Soares J.M. Jr, Santiago R.C., Maganhin C.C.,Machado F., de Miranda Cota A.M., Baracat E.C.: “Effects ofestradiol on the cognitive function of postmenopausal women”.Maturitas., 2008, 60, 230.
[6] Galhardo C.L., Soares J.M. Jr, Simões R.S., Haidar M.A.,Rodrigues de Lima G., Baracat E.C.: “Estrogen effects on thevaginal pH, flora and cytology in late postmenopause after a longperiod without hormone therapy”. Clin. Exp. Obstet. Gynecol.,2006, 33, 85.
[7] Hunter M., O’dea: “An evaluation of a health education interven-tion for mid-aged women: five year follow-up of effects uponknowledge, impact of menopause and health”. Patient Educationand Counseling, 1999, 38, 249.
[8] Tremblay A., Sheeran L., Aranda S.K.: “Psychoeducational inter-ventions to alleviate hot flashes: a systematic review”. Menopause:The Journal of Menopause Society, 2008, 15, 193.
[9] Reyes-Morales H., Flores-Hernandez S., Tome-Sandoval P.,Perez-Cuevas R.: “A multifaceted education intervention forimproving family physicians’ case management”. Fam. Med.,2009, 41, 277.
[10] Kupperman H.S., Blatt M.H., Wiesbader H., Filler W.: “Compar-ative clinical evaluation of estrogenic preparations by themenopausal and amenorrheal indices”. J. Clin. Endocrinol.Metab., 1953, 13, 688.
[11] Hunter M.S.: “The Women’s Health Questionnaire (WHQ): Fre-quently Asked Questions (FAQ)”. Health and Quality of Life Out-comes, 2003, 1, 41.
[12] Silva Filho C.R., Baracat E.C., Conterno Lde O., Haidar M.A.,Ferraz M.B.: “Climacteric symptoms and quality of life: validityof women's health questionnaire”. Rev. Sau Publ., 2005, 39, 333.
[13] da Mota Falcão D., Ciconelli R.M., Ferraz M.B.: “Translation andcultural adaptation of quality of life questionnaires: an evaluationof methodology”. J. Rheumatol., 2003, 30, 379.
[14] Washburn R.A., Smith K.W., Jette A.M., Janney C.A.: “The Phys-ical Activity Scale for the Elderly (PASE): development and eval-uation”. J. Clin. Epidemiol., 1993, 46, 153.
[15] Sichieri R., Everhart J.: “Validity of a Brazilian food frequencyquestionnaire against dietary recalls and estimated energy intake”.Nutrition Research., 1998, 18, 1649.
[16] De Lorenzi D.R.S., Baracat E.C.: “Climatério e qualidade devida”. Femina, 2005, 33, 899.
[17] Satoh T., Ohashi K.: “Quality-of-life assessment in communitydwelling, middle aged, healthy women in Japan”. Climateric.,2005, 8, 146.
[18] Rapkin A.J.: “Vasomotor symptoms in menopause: physiologiccondition and central nervous system approaches to treatment”.Am. J. Obstet. Gynecol., 2007, 196, 97.
[19] McKinlay S.M., Brambilia D.J., Posner J.G.: “The normalmenopause transition”. Maturitas., 1992, 14, 103.
[20] Col N.F., Guthrie J.R., Politi M., Dennerstein L.: “Duration ofvasomotor symptoms in middle-aged women: a longitudinalstudy”. Menopause., 2009, 16, 453.
[21] Utian W.H.: “Psychosocial and socioeconomic burden of vasomo-tor symptoms in menopause: a comprehensive review”. HealthQual Life Outcomes, 2005, 5, 3.
[22] Brown W.J., Dobson A.J., Mishra G.: “What is a healthy weightfor middle aged women?”. Int. J. Obesity, 1998, 22, 520.
[23] Sabia S., Fournier A., Mesrine S., Boutron-Ruault M.C., Clavel-Chapleon F.: “Risk factors for onset of menopausal symptomsresults from a large cohort study”. Maturitas, 2008, 60, 108.

I.C.E. Sorpreso, L.H.L. Vieira, M.A. Haidar, M.G. Nunes, E.C. Baracat, J.M. Soares Júnior 286
[24] Nies M.A., Kershaw T.C.: “Psychosocial and environmental influ-ences on physical activity and health outcomes in sedentarywomen”. J. Nurs. Scholarship, 2002, 34, 243.
[25] Escamilla R., Putnik P.: “The role of acculturation in nutrition,lifestyle, and incidence of type 2 diabetes among Latinos”. J.Nutr., 2007, 137, 860.
[26] Brown T.J.: “Health benefits of weight reduction in post-menopausal women: a systematic review”. J. Br. Menopause Soc.,2006, 12, 164.
[27] Gupta R., Misra A., Pais P., Rastogi P., Gupta V.P.: “Correlation ofregional cardiovascular disease mortality in India with lifestyleand nutritional factors”. Int. J. Cardiol., 2006, 108, 291.
[28] Bouchard D.R., Soucy L., Sénéchal M., Dionne I.J., Brochu M.:“Impact of resistance training with or without caloric restriction onphysical capacity in obese older women”. Menopause, 2009, 16,66.
Address reprint requests to:I.C.E. SORPRESO, M.D.Rua Madre Cabrini, 332, Bloco B, apt 153CEP 04020-001-São Paulo (Brazil)e-mail: [email protected]

287
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication January 14, 2010
Reproductive outcomes after hysteroscopic metroplasty for uterine septum
F. Sendag, T. Mermer, S. Yucebilgın, K. Oztekin, O. BilginDepartment of Obstetrics and Gynecology, Faculty of Medicine, Ege University, Izmir (Turkey)
[1080/29]
Introduction
Because of the wide variation in clinical presentationand differences in the diagnostic criteria and techniquesused for diagnosis, the reported prevalence of Mulleriananomalies has ranged from 0.16% to 10% [1]. It is 2-3%in fertile women, 3% in infertile women, 5-10% inwomen with recurrent miscarriages and more than 25%in women with late miscarriages and preterm deliveries[2]. Uterine septum is the most common type of Muller-ian canal defect, with an incidence of 34.9% [3]. Thiscondition is the result of partial or incomplete failure ofthe resorption of the uterovaginal septum after fusion ofthe paramesonephric ducts other they are generally asso-ciated with impaired reproductive performance such asrecurrent pregnancy loss and preterm births [4, 5]. Preva-lence of septa in women with recurrent spontaneous preg-nancy loss ranges from 26% to 94% [1]. Hysteroscopicmetroplasty seems to be the most effective approach forpatients who have obstetric problems in the history [6, 7].
Materials and Methods
This was a retrospective study comprising 30 women whocame to us with a desire to conceive, and who were diagnosedwith different degrees of septate uterus at the Department ofObstetrics and Gynecology of Ege University Education andResearch Hospital during 2003-2008. The mean age was 34years (range was 23-45 years). In all cases the procedure wasperformed by resectoscope and monopolar energy modality.Surgical sections were applied under general anesthesia in thefirst part of the cycle. the cervix was dilated to 10 mm by Hegarbougies and a rigid hysteroscope was introduced, mounted witha 26F gauge resectoscope (Storz, Tuttlingen, Germany). The
uterine cavity was distended with a non-conductive, hyposmo-lar solution of mannitol 0.54%. Total septal resection was com-pleted with the first application. No medication was used pre-operatively. No patient required treatment after surgery.
Results
We achieved sufficient results at the first hysteroscopyin all patients. All of uterine septa were totally resectedwithout complications such as fluid overload syndromeand uterine perforation. The mean period of follow-upwas 12 + 36 months after metroplasty.
Patients had a total of 74 pregnancies before metroplasty.Of these, ten (14%) were carried to term, six (8%) endedin preterm delivery, and 58 (78%) ended in spontaneousabortion. At least one year of follow-up after hysteroscopicmetroplasty occurred with a total of 20 spontaneous preg-nancies. Prognosis of pregnancy improved dramaticallyfollowing the procedure. Of these, 11 (55%) were carriedto term, two (10%) ended in preterm delivery, and seven(35%) ended in spontaneous abortion (Table 1).
Discussion
There is no study that compares outcomes of treatedand nontreated patients in the literature reporting hystero-scopic metroplasty. It may be because performing hys-teroscopic metroplasty for uterine septum is a safe and
Summary
Purpose of Investigation: To evaluate reproductive outcome after hysteroscopic metroplasty. Methods: We analyzed the reproduc-tive outcome of 30 patients with different degrees of septate uterus undergoing hysteroscopic metroplasty. In all cases the procedurewas performed by resectoscope. Results: The patients had a total 74 pregnancies before metroplasty. Of these, ten (14%) were carriedto term, six (8%) ended in preterm delivery, and 58 (78%) ended in spontaneous abortion. At least one year following hysteroscopicmetroplasty a total of 20 pregnancies occurred. Of these, 11 (55%) were carried to term, two (10%) ended in preterm delivery, seven(35%) ended in spontaneous abortion. Conclusion: Correction of uterine septum significantly improves the prognosis of the preg-nancies in patients with a history of severe obstetric problems. These results are similar to the results reported in the literature. Ourdata analysis suggests that hysteroscopic metroplasty for uterine septum improves pregnancy outcome of patients who come to uswith a desire to conceive.
Key words: Septate uterus; Hysteroscopy; Metroplasty.
Table 1. — Reproductive outcome before and after theprocedure in the study groups.
Before metroplasty After metroplasty
Pregnancies 74 20Abortion 58 (78%) 7 (35%)Preterm deliveries 6 (8%) 2(10%)Term deliveries 10 (14%) 11 (55%)

F. Sendag, T. Mermer, S. Yucebilgın, K. Oztekin, O. Bilgin 288
effective procedure for achieving a normal uterine cavity[7-15]. Any complications that occurred in our study groupresemble those reported by other authors [10, 11, 16].
Uterine septa have generally been associated with poorobstetric outcomes. Reasons for complications may bereduced vascularization or altered relationships betweenthe myometrial and endometrial vessels for first trimesterabortion and decreased volume of the uterine cavity forsecond trimester abortion [17]. In many wade case series,the rate of spontaneous abortion and preterm deliveryranged from 86.3-91% and 6-9.4% in these woman,respectively [5, 6, 16]. Improvement of obstetrical prog-nosis after this prosedure has been shown by numerousstudies [3, 5-7, 14-16, 18-20].
Also important for visualization is a thin endometriallining, which may be achieved either by performing theprocedure in the early follicular phase or by followingpharmacologic suppression of the endometrial lining.Options include GnRH agonists or gonadal steroids suchas danazol, oral progestins, or continuous combinationoral contraceptives [21]. GnRH agonists are more expen-sive and may make the procedure more difficult by reduc-ing uterine size [22].
In our study, we did not perform insertion of anintrauterine device with the aim of reducing the forma-tion of adhesions after metroplasty. However, somepatients received estrogen therapy. The benefit of thisapplication is controversial at present [6, 16, 23-25].Moreover, intrauterine adhesions after hysteroscopicmetroplasty are a rare finding and usually filmy [4].
Most authors have suggested a postprocedural evalua-tion of the endometrial cavity for possible septal rem-nants [3]. A fundal notch smaller than 1 cm does notseem to reduce the reproductive performance [26]. Hys-terosalpingogram, ultrasound or second-look hys-teroscopy can be used for this purpose [10]. If ultrasoundcan be applied, it is better to perform it in the secretoryphase of the cycle after surgery [21].
The rate of conception in infertile women is muchlower, and does not seem to be influenced by metroplasty[10]. Its performance may also be required in infertilepatients and in women desiring pregnancy to minimizethe risk of future gestational failure [21].
Conclusion
The correction of uterine septum significantly improvesthe prognosis of pregnancies in patients with a history ofsevere obstetrical problems (Table 2). Recently, this pro-cedure has also been shown to be minimally invasive andhave a short hospitalization time [6, 8]. These results aresimilar to the results reported in the literature [3, 5-7, 14-16, 18-20]. Our data analyses suggest that hysteroscopicmetroplasty for uterine septum improves pregnancyoutcome of patients who wish to conceive in the future.
References[1] Troiano R.N., McCarthy S.M.: “Mullerian duct anomalies:
imaging and clinical issues”. Radiology, 2004, 233, 19.[2] Acien P.: “Incidence of Mullerian defects in fertile and infertile
women”. Hum. Reprod., 1997, 12, 1372.[3] Grimbizis G.F., Camus M.: “Clinical implications of uterine mal-
formations and hysteroscopic treatment results”. Hum. Reprod.Update, 2001, 7, 161.
[4] Homer H.A., Li T., Cooke I.D.: “The septate uterus: a review ofmanagement and reproductive outcome”. Fertil. Steril., 2000, 73, 1.
[5] March C.M., Israel R.: “Hysteroscopic management of recurrentabortion caused by septate uterus”. Am. J. Obstet. Gynecol., 1987,156, 834.
[6] Daly D.C., Maier D., Soto-Albors C.: “Hysteroscopic metroplasty:six years experience”. Obstet. Gynecol., 1989, 73, 201.
[7] Fedele L., Bianchi S.: “Hysteroscopic metroplasty for septateuterus”. Obstet. Gynecol. Clin. North Am., 1995, 22, 473.
[8] Chervenak F.A., Neuwirth R.S.: “Hysteroscopic resection of theuterine septum”. Am. J. Obstet. Gynecol., 1981, 141, 351.
[9] Candiani G.B., Vercellini P., Fedele L., Garsia S., Brioschi D.,Villa L.: “Argon laser versus microscissors for hysteroscopic inci-sion of uterine septa”. Am. J. Obstet. Gynecol., 1991, 164, 87.
[10] Fedele L., Arcaini L., Parazzini F.: “Reproductive prognosis afterhysteroscopic metroplasty in 102 women: life table analysis”.Fertil. Steril., 1993, 59, 768.
[11] Guarino S., Incandela S., Maneschi W., Vegna G., D’Anna M.R.,Leone S., Maneschi F.: “Hysteroscopic treatment of uterineseptum”. Acta Eur. Fertil., 1989, 20, 321.
[12] Israel R., March C.M.: “Hysteroscopic incision of the septateuterus”. Am. J. Obstet. Gynecol., 1984, 149, 66.
[13] Jacobsen L., De Cherney A.: “Results of conventional and hystero-scopic surgery”. Hum. Reprod., 1997, 12, 1376.
[14] Saygili E., Yildiz S.: “Reproductive outcome of septate uterus afterhysteroscopic metroplasty”. Arch. Gynecol. Obstet., 2003, 268, 289.
[15] Porcu G., Cravello L.: “Hysteroscopic metroplasty for septateuterus and repetitive abortions: reproductive outcome”. Eur. J.Obstet. Gynecol. Reprod. Biol., 1999, 88, 81.
[16] Valle R.E., Sciarra J.J.: “Hysteroscopic treatment of the septateuterus”. Am. J. Obstet. Gynecol., 1986, 67, 253.
[17] Candiani G.B., Fedele L., Zamberletti D., De Virgillis D., CarinelliS.: “Endometrial patterns in malformed uteri”. Acta Eur. Fertil.,1983, 14, 311.
[18] Perino A., Mencaglia L., Hamou J., Cittadini E.: “Hysteroscopyfor metroplasty of uterine septa: report of 24 cases”. Fertil. Steril.,1987, 48, 321.
[19] Pabuccu R., Atay V., Orhon E., Urman B., Ergun A.: “Hystero-scopic treatment of intrauterine adhesions is safe and effective inthe restoration of normal menstruation and fertility”. Fertil. Steril.,1997, 68, 1141.
[20] Cararach M., Penella J., Ubeda A., Labastida R.: “Hysteroscopicincision of the septate uterus: scissors versus resectoscope”. Hum.Reprod., 1994, 9, 87.
[21] Fedele L., Bianchi S., Frontino G.: “Septums and synechiae:approaches to surgical correction”. Clin. Obstet. Gynecol., 2006,49, 767.
[22] Fedele L., Bianchi S., Gruft L., Bigatti G., Busacca M.: “Danazolversus a gonadotropin-releasing hormone agonist as preoperativepreparation for hysteroscopic metroplasty”. Fertil. Steril., 1996,65, 186.
Table 2. — Reproductive outcomes before and aftermetroplasty in the selected study groups.
Cararach Daly Valle Perino Pabuccu Fedele Israel Grimbiziset al. [20] et al. [6] et al. [16] et al. [18] et al. [19] et al. [7] and March et al. [3]
(n: 62) (n: 55) (n: 115) (n: 27) (n: 49) (n: 71) (n: 57) (n: 57)
Miscarriages 160 130 258 24 96 > 139 212 69(91%) (87%) (86%) (89%) (89%) (88%) (90.1%)
Preterm 11 13 28 3 11 NR 21 2deliveries (6%) (9%) (9%) (11%) (10%) (9%) (2.6%)Term 5 7 13 0 1 NR 7 5deliveries (3%) (5%) (4%) (1%) (3%) (6.6%)Miscarriages 12 15 12 1 2 10 8 11
(29%) (20%) (12%) (7%) (4.5%) (16%) (14%) (25.6%)Preterm 0 5 7 0 2 10 4 2deliveries (7%) (7%) (4.5%) (16%) (7%) (4.6%)Term 29 55 84 14 40 45 44 30deliveries (71%) (73%) (81%) (93%) (91%) (69%) (79%) (69.8%)A
fter
met
ropl
asty
Bef
ore
met
ropl
asty

Reproductive outcomes after hysteroscopic metroplasty for uterine septum 289
[23] Fayez J.A.: “Comparison between abdominal and hysteroscopicmetroplasty”. Obstet. Gynecol., 1986, 68, 399.
[24] DeCherney A.H., Russell J.B., Graebe R.A., Polan M.L.: “Resec-toscopic management of mullerian fusion defects”. Fertil. Steril.,1986, 45, 726.
[25] Dabirashrafi H., Mohammad K., Moghadami-Tabrizi N., Zandine-jad K., Moghadami-Tabrizi M.: “Is estrogen necessary after hys-teroscopic incision of the uterine septum?”. J. Am. Assoc. Gynecol.Laparosc., 1996, 3, 623.
[26] Querleu D., Leroy Brasme I., Parmentier D.: “Ultrasound guidedtranscervical metroplasty”. Fertil. Steril., 1990, 54, 995.
Address reprint requests to:F. SENDAG, M.D.Ege University School of MedicineDepartment of Obstetrics and GynecologyBornova, Izmir, 35100 (Turkey)e-mail: [email protected]

[789/27]
290
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication August 13, 2009
Fertility sparing in young women with ovarian tumors
F. Ghaemmaghami1, M. Karimi Zarchi2, A. Naseri1, A.S. Mousavi1, M. Modarres Gilani1, F. Ramezanzadeh3, E. Rezaiof3
1Department of Gynecology Oncology, Vali-e-Asr Hospital, Tehran University of Medical Sciences, Tehran2Gynecologic Oncology Fellowship, Shahid Sadoughi University of Medical Science, Yazd
3Vali-e-Asr Reproductive Health Research Center, Tehran University of Medical Sciences, Tehran (Iran)
[1036/29]
Introduction
Although ovarian malignancy is predominantly adisease of aging, there is an increasing number ofwomen that survive these malignancies before or duringreproductive years. Eighty-nine percent of ovariantumors occur after the age of 40 and the rest occurbefore this age [1].
The standard treatment for borderline and malignantovarian tumors is cytoreductive surgery such as hys-terectomy, oophorectomy, partial omentectomy and sur-gical staging. Surgical staging reveals the need for adju-vant chemotherapy to detect extension of the disease.Cytoreductive surgery causes infertility and, due to this,conservative surgery has been introduced [2, 3].
Conservative surgery consists of unilateral salpingo-oophorectomy, omentectomy, surgical staging, anddebulking of metastases in germ cell tumors [4].
The 5-year survival of patients with Stage IA, grade 1,epithelial ovarian tumor who were treated conserva-tively is 90% [5, 6]. Germ cell tumors represent most(80%) of the pre-adolescent malignant ovarian neo-plasms.The mean age at diagnosis is 16 to 20 years andthe tumors may occasionally be diagnosed during preg-nancy or puerpurium [7-10]. Sex cord-stromal tumors(SCSTs) are characterized by 85-100% long-term sur-vival rates for Stage IA tumors, and they have a propen-sity for late recurrences [11]. Sertoli-Leydig cell tumorsaccount for less than 0.5% of all ovarian tumors, and75% of these neoplasms are diagnosed in womenyounger than 40 years of age [11].
In Ayhan et al.’s study, it was noted that diagnosis ofovarian tumors in the premenopausal period has increasedby improvement of diagnostic methods and regular gyne-cologic examination. Ovarian tumors that have beendiagnosed in the premenopausal period are mostly intheir early stage and lower grade and can be treated by aconservative surgery [4].
Although a variety of studies have tried to documentthe impact of conservative treatment aimed at preservingovarian function and reproductive ability, little informa-tion is available regarding survivors [5, 12, 13].
Many studies have shown that conservative surgery inpatients with germ cell ovarian tumors is successful inoutcome and preservation of fertility [8-10].
In a series of borderline tumors (82 patients) with con-servative management, fertility and survival have beenacceptable after a 25-year follow-up [14].
In another study on 17 patients with Stage II and IIIborderline ovarian tumors, eight spontaneous pregnanciesoccurred. After conservative surgery, studies show theeffect of conservation surgery on patients with anadvanced stage of borderline ovarian tumors [15].
Another study on borderline ovarian tumors shows thatthere is no significant difference regarding the survival ofpatients who are treated by conservative surgery orradical surgery, although there are more recurrences inpatients with conservative surgery. They were treated bysecond-look surgery and there was no death reported tohave occurred in these groups [16].
Recently, conservative surgery has been conducted onpatients with epithelial ovarian tumors in early stage evenwith adjuvant chemotherapy in Stage IC and grade 3 [17].In addition, in another study on ten patients with high-
Summary
Background: Surveys have shown that fertility sparing in patients with ovarian tumors has proven to be effective. Thus thisapproach in ovarian tumor cases has been carried out. The purpose of this study was to evaluate the clinical outcome and pregnan-cies in women who suffered from ovarian tumor and underwent conservative treatment. Materials and Methods: All cases whoreceived conservative treatment and those who had recurrence of the disease during the follow-up period were evaluated at Vali-AsrHospital from 2000-2004. Results: 60 of 410 patients with ovarian tumor (age range: 13-34) were treated conservatively. Threepatients (5%) were infertile. Histology of tumors showed: 26 (43.3%) germ cell tumors, 15 (25%) borderline tumors, ten (16.7%)epithelial tumors and nine (15%) sex cord tumors. The cases were followed for 12-48 months. Seven term pregnancies occurred insix patients. Three in the borderline group, two in the germ cell group, one in the epithelial group and one in the sex-cord group.Nine recurrences were reported among our cases. Two of the patients (serous carcinoma and immature teratoma, both Stage IIIc)died during follow-up due to refusal to undergo radical surgery. Conclusion: Fertility preserving surgery in young women withepithelial ovarian tumors, borderline and sex-cord tumors Stage I, grade 1 and 2 is recommended.
Key words: Ovarian tumors; Young women; Desire of fertility; Fertility sparing; Epithelial ovarian tumor; Germ cell tumor; Border-line ovarian tumor.

Fertility sparing in young women with ovarian tumors 291
stage and high-grade epithelial ovarian tumors, thismodality for treatment has been performed [18].
The aim of the present study was to evaluate theoutcome of patients who were treated conservatively forStage I epithelial ovarian tumors, any stage borderlinetumors, malignant ovarian germ cell tumors (MOGTs),and Stage I sex cord stromal tumors (SCSTs).
Materials and Methods
This was a retrospective study performed on patients withovarian tumors who had been referred to the Gynecology-Oncology Department of Vali-Asr Hospital, Tehran, Iran in2000-2004.
Among 410 patients with ovarian tumors who had beenreferred or were treated by different treatment modalities, 60who had conservative ovarian surgery were evaluated for preg-nancy and recurrence of the disease within 12 to 48 months offollow-up.
The selection criteria were diagnosis of Stage I epithelialovarian tumors, any stage borderline ovarian tumors MOGCTs,Stage I SCSTs, primary conservative surgical treatment, and ageunder 40. One patient with a Stage IIIC epithelial ovarian tumorhad refused to undergo a radical surgery in another hospital andwas referred to our center with recurrence after five months.
Gynecologic pathologists of Vali-Asr Department of Pathol-ogy performed histology. Histopathology was classified accord-ing to the WHO criteria. Tumors were staged according to theInternational Federation of Gynecology and Obstetrics (FIGO)classification system. All the patients underwent surgery as theprimary treatment. Conservative surgery comprised tumor exci-sion with preservation of the uninvolved ovarian tissue or uni-lateral salpingo-oophorectomy (USO). In all cases, surgicalstaging was performed with peritoneal washing, omentectomy,multiple peritoneal biopsies, retroperitoneal sampling, lym-phadenectomy, and debulking of metastasis implants forMOGCTs tumors.
No chemotherapy was given to the patients with Stage IA (G1)epithelial ovarian cancer, with borderline ovarian tumors unlessinvasive implants were present, with pure dysgerminoma StageIA, with immature teratoma Stage IA grade 1, or with Stage IAsex cord stromal tumors. Only the patients with Stage I Sertoli-Leydig cell tumors that were poorly differentiated or containedheterologous elements were treated with chemotherapy.
The patients with stage > IA epithelial ovarian tumorsreceived cisplatin in combination with cyclophosphamide orpaclitaxel. Those with MOGCTs and Stage IA and grade 2, 3were treated with BEP regimen (cisplatin, etoposide,bleomycin). This regimen was also administered to the patientswith stage > IA SCSTs. The number of cycles depended on sur-gical staging, the patient’s tolerance to chemotherapy and theobjective response of any measurable disease. The different reg-imens were usually administered for four to six courses. Afterthe primary surgery of chemotherapy in the case of adjuvanttreatment, the patients were evaluated at regular intervals ofthree months in the first year and every six months thereafter.Follow-up examinations consisted of physical and gynecologi-cal examination, imaging of the abdomen and pelvis, and meas-urement of tumor markers.
Clinical data collected were age at diagnosis, desire of preg-nancy, date of primary surgery, histology results, stage, grade,adjuvant treatment, second-look procedure, menstrual history,pregnancies and deliveries after treatment, diagnosis of relapse,and tumor status. Information was obtained from medical
records and from a questionnaire mailed to all patients whowere at least 13 years old at the time of the diagnosis. Theproject was approved by our Institutional Review Board, and acover letter included the elements of informed consent, such asprovision for confidentiality.
Results
Among 60 patients in this study, ten patients (16.6%)presented epithelial tumors (9 Stage I and 1 Stage IIICwho refused radical surgery), 15 (25%) borderlineovarian tumors (14 Stage I, 1 Stage III with no invasiveimplants), 26 (43.3%) MOGCTs tumors (13 Stage IA, 1Stage IB, 1 Stage IC, 1 Stage IIA, 3 Stage IIIA and 6IIIC), seven unknown stage endodermal sinus tumors(EST), and nine (15%) SCSTs (7 Stage IA, 2 Stage IC).(Table 1). The youngest patient was 13 and the oldest was34 years old (mean age 23.2 years). The range of follow-up was 12 to 48 months.
Seven patients with epithelial ovarian tumors (7/10)undergoing conservative surgery received adjuvantchemotherapy (more than Stage IA or more than grade1). Five received taxol + carboplatine (TC) and the othertwo received cyclophosphamide + cisplatinum (CP)courses. One of them had a successful pregnancy with ahealthy child (she had a history of infertility).
Two cases had recurrence. One was in Stage IC andhad recurrence after ten months. The recurrence wastreated by omentectomy, appendectomy, and six coursesof TC. She is in remission for the time being. The otherpatient was in Stage IIIC and had recurrence after fivemonths. She was treated by a radical surgery (TAH +BSO + omentectomy) and six courses of TC, but sheexpired due to progression of the disease.
Eleven (11/15) ovarian borderline tumor patientsdesired pregnancy (including 2 cases with a history ofinfertility). The age range of these patients was 16 to 35.
Histologically, ten cases had serous and five cases hadmucinous types. Primarily performed surgeries were 14unilateral salpingo-oophorectomy and one cystectomy +cesarean section. Surgical staging was performed in ten
Table 1. — Characteristics of patients with ovarian tumorsundergoing conservative surgery.
Histological type EOC BOT MOGCT SCSTNo. of patients 10 (16%) 15 (25%) 26 (43.3%) 9 (15%)
Stage I Stage IA (7) Stage IA (7) Stage IA (13) Stage IA (7)Stage IC (2) Stage IB (2) Stage IB (1) Stage IC (2)
Stage IC (1)
Stage > I Stage IIIC Stage IIIA (1) Stage IIA (1)UK (5) Stage IIIA (3)
Stage IIIC (6)UK (EST)
Adjuvant 5/10 13/26 2/9chemotherapy
Pregnancy 1 31 term 2 12 preterm
Recurrence 2 3 2 2DOD = 1 Stage IIIC DOD = 1 Stage IIIC
EOC: epithelial ovarian cancer; BOT: borderline ovarian tumor; MOGCT: malignantovarian germ cell tumors; SCST: sex cord-stromal tumors; DOD: died of disease.

F. Ghaemmaghami, M. Karimi Zarchi, A. Naseri, A.S. Mousavi, M. Modarres Gilani, F. Ramezanzadeh, E. Rezaiof 292
patients and the other patients without surgical stagingwere in Stage I formally at the suggestion of surgeons.Three of these cases had successful pregnancies (1 term+ 2 preterm but all of them were healthy). Three caseshad recurrence, one after five months and the other twoafter seven months from the primary treatment. All are inremission for the time being.
Eight (8/26) germ cell tumor patients desired preg-nancy (age range; 13-33 years). Thirteen patients haddysgerminoma, four immature teratoma, four embryonaltumors, three mixed germ cell tumors, and two had yolksac tumors. Primarily performed surgeries included 24unilateral salpingo-oophorectomies and one bilateralsalpingo-oophorectomy with preservation of the uterus
Table 2. — Comparison of current series and other studies.
Field Authors Year Patient number Histologic type Mean age Follow-up Recurrence Preg.
Non-epithelial Koji Kanazawa 1981-96 31 Dys (7) 18.6 – – 8 (6)cell tumors et al. 2000 [8] Yolk sac (10)
Immature (7)Chorio (1)Mixed (6)
EI-Lamie 1994-99 16 Dys (6) 20.5 (13-40) 30.5 mo. 1 immature Tratoma 3et al. (2000) [9] Immature (6) (Stage IIIC)
Endodermal (4)Zanagnolo 20 yrs 36 Dys (12) 20.5 (13-22yr40) 129 mo. – 11 (9)et al. (2004) [10] Immature (6)
Yolk sac (4)Endodermal (6)Mixed (8)
Current series 2000-2004 26 Dys (13) 20.3 (13-33) 30 mo. 1 dysgerminoma 2 (1)(2005) (5 yrs) Immature (4) (Stage IIA)
Embryomal (4)Mixed (2)Yolk sac (1) 22 Granulosa 1Granulosa (8) (2 Stage IA)Androblastoma (I)
Borderline tumors Gotlieb 25 yrs 39 Serous (22) muc (17) – 69 mo. – 22 (15)et al. (1998) [14]Camatte 10 yrs 17 – – 50 mo. – 8 (7)et al. (2002) [15]Donnez 1989-2001 16 – – – – 12 (7)et al. (2003) [16]Current series 2000-2004 15 Serous (8) muc (7) 24 yr (16-35) 30 mo. Ser (Stage IB) 3(2005) (5 yrs) Ser (IIC)
Muc (Stage IIIA)
Epithelial ovarian Zanetta 10 yrs 99 – – 30 mo. – 25 (17)tumors et al. (1996) [17]
Raspagliesi 1980-94 10 22.7 yrs Ser (5) 70 mo. – 3et al. (1997) [18] MUC (4)
Undiff (1)Morice 1982-99 25 24 yrs Ser (16) 42 mo. 7 4et al. (2001) [19] MUC (19)
Muc (21)Ser (3)
Morice 1987-2004 34 27 yrs (14-36) Endometrial (5) 60 mo. 10 10 (9)et al. (2005) [20] Small cell (2)
Mixed (3)Current series 2000-2004 10 26.2 yrs (19-32) Ser (5) 30 mo. 2 serous Stage IC, 1(2005) (5 yrs) Muc (4) Stage IIIC
Brenner (1)Zanetta 10 yrs 99 – – 30 mo. – 25 (17)et al. (1996) [17]Raspagliesi 1980-94 10 22.7 yrs Ser (5) 70 mo. – 3et al. (1997) [18] MUC (4)
Undiff (1)Morice 1982-99 25 24 yrs Ser (16) 42 mo. 7 4et al. (2001) [19] MUC (19)
1987-2004 34 27 yrs (14-36) Muc (21)Morice Ser (3) 60 mo. 10 10 (9)et al. (2005) [20] Endometrial (5)
Small cell (2)Mixed (3)
Current series 2000-2004 10 26.2 yrs (19-32) Ser (5) 30 mo. 2 serous Stage IC, 1(2005) (5 yrs) Muc (4) Stage IIIC
Brenner (1)Dys: dysgerminoma; Muc: mucinous; Chorio: choriocarcinoma; Ser: serous.

Fertility sparing in young women with ovarian tumors 293
and one case of cystectomy + cesarean section (in yolksac tumor patients). Surgical staging was performed in 25(25/26) cases.
Thirteen cases who had dysgerminoma or immatureteratoma with stage > IA, grade 3 and EST treated byBEP (bleomycin, etoposide, and cisplatinum). Two preg-nancies had occurred in a patient. One patient 14 yearsold, had immature teratoma and died in Stage IIIC afterthree courses of BEP and one course of VAC (vincristine,actinomycine, cyclophosphamide) without any responseto the treatment ten months after diagnosis.
Four (4/9) sex cord tumor patients desired pregnancy.Eight (8/9) patients had granulosa cell tumors and theother one androblastoma.
Primarily performed surgeries in these groups includedone salpingo-oophorectomy+cesarean section and eightunilateral salpingo-oophorectomies. Surgical staging wasperformed in all the cases. Seven were in Stage IA andtwo in Stage IC. Two cases with Stage IC were treated byBEP chemotherapy, but they had recurrences. The firstrecurrence occurred after 24 months and was treated bydebulking surgery followed by four BEP courses. Thesecond one occurred after five months and was treated byTC chemotherapy. Both of these patients are in remissionfor the time being.
In summary, conservative surgery and fertility out-comes were evaluated in 60 patients less than 40 years ofage, considering the fact that there were only 26 patients(26/60) who desired pregnancy and there was a history ofinfertility in three patients. Seven pregnancies occurred(in 6 patients) during the follow-up period. Two pregnan-cies were preterm in patients with borderline ovariantumors but all of them were healthy. Nine patients hadrecurrence and seven are in remission after the secondarytreatment.
Discussion
This study may emphasize the point that conservativesurgery can be performed on premenopausal patientswith a selective histological type of ovarian tumors, whodesire to preserve fertility, even in a higher stage or grade.However, in epithelial ovarian tumors, it can be done justin early stages (up to Stage IC).
Thus the type of surgery should be decided dependingmainly on age of the patient and her desire for fertilitypreservation. Surgical staging should be performed in allcases to evaluate the extent of the disease, to determineprognosis, and to guide postoperative management. Uni-lateral salpingo-oophorectomy with preservation of thecontralateral ovary and the uterus is now considered anappropriate surgical treatment for patients with Stage IA,grade 1 epithelial ovarian cancer, any stage borderlineovarian tumors with no invasive implants, SCSTs andMOGCTs, and even an advanced germ cell disease, par-ticularly if the contralateral ovary is normal. Removal ofthe preserved ovary should be considered after comple-tion of pregnancy (ies) in order to reduce the risk ofovarian tumor recurrence [1].
In a current study on 26 patients with a germ cellovarian tumor, two pregnancies occurred in eight patientswho desired pregnancy during the follow-up. One ofthese cases had recurrence which is comparable to otherstudies (Table 2).
In Kanazawa et al.’s study on 31 germ cell tumors(during 15 years), eight pregnancies occurred in sixpatients [8]. In El-Lamie et al.’s study on 16 patients(over 5 years, with a 30.5 month follow-up), two patientshad three pregnancies and there was one case of recur-rence [9].
In the study by Zanagnolo et al. on 36 germ cell tumors(with a 10-year follow-up), nine patients had 11 pregnan-cies with no report of recurrence [10]. In sex cord tumorpatients, four desired pregnancy and one pregnancyoccurred. These data could show the possibility of con-servative surgery on the patients as well.
In 15 patients with borderline tumors in our study, threepregnancies occurred (only 11 were desired pregnanciesand there was a history of infertility in 2 of them).
Table 3 shows different studies in which borderlinetumors were treated by conservative surgery. In Gotlieb etal.’s study on 39 patients (with 69 months of follow-up),there were 22 pregnancies in 15 patients (there were 3abortions, 1 early pregnancy, and 1 twin pregnancy) [14].
In Camatte’s study on 17 patients (with 50 months offollow-up), eight pregnancies occurred in seven patients[15]. In Donnez et al.’s study on 16 patients (during 12years), 12 pregnancies occurred in seven patients [16].
Conservative surgery can be performed on patientswith early-stage epithelial tumors, but it is necessary tohave adjuvant chemotherapy in high-grade cases. Table 4compares different studies on epithelial ovarian tumors.
Zanetta et al.’s study (with 30 months of follow-up) on99 Stage IA epithelial ovarian tumor patients showed 25pregnancies in 17 patients [17]. Thus conservative therapycan be performed on Stage IA epithelial tumor patients.
In another study by Raspagliesi et al. on ten epithelialtumor patients with a higher grade or stage undergoingconservative surgery (with 70 months of follow-up), threepregnancies occurred and there was no recurrence [18].
In two other studies, one in 2001 and another of multi-central type in 2005, Morice et al showed that conserva-tive surgery should be performed on patients with StageIA, grade 1 and it can also be considered for grade 2 [19,20] (Table 4).
The results from our study confirm that management ofStage I (grade 1, grade 2) epithelial ovarian cancer, anystage borderline ovarian tumors with no invasive implants,MOGCTs and SCSTs with fertility-sparing surgery is asafe, practicable treatment option. Of course, furtherstudies are recommended to evaluate this important issue.
References[1] Zanagnolo V., Sartori E., Trussardi E., Pasinetti B., Maggino T.:
“Preservation of ovarian function, reproductive ability and emo-tional attitudes in patients with malignant ovarian tumors”. Eur. J.Obstet. Gynecol. Reprod. Biol., 2005, 123, 235.

F. Ghaemmaghami, M. Karimi Zarchi, A. Naseri, A.S. Mousavi, M. Modarres Gilani, F. Ramezanzadeh, E. Rezaiof 294
[2] Amos C.I., Struewing J.P., Berchuck A.: “Epithelial ovariancancer”. In: P.J. Disaia, W.T. Creasman (eds.). Clinical Gynecol-ogy Oncology, 6th edition, St. Louis, Mosby, 2002, 289.
[3] Berek J.S., Greenlee R.T., Scully R.E.: “Epithelial ovariancancer”. In: J. Berek, N.F. Hacker (eds.). Practical GynecologyOncology, 4th edition, Philadelphia, Williams & Wilkins, 2005,443.
[4] Ayhan A., Celik H., Taskiran C., Bozdag G., Aksu T.: “Oncologicand reproductive outcome after fertility-saving surgery in ovariancancer”. Eur. J. Gynaecol. Oncol., 2003, 24, 223.
[5] Morice P., Wicart-Poque F., Rey A., El-Hassan J., Pautier P.,Lhommé C. et al.: “Results of conservative treatment on epithe-lial ovarian carcinoma”. Cancer, 2001, 92, 2412.
[6] Seracchioli R., Venturoli S., Colombo F.M., Govoni F., MissiroliS., Bagnoli A.: “Fertility and tumor recurrence rate after conser-vative laparoscopic management of young women with early-stageLMP ovarian tumors”. Fertil. Steril., 2001, 76, 999.
[7] Talerman A.: “Blaunstein’s pathology of the female genital tract.Germ cell tumors of the ovary”. In: Kurman J.K. (ed.). Blaun-stein’s Pathology of the Female Genital Tract. New York, Springer,2002, 967.
[8] Kanazawa K., Suzuki T., Sakumoto K.: “Treatment of malignantovarian germ cell tumors with preservation of fertility: reproduc-tive performance after persistent remission”. Am. J. Clin. Oncol.,2000, 23, 244.
[9] E1-Lamie I.K., Shehata N.A., Abou-Loz S.K., El-Lamie K.I.:“Conservative surgical management of malignant ovarian germcell tumors: the experience of the Gynecologic Oncology Unit atAin Shams University”. Eur. J. Gynaecol. Oncol., 2000, 21, 605.
[10] Zanagnolo V., Sartori E., Galleri G., Pasinetti B., Bianchi U.:“Clinical review of 55 cases of malignant ovarian germ celltumors”. Eur. J. Gynaecol. Oncol., 2004, 25, 315.
[11] Young R.H., Scully R.E.: “Ovarian sex cord stromal tumors:recent advances and current status”. Clin. Obstet. Gynaecol.,1984, 11, 93.
[12] Tangir J., Shwartz P.E.: “Fertility preservation in the managementof germ cell ovarian cancer”. CME J. Gynecol. Oncol., 2003, 8,117.
[13] Duska L.R., Chang Y.C., Flynn C.E., Chen A.H., Goodman A.,Fuller A.P., Nikrui N.: “Epithelial ovarian carcinoma in the repro-ductive age group”. Cancer, 1999, 85, 2623.
[14] Gotlieb W.H., Flikker S., Davidson B., Korach Y., Kopolovic J.,Ben-baruch G.: “Borderline tumors of the ovary: fertility treat-ment, conservative management, and pregnancy outcome”.Cancer, 1998, 82, 141.
[15] Camatte S., Morice P., Pautier P., Atallah D., Duvillard P., Cas-taigne D.: “Fertility results after conservative treatment ofadvanced stage serous borderline tumour of the ovary”. BJOG,2002, 109, 376.
[16] Donnez J., Munschke A., Berliere M., Pirard C., Jadoul P., SmetsM., Squifflet J.: “Safety of conservative management and fertilityoutcome in women with borderline tumors of the ovary”. Fertil.Steril., 2003, 79, 1216.
[17] Zanetta G., Chiari S., Rota S., Bratina G., Maneo A., Torri V.,Mangioni C.: “Conservative surgery for stage I ovarian carcinomain women of childbearing age”. Br. J. Obstet. Gynaecol., 1997,104, 1030.
[18] Raspagliesi F., Fontanelli R., Paladini D., di Re E.M.: “Conserva-tive surgery in high-risk epithelial ovarian carcinoma”. J. Am.Coll. Surg., 1997, 185, 457.
[19] Morice P., Wicart-Poque F, Rey A., Camatte S., Rouzier R.,Pautier P. et al.: “Results of conservative treatment in epithelialovarian carcinoma”. Cancer, 2001, 92, 2412.
[20] Morice P., Leblanc E., Rey A., Baron M., Querleu D., Blanchot J.et al.: “Conservative treatment in epithelial ovarian cancer: resultsof a multicentre study of the GCCLCC (Groupe des Chirurgiensde Centre de Lutte Contre le Cancer) and SFOG (SociétéFrançaise d’Oncologie Gynécologique)”. Hum. Reprod., 2005, 20,1379.
Address reprint requests to:F. GHAEMMAGHAMI, M.D.Department Gynecology OncologyVali-e-Asr HospitalImam Khomeini Hospital ComplexKeshavarz Blvd.Tehran (Iran)e-mail: [email protected]

295
Revised manuscript accepted for publication July 27, 2010
Laparoscopic sacral colpopexy for uterine prolapse with prolene mesh
L. Hong, X. Xu, L. Chen, Q. FuDepartment of Gynaecology and Obstetrics, Renmin Hospital of Wuhan University, Hubei, Wuhan (China)
[1145/30]
Introduction
Pelvic organ prolapse (POP) is a common clinical con-dition that affects the social, occupational, domestic, psy-chological and sexual lives of women with an estimatedprevalence of up to 50% of parous women. Uterine pro-lapse and vaginal wall bulge are common types of POP.Uterine prolapse occurs when the pelvic floor musclesand ligaments stretch and weaken, providing inadequatesupport for the uterus [1]. The disorder is among the mostdemanding and technically challenging problems offemale reconstructive surgery. Several surgical optionsare available to women with the afflicton and the resultsvary widely. Although traditional surgical methods likevaginal hysterectomy and anterior/posterior colpor-rhaphia have short-term recovery rates, the rate of pro-lapse recurrence is rising year by year. The levator plica-tion procedure is still an effective procedure, but,postoperatively, 27-50% of women report pain duringintercourse [2].
Sacral colpopexy placing synthetic mesh throughlaparoscopic techniques in the rectovaginal septum andveslcovaginal septum seems to be the more reliable pro-cedure for the the cure of uterine prolapse. In this paper,we describe this novel approach to the surgical manage-ment of uterine prolapse. The surgery involved a laparo-scopic approach to sacral colpopexy and anterior/poste-rior colporrhaphia with prolene mesh, which producesexcellent results with very few complications. To ourknowledge a similar study has not previously beenreported in the literature.
Patients and Methods
From October 2006 to November 2009, a total of 42 womenwith uterine prolapse presented at the Department of Gynecol-ogy II, Renmin Hospital of Wuhan University. The age range atsurgery was 35-57 (mean 41.1 ± 9.4) years. Consent wasobtained from each patient and we did not take extra blood ortissues from any patient. All medical records were reviewed.Ethical approval was obtained from the Research Ethics Com-mittee of our hospital. All assessments in the study were carriedout by a gynaecologist who had not performed the operation.
The stage of prolapse was assessed using the InternationalContinence Society pelvic organ prolapse quantification (ICSPOP-Q) [3] system. The patients were selected on the basis ofPOP-Q stage 2-4. Women with POP-Q stage 1 of prolapse andrepeat surgery for recurrent prolapse were excluded.
All patients had a preoperative evaluation which included adetailed history, physical examination, gynaecological exami-nation, routine preoperative examination and thinprep cytologictest (to eliminate cervical lesions). Appropriate antibiotic cov-erage was given perioperatively. After surgery, total operatingtime and blood loss during surgery were recorded. The postop-erative Foley catheter was removed within 24 hours. Routinephysical examination and gynaecological examination wererepeated ranging from 2-36 months. Minimum follow-up wastwo months for all patients. These patients were asked the samequestions with respect to possible complaints including tenes-mus, dysuria, dyschesia, and dyspareunia. Prolapse recurrencewas considered as any symptomatic prolapse or stage at orabove 2. The end of follow-up was defined as recurrence of pro-lapse and any complaint mentioned above.
Comparison between preoperative and postoperative POP-Qscores was conducted with use of the t test (Table 1). Chi-squaretests were performed to investigate the influence of tenesmus,dysuria, dyschesia, and dyspareunia (Table 2). A p value lessthan 0.05 was considered to be significant and less than 0.01 tobe highly significant. Prolene mesh (Johnson & JohnsonMedical Ltd., Shanghai, China) was used during surgery for allcases.
SummaryObjective: To analyze the clinical effects of laparoscopic sacral colpopexy using prolene mesh for patients with pelvic organ pro-
lapse. Methods: Laparoscopic placement of prolene mesh in the rectovaginal septum and veslcovaginal septum of 42 women withuterine prolapse with bladder and rectum prolapse. One mesh was fixed to the round ligaments and another to the periosteum of thesacral vertebrae. Operation time, blood loss, complication rate and follow-up surgery results were recorded monthly and analyzedaccording to the POP-Q system. The uterus was preserved in all cases. Results: The mean operating time was 92 ± 12 min and themean blood loss during surgery was 98 ± 11 ml. Postoperatively, both prolapse and symptoms were highly significantly improved (p< 0.001) according to the pelvic organ prolapse quantification (POP-Q) system. Conclusions: Laparoscopic sacral colpopexy for uterineprolapse using prolene mesh is a minimally invasive and effective new technique that offers a chance for patients who desire to pre-serve their uterus.
Key words: Uterine prolapse; Laparoscopy; Sacral colpopexy; Mesh.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
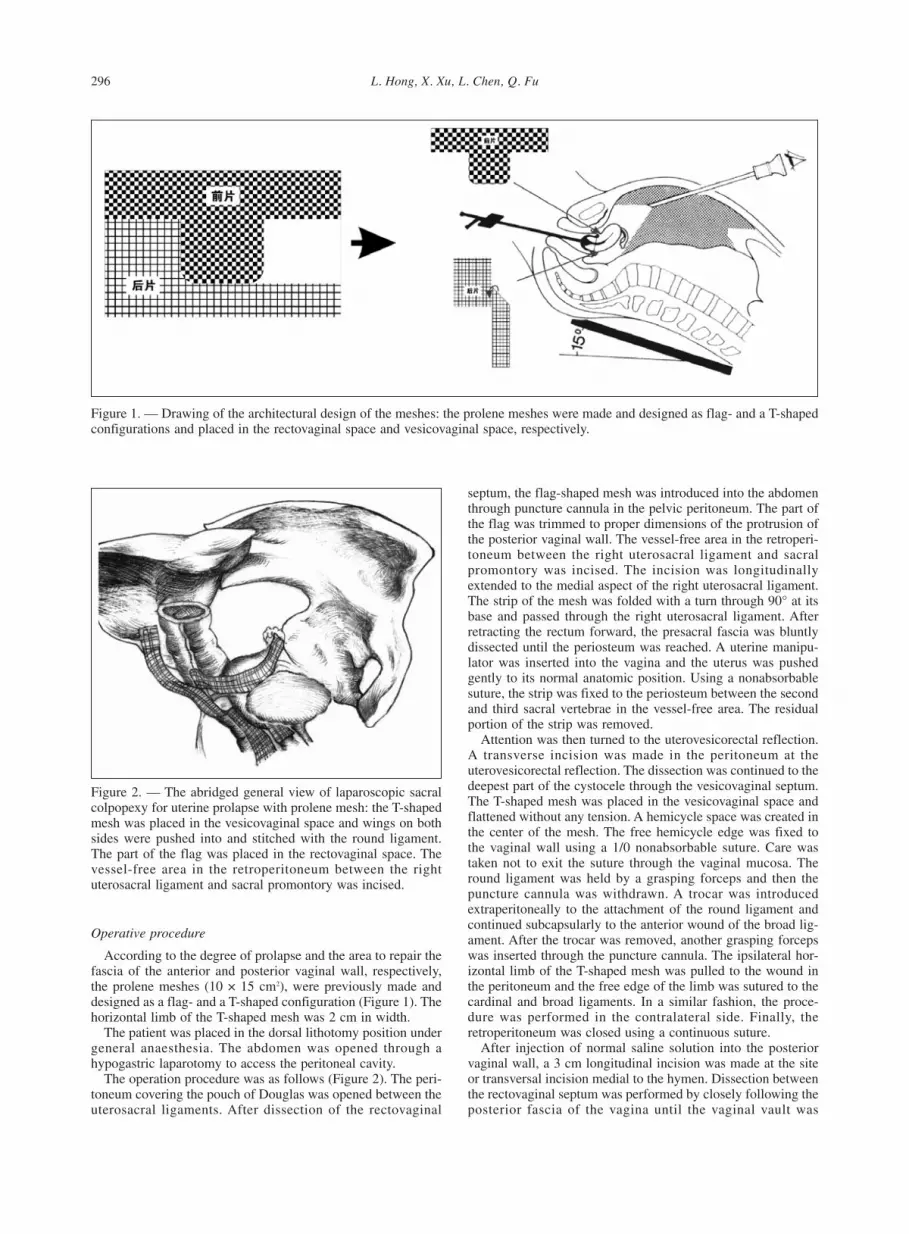
L. Hong, X. Xu, L. Chen, Q. Fu 296
Operative procedure
According to the degree of prolapse and the area to repair thefascia of the anterior and posterior vaginal wall, respectively,the prolene meshes (10 × 15 cm2), were previously made anddesigned as a flag- and a T-shaped configuration (Figure 1). Thehorizontal limb of the T-shaped mesh was 2 cm in width.
The patient was placed in the dorsal lithotomy position undergeneral anaesthesia. The abdomen was opened through ahypogastric laparotomy to access the peritoneal cavity.
The operation procedure was as follows (Figure 2). The peri-toneum covering the pouch of Douglas was opened between theuterosacral ligaments. After dissection of the rectovaginal
septum, the flag-shaped mesh was introduced into the abdomenthrough puncture cannula in the pelvic peritoneum. The part ofthe flag was trimmed to proper dimensions of the protrusion ofthe posterior vaginal wall. The vessel-free area in the retroperi-toneum between the right uterosacral ligament and sacralpromontory was incised. The incision was longitudinallyextended to the medial aspect of the right uterosacral ligament.The strip of the mesh was folded with a turn through 90° at itsbase and passed through the right uterosacral ligament. Afterretracting the rectum forward, the presacral fascia was bluntlydissected until the periosteum was reached. A uterine manipu-lator was inserted into the vagina and the uterus was pushedgently to its normal anatomic position. Using a nonabsorbablesuture, the strip was fixed to the periosteum between the secondand third sacral vertebrae in the vessel-free area. The residualportion of the strip was removed.
Attention was then turned to the uterovesicorectal reflection.A transverse incision was made in the peritoneum at theuterovesicorectal reflection. The dissection was continued to thedeepest part of the cystocele through the vesicovaginal septum.The T-shaped mesh was placed in the vesicovaginal space andflattened without any tension. A hemicycle space was created inthe center of the mesh. The free hemicycle edge was fixed tothe vaginal wall using a 1/0 nonabsorbable suture. Care wastaken not to exit the suture through the vaginal mucosa. Theround ligament was held by a grasping forceps and then thepuncture cannula was withdrawn. A trocar was introducedextraperitoneally to the attachment of the round ligament andcontinued subcapsularly to the anterior wound of the broad lig-ament. After the trocar was removed, another grasping forcepswas inserted through the puncture cannula. The ipsilateral hor-izontal limb of the T-shaped mesh was pulled to the wound inthe peritoneum and the free edge of the limb was sutured to thecardinal and broad ligaments. In a similar fashion, the proce-dure was performed in the contralateral side. Finally, theretroperitoneum was closed using a continuous suture.
After injection of normal saline solution into the posteriorvaginal wall, a 3 cm longitudinal incision was made at the siteor transversal incision medial to the hymen. Dissection betweenthe rectovaginal septum was performed by closely following theposterior fascia of the vagina until the vaginal vault was
Figure 1. — Drawing of the architectural design of the meshes: the prolene meshes were made and designed as flag- and a T-shapedconfigurations and placed in the rectovaginal space and vesicovaginal space, respectively.
Figure 2. — The abridged general view of laparoscopic sacralcolpopexy for uterine prolapse with prolene mesh: the T-shapedmesh was placed in the vesicovaginal space and wings on bothsides were pushed into and stitched with the round ligament.The part of the flag was placed in the rectovaginal space. Thevessel-free area in the retroperitoneum between the rightuterosacral ligament and sacral promontory was incised.

Laparoscopic sacral colpopexy for uterine prolapse with prolene mesh 297
reached. The free edge of the flag-shaped mesh was pulleddown to the lowest position of the posterior vaginal wall andthen fixed to the perineal body and bilateral levator ani muscles.The wound in the vaginal wall was closed.
Results
Total operating times ranged from 80 to 104 (average92 ± 12) min. The mean intraoperative blood loss was 92ml (range 98 ± 11 ml). No complications occurred duringthe surgery. Of all cases, there were two with urine diffi-culty (4.76%) who were released after three continuousurinary catheterisations. Five cases had passing stool dif-ficulty (11.90%), in whom four recovered after symptomtreatment, and one recovered one month after surgery.Three cases experienced sexual discomfort (7.14%), inwhom two were one month after surgery, and one wasthree months after surgery. All patients were followedmonthly through outpatient department visits and tele-phone surveys and accurate outcome data of the lastfollow-up (range 2-36 months) were obtained with thefollow-up rate being 97.62%. One patient was lost tofollow-up. There was no recurrent prolapse in any of the41 followed patients. Mesh infection or erosion was notobserved. Pre- and postoperative POP-Q scores wereassessed, respectively. The index point C, Aa, Ba, Ap, andBp in all 41 patients was ≤ 1, that is, 1 cm superior to themargin of the hymen, less than grade 2 by the POP level.The vaginal index points of preoperative and postopera-tive follow-up (last follow-up) are shown in Table 1. Cal-culating the scores gave p values less than 0.0001. Therewere highly significant differences between the pre- andpostoperative POP-Q scores (Table 1). Table 2 shows thepreoperative and postoperative pelvic floor function.There were statistically highly significant differences inthe number of patients with tenesmus, dysuria and dys-pareunia (p < 0.0001), and significant differences withdyschesia (p < 0.01) (Table 2).
Discussion
Uterine prolapse is the herniation of the uterus into orbeyond the vagina as a result of failure of the ligamen-tous and fascial support. A large number of correctivesurgical approaches have been described in the literaturefor uterine prolapse. One concept prevails: if surgerybecomes necessary, it allows relief of the symptoms andrestores the pelvic organs to their anatomical position.Moreover, the intervention can reduce postoperativecomplications and incidence of recurrence.
DeLancey et al. [4] described three levels of a supportsystem as follows: level 1, superior suspension of thevagina to the cardinal-uterosacral complex; level 2,lateral attachment of the upper two-thirds of the vagina;and level 3, distal fusion of the vagina into the urogenitaldiaphragm and perineal body. They noted that uterineprolapse was often associated with defects of the cardinalligaments, rectovaginal and cervical fascia. Delancey’sthree levels of support are now accepted worldwide.
Vaginal hysterectomy with posterior vaginal wall repairhas failed to correct the loss of integrity of the cardinal-uterosacral ligament complex. In addition, postoperativescarring can cause vaginal discomfort during penetration.In a retrospective study, Jin et al. [5] found that the recur-rence rate was 11.6-31.1% in women who had undergonethis procedure. Sacral colpopexy could offer goodanatomical and functional results and the reportedsuccess rate has been generally as high as 68-100% [6].
A variety of surgical procedures are available for sacralcolpopexy. In 1957, Ameline Hugier et al. [7] made adetailed description of open sacral colpopexy in whichthe vaginal vault was suspended to the anterior perios-teum of the sacrum with unabsorbable material. Scali etal. [8] in 1974 proposed the suspension by the placementof synthetic slings. However, adequate exposure of therectovaginal septum could not be obtained completelyfrom the vaginal approach. In 1993, Dorsey et al. werethe first to describe laparoscopic sacral colpopexy [9].This minimally invasive surgery implied the placement ofprosthetic mesh to restore and confer an adequate rein-forcement of the pelvic tissues. Presently, this techniqueis considered as an excellent option for uterine prolapse[2, 10, 11].
Gynacologists favour the laparoscopic approachbecause of its few complications and quick recovery,which are particularly important for patient quality oflife. The use of mesh in prolapse repair avoids depend-ence on the patient’s own weak tissues and maintainsvaginal capacity. The dimension of the flag-shaped and T-shaped mesh is individualised and based on the size ofthe patient defect at the tension-free state. Our resultsreflect benefits of the laparoscopic approach, includingexcellent vision, less trauma, less blood loss, less postop-erative pain, minimal tissue damage and scarring, no lon-gitudinal incision in the anterior vaginal wall, which canpreserve the uterus, decreased discomfort in sexual activ-ity and improvement in quality of life, better than otherreports obviously [12].
Table 1. — POP-Q measurements before surgery and at finalfollow-up.
C Aa Ba Ap Bp
Preoperation +3.11 ± 3.23 1.12 ± 1.70 +1.37 ± 1.51 -2.43 ± 1.37 -1.01 ± 1.71Final follow-up -7.12 ± 0.61 -2.51 ± 0.43 -2.17 ± 0.55 -2.49 ± 0.85 -2.61 ± 0.17T-test* 20.066 13.206 14.290 18.916 5.985The Pelvic Organ Prolapse Quantification (POPQ): Point C represents the position of the cervix orvaginal cuff. The anterior and posterior points A (Aa, Ap) are located on the midline vaginal wall 3cm proximal to the hymen (range ± 3 cm). The anterior and posterior points B (Ba, Bp) representthe maximum extent of prolapse of the anterior and posterior vaginal wall (range -3 cm to totalvaginal length [tvl]); p < 0.01.
Table 2. — Summary of the comparison of preoperative andpostoperative pelvic floor function.
Symptoms Tenesmus Dysuria Dyschesia DyspareuniaTime Cases (%) Cases (%) Cases (%) Cases (%)
Preoperation 34 80.95% 21 50.00% 17 40.48% 31 73.81%Postoperation 06 14.29% 02 04.76% 05 11.90% 03 07.14%χ2 33.939 18.894 7.128 35.230
p < 0.01.

L. Hong, X. Xu, L. Chen, Q. Fu 298
Our procedure simultaneously repairs vaginal walldefects of both levels 1 and 2. The pelvic floor is rein-forced by fascia repair and ligament reconstruction.During sacral colpopexy, care must be taken not to injurethe anterior sacral nerves or the vessels at the lateralborder of the sacrum. The round ligaments are suturedwith mesh and then combined with uterosacral ligamentmesh. This procedure stabilizes the uterus in a neutralposition which puts the vaginal vault and uterus in thecenter part of pelvic cavity, preventing the uterus frompressing on the rectum and the occurrence of cystoceleand stress urinary incontinence. The retroperitoneal posi-tion of mesh has the potential to decrease the risk ofintestinal adhesion and occurrence of a hernia beneath themesh. Adequate exposure of rectovaginal septum can bemade easier by the laparoscopic approach and the meshcan be placed into the interspace of the anterior and pos-terior vaginal walls for fascial reinforcement.
After surgery, the prolene mesh provokes a fibroticreaction and scar-tissue formation. Collagen depositionin mesh is sufficient to support the vaginal wall andprevent recurrence [13]. The use of prolene mesh theoret-ically has a lower risk of wound infection and tissueerosion [14], and these complications were not observedin our series.
The indication for this technique is women presentingwith uterine prolapse of stage 2 or more, especiallywomen who desire an active sexual life with a preserveduterus and potential fertility. The contraindicationsincluded active infection or cancer. The relative con-traindication is severe anterior and posterior vaginal wallprolapse.
This study is limited in that it is a retrospective surveyin a small population and further long-term follow-up isrequired.
In conclusion, laparoscopic sacral colpopexy withprolene mesh can effectively restore optimal vaginalfunction and anatomy and prevent prolapse recurrence,and preserve the uterus. We therefore believe that thistechnique produces excellent results.
References[1] Cutner A., Kearney R., Vashisht A.: “Laparoscopic uterine sling
suspension: a new technique of uterine suspension in womendesiring surgical management of uterine prolapse with uterineconservation”. Int. J. Gynecol. Obstet., 2007, 114, 1159.
[2] Lin L.L., Haessler A.L., Ho M.H., Betson L.H., Alinsod R.M.,Bhatia N.N.: “Dyspareunia and chronic pelvic pain afterpolypropylene mesh augmentation for transvaginal repair of ante-rior vaginal wall prolapse”. Int. Urogynecol. J. Pelvic Floor Dys-funct., 2007, 18, 675.
[3] Bump R.C., Mattiasson A., Bo K., Brubaker L.P., DeLancey J.O.,Klarskov P. et al.: “The standardization of terminology of femalepelvic organ prolapse and pelvic floor dysfunction”. Am. J. Obstet.Gynecol., 1996, 175, 10.
[4] DeLancey J.O.: “Anatomy and biomechanics of genital prolapse”.Clin. Obstet. Gynecol., 1993, 36, 897.
[5] Jin L., Wang J., Zhang X. et al.: “Clinical analysis of the relapseand its related factors in patients with pelvic organ prolapse”.Chin. J. Clin. Obstet. Gynecol., 2005, 6, 8.
[6] Ameline A., Huguier J.: “Posterior suspension to the lumbo-sacraldisk; abdominal method of replacement of the utero-sacral liga-ments”. Obstet. Gynecol., 1957, 56, 94.
[7] Maher C., Baessler K., Glazener C.M., Adams E.J., Hagen S.:“Surgical management of pelvic organ prolapse in women: a shortversion Cochrane review”. Neurourol. Urodyn., 2008, 1, 3.
[8] Rozeta F., Mandron E., Arroyo C., Andrews H., Cathelineau X.,Mombet A. et al.: “Laparoscopic sacral colpopexy approach forgenito-urinary prolapse: experience with 363 cases”. Eur. Urol.,2005, 47, 230.
[9] Dorsey J.H., Sharp H.T.: “Laparoscopic sacral colpopexy andother procedures for prolapse”. Baillière’s Clinical Obstetrics andGynaecology, 1995, 9, 749.
[10] Novara G., Galfano A., Mancini M., Ficarra V., Artibani W.: “Crit-ical assessment of pelvic floor surgical reconstruction outcome”.EAU-EBU Update Series, 2006, 4, 202.
[11] Hinoul P.: “Review of surgical techniques to insert implants inurogynaecology”. Gynaecol., Obstet., and Reprod. Med. DailyPract., 2005, 1279, 398.
[12] Limb J., Wood K., Weinberger M., Miyazaki F., Aboseif S.:“Sacral colpopexy using mersilene mesh in the treatment ofvaginal vault prolapse”. World J. Urol., 2005, 23, 55.
[13] Pascual G., Rodriguez M., Gomez-Gil V., Garcia-Honduvilla N.,Buján J., Bellón J.M.: “Early tissue incorporation and collagendeposition in lightweight polypropylene meshes: bioassay in anexperimental model of ventral hernia”. Surgery, 2008, 144, 427.
[14] Milani R., Salvatore S., Soligo M.: “Functional and anatomicaloutcome of anterior and posterior vaginal prolapse repair withprolene mesh”. BJOG, 2005, 1, 107.
Address reprint requests to:XU X., M.D.Department of Gynaecology and ObstetricsRenmin Hospital of Wuhan UniversityJiefang Road 238Wuhan, Hubei (China) 430060e-mail: [email protected]

299
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication November 26, 2009
Development of secondary ovarian lesions after hysterectomywithout oophorectomy versus unilateral oophorectomy for
benign conditions: A retrospective analysis of patients duringa nine-year period of observation
A. Baloglu, I. Bezircioglu, B. Cetinkaya, L. Karcı, M. BicerDepartment of Obstetrics and Gynecology, Ataturk Training and Research Hospital. Izmir (Turkey)
[1068/29]
Introduction
It is controversial to preserve normal appearing ovariesduring gynecological surgery for benign disease in pre-menopausal women. The incidence of re-operation for denovo developed ovarian pathologies after hysterectomy issuggested to be 3.95%. This risk of re-operation is higherduring the first three years. The risk of ovarian pathologyis significantly higher among patients in whom only oneovary is saved after hysterectomy [1].
Age, primary histological findings, and degree of peri-toneal trauma are the most important factors affectingdevelopment of ovarian pathologies after performingvaginal, laparoscopic, and abdominal hysterectomy [2].
In this study, the incidence of developed pathologiesrequired relaparotomy after hysterectomy due to benigngynecologic disease and the consequences of saving oneor both ovaries on the de novo developed pathologieswere investigated. As a conclusion of our survey, the riskof pathological outcome of retained ovaries is discussedbecause of benign gynecological disease after hysterec-tomy.
Materials and MethodsIn this retrospective analysis, data obtained from patients who
had undergone total abdominal hysterectomy with unilateraloophorectomy or without oophorectomy in the Obstetrics andGynecology Department of Izmir Ataturk Training andResearch Hospital between 01/06/2000 and 01/06/2009 wereevaluated. Selection criteria for this study included women whohad undergone hysterectomy for benign conditions where atleast one ovary was saved. The patients could be contacted byenrolled address and telephone numbers, and were invited toregular examinations annually in the outpatient clinic. Thepatients who responded to our invitation for evaluation wereasked whether or not they had developed any adnexal/ovarianpathological findings and required further gynecologic exami-nation. Ovaries and salpinges were evaluated transvaginally byultrasound. The patients presenting ovarian pathology weretreated by a medical or surgical approach after hysterectomywas registered. The time interval and histopathologic results ofdeveloped de novo ovarian pathological lesions after hysterec-tomy were recorded.
SPSS 15.0 software was used for statistical analysis. Para-metric data were tested for their normal distribution and resultsare presented by using figures with the percentages. Continuedvariables of the groups of total abdominal hysterectomy withoutoophorectomy and with unilateral oophorectomy were testedusing Mann-Whitney U-tests. Categorical variables of thegroups with total abdominal hysterectomy without oophorec-tomy and with unilateral oophorectomy were tested usingPearson’s and Fisher’s exact tests. Spearman’s correlation andlogistic regression analysis were performed. A value of p <0.005 was considered as significant.
Summary
Purpose: The effect of retained one or both ovaries on the de novo ovarian pathologies required re-operation after hysterectomydue to benign gynecologic conditions were investigated retrospectively. This study was done to determine the occurrence of diseasein retained ovaries after hysterectomy. Methods: A retrospective analysis of patient charts was performed, comparing the patientreports of women who had secondary ovarian lesions those whose previously undergone total abdominal hysterectomy with unilat-eral oophorectomy or without oophorectomy in our Department during the nine year period of observation (2000-2009). The studyincluded 1242 women with at least one ovary saved after hysterectomy for benign indications. Results: De novo ovarian disease wasestablished in 5.1% of patients of hysterectomy without oophorectomy and in 17.6% of patients of at least one ovary saved afterhysterectomy for benign indications (p = 0.005). Ovarian pathology requiring re-operation developed in 3.8% of patients who under-went hysterectomy without oophorectomy and in 5.9% of patients who underwent hysterectomy with unilateral oophorectomy (p =0.536). Conclusion: Women with unilateral oophorectomy at the time of hysterectomy had more than twice the risk of secondaryovarian lesions, compared with those without oophorectomy at hysterectomy. Determinants, such as age, parity and gravidity mustbe considered when deciding whether or not to perform oophorectomy at hysterectomy.
Key words: Hysterectomy with unilateral oophorectomy; Hysterectomy without oophorectomy; Secondary ovarian lesions.

A. Baloglu, I. Bezircioglu, B. Cetinkaya, L. Karcı, M. Bicer 300
Results
Total abdominal hysterectomy without oophorectomyand with unilateral enrolled oophorectomy was per-formed on 1,531 patients between 01/06/2000 and01/06/2009. We reached 12,871 of them by post and tele-phone calls and 1,242 patients responded to our invita-tion. There was no presenting pathological finding at thelast gynecological and transvaginal ultrasound examina-tions. After the patients had undergone hysterectomy, anadnexal mass developed in 102 patients, and re-operationwas performed on 54 of them. There were no differencesbetween the groups of hysterectomy without oophorecto-my and with unilateral oophorectomy in terms of age,menarche age, gestation, and parity (Table 1).
There were also no differences between the groups interms of infertility, systemic disease, genital disease,breast disease and any familial cancer. Preoperative ovar-ian diseases were encountered more in the group of hys-terectomy with unilateral oophorectomy (Table 2).
Indications and histopathological results of the hys-terectomies are summarized in Table 3. Mostly the formerindication of the operation was leiomyoma in the group ofpatients who underwent hysterectomy without oophorec-tomy, while endometrial hyperplasia, endometriosis, andan adnexal mass were significantly more frequent in thegroup of patients who underwent hysterectomy with uni-lateral oophorectomy.
Mean follow-up time was 38.51 months in the group ofpatients without oophorectomy and 52.57 months in thegroup of patients with unilateral oophorectomy. Duringthis period, ovarian disease was established in 48 (5.1%)patients of the group with hysterectomy without oophorec-tomy, and re-operation was performed in 36 (3.8%) ofthem. Ovarian diseases developed in 54 (17.6%) patients inthe group with hysterectomy and unilateral oophorectomy,and 18 (5.9%) were re-operated. The frequency of ovarianpathologies requiring re-operation after hysterectomy was3.8% in patients with both ovaries preserved, 5.9% inpatients with only one ovary preserved, and 4.3% in allpatients. There were no significant differences between thegroups with or without re-operation according to age,menarche, gestation, parity, and follow-up time (Table 4).
Histopathologic results of the surgical specimens: func-tional ovarian cysts in six patients and benign tumors in
the other 48 patients. Mean time-interval after hysterecto-my and re-operation was 26.33 months for all patients.The mean-time intervals were 25.50 months in only hys-terectomy patients, and 28.00 months in hysterectomywith unilateral oophorectomy patients.
There were weak correlations between development ofovarian pathologies after hysterectomies done for indica-
Table 1. — Continued variables of the group that underwenttotal abdominal hysterectomy without oophorectomy and thegroup with unilateral oophorectomy. Mann-Whitney U tests wereperformed.
TAH TAH+USO p valuemean ± SD range mean ± SD range
Age 39.72 ± 4.94 20-47 41.25 ± 5.69 28-54 0.080Menarche 13.15 ± 1.34 9-16 13.41 ± 1.52 11-17 0.868Gestation 2.94 ± 1.86 0-9 3.37 ± 1.72 1-7 0.171Parity 2.32 ± 1.45 0-6 2.39 ± 1.20 1-6 0.836Follow-up
time (month) 38.51 ± 31.25 1-112 52.57 ± 31,37 1-111 0.005Reop. interval
(months) 25.50 ± 13.17 11-49 28.00 ± 7.81 19-33 0.517
Table 2. — Categorical variables of the group that underwenttotal abdominal hysterectomy without oophorectomy and thegroup with unilateral oophorectomy.
TAH TAH+USO p valuenumber percent number percent
Infertility 84 9.0 0 0 0.024#
Systemic disease 420 44.9 108 35.3 0.230*
Genital disease 48 5.1 36 11.8 0.101*
Breast disease 24 2.6 0 0 0.574#
Familial cancer history 48 5.1 0 0 0.204#
Postoperative ovariandisease 48 5.1 54 17.6 0.005*
Re-operation required (ovarian disease) 36 3.8 18 5.9 0.536*
*Pearson’s and #Fisher’s exact tests were performed.
Table 3. — Indications and histopathology of thehysterectomies were compared with *Pearson’s and #Fisher’sexact tests.
TAH TAH+USO p valuenumber percent number percent
IndicationsUterine myoma 726 77.6 138 45.1 0.000*
Dysfunctional uterinebleeding 72 7.7 24 7.8 0,972*
CIN 36 3.8 24 7.8 0.248*
Uterine atonia 48 5.1 0 0 0.204#
Hydatiform mole 12 1.3 0 0 1.000#
Endometrial hyperplasia 42 4.5 24 7.8 0,003#
Pelvic inflammatorydisease 0 0 24 7.8 0.354*
Endometriosis 0 0 12 3.9 0.060#
Adnexal mass 0 0 60 19.9 0.000*
PathologyLeiomyoma 630 67.3 162 52.9 0.064*
Adenomyosis 108 11.5 48 15.7 0.437*
Infection-dependent variables 12 1.3 12 3.9 0,255#
Pregnancy-dependentvariables 36 3,8 0 0 0,340#
CIN 36 3.8 12 3.9 1.000#
Endometrial hyperplasia 42 4.5 24 7.8 0.354*
Others 72 7.7 48 15.7 0.093*
Table 4. — Groups with or without re-operation werecompared with Mann-Whitney U tests.
The group with re-operation The group without re-operation p value(n: 9) (n: 198)
mean ± SD range mean ± SD range
Age 41.11 ± 6.17 33-49 40.06 ± 5.12 20-54 0.833Menarche 13.11 ± 1.05 12-15 13.22 ± 1.40 9-17 0.764Gestation 3.44 ± 1.23 2-5 3.03 ± 1.85 0-9 0.333Parity 2.78 ± 1.20 1-4 2.32 ± 1.40 0-6 0.180Follow-up
time (months) 59.56 ± 31.25 28-104 41.18 ± 31.78 1-112 0.064

Development of secondary ovarian lesions after hysterectomy without oophorectomy versus unilateral oophorectomy for benign etc. 301
tions of endometrial hyperplasia (rho: –0.243, p < 0.001),adnexal mass (rho: –0.179 p: 0.010), and unilateraloophorectomy (rho: –0.196, p: 0.005). There was also aweak correlation between pathologies requiring re-opera-tion after hysterectomy and indications of an adnexalmass (rho: 0.173, p: 0.013).
Discussion
There is no consensus concerning optimal adnexal sur-gery during abdominal hysterectomy, when continuedhormonal function is desired, associated with reducedsequelae in the future.
Oophorectomy was performed for the purpose of pre-venting ovarian cancer in 78% of hysterectomies ofwomen between age 45 and 64. However the rate of mor-tality for ovarian cancer is less than the rate of mortalityfor cardiovascular disease and hip fracture in these ageintervals. Hysterectomy alone has been shown to reducethe risk of developing ovarian cancer by an average of46% [3]. Prophylactic oophorectomy has been shown toreduce the incidence of ovarian cancer by 8-18% in theliterature from developed countries. However, in thecountries in which incidence of ovarian cancer is muchlower than those in developed countries, prophylacticoophorectomy in women undergoing hysterectomyreduced the ovarian cancer incidence by 0.4-3.2% [4].
Hormonal analysis showed that the functions of the dis-missed ovaries were more rapidly lost than the controls ofthe same age intervals. The results of Chan’s study sug-gested that hysterectomy with ovarian conservation couldpreserve a woman’s normal hormonal milieu. The uteruscould have a control mechanism on ovulation, and hys-terectomy might stimulate early menopause [5].
The changes in the ovaries were investigated in patientswho had undergone abdominal hysterectomy with con-servation of the ovaries for benign conditions [6]. It wasestablished that hysterectomy affected ovarian blood sup-ply and function. Women with hysterectomy had signifi-cant elevated serum FSH level and lower ovarian stromalblood flow as compared with healthy women. There wasgood correlation between Doppler and endocrine param-eters [7-9]. There was an increase in ovarian vascularresistance following hysterectomy. These changes may beresponsible for altered ovarian function hysterectomy.
Bukovsky et al. examined ovarian function followingabdominal hysterectomy with or without unilateraloophorectomy and they reported that 35% of patientsundergoing unilateral oophorectomy demonstratedimpaired ovarian function six months after the operation,whereas only one of the patients with both ovaries pre-served demonstrated impaired ovarian function. Thus, ifthe ovaries are to be preserved at hysterectomy, it seemsto be more beneficial to preserve both ovaries [9].
In an experimental rat model, histopathologic evalua-tion of the ovaries after hysterectomy showed that ovariesof the hysterectomized group had significantly fewer pri-mary, preantral, and antral follicles, and significantlymore corpora lutea, atretic, and cystic follicles [10].
The results of this experimental rat model suggest thathysterectomy may affect ovarian function. Therefore,when continued ovarian function following abdominalhysterectomy is desired and ovarian cystic pathologiesare not encountered, preservation of both ovaries seems tobe more beneficial [10].
Holub et al. found that the rate of adnexal pathologiesrequiring re-operation after abdominal hysterectomy was5.67%. They suggested that the important factors affect-ing re-operation rate were age, primary histologic find-ings, and smaller peritoneal trauma [2].
Plöckinger et al. published a study which included1,265 women with at least one ovary saved after hysterec-tomy for benign indications [1]. They found that develop-ment of ovarian pathologies requiring re-operation afterhysterectomy was suggested to be 3.95% of patients. Ofthe patient group with prior hysterectomy, 7.63% hadsome pathologies in the retained ovary. Among patientswith hysterectomy only, 3.47% developed ovarianpathologies requiring re-operation. In our study, 4.3%required re-operation. This ratio was found to be 3.8% forpatients with both ovaries saved, while 5.9% for patientswith one ovary saved after hysterectomy. This differencewas not statistically significant. The re-operated patientsin Plöckinger’s study had undergone hysterectomy at ayounger age, had less parity, and had more nulliparitythan the patients who were not re-operated. We did notfind any difference in age, parity and gravidity betweenthe patients with and without re-operation. The meanintervals between hysterectomy and re-operation were29.5 (1-120) months in Plöckinger’s study, and 26.3 (11-49) months in our study. Follow-up time of the groups inour study showed re-operation interval was longer, butnot statistically significant. Longer follow-up time maylead to more established pathologies.
A decrease in blood flow and endocrine functions werenoted in ovaries preserved after hysterectomy in variousstudies [10]. Ovarian function loss was earlier in cases inwhom one ovary was left than cases in whom both ovarieswere left. On the other hand, when one ovary was left, theincidence of developing an ovarian pathology whichmight require re-operation was more frequent. More stud-ies are needed to determine the factors which affect thedevelopment of secondary ovarian lesions when single orboth ovaries are left. Simply, after the results of thesestudies the final decision to perform elective oophorecto-my at the time of hysterectomy for benign disease couldbe established on an individual basis.
Conclusion
Women with unilateral oophorectomy at the time ofhysterectomy had more risk of secondary ovarian lesionscompared with those without oophorectomy at hysterec-tomy. Determinants such as age, parity and gravidity mustbe considered when deciding whether or not to performoophorectomy at hysterectomy.

A. Baloglu, I. Bezircioglu, B. Cetinkaya, L. Karcı, M. Bicer 302
References[1] Plöckinger B., Kölbl H.: “Development of ovarian pathology after
hysterectomy without oophorectomy”. J. Am. Coll. Surg., 1994,178, 581.
[2] Holub Z., Jandourek M., Jabor A., Kliment L., Wágnerová M.:“Does hysterectomy without salpingo-oophorectomy influence thereoperation rate for adnexal pathology? A retrospective study”.Clin. Exp. Obstet. Gynecol., 2000, 27, 109.
[3] Parker W.H., Broder M.S., Liu Z., Shoupe D., Farguhar C., BerekJ.S.: “Ovarian conservation at the time of hysterectomy for benigndisease”. Clin. Obstet. Gynecol., 2007, 50, 354.
[4] Charoenkwan K., Srisomboon J., Suprasert P., Phongnarisorn C.,Siriaree S., Cheewakriangkrai C.: “Role of prophylactic oophorec-tomy at the time of hysterectomy in ovarian cancer prevention inThailand”. J. Obstet. Gyneacol. Res., 2004, 30, 20.
[5] Chan C.C., Ng E.H., Ho P.C.: “Ovarian changes after abdominalhysterectomy for benign conditions”. J. Soc. Gynecol. Investig.,2005, 12, 54.
[6] Xiangying H., Lili H., Yifu S.: “The effect of hysterectomy onovarian blood supply and endocrine function”. Climacteric, 2006,9, 283.
[7] Petri Nahás E.A., Pontes A., Nahas-Neto J., Borges V.T., Dias R.,Traiman P.: “Effect of total abdominal hysterectomy on ovarianblood supply in women of reproductive age”. J. Ultrasound Med.,2005, 24, 169.
[8] Sezik M., Ozkaya O., Demir F., Sezik H.T., Kaya H.: “Total salp-ingectomy during abdominal hysterectomy: effects on ovarianreserve and ovarian stromal blood flow”. J. Obstet. Gyneacol.Res., 2007, 33, 863.
[9] Bukovsky I., Halperin R., Schneider D., Golan A., Hertzianu I.,Herman A.: “Ovarian function following abdominal hysterectomywith and without unilateral oophorectomy”. Eur. J. Obstet.Gynecol. Reprod. Biol., 1995, 58, 29.
[10] Tapisiz O.L., Gungor T., Aytan H., Zergeroglu S., MulazimogluB., Bilge U., Mollamahmutoglu L.: “Does hysterectomy affectovarian function? Histopathologic evaluation and serum FSH,inhibin A, and inhibin B levels in an experimental rat model”. Eur.J. Obstet. Gynecol. Reprod. Biol., 2008, 140, 61.
Address reprint requests to:A. BALOGLU, M.D.Talatpasa Street Number: 61/4Alsancak, Izmir (Turkey) 35220e-mail: [email protected]

303
Revised manuscript accepted for publication November 26, 2009
Unwanted pregnancy and induced abortion among youngwomen 16-22 years old in Greece:
a retrospective study of the risk factors
N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. IavazzoFamily Planning Unit, 2nd Department of Obstetrics and Gynecology,
Aretaieio Hospital, University of Athens Medical School, Athens (Greece)
[1064/29]
Introduction
Unwanted pregnancy, defined as a pregnancy occurringaccidentally and against the individual’s will and deci-sion, is a public problem with severe health and socioeco-nomic consequences. Unfortunately, its effects and thesubsequent induced abortions are quite enlarged inyouths. There is evidence that, compared to women whoabort at an older age, women who abort as teens are sig-nificantly more likely to report more severe emotionaland medical complications related to their abortions; afinding which is supported by the fact that women, whoaborted as teens, participate in disproportionately largenumbers in post-abortion counseling programs [1]. On theother hand, if an unintended, and most of the timesunwanted pregnancy of a young individual ends up in alive birth, the future is rarely optimistic, since such preg-nancies are frequently associated with a number ofadverse circumstances, like low academic and profession-al achievements, single parenthood and child abuse [2].Moreover, giving birth while still a teenager is stronglyassociated with disadvantages in later life. On average,according to UNICEF, across 13 countries of theEuropean Union, women who gave birth as teenagers aretwice as likely to be living in poverty. In other words,reducing teenage births offers an opportunity to reduce thelikelihood of poverty and of its perpetuation from one gen-eration to the next [3]. However, most adolescents chooseto have an abortion because they have concerns about howa baby would change their lives (e.g., completing theireducation), they worry about financial problems, or theyfeel that they are not mature enough to become a parent[4]. Although, according to the official recorded evidence
of UNICEF, adolescent birth rates in Greece have fallenmore than three times in the last 30 years, we still have oneof the highest rates of abortions in Europe [3]; a realityshowing at large that more action has to be taken to reducethese numbers and ameliorate the lives of thousands ofyoung people. In our country, there were two remarkableevents that took place in the 1980s and contributed to thelimitation of unwanted pregnancy: the development offamily planning clinics in 1980, which aimed at a higherlevel of sex education provided in our population, and thelegislation of abortion in 1986, for the struggle againstunsafe abortions and their complications, like infection,sepsis, perforation of the uterus, subfertility, upcomingpsychological problems, troubled relationships and, evenworse, maternal death. Despite the efforts that havealready been performed by the state, preventive policiesare still weak in Greece, making women rely on abortionto control births [5]. These policies must be directlyderived from studying the risk factors for the persistenceof this situation in youths: Low level of sex education?Low use of safe-reliable methods of contraception? Lowlevel of consultation before or after the abortion by gyne-cologists? High number of lifetime sexual partners? Self-destructive behaviors (alcohol or drug abuse, smoking,suicidal ideation, etc.)? Others? Furthermore, we have towonder deeply who is really responsible for this socialabnormality; our schools, our families, the media, the doc-tors, the state or, just the young people themselves?
It is an extremely disheartening fact that there is almostcomplete lack of evidence in the field of induced abor-tions in Greece, especially in youths, since the existenceof any official records would indeed promote the under-standing of the possible risk factors which are involved inthe phenomenon, and would underline the best strategythat could be followed towards the elimination of thissocial scourge. The main reason for this deficiency of
SummaryUnwanted pregnancies and the subsequent induced abortions are common problems of our youths in modern Greece. The aim of this
study was to recognize the risk factors of the problem in an effort to find the best possible solution out of this social dead end. Mate-rials and Method: We interviewed 1,320 young female individuals and analyzed their answers using statistical analysis. Results: Severaluseful conclusions were reached concerning the forces that are involved in unwanted pregnancy/induced abortions. Discussion: Wehave tried to underline the strategy to combat the problem. Conclusion: Sexual education and the proper use of contraception remainthe essential tools in this effort.
Key words: Unwanted pregnancies; Induced abortions; Risk factors; Contraception; Sexual education.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. Iavazzo 304
recorded evidence is that induced abortions are oftenunder-reported in national surveys, since they are stillconsidered to be a social taboo and the majority, whichare mainly carried out in the private sector (94%), remainunregistered [6]. Of course, the problem is maximizedwhen, in an effort to clarify the correlation between thefactors of unwanted pregnancy and its further socioeco-nomic results, we try to make records of the total percent-age of unintended pregnancy among young people, notonly those which end up in abortion but also those whichare carried out to term. Nevertheless, we have to realizethat the matter in question is multidimensional, concern-ing both its causes and its results, and from this point ofview we have to search in many fields in an attempt todetect the factors which enhance the disease, and to pointout the several repercussions in our lives. The purpose ofthis study was to investigate a complex interplay of forceswhich are supposed to present the risk factors for unwant-ed pregnancy and induced abortions among women 16-22years-old within the Greek society and, finally to reach astrategy that could be followed in order to confront thismajor social problem.
Materials and Methods
Data were gathered from a population-based survey whichwas conducted among women in the late and post adolescenceyears (16-22 years-old) who reported that they had alreadyexperienced sex. We approached by interviewing them throughanonymous questionnaires and studied the experience and opin-ions of each of 1,320 young women on certain issues concern-ing sexual health, unwanted pregnancies and induced abortions.Recruitment was performed by approaching the youths in manyareas throughout the country – urban or rural –, like highschools and universities (during sexual education programmes),homes and several working places (through invitation letters),giving information about the study. An interview was arrangedwith each potential participant to administer the questionnaire.The interviews were conducted in a variety of places (at home,in the work place, at schools or in the universities of the inter-viewees) and sensitive questions, like those on abortion, wereanswered in a self-completed questionnaire. Finally, we gath-ered data from 730 pupils in high school, 400 students in sever-al universities and 190 female individuals (either employees orunemployed). Permission to use this sensitive data was obtainedfrom each participant through the Ministry of Health and theMinistry of Education. The questionnaires used were plain and
Table 1. — Questionaire on sexual health.
Measure Question Categoriesb
Education (e) How many years have you studied? “e < 6 years” (less than 6: rudimentary school, now working orunemployed)? “> 6 e < 9 years” (more than 6 but less than 9: gym-nasium or working unemployed)? “> 9 e < 12 years” (more than 9but less than 12: high school or working unemployed)? “> 12 yearse“(more than 12 university or working unemployed)?
Habits Have you ever used or been addicted “yes”, “no”to any kind of substance?(Alcohol? Drugs? Smoking?)
Medical history Have you ever been diagnosed to suffer “yes”, “no”from any psychological conditions?(Official diagnosis of stress, depression, self-destructive behavior, suicidal attempts, suicidal ideation?)
Age at first How old were you at your first coitus? “< 15”,“15”,“16”,“17”,“18”,“19”,“> 19”intercourse years-oldNumber of pregnancies How many times have you been pregnant? “0”, “1”, “> 1”Number of children How many children do you have? “0”, “1”, “> 1”Miscarriages Did you ever have at least 1 miscarriage “yes”, “no”
in the past? If “yes”: “1?” , “> 1?”Number of Have you ever had an induced abortion? “yes”, “no”induced abortions If “yes”, how many times have you If “yes”, “1?” / “2?”/ “> 2?”
experienced that?Time of abortion(s) If you have children and you have also e.g. abortion – birth - abortion
undergone abortion(s), could you describethe sequence of these events?
Quality of information How well do you feel that you have been “satisfying” , “not satisfying”(consultation) given informed by the specialist on the field of by the specialist induced abortion before or after having one?before and after (only for those who had an abortion in the past)the abortionSources of sexual Pick up the main and the secondary source “school”, “family”, “friends”, “media”, “doctors”education of your sexual education Use and type of What contraceptive methods do you usually “withdrawal”, “condom”, “IUD”, “pill/OCs”, “abstinence”, contraception use? (pick up to two) “emergency contraception”, “other” (like the rhythm method),
“no/none”Number of lifetime How many sexual partners have you had “1”, “2” , “> 2”sexual partners in your life?

Unwanted pregnancy and induced abortion among young women 16-22 years old in Greece: a retrospective study of the risk factors 305
simple to comprehend and the key questions and measuresderived from them are given in Table 1. We obtained informa-tion on nationality, age, religion, education, habits, medical his-tory, marital status and number of children, age at first inter-course, number of abortions in the past, sources of sexual edu-cation, use and type of contraception, and number of lifetimesexual partners.
Age, nationality, and religion were the information needed toconfirm that the interviewees were 16-22 years-old, Greeks, andOrthodox Christians. In this way, we prevented any differencesin the participants’ opinions to be attributed to nationality orreligious influences and consequently, we tried to present thestance and experience of the average young individual with anactive sexual life in the Greek society; a reality for which thissurvey was conducted. Statistical analysis of the data was donewith SPSS (Statistical Package for Social Sciences). The chi-square criterion was used to investigate whether distributions ofseveral categorical variables differ from one another (signifi-cance level of our study = 0.01, meaning that when p (probabil-ity) > 0.01 in certain df – degrees of freedom – (which meansthat p value in the χ2 test is < 0.01), the results are statisticallysignificant and the null hypothesis of independence is rejected).
Results
The results of the above questionnaire are cited belowin Table 2, and the analysis of each potential risk factorfollows next.
Education (e): 41 women (group A) reported education“e < 6 years” (and now working or unemployed), 110(group B) answered “> 6 years e < 9 years” (and nowworking or unemployed), 752 (group C) “> 9 years e <12 years” (high school, working unemployed) and 417(group D) “> 12 years e” (university, working unem-ployed). Females, who had had one or more induced abor-tions (435), are distributed as follows according to theireducation level: 38 women (92, 68% of group A) in the“e < 6 years” category, 96 (87, 27% of group B) in “> 6years e < 9 years”, 200 (26, 59% of group C) in “> 9years e < 12 years” and 101 (24, 22% of group D) in“> 12 years e” category. Using the chi square test, we findp > 0.01, a statistically significant relation between thetwo values (education, abortion) and, to be more precise,there is a negative correlation between the level of edu-cation, as a risk factor, and the possibility of inducedabortion. In simple words, the less educated someone is,the more likely she is to undergo an abortion.
Habits: 468 youths in our survey (35.45%) answered“yes” to the question and 852 (64.55%) “no”. We noticedthat 197 women (42.9% of the “yes” group) that reportedhaving “bad habits” (smoking, alcohol etc.) had under-gone one or more induced abortions, while 271 (31.81%of the “no” group) of the second group had had the sameexperience. Statistical calculations of the data revealed χ2
> 6.635 (df = 1), p > 0.01. “Bad habits” seem to positive-ly affect the incidence of induced abortions.
Medical history: 149 young females answered “yes” tothe question. To be more specific, 89 women who report-ed to have experienced at least one pregnancy before(17.25% of the group of 516 women – see Table 2 “num-ber of pregnancies”), answered that they had had a posi-tive medical history for psychological conditions in thepast and they had visited a specialist for this reason atleast once in their lifetime. On the other hand, 60 women,out of those who had had no pregnancy in the past (804),gave the same answer as the previous group (7.46% ofthis population). According to the chi-square test, χ2 >6.635 (df = 1), p > 0.01, which means that the nullhypothesis – that pregnancy in this age group is independ-ent of psychological medical history – is rejected. In otherwords, we observe that there is a positive relationshipbetween pregnancy rates and psychological conditions in16-22 year-old women.
Age at first intercourse: 752 (56.97%) women answeredthat they had had their first sexual intercourse < 18 years ofage and 568 (43.03%) reported age at first coitus > 18years old. The mean age of first coitus of the sample was17.56 years old. The statistical study of its distributionamong young women, in relation to any potential inducedabortions, revealed that the earlier a female had had her
Table 2. — Answers to the sexual health questionaire.
Measure Number of individuals/interviewees
Education (e) “e < 6 years”: 41 , “> 6 e < 9 years”: 110, “>9 e < 12 years”: 752, “> 12 years e”: 417
Habits “yes”: 468 , “no”: 852Medical history “yes”: 149, “no”: 1171Age at first intercourse Mean age: 17.56 years oldNumber of pregnancies “0”: 804 , “1”: 251 , “> 1”: 265Number of children “0”: 1175, “1”: 122, “> 1”: 23Miscarriage(-s) “yes”: 90, “no”: 1230 / “1”: 58, “> 1”: 32Number of induced “yes”: 435,“no”: 885 / “1”: 338, “2”: 72, “>abortions 2”: 25Time of abortion(s) “abortion after birth”: 79, “abortion before
birth”: 28Quality of information “satisfying”: 151 , “not satisfying”: 284given by the specialistbefore and after theabortionSources of sexual “school”: 217, “family”: 341, “friends”: 1134education “media”: 688, “doctors”: 260Use and type of “withdrawal”: 470, “condom”: 780, “IUD”:contraception 170, “pill/OCs”: 109, “abstinence”: 85,
‘emergency contraception”: 792, “other”(like the method of the rhythm): 65,“no/none”: 169
Number of lifetime “1” : 732 ,” “2”: 428 , “> 2”: 160sexual partners
Table 3. — Pregnancies categorized by parity, abortions or miscarriages.
Number of women reporting Children “1” Children “> 1” Abortion: “1” Abortions: “2” Abortions: “> 2” Miscarriages (at least one)
Pregnancy : “1” 22 - 216 - - 13Pregnancy: “> 1” 100 23 122 72 25 77Total 122 23 338 72 25 90

N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. Iavazzo 306
first coitus, the more likely she would have undergone anabortion.
Number of pregnancies: 516 women answered that theyhad experienced at least one pregnancy before and, more-over, 265 individuals out of the above-mentioned group (ofthese 516 women) reported more than one pregnancy - seeTable 3.
Number of children: 122 young females reported hav-ing had one child, while another 23 had more than one.Twenty-two women had had just one pregnancy in thepast that had ended up in a live birth, 85 reported an abor-tion before or after their child’s birth, five had had twoabortions and had given one live birth, one had had morethan two abortions and had given one birth, nine reportedone live birth and medical history of miscarriage(s), sixhad had two children and no abortion or miscarriage intheir medical history, 14 had had an abortion before orafter two live births, one answered three live births andone abortion in her medical history, one reported two livebirths and two abortions and finally, one answered twobirths and history of miscarriage(s) - see Table 4.
We can clearly conclude that 91 women had had onechild and history of abortion (group A), while 16 women,having had the same medical history, answered “morethan one child” (group B). Sixty-three women in group Aand 16 in group B (all of them) reported that the abor-tion(s) had taken place after the birth of their child(ren).The chi square test reveals again p > 0.01. Number ofchildren is a factor which affects a woman’s decision toabort. The more children a female has, the more likely sheis to decide on abortion to control births.
Miscarriage: 90 (6.81% of the population we studied)women (of all groups: with or without any children, withor without having had any abortions) answered positivelythat they had experienced at least one miscarriage in theirlife. Fifty-eight females reported just one miscarriage intheir medical history, while 32 reported more than one.
Number of abortions: 435 (32.95%) female individuals,either parous or nulliparous, reported having undergoneat least one abortion in the past, while 1/6 (72 women) ofthem (435) reported two and 1/17 (25 women) had expe-rienced more than two abortions. Two hundred and six-teen women answered that they had had only one preg-nancy before which had ended up in induced abortion and122 reported an abortion before or after birth or miscar-riage.
Quality of information (consultation) given by the spe-cialist before and after the abortion: 284 women (out of435 that had had at least one abortion) answered “not sat-
isfying” and 151 “satisfying”: 208/284 (61.54% of thegroup of 338 women reporting only 1 abortion) hadundergone one abortion in the past, 54/284 two (75% ofwomen with 2 abortions) and 22/284 more than two(88% of the women with > 2 abortions). Statistical analy-sis (χ2 test) showed that the quality of information givenby the specialist before and after the abortion plays animportant role in the prevention of future induced abor-tions.
Sexual education: In Greece, like in all the Westernworld, there are several potential sources of sexual edu-cation such as school, family, friends, media and doctors.According to our study, 12.95% (171) of female youthssupported “school” as the main source of sexual educa-tion, 9.55% (126) chose “family”, 38.79% (512)“friends”, 22.58% (298) “media” and 16.13% (213)“doctors”. As far as the secondary source of sexual edu-cation is concerned, 3.48% (46) answered “school”,16.29% (215) “family”, 47.12% (622) “friends”, 29.55%(390) “media” and 3.56% (47) “doctors” - see Table 5.
We can clearly make out that the main influence onthis field is coming from “friends” (1,134 individualshave picked it up either as a main or secondary factor /85.91%), then from “media” (688/52, 12%), “family”(341/25, 83%), “doctors” (260/19, 697%) and, finally,“school” (217/16, 44%). We noticed that school, familyand doctors (their proportion was diminished in thegroup A category) are more reliable sources of sexualeducation than friends and media (their proportion wasincreased in the group A category) in our society, sincestatistical analysis using the chi square test and evalua-tion of each proportion have revealed p > 0.01; meaningthat the null hypothesis (abortions are independent of thequality of sexual education/information) is rejected.
Contraception: The use and type of contraception cho-sen in the questionnaire were the following: “withdrawal”(470/35.61%), “condom” (780/59.09%), IUD(170/12.88%), “pill/OCs” (109/8.26%), “abstinence”(85/6.44%), “emergency contraception” (792/60%),“other” like the rhythm method (65/4.92%) and “none”(169/12.80%). We notice that the main preferences in con-traception of these young women were “emergency con-traception” and “condom”, then “withdrawal”, “IUD”,“pill/OCs”, “abstinence” and in the end, several “other”methods. Of youths, 12 (80%) reported that they had notused any kind of contraception during sexual intercourse -see Table 6.
Statistical analysis of the above data showed that the useand the type of contraception are very important in the pre-vention of an unwanted pregnancy and the following abor-tion(s). Traditional methods of contraception like with-drawal, condoms and others appear to be a statistically sig-nificant increased proportion in women reporting abor-tion(s), whereas, in women without abortions, the percent-ages, which are increased, point to more contemporarymethods that are available to the common woman (IUD,pill/OCs, emergency contraception). It is obvious that con-temporary methods are more reliable than traditional ones.As far as abstinence is concerned, it is undoubtedly a tradi-tional and efficient way to prevent an unwanted pregnancy.
Table 4. — Medical history of abortions and miscarriages inrelation to parity.
No. of children = 1 No. of children > 1
No abortion/no miscarriage 22 6History of 1 abortion 85 15History of 2 abortions 5 1History of > 2 abortions 1 0History of miscarriages 9 1

Unwanted pregnancy and induced abortion among young women 16-22 years old in Greece: a retrospective study of the risk factors 307
Number of lifetime sexual partners: 732 (55.45%) indi-viduals reported having had one sexual partner until thetime of the survey, 428 (32.42%) reported two and 160(12.12%) more than two lifetime sexual partners - seeTable 7.
We noticed that 117 women that had had live births wereincluded in the category of “one lifetime sexual partner”,23 in the “two lifetime sexual partners” category and fivein “more than two lifetime sexual partners”. The chi-squaretest showed p > 0.01 for all the above categories, meaningthat parity is related (negatively) to the number of lifetimesexual partners in this age group (the null hypothesis:«number of lifetime sexual partners / parity» is rejected).Moreover, we made out that, of the 435 females who hadundergone one or more induced abortions, 169 (23.8% ofthe subgroup) were coming from the first category, 187(43.69%) from the second and finally, 79 (49.37%) fromthe third category. The chi-square test revealed p > 0.01,showing that the more lifetime sexual partners someonereports, the more likely she is to have undergone an abor-tion (the null hypothesis: «number of lifetime sexual part-ners / possibility of abortion» is rejected).
Discussion
Recently it has been noted that teenagers are sexuallyactive in younger ages and demonstrate lower complianceto contraceptive methods. An unintended, and most of thetime unwanted pregnancy brings teenagers to a crisis. The
decision to interrupt a pregnancy is today taken frequent-ly. Although the teenage birthrate declined from 9.0% in1985 to 5.2% in 2003, teenage pregnancy still remains aserious medical and social problem and abortion rates arestill extremely high during adolescence [7].
In our study, the prevalence of self-reported abortionswas highest among 16-22 year-old women with a lowlevel of education and/or “bad” habits and/or medical his-tory of psychological disturbances and/or high number oflifetime sexual partners and/or earlier age at first inter-course. Additionally, women who were parous (havingone or more children), misinformed by specialists on thematter of abortions, without any proper sexual educationand using mostly unreliable methods of contraception orno contraception at all were more likely to experience anunwanted pregnancy and a following induced abortion. Itseems that this problem reflects more extensive and seri-ous abnormalities in several sectors of our modern socie-ty which need to be addressed.
Education: The state must take measures to promotethe level of youth’s education. Teaching people to thinkfreely, to understand human values, and to act with merit,is the first step to enhance the social balance and to solvemany of our contemporary problems, like the scourge ofunwanted pregnancies. The more responsible people arein their lives, the more respected the idea of reproductionand birth become. Not only do we have to combat illiter-acy, but also it is essential to improve the current way oflearning and lead it towards the human principles. This isthe deduction from our study in the sector of education –the family, schools and state have to realize that adoles-cents and young people must be given the chance of highquality education in order to prevent future unwantedpregnancies and induced abortions.
Bad habits: In our study there was a significant differ-ence in the abortion rate between females with alcoholabuse or smoking and females without such habits. Thefamily could play an important role through consultation
Table 5. — Sources of sexual education in women who underwent abortions or not.
Categories School Family Friends Media Doctors
A: Women reporting 20 (8 1st choice, 63 (14.48%) 433 (99.54%) 308 (70.80%) 46 (10.57%)abortion(s) 12 2nd choice) 4, 1st: 30, 2nd: 33 1st: 238, 2nd: 195 1st: 125, 2nd: 183 (1st: 33, 2nd: 13)in the past (435) 60% of group AB: Women without 197 (1st: 163, 2nd: 34) 278 (31.41%) 701 (79.21%) 380 (42.93%) 214 (24.18%)abortion(s) in their 22.26% of group B 1st: 96, 2nd: 182 1st: 274, 2nd: 427 1st: 173, 2nd: 207 1st: 180, 2nd: 34medical history (885)
217 341 1134 688 260
Table 6. — Use and type of contraception in women who had abortions and those who did not.
Categories Withdrawal Condom IUD Pill/OCs Abstinence Emergency Other None
A: Women reporting 195 312 33 19 9 178 39 85abortion(s) (44.83% of (71.72%) (7.59%) (4.37%) (2.07%) (40.92%) (8.97%) (19.54%)in the past (435) this group A)B: Women without 275 468 137 90 76 614 26 84abortion(s) in their (31.07% of (52.88%) (15.48%) (10.17%) (8.59%) (69.38%) (2.94%) (9.49%)medical history (885) this group B)
470 780 170 109 85 792 65 169
Table 7. — Lifetime sexual partners and pregnancy outcome.
Categories Live births (145) Abortions (435)
“One lifetime sexual partner” (732) 117/145 169/435“Two lifetime sexual partners” (428) 23/145 187/435“More than two lifetime sexual
partners” (160) 5/145 79/435

N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. Iavazzo 308
on this subject, and so as the state, through laws, and theschool, through providing a better education. “Bad”habits, as a sign of personal weakness, can be successful-ly eliminated, thus helping us to suppress in a more effi-cient way the abortion rates among our youths.
Medical history: According to our survey unwantedpregnancies and the consequences (induced abortions,undesired births and children, child abuse, etc.) can belimited if we fight several taboos in the area of a psychol-ogist’s consultation. It is necessary for young person toseek and accept a specialist’s advice, when needed, andthis should not become a social stigma. In this way, manyunwanted pregnancies can be prevented and well beingcan be established among young women.
Apart from the above-mentioned character of the prob-lem in question, there is another and more practical sidewhich needs to be approached, as cited below:
Sexual education: As the sexual activity rate in adoles-cence is reportedly increasing worldwide, improvingknowledge concerning sexual education in adolescentsmight contribute to improving reproductive health issuesin such age groups [8]. This should be provided mainly bythe school, family and doctors. Media and friends caneasily mislead and confuse young females. Unfortunately,sex education is still not included in the Greek school cur-riculum, and only sporadic information is given [5].Moreover, many parents still believe that there is no needfor sexual information at school due to personal taboos.However, the Ministry of Education and several non gov-ernmental organizations, such as the Greek Society ofFamily Planning, organize teaching programmes onHealth Education for adolescents [6]. We just have to sup-port this effort in order to reach, via our schools, a satis-fying level of sexual education. We should improve theattitudes, beliefs and knowledge of Greek adolescentsregarding sexual intercourse, contraception and sexuallytransmitted diseases through organizing better pro-grammes on sexuality for youths [9]. Also parents can betrained so as to develop an understanding and properbehavior on this topic towards their children. The role ofthe gynecologists of course is very important and we haveto urge youths to have regular visits.
Quality of information (consultation) given by the spe-cialist before and after an abortion: Our study has clear-ly shown that 65.29% of the women who had had at leastone abortion in their medical history, were not satisfiedwith the quality of consultation by their doctor before andafter the abortion. This is in accordance with what theNon-Aligned Women’s Movement in 1992 argued:despite the fact that abortions were legalized in 1986 andcovered by insurance funds, some women were beingtreated in a hostile way by doctors and social workers inthe public hospitals [6]. Doctors must be convinced that awoman having an abortion is in a sensitive and vulnerableposition, needing information and psychological supportbefore and after the procedure. Younger women have aneven more difficult time adjusting to their abortions. Onestudy found that teenage aborters were more likely toreport severe nightmares following abortion and to score
higher on scales measuring antisocial traits, paranoia,drug abuse and psychotic delusions than older aborters[1]. Considering the above, we understand the necessityof proper information given by the doctor to the patient.Another problem, which can be prevented, is “replace-ment pregnancies”. Young people tend to repeat pregnan-cies; a symptom of youths “acting out” unresolved abor-tion issues and the desire to “replace” the lost pregnancywith another child, which is often aborted because thewoman faces the same pressures as she did the first time,and sometimes even more so [1]. To sum up, a high qual-ity of consultation contributes to the decrease of futureand repeated unwanted pregnancies and induced abor-tions in youths.
Use and type of contraception: In Greece poor educa-tion on the issue of contraception still remains a majorproblem among teenagers contributing to the increasedprevalence of undesired pregnancies and abortions [10].Greek society has not fully adopted the modern methodsof contraception, and appears to have one of the lowestrates of modern contraceptive use in Europe [5]. Coitusinterruptus and condom use are the most commonly usedmethods in our country, whereas the pill and other reli-able contraceptive methods appear to have low use rates.Contraception is the proper way in which sexual behavioris expressed; the personality and level of the general andsexual education of the individual, as well as the maturi-ty of her environment, are reflected thoroughly in theindividual’s contraceptive consciousness. Consequently,abortion in our country is a part of the Greek contracep-tive culture [11] and from this point of view, it is veryimportant that contraception-related topics be introducedas a part of sexual education, despite several adverse cir-cumstances, like the generation gap between parents andchildren, the lack of teachers trained in sexual educationand discussion and other barriers [12].
Conclusion
The matter of unwanted pregnancies and their follow-ing induced abortions among youths 16-22 years-old inGreece is existent and extremely important to be solved toameliorate the everyday life of thousands of young peo-ple. We have to concentrate on the risk factors for the phe-nomenon and try to find the path away from this scourge.Sexual education and the proper use of contraceptionremain the essential tools in our effort.
References[1] Sobie A.R., Reardon D.C.: “Detrimental effects of adolescent
abortion”. Post-Abortion Review, 2001, 9 (1).[2] Panagopoulos P., Salakos N., Bakalianou K., Davou E., Iavazzo
C., Paltoglou G., Liapis A.: “Adolescent pregnancy in a Greekpublic hospital during a six-year period (2000-2005). A retrospec-tive study”. J. Pediat. Adolesc. Gynecol., 2008, 21, 265.
[3] UNICEF: “A league table of teenage births in rich nations”,Innocenti Report Card No.3, July 2001. UNICEF InnocentiResearch Centre, Florence.

Unwanted pregnancy and induced abortion among young women 16-22 years old in Greece: a retrospective study of the risk factors 309
[4] http://www.childtrendsdatabank.org/indicators/27TeenAbortions.cfm[5] Ioannidi-Kapolou E.: “Use of contraception and abortion in
Greece: A review”. Reprod. Health Matters, 2004, 12 (suppl. 24),174.
[6] Salakos N., Bakalianou K., Gregoriou O., Iavazzo C., PaltoglouG., Creatsas G.: “Abortion rates and the role of family planning: apresentation of the Greek reality”. Clin. Exp. Obstet. Gynecol.,2008, 35, 279.
[7] Deligeoroglou E., Christopoulos P., Creatsas G.: “Pregnancy andabortion in greek adolescent gynecologic clinics” Akush Ginekol(Sofiia), 2004, 43 (suppl. 4), 37.
[8] Bakalianou K., Salakos N., Iavazzo C., Liapis A., Gregoriou O.,Papadias K.: “Greek students’ experiences, attitudes and knowl-edge about reproductive health”. 2nd Department of Obstetrics andGynecology, University of Athens, Aretaieion Hospital, Athens,Greece.
[9] Bakalianou K., Salakos N., Iavazzo C., Gregoriou O., Botsis D.,Papadias K.: “Adolescent sexuality: The Greek reality”. 2nd
Department of Obstetrics and Gynecology, University of Athens,Aretaieion Hospital, Athens, Greece.
[10] Mavroforou A., Koumantakis E., Michalodimitrakis E.:“Adolescence and abortion in Greece: women”s profile and per-ceptions”. J. Pediat. Adolesc. Gynecol., 17, 321.
[11] Georges E.: “Abortion policy and practice in Greece”. Soc. Sci.Med., 1996, 42, 509.
[12] Regushevskaya E., Dubikaytis T., Laanpere M., Nikula M.,Kuznetsova O., Haavio-Mannila E. et al.: “Risk factors for inducedabortions in St. Petersburg, Estonia and Finland. Results from sur-veys among women of reproductive age”. Eur. J. Contracep.Reprod. Health Care, 2009, 14, 176.
Address reprint requests to:A. KOUMOUSIDIS, M.D.Grigoriou Lambraki 112-114Pireas, PC 18532 (Greece)e-mail: [email protected]

310
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
[789/27]
Revised manuscript accepted for publication December 23, 2009
Conservative and surgical treatment of abnormalplacentation: Report of five cases and review of the literature
M. KazandiDepartment of Obstetrics and Gynecology, Ege University Faculty of Medicine, Bornova, Izmir (Turkey)
[1073/29]
Introduction
Adherent placenta is one of the major causes of hem-orrhage during pregnancy [1]. Adherent placenta isknown as abnormal attachment of placental villi throughthe uterine wall. It has three distinct groups known as pla-centa accreta, increta and percreta [2]. The etiology isunknown but the incidence of adhesive placenta increaseswith advanced maternal age, history of previous cesareansection and placenta previa totalis in pregnancy [3]. Themajor problem with placental adhesive disorder ismassive hemorrhage. We report five cases at risk forobstetric hemorrhage because of adherent placenta andplacenta previa totalis.
Case Reports
Case 1
A 33-year-old multi gravida was admitted to our departmentbecause of vaginal bleeding. She was at 28-29 weeks of gesta-tion. She had had a regular antenatal follow-up with two previ-ous cesarean sections. In her physical examination vaginalbleeding was determined. Obstetrical examination at admissionshowed a 28-29 week uterus without signs of active labor. Whenshe was at 32 weeks of gestation, cesarean section was per-formed and a 1,800 g live baby was delivered with an apgarscore of 1 and 5 min of 10 and 10, respectively, because ofvaginal bleeding and being in active labor. Before cesareansection, magnetic resonance imaging (MRI) was performed. InMRI placenta previa totalis and increta was reported. Within theoperative exploration both myometrial invasion and serosa-bladder adhesions were observed. Bilateral uterine and hipogas-tric arteries was ligated after delivery and the operation wasended. Three units perioperatively and three units postopera-tively red blood cell packages were transfused. In the postoper-ative period hysterectomy was performed by explorativelaparatomy because of unpreventable vaginal bleeding.
Case 2
A 28-year-old primigravida was admitted to our departmentfor a planned cesarean section. She was at 35 weeks of gesta-tion. She had had regular antenatal follow-up with no remark-able medical or physical findings. Obstetrical examinationincluded a 35-36 week uterus that was not in active labor withan intact amniotic membrane. When she was at 36 weeks ofgestation, elective cesarean section was performed and a 3,000g live baby was delivered with an apgar score of 1 and 5 min of8 and 10, respectively. MRI, which was performed before thecesarean, showed placenta previa totalis. Myometrial andserosal invasion were also noted. In gray scale ultrasonography(US), more than six irregular and large placental lacunale weredefined. There were no focal exophytic masses invading thebladder serosa and wall. The hyperechoic serosa-bladder inter-face was not intact. The subplacental sonolucent area was irreg-ular. A hypervascular serosa-bladder interface was seen. Withthese findings we supposed the case was placenta percreta. Pre-operative exploration was both definitive and diagnostic ofpathology. Placenta percreta was suspected before delivery.After delivery hysterectomy was performed. Five units of redblood cells were transfused peroperatively. No postoperativecomplication was observed. The patient was discharged on thefourth postoperative day with a healthy baby. Pathologicalexamination confirmed the clinical and surgical diagnosis asplacenta percreta.
Case 3
A 38-year-old gravida 7, para 4 women was admitted to ourdepartment because of vaginal bleeding. She was at 31-32weeks of gestation. She had had regular antenatal follow-up anda previous cesarean section. Obstetric examination included a31-32 week uterus that was not in active labor. In her physicalexamination only vaginal bleeding was determined. Cesareansection was performed with a median incision below the umbli-cus and a 2,200 g live baby was delivered with an apgar scoreof 1 and 5 min of 8 and 10, respectively. Before cesareansection MRI was performed and placenta previa totalis and pla-centa increta were determined. After delivery the placenta wasnot separated so hysterectomy was performed. Pathologicalexamination revealed placenta percreta.
Summary
Abnormal placentation is a serious complication of pregnancy. The disorder is also associated with significant maternal morbid-ity. Abnormal placentation, comprised of placenta accreta, increta, and percreta, is a leading cause of postpartum hemorrhage andindication for gravid hysterectomy. We present five cases of successful conservative and surgical management of abnormal placen-tation managed at our institution, together with a review of the literature.
Key words: Abnormal placentation; Cesarean hysterectomy; Hemorrhage.

Conservative and surgical treatment of abnormal placentation: Report of five cases and review of the literature 311
Case 4
A 34-year-old gravida 2, para 1 pregnant woman was referredto our department because of the diagnosis of placenta previatotalis and placenta percreta. She had had a previous cesareansection and a regular antenatal follow-up. Obstetric examinationshowed a 38-week uterus that was not in active labor. MRIreported myometrial invasion with the suspicion of bladder wallinvasion. An elective cesarean section was performed with amedian incision below the umblicus. Operative exploration wasdefinitive and diagnostic of pathology. Bladder invasion wasseen before delivery. An oblique uterine incision was done closeto the fundus of the uterus and a 3,000 g live baby was bornwith 1 and 5 min apgar scores of 8 and 10, respectively. Hys-terectomy was not performed because of the tight bladder inva-sion. The placenta was left in the uterus and the operation wascompleted. After the surgery methotroxate was given five timeswith the dose of 100 mg for each treatment. However the pla-centa did not separate from the uterus after all the medicaltherapy. Thus second-look laparotomy was done 50 days laterand the placenta was separated by sharp curretage.
Case 5
A 28-year-old gravida 2, para 1 pregnant woman was hospi-talized in our department because of placenta previa totalis andplacenta percreta. She was at 32 weeks of gestation and she wasin active labor. Obstetrical examination showed a 32-weekuterus and the amniotic membrane was not intact. She had hada previous cesarean section. She had had regular antenatalfollow-up in our department and when she was at 28 weeks ofgestation MRI was performed. At MRI placenta previa totalisand placenta percreta were shown. There was also a report ofbladder invasion at MRI. Gray scale and color Doppler US werealso performed and findings revealed the case was placentapercreta with bladder invasion. A medial incision below theumblicus was performed and in perioperative exploration therewas no sign of bladder invasion but myometrial invasion wasnoted. A 1,800 g live baby was born with 1 and 5 min apgarscores of 8 and 10, respectively. The placenta was not separatedand hysterectomy was performed. Three units of red blood cellswere transfused. The patient was discharged on the fourth post-operative day without complications.
Discussion
Adherent placenta is an implantataion defect character-ized by the placental villi growing into the myometriumand serosa [4]. There is an absence or defiency inNitabuch’s layer or desidua basalis. It has three distinctsubgroups known as placenta accreta, increta and perc-reta. The incidence of adherent placentation varies fromone in 540 to one in 93,000 deliveries [5]. Adherant pla-centa is one of the major causes of obstetric hemorrhageand itis associated with an increasing number of cesareansections.
The etiology of adherent placenta is unknown. It maybe related to damage of the decidua basalis, which allowsplacental invasion into the myometrium. The barrierfunction of the decidua is absent and invasive tro-phoblasts may invade the myometrium. Several condi-tions are associated with abnormal placentation; placentaprevia, a previous cesarean section, multiple pregnancies,a history of dilatation and curettage, a history of manual
extraction of the placenta, high parity and advancedmaternal age [6]. These may be named risk factors, butthey are rarely the sole cause of adherent placenta. Inrecent studies in women with placenta previa totalis, theadherent placentation risk ranges from 2% to 39% withmaternal age older than 35 and two or more previouscesarean sections [2]. The rising cesarean section ratemay be the cause of an increased rate of placenta percretain recent years.
In all five case the patients had placenta previa totalis.In cases 1, 3, 4 and 5 the patients had a history ofdamaged decidua basalis.
The diagnosis of adherent placenta is difficult, but veryimportant due to the possible fatal and maternal outcomes.It is a significant risk factor for maternal and fetal mortal-ity. Several diagnostic modalities have been introduced inrecent years. These include transvaginal and transabdom-inal US with color Doppler imaging [7-9] and MRI. Ingray scale US the subplacental sonolucent zone, regularhyperechoic serosa-bladder zone and lacunale are signifi-cant in the diagnosis of adherent placenta [10, 11]. Anirregular and thick subplacental sonolucent zone andlarge, irregular and more than six lacunale with turbulentblood flow can be seen [12, 17]. It has been suggested thatthe single most important factor affecting outcome isantepartum identification of abnormal placentation [18].This represents a possibility of accurate planning of labor.It is important for the obstetrician to be aware of the dif-ferent strategies of management.
In all five cases we performed MRI imaging and two ofthese cases were also studied by US. In cases 2 and 5 thegray scale and color Doppler US findings indicated pla-cental adhesion disorders, where the placenta was notseparated and hysterectomy was performed.
Two main options have been introduced for the man-agement of placenta percreta [19-22]: surgical removal ofthe uterus and involved tissues, and conservative therapy[23-25]. The latter includes, leaving the placenta in situwith packing, piecemeal blunt dissection with packing,uterine curettage with packing, closing of the uterinedefect, localized excision and uterine repair, uterinepacking with uterine and even hypogastric artery ligation,and adjuvant chemotherapy [22-25].
Hysterectomy has been the traditional treatment forplacenta percreta [4, 20]. This is based on the belief thatconservative treatment gives a much higher maternalmortality rate. Conservative management is beneficial inpreserving future fertility, and may reduce the need fortransfusion [19, 23-25].
We performed a median abdominal incision below theumblicus and uterine incision close to the uterine fundusin all five cases. In case 4 we could not perform hysterec-tomy and did conservative therapy. We left the placentain situ and ligated both the uterine and hypogastric arterybilaterally and continued with methotrexate treatment.However the result was not satisfactory. We performedsecond-look surgery and separated the placenta withuterine curretage.
The main complication of placenta percreta is severe

M. Kazandi 312
bleeding [18]. Other serious complications are rupture ofthe uterus, coagulation problems, invasion of adjacentorgans, uterine inversion secondary to attempted manualremoval of the placenta, fistula formation and loss ofreproductive organs [11, 14, 17, 18].
The wish to preserve fertility and control bleedingduring the operations made it possible to choose a con-servative surgical technique.
References[1] Chou M.M., Ho E.S., Lee Y.H.: “Prenatal diagnosis of placenta
previa accreta by transabdominal color Doppler ultrasound”.Ultrasound Obstet. Gynecol., 2000, 15, 28.
[2] Masselli G., Brunelli R., Casciani E., Polettini E., Piccioni M.G.,Anceschi M., Gualdi G.: “Magnetic resonance imaging in the eval-uation of placental adhesive disorders:correlation with colorDoppler ultrasound”. Eur. Radiol. 2008, 18, 1292
[3] Yang J.I., Lim Y.K., Kim H.S., Chang K.H., Lee J.P., Ryu H.S.:“Sonographic findings of placental lacunae and the prediction ofadherent placentain women with placenta previa totalis and priorcesarean section”. Ultrasound Obstet. Gynecol., 2006, 28, 178.
[4] Bodner L.J., Nosher J.L., Gribbin C., Siegel R.L., Beale S., ScorzaW.: “Balloon-assisted occlusion of the internal iliac arteries inpatients with placenta accreta/percreta”. Cardiovasc InterventRadiol., 2006, 29, 354.
[5] Hsu T.Y.: “Abnormal invasive placentation-placenta previa incretaand percreta”. Taiwan J. Obstet. Gynecol., 2009, 48, 1.
[6] Hung T.H., Hsieh C.C., Hsu J.J., Chiu T.H., Lo L.M., Hsieh T.T.:“Risk factors for placenta previa in an Asian population”. Int. J.Gynaecol. Obstet., 2007, 97, 26.
[7] Japaraj R.P., Mimin T.S., Mukudan K.: “Antenatal diagnosis ofplacenta previa accreta in patients with previous cesarean scar”. J.Obstet. Gynaecol. Res., 2007, 33, 431.
[8] Thia E.W., Lee S.L., Tan H.K., Tan L.K.: “Ultrasonographical fea-tures of morbidly-adherent placentas”. Singapore Med. J., 2007,48, 799.
[9] Wong H.S., Cheung Y.K., Zuccollo J., Tait J., Pringle K.C.: “Eval-uation of sonographic diagnostic criteria for placenta accreta”. J.Clin Ultrasound., 2008, 36, 551.
[10] Sumigama S., Itakura A., Ota T., Okada M., Kotani T., HayakawaH. et al.: “Placenta previa increta/percreta in Japan: a retrospectivestudy of ultrasoundfindings, management and clinical course”. J.Obstet. Gynaecol. Res., 2007, 33, 606.
[11] Hasegawa J., Matsuoka R., Ichizuka K., Mimura T., Sekizawa A.,Farina A., Okai T.: “Predisposing factors for massive hemorrhageduring Cesarean section in patientswith placenta previa”. Ultra-sound Obstet. Gynecol., 2009, 34, 80.
[12] Tuzovi L., Djelmis J., Iliji M.: “Obstetric risk factors associatedwith placenta previa development: case-control study”. Croat.Med. J., 2003, 44, 728.
[13] Levine D., Hulka C.A., Ludmir J., Li W., Edelman R.R.: “Placentaaccreta: evaluation with color Doppler US, power Doppler US,and MR imaging”. Radiology, 1997, 205, 773.
[14] Chou M.M., Chen W.C., Tseng J.J., Chen Y.F., Yeh T.T., Ho E.S.:“Prenatal detection of bladder wall involvement in invasive pla-centation withsequential two-dimensional and adjunctive three-dimensional ultrasonography”. Taiwan J. Obstet. Gynecol., 2009,48, 38.
[15] Lerner J.P., Deane S., Timor-Tritsch I.E.: “Characterization of pla-centa accreta using transvaginal sonography and color Dopplerimaging”. Ultrasound Obstet. Gynecol., 1995, 5, 198.
[16] Takai N., Eto M., Sato F., Mimata H., Miyakawa I.: “Placentapercreta invading the urinary bladder”. Arch. Gynecol. Obstet.,2005, 271, 274.
[17] Comstock C.H.: “Antenatal diagnosis of placenta accreta: areview”. Ultrasound Obstet. Gynecol., 2005, 26, 89.
[18] Shih J.C., Palacios Jaraquemada J.M., Su Y.N., Shyu M.K., LinC.H., Lin S.Y., Lee C.N.: “Role of three-dimensional powerDoppler in the antenatal diagnosis of placentaaccreta: comparisonwith gray-scale and color Doppler techniques”. UltrasoundObstet. Gynecol., 2009, 33, 193.
[19] Ferrazzani S., Guariglia L., Triunfo S., Caforio L., Caruso A.:“Conservative management of placenta previa-accreta by prophy-lactic uterine arteries ligation and uterine tamponade”. Fetal.Diagn. Ther., 2009, 25, 400.
[20] Carcopino X., d’Ercole C., Bretelle F.: “Optimal managementstrategies for placenta accreta”. BJOG, 2009, 116, 1538.
[21] Kent A.: “Management of placenta accreta”. Rev. Obstet.Gynecol., 2009, 2, 127.
[22] Eller A.G., Porter T.F., Soisson P., Silver R.M.: “Optimal manage-ment strategies for placenta accreta”. BJOG, 2009, 116, 648.
[23] Palacios-Jaraquemada J.: “Uterus-conserving surgery: tactics toavoid bleeding in placenta percreta”. BJOG, 2008, 115, 1717.
[24] Tong S.Y., Tay K.H., Kwek Y.C.: “Conservative management ofplacenta accreta: review of three cases”. Singapore Med J., 2008,49, e156.
[25] Timmermans S., van Hof A.C., Duvekot J.J.: “Conservative man-agement of abnormally invasive placentation” (review). Obstet.Gynecol. Surv., 2007, 62, 529.
Address reprint requests to:M. KAZANDI, M.D.Ege University, Faculty of MedicineDepartment of Obstetrics and GynaecologyBornova, Izmir 3100 (Turkey)e-mail: [email protected]

313
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication January 7, 2010
Abuse Assessment Screen (AAS) questionnaire:the Greek validation
E. Antoniou1,2, E. Ioannidi-Kapolou2, M. Daglas1,2, V. Vivilaki1, D. Karamitros1, V. Dafermos3
G. Iatrakis1
1Department of Midwifery, Technological Educational Institute of Athens (TEI), Athens2Department of Sociology, National School of Public Health, Athens
3Department of Political Sciences, University of Crete, Rethymno (Greece)
[1077/29]
Introduction
Violence against women is a complex social phenome-non of a global dimension. At the European level, theofficial definition of violence [1] against women includesany act of gender-based violence that results in or islikely to result in physical, sexual or psychological harmor suffering to women including threats of such acts,coercion or arbitrary deprivation of liberty whetheroccurring in public or private life.
Domestic violence is a social and clinical problem withincreasing dimensions influencing the lives of manypregnant women and their children [2]. The impact ofabuse on a pregnant woman’s health is significant regard-less of whether it is associated with violent acts leadingto injuries or not [2] Domestic violence prevalenceduring pregnancy is estimated at 0.9%-20.1% and domes-tic violence prevalence in general ranges from 9.7% to29.7% [3].
The abuse of pregnant women in our country has notbeen systematically and adequately studied by the scien-tific community. All attempts made are mainly a revisionof studies carried out abroad and do not include empiricaldata related to the Greek reality [4]. The difficulty in col-lecting data is mainly due to the lack of adequate data pro-vided by the various structures to which abused womengo. Thus, it is difficult to evaluate the degree, nature, seri-ousness and consequences of the phenomenon [5].
The aim of this study was the translation, cultural adap-tation and validation of a special research tool in the
framework of studying the issue of abuse against preg-nant women, that will become a model diagnostic tool inorder to record, assess and evaluate the results withregard to the abuse of pregnant women in our country.
Materials and Methods
Various methods have been recommended in the last twodecades for the screening for domestic violence. Nevertheless,few screening tools have been evaluated as diagnostic tools. TheAbuse Assessment Screen (AAS) questionnaire [6] (Table 1) isa useful, fast and easy-to-use tool to detect domestic violenceduring pregnancy and this is why it is widely used in clinicalpractice [7, 8]. It includes five questions but a shorter versionwith three questions has also been used [7]. It includes bodymaps to demonstrate the areas where body injuries have beeninflicted.
The questionnaire has been proven to effectively detectabused pregnant women [9], especially in their first regular visitfor their pregnancy [10]. In this research, each positive answerto each one of the five questions of the questionnaire was takenas one point. The cutting score was three and a total gradingwas used to verify the presence of violence during pregnancy ornot [11]. Dichotomous variables included in the questionnaireconcern questions about physical, psychological or sexual vio-lence during pregnancy and the previous year. The answers tothese questions are of the closed type (yes-no) and the psycho-metric data of the English version of the questionnaire havebeen documented in various studies [9, 12].
Translation
The translation process into Greek was the one suggested bythe Trust Scientific Advisory Committee [13]. The aim was totranslate the questionnaire from English into Greek, while
Summary
Aim: Domestic violence is a social problem with increasing dimensions worldwide. The various forms of abuse and especiallyviolence during pregnancy have not been sufficiently studied by the Greek scientific community. The aim of this study was to trans-late, culturally adapt and validate a special research tool that can be used by health professionals as a diagnostic tool for violenceduring pregnancy. Methods: The Abuse Assessment Screen (AAS) questionnaire was chosen as a screening tool. The questionnairewas translated into Greek in accordance with the procedure suggested by the ‘Trust Scientific Advisory Committee’, followed bythe cultural adaptation of the questionnaire to the Greek reality. Results: Specific psychometric tests were used for the validation ofthe questionnaire in order to assess the questionnaire’s reliability and validity, and a factor analysis was also carried out. The inter-nal consistency for all the parties who were questioned (n = 262), as expressed by Cronbach’s alpha coefficient for the AAS, was0.806 which is quite satisfactory and the results of our study suggest that the Greek translation of the AAS has a high correlationindex compared to relevant international studies. Conclusions: The AAS questionnaire in the Greek version seems to be a reliableand valid tool for the diagnosis of violence during pregnancy.
Key words: Abuse Assessment Screen questionnaire; Domestic violence; Screening tool; Pregnancy.

E. Antoniou, E. Ioannidi-Kapolou, M. Daglas, V. Vivilaki, D. Karamitros, V. Dafermos, G. Iatrakis 314
maintaining the basic characteristics of the questionnaire.According to the above-mentioned instructions, the Englishquestionnaire was translated into Greek (forward translation) bytwo different translators without each one knowing the work ofthe other. There were no significant differences in the interpre-tation of the words in the forward translation. The first versionof the questionnaire in Greek was the result of the comparisonof the two translations. This version was then translated intoEnglish (back translation) by a bilingual person (mother-tongueEnglish) with knowledge of the terminology (midwife), but didnot know the initial version of the English questionnaire. Fol-lowing that, a meeting took place with the participation of athird party, an expert in the process, and following a unanimousdecision, the first version of the questionnaire in Greek wascreated (1st reconciliation version). In the end, the English trans-lation (back translation) was sent for comments to a researchgroup of midwives at the University of Salford, studying issuesof women’s abuse. These comments were taken into considera-tion, resulting in the second version (2nd reconciliationversion).
Cultural adaptation
Taking into account the way the specific research tool wasculturally adapted in similar international studies [6, 14-16], thesecond version of the questionnaire was used in a random
sample of pregnant women for the cultural adaptation in ourcountry, as suggested in the cognitive debriefing process [13].Thus, the AAS questionnaire was given at the beginning of June2007 to five random pregnant women who visited the Outpa-tient Obstetrics Clinics of the two biggest hospitals – maternityhospitals of Athens – in order to be examined. The pregnantwomen were asked whether each question was understood andif they needed to rephrase it in their own words or preferred aspecific word in a question to be changed so that the questioncould be better understood (cognitive debriefing interview). Thequestionnaire during the cultural adaptation was in generalunderstood and easy according to the pregnant women’s com-ments. Their proposals were integrated into the second versionof the questionnaire and the final version of the questionnaire’sGreek translation was created. The randomization of the preg-nant women’s sample for the cultural adaptation of the ques-tionnaire was carried out on the basis of the simple randomsampling which is the simplest form and a flexible and inte-grated model [17].
Pilot application
Prior to distributing the final questionnaire to the pregnantwomen, it was distributed on a pilot basis to women selectedwith the method of simple random sampling during pregnancy.More specifically, the AAS questionnaire was given to tenrandom pregnant women who visited the Outpatient ObstetricsClinics of the two biggest hospitals – maternity hospitals ofAthens in order to be examined. The women’s sample used forthe pilot control had similar characteristics with the character-istics of the people included in the final samples. The aim of thepilot control was to verify:
1) The consistency and whether the questions were under-stood;
2) The adequacy of the alternative answers to all closed ques-tions;
3) Possible flow problems related to the size of the question-naire and the time required to fill it in; and
4) The need for changes and clarifications. In general terms, during the pilot application, no special
problems or questions arose and it was characterized by thewomen as an easily understood questionnaire.
Collection of research material
In the period June-September 2007, following the pilot appli-cation, the questionnaire was distributed to 262 pregnantwomen who visited the Outpatient Obstetrics Clinics of theabove-mentioned public hospitals – maternity hospitals ofAthens – to be examined. Prior to that, the scientific councils ofboth hospitals after studying the research protocol approved thequestionnaire to be used for a study. Before filling in the ques-tionnaire, all pregnant women were informed orally and inwriting by the researcher – midwife for the aim of this studyand the possible impacts of the results on the society; all thewomen signed a consensus form. The SPSS, version 15, statis-tical programme was used for the statistical analysis of the data.
Results
Application of psychometric tests (questionnaire’s vali-dation)
Specific psychometric tests were performed for thequestionnaire’s validation to evaluate the questionnaire’sreliability and validity and a factor analysis was also con-
Table 1. — The Abuse Assessment Screen (AAS) questionnaire.

Abuse Assessment Screen (AAS) questionnaire: the Greek validation 315
ducted. More specifically, the reliability was evaluated bymeasuring the internal consistency in order to check onepoint vs the other (measuring Cronbach’s alpha coeffi-cient).
The internal consistency for all the participants (n =262) as expressed with Cronbach’s alpha coefficient forthe AAS scale was 0.806, which is quite satisfactory.Table 2 shows the change of Cronbach’s alpha coefficientfor the internal consistency when a specific variable isabstracted from our factorial model. The variables arefive, as many as the questions of the AAS questionnaire.
The exploratory factor analysis
The exploratory factor analysis was performed with theuse of the principal components analysis method withVarimax with Kaiser Normalization (rotation method),looking for the special factors making up the question-naire. The factorial analysis with the method of principalcomponents was used because we wanted no interactionbetween the factors so that the groups of variables couldbe distinguished. In the end, our model showed just onegroup of variables (Table 3).
The application of the exploratory factor analysisshowed that the categories (factors) that may constitute
specific characteristics of the questionnaire, as shown inthe Screen Plot (Figure 1) are one. More specifically, asshown in Table 3, no latent value of any factor is morethan one, so our model is one-dimensional.
The method inter-item correlation matrix was used forthe analysis of the examination of the correlation of thevarious items. The specific analysis showed that all thequestions are correlated to a very good degree, as allCronbach’s alpha values were higher than 0.7 (Table 4).
Discussion
The AAS questionnaire is a useful, fast and easy to usetool to detect domestic violence during pregnancy andthis is why it is widely used in clinical practice [8, 12]. Ithas been found that the questionnaire effectively detectsabused pregnant women [9], especially during their firstregular visit of their pregnancy [10].
The size of the sample used for the weighing of thequestionnaire in the Greek language and the factorialanalysis was adequate (KMO measure of sampling ade-quacy = 0.780). The validation of the questionnaire inGreece showed that the internal consistency, as expressedwith Cronbach’s alpha coefficient for all pregnant womenthat participated (n = 262) was 0.806, which is quite sat-isfactory. Our factorial model, thus, has a high consis-tency index. Relevant studies have found that Cronbach’salpha coefficient for the AAS questionnaire rangesbetween 0.79-0.89 [9, 18] with 0.88 being the final valuewhich is higher than the one of the Greek edition but thedifference is not so great.
The AAS questionnaire in the Greek version seems tobe reliable, as it has good internal consistency (Cron-bach’s alpha = 0.780), as shown in relevant studies [19].Furthermore, our results show that the Greek translationof the AAS scale has a high correlation index comparedto relevant international studies [20, 21].
Table 2. — Item total statistics.
Scale mean if Scale variance if Corrected item- Cronbach’s alphaitem deleted item deleted total correlation if item deleted
Question 1 7.31 1.436 0.470 0.823Question 2 6.97 1.313 0.759 0.712Question 3 6.86 1.671 0.546 0.784Question 4 6.82 1.788 0.512 0.797Question 5 6.98 1.299 0.764 0.709
Table 4. — Correlation control of AAS questions.
Question 1 Qustion 2 Question 3 Question 4 Question 5
Question 1 1.000 0.434 0.297 0.254 0.489Question 2 0.434 1.000 0.554 0.481 0.795Question 3 0.297 0.554 1.000 0.432 0.475Question 4 0.254 0.481 0.432 1.000 0.494Question 5 0.489 0.795 0.475 0.494 1.000
Table 3. — Total variance explained.
Component Initial eigenvalues (a) Extraction sums of squared loadings
Total % of Cumulative Total % of Cumulativevariance % variance %
Raw 1 .488 61.442 61.442 .488 61.442 61.442Raw 2 .153 19.242 80.684Raw 3 .070 8.791 89.475Raw 4 .049 6.157 95.632Raw 5 .035 4.368 100.000Rescaled 1 .488 61.442 61.442 2.824 56.471 56.471Rescaled 2 .153 19.242 80.684Rescaled 3 .070 8.791 89.475Rescaled 4 .049 6.157 95.632Rescaled 5 .035 4.368 100.000
Figure 1. — Exploratory factor analysis.
Screen Plot
Eig
enva
lue
Component number

E. Antoniou, E. Ioannidi-Kapolou, M. Daglas, V. Vivilaki, D. Karamitros, V. Dafermos, G. Iatrakis 316
Acknowledgment
This research project was funded by the Mental Health Hos-pital of Chania, Crete, Greece.
References[1] The United Nations, Department of Public Information: “4th World
Conference of Women”. China, September 4-15, 1995.[2] Campbell J.C.: “Health consequences of intimate partner vio-
lence”. Lancet, 2002, 359, 1331.[3] Gazmararian J.A., Lazorick A., Spitz A.M., Ballard T.J., Saltzman
L., Marks J.S.: “Prevalence of violence against pregnant women”.JAMA, 1996, 275, 1915.
[4] Mouzakitis K. Marital Violence: “Aetiology, consequences, inter-vention”. Social Work, 1989, 16, 217.
[5] Chatzifotiou S., Dobash R.: “Seeking informal support: Maritalviolence against women in Greece”. Violence Against Women: J.,2001, 7, 124.
[6] Brown J.B., Lent B., Brett P.J.: “Development of the woman abusescreening tool for use in family practice”. Fam. Med., 1996, 28,422.
[7] McFarlane J., Parker B., Soeken K., Bullock L.: “Assessing forabuse during pregnancy: severity and frequency of injuries andassociated entry into prenatal care”. JAMA, 1992, 267, 3176.
[8] Pearce J.W., Hawkins C.W., Kaerney M., Peyton C.E., Dwyer J.,Haggerty L.A. et al.: “Translation of domestic violence instru-ments for use in research”. Violence Against Women J., 2003, 9,859.
[9] Parker B., McFarlane J., Soeken K., Torres T., Campell D.: “Phys-ical and emotional abuse in pregnancy: A comparison of adult andteenage women”. Nursing Res., 1993, 42, 173.
[10] Glander S., Lou M., Michielutte R., Parsons L.H.: “The prevalenceof Domestic Violence among women seeking abortion”. Obstet.Gynecol., 1998, 91, 1002.
[11] Espinosa L., Osborne K.: “Domestic violence during pregnancyimplications for practice”. J. Midwifery Women’s Health, 2002, 47,305.
[12] McFarlane L., Greenberg L., Weltge A., Watson M.: “Identifica-tion of abuse in emergency departments: effectiveness of a two-question screening tool”. J. Emergency Nursing, 1995, 21, 391.
[13] Medical Outcomes Trust: “Trust introduces new translation crite-ria”. Trust Bulletin, 1997, 5, 1.
[14] Sherin K.M., Sinacore J.M., Li X.: “HITS: A short domestic vio-lence screening tool for use in a family practice setting”. Fam.Med., 1998, 30, 508.
[15] Feldhaus K.M., Koziol-McLain J., Amsbury H.L.: “Accuracy of 3brief screening questions for detecting partner violence in theemergency department”. JAMA, 1997, 277, 1357.
[16] Yeager K., Seid A.: “Women’s mental health: primary care andvictims of domestic violence”. Primary Care: Clinics in OfficePractice, 2002, 29, 125.
[17] Dafermos V.: “Social Statistics with SPSS”. Zitis Publications,Athens 2005.
[18] Leung W.C., Leung T.W., Lam Y.Y. et al.: “The prevalence ofdomestic violence against pregnant women in a Chinese commu-nity”. Int. J. Gynecol. Obstet., 1999, 66, 23.
[19] Sinoff G., Ore L., Zlotogorsky D., Tamir A.: “Short AnxietyScreening Test-a brief instrument for detecting anxiety in theelderly”. Int. J. Geriatr. Psych., 1999, 14, 1062.
[20] Cox J.L., Holden J.M., Sagovsky R.: “Detection of postnataldepression”. Br. J. Psych., 1987, 150, 782.
[21] Pop V.J., Komptroe I.H., Van Son M.: “Characteristics of the Edin-burgh Postnatal Depression Scale (EPDS) in the Netherlands”. J.Affect Disord., 1992, 26, 105.
Address reprint requests to:E. ANTONIOU, R.M.50 Kodrigtonos Str. 11251Athens (Greece)e-mail: [email protected]

317
Revised manuscript accepted for publication June 15, 2009
Twin pregnancy after in vitro fertilization in a womanwith a unicornuate uterus
S. SugayaDepartment of Obstetrics and Gynecology, Niigata Workmen’s Accident Hospital, Joetsu City (Japan)
[996/29]
Introduction
A unicornuate uterus is a rare congenital anomalywhich is observed in only 4.4% of uterine anomalies [1].This condition is associated with a high rate of primaryinfertility and poor fetal survival [2]. This study describesthe successful outcome of a twin gestation following invitro fertilization in a woman with a unicornuate uterus.
Case Report
The patient was a 32-year-old null gravid female with a 5-year history of primary infertility. She was diagnosed with aunicornuate uterus with a non-communicating right rudimenta-ry horn, and thereafter underwent a resection of the right horn at23 years of age to treat dysmenorrhea. She first presented at theNiigata Workmen’s Accident Hospital in May 2003.
Her menstrual cycles were regular and her hormonal testingwas normal. The husband’s sperm test findings were also nor-mal. Magnetic resonance imaging (MRI) of the pelvis showed asmall uterine body with a decreased muscular mass (Figure 1).A left ovarian endometrial cyst was also noted on pelvic MRI.Hysterosalpingography showed a banana-shaped uterine cavity(Figure 2). The tubal passage of the left side was normal.
The patient underwent ovarian stimulation with 100 mgclomiphene citrate on days 4-8 of her menstrual cycle and fourrounds of intrauterine insemination. Thereafter she elected toundergo in vitro fertilization. The patient received 900 μg ofbuserelin acetate (Suprecur; Aventis Pharma Inc.) daily, startingat the midluteal phase of the pretreatment cycle and ending atthe time of hCG injection. The patient received 150 IU of hMG(HMG NIKKEN; NIKKEN CHEMICALS CO., LTD. Japan)daily from day 3 of the treatment cycle until the day before theadministration of 10,000 IU of hCG (HCG Mochida; MochidaPharmaceutical Co., Ltd., Tokyo, Japan). HCG was adminis-tered when at least two follicles reached a diameter of ≥ 18 mm.Transvaginal follicular aspiration was performed approximately34 hr after hCG injection. Five oocytes were retrieved.
Conventional insemination was performed. Three oocytes werefertilized. Embryo transfer was performed on day 3 of culture.Two good quality embryos were then transferred. A twin preg-nancy was identified in the uterus at six weeks’ gestation. A pro-phylactic Shirodkar cervical cerclage was put in place at 14weeks’ gestation.
The woman was hospitalized for premature labor and a short-ened cervical length at 22 weeks’ gestation. Intravenous tocoly-sis with a β-sympathomimetic agent and bed rest were initiated.Intravenous tocolysis was continued until delivery.
A spontaneous rupture of the membrane and labor occurred at36 1/7 weeks’ gestation. An emergency cesarean section wasperformed due to the twin gestation. A low transverse cesareansection resulted in the delivery of 2,002 g and 2,164 g infants incephalic-cephalic presentation. No uterine atony occurred. Thesubsequent postoperative course was unremarkable.
Discussion
A unicornuate uterus is associated with a poor repro-ductive outcome [3]. There is a spontaneous abortion rateof 37.1%, a preterm delivery rate of 16.4%, and a livebirth rate of 55.1% in patients with this condition [4]. Thereproductive success rate depends on variations in thevascular contribution of a uterus, the extent of the reduc-tion of muscular mass of a uterus, and the degree of cer-vical incompetence [3]. Women presenting with thisanomaly should therefore be considered high-risk obstet-rical patients.
A decision regarding the number of embryos trans-ferred was necessary in the present case, since there wasconcern that the patient’s condition would preclude a suc-cessful outcome if a twin pregnancy occurred.
To reduce the number of multiple pregnancies, singleembryo transfer has become the standard in the Nordiccountries using IVF treatment. Sweden at present has70% single embryo transfer, with 5% twins and a preg-nancy rate per transfer remaining constant at 30% [5].
Van Montfoort et al. [6] reported that the ongoing preg-nancy rates after an elective single embryo transfer in anunselected group of patients to be significantly lower in
SummaryA unicornuate uterus is a rare congenital uterovaginal anomaly. A unicornuate uterus is associated with infertility, cervical incom-
petence, and premature labor. A case of a 32-year-old null gravid female with a unicornuate uterus who had wished to bear a childfor five years is reported. After undergoing insemination treatment with the husband’s semen, in vitro fertilization was performedand a twin pregnancy occurred. A successful outcome was achieved with the delivery of viable infants following intensive obstet-ric management.
Key words: Unicornuate uterus; In vitro fertilization; Twin pregnancy.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

S. Sugaya 318
comparison to double embryo transfer (21.4% vs 40.3%).In contrast, the ongoing pregnancy rates in selectedgroups of patients did not differ between elective singleembryo transfer and double embryo transfer. They con-cluded that the pregnancy rates after single embryo trans-fer in all patients would therefore decrease two-fold incomparison to double embryo transfer.
Two-embryo transfer was therefore selected in the cur-rent patient in order to increase the pregnancy rate and, asa result, a twin gestation occurred. In this case, prophy-lactic cervical cerclage was performed at 14 weeks’ ges-tation to prevent to a preterm delivery. A successful out-come was achieved with the delivery of viable infants fol-lowing intensive obstetric management. The presence ofa unicornuate uterus is therefore not considered to be anabsolute contraindication for two-embryo transfer follow-ing in vitro fertilization.
Conclusion
A successful outcome was achieved in a patient with aunicornuate uterus and twin gestation. Two-embryo trans-fer is therefore not considered to be contraindicated insuch patients.
References[1] Acien P.: “Incidence of Mullerian defects in fertile and infertile
women”. Hum. Reprod., 1997, 12, 1372. [2] Heinonen P.K., Saarikoski S., Pystynen P.: “Reproductive perform-
ance of women with uterine anomalies”. Acta. Obstet. Gynecol.Scand., 1982, 61, 157.
[3] Taylor E., Gomel V.: “The uterus and fertility”. Fertil. Steril., 2008,89, 1.
[4] Grimbizis G.F., Camus M., Tarlatzis B.C., Bontis J.N., Devroey P.:“Clinical implications of uterine malformations and hysteroscopictreatment results”. Hum. Reprod. Update, 2001, 7, 161.
[5] Nygren K.G.: “Single embryo transfer; the role of naturalcycle/minimal stimulation IVF in the future”. Reprod. Biomed.Online, 2007, 14, 626.
[6] Van Montfoort A.P., Fiddelers A.A., Janssen J.M., Derhaag J.G.,Dirksen C.D., Dunselman G.A., Land J.A., Geraedts J.P., EversJ.L., Dumoulin J.C.: “In unselected patients, elective single embryotransfer prevents all multiples, but results in significantly lowerpregnancy rates compared with double embryos transfer: a random-ized controlled trial”. Hum. Reprod., 2006, 21, 338.
Address reprint requests to:S. SUGAYA, M.D.Department of Obstetrics and GynecologyJoetsu General Hospital148-1, Daidofukuda943-8507, Joetsu City (Japan)e-mail:[email protected]
Figure 1. — Magnetic resonance imaging of the pelvis. Asmall uterine body with a decreased muscular mass and a leftovarian endometrial cyst were noted.Figure 2. — Hysterosalpingogram showing a banana-shapeduterine cavity.
Fig. 1 Fig. 2

319
Revised manuscript accepted for publication January 7, 2010
Clinical significance of procalcitonin in cervico-vaginalsecretions of women with preterm rupture of membranes
U. Kuyumcuoglu1, K. Kangal1, A.I. Guzel1, Y. Celik2
1Department of Obstetrics and Gynecology2Department of Biostatistics and Medical Informatics, Faculty of Medicine, Dicle University, Diyarbakir (Turkey)
[1074/29]
Introduction
Preterm premature rupture of membranes (PPROM) isdiagnosed when rupture of amniotic membranes occursprior to the completion of the 36th week of gestation, andthe incidence is reported to be between 6% and 10%,with almost 80% of these cases occurring at term [1, 2].Preterm PROM is largely a clinical diagnosis. It is typi-cally suggested by a history of watery vaginal dischargeand confirmed on sterile speculum examination. The dif-ferential diagnosis includes leakage of urine (urinaryincontinence); excessive vaginal discharge, such as phys-iologic discharge or bacterial vaginosis; and cervicalmucus (show) as a sign of impending labor [3]. The peri-natal complications of PPROM change with gestationalage at rupture requiring a gestational age approach totreatment. There is little maternal benefit to conservativemanagement, but there can be significant neonatalbenefit, especially in the late second and early thirdtrimester. The benefits of conservative management aremainly in prolonging pregnancy, which has the potentialto decrease gestational age-related morbidity associatedwith preterm birth. This must be balanced with the risksof conservative management, which include cord pro-lapse, placental abruption, perinatal infection, emergentdelivery for a non-reassuring fetal status and fetal death[4]. The number of clinical methods of detecting womensuspected of subclinical intrauterine infection is modestand limited. Non-invasive methods of detecting intrauter-ine infection are desirable. Some mediators may bedetected in vaginal or cervical secretions and it seems
probable that the concentrations the vaginal compart-ment, especially after PROM, are representative of theirintra-amniotic concentrations [5].
PCT is recognized as a specific marker of generalizedbacterial infections [6, 7]. Although there is an increasingawareness of the usefulness of assessing PCT levels inclinical practice, there are only a few published dataabout PCT being evaluated during term and preterm par-turition [8, 9].
The purpose of this study was to evaluate and compareconcentrations of PCT in cervico-vaginal secretions inpregnancies complicated by PPROM and healthy preg-nant women and to determine clinical significance PCTlevels in clinical amnionitis cases.
Methods
This study was performed at Dicle University, School ofMedicine, Department of Obstetrics and Gynecology, from Sep-tember 2008 to September 2009 on 100 pregnant women.Written informed consent was obtained from all patients. Thestudy consisted of 50 pregnant patients and a control group wascreated consisting of 50 normal pregnant women.
The study group consisted of patients admitted with a diag-nosis of PPROM (24-36 weeks gestation). All patients in thisgroup developed spontaneous rupture of membranes. PPROMwas diagnosed by traditional methods such as vaginal fluiddrainage, vaginal discharge and perineal wetness. Rupture ofmembranes was diagnosed by sterile speculum examinationconfirming fluid leakage from the cervical canal or pooling offluid in the posterior vaginal fornix. All pregnant patients in thisgroup were hospitalized at our clinic and followed-up untildelivery. From admission to delivery patients received prophy-lactic antibiotics (sulbactam-ampiciline 1g 4x1 IV). Steroidtherapy (betamethasone 12 mg 2x1 IM) was used in casesbefore 34 gestational weeks. Patients were restricted to bed rest,
SummaryPurpose: To compare vaginal fluid procalcitonin (PCT) concentrations in cases of preterm premature rupture of membranes
(PPROM) and healthy pregnant women, and to determine whether the PCT concentrations are of value in the diagnosis of PPROMcases and clinical amnionitis. Methods: 50 cases with PPROM and 50 healthy pregnant women were enrolled in the study. In thePPROM group, analysis was conducted on PCT concentrations with reference to serum leucocytosis, serum C-reactive protein leveland urine analysis, as well as to presence/absence of clinical amnionitis. Statistical analyses were carried out by using the statisticalpackages for SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, USA). Results: Procalcitonin levels in the PPROM group were signif-icantly higher than in cases of healthy pregnant women (1.17 vs 0.05 ng/ml; p < 0.001). In the PPROM group PCT concentrationsbetween the patients with and without clinical amnionitis were comparable. Also, a significant correlation was observed between PCTand leucocytosis (r = 0.64; p < 0.001) and C-reactive protein (r = 0.90; p < 0.001). Conclusion: These findings suggest that the valueof vaginal fluid PCT determinations can be useful for diagnostics of PPROM cases suspected of intrauterine infection.
Key words: Premature rupture of membranes; Procalcitonin; C-reactive protein.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

U. Kuyumcuoglu, K. Kangal, A.I. Guzel, Y. Celik 320
and fetal heart monitoring with uterine activity assessment wasperformed twice daily.
The control group consisted of pregnant women (20-37weeks gestation), who were admitted to our clinic for routinecontrol of pregnancy. This group was without complaints,vaginal discharge, or any infection and diagnosis of PPROMhad been ruled out of by traditional methods.
In all patients of the study group, vaginal fluid was aspiratedwith a 5-ml plastic syringe from the cervical canal or the pos-terior vaginal fornix at the first examination. In the controlgroup 5 ml sterile saline solution was administered to the pos-terior fornix and after 1 min aspirate was taken. The fluid spec-imens were collected in polypropylene tubes. For the measure-ment of PCT concentration, immunoluminometric assay wasperformed. Cervical dilatations (1 to 10 cm) and effacements (0to 100%) were noted. In both groups blood samples for whiteblood cell count (WBC) and C-reactive protein (CRP) and urineanalyses for leucocytes were taken. Also in both groups ultra-sound examination was performed for detection of gestationalweek and amnionic fluid index (AFI).
The patient group was evaluated in terms of delivery type,maternal infection and fetal condition and they were also cate-gorized according to clinical amnionitis situations. Fetal tachy-cardia (> 160/m), maternal fever (> 38°C), maternal tachycar-dia (> 100/m without any other explanation) or uterinesensitivity were evaluated as clinical amnionitis.
The mean and standard deviation (SD) were calculated forcontinuous variables. The normality of the variables was ana-lyzed by Kolmogorov-Smirnov test. The chi-square test andStudent’s t-test evaluated associations between the categoricaland continuous variables. Two-sided P values were consideredstatistically significant at p < 0.05. Statistical analyses werecarried out by using the statistical packages for SPSS 12.0 forWindows (SPSS Inc., Chicago, IL, USA).
Results
The demographic and clinical characteristics of groupsare shown in Table 1. There were no significant differ-ences in maternal and gestational age between groups.However cervical dilatation and effacements were signif-icantly higher in the study group than the control group.Also AFI was significantly lower in the study group.
Serum WBC counts (10.97 vs 13.81k/ul; p < 0.001)and serum CRP level (6.22 vs 25.42 mg/l; p = 0.005)were found to be statistically different between the studyand control group, and both of these values were higherin the study group.
Vaginal fluid concentrations of PCT in patients withPPROM were significantly higher than in the controlgroup (1.17 vs 0.05 ng/ml; p < 0.001). Significant corre-lations were observed between PCT levels with CRP (r-0.90, p < 0.001) and WBC (r-0.64; p < 0.001).
Of the study group and control group cases leukocyteswere detected in the urine analysis in 44% and 24%,respectively, and the difference was statistically signifi-cant (p < 0.05).
Study group cases were evaluated for clinical amnioni-tis within themselves and 24% of cases were detected.Detected and non detected clinical amnionitis cases wereevaluated and vaginal fluid PCT concentrations (2.85 vs0.22 ng/L p < 0.001), CRP (56.10 vs 8.16 mg/l p < 0.001)
and WBC count (16.77 vs 12.15 k/l p < 0.001) were sig-nificantly higher in detected cases of clinical amnionitis.The 5 min Apgar score (6.43 vs 5.16 p = 0.009) was sig-nificantly higher in non detected clinical amnionitis casesversus detected cases.
Twenty-eight (56.2%) patients of the study group weredelivered by cesarean section and 21 (43.8%) patients weredelivered vaginally. When delivery type was comparedwith clinical amnionitis, cesarean section rate was signifi-cantly higher in the clinical amnionitis group (p = 0.035).
Discussion
Rupture of the membranes is thought to result from theeffects of physical forces in localized areas of membranesweakened by degradation of structural collagens [10].The pathogenesis of PPROM resulting in preterm birthremains unknown, but many hypotheses have been sug-gested. These factors include maternal infection, geneticpredisposition, mechanical damage, smoking, nutritionaland vitamin deficiencies and plasminogen activation.Intrauterine infection and subsequent inflammation maysynergistically weaken the membranes because of thecombined effects of microbial, host inflammatory cells,and cytokine-regulated protease production [11]. Thefirst goal of this study was to determine whether vaginalfluid PCT levels in PPROM cases and healthy pregnantwomen were different or comparable. It was observedthat PCT levels in PPROM were significantly higher thanin healthy pregnant women, thus adding additional evi-dence to confirm the hypothesis about the infectious eti-ology of PPROM.
The current management of patients with PPROM at agestational age lower than 34 weeks consists of corticos-teroid and antibiotic administration, and expectant man-agement until fetal or maternal signs of infection becomeevident [12]. Optimal expectant management of PPROMrequires early detection of chorioamnionitis. To date, nouniversally sensitive and specific marker for diagnosis ofsubclinical intrauterine infection has been identified.
Table 1. — Demographic and clinical characteristics of thestudy and control groups.
Characteristic Study group Control study p value(n = 50) (n = 50)
Maternal age (years) 27.38 ± 6.02 27.72 ± 6.60 0.60(mean ± SD)
Parity (mean ± SD) 2.16 ± 2.24 3.36 ± 2.79 0.02Gestational age (weeks) 30.40 ± 3.18 29.74 ± 4.04 0.36
(mean ± SD)Cervical dilatation (cm)
(mean ± SD) 25.60 ± 17.39 8.40 ± 5.84 < 0.001Cervical effacements (%) 1.61 ± 1.22 0.80 ± 0.53 < 0.001
(mean ± SD)AFI (cm) 4.86 ± 2.98 12.84 ± 1.73 < 0.001
(mean ± SD)WBC (g/l) 10.97 13.81 < 0.001CRP (mg/l) 6.22 25.42 0.005Procalcitonin (ng/l) 1.17 0.05 < 0.001p � 0.05 is accepted to be statistically significant. CRP: C- reactive protein. AFI:Amiotic fluid index. WBC: White blood cells.

Clinical significance of procalcitonin in cervico-vaginal secretions of women with preterm rupture of membranes 321
Torbé et al. [13] found that increased vaginal fluid PCTlevel is associated with subclinical intraamnionitic infec-tion in PPROM cases; likewise in our study high vaginalfluid PCT levels were detected in clinical amnionitis.Rizzo et al. [14] and Jun et al. [15] demonstrated that themeasurement of interleukin-6 in cervical secretions ofpatients with PPROM is a noninvasive and sensitivemethod to identify the patient at risk for microbial inva-sion of the amniotic cavity, impending preterm delivery,or neonatal complications. Di Naro et al. [12] found thatincreased vaginal fluid C-reactive protein concentrationis associated with intraamniotic infection and funisitisand that there is a significant correlation between amni-otic fluid and vaginal fluid concentrations.
Conclusion
Procalcitonin is a new parameter used in the diagnosisof generalized or systemic infectious diseases. So far, notmuch is known about its use among pregnant women. Inview of the probably infectious etiology of PPROM oneof the purposes of this study was to determine whethervaginal fluid concentrations of PCT immediately afterPPROM might have any value in the diagnosis of caseswith suspected subclinical intrauterine infection.
References[1] McCaul J.F., Rogers L.W., Perry K.G. Jr., Martin R.W., Allbert
J.R., Morrison J.C.: “Premature rupture of membranes at termwith an unfavorable cervix: Comparison of expectant manage-ment, vaginal prostaglandin, and oxytocin induction”. South Med.J., 1997, 80, 1229.
[2] Stringer M., Miesnik S.R., Brown I., Martz A.H., Macones G.:“Nursing care of the patient with preterm premature rupture ofmembranes”. MCN Am. J. Matern. Child Nurs., 2004, 29, 144.
[3] Caughey A.B., Robinson J.N., Norwitz E.R.: “Contemporary diag-nosis and management of preterm premature rupture of mem-branes”. Rev. Obstet. Gynecol., 2008, 1, 11.
[4] Simhan H.N., Canavan T.P.: “Preterm premature rupture of mem-branes: diagnosis, evaluation and management strategies”. BJOG,2005, 112 (suppl. 1), 32.
[5] Rizzo G., Capponi A., Rinaldo D., Tedeschi D., Arudini D.,Romanini C.: “Interleukin-6 concentrations in cervical secretionsidentify microbial invasion of the amniotic cavity in patients withpreterm labor and intact membranes”. Am. J. Obstet. Gynecol.,1996, 175, 812.
[6] Meisner M.: “Pathobiochemistry and clinical use of procalci-tonin”. Clin. Chim. Acta, 2002, 323, 17.
[7] Monneret G., Laroche B., Bienvenu J.: “Procalcitonin is not pro-duced by circulating blood cells”. Infection, 1999, 27, 34.
[8] Torbé A., Czajka R.: “Maternal plasma procalcitonin concentra-tions in patients with preterm labor and intact membranes - pre-diction of preterm delivery and admission-to-delivery interval”. J.Perinat. Med., 2004, 32, 332.
[9] Torbé A., Czajka R.: “Procalcitonin in cervico-vaginal secretion inpregnancies complicated by preterm labor - a preliminary report”.Eur. J. Obstet. Gynecol. Reprod. Biol., 2004, 116, 177.
[10] Maymon E., Romero R., Pacora P., Gervasi M.T., Bianco K.,Ghezzi F., Yoon B.H.: “Evidence for the participation of intersti-tial collagenase (matrix metalloproteinase 1) in preterm prematurerupture of membranes”. Am. J. Obstet. Gynecol., 2000, 183, 914.
[11] Draper D., McGregor J., Hall J. et al.: “Elevated protease activi-ties in human amnion and chorion correlate with preterm prema-ture rupture of membranes”. Am. J. Obstet. Gynecol., 1995, 173,1506.
[12] Di Naro E., Ghezzi F., Raio L., Romano F., Mueller M.D.,McDougall J., Cicnelli E.: “C-reactive protein in vaginal fluid ofpatients with preterm premature rupture of membranes”. ActaObstet. Gynecol. Scand., 2003, 82, 1072.
[13] Torbé A., Czajka R.: “Are vaginal fluid procalcitonin levels usefulfor the prediction of subclinial infection in patients with pretermpremature rupture of membranes?”. J. Obstet. Gynaecol. Res.,2005, 31, 464.
[14] Rizzo G., Capponi A., Vlachopoulou A., Angelini E., Grassi C.,Romanini C.: “Interleukin-6 concentrations in cervical secretionsin the prediction of intrauterine infection in premature rupture ofthe membranes”. Gynecol. Obstet. Invest., 1998, 46, 91.
[15] Jun J.K., Yoon B.H., Romero R., Kim M., Moon J.B., Ki S.H.,Park J.S.: “Interleukin-6 determination in cervical fluid have diag-nostic and prognostic value in preterm premature rupture of mem-branes”. Am. J. Obstet. Gynecol., 2000, 183, 868.
Address reprint requests to:A.I. GUZEL, M.D.Department of Gynecology and ObstetricsDicle University School of Medicine 21280 Diyarbakir (Turkey)e-mail: [email protected]

322
[789/27]
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication November 26, 2009
Placental growth factor: a putative screening test forgestational diabetes mellitus in first trimester
M. Kazandi1, P.S. Hasdemir1, B. Zeybek1, A. Akcay2
1Department of Obstetrics and Gynecology, 2Department of BiochemistryEge University School of Medicine, Bornova, Izmir (Turkey)
[1065/29]
Introduction
Gestational diabetes is defined as the glucose intole-rance of variable severity with onset during pregnancyand characterized by defective insulin secretion or insu-lin resistance. The incidence ranges from 2.2% to 8.8%of all pregnancies and this is the most common medicalcomplication of pregnancy [1, 2]. Several studies havebeen done to find an optimum screening test as the highconcentrations of glucose, especially in the first trimes-ter of pregnancy, may cause several complications suchas miscarriages, congenital defects, macrosomia, hypog-lisemia, prematurity, cardiomyopathy and respiratuardistress. Early diagnosis and optimazing maternal bloodglucose levels will decrease the complication rates andfetomaternal morbidity. The 50 g oral glucose tolarancetest (OGTT) is now widely accepted all over the worldas a screening test between 24-28 weeks of pregnancy;however, a screening test which can be performed in thefirst trimester may be a better alternative.
Diabetic pregnancy causes abnormal placental growthand fetal development. Placental growth is regulated byseveral growth factors including placental growth factor(PLGF), vascular endothelial growth factor (VEGF) andfibroblast growth factor (FGF). PLGF is a member of theVEGF family and the main source of PLGF during preg-nancy is the placental trophoblasts [3]. It is a key mole-cule in angiogenesis and contributes to the regulation ofplacental function.
The aim of this study was to investigate PLGF as ascreening test for gestational diabetes mellitus in the firsttrimester.
Material and Methods
The study was condıcted in accordance wtih the guidelinesand approval given by the Ethical Committee of the Ege Univer-sity Hospital. Sixty-seven 11-14-week pregnant women admit-ted to the outpatient clinic of Ege University Obstetrics andGynecology Department consecutively for first trimester bio-analysis between May 2005 and February 2006 were included inthe study. All selected pregnant women demonstrated intermedi-ate or high-risk factors for diabetes according to the AmericanDiabetes Association [4]. Out of 67 pregnancies three were twinpregnancies, whereas 64 were singleton pregnancies. The studygroup (n = 15) with gestational diabetes were compared with acontrol group (n = 52) with normal oral glucose tolerance tests.OGTTs (50 or 100 g) were performed on all pregnant women atthe 24th week of pregnancy. The first-hour glucose level above140 mg/dl in the 50 g OGTT was accepted as abnormal; 100 g-3-hour OGTT was performed after an overnight fast. Gestationaldiabetes was diagnosed with two or more high glucose levelsduring fasting, first hour, second hour and third hour glucoselevels [5]. Blood samples were collected from the antecubitalveins into heparinized vacutainer tubes. After centrifugation at1000 g for 15 min, serum samples were incubated at –80ºC andanalyzed in the Biochemistry Department laboratory. PLGF wasstudied with the ELISA method (human PGIF, ELIZA kit,Quantikine, R&D systems, USA).
Statistical Analysis
Statistical analysis was performed using the SPSS v. 12.0program. Spearman’s rho test was used for correlation analysisand the Mann-Whitney U test was used to compare groups. Thelevels were expressed in mean ± standard deviation.
ResultsAge of the pregnant women (n = 67) ranged from 22 to
44 years (31 ± 4 years) and mean parity was 0.5 ± 0.7.Maternal levels of PLGF did not correlate with age. Themean birth week and birth weight were 38 ± 1.93 weeks
Summary
Purpose of Investigation: To evaluate placental growth factor as a screening test for gestational diabetes mellitus in the firsttrimester. Methods: Sixty-seven pregnant women who were admitted to the outpatient clinic of Ege University Obstetrics and Gyne-cology Department consecutively for first trimester bioanalysis between May 2005 and February 2006 were included in the study.The cohort of patients underwent 50 g or 100 g oral glucose tolerance tests at the 24th week of pregnancy. Placental growth factorlevels were analyzed by ELISA (human PGIF, ELIZA kit, Quantikine, R&D systems, USA) from the maternal blood collected atthe time of first trimester screening. Results: The study group of 15 patients with gestational diabetes were compared with a controlgroup of 52 pregnant women with normal oral glucose tolerance tests. The level of placental growth factor was mean 35.79 ± 16.79pg/ml in the study group whereas it was mean 45,12 ± 28.07 pg/ml in the control group. There was no significant difference betweeneither group for placental growth factor maternal serum levels. Conclusion: Maternal placental growth factor serum levels are notuseful in predicting gestational diabetes mellitus.
Key words: Placental Growth Factor; Gestational Diabetes; First trimester.

Placental growth factor: a putative screening test for gestational diabetes mellitus in first trimester 323
and 3.296 ± 561 g, respectively. There was also no corre-lation between birth weight and PIGF levels. The level ofplacental growth factor was mean 35.79 ± 16.79 pg/ml inthe study group whereas it was mean 45.12 ± 28.07 pg/mlin the control group. There was no significant differencebetween either group for placental growth factor maternalserum levels (Table 1).
Fifty pregnant women underwent cesarean (C) section(74.5%). The major indication for cesarean sections wasprevious C section (n = 8). Others included macrosomia,fetal distress, placenta previa, prolonged labor, and bre-ech presentation. The most common complication of thenewborns was prolonged jaundice (n = 5, 7.4%). Othercomplications were prematurity, hypoglycemia, cardiacdefects and extremity abnormalities (n = 8, 12%).According to the correlation analysis, there was no relati-onship between the apgar scores of the newborns andmaternal serum PLGF levels.
Mean weight gain of the pregnant women was 13.59 ±5.09 kg and out of the 67, seven had excessive weightgain (� 20 kg). The weight gain of the pregnant womendid not correlate with PLGF levels.
DiscussionThe placenta has a very critical role for both fetal deve-
lopment and maintenance of pregnancy. Development ofthe placenta is regulated by several growth factors such asPLGF, VEGF, FGF and abnormal placentation may resultin a wide range of pregnancy complications.
PLGF is a homodimeric glycoprotein that is involved inthe VEGF family. During pregnancy, it is expressed introphoblasts and contributes to proliferation, migrationand endothelial cell activation [6, 7]. Studies with trisomy21 fetuses showed higher maternal serum levels of PLGF[8, 9], whereas pregnancies complicated with preeclamp-sia and fetal growth restriction showed lower maternalserum levels as these fetuses have defective placentaldevelopment and vascularization [10].
Although there are several studies about PLGF, there islimited data about the relationship between PLGF anddiabetes. It is now known that pregnancies which arecomplicated with gestational or pregestational diabeteshave higher placental weight and this is accomponiedwith a delay of placental maturation [11].
Loukovaara et al. [12] compared the umbilical cordPLGF levels of 62 normal pregnant women, 67 pregnantwomen with type 1 diabetes and 28 pregnant women withgestational diabetes treated with insulin. There was no
statistically significant difference between three groups.Cord serum PLGF levels did not correlate with birthwe-ight as it was the same in our study.
Ong et al. [13] evaluated maternal serum PLGF levels of82 diabetic pregnancies and 400 normal controls. Therewere four groups in the study including pregnant womenwith type 1 diabetes, type 2 diabetes, gestational diabetesand healthy pregnant controls. PLGF levels were signifi-cantly higher in the type 2 and gestational diabetes groupthan the control group. On the other hand, there was no sta-tistically significant difference between the type 1 diabetesgroup and the controls. This was attributed to insulin resis-tance which is the common pathogenetic mechanism ofboth type 2 diabetes and gestational diabetes.
Early diagnosis of gestational diabetes is very impor-tant as maternal and fetal complications may be decrea-sed due to the early optimization of serum glucose con-centration. In this study, we did not find any relationshipbetween maternal serum PLGF levels and gestational dia-betes; however more studies with large patient populati-ons are needed for definitive results.
References[1] Cheung N.W.: “The management of gestational diabetes”. Vasc.
Health Risk Manag., 2009, 5, 153.[2] American Diabetes Association: “Gestational Diabetes Mellitus”.
Diabetes Care, 2002, 25, 594. [3] Koh P.O., Sung J.H., Won C.K., Cho J.H., Moon J.G., Park O.S.,
Kim M.O.: “Streptozotocin induced diabetes decreases placentagrowth factor (PIGF) levels in rat placenta”. J. Vet. Med. Sci.,2007, 69, 877.
[4] American Diabetes Association: “Gestational Diabetes Mellitus”.Diabetes Care, 2003.
[5] Carpenter M.W., Coustan D.R.: “Criteria for screening tests forgestational diabetes”. Am. J. Obstet. Gynecol., 1982, 144, 768.
[6] Shore V.H., Wang T.H., Wang C.L., Torry R.J., Caudle M.R., TorryD.S.: “Vascular endothelial growth factor, placental growth factorand their receptors in isolated human trophoblast”. Placenta,1997, 18, 657.
[7] Zieche M., Maglione D., Ribatti D.: “Placenta growth factor-1 ischemotactic, mitogenic, and angiogenic”. Lab. Invest., 1997, 76, 517.
[8] Spencer K., Liao A.W., Ong C.Y., Geerts L., Nicolaides K.H.:“First trimester maternal serum placenta growth factor (PIGF)con-centrations in pregnancies with fetal trisomy 21 or trisomy 18”.Prenat. Diagn., 2001, 21, 718.
[9] Su Y.N., Hsu J.J., Lee C.N., Cheng W.F., Kung C.C., Hsieh F.J.:“Raised maternal serum placental growth factor concentrationlevel during the second trimester is associated with Down syn-drome”. Prenat. Diagn., 2002, 22, 8.
[10] Helske S., Vuorela P., Carpen O., Hornig C., Weich H., Halmes-maki E.: “Expression of vascular endothelial growth factor recep-tors 1, 2 and 3 in placentas from normal and complicated pregnan-cies”. Mol. Hum. Reprod., 2001, 7, 205.
[11] Lao T.T., Lee C.P., Wong W.M.: “Placental weight to birthweightratio is increased in mild gestational glucose intolerance”. Pla-centa, 1997, 18, 227.
[12] Loukovaara M., Leinonen P., Teramo K., Andersson S.: “Concen-tration of cord serum placenta growth factor in normal and dia-betic pregnancies”. BJOG, 2005, 112, 75.
[13] Ong C.Y., Lao T.T., Spencer K., Nicolaides K.H.: “Maternal serumlevel of placental growth factor in diabetic pregnancies”. J.Reprod. Med., 2004, 49, 477.
Address reprint requests to:M. KAZANDI, M.D.Department of Obstetrics and GynecologyEge University School of MedicineBornova, Izmir (Turkey)e-mail: [email protected]
Table 1. — Patient characteristics and PLGF levels (n = 67)(mean ± SD).
GDM group (n = 15) Control group (n = 52)
Age* 33.30 ± 4.89 29.90 ± 3.81Birth week† 37.47 ± 2.13 38.22 ± 1.85Birth weight† 32.76 ± 500 33.02 ± 581Parity* 0.87 ± 0.83 0.42 ± 0.60PlGF levels† 35.79 ± 16.79 45.12 ± 28.07*Statistically significant difference between both groups (p > 0.05).†Statistically insignificant difference between both groups (p > 0.05).

324
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
[789/27]
Revised manuscript accepted for publication March 13, 2010
Haemophilus parainfluenzae infective endocarditis associatedwith pelvic abscess: an uncommon complication
of endometriosis
T. Miquel-Goulenok1, A. Le Tohic2, J.J Laurichesse1, B. Iung3, C. Leport1, P. Longuet1
1Department of Infectious Diseases, 2Department of Gynaecology, 3Department of CardiologyCHU Bichat, Paris (France)
[1090/30]
Introduction
Common predisposing factors for salpingitis andgynaecologic abscess include sexual behaviour [1],increased age, diabetes and immunocompromised statusdue to HIV infection or renal transplantation.Endometriosis, which is found in 25-40% of women withinfertility and in 2-5% of the general population [2], hasbeen suspected to increase occurrence of gynaecologicabscess [3]. Although Haemophilus influenzae (HI) is acommon respiratory tract pathogen in humans but, rarelyisolated from fallopian tubes, few reports have describedHI salpingitis and tuboovarian abscess [4-7] and only twoHaemophilus parainfluenzae (HPI) genital infectionshave been reported [5, 6]. HI and HPI are also recognisedas rare causative agents ofpathogens implicated in bacte-rial infective endocarditis (IE) [8].
We report an unusual case of Haemophilus parainfluen-zae endocarditis IE associated with a gynaecologicabscess in a patient with endometriosis.
Case Report
A 33-year-old woman, gravida 0, para 0, suffering fromsevere endometriosis (Stage IV) and ovarian cysts was known tohave a heart murmur, never explored. In March 2008, she pre-sented suddenly with a flu-like syndrome and was prescribedibuprofen and paracetamol. Laboratory investigations were nor-mal. Four days later, the patient was still febrile (38.6°C) andcomplained of pelvic pain. Blood samples revealed a throm-bopenia (28 g/l). White blood cell count was 23.0 g/l with a pre-dominance of polymorphonuclear leukocytes and the C-reactiveprotein level was 437 mg/dl. At hospital admission, her temper-ature was 39.1°C, while her blood pressure and pulse rate werenormal. A mitral insufficiency murmur was audible. No sign ofheart failure, palpable spleen or peripheral cutaneous lesions
were observed. Dental examination and radiography were nor-mal. There was localised mild tenderness in the lower abdomi-nal quadrant. Vaginal examination resulted in severe pain.Ultrasound exam revealed a right tuboovarian abscess (62 x 43mm). Abdomino-pelvic computed tomography (CT) showedthat the lesion was non homogeneous, with enhancement aftercontrast administration (56 x 45 mm) and was associated with aperipheric abscess in the Douglas pouch (63 x 54 mm). Sternalpunction confirmed the peripheric thrombopenia. Amoxicillin-clavulanate (1 g x 3 per day), ofloxacine (200 mg x 2 per day)and gentamycin (150 mg per day) were started after bacteriolog-ical samples (blood, urine and vaginal cultures). Twenty-fourhours later, 3/3 blood cultures became positive with small gram-negative rods. Urinalysis was negative. Microbiological identi-fication confirmed a multi sensible HPI. Transthoracic and tran-soesophageal echocardiography were performed and confirmedthe diagnosis of endocarditis, with vegetation on the mitralvalve and a mitral prolapse. Left ventricular function was nor-mal, but mitral regurgitation was evaluated Stage III.Antibiotherapy was switched to amoxicillin (12 g per day) plusgentamycin. Antinuclear factors, rheumatoid factor, comple-ment and antiphospholipid antibodies were negative. Noimmunosuppression or sexually transmitted diseases were diag-nosed (B and C hepatitis, TPHA VDRL and HIV serologieswere negative). Because of persistent abdominal pain,laparoscopy was done ten days after initiation of antibiothera-pyin. Examination of the pelvic cavity revealed the presence ofmoderate adhesions of the ileum, and a right abscess in theDouglas pouch. The ovaries were normal and an abscess haddeveloped on an underlying pseudo-cyst of endometriosis.Drainage of the cavity was performed. Culture and 16S riboso-mal RNA gene sequencing of perioperative sampling were neg-ative, probably because of previous antibiotherapy. Biopsy wasperformed in the Douglas pouch and histological analysisshowed typical lesions of endometriosis, with inflammatoryreaction and altered polymorphonuclear leukocytes. After 24hours, fever disappeared, abdominal pains and inflammatorysyndrome decreased and further outcome was favourable.Control blood cultures were negative. After three weeks ofamoxicillin, results of MIC allowed switching to ceftriaxone 2 ga day IM, for three weeks to simplify the treatment. Control of
Summary
The case of a woman with native mitral valve endocarditis due to Haemophilus parainfluenzae (HPI) associated with a pelvicabscess and endometriosis is reported. Although HPI is an infrequent pathogen involved in endocarditis, association to a gynaeco-logical infection has never been reported. Endometriosis could increase this risk.
Key words: Haemophilus parainfluenzae; Infective endocarditis; Endometriosis.
Case Reports

Haemophilus parainfluenzae infective endocarditis associated with pelvic abscess: an uncommon complication of endometriosis 325
echocardiography showed stability of valvular damage, withpersistence of mitral regurgitation Stage III. There have been nomanifestations of valvular infection during the five followingmonths and mitral valvuloplasty was performed to correct thevalvular defect in September. LHRH analogues were dispensedto treat the endometriosis after this acute infection.
Discussion
This patient had an IE due to HPI (positive blood cul-tures and echocardiographic findings). Haemophilus sppare a rare responsible pathogen of IE (3%) [8]. Darras-Joly et al. reported 42 cases of Haemophilus spp endo-carditis [9]: HPI was the main pathogen (26/42), like inVasquez et al’s study. In this study, the mean age was 27years, 60% of patients had no identifiable predisposingillness [10]. Although surgery is often necessary, HPIendocarditis has a favourable outcomeprognosis [9].
In previous reports, origin of the micro-organism wasunknown in 70-80% of cases and no case of gynaecologicinfection was noted. In our case, a pelvic abscess was pres-ent. The lack of isolation of HPI from this site may beexplained by the fact that samples were performed ten daysafter the onset of antibiotherapy. The role of HPI in genitalinfections has been described. HI is a small gram-negativerod that commonly inhabits the upper respiratory tract. HIbiotypes II and III are found to predominate among strainsfrom the respiratory tract and biotypes II and IV amongstrains from the genital tract. HPI, biotype II, is most fre-quent in both sites [11]. It has rarely been isolated intuboovarian abscesses, salpingitis, endometritis and otherobstetrical infections. In Vasquez et al’s. study [6],Haemophilus spp was isolated from 2.8% of 5,572 genitalspecimens; of whom HPI was detected in 64.5% and HI in29% of cases. Their pathogenic role is evocated when it isisolated as the single pathogen in infections as urethritis inmen or Bartholin’s abscess in women [6]. To explain uro-genital infection with HPI, few hypotheses have been sug-gested: role of orogenital sexual contact or colonization bya reservoir in the colon. Genital infections with bacteremiacaused by Haemophilus spp have been described [7], sug-gesting a possible risk of endocarditis in case of underlyingvalve disease. In our case, the origin of infection was prob-ably gynaecologic.
Since it is of outstanding to describe HPI endocarditisfrom genital infection, it is a hypothesis that endometrio-sis may have favoured this rare complication. Occurrenceof tuboovarian abscess seems to increase in women withendometriosis [12], particularly in women with Stage IIIand IV, at the age between 20 and 29 and those older than40 [3]. It has been suggested that endometriosis could beresponsible for impairment of local immunity (particular-ly cystic wall and ovarian epithelium) and that the pres-ence of old blood in an endometrioma may provide a cul-ture medium for bacteria to grow slowly after transvagi-nal inoculation and facilitate the spread of infection.Thus, infected endometriosis could be a risk factor forendocarditis, like any other infected site (dental, diges-tive...), particularly in case of underlying heart disease.The most probable mechanism is a bacteremia but we can
wonder if migration of cells (like catamenial pneumotho-rax) could be incriminated.
In conclusion, we report an unusual case of HPI infec-tive endocarditis probably related to endometriosis withpelvic abscess. Evolution was favourable with adaptedantibiotherapy and surgery treatment. The patientremained asymptomatic for 15 months. The present casereport suggests that in women with Haemophilus sppendocarditis, it may be of interest to detect pelvic inflam-matory disease or endometriosis if no origin of infection(particularly dental) is identified. Gynaecologic tractinfection is probably an underestimated cause of endo-carditis, particularly in young women. It highlights theimportance of considering the potential role ofendometriosis in these settings. Prospective larger cohortsof patients with endometriosis would be necessary todefine incidence and types of infective complications.Practioners should consider Haemophilus species as apotential pathogen in extra respiratory or oto-rhino-laryn-gologic infections.
References[1] Pastorek J.G.: “Pelvic inflammatory disease and tubo-ovarian
abscess”. Obstet. Gynecol. Clin. North. Am., 1989, 16, 347.[2] Hickman T.N.: “Impact of endometriosis on implantation”. J.
Reprod. Med., 2002, 47, 801.[3] Chen M.J., Yang J.H., Yang Y.S., Ho H.N.: “Increased occurrence
of tubo-ovarian abscesses in women with Stage III and IVendometriosis”. Fertil. Steril., 2004, 82, 498.
[4] Albritton W.L., Hammond G.W., Ronald A.R.: “BacteriemicHaemophilus influenzae genitourinary tract infections in adults”.Arch. Intern. Med., 1978, 138, 1819.
[5] Kragsbjerg P., Nilsson K., Persson L., Tornqvist E., Vikerfors T.:“Deep obstetrical and gynaecological infections caused by non-typable Haemophilus influenzae”. Scand. J. Infect. Dis., 1993, 25,341.
[6] Vazquez F., Andrés M.T., Palacio V., Vazquez S., de Lillo A., FierroJ.F.: “Isolation of Haemophilus influenzae and Haemophilusparainflueanzae in genitourinary infections: a 4-year review”.Enferm. Infec. Microbiol. Clin., 1996, 14, 181.
[7] Carmeci C., Gregg D.: “Haemophilus influenzae salpingitis andsepticemia in an adult”. Obstet. Gynecol., 1997, 89, 863.
[8] Scheld W.M., Sande M.A.: “Endocarditis and intravascular infec-tions”. In: Mandel G.K., Bennett J.E., Dolin R. (eds.). Mandell,Douglas and Bennett’s Principles and Practice of InfectiousDiseases. 4th edition, Vol 1. New York: Churchill Livingstone,1995, 740.
[9] Darras-Joly C., Lortholary O., Mainardi J.L., Etienne J., GuillevinL., Acar J.: “Haemophilus endocarditis: report of 42 cases in adultsand review. Haemophilus Endocarditis Study Group”. Clin. Infect.Dis., 1997, 24, 1087.
[10] Lynn D.J., Kane J.G., Parker R.H.: “Haemophilus para influenzaeand influenzae endocarditis: a review of forty cases”. Med.(Baltimore), 1977, 56, 115.
[11] Sturm A.W.: “Isolation of Haemophilus influenzae andHaemophilus parainfluenazae from genital-tract specimens with aselective culture medium”. J. Med. Microbiol., 1986, 21, 349.
[12] Kubota T., Ishi K., Takeuchi H.: “A study of tubo-ovarian and ovar-ian abscesses, with a focus on cases with endometrioma”. J.Obstet. Gynaecol. Res., 1997, 23, 421.
Address reprint requests to:T.M. GOULENOK, M.D.Department of Infectious DiseasesCHU Bichat Claude BernardAP-HP, 75018 Paris (France)e-mail: [email protected]

326
[789/27]
Revised manuscript accepted for publication September 19, 2009
A rare case of congenital pulmonary lymphangiectasia,hydrothorax and ascites in a male embryo aborted
at 20 weeks of gestation
D. Hassiakos, K. Bakalianou, C. Iavazzo, A. Liapis, C. Dastamani, A. Kondi-Pafiti2nd Department of Obstetrics and Gynecology, Pathology Department, Aretaieion Hospital, University of Athens (Greece)
[1048/29]
Introduction
Congenital pulmonary lymphangiectasia is a rare con-dition, characterized by extensively dilated pulmonarylymphatics in the bronchovascular connective tissuealong the interlobular septa and in the pleura [1, 2]. Thisdisease is usually fatal within a few hours or days of life.Its etiology is heterogenous [3-5]. It may present as partof syndromes such as Noonan, Turner or Down , but mostcases are sporadic [5]. The incidence of congenital pul-monary lymphangiectasia is one in 10,000 gestations,with a 2:1 male/female ratio [1, 2].
Case Report
A 33-year-old primigravida visited our hospital at 20 weeksof an uneventful gestation for a routine check-up. The ultra-sound of the second trimester revealed bilateral pleural effusionespecially in the left thoracic cavity and ascites.
The first semester check-up showed that the patient wasCMV (+), toxoplasma (-), coxsackie (-), rubella (±) and Prader-Willi syndrome (-). No fetal defects were mentioned in the pre-vious ultrasound.
The patient underwent a therapeutic abortion after giving aninformed consent. The aborted embryo was male and weighed381 g; its length from head-foot was 25.5 cm and from head-hips 15.5 cm. The foot sole length was 3.3 cm. The head, tho-racic and abdominal circumference were 19 cm, 16.5 cm, and16 cm, respectively.
On gross examination, extensive abdominal distension wasobserved. The face (ears, nose, mouth) was normal and the eyeswere closed. The extremities were normal and the external gen-italia were male. The thoracic and the peritoneal cavity werefull of pellucid, serous fluid and the viscera were congestive,normal in position and size. The brain weighed 43 g. The brainventricles were full of cerebrospinal fluid and the meningeswere congestive. The thoracic cavity was dilated and full ofserous fluid. The lungs showed extensive, hemorrhagic infiltra-tion especially the left lung. The heart revealed an atrial septal
defect and patent ductus arteriosus, whereas the aorta and thepneumonic artery were normal. The peritoneal cavity was alsodilated and full of serous fluid. The viscera were congestive andfetal weight was within normal limits for the fetal age.
Microscopic examination of the lungs revealed many cysticspaces filled with fluid, lined by endothelium and distributedunder the pleura, in the interlobar spaces and round vessels(Figures 1, 2). Hydrothorax, ascites and visceral congestionwere also present.
The placenta was discoid measuring 10.5 x 10.5 x 3 cm andweighing 208 g with an eccentric outgrowth of the umbilicalcord. The coloboma of the umbilical cord had three vessels. Itsdiameter was 1.2 cm and length 10.5 cm. Furthermore, focal,dispersive, white lesions measuring 0.2 cm were found in theplacenta.
Microscopic examination showed:a) intensive vascular congestion and elevated vascularization
of the chorionic villi;b) dilatation and congestion of the lung vessels;c) old and recent focal placenta infracts;d) lesions of placentitis;e) lesions of chorioamnionitis.
Discussion
Congenital pulmonary lymphangiectasia is a ratherfatal disease. There are three forms of the disorder [3]:
a) isolated congenital pulmonary lymphangiectasia(poor prognosis) [4];
b) congenital pulmonary lymphangiectasia associatedwith pulmonary venous obstruction;
c) congenital pulmonary lymphangiectasia associatedwith a generalized defect in lymphatic development.
Certain genes are implicated in such a pathology e.g.,FOXC2 transcription factor on chromosome 16q24.3,VEGFR3 mutation in the endothelial growth factorreceptor 3, and integrin alpha-9-beta-1 receptor for extra-cellular matrix protein [5].
The pleural effusion is usually chylous and occurs inthe right pleural space (our case occurred in the leftpleural space) [1]. In a retrospective study of eight
SummaryA case of a male embryo aborted at the 20th week of gestation with extensive ascites, hydrothorax, pulmonary lymphangiectasia and
pulmonary hypoplasia is presented together with the pathological findings, the etiology, differential diagnosis, course and therapy ofthis pathologic entity. Also a short review of the literature is discussed.
Key words: Hydrothorax; Pleural effusion; Ascites; Lymphatics.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

A rare case of congenital pulmonary lymphangiectasia, hydrothorax and ascites in a male embryo aborted at 20 weeks of gestation 327
aborted fetuses (7 males, 1 female), the fetuses weighed463.4 g (range 177-681 g) [4]. Our case was a maleembryo weighing 381 g. Six were aborted between 19and 24 weeks of gestation for multiple malformations oranencephaly and two were spontaneously aborted [4].Our case underwent a therapeutic abortion at 20 weeks ofgestation. The main characteristics are the dilatation ofsubpleural and septal lymphatic space and the positiveD2-40 immunostaining of lymphatic endothelium [1].
The differential diagnosis includes chromosomal,cardiac and infectious parameters. The diagnosis is con-firmed by the postnatal lung biopsy. The prognosisdepends on the severity of the symptoms. The infantsusually die due to respiratory distress shortly after birth[6]. A subgroup of children with congenital pulmonarylymphangiectasia – if treated aggressively – may have agood prognosis for long-term survival [7]. Prenatal coun-seling should be proposed to the parents.
References[1] Wilson R.D., Pawel B., Bebbington M., Johnson M., Lim F.Y.,
Stamilio D. et al.: “Congenital pulmonary lymphangiectasissequence: a rare, heterogeneous, and lethal etiology for prenatalpleural effusion”. Prenat. Diagn., 2006, 26, 1058.
[2] Barker P.M., Esther C.R. Jr., Fordham L.A., Mayganden S.J.,Funkhouser W.K.: “Primary pulmonary lymphangiectasia ininfancy and childhood”. Eur. Respir. J., 2004, 24, 413.
[3] Noonan J.A., Walters L.R., Reeves J.T.: “Congenital pulmonarylymphangiectasia”. Am. J. Dis. Child., 1970, 120, 314.
[4] Bouchard S., Di Lorenzo M., Youssef S., Simard P., Lapierre J.G.:“Pulmonary lymphangiectasia revisited”. J. Pediatr. Surg., 2000,35, 796.
[5] Stevenson D.A., Pyscher T.J., Ward R.M., Carey J.C.: “ClinicalReport of familial congenital non immune hydrops, chylothoraxand pulmonary lymphangiectasia”. Am. J. Med. Genet., 2006,140A, 368.
[6] Hirano H., Nishigami T., Okimura A., Nakasho K., Uematsu K.:“Autopsy case of congenital pulmonary lymphangiectasis”. Pathol.Int., 2004, 54, 532.
[7] Chung C.J., Fordham L.A., Barker P., Cooper L.L.: “Children withcongenital pulmonary lymphangiectasia: after infancy”. AJR Am. J.Roentgenol., 1999, 173, 1583.
Address reprint requests to:A. KONDI-PAFITI, M.D.Department PathologyAretaieion Hospital76, Vas. Sofias Ave11528 Athens (Greece)e-mail: [email protected]
Figure 1. — Histological section of fetal lung showing dilatedlymphatic spaces in subpleural and interlobar spaces (hema-toxytin-eosin, x 25).Figure 2. — Histological section of interlobar spaces showingdilated lymphatics (hematoxytin-eosin, x 250).
Fig. 1
Fig. 2

328
[789/27]
Revised manuscript accepted for publication January 14, 2010
Successful pregnancy after radiotherapy with 131Ifor differentiated thyroid cancer.
A case report and review of the literature
I. Grammatikakis, E. Trakakis, N. Evangelinakis, E. Hintipas, G. Salamalekis, D. Kassanos3rd Department of Obstetrics and Gynecology, Medical School of Athens, General University hospital “Attikon” (Greece)
[1038/29]
Introduction
Radioactive iodine (131I) has been used effectively inthe diagnosis and treatment of thyroid diseases. It is most-ly used in differentiated thyroid cancer (DTC) [1, 2],where it has been proven to prevent relapses and treatmetastases. DTC has a female predominance and morethan 50% of cases occur in the reproductive years. Itseems that certain reproductive and hormonal factors thatoccur during pregnancy and during the first years aftergiving birth may predispose to the development of thethyroid cancer. The prognosis for DTC is good [3, 4], andtreatment with 131I prolongs life, even when distantmetastases occur [5, 6]. Since radiation is delivered to thewhole body, including the ovaries, it is a reasonable con-cern as to whether there is a possibility of mutageniceffect on germ cells. The relevance of the mutageniceffects of radiation as assessed by untoward pregnancyoutcomes, such as miscarriages, congenital abnormalitiesand malignancies in offspring, remains to be clarified inhumans. One extensive study of Japanese atomic bombsurvivors and two large studies of patients who had beenexposed to abdominal radiation during childhood andadolescence did not detect any statistically significanteffects of radiation on pregnancy outcome [7-9]. Despitethat, the relevance of the mutagenic effects of radiation onthe fertility and well-being of the offspring is still debat-ed and discussed in cases of high-dose 131I treatment forDTC because large and conclusive data have not yet aris-en. Hence, further research in this field is urgently need-ed so that a significant body of data can be collected. It isinteresting that a recent study reported increased risk of
leukemia in offspring whose fathers were exposed to radi-ation preconceptionally [10].
The radiation dose delivered to the ovary is approxi-mately 0.14 cGy after administration of 37 MBq (1 mCi)1311 in normal subjects [11]. Thyroid cancer patientsreceive diagnostic doses of I131 ranging from 1-5 mCiand therapeutic doses ranging from 30 to 150 mCi ormore. In many cases functioning metastases are in closeproximity to the ovary having as a consequence greaterdoses of radiation delivered to them. Furthermore, manypatients during radiotherapy exhibit hypothyroidism dueto insufficient thyroid hormone replacement therapy. Thiscondition decreases renal iodine clearance, resulting inprolonged gonadal exposure [12].
Case Report
We report the case of a 33-year-old woman who complainedof local pain in the glandular thyroid location. She also com-plained of weight loss during the previous few months. Ultra-sound and scintigraphy examinations revealed a mass of 2.5 cmin the thyroid gland and fine needle aspiration (FNA) was sug-gested. The results of the FNA were suggestive of a differenti-ated papillary carcinoma. Thyroid hormone levels at that timewere as follows: TSH: 2.1 mU/l, T4: 7.3 μg/dl, T3: 110 ng/dl,CEA: 3.5 ng/ml, calcitonin:18 pg.ml.
The patient underwent a chest and abdominal computedtomography (CT) scan and a body scintigram, but neithermetastases nor nodules were found. Also, the capsule of thethyroid gland did not seem infiltrated. According to the TNMclassification it was a T2N0M0 tumor. The woman underwenta total thyreoidectomy and pathological examination confirmedFNA findings and preoperative classification, adding that it wasa grade 3 papillary carcinoma.
The case was discussed in the oncologic council and it wasconcluded that thyroid hormone replacement therapy should be
SummaryBackground: Radioactive iodine has been used effectively in the diagnosis and treatment of thyroid diseases. Since radiation is deliv-
ered to the whole body, including the ovaries, there is reasonable concern as to whether there is a possibility of mutagenic effect ongerm cells. Case Report: A 33-year-old woman with a differentiated papillary carcinoma. (T2N0M0), underwent radiotherapy threeweeks after surgery and one year afterwards she became pregnant. At the 38th week of gestation she delivered vaginally a healthy femaleneonate weighing 3100 g. The child at the age of five years is healthy with no signs of malignancy or other disease. Discussion: Washoutof 131I of the whole body takes place in a few days. Nevertheless, most guidelines recommend avoiding pregnancy for four to six oreven 12 months after RAI treatment or scanning. As reported in our case a normal uncomplicated pregnancy can follow an operativeand complementary treatment of thyroid cancer.
Key words: Radiotherapy; Differentiated thyroid cancer; Pregnancy.
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010

Successful pregnancy after radiotherapy with 131I for differentiated thyroid cancer. A case report and review of the literature 329
prescribed and that surgery should be followed by percutaneousradiotherapy.
The woman underwent the radiotherapy three weeks after thesurgery. The dose was 80 mCi (= 2960 MBq) of 131I. After-wards thyroid hormone replacement therapy was started. TSHvalues were evaluated to confirm the expected TSH suppres-sion, since TSH seems to reflect the growth of tumor cells ofthe thyroid. TSH values were lower than normal range.
Three months after surgery the following parameters werechecked: lung parenchyma (chest X-ray), thyroid hormonelevels, TRH test, erythrocyte count and TKE, and there were noindications of metastases. Six and 12 months after surgery thischeckup was repeated without any remarkable findings.
One year after finishing her therapy the patient became preg-nant. She had a normal and uncomplicated pregnancy and at the38th week of gestation she delivered vaginally a healthy femaleneonate weighing 3100 g. The apgar score was 9 at the 1st and10 at the 5th minute. During the pregnancy the woman did notundergo any radioactive examination. After delivery follow-upof the above-named parameters was continued every sixmonths. The child at the age of five years is healthy with nosigns of malignancy or other disease associated with radioactivetherapy.
Discussion
The most important limitation in any study trying toclarify the effect of radiotherapy with 131I on pregnancyoutcome is to eliminate all other cofactors that couldinfluence mother or the infant. Age at conception, socioe-conomic class, alcohol intake, and smoking, as well asadequacy and fluctuation of thyroid hormone replace-ment and radiation dose to the ovaries are biases difficultto overcome. The physical half-life of 131I is 8.04 days[13], and the median effective half-life is at least 14 hours[14], with substantial variations. Consequently, washoutof 131I of the whole body takes place in a few days.Nevertheless, most guidelines recommend avoidingpregnancy for four [15] to six [16] or even 12 monthsafter radioactive iodine (RAI) treatment or scanning [17,18]. Despite instructions to patients unexpected pregnan-cies may occur. If radiotherapy followed conception withan interval of less than ten weeks it is essential to esti-mate the dose to the fetal thyroid and whole body andcounsel the couple regarding their options. The tendencyto adopt the recommendation for avoiding pregnancy upto one year after radiotherapy is based on two facts. Thefirst one is that a greater miscarriage rate [18] and someuntoward pregnancy outcomes such as birth defects [19],Edward’s syndrome [20], and aplastic anemia [20] havebeen described to occur in pregnancies conceived withinthe first post-RAI year. The second one is that during thatannual interval complete remission of the disease can beconfirmed and the thyroid hormonal status controlled[18]. Therapeutic abortion has been a quite commonapproach for accidental RAI administration in the firsttrimester of pregnancy [21]. Knowledge of the timing offetal thyroid development and the potential effect on thefetal thyroid and whole body irradiation on a developingembryo can guide management. The fetal thyroid begins
to develop and differentiate into follicles at ten weeks ofgestation. Consequently, if maternal RAI is administeredafter the 10th week of gestation it is quite possible thatfetal hypothyroidism will appear [22]. To avoid suchinadvertent events, patients should be strongly counseledto avoid pregnancy before radiotherapy, while determin-ing the date of the woman’s last menstrual period andcontraception practice, and providing pregnancy testingwithin 48 hours before RAI administration are good pro-cedural safeguards [23]. Since, DTC is considered amalignancy with a very good prognosis and slow growthrate, guidelines recommend delaying thyroid surgery andany RAI investigations until after delivery [15]. Someauthors support the concept that hCG binds to the TSHreceptor, stimulating the growth of benign and malignantthyroid tissue. Endogenous estrogen binding activity inneoplastic thyroid cells is described by some researchers.Diethylstilbestrol also was shown to have a relationshipto thyroid neoplasia in C57BL/6 mice. Pregnancy termi-nation or thyroidectomy during pregnancy is considereda rare approach, and mostly employed when diagnosis ismade in the first trimester. The most commonly adoptedapproach is to keep the pregnancy, deferring thyroidecto-my to either the second trimester or even until after deliv-ery. The most important prognostic factors seem to bematernal age at the time of diagnosis. Tumor size, grad-ing and other pathologic findings are of less importance.Thyroid cancer during pregnancy is reported to be asso-ciated with increased fetal loss, especially if more exten-sive surgery, including neck lymph node dissection isperformed. Although most of the studies have failed toreveal any statistically significant effect of radiation suchas 131I on fertility [24-26], ovarian [27] or testicularfunction [28], childhood cancers [29], congenital malfor-mations [30], chromosomal abnormalities [31], or, somestudies have demonstrated a greater frequency of chro-mosomal aberrations in the peripheral lymphocytes ofpatients treated with 131I [10, 32] or suggested an asso-ciation between ionizing radiation of the father and anincreased risk of congenital abnormalities [33] andleukemia [10]. Women previously irradiated for Wilms’tumor or other cancers with abdominal doses of 20 to 30Gy are reported to have an increased rate of miscarriages,but this increase was attributed mostly to somatic dam-age to the abdominopelvic organs [34]. Recently contro-versial reports have been published showing an apparentincrease in the number of leukemias in young people,whose fathers worked at the Sellafield nuclear reprocess-ing plant in Northwest England and were occupationallyexposed to radiation [10], raising new concerns aboutthese effects at low doses. It is quite interesting that themost profound reproductive effect of the Chernobyl acci-dent was a sharp increase in elective terminations ofpregnancy in Europe, which most of the time was unjus-tified after negligible exposure [32]. Therefore, theimportance of clarifying the effect of 131I on pregnancyoutcome is important not only for the management ofpatients with DTC, but also for assessment of the impactof ionizing radiation on human health in general.

I. Grammatikakis, E. Trakakis, N. Evangelinakis, E. Hintipas, G. Salamalekis, D. Kassanos 330
Conclusion
Although the number of children born to mothersexposed to radioiodine is relatively small, there is no rea-son for patients exposed to radioiodine to avoid pregnan-cy. Radioiodine treatment of differentiated thyroid cancerdoes not affect female fertility nor is it associated withany genetic risk to the offspring. A washout period of oneyear is a reasonable approach. During pregnancy, thyroidfunction needs to be closely monitored and given theseprecautions RAI is a safe treatment method in youngwomen.
As reported in our case a normal uncomplicated preg-nancy can follow an operative and complementary treat-ment of thyroid cancer. Non differentiated thyroid carcino-mas, as in our report, can be treated by total thyroidecto-my followed by percutaneous radiotherapy, and the doseof thyroid hormone replacement therapy has to be veryhigh in order to develop TSH suppression, since TSHseems to have a growth effect on the thyroid tumor cells.Our report is in accordance with the recent medical litera-ture, stating that a one-year interval between radiotherapywith 131I for DTC and pregnancy is a safe option.
References [1] Maxon H.R., Smith H.S.: “Radioiodine-131 in the diagnosis and
treatment of metastatic well-differentiated thyroid cancer”.Endocrinol. Metab. Clin. North Am., 1990, 19, 685.
[2] Mazaferri E.L., Jhiang S.M.: “Long-term impact of surgical andmedical therapy on papillary and follicular thyroid cancer”. Am. J.Med., 1994, 97, 418.
[3] Beenken S., Guillamondegui O., Shallenberger R., Knapp C.,Ritter D., Goepfert H.: “Prognostic factors in patients dying ofwell differentiated thyroid cancer”. Arch. Otolaryngol. Head NeckSurg., 1989, 115, 326.
[4] Tubiana M., Schlumberger M., Rougier P., Laplanche A.,Benhamou E., Gardet P. et al.: “Long-term results and prognosticfactors in patients with differentiated thyroid carcinoma”. Cancer,1985, 55, 794.
[5] DeGroot L.J., Kaplan E.L., McCormick M., Straus F.H.: “Naturalhistory, treatment and course of papillary thyroid carcinoma”. J.Clin. Endocrinol. Metab., 1990, 71, 414.
[6] Mazzaferri E.L., Kloos R.T.: “Current approaches to primary ther-apy for papillary and follicular thyroid cancer”. J. Clin.Endocrinol. Metab., 2001, 96, 1447.
[7] Schull W.J., Otake M., Neel J.V.: “Genetic effects of atomicbombs: A re-appraisal”. Science, 1981, 213, 1220.
[8] Hawkins M.M., Draper G.J., Smith R.A.: “Cancer among 1348offspring of survivors of childhood cancer”. Int. J. Cancer, 1989,43, 975.
[9] Hawkins M.M.: “Is there evidence of a therapy related increase ingerm cell mutation among childhood cancer survivors?”. J. Natl.Cancer Inst., 1991, 83, 1643.
[10] Gardner M.J., Snee M.P.. Hall A.J., Powell C.A., Downes S.,Terrell J.D.: “Results of a case control study of leukemia and lym-phoma among young people near Sellafield nuclear plant in WestCumbria”. Br. Med. J., 1990, 300, 423.
[11] MIRD. MIRD primer for absorbed dose calculations. Reston,VA:Society of Nuclear Medicine, 1988.
[12] Izembart M., Chavaudra J., Aubert B., Vallee G.: “Retrospectiveevaluation of the dose received by the ovary after radioactiveiodine therapy for thyroid cancer”. Eur. J. Nuci. Med., 1992, 19,243.
[13] Harbert J.C.: “Radioiodine therapy of differentiated thyroid carci-noma”. In: Harbert J.C., Eckelman W.C., Neumann R. (eds.).Nuclear medicine: Diagnosis and therapy. New York, Thieme,1996, 975.
[14] North D.L., Shearer D.R., Hennessey J.V., Donovan G.L.:“Effective half-life of 131I in thyroid cancer patients”. HealthPhys., 2001, 813, 325.
[15] British Thyroid Association and Royal College of Physicians ofLondon. Guidelines for the management of thyroid cancer inadults. London, UK: British Thyroid Association and RoyalCollege of Physicians of London, 2002.
[16] American Association of Clinical Endocrinologists and AmericanCollege of Endocrinology. AACE/AAES medical/surgical guide-lines for clinical practice: Management of thyroid carcinoma.Endocr. Pract., 2001, 73, 202.
[17] Casara D., Rubello D., Saladini G., Piotto A., Peliozzo M.R.,Girelli M.E., Busnardo B.: “Pregnancy after high therapeutic dosesof iodine-131 in differentiated thyroid cancer: Potential risks andrecommendations”. Eur. J. Nucl. Med., 1993, 203, 192.
[18] Schlumberger M., De Vathaire F., Ceccarelli C., Delisle M.J.,Francese C., Couette J.E. et al.: “Exposure to radioactive iodine-131 for scintigraphy or therapy does not preclude pregnancy inthyroid cancer patients”. J. Nucl. Med., 1996, 374, 606.
[19] Smith M.B., Xue H., Takahashi H., Cangir A., Andrassy R.J.:“Iodine 131 thyroid ablation in female children and adolescents:long-term risk of infertility and birth defects”. Ann. Surg. Oncol.,1994, 12, 128.
[20] Ayala C., Navarro E., Rodriguez J.R., Silva H., Venegas E.,Astorga R.: “Conception after iodine-131 therapy for differentiat-ed thyroid cancer”. Thyroid, 1998, 811, 1009.
[21] Stoffer S.S., Hamburger J.I.: “Inadvertent 131I therapy for hyper-thyroidism in the first trimester of pregnancy”. J. Nucl. Med.,1976, 1702, 146.
[22] Berg G.E., Nystrom E.H., Jacobsson L., Lindberg S., LindstedtR.G., Mattsson S. et al.: “Radioiodine treatment of hyperthy-roidism in a pregnant women”. J. Nucl. Med., 1998, 392, 357.
[23] Gorman C.A.: “Radioiodine and pregnancy”. Thyroid., 1999, 97,721.
[24] Sarkar S.D., Beirwaltes W.H., Gill S.P., Cowiley B.J.: “Subsequentfertility and birth histories of children and adolescents treated with131I for thyroid cancer”. J. Nucl. Med., 1976, 17, 460.
[25] Edmonds C.J., Smith T.: “The long-term hazards of the treatmentof thyroid cancer with radioiodine”. Br. J. Radiol., 1986, 59, 45.
[26] Balan K.K., Critchley M.: “Outcome of pregnancy following treat-ment of well differentiated thyroid cancer with 131I”. BJOG,1992, 99, 1021.
[27] Vini L., Hyer S., Al-Saadi A., Pratt B., Harmer C.: “Prognosis forfertility and ovarian function after treatment with radioiodine forthyroid cancer”. Postgrad. Med. J., 2002, 78, 92.
[28] Hyers S., Vini L., O’Connell M., Pratt B., Harmer C.: “Testiculardose and fertility in men following 131I therapy for thyroid can-cer”. Clin. Endocrinol., 2002, 56, 755.
[29] Hjalmars U., Kulldorf M., Gustafsson G.: “Risk of acute childhoodleukaemia in Sweden after the Chernobyl reactor accident”. Br.Med. J., 1994, 309, 154.
[30] Czeizel A.: “Hungarian surveillance of germinal mutations: Lackof detectable increase in indicator conditions caused by germinalmutations following the Chernobyl accident”. Hum. Genet., 1989,82, 359.
[31] Harjuletho-Mervaala T., Salnone R., Aro T., Saxen H.: “The acci-dent at Chernobyl and trisomy 21 in Finland”. Mutat. Res., 1992,275, 81.
[32] Bertollini R., Di Lallo D., Mastroicovo P., Perucci C.A.:“Reduction of births in Italy after the Chernobyl accident”. Scand.J. Work Environ Health, 1990, 16, 96.
[33] Sever L.E., Gilbert E.S., Hessol N.A., McIntyre J.M.: “A case-con-trol study of congenital malformations and occupational exposureto low-level ionizing radiation”. Epidemiol 1988, 127, 226 .
[34] Smith R.A., Hawkins M.M.: “Pregnancies after childhood cancer”.Br. J. Obstet. Gynaecol., 1989, 96, 378.
Address reprint requests to:E. TRAKAKIS, M.D.Maikina 41Zografos, Athens (Greece)Zip code: 15772e-mail: [email protected]

331
Clin. Exp. Obst. & Gyn. - ISSN: 0390-6663XXXVII, n. 4, 2010
Revised manuscript accepted for publication November 26, 2009
Sequential methotrexate treatment with and estrogen and progestin in a retained adhesive placenta
T. Mizuno1, H. Takagi2, K. Matsunami2, A. Imai2
1Department of Obstetrics and Gynecology, Gifu University School of Medicine, Yanagido, Gifu2Department of Obstetrics and Gynecology, Matsunami general Hospital, Kasamatsu, Gifu (Japan)
[1067/29]
Introduction
The incidence of placental adhesive disorders has dras-tically increased in recent years, due to the increasingcesarean rates in most countries [1]. Though hysterec-tomy is the definite and recommended treatment, conser-vative management may be considered in patients desir-ing future pregnancy [2, 3]. We present a successful caseof conservative treatment with methotrexate and estro-gen-progestin.
Case Report
A 33-year-old woman, gravida 1, para 1, at 38 weeks and oneday of pregnancy had a cesarean delivery because of previoushistory of myomectomy. On ultrasound a finding of placentalretention was noted, thus curettage was attempted two weekspostpartum but moderate fresh bleeding was induced. She wasreferred to us for further management. On admission, since theuterus became firmly contracted and the patient was hemody-namically stable, she wanted to conserve her uterus. Magneticresonance imaging showed a retained placental mass with roughborders. The mass, which measured 75 x 70 x 65 mm, waslodged on the posterior wall with minimum myometrial inva-sion (Figure 1a). Contrast-enhanced computed tomographydepicted the multiple vessels within the intrauterine mass andthe absence of deep myometrial invasion. Neither solid compo-nents nor calcifications could be identified (Figure 1b). Herhuman chorionic gonadotropin (HCG) level was 78.0 mIU/ml,and a general examination revealed no other abnormality. Thepatient received four doses of 50 mg of methotrexate intramus-
culary every other day, alternating with four doses of 15 mg offolic acid. She was carefully monitored for vaginal bleeding andsepsis. After four cycles (one cycle per 2 weeks), color Dopplerultrasound scan showed that the placenta had shrunk in size anddecreased in its vascurality, indicative of necrotic tissue. SerumHCG became negative. An attempt to evacuate the necrotictissue along with withdrawal bleeding was successful after threecourses of sequential conjugated estrogen (0.25mg)-progestin(5 mg) therapy. Subsequent ultrasonographic examination doc-umented an empty uterine cavity.
Discussion
Methotrexate affects placental tissue by decreasing vas-cularity leading to necrosis [1]. The sensitivity of chori-onic tissue to methotrexate is well documented by its usein gestational trophoblastic neoplasia, abnormal preg-nancy, and medical termination of pregnancy [1]. Thereare some reports of successful use of methotrexate incases of placenta accreta or placenta increta [2, 3]. Thisreport adds another and justifies its use in selected cases.The patient in this report received estrogen and progestinderivatives to effectively protect the endometrium, induceregular withdrawal bleeding and hasten expellingretained necrotic placenta. Combined sequential estrogenreplacement regimens with progestin given very rarelyfail to protect the endometrium, rather than surgical cur-retage [4]. The use of estrogen and progestogen and ofmethotrexate in combination may be simple and poten-tially effective for placenta accreta and placenta increta.Though experience in the management of placental adhe-sive disorders with this protocol is limited and should bestrictly supervised, it should be taken into considerationif the patient desires future fertility.
Summary
Background: Hysterectomy is the definite and recommended treatment of a retained adhesive placenta. Case: A 33-year-oldwoman at 38 weeks plus one day of gestation had a cesarean delivery due to previous history of myomectomy. On ultrasound pla-cental retention was noted thus curettage was attempted two weeks postpartum but it induced moderate fresh bleeding. A contrast-enhanced computed tomography scan depicted the multiple vessels within the intrauterine mass and the absence of deep myome-trial invasion. The patient received four doses of 50 mg of methotrexate intramuscularly every other day, alternating with four dosesof 15 mg of folic acid. An attempt to evacuate the necrotic tissue along with withdrawal bleeding was successful after three coursesof sequential conjugated estrogen (0.25 mg)-progestin (5 mg) therapy. Conclusion: The use of estrogen and progestogen togetherwith methotrexate in combination may be simple and potentially effective for placenta accreta and placenta increta.
Key words: Placental adhesive disorders; Methotrexate; Placenta increta; Placenta accreta.

T. Mizuno, H. Takagi, K. Matsunami, A. Imai 332
References[1] Bretelle F., Courbière B., Mazouni C., Agostini A., Cravello L.,
Boubli L. et al.: “Management of placenta accreta: Morbidity andoutcome”. Eur. J. Obstet. Gynecol. Reprod. Biol., 2007, 133, 34.
[2] Crespo R., Lapresta M., Madani B.: “Conservative treatment ofplacenta increta with methotrexate”. Int. J. Gynaecol. Obstet.,2005, 91, 162.
[3] Mussalli G., Shah J., Berck D., Elimian A., Tejani N., Manning F.:“Placenta accreta and methotrexate therapy: Three case reports”.J. Perinatol., 2000, 20, 331.
[4] Burch D., Bieshuvel E., Smith S., Fox H.: “Can endometrial pro-tection be inferred from the bleeding pattern on combined cyclichormone replacement therapy”. Maturitas, 2000, 34, 155.
Address reprint requests to:A. IMAI, M.D.Institute of Endocrine-Related CancerMatsunami General HospitalKasamatsu, 501-6062 (Japan)e-mail: [email protected]
Figure 1. — Retained adhesive placenta. a; sagittal T2-weightedMRI showing a placental mass embedded in the uterine poste-rior wall with minimum myometrial involvement (arrow), inaccord with placenta accreta. b; horizontal contrast-enhancedCT showing the highlighted area of increased vascularity thatdoes not cross the uterine wall (arrow).
a) b)

Executive Board:
PIERLUIGI BENEDETTI PANICI (Italy)
CARLOS F. DE OLIVEIRA (Portugal)
GIUSEPPE DE PALO (Italy)
SANTIAGO DEXEUS (Spain)
WILLIAM DUNLOP (UK)
STELIOS FOTIOU (Greece)
GERALD GITSCH (Austria)
A. PETER M. HEINTZ (Netherlands)
MICHAEL HOECKEL (Germany)
JAN JACOBS (UK)
JACQUES LANSAC (France)
TIZIANO MAGGINO (Italy)
HARALD MEDEN (Germany)
JOSEPH MONSONEGO (France)
LASZLÓ PÁLFALVI (Hungary)
SERGIO PECORELLI (Italy)
DENIS QUELLEU (France)
STELIO RAKAR (Slovenia)
PIERO SISMONDI (Italy)CLAES TROPÉ (Norway)LÁSZLÓ UNGÁR (Hungary)ANDRÉ VAN ASSCHE (Belgium)RAIMUND WINTER (Austria)
International Advisory BoardChairman: Antonio Onnis (Italy)
HUGH ALLEN (Canada)CURT W. BURGER (Netherlands)ALBERTO COSTA (Italy)ANDRÉ GORINS (France)NEVILLE F. HACKER (Australia)MARIA MARCHETTI (Italy)STELIOS P. MICHALAS (Greece)MARIA TERESA OSORIO (Portugal)ULF ULMSTEN (Sweden)JAN B. VERMORKEN (Belgium)GEORGE D. WILBANKS (USA)JAN ZIELINSKI (Poland)
www.cme.hu
Administrative Office:1301 Budapest, P.O. Box 46 - Hungary
Fax (36 1) 4290318 - E-mail: [email protected]
EAGC
EUROPEAN ACADEMYOF GYNAECOLOGICAL CANCER, EAGC
Chairman: Péter B´osze (Hungary)
All questions concerning the Accademy may be sent to:
PETER BOSZE, M.D. - P.O. Box 46 - Budapest 1301 (Hungary)Phone: +36 1 4290317 - Fax: +36 1 2752172 - E-mail: [email protected]

Founding EditorA. Onnis
Montréal (CND)
Editors-in-ChiefM. Marchetti J.H. CheckMontréal (CND) Camden, NJ (USA)
Assistant EditorJ. Wilson
San Diego - CA (USA)
Editorial BoardAllen H.H., Montréal (Canada)Axt-Fliedner R., Lübeck (Germany)Basta A., Krakow (Poland)Bender H.J., Dusseldorf (Germany)Bhattacharya N., Calcutta (India)Bonilla Musoles F., Valencia (Spain)Charkviani T., Tbilisi (Georgia)Dexeus S., Barcelona (Spain)Di Paola G., Buenos Aires (Argentina)Eskes T.K.A.B., Nijmegen (The Netherlands)Franchi M., Verona (Italy)Friedrich M., Krefeld (Germany)Gomel V., Vancouver (Canada)Gorins A., Paris (France)Grella P.V., Padua (Italy)Holub Z., Kladno (Czech Republic)Jordan J.A., Birmingham, England (UK)Kaplan B., Petach Tikva (Israel)Kralj B., Ljubljana (Slovenia)Markowska J., Poznan (Poland)Marth C., Innsbruck (Austria)Meden-Vrtovec H., Ljubljana (Slovenia)Ohara N., Kobe (Japan)Papadopoulos N., Alexandroupolis (Greece)Rakar S., Ljubljana (Slovenia)Sciarra J.J., Chicago, IL (USA)Stelmachow J., Warsaw (Poland)Varras M.N., Athens (Greece)Vîrtej P., Bucharest (Romania)Winter R., Graz (Austria)
CLINICAL AND EXPERIMENTALOBSTETRICS & GYNECOLOGY
an International Journalwww.irog.net
The Journal publishes original research and clinical contri butions, prefe rably
briefly reported, in the fields of Gynaecology, Obstetrics, Foetal Medi cine, Gynaeco -
logical Endocrinology, Fertility and Sterility, Menopause, Uro-gynae cology, Ultra -
sound, Sexually transmitted diseases and related subjects, from all over the world.
Founded in 1974 (ISSN 0390 6663) Issued quarterly in English, the Journal is
covered by INDEX MEDICUS, MEDLINE (PUBMED), EMBASE/Excerpta Medica,
INDEX COPERNICUS.
We hope to have you as a subscriber of our Journal which is improving its
scientific and clinical interdisciplinary activity and value and which is approaching its
XXXIII year of life.
You can subscribe or renew your subscription by sending us the following form.
Yes, start my subscription.
CLINICAL AND EXPERIMENTAL OBSTETRICSAND GYNECOLOGY
an International Journal
SUBSCRIPTION ORDER CARD 2011
ISSN 0390-6663. • Published threemonthly. All subscriptions are entered on a calendar-yearbasis. Individual rate is not applicable if payment is made through an Institution.Subscriptions ARE ENTERED WITH PREPAYMENT ONLY.
Please enter my subscription at the rate I’ve checked:
Institutional: 280 $US Individual: 170 $US
For Air Mail add 20 $US Receipt add 10.00 $US
Please send me a free sample copy
I’am paying by: (U.S. CURRENCY ONLY)
Check (enclosed)
Credit Card: American Express Visa Diners
N°
Signature Date
Exp. Date
I.R.O.G. CANADA, Inc. - 4900 Côte St-Luc - Apt # 212Montréal, Qué. H3W 2H3 (Canada)
Tel. +514-4893242 - Fax +514-4854513 - E-mail: [email protected] - www.irog.net
�
Issues are to be mailed to:
Mastercard
I.R.O.G. CANADA, Inc. - 4900 Côte St-Luc - Apt # 212Montréal, Qué. H3W 2H3 (Canada)
Tel. +514-4893242 - Fax +514-4854513 - E-mail: [email protected] - www.irog.net
Edited by:A. ONNIS
an International Journal
ISSN: 0390-6663
ISSN: 0390-6663
Published three monthly
Pubblicità Experimental con cedola
Bank BANK OF NOVA SCOTIA TRANSIT #90001 Tour Scotia, Montreal, Quebec, CanadaTel.: 514-499-5432 - Fax: 514-499-4701

EDITORIAL ARTICLESA practical approach to the prevention of miscarriage: Part 2 - active immunotherapy - J.H. Check . . . . . . .Misoprostol for second trimester abortion in women with prior uterine incisions - M. Varras, Ch. Akrivis . . . . .
ORIGINAL ARTICLESReproductive Biology SectionIncreasing the dosage of progesterone (P) supplemention from the mid-luteal phase in women not attaining a mid-lutealhomogeneous hyperechogenic (HH) pattern with sonography improves pregnancy rates (PRS) following frozen embryotransfer (ET) - J.H. Check, C. Dietterich, R. Cohen, J.K. Choe, J. Amui, D. Brasile . . . . . . . . . . .Successful pregnancies following embryo transfer despite very thin late proliferative endometrium - E. Dix, J.H. CheckFertilization by intracytoplasmic sperm injection with sperm with subnormal morphology using strict criteria results inlower live delivered pregnancy rates following frozen embryo transfer rather than eggs fertilized conventionally - J.H. Check, E. Dix, A. Bollendorf, D. Check . . . . . . . . . . . . . . . . . . . . .
General SectionEndometriosis: a possible cause of right shoulder pain - A.A. Seoud, M.M. Saleh, A.H. Yassin . . . . . . . .Troponin I and homocysteine levels in mild and severe preeclampsia - A. Atis, Y. Aydin, E. Basol, N. Göker . . . . .Preliminary results of objective assessment of mammographic percent density - G. Iatrakis, S. Zervoudis, P. Malakassis, I. Navrozoglou, F. Pechlivani, P. Peitsidis, P. Economides, D. Polyzos . . . . . . . . . . . . . .Correlations of fetal-maternal outcomes and first trimester 3-D placental volume/3-D power Doppler calculations - N. Bozkurt, A. Basgül Yigiter, H. Gokaslan, Z.N. Kavak . . . . . . . . . . . . . . . . . .Previous cesarean section increases the risk for breech presentation at term pregnancy - I. Kalogiannidis, N. Masouridou,T. Dagklis, S. Masoura, M. Goutzioulis, Y. Prapas, N. Prapas . . . . . . . . . . . . . . . . .The effect of amniocentesis on preterm delivery rate in women with uterine myoma - S. Buyukkurt, A. Yuksel, G. Seydaoglu,R. Has, O. Kadayifci . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal diagnoses of cytomegalovirus (CMV), rubella, toxoplasmosis, varicella, parvovirus, herpes simplex and syphilis.The Lagos programme experience - G.O. Ajayi, S.A. Omilabu . . . . . . . . . . . . . . . . .The relationship between cardiac adaptation to uteroplacental Doppler flow and perinatal outcome in pregnant women withdiabetes - H.A. Parlakgumus, T. Durukan . . . . . . . . . . . . . . . . . . . . . .Do maternity hospital practices support Greek mothers’ decision to breastfeed? - M. Daglas, V. Petoussi, G. Dionysiou, I. Athanassakis . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Effects of selective and non-selective cyclooxygenase (COX) inhibitors on postoperative adhesion formation in a rat uterinehorn model - T. Guvenal, O. Yanar, Y. Timuroglu, M. Cetin, A. Cetin . . . . . . . . . . . . . . .Dinoprostone vaginal insert versus intravenous oxytocin to reduce postpartum blood loss following vaginal or cesareandelivery - E. Ozalp, H.M. Tanir, T. Sener . . . . . . . . . . . . . . . . . . . . . .Psychological factors of hyperemesis gravidarum by using the SCL-90-R questionnaire - Z.M. Pirimoglu, K. Guzelmeric,B. Alpay, O. Balcik, O. Unal, M.C. Turan . . . . . . . . . . . . . . . . . . . . . .
CASE REPORTSSpontaneous uterine rupture in a nulligravida female presenting with unexplained recurrent hematometra - M. Gowda, L.Garcia, E. Maxwell, R. Malik, L. Gulyaeva, M.C. Tsai . . . . . . . . . . . . . . . . . . .Emergent intrauterine resuscitation in a fetus with transient congenital anemia - case report - N. Demir, M.T. Canda, O. SezerChondrosarcoma in the left hemipelvis imitating a pelvic ovarian mass in pregnancy: a case report - G. Somoye, S. Havenga D-dimer levels as a predicting factor for DIC following single twin death: a case report and review of the literature - A.Daniilidis, C. Sardeli, T. Tantanasis, K. Dinas, M. Mavromichali, J. Tzafettas . . . . . . . . . . . . .Heterotopic pregnancy: case report - E. Sturlese, G. Retto, V. Palmara, A. Tripodi, M. Tripodi, M. Sorace, R. De Dominici,A. Retto . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Idiopathic infantile arterial calcification: prenatal diagnosis and postnatal presentation - A. Cansu, A. Ahmetoglu, M. Mutlu, S. Guven, M.A. Osmanagaoglu . . . . . . . . . . . . . . . . . . . . . .
5
10
1315
17
1921
24
26
29
33
37
39
43
49
53
56
606365
67
69
73
CLINICAL AND EXPERIMENTALOBSTETRICS & GYNECOLOGY
Editors-in-Chief: A. Onnis - Montréal (CND), J.H. Check - Canden, NJ (USA)
General index - Volume XXXVII, 2010No. 1, January-February-March

No. 2, April-May-June
EDITORIAL ARTICLESA practical approach to the prevention of miscarriage: part 3 – passive immunotherapy - J.H. Check . . . . . .Advantages of using a lower vs higher dosage of gonadotropins for follicular maturation including cycles of in vitro fertil-ization-embryo transfer - J.H. Check . . . . . . . . . . . . . . . . . . . . . . .
REVIEW ARTICLEThe slow levonorgestrel-releasing intrauterine system (LNG-IUS) 20 mcg/day: a literature review - N. Salakos, A.Koumousidis, C. Iavazzo, G. Paltoglou, K. Bakalianou, O. Gregoriou . . . . . . . . . . . . . . .
ORIGINAL ARTICLESReproductive Biology SectionA novel method to assess the effect of uterine senescence by comparing pregnancy outcome in younger donors vs olderrecipients who are sharing a common pool of oocytes - J.H. Check, B. Katsoff, T. Jamison, J.K. Choe, D. Brasile, J. AmuiCryopreservation of blastocysts using a modification of a simplified freezing protocol with a one step removal ofcryoprotectant successfully used previously to freeze 2 pronuclear or multi-cell embryos - D. Summers-Chase, J.H. Check,D. Horwath, W. Yuan, K. Swenson, M. Press . . . . . . . . . . . . . . . . . . . . .Serum retinol-binding protein-4 levels in polycystic ovary syndrome patients undergoing controlled ovarianhyperstimulation for in-vitro fertilization cycle - R. Orvieto, V. Shuhat, G. Liberty, R. Homburg, E.Y. Anteby, R. Nahum,J. Rabinson, S. Meltcer . . . . . . . . . . . . . . . . . . . . . . . . . . .A comparison of pregnancy rates following fresh and frozen embryo transfer according to the use of leuprolide acetate vsganirelix vs cetrorelix - J.H. Check, C. Wilson, J.K. Choe, J. Amui, B. Katsoff . . . . . . . . . . . .The effect of endometriosis on pregnancy outcome following in vitro fertilization-embryo transfer (IVF-ET) in women withdecreased egg reserve - J.H. Check, J.R. Liss, J.W. Krotec, J.K. Choe, D. Brasile . . . . . . . . . . . .Association of the change in serum estradiol (E2) levels from the day of to the day after human chorionic gonadotropin(hCG) injection and pregnancy outcome following in vitro fertilization-embryo transfer (IVF-ET) in less than averageresponders - J.H Check, J.K. Choe, J. Amui, D. Brasile . . . . . . . . . . . . . . . . . .
General SectionEffects of tamoxifen on tissue nitrite/nitrate levels and plasma lipid peroxidation in female rats - M. Gharehbagni,F. Sendag, F. Akercan, B. Zeybek, E. Sezer, M.C. Terek, N. Karadadas . . . . . . . . . . . . . .Successful treatment of a female with chronic pseudo-intestinal obstruction with sympathomimetic amines and thyroidhormone replacement - J.H. Check, R. Cohen . . . . . . . . . . . . . . . . . . . . .Emergency obstetric hysterectomy at two tertiary centers: a clinical analysis of 11 years experience - M. Varras, Ch. Akrivis, Ch. Plis, G. Tsoukalos . . . . . . . . . . . . . . . . . . . . . . . .Comparision of reproductive outcome of the women with hypogonadotropic hypogonadism and tubal factor infertility - G. Yildirim, C. Ficicioglu, R. Attar, O. Akcin, N. Tecellioglu . . . . . . . . . . . . . . . . .Effect of long-time administration of tibolone on vaginal cytology of castrated rats - H.N. Henriques, A.C. Bergmann deCarvalho, J.A.S. Pantaleão, M.A. Guzmán-Silva . . . . . . . . . . . . . . . . . . . .Vaginal fluid pH, cervicovaginitis and cervical length in pregnancy - F. Sendag, M. Kazandi, F. Akercan, A.C. Kazandi, N. Karadadas, S. Sagol . . . . . . . . . . . . . . . . . . . . . . . . . . .Perineal ultrasound evaluation of urethral mobility after the TVT-O procedure - L. Di Pietto, C. Scaffa, A. Lambiase, M. Torella, C. Sciorio, E. Dato, A. Nocerino, M.L. Di Petrillo, R. Fusco, M. Rotondi, E.M. Messalli, N. ColacurciIs placebo as effective as estrogen regimens on vasomotor symptoms in women with surgical menopause? - H. Hassa, H.M.Tanir, T. Oge . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tubal ectopic pregnancy in the north of Jordan: presentation and management - B. Obeidat, F. Zayed, Z. Amarin, N. Obeidat,M.F. El-Jallad . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Umbilical cord prolapse in the southeast region of Turkey: evaluation of 79 cases - M. Erdemoglu, A. Kale, U. Kuyumcuoglu,N. Akdeniz, A.I. Güzel . . . . . . . . . . . . . . . . . . . . . . . . . . .Adolescent pregnancies and obstetric outcomes in Southeast Turkey: data from two regional centers - D.C. Arıkan, M. Kaplanoglu, H. Kıran, A. Özer, A. Coskun, E. Turgut . . . . . . . . . . . . . . . . . .Pregnancy-related acute renal failure in the southeast region of Turkey: analysis of 75 cases - M. Erdemoglu, U. Kuyumcuoglu, A. Kale, N. Akdeniz . . . . . . . . . . . . . . . . . . . . . . .An analysis of hysteroscopy experience over a seven-year period - E. Ozturk, M.G. Ugur, O. Balat, I. Kutlar, E. Dikensoy,B. Cebesoy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Is insulin-dependent diabetes and obesity a predisposition for endometrial and pancreatic carcinoma? - M. Gojnic, V. Dugalic, M. Brankovic, I. Stojanovic, M. Acimovic, B. Vasiljevic . . . . . . . . . . . . . . .
CASE REPORTSPeripartum cardiomyopathy and Klippel-Trenaunay syndrome - G. Carta, V. De Lellis, M. Di Nicola, D. KaliakoudasNovel therapeutic strategy for uterine arteriovenous fistulas: case report - R. Kizaki, J. Fujimoto, E. Sato, T. TamayaBook Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
81
84
89
97
99
100
105
108
110
112
115
117
120
123
127
131
135
138
141
144
148
150
152
155158161
336 Contents - Volume XXXVII, 2010

Contents - Volume XXXVII, 2010 337
No. 3, July-August-September
EDITORIAL ARTICLES
Antisperm antibodies and human reproduction - J.H. Check . . . . . . . . . . . . . . . . .
Recurrent aneuploidy - fact or fiction - R. Cohen, J.H. Check . . . . . . . . . . . . . . . . .
ORIGINAL ARTICLES
Reproductive Biology Section
Evidence that high serum progesterone (P) levels on day of human chorionic gonadotropin (hCG) injection have no adverseeffect on the embryo itself as determined by pregnancy outcome following embryo transfer using donated eggs - J.H. Check,C. Wilson, J.K. Choe, J. Amui, D. Brasile . . . . . . . . . . . . . . . . . . . . . .
Effect of the length of time that donated embryos are frozen on pregnancy outcome - C. Wilson, J.H. Check, D. Summers-Chase, J.K. Choe, J. Amui, D. Brasile . . . . . . . . . . . . . . . . . . . . . . .
Effect of fertilization by intracytoplasmic sperm injection versus conventional insemination on embryo cleavage rates - J.H.Check, A. Bollendorf, E. Dix, D. Katsoff . . . . . . . . . . . . . . . . . . . . . .
Length of time of embryo storage does not negatively influence pregnancy rates after thawing and transfer - J.H. Check,D. Summers-Chase, W. Yuan, K. Swenson, D. Horwath . . . . . . . . . . . . . . . . . .
Pretreatment of sperm with low hypo-osmotic swelling tests with chymotrypsin prior to intrauterine insemination (IUI) andavoidance of unprotectected intercourse results in pregnancy rates comparable to IUI for other male factor problems -G. Citrino, J.H. Check, A. Diantonio, A. Bollendorf, D. Katsoff . . . . . . . . . . . . . . . .
General Section
Evaluation of the feasibility of a new method for performing chorion villus sampling - S. Buyukkurt, G. Seydaoglu, C. Demir, F.T. Ozgunen, C. Evruke, A.B. Guze, U.K. Gulec, O. Kadayifci . . . . . . . . . . . . .
Expression of matrix metalloproteinase-9 (MMP-9) in human midpregnancy amniotic fluid and risk of preterm labor - A. Di Ferdinando, F. Patacchiola, M.G. Perilli, G. Amicosante, G. Carta . . . . . . . . . . . . . .
Diabetes supersedes dobutamine stress echocardiography in predicting cardiac events in female patients - H. Isma’eel, W. Shamseddeen, M. El Khoury, A. Dimassi, A. Nasrallah, M.S. Arnaout . . . . . . . . . . . . . .
What kind of care and support do infertile women undergoing fertility treatment in Greece expect? A questionnaire survey -K. Lykeridou, K. Gourounti, A. Sarantaki, Z. Roupa, G. Iatrakis, S. Zervoudis, G. Vaslamatzis . . . . . . . .
Comparison of bolus remifentanil-propofol versus bolus fentanyl-propofol for dilatation and sharp curettage - M. Ogurlu, M. Küçük, F. Bilgin, A. Sizlan, Ö. Yanarate, S. Eksert, E. Karasahin, E. Kurt . . . . . . . . . . . . .
Factors affecting maternal and perinatal outcomes in HELLP syndrome: evaluation of 126 cases - M. Erdemoglu, U. Kuyumcuoglu, A. Kale, N. Akdeniz . . . . . . . . . . . . . . . . . . . . . . .
Evaluation of serum levels of interleukin-10, interleukin-11 and leukemia inhibitory factor in differentiation of eutopic andtubal ectopic pregnancies - A.C. Iyibozkurt, I. Kalelioglu, S. Gursoy, A. Corbacioglu, N. Gurelpolat, G.E. Karahan, H. Saygili, E. Bengisu . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis of uterine rupture cases in Agri: a five-year experience - M. Kara, E. Töz, E. Yilmaz, T. Öge, I·. Avcı, I·. Eminli,S. Sentürk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pregnancy and adnexal torsion: analysis of 20 cases - M. Erdemoglu, U. Kuyumcuoglu, A. Kale . . . . . . .
CASE REPORTS
Intrauterine fetal demise due to streptococcal toxic shock syndrome: a case report - T. Ishiguro, H. Matsushita, T. Yanase,T. Kurabayashi, S. Yoshida, Y. Iinuma . . . . . . . . . . . . . . . . . . . . . . .
A novel highly effective therapy for severe vasomotor symptoms in an estrogen deficient woman - case report - J.H. Check,R. Cohen, D. Check . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Anencephalic conjoined twins with mirror-image cleft lip and palate - R. Deveer, Y. Engin-Ustun, I. Kale, A. Aktulay, N. Danisman, L. Mollamahmutoglu . . . . . . . . . . . . . . . . . . . . . . . .
Ovarian torsion; early diagnosis by MRI to prevent irreversible damage - K. Hiei, H. Takagi, K. Matsunami, A. Imai
Idiopathic edema, a condition associated with pelvic pain and other symptoms in women, as a remedial cause of chroniccold induced urticaria - J.H. Check, R. Cohen, D. Check . . . . . . . . . . . . . . . . . .
Huge endometriosis presenting like an ovarian tumor: CT appearance - H. Yerli, N. Askar, O. Zekioglu, Z. Baglan, N. Elmas
Case report: sacral parasitic twins - M. Kara, E. Yılmaz, I·. Eminli, E. Töz, I·. Avc, T. Öge, E. Cigerciogulları . . . .
Book Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
169
175
179
181
183
185
187
190
193
197
201
209
213
217
221
224
226
229
231
233
235
237
240
242

338 Contents - Volume XXXVII, 2010
No. 4, October, November, December
EDITORIAL ARTICLESThe multiple uses of ethinyl estradiol for treating infertility - J.H. Check . . . . . . . . . . . . . .A practical approach to the prevention of miscarriage: Part 4 - role of infection - J.H. Check . . . . . . . .
REVIEW ARTICLEAcute intermittent porphyria in pregnancy: A common misdiagnosis - A. Farfaras, F. Zagouri, G. Zografos, A.Kostopoulou, T.N. Sergentanis, S. Antoniou . . . . . . . . . . . . . . . . . . . . .
ORIGINAL ARTICLESReproductive Biology SectionPregnancy following calcium ionophore oocyte activation in an oligozoospermia patient with repeated failure offertilization after ICSI - S. Sugaya . . . . . . . . . . . . . . . . . . . . . . . .
Artificial oocyte activation with calcium ionophore allowed fertilization and pregnancy in a couple with long-termunexplained infertility where the female partner had diminished EGG reserve and failure to fertilize oocytes despiteintracytoplasmic sperm injection - J.H. Check, D. Summers-Chase, R. Cohen, D. Brasile . . . . . . . . .
General SectionImmediate and perioperative outcomes of polypropylene mesh in pelvic floor repair in a predominantly obese population -T.O. Adedipe, S.J. Vine . . . . . . . . . . . . . . . . . . . . . . . . . . .
Relation between Doppler findings and perinatal outcomes in fetuses with intrauterine growth restriction - M. Kazandi, C. Guven, F. Akercan, B. Zeybek, T. Cirpan, M. Ergenoglu, O. Yeniel, A. Akdemir, S. Ozsener . . . . . . . . .
Impact of the medicalization of labor on mode of delivery - U. Indraccolo, S. Calabrese, R. Di Iorio, L. Corosu, E. Marinoni, S.R. Indraccolo . . . . . . . . . . . . . . . . . . . . . . . . .
Maximizing the benefits of screening mammography for women 40-49 years old - K. Bastardis-Zakas, G. Iatrakis, I. Navrozoglou, P. Peitsidis, N. Salakos, P. Malakassis, S. Zervoudis . . . . . . . . . . . . . . .
Multidisciplinary approach during menopausal transition and postmenopause in Brazilian women - I.C.E. Sorpreso,L.H.L. Vieira, M.A. Haidar, M.G. Nunes, E.C. Baracat, J.M. Soares Júnior . . . . . . . . . . . . .
Reproductive outcomes after hysteroscopic metroplasty for uterine septum - F. Sendag, T. Mermer, S. Yucebilgın, K.Oztekin, O. Bilgin . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Fertility sparing in young women with ovarian tumors - F. Ghaemmaghami, M. Karimi Zarchi, A. Naseri, A.S. Mousavi,M. Modarres Gilani, F. Ramezanzadeh, E. Rezaiof . . . . . . . . . . . . . . . . . . . .
Laparoscopic sacral colpopexy for uterine prolapse with prolene mesh - L. Hong, X. Xu, L. Chen, Q. Fu . . . . .
Development of secondary ovarian lesions after hysterectomy without oophorectomy versus unilateral oophorectomy forbenign conditions: A retrospective analysis of patients during a nine-year period of observation - A. Baloglu, I. Bezircioglu,B. Cetinkaya, L. Karcı, M. Bicer . . . . . . . . . . . . . . . . . . . . . . . . .
Unwanted pregnancy and induced abortion among young women 16-22 years old in Greece: a retrospective study of therisk factors - N. Salakos, A. Koumousidis, K. Bakalianou, G. Paltoglou, Th. Kalampokas, C. Iavazzo . . . . . .
Conservative and surgical treatment of abnormal placentation: Report of five cases and review of the literature - M. Kazandi
Abuse Assessment Screen (AAS) questionnaire: the Greek validation - E. Antoniou, E. Ioannidi-Kapolou, M. Daglas, V. Vivilaki, D. Karamitros, V. Dafermos, G. Iatrakis . . . . . . . . . . . . . . . . . . .
Twin pregnancy after in vitro fertilization in a woman with a unicornuate uterus - S. Sugaya . . . . . . . . .
Clinical significance of procalcitonin in cervico-vaginal secretions of women with preterm rupture of membranes - U. Kuyumcuoglu, K. Kangal, A.I. Guzel, Y. Celik . . . . . . . . . . . . . . . . . . . .
Placental growth factor: a putative screening test for gestational diabetes mellitus in first trimester - M. Kazandi, P.S. Hasdemir, B. Zeybek, A. Akcay . . . . . . . . . . . . . . . . . . . . . . .
CASE REPORTSHaemophilus parainfluenzae infective endocarditis associated with pelvic abscess: an uncommon complication ofendometriosis - T. Miquel-Goulenok, A. Le Tohic, J.J Laurichesse, B. Iung, C. Leport, P. Longuet . . . . . . .A rare case of congenital pulmonary lymphangiectasia, hydrothorax and ascites in a male embryo aborted at 20 weeks ofgestation - D. Hassiakos, K. Bakalianou, C. Iavazzo, A. Liapis, C. Dastamani, A. Kondi-Pafiti . . . . . . . .Successful pregnancy after radiotherapy with 131I for differentiated thyroid cancer. A case report and review of theliterature - I. Grammatikakis, E. Trakakis, N. Evangelinakis, E. Hintipas, G. Salamalekis, D. Kassanos . . . . . .Sequential methotrexate treatment with and estrogen and progestin in a retained adhesive placenta - T. Mizuno, H. Takagi,K. Matsunami, A. Imai . . . . . . . . . . . . . . . . . . . . . . . . . . .Contents index XXXVII, 2010 . . . . . . . . . . . . . . . . . . . . . . . . .Authors index XXXVII, 2010 . . . . . . . . . . . . . . . . . . . . . . . . .
249252
256
261
263
266
269
273
278
283
287
290
295
299
303
310
313
317
319
322
324
326
328
331335339

Acimovic M., 152 Adedipe T.O., 266 Ahmetoglu A., 73 Ajayi G.O., 37Akcay A., 322Akcin O., 120 Akdemir A., 269 Akdeniz N., 141, 148, 213Akercan F., 112, 127, 269Akrivis Ch., 10, 117Aktulay A., 231 Alpay B., 56 Amarin Z., 138 Amicosante G., 193 Amui J., 13, 97, 105, 110, 179, 181 Anteby E.Y., 100 Antoniou E., 313 Antoniou S., 256Arıkan D.C., 144Arnaout M.S., 197Askar N., 237 Athanassakis I., 43Atis A., 21Attar R., 120 Avc I
·., 240
Avcı I·., 221
Aydin Y., 21
Baglan Z., 237 Bakalianou K., 89, 303, 326 Balat O., 150Balcik O., 56 Baloglu A., 299 Baracat E.C., 283 Basgül Yigiter A., 26Basol E., 21Bastardis-Zakas K., 278 Bengisu E., 217Bergmann de Carvalho A.C., 123 Bezircioglu I., 299 Bicer M., 299Bilgin F., 209 Bilgin O., 287Bollendorf A., 17, 183, 187Bozkurt N., 26Brankovic M., 152 Brasile D., 13, 97, 108, 110, 179,
181, 263Buyukkurt S., 33, 190
Calabrese S., 273 Canda M.T., 63 Cansu A., 73 Carta G., 155, 193 Cebesoy B., 150Celik Y., 319Cetin A., 49Cetin M., 49Cetinkaya B., 299 Check D., 17, 229, 235Check J.H., 5, 13, 15, 17, 81, 84,
97, 99, 105, 108, 110, 115, 169,175, 179, 181, 183, 185, 187,229, 235, 249, 252, 263
Chen L., 295 Choe J.K., 13, 97, 105, 108, 110,
179, 181
Cigerciogulları E., 240Cirpan T., 269 Citrino G., 187 Cohen R., 13, 115, 175, 229, 235,
263Colacurci N., 131Corbacioglu A., 217 Corosu L., 273 Coskun A., 144
Dafermos V., 313 Dagklis T., 29 Daglas M., 43, 313 Daniilidis A., 67 Danisman N., 231 Dastamani C., 326 Dato E., 131De Dominici R., 69 De Lellis V., 155 Demir C., 190 Demir N., 63Deveer R., 231 Di Ferdinando A., 193 Di Iorio R., 273 Di Nicola M., 155 Di Petrillo M.L., 131 Di Pietto L., 131 Diantonio A., 187 Dietterich C., 13Dikensoy E., 150Dimassi A., 197 Dinas K., 67 Dionysiou G., 43Dix E., 15, 17, 183Dugalic V., 152 Durukan T., 39
Economides P., 24Eksert S., 209 El Khoury M., 197 El-Jallad M.F., 138Elmas N., 237Eminli I
·., 221, 240
Engin-Ustun Y., 231 Erdemoglu M., 141, 148, 213, 224Erdenoglu M., 269 Evangelinakis N., 328 Evruke C., 190
Farfaras A., 256 Ficicioglu C., 120 Fu Q., 295Fujimoto J., 158 Fusco R., 131
Garcia L., 60 Ghaemmaghami F., 290 Gharehbagni M., 112Gojnic M., 152Gokaslan H., 26Göker N., 21Gourounti K., 201 Goutzioulis M., 29 Gowda M., 60 Grammatikakis I., 328Gregoriou O., 89Gulec U.K., 190
Gulyaeva L., 60 Gurelpolat N., 217 Gursoy S., 217 Guven C., 269 Guven S., 73 Guvenal T., 49Guze A.B., 190 Güzel A.I., 141, 319Guzelmeric K., 56 Guzmán-Silva M.A., 123
Haidar M.A., 283 Has R., 33Hasdemir P.S., 322 Hassa H., 135Hassiakos D., 326 Havenga S., 65Henriques H.N., 123 Hiei K., 233 Hintipas E., 328 Homburg R., 100 Hong L., 295 Horwath D., 99, 185
Iatrakis G., 24, 201, 278, 313Iavazzo C., 89, 303, 326Iinuma Y., 226Imai A., 233, 331Indraccolo S.R., 273Indraccolo U., 273 Ioannidi-Kapolou E., 313 Ishiguro T., 226 Isma’eel H., 197 Iung B., 324 Iyibozkurt A.C., 217
Jamison T., 97
Kadayifci O., 33, 190Kalampokas Th., 303 Kale A., 141, 148, 213, 224 Kale I., 231 Kalelioglu I., 217Kaliakoudas D., 155Kalogiannidis I., 29 Kangal K., 319 Kaplanoglu M., 144 Kara M., 221, 240 Karadadas N., 112, 127Karahan G.E., 217 Karamitros D., 313 Karasahin E., 209 Karcı L., 299 Karimi Zarchi M., 290 Kassanos D., 328Katsoff B., 97, 105Katsoff D., 183, 187Kavak Z.N., 26Kazandi A.C., 127 Kazandi M., 127, 269, 310, 322Kıran H., 144 Kizaki R., 158 Kondi-Pafiti A., 326Kostopoulou A., 256 Koumousidis A., 89, 303 Krotec J.W., 108 Küçük M., 209
Kurabayashi T., 226 Kurt E., 209Kutlar I., 150Kuyumcuoglu U., 141, 148, 213,
224, 319
Lambiase A., 131 Laurichesse J.J., 324 Le Tohic A., 324 Leport C., 324 Liapis A., 326 Liberty G., 100 Liss J.R., 108 Longuet P., 324Lykeridou K., 201
Malakassis P., 24, 278Malik R., 60 Marinoni E., 273 Masoura S., 29 Masouridou N., 29 Matsunami K., 233, 331 Matsushita H., 226 Mavromichali M., 67 Maxwell E., 60 Meltcer S., 100Mermer T., 287 Messalli E.M., 131 Miquel-Goulenok T., 324 Mizuno T., 331 Modarres Gilani M., 290 Mollamahmutoglu L., 231Mousavi A.S., 290 Mutlu M., 73
Nahum R., 100 Naseri A., 290 Nasrallah A., 197 Navrozoglou I., 24, 278Nocerino A., 131Nunes M.G., 283
Obeidat B., 138 Obeidat N., 138 Ogurlu M., 209 Öge T., 135, 221, 240Omilabu S.A., 37Orvieto R., 100 Osmanagaoglu M.A., 73Ozalp E., 53 Özer A., 144Ozgunen F.T., 190 Ozsener S., 269Oztekin K., 287 Ozturk E., 150
Palmara V., 69 Paltoglou G., 89, 303 Pantaleão J.A.S., 123Parlakgumus H.A., 39Patacchiola F., 193 Pechlivani F., 24Peitsidis P., 24, 278Perilli M.G., 193 Petoussi V., 43Pirimoglu Z.M., 56Plis Ch., 117
339
Index of Authors in alphabetical order

Polyzos D., 24Prapas N., 29Prapas Y., 29 Press M., 99
Rabinson J., 100 Ramezanzadeh F., 290 Retto A., 69Retto G., 69 Rezaiof E., 290Rotondi M., 131 Roupa Z., 201
Sentürk S., 221Sagol S., 127Salakos N., 89, 278, 303 Salamalekis G., 328 Saleh M.M., 19Sarantaki A., 201 Sardeli C., 67 Sato E., 158 Saygili H., 217 Scaffa C., 131 Sciorio C., 131
Sendag F., 112, 127, 287 Sener T., 53Seoud A.A., 19Sergentanis T.N., 256 Seydaoglu G., 33, 190 Sezer E., 112 Sezer O., 63Shamseddeen W., 197 Shuhat V., 100 Sizlan A., 209 Soares Júnior J.M., 283Somoye G., 65 Sorace M., 69 Sorpreso I.C.E., 283Stojanovic I., 152 Sturlese E., 69 Sugaya S., 261, 317Summers-Chase D., 99, 181, 185,
263 Swenson K., 99, 185
Takagi H., 233, 331 Tamaya T., 158Tanir H.M., 53, 135
Tantanasis T., 67 Tecellioglu N., 120Terek M.C., 112 Timuroglu Y., 49Torella M., 131 Töz E., 221, 240 Trakakis E., 328 Tripodi A., 69 Tripodi M., 69 Tsai M.C., 60Tsoukalos G., 117Turan M.C., 56Turgut E., 144Tzafettas J., 67
Ugur M.G., 150Unal O., 56
Varras M., 10, 117Vasiljevic B., 152Vaslamatzis G., 201Vieira L.H.L., 283 Vine S.J, 266Vivilaki V., 313
Wilson C., 105, 179, 181
Xu X., 295
Yanar O., 49Yanarate Ö., 209 Yanase T., 226 Yassin A.H., 19Yeniel O., 269 Yerli H., 237 Yildirim G., 120 Yilmaz E., 221, 240 Yoshida S., 226 Yuan W., 99, 185 Yucebilgın S., 287 Yuksel A., 33
Zagouri F., 256 Zayed F., 138Zekioglu O., 237 Zervoudis S., 24, 201, 278Zeybek B., 112, 269, 322 Zografos G., 256
340





























