Embed Size (px)
Citation preview
h, J. Nurs. Srud., Vol. 30. No. I, pp. 65-80. 1993 Prmted in Great Bntain.
0020.7489/93 l6.00+0.00 mtl, 1993 Pergamon Press Ltd
A classijication of nursing and midwifery shift systems
J. BARTON
E. R. SPELTEN
L. R. SMITH
P. A. TOTTERDELL
S. FOLKARD Shifiwork Reseurch Team.
MRCjESRC Social and Applied Psychology Unit, P.0.Bo.x 604.
The Univer.sit.~~, Sheffield SIO IFP. U.K.
Abstract-A classification of 122 shift systems worked by nurses and midwives in the larger general hospitals (400+ beds) in England and Wales was made. The systems were classified along two main dimensions: the degree of flexibility for shift rostering (either regular, irregular or flexible); and the speed of rotation between night and day work (either a permanent night shift or systems of fast or slow internal rotation). This resulted in nine possible categories of shift systems. The most common shift system was a flexible day shift with a permanent night shift. Other features of the systems are discussed, e.g. the start times and durations of shifts, and the relative influence of flexible rostering on these features. This classification is a prerequisite for a further research project aimed at identifying those features of shift systems which are likely to cause the least detrimental effects for the individual nurses concerned.
Introduction
There appears to be little published information concerning the range of shift systems for nurses and midwives in England and Wales. However, the pattern of shift rostering which
65

66 J. BARTON et ui.
exists does not appear to be uniform either within, or across, the different Health Regions. with shift systems tending to be unique to individual hospitals. The present study was set up to try to identify and classify the different shift systems in operation within the larger general hospitals in England and Wales. The study forms part of a larger research project concerning nurses and midwives, aimed at trying to identify those shift systems, or features of shift systems, which are likely to have the least detrimental effects on the health and well- being of the individual nurses concerned. Problems are known to exist for many individuals engaged in shiftwork (e.g. Ernst et al., 1984; Adams et al., 1986; Folkard, 1990). These can be classified into three broad categories: biological, which centre on the disturbance of physiological rhythms including the sleep/wake cycle (Tepas and Mahan, 1989; Akerstedr, 1990; Mahan et al. 1990); impairment of physical and psychological health (Rutenfranz rt al., 1985; Bohle and Tilley, 1989); and social and domestic disruption (Walker, 1985; Volger et al., 1988). The primary reason for the existence of these problems appears to be that as humans we have evolved as a diurnal species who habitually sleep at night and stay awake during the day. Pronounced and predictable changes in many of our bodily processes have been shown to vary consistently over the 24 hour day (Minors and Waterhouse, 1985) these being termed “circadian rhythms”. These rhythms are thought to be under the control of some internal timing system commonly referred to as the “body clock”, although the sleep/wake cycle also appears to be influenced by strong external time cues (Zeitgbers) such as the light/dark cycle, clock time and knowledge of others’ behaviour. In the absence of these external cues many rhythms have been shown to run with a period of approximately 25 hours. It is the presence of these external cues which appear to entrain many of these rhythms to a 24 hour period.
Consequently, problems associated with shiftwork are believed to result when a mismatch occurs between our internal body clocks and the external time cues. In particular, shift workers are required to stay awake when their rhythms are preparing them for sleep, and to sleep when preparing for wakefulness, i.e. the time of day which is least appropriate for sleep (Akerstedt and Gillberg, 1981). However, the extent to which the circadian rhythms of the shiftworker will adjust to this new routine of night time work and day time sleep may greatly influence the severity of the problems experienced. Different rhythms are known to adjust at different rates, and indeed it may often be the case that the circadian system may never fully adjust. One solution may be to work a schedule of permanent night shifts in order to give the body an opportunity to adapt, though this would only be effective if a nocturnal routine was to be maintained even on days off. Given the many other factors to take into consideration, e.g. social and domestic issues, this solution appears rather impractical.
The process of identifying those shift systems or features of shift systems which are likely to result in the fewest problems for the individuals concerned is particularly important given that changes in shift rostering appear to be taking place within the nursing profession (Pownall, 1990). One of the changes which has received a lot of attention within the literature is the movement away from shift systems which tend to be very rigid and regular, towards those which tend to be more flexible in nature (Keene, 1986; Shade, 1988). The practice of flexible rostering would give the individuals concerned more control over the organization of their hours of work. In addition, flexible rostering is believed to have positive benefits for the actual hospitals. These include: opportunities to increase the number of staff during peak hours of the day; attempts to improve communication among personnel during changes of shifts; and attempts to decrease absenteeism and overtime (Elliot, 1989). Flexible

NURSING AND MIDWIFERY SHIFT SYSTEMS 67
rostering has been shown to increase job satisfaction (Elliot, 1989) and has generally been positively appraised by individual nurses (Shade, 1988).
Other significant changes which appear to be taking place include: the movement away from a permanent day or night shift system towards a system of internal rotation (Sadler, 1990); and greater variation in the duration of the shifts worked. Many examples exist of the day shift being increased from around 8 hours to either 10 or 12 hours (Beach, 1986; Bowers Hutto and Davis, 1989; Thompson, 1989; Urgovics and Wright, 1990), while the length of the night shift appears to have been reduced (Pownall, 1990).
Our first aim therefore was to classify existing shift systems according to specific features of theoretical interest. The next stage will be to survey various groups of nurses using questionnaires and hand held computer techniques. The measures which will be taken will include levels of sleep disruption, physical health and general well-being, the use of coping strategies, and various measures of personality. The present paper reports the results of the first part of the project, the classification of shift systems.
Method
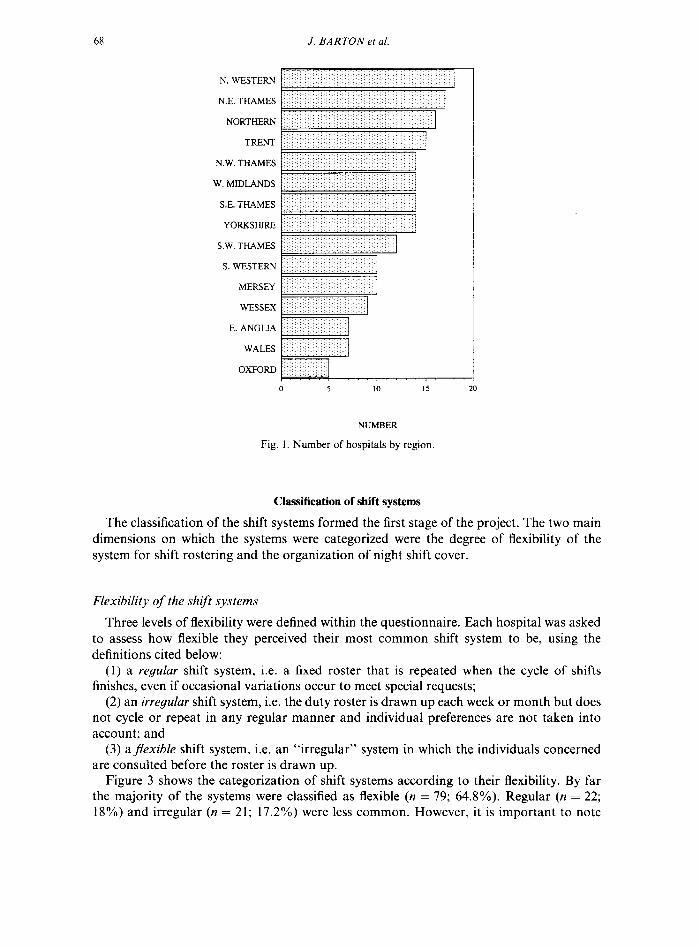
All General hospitals in England and Wales with more than 400 beds (as detailed in The Hospitals and Health Services Year Book, 1989), were surveyed by postal questionnaire. The hospitals were spread across the 14 Health Regions of England, with the whole of Wales being considered as an additional region. Figure 1 shows the number of hospitals surveyed within each geographical Health Region.
The questionnaire contained information which fell broadly into two categories. The first part asked for information on the number of registered beds, the number of full-time, part- time and bank nurses employed altogether, and on duty at any one time, and the number of hours that each nurse was contracted to work. The second part asked for information concerning the features of their most common shift system. Those which were thought to be of most theoretical interest included: the start and finish times of shifts, the durations of shifts, the sequencing of shifts, the number of successive shifts worked of any one kind, and in total before having a day off, the flexibility of the system for shift rostering. and the principal method of night shift rostering.
In total, 182 questionnaires were sent by post to the General Manager of each hospital. to be completed by a member of the nurse management.
Results
One-hundred and three questionnaires were returned giving a response rate of 57%. Even though the questionnaire asked for information concerning the “most common shift system” in operation within the hospital, 19 of the hospitals gave information concerning more than one shift system, namely a separate day and night shift system. In total 124 different shift systems were identified. Of these, two could not be used due to incomplete information. The results are therefore based on the analysis of 122 shift systems.
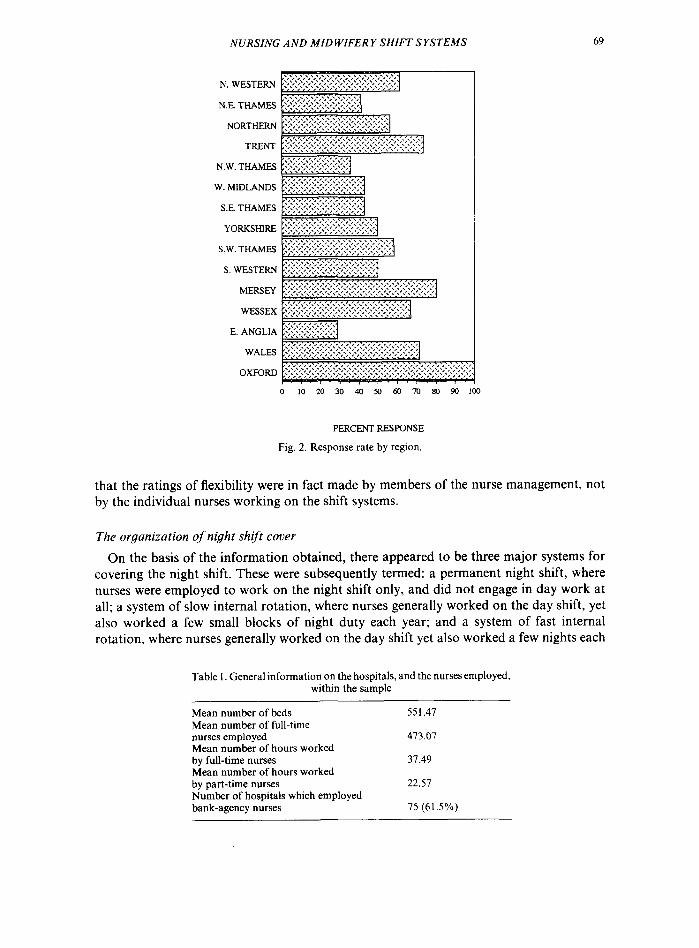
The hospitals which made up the sample were spread across the 15 Health Regions surveyed. Figure 2 shows the breakdown of the sample by Health Region. Table I gives some general information on the size, and the number of nurses employed in the hospitals included in the sample.
68 J. BARTON el ul.
N. WESTERN
N.E. THAMES
NORTHERN
TRENT
N.W. THAMES
W. MIDLANDS
SE. THAMES
YoRKsHIRE
S.W. THAMES
S. WESTERN
MERSEY
WESSEX
E. ANGLLA
WALES
OXFORD
0 5 10 15
NUMBER
Fig. 1. Number of hospitals by region.
Classification of shift systems
The classification of the shift systems formed the first stage of the project. The two main dimensions on which the systems were categorized were the degree of flexibility of the system for shift rostering and the organization of night shift cover.
Flexibility of the shifr systems
Three levels of flexibility were defined within the questionnaire. Each hospital was asked to assess how flexible they perceived their most common shift system to be, using the definitions cited below:
(1) a regular shift system, i.e. a fixed roster that is repeated when the cycle of shifts finishes, even if occasional variations occur to meet special requests;
(2) an irregular shift system, i.e. the duty roster is drawn up each week or month but does not cycle or repeat in any regular manner and individual preferences are not taken into account; and
(3) aflexible shift system, i.e. an “irregular” system in which the individuals concerned are consulted before the roster is drawn up.
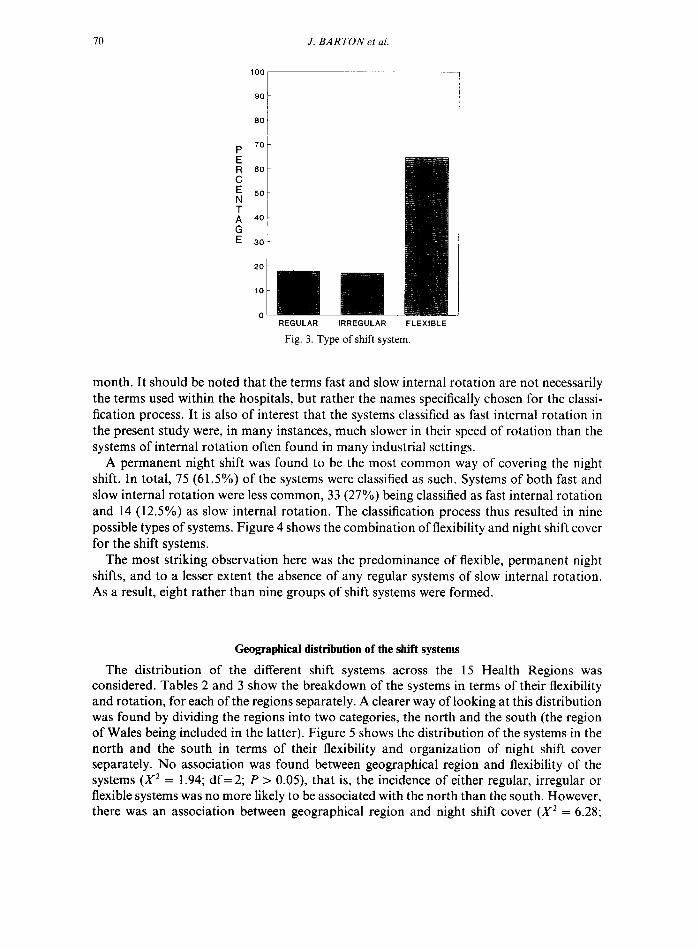
Figure 3 shows the categorization of shift systems according to their flexibility. By far the majority of the systems were classified as flexible (n = 79; 64.8%). Regular (n = 22; 18%) and irregular (n = 21; 17.2%) were less common. However, it is important to note
NURSING AND MIDWIFERY SHIFT SYSTEMS 69
N. WESTERN
NE. THAMES
NORTHERN
TRENT
N.W. THAMES
W. MIDLANDS
S.E. THAMES
YORKSHIRE
S.W. THAMES
S WESTERN
MERSEY
WFSSFX
E. ANGLIA
WALES
OXFORD
0 IO 20 30 40 50 60 70
PERCENTRESPONSE
Fig. 2. Response rate by region.
that the ratings of flexibility were in fact made by members of the nurse management, not by the individual nurses working on the shift systems.
The organization of night shift cover
On the basis of the information obtained, there appeared to be three major systems for covering the night shift. These were subsequently termed: a permanent night shift, where nurses were employed to work on the night shift only, and did not engage in day work at all; a system of slow internal rotation, where nurses generally worked on the day shift, yet also worked a few small blocks of night duty each year; and a system of fast internal rotation, where nurses generally worked on the day shift yet also worked a few nights each
Table I. General information on the hospitals, and the nurses employed, within the sample
Mean number of beds Mean number of full-time nurses employed Mean number of hours worked by full-time nurses Mean number of hours worked by part-time nurses Number of hospitals which employed bank-agency nurses
551.47
473.07
37.49
22.57
75 (61.5%)
70 J. BARTON et al.
100 y----
R 60 C ; 60
; 40
G E 30
20
REGULAR IRREGULAR FLEXIBLE
Fig. 3. Type of shift system.
month. It should be noted that the terms fast and slow internal rotation are not necessarily the terms used within the hospitals, but rather the names specifically chosen for the classi- fication process. It is also of interest that the systems classified as fast internal rotation in the present study were, in many instances, much slower in their speed of rotation than the systems of internal rotation often found in many industrial settings.
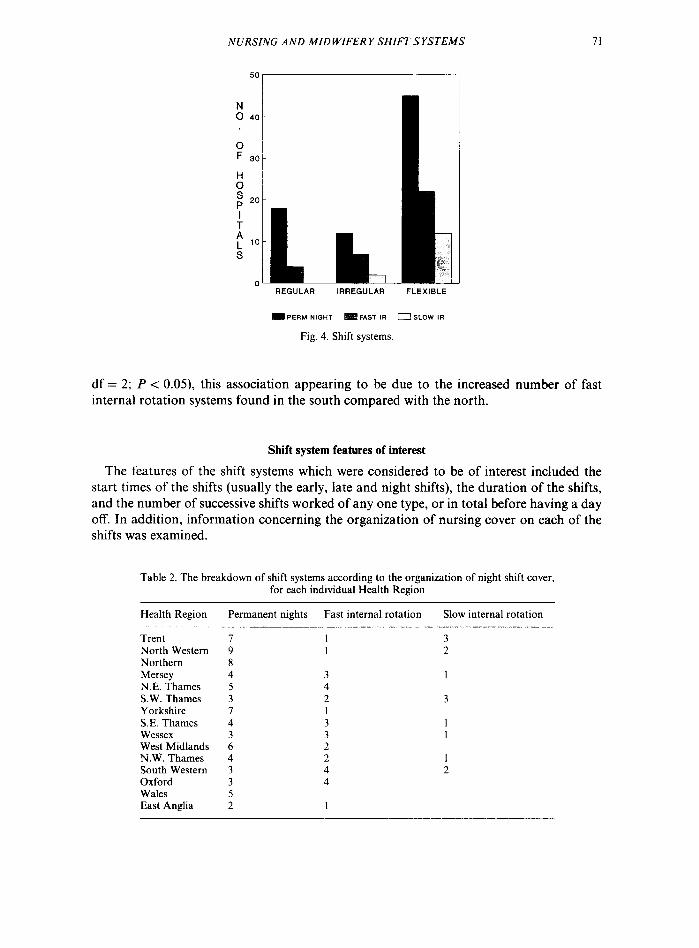
A permanent night shift was found to be the most common way of covering the night shift. In total, 75 (61.5%) of the systems were classified as such. Systems of both fast and slow internal rotation were less common, 33 (27%) being classified as fast internal rotation and 14 (12.5%) as slow internal rotation. The classification process thus resulted in nine possible types of systems. Figure 4 shows the combination of flexibility and night shift cover for the shift systems.
The most striking observation here was the predominance of flexible, permanent night shifts, and to a lesser extent the absence of any regular systems of slow internal rotation. As a result, eight rather than nine groups of shift systems were formed.
Geographical distribution of the shift systems
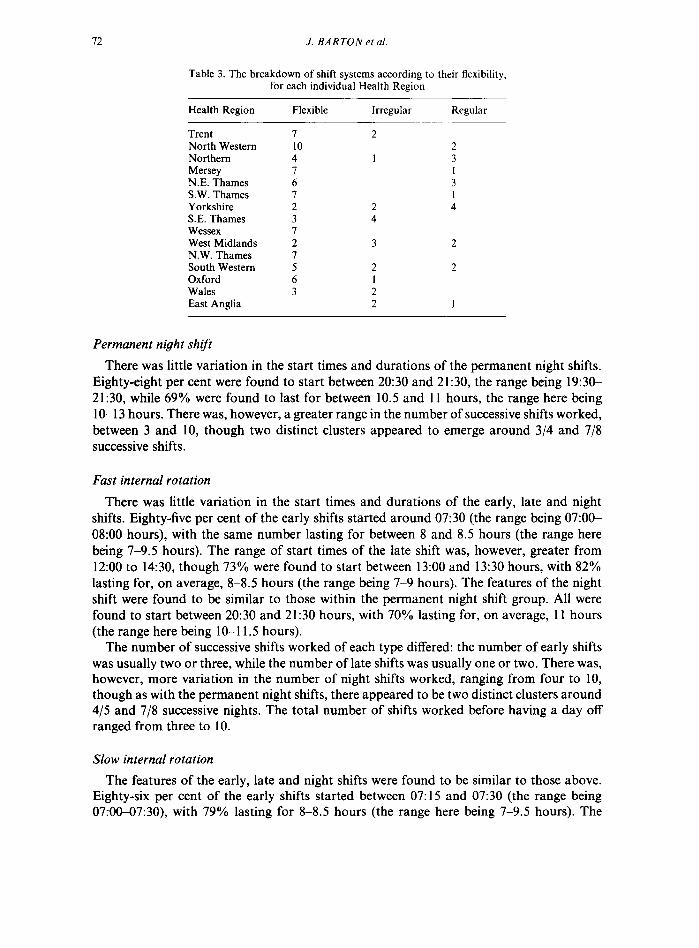
The distribution of the different shift systems across the 1.5 Health Regions was considered. Tables 2 and 3 show the breakdown of the systems in terms of their flexibility and rotation, for each of the regions separately. A clearer way of looking at this distribution was found by dividing the regions into two categories, the north and the south (the region of Wales being included in the latter). Figure 5 shows the distribution of the systems in the north and the south in terms of their flexibility and organization of night shift cover separately. No association was found between geographical region and flexibility of the systems (X2 = 1.94; df = 2; P > 0.05), that is, the incidence of either regular, irregular or flexible systems was no more likely to be associated with the north than the south. However, there was an association between geographical region and night shift cover (X2 = 6.28;
NURSING AND MIDWIFERY SHIFT SYSTEMS 71
0 F ao
:: ; 20
I
i L ‘O S
0 REGULAR IRREGULAR FLEXIBLE
J lPERM NIOHT FAST IR 0 SLOW IR
Fig. 4. Shift systems.
df = 2; P < 0.05), this association appearing to be due to the increased number of fast internal rotation systems found in the south compared with the north.
Shift system features of interest
The features of the shift systems which were considered to be of interest included the start times of the shifts (usually the early, late and night shifts), the duration of the shifts, and the number of successive shifts worked of any one type, or in total before having a day off. In addition, information concerning the organization of nursing cover on each of the shifts was examined.
Table 2. The breakdown of shift systems according to the organization of night shift cover, for each individual Health Region
Health Region Permanent nights Fast internal rotation Slow internal rotation
Trent North Western Northern Mersey N.E. Thames SW. Thames Yorkshire S.E. Thames Wessex West Midlands N.W. Thames South Western Oxford Wales East Anglia
7 9 8 4 5 3 I 4 3 6 4 3 3 5 2
I 3 I 2
3 I 4 2 3
3 I 3 I 2 2 1 4 2 4
I
J. BARTON et al
Table 3. The breakdown of shift systems according to their flexibility, for each individual Health Region
Health Region Flexible Irregular Regular
Trent I 2 North Western 10 2 Northern 4 1 3 Mersey 7 1 N.E. Thames 6 3 SW. Thames 7 I Yorkshire 2 2 4 S.E. Thames 3 4 Wessex 7 West Midlands 2 3 2 N.W. Thames 7 South Western 5 2 2 Oxford 6 1 Wales 3 2 East Anglia 2 I
Permanent night shift
There was little variation in the start times and durations of the permanent night shifts. Eighty-eight per cent were found to start between 20:30 and 21:30, the range being 19:3CL 21:30, while 69% were found to last for between 10.5 and 11 hours, the range here being 10-13 hours. There was, however, a greater range in the number of successive shifts worked, between 3 and 10, though two distinct clusters appeared to emerge around 3/4 and 7/8 successive shifts.
Fast internal rotation
There was little variation in the start times and durations of the early, late and night shifts. Eighty-five per cent of the early shifts started around 07:30 (the range being 07:OC 08:OO hours), with the same number lasting for between 8 and 8.5 hours (the range here being 7-9.5 hours). The range of start times of the late shift was, however, greater from 12:00 to 14:30, though 73% were found to start between 13:00 and 13:30 hours, with 82% lasting for, on average, 8-8.5 hours (the range being 7-9 hours). The features of the night shift were found to be similar to those within the permanent night shift group. All were found to start between 20:30 and 21:30 hours, with 70% lasting for, on average, 11 hours (the range here being 10-l 1.5 hours).
The number of successive shifts worked of each type differed: the number of early shifts was usually two or three, while the number of late shifts was usually one or two. There was, however, more variation in the number of night shifts worked, ranging from four to 10, though as with the permanent night shifts, there appeared to be two distinct clusters around 4/5 and 7/8 successive nights. The total number of shifts worked before having a day off ranged from three to 10.
Slow internal rotation
The features of the early, late and night shifts were found to be similar to those above. Eighty-six per cent of the early shifts started between 07: 15 and 07:30 (the range being 07:00-07:30), with 79% lasting for 8-8.5 hours (the range here being 7-9.5 hours). The
NURSING AND MIDWIFERY SHIFT SYSTEMS 73
E 60
E 50 N ;f 40
; 30
20
10
0 FLEXIBLE IRREGULAR REGULAR
m NORTH SOUTH
P 70
g 60
E 50 N T 40
t 30 E
20
10
0 PERM NIGHT FAST IR SLOW IR
m NORTH SOUTH
Fig. 5. Geographical distribution of systems.
range of start times of the late shift was, however, greater, from 12:30 to 14:00 hours, though 71% were found to start between 13:00 and 13:30 hours, lasting for on average 8- 8.5 hours (a range of 7-9.5 hours). The start times of the night shift showed little variation, all starting between 20:30 and 21:30, and lasting for between 10 and 11 hours.
14 J. BARTON et al.
The number of successive shifts worked was different for the early, late and night shifts, and resembled closely those within the fast internal rotation systems: 2/3 early shifts, l/2 late shifts, between three and eight night shifts, and between four and nine shifts of any kind before having a day off.
The influence of flexible rostering
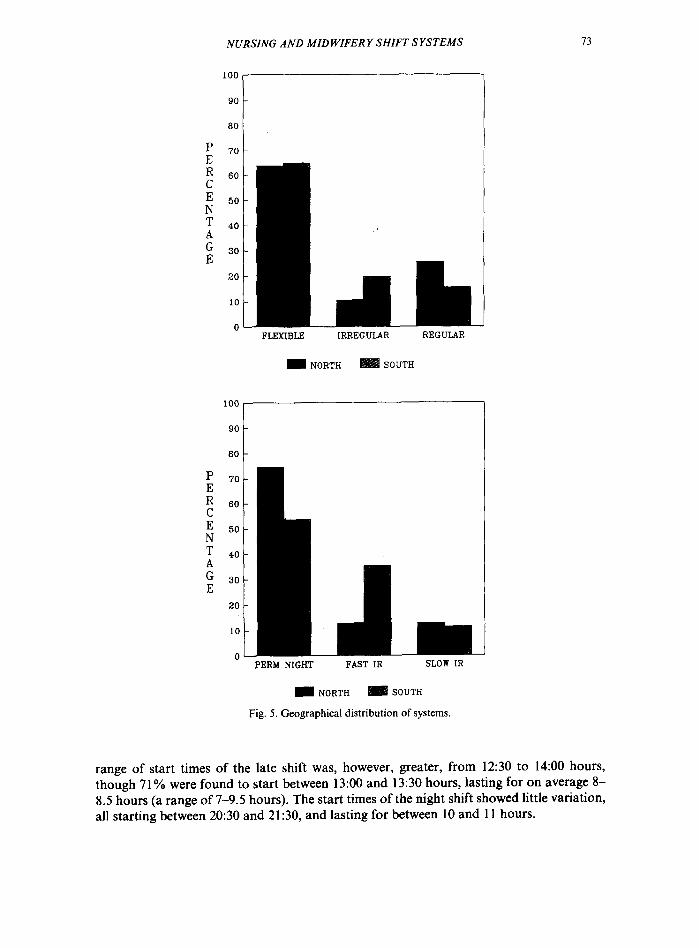
Given the limited variation in the features of the shift systems described above, the influence of flexible, irregular and regular rostering on these features was examined. Figure 6 shows the range of start times for the different shifts, for regular, irregular and flexible systems separately.
Regular
. . . . . . ~-a#= ----__-__-- m&l&
EARLY
700 21.5 730 745 8:OO I I I I 1
LATE
< 1200 1200 1230 13:oo 13:30 14:oo 1430 + 1 I I I I I 1
NIGHT 1930 2o:oa m30 21:oo 21:30 t
1 I I I I
Fig. 6. Range of start times of the early, late and night shifts for regular, irregular and flexible systems.
It is interesting to note that even though there was some variation in the start times of shifts, the actual range of start times was not found to be greater within flexible systems as opposed to either regular or irregular systems. In terms of shift duration, there did appear
NURSING AND MIDWIFERY SHIFT SYSTEMS 15
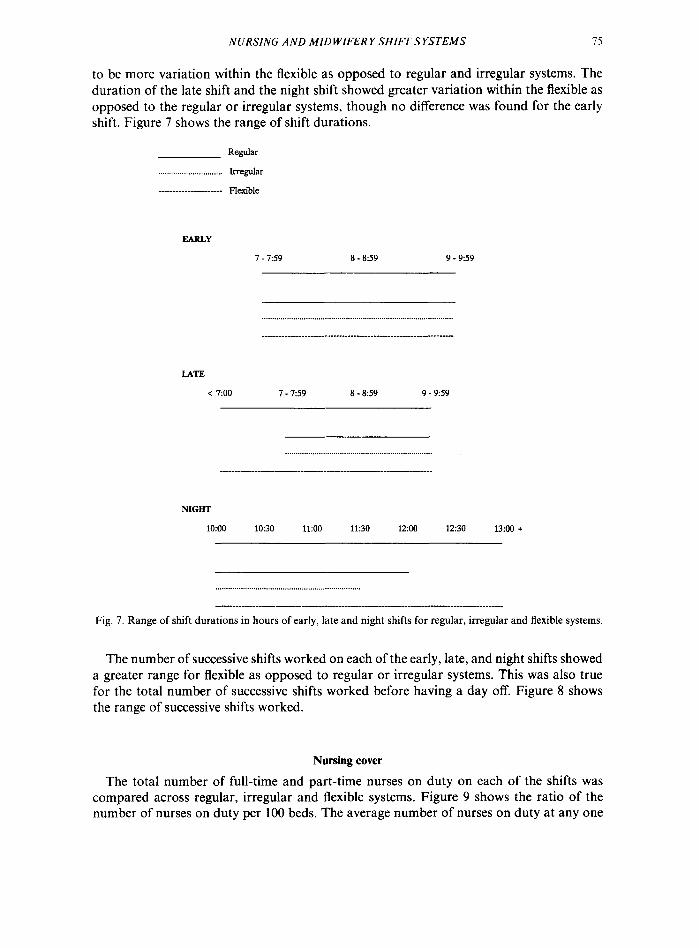
to be more variation within the flexible as opposed to regular and irregular systems. The duration of the late shift and the night shift showed greater variation within the flexible as opposed to the regular or irregular systems, though no difference was found for the early shift. Figure 7 shows the range of shift durations.
Regular
. . . Irregular
--------- _ ______ __ ___- Fl&-&
EARLY
l-7:59 8 - a:59 9 - 959
LATE
< -Loo l-7:59 a-8:59 9 - 959
NIGHT
IO:00 10:30 11:oo 11:30 1200 1230 13:oo +
Fig. 7. Range of shift durations in hours of early, late and night shifts for regular, irregular and flexible systems.
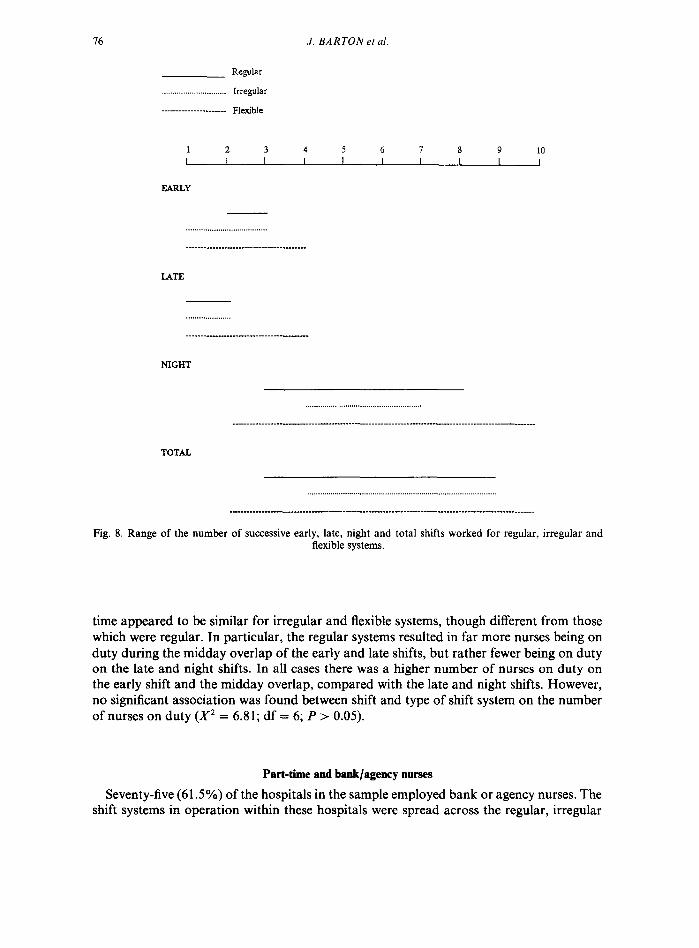
The number of successive shifts worked on each of the early, late, and night shifts showed a greater range for flexible as opposed to regular or irregular systems. This was also true for the total number of successive shifts worked before having a day off. Figure 8 shows the range of successive shifts worked.
Nursing cover
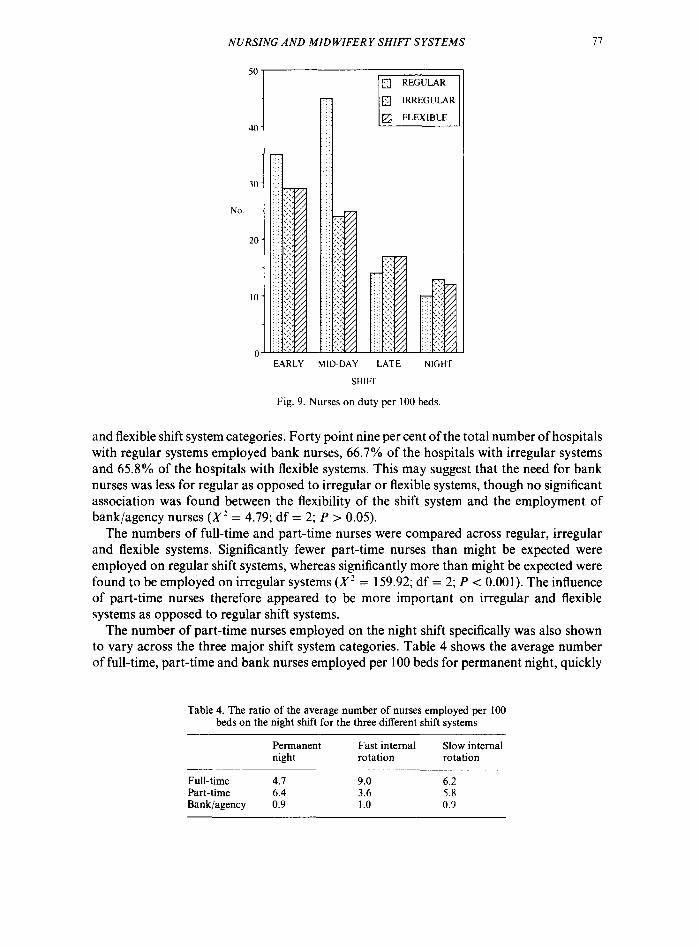
The total number of full-time and part-time nurses on duty on each of the shifts was compared across regular, irregular and flexible systems. Figure 9 shows the ratio of the number of nurses on duty per 100 beds. The average number of nurses on duty at any one
J. BARTON et al.
RegUhr
Irregular
-----------.--_.______ lq&tJle
1 2 3 4 5 6 7 8 9 10 I I I I I I I I I I
EARLY
-------- ___________-__- --------- ._______
LATE
NIGHT
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . _____ -__-__- _________ - ____________ __- _________.___________~_ - ____________ - _________ -_-______
TOTAL
Fig. 8. Range of the number of successive early, late, night and total shifts worked for regular, irregular and flexible systems.
time appeared to be similar for irregular and flexible systems, though different from those which were regular. In particular, the regular systems resulted in far more nurses being on duty during the midday overlap of the early and late shifts, but rather fewer being on duty on the late and night shifts. In all cases there was a higher number of nurses on duty on the early shift and the midday overlap, compared with the late and night shifts. However, no significant association was found between shift and type of shift system on the number of nurses on duty (X2 = 6.81; df = 6; P > 0.05).
Part-time and bank/agency nurses
Seventy-five (61.5%) of the hospitals in the sample employed bank or agency nurses. The shift systems in operation within these hospitals were spread across the regular, irregular
NURSING AND MIDWIFERY SHIFT SYSTEMS
EARLY MID-DAY LATE NIGHT
SHIFT
Fig. 9. Nurses on duty per 100 beds.
and flexible shift system categories. Forty point nine per cent of the total number of hospitals with regular systems employed bank nurses, 66.7% of the hospitals with irregular systems and 65.8% of the hospitals with flexible systems. This may suggest that the need for bank nurses was less for regular as opposed to irregular or flexible systems, though no significant association was found between the flexibility of the shift system and the employment of bank/agency nurses (X2 = 4.79; df = 2; P > 0.05).
The numbers of full-time and part-time nurses were compared across regular, irregular and flexible systems. Significantly fewer part-time nurses than might be expected were employed on regular shift systems, whereas significantly more than might be expected were found to be employed on irregular systems (X2 = 159.92; df = 2; P < 0.001). The influence of part-time nurses therefore appeared to be more important on irregular and flexible systems as opposed to regular shift systems.
The number of part-time nurses employed on the night shift specifically was also shown to vary across the three major shift system categories. Table 4 shows the average number of full-time, part-time and bank nurses employed per 100 beds for permanent night, quickly
Table 4. The ratio of the average number of nurses employed per 100 beds on the night shift for the three different shift systems
Permanent Fast internal night rotation
Slow internal rotation
Full-time 4.7 9.0 6.2 Part-time 6.4 3.6 5.8 Bank/agency 0.9 1.0 0.9

78 J. BARTON <‘I cd.
rotating, and slowly rotating shift systems. The number of part-time nurses employed appears to be greatest on the permanent night shifts, compared with the other two shift systems. Significantly more part-time nurses were found to be employed on the permanent night shift than might be expected, compared with significantly fewer on either system of internal rotation (X’ = 323.21; df = 4; P < 0.001).
Hours of work
The average number of hours worked per 7 days, by full-time, part-time and bank nurses, on regular, irregular and flexible systems is presented in Table 5. The data would suggest that the role of flexibility did not appear to influence the number of hours worked by the individual nurses.
Table 5. The average number of hours worked per 7 days for full-time, part-time and bank nurses
Full-time Part-time Bank/agency
Regular Irregular Flexible
37.50 37.50 37.49 21.23 23.94 22.53 13.69 12.10 14.43
Discussion
The aim of the study was to form a classification of the most common nursing and midwifery shift systems in operation in England and Wales. This has been produced with a view to surveying selected groups of nurses working on these different shift systems, in order to try to identify those shift systems, or individual features of shift systems, which are likely to result in the fewest problems for the individuals concerned. The two main criteria on which the systems were classified were the degree of flexibility and the speed of rotation between day and night work. Three levels were identified on each variable, giving a possible total of nine individual categories. Only eight of the possible nine were found within the sample.
In line with the shift rostering developments cited within the nursing literature (e.g. Elliot, 1989; Shade, 1990), the majority of the systems identified were in fact flexible in nature. This situation is, however, very different from the shift systems often found within industrial settings, e.g. the fixed, regular systems found within the nuclear power industry (Smith and Folkard, 1991) or in the gas industry (Totterdell, 1990). In addition, the rotating nursing shift systems (either fast or slow), again bear little resemblance to the rotating shift systems found in industry or other public services. For example, the shift systems in operation within the British Police Force, which tend to rotate more frequently between day and night work (e.g. Totterdell and Smith, 1991).
It is also interesting to note that the majority of systems identified were in fact permanent night shift systems. This is perhaps surprising given the apparent movement within the nursing profession away from a permanent day or night shift system towards a system of internal rotation (Sadler, 1990). This finding could be due to the fact that our survey specifically asked for information relating to the most common shift system in operation

NURSING AND MID WIFER Y SHIFT SYSTEMS 79
within each hospital, whereas many of the changes in shift rostering which are taking place are still under trial, usually on specific wards or selected groups of nurses. This would probably also account for the absence of 10 and 12 hour day shifts within our sample.
The levels of the two variables, flexibility and rotation, are thought to be sufficiently powerful to have a differential influence on a range of outcome effects experienced by the individuals concerned. Flexibility implies a certain degree over control of ones’ hours of work (e.g. Shade, 1988). Control appears to be an important moderator in many of the more common problems experienced by a large proportion of shiftworkers (Barton and Smith, 1991). For example, the higher subjective ratings of well-being of nurses who had chosen to work on a particular shift schedule, as opposed to those who were employed on a rotating shift system with little control over their hours of work (Verhaegen et al., 1987). The frequency of rotation between day and night work has also been shown to produce differential effects on many outcome measures, e.g. higher levels of self-reported stress reported by nurses working on a system of slow internal rotation, compared with nurses working on either a permanent day or a permanent night shift system (Barton and Folkard, 1991).
It is therefore on the basis of this classification that the next stage of the project will be based. Within this classification, certain features of the systems which have been shown to vary, such as the number of successive night shifts worked, and the total number of shifts worked before having a day off, will be taken into account when comparing the responses of individuals and groups of nurses.
Acknowledgemenrs-We wish to thank the Department of Health for financial support, Miss E. J. C. Scott of the Research Management Division for her advice and encouragement, and the Hospital General Managers and their colleagues for completing our questionnaire.
References
Adams, J., Folkard, S. and Young, M. (1986). Coping strategies used by nurses on night duty. Ergonomics 29(2), 185.-196.
Akerstedt, T. (1990). Psychological and psychophysiological effects of shiftwork. Scund. J. Work Environ. Health 16,67-73.
Akerstedt, T. and Gillberg, M. (1981). The circadian variation of experimentally displaced sleep. Sleep 4, 159 169.
Barton, J. and Folkard, S. (1991). The response of day and night nurses to their work schedules. J. Occupational Psychol. 64,207-2 18.
Barton, J. and Smith, L. R. (1991). Choice and Control: Implicationsfor Shiftworkers. SAPU Memo No. 1238., The University, Sheffield.
Beach, L. L. (1986). Design and Implementation of a ten-hour work schedule for an ED nursing staff. J. Emergenq Nurs. 12(l), 3634.
Bohle, P. and Tilley, A. J. (1989). The impact of night work on psychological well-being. Ergonomiu 32(9). 108Y- 1099.
Bowers Hutto, C. and Davis, L. L. (1989). 12-Hour shifts: panacea or problem? Nurs. Management 20(8), 56A 56H.
Elliot. T. L. (1989). Cost analysis of alternative scheduling. Nurs. Management 20(4), 42-47. Ernst, G., Knauth, P., Nachreiner, F. and Rutenfranz, J. (1984). The effects of different sleep patterns on the
utility of time under different shift systems. In Psychological Aspecfs of Shifwork (Wedderburn, A. A. and Smith. P., Eds). Heriot-Watt University, Edinburgh.
Folkard, S. (1990). Circadian performance rhythms: some practical and theoretical implications. Phil. Trans. R. Sac. Lend. B 321,543-553.
Keene, L. (1986). Working day and night. New Zealand Nurs. J. November. Mahan, R. P., Carvalhais, A. B. and Queen, S. E. (1990). Sleep reduction in night shiftworkers: is it sleep
deprivation or a sleep disturbance disorder? Perceptuul and Motor Skills 70, 723 -730.

80 J. BARTON et ul.
Minors, D. S. and Waterhouse, J. M. (1985). Introduction to circadian rhythms. In Hours of Work: Temporal Factors in Work Scheduling (Folkard, S. and Monk, T. H., Eds). Wiley, Chichester.
Pownall, M. (1990). Shifting ground. Nurs. Times 86,44. Rutenfranz, J., Haider, M. and Koller, M. (1985). Occupational health measures for night workers and shift
workers. In Hours of Work: Temporal Factors in Work Scheduling (Folkard, S. and Monk, T. H., Eds). Wiley, Chichester.
Sadler, C. (1990). Beat the clock. Nurs. Times 86,44. Shade, P. (1988). Flexible friend. Nurs. Times 84(44), 32-34. Smith, L. R. and Folkard, S. (1991). The Impact of Shifrwork on Workers in a High Hazard Industry. SAPU
Memo No. 1195., The University, Sheffield. Tepas, D. I. and Mahan, R. P. (1989). The many meanings of sleep. Work and Stress 3(l), 93-102. Thompson, J. (1989). Rigour round the clock. Nurs. Times 85, 18. Totterdell, P. (1990). NALGO Gas Storage Shlftworkers: Survey Results. SAPU Memo No. 1194, The University,
Sheffield. Totterdell, P. and Smith, L. R. (1991). An Evaluation of the Ottawa Shift System. SAPU Memo No. 1225, The
University, Sheffield. Urgovics, A. and Wright, J. (1990). 12-Hour shifts: does fatigue undermine ICU nursing judgements? Nurs.
Management 21, 1. Verhaegen, P., Cober, R., DeSmedt, M., Dirkx, J., Kerstens, J., Ryvers, D. and Van Daele, P. (1987). The
adaptation of night nurses to different work schedules. Ergonomics 38(9), 1301-1309. Volger, A., Ernst, G., Nachreiner, F. and Hanecke, K. (1988). Common free time of family members under
different shift systems. Appl. Ergonomics 19(3), 213-218. Walker, J. (1985). Social problems of shiftwork. In Hours of Work: Temporal Factors in Work Scheduling
(Folkard, S. and Monk, T. H., Eds). Wiley, Chichester.
(Received 5 July 1991; acceptedforpublication 27 November 1991)





























