Embed Size (px)
Citation preview
Carsten RöckerRWTH Aachen University, Germany
Martina ZiefleRWTH Aachen University, Germany
E-Health, Assistive Technologies and Applications for Assisted Living:Challenges and Solutions
Hershey • New York
MEDICAL INFORMATION SCIENCE REFERENCE

E-health, assistive technologies and applications for assisted living: challenges and solutions / Carsten Röcker and Martina Ziefle, editors. p. cm. Includes bibliographical references and index. Summary: “This book reviews existing literature in assistive technologies and provides suggestions and solutions for improving the quality of assisted living facilities and residences through the use of e-health systems and services”--Provided by publisher. ISBN 978-1-60960-469-1 (hardcover) -- ISBN 978-1-60960-471-4 (ebook) 1. Medical informatics. 2. Assistive computer technology. 3. Congregate housing. I. Röcker, Carsten, 1975- II. Ziefle, Martina, 1962- R858.E225 2011 610.285--dc22 2010048865
British Cataloguing in Publication DataA Cataloguing in Publication record for this book is available from the British Library.
All work contributed to this book is new, previously-unpublished material. The views expressed in this book are those of the authors, but not necessarily of the publisher.
Director of Editorial Content: Kristin KlingerDirector of Book Publications: Julia MosemannAcquisitions Editor: Lindsay JohnstonDevelopment Editor: Myla HartyTypesetters: Michael Brehm, Milan Vracarich Jr.Production Editor: Jamie SnavelyCover Design: Nick Newcomer
Published in the United States of America by Medical Information Science Reference (an imprint of IGI Global)701 E. Chocolate AvenueHershey PA 17033Tel: 717-533-8845Fax: 717-533-8661 E-mail: [email protected] site: http://www.igi-global.com/reference
Copyright © 2011 by IGI Global. All rights reserved. No part of this publication may be reproduced, stored or distributed in any form or by any means, electronic or mechanical, including photocopying, without written permission from the publisher.Product or company names used in this set are for identification purposes only. Inclusion of the names of the products or companies does not indicate a claim of ownership by IGI Global of the trademark or registered trademark.
Library of Congress Cataloging-in-Publication Data
76
Copyright © 2011, IGI Global. Copying or distributing in print or electronic forms without written permission of IGI Global is prohibited.
Chapter 4
Martina ZiefleRWTH Aachen University, Germany
Carsten RöckerRWTH Aachen University, Germany
Wiktoria WilkowskaRWTH Aachen University, Germany
Kai KasugaiRWTH Aachen University, Germany
Lars KlackRWTH Aachen University, Germany
Christian MölleringRWTH Aachen University, Germany
Shirley BeulRWTH Aachen University, Germany
A Multi-Disciplinary Approach to Ambient Assisted Living
ABSTRACT
This chapter illustrates the different disciplinary design challenges of smart healthcare systems and presents an interdisciplinary approach toward the development of an integrative Ambient Assisted Living environment. Within the last years a variety of new healthcare concepts for supporting and assisting users in technology-enhanced environments emerged. While such smart healthcare systems can help to minimize hospital stays and in so doing enable patients an independent life in a domestic environment, the complexity of such systems raises fundamental questions of behavior, communication and technology acceptance. The first part of the chapter describes the research challenges encountered in the fields of medical engineering, computer science, psychology, communication science, and architecture as well as their consequences for the design, use and acceptance of smart healthcare systems. The second part of the chapter shows how these disciplinary challenges were addressed within the eHealth project, an interdisciplinary research project at RWTH Aachen University.
DOI: 10.4018/978-1-60960-469-1.ch004
77
A Multi-Disciplinary Approach to Ambient Assisted Living
INTRODUCTION
The increased life expectancy and improved general health states of citizens in most western countries will inevitably result in more and more elderly people requiring medical care in the near future (Wittenberg et al., 2006). At the same time, considerable bottlenecks arise from the fact that increasingly fewer people are present, who may take over the nursing (Leonhardt, 2005). In order to master the requirements of an aging society, innovations in information and communication as well as medical engineering technologies come to the fore, which offer novel or improved medical diagnosis, therapy, treatments and rehabilitation possibilities (Weiner et al., 2003; Warren & Craft, 1999). Though, recent research shows that accep-tance barriers are prevalent, which might be due to the fact that development praxis predominately focuses on technical feasibility, while the “human factor” in these systems is fairly underdeveloped. In order to fully exploit the potential of e-health applications, acceptance and usability issues of e-health applications need to be considered, especially for older users, who have specific needs and requirements regarding usability and acceptance issues (Melenhorst et al., 2006; Arning & Ziefle, 2009; Zimmer & Chappell, 1999). As the knowledge about the antecedents of e-health acceptance and utilization behavior is restricted, it is necessary to explore the acceptance and fit of e-health technologies within homes and private spheres (Wilkowska & Ziefle, 2009; Gaul & Ziefle, 2009; Röcker & Feith, 2009).
DISCIPLINARY CHALLENGES
The following sections outline the research challenges encountered in the fields of medi-cal engineering, computer science, psychology, communication science, and architecture as well as their consequences for the design, use and ac-ceptance of smart healthcare systems.
Medical Engineering
Major changes in the demographic and social structure of most western countries bring up new challenges, not only for the health care systems in general, but also for the development of new medical technologies. In such an aging society, where medical progress leads to a considerably increased life expectancy, age-related chronic diseases require constant medical assistance by a new generation of medical care equipment (Röcker et al., 2010). In situations, where patients cannot be treated in institutional setting alone anymore, individual and personalized care in the patients’ home environment plays a more and more impor-tant role (Ziefle et al., 2009).
Those technologies and devices have to pro-vide the essential, established attributes of today’s medical devices, to be functional, safe and reliable, but furthermore in the future they also have to be mobile (can be used in professional and home environments), adaptive (can be run by patients and professionals) and ergonomic (easy to use and accepted by users). To implement those new aspects in medicine technology is a great chal-lenge because most medical devices influence the patients´ health in a direct way and are highly critical in terms of patient safety. The decentral-ized application of such devices puts users in the centre of attention and it will give them a high degree of independency and self-control of the therapy, but also a high degree of responsibility.
The most important modification in the de-velopment approaches in the field of medical engineering is to include the user actively in the design process. A coherent user-centered design of medical devices will result in a medical technol-ogy, which is not only functional in an engineering way of thinking, but also addresses fundamental user needs in terms of appearance, ease of use and privacy.
Especially medical assistance devices for the elderly are often perceived to be stigmatizing and therefore not used efficiently. One example is the
78
A Multi-Disciplinary Approach to Ambient Assisted Living
emergency button, which is supposed to be used by fragile patients in case of an emergency event (e.g., fall) where external help is required (Beul et al., under revision; Klack et al., under revision). Most of the users don’t carry that device with them because it marks them as diseased or dependent. Another example is rehabilitation therapy, where the therapy success is often decelerated because patients do not want to wear medical equipment in public or even at home because they feel stig-matized. But even in life critical situations patients sometimes decide against the implantation of a medical device because their fear of a loss of control or independency is to high. In the light of these problems, a user-centered design approach bears a high potential for the optimization of therapy compliance and overall therapy success.
With a focus on an aging society, one of the most striking challenges for medical engineers is to develop medical support devices for the needs of the elderly, and especially for chronically diseased people in their home environments. The develop-ment of sensor devices, which can monitor the patients vital data, identify emergency situations, as well as discover slow changes or trends in the patients health state and give preventive advise is promising. In order to achieve a broad user acceptance and even a desire for those systems
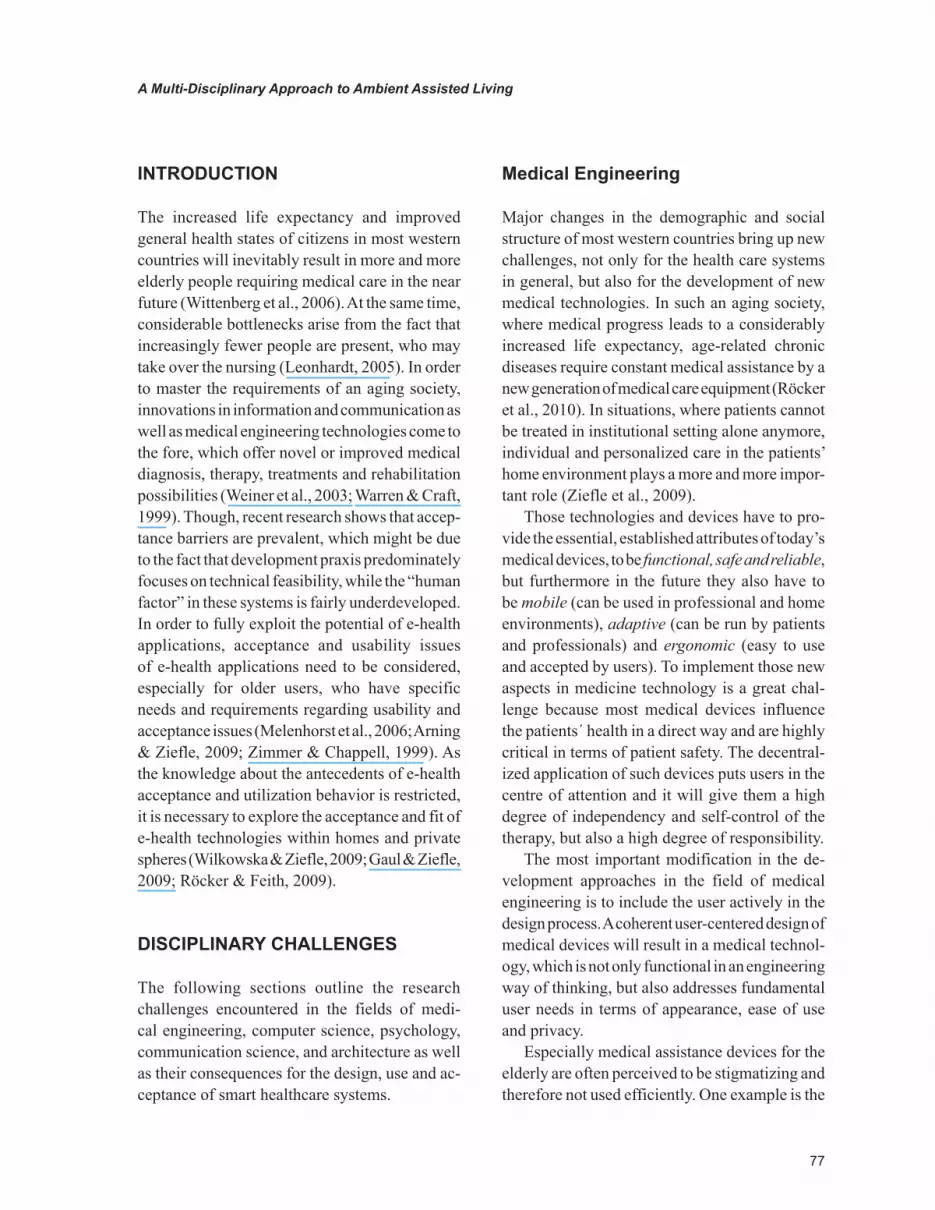
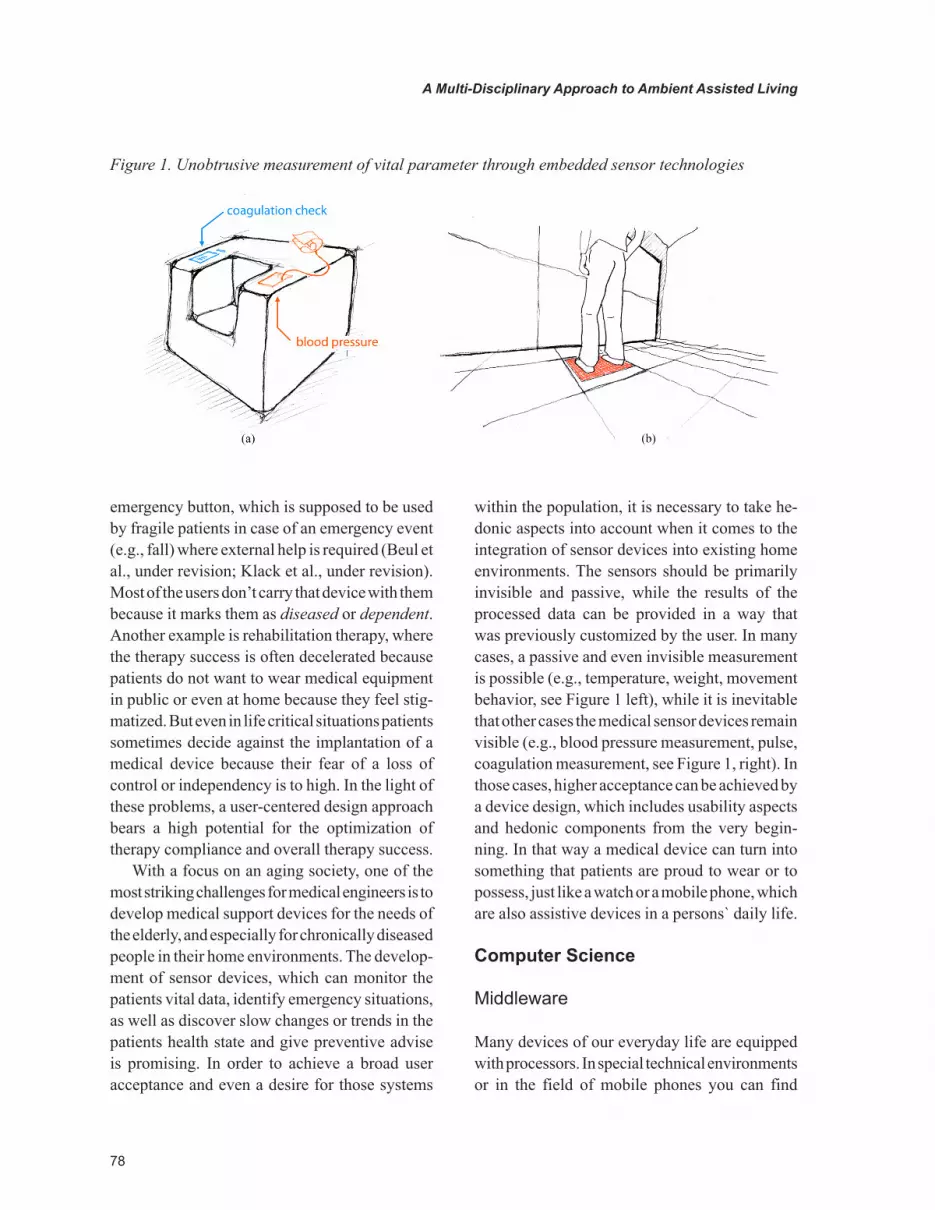
within the population, it is necessary to take he-donic aspects into account when it comes to the integration of sensor devices into existing home environments. The sensors should be primarily invisible and passive, while the results of the processed data can be provided in a way that was previously customized by the user. In many cases, a passive and even invisible measurement is possible (e.g., temperature, weight, movement behavior, see Figure 1 left), while it is inevitable that other cases the medical sensor devices remain visible (e.g., blood pressure measurement, pulse, coagulation measurement, see Figure 1, right). In those cases, higher acceptance can be achieved by a device design, which includes usability aspects and hedonic components from the very begin-ning. In that way a medical device can turn into something that patients are proud to wear or to possess, just like a watch or a mobile phone, which are also assistive devices in a persons` daily life.
Computer Science
Middleware
Many devices of our everyday life are equipped with processors. In special technical environments or in the field of mobile phones you can find
Figure 1. Unobtrusive measurement of vital parameter through embedded sensor technologies
79
A Multi-Disciplinary Approach to Ambient Assisted Living
some specific communication, but in broad areas inter-device communication is not taking place (Bottaro & Gérodolle, 2008). In order actively support people in their homes integrated sensors and actuators have to communicate intensively, giving the system context information on what is going on. This task is a huge challenge in technical sense. Within the context of our project, we do not only look at the technical integration of different devices, spatial sensors, multimedia, personal and medical devices, but also on the usability and acceptance of smart homecare applications based on these new systems (Röcker et al., 2010).
One of the main goals of our investigations is the generation of reliable context. While a considerable amount of work has been done on context awareness, usability aspects are largely unexplored due to their tremendous complexity (Ye et al., 2008). Furthermore, capturing and aggregating personal data could lead to serious privacy infringements, especially in home envi-ronments, which are traditionally perceived as very private places (Armac et al., 2009; Röcker & Feith, 2009). Thus, the integration of privacy aspects in context-adapted frameworks is another focus of our work.
As a precondition of further steps, the contex-tual data of all input devices has to be integrated
on a middleware platform. Besides the OSGi-based OpenAAL platform, which has been developed in the SOPRANO project (Wolf et al., 2008), a follow-up of the AMIGO project (Vallée et al., 2006), there are also other interesting approaches. The Distributed Wearable Augmented Reality Frame-work (DWARF) developed at the Technical Uni-versity Munich (Bruegge & Klinker, 2005), has its focus on mobile nodes. Another framework focusing on mobile, autonomous nodes is the OpenWings framework, which is hosted by Gen-eral Dynamics and mainly used for military purposes. The Java Context Awareness Framework (JCAF) by Badram (2005) is still not very broad-ly implemented. Similar commercial frameworks are COBA of LONIX Ltd., Finland, or the dSS of digitalSTROM.org, Switzerland, where the latter mainly aims on energy management at home.
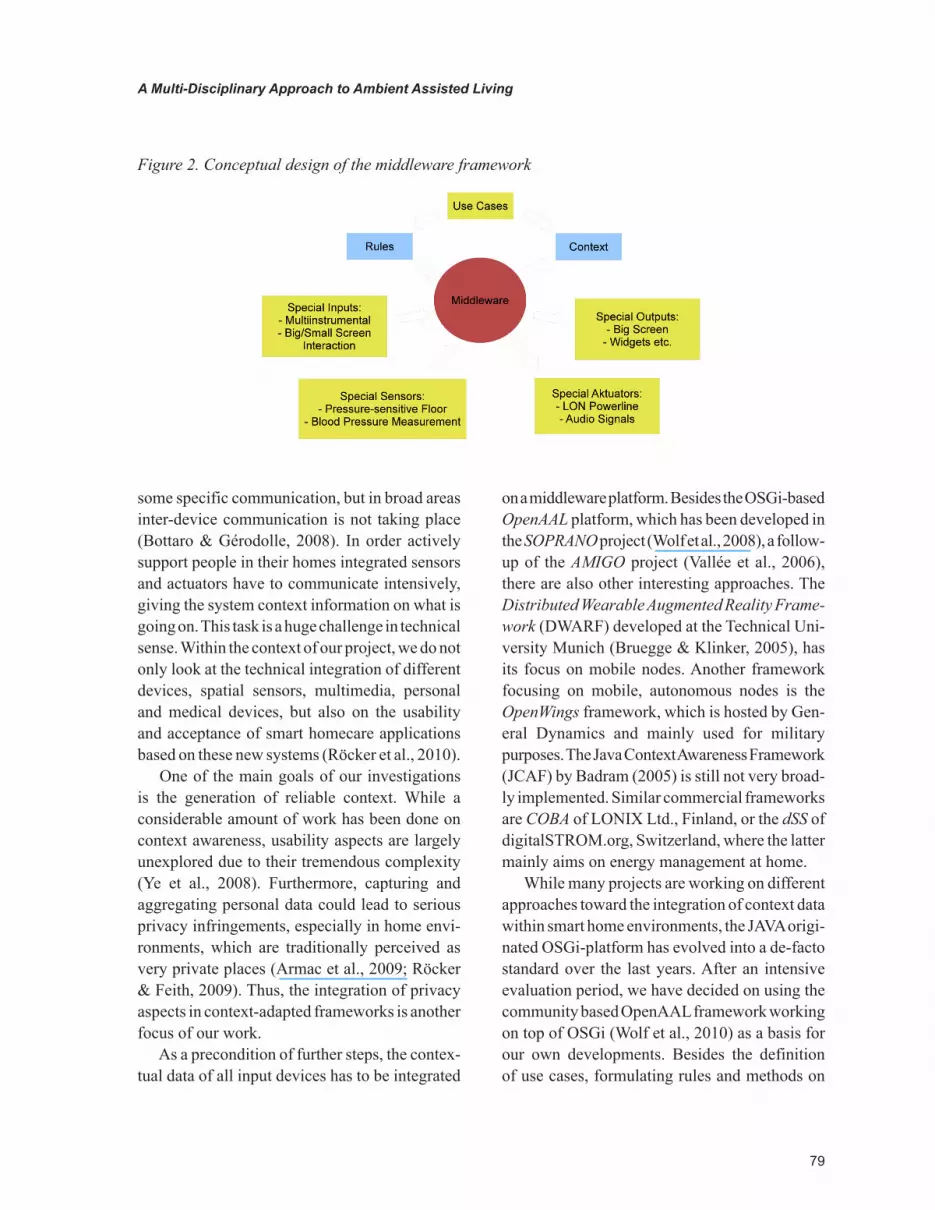
While many projects are working on different approaches toward the integration of context data within smart home environments, the JAVA origi-nated OSGi-platform has evolved into a de-facto standard over the last years. After an intensive evaluation period, we have decided on using the community based OpenAAL framework working on top of OSGi (Wolf et al., 2010) as a basis for our own developments. Besides the definition of use cases, formulating rules and methods on
Figure 2. Conceptual design of the middleware framework

80
A Multi-Disciplinary Approach to Ambient Assisted Living
aggregating and analyzing the vast amount on input data towards reasonable context will lead to higher acceptance of the suggested technologies. In addition to usual sensors and actuators, our lab covers work on big screens and their usability as well as the seamless integration of medical devices, starting with chronic heart diseases and evolving into ambient assistance in a wider sense (Klack et al., 2010).
User Interfaces
In contrast to traditional information and com-munication technologies, assistive medical devices are mostly used by older and diseased persons, who have very specific needs (Ziefle, 2010). Compared to the average computer user, older people differ considerably regarding their cognitive as well as motor skills. As known from a vast body of literature (see, e.g., Craik & Sal-thouse, 1992 or Fisk & Rogers, 1997) the ageing process impedes the interaction of older users with technical devices to a considerable extent. Age-related changes in the cognitive system usually lead to a decline in working-memory capacities and cause a general slow down in processing speed as well as a reduction of spatial abilities (Pak, 2001). As a result, persons with reduced spatial abilities frequently experience disorienta-tion when navigating through menu structures of computer systems. A reduced working memory capacity hampers the untroubled menu navigation additionally, especially when using small screen devices, where the provision of optimized or ad-ditional information is often not possible due to the limited screen estate (Ziefle & Bay, 2006). In the context of medical technology usage such declines become especially critical when task demands are high, as for instance when using novel or complex devices, or when it is the mat-ter of sensitive data like in health-related context. As a result, older people face greater difficulties in extracting relevant information from techni-cal systems or they are simply overwhelmed by
the high information density in applications and technical devices.
When discussing aging and technology usage, the willingness of older people to use computer technology or to interact with medical systems is a crucial aspect that needs to be carefully consid-ered. A number of earlier studies (e.g., Wilkowska & Ziefle, 2009) examining the interaction with technology have shown that the success of tech-nological innovations is largely influenced by the extent to which users accept the technology. Empirical evidence suggests that different age groups have different reasons to accept or reject medical technologies. In this context, it is very likely that the actual impulse to use a specific device is largely influenced by motivational fac-tors. On the one hand, usage motives are related to perceived advantages and gains, which at the same time support the positive attitude toward the technology. However, disadvantages and barriers can overshadow the intended interaction, and – as a consequence – provoke an averseness to accept and use the system. On the other hand, user mo-tives to employ medical technologies might also interact with the their individual characteristics such as gender, educational level, previous tech-nical learning history or the resulting technical self-confidence. Thus, emotional factors need to be carefully considered in the analyses of usability and acceptability aspects of medical systems.
Psychology
In the history of information technology (IT) there was long enough a perfunctory development of technical devices, systems and applications that disregarded or simply did not include users and their opinions about the products’ usability, accep-tance or design. From an economical perspective, this resulted frequently in higher expenditure and additional costs in comparison to the yielded ben-efits. Nowadays, it seems indeed to be increasingly realized that technical products are accepted and utilized by the people only if usability issues are

81
A Multi-Disciplinary Approach to Ambient Assisted Living
appropriately considered within device designs (e.g., cognitive complexity, key design, navigation structure, icon usage, language usage - naming and categorizing of function names -, and com-munication dialogues), because technical end products without such framework conditions are foredoomed to fail in an age of global economical crisis with keen competition in IT sector.
Thus, integrating potential customers into development of technical systems from the be-ginning on is indispensable. Especially in case of Ambient Assisted Living and Smart Healthcare systems this is of great importance for at least two reasons. Firstly, for most people there is no other place, which is more intimate and confiding than “the own four walls”. Yet, according to Maslow’s Hierarchy of Needs (Maslow, 1954) accommoda-tion is extremely important in human’s life for reasons of perceived safety, and it belongs to the basic human needs to feel protected, stable and secure. Secondly, health is the greatest wealth and therefore a very sensitive and delicate topic – there is no higher good than this and everyone tries to protect it as long as somehow possible. Thus, putting these two relevant aspects of human life together, it is all the more understandable that the involvement of end users, their perspectives, wishes and needs, into every step of the develop-ment process plays a great role for a successful rollout. The integration, though, is connected with some considerable challenges.
First of all, Ambient Assisted Living enhanced by modern health supporting technologies is connected with plenty of emotions: barriers and restraints on the one hand, as well as motivational aspects and positive stimuli to perceive the ad-vantages of such a tool on the other hand. Also, in contrast to traditional information technologies, medical assistance devices address mostly older, frail and diseased people, whose health condition, i.e. some of their vital parameters (e.g., blood pressure, body temperature, weight), have to be regularly controlled. However, elderly as well as chronically ill or handicapped persons have very
specific and wide-ranged needs requiring from modern medical systems individually adapted input and output devices. For instance, there is another need regarding the communication with the system for a mobility-impaired person in comparison to a user with hearing deficien-cies but otherwise unlimited mobility. The same problem applies to the cognitive skills, or more specifically to their degree of decline, to techni-cal self-confidence and not at least to the will-ingness to use such modern technologies in the own home. Hence, there is a great necessity for a comprehensive and sensible identification of factors that influence the usage behavior of such medical systems. In addition, it should be kept in mind that all the processes, trends and mean-ings about technology as well as health states and abilities may change over the years. This fact alone demands an enormous flexibility and adaptability from the assistive devices. Reflect-ing this dynamic character of human progress it follows that different input and output modalities are necessary for covering the broadest possible range of existing requirements in order to assure the users’ straightforward interaction with a system. While sophisticated technological solutions are on the threshold to merge, the analysis of actual user needs and the identification of appropriate interaction modalities still remains a challenge from a psychological perspective.
In order to meet the complexity of users’ de-mands and to understand the resulting acceptance patterns, complex methodology is necessary. Thereby, not only for satisfaction reasons of sci-entific ethos, but especially because of preferably highest effectiveness of psychological analysis, both qualitative and quantitative methods are essential.
For the examination of different aspects influ-encing acceptance and usage behavior of medi-cal assistance technology (e.g., users’ diversity, requirements, motivational factors, barriers) a user-centered approach is needed that consid-ers characteristics of highly heterogeneous user
82
A Multi-Disciplinary Approach to Ambient Assisted Living
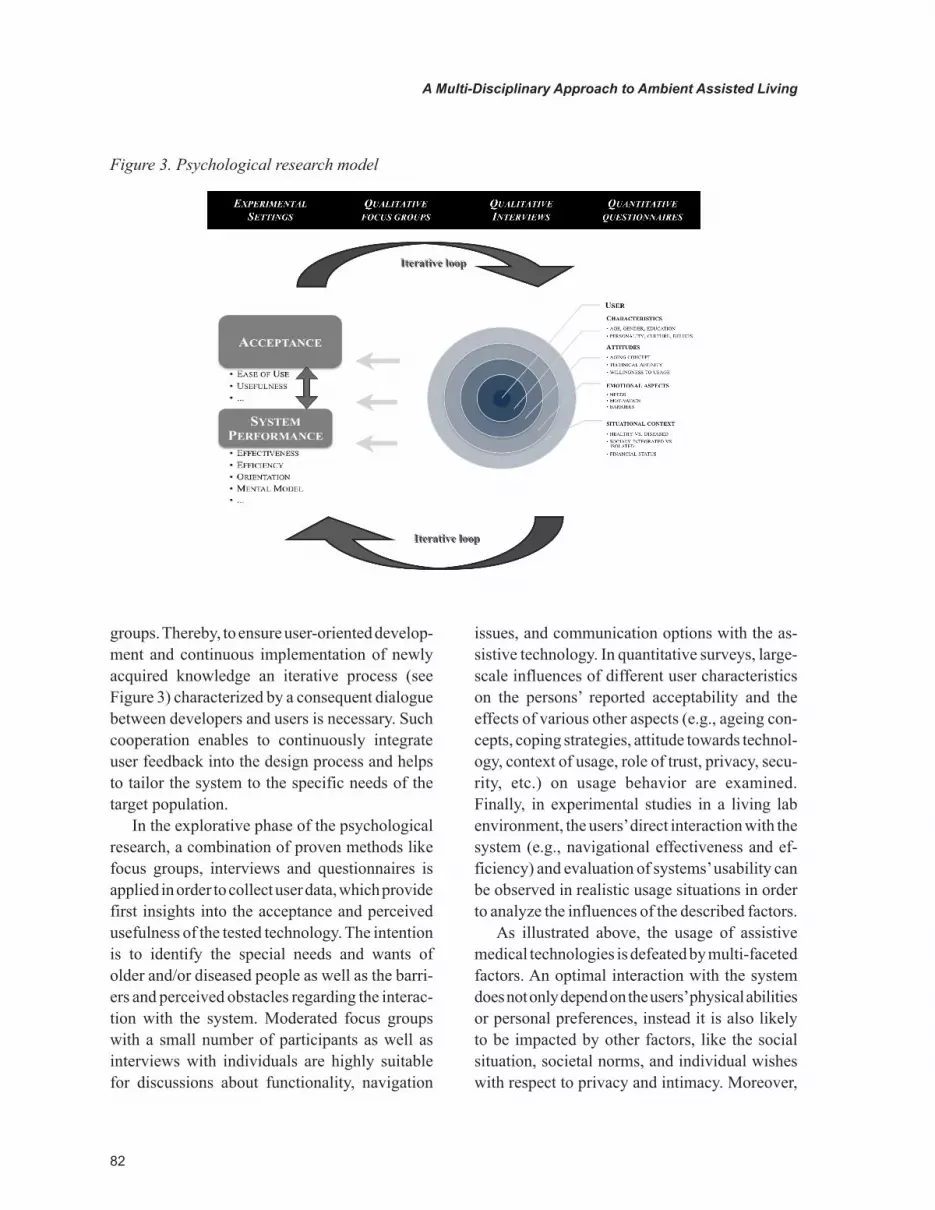
groups. Thereby, to ensure user-oriented develop-ment and continuous implementation of newly acquired knowledge an iterative process (see Figure 3) characterized by a consequent dialogue between developers and users is necessary. Such cooperation enables to continuously integrate user feedback into the design process and helps to tailor the system to the specific needs of the target population.
In the explorative phase of the psychological research, a combination of proven methods like focus groups, interviews and questionnaires is applied in order to collect user data, which provide first insights into the acceptance and perceived usefulness of the tested technology. The intention is to identify the special needs and wants of older and/or diseased people as well as the barri-ers and perceived obstacles regarding the interac-tion with the system. Moderated focus groups with a small number of participants as well as interviews with individuals are highly suitable for discussions about functionality, navigation
issues, and communication options with the as-sistive technology. In quantitative surveys, large-scale influences of different user characteristics on the persons’ reported acceptability and the effects of various other aspects (e.g., ageing con-cepts, coping strategies, attitude towards technol-ogy, context of usage, role of trust, privacy, secu-rity, etc.) on usage behavior are examined. Finally, in experimental studies in a living lab environment, the users’ direct interaction with the system (e.g., navigational effectiveness and ef-ficiency) and evaluation of systems’ usability can be observed in realistic usage situations in order to analyze the influences of the described factors.
As illustrated above, the usage of assistive medical technologies is defeated by multi-faceted factors. An optimal interaction with the system does not only depend on the users’ physical abilities or personal preferences, instead it is also likely to be impacted by other factors, like the social situation, societal norms, and individual wishes with respect to privacy and intimacy. Moreover,
Figure 3. Psychological research model

83
A Multi-Disciplinary Approach to Ambient Assisted Living
different users face various difficulties in this interaction. Thus, the understanding of users’ capabilities and limitations as well as the detection of possible influences, which determine a smooth and ergonomically favorable interaction with the assistive technology, is the task and the goal of psychology in this multidisciplinary approach.
Communication Science
Monitoring older and/or chronically ill people requires the implementation of tele-medical ser-vices in an AAL system. Physicians and patients have to communicate regularly with each other for exchanging and discussing medical data con-cerning the patients’ conditions, adjusting their treatment (e.g., medication) and negotiating their conditions. Due to the demographic change, the number of medical professionals declines while the number of (older) patients increases (Beul et al., 2010). Moreover, older patients’ mobility di-minishes because of the appearance of senescence or disease phenomena (Mollenkopf et al., 2004). Therefore, the human resources of doctors have to be allocated as efficient as possible, while at the same time the treatment of patients has to be organized as comfortable as possible. For this reason, tele-medical services between doctors and patients in their homes are a promising solution. To put this vision into practice, three major challenges have to be met: grasping and operationalizing the communicative scenario, realizing face-to-face interactions on novel types of information and
communication technologies (ICT) like, e.g., wall-sized interactive displays, and enhancing the participants trust in the tele-medical service.
Doctor-patient communication is traditionally taking place in a face-to-face interaction (Roter & Hall, 1989): Patients either consult doctors in their surgery or doctors visit patients in their home environment. With the implementation of an ICT-based communication channel, both par-ties can stay in their original location. Because neither party moves physically, their perspectives on the communicative scenario diverge. Thus, it cannot be classified clearly as a surgery visit by the patient or a home visit by the physician, which leads to the challenge of characterizing the com-municative scenario in this tele-medical service.
Furthermore, the formerly physically realized interaction has to be transferred into a media-supported interaction with an interactive wall. For this, it is necessary to identify patients’ and doctors’ requirements on the design of the communication channel. The appropriate communicative modes dependent on user types have to be detected (e.g., verbal only interaction, combination of images and verbal interaction, or video interaction). In addi-tion, the usage of an interactive wall for the real-ization of doctor-patient communication opens up new opportunities with respect to the presentation of the interlocutor: Owing to the size of the screen, it is possible to interact while walking, standing or sitting in the room. Additional media (e.g., X-ray images) can be integrated into the interaction to facilitate the participants understanding.
Figure 4. Possible perspectives of patients on the doctor

84
A Multi-Disciplinary Approach to Ambient Assisted Living
On account of these new possibilities of pre-sentation, personal preferences of the interlocutors have to be identified. The support of individual communicative skills, styles and strategies of the participants should be considered, too.
Lastly, the patients’ and doctors’ requirements on the design and the features of the tele-medical service, realized as an application, should be investigated. One key feature of the tele-medical service is the exchange of medical data (e.g., blood pressure and blood coagulation data) between doc-tor and patient as a precondition for the medical consultation. The data can be seen as the subject of their talk. Therefore, privacy and trust issues must be regarded. Feedback reports have to be imple-mented to inform patients about the transfer of their medical data and to give them a feeling of control over their data. Besides feedback, the graphical user interface must be designed user-friendly to increase the participants’ trust in the system (Fruhling & Sang, 2006). Cognitive-ergonomic issues as well as linguistic and semiotic means have to be considered to contribute to a pleasur-able usage of the application (Wirtz et al., 2010).
Architecture
In the course of advancements in sustainable building design, buildings are changing from being static to dynamic. Building automation and intel-ligence are allowing for automated maintenance making buildings adaptable and reactive to envi-ronmental changes. Temperature, humidity, and position of the sun are typical parameters that an intelligent building reacts to, in order to optimize climate and ergonomics of the working or living environment it houses. Apart from adaptability to environmental changes, technological advances provide more potential in integrating modern technology into buildings and homes. Especially, elderly and ill inhabitants can benefit consider-ably from medical technology that is seamlessly integrated into their apartments. The concept of Ambient Assisted Living integrates information
and communication technology, and sensors into the everyday living environment. Buildings will no longer “only” react to environmental changes, but also to the context and the situation of the user.
As described earlier, medical technology can be stigmatizing if visually prominent with explicit focus on the disease of the patient. This stigma can be potentially minimized especially with information and communication technology that has long overcome exclusiveness in purpose. Hence, hedonic aspects have to be taken into ac-count along with ergonomics and usability when designing health technology, as they will greatly affect the acceptance and actual use of the de-vice or the system. The less medical technology is visible, the more it becomes part of the room and eventually the architecture. But how do users interact with rooms and architecture in general? Human-Computer Interaction (HCI) covers the broad field of research and development between technology and technical products on the one hand and human factors on the other hand (Dix et al., 2003). With the technological advances, research in HCI today includes addressing challenges in creating intuitive, easy to use and elegant interfaces for mobile, wearable and ubiquitous technology. As information and communication technologies are not longer restricted to technical products but increasingly enter living spaces, HCI research will also need to cover architectural issues.
Rapid advances in display technology in the recent years, large displays are entering our everyday urban experience. Important informa-tion is displayed in train stations and airports, advertisements are shown on facades and LED billboards, and events are broadcasted on large screens for public viewing. It is only a matter of time before large displays will also find their way into our homes. As walls become displays, they become part of an architectural space. Kasugai et al. (2010) introduce the concept of spatially, func-tionally and socially extending a space through large screen technology in an Ambient Assistive Living environment.

85
A Multi-Disciplinary Approach to Ambient Assisted Living
Wenger et al. (1996) state that lack of social support and networks as well as changing health can lead to the feeling of loneliness and seclud-edness, which is correlated with old age, often resulting in the emergence of depression. Socially extending a space can potentially help overcome these feelings. Creating social network ties may help people to protect their health and to develop coping strategies (Penninx et al., 1999).
By spatially extending a room and seamlessly merging virtual and physical spaces, new standards of communication between doctors and patients can be established (Kasugai et al., 2010). This provides an opportunity to immerse users into a life-like videoconference, who were previously not exposed to any video chat technology.
In this context, the main architectural challenge we seek to address in our research is to combine, integrate and answer medical demands, as well as usability and technology acceptance aspects in an architecturally satisfying space.
TOWARDS A MULTI-DISCIPLINARY SOLUTION
eHealth – Enhancing Mobility with Aging
The project “eHealth – Enhancing Mobility with Aging” aims at approaching the disciplinary challenges outlined above in an integrative and multidisciplinary fashion. The project started in January 2009 as part of the Human Technology Centre, a newly established project house, funded by the Excellence Initiative of the German fed-eral and state governments. Its main focus is on the design of adaptive immersive interfaces for personal healthcare systems and the development of novel, integrative prototypes of user-centered healthcare systems. This includes new concepts of electronic monitoring systems within ambient living environments, suited to support persons in-dividually (according to user profiles), adaptively
(according to the course of disease) and sensitively (according to living conditions).
Threefold Strategy
Due to the complexity of the topic, the inter-disciplinary research concept includes three complimentary strategies: (1) Methodological Strategy: The project bridges competencies of different disciplines in order to develop a truly interdisciplinary approach for a human-centered development of future healthcare technologies. (2) Spatial Strategy: As a continuous exchange of ideas is needed, and the disciplinary perspectives have to be transformed into an interdisciplinary methodology, a new research house, the Human Technology Centre, was created that allows the teams to research under one roof. At the same time, researchers maintain close relationships to their “home” institutes, enabling continuous exchange of disciplinary and interdisciplinary knowledge. (3) Educational Strategy: Through its integration into the academic context, the e-health program offers young academics the opportunity to par-ticipate in interdisciplinary research quite early in the educational process. In addition, new teaching concepts, as, e.g., the interdisciplinary school of methods, foster holistic education concepts and form the next generation of researchers.
Overall Research Goals
The three-year research plan focuses on homecare solutions for patients with chronic heart disease as a key application with high clinical demand, recurrent hospital stays, high morbidity, and mor-tality. Due to ageing, incidence and prevalence is considerably increasing (Murray et al., 1994). The project follows a multidisciplinary approach regarding the development of user-centered smart healthcare technologies, which integrate perspec-tives of different disciplines, including computer science, medicine, engineering, psychology, com-munication science and architecture.

86
A Multi-Disciplinary Approach to Ambient Assisted Living
The research duties aim at age-sensitive con-cepts for technical devices within living environ-ments enabling old and ill patients suffering from chronic heart disease to live independently at home. Devices should be perceived as personally helpful, supportive, safe and secure, and should evoke feelings of trust and reliability, while at the same time respect patients’ desire for intimacy, independence, and dignity. In addition, the way devices are communicating with their owners must be easily understandable at any time. Devices are conceptualized as context-adaptive, smart and im-mersive. Thus, they are not only communicating with patients, but also with the environment (fur-niture, walls, floor), family members, doctors or emergency personnel. The main issues addressed within the project are the systematic evaluation and consecutive optimization of the interrelation of medical, environmental, technical, communica-tive, psychological and social factors, and their consequences for the design, use and acceptance of personal healthcare systems.
Integrative Approach
To examine how patients communicate with smart homecare environments, how they deal with invis-ible technology, and how the information is to be delivered such that it meets the requirements of timeliness, data protection, dignity as well as medi-cal demands, an experimental space is necessary, which enables to study patients “life at home”. It is planned to develop a full-scale prototype room as part of a smart apartment in order to test various smart healthcare systems. The room will consist of a simulated home environment, which enables researchers to use experimental interfaces with test persons of different ages and health states. Out of validity reasons, the experimental space is of central importance, as patients and care givers need to experience and “feel” the technology to be used, in order to fairly evaluate it (Woolham & Frisby, 2002). Further, persons might overempha-size their sensitiveness towards privacy violations
if their judgments only rely on the imagination of using it (Cvrcek et al., 2006).
Therefore, different evaluation methods and scenarios will be used, ranging from empirical and experimental procedures, psychometric testing, questionnaire methods and behavioral observations. In order to realize this ambient living concepts, which represent the daily situ-ation of patients at home, communication and interaction mechanisms as well as bio signals have to be integrated into architectural concepts and components (furniture, walls, floor).
The design will follow several cycles, in which the technological design is carefully harmonized and weighted with acceptance and/or usabil-ity demands. Patients differing in gender, age, health status, emotional and cognitive factors, and severity of disease will be involved in the design cycles. In a first step, we will concentrate on the two opposite ends of the design space, a small personal device (“a medical helper”) and an interactive wall, with which patients can directly interact. In a second step, a smart floor will be included to complement the smart environment.
The complexity of the topic and the concurrent research of many different disciplines need a spe-cific working rationale, in which each discipline has its own research focus (following disciplinary research habits), but at the same time an inter- and transdisciplinary working mode, in which the different parts are combined and harmonized.
Figure 5. Iterative design cycle illustrating the interdisciplinary research approach

87
A Multi-Disciplinary Approach to Ambient Assisted Living
Visualizing this novel approach, in Figure 5, the working mode of the different disciplines, their interlocking within the iterative cycle of user-centered designs is pictured.
First Steps towards a Living Lab Environment
Currently, first technical components of the intel-ligent home environment are built. As such, inter-acting mechanisms, cognitive ergonomic issues of the interface, but also spatial, architectonical and communication demands are discussed, conceptualized, realized and iteratively tested. Figure 6 shows a vision scribble of the interactive environment with a large-scale interactive wall and a smart floor.
From a medical-engineering perspective, a flexible, home-based therapy assistance system for people with different health and life conditions has to be created. The medical focus considers a
broad range of disease states, ranging from persons with beginning coronary, ischemic or hypertensive heart diseases, heart failures or congenital heart diseases up to high-urgency transplant patients. Though the medical focus is on chronic heart patients, the system is open for a much larger range of users. The sensoric part of the system consists of biosensors that acquire patients’ vital data. A special middleware merges different data streams and analyses the data on a central proces-sor unit. The actoric part provides therapeutic advises to the patient and, in case of blood pump patients, optimizes the performance of the me-chanical assistive device based on patients’ ac-tual vital conditions. Our field studies (Alagöz et al., 2010) in leading heart centers (Bad Oeynhau-sen, Germany and Leuven University, Belgium) showed that four prominent vital parameters are essential: blood pressure, blood coagulation, body temperature, and weight. To achieve this, various state-of-the-art sensor technologies for non-
Figure 6. Vision scribble of the interactive environment

88
A Multi-Disciplinary Approach to Ambient Assisted Living
contact or minimal invasive vital data monitoring will be evaluated in our living lab. In parallel, first studies regarding users’ acceptance of medical home technology are currently running, which take users of different age, upbringing and health states into account.
OUTLOOK & FUTURE WORK
The insights gained during the formative studies will be used to design the “Future Care Lab”, an experimental space for studying users’ “life” at home and examining how they interact and com-municate with invisible technology (Ziefle et al., 2009). The lab will enable to explore how future homecare environments have to be designed such that they meet technical and medical requirements and at the same time satisfy fundamental user needs regarding data protection, dignity, and intimacy.
Within the Future Care Lab, the development of user-centered smart healthcare technologies will be realized by a truly multidisciplinary team of individuals coming from the fields of psychol-ogy, communication science, computer science, medicine, engineering, and architecture. The Fu-ture Care Lab will provide a full-scale technical infrastructure to test various immersive systems. It will consist of a simulated home environment, which allows researchers to use various prototype interfaces with test persons of different ages and health states.
The lab will provide an intelligent care in-frastructure, consisting of different mobile and integrated devices, for supporting elderly people in technology-enhanced home environments. The setup of the lab will enable in-situ evaluations of new care concepts and medical technologies by observing different target user populations in realistic usage situations. As the lab will rely on a modular technical concept, it will be possible to expand it with other technical products, systems and functionalities, in order to address different user groups as well as individuals with differ-
ences in their cognitive, health-related or cultural needs. By this the lab will have the potential to be sensibly adapted to new technical developments as well as societal changes and needs.
ACKNOWLEDGMENT
This research was funded by the Excellence Initia-tive of the German federal and state governments.
REFERENCES
Alagöz, F., Wilkowska, W., Roefe, D., & Klack, L. Ziefle, M. & Schmitz-Rode (2010). Technik ohne Herz? Nutzungsmotive und Akzeptanzbarrieren medizintechnischer Systeme aus der Sicht von Kunstherzpatienten. In Proceedings of the Third Ambient Assisted Living Conference (AAL’10), Berlin, Germany: VDE. CD-ROM.
Armac, I., Panchenko, P., Pettau, M., & Retkowitz, R. (2009). Privacy-Friendly Smart Environments. In K. Al-Begain (Ed.). Proceedings of the Third International Conference and Exhibition on Next Generation Mobile Applications, Services and Technologies (NGMAST 2009), Cardiff, U (pp. 425-431). London: IEEE Computer Society, 2009.
Arning, K., & Ziefle, M. (2009). Effects of cognitive and personal factors on PDA menu navigation performance. Behaviour & Information Technology, 28(3), 251–268. doi:10.1080/01449290701679395
Arning, K., & Ziefle, M. (2009). Different Per-spectives on Technology Acceptance: The Role of Technology Type and Age. In Holzinger, A., & Miesenberger, K. (Eds.), Human – Computer Interaction for eInclusion. LNCS 5889 (pp. 20–41). Berlin, Heidelberg: Springer.

89
A Multi-Disciplinary Approach to Ambient Assisted Living
Bardram, J. E. (2005). (JCAF) – A Service In-frastructure and Programming Framework for Context-Aware Applications. In Pervasive Com-puting (pp. 98–115). The Java Context Awareness Framework. doi:10.1007/11428572_7
Beul, S., Klack, L., Kasugai, K., Möllering, C., Röcker, C., Wilkowska, W., & Ziefle, M. (2010). Between Innovation and Daily Practice in the Development of AAL Systems: Learning from the experience with today’s systems. 3rd International ICST Conference on Electronic Healthcare for the 21st century (ehealth 2010).
Beul, S., Mennicken, S., Ziefle, M., & Jakobs, E.-M. (2010). What Happens After Calling the Ambulance: Information, Communication, and Acceptance Issues in a Telemedical Workflow. In C.A Shoniregun & G.A. Akmayeva (Eds.). In Proceedings of the International Conference on Information Society (pp. 111-116). London: Infonomics Society.
Bruegge, B., & Klinker, G. (2005). DWARF - Dis-tributed Wearable Augmented Reality Framework (White Paper). Technische Universität München, Chair for Applied Software Engineering.
Craik, F. I. M., & Salthouse, T. A. (1992). Hand-book of Ageing and Cognition. Hillsdale, NJ: Lawrence Erlbaum Associates.
Cvrcek, D. Kumpost, M., Matyas, V., & Danezis, G. (2006). A Study on the Value of Location Pri-vacy. In: Proceedings of the ACM Workshop on Privacy in the Electronic Society (pp. 109-118). New York: ACM.
Dix, A., Finlay, J., Abowd, G., & Beale, R. (2003). Human-Computer Interaction (3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Fisk, A. D., & Rogers, W. A. (1997). Handbook of Human Factors and the Older Adult. San Diego, CA: Academic Press.
Fruhling, A., & Lee, S. M. (2006). The Influence of User Interface Usability on Rural Consumers’ Trust of e-Health Services. International Journal of Electronic Healthcare, 2(4), 305–321.
Gaul, S., & Ziefle, M. (2009). Smart Home Technologies: Insights into Generation-Specific Acceptance Motives. In Holzinger, A. (Eds.), Hu-man – Computer Interaction for eInclusion. LNCS 5889 (pp. 312–332). Berlin, Heidelberg: Springer.
Hauber, J., Regenbrecht, H., Billinghurst, M., & Cockburn, A. (2006). Spatiality in videoconfer-encing: trade-offs between efficiency and social presence. In CSCW ’06: Proceedings of the 20th anniversary conference on computer supported cooperative work (pp. 413–422). New York: ACM.
Kasugai, K., Ziefle, M., Röcker, C., & Russell, P. (2010). Creating spatio-temporal contiguities between real and virtual rooms in an assistive living environment. In Bonner, J., Smyth, M., O’Neill, S., & Mival, O. (Eds.), Proceedings of create 10 (pp. 62–67). Loughborough, UK: Institute of Ergonomics & Human Factors.
Klack, L., Kasugai, K., Schmitz-Rode, T., Röcker, C., Ziefle, M., Möllering, C., et al. (2010). A Personal Assistance System for Older Users with Chronic Heart Diseases. In: Proceedings of the Third Ambient Assisted Living Conference (AAL’10). Berlin, Germany: VDE (CD-ROM).
Klack, L., Möllering, C., Ziefle, M., & Schmitz-Rode, T. (2010). Future Care Floor: A sensitive floor for movement monitoring and fall detection in home environments, 1st International ICST Conference on Wireless Mobile Communication and Healthcare - MobiHealth 2010.
Leonhardt, S. (2005). Personal Healthcare De-vices. In S. Mekherjee et al. (Eds.), Malware: Hardware Technology Drivers of AI (pp. 349-370). Dordrecht, NL: Springer.
Maslow, A. (1954). Motivation and Personality. New York: Harper.
90
A Multi-Disciplinary Approach to Ambient Assisted Living
Melenhorst, A.-S., Rogers, W., & Bouwhuis, D. (2006). Older Adults’ Motivated Choice for Technological Innovation. Psychology and Aging, 21(1), 190–195. doi:10.1037/0882-7974.21.1.190
Mollenkopf, H., Marcellini, F., Ruoppila, I., & Tacken, M. (2004). Ageing and Outdoor Mobility. A European Study. Amsterdam: IOS Press.
Murray, D., Hannan, P. J., Jacobs, D. R., McGoven, P. J., Schmid, L., Baker, W. L., & Gray, C. (1994). Assessing Intervention Effects in the Minnesota Heart Health Program. American Journal of Epi-demiology, 139, 91–103.
Pak, R. (2001). A Further Examination of the Influence of Spatial Abilities on Computer Task Performance in Younger and Older Adults. In Pro-ceedings of the Human Factors and Ergonomics Society 48th Annual Meeting (pp. 1551 – 1555). Santa Monica, CA: The Human Factors and Er-gonomic Society.
Penninx, B., van Tilburg, T., Kriegsman, D., Boeke, A., Deeg, D., & van Eijk, J. (1999). Social network, social support, and loneliness in older persons with different chronic diseases. Journal of Aging and Health, 11(2), 151–168. doi:10.1177/089826439901100202
Riva, G. (2003). Ambient intelligence in health care. Cyberpsychology & Behavior, 6(3), 295–300. doi:10.1089/109493103322011597
Röcker, C., & Feith, A. Revisiting Privacy in Smart Spaces: Social and Architectural Aspects of Privacy in Technology-Enhanced Environments. Proceed-ings of the International Symposium on Computing, Communication and Control (2009) 201-205.
Röcker, C., Wilkowska, W., Ziefle, M., Kasugai, K., Klack, L., Möllering, C., & Beul, S. (2010). Towards Adaptive Interfaces for Supporting Elderly Users in Technology-Enhanced Home Environments. In Proceedings of the 18th Biennial Conference of the International Communications Society: Culture, Communication and the Cutting Edge of Technology. Tokyo, Japan. CD-ROM.
Roter, D. L., & Hall, J. A. (1989). Studies of Doctor-Patient Interaction. Annual Review of Public Health, 10, 163–180. doi:10.1146/annurev.pu.10.050189.001115
Singh, V. K., Pirsiavash, H., Rishabh, I., & Jain, R. (2008). Towards environment-to-environment (e2e) multimedia communication systems. In Same ’08: Proceeding of the 1st ACM international workshop on semantic ambient media experiences (pp. 31–40). New York: ACM.
Vallée, M., Ramparany, F., & Vercouter, L. (2005). A Multi-Agent System for Dynamic Service Com-position in Ambient Intelligence Environments. In: Advances in Pervasive Computing, Adjunct Proceedings of the Third International Confer-ence on Pervasive Computing (Pervasive’05), May 8-11, 2005, Munich, Germany.
Warren, S., & Craft, R. L. (1999). Designing Smart Health Care Technology into the Home of the Future. Engineering in Medicine and Biology, 2, 677–681.
Weiner, M., Callahan, C., Tierney, W., Overhage, M., Mamlin, B., Dexter, P., & McDonald, C. (2003). Using Information Technology To Im-prove the Health Care of Older Adults. Annals of Internal Medicine, 139, 430–436.
Wenger, G. C., Davies, R., Shahtahmasebi, S., & Scott, A. (1996). Social isolation and loneliness in old age: Review and model refinement. Age-ing and Society, 16(03), 333–358. doi:10.1017/S0144686X00003457
Wilkowska, W., & Ziefle, M. (2009). Which Fac-tors Form Older Adults’ Acceptance of Mobile Information and Communication Technologies? In Holzinger, A., & Miesenberger, K. (Eds.), Hu-man – Computer Interaction for eInclusion. LNCS 5889 (pp. 81–101). Berlin: Springer.

91
A Multi-Disciplinary Approach to Ambient Assisted Living
Wirtz, S., Jakobs, E.-M., & Beul, S. (2010) Pas-senger Information Systems in Media Networks – Patterns, Preferences, Prototypes. In Proceedings of the International Professional Communication Conference 2010 – Communication in a self-service society (IPCC 2010), Twente, Netherlands.
Wittenberg, R., Comas-Herrera, A., King, D., Malley, J., Pickard, L., & Darton, R. (2006). Future Demand for Long-Term Care, 2002 to 2041: Projections of Demand for Long-Term Care for Older People in England (PDF). PSSRU Discussion Paper 2330. London: London School of Economics.
Wolf, P., Schmidt, A., & Klein, M. (2008). SO-PRANO - An Extensible, Open AAL Platform for Elderly People Based on Semantical Contracts. Paper presented at the 3rd Workshop on Artificial Intelligence Techniques for Ambient Intelligence (AITAmI’08), 18th European Conference on Ar-tificial Intelligence (ECAI 08), Patras, Greece.
Woolham, J., & Frisby, B. (2002). Building a Local Infrastructure that Supports the Use of Assistive Technology in the Care of People with Dementia. Research Policy and Planning, 20(1), 11–24.
Wright, P., McCarthy, J., & Meekison, L. (2005). Making sense of experience. In Blythe, M., Overbeeke, K., Monk, A., & Wright, P. (Eds.), Funology: from usability to enjoyment (pp. 43–53). Norwell, MA: Kluwer Academic Publishers.
Ziefle, M. (2010). Modeling Mobile Devices for the Elderly. Proceedings of the 3rd International Conference on Applied Human Factors and Er-gonomics (AHFE’10): Miami, Florida.
Ziefle, M., & Bay, S. (2006). How to Over-come Disorientation in Mobile Phone Menu. A Comparison of Two Different Navigation Aids. Human-Computer Interaction, 21(4), 393–432. doi:10.1207/s15327051hci2104_2
Ziefle, M., Röcker, C., Kasugai, K., Klack, L., Jakobs, E.-M., Schmitz-Rode, T., et al. (2009). eHealth – Enhancing Mobility with Aging. In M. Tscheligi, B. de Ruyter, J. Soldatos, A. Meschtscherjakov, C. Buiza, W. Reitberger, N. Streitz, T. Mirlacher (Eds.), Roots for the Future of Ambient Intelligence, Adjunct Proceedings of the Third European Conference on Ambient Intel-ligence (AmI’09 (pp.25-28). Salzburg, Austria.
Zimmer, Z., & Chappell, N. (1999). Receptivity to New Technology among Older Adults. Disability and Rehabilitation, 21(5/6), 222–230.
ADDITIONAL READING
Aarts, E., Harwig, R., & Schuurmans, M. (2002). Ambient Intelligence. In Denning, P. J. (Ed.), The Invisible Future - The Seamless Integration of Technology in Everyday Life (pp. 235–250). New York: McGraw-Hill.
Aarts, E., & Marzano, S. (2003). The New Every-day - View of Ambient Intelligence. 010 Publishers.
Adam, S., Mukasa, K. S., Breiner, K., & Trapp, M. (2008). An apartment-based metaphor for intuitive interaction with ambient assisted living applications. Proceedings of the 22nd British HCI Group Annual Conference on HCI 2008: People and Computers XXII: Culture, Creativity [Liver-pool: United Kingdom.]. Interaction, 1, 67–75.
de Ruyter, B., & Aarts, E. (2004). Ambient intel-ligence: visualizing the future. Proceedings of the working conference on advanced visual interfaces (pp. 203 – 208). New York: ACM.
Ellis, D., & Allaire, J. (1999). Modelling Com-puter Interest in Older Adults: The Role of Age, Education, Computer Knowledge and Com-puter Anxiety. Human Factors, 41, 345–364. doi:10.1518/001872099779610996

92
A Multi-Disciplinary Approach to Ambient Assisted Living
Fuchsberger, V. (2008). Ambient assisted living: elderly people’s needs and how to face them. Pro-ceeding of the 1st ACM international workshop on Semantic ambient media experiences (pp.21-24). Vancouver, British Columbia, Canada.
Gaul, S., Ziefle, M., Arning, K., Wilkowska, W., Kasugai, K., Röcker, C., & Jakobs, E.-M. (2010). Technology Acceptance as an Integrative Com-ponent of Product Developments in the Medical Technology Sector. In: Proceedings of the Third Ambient Assisted Living Conference (AAL’10). Germany: VDE. CD-ROM.
Jähn, J., & Nagel, K. (2003). e-Health. Heidel-berg: Springer.
Kasugai, K., Ziefle, M., Röcker, C., & Russell, P. (2010). Creating Spatio-Temporal Contiguities Between Real and Virtual Rooms in an Assistive Living Environment. In J. Bonner, M. Smyth, S. O’ Neill, & O. Mival (Eds.). Proceedings of Create 10 innovative interactions (pp. 62-67). Loughborough: Elms Court.
Röcker, C. (2010). Living and Working in Auto-mated Environments - Evaluating the Concerns of End-Users in Technology-Enhanced Spaces. In V. Mahadevan, & Z. Jianhong (Eds.), Proceedings of the Second International IEEE Conference on Computer and Automation Engineering (pp.513-551), Singapore: IEEE.
Röcker, C., & Feith, A. (2009). Revisiting Pri-vacy in Smart Spaces: Social and Architectural Aspects of Privacy in Technology-Enhanced En-vironments. In Proceedings of the International Symposium on Computing, Communication and Control (ISCCC’09) (pp. 201 – 205), Singapore: IACSIT.
Röcker, C., Hinske, S., & Magerkurth, C. (2008). Information Security at Large Public Displays. In Gupta, M., & Sharman, R. (Eds.), Social and Human Elements of Information Security: Emerg-ing Trends and Countermeasures. Hershey, PA: IGI Publishing.
Salthouse, T. A. (1991). Theoretical Perspectives on Cognitive Aging. Hillsdale, NJ: LEA.
Tan, J. (2005). E-Health Care Information Sys-tems. San Francisco: Jossey-Bass.
Weiser, M. (1991). The Computer for the Twen-ty-First Century. Scientific American, 265(3), 94–104. doi:10.1038/scientificamerican0991-94
Ziefle, M. (2008). Age Perspectives on the Use-fulness on eHealth Applications. In Proceed-ings of the International Conference on Health Care Systems, Ergonomics, and Patient Safety (HEPS’08). CD-ROM.
Ziefle, M., & Röcker, C. (2010). Acceptance of Pervasive Healthcare Systems: A comparison of different implementation concepts. Full paper on the Workshop User-Centred-Design of Pervasive Health Applications (UCD-PH’10). In Proceed-ings of the 4th ICST Conference on Pervasive Computing Technologies for Healthcare 2010. CD-ROM.
KEY TERMS AND DEFINITIONS
Ambient Intelligence: The concept of Ambi-ent Intelligence (AmI) describes the integration of a variety of tiny microelectronic processors and sensors into almost all everyday objects, which enables an environment to recognize and respond to the needs of users in an almost invisible way. The term Ambient Intelligence was coined within the European research community as a reaction to the term ‘Ubiquitous Computing’ (see above), which was introduced and frequently used by American researchers. In contrast to the more technical notion of Ubiquitous Computing, Ambient Intel-ligence includes also aspects of Human-Computer Interaction and Artificial Intelligence. Hence, the emphasis of AmI developments is usually on greater user-friendliness, more efficient services support, user-empowerment and support for hu-man interactions. Ambient Intelligence applica-

93
A Multi-Disciplinary Approach to Ambient Assisted Living
tions are generally characterized by a high degree of embeddedness, using computers integrated into the physical environments in order to provide a variety of context-adapted user services.
Ambient Assisted Living: Ambient Assisted Living (AAL) is one domain of Ambient Intel-ligence and integrates information and commu-nication technology, and sensors into the living space to enable context awareness and to assist inhabitants in everyday situations.
Intracorproral Technology: Medical, techni-cal devices that are implanted in the human body or any structure anatomically called the corpus. Such devices can range from functional support structures like stents placed in blood vessels to guarantee a good blood flow or prothesis that functionally replace bone structures up to im-planted mechanical machines like for example an artificial heart.
Smart Materials: Smart Materials or Textiles can be defined as the materials and structures, which have sense or can sense the environmental conditions or stimuli and can react or respond on those stimuli. These stimuli as well as response, could be thermal, chemical, mechanical, electric, magnetic or from other source.
User Diversity: The term user diversity de-scribes in this context users’ characteristics like age, gender, physical condition as well as the moderating influence of users’ level of education and financial status.
Ease of Use: The ease of use describes the extent to which users believe a technical system to be free from effort and easy to handle.
Usability: The term describes users’ effective-ness, efficiency, and satisfaction with which users achieve specified goals in a technical system.
Aging Concept: Aging concept described here refers to the comprehensive view of aging process and its consequences to the person concerned. It includes 1) the perceived quality of life regarding autonomy, social life and healthcare, 2) misgivings about aging concerning dependency of others, social loneliness and health issues, as well as 3) the active vs. passive attitude towards aging itself.
Technology Acceptance: Technology accep-tance deals with the approval, favorable reception and ongoing usage of newly introduced devices and systems, and explores the relation of end-users using motives, cognitive and affective attitudes toward the respective technology and the techno-logical impact assessment.
Middleware: Part of a information system which integrates software components in an inter-process way, in our field especially between sen-sors and actuators on one hand and abstract tasks, context information, human machine interaction on the other.





























