Embed Size (px)
Citation preview

A study of the effects of training in
independent living skills on the quality of
life of people with intellectual disabilities
living independently.
Thesis submitted for the degree ofMSc. In Human Resource Development/Human Resource
Managementat the University of Leicester
byBarry Spearman
March 2012
Abstract
The concept of Quality of Life has been used in the past to assess the effectiveness of service delivery and supports to people with disabilities. Quality of Life in the case of people without disabilities was measured in terms of economic and social indicators which included such things as material possessions and social supports,in fact all the items which would be associated with independent livingand self determination. Quality of Life for people with disabilities living independently is now gaining in importance, as is the recognition that appropriate training must be provided to make independent living viable. This is particularly true in the case of people with Intellectual disabilities.
The effect of this training on ten adults with Intellectual Disability who had recently moved to independent living was the subject of this study. The study was carried out in a city in Ireland, which has not been named in order to protect the anonymity of the participants. The aim of the study was to determine whether or not training in daily living skills improved the Quality of Life of a group of people with Intellectual Disabilities who had recently moved to independent living.
A purposive non random sample of participants was used due to the fact that the numbers in the category to be studied were very small. This small number also prevented the results from being generalisable to a wider population
A Quantitative Methodology to gather the data was employed using a questionnaire format. The Quality of Life questionnaire was based on Cummins Personal Well Being Index-Intellectual Disability (2005) and the training questionnaire was modelled on this same format.
The data from the PWI-ID was compared to the data obtained in this study and it was seen that there was comparability between the Irish and Australian results. The results obtained from the data showed that the training programmes did bring Quality of Life gains to those who participated in the study. Of particular note was the high value placedon Social Skills training and also how personal safety was of major concern for participants.
i
AcknowledgementsI would like to thank my family for their support during this undertaking. It would not have been possiblewithout their patience and assistance. I am also grateful for the advice and assistance of my Supervisor, Dr. Sarah Earle whose insight and suggestions proved invaluable to me. My thanks also to my employerswho would prefer to remain nameless, and finally my sincere thanks to the people who participated in this study and without whose co-operation it would not have been possible.
Table of contents PageChapter 1 Introduction Historical context………………………………………………………………….1 The effect of economics…………………………………………………………...2
Chapter 2 Aims of the Present Study and Hypotheses: Research Participants
Chapter 3 Literature Review on Quality of Life.
Introduction……………………………………………………………………….4
ii
From the Medical Model to the Social Model of
Care…………………………....5
Historical origins of the concept of Quality of
Life……………………………….7
The Modern Origins of Quality of
Life……………………………………………7
Normalisation and Community
Integration………………………………………..8
Towards Defining Quality of Life…………………………………………………9
Measuring Quality of Life……………………………………………………….. 10
The subjective v. objective measurement
debate…………………………………14
The Domains of Quality of Life…………………………………………………..15
Criticisms of Cummins……………………………………………………………17
Summary…………………………………………………………………………..18
Chapter 4
Literature Review on Training Introduction………………………………………………………………………..18 Modern trends in education and training for people
with Intellectual Disability…18
The pros and cons of
Mainstreaming……………………………………………...18
The evolution of a training model for people with
Intellectual Disabilities………20
Learning Styles and people with Intellectual
Disabilities…………………………21
iii

The Importance of Social Skills
Training…………………………………………23
Effective Training Strategies for training people with
Intellectual Disability……..24
Social Skills v. Social Problem Solving
Skills……………………………………28
The illusion of independence……………………………………………………...29
Literacy and Numeracy Training………………………………………………….30
Practical skills required for independent
living…………………………………...31
Conclusion………………………………………………………………………...33
Summary…………………………………………………………………………..36
Chapter 5 Methodology
Introduction…………………………………………………………………………36
Hypothesis…………………………………………………………………………..37
Literature Review……………………………………………………………….......38
Research Philosophy………………………………………………………………..39
Methodology………………………………………………………………………..40
Sampling……………………………………………………………………………40
Limitations of Sample Size…………………………………………………………41
Ethics……………………………………………………………………………….42
Permission……………………………………………………………………….....42
Informed Consent………………………………………………………………......42
Negotiating participation…………………………………………………………...42
Co-operation………………………………………………………………………...42
iv
Credibility…………………………………………………………………………...43
Legality …………………………………………………………………………......43
Context of the Research…………………………………………………………......43
Bias and Acquiescence……………………………………………………………...43
Structured Interview - Personal Well-being Index-
Intellectual Disability (PWI-ID).44
Historical Development of the Personal Well-Being
Index (IWB, 2006)…………..44
The Personal Well-Being Index (Cummins & Lau, 2005)
………………………….44
The Personal Well-being Index - Intellectual
Disability…………………………….45
Measuring Quality of Life using the PWI-
ID……………………………………….46
Using the PWI-ID in preference to any other measuring
tool………………………46
Summary…………………………………………………………………………….47
Chapter 6Data Interpretation…………………………………………………………………..48
Discussion…………………………………………………………………………….54
Summary and Recommendations…………………………………………………..56
v
Bibliography………………………………………………………………………………………58
Appendix 1. Participant Consent Letter……………………………………………….76
Appendix 2. Informed Consent Letter…………………………………………………78
Appendix 3. Information Sheet for Next of
Kin……………………………………….79
Appendix 4. Easy Read Likert Scale…………………………………………………...80
Appendix 5. Quality of Life and Training
Questions…………………………………..81
Appendix 6. Excel Statistics…………………………………………………………...82
vi
Chapter 1
IntroductionHistorical Context
Historically, people with Intellectual Disability had been cared for in
Institutional settings. Very often, the buildings were large 19th
century hospitals more akin to prisons. The austere environment was
reflected in the manner in which the residents were cared for.
Gradually over time, a distinction came to be made between those with
Psychiatric Illness and those with an Intellectual Disability. People
with an intellectual disability had varying degrees of disability and
those with Low or Moderate levels could be trained to do certain tasks.
This brought about the introduction of sheltered workshops or
“Industrial Therapy Units” as some were known. One of the consequences
of the sheltered workshops was that the people with Intellectual
Disability who worked in them considered themselves as doing productive
work which lessened the barriers between them and non disabled people.
In other words they thought they had a job, went out to work in the
morning and came home in the evening and received some payment for it.
The days passed reasonably quickly because they were busy. Their self
esteem rose and possibly, as a result, their quality of life improved
also.
Driven by economics and the realisation that large institutions were no
longer suited to the needs of the people within, there was shift in the
thinking of how services should be delivered in the 1970s and 1980s. It
was thought that social skills and general well-being might be improved
by placing people with Intellectual disability into a community
setting. Instead of living in large confined institutions and sleeping
1
in dormitories, people were sent to live in houses spread out among the
local community. Usually, 4 to 5 people shared a house. In most cases
they had their own bedroom or only had to share with one other. The
houses were supposed to replicate normal family living, were
comfortable and well decorated and appointed. They were staffed with
care staff that provided care on a 24hr basis, 7 days per week. One of
the intentions of this shift in service delivery was that of community
integration. In fact these houses were microcosms of the institutions
that these people had lived in previously. While the surroundings were
more comfortable and less forbidding, their opportunities for self-
determination were very limited. The staff looked after their every
need and made all the decisions for them. In effect it was still
institutionalisation only on a smaller scale. During the day, these
service users attended Day Services. With the virtual demise of the
Sheltered Workshops in Ireland, Day Services became more associated
with recreational activities, sport and arts and crafts. The service
users of moderate to higher ability found the days passed slowly and
there was no programme of activities to occupy them in the evenings in
the houses
either. This situation continued up to recent times. The service users
in the community houses had a
certain quality of life that was better than they had experienced in
the institutions mainly due to the more pleasant surroundings. However,
freedom of choice and opportunities to learn by their mistakes were
severely limited.
The effect of economics.
It was recognised that some service users were capable of accepting
more responsibility and making choices and doing things for themselves.
However, under the prevailing culture this was a risk that few
2
organisations were prepared to take, and that individual Social Care
staff were afraid to take. Economics again forced a rethink on how
services were delivered, particularly in the light of the high cost of
employing staff and the high Staff to Service User ratio. The solution
was to assess the service user population in the community houses to
find a group with sufficient ability to live semi independently with
much reduced staff support. This is in the very early stages in
Ireland, and a few of the Intellectual Disability Service providers in
Ireland have recently embarked on such a programme. In the region in
which this research was carried out, 10 moderate to high ability
service users with Intellectual Disability have been moved into new
apartments. Some are living alone, and others are sharing with one
other who is well known to them. These apartments are situated in a
small development in the suburbs of the city. There are regular bus
services from the immediate area to the city centre, which in time will
facilitate even more independence for the individuals. Shortly after
moving in, a training programme was initiated to give these people the
skills to live independently with confidence. My hypothesis is that
their Quality of Life will be measurably improved living independently
in their new homes, as a result of the training they received and the
new skills acquired as a result.
Chapter 2Aims of the Present Study and Hypotheses:This study aims to examine the Quality of Life of a group of people
with Intellectual Disabilities who have recently begun to live
independently. In particular, it aims to study whether training in
independent living skills has enhanced their experience of living
3
independently, and by extension, their Quality of Life, if so, to what
degree?
Quality of Life will be quantified using the Personal Well-Being Index
for people with Intellectual Disabilities, which was devised by Robert
Cummins in 2005. This investigation will examine objective and
subjective Quality of Life measurements. These are composed of eight
domains, namely:
Standard of living
Health
Life achievement
Personal relationships
Personal safety
Feeling part of community.
Future security
Life as a whole
The null hypothesis to be investigated is as follows:
4
That people with an Intellectual Disability living independently
experience Quality of Life gains just from the process of living
independently.
The alternate hypothesis to be investigated is as follows:
That people with an Intellectual Disability living independently
experience Quality of Life gains from the appropriate independent
living skills training received.
Research ParticipantsTen subjects, comprised of 9 males and 1 female, ranging in age from 40
to 69yrs were selected to participate in this study. They were part of
a group of 15 adults in a Service for Adults with Intellectual
Disabilities who had recently moved from Community House settings to
Independent Living. They were all classified as being in the High
Moderate Level of Intellectual Disability. All had been in the service
for most of their lives, ranging from 25 years for the youngest to 40
years for the oldest. 5 of the 15 declined to take part in the
research. 3 because they did not feel like answering questions and 2
because their families thought participation might be detrimental to
their mental health and to them settling in successfully to their new
environment. They all attend day services, some attending workshops
were contract work is carried out, while others attend services
offering a variety of recreational and educational activities. As part
of the transition process from Community House to Independent Living, a
programme of special training modules was devised to specifically
address the new situations confronting them and to provide them with
the skills to successfully adapt to their new surroundings.
5
The reality of the transition was that they were coming from houses
with 5 or 6 sharing, and fulltime care staff living in, to a 1 or 2
bedroom apartment, sharing with one other, or living alone, and no
staff living in. There is a staff on duty in the vicinity in case of
emergency and who makes regular visits but in effect, the subjects are
living independently.
Chapter 3
Literature Review on Quality of Life.
IntroductionThis research will demonstrate that, while Quality of Life is an
aspiration for everyone, it has proved difficult to define exactly what
it is. Due to these challenges, it has also proved difficult to
measure. The issue of defining and measuring the Quality of Life of
people with Intellectual Disability has proved even more difficult
because of disagreements as to whose opinions should be taken into
account? The carers and medical professionals’ objective opinions? Or
the subjective opinions of the individuals themselves?
Or is it a case that both could be used?
This Literature Review is divided into two parts, the first part
dealing with the issue of what constitutes Quality of Life, the
evolution of the concept and how it is now applied to people with
Intellectual Disabilities. Issues relating to its measurement are then
discussed, and in relation to this particular study, the question of
the most appropriate measurement instrument is investigated.
The second part examines the training of people with Intellectual
Disability, an examination of the various training methods used in
6
training people with Intellectual Disabilities, the range of skills
requiring training, and how this training can affect their Quality of
Life.
As both the concept of Quality of Life and Training regimes appropriate
to people with Intellectual Disabilities are relatively recent
developments, their evolution is discussed to set the context in which
this research is framed.
The terms Intellectual Disability and Learning Disability are
interchangeable and both are found in this review. The reason being
that the term Learning Disability was found more frequently in the
literature relating to the education and training of people with an
Intellectual Disability, and therefore it is appropriate that it be
retained in the chapter relating to Training.
From the Medical Model to the Social Model of CareUp to the 1980s, the traditional method of treatment for people with
Intellectual Disability was institution based, where the person’s
disability was defined as a medical condition. The institutionalisation
of people with Intellectual Disability became known as the Medical
Model of Social Care, whereby individual’s conditions were researched
and diagnosed in order to prevent, cure or treat the condition. This
system had some successful outcomes such as the eradication of
preventable disabilities through vaccination programmes, and ongoing
research led to better diagnoses and early intervention programmes.
Intellectual Disability was seen as a medical condition and medical
professionals ran the institutions, the objective,
according to Bradley et al (1994), being “to separate people who were
designated sick and vulnerable from the rest of society”.
7
However the Medical Model was deficient in recognising the social needs
of people with Disability, in that it created a regime of dependence,
disempowerment and segregation. A paradigm shift began to take place in
Scandinavia in the 1970s, which gradually spread further afield. The
concept of Normalisation, which will be discussed later, was brought to
the United States by Wolfensberger (1972). He was influenced by the
works of Bank-Mikkelsen (1969), Nirje (1969), and Grunewald (1969), who
wrote about developments in Sweden and Denmark.
However, independent of events in Scandinavia, the Civil Rights
Movement in the U.S. encouraged the Union of Physically Impaired
Against Segregation (UPIAS), to demand equal rights for people with
disabilities. They asserted that it was society that disables people;
the real disability is imposed by society on top of their impairments,
by being unnecessarily excluded from full participation in society.
Therefore, as Oliver (1991) noted, a distinction was made between the
physical or mental impairment- and the disability of being socially
excluded.
The change in paradigm resulted in a new course of action being
pursued; namely that of social change. According to Barnes (1991), if
disability could be proven to be the result of discrimination, then
campaigners saw the solution in Anti Discrimination Legislation. This
eventually came to pass with the enactment of the Americans with
Disabilities Act (1990) in the U.S., the various Equal Opportunities
Acts in the U.K., and the Equality Acts 1998 and 2004 in Ireland, to
give just a few examples.
The net result of the change in attitude was the replacement of a
system of services to a system of supports. The large institutions were
gradually phased out in favour of the new Social Model of Care. This
8
Model was defined by the creation of group homes and sheltered
workshops that were physically located in the community. This was the
first attempt at community integration. However, the fact that
specialised services were provided, and that the group homes were
socially segregated from the community, still gave the impression of
institutionalisation, albeit on a much smaller scale. The group homes
were fully staffed and the service users had little or no independence.
Research by Bruininks, Hill, Weathersman and Woodcock (1985) found that
significant improvements in adaptive functioning and social adjustment
can be attributed to residents transferring from large institutions to
smaller community units, and particularly in people with moderate to
severe levels of disability. Hemmings et al (1981) found in a two-year
longitudinal study, of people who had moved from large living units to
bungalow style accommodation, that there were increases in independent
functioning, language development, numeracy, domestic skills, and the
development of self-direction and self-responsibility. However,
according to McVilly and Rawlinson, (1998) physical relocation does not
have an automatic and positive effect on the quality of life of people
with disabilities, and deinstitutionalisation
involves more than just placing people in a small community based
programme. Likewise, Lakin, Bruininks and Sigford (1981) noted that the
social status and personal power of mentally retarded persons remain
unchanged, even though their place of residence may have changed.
Therefore it appears that by 1981, improvements were already beginning
to be seen in people with intellectual disabilities who had moved from
the Medical Model of Care to the Social Model in the area of
challenging behaviour but as we have seen, researchers disagreed as to
the extent of these improvements. Clearly, other interventions were
needed to continue the improvements brought about by the move to
community settings.
9
The Social Model continued to be refined, and as Bradley et al. (1994)
note, we are now in the era of community membership, “which is marked
by an emphasis on functional supports to enhance inclusion and quality
of life, as defined by physical as well as social inclusion”. In
effect, these functional supports include training in the type of
skills necessary to equip an individual with a disability to live
independently in the community, making their own choices and being
supported by the service providers. This then, is the next logical step
in the evolution of the Social Model of Care, individuals with an
Intellectual Disability living independently in the community.
Therefore as we have seen, the first major shift was the movement of
people with Intellectual Disabilities out of the big institutions and
into smaller units in the community where it was assumed their quality
of life would be improved. Let us examine what this assumption was
based on.
Historical origins of the concept of Quality of LifeThe historical context of the concept of Quality of Life was based on
the measurement of Economic Indicators of Social Welfare where Quality
of Life was presumed to flow from accumulation of material wealth. This
view was prevalent from the early part of the 20th century up to the
1960s, where the efforts to collect and analyse the data became more
systematic. Governments and other organisations published Social
Reports containing statistics and analyses of social change and social
trends in areas such as Housing, Consumption, Education, Income and
Medical Care among others. According to Bognor (2006), the impetus for
gathering such data from these Social Indicators came from
dissatisfaction with the perceived limitations of Economic Indicators 10
of Social Welfare. It was realised among researchers that material
wealth in itself was only one of a wide range of attributes that had
the potential to make an individual satisfied, if not happy. The
proponents of the Social Indicators concept felt that the Economic
Indicator model was too narrow and confining and did not sufficiently
evaluate how well the lives of people go in a society. Eventually it
was realised that some of these Social Indicators might also impact on
the thoughts and perceptions of people with disabilities.
The Modern Origins of Quality of LifeThe term “Quality of Life” in its modern meaning, is attributed by
Cummins (1997b.117), to a 1964 speech by President Lyndon Johnson where
he stated the progress on social goals “ cannot be measured by the size
of our bank balance, they can only be measured by the quality of the
lives our people lead.” Noll (2000), also credits President Johnson
with coining the phrase, albeit in a different speech, where he said “
the great society is concerned not with how much, but with how good –
not with the quantity of goods but with the quality of their lives “.
It took quite some time before the concept of Quality of Life was
applied to the lives of people with Disabilities, and in particular
Intellectual Disabilities. This is because, unlike those individuals
with physical disabilities, who were able to articulate their
grievances individually and collectively, the intellectually disabled
were not in a position to do the same. Borthwick-Duffy (1992), found
that a publication by Meyers (1978) in the American Association on
Mental Deficiency entitled” Quality of Life in Severely and Profoundly
Mentally Retarded People: Research Foundations for Improvements”, did
11
not in fact refer to Quality of Life in the present context. Rather it
referred to reducing challenging behaviour through teaching techniques.
Campo, Sharpton, Thompson and Sexton (1997) found that the main
concerns of Quality of Life issues for people with Intellectual
Disability during the 1970s and 1980s, centred on issues of adaptive
behaviour skills and scoring in intelligence tests. Wolfensberger
(1972) proposed the notion of normalisation, which was the first
attempt to equate the quality of life aspirations of people with
intellectual disability with those of their non disabled peers. This
principle of normalisation asserted the right of people with
intellectual disabilities to be treated and respected like other
members of the community and to be given an opportunity to enjoy an
ordinary life in the community.
O Brien (1987) noted five conditions required to achieve normalisation:
1. Community presence: the facility for people with intellectual
disabilities to live in local communities in ordinary
settings.
2. Choice: to have autonomy over decisions affecting everyday
living.
3. Respect: the eliminating of difference making conditions which
stereotype people with intellectual disabilities as being inferior or
different.
4. Competence: the opportunity to develop new skills.
12
5. Community participation: opportunities for people with intellectual
disabilities to form networks and social relationships within the
community.
These 5 conditions, if fulfilled, may lead to normalisation and
therefore increased Quality of Life, but some require training in order
to be achieved and respect requires a change in attitude from the
general public.
Normalisation and Community Integration.The principle of normalisation might provide the foundations for an
environment where quality of life might improve, and around that time
there was a shift in the way services for the intellectually disabled
were provided. Many of the old institutions were replaced by a new
system of community living whereby small groups of service users were
placed in houses in residential areas and where their care staff lived
with them. This was the first attempt at community integration, but as
Jahoda, Cattermole and Markova (1990) discovered, despite participating
more in community based activities, their contact with non disabled
people was very limited and so there was a measure of discontent with
their social lives. Holm, Holst and Perlt (1994) asserted that the
development of cultural, vocational and social activities were required
in local areas to allow people with intellectual disability to show
they can manage on their own without the well meaning interventions of
professionals and care staff who “know better”.
Community integration is one of the recurring themes in the literature
and Townsend –White et al (2011) have stated that Human Rights
frameworks recognise the right of people with a disability to have full
13
and effective participation equal to other members of society
generally, and particularly in relation to matters directly concerning
them. To quote from a recent United Nations paper (2011) “The rights of
individuals with disabilities are grounded in a human rights framework based on the United
Nations Charter, the Universal Declaration of Human Rights, international covenants on human
rights and related human rights instruments. Persons with disabilities are entitled to exercise
their civil, political, social, economic and cultural rights on an equal basis with others under all
the international treaties. The full participation of persons with disabilities benefits society as
their individual contributions enrich all spheres of life and this is an integral part of individual's
and society's well-being and progress for a society for all - with or without disabilities.” A good
example of this in practice is the recent move towards
Individualisation, where the individual and not the service will be
funded, in effect allowing the person with Intellectual Disability to
choose his or her Care Organisation.
Towards Defining Quality of LifeChoice, therefore, is one of the prerequisites for normalisation and by
extension, a better quality of life. But quality of life as an overall
concept is difficult to define. Hughes et al (1995) survey identified
44 different definitions between 1970 and 1993. Cummins (1997a :1-2)
noted well over 100 definitions and models, with some being relevant
to the commonly accepted notion and others vaguely related. Examples of
some of the more relevant definitions include the following:
“Quality of Life is the discrepancy between the persons achieved,
and unmet, needs and desires.” This definition presumes that the
greater the discrepancy, the poorer the quality of life. (Brown,
Bayer, and McFarlane ,1988)
14
“ An overall general well-being which comprises objective
descriptors and subjective evaluations of physical, material,
social and emotional, together with the extent of personal
development and purposeful activity all weighted by a personal set
of values.” Felce and Perry (1993:13)
“Quality of Life encompasses the basic conditions of life such as
adequate food, shelter and safety, plus life enrichers such as
inclusive social leisure, and community activities.” These
enrichers are based on the individual’s values, beliefs, needs and
interests according to Schalock and Parmenter (2000:7)
Quality of Life is both objective and subjective, each axis being
the aggregate of seven domains: material well-being, health,
productivity, intimacy, safety community and emotional well-being.
Objective domains comprise culturally relevant measures of
objective well-being. Subjective domains comprise domain
satisfaction weighted by their importance to the individual.”
(Cummins, 1997a: 6)
Rapley (2003) favours Cummins` (1997a:6) definition as the most
influential and comprehensive. However, there have been many more
definitions since Cummins counted 100 in 1997, therefore it is fair to
say that there is agreement as to the general characteristics but
researchers still disagree as to what constitutes the absolute
definitive characteristics, and by extension how it can be measured.
Measuring Quality of LifeThe measurement of quality of life has evolved from the simple
recording of whether people who left institutions remained in the 15
community or were reinstitutionalised, and the monitoring of daily
activity patterns (Bjannes and Butler, 1974, O’Connor 1976, and
Birenbaum and Re 1979), assuming that daily activity patterns could be
directly equated with variations in quality of life. The research
involved the degree of independent action exhibited by individuals, and
the amount of social contact achieved as a
result of participation in activities. The measuring tools of that time
employed participant observations and respondent based ratings supplied
by care staff (Sullivan et al, 1988). However the concept was further
refined when it was realised that quality of life was intrinsically
linked to the individual’s environment and the opportunities to develop
adaptive behaviours and positive social adjustment. These in turn
facilitated more opportunities for social contact. In this instance,
the process was as important as the outcomes. So why is it so important
to measure the Quality of Life for people with Intellectual Disability
compared with non disabled people? Simply because, unlike non disabled
people, those with an intellectual disability are completely dependent
on others who make decisions as to what is good and not good for them.
People with Intellectual Disability are given a voice when included in
the measurement process.
One of the common threads running through the literature is that to
measure Quality of Life is an attempt to measure subjective feelings of
well-being. Early research in the field concentrated on client ill
health with an emphasis on morbidity, mortality and service
utilisation. Recently the concept of health has taken on a wider
meaning to include social and psychological as well as physical
aspects. These physical aspects could equate to what Antonovsky (1979),
cited in Lindstrom and Eriksson (2005), and defined as General
Resistance Resources (GRR). In essence these are material, biological,
and psychosocial factors, which make it easier for people to see their
16
lives as having some structure and consistency. Lindstrom and Eriksson
(2005) give examples of GRR, which Antonovsky (1979) claimed to promote
good health through elimination of stress, which are remarkably similar
to those items, assumed to increase quality of life. E.g.:
Money Knowledge,
Experience,
Self Esteem,
Intelligence,
Traditions
View of life
Early research into Quality of Life issues among the Intellectually
Disabled took an objective view based on the comments and observations
of third parties. In recent times there has been a shift in emphasis
towards the individuals own subjective feelings of their health or
situation, rather than the opinion of their physicians or carers.
According to Bowling (1997), as there was no agreed definition of
Quality of Life, so in order to effect a measurement, it was necessary
to include measurements of functional ability, health status,
psychological well-being, social networks and social support, life
satisfaction and morale. These are roughly in line with the five clear
areas of well being, which, according to Felce and Perry (1997), set
the theme for major understanding of Quality of Life:
1. Physical well-being.
2. Material well-being.
3. Social well-being.
4. Emotional well-being.
5. Productive well-being.
17
But even as the domains of everyday life, which appeared to affect the
individual’s quality of life, were being refined and apparently
converging, the debate over subjective versus objective measurement
continued. According to Brown (1998), the perception of individuals,
particularly in relation to their carers and professionals, illustrates
their understanding of choice, but frequently they are regarded with
suspicion due to the nature of their subjective responses. Browns view,
which is shared by Andrews (1974), is that these perceptual responses
can be considered to be the way that individuals respond to what they
believe, rather than objective realities. What they feel about them
selves is likely to be a major determinant of behaviour.
Schalock (2004) distinguished the difference between the construct of
individual quality of life as separate from family or health related
quality of life. The emphasis on quality of life has previously been
applied to the area of ill health and palliative care. It was some time
later when the concept was applied to people with intellectual
disability.
Schalock et al (2004) examined the reasons for the rise in interest in
quality of life and concluded it arose from four sources:
1. The realisation that scientific, medical, and technological
advances alone, would not result in improved life, leading
to the understanding that personal, family, community, and
societal well-being emerge from a complex mixture of these,
plus values, perceptions and environmental factors.
2. This realisation led to the belief that normalisation was
achievable more effectively through community based services,
18
and measuring outcomes from the individuals life in the
community.
3. There was a rise in consumer empowerment and patients rights
movements and their emphasis on person centred planning,
personal outcomes and self-determination.
4. The emergence of sociological changes that introduced the
subjective and perceptual aspects of quality of life.
However, another aspect of the debate has centred on the outcomes from
the measurement of quality of life. The area of quality of life
measurement has been impacted by two factors; the movement towards
assessing the value and quality of the different programmes based on
consumer satisfaction and personal outcomes, and the development of new
service delivery initiatives.
The importance of measuring quality of life for people with
intellectual disability was highlighted by McVilly and Rawlinson (1998)
when they remarked, that in a time of finite resources and non finite
demands, the failure to objectively evaluate changes to service
delivery in terms of improvement of quality of life, could hazard a
return to the traditional institution based services.
Schalock (2004) asserts that the most effective method of determining
whether people with intellectual disability are as satisfied with life
as other population subgroups is to assess subjective well-being and
compare. Schalock also specifies two standards, which will allow the
organisation, in terms of improved service delivery, and the
individual, in terms of quality of life measurement, to align the
delivery of service to meeting the individual’s needs. In the case of
the individual, the standards are: Individual Performance Outcomes and
Individual Value Outcomes. It is significant that Schalock includes
19

“activities of daily living, and instrumental activities of daily
living” under the heading of Individual performance. These activities
would include: eating, transfer, toileting, dressing, bathing, meal
preparation, housekeeping, taking medication, money management and
telephone use. In the context of people with intellectual disability
who have spent most of their lives residing in Community Houses, these
are the activities that the care staff carried out for them. It follows
that these are the areas in which training is required in order for
them to live with a degree of independence.
According to Schalock (2004), it is the ability to carry out these
activities that leads to Individual Value Outcomes such as emotional
well-being, personal development, self-determination, social inclusion
and rights. There are advantages to be gained for the care
organisations as well. Keith and Schalock (2000) have opined that, by
taking advantage of the resources of family, friends, and
neighbourhood, it is possible to avoid expensive programmes to promote
social inclusion, and that efforts to connect quality of life of people
with intellectual disabilities to that of other citizens should
continue to be made.
But, as Rapley (2000), and Reinders (2002) have pointed out, there is a
difference between being “in” the community and being “of” the
community. Being “of “the community denotes acceptance and integration
in-to the community, participating in community activities, and most
importantly, feeling a sense of security and acceptance. Being “of” the
community promotes a sense of well-being and as such, is one of the
expected benefits of community integration. However, this level of
integration requires the proper supports and training programmes to be
put in place.
20
Costanza et al (2007) are critical of quality of life measures on the
basis that they only represent a snapshot in time, that because humans
and their environment are constantly evolving, a single snapshot is
insufficient to develop an effective knowledge base. Measurement data
used for predictive purposes would need to be collected over a much
longer time period. This true in most cases where the pattern of daily
living has remained unchanged for a considerable period of time.
However it is not logical to assert that this holds true when there has
been a major change in someone’s life, like for example the transition
from community house living to semi independence. In this case a
snapshot of quality of life is appropriate. This first snapshot is used
to get a baseline measurement and to establish the general principle,
i.e., has this change resulted in a perception of increased Quality of
Life? As will be seen in the Methodology chapter, Cummins uses a
process of taking snapshots at regular intervals in order to track
fluctuations in the Quality of Life data.
Also, in the context of this research, Bonham et al (2004), state that
quality of life outcome data can inform a range of stakeholders as to
whether, and to what extent, service users experience changes in the
quality of life as a result of service interventions, and whether
outcomes are being achieved.
The subjective v. objective measurement debate.It was a convenient assumption that quality of life for people with
disabilities improved as their circumstances improved. These “improved
circumstances” were usually determined by professionals or care staff.
These “improved circumstances” being based upon what non-disabled
people would consider as being desirable in their lives. However,
whether for future service improvement initiatives or for a genuine 21
desire to improve the well being of people with disabilities, it was
necessary to collect data and measure exactly what this quality of life
is. Following on from the many and varied definitions, there were
numerous and mixed attempts at measuring this elusive concept, most
concentrating on what exactly should be measured?
According to Cummins (1997), the traditional method of measuring
quality of life for people with intellectual disability has been
through an objective measurement of their life circumstances. The
criteria
used have included their standard of accommodation, patterns of time
expenditure, and extent of interaction with the community to name just
a few. This data was usually in the form of counts or frequency, and
when applied to the general population standards, the result was some
degree of normalisation. (Wolfensberger and Glenn 1975, Wolfensberger
and Thomas 1983). Cummins has criticised these on the basis that they
are ideologically driven. According to him, they are based on the
assumption that the people concerned should all live under the same
objective life circumstances as the rest of the general population.
Cummins contends that this is an overly simplistic view, based on the
perceptions of third parties and not on the individual preferences of
the people who are intellectually disabled. Cummins view is that
responses supplied by proxies and third parties often bear little
relationship to how the person actually feels. The debate regarding
Subjective v. Objective measurement is one that heavily influenced
Cummins in his quest for the most appropriate measurement scale. He
concluded that measuring quality of life means asking people about how
they feel about their lives and these questions are usually enquiries
about satisfaction levels with various life domains.
22
The Domains of Quality of LifeQuality of life is measured using a set of factors which, when brought
together, create personal well-being. These factors, or Domains as they
are called in the literature, comprise of a multi element framework. In
a study of the then current literature by Schalock and Verdugo in 2002,
the vast majority of these domains were aggregated into eight core
domains. The Domains most frequently referred to were (in order of
importance):
1. Interpersonal Relations
2. Social Inclusion.
3. Personal Development.
4. Physical Well-being
5. Self Determination.
6. Material Well-being
7. Emotional Well-being
8. Rights
It is interesting that although Felce and Perry`s 1997 five core areas
of well-being are represented in this list, they are not in the same
order of importance, reflecting how different researchers agree in
general but disagree in specifics when it comes to measuring quality of
life. It is perhaps not surprising that Interpersonal Relations and
Social Inclusion were the two Domains most frequently referenced.
However, the fact that Personal Development and Self Determination
figured so prominently indicates the degree to which individuals with
intellectual disability recognised that they were in a fluid
environment and would benefit from training in Personal Development
23
Townsend-White et al (2011) in their systematic review of quality of
life measures for people with Intellectual Disability noted that
response bias has been well documented in self-report measures among
people with Intellectual Disability. (Sigelman et al 1980, and Verri
et al 1999). They also note that adolescents and adults with
Intellectual Disability are prone to presentation bias and choose the
most positive alternative. Townsend-White et al (2011) took this into
account when reviewing the available quality of life scales, and
specifically examined whether the instrument contained screening tools,
pre-tests, or acquiescence scales to assess a person’s capacity to
understand the questions. Cummins Personal Well-being Index-
Intellectual Disability Scale (2005) was found to contain a method of
assessing acquiescent responding that was far more rigorous that those
contained in the other scales. Cummins (2005) scale uses a series of
pre-tests which the individual must complete before they can proceed to
the main questionnaire. Success in the pre-test stage shows that the
respondent understands what is being asked of him/her and also
demonstrates an ability to score his/her answers on a Likert type
scale.
Townsend –White et al (2011) also considered the question of subjective
v. objective assessment. They found that some instruments based their
findings on the opinions and observations of the Care Staff, while
others asked the Service Users directly. Townsend –White et al found
that the Cummins scale was the only one to measure Domains on both
subjective and objective quality of life, as recommended in the
literature.
Instrument brevity was another important consideration in the
measurement of outcomes. Briefer instruments reduce the data collection
burden and Cummins PWI-ID 2005 is one of these briefer instruments.
24

Bickman et al (1998) and Hermann et al (2000) also found that briefer
instruments promote routine collection by clinicians. Hartley and
McLean (2006) conducted a review of the literature regarding the
reliability and validity of Likert type scales for people with
Intellectual Disability and found that the level of Intellectual
Disability significantly affects the reliability of responses on Likert
type scales. Individuals with mild or borderline Intellectual
Disability were better able to contend with Likert type scales. McVilly
and Rawlinson (1998) similarly agreed that Likert Type scales were not
suited to people with moderate to severe levels of intellectual
disability.
One of the problems encountered when surveying people with intellectual
disability is their potential to acquiesce and provide answers that
they think will be favourably received by the interviewer. In fact this
is an issue in all social research and is an issue that will be
discussed in the Methodology chapter. Burnett (1989) advocates that
yes/no formats should be avoided, and caution exercised regarding item
comprehension and the ability to discriminate between such constructs
as happy or sad, or like and dislike. He also found that participants
with intellectual disability were prone to mood changes and that their
prevailing mood significantly influenced their responses.
Another difficulty arises when trying to formulate questions which lie
within the cognitive capacity of the respondents. For people with
intellectual disability, comprehension at the abstract level that is
inherent in subjective measurement is difficult or even impossible.
Pretesting is important to establish the respondents’ level of
cognitive understanding, and capacity to validly respond to the
questions asked. So by keeping the questions as simple as possible, the
25
sentences short and avoiding negatives, will assist with this.
Interestingly, this same strategy is recommended for use in the
training of people with intellectual disabilities.
On the issue of proxy respondents, McVilly and Rawlinson (1998)
consider them to be an important data source, particularly in relation
to service related decisions regarding people with intellectual
disability. Data obtained from proxies may be necessary as the
individuals themselves may not be able to give reliable responses on
all relevant issues. In spite of this, Burnett (1989) found that staff
were poor predictors of resident’s satisfaction. Therefore on the basis
of probability that the subject knows best what he/she likes best, and
is happy with, Cummins measuring tool PWI-ID would appear to offer the
best method of subjective assessment due to its element of pretesting,
which promotes a comfortable atmosphere while asking questions and
allows the interviewer to assess the respondents level of
comprehension. But Cummins does not dismiss the value of objective
measurements entirely, stating that when aggregated with subjective
measurements, they both provide balance and therefore supply a total
quality of life construct. But in isolation they would not have
sufficient validity.
Criticisms of CumminsAger and Hatton (2002) have issues with Cummins defence of subjective
measurements. They assert that reliance on self-report raises a number
of methodological issues, including the reliability and validity of
responses by people with intellectual disability, and the validity of
proxy responses, particularly concerning more subjective aspects of
experience. Therefore, they propose that, if the reliability and
validity of quality of life interviews cannot be established for a
majority of people with intellectual disability, then the utility of 26
self rated quality of life measures for general service evaluation is
questionable. Ager and Hatton (2002) cited a study of 154 adults with
intellectual disability that Perry et al (2000) carried out in the UK
to illustrate their argument. This sample of adults was selected to
reflect the full range of ability using norms on the Adaptive Behaviour
Scale part 1. (ABS) (Nihira at al, 1993). The data established that few
respondents with below average ABS scores responded to questions, and
of those that did, all demonstrated response bias. However, only the
sub sample of respondents within the top 30% of ABS scores recorded
response rates above 75%, and rates of response bias below 25%.
On the basis of these findings, Ager and Hatton (2002) maintain that
quality of life interviews will not produce valid and reliable
information with the majority of people with intellectual disabilities.
In defence of Cummins (1997), the people most likely to be asked for
their subjective opinions on their own perception of quality of life
are those within the top 30% of ABS scores, that is, those with higher
levels
of comprehension and cognitive ability. The fact that those with lower
ABS scores would have difficulty both comprehending and communicating,
would mean that only third parties could give any meaningful objective
responses. Given this, Ager and Hattons criticism of Cummins are not
completely convincing.
SummaryQuality of Life only became an issue for people with Intellectual
Disabilities when the model of care changed from the Medical to the
27
Social. It has evolved from a measurement of material well being to a
measurement of social well-being. The social indicators were eventually
refined into a list of Domains, these areas of a person’s life, which
when aggregated, constituted a perception of well-being, which could be
measurable. The debate over whose perception of these Domains should be
measured, the individual him or herself, or a third party, is ongoing
but it appears that a combination of both may be valuable considering
the circumstances.
Chapter 4Literature Review on TrainingIntroduction
This section begins by exploring the linkages between the Education
Systems and the Vocational Training Systems when applied to individuals
with Intellectual Disabilities. It then discusses the shift in focus
from segregated education and training to an integrated model and
whether participants and professionals view this as progress. Moving
on, the question of “to what degree are people with Intellectual
Disabilities actually trainable” is discussed and what conditions are
necessary to facilitate this? The section concludes with a review of
actual training strategies and the specific skills set needing to be
taught to make the transition to independent living successful and
capable of bestowing Quality of Life gains.
Modern trends in education and training for people with
Intellectual Disability.Education and training is inextricably linked for people with
disabilities as well as the non-disabled. All children begin learning
from an early age through socialisation from their parents and their
environment (Bandura 1977). Likewise, training in many of the basic 28
activities required for daily living takes place from an early age and
continues through the early school years. As they finish their formal
education, many continue on to be trained for specific roles or tasks.
However, many young people with intellectual disabilities have been
denied access to mainstream education for years, although this is now
changing. For the intellectually disabled child, there was a parallel
system of education consisting of special schools with specially
trained teachers, a different teaching regime and supports specific to
the teaching of children with an Intellectual Disability.
The pros and cons of MainstreamingDebate continues as to the benefits of including children with
Intellectual Disability in mainstream education. The benefit most
frequently cited is that of socialisation, which is mixing with a more
diverse group than they would meet in a specialised setting, and the
acquisition of social skills that follow from this. This is very
similar to the normalisation and community integration principles that
brought about the transition from the medical to the social model of
care.
However, in the eyes of many, including parents and teachers,
mainstreaming was a retrograde step.
Lieberman (1992) points out that many advocates (primarily parents) for
those with learning disabilities have significant concerns about the
wholesale move toward inclusion. Their concerns stem from the fact that
they have had to fight long and hard for appropriate services and
programs for their children. They recognize that students with learning
disabilities do not progress academically without individualized
attention to their educational needs. These services have evolved
primarily through a specialized teacher working with these students
individually or in small groups, usually in a resource room setting. 29
Mainstream teachers are not trained to, and do not have the resources
to effectively teach children with Intellectual Disability, and also do
not have the necessary time to devote to them either. Tornillo (1994)
explains that "the disabled children are not getting appropriate,
specialized attention and care, and the regular students' education is
disrupted constantly."
Shearman and Sheehan (2000), also have views on how the move towards
mainstreaming of training will impact on trainees with Intellectual
Disabilities, which mirrors the concerns raised regarding mainstreaming
in education. They report that industry-qualified teachers, e.g., a
catering teacher, train many students with intellectual disabilities in
mainstream classes. While this teacher may be knowledgeable on catering
matters, it is unlikely that they are knowledgeable on disability
matters. Therefore, it is necessary to have a second teacher,
specialising in disabilities, as a support teacher. This support
teacher assists the industry teacher by determining appropriate
training strategies and by preparing adapted teaching materials. Having
a second teacher with disabilities expertise results in a lower student
teacher ratio and allows for more individual attention. The main reason
however for employing a second teacher is his/her expertise in
strategies for implementing reasonable adjustments. Reasonable
adjustment is one of the key areas considered when designing training
for people with intellectual disabilities. In most instances, it is not
financially viable to employ a second teacher, but the inference is
that skills should be taught with patience and over a longer time frame
when dealing with people with intellectual disabilities.
FÁS, the Irish Vocational Training Authority, in its Vocational
Training Strategy published in 1996, reached the same conclusions
regarding the supports required by trainees with a disability, as Ball
30
did in 2000. FÁS stated that “there is a need for additional resource
supports (psychologists and specialist disability advice) in FÁS
training centres, especially for frontline staff and trainers, in
dealing with people with disabilities.
FÁS defines vocational training as “supplementary to initial training
which is part of an ongoing process designed to ensure that a persons
knowledge and skills are related to the requirements of his/her job,
and
are continuously updated.” This does not differ greatly from the
requirements of training to live independently, which is also an
ongoing process and needing constant updating. In fact, the whole
transition from the medical model to the social model of care was a
period of adaptation and learning to adjust to the new environment.
Part of this transition process, with regard to training services, as
has been discussed, was the concept of mainstreaming. Mainstreaming is
the systematic integration of people with disabilities on to the open
labour market, by actively creating conditions whereby people with
disabilities can compete on an equal basis with their non-disabled
peers. (FÁS Vocational Training Strategy 2006).
For people of a certain age with an Intellectual Disability, they were
educated in the special system, as mainstreaming was not yet available.
Therefore, on reaching school leaving age, the only option for further
education was through the Vocational training system. This in effect
meant that their choice of career was limited and was decided for them
by someone “who knew better”. Very often, training in the basic
activities of daily living was not provided because of the particular
model of care that prevailed at the time. This discrimination denied
the opportunities for personal development that would have given more
31
freedom of choice at a later age. As Barnes (1994) writes “The aims of
education for all children and young people include the achievement of
responsible personal autonomy and full participation in the communities
in which they live. In practice, this usually means employment and a
relatively autonomous lifestyle. The type of education that the
overwhelming majority of young people with impairments receive does not
provide them with the necessary skills and opportunities to achieve
either”. It is now known, as will be discussed later, that people with
intellectual disabilities are both educable and trainable given the
appropriate conditions. Therefore, as education and training are both
relevant in the pursuit of autonomy and independence for people with
intellectual disabilities, it is pertinent to discuss both in the
present context.
It is also worth mentioning that all of the participants in this
research attended special schools. The option of mainstreaming was not
available to them at that time.
The evolution of a training model for people with
Intellectual Disabilities.Training in the context of disabilities has historically revolved
around two issues: the training of staff to work with people with
disabilities, and the issue of vocational training to prepare
individuals with disabilities for supported or sheltered employment.
The literature on training people with disabilities, and particularly,
those with intellectual disabilities, to acquire the necessary skills
to live independently, has grown in recent years to complement the
literature concerning vocational training. In fact, as will be seen
later, many of the skills necessary for the transition from training
into employment are also necessary for transition into independent
living.
32
In the past, training services for people with disabilities were geared
towards obtaining vocational skills to enter employment. Initially,
most of those employment opportunities were in Industrial Therapy Units
attached to large hospitals. Another alternative was the various types
of sheltered employment run by service providers under the Medical
Model of Disability. The Social Model of Disability questioned the
segregated nature of training and employment services for people with
disabilities.
In the Irish context FÁS, the Irish Training and Employment Authority,
following the recommendations of the Commission on People with
Disabilities (1996), entitled “ Strategy for Equality”, and set about
implementing the recommendations based on the Social Model of
Disability. The emphasis was on providing occupational guidance and
training services for the disabled based on integrated settings and
offering greater choice than was previously available. The sequence to
be followed was first, to develop a seamless progression from
rehabilitative training to vocational training, then the provision of
bridging programmes to mainline training, with the ultimate goal of
progression to employment. Rehabilitative training in this instance is
taken to mean the basic skills of numeracy, literacy, communication and
social skills, which are the foundations of choice, self-determination,
social integration and independence.
Lacey (2000, pp100-2), cited by Lisle (2007), asserted that “learning
disability is a multi professional, multi disciplinary topic and
therefore educationalists should get involved with the care of adults
with intellectual disability because their care is dominated by the
medical profession and therefore, this group of people does not get
access to the education they deserve”. He further suggests “people with
33
learning difficulties find learning difficult by definition, so their
need for help is greater”. Prior to this time, the fact that people
with learning disabilities might have different learning styles did not
seem to enter the equation.
Learning Styles and people with Intellectual Disabilities.Gardner (1993) suggests that western education favours the auditory
learning style over the visual and kinaesthetic styles. In fact,
Gardners eight learning styles, with their idea that certain learning
styles were particularly suited to certain careers, appeared to ignore
the possibility that people with learning disabilities might have
preferred learning styles as well.
Shearman and Sheehan (2000) state “all people with an intellectual
disability need information which is delivered with precision and
clarity”. However, they comment that people with intellectual
disabilities are not a homogeneous group, they do not all have the same
educational requirements. There is a perception that reasonable
adjustments are necessary for people with certain types of disability,
e.g., wheelchair users need physical access, deaf people require
interpreters/note takers etc. However, there is often less recognition
of the need to provide reasonable adjustments for people with
Intellectual Disability. According to Shearman and Sheehan (2000), some
vocational education and training staff believe that because people
with Intellectual disability are slower at learning, it is sufficiently
reasonable for adjustment to provide them with longer time to learn,
and with smaller class ratios. Shearman and
Sheehan (2000) also believe that it is not sufficient just to provide
more of the same training given to students without a disability.
Instruction must be systematic and information must be clear and 34
concise. This requirement is a recurring theme throughout the
literature as one of the basic foundations in the training of people
with intellectual disabilities.
Ball (2000) provided details of enabling courses for Australian
students in the Vocational Education and Training sector. These courses
were open to both disabled and non-disabled students. The main aim of
these courses was to provide guidance to those unsure of a career
choice on entry, or in preparation for re-entry into the labour market.
However, individuals when taking these courses can also acquire
important basic skills, which allow them to lead more independent lives
and participate in social and community activities. Ball (2000) also
noted that the success rates for students with disabilities completing
enabling courses were broadly similar to the results of non disabled
students. One interesting point in this research was that students with
an intellectual disability performed better than students with other
types of disability, and these students performed better than students
who reported that they did not have a disability.
One of the three guiding principles adopted by the Commission for the
Status for People with Disabilities in 1996 was the principle of
Independence and Choice. Independence and Choice had a very different
meaning in 1996 to what we understand today. Independence was an
aspiration whereby people with disabilities should have control over
how their needs are met. In the context of training and development,
choice was geared towards assisting a potential trainee or job seeker
to identify his/her needs and then finding a suitable course and
providing the supports needed to sustain that trainee. In the main,
this approach was aimed at the physically disabled, who had their full
range of mental faculties, rather than the intellectually disabled.
Some of the physically disabled were able to live at home and attend
35
these training workshops, but generally, most users, and especially,
the intellectually disabled, lived in institutions, and attended what
were known as Industrial Therapy Units. Therefore independence of
choice regarding training and occupation was a relatively new concept
at that time, but independence as regards where to live and who to live
with, was an idea whose time had not yet come. Despite the emphasis on
appropriate training, and independence of choice, Wells (2006)
commented that the main transformation activities that took place in
the Industrial Therapy Units was the structuring of the day for users,
through occupational activities and monitoring their mental and
physical state.
The Importance of Social Skills TrainingA recurring theme running through the literature on the training of
people with Intellectual Disabilities is the importance of Social
Support. Ruesch et al (2004) state that this aspect of social support
generated through occupation is highly valued by users. Wells (2006)
also found this to be the case in his study in (2006), but he also
noted that many felt discontent at not being paid adequately for their
efforts.
Training and the concept of quality of life is linked. In order to
express satisfaction or happiness with a specific situation, the person
must be able to identify the particular emotion e.g., satisfaction,
happiness etc. Dagnan et al (1997) (2000) found that only 10% of
participants with intellectual disability could understand “cognitive
mediation”. Successful performance was positively associated with
language comprehension. The authors concluded that people with mild
intellectual disability may already possess some Cognitive Behaviour
Therapy Skills, but would benefit from some preparatory training. 36
However, recognition of facial cues and other elements of body language
may be as important as language comprehension.
McAlpine et al (1991) and Hobson et al (1989) noted that this skill is
often impaired for people with an intellectual disability. However,
McAlpine at al (1991) suggested that this lack might be remedied to
some degree by social skills training. Walker (1981) found that, by
misperceiving facial expressions, the individual misses important clues
regarding the process and outcomes of interpersonal exchanges, and that
this could result in inappropriate social responses. Furthermore, the
consequences of these inappropriate social responses will not be
reinforced, thereby leading to increased withdrawal from social
interaction. By the same token, the inability to communicate their own
feelings to others, will reduce the probability of help-seeking
behaviour.
According to Rydin-Orwin et al (1999), reviews of intervention studies
showed that a variety of social skills can be taught to people with
intellectual disabilities. These skills included assertiveness and eye
contact (Stacy et al, 1979), increasing positive social behaviour,
(Meredith et al, 1980), and smiling, (Nelson, Gibson, and Cutting,
1973). In addition, Tarkington et al. (1973) and Liberman, (1972), have
suggested that group training in these skills is more advantageous than
one to one training. They assert that the group format is more
economical and provides a more realistic setting for interpersonal
learning, through multiple learning models and multiple sources of
social instruction and reinforcement.
In the context of training people with intellectual disabilities to
live independently, they must be able to identify with the emotions
associated with doing for themselves in a way that they never had to
37
previously. In particular, things like spending time on their own and
ceasing to rely on care staff to a high degree. In some cases, this new
found freedom from 24/7 observation may bring about positive emotions,
in others, the fear of abandonment and the unknown, may bring on a
different set of emotions.
A study by Bruce et al (2010) found that preparatory training in
Cognitive Behaviour Therapy led to significant improvements in
participant’s ability to link thoughts and feelings, and this skill was
generalised to new materials. This is relevant as a prerequisite to
completing a quality of life questionnaire in that the respondent can
think about his/her situation and determine whether he /she is happy or
not, and to what degree. As for actively participating in the training,
as Dunfee (2000) observed, “where vocational education and training is
not, or does not appear to be relevant to an individuals needs or life
experiences,
the motivation to participate in and complete training is reduced”.
Dunfee (2000) also itemises the four core skills that are a
prerequisite for entry into the labour market, but equally these same
core skills are just as relevant in the attainment of a satisfactory
level of independent living. These are:
1. Literacy and Numeracy
2. Communication skills
3. Team skills
4. Acceptable behaviour, ethics and image.
38
Effective Training Strategies for training people with
Intellectual DisabilityDunfee (2000) states that these core skills do not simply materialise,
they actually need to be developed. Training methods used by corporate
trainers were investigated by Allen and Walker (1996) with a view to
determining their efficacy in training workers with disabilities. They
found that the education system has a much better classification of
students than industry does of employees and that this hinders the help
that Corporations give to employees. This manifests itself in the
integrated corporate classroom. The problem with this is that, in
student’s transition from education to industry, they lose many of the
labels that allow trainers to identify their specific needs. Allen and
Walker (1996) also state that corporate training in industry differs
slightly from teaching in the career and technology classroom, due to
the age difference of the learners. The age aspect is also a factor
when training people with intellectual disabilities to live
independently after years of living in staffed houses. Most of these
individuals are over 40yrs and therefore a training programme
incorporating some of the corporate training techniques might prove
more effective.
Allen and Walker (1996) recommend On the Job Training because it takes
place instantly and at the time it is needed, and Computer Based
Training because it can simulate the required environment, and help the
individual solve the task on the computer before trying to do so in
real life. In practical terms, this means for example, that a person
can practice making an ATM withdrawal on a computer, where mistakes can
easily be corrected, and the environment is secure, before going out to
a real ATM for “On the Job” practice under the trainer’s supervision.
Allen and Walker (1996) also suggest that a reasonable accommodation to39
employees with learning disabilities, can be provided by the trainer at
a minimum expense, e.g., creating an environment with as few
distractions as possible. The trainer must be willing to:
Provide extra time if necessary to the trainee with an
intellectual disability.
Prepare an individual learning plan.
Share in advance the expectations and requirements of the training
with the trainee.
Asking short, one-concept questions.
Breaking down the concepts and procedures into the smallest
possible components, and,
Frequently summarising the content.
Even a small thing like the seating arrangements can help maintain
better concentration by the individual trainees. On the question of
specific training in Social Skills, Sheppard (2006) noted that these
skills are acquired naturally as part of the maturation process. But
for people with intellectual disability, this does not occur in the
same way, and so special training is required. Some researchers
(Chandler and Panaskie, 2004, and Wehmeyer et al, 2004) conclude that
the significant social skills to learn include:
How to listen
Ask questions
40
Consider the needs of others
Compromise
Resolve conflict
Deal with teasing
Stand up for friends, and
Share common interests with peers.
The importance of training in social skills, was highlighted by
Chadsey-Rusch et al (1997) who found that inadequate social skills was
a major cause of job loss for people with intellectual disability.
Therefore, they concluded that it is not surprising that many
vocational and rehabilitative schemes incorporated social skills within
their training.
Chadsey and Bayer (2001) identify two types of approach that have been
used to develop social skills in the workplace. One is a number of
strategies designed to change the social behaviour of workers with
learning disabilities. These include:
Social skill instruction through role play and scripts,
Problem solving strategies,
Self-management using checklists, picture prompts, self-monitoring
of behaviour and tape recorded guides.
41
These strategies can also be applied outside the workplace. The other
approach involved co-workers acting as trainers and social bridges.
Chadsey and Beyer (2001) found the second approach to be the least
effective. This is in contrast to the findings of Curl at al (1992) who
described the training and payment of co-workers to train employees
with a disability, and reported superior outcomes as compared with a
contrast group without co-worker support.
These outcomes included:
A longer average job retention (7.9 versus 3.9 months).
Better employer ratings ( 3.5 versus 2.8).
Less job coach time (10 versus 18 hrs per month).
Mank, Cioffi and Yovanoff (1998) also found that provision of co-worker
training was associated with better outcomes for supported employees
with severe disabilities. The same authors found in a previous study
(1997a, b) that employment practices for supported employees that were
typical of practices for other employees in the same workplace were
strongly associated with better wage and social integration outcomes.
Farris and Stancliffe (2001) found in a study on the co-worker training
model, that there was a high level of co-worker involvement with
supported employees in the co-worker training group. They also found
that this was consistent with the claim by Rogan et al (1993), that
social integration is more successful in work settings where natural
supports are emphasised.
Sharing common interests with peers is one of the significant social
skills required according to Chandler and Panaskie (2004) and Wehmeyer
42
et al (2004), and building on those observations, Peterson and Adderly
(2002) noted that positive peer relationships boost self-esteem, but
Spooner and Wood (2004) have commented that peer relationships can be
adversely affected by poor individual hygiene. Bender et al
(1996) state that teaching skills in personal hygiene to people with
Intellectual Disability can reduce dependence on others, enhance
acceptance in the community and help with developing peer friendships.
It is therefore an important personal development skill, particularly
in the transition from community to independent living.
Sheppard (2006), citing Cook et al (2001) and Gresham at al (2001),
recommend the use of a broader range of instructional strategies and
more opportunities for practice when learning new skills for people
with intellectual disability. These strategies must be frequent and
intense, and linked to student’s specific learning deficits. Examples
are:
Presenting material in a contextually relevant way,
Allowing sufficient time for new learning,
Providing opportunities for deepening understanding by applying
the same skills to different situations.
Using verbal and visual clues (coaching),
Providing multiple demonstrations (modelling),
Using step-by-step instructions with prompting, feedback, and
reinforcement to shape desired skills.
43
Sitlington et al (2000) came up with a nearly identical set of
strategies. Training using repeated opportunities for guided practice
ensures a skill is more likely to be learned correctly, become over
learned and be available in different contexts and situations. (Anctil
and Degeneffe, 2003).
Beyer and Robinson (2009) observed that the nature of the learning
disability has implications for Vocational Training, Learning, and
keeping a job, for the following reasons:
People with learning disabilities have difficulty with reading and
writing, this makes learning the tasks of a job difficult.
Substantial numbers of people will have some difficulty
understanding receptive language, questioning and responding in a
fully appropriate way.
People are heavily dependent on the stimuli in one context or
place. They then find it difficult to take tasks learned in one
place and to generalise them to another. This makes pre training
difficult.
Many people with mild learning disabilities, who cannot respond
fully to verbal instructions, will respond positively to
demonstrations of tasks. People with greater needs will respond to
more detailed demonstration, structured learning, and direct
physical help to carry out the tasks.
44
Beyer and Robinson (2009) also note that task training for people with
learning disability commonly involves breaking down tasks into
component steps and the use of a prompting hierarchy by the trainer to
give just enough information to the person to do the job without
creating dependency.
Social Skills v. Social Problem Solving SkillsSome writers have asserted that Social Skills on their own are not
sufficient to promote full social integration. Loumidis and Hill (1997)
suggest that it is theoretically possible to distinguish between social
skills training and social problem solving skills training. Marchetti
and Campbell (1990) define social skills as” a wide variety of applied
behaviour analytic and intervention techniques aimed at helping clients
to acquire responses which, when displayed during interpersonal
interactions, are deemed appropriate for the situation.” In contrast,
Loumidis and Hill (1997) define social problem solving skills as “the
cognitive behaviour process of discovering an effective course of
action.” Training in this context aims to equip people with
generalisable strategies that can be applied in a wide range of
situations, thus enhancing their skills for coping with future
problems.
D`Zurilla and Goldfried (1971) claimed that this cognitive behavioural
process involved the following components:
Problem identification and definition
Generation of alternative solutions.
Solution evaluation and decision-making.
45
Solution implementation.
Verification.
One of the main benefits of training people with Intellectual
Disabilities in social problem solving skills, as pointed out by
Loumidis (1992), is that successful integration into the community, a
process at the very
heart of normalisation, is less likely to be accomplished unless social
problem solving skills are relatively well developed.
The training programme devised by Loumidis and Hill (1997) differed
from the standard training methods in so far as the objectives were
abstract, therefore the training had to be based on the abstract too.
Participants were presented with seven assessment vignettes and were
then asked a series of questions to gauge their understanding of the
issues raised. The results of the study were inconclusive. When
compared with the social skills training, it is perhaps reasonable to
assume that training for people with disability is more successful when
there is a set of tangible goals to be attained.
The illusion of independenceWhen attempting to define independence, the interpretations of support
service personnel will no doubt be different from those of service
users, reminiscent of the subjective v. objective debate in Quality of
Life measurements. Oliver (1990:84) argues that this unsatisfactory
state is compounded by the terms political connotations: “independence
suggests that the individual needs no assistance whatsoever from anyone
else, and this fits nicely with the current political rhetoric which
stresses competitive individualism. In reality, of course, no one in a
modern industrial society is completely independent. We live in a state46
of mutual interdependence. The dependence of disabled people therefore
is not a feature which marks them out as different in kind from the
rest of he population, but different in degree”. Recently, self
determination has emerged as a key area of outcome for people with a
learning disability, with Wehmeyer (1994) recommending that it should
be pursued through all services and activities.
Rehabilitative Training, according to the “Guidelines for Health Board
Funded Training for People with Disabilities (2001:1), is defined as: “
programmes for people with disabilities that are designed to equip
participants with foundation level social and work skills that will
enable them to progress to greater levels of independence and
integration”. Therefore Rehabilitative Training programmes are
concerned with areas such as:
Personal Development
Community and Life skills
Social and Leisure activities, and
Some Vocational Exploration.
This appears to confirm the belief that Social Skills are the most
important skills to be taught to people with an intellectual disability
who are moving to independent living. It is precisely because they will
not be “independent”, but actually “interdependent” with everyone else
in their community, that they need to be able to blend in effortlessly.
Literacy and Numeracy Training47
While the acquisition of social skills is one of the prerequisites for
social integration, literacy and numeracy are vital for any measure of
independent living, and more so if any form of vocation employment is
envisaged. The organisation for Economic Development and Co-Operation
(OECD, 2000) divides Literacy into 5 levels:
1. People with very poor skills.
2. People who can deal only with very simple material.
3. Roughly the skill required for successful secondary school
completion and college entry.
4/5 People who demonstrate command of higher order information
processing skills.
According to Lacey et al. (2007), most people with learning
difficulties will only reach levels 1 or 2. Teaching literacy skills to
people with intellectual disabilities using text alone is a slow
process with little guarantee of success. However using symbols as an
aid to reading was found to be a more successful approach. Lacey et al.
(2007) found that the importance of symbols as teaching aids was
emphasised by teachers because of their ubiquity in the world in
general. The teachers in the study pointed out that even if the pupils
with learning difficulties were not going to become independent readers
in the conventional sense, they could use their symbol literacy to read
supermarket names, logos, toilet and emergency exit signs etc.
One definition of numeracy is “use of mathematics effectively to meet
the general demands of life at home, in paid work, and for
participation in community and civic life.” (Australian Association of
Mathematics Teachers, 1997). Therefore it is reasonable to assume that
a basic understanding of numeracy will enhance the quality of life and
independence of people with intellectual disabilities. Buckley (2007)
48
defines basic numeracy as the ability to count and calculate with
numbers up to 100. Counting, adding and subtracting are the most useful
operations to understand. In a study by Byrne et al. (2002), the
progress of children with Down Syndrome in learning to count was
compared with non disabled children of the same age range. To learn to
count, children (or adults) with intellectual disability, first have to
learn the “number words” or the “count sequence”, that is, to recite
the numbers 1 to 20 in the correct order. This requires good short-term
memory skills. The object of the teaching is to know that the last word
in the count sequence tells “how many” they have. In the study, it was
found that the children with Down Syndrome had learned a smaller
section of the count sequence than their non disabled peers. Bird et
al. (2001) also noted that the numeracy skills for children with Down
Syndrome were two years behind their literacy skills. Numeracy is a
difficult concept for individuals with Intellectual Disabilities,
particularly, as
Buckley (2007) argues that short term memory is important for learning
longer number sequences and doing mental arithmetic. Many research
studies have shown that there are specific speech, language and working
memory delays associated with individuals with intellectual disability.
Buckley (2007) is also of the opinion that breaking tasks into smaller
steps and giving the opportunity for more practice, is possibly the
best way to reduce memory demands and therefore ensure that learning is
taking place. Task analysis and the breaking down of the process into
smaller steps over a longer period, is deemed to be the most effective
method of teaching /training people with an intellectual disability.
As is evident from the above, it is not sufficient just to create the
right conditions for learning, i.e., time, physical surroundings,
49
innovative teaching aids, and other adjustments. The trainers must also
adopt a
Training approach based on simple clear language, short sentences and
recognition of the danger of information overload. If learning is made
difficult for the learners, their motivation to learn will be
diminished which will in turn reduce the possibility of successful
independent living, with consequences for their ensuing Quality of
Life.
Practical skills required for independent living.The use of pictorial teaching aids, the necessity of task analysis and
breaking tasks down into smaller steps, combined with longer adjustment
periods is a common theme in the literature regarding the training of
people with intellectual disabilities. It is particularly relevant in
the training of practical household skills necessary for independence
in the home.
Food preparation skills are a widely popular objective within training
programmes for people with intellectual disabilities, (Melton 1998,
Rodi & Hughes 2000). Gines et al. (1990), and Schloss et al. (1993)
assert that this is because of the importance of food and drink
preparation skills for independent living. However, as Agran et al.
(1992), and Lancioni et al. (1995,1998) have observed, another reason
for its importance is the usefulness of such skills in areas such as
leisure engagement, and domestic, occupational and work involvement.
Lancioni and O`Reilly (2002) found that the training of food
preparation, in the context of independent living, tended to be more
extensive, highly structured and generally pursuing high performance
targets. Even despite aiming for high performance targets, the actual
teaching seemed to be fairly relaxed, there was no pressure to achieve 50
higher output, rather, the emphasis was on quality and hygiene from a
Health and Safety point of view. The actual teaching methods were based
on systems using pictorial instructions, either on printed cards or on
a computer. Another method used a systematic prompting strategy, and a
combination of time delay prompting to supplement pictorial cards.
The system using pictorial instructions printed on cards constituted
the most widely used approach for teaching chained tasks to people with
Intellectual Disabilities (Johnson and Cuvo 1981, Wacker et al
1985). The pictures serve as permanent cues, which guide the
participants through their tasks step by step (Steed and Lutzker 1997).
Some physical and verbal prompts were required to establish and
reinforce the pictorial cues. Studies by Martin et al. (1982), and
Sanders and Parr, (1989) confirmed the efficacy of these training
methods in relation to the preparation of different nutritionally
balanced meals.
The use of computer programs to teach food preparation has advantages
over the use of cards, particularly in the training of higher
functioning individuals. Lancioni and O`Reilly (2002) note the
advantages as:
Avoiding errors and confusion with the handling of cards.
Dealing with losses of concentration and breaks in performance of
the tasks automatically. (the computer had built in reminders and
encouragements.)
Lancioni et al (1999) used a portable computer to present task
instructions to 4 adults with Intellectual Disabilities. On completion
51
of each step in the process, the trainee pressed a key, (there was only
one key available). This brought on a pictorial representation of the
next step. If the key was not pressed, the computer issued a verbal
reminder after a set period of time. Gradually the pressing of the key
initiated two instructions in sequence. The research showed that the
respondents went from a 10% correct responding rate in the early stages
of training, to 90% correct responding rate post training.
It was also discovered that clustering the task instructions increased
performance, whereas, the withdrawal of the instructions led to lower
performance. The fact that this study involved people with severe
intellectual disabilities confirmed what Simmons and Flexer (1992) said
about the ability of anyone with an intellectual disability to be
trained.
Food preparation was an ideal task in which to test the effectiveness
of these training methods. There is a set sequence to the tasks
involved and there are spaces between the tasks, which facilitates the
use of prompts or cues.
The studies using systematic prompting strategies (Wright and Schuster
1994, Jones and Collins 1997), introduced a time delay of 5 seconds,
during which time, the researcher waited to see if a prompt was
required. The ultimate goal was to have the tasks completed without any
prompting being given. The data showed that this goal was reached for
each of the individuals taking part. The success was further underlined
when it was reported that the task performance was generalised to the
home environment.
Griffen at al. (1992) carried out a study where pictorial cards,
augmented by time delay prompts were used to train a group of
52
adolescents with moderate intellectual disabilities to make milk shakes
and scrambled eggs. A comparison of the 4 training methods showed the
method using the time delayed prompts and the cards with time delayed
prompts were emphatically more successful that the methods using cards
alone, and the computer program, (Lancioni and O`Reilly 2002). Even
allowing for the fact that the levels of intellectual disability were
different in some of the studies, it is still noteworthy that the two
most successful methods involved some interaction with other human
beings as opposed to cards and computers. This perhaps strengthens the
argument for the personal touch when training people with intellectual
disabilities. It also confirms that people with Intellectual
disabilities can be trained in basic food preparation. Those with
higher ability can be trained to accomplish more complex tasks, and in
the area of food preparation, this is another milestone on the road to
true independent living.
ConclusionPrior to the 1970s, there was a belief that having a learning
disability meant that one had little chance of attaining independence
and becoming vocationally productive. (Beyer and Robinson, 2009).
Subsequently, a number of researchers challenged that notion by
demonstrating, that given small scale, individual teaching, people with
learning disabilities could (and should) be taught on the job.
(Bellamy, Horner and Inman 1979, Rusch and Scutz 1979, Wehman, Hill and
Keolher 1979). This effective approach was the use of applied behaviour
analysis and systematic instruction, breaking tasks down into stimulus-
response chains, and using prompting hierarchies and reinforcement to
teach them. (Bellamy, Horner, and Inman, 1979). Simmons and Flexer
(1992) showed that these methods could be used to train people,
regardless of their level of disability.
53

As a result, the training of people with intellectual disability has
become more organised and integrated in many places throughout the
world. A fairly standard set of criteria has been developed to produce
a training strategy that best meets the requirements for training
people with intellectual disability. A typical example of this approach
is the training package developed by the Dept. of Employment, Training,
and Industrial Relations, in Australia in 1999. The core elements of
this training package, which was aimed at non-disabled people also,
could be summarised as follows:
Individual training programmes based on an assessment of learners
needs.
Customisation of the learning resources to suit the learner’s
requirements.
Customisation of the assessment instruments to suit the learner.
Availability of the necessary support personnel or equipment
required to achieve competency, .e.g., interpreters for the deaf,
literacy and numeracy tutors.
Extension of time to develop competency if required.
All the above were incorporated into an accredited Training Programme
called the Certificate 1
In Workplace Preparation and Practices, by the D.E.T.I.R. in 2000. This
programme was built on a number of key elements:
54
1. An initial pre-assessment to identify literacy and numeracy needs
and learning pathways.
2. Formulation of a personal learning plan.
3. Regular reviews of the personal learning plan to ascertain
competency attainment.
This training product is designed to formulate programmes that increase
confidence and competency in:
Communication skills
Techniques to develop life long learning.
Personal skills and knowledge.
Job seeking and retention skills.
Work readiness skills.
Entry level vocational skills.
The acquisition of, and proficiency in these skills should enhance the
quality of life of people with intellectual disabilities by maximising
the potential for successful independent living. However, a couple of
issues need to be raised in this context; the foregoing would appear to
suggest, that because of the specific needs of individuals with
Intellectual Disabilities in regard to training, specialised rather
than mainstreamed settings appear to offer the best chance of a
successful outcome. However, with integration in to the community as
55
the ultimate goal, how effective can the teaching of social skills be,
if done in segregation from the rest of society? It is acknowledged
that the acquisition of Social Skills is required above all other
skills, if the person with Intellectual Disability is to live
independently. But as Oliver (1990) has intimated, real independence
can be isolating which does not lead to any gains in Quality of Life.
Therefore the ideal goal is one of training for interdependence, where
individuals are trained how to behave in society and also how to ask
for help when it’s needed.
Lozano (1993) has argued that training of itself is not sufficient to
encourage integration, it is the need to
use this training which requires interaction with the wider community
and also forces retention of what has been learned to-date. When staff
are withdrawn, people with Intellectual Disability have to fend for
them selves or go without. The training they have received gives them
the foundation skills to build upon. Lozano (1993) found that the real
experience of independent living accounted for improvement or
maintenance of skills, not the amount of independent living skills
training. Similarly, Levine and Langness (1985) found that competence
at Supermarket shopping was unrelated to age, sex, IQ, or amount of
training. They found the most competent shoppers were those whose
circumstances required them to shop independently as adults. Therefore
it would appear that the most effective training for social and other
skills is in a real world setting. Stancliffe and Keane (2000) assert
that integration and interdependence provide this setting because more
opportunities for participation are found in ordinary domestic and
community environments. This confirms Rapleys (2000) argument that
being “of “ the community is more likely to lead to a better Quality of
Life than merely being “in” the community also confirms why Cummins
found the following 3 Domains, interpersonal relations, social
56
inclusion, and personal development, to be the most important
ingredients in the quest for Quality of Life.
SummaryThis first part of this chapter explored the relevant literature on
Quality of Life and its evolution from a general measurement of
economic well-being of a whole population, to its application to
specific sections of the population such as people with Intellectual
Disabilities. In addition the change in focus from economic indicators
to social indicators led to an investigation as to what brought
satisfaction to an individual on a personal basis, and to a debate as
to whether the opinions of the individual or a third party speaking on
behalf of the individual were more important. This part concluded with
a discussion on the Domains that constitute daily living activities and
how best these can be measured to provide data on individual’s Quality
of Life, and which is the most appropriate measuring instrument.
The second part of this chapter examined how the segregated education
and training of people with intellectual disabilities became the
preferred method of education and training, after the mainstreaming/
integrative approach was found to be deficient. Continuing with an
examination of the various types of training environments available to
people with intellectual disabilities, from Hospital Therapy Units
through Vocational Educational and Training initiatives to practical
skills training for independent living, and concluding with a review of
practical training methods designed to enhance the effectiveness of
training people with Intellectual Disabilities.
57
Chapter 5Methodology
IntroductionThe purpose of this study was to examine the Quality of Life gains for
10 individuals with Intellectual disability, who had recently moved out
from community houses in to their own apartments and who were receiving
specific training to allow them to live independently. There are 9
males and 1 female, all in the High Moderate category of intellectual
disability. They range in age from 40yrs to 69 yrs. All had been in the
service for at least 25yrs (25 years for the youngest to 40 years for
the oldest). In the service means they lived in an institutional
setting before moving to a Community House as part of the change to
Social Model of Care. All had been living in staffed community houses
for an average of 20 years before being deemed suitable to live
independently in the community, with supports from the organisation and
through participating in a comprehensive training programme designed to
equip them with the necessary skills for successful independent living.
The training was designed to provide them with:
Improved Social and Communication skills.
Literacy and Numeracy Skills.
Money Management and Shopping skills.
Basic Cooking and Baking skills.
Use of Public Transport.
58
Health and Safety inside and outside the home.
Personal Hygiene skills.
HypothesisIn this study, I wish to test the Hypothesis that people with an
intellectual disability who move from community living into semi-
independent living and, who receive appropriate living skills training,
will experience positive quality of life gains. The purpose of the
training is to help the participants to achieve a level of independence
much greater than what they were used to. There are two variables here
that can affect the outcome. One is the fact that by merely being
allowed to make decisions for themselves and not live a regimented
existence will be sufficient to increase their quality of life by their
own perceptions. This will be measured against the Western Normative
figures as found in other studies using Cummins PWI-ID (2005). The
second variable to be considered is the daily living skills training
programme, and whether this will enhance the experience of independent
living and thus bring further Quality of Life gains.
The objective of this study is to gather data, against which future
studies of this same group, or other groups embarking on the same
programme of independent living, can be compared. The sample size was
too small to generalise to the wider population, but that was not the
objective. Also as this is the first group to move out to independent
living and receive this specialised training, there was no other
similar group to compare with.
59
In trying to ascertain which research philosophy is best suited to this
particular research, I used the following list of attributes to guide
me:
This is a study of human beings and how they perceive changes that
have occurred in their lives.
These changes will involve intangibles such as their opinions and
feelings.
The depth of these opinions and feelings will be quantified on to
a Likert type scale.
The reality of the changes in circumstances (some found it harder
to adjust to spending time on their own than others).
All went through the same training programme.
The degrees of satisfaction or dissatisfaction may differ between
individuals depending on their perceptions.
The differing degrees of satisfaction and dissatisfaction can be
measured quantitatively to determine whether the theory being
tested is valid.
Literature ReviewA review of the comprehensive body of literature on Quality of Life
revealed that Quality of Life as a concept was difficult to define with
any absolute definition that satisfied all researchers concerns, but
one (Cummins 1997) was found to be more acceptable than the others. 60
There was also debate over the actual conditions (domains) deemed to
contribute to Quality of Life, but on closer examination, a common
theme emerged regarding what aspects of an individuals life, when
measured, provided an indication of that individuals satisfaction with
his/her life in general.
The review of the literature on the Training of people with
Intellectual Disability showed that the desire to promote equality
through mainstreaming of training and education, while praiseworthy
from an inclusivity point of view, was not as effective in addressing
the education and training needs of people with Intellectual
Disabilities. A dichotomy emerged whereby formal education and training
was more effective in a segregated setting, but the most effective
informal learning took place when having to interact with the wider
community out of necessity. This interaction, through social
integration, and active participation in the community, emerged as the
catalyst for both ongoing learning and increased Quality of Life
Research PhilosophyTherefore, as this research will attempt to test the theory that
training will enhance the quality of life of people with intellectual
disabilities who have recently moved to independent living for, by
measurement of facts (i.e., how respondents assign numbers to portray
their thoughts and feelings), it seems to fall within the Positivist
Research Philosophy. Burrell and Morgan (1985:4) have described the
Positivists view of social existence as treating reality as an external
61
fact, independent of us as individuals, therefore comprising of “hard,
tangible, immutable structures”.
The questions being asked will draw on the personal feelings and
subjective observations of the respondents, which may indicate a strong
link to Interpretivist Research Philosophy. However, in this research,
the respondent’s subjective evaluations of how they feel at a
particular point in the training may or may not reflect how they will
feel at a future point. The Hypothesis is based on an assumption that a
positive change in people’s lives (positive in the objective opinion of
third parties) will bring positive outcomes. But Creswell (2003:7) has
stated “we cannot be “positive” about our claims of knowledge when
studying the behaviour and actions of humans”. If this Hypothesis is
the starting point, the fundamentals of the Positivistic approach
namely: that is logical, objective, rational, replicable and capable of
being generalised to the wider population (CLMS notes 2-11) would be an
appropriate approach to Theory Testing.
Having established that there are elements in this research where both
Positivist and Interpretivist Philosophies have relevance, it would
seem to present a problem as both Philosophies differ fundamentally in
approach. This is not the case, and as Stiles (2006) has argued, the
two aims of gathering facts and values are actually compatible if a
Post Positivist theory building approach is taken (CLMS notes 2-14).
The Post Positivist researcher assumes a learning role rather than a
testing one (Ryan 2006, citing Agar 1988: 12). Wolcott (1990: 19)
claims that the Post Positivist researcher regards himself or herself
as someone who conducts research among other people, learning with them
rather than conducting research on them. Stiles (2006) further states
that this Post Positive approach can complement and be enhanced by, the
62
“enriching “ approach, which aligns more with the Interpretivist
Philosophy of Research.
Therefore, the outcomes to be determined in this research cannot be
reduced to the simple questions of “are you happy or unhappy?” This
yes or no type response would produce raw quantifiable data but it
would be insufficient to draw any further conclusions to expand the
hypothesis. The important question here is, not simply whether one is
happy or unhappy, but the degree to which one is happy or unhappy. The
answers to these questions, when presented on a scale, will give an
insight into the feelings and subjective perceptions of those being
interviewed.
MethodologyThe Quantitative methodology as described by Patton (1997:213) whereby
the focus is on the measuring of things that can be counted using
predetermined categories and subjected to statistical analysis, is
wholly appropriate in this instance. The actual survey is structured
and so provides statistics, which will be applied to a Quality of Life
scale. The results will either agree or disagree with the Hypothesis.
However, the questions do not have merely yes or no answers; the
answers will depend on the feelings and perceptions of the respondents
at the time. The questions relation to the Training programme will
create another complementary element of the research. In the case of
multiple-choice answers similar to a Likert Scale, while the answers
may be represented numerically, the choice of answer is dependent on
the respondents’ feelings, values, and frame of mind at that particular
time.
Punch (1998: 29) defines Quantitative research as using numerical data
and typically structured and predetermined research questions, 63
concepts, frameworks and designs. According to Bryman (1998),
quantitative methodologies can be used to test hypotheses, which are
invariably assumed to take the form of expectations about likely causal
connections between concepts, which are the constituent elements of the
hypothesis. In the context of this research, the focus is narrow, which
Kumar (2005) and Punch (1998) agree is one of the hallmarks of
quantitative research.
Punch (1998) also permits that quantitative research can also be used
in more “naturalistic “settings, where the researcher collects data in
everyday settings rather than “contriving situations for research
purposes”. In this case, a quantitative methodology is consistent with
a Post Positivistic epistemology as it fulfils the requirement of being
a standardised approach, which can be reported clearly and replicated
easily. (CLMS notes 2-33)
SamplingThe individuals chosen to take part in this research were chosen on the
basis of purposive non-probability sampling, meaning that they were
chosen because they fulfilled a specific set of criteria. A total of 15
individuals with the highest levels of ability in the service were
chosen to receive training in independent living skills and to commence
living independently. 5 declined to participate in the study and 10
agreed. The group I decided to study were similar in so many ways that
they conform to what Patton (1990:82) calls Homogenous Sampling and
it’s this similarity that makes them such appropriate subjects for this
research. Glaser and Strauss (1967) also commented on the homogeneity
of research samples, stating that minimising the differences between
members of a sample may make the early stages of theory development
more streamlined by reducing the possibilities of variation. 64
Even with such a small number as 10 participants, Raddon (2006) claims
that this number is capable of producing accounts and knowledge which
will resonate with the wider population and expand our understanding of
the issues being researched. Therefore, as Raddon (2006) suggests, the
data gleaned from small samples is capable of being generalised to a
wider population. As the practice of preparing people with intellectual
disability for independent living through appropriate training
programmes is a relatively new phenomenon, the data on whether they
themselves consider this training suitable and quality of life
enhancing, would be of interest when other such initiatives are being
planned.
A non probability sampling method can have advantages over
representative sampling in the areas of cost and ease of use (CLMS
notes 2-31) This was a bonus in this research, but under the
circumstances, bearing in mind the purpose of the research, random
sampling was not an option. According to Pole and Lampard (2002) non-
probability sampling is often used where the aim is not to generalise
the results to the wider population which is true in this case.
Limitations of Sample SizeThe total number of people, who could have been included in this study
because they fulfilled the criteria, was only 15. In the end 10 agreed
to take part. The conditions I wished to study were quite specific to
these, that is, they recently moved to independent living. Therefore,
it was not possible, nor was it the intention to apply the findings to
the wider population of people with mild Intellectual Disability. Even
within the specific group of 15, one third elected not to participate,
and it was also not possible to generalise the findings of the two
thirds who did take part to the whole group. As, previously stated, the65
aim of the study was to measure the effects of the living skills
training on the Quality of Life of this group.
EthicsEthics refers to rules of conduct, typically to conform to a Code or
set of principles (Reynolds, 1979).
Permission
As Denscombe (2010) notes, although responsibility rests with the
researcher, increasingly, the consent of the organisations Ethics
Committee must be sought and it is so in this case. I sought and was
granted permission from my organisations Ethics Committee, making the
case for the project and that the participants will not be adversely
affected by participating in the research.
Informed consent
In doing research with people with Intellectual Disability, the
question of an Ethical approach is a vital consideration because of the
nature of the people being surveyed and whether or not they understand
what’s being asked in order to give informed consent. Individuals who
provide informed consent indicate that they understand the basis of the
project and their willingness to take part. In order for this to
happen,
the person must be given balanced and accurate information about the
project. The person must be capable of making a decision about
regarding part in the project and that choice must be voluntary without
coercion or pressure. On the question of obtaining informed consent
from people with Intellectual Disability, Herrera (1999) asks, “Is
their consent fully informed?” Under such circumstances, researchers
66
may resort to covert methods, but Clarke (1999) counsels against this
and this highly unethical practice was definitely not used in this
project. There were no covert methods employed to persuade individuals
to participate in this study and assurances were given that no
information that could be used to identify either the participants or
the organisation would be disclosed.
Negotiating participationThis is difficult when researching issues affecting people with
Intellectual Disability. In the case of my particular research project,
some of the people I wished to survey did not fully understand the
purpose of the research and how it will impact on them. In recognition
of this, and as recommended by the Ethics Committee, I produced an Easy
Read consent form where the questions were asked in simple, easily
understood words and supplemented by graphical illustrations. (See
Appendix 1). When it was clear that the individuals understood what was
being asked of them, only then were they asked to sign the form. While
it is proper to approach the people involved on an individual basis, as
adults entitled to speak on their own behalf, their participation will
still have to be made known to their guardians or next of kin, at least
out of courtesy, as recommended by Esbensen at al. (1996).
Co-operationObtaining the cooperation of the next of kin was not necessary in this
case, as the Ethics Committee were of the opinion that all those I
wished to interview were adults and capable of deciding for themselves
whether they would participate or not. However, it was courteous to
inform the next of kin of my intention to request the cooperation of
their family member, which I duly did. A copy of the letter is included
in Appendix 2. I also included an information letter detailing the
nature of the study and appraising them of its value and how it relates67
to their family member and to the wider intellectually disabled
community (Appendix 3). I sought to emphasise that the participants
will not be pressurised in any way during the process, that I do not
have an agenda and am not looking for specific answers. I merely wanted
them to be at their ease and talk to me like they always do. Since I am
known to all those I surveyed, as I meet with them occasionally in
their own homes, and informally in other places, they were used to me
asking questions like;” Is everything ok?, Are you happy? How are you
getting on? However I do not work directly with them, I deal mainly
with the staff, but also with the families quite a lot and it’s always
in the context of seeking to improve the quality of life of the service
users. Therefore, the question of cooperation was not an issue, and in
the context of this research the goal was to measure whether these
changes have brought about a better quality of life. Because I do not
work directly with the participants, our relationship has been one of
friendship rather than authority. They were never intimidated by me and
therefore never showed any acquiescence when speaking with me in the
past and therefore I did not expect this to be an issue in this
research. In fact, this was proved when 3 said they did not want to
take part and felt free to say this to me.
CredibilityThe fact that this research was carried out as part of Academic
research was important in bestowing it with credibility in the eyes of
the Ethics Committee. However, as Bell (1997) remarks, the organisation
needs to know what exactly they will be asked to do, what use will be
made of the information they provide and that the research is
legitimate and of value. All this information was supplied to the
Ethics Committee when seeking their approval
68
Legality This research was carried out legally, which means it did not commence
until my Organisations, and the University of Leicester’s Ethics
committees granted permission to proceed
Context of the ResearchThe interviews were conducted in the service user’s apartments at a
time that was convenient for them. Generally this was after tea in the
evenings when they were relaxed, and this was also the time they were
most used to seeing me call. I gave all those taking part prior notice
before calling to do the interviews. Therefore, the question of
cooperation was not an issue, as the context of this research is to
measure whether these changes have brought about a better quality of
life.
Bias and AcquiescenceAs the interviews were conducted using Cummins PWI-ID 2005, which is a
questionnaire with preset questions, the interviewer had no control
over the formulating of the questions and therefore was not in a
position to influence either the way the questions were worded or how
they were asked. The questions were designed to be simply understood
and requiring little or no further explanation.
A test for acquiescence is built in to the measuring instrument which
tests whether or not the respondent is likely to agree with the
question whether it is true or not. If this happens, no further testing
can take place
as the respondent has failed the acquiescence test. A further safeguard
against acquiescent responses is the fact that the respondent has to
69
justify his/her answer by choosing the degree of agreement/
disagreement on a numerical scale.
Structured Interview - Personal Well-being Index-Intellectual
Disability (PWI-ID)The PWI-ID was used in this study as the primary outcome measure of
subjective QOL also known as subjective well-being (SWB). It was
administered in the form of a structured interview. The aim was to
interview each participant twice using this scale. The following
information was extracted directly from the PWI-A Manual (International
Well-being Group (IWB), 2006) and the PWI-ID manual (Cummins & Lau,
2005), which gives details of the history and evolution of the
instrument, and also the rationale behind the methodology used in data
analysis.
Historical Development of the Personal Well-Being Index (IWB,
2006)The PWI scale was created from Cummins' (1997b; 1997c) original
Comprehensive Quality of Life scale (ComQol) (Cummins, McCabe, Romeo &
Gullone, 1994). The ComQol comprised both an objective and subjective
measure of life quality. In 2001, the ComQol was discontinued because
of two major flaws. One was that, despite repeated modification, 21
items on the objective scale did not factor in as intended. Secondly,
the use of importance as a weighting for client satisfaction was found
to be invalid. (Townsend-White. 2011) The reasons for the
discontinuance of the ComQol are available in Cummins (2002).
A major difference between the PWI and ComQol is the change in the
response scale format. This involved the replacement of the original 7-
70
point Likert scale with an 11-point Likert Scale. There were several
reasons for this decision, the details of which have been described in
Cummins and Gullone (2000). The 11-point (0-10) choice is preferred as
it optimises respondent discriminative capacity and is simple to
understand.
The Personal Well-Being Index (Cummins & Lau, 2005)The PWI was developed to measure the subjective dimension of QOL, also
known as subjective wellbeing (SWB). It is generally agreed that SWB
can be measured through questions of satisfaction directed to people's
feelings about themselves. The PWI is designed as a simplification the
concept of QOL. It is based on a global, abstract question - "How
satisfied are you with your life as a whole?"
This scale can be used with many sections of the population. There are
three versions of the adult PWI (PWI-A). The PWI-PS is for use with
children and adolescents attending school, PWI-PS is for pre-school age
children, while PWI-ID is designed for people who have an intellectual
disability or another form of cognitive impairment. For this research,
the PWI-ID version was used.
The Personal Well-being Index - Intellectual DisabilityThe PWI-ID scale differs from the PWI-A in that it incorporates a pre-
testing protocol to determine whether, and to what level of complexity,
respondents understand the scale. Questions on 'satisfaction' from the
PWI-A are substituted by the term 'happiness' in the PWI-ID scale.
While these two terms are not equivalent, they yield very similar data
(Lau, Cummins & McPherson, 2005). The ID version also uses simpler
wording. An additional question, which asks how happy or sad the
respondent is with life as a whole, is included. A reduced choice 71
format, illustrated as a series of faces, from very sad to happy, can
also be used if participants cannot cope with the Likert scale format.
In addition, the sixth question of the PWI-A, which taps into SWB of
‘community connectedness’, was changed in the PWI-ID. This concept was
considered too complex and abstract. In the current PWI-ID scale, the
question "How happy do you feel about doing things outside your home?"
replaces "How satisfied are you with feeling part of your community?"
in the PWI-A version. This question attempts to ascertain the level of
satisfaction that the person feels at being part of their community.
The PWI is very similar in structure to the original subjective ComQol
sub-scale. The psychometric performance of each is also much the same.
The satisfaction scores from all domains are simply summed to produce a
mean satisfaction value, known as the PWI.
The PWI is also unique because it is embedded in the Australian Unity
Wellbeing Index, which has been used since 2001 in regular quarterly
surveys of the Australian general population to measure how satisfied
people are with their lives. The scale has demonstrated extraordinary
stability over time, and continues to prove to be a valid, reliable and
sensitive instrument (Cummins et al. 2007). In addition, McGillivray et
al
(2009) found that Cronbach lies between 0.7 and 0.8, and the seven
domains of the scale form a single stable factor that predicts over 50%
of the variance in ‘satisfaction with life as a whole’. The extensive
use of the scale as part of the Australian Unity Wellbeing Index
provides data from the general population that can be used to norm-
reference findings obtained from sub-populations such as people with
ID.
72
Measuring Quality of Life using the PWI-IDThe PWI-ID measures life satisfaction across 7 areas of every day life,
called domains. A Likert scale forced response format is then used to
indicate the person's level of expressed satisfaction. The strength of
this approach derives from the unambiguous wording of the questions
(CLMS notes 3-20), and also in this context, the use of Liker Scale is
likely to provide reliable responses as Hartley and MacLean (2006)
found that individuals with borderline to mild Intellectual disability
responded more consistently to Liker Scales than those with moderate to
severe Intellectual Disability. Here, questions refer to specific life
domains (life aspects) and the scores are averaged to produce a global
measure of SWB.
There are 7 items in the scale.
These include:
standard of living;
health;
life achievement;
personal relationships;
personal safety;
community connectiveness;
future security.
73
Evidence for the adoption of these seven domains has been presented by
Cummins (1996); Cummins (1997); Cummins (2005); Cummins, McCabe, Romeo,
Reid and Waters (1997).
In this study, responses from the PWI-ID will be measured
quantitatively using the guidelines in Cummins and Lau (2005).
Using the PWI-ID in preference to any other measuring tool.A clear advantage of the PWI scale is that while it has been used
predominantly in the general population, there is a parallel version
(PWI-ID) designed for people who have ID or other forms of cognitive
impairment. To date, however, no studies have described or demonstrated
the use of the PWI-ID. Therefore, the first aim of this paper is to
introduce and describe the PWI-ID as an appropriate tool for the
measurement of SWB in people with ID. It is unique amongst SWB scales
because, in addition to the availability of parallel versions,
it includes a well-structured pre-testing protocol to determine
whether, and to what level of complexity, respondents with mild or
moderate ID are able to use it. This ensures that individuals, whose
response to scales is unlikely to be valid, such as those with severe
or profound ID, are excluded from the sample (Sigelman et al. 1981;
Chadsey-Rusch et al. 1992; Petry & Maes 2006).
The PWI-ID appears to be the most reliable and valid measurement
instrument for use with intellectual disabilities in use at the present
time (Cummins & Lau, 2005). In Australia, the scale has yielded a
Cronbach α of 0.76 for persons with Intellectual Disability and 0.80
for the population in general. In a study of the Utility of the PWI-ID,
McGillivray et al (2009) found that “the seven domains individually met
the criterion for inclusion within the scale by contributing
significant unique variance to the prediction of satisfaction with life74
as a whole. The PWI-ID scores obtained from the different response
formats did not differ significantly, which indicates that when
combined into one sample, they did not falsely over- or under-state the
PWI score. Thus, it can be concluded that the PWI-ID is reliable and
valid for individuals
with mild and moderate levels of ID. Further, its psychometric profile
identified previously amongst the general population has been confirmed
in the present study.”
From these findings, it appears that the PWI-ID fulfils the statistical
requirements of being reliable and valid (Cummins et al., 2009). The
particular strengths of this scale are that its construction is
theoretically embedded and that its output can be compared with
normative values. It is also unique among scales of this type in having
a pre-testing protocol that attempts to ensure that the people who
complete the
questions of satisfaction have the intellectual capacity to do so
reliably. According to Cummins et al. (2009:13), the "PWI-ID represents
the state of the art for the measurement of SWB for people with an
intellectual disability".
SummaryIn this chapter, the methodological design and related issues have been
discussed in some detail. It has presented the method used to gather
the data to answer the research question identified from the
Literature. The rationale for the study has been discussed and I have
explained how the process unfolded. The nature of the data gathered and
the approach to analysis were discussed. In the next chapter, the data
is analysed and discussed.
75
Chapter 6Data Interpretation.Interviews were held with the 10 individuals in their own homes. Each
interview took approximately 1 hour to complete. After pretesting with
the 3 and 5 point scales contained in the PWI-ID to determine the
participants’ level of understanding and to screen for acquiescent
responding, it was deemed appropriate to use the 11 point scale for the
interviews. See Appendix 4 for an example of the 11 point scale
reproduced in simple terms.
According to Cummins (2005). “the data derived from the Personal
Wellbeing Scale may be used either at the level of the individual
domains or the domain scores may be aggregated to form the Personal
Wellbeing Index.” In the PWI-ID (2005), Cummins presents two methods
for analysing the data derived from the questionnaire using the means
of the domain scores. One method relates to the scores of individual
persons whereby these can be referenced to the normal distribution of
individuals within a population. The Australian normative range for
individuals is 50-100 points.
The other method is referencing the mean score of a group to the normal
distribution of group means. The points are calculated by taking the
data from the 11 point Likert scale and moving the decimal point one
step to the right e.g. a value of 6.0 becomes 60 points, thereby 76
standardising the units into Percentages of Scale Maximum (%SM) on a 0-
100 distribution.
The full questionnaire comprising of 8 Quality of Life questions and 10
Training questions can be found in appendix 5.
According to Cummins (2005), the normative range for Western means is
70-80 points compared with 73.4-76.4 points for Australia. Using the
above methods of interpretation, the total group mean was calculated to
be 79.67 points which was within the normative range for Western group
means of 70-80 points. (The group means for Quality of Life and
Training which were 79.37 and 79.9 respectively were also within the
Western normative range.)
Taking the scores for individuals spread over all the domains, the
scores ranged from 70 points to 92 points, which were within the
Australian normative range for individuals of 50-100 points. See
Appendix 6 (Excel Sheet)
Table 1
77
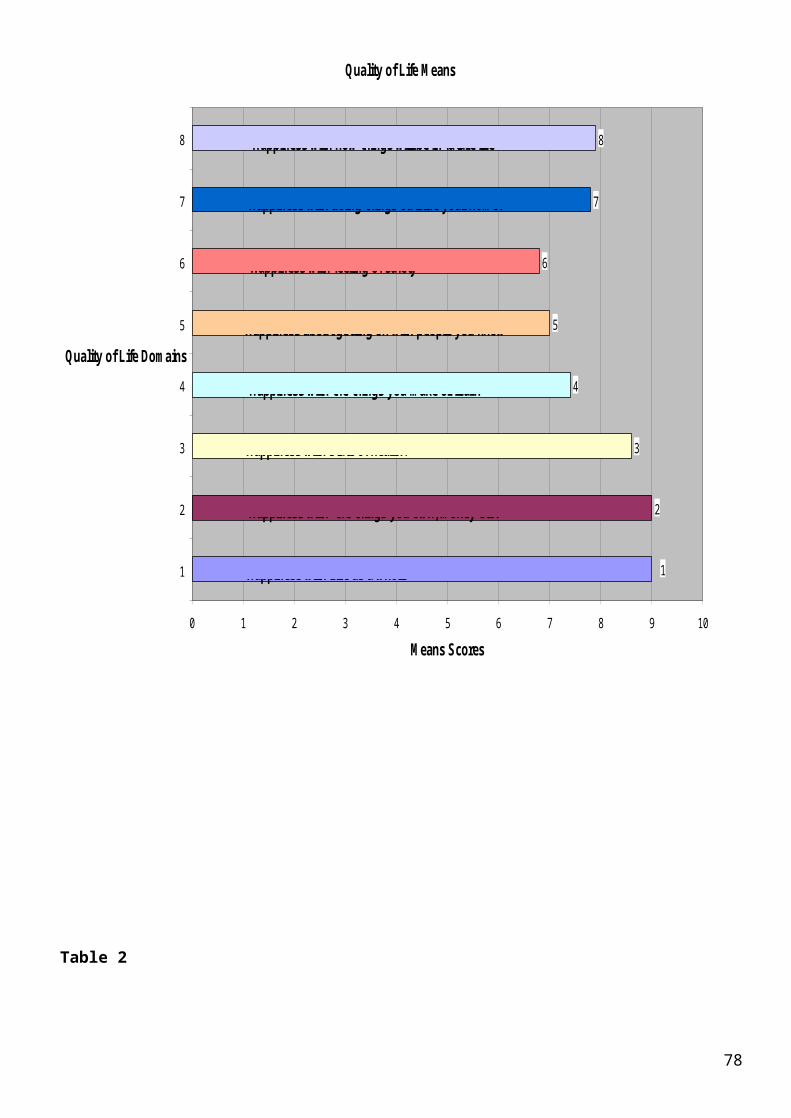
Quality of Life M eans
2
3
4
5
6
7
8
1
0 1 2 3 4 5 6 7 8 9 10
1
2
3
4
5
6
7
8
Quality of Life Dom ains
M eans Scores
Happiness with the things you m ake or learn
Happiness with Life as a whole
Happiness with the things you own, m oney etc.
Happiness with state of health.
Happiness about getting on with people you know
Happiness with feeling of safety
Happiness with doing things outside your hom e.
Happiness with how things will be in future life
Table 2
78
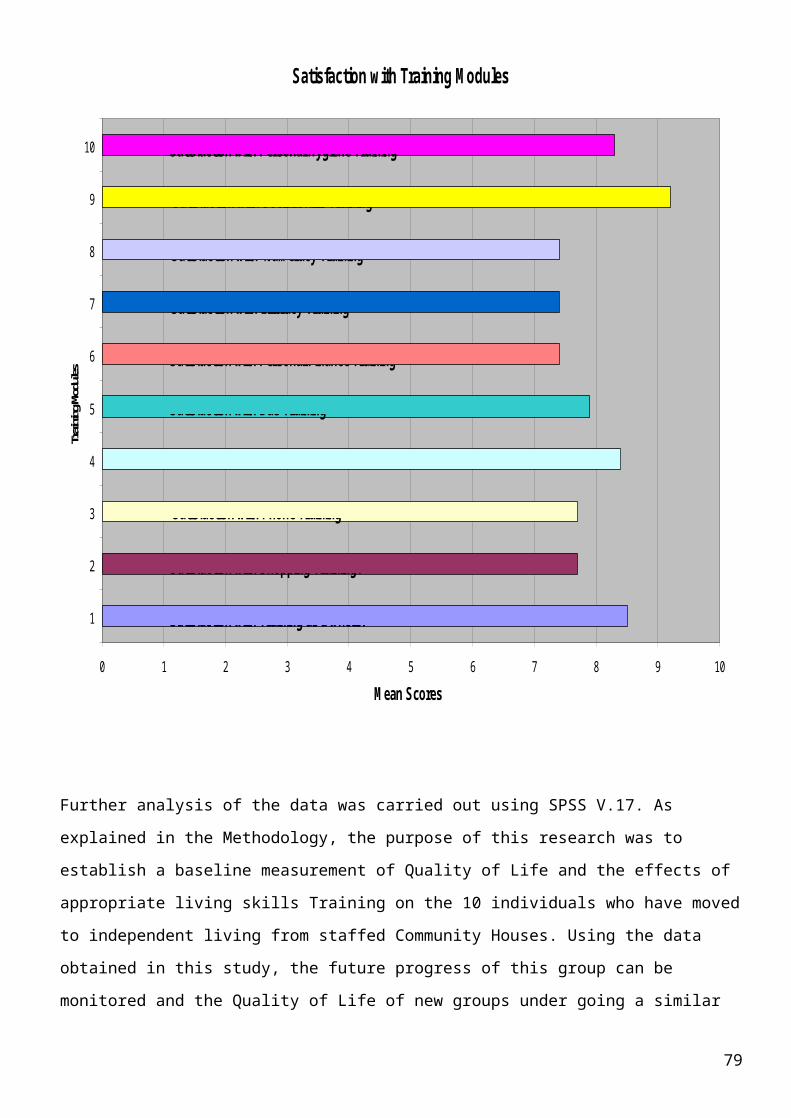
Satisfaction w ith Training M odules
0 1 2 3 4 5 6 7 8 9 10
1
2
3
4
5
6
7
8
9
10
Training Modules
M ean Scores
Satisfaction with Training as a whole.
Satisfaction with Shopping Training.
Satisfaction with Phone Training
Satisfaction with Cookery Training
Satisfaction with Bus Training
Satisfaction with Personal Finance Training
Satisfaction with Literacy Training
Satisfaction with Num eracy Training
Satisfaction with Social Skills Training
Satisfaction with Personal Hygiene Training
Further analysis of the data was carried out using SPSS V.17. As
explained in the Methodology, the purpose of this research was to
establish a baseline measurement of Quality of Life and the effects of
appropriate living skills Training on the 10 individuals who have moved
to independent living from staffed Community Houses. Using the data
obtained in this study, the future progress of this group can be
monitored and the Quality of Life of new groups under going a similar
79
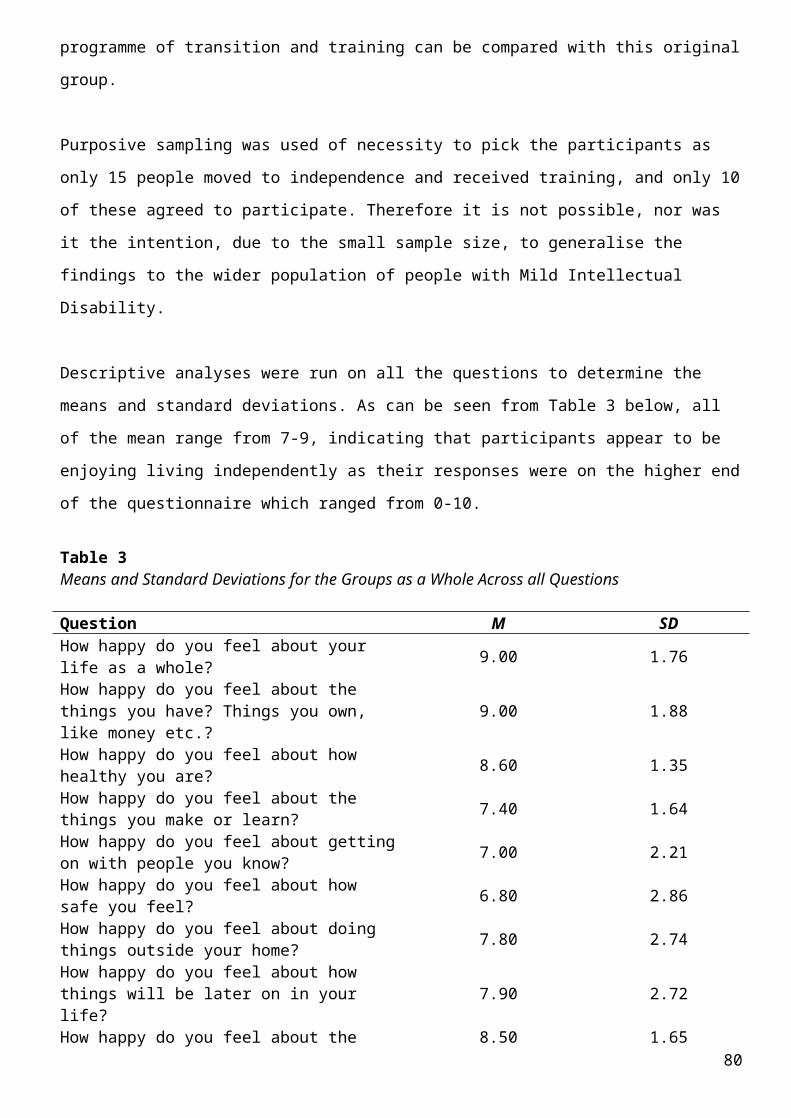
programme of transition and training can be compared with this original
group.
Purposive sampling was used of necessity to pick the participants as
only 15 people moved to independence and received training, and only 10
of these agreed to participate. Therefore it is not possible, nor was
it the intention, due to the small sample size, to generalise the
findings to the wider population of people with Mild Intellectual
Disability.
Descriptive analyses were run on all the questions to determine the
means and standard deviations. As can be seen from Table 3 below, all
of the mean range from 7-9, indicating that participants appear to be
enjoying living independently as their responses were on the higher end
of the questionnaire which ranged from 0-10.
Table 3Means and Standard Deviations for the Groups as a Whole Across all Questions
Question M SDHow happy do you feel about your life as a whole? 9.00 1.76
How happy do you feel about the things you have? Things you own, like money etc.?
9.00 1.88
How happy do you feel about how healthy you are? 8.60 1.35
How happy do you feel about the things you make or learn? 7.40 1.64
How happy do you feel about gettingon with people you know? 7.00 2.21
How happy do you feel about how safe you feel? 6.80 2.86
How happy do you feel about doing things outside your home? 7.80 2.74
How happy do you feel about how things will be later on in your life?
7.90 2.72
How happy do you feel about the 8.50 1.6580
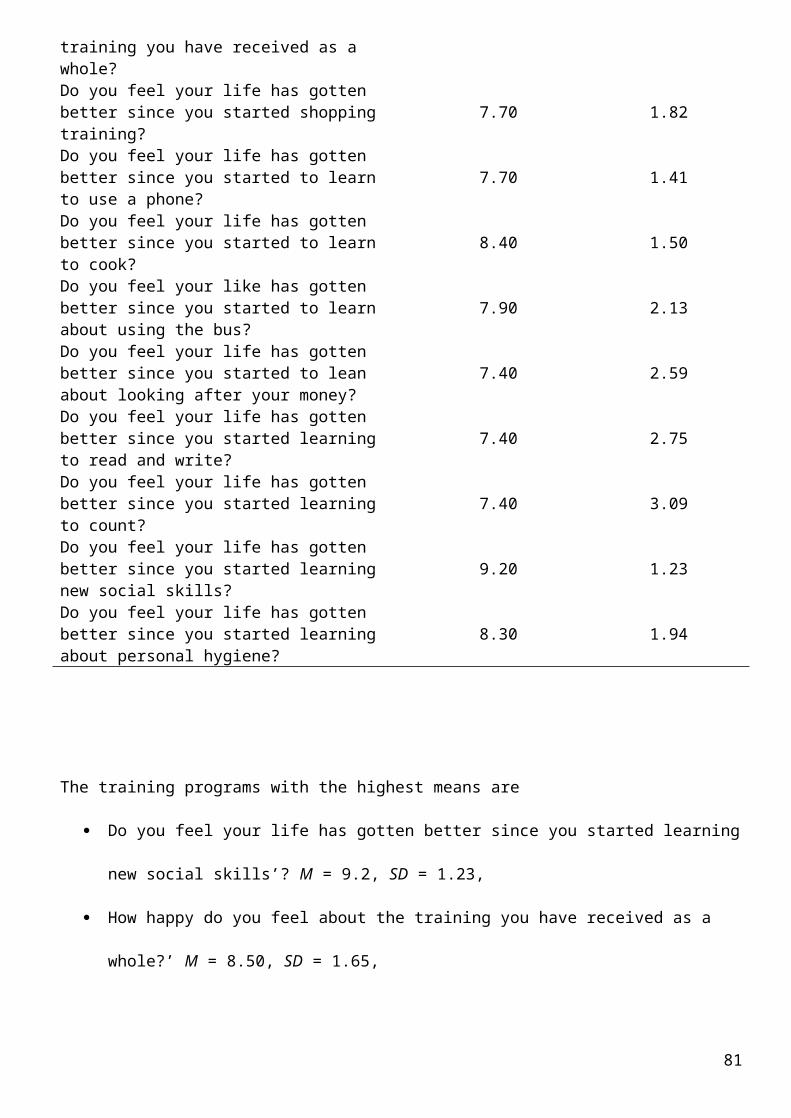
training you have received as a whole?Do you feel your life has gotten better since you started shopping training?
7.70 1.82
Do you feel your life has gotten better since you started to learn to use a phone?
7.70 1.41
Do you feel your life has gotten better since you started to learn to cook?
8.40 1.50
Do you feel your like has gotten better since you started to learn about using the bus?
7.90 2.13
Do you feel your life has gotten better since you started to lean about looking after your money?
7.40 2.59
Do you feel your life has gotten better since you started learning to read and write?
7.40 2.75
Do you feel your life has gotten better since you started learning to count?
7.40 3.09
Do you feel your life has gotten better since you started learning new social skills?
9.20 1.23
Do you feel your life has gotten better since you started learning about personal hygiene?
8.30 1.94
The training programs with the highest means are
Do you feel your life has gotten better since you started learning
new social skills’? M = 9.2, SD = 1.23,
How happy do you feel about the training you have received as a
whole?’ M = 8.50, SD = 1.65,
81
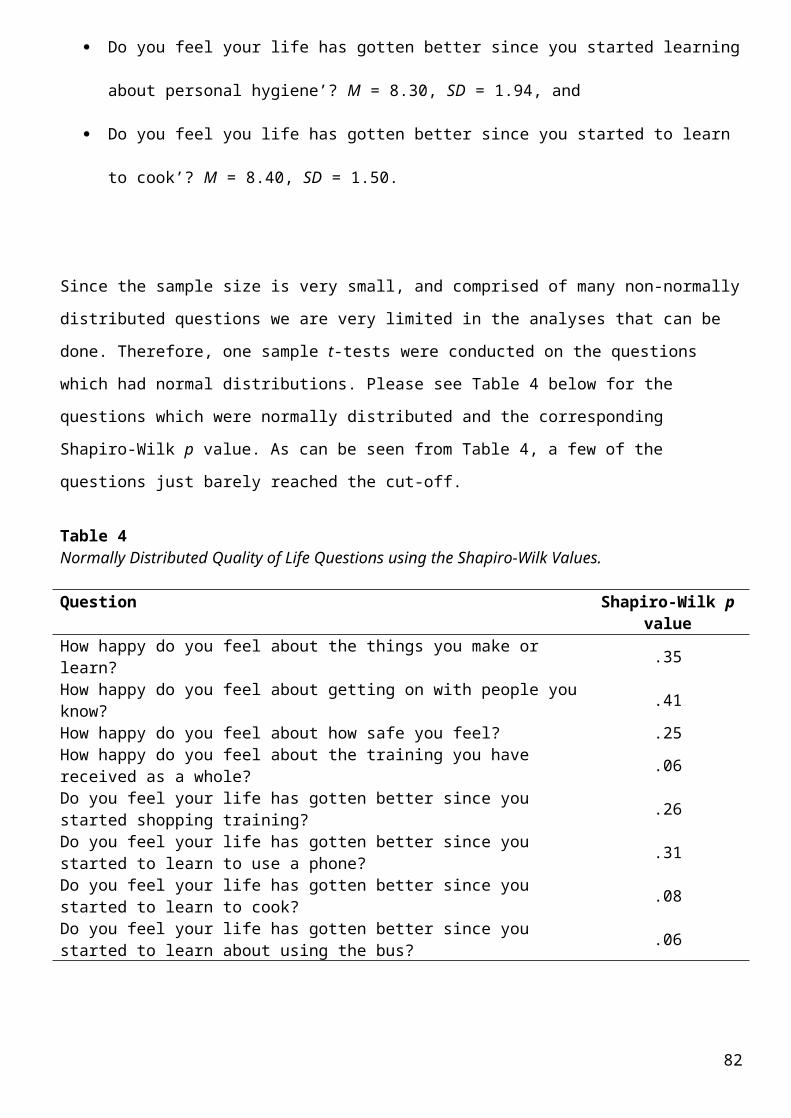
Do you feel your life has gotten better since you started learning
about personal hygiene’? M = 8.30, SD = 1.94, and
Do you feel you life has gotten better since you started to learn
to cook’? M = 8.40, SD = 1.50.
Since the sample size is very small, and comprised of many non-normally
distributed questions we are very limited in the analyses that can be
done. Therefore, one sample t-tests were conducted on the questions
which had normal distributions. Please see Table 4 below for the
questions which were normally distributed and the corresponding
Shapiro-Wilk p value. As can be seen from Table 4, a few of the
questions just barely reached the cut-off.
Table 4Normally Distributed Quality of Life Questions using the Shapiro-Wilk Values.
Question Shapiro-Wilk pvalue
How happy do you feel about the things you make or learn? .35
How happy do you feel about getting on with people youknow? .41
How happy do you feel about how safe you feel? .25How happy do you feel about the training you have received as a whole? .06
Do you feel your life has gotten better since you started shopping training? .26
Do you feel your life has gotten better since you started to learn to use a phone? .31
Do you feel your life has gotten better since you started to learn to cook? .08
Do you feel your life has gotten better since you started to learn about using the bus? .06
82
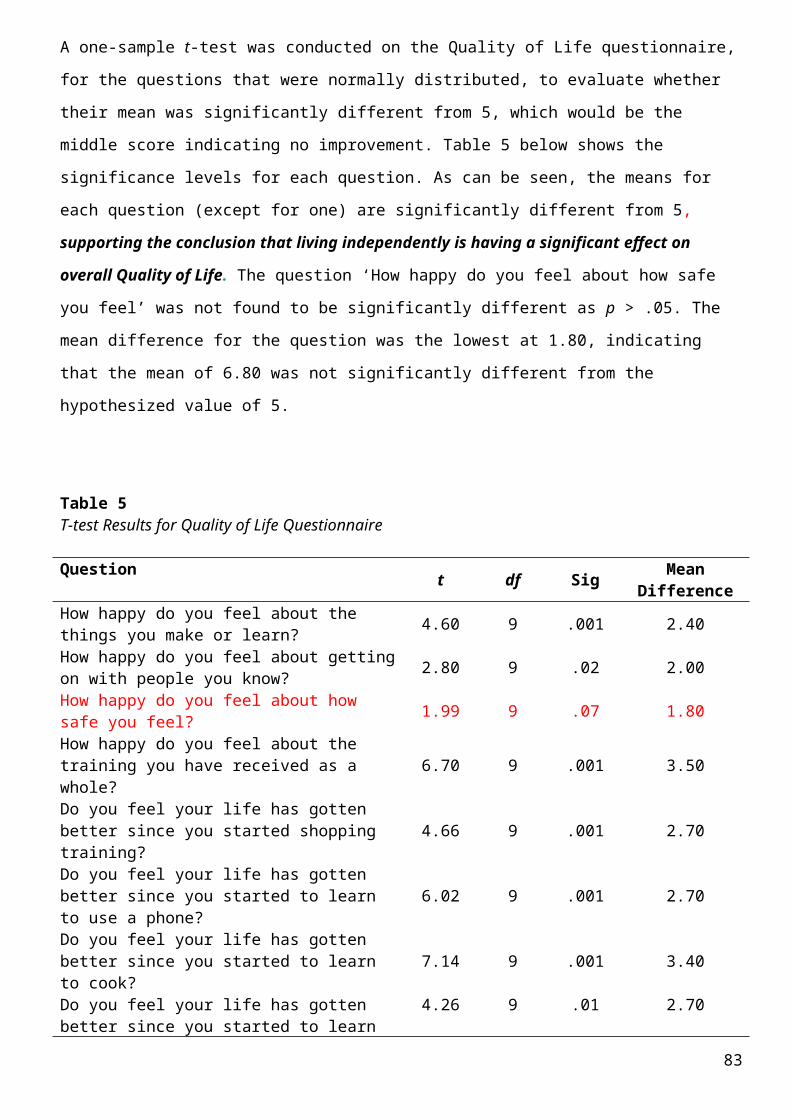
A one-sample t-test was conducted on the Quality of Life questionnaire,
for the questions that were normally distributed, to evaluate whether
their mean was significantly different from 5, which would be the
middle score indicating no improvement. Table 5 below shows the
significance levels for each question. As can be seen, the means for
each question (except for one) are significantly different from 5,
supporting the conclusion that living independently is having a significant effect on
overall Quality of Life. The question ‘How happy do you feel about how safe
you feel’ was not found to be significantly different as p > .05. The
mean difference for the question was the lowest at 1.80, indicating
that the mean of 6.80 was not significantly different from the
hypothesized value of 5.
Table 5T-test Results for Quality of Life Questionnaire
Question t df Sig MeanDifference
How happy do you feel about the things you make or learn? 4.60 9 .001 2.40
How happy do you feel about gettingon with people you know? 2.80 9 .02 2.00
How happy do you feel about how safe you feel? 1.99 9 .07 1.80
How happy do you feel about the training you have received as a whole?
6.70 9 .001 3.50
Do you feel your life has gotten better since you started shopping training?
4.66 9 .001 2.70
Do you feel your life has gotten better since you started to learn to use a phone?
6.02 9 .001 2.70
Do you feel your life has gotten better since you started to learn to cook?
7.14 9 .001 3.40
Do you feel your life has gotten better since you started to learn
4.26 9 .01 2.70
83
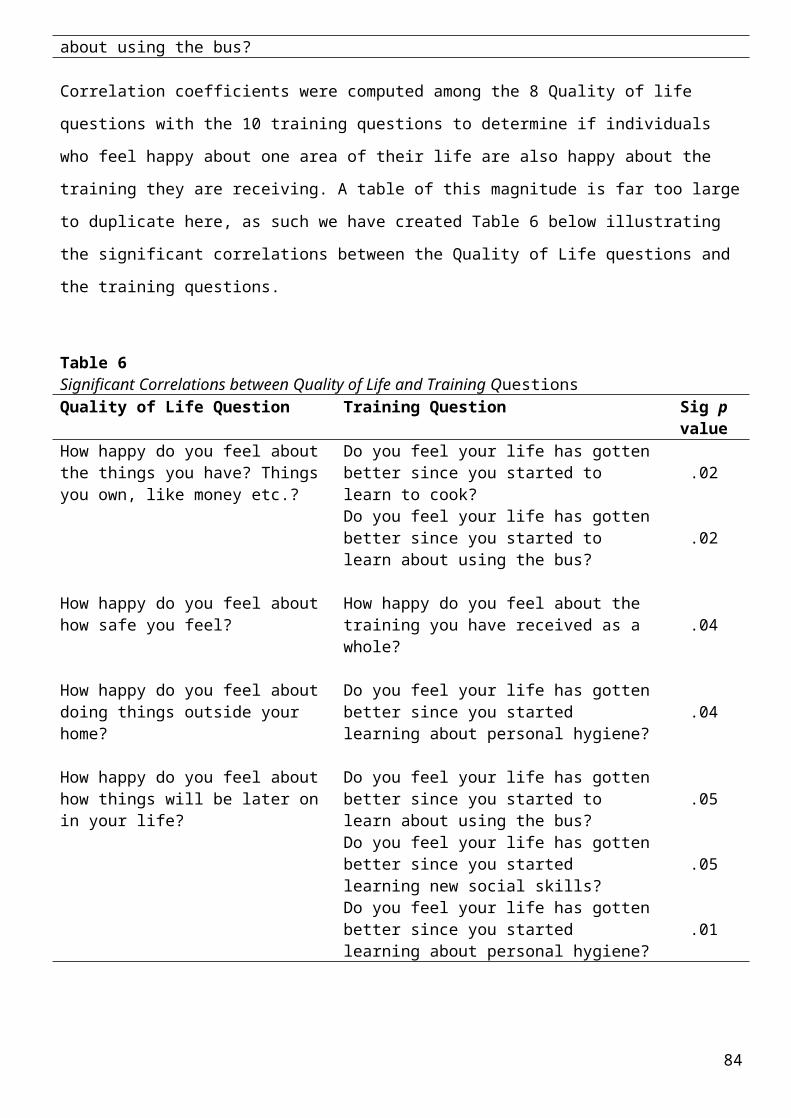
about using the bus?
Correlation coefficients were computed among the 8 Quality of life
questions with the 10 training questions to determine if individuals
who feel happy about one area of their life are also happy about the
training they are receiving. A table of this magnitude is far too large
to duplicate here, as such we have created Table 6 below illustrating
the significant correlations between the Quality of Life questions and
the training questions.
Table 6Significant Correlations between Quality of Life and Training QuestionsQuality of Life Question Training Question Sig p
valueHow happy do you feel about the things you have? Things you own, like money etc.?
Do you feel your life has gottenbetter since you started to learn to cook?
.02
Do you feel your life has gottenbetter since you started to learn about using the bus?
.02
How happy do you feel about how safe you feel?
How happy do you feel about the training you have received as a whole?
.04
How happy do you feel about doing things outside your home?
Do you feel your life has gottenbetter since you started learning about personal hygiene?
.04
How happy do you feel about how things will be later on in your life?
Do you feel your life has gottenbetter since you started to learn about using the bus?
.05
Do you feel your life has gottenbetter since you started learning new social skills?
.05
Do you feel your life has gottenbetter since you started learning about personal hygiene?
.01
84
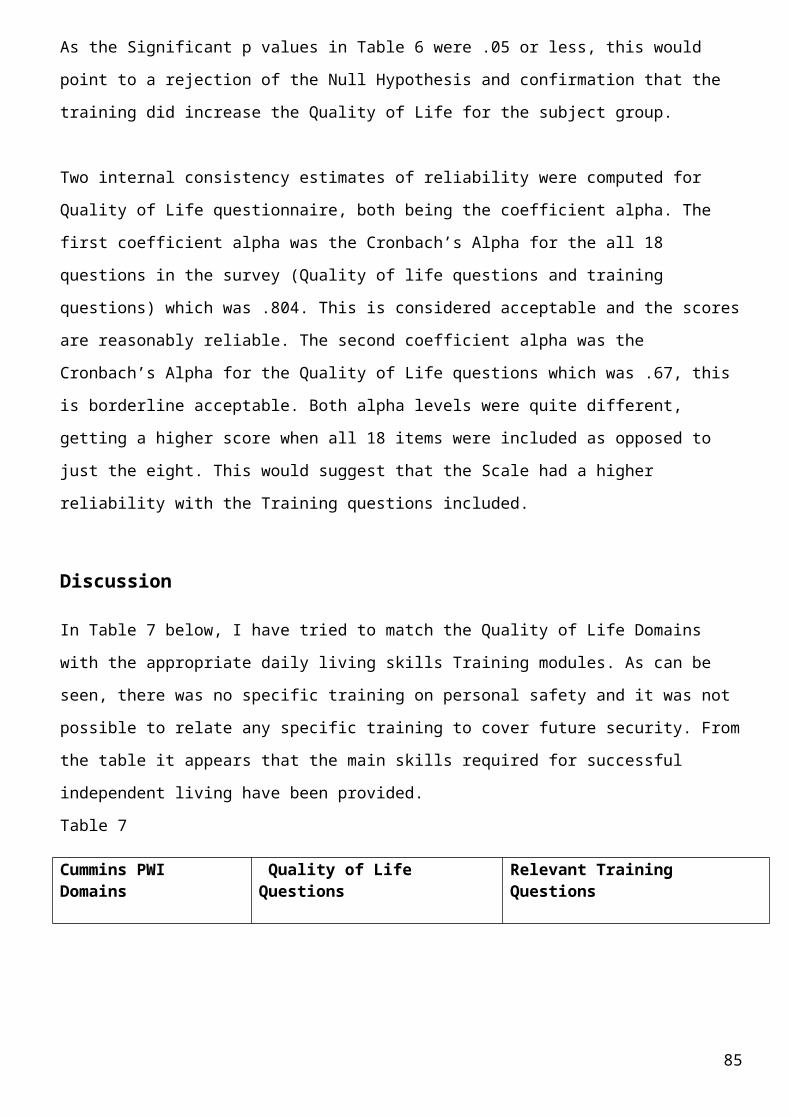
As the Significant p values in Table 6 were .05 or less, this would
point to a rejection of the Null Hypothesis and confirmation that the
training did increase the Quality of Life for the subject group.
Two internal consistency estimates of reliability were computed for
Quality of Life questionnaire, both being the coefficient alpha. The
first coefficient alpha was the Cronbach’s Alpha for the all 18
questions in the survey (Quality of life questions and training
questions) which was .804. This is considered acceptable and the scores
are reasonably reliable. The second coefficient alpha was the
Cronbach’s Alpha for the Quality of Life questions which was .67, this
is borderline acceptable. Both alpha levels were quite different,
getting a higher score when all 18 items were included as opposed to
just the eight. This would suggest that the Scale had a higher
reliability with the Training questions included.
Discussion
In Table 7 below, I have tried to match the Quality of Life Domains
with the appropriate daily living skills Training modules. As can be
seen, there was no specific training on personal safety and it was not
possible to relate any specific training to cover future security. From
the table it appears that the main skills required for successful
independent living have been provided.
Table 7
Cummins PWI Domains
Quality of Life Questions
Relevant Training Questions
85
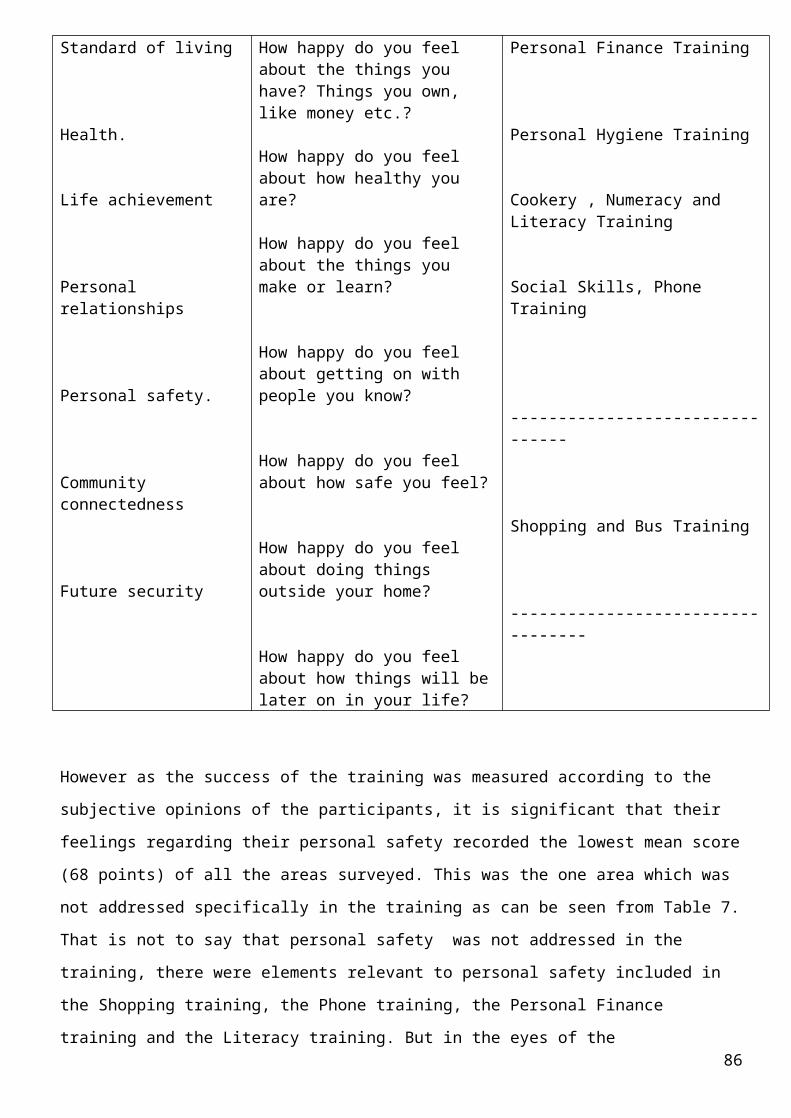
Standard of living
Health.
Life achievement
Personal relationships
Personal safety.
Community connectedness
Future security
How happy do you feel about the things you have? Things you own, like money etc.?
How happy do you feel about how healthy you are?
How happy do you feel about the things you make or learn?
How happy do you feel about getting on with people you know?
How happy do you feel about how safe you feel?
How happy do you feel about doing things outside your home?
How happy do you feel about how things will belater on in your life?
Personal Finance Training
Personal Hygiene Training
Cookery , Numeracy and Literacy Training
Social Skills, Phone Training
--------------------------------
Shopping and Bus Training
----------------------------------
However as the success of the training was measured according to the
subjective opinions of the participants, it is significant that their
feelings regarding their personal safety recorded the lowest mean score
(68 points) of all the areas surveyed. This was the one area which was
not addressed specifically in the training as can be seen from Table 7.
That is not to say that personal safety was not addressed in the
training, there were elements relevant to personal safety included in
the Shopping training, the Phone training, the Personal Finance
training and the Literacy training. But in the eyes of the 86
participants, this did not equate to a full training module on personal
safety.
What is also significant about these findings is the importance
attached to Social Skills Training with a mean score of 92 points. This
is in agreement with the findings of Schalock and Verdugo (2002) who
found that Interpersonal Relations and Social Inclusion were the two
domains of Quality of Life most frequently referred to the their review
of the QoL literature. It also reflects a desire by people with an
Intellectual Disability to be, as Rapley (2000) and Reinders (2000)
pointed out, being “of “the community rather than merely being “in” the
community.”Being “of “the community denotes acceptance and integration
in-to the community, participating in community activities, and most
importantly, feeling a sense of security and acceptance. Being “of” the
community promotes a sense of well-being and as such, is one of the
expected benefits of community integration. However, this level of
integration requires the proper supports and training programmes to be
put in place.” It is reasonable to assume that in this study, the
proper supports and training is being effective as the participants
recognise the benefits of Social skills training and how it has lead to
a level of community integration not experienced heretofore. Ruesch et
al (2004) state that this aspect of social support is highly valued by
users. Wells (2006) also found this to be the case in his study in
(2006),
The high satisfaction score for that Social Skills training may also be
attributable to the training methods used. Participants were trained in
groups and role play was a major element. Tarkington et al. (1973) and
Liberman, (1972), have suggested that group training in these skills is
more advantageous than one to one training. They assert that the group
format is more economical and provides a more realistic setting for
87
interpersonal learning, through multiple learning models and multiple
sources of social instruction and reinforcement.
All of the Training modules recorded scores above the halfway point of
5 points, the lowest being 74 points and the highest being 92 points.
Cookery training received the second highest score (84 points) which
showed the importance attached to food preparation as one of the basic
skills required to life independently in ones own home. Cookery in this
case meant the production of fairly basic meals but it was recognise
that cooking is an evolving skill where the variety of foods and
preparation methods available mean that participants will continue to
learn as life goes on. As time goes on and cooking skills improve, new
recipes and new cooking methods will be tried out. Participants will
learn how to Grill, Roast and Microwave, thus enhancing their range of
capabilities. This is in contrast for example, with Phone and Bus
training which don’t have much scope for variety and evolutionary
learning.
Summary and Recommendations
This study was limited in the conclusions it could draw due to the
small sample size. Therefore it is not possible to generalise the
findings to the wider population. However, this was not the intention
either. On the basis of the assumption that a change to independent
living would bring quality of life gains, that data shows that with a
mean score of 90 points out of 100 for the Question of Happiness with
life as a Whole, in would indeed appear that this transition did in
88
fact bring Quality of Life gains. The aim of the study was to see if
the particular training that the participants received would increase
this Quality of Life score. The mean for the Training received as a
Whole was lower at 85 points compared to 90 points for the Quality of
Life as a whole. This does not mean that the Training did not lead to
Quality of Life gains. Three out of the ten participants gave low
scores for their satisfaction with their feelings of personal safety,
two were borderline and one gave it only 10 points out of 100. There
was no equivalent Training module to specifically address the question
of Personal Safety. If there had been training to address this concern,
it is likely that the overall Training mean would have exceeded the
overall Quality of Life mean.
As this study hopes to establish a baseline against which future
studies of this group, and new groups can be measured against, it
clearly shows the need to include training on Personal Safety matters
in the future. There is a high level of satisfaction with all the other
training modules.
According to the National Intellectual Disability Database 2010, there
were 26484 Adults with Intellectual Disability registered in Ireland,
of these, 6706 were categorised as being in the Mild category.
As the trend now is for people with Mild Intellectual Disability to be
prepared for Independent Living, I would hope that this study shows
what training these people require in order for this transition to be
successful and how they view the training in their own minds. This
consultation process is an integral part of independence. With 6706
possible candidates, there is definitely scope for further research in
this area
89

Bibliography90
A Framework for the Training and Employment of People with Mental
Health Difficulties. Mental Health Forum Report. Health Service
Executive, 2007. Dublin.
Ager, A., and Hatton, C. (2002) Quality of Life Measurements and People
with Intellectual Disabilities: A reply to Cummins. Journal of Applied
Research in Intellectual Disabilities, 15, 254-260
Agran, M., Fodor-Davis, J., Moore, S.C.,& Martella, R.C. (1992) The
effects of peer delivered self instructional training on a lunch making
work task for students with severe disabilities. Education and Training
in Mental Retardation, 27, 230-240.
Allen, J., and Walker, M. (1996) Training Employees with Disabilities:
Strategies from Corporate Training. Journal for Vocational Special
Needs Education. Vol.18, No. 3.pp 105-108.
Anctil, T.M., and Degeneffe, C.E. (2003) “ Self management and Social
Skills Training for Persons with Developmental Disabilities: Tools for
the Rehabilitation Counsellor to facilitate success in Community
Settings: A Literature Review.” Journal of Applied Rehabilitation
Counselling, 34 (1): 17-24.
Andrews, F.M., (1974) Social Indicators of Perceived Life Quality.
Social Indicators Research, 1, pp279-299.
Antonovsky, A. (1979) Health, Stress and Coping. Jossey-Bass, San
Francisco
91
Australian Association of Mathematics Teachers.(1997) Numeracy =
Everyone's Business. The report of the Numeracy Education Strategy
Development Conference. Commonwealth of Australia, Canberra.
Ball, K. (2000) Outcomes for people with a disability in Vocational
Education and Training. Pathways 5 Conference, Canberra, Dec 2000.
Available online at https ://www.edu.au/view.apx?id=3937
Bandura, A. (1977). Social Learning Theory. New York: General Learning
Press.
Bank-Mikkelsen, N.E. (1969) A metropolitan area in Denmark,
Copenhagen. In R.Kugel & and W. Wolfensberger (eds.) Changing pattern
in residential services for the Mentally Retarded. Washington. D.C.,
Presidents Committee on Mental Retardation.
Barnes, C. (1991) Disabled People in Britain and Discrimination.
London: Hurst & Co.
Barnes, C. (1994): Disabled People in Britain and discrimination: A
case for Anti Discrimination Legislation. (Second impression) London.
Hurst and Co.
Bell, J. (1997) Doing you Research Project. A Guide for First Time
Researchers in Education and Social Science, (2nd Edn.) Buckingham: OU
Press
Bellamy, G.T., Horner, R.H., and Inman, D.P. (1979) Vocational
Rehabilitation of Severely Retarded Adults: A direct Service
Technology. Baltimore: University Park Press.
92
Bender, M., Valletutti, P.J., and Baglin, C.A. (1996) A functional
curriculum for teaching students with Disabilities. 3rd Edn. Vol.1.
Austin, Texas. Pro-Ed.
Beyer, S., and Robinson, C. (2009) A Review of the Research Literature
on Supported Employment: A Report on the Cross Government Learning
Disability Employment Strategy Team. Available online at
http://www.cabinetoffice.gov.uk/media/217094/
supported_employment_lit_review.pdf
Bickman, L., Nurcombe, B., Townend, C., Belle, M., Schut, J., and
Karver, M. (1998) Consumer measurement systems and child and
adolescent mental health. Dept. of Health and Family Services ,
Canberra, Australian Capital Territory.
Bird G, Buckley S. (2001) Number Skills for Individuals with Down Syndrome - An
Overview. Portsmouth, UK: Down Syndrome Education International.
Birenbaum, A., & Re, M., (1979) Resettling mentally retarded Adults in
the community- almost four years later.- American Journal of Mental
Deficiency., 83, 323-329
Bjaanes, A., & Butler, E. (1974) Environment variation in Community
Care facilities for mentally retarded persons. American Journal of
Mental Deficiency, 78, 429-439.
Bognar, G. (2006) The Concept of Quality of Life. Social Theory and
Practice, Vol 31, No. 4, 561-580
93
Bonham, G.S., Basehart, S., Schalock, R.L., Marchan, C.B., Kirchner,
N., and Rumenap, J.M. (2004) Consumer based Quality of Life assessment:
The Maryland Ask Me! Project. Mental Retardation, 42, 338-55.
Borthwick-Duffy, S.A. (1992) Quality of Life and quality of care in
mental retardation, in Mental Retardation in the Year 2000., (ed. L.
Rowitz), Springer-Verlag, New York.
Bowling, A. (1997) Measuring Health: A review of Quality of Life
Measurement Scales. Open University Press. Buckingham.
Bradley, V.J., Ashbaugh, J.W., & Blaney, B.C. (1994) Creating
Individual Supports for People with Developmental Disabilities: A
mandate for change at many levels. Baltimore, Maryland: Brookes
Brown, R.I., Beyer, M.B., and McFarlane, C. (1988) Quality of Life
amongst handicapped adults. In: R.I. Brown (ed.) Quality of Life for
Handicapped People. pp 111-140. Croom-Helm: London.
Brown, Roy.I. (1998) The effects of Quality of Life Models on the
development of Research and Practice in the field of Down Syndrome.
Down Syndrome Research and Practice Vol 5, No.1.pp 39-42.
Bruce, M., Collins, S., Langdon, P., Powlitch, S., and Reynolds, S.
(2010) “Does training improve understanding of core concepts in
Cognitive Behaviour Therapy by people with Intellectual Disabilities?”
A randomised experiment. British Journal of Clinical Psychology (2010)
49, 1-13.
94
Bruininks, R.,Woodcock, R.,Weatherman, R.,& Hill.B.(1985) Scales of
Independent Behaviour. Chicago: DLM Teaching Resources.
Bryman, A. (1998) Quantity and Quality in Social Research. London :
Unwin Hyman
Buckley SJ. (2007) Teaching numeracy. Down Syndrome Research and
Practice.;12(1);11-14.
Burrell, G. & Morgan, G. (1985) Sociological Paradigms and
Organisational Analysis Elements of the Sociology of Corporate Life.
(Reprinted Edition) Aldershot: Ashgate.
Burnett, P. (1989) Assessing satisfaction in people with an
intellectual disability living in community based residential
facilities. American Disability Review, 1, 14-19.
Byrne A, MacDonald J, Buckley SJ.( 2002) Reading, language and memory
skills: A comparative longitudinal study of children with Down syndrome
and their mainstream peers. British Journal of Educational Psychology.;72:513-529.
Campo, S.F., Sharpton, W.R., Thompson, B., and Sexton, D. (1997)
Correlates of the quality of life for adults with severe or profound
mental retardation.. Mental Retardation, 35(5), 329-337
Chadsey, J., and Beyer, R. (2001) Social Relationships in the
Workplace. Mental Retardation and Developmental Disability Research
Reviews. 7, 128-133.
Chadsey-Rusch, J., Linneman, D., and Rylance, B.J. (1997) Beliefs
about Social Integration from the perspectives of Persons with Mental
95
Retardation, Job Coaches and Employers. American Journal on Mental
Retardation. 102.1.1-12.
Chadsey-Rusch, J., DeStefano, L., O’Reilly, M., Gonzalez, P. & Coller-
Klingenberg, L. (1992) Assessing the loneliness of workers with mental
retardation. Mental Retardation , 2, 85-92
Chandler, S.K., and Panaskie, S.C. (2004) “ Socialisation, Peer
Relationships and Self Esteem.” in P Wehman and J. Kriegel (eds.)
Functional Curriculum for Elementary, Middle and Secondary Age students
with Special Needs.2nd Edn. pp 165-203. Austin Texas. Pro-Ed.
Clarke, S. (1999) Justifying Deception in Social Science Research.
Journal of Applied Philosophy. 16, 151-66
CLMS (2010) MSc in Training and Human Resource Management, Module 4 (Version
3.1). Units 2 & 3, Leicester: Centre for Labour Market Studies
Coffey, A. (2004) “Accessing the Curriculum: a case study of pupils
with special education needs in a mainstream Irish primary school.
REACH Journal of Special Education in Ireland. 17(2) 93-103.
Cook, B.G., Trevino, C., Cook, L., and Tankersley, M. (2001) “
Instructional Strategies”, in R.W. Flexor, J.J. Simmons, P. Luft, and
R.M. Bayer, (eds) “Transition Planning for Secondary Students with
Disabilities. Upper Saddle River, N.J. Prentice-Hall.
96
Costanza, R. et al. (2007) Quality of Life: An approach integrating
opportunities, Human Needs and Subjective Wellbeing. Ecological
Economics, 61, 267-276.
Creswell, J.W. (2003) Research Design: Qualitative, Quantitative and
Mixed Methods Approaches. (2nd. Edn.) London: Sage
Cummins, R.A. 1996. The domains of life satisfaction: an attempt to
order chaos. Social
Indicators, 35:303-332.
.
Cummins, R.A. (1997a). Self Rated Quality of Life Scales for People
with an Intellectual Disability. A Review. Journal of Applied Research
in Intellectual Disabilities, Vol.10, No.3, pp 199-216
Cummins, R.A. 1997b. Comprehensive Quality of Life Scale - Adult Manual
(5th Edition).
Deakin University, Melbourne: School of Psychology.
Cummins, R.A. 1997c. Comprehensive Quality of Life Scale -
Intellectual/Cognitive
Disability Manual (5th Edition). Deakin University, Melbourne: School
of Psychology
Cummins, R.A., McCabe, M.P., Romeo, Y., Reid, S. & Waters, L. 1997. An
initial evaluation
of the Comprehensive Quality of Life Scale - Intellectual Disability.
International Journal of Disability, Development and Education, 44:7-
19.
97
Cummins, R.A. & Gullone, E. 2000. Why we should not use 5-point Likert
scales: The case
for subjective quality of life measurement. Proceedings, Second
International Conference on Quality of Life in Cities (pp. 74-93).
Singapore: National University of Singapore.
http://acqol.deakin.edu.au/instruments/PWI/2000
Cummins, R.A. 2001. Living with support in the community: predictors of
satisfaction with
life. Mental Retardation and Developmental Disabilities, 7:99-104.
Cummins, R.A. 2002. Vale ComQol: Caveats to using the Comprehensive
Quality of Life
Scale: Welcome the Personal Wellbeing Index. Melbourne: Deakin
University.
http://acqol.deakin.edu.au/instruments/Caveats_ComQol_scales.doc
Cummins, R.A. 2005. Moving from the quality of life concept to a
theory. Journal of
Intellectual Disability Research, 49(10): 699-706.
Cummins, R.A., (2002) Proxy responding for subjective well being.
International Review of of Research in Mental Retardation 25, 183-207.
Cummins, R.A., & Lau, A.L.D. (2005) Personal Wellbeing Index-
Intellectual Disability, 3rd Edition. Deakin University, Melbourne,
Victoria.
98
Curl, R.M., Hall, S.M., Chisholm, L.A., and Rule, S. (1992) Co-workers
as trainers for entry level workers; a competitive employment model for
individuals with developmental disabilities. Rural Special Education
Quarterly, 11(1) 31-35.
Dagnan, D., and Chadwick, P. (1997) Cognitive Behaviour Therapy for
people with Learning Disabilities: Assessment and Interventions.In
B.Stenfert-Kroese, D.Dagnan, and K. Loumidis (eds.) Codniitive
Behaviour Therapy for people with Learning Disabilities. Routledge.
London. (pp 110-123)
Dagnan, D., Chadwick, P. and Proudlove, J. (2000) Towards and
assessment of suitability of people with mental retardation for
Cognitive Therapy. Cognitive Therapy and Research, 24.627-636.
Denscombe, M. (2010) “Ethics in Ground Rules for Social Research:
Guidelines for good Practice (2nd Edn.) pp. 59-80 Berkshire: McGraw-
Hill, Open University Press
D.E.T.I.R. (1999) Outcomes of the visits to other States and
Territories to investigate issues relating to the implementation of
Training Packages. Report to the Director General-Unpublished.
D.E.T.I.R. (1999) Access and Equality Research Report. Evaluations of
the Implementation and Inclusiveness of National Training Packages for
People with Disabilities. Brisbane, Dept. of Employment, Trade and
Industrial Relations.
99
Dunfee, N. (2000) Bridging the Gap. Pathways to National Training
Packages, a Queensland System Response. Pathways 5 Conference, Dec.
2000. Available online at https//: www.edu.au/view.apx?id=3937
Dunlap, W.R., and Iceman, D. (1985) The Development and Validation of a
set of instruments to assess Independent Living Skills. Journal of
Rehabilitation. In Press. Oct/Nov/Dec. 1986.
Dunlap, W.R., and Iceman, D. (1989) Classification by Functional
Ability for Independent Living. British Journal of Special Education.
Vol.16 (1) 23-26.
D`Zurilla, T.J., and Goldfried, M.R. (1971) Problem Solving and
Behaviour Modification. Journal of Abnormal Psychology, 78, 107-126.
Esbensen, F.A., Deschenes, E.P., Vogel, R.E., West, J., Abbott, K. and
Harris, L. (1996) Active Parental consent in School Based research: an
examination of ethical and methodological issues. Evaluation Review,
20, 737-53.
Evans, K. and Niemeyer, B. (2004) “ Re-enter and Reconnect- but whose
problem is it?” In K.Evans and B. Niemeyer (eds.) Reconnection:
countering social exclusion through situated learning, pp 1-28.
Dordrecht, Kluwer Academic Publishers.
FÁS, Vocational Training Strategy for Disabled People, April 2006.
Available online at https:// FÁS.ie/en/Equality/ Disability/
Disability+Publications+and+Newsletters.htm
100
Felce, D., and Perry. J.(1993) Quality of Life: A contribution to its
definition and measurement. Mental Handicap in Wales, Applied Research
Unit, University of Wales College of Medicine.
Felce, D., and Perry. J. (1997). Quality of Life: the scope of the term
and its breadth of measurement. In Roy I. Brown, (ed.) Quality of Life
for People with Disabilities.Models, Research and Prectice. London:
Stanley Thornes.
Farris, B., and Stacliffe, R.J. (2001) The Co-Worher Training Models:
Outcomes of an open employment project. Journal of Intellectual and
Developmental Disability Vol 26(2) 143-159
Gines, D.J., Schweitzer, J.R., Queen-Autrey, T., and Carthon, P. (1990)
Use of colour coded food photographs for meal planning by adults with
mental retardation. Mental Retardation, 28, 189-190.
Glaser, B.G., and Strauss, A.L. (1967) The Discovery of a Grounded
Theory: Strategies for Qualitative Research. New York: Aldine
Gresham, F. M., Sugai, G., & Horner, R. H. (2001). Interpreting
outcomes of social skills training for students with high-incidence
disabilities. Exceptional Children, 67(3), 331-344.
Griffen, A.K., Wolery, M., and Schuster, J.W. (1992) Triadic
instruction of chained food preparation responses: acquisition and
observational learning. Journal of Applied Behaviour Analysis, 25, 193-
204.
101
Grunewald, K. (1969) A rural county in Sweden, Malmous. In R.Kugel &
and W. Wolfensberger (eds.) Changing pattern in residential services
for the Mentally Retarded. Washington. D.C., Presidents Committee on
Mental Retardation.
Hartley, S.L., and McLean, W.E. Jr. (2006) A review of the reliability
and validity of Likert-type scales for people with Intellectual
Disability. Journal of Intellectual Disability Research , 50, 813-27.
Hemming, H., Lavender, T.,& Pill, R. (1981) Quality of Life of mentally
retarded adults transferred from large institutions to new small units.
American Journal of Mental Deficiency, 86, 157-169
Hensel, E., Rose,J., Kroese, B., Stenfert, B., and Banks-Smith, J.
(2001) Subjective judgements of Quality of Life: a comparison study
between people with Intellectual Disabilities and those without
Disabilities. Journal of Intellectual Disability Research. Vol 46, pp
95-107.
Hermann, R.C., Leff, H.S., Palmer, R.H., Young, D., Teller, T.,
Provost, S., et al. (2000) Quality Measures for Mental Health Care :
Results from a National Survey.
Herrera, C.D. (1999) Two Arguments for Covert Methods in Social
Research. British Journal of Sociology, 50, 331-43
102
Holm, P., Holst, J., and Perlt, B. (1994) Co-Write Your Own Life:
Quality of Life as Discussed in the Danish Context. In D. Goode (Ed.)
Quality of Life for Persons with Disabilities. (pp. 1-21) Cambridge ,
M.A. : Brookline Books.
Hironen, M. (2011) From Vocational training to open learning
environments: Vocational special needs education during change. Journal
of Research in Special Education Needs. Vol 11 (2) 141-148
Hobson, R.P., Ouston, R.P., and Lee, A. (1989) Naming emotion in faces
and voices. Abilities and Disabilities in Autism and Mental
Retardation. British Journal of Developmental Psychology, 7, 237-50.
Hughes, C., Kwang, B., Kim, J.H., Eisenman, L.T., and Kilian, D.J.
(1995) Quality of Life in applied research: a review and analysis of
empirical measures. American Journal on Mental Retardation, 99, 6: 623-
41
Jahoda, A., Cattermole, M., and Markova, I. (1990) Moving out: an
opportunity for friendship and broadening social horizons? Journal of
Mental Deficiency Research, 34, 127-139.
Johnson, B.F., and Cuvo, A.J. (1981) Teaching Mentally Retarded
Adults to Cook. Behaviour Modification, 5, 187-202.
Jones, G.Y., and Collins, B.C. (1997) Teaching Microwave skills to
adults with disabilities: acquisition of nutrition and safety facts
presented as non target information. Journal of Developmental and
Physical Disabilities, 9, 59-78.
103
Keith, K.D., and Schalock, R.L. (2000) Cross Cultural Perspectives on
Quality of Life.American Association on Mental Retardation, Washington
D.C.
Kumar, R. (2005) Research Methodology: A Step-By-Step Guide for
Beginners, (2nd Edition). London: Sage
Lacey, P., Layton, L., Miller, C., Goldbart, J., and Lawson, H. (2007)
What is Literacy for Students with severe learning difficulties?
Exploring conventional and inclusive literacy. Journal of Research in
Special Educational Needs, Vol.7, No. 3, 149-160.
Lakin, K., Bruininks, R., & Sigford, B. (1981) Deinstitutionalisation
and community adjustment.A summary of research issues. In R.Bruininks,
C. Meyers, B. Sigford, & K. Lakin. (Eds.) Deinstitutionalisation and
community adjustment for mentally retarded people. American Association
on Mental Retardation. Washington D.C.
Lancioni, G.E., and O`Reilly, M.F., Seedhouse, P., Furness, F., and
Cunha, B. (1999b) Evaluation of a computer- aided system providing
pictorial task instructions and prompts to people with severe
intellectual disability. Journal of Intellectual Disability Research,
43, 61-66.
Lancioni, G.E., and O`Reilly, M.F. (2002) Teaching food preparation
skills to people with Intellectual Disabilities. Journal of Applied
Research in Intellectual Disabilities, 15, 236-253.
Lau, A.L.D., Cummins, R.A. & McPherson, W. 2005. An investigation into
the cross-cultural
104
equivalence of the Personal Wellbeing Index. Social Indicators
Research, 72(3):403432
Levine, H.G. and Langness, L. L. (1985) Everyday Cognition Among Mildly
Mentally Retarded Adults: An Ethnographic Approach. American Journal of
Mental Deficiency, 90, 18-26
Liberman, R.P., (1972) Behavioural Methods in Group and Family
Therapy. Seminars in Psychiatry, 4, 145-156.
Lieberman, L. M. (1992). Preserving special education...for those who
need it. In W. Stainback, & S. Stainback (Eds.), Controversial issues
confronting special education: Divergent perspectives. Boston: Allyn
and Bacon.
Lindstrom, B., and Eriksson, M. (2005) .Contextualizing salutogenesis
and Antonovsky in Public Health Development. Health Promotion
International, Vo l . 2 1 No. 3.
Lockett, T. (1980) Role Modelling; Alternative Pre Vocational Training
for the Deaf-Blind. Paper presented to the Michigan State Board of
Education / Mid West Regional Centre.
Loumidis, K.S., (1992) Can social problem solving skills help people
with learning difficulties? In D.R. Trent (Eds.) The Promotion of
Mental Health. Aldershot: Avebury Press.
Loumidis, K.S., and Hill, A. (1997) Training social problem solving
skills to reduce maladaptive behaviours in Intellectual Disability
Groups: The influence of Individual Difference Factors. Journal of
Applied Research in Intellectual Disabilities, Vol. 10, No.3, 217-237.
105
Lozano, B. (1993). Independent living: Relation among training, skills,
and success: American Journal on Mental Retardation Vol 98(2) Sep 1993,
249-262.
Mank, D., Cioffi, A., and Youvanoff, P. (1997a) Analyses of the
typicalness of Supported Employment jobs, natural supports and
integration outcomes. Mental Retardation, 35, 185-197.
Mank, D., Cioffi, A., and Youvanoff, P. (1997b) Patterns of support for
employees with severe mental disabilities. Mental Retardation, 35,
433-447.
Mank, D., Cioffi, A., and Youvanoff, P. (1998) Employment outcomes for
people with severe disabilities: Opportunities for improvement. Mental
Retardation, 36, 205-216.
Marchetti, A.G., and Campbell, V.A. (1990) Social Skills . In J.L.
Matson, (Ed.) Handook of Behaviour Modifications with the Mentally
Retarded (2nd.edition) New York: Plenum Press.
Martin, J.E., Rusch, F.R., James, V.L., Decker, P.J., and Trtol, K.A.
(1982b) The use of picture cues to establish control in the
preparation of complex meals by mentally retarded adults. Applied
Research in Mental Retardation, 3, 105-119.
McAlpine, C., Kendall, K.A., and Singh, N.N. (1991) Recognition of
Facial Expressions of Emotion by Persons with Mental Retardation.
American Journal on Mental Retardation, 96, (1), 29-36.
106
McGillivray, J. A., Cummins, R.A., Lau, A. L. D., and Davey, G. (2009)
The Utility of the Personal Wellbeing Index Intellectual Disability
Scale in an Australian Sample. Journal of Applied Research in
Intellectual Disabilities 2009, 22, 276-286
McVilly, K.R., & Rawlinson , R.B. (1998) Quality of Life issues in the
development and evaluation of services for people with Intellectual
Disability. Journal of Intellectual and Developmental Disability,
Vol.23.No.3 pp199-218.
Melton, J. (1998) How do clients with Learning Disabilities evaluate
their experience of cooking with the Occupation Therapist? British
Journal of Occupation al Therapy, 61, 106-110.
Meredith, R.L., Saxon, S., Doleys, D., and Kyzer. B. (1980) Social
Skills Training with Mildly Retarded young adults. Journal of Clinical
Psychology 36(4) 1000-1009
Meyers, C.E. (1978) Quality of Life in Severely and Profoundly Retarded
People: Research Foundations for Improvement. American Association on
Mental Deficiency. Washington D.C.
National Federation of Voluntary Bodies (2003) Interim Report on
Quality of Life of young people with Intellectual Disability in
Ireland. Report to the Health Research Board. Available online at
https://fedvol.ie/National_Federation_Publications/default.757.html.
National Intellectual Disability Database 2010. Available online at http://www.hrb.ie/health-information-in-house-research/disability/ddu-publications/ddu-publication/publications//562/
107

Nelson, R., Gibson, F., and Cutting , D.S., (1973) Cited in I.
Robertson, A.M. Richardson amd S. Youngson (1984) Social Skills
Training with Mentally Handicapped People: A Review. British Journal
of Clinical Psychology. 23, 241-64
Nihira, K., Leland, H, and Lambert, N. (1993) Adaptive Behaviour
Scale 2nd Edition. American Association on Mental Deficiency.
Washington, D.C.
Nirje, B. (1969) The Normalistaion Principle and its Human management
implications. In R.Kugel & and W. Wolfensberger (eds.) Changing pattern
in residential services for the Mentally Retarded. Washington. D.C.,
Presidents Committee on Mental Retardation.
Noll, H.H. (2000) The European System of Social Indicators: An
Insturment for Social Monitoring and Reporting. Mannheim: ZUMA.
O`Brien, J. (1987) A guide to personal futures planning, in Brookes,
P.H.: A Comprehensive Guide to the Activities Catalogue: An Alternative
Curriculum for Youths and Adults with Severe Disabilities. Baltimore,
Maryland.
O`Connor, G., (1976) Home is a good place: a national perspective of
community residential facilities for developmentally disabled persons.
Washington D.C. American Association on Mental Retardation.
Oliver, M. (1990) The Policies of Disablement. London: MacMillan.
108
Organisation for Economic Co-Operation and Development (OECD) (2000)
Literacy in the Age of Information. Final Report. Paris, France: OECD.
https://www.literacytrust.org.uk/database/internat.html.
Patton, M.Q. (1990) Qualitative Evaluation and Research Methods. (2nd
Edn) Newbury Park, CA: Sage
Perry, J., Felce, D., and Lowe, K. (2000) Subjective and Objective
Quality of Life assessments: their interrelationship and determinants.
Welsh Centre for Learning Disabilities. University of Wales College of
Medicine, Cardiff.
Petersen, L., and Adderly, A. (2002) Stop, Think, Do. Social Skills
Training: Middle years of Schooling Ages 8-12, Camberwell, Victoria.
Australian Council for Educational Research.
Petry, K. & Maes, B. (2006) Identifying expressions of pleasure and
displeasure by persons with profound multiple disabilities. Journal of
Intellectual and Developmental Disability. 31, 28-38.
Pole, C.J., and Lampard, R. (2002) “Suitable Sample: Selecting,
Obtaining and Profiting from Them”, in Practical Social Investigation:
Qualitative and Quantitative Methods in Social Research. Pp.32-69.
Harlow: Prentice Hall.
Punch, K.F. (1998) Introduction to Social Research: Quantitative and
Qualitative Approaches. London: Sage.
109
Raddon, A. (2006) “Academic Journeys and Gendered Stories: Careers in
UK Higher Education.” In RIHE (ed.) Gender and Higher Education. Pp27-
46. Hiroshima, Japan: Hiroshima University Press.
Rapley, M.(2000) The Social Construction of Quality of Life : The
interpersonal production of wellbeing revisited. In: Cross Cultural
Perspectives on Quality of Life. (eds. K.D.Keith and R.L. Schalock.) pp
155-72. American Association on Mental Retardation. Washinton D.C.
Rapley, M. (2003) Quality of Life Research: A Critical Introduction.
London: Thousand Oaks.
Reinders, J.S. (2002) The good life for citizens with Intellectual
Disability. Journal of Intellectual Disability Research, 46, 1-5.
Report of the Special Education Review Committee, (1993) Dept. of
Education, Stationery Office, Dublin.
Reynolds, P.D. (1979) Ethical Dilemmas and Social Science Research.
San Francisco: Jossey-Bass.
Rodi, M.S., and Hughes, C. (2000) Teaching communication book use to a
high school student using a milieu approach. Journal of the Association
for Persons with Severe handicap, 25, 175-179.
Rogan, P., Hagner, D., and Murphy, S. (1993) Natural Suports:
reconceptualising Job Coach roles. Journal of the Association for
Persons with Severe Handicaps., 18, 275-281.
Ruesch, P., Graf, J., Meyer, P.C., Rossler, W., and Hell, D. (2004)
Occupation Social Support and Quality of Life in persons with
110
Schizophrenic or Affective Disorders. Social Psychiatry and Psychiatric
Epidemiology, 39, 686-694.
Rusch, F.R., and Scutz, R.P., (1979) Non sheltered Employment of the
Mentally Retarded Adults: Research to Reality? Journal on Contemporary
Business, 8,4, 85-89.
Ryan, Anne B. (2006) Post-Positivist Approaches to Research. In: Researching and
Writing your thesis: a guide for postgraduate students. MACE: Maynooth
Adult and Community Education, pp. 12-26.
Rydin-Orwin, T., Drake, J., and Bratt, A. (1999) The effects of
Training on Emotion Recognition Skills for Adults with and Intellectual
Disability. Journal of Applied Research in Intellectual Disabilities,
Vol 12, No 3, 253-262.
Sanders, M.R., and Parr, J.M. (1989) Training developmentally disabled
adults in independent meal preparation. Behaviour Modification, 13,
168-191
Sanderson, R.G., (1980) The need for Independent Living Skills for
Employment of Severely Deaf individuals. Independent Living Skills for
Severely handicapped Deaf People. American Deafness and Rehabilitation
Association. 5, 4-7
Schalock, R.L.,(2003) The emerging Disability Paradigm and its
challenges in the field. Journal of Disability Policy Studies (in
press)
111
Schalock, R.L.,(2004) The Concept of Quality of Life: what we know and
what we don’t know. Journal of Intellectual Disability Research,
Vol.48.3. pp 203-216. March 2004
Schalock, R.L.,Verdugo, M. (2002) Handbook on Quality of Life for Human
Service Practitioners.American Association on Mental Retardation.
Washington D.C.
Schalock, R.L., Brown, I., Brown, R., Cummins, R.A., Felce, D.,
Mattika, L., Keith. K.D., and Parmenter, T. (2002). Conceptualisation,
Measurement, and application of Quality of Life for persons with
Intellectual Disabilities: results of an international panel of
experts. Mental Retardation, 40,457-470
Schalock, R.L., and Parmenter, T. (2000) Preface, In: Quality of Life,
its Conceptualisation, Measurement, and Application. A Consensus
Document. Washington: IASSID.
Schloss, P.J., Alexander, N., Hornig, E., Parker, K., and Wright, B.
(1993) I can cook! A template system or teaching meal preparation
skills. Teaching Exceptional Children, 25, 7-12.
Shearman, F., and Sheehan, C. (2000) Training People with I.D. in
Vocational Skills. Paper presented at the Pathways 5 Conference,
Canberra, Dec 2000. Available online at https//:www.edu.au/view.apx?
id=3937
Sheppard, L.(2006) Growing Pains: a personal development program for
students with Intellectual and Developmental Disabilities in a
Specialist School. Journal of Intellectual Disabilities. 2006, 10:121.
112
Shevlin, M., Kenny, M., and Loxley, A. (2008) A time of transition:
exploring Special Education Provision in the Republic of Ireland.
Journal of Research in Special Educational Needs, Vol 8, (3) 141-152.
Siegelman, C., Schoenruck, C., Spanhel, C., Hromas, S., Winer, J.,
Budd, E., et al. (1980). Surveying Mentally Retarded: Responsiveness
and Response Validity in 3 samples. Americal Journal of Mental
Deficiency, 84, 479-84
Siegelman, C. K., Schoenrock, C. &Winer, J. (1981) Issues in
interviewing mentally retarded persons: an empirical study. In:
Deinstitutionalization and Community Adjustment of Mentally Retarded
Persons (eds R. H. Brunininks, C. Meyers, B. Sigford & K. Lakin).
American Association on Mental Deficiency, Washington, DC.
Simmons, T.J., and Flexer, R.W. (1992) Community based job training for
persons with Mental Retardation- an acquisition and performance
replication. Education and Training in Mental Retardation and
Developmental Disabilities. 27, 3, 261-272.
Sitlington, P.L., Clarke, G.M., and Kolstoe, O.P. (2000) Transition
Education and services for adolescents with disabilities: Boston:
Alleyn and Bacon.
Spooner, F., and Wood, M.W., (2004) “Teaching Personal Care and Hygiene
Skills”, in P Wehman and J. Kriegel (eds.) Functional Curriculum for
Elementary, Middle and Secondary Age students with Special Needs.2nd
Edn. pp 317-356. Austin Texas. Pro-Ed.
Stacey, D., Doleys, D., and Malcolm, R. (1979) Cited in I. Robertson,
A.M. Richardson and S. Youngson (1984) Social Skills Training with
113
Mentally Handicapped People: A Review. British Journal of Clinical
Psychology. 23, 241-64
Stancliffe, R. J., & Keane, S. (2000). Outcomes and costs of community
living: A matched comparison of group homes and semi-independent
living. Journal of Intellectual & Developmental Disability, 25(4), 281-
305.
Steed, S.E., & Lutzker, J.R. (1997) Using picture prompts to teach an
adult with developmental disabilities to independently complete
vocational tasks. Journal of Developmental and Physical Disabilities.
9, 117-133.
Stiles, W.B. (2006) “Numbers can be enriching”, New ideas in
Psychology. 24(3): 252-262
Strategy for Equality, 1996, Commission on the Status of People with
Disabilities. Available online at
https://nda.ie/cntmgmtnew.nsf/0.9007e317368ada63802578d0037224?open
document.
Sullivan, C., Vitello, S., & Foster, W. (1998) Adaptive Behaviour of
adults with mental retardation in a group home: an intensive case
study. Education and Training in Mental Retardation., March 1988, 76-
81.
Townsend-White, C., Pham, A.N.T., And Vassos, M.V. (2011) Journal of
Intellectual Disability Research 10.1111/; 1365-2788
114
Tornillo, P. (1994, March 6). A lightweight fad bad for our schools?
Orlando Sentinel.
United Nations (2011) Background Paper prepared by the Division for
Social Policy and Development of the United Nations Secretariat for the
“Informal Consultative Meetings on International Norms and Standards
for Persons with Disabilities.” (9 February 2001). Accessed online 21-
10-11 http://www.un.org/esa/socdev/enable/rights/humanrights.htm#_ftn3
Verri, A., Cummins, R.A., Petito, F., Vallero, E., Monteath, S.,
Gerosa, E., et al. (1999) An Italian-Australian comparison of Quality
of Life among people with an Intellectual Disability living in the
community. Journal of Intellectual Disability Research 43, 513-22
Wacker, D.P., Berg, W.K., Berrie, P., and Swatta, P. (1985)
Generalisation and maintenace of of complex skills by severely
handicapped adolescents following picture prompt training. Journal of
Applied Behaviour Analysis, 18, 329-336.
Walker, E. (1981) Emotion Recognition in Disturbed and Normal
Children. A Research Note. Journal of Child Psychology and Psychiatry.
22, 263-268
Wehman, P., Hill J.W., and Keohler, F. (1979) Placement of
Developmentally Disabled Individuals in Competitive Employment: Three
Case Studies. Education and Training of the Mentally Retarded. . 14,
269-276.
Wehmeyer, M.L. (1994) Employment Status and Perceptions of Control of
Adults with Cognitive and Developmental Disabilities. 15, 2,119-131.
115

Wells, J.S.G., (2006) Hospital Based Industrial Therapy Units and the
People who work in them. Journal of Psychiatric and Mental Health
Nursing. Blackwell Publishing, 13, 139-147.
W.H.O. (2001) International Classification of Functioning, Disability
and Health. (ICF). Geneva, Switzerland.
W.H.O. Programme on Mental Health.WHO/MSA/MNH/PSF 97.4.
Available online at www.who.int/Mental_Health/Media/68.Pdf
Wolcott, H.F. (1990). Writing up qualitative research. London: Sage.
Wolfensberger, W. (1972) The Principle of Normalisation in Human
Services. National Institute on Mental Retardation: Toronto.
Wolfensberger, W. and Glenn, L. (1975). Program Analysis of Service
Systems (PASS) : A method for the Quantitative Evaluation of Human
Services Field Manual. (3rd Edn.) Toronto : National Institute on
Mental Retardation.
Wolfensberger, W., and Thomas, S. (1983) PASSING ( Program Analysis of
Service Systems Implementation of Normalisation Goals): Normalisation
Criteria and Ratings Manual. Toronto: National Institute on Mental
Retardation.
Wright, C.W., and Schuster, J.W. (1994) Accepting specific versus
functional student responses when training chained tasks. Education and
116

Training in Mental Retardation and Developmental Disabilities, 29, 43-
56.
117
Appendix 1
My name is Barry Spearman
I am going to college
As part of my study, I am going to do a questionnaire
Would you like to take part? Yes No (Tick)
Would you like more information? Yes No (Tick)
118
I will ask you some questions
I will write down your answers
This information is private
You can stop at any time.
Signature___________________________________
Signature of Researcher_______________________
Date______________________________________
119
Appendix 2
Date
Name
Address
RE:
DATA PROTECTION / INFORMED CONSENT LETTER
Dear ………………..
I wish to inform you as guardian/ next of kin, of my intention to speakto…………………. in a research project concerning Quality of Life Measurements for people with Intellectual Disability. I am undertaking this project as part of an MSc. Degree which I am studying with the University of Leicester.
The project I am working on is examining the Quality of Life gains (if any), for people who have moved out into semi Independent accommodationand who have received training to assist this transition.
120
………… …. was selected to take part in this research because he/she has recently commenced living semi independently.
………. ….can withdraw from this study at any time. If he/she is happy totake part in this research, however, I will them to sign a consent formgiving their agreement. He/she can still withdraw from the research after signing the form.
The interview will last for approximately 1 hour. I will ask a series of questions and will give ……….. the opportunity to ask me any questions he/ she may have. I would like to reassure you that any information provided in the course of the interview will be treated in the strictest of confidence. All data collected will be treated in accordance with ethical codes set out in the British Sociological Guidelines (or other appropriate ethical guidelines such as the Data Protection Act or the ethics policy of the Brothers of Charity Services). In addition, all answers will be unattributed.
The data gathered during the interview will only be used for my MSc. Dissertation. Individual data will be completely anonymous and no one will be identifiable. The data will be aggregated so no individual datawill be presented.
If you have any questions at any stage of the project please do not hesitate to contact me.
Yours sincerely
Appendix 3
Information sheet fornext of kin.
In the past 20 years, the concept of Quality of Life for people with disabilities has gained significance, in that the
121
level of satisfaction or dissatisfaction with services was going to impact how those services were designed and delivered. Initially, the observations regarding whether a service user was satisfied or dissatisfied, were made by a third party. Usually either a care giver of a family member. These third party observations were objective and made in good faith, but the process excluded the service user him or herself, and their feelings may not have concurred with thoseof the third party.As services for people with disabilities progressed, it was realised that the views of the service users had to be taken into account when designing appropriate services. This subjective approach involved finding a suitable method of asking people for their views and preferences, while avoidingthe possibility that they may be influenced in their answers by the person asking the questions.
The concept of Quality of Life is one where a person’s satisfaction with life in 8 key areas is measured to ascertain their overall happiness with their life, and this can be compared with the results already known for non disabled people. Many instruments have been invented to obtain this measurement; all have been refined over time. In comparisons by researchers, Cummins Personal Well Being Indexfor People with Intellectual Disability has been found to be the most appropriate, because of its ease of administering, through simple but comprehensive questions, and ease of scoring. It contains just seven questions, carefully designed to elicit information without being too onerous or complicated for the person being interviewed. The answers just require ticking a box on a scale, left or right of centre to denote happiness or unhappiness. It is particularlyappropriate for use in measuring the happiness or otherwise of people with Intellectual Disabilities who have recently begun living Semi Independently and are receiving training toassist them to do so successfully. My research project, underthe guidance of Leicester University is to find out has this move to Semi Independent living, with the training supports, brought Quality of Life improvements to those involved.
122

Barry Spearman
123

Appendix 4 Easy Read Likert Scale
124
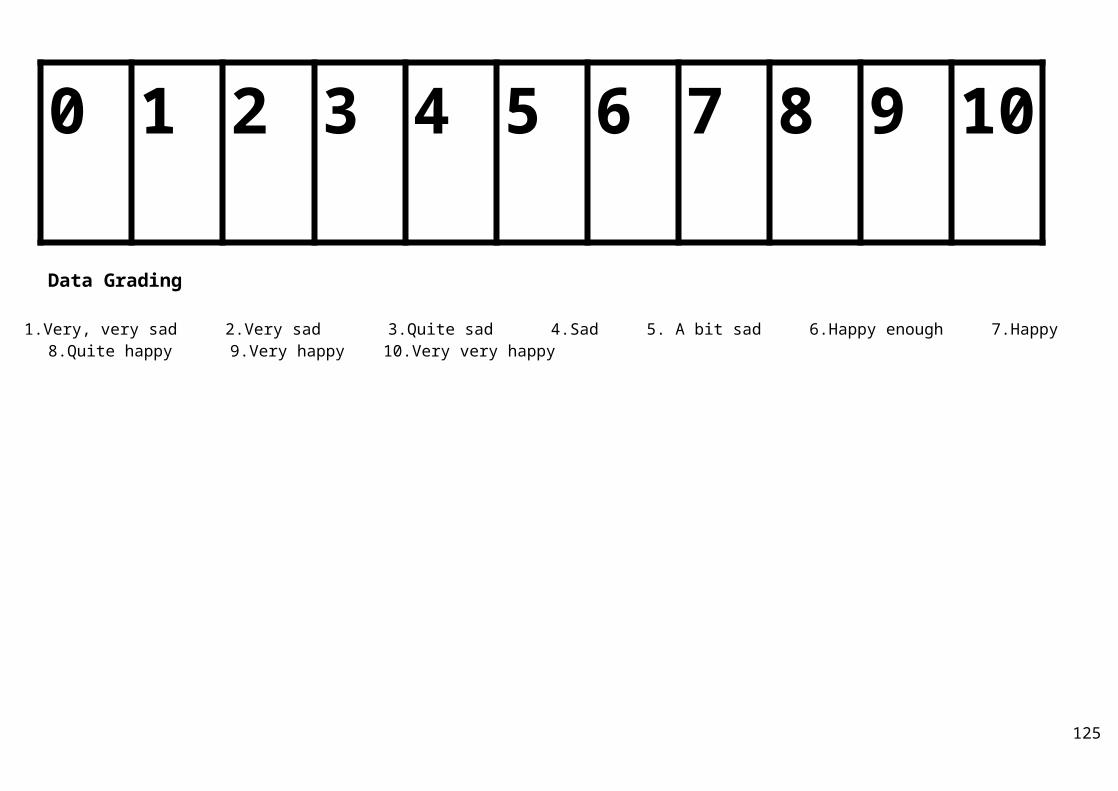
0 1 2 3 4 5 6 7 8 9 10
Data Grading
1.Very, very sad 2.Very sad 3.Quite sad 4.Sad 5. A bit sad 6.Happy enough 7.Happy 8.Quite happy 9.Very happy 10.Very very happy
125
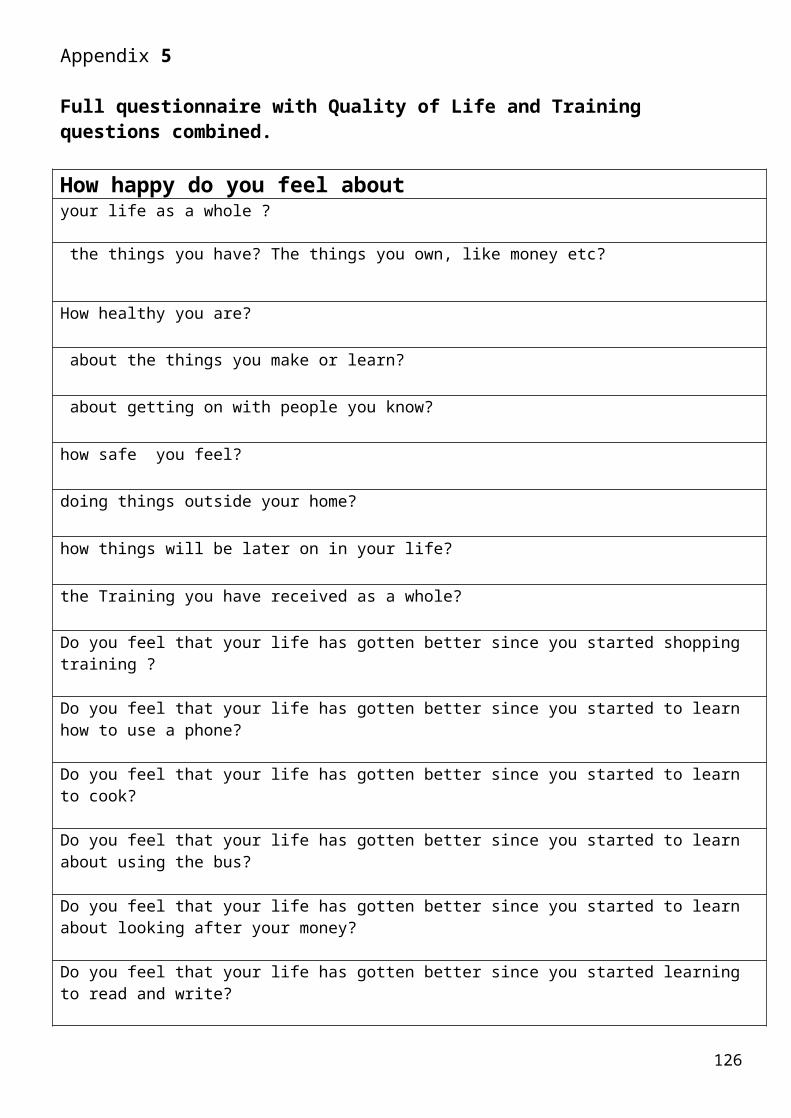
Appendix 5
Full questionnaire with Quality of Life and Training questions combined.
How happy do you feel aboutyour life as a whole ?
the things you have? The things you own, like money etc?
How healthy you are?
about the things you make or learn?
about getting on with people you know?
how safe you feel?
doing things outside your home?
how things will be later on in your life?
the Training you have received as a whole?
Do you feel that your life has gotten better since you started shopping training ?
Do you feel that your life has gotten better since you started to learn how to use a phone?
Do you feel that your life has gotten better since you started to learn to cook?
Do you feel that your life has gotten better since you started to learn about using the bus?
Do you feel that your life has gotten better since you started to learn about looking after your money?
Do you feel that your life has gotten better since you started learning to read and write?
126
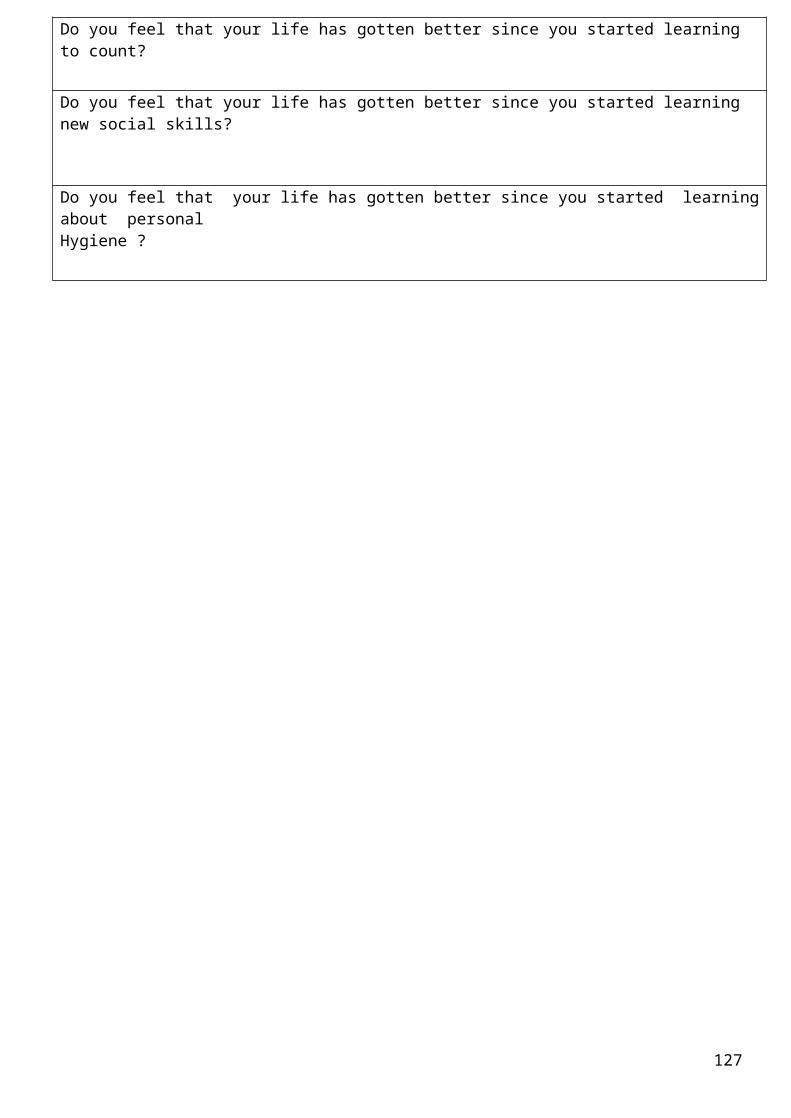
Do you feel that your life has gotten better since you started learning to count?
Do you feel that your life has gotten better since you started learning new social skills?
Do you feel that your life has gotten better since you started learningabout personalHygiene ?
127
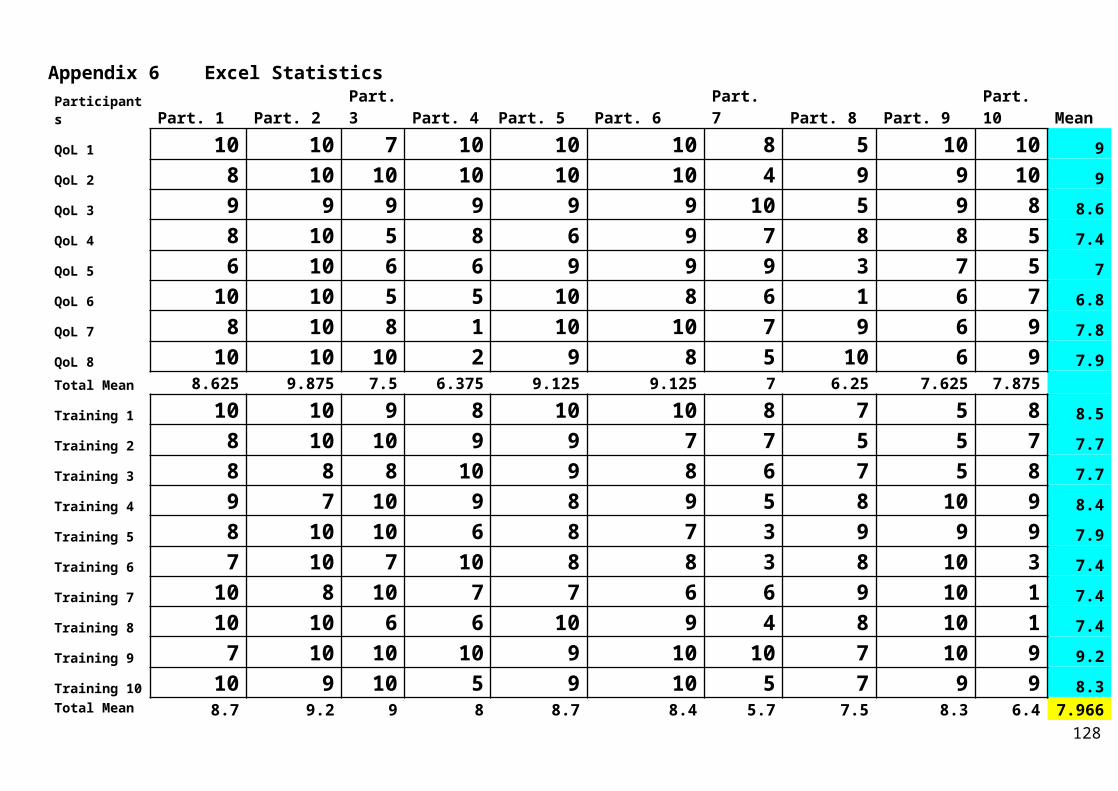
Appendix 6 Excel StatisticsParticipants Part. 1 Part. 2
Part.3 Part. 4 Part. 5 Part. 6
Part. 7 Part. 8 Part. 9
Part. 10 Mean
QoL 1 10 10 7 10 10 10 8 5 10 10 9QoL 2 8 10 10 10 10 10 4 9 9 10 9QoL 3 9 9 9 9 9 9 10 5 9 8 8.6QoL 4 8 10 5 8 6 9 7 8 8 5 7.4QoL 5 6 10 6 6 9 9 9 3 7 5 7QoL 6 10 10 5 5 10 8 6 1 6 7 6.8QoL 7 8 10 8 1 10 10 7 9 6 9 7.8QoL 8 10 10 10 2 9 8 5 10 6 9 7.9Total Mean 8.625 9.875 7.5 6.375 9.125 9.125 7 6.25 7.625 7.875 Training 1 10 10 9 8 10 10 8 7 5 8 8.5Training 2 8 10 10 9 9 7 7 5 5 7 7.7Training 3 8 8 8 10 9 8 6 7 5 8 7.7Training 4 9 7 10 9 8 9 5 8 10 9 8.4Training 5 8 10 10 6 8 7 3 9 9 9 7.9Training 6 7 10 7 10 8 8 3 8 10 3 7.4Training 7 10 8 10 7 7 6 6 9 10 1 7.4Training 8 10 10 6 6 10 9 4 8 10 1 7.4Training 9 7 10 10 10 9 10 10 7 10 9 9.2Training 10 10 9 10 5 9 10 5 7 9 9 8.3Total Mean 8.7 9.2 9 8 8.7 8.4 5.7 7.5 8.3 6.4 7.966
128
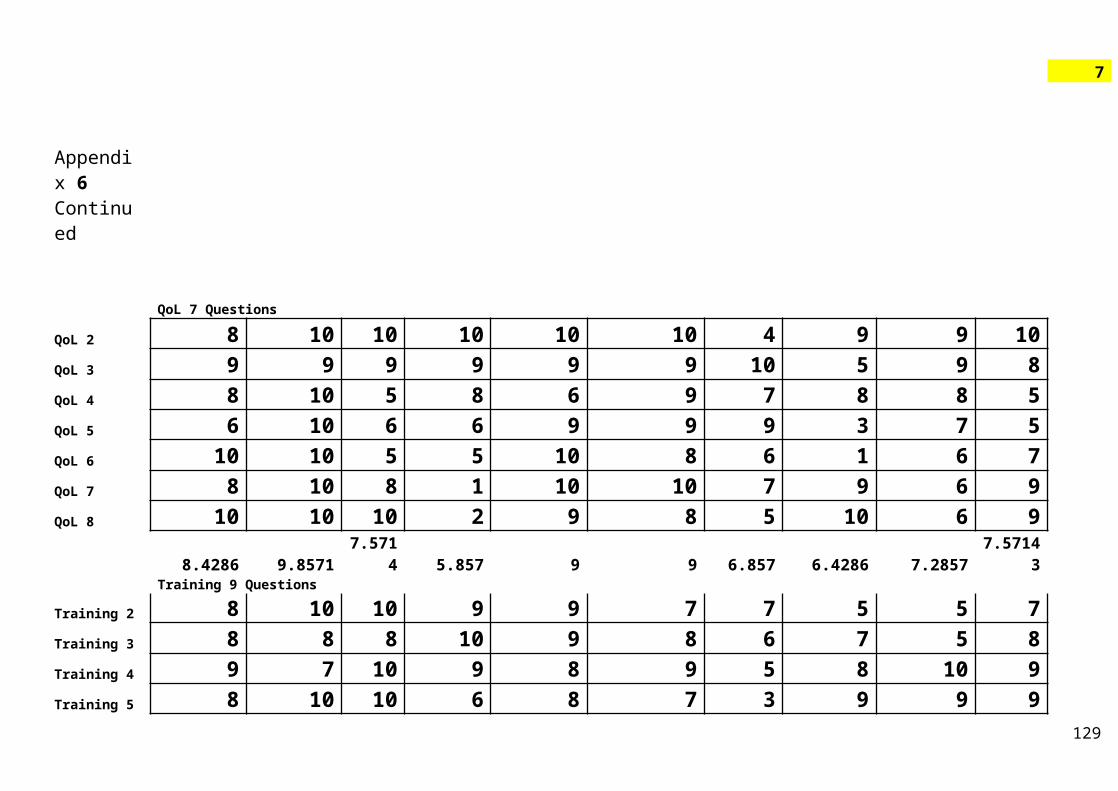
7
Appendix 6 Continued
QoL 7 Questions
QoL 2 8 10 10 10 10 10 4 9 9 10QoL 3 9 9 9 9 9 9 10 5 9 8QoL 4 8 10 5 8 6 9 7 8 8 5QoL 5 6 10 6 6 9 9 9 3 7 5QoL 6 10 10 5 5 10 8 6 1 6 7QoL 7 8 10 8 1 10 10 7 9 6 9QoL 8 10 10 10 2 9 8 5 10 6 9
8.4286 9.85717.571
4 5.857 9 9 6.857 6.4286 7.28577.5714
3Training 9 Questions
Training 2 8 10 10 9 9 7 7 5 5 7Training 3 8 8 8 10 9 8 6 7 5 8Training 4 9 7 10 9 8 9 5 8 10 9Training 5 8 10 10 6 8 7 3 9 9 9
129
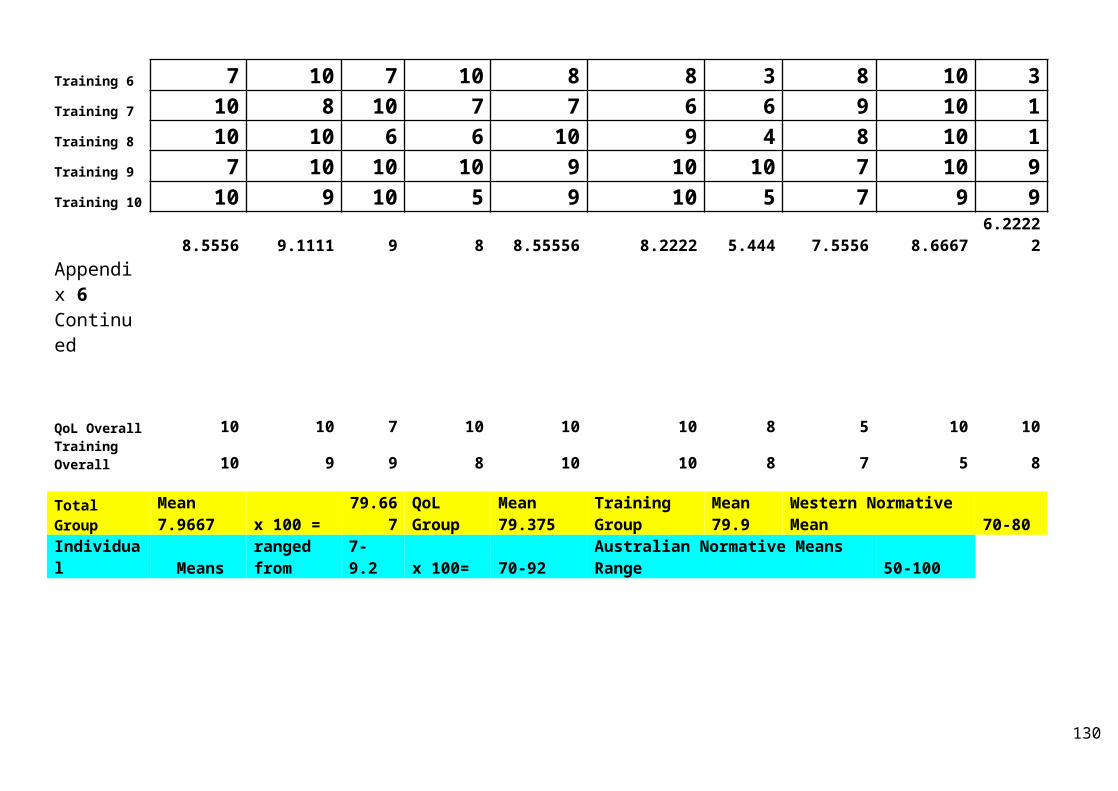
Training 6 7 10 7 10 8 8 3 8 10 3Training 7 10 8 10 7 7 6 6 9 10 1Training 8 10 10 6 6 10 9 4 8 10 1Training 9 7 10 10 10 9 10 10 7 10 9Training 10 10 9 10 5 9 10 5 7 9 9
8.5556 9.1111 9 8 8.55556 8.2222 5.444 7.5556 8.66676.2222
2Appendix 6 Continued
QoL Overall 10 10 7 10 10 10 8 5 10 10Training Overall 10 9 9 8 10 10 8 7 5 8
Total Group
Mean 7.9667 x 100 =
79.667
QoL Group
Mean 79.375
Training Group
Mean 79.9
Western Normative Mean 70-80
Individual Means
ranged from
7- 9.2 x 100= 70-92
Australian Normative Means Range 50-100
130

131

132
133

134

135

136

137





























