Embed Size (px)
Citation preview

October 27, 2021
Shalom LaForge, D.C.
Dear Chairman Erickson and committee members,
I am writing this testimony to add my voice to the many calling out for justice and appeal for relief from the present tyranny from mandates.
I am a life-long Kansan, wife, mother of three, educated and licensed to support natural health through Chiropractic care. I have taken the last 10 years away from active practice to focus on raising my own children, but health remains a passion and focus. God, my family, and health are my top priorities.
When in practice, I cared for many families who had experienced vaccine injuries and their lives were changed forever. These families had virtually no recourse to the damage a family member will deal with their entire life. Since the Covid biological injections were given EAU authorization and administered, we have seen many alarming reports of severe and deadly reactions to these procedures, and it is still in the experimental stages. Many more effects will undoubtedly be discovered. Those damaged by these shots have absolutely no recourse for injuries and death. This is criminal and inhumane.
The science shows us that the Covid biological injections do not prevent infection or transmission, so are therefore not giving any protection to our community. No one should be forced or coerced to have this procedure done, especially to remain in the workplace and schools.
I stand against government mandates of COVID-19 shots, tests, and other related restrictions. We rely on our elected officials and others in positions of power to protect our rights and freedoms. You must join us in this fight against mandates that force individuals against their will to get a medical procedure, especially experimental and potentially lethal procedures. Stand with us against these imposed mandates and restrictions on our freedoms and rights and do all in your power to stop this present assault and future attacks.
Your’s in health,
Shalom M. K. LaForge, D.C.
10/27/2021
Chairman Erickson and committee members,
TLDR: I am AGAINST the government mandate of the COVID-19 vaccine.
My name is Parker LaGree. I live in Wichita and work at Spirit Aerosystems as an engineer, where I have
been employed for the past 5 years. I am being threatened with the loss of my job if I refuse the shot.
This mandate is an unacceptable overreach by our government, who neither understands nor cares
about my specific medical needs. Furthermore, using employers as a means of enforcement has created
a stressful, hostile, and unproductive work environment. Even if I apply for a religious or medical
accommodation, I will likely be told to wear masks and get tested weekly at my own expense, which is
completely discriminatory in nature. This is happening all across my industry, so even finding another
job will likely involve a career change, which means I’d be starting at the bottom again and set me back
10+ years that I have been working in the industry.
Medical care should be a personal choice. Regardless of our personal opinions about COVID-19 shot
itself, the premise that the government can mandate an elective medical procedure (one that is not
even FDA approved) is unacceptable and sets a dangerous precedence for further such actions. I don’t
enjoy protests or writing letters, but I am seeing our civil liberties eroded. I hope you can see how this
mandate undermines our identity as a country and everything we stand for. Thanks for listening.
Sincerely,
Parker LaGree
Written Testimony to STOP Mandatory government OverreachCOVID-19 Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
BAN MANDATORY COVID-19 VACCINATIONS!
This should be a choice!!! Especially when ones life is on the line! Nobody takes the blame when adverse reactions happen or worsedeath! This should be left up to the individual not the government! Please give us back our freedoms!!!
KristiLangley
10/27/2021
Written Testimony to Stop Government Overreach Covid-19 Mandates
Dear Chairman Erickson and Committee Members,
I am giving written testimony in opposition to Covid-19 Vaccine Mandates. I am against any type of
government mandate that violates body autonomy. I work at one of the large hospitals in Wichita. This
hospital has yet to mandate any type of Covid-19 vaccine. But everyday I have to worry if today or
tomorrow or anytime in the near future they will make it mandatory. We are already VERY short staffed
in my department but I am willing to leave my position or get fired if the vaccine becomes mandatory. I
absolutely do not want too but I will and there are others that will follow. I have talked to people that
have had it mandated by their employer and they will lose their job if they don’t take vaccine. This is not
about freedom but is about control and it needs to be put in check. There needs to be something done
to keep our freedom to choose about our own healthcare decisions and not having our employer
mandate it for us in order to keep a job. I am also concerned these Covid-19 vaccines will be mandated
to attend public school. There should be laws put in place to protect not only employees but also
students from this obvious overreach of power. Please step up to help protect our freedoms.
Courtney Lee (ASCP)CM
Chairwoman Erickson & Committee:
It is with great remorse that I write this letter to you today. Remorse for my district. Remorse for my state. Remorse for my country. Like many of my constituents I grieve what we are witnessing in Kansas and across the USA.
We are witnessing tyranny at every level. The freedom to not get to see our loved ones in nursing homes and hospitals, the freedom to send our children to school without facemasks, and the freedom to have bodily autonomy to make decisions for our health as we see fit.
We are under attack. I would like to say that it’s just from the federal government. But businesses in Kansas and elsewhere seem to have drank the communist Kool-Aid as well. When has it ever been okay for a company to discriminate against an employee or a school against a child for expressing their constitutional right of life, liberty and the pursuit of happiness? It’s contrary to the divine nature of “one nation under God and it’s contrary to the lifeblood of what has kept this country a Republic since the signers of the Declaration declared us so.
The courage of the 56... The signers of the declaration put everything on the line to defend and protect their innate freedoms. They were willing to lose their lives, their fortunes and their families. And most of them lost all three. The only thing they have kept is the honor in which we bestow them now.
But are we giving them honor at this time in history? The courage of the 56 is admirable. We talk about it as though we understand the sacrifice, they endured to have historical accolades written about them now.
But do we have the courage to be the 57th signer? Are we as legislators and as “we the people” willing to stand and risk it all for the sake of keeping our republic and all that entails?
In order to have a more perfect union, our elections must be secure and our freedoms must stand as impenetrable pillars of truth. Nothing about our elections or the legislative process feels honest at this point. Are we living in a banana republic? Can we as the legislature be trusted to have the courage of those that have gone before us to lay it all on the line?
I would say our performance thus far is dismal. We have let our constituents down. Instead of a loyalty to our oath some have succumbed to the pressure of the elite. But we aren’t a country of elite. We are a country of patriots. Hark working Americans that just want to live their lives, raise their families and work hard to provide for them.
Today you have heard from Kansans from every quadrant of the state and in every industry. You’ve heard from moms and dads, pastors, students & firefighters, grandmas and grandpas, young and old.
And now it’s time to do your jobs that you were elected to do. We must not let the fear of elections; leadership positions or committee assignments dictate our moral obligations to honor the oath that we have taken.
I think this committee is a stall tactic by our leadership to act forthrightly to make the hard decisions.
Respectfully, my constituents didn’t hire you to make decisions for them. They hired me. We need to gather the information presented the last two days, bring the entire delegation of the legislature back to Topeka and carry out the will of the people to protect and defend them. Should this not be the immediate findings of this committee, I submit that all of us rightfully lose our coveted positions as servants of the public and allow others with more grit and fortitude the honor of replacing us to save the public from the government they elected.
Colleagues, these are strong words because the war we fight is real. The war to keep our republic is real.
May God be with you and have mercy on us all. And may His conviction fall on all of us like heavy coals on our heads lest we forgo the holy and hard decisions set before us at this time in history.
Respectfully,
Representative Tatum Lee from the 117th District
Dear Committee,
Thank you for taking the time to hear from us. We are asking for your help in stopping this Covid shot
mandate. We are free Americans and this mandate is very UNAMERICAN! And now they are coming for
our babies! I am scared. So many of us are in disbelief that this Mandate is really happening! Please
please,please stand up for us and be a shining example in Kansas and the rest of the country in
STOPPING this Government Overreach!
MaryAnn Leo
Deana Lesher, OTR/L Owner 7235 W. 162nd Terr * Overland Park, KS 66085
ph. 913-257-5808 * fax. 844-270-5788PediatricConnectionsOT.com
To: Chairman Erickson and committee membersPosition: AGAINST MANDATES
I’m Deana Lesher. I own Pediatric Connections which is a private outpatient clinic for Occupational and Speech Therapy in the KC area. My team treats many students in the surrounding school districts. We are the area ex-perts in nervous system development and provide services for children with autism, ADHD and a multitude of other diagnoses.
We all agree that keeping kids safe is our number 1 priority. This also includes keeping their mental health safe.
I’m here to present a different perspective of safety for you to consider. My team is well versed in Dr Stephen Porges’ Poly Vagal Theory, TBRI (Trust Based Relational Interventions) and other protocols that teach social connection and felt safety.
Porges’ theory identifies the vagus nerve as the safety gauge for our nervous system and the key driver of our emotional regulation, social connection and fear responses.
When we are in our restful/safe state we are better able to self-regulate, sustain attention, and calm down after a stressful experience. This capacity to regulate our emotional response and behavior helps nurture and support healthy relationships and allows us to respond appropriately to interpersonal stressors and demands.
This theory explains how a part of the vagal nerve literally connects to your facial muscles associated with ex-pression, vocal communication and social behavior through its activation of the muscles of the face and neck including those that influence facial expression, like smiling, and vocal resonance.
All of that to say how important it is to see the WHOLE picture of facial expression. We cannot discount the long-term effects of kid’s missing this part of connection. We get signals of safety by reading the whole face.
We have an amazing nervous system that will protect us and our survival states kick in when needed. However, we were never meant to live in states of survival for long periods of time. Fear lodges in the amygdala and into the Limbic system which is the most primal areas of the brain. This is where our fight flight and freeze responses come from. Being in a hyper vigilant state increases stress hormones which has many damaging effects on the body. We see kids that have difficulty with sleep, appetite, transitions, social connections, anxiety, shut down and depression. Masked faces give the signal of fear and that something is abnormal to the amygdala. This per-petuates the fear response at a subconscious level.
Mental health issues, including depression, anxiety and suicide are on the rise in the last 18 months. But, we know we can’t bubble wrap our life. There is always risk. Everything we do in our activities of daily living has a calculated risk and benefit. Allowing mask choice is not a reckless risk. Long term effects of being in a state of survival will take its toll on our ability to function as healthy, adaptable children and adults. Our nervous systems beg for connection and safety. Reading signals from the whole face facilitates a sense of connection.
We are not created to have a spirit of fearfulness, but we were created to have a spirit of power, love and disci-pline.
Thank you for your consideration.
Deana LesherOccupational TherapistOwner, Pediatric Connections
Dear Chairman Erickson and committee members,
Please accept this written testimony AGAINST government mandates of COVID-19 vaccines. It is time to
stand up for the people of Kansas and stop this unconstitutional overreach. Please stop COVID-19
vaccine mandates.
Thank you,
Kristen Lettow

October 27, 2021
Chairman Erickson and Committee Members:
I had Covid last year. I have natural immunity. I am absolutely against the Covid-19 vaccine mandate!
The government has no authority to force me to inject myself with a substance that carries a risk that
may leave me disabled and unable to provide for my family or force me to leave my job. This is a free
country, and as such I have the freedom to choose, and the government’s job is to protect my rights. It is
not right that the federal government step in and impose a medical procedure on anyone if it is against
their conscience or religion. All medical decisions must be left solely with the individual with the help
and guidance from a respected medical professional of their choosing.
You have been elected to represent me, my family, and my co-workers, that simply want to provide for
our families without threat of government overreaching further that they already have for decades. I
respectfully urge you to do whatever you can do to hold true to your oath to defend the Constitution,
especially the inalienable, individual rights of Kansas citizens. If you don’t stand up and find the
backbone to represent us and we want and need, I will work to replace you with others who will.
Thank you for your time.
Linda Liester
Written Testimony only
WRITTEN TESTIMONY TO STOP GOVERNMENT OVERREACH OFCOVID-19 MANDATORY VACCINES
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Chairman Erickson and Committee Members:
This letter is to inform you of our concern regarding government overreach regarding mandatory vaccines in Kansas.
You have been elected by the citizens of Kansas to “protect our Constitutional rights.” Therefore, we are pleading with you, aswell as praying…that you have the courage to stand up for FREEDOM and to vote NO for mandatory Covid-19 vaccines.
This ridiculous mandate has caused not only emotional strife…but economic destruction to many families and businessesthroughout our great state. Sadly…”true” science is ignored when it comes to politics.
Several of our friends and family members have lost positions due to “workplace bullying “ and blackmail regarding thisabhorrent mandate.
If our freedoms to be in charge of our own health ends…then it is the “beginning of the end” for our other constitutionalfreedoms as well. After all…will booster shot mandates be next?? Or…during the next “plandemic”, will other “newexperimental” vaccines also be mandated??
We ask you to consider taking a patriotic stance and have courage to KEEP KANSAS STRONG, FREE, AND EMPLOYED!!
Sincerely,
Gary & Shauna Long
Sent from my iPhone
To: Chairman Erickson & committee members I am against a vaccine mandate of COVID-19 vaccines. Per our U.S. Constitution no one should be forced to put something into their body against their will. The mandatory vaccination policy is unethical and unlawful and equates to a form of assault. Any medical procedure performed on a patient without their informed consent amounts to assault. Requiring a person to take the vaccine or lose their job flies in the face of every right guaranteed to us in the Constitution. If we lose our rights, we are destroying our Constitutional freedoms and becoming like a communist country. In addition, these mandates violate the Nuremberg Code, which was set up after WWII which guarantees no medical experimentation without full informed consent. If you do not know what the Nuremberg Code is, you need to look that up because you are about to violate this code if you mandate this vaccine. Withholding the risks vs benefits and ingredients violates this internationally agreed upon code of ethics. I would not want the repercussions of violating this international code if I was the one making these decisions. Informed consent involves the risk vs benefit disclosure which includes the data currently listed in the VAERS database and knowledge of ingredients in the vaccines. I have searched high and low for an ingredient list & have even asked my medical friends for a vaccine insert so that I can research what I am putting into my body. I have been unable to find that ingredient list. I also have not been able to find an ingredient list on Pfizer & Moderna's site with the information about the vaccines. Knowing that Pfizer, Moderna and Johnson & Johnson have been granted immunity for any damages that these vaccines cause, is the Kansas State Legislature taking on the liability for damages caused since you are the ones mandating this vaccine, including neurological damages, paralysis, seizures and death to name a few? Sue Lucas
October 27, 2021
Jennifer Luedeke
Chairman Erickson and Committee Members,
This testimony is written AGAINST Government Mandates.
Fear and Lack of Trust. These are tied together. No trust in government. No trust in
corporations. No trust between neighbors. And then following the lack of trust is fear.
What will happen when a person chooses to not be controlled by ever-changing
contradicting mandates?
Will I be allowed into the grocery store while breathing air? Will Menard’s kick me out
of their store because I want my son to participate in a home project? Can I get my
glasses prescription updated while breathing air? Where is it possible to go out for a
date with my husband? Will I be allowed into the clinic to get a sonogram to see if I had
a miscarriage?...I put on the mask (handed to me with a ridiculous hotdog tongs!) this
particular day because they wouldn’t let me in otherwise, and I nearly had a full-blown
anxiety attack. I was not being political…I was there to find out if I lost my baby which is
traumatic enough!
Lack of trust. Even this public meeting today…is this really for our benefit or is this just a
way to collect information on those who are not submitting. A voluntary checklist of
people to go after next? What really is the point of this meeting and how will it benefit
us? Can anyone in government be trusted anymore?
We homeschool our children, so thankfully we were not so terribly uprooted in our
education. So while we haven’t used our tax dollars for public education, we have
always made use of our tax dollars in the library system. We used to visit the library
every week with sometimes near 100 books out at a time depending on what each kid
was studying in various subjects and their interests. Funny, how libraries were shut
down when kids were no longer able to attend school. They shut down access to
books, which is access to information that is not controlled by the media and evil powers
that be. [Please check into burning of books and communism.] Even now, one is made
to feel a criminal to browse with the “Masks and Social Distancing Strongly
Encouraged!” We barely check out any book anymore, because of the fight to be
normal!
Last year, publishing companies were shut down in various states. So I am always
trying to think way ahead in what curriculum I will need in the future, in case they decide
to shut them down again and they are unable to ship homeschool materials.
We left our church because the propaganda for masking, social distancing and
vaccinations was so heavy. How did the evil powers that be get the churches to do their
dirty work?! We left that church because we were the only ones that believed it was
wrong to cover up the beautiful faces that God intricately designed…especially the
smiles! We left because this church stopped all Bible studies and anything that was
originally designed to bring the body of believers together. We left because this church
wouldn’t even allow the parents, ME, to bless our own children during Confirmation,
which has been a tradition since the very beginning of this church. Why? It was too
dangerous! We left because we know that God made people to be with people and the
“social distancing” oxymoron has no place in churches or society…the outcome of
loneliness is despair which can lead to all other evils—abuse, alcohol & drugs, murder
and suicide. The evil has infiltrated the churches.
In addition to this, my husband is facing job loss or accommodations, which is to be
branded indefinitely and never allowed to breathe straight air again while at work.
We know that the true God has always faithfully provided for our family and He’s not in
the abandoning business. But trusting in God to provide doesn’t mean that we sit back
and watch the world crumble around us. He told us to be active and watchful. We fight
in prayer and in the physical against evil. These mandates and guidelines are created
to divide our nation and completely crumble it. Jesus himself declared this, “Every
kingdom divided against itself is brought to desolation, and every city or house divided
against itself will not stand” Matthew 12:25.
Sincerely,
Jennifer Luedeke
HEATHER MACKENZIE •
27 October, 2021
Dear Chairman Erickson and Members of the Special Committee on Government Overreach and Impact of COVID-19 Mandates,
Please accept my written testimony with respect to your 30 October meeting in Topeka.
I am adamantly OPPOSED to government mandates of COVID-19 injections.
These injections are neither safe nor effective. Nonetheless, I support the rights of those who choose to get them. It is equally important to preserve the rights of those of us who do not want them. Many of us believe that the risks posed by these experimental shots outweigh any benefit they may provide. I stand for health freedom, and I ask you do to the same.
Since the mid-80s, the pharmaceutical companies have been completely indemnified by our government. Drug manufacturers are shielded from any responsibility for the deaths and injuries that result from the use of their products. No other industry has this protection.
Data from the Centers for Disease Control and Prevention (CDC)’s Vaccine Adverse Event Reporting System (VAERS) clearly shows that the shots are NOT safe.
“Data released on 15 October by the Centers for Disease Control and Prevention showed that between Dec. 14, 2020 and Oct. 8, 2021, a total of 798,636 adverse events following COVID vaccines were reported to VAERS. The data included a total of 16,766 reports of deaths — an increase of 456 over the previous week, and two more reports of teens who died after being vaccinated.
There were 117,399 reports of serious injuries, including deaths, during the same time period — up 5,478 compared with the previous week. Excluding “foreign reports” to VAERS, 604,160 adverse events, including 7,674 deaths and 48,958 serious injuries, were reported in the U.S. between Dec. 14, 2020 and Oct. 8, 2021.
Of the 7,674 U.S. deaths reported as of Oct. 8, 11% occurred within 24 hours of vaccination, 16% occurred within 48 hours of vaccination and 28% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.”
This is horrendous.
There are no long-term studies of the effects of these injections. And there never will be reliable long-term data because every one of the drug manufacturers unblinded their studies, offering the people in the control groups the shots, eliminating the control groups.
There are safe, inexpensive treatments that are effective against SARS CoV2, such as ivermectin and hydroxychloroquine (a Zinc ionophore), in tandem with Zinc and Vitamins D and C. Some researchers are even looking into lysine therapy. I’d be happy to submit study namesand data if you like.
The COVID shots received Emergency Use Approval (EUA) under the false claim that no effective treatments exist. These shots do not meet the long-standing legal or medical definition of the term “vaccine” and should never have been granted an EUA.
The injections do not prevent infection or transmission.
A recent study entitled “Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States” looks at the relationship between the percentage of population fully vaccinated and new COVID cases across 68 countries and 2,947 U.S. counties that had second dose vaccine, and available COVID case data.
For seven days preceding Sept. 3, researchers computed COVID cases per one million people for each country, as well as the percentage of population that was fully vaccinated.
Notably, Israel with more than 60% of its population fully vaccinated, had the highest COVID cases per 1 million people during the seven-day period. Iceland and Portugal, with more than 75% of their populations fully vaccinated, had more COVID cases per 1 million people than countries such as Vietnam and South Africa, where only about 10% of the population is fully vaccinated.
Across U.S. counties, the median new COVID cases per 100,000 people during the seven-day period was similar across the categories of percentage of population fully vaccinated.
The researchers found a substantial county variation in new COVID cases within categories of percentage of population fully vaccinated. There also appeared to be no significant signaling of COVID cases decreasing in counties where a higher percentages of the population was fully vaccinated.
Of the top five counties with the highest percentage of population fully vaccinated (99.9% – 84.3%), the Centers for Disease Control and Prevention (CDC) identified four as “high” transmission counties.
Three of the four counties classified as “high” transmission had fully vaccinated rates of 90% or higher. Conversely, of the 57 counties classified as “low” transmission by the CDC, 15 had fully vaccinated rates of 20% or lower.
The authors said stigmatizing populations over vaccines can do more harm than good, and non-pharmacological prevention efforts needs to be renewed in order to learn to live with COVID “in the same manner we continue to live 100 years later with various seasonal alterations of the 1918 Influenza virus.”
Further, the CDC said the number of COVID vaccine breakthrough infections reported to the agency are an undercount of all SARS-CoV-2 infections among fully vaccinated persons, especially of asymptomatic or mild infections.
Please look at the data. Vote AGAINST mandates and for the greater good of ALL Kansans.
Sincerely, Heather MacKenzie
Written Testimony Against Covid Vaccine Mandates October 27, 2021
I am writing to express my opinion on the current Biden Administration Covid 19 Vaccine Mandate. I am against these mandates for the following reasons:
• I have a right to decide what chemicals go into my body
• It is unconstitutional for the government to decide whatchemicals/vaccines/medications go into my body
• I, or a family member, have an allergy to one of the vaccine ingredientsand/or I have a religious reason why I do not want to take the vaccine.
• I, or a family member, have had Covid in the past 3 months and havenatural lasting strong immunity against the virus. See 2 articles attached.There are more if you research.
o https://medicine.wustl.edu/news/good-news-mild-covid-19-induces-lasting-antibody-protection/
o https://news.emory.edu/stories/2021/07/covid_survivors_resistance/index.html
• The vaccines DO NOT stop the spread of the virus and need to be re-administered every 6 months. Clearly they are not as effective as naturalimmunity, are not lasting as long as initially thought by the medicalcommunity. Natural, acquired immunity is being ignored in favor ofvaccines that generate millions in profits for vaccine manufacturers.
o I personally know more people who have had Covid in the past 3months and have been fully vaccinated, than people who havehad Covid in the past 3 months and have not been vaccinated.These are not “random breakthrough” cases and these peoplespread the virus the same as the unvaccinated.
o The false narrative that vaccines stop the spread, and is our “wayout” of the pandemic along with the false narrative that it is theunvaccinated who are spreading the disease needs to stop.
In closing, I ask that you take action and vote to abolish the current Biden vaccine mandate. Julie and Steve Malecki
Leslie D. Mark
27 October 2021
Written Testimony to the Special Committeeon Government Overreach and Impact of COVID-19 Mandates
Chair, Senator Renee EricksonSaturday, October 30, 2021
10:00 AM Room 346-SKansas Legislative Research Department, [email protected]
Position – Support COVID-19 Vaccination Mandates to Protect Public Health
Chair Erickson and Committee Members,
I appreciate the opportunity to provide testimony regarding the impact of COVID-19 mandates on Kansans. COVID-19 has disrupted every aspect of life in this country and our state is no exception. Indeed, with a mere 51% of us fully vaccinated, we have still to put this pandemic behind us. However, we have the tools to do just that — with safe, effective, and widely available vaccines. It is my opinion that this is a time to be pushing towards the finish line, not turning and running in the wrong direction.
Kansans need our elected officials — individuals we’ve entrusted with the necessary power to guide our state out of the pandemic — to support scientifically proven endeavors to protect public health. It is not your mandate to create false narratives around vaccines and committee members must move beyond political posturing to identify ways to work together with public health officials to get Kansans vaccinated.
Let’s recall that vaccine mandates are hardly a new tool, having been used to protect students and workers in crowded spaces throughout our country’s history. As we saw in the mid-fifties with polio, they are effective in stopping deadly illness. COVID-19 is much more virulent and deadly than polio and a myriad of other childhood diseases we have eliminated. It’s time that we add COVID-19 to that list, and the only way to do so is by supporting vaccines in every way that we can.
Thank you for reviewing my testimony.

Written Testimony to Stop Government Overreach COVID-19 Mandates: Chairman Erickson and committee members, Thank you for forming this committee to listen to our concerns including my concerns about the recent events to mandate COVID-19 vaccination. These have attacked our liberties regarding health freedoms and bodily autonomy. In Kansas, people are being coerced into injecting a new product into their bodies that they do not want and they do not believe they need because their very livlihood and means of income are being threatened. I am an LPN at a local hospital and have been working on the front lines by testing patients for COVID-19, and I continue to do so. I will lose my job if my facility mandates this experimental COVID-19 vaccine. I have working for the last 18+ months of the pandemic to provide care to thousands of patients. I have thouroughly reasearched COVID-19 and its vaccines for hundreds of hours and have come to the conclusion that it is not in my best interest, nor the best interest of those around me to take the vaccine. My age and health status put me at incredibly low risk for severe complications from COVID-19. An unpopular truth of the COVID-19 vaccines is that they clearly do not stop transmission. I have seen many breakthrough cases of COVID-19. They are not rare. How will mandating a product that clearly does not stop transmission of COVID-19 help me to protect others from contracting it? In addition, I have very little faith in the safety monitoring systems that our country has to monitor adverse reactions from the COVID-19 vaccines. As a healthcare worker at the beginning of the pandemic, I was offered addition training on how to don and doff PPE to prepare for COVID-19 patients. I also received additional education on how to insert a nasopharyngeal swab to test for Sars-CoV 2. These are all things I had learned in nursing school. However, as the COVID-19 vaccines were about to roll out to the public, I was offered no education on what is required by law for healthcare professional to report as potential vaccine injury or adverse affects to VAERS, or how to report to VAERS. I don’t understand why this wasn’t done in the midst of the largest vaccine campaign of our time with a new vaccine product that does not have years of use. By the way, I was never taught in nursing school about how to report a potential vaccine injury to VAERS. I have never been encouraged to report or shown how to in any on-the-job training. I personally know people who have suffered great health problems in the hours, weeks or months after reciving a COVID-19 vaccine: unexplained heart tachycardia and heart irregularities, bleeding and blood cloting issues, new diagnosis of diabetes, menstrual cycle irregularities and heavy bleeding, new frequent migraines, hospitalization, progressive degeneration, and even death. The timely nature of these problems does not prove a causation to a vaccine, but one can not say that the vaccine definitviely did not contribute or increase the risk of the adverse effect. These effects are suppose to be recorded and logged for study regardless of proof of cause. This is science. However, I know this is not being done as it should and as required by law. Where there is risk, there must be choice! In additon, the studies that were done to produce the authorization and approval of the COVID-19 vaccines had such short monitoring periods, sometimes as low as 2 months. There is no way for us to determine what the long term effects of the vaccines might be in humans. I personally know a COVID-19 vaccine trial participant who was unblinded and notified of the placebo status so that the person could

choose to get the vaccine. How are we supposed to know the effects of these products when trials have been ruined by unblinding.
Please help us keep our country routed in the principles of the constitution. The power of the country lies with the people. We have a voice to be heard. Our country used to understand that major changes needed to be accomplished by changing the law, as done with the ammendments that both began and repealed the prohibition of alcohol. Now, our government has been ursurping and distorting its powers with unconstitutional executive orders and mandates that give the executive branch power that it does not rightfully have.
Please fight for Kansans. Please help us to keep our health freedoms and bodily autonomy. Please help stop the unlawful COVID-19 mandates.
Michael Marsh
Testimony to STOP the vaccine mandate
EXTERNAL: This email originated from outside the organiza�on. Do not click any links or open any a�achments unless you trust thesender and know the content is safe.
Chairman Erickson and commi�ee members:
I am providing this communica�on AGAINST the government overreach on the COVID-19 vaccine mandate.
First of all this mandate is not a law, has not been ra�fied by our congressional body and therefore should notbe enforceable by any en�ty. If Kansas does not take a stand against this mandate 1,000’s of people will be outof work crea�ng a catastrophic economic crisis that is un-precedented and illegal. Kansas is a “Right-To-Work”state and everyone who is willing to work should have that right.
Kansans should not be forced to inject something into their bodies that is not yet proven safe or effec�ve. Eventhe FDA admits, “Under the EUA, it is your choice to receive or not receive the vaccine.” The “Comirnaty” shotis not yet available to the public, and nothing else has FDA approval. I have family members who haveexperienced the horrific side effects from the shot as well as physicians using “protocols” that literally“murder” those with COVID-19 and or respiratory issues. The “protocol” even uses a non-FDA approved drugwhich comes with its own horrific side effects. I witnessed the following these “protocols” even when thepa�ent exhibited symptoms that should have merited a different course of ac�on. When I ques�oned thedoctor about the contraindica�ons he said “that’s the protocol I have to follow”.
My husband and I should be sailing into re�rement, instead we are figh�ng to maintain his 26 year career. Ifour governing body is not in alignment with “We The People” and seeking the truth and protec�ng our Godgiven rights by The United States Cons�tu�on then you are not fulfilling the du�es of your elected posi�on.We have championed you to follow the law and The United States Cons�tu�on and this calling supersedes theagenda that is being forced upon us. When you accepted your posi�on and raised your right hand under oathyou swore to protect and serve the people of this great na�on. We have entrusted you to do your job withintegrity and with your elected authority you should be standing against this tyranny that is destroying “WeThe People”.
Kansan’s deserve their elected officials to DO WHAT IS MORALLY & ETHICALLY RIGHT by notmandating this experimental biochemical agent into our bodies against our will in order to keep our jobs andlivelihood.
Rober AlumbaughClelleshia MartinHard Working ~ Tax Payers ~ God Fearing American Citizens
Written Testimony to STOP Government Overreach COVID-19Mandates (written testimony)
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
To Chairman Erickson and committee members:
I am writing the email so say I do not stand for COVID-19 Mandates. I work in law enforcement and have for 32 years. I believe in thefreedoms this country has provided to each individual through our founding documents and bill of rights.
I do not in believe Government mandates against individual freedoms, whether I believe in that person's point of view or not. No othercountry in the world has ever been created on individual freedoms. Now we are telling people what they can and can't do based on avaccine.
Companies say they will grant religious and medical exemptions then place those individuals, who are granted those exemptions, on unpaidleave, basically forcing them to quit. What did they actually grant? This is a violation of our civil rights. People are being forced to choosebetween their jobs, which in most cases the employee loves to do, and what their freedoms are. Our religious beliefs are being swept aside.
Communities, around the country, are becoming less secure as police, fire and EMS are being forced out of their jobs. Losing 20% or moreof their public servants is not acceptable to keeping a community safe. How would you feel, driving to the State Capital every day if youknew there were 20% less police officers there to protect you and how hard it is to replace them.
You can see around this country how police, fire, ems and medical care workers are standing up against vaccine mandates. A lot thesepeople have had COVID-19 and are being denied medical exemptions even with natural immunity. Some are vaccinated and just believeeveryone should have the right to choose what goes into their body. It is not different in Kansas. People everywhere across this statebelieve in freedom, including medical freedom.
I went to hear Senator R. Marshall at a townhall meeting. He stated he was being contacted by doctors all over of the state asking him forhelp in stopping these mandates. He said there were doctors in rural Kansas, sometimes the only doctor for 60 miles, that were going toquit their practice over the mandates. He also said there were doctors from KU Med saying they were going to quit. This is driving ourdoctors, nurses, CNA's, respiratory therapist out of work. I know when I need care, I would like to think there was going to be a doctorthere to care for me. Now I am starting to doubt whether that will happen.
I can go on and on about manpower shortages from Walmart to Wolfe Creek. I can't even imagine what would happen at Wolfe Creek in asevere manpower shortage. Don't force us to choose between our beliefs and a vaccine. The beliefs will win and the country and state willlose. We have worked through this pandemic for almost two years and things are normal in the community I live in, there are a reported 71active cases and 4 in the hospital at the time of this writing. People gather for large events from bike races, to disc golf tournaments, toparades. We are all living side by side with no problems. Let us continue to live our lives. Support those who chose to live a life free of thevaccine, if they choose.
My last thing is to understand who is fully vaccinated. We currently say that if you have had both doses of Phyzer or Moderna or one doseor J&J then you are fully vaccinated. But now that is being reconsidered to saying you have to have a booster shot. This can be a mix andmatch kind of thing (how confusing). What if the efficiency of the boosters wear off like the orginal shots. Then are we going to have tohave a second booster to be considered fully vaccinated? What about variants? There are reports that the current vaccines may not work

against new variants. Are we going to be considered fully vaccinated if that happens and we choose not to get those shots? When will it end? It only continues to enrich the vaccine makers. It will never end.
Let freedom ring loud and strong.
--
Ray Mattas
Written Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Chairman Erickson and Committee members,
My name is Katrina Mattingly and I reside at .
I am against government mandates of COVID-19 vaccines.
I do not believe it is right for the government to mandate that we the people have to take the Covid-19 vaccine. We live in a free country and should be able to make our own decision whether to take the vaccine or not. I have nothing against anyone choosing to take the vaccine. That is their right. Just like I should have the right to refuse the vaccine without worrying about losing my job.
My husband is a civil service employee at Fort Riley Kansas. Since he works for the federal government he is required to take the vaccine or lose his job. This is so wrong for so many reasons. He has worked there for 19 years and only has 3 years until he will retire. He did not want to take the vaccine. He does have health issues that concerned him due to side effects of the vaccines, but his doctor would not give him an exemption. His only choice was to be vaccinated. This is wrong!! My husband should have the right to decide for himself. He was even willing to be tested weekly, but that was taken off the table pretty quick. He no longer had a choice.
This is wrong!
Everyday I hear more and more people fearing for their jobs. They are given no choice. Get vaccinated or lose your job.
Everyone is getting backed into a corner. Get vaccinated or lose your job. It doesn't make sense for this to be happening in the United States of America.
We live in a FREE country.
We need You to stop the Biden Administration from forcing our citizens to be vaccinated against their will.
I am against government mandates of Covid-19 vaccines.
We need you to protect the jobs of those who have moral, ethical, religious, or other objections to being coerced into taking the Covid-19 vaccine.
Thank you for your time.
Katrina Mattingly
October 27, 2021
Chairman Erickson and Committee Members:
This is the first letter I have ever written concerning an issue that I feel so strongly about. I recently was
told I had to get the Covid 19 vaccination by November 22, 2021 if I wanted to continue to serve on my
Logan County FSA Committee. I am elected not hired by fellow farmers, but yet they and myself will not
have a voice if I won’t take the vaccine. This notification spurred me on to do my own research beyond
Facebook or other social media. I now fully understand that the Covid 19 vaccine is only authorized for
emergency use and not fully approved by the FDA. There have been thousands of deaths and side
effects to the vaccine. I am no doctor, but have learned that there are also many treatments to help
Covid patients, which are not being used. It is not worth the risk of my life or others to receive the
vaccine. It has not been proven to prevent Covid 19, so why would it be required.
I also began to researching my own constitutional rights to see where I stand. I urge you to uphold the
constitution where the federal government cannot mandate vaccine and mask requirements on States,
local governments or individuals. It is my inalienable, individual right at a Kansas citizen to refuse any
medical procedure that is against my conscience or religion. I believe all medical decisions must be left
solely with the individual with the help and guidance from respected medical professional of individual
choosing. It is inconceivable to me that individuals must make the choice to provide for their families by
taking an experimental vaccine or lose a way to support and provide for their families.
I consider the mask and vaccine requirements to be a loss of freedom as a US citizen. I urge you to stand
on the side of freedom on which the United States was founded. The vaccine card seems similar to the
arm band that the Jews had to wear in Germany. They lost their livelihood to provide for their families
and ultimately their lives. Do not turn your back on the freedoms that America was founded on.
Remember that the inalienable rights are for each and every person!
Thank you for your time and consideration in these matters.
Julie Maurath
Written Testimony to Stop Government Overreach Covid-19
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Katrina McCrummen
This is for written testimony only for Chairman Erickson and committee members.I am against government mandates of the covid 19 vaccine. I have been affected by the quarantine order, losing business during that time. Hospitals need to do what works and not what brings in the bucks. Thank youKatrina McCrummen
Sent from Yahoo Mail on Android
October 27, 2021
Dear Chairman Erickson and committee members:
As a Kansas citizen, I am strongly against health mandates, in particular vaccine mandates. I served in the US Navy and received a large number of vaccines from which I was very ill and have permanent damage. Additionally, each of the covid vaccines currently available is associated with aborted fetal cell lines whether in testing or development. As a strong supporter of the unborn, I have serious objections to this practice.
While I have had other vaccinations in the past that used aborted fetal cells, I took them without the knowledge of their ingredients or development process.
I am now waiting to hear if my company will accept my religious exemption. It is completely unfathomable that they have a right to determine if my religious beliefs are acceptable to them. I can work, I want to work, there is no reason whatsoever that I should be declined that right because I am a man of faith in this ‘free’ country.
These vaccines were never designed to protect those around you, they were solely produced to protect those who decided to take them. Never has a mainstream news outlet, that I have seen, promoted weightloss, highly nutritious diet, vitamin D, consistent sleep schedule, exercise and other health-promoting practices. That is a shame. There are preventative measures that people can take and for those that live in fear, they are welcome to take all the vaccines they would like, I support their freedom to choose what is best for them.
I served my country to support freedom. Now I expect you, in leadership, to do the same.
Thank you, Colin McDonald
October 27, 2021
Dear Chairman Erickson and committee memebers:
I am a citizen of the State of Kansas, and I am extremely concerned about the potential of encroachments on my medical freedom. I have many concerns about vaccine mandates, but chiefly is the destruction of choice when it comes to personal health and treatment decisions. In the past, it was understood that individuals had the freedom to make choices about what goes into their bodies. Recently, this freedom to follow one’s moral, ethical and personal convictions is being threatened. The Kansas Legislature must act as soon as possible to enact laws to protect the freedom of Kansans to do business and interact with society, while still being able to make individual choices.
My second concern is that of the health and safety of those who would be impacted by proposed mandates. Personally, I am very concerned about the long-term effects. I am 20 years old – I have no idea what potential impacts I could see 1 year, 5 years, or 20 years after receiving the dose. There are already well documented cases of heart issues and blood clotting. These cases show up more frequently in young men especially.
There are also many studies and evidence to support the idea that this vaccine and this illness do not warrant such extreme reaction. I and many others are making a prudential judgment as to our risk of serious infection due to Covid, versus our risk of one of the many documented potentially negative side affects to receiving the injection. I have already contracted Covid and recovered from it. According to what used to be common knowledge about viruses, as well as several recently published studies, those who have recovered from a viral infection are virtually immune to future reinfection. Even those who have not contracted Covid on average face a very small rate of potential serious infection. On top of that, forcing every citizen to receive the vaccine is not about protecting others, as those with the vaccine can still transmit the virus just like anyone else. Mandating a treatment for an illness I will never face a risk from does not make any logical sense.
You must stand against this tyrannical assault on our freedom to conduct business and live life without being forced to take arbitrary treatments. If this is allowed to continue, it will not be the last instance of forcible overreach into the lives of Kansans. If you don’t stand up to this and keep it out of Kansas, this will be the beginning of the end of our republic, and you will be at least partially to blame for it. Think long and hard about how you proceed.
Connor McDonald
October 24, 2021
Dear Chairman Erickson and committee members,
I am a resident of Miami County, Kansas and very much against the government mandates.
We can never vaccinate our way to health. Never in history have we been asked to vaccinate for an illness we have already had. Secondly, the long term safety data is not available, we have no idea if this will cause significant cancer as the Polio vaccine did in the late 1950’s. Early research published by Sloan Kettering did show that mRNA vaccines did inactivate cancer prevention genes which is very concerning, I have known a LOT of people recently diagnosed with cancer. What if long term research ends up showing the creation of prions that then cause Alzheimer’s disease?
Each of the covid vaccines currently available is associated with aborted fetal cell lines whether in testing or development. Based on my sincerely held religious convictions, I cannot subject my body to this injection.
While we may have religious exemptions available now, that may not be the case in the future so we have to protect the people from government overreach.
My husband, the primary breadwinner in our family, is facing a job loss. We are very healthy people, we work hard to maintain a health weight, avoid sugar and other health degrading foods and do all we can to make ourselves healthy. We are also very willing to work and contribute to society. What good does it do to deprive us of jobs? What good will it do to do the same to so many across the state of Kansas?
I urge you to do the right thing and protect Kansans for mandated health requirements. There is so much at stake now. Thank you for supporting freedom in America.
Melissa McDonald MelissaMcDonald

Janine McGlachlin
This is my written testimony. I won’t be able to be in Topeka on Saturday.
Chairman Erickson and Committee Members,
I am strongly against the COVID-19 vaccine mandates, quarantines, school masks, social distancing.
I teach 2nd grade. Last year I had a perfectly healthy boy who had to be quarantined for 2 months
because his dad and sister tested positive. He was quarantined longer than they were because of the
mandates. His reading scores were already low, so he was receiving special inclusion services at school.
During quarantine, his family was unable to provide the instruction he needed, the zooms meetings
were not effective and he lacked motivation being isolated from his peers. When he returned to school
after the 2 month quarantine his reading scores were lower and he had to be placed in a pull out
situation. Again, he was away from his class. His self-esteem was low. He told my para that he couldn’t
read. It broke my heart!We will never know what his reading ability would have been if he was
permitted to stay in school those 2 months and if he could have finished 1st grade in person, during the
shut down.
We currently have a flow chart that determines if a student has to be quarantined or not. It depends on
whether you have been “vaccinated” and if you are wearing a mask.Nowhere on the flow chart does it
give any credit to having had covid and therefore having your own God given antibodies! This is
ridiculous!
It is a sad sight to see half of a class leaving, carrying their books and crying because they all have to be
quarantined due to contact tracing during lunch. Those 9 and 10 year old boys had to miss their first
football game because they were within 6 feet of a person who tested positive. Now, they eat in
assigned seats, in a “satellite” lunchroom and are 6 feet apart. Is that how you like to eat your meals?
Not making students be quarantined if they wear masks, means that more children are wearing them.
No more smiles to that student that is having a bad day. It is very sad. Last year, I had a student that had
her mask accidently fall in the toilet. She was scared to be caught by the nurse without it so she got it
out of the toilet and put it back on! Another student wasn’t feeling well and he ended up vomiting in his
mask. These are very sad but true stories about what is happening to our children around the country!
Please, let Covid be like the flu. Sick people stay home, healthy people continue to go about their lives.
Dear Chairman Erickson and committee members,
I am completely against government mandates of COVID-19 vaccines, masks or
any medical mandate. We must have freedom over our bodies and our health or we
have no freedoms at all.
Check out the VAERS website (openvaers.com/covid-data) to see that there is
risk involved here. Where there is risk, we must have a choice. Don’t I have freedom to
make decisions for myself and my family? What kind of state, country or world will we
have if we do not have the right to make decisions about our own health? Where will we
be if parents don’t have the right to choose what is best for their child? No one knows
our children like we do and there is no way that someone else is going to know what
they need more than my husband and I. We are definitely thankful for the doctors and
nurses in our healthcare that we can call on when needed, but that in no way should
eliminate us from the position of guardian of our children.
We must all stand up together against this tyranny. We must fight for the
freedoms that our military have, and continue to fight for.
This is definitely a moment in history that will be remembered. Which side of
history will you be on? Medical decisions should be made by each individual and their
physician only. Medical information should be kept private. Medical procedures should
never be forced. It is not possible that this is the right decision for everyone across this
state, let alone the entire country or world. It should be a choice.
Please stand for medical freedom. Please protect all Kansans. Please stop the
mandates immediately.
Thank you for you time.
Joy McGuire
To Chairman Erickson and committee members,
Please accept this testimony as against the government mandates of COVID-10 vaccines. I have been an
employee of Kansas State University for almost 10 years and very much a part of a team and family with
my coworkers and supervisor. We provide integral support for our university main admissions office,
and we are facing short staff numbers like we have never seen before due to the mandate ultimatum.
We are already understaffed by 11 employees and uncertainty of how many more we will lose will be
detrimental to our university.
Personally, my family depends on my income to provide food, shelter and basic needs to live. I have now
been given an ultimatum of comply to this vaccine mandate or be terminated by December 8, 2021. I do
not believe it is right, ethically or constitutionally, to force someone to take an experimental drug, and
the only other option is to lose my career I have worked so hard to obtain.
Thank you,
Holly McHugh
Written Testimony to the Special Committee on GovernmentOverreach and Impact of COVID-19 Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Written Testimony to the Special Committee on Government Overreach and Impact of COVID-19 Mandates
Chair, Senator Renee EricksonSaturday, October 30, 2021, 10:00 AM Room 346-SKansas Legislative Research Department, [email protected]
Position – Support COVID-19 Vaccination Mandates to Protect Public Health
Chair Erickson and Committee Members,
Thank you for the opportunity to provide testimony regarding the impact of COVID-19 mandates on Kansans.COVID-19 has turned our lives upside down, and many of us have lost family and friends, or feared for the health ofloved ones as they struggled through a COVID-19 infection. Sadly, COVID-19 is still very much an active virus,and we should be continuing to take every step we can to combat it through making sure that every eligible personis vaccinated. We must not give up the fight now.
The special committee should not be political - addressing COVID-19 is not a political issue - but one of immenseimportance to each and every Kansan. It is important for everyone to work together to solve this crisis. Now asthe vaccine has been approved for children as young as five, we should be focussing our efforts to make sure thatall school age children are safe and healthy. Our elected officials should be supporting scientifically proven ways toprotect public health, not widely sharing false information about vaccines and COVID-19 prevention strategies.
Federal vaccine mandates are not new - they have been used in the United States since 1904 - and have beenupheld by the Supreme Court. Vaccines have been shown to be safe and effective in stopping deadly illnesses anderadicating childhood diseases. I am so grateful for my childhood vaccinations - my mother talked often of her fearof contracting polio as a child and how miserable she felt when she had the mumps and measles. She helped me tounderstand at a young age how important vaccines were to my health and the health of others. When the COVID-19vaccine was approved, I cried tears of joy, knowing that it was going to radically change the course of the pandemicand save lives...and it has. But it will be most effective if as many eligible people are vaccinated as possible.Therefore, it is time for Kansas Lawmakers to support the COVID-19 vaccine mandate and work hard to help alleligible Kansan's get vaccinated.
Thank you for considering my testimony.
Respectfully,
Anne Melia
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless you trust the sender and know the content is safe.
Chairman Erickson and Committee Members,
I am a life-long Kansas resident and am strongly opposed to government mandates of any kind related to the current health scare. The statistical information shows this current “virus” is not as deadly as the treatments, including shots, have proven to be.
Safe cheap and commonly used medications have been kept out of the public sphere for the most part. We should have access to these, not government interference, in our health care choices!
In July of this year, I asked my family doctor for a prescription to have either HCQ or Ivermectin on hand, as I am over 65. He said to call the office and we could discuss it, if I had symptoms. When I got sick and went to the doctor’s office a month later, I was immediately sent to the Emergency Room, diagnosed with Covid Pneumonia. After being admitted, I was also diagnosed with bacterial pneumonia. The good news is that I received antibiotics and had the good sense to leave the hospital in less than 24 hours! I was prepared to go “against medical advice” to leave, if necessary.
After being discharged, I continued to heal over the course of several weeks. However, the family doctor did not call, or see me for three and a half weeks.
Since then, I have a new doctor and am sure I also have natural immunity going forward!
What government mandates and intrusion into health care means for Kansas citizens of any age is interference with our established relationships. It is an overreach of authority, any way you write or regulate it.
Please don’t make the world-wide healthcare debacle worse here! Back away from the urge to regulate our lives based on what others are doing. Let Kansans live by our state motto, “to the stars through difficulties”, through the good health that comes to us from many, many sources. Good health is our choice and I do not want any of our citizens to be hurt by well meaning efforts outside of their control.
Sincerely,Elizabeth Meunier
Mandate over reach
EXTERNAL: This email originated from outside the organiza�on. Do not click any links or open any a�achments unless you trust thesender and know the content is safe.
Internal Use Only
To whom it may concern
The mandates are so far out of bound for the defini�on of people living in a free republic.Emergency use authoriza�on means NON Mandatory! I have spoken to my doctor on thisAnd voiced my concerns in terms of some of my personal underlying condi�ons. He flat outSaid they do not have those answers. If they ever do, it most likely will not be available un�lAround the second quarter of 2023. By then if something of concern is found it will be too late.Vaccine injury is a real thing. MIT just recently published a paper advoca�ng a precau�onaryapproach. In addi�on it faulted all those as part of this solu�on of being very deficient in doing li�le,if anything in terms of providing the public with prophylac�c approaches that have been proven toprevent or greatly mi�gate the affects of Covid-19. Instead we are being beli�led in the media,shouted down using the talking point “Sound Science” as if that is an end all To all further discussion. At a minimum 57 people a day, and that number is in all likely being vastly underreported,Are being killed by the virus. Not confirmed yet, but a friend of mine may have been one of those killed by aTreatment he was very reluctant to take. By the way, the original covid outbreak of SARS had a vaccine createdThat was very promising, looked like it had great protec�on but fell failed disastrously when exposedlater to a wild variant. Precursor to something like Delta, or Mu? And blaming the un-vaxxed for causingthe variants. Variant happen when the virus makes gene�c changes to overcome the defenses of someonewho has already been vaccinated. That has been known for over 100 years. I am sick of the media. They are not telling us the truth. This is too overhanded and poli�cized to be trusted anymore. Watch them. Look at who is providing the greatest revenues in terms of adver�sements come fromthose said companies that will profit with full indemnity and at the same �me insist that we shouldhave no choice or any fundamental rights as well as protec�ons. Everything has gone too far. Time to reel the overreach in.
Sincerely,
Jerry Meyer
Ava Mikesell
October 30, 2021Dear Chairman Erickson and committee members,
Thank you for your time and efforts put into our Kansas legislation. Regarding
government mandates of COVID- 19 vaccines, I am against forced compliance. There is no
consent if it is mandated which violates our rights as human being.
My position on this argument has come with much time and experience. As of February
2020, my unit at Ascension Via Christi St. Francis became the COVID intensive care unit. When
February came I was not prepared for what I was about to endure as a healthcare worker. I can
not begin to describe the feelings and emotions of going to work, attending work, and leaving
work without getting choked up. The trauma that many of the healthcare workers endured will
leave a permanent mark on us. As the days went from weeks to months I realized that this will be
our new “normal”. The promises from our government officials saying if you wear a mask it will
end and it indeed did not. Then a promise of if you get the vaccine it will end and it indeed did
not. This is now the turning point that we must not instill fear into others yet get back to the
basics of nutrition, sleep, and a healthy lifestyle.
I hope as your read and hear many of the testimonies that you take into consideration the
people who went into the fires as others ran far from the situation. We were there for these
individuals when no one else was, I get asked “how many people have you seen pass away” and
my answer is “too many”. Mandating will only make the situation worse. We are putting into
jeopardy the lives of our patients by firing those who think differently and choose medical
freedom. It is our time to rise above and put our egos aside and listen to the people who think
differently. In a country that requires consent and can go to jail for violation of consent, it is
getting blurry. We shall allow others to make their own decisions because it is their body and we
shall not be shamed become of it. Thank you.
Sincerely,Ava Mikesel
My name is Holley Million. This is a written testimony only to my legislators in Topeka, Ks.
Dear Chairman Erickson and Committee Members,
My name is Holley Million, and I’m writing you this written testimony to explain to you why I amAGAINST government mandates of covid 19 vaccines.
I have worked as a physician assistant for over 18 years and will be losing my job if I don’t takethe covid-19 vaccine by my employer Ascension Healthcare by Nov. 12, 2021. I was denied areligious exemption request against taking the Covid-19 vaccine by Ascension on Oct. 18,2021.I was also denied a religious exemption for the influenza vaccine that my local Ascensionhospital in Wichita, KS, gave me a LIFETIME exemption for in 2018. This lifetime exemptionwas revoked this year all of a sudden. This year, our local Ascension hospital no longer wasallowed to review and handle exemptions locally and the decision was decided by CorporateAscension. I should have a right to refuse anything that I feel is unclean or potentially harmful tomy body. Despite a biblically, scripture based religious exemption I was told they were unable toaccept my request for religious exemption because of insufficient information. How are myreligious beliefs insufficient? A few days later I received a follow up email that stated if I couldprove to not be in direct patient care that I could provide additional information and send in anew request but I do provide direct patient care. I am being discriminated against for my upheldreligious beliefs to refuse to take something that is potentially and has proven to be harmful tomany people. Natural immunity has always been the best course of action and the healthcaresystem always pride themselves from A Doctors Oath ‘First do no Harm’. They will be and havebeen harming many people by forcing a vaccine that was approved for emergency use and hasnot been fully tested or given enough time to see the lasting affects it could and has shown to becausing now. I’m the sole provider for my family and have been since my husband left a greatjob with benefits and retirement from the Wichita Fire Dept in 2008 to be a stay at home dadbecause of my very busy job as a PA. My job provided for my entire family so one of us couldstay home and care for our three children. My husband is now being forced to go find workbecause of this vaccine mandate and me losing my job because I was denied religiousexemption. My kids have been affected repeatedly by mask mandates at their school and hascaused depression for both my daughters and we did not put our son in pre-k last year just sohe would be protected against wearing a mask all day and with him being so young not knowingwhen his breathing could be affected and recognizing the need to pull the mask down to breathelike my older daughters know and did despite repeatedly getting In trouble for doing so. Not tomention the multiple times my oldest teenager was quarantined due to a ‘close contact’ caseand missed out on many school functions as a result and many school functions were cancelleddue to too many students being not in school and were at home quarantined. My other daughterhas already been quarantined this year and missed two volleyball games, practice and justbeing able to get out of the house as a 12 year old and it affected her mind set as well. As aparent we are doing everything we can to protect our children but our rights are being takenaway from us. We can’t go to ball games if we don’t wear a mask , my daughters’ band and
choir concerts were cancelled because they couldn’t be too close to sing or play theirinstruments but yet football and basketball teams got to play at the school. And when mydaughter did get to play in Band later on she had to wear a mask with a hole in it to play herflute and then there was another mask covering the end of her flute. She came home daily withheadaches and exhaustion because of not being able to breath. No one at the school inSedgwick cared. I shouldn’t have to lose my job from making a personal choice to not take avaccine. I’m an American Citizen and I should have a right to decide what goes into my bodyand not be controlled by my own government who is treating this nation like we are no longerfree citizens. I’ve lost my 1st Amendment right and live under a tyrannical government wholonger cares for its citizens and their rights. I’ve taken care of COVID-19 patients in the hospital,I’ve worn a mask every single day at work because I was forced to and yet this same hospital isrefusing my religious exemption and forcing me out and will suspend my privileges and I can nolonger work there. Now I risk losing everything, not only my job but my home, medical, dental,eye insurance, lifestyle and the added stress that will incure when I’m no longer able to providefor my family.
Sincerely,Holley Million
Chairman Erickson and Committee Members,
My name is Barbara Minton and I am providing my written testimony AGAINST Government
mandates.
Covid 19 shots – regardless of brand - ARE a medical procedure and, as such, carry inherent
risks. Our innate freedom includes our right to pursue or decline this medical procedure. The risk
MUST mean we have a PERSONAL CHOICE for ourselves and our families.
Our God-given right to bodily autonomy is, or at the least should be, unequivocally a freedom
guaranteed to all citizens of our country and this state. Freedom is not a right or left, conservative
or liberal, or republican or democrat concept – freedom is a HUMAN concept. Mandates,
particularly medical mandates, are the antithesis of that concept. Our human freedom to choose
to pursue a medical procedure, or not, MUST be a personal decision! The government, in
initiating these mandates, has vastly overstepped the bounds of authority provided by “We the
People”.
This overstep of government mandates against freedoms has led to the incentivizing of
companies to push this product on employees and has become a “take the jab or lose the job”
concept. This is not a choice, but rather a coercion. Currently, thousands of employees will either
walk away from jobs they love because they will not compromise their freedom OR they will be
fired for their choice and belief – again, this is not a choice, but rather a coercion!
For the last 12 years I have spent several thousand dollars to help by body clear all the poison injected
when I had massive chemotherapy. Which I now realize, I should never have had done because of all
the damage to organs that were previously fine, i.e. heart, liver, kidney and the brain (which cannot be
officially documented). I certainly do not want to further inject chemicals into my body that can
further damage me.
As elected officials, you work for WE the PEOPLE and WE have spoken! We are begging you
to protect our human right to freedom to choose for ourselves regarding medical procedures. We
are begging you to support the citizens of Kansas, not business entities, not government acronym
entities – support us, the PEOPLE whom you serve.
Please, STOP the MANDATES! Protect employees from termination for choices for personal
freedom! Protect we the people from government overstep.
Sincerely,
Barbara Minton
Chairman Erickson and Committee Members,
My name is Sammy Minton and I am providing my written testimony AGAINST Government
mandates.
Covid 19 shots – regardless of brand - ARE a medical procedure and, as such, carry inherent
risks. Our innate freedom includes our right to pursue or decline this medical procedure. The risk
MUST mean we have a PERSONAL CHOICE for ourselves and our families.
Our God-given right to bodily autonomy is, or at the least should be, unequivocally a freedom
guaranteed to all citizens of our country and this state. Freedom is not a right or left, conservative
or liberal, or republican or democrat concept – freedom is a HUMAN concept. Mandates,
particularly medical mandates, are the antithesis of that concept. Our human freedom to choose
to pursue a medical procedure, or not, MUST be a personal decision! The government, in
initiating these mandates, has vastly overstepped the bounds of authority provided by “We the
People”.
This overstep of government mandates against freedoms has led to the incentivizing of
companies to push this product on employees and has become a “take the jab or lose the job”
concept. This is not a choice, but rather a coercion. Currently, thousands of employees will either
walk away from jobs they love because they will not compromise their freedom OR they will be
fired for their choice and belief – again, this is not a choice, but rather a coercion!
There are many reasons people would not consider taking these shots. There are unknown health risks,
some of which are severe, up to and including death. For these reasons alone, NO shots should be
mandated to the point of losing your job or possibly dying. I have worked in emergency medicine
field for more than 30 years and have seen so-called vaccines vary greatly in their effectiveness, if at
all. Therefore vaccines should be a personal choice to receive or NOT.
As elected officials, you work for WE the PEOPLE and WE have spoken! We are begging you
to protect our human right to freedom to choose for ourselves regarding medical procedures. We
are begging you to support the citizens of Kansas, not business entities, not government acronym
entities – support us, the PEOPLE whom you serve.
Please, STOP the MANDATES! Protect employees from termination for choices for personal
freedom! Protect we the people from government overstep.
Sincerely,
Sammy Minton
27 October 2021
Dear Chairman Erickson and Committee:
I am writing to encourage your opposition against all COVID-19 vaccine mandates.
President Biden and many members of Congress are calling for regulations that would punish private companies with 100+ employees. If this goes through, I will lose my job which I have had for more than 26 years.
Please stand up for your constituents and help Kansas follow the example of Texas, Indiana and Montana in prohibiting employees from terminating employees who refuse the vaccine.
Thank you for all you do.
Sincerely,
Ric Mitchell
Written Testimony Against Government Overreach and the impact ofCovid-19 Vaccine Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Rosalind Mitchell
My personal testimony about Covid 19I wanted to share what Covid-19 has done to me,my family and the medical profession. Personally I hadCovid in late May 2021.I was fortunate to have a mild case and my recovery was greatly helped by my Dr's order for MonoclonalAntibodies early treatment. Which sadly now either is not not widely available in Kansas or is beinglimited by the federal Government. I have developed natural immunity and do not feel the need forvaccination. And would object to taking it due to the use of aborted fetal cells in testing and formulatingthe vaccine which are against my religious beliefs.So personally I am a black woman and my family has been negatively affected by this currentadministration's handling of covid -19. We are a small family and we used to enjoy gatherings.Recently, We have become divided. Hardly speaking to one another because of our personal choicesabout the vaccine and due to disinformation they have heard from the Federal Government and the CDC.In my family we can't have conversations about this. Half my family believes everyone should fall in lineand for what the Government says. I personally do not and there is no more freedom in familydiscussions. I hope we will have a time to celebrate Thanksgiving and Christmas as a family this year
I have been a registered nurse for over 30 years and in all of my years of practice I have seen treatmentsrecommended like "flu" shots and have been a Nurse long enough to see the "flu" be more deadly forexample with the H1N1 strains and there was no push for everyone to be Vaccinated by that DemocraticFederal Administration. The medical community participating in withholding vital early treatments forCovid-19 is unprecedented. I am semi- retired and this Covid-19 itself has cost me several months out ofwork in 2020. With me only restarting work in the fall of 2020. I am currently working full time to catchup from the losses of 2020 in 2021. I don’t know when I will be able to fully retire.
I feel all the mixed messages coming from the federal government, the current president, the CDC andmany members of the current administration have fostered a lack of trust in the african americancommunity. These mandates should not be followed and they should not be forcing adults and nowChildren to take these vaccines with hardly any research on the long-term effects. What a damaging planby this Federal Administration. And Hopefully Kansas will not enforce this and stand up against it.
October 27, 2021
Chairman Renee Erickson and Committee Members Special Committee on Government Overreach and Impact of Covid-19 Mandates Kansas State Capitol 10th and Jackson, Room 546S Topeka, Kansas 66612
Re: Written Testimony to STOP Government Overreach Covid-19 Mandates
Dear Chairman Erickson and Committee Members:
My name is Debbie Mize. I reside in Louisburg and have grave concerns not only for myself but for my children and grandchildren.
II have presented to this legislature and to my County Commissioners since May of 2020. The overreach of this state’s government officials, private businesses and government organizations to attack our Constitution has been disheartening. Now, the freedom afforded to us by our Constitution is being further eroded as we watch residents being fired from their jobs or forced to vaccinate. We watch helplessly as the Kansas Board of Healing Arts, Kansas Department of Health and Environment and the CDC continue push for mask mandates and forced vaccination with data that manipulates COVID-19 numbers.
Now, this week, I watched as the FDA manipulated data and science to rush a dangerous vaccine to market for young children, the most precious and vulnerable population of Kansas. It is beyond dispute that vaccines for COVID have not been studied and tested in the normal sense, yet we are ready to inject these into our five-year old’s.
By failing to pass S.B 212 the legislature left the door wide open for an agency that has been out of control the past two years, the Kansas Department of Health and Environment. With this open door they are free to mandate this dangerous vaccine simply by a regulation. How will you protect Kansas children if the KDHE mandates this vaccine once it is officially approved in a few weeks?
Many people in Kansas have became complacent but I see many of my friends and neighbors who are now engaged who WILL hold each of you accountable for your decisions. Be advised that people who are not satisfied with an unwillingness to protect our jobs, our children and our grandchildren, will likely not be your supporters in 2022. Please support SB 212 to restrict the power of the KDHE to mandate this vaccine.
Most respectfully, Debbie Mize Vice President/Lobbyist Louisburg, Kansas
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates
Dear Chairman Erickson and Committee Members,
I am against government mandates of COVID-19 vaccines.
Government handling of COVID-19 procedures and mandates of COVID-19 vaccines have hada massively adverse effect on our populace -- physically, mentally, and emotionally. First, therewas the knee-jerk reaction to increased cases of COVID that isolated many elderly and lonelyindividuals leaving them with feelings of more hopelessness. Forcing a reduction in respect offree movement and visitation has caused many deaths, including untold suicides. Governmentson any level have yet to acknowledge these citizens they harmed or to take responsibility fortheir damaging decisions. Our government was never established to dictate how we could moveor travel. Well, actually, slave states did that for many decades. So I guess governmentrestrictions of today should proudly cite that precedent.
And yet, the abusive dictates roll on. For many months, various pharmaceutical companies haveoffered their version of the COVID vaccine. In a normal setting, taking an injection of anythinginto your body has been a choice -- insulin, antihistamine, rheumatoid arthritis medication, etc.None of these are required medical actions, even if you have diabetes, allergies, or RA. I’m surethe counter-argument to that last sentence is, “But none of those afflictions are communicable.COVID kills, so you better take the vaccine.” Are we not seeing vaccinated people get COVID?Can’t a vaccinated person spread COVID too? The answer to these two questions is yes!
But that’s not all. A simple web search of “can vaccinated people spread COVID” results inmany articles confirming that they can. So why is the spread of COVID vehemently being laid atthe feet of the unvaccinated? An article from FactCheck.org on the topic of “COVID spread fromthe vaccinated” significantly downplays the chance that vaccinated people can spread the virus,but still admits its possibility. Furthermore, that article admits that the vaccine can be effectiveagainst the Delta variant at a range of 39% to 84%. That’s a heck of a range! That is not at allconvincing that citizens should be bullied and/or threatened to participate in this stillexperimental vaccine. I call it “experimental” because the results have not been studiedlong-term, nor have political interests been taken out of policies.This same article also reportsthat the CDC has changed its definition of “breakthrough cases” as of May 2021. Previously, allpositive tests from vaccinated people were “breakthrough cases”, but for the past 5 months onlysevere cases are reported as “breakthrough”. Making this reporting change has no doubt keptvaccinated people out of the cross-hairs and has thrust the unvaccinated further under the buswheels. When you change the rules during the game, that’s not science but agenda. Thisever-changing “science” is the basis for blame against those people who have chosen not tosubject themselves to vaccine injection(s) that are not proven nearly as effective as first toutedand not reported widely enough as possible medical threats to healthy or youthful recipients.
When tracking how someone has gotten COVID, there is no sure way to know the source.Possible reasons, such as large gatherings or unmasking, are usually to blame, but these are
not proven reasons. Ridiculous reporting still dominates the airwaves and internet. Announcingthat someone has gotten COVID from an unvaccinated person is unprovable, yet ourgovernment is going after such people as though they have committed a crime.
Threatening behavior generally falls into long-existing “zero tolerance” policies of thousands ofbusinesses, churches, and institutions. Government must adhere to just such policies. In suchwords and actions, they are exuding power without authority. Their actions arecounter-Constitutional. Courts have and may continue to find restrictions and mandatesunconstitutional. But even if they don’t make that official declaration, we citizens know whengovernment has gone too far. The Amendments are great examples of knowing whengovernment should be limited. Contrary to public belief, the 1st Amendment does not state thatgovernment gives the right of speech, religion, press, etc. It protects the government frominfringing on those rights that we already have. The 2nd Amendment is very much the same --we have the right to bear arms, not the government is giving it to us. Further amendmentsspeak to giving people more freedoms because government restrictions and declarations havenot done so. The 13th through 15th, the 19th, and the 26th Amendments all broke downrestrictions that were at some point likely imposed “to protect society”. Restrictive and forcefulgovernments are never the good guys in history, despite their many power grabs claimed “forthe greater good”. If someone were in a personal relationship where their partner was forcingthem into medical practices against their will, restricting their movements if not obeyed, andthreatening their job status if not followed, that would clearly be an abusive relationship thatanyone would strongly advise leaving immediately. Yet our government talks as though we arethe problem. An abusive and narcissistic person acts this way toward others, explaining that hemust act this way against you because you are creating a toxic environment that makes him actso forcefully.
Creating a “one way fits all” policy of vaccination only through injection is also bad governanceand bad science. For example, single-payer health care systems have long been rejectedbecause citizens would no longer have choices. Vaccination status is currently split into only twocamps -- vaccinated and unvaccinated. Yet, the “unvaccinated group” does not get to defineitself. I have had COVID, which is why I am not planning to get a COVID vaccine. Getting aninjection of the same disease that I have survived and built up a natural immunity to is reason tonot get any particular vaccine, not just the COVID one. Getting the vaccine and getting COVIDare medically the same thing. However, I am cast by others into the “unvaccinated group” asthough I don’t care what happens to others. I was under the impression that societyencourages each person to identify as they choose and to reject what others impose on them. Iguess that only counts for other categories. Seriously, though, where are the tests and studieson COVID transmission involving the millions of Americans having survived COVID? This giantsector of Americans are ignored; their status is not respected. The governmental and mediabullies simply refrain, “Vaccinated good, unvaccinated bad”. Or as the brainwashed geese inAnimal Farm chorused, “Two legs good, four legs bad!” That novel, by the way, exposestyrannical governments that try to “reward” their people by re-establishing societal status quoonly after obeying forced government requirements. Getting to gather for a family reunion, whichI had the right to do all along, only after getting a vaccine injection is not an incentive; it’s a
ransom. An abductor releasing a kidnapped person is not credited with giving the abductee theirfreedom. We are simply hearing shouts of uneducated mottos and victories, not real science norproper authority.
We cannot stand as real citizens if COVID vaccine mandates continue. Various governmentrestrictions do and will continue to frustrate us in many political categories, but forcing andthreatening free people whom the government is called to serve is tyrannical. Thank you foryour time.
Sincerely,Andy Monday
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates
Dear Chairman Erickson and Committee Members,
I am against government mandates of COVID-19 vaccines. I am aware that the Emergency UseAuthorization (EUA) status has been removed from the covid vaccines, and that is the excusethat is being used to justify this vaccine mandate. But that is only the removal of a title.According to the College of Physicians of Philadelphia in 2018, “vaccine development is a long,complex process, often lasting 10-15 years and involving a combination of public and privateinvolvement.”
Covid was first seen in the United States early in 2020, yet a vaccine was released to the publica mere nine or ten months later, and by October of 2021, a mandate is being called for. There isno way that the large scale, double blind trials have taken place to determine the full realm ofside effects. In fact, I see quite the opposite. As millions of Americans chose to or feel pressuredto receive the vaccine, huge numbers of serious side effects are being reported, bothanecdotally and to the Vaccine Adverse Event Reporting System (VAERS) that was establishedfor this exact purpose by the FDA and CDC. Yet the only message that is coming through fromthe media is that the vaccine is safe and effective.
The VAERS website (https://openvaers.com/covid-data) states that “it is a voluntary reportingsystem that has been estimated to account for only 1% of vaccine injuries”, yet it currently postswell beyond 1.6 million adverse reactions to the covid vaccine, including more than 17,000deaths and 83,000 hospitalizations. And that could be just 1% of the vaccine injuries? Yet thevaccine is pushed as “safe” and now falls under a mandate.
The vaccine is touted as effective, and that those who are vaccinated are less likely to contractcovid or to have serious cases. I don’t see that happening any more than the vaccine provingsafe. On a small scale, I have a friend who is a substitute teacher at a small private school. Ofthe seven faculty that she has substituted for following their positive covid tests, six of themwere vaccinated. If there are only 1 in 5,000 “break through” cases (positive tests followingvaccination), how can six of seven cases on a small faculty be vaccinated? That does not comeclose to lining up mathematically! On a much larger scale, according to one report, 45% of thosehospitalized in New York City are vaccinated. The vaccine is not nearly as effective as it isclaimed to be!
Regardless of this data, which is disturbing, the fact remains that for any other vaccine, wewould still be in the exploratory stage of the vaccine development. Yet here we are beingmandated to receive the vaccine. When people choose to participate in a medical study, it istypically either because they are personally interested in the study or because they believe therisks of the trial medicine or vaccine are no worse than the risks of the disease. By beingmandated to receive a vaccine, we are being forced into a medical study. There is no databeyond a year for this vaccine, because it hasn’t even existed for a full year. The durability of
natural immunity from a personal case of covid is yet to even be explored. Evidence of sideeffects of the vaccine is being ignored. I have no desire to be a part of this “study”!
For many people, the risks of covid are marginal. Without comorbidity factors such as age andpre-existing heart and lung conditions, the chances of a severe case are slim - likely slimmerthan the prospect of side effects from the vaccine. I implore you, allow those who wish toparticipate in this vaccine trial to participate. I’m glad it exists for them. But for those who havereasons to not participate, please do not mandate the covid vaccine. Allow us to maintain ourfreedoms. There are serious dangers in many everyday activities that we accept and areallowed the freedom to participate. For example, we choose to drive our cars day in and dayout, despite the knowledge of car fatalities posted along major roadsides. Allow us, and not thegovernment, to also choose between the risks and benefits of a vaccine. Tying those mandatesto loss of employment, further hindering our economy, is ludicrous. Stop the mandate now.
Sincerely,Rachel Monday
Written Testimony to STOP Government Overreach COVID-19 Mandates 10/27/21 Dear Chairman Erickson and Committee members, I am AGAINST this government mandate for COVID-19 vaccines. I worked for Textron over the summer. I'd like to continue working for them again. I have already had covid. I've been natural vaccinated. Why don't my natural immunities count? Avery Morand
Written Testimony to STOP Government Overreach COVID-19 Mandates 10/27/21 Dear Chairman Erickson and Committee members, I am AGAINST this government mandate for COVID-19 vaccines. I started working for NIAR while I was still a high school student. I graduated this year and continue to work for NIAR to help pay my way through college. I have been working fine without a vaccine and without infecting anyone. I have already had Covid. As a young health 18-year-old male, my risk of getting myocarditis from the vaccine worries me more than getting Covid again. Why doesn't my natural immunities count? Cameron Morand
Written Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless you trust the sender and know the content is safe.
Dear Chairman Erickson and Committee members,
I am AGAINST this government mandate for COVID-19 vaccines. ThisGovernment overreach is a huge attack on this country's freedom.
In one breath they scream for a "Woman's Rights" to her body, (ie, theright to have an abortion), in the next breath they scream, "Who caresabout your freedoms!" This is life and death! No. Abortion is life anddeath. This is a massive case of attacking our constitutional rights,misinformation and corruption like this country has ever seen.
Please stand up for American Freedom and values and say, "No", to thisvaccine mandate.
Jayson Morand
Written Testimony to STOP Government Overreach COVID-19 Mandates 10/27/2021 Dear Chairman Erickson and Committee members, I am AGAINST this government mandate for COVID-19 vaccines. I, along with my husband and two sons work for four different federal contractors. In less than two months, this one mandate will wipe out a whole family’s ability to earn a living. I was considered an essential worker since the beginning and have never stopped going into the office. During this whole time, I have been able to do my job without being vaccinated and without infecting anyone. Please help us stop this insanity and preserve our way of life. Maria Morand
October 27, 2021
Dear Chairman Erickson and members of the Special Committee,
I am writing to express my opposition to government mandates of COVID-19 vaccines.
Since COVID-19 was unleashed on the world in 2019, governments have employed numerous unprecedented tactics to mitigate the virus’ damage, at enormous cost, both financially and in terms of human freedom.
Lockdowns only delayed the inevitable spread of the virus. Even island nations like New Zealand were forced to abandon their “COVID Elimination” strategy1. Many counties in Kansas locked down in hopes of sparing hospitals from being overwhelmed, but caused the unintended effect of putting rural hospitals out of business2.
Mask mandates have not been shown to have slowed the inevitable spread of the virus, yet have had negative consequences in terms of plastic pollution, hypercapnia, and stunting children’s social and emotional growth by hiding faces3.
When the first SARS-CoV2 vaccines were released in 2020, the world was united behind the hope that these vaccines would be as safe and effective as prior vaccines at eliminating lethal pathogens, such as Small Pox. Unfortunately, none of these hastily developed vaccines lived up to those expectations. The vaccines’ effectiveness at preventing SARS-CoV2 transmission wanes after a few months, with the J&J vaccine performing worst at 3% effeciveness after only 6 months4. Naturally acquired immunity, however, has been found to be effective for preventing reinfection for as long as data has been available5.
These novel Gene Therapy vaccines have also been found to be exceptionally dangerous, which is a predictable outcome after an experimental immunotherapy technology was rushed to market with no long-term clinical trials. Hundreds of thousands of Adverse Reactions have been reported to the CDC’s VAERS database, including over 7,000 deaths, which exceeds the number of deaths reported from all other vaccines since 19906.
Because SARS-CoV2 vaccines do not prevent the spread of the virus, mandating their use cannot be accurately described as Public Health. Vaccines are freely available to anyone who wishes to receive them, and may protect the Vaccinated from the most severe COVID-19 symptoms. Worst of all, the FDA is considering emergency approval of experimental vaccines for children aged 5-11, whose risk of harm from COVID-19 is far outweighed by the risk posed by the vaccines7. Forcing one citizen to be vaccinated against his will, without the justification of protecting other citizens’ health and safety is nothing short of tyranny.
1 https://www.cnn.com/2021/10/05/asia/new-zealand-ardern-covid-zero-intl-hnk/index.html 2 https://www.kansascity.com/opinion/editorials/article241215076.html 3 https://www.medrxiv.org/content/10.1101/2021.05.18.21257385v2 4 https://www.news-medical.net/news/20211019/Waning-COVID-vaccine-efficacy-especially-against-reinfection.aspx 5 https://www.wsj.com/articles/covid-vaccine-natural-immunity-infection-israel-study-cdc-11632151556 6 https://vaersanalysis.info/2021/10/22/vaers-summary-for-covid-19-vaccines-through-10-15-2021/ 7 https://nymag.com/intelligencer/2021/07/the-kids-were-safe-from-covid-the-whole-time.html
The United States of America was founded to protect the inalienable rights of the individual, including the rights to Life, Liberty, and Property. Every one of those rights is undergirded by Bodily Sovereignty. Without upholding the right of Bodily Soverignty, what is there to prevent the government from consigning undesirable citizens to the GULAG, as the USSR did by the millions and China does today? Even Australia, once considered a free country, is building concentration camps for COVID quarantine8. It is the duty of American Government at all levels to protect citizens’ bodily sovereignty.
Lockdowns, Mask Mandates, and Vaccine Mandates all constitute government overreach. It is the duty of the Kansas Legislature to enact laws blocking such tyranny to the fullest extent possible under the Federal and State constitutions. Please stand up for the fundamental inalienable rights of Kansans.
Sincerely,
David Morgan
8 https://townhall.com/tipsheet/mattvespa/2021/08/26/australia-has-begun-building-covid-concentration-camps-n2594763
TO: Chairman Erickson and committee members FROM: Mark & Lynn Mowrey, 1411 N 3rd St E, Louisburg, KS 66053, 913-280-0720 DATE: October 27, 2021 RE: WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates We are vehemently opposed to the COVID19 Mandates being imposed in Kansas and are grateful for the opportunity to express this to your committee. We both had COVID in November of 2020 and maintain high levels of natural immunity, which according to many credible scientific studies, is up to 20% more effective than the vaccine could ever deliver. The company I work for in Olathe has requested information regarding my vaccination status. I have chosen not to answer this, as I see this as a violation of my HIPPA rights. This company has paid a bonus to employees that chose to take the vaccine, however that incentive has lapsed, and I fear their next tactic will be to impose proof of vax or be fired. This would be a violation of my First Amendment rights and should be illegal. We are urging your committee to take whatever steps necessary so that we, and all citizens in Kansas, can be assured of the freedom to make our own choices regarding healthcare matters. Mm/Lm
10/27/2021
Andrea Mukhija
RE: Written testimony to stop government overreach and COVID-19 mandates
Dear Chairman Erickson and Committee Members -
I would like to express my wholehearted support AGAINST government overreach and COVID-19
mandates, including vaccine requirements, mask mandates, and business / school shutdowns.
My position can be summarized simply:
“Healthcare is not (and never can be) one-size-fits-all. Therefore, health works
best when managed by the individual, not the collective.”
We all have varying…
• Genetics
• Health histories
• Diets
• Lifestyles
• Sensitivities
• Tolerances
• …the list goes on
Therefore, we simply CANNOT universally mandate our way to good health.
For me, the risk of dying from or being permanently injured by COVID is SIGNIFICANTLY less than
dying or being permanently injured by a mask or vaccine. Why?
• I have elevated heart and blood markers that increase my risk of heart attack or stroke. They
also impede my ability to properly oxygenate my blood / body. Therefore, masks make me
lightheaded and increase my risk of having a heart-related adverse event.
• I have quadruple MTHFR gene mutations that inhibit my body’s ability to detox vaccine
ingredients. (Vaccines require adjuvants and other ingredients to hyper-stimulate the body
to produce an immune response. Some people can more safely detox these ingredients after
they have done their job, I cannot). **Yet I STILL cannot obtain a medical vaccine
exemption.
• I have strong evidence to suggest that my left-sided thyroid and kidney conditions were
caused by my childhood Polio vaccine. I was then further injured by the aborted fetal cell-
laden chicken pox vaccine. However, these injuries were not recognized when I was a child
or put in my medical chart. Therefore, I cannot obtain a medical exemption today. In my
opinion, this is a GROSSLY UNDERSTATED PROBLEM with the vaccine program - many vaccine
reactions remain undetected for months, years, or even decades, and therefore never
connected.
I lived most of my life with cascading health issues caused by the pharmaceutical industry’s “safe
and effective” products. The mainstream medical community offered me no help, except to put me
on an ever-increasing list of lifelong medications that only created secondary symptoms and
disease.
Thankfully, I was introduced to a functional medicine doctor that specializes in Epigenetics. He
turned my health (and my life) completely around. He reversed decades-old chronic disease in my
body. I no longer take even a single medication.
The downside: those alternative treatments came with a huge personal financial burden. Because
of the pharmaceutical companies’ stronghold on our country, natural healthcare providers are
suppressed and not covered by insurance. For me to be healed of my pharma-caused chronic
diseases, I had to pay out of pocket.
Meanwhile, vaccine makers are laughing all the way to the bank with their
record-level vaccine profits, lack of liability for injury, and secondary profits
from selling medications to treat the very conditions caused by their vaccines.
This is unacceptable. If vaccine makers and administrators are exempt from liability,
then we all should also be exempt from their products.
In short: health belongs in the hands of the individual and family, NOT the government,
school, or employer. Vaccines, masks, and other medical interventions should be OPT IN
based on personal choice and consideration, not OPT OUT due to universal mandates.
I thank you for your time and I sincerely hope this committee will act to stop health-related
mandates. If not, we may be taking our family and multiple businesses to a more health freedom-
loving state.
Most sincerely,
Andrea Mukhija
Dr. Joseph Myers Professor of Science and Math October 26, 2021
Vaccine Mandates Make No Sense Science is against mandating the current COVID-19 vaccines.
Thank you very much for your scientific opposition to vaccine mandates in Kansas.
Before I continue, let me say I have no opposition to vaccines in general. I would even be
willing to help out as a volunteer to aid in the future development of vaccines. However, my
conscience will not let me stay silent about the shockingly insane and utterly non-scientific
current vaccine mandates.
Political pressure is in favor of these mandates. However, there is no scientific evidence that
they have helped at all.
All the real scientific evidence points to a dismal failure of these rapidly-developed
emergency vaccines. Despite many months of false advertising of 90-99% efficacy, the real
efficacy rates, even those of the "gold-standard" vaccines like the Pfizer vaccine, have fallen to a
mere 39-45% of fully vaccinated people who will successfully experience an asymptomatic
reaction upon exposure. This has no statistical difference from the pre-existing immunity rate of
those within the general population who are already asymptomatic to covid, which is within this
interval.
Moreover, scientific study supports the hypothesis that the only real driver of herd
immunity and lessening spread of the disease is natural immunity of those who have had it
according to mathematical logistic growth model of disease distribution. According to the largest
study in the world, it is well-known now that natural immunity is 27 times more effective than
being fully-vaccinated with any of the vaccines alone.
Vaccines are not immune systems. Vaccines are merely an immunological mechanism for
stimulating the immune system. So-called "immunity" from a vaccine is in reality immunity
provided by the immune system as a result of the vaccine's attempt to stimulate some of the effect
KS LEGISLATURE TESTIMONY 1
of natural immunity. The idea that a vaccine can magically provide immunity greater than the
natural immunity which it is trying to stimulate is absolutely ridiculous. This is the logical
equivalent to saying that an athlete can pick themselves up off the ground by their own
bootstraps and lift themselves into the sky if they only become strong enough.
The danger of the vaccines is also shocking. A co-worker of mine almost died from the
"vaccine." One of the side effects was joints so swollen that he could not even turn a door knob.
The scope and duration of the vaccine's massive detrimental effects on my co-worker were little
different from being placed into a month-long coma. A childhood friend did die from it as well as
two other family friends who died from the vaccine. Our family doctor had a patient receive the
vaccine who died within 30 minutes from an adverse reaction in the doctor's office. I personally
know of eight deaths near my family from the vaccine as well as four more deaths from
COVID-19 in fully vaccinated individuals. In fact, out of many whom I know who have been
fully vaccinated, only one person did not contract a COVID-19 infection upon exposure for the
first time to COVID-19 after being fully vaccinated.
To any scientifically-minded person, this would be more than enough evidence to show that
we need to develop new and better vaccines, not to continue using the failed experimental first-
generation vaccines that were developed more than 12 months ago. Why are we still using a beta
version of a "vaccine" after so many months instead of spending our efforts to develop better
ones? That is the question that a real scientist would be asking.
Yet the debate that rages on is not about science at all. If it were about science, the medical
world would be rushing to develop second-generation vaccine, a third-generation vaccine, etc.
They would be iteratively improving vaccines based on the scientific method using feedback from
both the success and failures of each prior attempt.
Yet is this scientific approach happening?
Not at all.
A real vaccine carefully developed over 10-30 years of time with an eye to both short-term
efficacy and long-term effects would be supported by scientists such as myself, but these shots are
at best a "rough draft" and not credible vaccines at all. Calling something that didn't even exist 18
months ago a "vaccine" is an insult to the true meaning of science and medicine.
There is no impartial scientific discussion fostered by our national government about
improving the vaccine.
KS LEGISLATURE TESTIMONY 2
There is only political discussion about mandating the vaccine.
You can see this absurd and non-scientific political nonsense every day.
And sadly, some scientists are selling their souls for funding by a government who has gone
off the deep end, trying to cling to the false idea that the vaccines are effective, when they are
not, just as the Emperor tried to cling to the false reality of his clothes in the famous fairy tale of
The Emperor's New Clothes.
Please perform your sacred and scientific duty as our elected Kansas officials, and act
immediately to ban and forbid all public and private vaccine mandates in Kansas except for
those vaccines supported by at least 30 years of long-term safety data and fully approved and
endorsed by both local and state medical authorities in Kansas.
Sincerely,
Dr. Joseph Myers
KS LEGISLATURE TESTIMONY 3

Written testimony in support of vaccines
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
I fully support the Covid-19 vaccines and the directives requiring masks when indoors. Ourcountry has seen plagues and pandemics before and have survived them by adoptingcommon actions to prevent the spread of the disease. Job #1 for any government is to keepits population safe. Any individual who claims they have the "right" to spread the disease anddeath to children and elders by refusing the vaccines or defying mask mandates has misreadthe Constitution.
--Linda Mary Neal, Esq.
"We are in a battle for the soul of this nation. And in this moment, we all have a responsibility to declare with conviction that hatred and bigotry and white supremacy have no place in America. We will give hate no safe harbor. "
The Missouri Bar Disciplinary Counsel requires all Missouri attorneys to notify all recipients of email that (1) email communication is not a secure method of communication; (2) any email that is sent to you or by you may be copied and held by various computers it passes through as it goes from me to you or vice versa; (3) and persons not participating in our communication may intercept our communication by improperly accessing you computer or my computer or even some computer unconnected to either of us which the email passed through. I am communicating to you via email because you have consented to receive communications via this medium. If you change your mind and want future communications to be sent in a different fashion, please let me know at once.
WRITTEN Testimony to STOP Goverment Overreach COVID-19 Mandates
Written correspondence only, will not be able to attend in person.
TO: Chairman Erickson and committee Members
I am adamantly opposed to Government Mandates for the following reasons:
Wed, Oct 27, 2021 at 11 :12 AM
1. Religious beliefs. No difference between the Communist in China harvesting organs from disadents, and Americainsharvesting cell lines from "almost newborns." This blood will not be on my hands. This is purley Demonic / Evil. Directlybenefiting from this innocent life is mortal sin.2. Unprecedented and intentional deception on the part of federal officials that we have traditionally believed. At presenttime there are no FDA approved COVID-19 vaccines available to US citizens. "Pfizer lnc/BioNTech which has beennamed Comirnaty" was approved but not available. All available vaccines remain under the legal status of EmergencyUse Authorization.3. Government overreach is a friendly politically correct term. Be concise, the mandates are unlawful andunconstitutional.4. Traditionally, Medical science has developed therapeutics prior to vaccines. It is my understanding that the US hadstockpiled therapeutics for just this type of pandemic. That these therapeutics are beneficial and available to members ofthe Federal government, and that over 200 have taken advantage of them. These same therapeutics are almostimpossible for citizens to receive. Even if a doctor is found that will prescribe them, the pharmacy probably won't fill them.5. Many respected sources have desperately tried to penetrate mainstream news (sponsored by Pfizer) with data/scienceshowing the benefits of naturally occurring antibodies within those who have had and recovered from said COVID. Is thisignorance, or just part of the deception mentioned in bullet 2 ?6. Despite all the reported efficacy rates, why a booster, and the admission that boosters may be needed well into thefuture?
ROBERT NEWMAN

WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Dear Chairman Erickson and committee members.
I am against the government mandates for the COVID 19 vaccine mandates. I have had COVID. I continue to test high on my antibodies even being11 months out from my negative COVID test after only being symptomatic for 2 days with a positive test. I am most concerned for these mandatesbecause they do not acknowledge the fact that I have antibodies already, and do not need the vaccine. This is very obviously about control and moneyand the majority of us can see that. Know that if these vaccine mandates go into effect, it doesn’t stop there. America will be at risk of loosing herheart and soul of who she really is. This will no longer be a free country but a country enslaved to the elite on its way to socialism. Stop thesemandates. We want the whole truth.
Sincerely,Dr. Addison Nichols, DPT
To: Chairman Erikson and the Committee on Government Overreach and Impact
of Covid Mandates
I am against government Covid mandates of all kinds, especially covid shot mandates.
I also represent the other 4 voting members of my family who hold the same
perspective.
Mandates from government officials, even though they come through the workplace,
requiring the people of Kansas and the united States to get an injection put into their
body is illegal, unlawful, and unconstitutional. Citizens in this country have liberty given
by God, and protected in the Constitution which cannot be infringed upon. As the
Kansas Constitution says: § 1. Equal rights. All men are possessed of equal and inalienable natural
rights, among which are life, liberty, and the pursuit of happiness.
These rights apply to individuals, not businesses or corporations!
People who are sick enough to pass a virus stay home to recuperate. There is plenty
of evidence to show that people without symptoms of covid who test positive for the
virus, do not pass the virus to others. (see articles listed below)
As with other diseases, survivors of COVID-19 have acquired natural immunity,
which has long been known to be superior to an injected “immunity”, and
therefore do not endanger anyone else.
Those who choose to not get covid shots should not be required to participate
in a genetic manipulation product that has unknown long term effects. The
Nuremberg Code also exists to help protect people from such involuntary
experimentation.
“The “vaccinate or terminate” policy is no less wrong because [an] employer is a private
company (meaning, not run by government). The reason is because [a] private employer would
not have done this BUT FOR the government coercing them to. The government can’t do
something THROUGH a private actor that it would be illegal to do directly. See, e.g.,
Hammerhead Enterprises, Inc. v. Brezenoff, 707 F. 2d 33 (2d. Cir. 1983) (“Where comments of a
government official can reasonably be interpreted as intimating that some form of punishment
or adverse regulatory action will follow the failure to accede to the official’s request, a valid
claim can be stated.”)”.(Coffee and Covid, Monday, October 11, 2021)
When government health departments are asked about the long term efficacy of
the covid shots – they don’t know. When asked about the long term efficacy of
acquired immunity – they don’t know. When asked about long term effects of
an experimental “vaccine” that injects foreign genetic material into your body –
they don’t know.
The number of breakout deaths from the covid shots far surpass any other
vaccine or medication in history. Typically, a new medication is pulled with just
a couple of dozen deaths. But there are thousands of deaths associated with
this “vaccine”. There is also increasing evidence that the covid shots are losing
efficacy faster than expected, and people who are fully vaccinated are still
capable of spreading the disease.
Covid mandates have wrecked havoc in many households and caused much
economic distress.
The mandates must stop! Kansas legislators must stand for the people and
against overreach of government officials! Do not allow those in power to take
away our liberties!
I have attached samples of articles that I found to be interesting. I am
completely aware that anyone can find articles that will discount my approach,
but I believe many of those articles, and people, are focused on behavioral
science rather than medical science.
Thank you for your attention to this matter!
Submitted by Linnea Nicholson
Written testimony only
Desomond Sutton, MD, et al., “Correspondence: Universal Screening for SARS-CoV-2 in Women
Admitted for Delivery,” New England Journal of Medicine 382 (April 13, 2020): 2163-64,
https://www.nejm.org/doi/full/10.1056/NEJMc2009316.
Travis P. Baggett et al., “COVID-19 Outbreak at a Large Homeless Shelter in Boston: Implications for
Universal Testing,” medRxiv preprint, April 15, 2020, https://doiorg/10.1101/2020.04.12.20059618.
Shiyi Cao et al., “Post-Lockdown SARS-CoV-2 Nucleic Acid Screening in Nearly Ten Million Residents of
Wuhan, China,” Nature Communications 11, article number 5917 (November 20, 2020),
https://www.nature.com/articles/s41467-020-19802-w.
Nuremburg Code: http://www.cirp.org/library/ethics/nuremberg/
U.S. Department of Health & Human Services
National Institute of Health
January 26, 2021
“Lasting immunity found after recovery from COVID-19”
https://www.nih.gov/news-events/nih-research-matters/lasting-immunity-found-after-recovery-covid-
19
Emory News Center
“COVID-19 survivors may possess wide-ranging resistance to the disease”
July 22, 2021
https://news.emory.edu/stories/2021/07/covid_survivors_resistance/index.html
Science Insider
“Having SARS-CoV-2 once confers much greater immunity than a vaccine-but vaccination remains vital”
August 26, 2021
https://www.science.org/content/article/having-sars-cov-2-once-confers-much-greater-immunity-
vaccine-vaccination-remains-vital
medRxiv – the PrePrint Server for Health Sciences
“Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus
breatkthrough infections”
August 24, 2021
https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1
Newsmax
“Vermont Sees Record COVID Cases Despite 80 percent Adult Full Vax Rate”
October 20, 2021
https://www.newsmax.com/newsfront/vermont-covid-record-infections/2021/10/20/id/1041357/
Washington University School of Medicine in St. Louis
“Good news: Mild COVID-19 induces lasting antibody protection”
May 24, 2021
https://medicine.wustl.edu/news/good-news-mild-covid-19-induces-lasting-antibody-protection/
From the Washington Post
“Natural immunity to covid is powerful. Policymakers seem afraid to say so.”
https://www.washingtonpost.com/outlook/2021/09/15/natural-immunity-vaccine-mandate/
September 15, 2021
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
To: Chairman Erickson and Committee Members
Please see the following testimony I have written to detail opposition to any governmentvaccine or health related mandates. This is an extremely important issue to me and myfamily as we have been tangibly impacted by these mandates, up to and includingemotional damage of my children and possible loss of my livelihood. The following is asummary of statements that illustrate the injustice behind these mandates, as well asshows the only logical and moral option for the question of "vaccine mandates" is to allowfor personal choice.
LogicEither the COVID "vaccines" work, or they do not.
Scenario #1: The vaccines work. Impact: Anyone who gets the vaccine is at no risk of contracting COVID. Outcome: Whoever believes they are at risk for serious health problems can bevaccinated and will be fully protected from those who are not. Logical Decision: Vaccinations are optional
Scenario #2: The vaccines do not work. Impact: Even if an individual is vaccinated, he still may contract or infect others withCOVID. Outcome: "Vaccinated" and unvaccinated people contract COVID and infect others Logical Decision: Vaccinations are optional
Scenario #3: The vaccines "kind of" workImpact: Even if an individual is vaccinated, he still may contract or infect others with
COVID. Depending on the situation (underlying health conditions, prior infections, age,etc.), vaccinated individuals may or may not see some reduction in symptoms orseverity. Outcome: Vaccinated and unvaccinated people contract COVID and infect others.Situation dependent impacts occur. Logical Decision: Due to individual variability impacts, a specific personal medicaldecision should be made. Vaccinations are optional.
Put another way, What we have done with COVID-19 mandates, to reference the greatphilosopher and saint Thomas Aquinas, is to subordinate the common good to theprivate good of individuals, thus making the common good an alien good for everyoneelse. We have done this by making a person’s individual life (a private good) an end, orfinal cause, to which every other good is ordered. The problem with this logic is that itleads directly to tyranny. In fact, for Aquinas, using law to direct people’s actions to theprivate good of individuals is the very definition of tyranny. Accordingly, everyone mustlose their human rights and access to the legitimate and necessary goods of humanflourishing so that a relatively small number of people won’t die. By this logic, no oneshould be allowed to drive either.
Data / RiskI searched extensively for data on the COVID survival rate for people my age. It turns outthat the CDC does not publish this data. (Msn.com: The age-specific "survival rates"listed in the post did not come from the CDC, however. CDC spokesperson JasmineReed told PolitiFact that the agency has not released any age-specific COVID-19survival rates, nor does it have mortality rates available). An obvious question is - whydoes the CDC not publish this data? Could it be that the survival rate does not fit the fearnarrative that is being pushed so prevalently across all media? All of the data I could findshows a very low overall hospitalization and death rate. In any case, there are manyextremely effective treatments for COVID that drastically reduce the risk ofhospitalization or death. Unfortunately, these treatments have been vilified because theydo not reinforce the money making and power reinforcing apparatus in the form of"vaccination mandates". The relatively low risk of COVID, combined with effectivetreatment options are important reasons why a mandate is unnecessary.
Additionally, it is a fact that many of the overall deaths related to COVID (world-wide andmost probably within KCS) had multiple factors involved in addition to COVID. Manymedical reports have stated that underlying factors, pre-existing health issues, age,weight, etc., all contribute to the relative risk of serious COVID concerns. This importantfact points in the direction that an appropriate response is not "one size fits all". It is alsoa fact that VAERS reporting from the CDC reports that through Sept 13, 2021, - 7,653people have died after taking the COVID shot, not to mention a very large number ofserious sickness and side effects. The site goes on to say it cannot make a definite linkbetween the shot and the death event. It's ironic this logic is used in the case of vaccinedeaths, but not when analysing whether there are other contributing factors to deathfrom/with COVID. The key point is every terrible situation that can be cited related to
death with COVID, or death with vaccine, has a lot of background information andhistory. I could personally relate a number of specific examples of people I know whohave been admitted into the hospital/ICU after the COVID injection. To state a generaldeath number without context or additional information for the purpose of persuasion byfear is unacceptable. Citing specific tragedies without context or backgroundcircumstances is not a legitimate reason to impose an injection mandate.
It is a fact that as the overall vaccination percentage of the U.S. population hasincreased over the past months, the percent positive cases have increased as well.Further, it is a fact that countries like India, during this same time period, have seenCOVID rates drop significantly (Reuters COVID 19 tracker), using alternative treatments.It is curious that the U.S. government administrative and medical bodies, in light of thiscontrast and superior results in India (and other countries), have not considered a moreeconomical and effective approach to reducing cases. It is also interesting that simplequestions like whether the vaccinations being pushed might be the cause (viral load) ofthe variant/cases are being buried. Or equally important, why are early treatment,FDA approved medications not being allowed to be filled by pharmacies? The success ofalternative treatment options is another reason why vaccine mandates do not makesense.
PoliticsI'm sure both sides of this issue can agree that the subject of vaccinations has beenpoliticized. There are a tremendous amount of instances on both sides of the issue thatcould be cited. The obvious example is President Biden's attempt to distract from theAfganistan situation by instituting an unconstitutional employer vaccine mandate.
Another more subtle instance of this tainted conversation is the former New York Timesreporter, Alex Berinsen. He was removed from twitter when he stated that the injections"do not stop infection or transmission... don't think about it as a vaccine". Although thisstatement resulted in his removal from Twitter, the CDC now agrees with him. The CDC,as of Sept 2021, has adjusted their past definition of a vaccine "producing immunity", toa substance that "stimulates the body’s immune response againstdiseases”. Consequently, mandating a therapeutic (not an immunity treatment), for asickness you do not have is unjust.
Faith / MoralityI am a Roman Catholic who follows the precepts of the Church to the best of my ability. Iregularly receive the sacraments of Reconciliation and Holy Eucharist. The concernsthat are present in light of my faith, with mandating an injection for COVID, are thetreatment's connection with aborted unborn children, and the church's teaching on theimmorality of coerced medical procedures.
Regarding the connection to aborted children, according to the "Vatican Letter From thePontifical Academy for Life": "some of the vaccines that are now ready to be approved or
applied use cell lines from voluntarily aborted fetuses in more phases of the process,while others use them in specific labratory tests". While some argue to lessen theculpability of these actions because the actions were taken from aborted baby "celllines" and not direct from the baby's cells, the fact remains these drugs would not beavailable for use without the aborted baby being involved.
Further, the Catholic church has repeatedly stated and taught that forced medicalprocedures are unjust and immoral. The Congregation for the Doctrine of the Faithstates, "practical reason makes evident that vaccination is not, as a rule, a moralobligation and that, therefore, it must be voluntary." Equally important,ArchBishop Joseph Naumann, to whose authority I submit myself as a member of hisCatholic Diocese, has published a lengthy statement on the vaccine mandates which inpart reads, "It is important that we reflect on the gravity of the violation involved incoercing a person to do something that he or she believes to be wrong. The SecondVatican Council, in its declaration "Dignitatis Humanae", asserted that both religious andcivil authorities have a duty to respect the consciences of persons as a civil right: "In allhis activity, man is bound to follow his conscience in order that he may come to God, theend and purpose of his life. It follows that he is not to be forced to act in a mannercontrary to his conscience."" ArchBishop Naumann goes on to say, "It is a fundamentalpillar of medical ethics that there should be free and informed consent and no coercionwhen deciding on a medical intervention."
One could argue that the government is not coercing individual employees of company'sto receive the treatment, as they could choose to forgo the shot and resign. However,this stance conflicts with the freedom and right to practice one's religion without fear ofretribution (loss of job). For these religious reasons, the only logical stance is to makethe injection optional.
Inclusion and AcceptanceVaccine mandates exclude employees of companies who cherish their right to medicalprivacy, and embrace preventative and aggressive COVID treatment options, vs aninjection, is not reflective of inclusion and acceptance. In fact, the aforementionedemployees are experiencing the opposite of inclusion, and potentially the loss of theirlivelihood.
My assessment of this situation is supported by the analysis and commentary ofMaximillian Forte, Professor of Anthropology at Concordia University - Montreal Canada,in his public statement of vaccine mandate non-compliance: "In particular, mandatoryvaccination pressures plainly and indisputably discriminate against employees who aremembers of particular religious and ethnic communities, in such a way and to such adegree that any claims to upholding “equity, diversity, and inclusivity” become completelyunravelled. Not sustaining this commitment in one area, and expecting it to be sustainedin other areas, is obviously neither credible nor tenable. Furthermore, the policy whichimposes such discrimination is in direct violation of a number of laws and human rightscodes, both here in Quebec and in the rest of Canada."
So from an "inclusive" perspective, a vaccine mandate is directly contrary to this value,and should be eliminated.
Thank you for your review of this information, and please let me know if I can answer any questions regarding the information on this email.
Respectfully,
Gil A. Niesen Jr.

Debra O’Leary-Kurtz
Chairman Erickson and Committee Members,
Subject: Written Testimony to STOP Government Overreach of the Covid-19 Mandates
I am very much opposed to this proposed mandate. I work in a facility that now requires me to have both of the Covid jabs or if I refuse, I now have to pay an extra $100 per month for my medical insurance. I have tested positive for Covid antibodies, have a strong immune system and I take the initiative to live a healthy lifestyle. I refuse to take these jabs due to there being too many unanswered questions regarding their ‘safety and effectiveness.’ For example, where are the long-range studies. Why are study participants who either were seriously injured, dropped out for various circumstances or even died not included in the final results of these trials. If I take these jabs and suffer serious consequences, who will pay for my medical treatments, therapies, ER visits, and chronic care if I am damaged in any way. These jabs are sanctioned under emergency use authorization and are not covered by our government as traditional vaccines are if one should suffer damages.
In consideration of my concerns, please vote “NO” to this Covid-19 mandate.
Regards,Debra O’Leary-Kurtz
Internal Use Only
Written Testimony to STOP Government Overreach COVID-19 Mandates
Mitchell Onnen
Written Testimony Only
Dear Chairman Erickson and Committee Members,
My name is Mitchell Onnen, and I am 100% AGAINST all Covid-19 Mandates. This has gone on long
enough. The government does not have the right to continuously impose these mandates on us. It
should be left up to an individual’s personal choice whether it be social distancing, masks, or
vaccinations. Forcing vaccinations on to individuals is completely immoral. Especially when not a single
person is being held liable for any adverse reactions to said vaccinations.
The vaccine mandate for federal contractors has put my job in jeopardy. I am lucky enough that my
employer has given me an accommodation for a religious exemption, but others have not been so lucky.
How long until a religious or medical exemption isn’t good enough? How long until the government
forces us to do something even worse.
I am tired of having my freedom of choice taken away from me. The government does not get to tell me
what to do. The government is there to do what we tell them. It stops here.
When schools were requiring children to wear masks to attend, I went along with it. I hated having my
children be forced to wear a mask all day. Especially for my son. He has asthma and already has issues
with breathing. When the school removed the requirement for masks I was happy for my children.
When there was discussions about forcing masks on the children again for the new school year I said I
had enough. I told my wife that if it was going to be a requirement again then we were removing them
and home schooling. I will do the same thing if a vaccine is required. Which I shouldn’t have to because
it should be stopped.
Enough is enough. We need to put an end to all Covid-19 mandates. We need to make it illegal to
require the covid-19 vaccination for employment or school. We need to stop the constant government
overreach into our daily lives.
27 October 2021
Dear Chairman Er ickson and Commit tee Members,
I am providing wr i t ten test imony to STOP government mandates of COVID-19 vaccines.
As a wel l - t ravel led, t ra ined and educated US Naval Off icer I have a const i tut ional duty to strongly advise against government mandates of COVID-19 vaccines.
As per OUR US Const i tut ion, that I and many others have fought (and died) to preserve, Americans have unal ienable and precious civ i l l ibert ies. Any government mandate regarding a vaccine, i .e. , personal heal th choice, i .e. , personal re l ig ious choice is in complete v io lat ion of the Const i tut ion, wrong and simply Un-American!
I have l ived in and spent many years working in countr ies that do not have a method to preserve personal c iv i l l ibert ies. The qual i ty of l i fe and abi l i ty for the people to thr ive is a f ract ion of what we have. I served our country in hopes that my daughter and al l of us can thr ive, not suf fer l ike much of the wor ld. I am speaking with a lot of f i rst -hand knowledge. We DO NOT want to al low our government to infr inge on our c iv i l l ibert ies. A government mandate of COVID-19 vaccines wi l l def in i te ly open the door for even more civ i l - l iberty infr ingement and a country run by the government, not run by the people. (NOT America)
I don’ t know i f you have l ived in a Communist country run by the government, I have…let me assure you i t is NOT what anyone wants. Even the pol i t ic ians suffer in Countr ies l ike th is. I f you al low these mandates, you are in v io lat ion of your oath and a t rai tor .
Kind Regards, USNR Lt. Char les Orr
October 27, 2021
RE: Covid-19 mandates
Chairman Erickson and Committee members,
This is my written testimony regarding the mandate; I regret I cannot do this in person.
I am absolutely AGAINST government mandates of Covid-19 vaccines!
I personally had a positive Covid test last February. As a business owner with one parttime employee who works one day a week, I had no option but to close my business for two weeks. My husband had to quarantine for three weeks. I was fortunate to not be very sick, so was able to work in my shop during my quarantine period. My husband is also self-employed, so was not terribly affected by his quarantine. We were lucky.
A year prior to my positive test, when our community had its first positive case, our local clinic evaluated me on the front lawn of said clinic because I had allergy symptoms. Cars drove by looking at me while the provider was in his hazmat gear. HIPAA flew out the window that day. HIPAA has been violated on many levels during this pandemic and it’s wrong.
I have no children in school and my elderly parents are deceased and, frankly, I thank God for that. The criminality of locking down nursing homes and isolating residents like prisoners is beyond belief.
And now a vaccine mandate? This is absolutely government overreach and should be shut down at every turn.
If the majority of the people of the State of Kansas believe this, your decision has been made. You, sirs and madams, work for us.
Jeana Padgham
October 27, 2021
RE: Written testimony to STOP government overreach/Covid-19 mandates
Chairman Erickson and Committee Members,
I am absolutely AGAINST mandating the Covid-19 vaccine!
This past February my wife tested positive for Covid. As a business owner with only one parttime employee one day a week, she had to close her business for two weeks. She was fortunate that she was not too sick so was able to work alone at her shop while it was closed. As her spouse, I had to quarantine for three weeks. I’m a self-employed crop consultant and could work from home, but could not get out and visit my customers. Overall, we were lucky we weren’t more affected.
My wife was treated on the front lawn of the clinic with the provider in a hazmat suit the day our County had its first positive case – this was nearly a year prior to her positive test. Cars were driving by, people walking by – a HIPAA violation in so many ways.
We have no children in school and no parents in nursing homes, but I am quite frankly thankful that my in-laws passed away before Covid hit as both were in our local nursing home. The lockdowns of nursing homes and alienating of residents from loved ones and even other residents has been criminal.
I am not anti-vaccine, but mandating this vaccine is government overreach and needs to be STOPPED NOW! The people in this State have the ability to make their own choice and should have that. “My body, my choice”, right? Vaccinated people can still get Covid, can still transmit Covid, and can die from Covid.
Where does this end for our country if this is allowed to happen?
Michael Padgham
I OPPOSE vaccine mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Written testimony:I staunchly oppose vaccine mandates in Kansas! Please stand for our constitutional rights!My whole family had covid, my dad died. I get it, covid is real and it sucks. I am still against mandates. No one should have the right to tellme what to inject in my body. Bodily autonomy is an inherent right. My husband's company (he is in vaccine development) is trying to force the shot. Now he has to choose between a career he loves and hasbuilt for the last 15 years or his personal health and ability to provide for his family. That is just ridiculous.My vaccine status has no effect on you. Freedom is at stake.Where there is risk, there must be choice.We have to stop this before it is even more out of control.Emily Paton
Written Testimony to STOP Government overreach COVID-19mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Dear Chairman Erickson and esteemed Committee Members,
Please consider the following written testimony AGAINST COVID-19 vaccine mandates. I urge you to put an end to all government mandates concerning COVID-19 vaccines, and to legislatively intervene to prevent private business from including them as conditions of employment.
I am personally facing the termination of my employment if I do not meet the following conditions: 1- Attest that I am fully vaccinated, and 2- provide documented proof of my vaccine status. The latter requirement is being asked for as a copy of a vaccine card that the company will keep on record, and out of an employee's control. I work in the healthcare sciences, and the ubiquity of these mandates means that I may not only lose this job, but also my entire career.These requirements force me to choose between providing for my family, and retaining the ability to make my own personal health care choices. Not only do the mandates constitute an overreach of a government's or employer's authority, but they also violate the sovereign freedoms that I am granted by the constitution, namely the right to life and religious freedom. While there may be some benefit to the vaccines, there is also some risk; where any risk exists, there must also be a choice.
As a citizen of the State of Kansas and the United States of America, I humbly request that you preserve my human right to choose what goes into my body, and protect my ability to earn a living.
Thank you for your consideration,
--Michael Paton

The Federal Vaccine Mandate has implications upon even our most rural and remote Kansas communities. All across our state, many impacted employees are considering the future of their employment with universities, federal government contractors, and large employers. I believe this policy will have significant negative impact upon our communities and sets the stage for further encroachment of government overreach upon our American freedoms. If this mandated vaccine policy is truly born out of concern for management of COVID, then it could be more constructively handled by offering employees a choice of vaccination, weekly rapid testing, or proof of natural immunity. Legislation that provides employees a pathway to opt-out of vaccination is imperative to the health, livelihood, and freedom of choice to every Kansan.
I understand that many of us have differences on views about this issue of COVID management and/or how we each feel individually about the vaccine. Regardless, as Americans we must come together and take a stand to help defend one another’s rights and freedoms to have a choice on this issue.
Respectfully,
Susan Penka
Chairman Erickson and committee members:
My name is Amanda Perron. I reside in Topeka, Kansas at 1829 SW Pembroke Lane. My
telephone number is (785) 806-1164. I am AGAINST government mandates of COVID-19 vaccines. Please
be advised this is my written testimony. I am a Registered Nurse licensed here in the state of Kansas.
Throughout the past 20 months, I have been on the frontline working directly with patients diagnosed
with COVID-19. We have worked with limited PPE, limited staff, long hours, and even at times looked
down on by the public as if we were ridden with disease. We have risked our lives for the public and
have even put our patients and careers before our own families. Now, many of us are faced with losing
our jobs just for making our own private health care decisions.
The very foundation of a nurse’s education is built on the principle that every person has the
right to informed consent and bodily autonomy. We do not discriminate or put our own values and
beliefs before our patients- even if the patient’s choices are causing more harm or result in death; even
if we do not understand or agree with their choices. That is the right of the patient. As a nurse, we can
educate and encourage them to make different choices and live healthier lifestyles, but it is up to them
and them alone to make those choices and I as the nurse must respect those decisions. I cannot stand
for any entity, person, or government that tries to take those liberties away. It goes against the very
core values of nursing. It goes against the core values American’s, as free people, have built our country
on. Vaccine mandates go against our basic liberties as human beings. No pharmaceutical product,
including vaccinations, are without risk. Where there is a risk, there must be a choice. I am not anti-
vaccine. I am pro-choice, pro-informed consent, and pro-medical freedom. I am a registered nurse
fighting for YOU to have a choice. Health care decisions are private and should be kept in confidence
between the patient and doctor.
Respectfully,
Amanda Perron, RN
October 27, 2021
Dear Senators,
Busy physicians too often rely blindly on our regulatory agencies sometimes to our patient’s detriment. In
2004, Dr. David Graham, senior drug safety FDA investigator described the Vioxx disaster as
“unparalleled in the history of the United States” and that it “constituted an unprecedented failure of the
nation’s system of drug approval and oversight.” The medical journal Lancet documented that Vioxx
increased a person’s risk of coronary artery disease by thirty – four percent. There are similar stories
concerning vaccines. In the 1960’s a RSV vaccine for children, despite being studied in animals,
enhanced the severity of the illness and was discontinued. In July 2016, the WHO announced their
recommendations for vaccinations against Dengue Fever in children ages 9-16 years of age which was
abruptly ended in November of 2017 when Sanofi admitted that the vaccine increased the risk of
hospitalization and cytoplasmic leakage syndrome in children who had no prior exposure to the virus due
to antibody dependent enhancement.
I have been personally shocked to learn that my own medical colleagues, including my children’s own
pediatrician were unaware of the Vaccine Adverse Event Reporting System (VAERS) yet they still
recommend the Covid vaccine to patients. Physicians are required to report any vaccine injury to this
system which then informs the FDA, the medical community and the public on how best to make informed
decisions about vaccinations. To date, the Covid vaccine has been associated with 7,848 deaths and
612,125 adverse events more than the total number of reports from all vaccines ever administered in the
U.S. over the last two plus decades. A study by Harvard Pilgrim Healthcare in 2009 of the VAERS
system found that the data entered was less than 1% of the actual post-vaccination side effects. An
urgent upgrade was recommended which to date has not been done. Jessica Rose, PhD, MSc, BSc, is
currently analyzing the VAERS database and has reported that there is a significant back log of entering
the data into the system which has added to even more under- reporting.
The foundation of medical decision making is true informed consent based on accurate, uncensored
medical information. Never in my 30-year medical career have a felt that medical information has been
censored until NOW!!! I am involved in numerous zoom meetings and email groups with medical
professionals literally all over the world and all medical professionals are seeing the limitation of medical
information being censored along with medical debate. This ranges from fraudulent data being published
in highly respected, premiere, peer-reviewed journals such as the New England Journal of Medicine and
the Lancet, to the shameful misinformation spread about the “toxicity” of proven safe, repurposed drugs
such as Hydroxychloroquine and Ivermectin taken by billions of people often available over the counter in
third world countries. All the way to the vilification of renowned, medical professions for simply
intellectually engaging in discussion about treatment of this new, novel disease COVID-19 and the
worldwide distribution of a new, novel vaccine. I have to ask you, do you personally want your doctor to
have limited access to academic, rigorous debate when they are helping you determine decisions about
the health of your family and community? That is exactly what has happened and I would strongly urge
you educate yourself about the Trusted New Initiative which includes the BBC, the EBU, Facebook,
Financial Times, First Draft, Google, The Hindu, The Wall Street Journal, Twitter, Microsoft, Associated
Press, Agence France-Presse, Reuters, CBC/Radio Canada, and the New York Times which engaged in
Project Origin with a mandate to identify non-authorized news stories and to set methods for
authentication for news and information. Who makes the decision about what medical news is provided to
the public and why have we heard only one narrative about Covid solutions:
1. “We have no early treatment to offer you.” This is medical neglect.
2. “When you get critical ill come to the hospital and we will try to save you.” This is medical futility.
3. “The only answer is a vaccine.” This is medical reductionism.
4. “The vaccine only has benefits and no risk.” This is medical “white washing”.
Does the vaccine only have benefits with no risk? Steven Hatfill, PhD, virologist who worked at the U. S.
Army Medical Research Institute of Infections Disease wrote a scientific summary of the risks of the
vaccine with medical journal references on July 28,2021. The vaccine utilizes messenger RNA (mRNA) to
ask your own cells to produce a protein which is not a concern but this protein has now been shown to be
pathogenic, meaning harmful to cells especially endothelial cells (contain ACE 2 receptors) which line all
the blood vessels of the body. The spike protein targets the ACE 2 receptor and when purified spike
protein was injected into a mouse there was widespread spike protein deposition demonstrated in brain
capillaries leading to swelling of tissue and microthrombi. ACE2 receptors are also present on platelets
and in COVID -19 infected patients they can present with low platelets with an additional pro-thrombotic
state leading to bleeding and clotting – stokes, myocardial infarctions, pulmonary embolisms etc. When
looking at the list of adverse effects from the vaccine it appears that this same scenario is present. For
example, numerous women are presenting with significant menstrual irregularities, rare cerebral venous
thrombosis and Thrombosis with Thrombocytopenia Syndrome. Based on testimony to the VRBPAC on
October 26, 2021 in regards to EUA approval for the Covid vaccine in children ages 5-11 years, Steven
Kirsh, Executive Director of COVID-19 Early Treatment Fund presented data from the VAERS system
showing a 570 times factor increase in pulmonary embolism, a 360 times factor increase in thrombosis,
an 80 times factor increase in stroke, and a 65 times factor increase in deep vein thrombosis in those
vaccinated. The spike protein can also attach to other organs that contain high concentrations of ACE 2
receptors such as the heart. Myocarditis can be seen in COVID -19 infection but the vaccine has led to
similar findings resulting in an FDA warning for Pfizer and Moderna vaccine for myocarditis especially in
young males under 30 years of age.
Currently as a medical professional despite spending over 100 hours invested in learning as much as I
can about COVID- 19, to date I have countless questions. I can not image how the public feels. Actually, I
can speak to that feeling in my community. They have lost all trust and confidence in my profession. My
questions are as follows:
1. The most obvious question is why are we mandating a vaccine that doesn’t address any of the
public health arguments for a mandated vaccine? We know that individuals that are fully
vaccinated still get infected, have high viral loads in the nose similar to the unvaccinated, are less
likely to get symptomatic therefore less likely to self-quarantine and can still spread the virus to
others. There have been several outbreaks in hospital settings even with fully vaccinated health
care workers, with masking where disease has spread in these care settings. Lastly, there is
worldwide date showing that countries with the highest vaccination rates continue to have high
rates of Covid infection. Correspondence in the European Journal of Epidemiology, September
30, 2021 entitled “Increases in COVID-19 are unrelated to levels of vaccination across 68
countries and 2947 counties in the United States”. It was pointed out that the Ministry of Health in
Israel showed the effectiveness of the Pfizer vaccine against preventing infection was reported to
be 39%. They also pointed out that the CDC had reported an increase from 0.01% to 9% and 0
to 15% (between January to May 2021) in the rates of hospitalizations and deaths in the US. The
conclusion stated that the sole reliance on vaccination as a primary strategy to mitigate COVID -
19 and its adverse consequences needs to be re-examined.
(Pnina et al, Nosocomial outbreak caused by Delta in an Israeli hospital. Finland study by
Hetemaki. WI Department of Health, by Riemersma concludes that the viral load in vaccinated
and unvaccinated symptomatic patients are similar and there was a higher percent of
asymptomatic unvaccinated detected therefore they are less likely to know they are sick to
quarantine.)
2. Why are we mandating a vaccine for everyone instead of strategically giving a vaccine based on
risk stratification? COVID 19, according to Dr. John Ioannidis, Professor of Medicine,
Epidemiology and Population Health and Biomedical Data Science at Stanford University, stated
in April of 2020 in the the Santa Clara study that the infection fatality rate was much lower than
previously feared around 0.17%. In June of 2020 he published a meta- analysis of 23 studies
which pegged the infectious fatality rate around 0.26%. In June of 2021 he discusses the 10,000-
fold difference in fatality rate between children and the elderly which shows the strong risk
stratification for this disease which means it is lethal for a small segment of the population
largely sparing the majority of the population. You can actually see this risk factor ratio of 10,000-
fold as a gift because we clearly should know what to do with this disease.
3. Why are we insisting that natural immunity be ignored when we all know that having a disease
infers immunity? An anesthesiology colleague early on in the pandemic was seen as “bullet proof”
and pulled into every Covid case because he had had the disease but now his job is threatened
due to a mandated vaccine that is not indicated. See Article on Brownstone Institutes website
written by Paul Alexander PhD, that provides 91 articles supporting natural immunity.
4. Why are we asking pregnant women to be vaccinated? Pregnant women were not studied in the
vaccine trials. We never expose patients to vaccines or drugs that have not been studied in a trial
especially pregnant women with a developing fetus. We have medication pregnancy categories to
avoid fetal exposure. We ask women to abstain from alcohol, smoking and even artificial
sweeteners etc. and yet the Obstetrical Colleges are recommending the vaccine and
obstetricians are refusing to write medical exemptions. I know personally a radiology resident
who reach out to me for help in regards to this ridiculous risk being placed on her unborn baby.
5. Why are we mandating a vaccine in the military where the majority of those needing to be
vaccinated would meet the criteria for being at risk for myocarditis and where the majority are at
no risk of dying from Covid?
6. Why are we vaccinating children where there can be no risk reduction from a disease that causes
no mortality in healthy children and hence the vaccine can only offer risk to healthy children?
The vaccine mandates are misguided based on all the arguments above and I mentioned nothing about
the abuse of civil liberties this represents. My work place has mandated the vaccine, put a consent form
in place that releases them from all liability while OSHA rewrites their rules to also protect the employer
and not the employee by stating that “OSHA does not wish to have any appearance of discouraging
workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers
vaccination efforts. As a result, OSHA WILL NOT ENFORCE 29 CFR 1904’s recording requirement to
require any employers to record worker side effects from COVID -19 vaccination at least through May
2022. This is criminal and wrong. Additionally, the actual FDA approved vaccine, Comirnaty, will not be
available until 2022 and are not being utilized for the mandates and the BNT162b2 vaccine will be used
instead. I have confirmation of this. The employee again is thrown under the bus as the BNT162b2
vaccine still leaves the pharmaceutical company without any liability. The only federal coverage for the
employee is the Countermeasures Injury Compensation Act (CICP) which offers limited protection rather
then being covered under the National Vaccine Injury Compensation Plan that would cover you if the
actual FDA product, Comirnaty was available. The public is totally unaware of all of this.
Lastly, the health care industry has entered a moral crisis and a soon to be workforce crisis that already
exist but will be exacerbated. Physician and nursing shortages are rampant. I personally have waited 6
months to see a subspecialist. The mandates are demoralizing those who are staying and driving others
from health care all together. This is the word on the street. Our entire state will suffer the consequences
of what these mandates will do to health care in enumerable ways. My question is why are we doing this?
As the voice of the citizen and their representative, I insist that you put into place legislation immediately
that would:
1. Protect citizens against mandated COVID vaccines bases on my arguments above.
2. Put in place protections for all health care workers to share their profession opinion without
reprisal for the sake of all patients in the state of Kansas. I chose not to testify in person for this
very reason. A sad state of affairs. I know three colleagues currently being investigated by the
Kansas licensing board.
3. Limit the ability of all new vaccine products from being administered in pharmacies. Full informed
consent can only be provided by a physician.
4. Investigate whether the FDA approved vaccine product, Comirnaty is being made available for
the mandates in the state of Kansas and if not, administration must be stopped.
My profession has lost its way. We took an oath to place the safety of the patient above all else and to
“first do no harm”. We are first and foremost patient advocates. The COVID vaccines have significant
safety signals. My professional duty and oath are to make this information known to the public. This is
also the duty of our public health agencies to investigate thoroughly these safety signals. It is the duty of
the media to allow medical experts to discuss and debate the facts. And it is your duty, Senator to listen
well with an open mind and protect the citizens of this great state.
Thank you for your effort on behave of the health of the citizens of the state of Kansas
Gayln Perry
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates From: Le Peters
October 27, 2021
Page 1 of 2
Subject: WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates This is Written Testimony only.
TO: Chairman Ericson and committee members.
I am AGAINST government mandates of GOVID-19 vaccines.
I am being affected, by COVID-19 Vaccine Mandates in the following way:
1. My job is being threatened that I need to be vaccinated.
2. My health is being threatened by a vaccine that will COMPRIMISE and WEAKEN
MY IMMUNE SYSTEM. There are many studies, including an Israeli study that
concludes: an individual’s immune system is 20 times better than the vaccine at
fighting COVID-19 after contracting COVID-19.
3. My Civil and Constitutional Rights are threatened by Government that DEMANDs
compliance to a Vaccine Mandate without accepting Religious or Medical
Exemptions. This is Unconstitutional Government Overreach.
I am a 69 year old male in average health.
I contracted COVID-19 in late 2019 on a trip. I recovered after 2 weeks with mild
symptoms. When the lockdown started, I worked to improve my immune system with
exercise, outside sunshine and Vitamins C, D3 and Zinc. Before 2020 I was sick twice
a year for 7 days with influenzas that usually settles in my chest requiring antibiotics to
recover. However, I have not been sick in the past 2 years since I improved my immune
system after contracting COVID-19.
I have been in contact with others during the past 2 years that have had COVID-19, but
I have NEVER again contracted COVID-19. I never use hand sanitizer and chew my
finger nails daily. Therefore, I am ingesting germs from surfaces at work, Dillion’s
grocery store, restaurants and from my travels out of state, into my mouth. Yet I have
not contracted COVID-19 again.
I therefore have a natural healthy immunity and DO NOT NEED THE COVID-19
VACCINE.
It would be extremely UNHEALTHY and UNWISE for me to take an EXPERIMENTAL
vaccine that will COMPRIMISE and WEAKEN MY IMMUNE SYSTEM, when I worked
hard to strengthen and maintain a HEALTHY immune system.
The local media and national media is declaring that all UNVACCINATED people
are infecting the vaccinated. THIS IS a TOTAL LIE. I am living proof.
It is terrifying to me that our government officials: President Biden and Governor Kelly
disregard science and trample our individual liberty to DEMAND everyone be
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates From: Le Peters Wichita, KS
October 27, 2021
Page 2 of 2
vaccinated REGARDLESS of my individual health and my Civil and Constitutional
RIGHTs. This is only their political bias for their political agenda.
TAKE the political agenda out of this issue. Get back to the Science. A COVID-19
vaccine is NOT necessary it is only enrichening Big Pharma. We must treat the
patient immediately with known treatments that are ignored by the CDC.
(See the FLCCC alliance article “Review of the Emerging Evidence Demonstrating the
Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19.)
It is your DUTY to STOP government Overreach which DEMANDS individuals comply
with COVID-19 vaccine mandates.
Thank you.
Respectfully,
L.
Liz Peters October 27, 2021
Page 1 of 1
Subject: WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates This is Written Testimony only.
TO: Chairman Ericson and committee members.
I am AGAINST government mandates of GOVID-19 vaccines.
To make myself clear from the very beginning, I am adamantly against Government
mandates for COVID-19 vaccine mandates.
I have been an RN for 35 years. The majority of my career was in a major teaching
University Hospital where drug trials were a routine occurrence. I not only administered
the trial medications to patients, but also took part in being a test subject. I saw first
hand how long it took, even a drug that exceeded expectations, to be approved for
routine administration.
At the beginning of COVID-19, I learned that the FDA was going to skip vital steps in
drug testing protocol. This set off major alarm bells for me. How can the FDA who
always in the past was so adamant in insuring patient safety, now does not care at all.
I also wondered why the immediate focus of the drug companies was to develop a
vaccine and not find a treatment that could be giving to patents at first diagnose to keep
them out of the hospital. Did the medical community every send a woman home without
treatment when breast cancer is first diagnosed with further instructions to wait until the
tumor is protruding from her breast, then we will start treatment? Absolutely NOT! So
why do we treat COVID-19 patients in a disposable manner and not provide treatments
immediately! There are known treatments which have been proven around the world in
India that is irradicating COVID-19, therefore a vaccine is not needed.
When the facts about the Nazi’s doing medical experiments on concentration camp
prisoners was revealed. The world was abhorred and the Nuremberg Code was
created and ratified by the United States in 1947. So why are American’s being
FORCED to take this experimental vaccine in direct violation of the Nuremberg Code?
This is an OUTRAGE and ILLEGAL Overreach of Government.
We need to stand for individuals rights and freedom of choice or we become
INHUMANE and RUTHLESS as were the Nazi’s.
YOU MUST VOTE TO STOP GOVERNMENT OVERREACH AND MANDATES OF
COVID-19 MANDATES.
Respectfully,
L.

Written testimony to stop government overreach COVID 19 mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless you trust the sender and know the content is safe.
Written testimony to stop government overreach COVID-19 mandates. Do not let the mandates pass. Thank you. From Betty Pfannenstiel, Sent from my iPhone
Written testimony to STOP government overreach COVID 19mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
I am writing this letter today to protect my families liberties and freedoms given to us at birth under the Constitution of theUnited States of America. I am AGAINST the COVID 19 mandates in all forms; masks, vaccines, passports, quarantine and anyother form of isolation.
We the People have had enough. We are done letting the government control us. This is a gross overreach of your power asGOD is our protector, not the government.
I have watched numerous people have negative side effects from the mandates. Enough is enough. The science and medicalproof has been provided and yet the government still wants to take our God given unalienable rights away and I will nolonger sit by and let that happen. We are Americans and we live in the land of the free! Stop any and all mandates and letWe the People make choices without government control.
Lacy PfannenstielProud American ����
October 27, 2021
RE: Position Against Government Mandates of Covid-19 Vaccines
Dear Chairman Erickson and Committee Members:
I am writing today to voice my opposition to mandated vaccines, for Covid-19 or any other illness.
Covid-19 has been proven to have a 99% survival rate to those who are healthy without co-morbidities, and it is appalling that these so-called “vaccines”, which are actually mRNA gene therapy injections are being mandated in the Unites States. This is against federal and state law, and just plain wrong. The truth is that vaccines have side effects that are under-reported to VAERS, not to mention the outright twisting of data by the CDC by classifying any death within 14 days of the 2nd injection as an “unvaccinated death”. Anyone who has been paying attention during this pandemic can see the blatant political agenda and government overreach. This is destroying our country, our families and our livelihoods and it needs to STOP NOW.
Let’s also mention how the Cominarty injection that has been FDA-approved is not even available on the market, and that the only thing available is the injection with the Emergency Use Authorization. This is unethically deceptive and morally wrong!!!
My own family and friend group is filled with stories of vaccine injury. I myself had recurring ear infections as a baby, toddler and child, and looking back in my records, it was always 2 – 4 weeks following vaccine injections. My Grandma got brachial neuritis from the flu shot and suffered from nerve pain in her arms, shoulder and neck for more than 2 years. My cousin’s daughter suffered from Henoch-Schonlein Purpora for years; she is now 15 years old and has lost 40% of her kidney function. That condition is listed as a side effect of vaccine inserts of the MMR, flu & varicella vaccines. My adult cousin experienced terrible gastrointestinal damage following the Tdap vaccine in 2012 and is still recovering. My friend’s son was injured from his 4 month vaccines and experienced cry encephalitis following those injections, which was high-pitched screaming for 7 hours per day for months on end. There are real side effects from vaccines, and on a cumulative basis, the ingredients build up in the body and can cause many types of reactions over the course of time.
A question we need to ask is, to what extent is money from these pharmaceutical companies - companies that have been convicted of fraud for lying about the safety of their products - influencing the CDC’s vaccine recommendations? Most Americans are completely unaware that the CDC is a private, for-profit corporation with direct ties to pHARMa, an inherent conflict of interest, like the fox guarding the hen house.
Instead of using coercion and threats to lose employments and livelihood, let’s mandate that individuals are free to make their own informed medical choices, made between themselves and their physicians without bureaucratic coercion. Let’s provide true advice that the key to a healthy immune system is a healthy diet, exercise, vitamin D, stress-management and more. If you are human and uninfluenced financially by pHARMaceutical interests, something in your soul has to be telling you something isn’t right with any of this, and we are literally begging you for your support to do the right thing for Kansans and for Americans.
Sincerely,
Jacia Phillips
October 27, 2021
RE: Position Against Government Mandates of Covid-19 Vaccines
Dear Chairman Erickson and Committee Members:
I am writing today to voice my opposition to mandated vaccines, for Covid-19 or any other illness.
Covid-19 has been proven to have a 99% survival rate to those who are healthy without co-morbidities, and it is appalling that these so-called “vaccines”, which are actually mRNA gene therapy injections are being mandated in the Unites States. This is against federal and state law, and just plain wrong. The truth is that vaccines have side effects that are under-reported to VAERS, not to mention the outright twisting of data by the CDC by classifying any death within 14 days of the 2nd injection as an “unvaccinated death”. Anyone who has been paying attention during this pandemic can see the blatant political agenda and government overreach. This is destroying our country, our families and our livelihoods and it needs to STOP NOW.
Let’s also mention how the Cominarty injection that has been FDA-approved is not even available on the market, and that the only thing available is the injection with the Emergency Use Authorization. This is unethically deceptive and morally wrong!!!
A question we need to ask is, to what extent is money from these pharmaceutical companies - companies that have been convicted of fraud for lying about the safety of their products - influencing the CDC’s vaccine recommendations? Most Americans are completely unaware that the CDC is a private, for-profit corporation with direct ties to pHARMa, an inherent conflict of interest, like the fox guarding the hen house.
Instead of using coercion and threats to lose employments and livelihood, let’s mandate that individuals are free to make their own informed medical choices, made between themselves and their physicians without bureaucratic coercion. Let’s provide true advice that the key to a healthy immune system is a healthy diet, exercise, vitamin D, stress-management and more. If you are human and uninfluenced financially by pHARMaceutical interests, something in your soul has to be telling you something isn’t right with any of this, and we are literally begging you for your support to do the right thing for Kansans and for Americans.
Sincerely,
Michael Phillips
October 27, 2021
To Chairperson Erickson and committee:
My name is Tara Pridgett. I am a pediatrician and child advocate. I have practiced in Topeka for over 20
years. In April I opened a solo practice. I did this so that I could respect and honor the role of parents in
the healthcare decisions for their children. I believe in health freedom for all citizens including children. I
am opposed to masking children in school and at all. The use of masks (cloth or surgical) is ineffective in
preventing virus spread as attested right on the package. Masking causes physical harm like headaches,
dizziness, nasal congestion, nosebleeds, asthma flares, acne flares, etc. Masking causes psychological
harm like fear, anxiety, panic attacks, depression, low self-esteem, etc. Masking is causing
developmental harm like delayed speech acquisition, impaired hearing, impaired social interaction, etc.
These are all harms I have seen in my patients. Our children are involuntary participants in an
experiment. We have never masked their faces for 6-8 hours a day for months at a time. We don’t know
the long-term effects of doing this. There is no proven benefit of doing this. The idea of stopping the
spread and reducing the risk to others is not attainable by wearing masks. I am compelled to first do no
harm. Masking is harmful and I am opposed to it.
Additionally, I am not in favor of vaccinating children against Covid-19. The CDC data confirms that
children have a statistically zero chance (.00003) of death from Covid-19 infection. Based on data
submitted to the Vaccine Adverse Events Reporting System (VAERS), there are substantial health risks to
children from the vaccine including death, neurologic injuries and cardiovascular injuries. Furthermore,
the vaccines are failing to prevent infection. Each manufacturer has sought approval for booster doses
related to waning immunity. At this point, I have personally taken care of only one patient with an
adverse reaction to a Covid-19 vaccine, but I am concerned that I will be seeing more. It doesn’t make
sense to risk injury from a product that need not be given. In the practice of medicine, it is understood
that one size does not fit all. What may benefit one child can prove harmful to another. Likewise, good
medication stewardship means I don’t prescribe a medication to a child unless it is beneficial to the
health and recovery of that child. We should not be vaccinating kids in order to protect adults.
I am opposed to any entity mandating vaccination as a condition of employment, travel, entertainment
or any other regard. We as citizens of the United States have a right to bodily autonomy. We the citizens
get to choose what is best for us, not the government, not the employer, not the school.
Thank you for your time.
Sincerely,
Tara D. Pridgett, MD
Mandate/Written testimony
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Please vote against any attempt to mandate COVID-19 vaccinations in the state of Kansas. Every person needs to individuallymake the decision of whether or not to take the vaccination!
Elaine Ratzlaff
Sent from my iPhone
Mandate/A written testimony
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Please vote against any attempt to mandate COVID-19 vaccination in the state of Kansas. It is every person‘s right to makethat decision for themselves.
John Ratzlaff
Sent from my iPhone
Written Testimony to STOP Government Overreach COVID 19 Mandates:
Name: Jeremy Rauch Address: Phone:Date: October 25th, 2021
Hello Chairman Erickson, Vice Chairman Landwehr Committee Members,
My name is Jeremy Rauch, and I am employed by Airbus Americas in Wichita Kansas, and I am writing you to submit written testimony that I am strongly AGAINST the government mandating COVID 19 vaccinations.
On October 13 of this year, we were informed that Airbus would require full vaccination against COVID 19 by December 8th. The mandate is very wooden, either have the vaccine or be placed on a mandatory unpaid leave of absence until December 20th after which time if, an employee remains un-vaccinated they will be terminated. I have been employed by Airbus for 10 years, during which I have received good reviews, and yet, a vaccine mandate, NOT merit determines my continued employment. I find it hypocritical, that mercy is extended o employees who under-perform and are not terminated, and an un-lawful government mandate that is impressed upon employees against their will can be enforced gracelessly.
Furthermore – This over reach by the Federal Government represents a shift from individual liberty to forced conformity to the collective whole. No longer does an individual or family have full control over their medical decisions, but is forced to submit to the judgement of (in the case of Airbus) un-named individuals who will review our medical and religious reasons for refusing the vaccine mandate. The individuals making these determinations have no personal relationship with us (as does our doctor) and yet act as an authority in charge of deeming our reasons for refusing the vaccine valid or not.
This represents a dangerous precedence without any boundaries of restraint, and therefore, I feel, must be stopped.
I thank you and the committee for your service, taking the time to consider my comments and look forward to helping you further if required.
Sincerely,
Jeremy Rauch
Subject: Written testimony-Stop Government Overreach/ Covid-19 Mandates
Beth Regehr
Written Testimony Only (Buhler Bands march in state competition Saturday; unable to attend in person)
Chairman Erickson and Committee Members:
I am against government “mandates” and believe the current governor has suffocated our great state of Kansas.
Government has almost stopped the Heartbeat of America in the Heartland of Kansas.
As a math tutor, I have never seen such a large number of struggling students and poor performance; not a single one
has had more than minimal symptoms of the chaos called Covid. As a parent, I was frustrated that our college student
was cheated out of in-person labs, shadowing and internship opportunities due to the government “mandated”
shutdowns. Our school system has never seen such a shortage of staff, from teachers leaving, to bus drivers and kitchen
staff unwilling to work under current mandates. Teens have committed suicide. I am most disappointed in the false and
inadequate information being handed out by our Health department and medical institutions. Public school teachers
should never bully students into believing that vaccination with experimental drugs is the only way to get back to
normal. Homeschooling in Reno County tripled with parents unwilling to sacrifice their children to pharmaceutical
experimentation.
After surviving months of providing ‘pandemic’ hospital and clinical care, nurses in our rural community are leaving their
facilities to avoid mandated vaccination and administrative practices with inaccurate data reporting. Hospice patients
should never endure last days without family. Our Senior Saints have suffered depression and misery during the No-
Visitor policies implemented at our care facilities; people died alone due to cruel and inhumane mandates at the
insistence of the government. Families and friends have been cheated out of the opportunity to console people as they
were unable to properly bury and celebrate the lives of their deceased. All of whom died of pre-existing conditions and
unavailable care due to “mandates”. Our food banks are constantly short of items because so many low-income families
have chosen to live off of the failing Department of Labor dollars, and yet, struggle to put food on their tables.
“Mandated” business closures’ ‘laid off’ then terminated a friend who has yet to receive their earned unemployment
benefits due to failure of state staff, ID theft, and fraud. All of these issues, and more, due to “mandates” that failed to
curtail the transmission of a lab concocted virus. Praise God our church has gotten very creative in maintaining worship
through this chaos, but shame on our state representatives for thinking mandating limited gathering capacities would
stop an ever-mutating virus from migrating through like the sin that permeates this nation.
The mask was supposed to stop the spread; even your scientists know how false & misleading that is. The lockdown and
social gathering stranglehold was to slow the spread; but instead only caused loss of revenue and trust. The vaccine was
promoted as prevention but has been relabeled as minimizing severity. I have yet to read an ingredient and side effect
label that hasn’t been redacted or ‘updated’. Vaccine by definition is a substance used to stimulate the production of
antibodies and provide immunity against one or several diseases, not to minimize severity of symptoms. Natural
Immunity has been proven the most effective. Herd immunity has created the decline in documented cases, not the
mandates. Now the government wants to booster the inadequate, emergency-authorized vaccine they promoted as
salvation. When will the insanity provide the results the government advertised? Covid-19 is still floating in the winds of
Kansas, despite all the government attempts to control “it”.
God provided me with a healthy immune system that successfully conquered the C-19 in 72 hours; I should be
congratulated not deprived of my constitutional freedoms of religion, speech, peaceable assembly, and to petition this
misguided government of grievances. As a voting tax payer, I request for the state government to stop mandating
employers discriminate against their employees because of medical choices. Governing representatives of Kansas do
not have the right to mandate medical choices, employment options, or control financial security. I stand firm in the
belief that God is the utmost authority. I request you return power to the people and Divine Providence to the State
House of Kansas.
I believe Kansas should be relieved of the governments’ cunning “mandates” and allowed to return to their freedoms to
live life as was intended by the authors of our constitution. Resuscitation of our failing economy, our no-longer
respected health care system, and our exhausted education system is needed immediately. I request that our state
representatives get out of the health care business. Govern pharmaceutical liability. Govern transparency and open
meetings. Govern immigrants and refugees screebubg for disease as part of their documentation. Stop dictating based
upon special interest groups. Remove the barrage of commercials bullying the public into thinking more injections are
needed to boost the emergency vaccine, and start educating of side effects caused by injecting unsafe chemicals.
Government mandates are killing Kansas. Stop Government Overreach.
Thank you for your time.
RESTRICTED
Chairman Erickson and Committee Members,
This is my written testimony concerning COVID-19 vaccine mandates. I am strongly
against these vaccine mandates. It is not an issue of health but an issue of our civil rights. I am
not an anti-vaxxer and do believe that wonderful products come from scientific progress;
however, forcing people to inject ANYTHING into their body is a complete overreach of
government power.
If we do not have even the freedom to decide what goes into our own bodies then what
freedoms will we have left. It is truly a disappointment that some people are being forced to
decide whether to stand up for their principals or take the shot (even though fearful of side
effects) just so they can feed their families. Fortunately, I have been able to keep my job, but I
am still experiencing discrimination and segregation as a result of not being vaccinated. I am
unable to carry out with certain aspects of my job that fully vaccinated individuals are allowed to
do which, as a result hinders my work performance. It is appalling to me that state officials are
not standing up to protect the rights of their people.
I urge you to stand up for the rights and liberties of the people you are representing and
stop government overreach.
Annie Regier
10/27/2021
Aaron Reimer
Jerrica Reimer
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates
Dear Chairman Erickson and committee members,
Thank you for the hard work you put forth for our great state every day. As proud
Americans and Kansas loving citizens, we wanted to state that we are against government
mandates of COVID-19 vaccines. We believe any medical decisions regarding our health
should be made in collaboration with our healthcare providers and not by government
officials.
The potential mandate will put our jobs at risk, affecting our livelihoods and family. As
contributing members to society, we feel our medical choices should not be forced by our
government or employers. Our wish is to keep our medical freedom and continue being a
productive member within our workforces. Our country is founded on freedom and we
believe medical freedom is a priority.
Thank you again for you service,
Aaron and Jerrica Reimer
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
(wri�en tes�mony only)
Dear Chairman Erickson and commi�ee members,
I am against government mandates of Covid-19 "vaccines." I am against the government telling me and my family what to do with my body, whether it be masks or "vaccines." My family had covid-19 in December and our symptoms were similar to the common cold. I was very grateful that my medical doctor offered to prescribe Ivermec�n but I declined only because the symptoms were mild. I was so grateful to have a doctor that was willing to treat me and get me be�er before ever needing to be admi�ed to the hospital. I am saddened to say that this is very unusual and many of my friends and colleges were told by their doctor to go home with their covid and come back to the hospital once their lips turned blue.
Last month, my friend's husband was admi�ed to the hospital with covid. The staff at NMC refused to treat him with anything other than the CDC protocol. They refused to treat his symptoms, instead they went through a generic checklist which has not been successful. He was treated poorly for reques�ng anything other than what is "poli�cally correct." Thankfully he has since come home and is recovering. However, an acquaintance of mine passed away this week a�er weeks of "care" for covid at NMC. I am extremely upset how NMC has treated my friends, so I have made sure my loved ones know to go elsewhere.
Government has no right to dictate how we care for our bodies.
Sincerely,
Becky Reimer
Chairman Erickson and committee members.
As a constituent, I am very concerned about the governmental overreach onCOVID-19 Mandates. I and millions of others are against these overreachingmedical mandates that are trying to inhibit medical freedom, bodily autonomy andsovereignty in the name of tyranny and coercion.There are just not 12; there aremillions. I am concerned about the lies, gaslighting and malevolence told to theAmerican people and world about the origins of COVID and the safety andefficacy of the vaccine.
How and why has the government allowed and decided to use taxpayer moneyto purchase 65 million doses of COVID vaccine for children BEFORE the FDAauthorization and CDC recommendation meetings? How many taxpayer dollarshave been given to Pfizer, Moderna and Johnson & Johnson? How and why isthe science behind masks being ignored? The particulate size of the CCP virusis so small that masks do nothing to stop it; however the government has‘decided’ to overreach and mandate our people and even worse our children tothis tyrannical behavior. Wake up!!
There have been scientific studies from Israel and other countries stating naturalimmunity is as good as, or some cases even better than the vaccine. An Israelistudy of 2.5 million people found the vaccinated group was seven times morelikely to get infected with COVID than those with natural immunity from aprevious infection.
Another Israeli study that included 700,000 people found those with priorSARS-CoV-2 infections were 27 times less likely to develop symptomaticinfection for a second time, compared to those who were vaccinated. In additionto having the best protection available, those with natural immunity also facehigher stakes when taking the COVID vaccine as their preexisting immunitymakes them more prone to side effects. However, our government continues toignore this data. Coercion is for cowards. Whereas, Choice creates!
How is our government and its officials so dictated by finances and monetarygains, that it has forgotten its own people; those people who assisted you as
government officials into the positions that you hold. As a constituent, I willobserve, choose and take action for those officials who listen to the people. Howhas the government tolerated and allowed federal research grants and use oftaxpayer money to universities and other organizations conductinggain-of-function research and risky research on potential pandemic pathogens?Enough!!!
Those in the front lines, the healthcare providers who took the risk and continuedto treat and be present in the midst of the battleground are now being punishedfor their own service and for their natural occurring immunity. Now medicalpersonnel-- the ones who braved the storm and took care of patients--are beingfired or asked to leave their positions due to the overarching mandates. Medicalpersonnel and frontline workers are now being scrutinized by governmentofficials with a pen and paper, who have not stood in the front lines. Being in thehealthcare field, I have seen a tremendous increase in depression, anxiety andsuicidal tendencies due to the rules, restrictions and limitations placed on thepeople with face coverings, arbitrary numbers of social distancing, and vaccinemandates. Those who are medically fragile, have developmental disabilities arebeing forced into actions that they themselves can not even possibly follow.Working with children and young adults with disabilities and also the youngchildren at school, one sees an increase in behaviors, anger, animosity as thesame is being portrayed at them. I constantly see soiled masks covered in spit,dirt, mucus, and drool that the children are wearing all day…. How is thathealthy?
Yet we impose these things on our children who according to a published data bythe CDC, 99.99815% of children who contract COVID survive. Children are not asignificant threat to the elderly as most COVID cases are spread from adults tochildren. Most adults and children that have developmental disabilities, etc areunable or unwilling to wear masks due to their disability and yet the governmentoverreaches again. The same goes with airline regulations and flying, there arethose who can not due to their diagnosis or disability wear masks or have avaccine mandate. Staff and medical personnel that are critical for the needs andrequirements of those with disabilities are losing their positions due to thesemandates. They sometimes are the only family that the client has and then thatclient is left with no one. No more community outings, no more socialengagement with others, no one to care for their daily needs and we wonder why
depression, sucicide and anxiety has skyrocketed. Ignoring science on naturalacquired immunity is an arrogance.
Has our overreaching government forgotten (or pretends to ignore) that bodysovereignty and medical freedom is a choice and belongs to each individual?
To be empowered, you do not have to be forceful or aggressive. One’s strengthdoes not have to be measured by how loud or boastful or overreaching you are.Coercion is for cowards. Please STOP the government overreach on COVID-19mandates!
Trina Rice
Rebecca rider
Written Testimony
To Chairman Erickson and Committee
Members,
I am writing today to Strongly Voice my
concern Against Mandates, especially
Mask and Vaccine Mandates.
As a mother of 5 children. I am extremely
concerned about any mandates that would
require my children to put substances in
their body against our religious and
parental objections. We have always been
thankful for religious exemptions for
school attendance as we have always
skipped certain vaccines for religious and
October 27, 2021
To: Chairman Erickson and committee members
From: Stephanie Sage Kansas Citizen
Re: Written Testimony to STOP Government Overreach COVID-19 Mandates I am against government mandates for this “experimental vaccine” for the following reasons.
1. Mandates are not constitutional and violate our human rights to making personal decisions regarding ourown healthcare.
2. I am confused as to why there is such a need to mandate a vaccine for widespread or mandatory usewhen the recovery/survival rate for the average person, including children is around 99.75% and onlythose in the population such as the elderly or those with a compromised immune system are at a higherrisk for death of any virus, cold, flu, pneumonia, etc. which is the norm in the past and most likely in thefuture.
3. I have read about the potentially dangerous side effects of this “EAU vaccine” as well as deaths that haveoccurred due the side effects of this “vaccine” and feel there has not been adequate testing on animalsand humans to substantiate the widespread use of these shots let alone mandating them. Normal testingfor vaccines takes anywhere from 7-10 years using testing groups that are supervised by medicalpersonnel. I believe there needs to be more testing and research done before we even continue with theuse of this vaccine.
4. I also want to note that I am not anti-vaccine as I have always had my children vaccinated when they wereyounger, and I take the flu shot every year and completed my shingles vax this past year. From myresearch there appears to many effective and affordable treatments for this virus that have not beenallowed for use that we need more research on.I am submitting my testimony to urge the medical and pharmaceutical professionals to research thesafety and efficacy of these shots for the safety of all humanity especially before mandating that everyonetake them, even though I still stand strong in my belief that mandates should not ever be made soeveryone is free to make that personal choice for themselves and their children.
Chairman Erickson and committee members:
Thank you for your consideration of my written testimony to stop government overreach. I send this,
pleading with you to fight ANY Covid-19 vaccine mandates for any U.S. citizen of any age,as I am against government mandates of Covid-19 vaccines. I am a mother of four children ages 9-17 years and a wife. I
wake up each morning worrying that my children may soon face a mandate to take the Covid-19
vaccine to attend school or my husband will be forced by his place of employment to take the vaccine
to continue the work he has very successfully done for them for almost 18 years. The thought of taking
such vaccines is horrifying to me, considering that: 1. These are experimental, phase 3 trials 2.This type
of mRNA vaccine has NEVER been put into human beings until the past year 3.We have NO long term
studies on their use in humans.
I know people who have died from Covid-19, but I know MANY more in my community who have
suffered life altering injuries from the Covid-19 vaccine. These injuries include blood clots in the lungs,
sinuses, and the brain, heart attacks (one in an individual as young as his late 30’s), disability, coding,
congestive heart failure, strokes, seizures, and a baby lost a few weeks before delivery.
There are safe, effective, and relatively cheap protocols that can be followed to prevent Covid-19 and
safe, effective and relatively cheap treatments to treat early Covid and prevent complications and
hospitalization. It is unethical and frustrating that these treatments are blocked by many physicians and
hospitals for political reasons, but rather they state that NOTHING can be done but get the vaccine. In
my opinion, it is both reckless and unethical to force these vaccines on people.
I ask that our elected officials put a law into place that will prevent any Covid-19 mandates. This
includes any mandates to attend schools or colleges, work in any workplace, or purchase any goods or
services. I ask that these laws protect those who choose not to vaccinate from having to mask and test for Covid-19 while those who are vaccinated do not have to mask and test. This is discrimination, considering the vaccinated are still contracting and spreading the virus. Studies have shown that the viral load is equal if not higher in the vaccinated vs the non-vaccinated. We cannot treat the non-vaccinated like 2nd class citizens!
In conclusion, please help protect all American's right to choose whether or not to vaccinate for Covid-19.
Thank you,
Jenifer Sauer
Mandate on the Vaccine
EXTERNAL: This email originated from outside the organiza�on. Do not click any links or open any a�achments unless you trust thesender and know the content is safe.
I have worked for a re�rement home for 28 ½ years. I am against the mandate that every America should get a vaccineshot or lose their jobs. I am sick of hearing people say if you do not get the vaccine you do not care for your elderlyresidents. I would never do anything to hurt or harm any elder person. I pray that God be with you all and that you taketo heart the things that our country was built on. For freedom to make our own choice what we can do and say. Godbless you all.
Confidentiality Notice. This email and its attachments may contain privileged and confidential information, including protectedhealth information (PHI) protected by federal and state privacy laws. It is intended only for the use of the recipient(s) namedabove. If you are not the intended recipient, you are hereby notified that any review, dissemination, distribution, or duplication ofthis communication is strictly prohibited. If you have received this email in error, please notify the sender immediately at800-336-8511 and permanently delete this email and any attachments.
Alvin Savage

October 27, 2021Cody Sawtelle
Position: AGAINST Government Mandates of COVID-19 Vaccines
Chairman Erickson and Committee Members,
I was born in Olathe Kansas in 1987. I have lived in Kansas my entire life. I love this state. I will raise my family here because I believe in the values that Kansas has exuded consistently. Unfortunately, a tyrannical, overreaching, unscientific, and vindictive Federal Measure is threatening these values and the welfare of Kansas throughout this beloved state.
I have my Masters Degree in Civil Engineering from the University of Kansas. In direct contradiction to what the Media would like people to believe, I am not a dumb person. Unfortunately for them I do not believe everything I hear. I am not a sheep. I do my own research from reputable sources, and I make my own decisions on what my risks to medication may, or may not, be. I believe in God and his Son Jesus Christ. I believe it is my responsibility to protect my body which God has trusted to me. I am not a general statistic to be mulled over by disconnected elites choosing my fate based on broad data that do not apply to my specific case. I am now a target because I refuse to bend the knee. The Biden Administration and the traditional media need me silenced and need me discredited. Biden blames all of the problems facing this country on me, and the people like me who value freedom. If Biden can make an argument that the freedom loving people of this country are the real source of this country’s difficulties, then he can attempt to justify why he is taking away our rights and our jobs. Biden said during a recent CNN Townhall answering a question of Anderson Cooper asking about people worrying about their freedom, “Freedom? I have the freedom to kill you with my Covid. No, I mean, come on.” This is a purposeful mischaracterization. A forceful slander. He wants to paint us as demons and murderers so he can come after our jobs and be cheered while doing so. He shows that his true motives are not safety, but control. Now he IS coming after our jobs and weaponizing corporations to do his dirty work because he can’t do it through legislation. He is using corporations to circumvent the constitution.
Our institutions have become critically politicized. The CDC and the FDA (where long-standing respected members have recently resigned) are simply arms of the Biden Administration. We can no longer trust that the recommendations and guidelines that come from these institutions are genuine and in the best interest of the individuals they seek to guide. We are told by them to “believe the science” as if it is a religion; as if the data doesn’t matter. We just have to believe what they say because they are the arborators of truth. When the data shows us something different, they delete it. They remove it from Youtube or from Twitter. They censor and they condemn. The values that this country was founded on, scribed in our Declaration of Independence, and in our Constitution protect our rights to make our own risk assessments as an individual with our own specific circumstances. I can read the data, they can’t censor it all, I can think critically; God and I are the only ones who can decide what is best for me. I certainly am not what Biden maliciously mischaracterized me to be. I do not want to infect others. I do not want to help propagate this virus. However, unlike the political actors in our institutions, I recognize natural immunity. I recognize the robustness of youth. I recognize the power of good metabolic function and a strong immune system. I encourage those who feel they need to get the vaccine to go ahead and make that decision as they see fit and protect themselves as this is their right. Unlike Joe Biden, I love and trust my fellow Americans to make the correct decision for themselves and for their community based on the data and their beliefs. I don’t believe that anybody in this country is looking to murder a fellow citizen with Covid19. Unlike Joe Biden, I do not believe that those who don’t agree with me should have their lives ruined.
That is exactly what I am experiencing and witnessing every day. I am watching the lives of coworkers be destroyed in front of my eyes. When they submit exemptions, I watch them have their religious beliefs challenged; poked and prodded; tested by faceless administrators; evaluated for being good enough or strong enough; they are manipulated with underhanded questions; their beliefs may be denied by people who do not share them. This is not only an attack on freedom, but it is a clear and malicious attack on believers. All under the umbrella of them losing their livelihood and ability to support their families. It is brutal. Below are just some of the statements I have heard over the last few weeks:
“I’ve worked my entire life to have this career. I carved it out of granite from the ground up. I sacrificed so much of my personal life to get here. I love building, and I don’t know anything else. I am on a great team with a good boss. November 15th it might all get taken away from me by some faceless group sitting in judgement of my faith”
“This has been emotionally, physically, mentally, and spiritually exhausting…”
“This has sucked the life out of me”
“I can’t help but think this is defeating a lot of us. I for one have felt that way. It has been a huge distraction to my everyday work with a fear or pit in my stomach that an email is going to come that I’m not a “good enough” Christian in their mind according to their questions that are being reviewed by legal. I can’t help but think that our founding fathers established the first amendment to be freedom of expression and religion because we should have that freedom and not have it be questioned. Sorry, just had to get it all out today…”
“I haven’t slept for two nights because I’m full of worry…”
This is inhumane treatment. Not just un-American. It is worse than that. If not checked, I fear where else it may lead.
This brings me to the parable of the monkey and the fish.
A typhoon stranded a monkey on an island. In a protected place on the shore, while waiting for the raging waters to recede, he spotted a fish swimming against the current. It seemed to the monkey that the fish was struggling and needed assistance. Being of kind heart, the monkey resolved to help the fish. A tree leaned precariously over the spot where the fish seemed to be struggling. At considerable risk to himself, the monkey moved far out on a limb, reached down, and snatched the fish from the waters. Scurrying back to the safety of his shelter, he carefully laid the fish on dry ground. For a few moments, the fish showed excitement but soon settled into a peaceful rest.
We are the Fish and the Biden Administration is the Monkey. The only difference from the parable is that the Biden administration is holding a stick (our jobs), and if we try to swim away to safety he is going to beat us into compliance by taking away our jobs.
We need help. We can’t fight this battle on our own. We are fighting, but we are being punished for our attempts. We need our elected officials to stand with us and put a barrier between the Federal Government and the law-abiding citizens of Kansas. One place to start would be to hold a special session before December 8th (deadline for vaccines as presented by feds) to debate on what actions can be taken in representation and protection of your constituents.
Sincerely,Cody Sawtelle

WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Chairman Erickson and committee members,
I am firmly AGAINST the assumption that the government has ANY right to tell me what I must do with my own body and health decisions, as well as my child’s. This is getting out of control. I recently went on a school field trip with my child and his 4th grade class. It was an outdoor field trip, and the kids and adults were required to wear masks the entire time, aside from lunch. Also, I attended a parent teacher conference in person, and the hour I spent in a mask was suffocating. I am appalled that this is required for a full day of school for kids and teachers. I know many parents who have pulled their children out of public school and enrolled in co-ops that do not require masking. If I want to or want my child to wear a mask, I/we should have the CHOICE.
Not only is information on the side effects and deaths related to the Covid vaccine censored, it doesn’t exist. I don’t trust that this vaccine is safe for my son or my self, and we will not be getting it. I trust that our bodies will be strong enough to overcome the virus and build a natural immunity. In the almost two years since it’s been around, we’ve managed to not become infected. I strongly believe that a lot of this “pandemic” was constructed by government officials to create a distraction and hide their real agenda. I don’t feel like the government can be trusted, and I sure as hell don’t want them or big pharmaceutical companies telling me what to do with my body. FDA-approved doesn’t mean anything to me. My boyfriend has congestive heart failure and was prescribed 20 different medications following his heart surgery, two years ago. The doctors refuse to wean him off the meds, not because they’re afraid of what will happen, but because it’s all a coordinated scheme. The medical industry is not paid for getting people healthy. They make their money off of sick people. Look at the funding for the FDA-BIG PHARMA! This is so clear, I can’t believe people are falling for it. I do not judge the people who have made their decision based on what they think is best for themselves and their children. However, forcing employers to mandate vaccination is going too far. Forcing healthy people to wear masks, too far! Kids and teachers stuck in masks all day, too far! You’ve stepped over our rights as parents and Americans. This needs to stop. Give us the FREEDOM of choice! You are robbing Americans of what our forefathers fought for us to have, our freedom! I’m proud to be an American! I’m grateful for what we stand for! By mandating vaccination and masking, you’re taking away everything that America is built upon. We should have the right to CHOOSE!
Sheena Schaupp
school.
I am terrified however that as there may be
FDA approval for children to begin
receiving the COVID-19 vaccine, and that
the public education system will be
overstepping its boundaries and forcing
children to get the vaccine as well. These
vaccine mandates are going to do nothing
but cause harm to this entire economy and
its family system.
Thank you for your time,
Wade and Beth Schmelzle
Vaccine mandate
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Kansas government has no business telling us how to live you were not elected for this. President Biden needs to realize we don't work for him and he obviously doesn't work for United states either. This whole sham should have people hanging from ropeslike Fauchi he's no doctor or he would not be killing people do something about it
Sent from Yahoo Mail on Android
David Schroeder
Testimony
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
There are now 72 vaccines available but 55% of Americans have debilitating diseases. Big pharma - follow the money. Andfarming techniques are destroying nutrition in USA!
Sent from my iPhone
Joella Schmidt
October 27, 2021 SUBJECT: WRITTEN Testimony to STOP Government Overreach - Covid-19 Mandates Dear Chairman Erickson and Committee Members My name is Kent Schmidt and I reside in Wichita, KS. I am sending this email to you in order to share my negative business and personal experiences regarding Covid-19 mandates. First some background…
Kent Schmidt literally grew up in the senior care industry. He is a second-generation entrepreneur and senior care owner, operator, general contractor, and Adult Care Home Administrator with many years (35+) in the industry. Kent has been blessed to have been involved in a wide variety of senior care project types (nursing facilities, memory care, assisted living, independent living, etc.), while experiencing hands-on involvement in nearly every aspect of those operations, including, but not limited to: project conception, development, construction, administration, marketing, maintenance, admissions, ongoing operations and facility sales. Over the years, he has served thousands of senior care clients.
...
Fast forward to 2020 and the forthcoming era of “pandemics?” Covid-19 has severely financially impacted most typical and traditional senior care projects, resulting in a freeze on resident admissions, and exasperated by an increase in resident deaths, resident depression due to isolation, liability insurance increases, increasing compliance costs, operational issues, staffing problems, cash flow problems and related.
Based upon my recent conversations with senior citizens, senior care staff and family members of senior citizens, because they cannot fathom a repeat of being stuck in their rooms and isolated from family and friends for months at a time, they are looking for other retirement options.
My business experiences regarding Covid-19 mandates: 1. Please see bolded red italicized sentence above. 2. For those with a long-history in the senior care / health care industry, “Trust(ing) the Science” looks like this….
My personal experiences regarding Covid-19 mandates: 1. Family members will likely lose their excellent jobs in the next couple months because they refuse the vaccine. a. Their reasons for refusing the vaccine include: i. Vaccine makers are immune from liability. ii. Vaccine makers are committing horrific crimes and sins by utilizing fetal cells taken from live births. https://americasfrontlinedoctors.org/2/frontlinenews/aborted-fetal-cells-and-vaccines-a-scandal-much-bigger-than-pfizers-whistleblower-ever- imagined/ iii. Vaccine makers inhumanely experimented on animals. iv. Vaccine makers and committed murder when they experimented on orphans. https://www.thegatewaypundit.com/2021/10/wasnt-just-beagles-monkeys-faucis-nih-also-funded-medical-experiments-aids-orphans-ny-city/ iii. There are dangerous “impurities" in the vaccines. https://freeworldnews.tv/watch?id=617805b37031df173f85c2d9 2. My mother was recently in an assisted living facility, made a decision to take the vaccine and soon after became very confused, unable to eat (uncontrollable nausea), and died about a month later. For we must all appear before the judgment seat of Christ, so that each one may be recompensed for his deeds in the body, according to what he has done, whether good or bad. - 2 Corinthians 5:10 Thank you for doing the right thing by STOPPING Government Overreach and especially mandating Covid-19 vaccines! Sincerely, Kent G. Schmidt @ LinkedIn Work Cell: 316-312-6980 [email protected]
M.S. Business Law M.S. Management - KeSch Senior Hybrid Housing - KeSch Construction - - Repair It Build It - - ABC Plumbing - - Kansas Licensed General Contractor - - Kansas Licensed Adult Care Home Administrator - CONFIDENTIALITY NOTICE: This electronic mail transmission is confidential, may be privileged and should be read or retained only by the intended recipient. If you have received this transmission in error, please immediately notify the sender and delete it from your system.
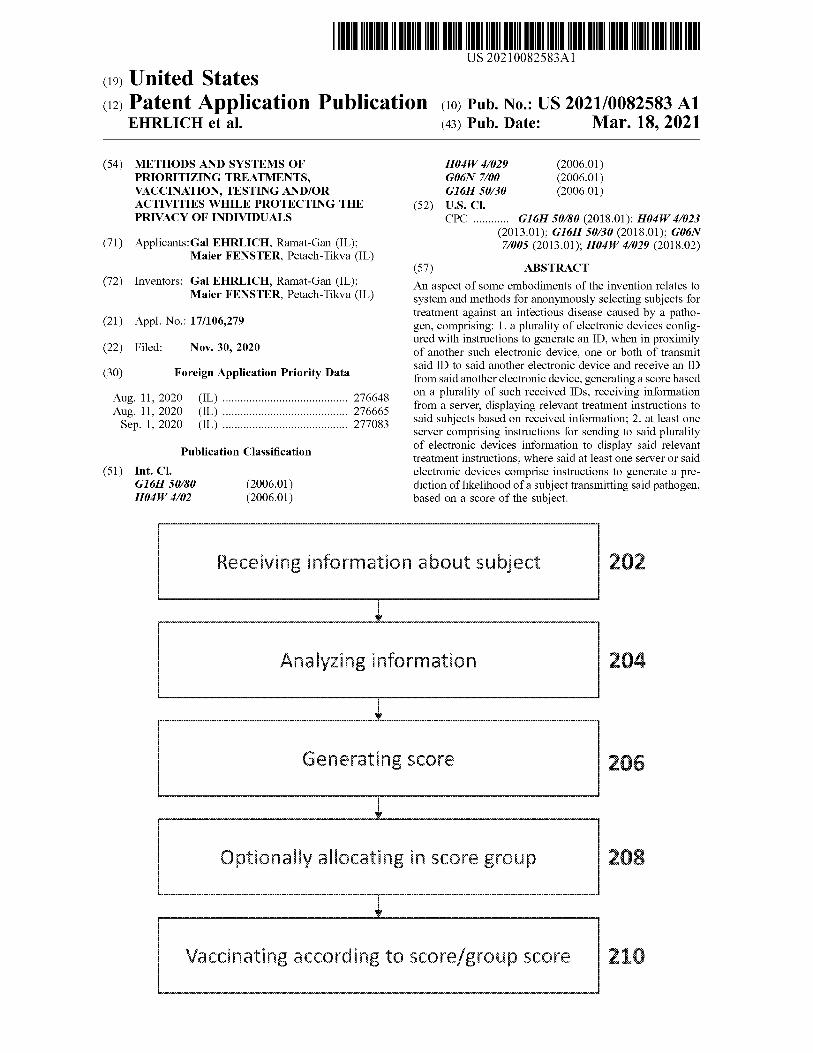
US 20210082583A1 IN
( 19 ) United States ( 12 ) Patent Application Publication ( 10 ) Pub . No .: US 2021/0082583 A1
EHRLICH et al . ( 43 ) Pub . Date : Mar. 18 , 2021
( 54 ) METHODS AND SYSTEMS OF PRIORITIZING TREATMENTS , VACCINATION , TESTING AND / OR ACTIVITIES WHILE PROTECTING THE PRIVACY OF INDIVIDUALS
H04W 4/029 ( 2006.01 ) GOON 7700 ( 2006.01 ) G16H 50/30 ( 2006.01 )
( 52 ) U.S. CI . CPC G16H 50/80 ( 2018.01 ) ; H04W 4/023
( 2013.01 ) ; G16H 50/30 ( 2018.01 ) ; GO6N 77005 ( 2013.01 ) ; H04W 4/029 ( 2018.02 ) ( 71 ) Applicants : Gal EHRLICH , Ramat - Gan ( IL ) ;
Maier FENSTER , Petach - Tikva ( IL )
( 72 ) Inventors : Gal EHRLICH , Ramat - Gan ( IL ) ; Maier FENSTER , Petach - Tikva ( IL )
( 21 ) Appl . No .: 17 / 106,279
( 22 ) Filed : Nov. 30 , 2020
( 30 ) Foreign Application Priority Data
( 57 ) ABSTRACT
An aspect of some embodiments of the invention relates to system and methods for anonymously selecting subjects for treatment against an infectious disease caused by a patho gen , comprising : 1. a plurality of electronic devices config ured with instructions to generate an ID , when in proximity of another such electronic device , one or both of transmit said ID to said another electronic device and receive an ID from said another electronic device , generating a score based on a plurality of such received IDs , receiving information from a server , displaying relevant treatment instructions to said subjects based on received information ; 2. at least one server comprising instructions for sending to said plurality of electronic devices information to display said relevant treatment instructions ; where said at least one server or said electronic devices comprise instructions to generate a pre diction of likelihood of a subject transmitting said pathogen , based on a score of the subject .
Aug. 11 , 2020 Aug. 11 , 2020 Sep. 1 , 2020
( IL ) ( IL ) ( IL )
276648 276665 277083
Publication Classification
( 51 ) Int . Ci . G16H 50/80 H04W 4/02
( 2006.01 ) ( 2006.01 )
Receiving information about subject 202
Analyzing information 204
Generating score 206
Optionally allocating in score group 208
Vaccinating according to score / group score 210
Patent Application Publication Mar. 18 , 2021 Sheet 1 of 12 US 2021/0082583 A1
Superspreader no
Non - Superspreader
Figure 1
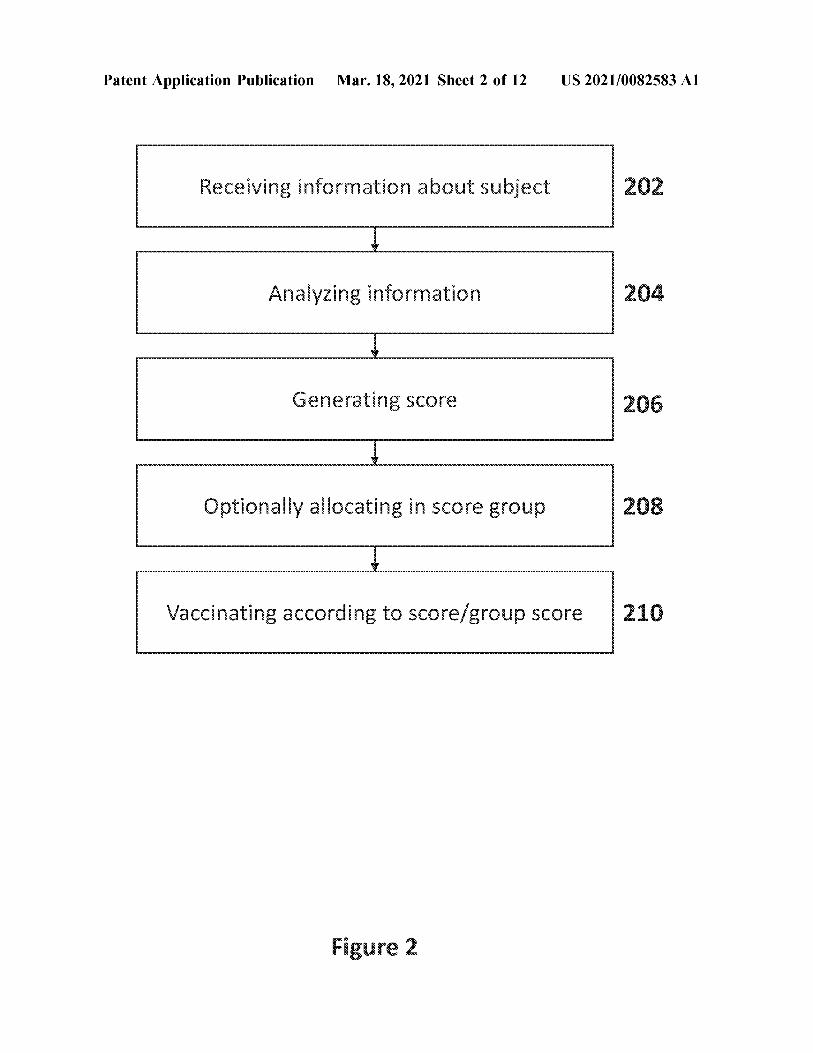
Patent Application Publication Mar. 18 , 2021 Sheet 2 of 12 US 2021/0082583 A1
Receiving information about subject 202
Analyzing information 204
Generating score 206
Optionally allocating in score group 208
Vaccinating according to score / group score
Figure 2
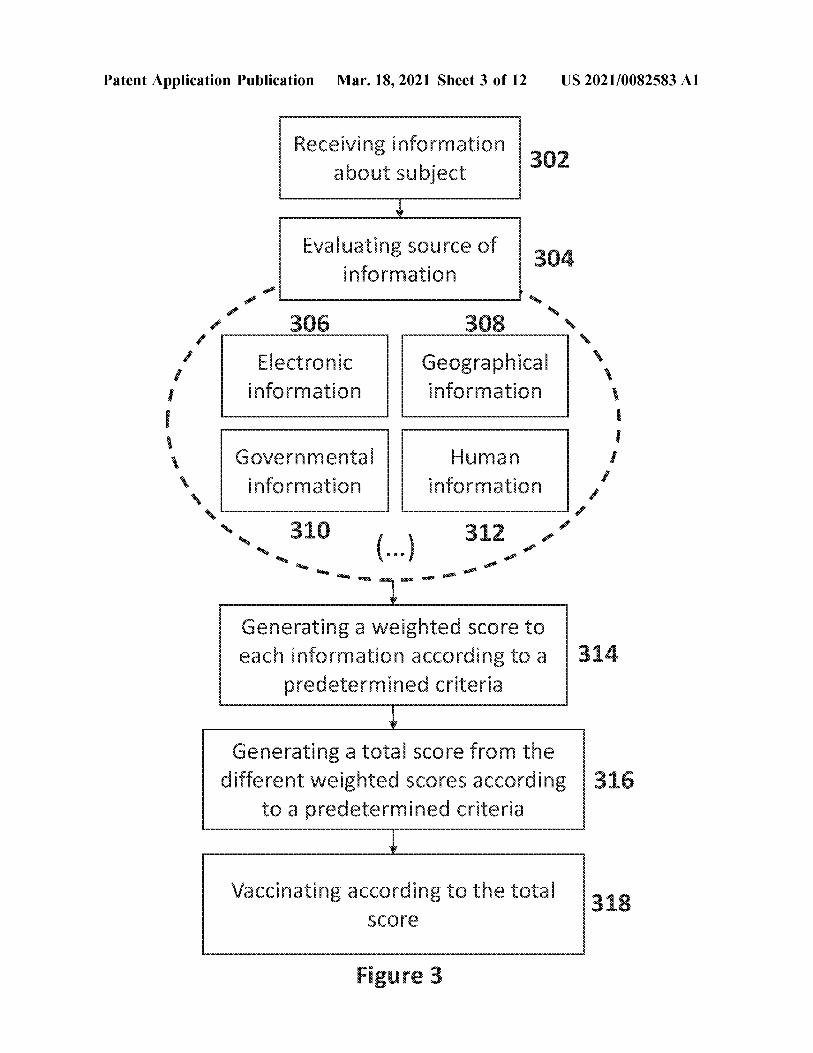
Patent Application Publication Mar. 18 , 2021 Sheet 3 of 12 US 2021/0082583 A1
Receiving information about subject 302
Evaluating source of information
AR 306 308
Electronic information
Geographical information
S.
Governmental information
Human information
310 312 SR ( ... ) RO
Generating a weighted score to each information according to a
predetermined criteria 314
Generating a total score from the different weighted scores according 316
to a predetermined criteria
Vaccinating according to the total 318 score
Figure 3
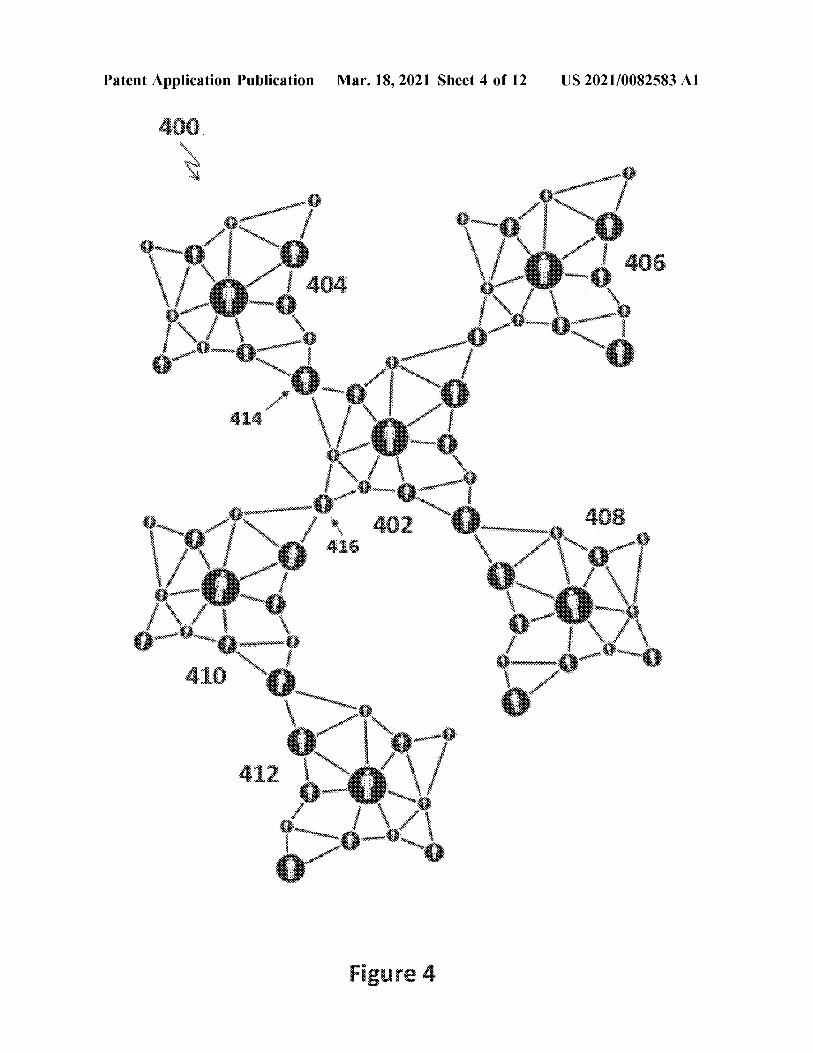
Patent Application Publication Mar. 18 , 2021 Sheet 4 of 12 US 2021/0082583 A1
NA
TE
www .
1
Sasapain 1
3
??????????
1
.
Les ***
Figure 4
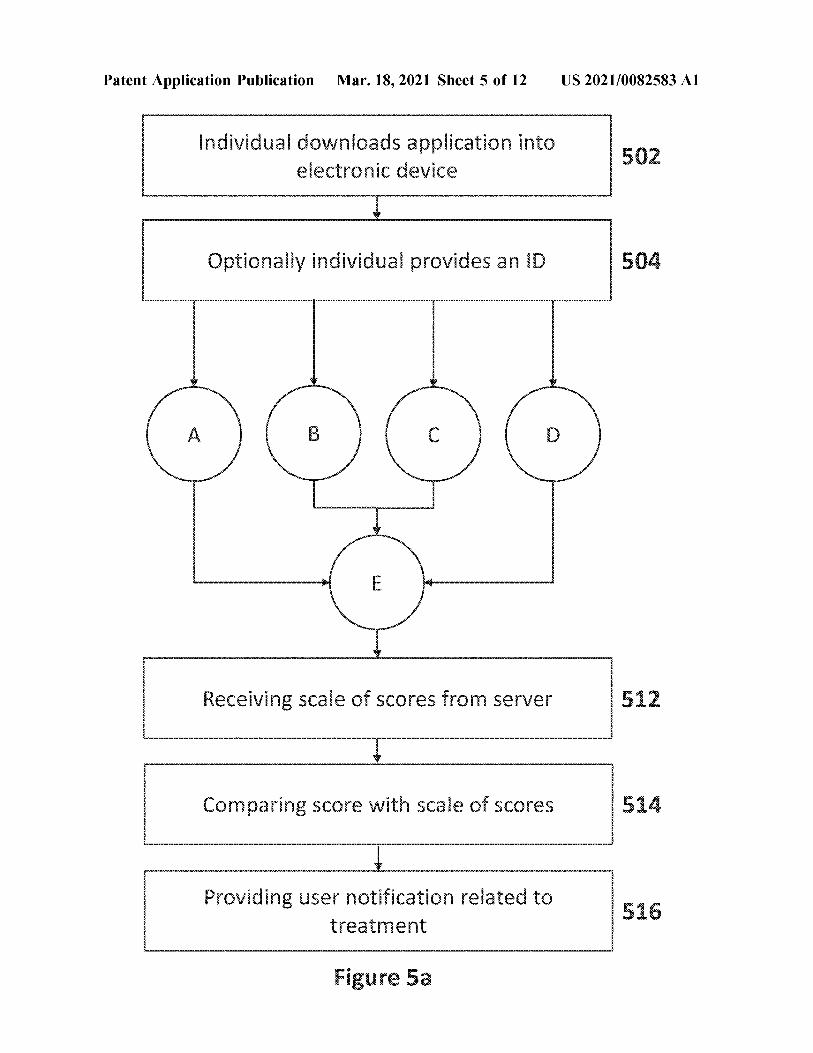
Patent Application Publication Mar. 18 , 2021 Sheet 5 of 12 US 2021/0082583 A1
Individual downloads application into electronic device 502
Optionally individual provides an ID
? B C ?
w E
Receiving scale of scores from server 512
Comparing score with scale of scores 514
Providing user notification related to treatment
516
Figure 5a
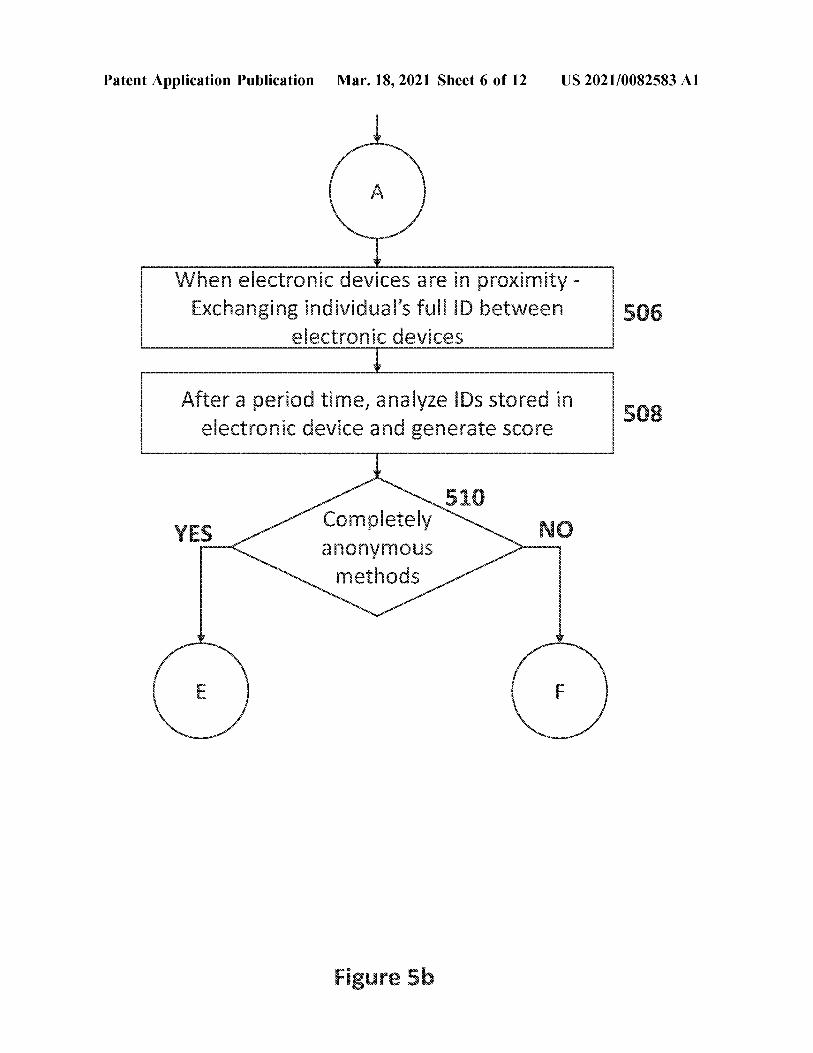
Patent Application Publication Mar. 18 , 2021 Sheet 6 of 12 US 2021/0082583 A1
?
When electronic devices are in proximity - Exchanging individual's full ID between
electronic devices 506
After a period time , analyze IDs stored in electronic device and generate score 508
YES 510
Completely anonymous methods
NO
( E F
Figure Sb
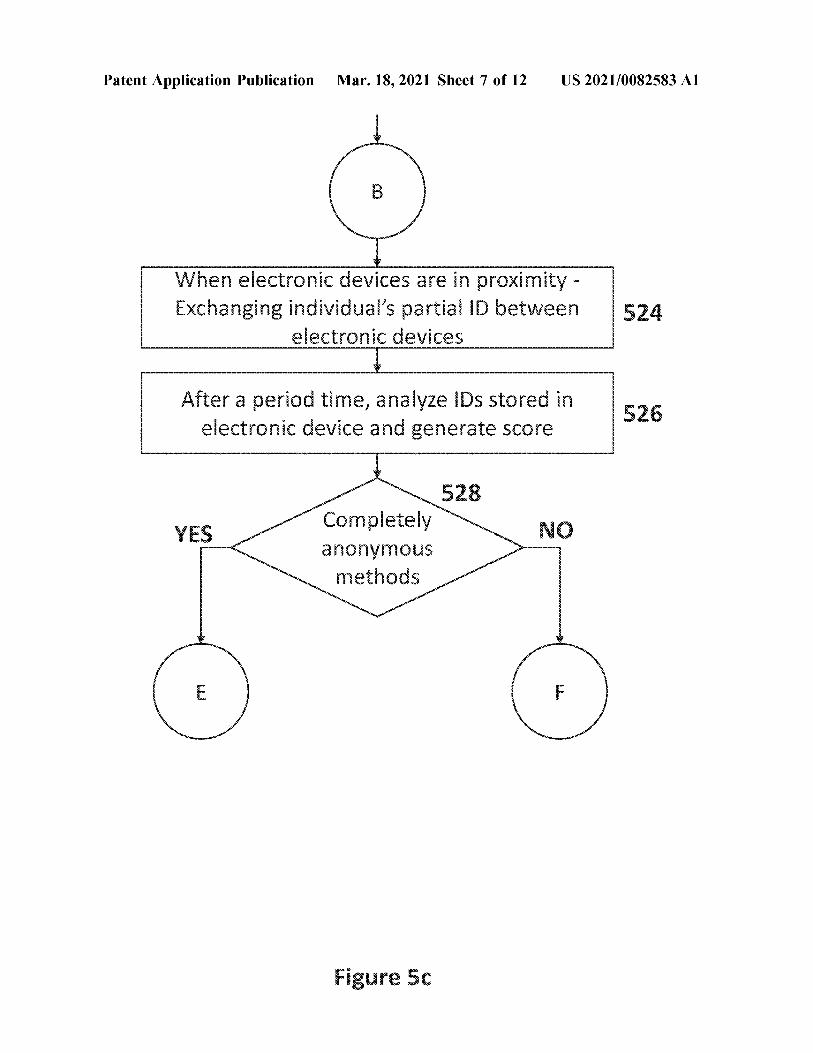
Patent Application Publication Mar. 18 , 2021 Sheet 7 of 12 US 2021/0082583 A1
B a
When electronic devices are in proximity - Exchanging individual's partial ID between
electronic devices 524
After a period time , analyze IDs stored in electronic device and generate score 526
528 Completely anonymous methods
NO
E F
Figure 5c
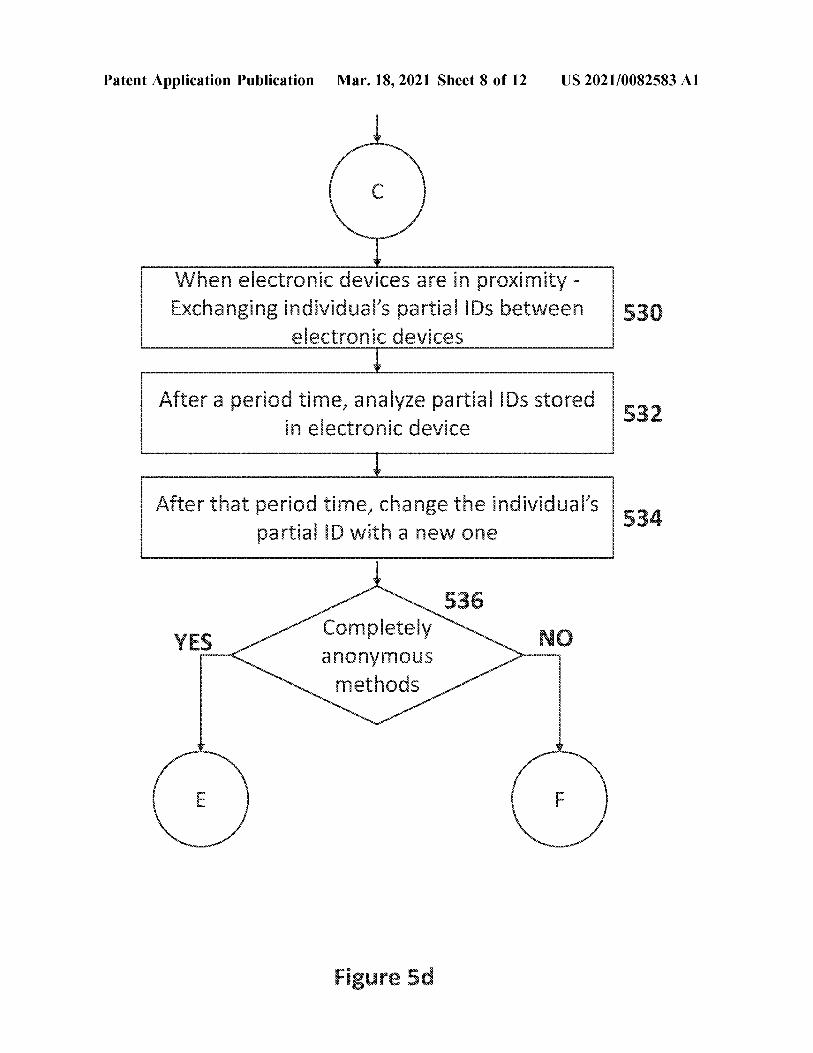
Patent Application Publication Mar. 18 , 2021 Sheet 8 of 12 US 2021/0082583 A1
C
When electronic devices are in proximity - Exchanging individual's partial IDs between
electronic devices 530
After a period time , analyze partial IDs stored in electronic device
1 XXXXXXX
After that period time , change the individual's partial ID with a new one 534
536 Completely anonymous methods
NO
E F
Figure 5d
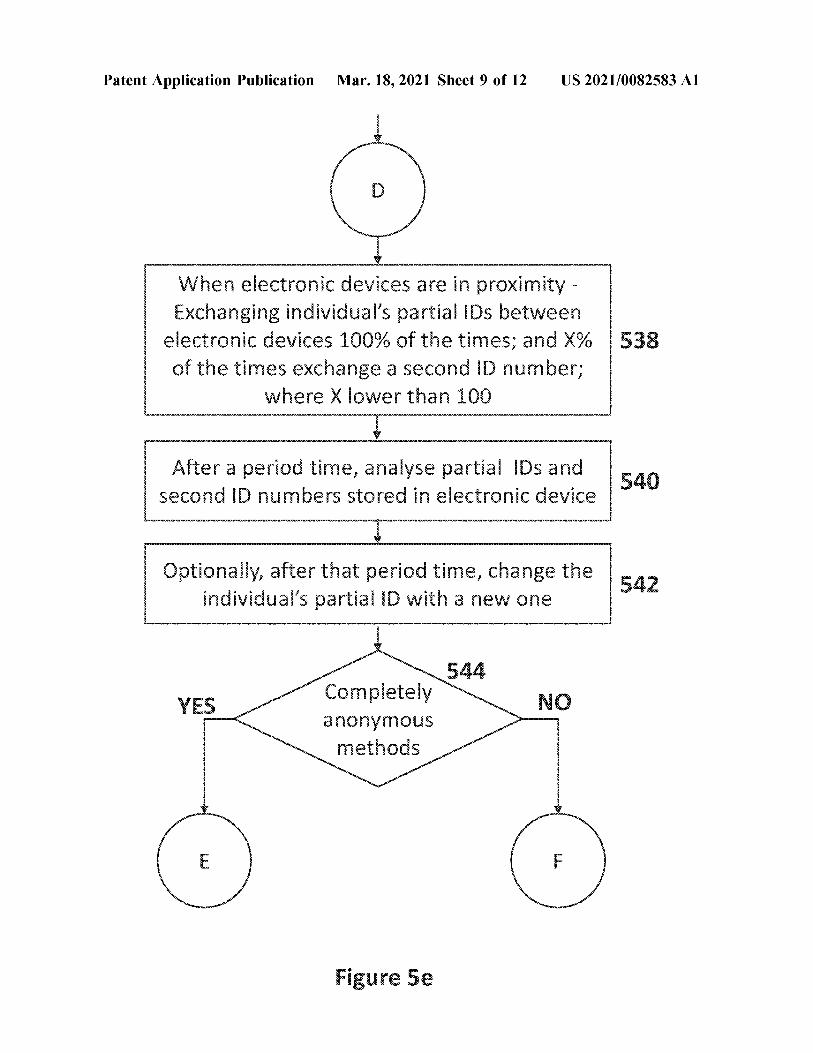
Patent Application Publication Mar. 18 , 2021 Sheet 9 of 12 US 2021/0082583 A1
D
When electronic devices are in proximity - Exchanging individual's partial IDs between
electronic devices 100 % of the times ; and X % of the times exchange a second ID number ;
where X lower than 100
538
After a period time , analyse partial IDs and second ID numbers stored in electronic device 540
Optionally , after that period time , change the individual's partial ID with a new one 542
544 YES NO Completely
anonymous methods
F
Figure 5e
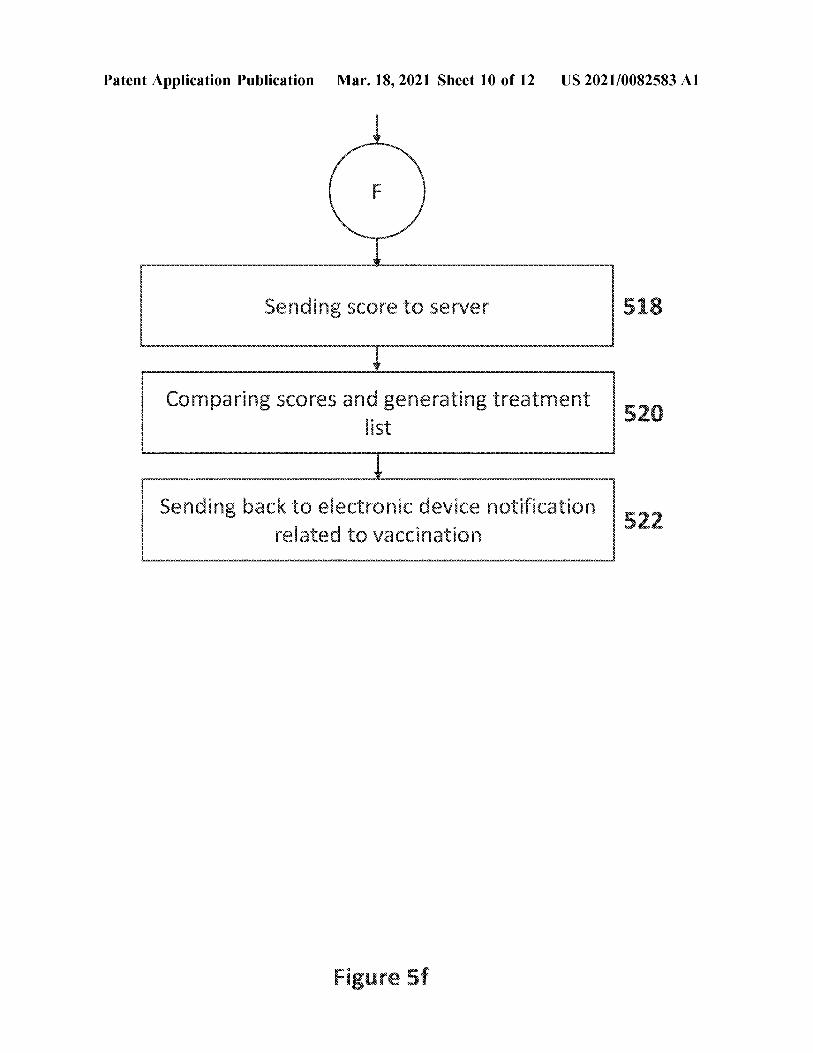
Patent Application Publication Mar. 18 , 2021 Sheet 10 of 12 US 2021/0082583 A1
best
Sending score to server 518
Comparing scores and generating treatment 520
Sending back to electronic device notification related to vaccination 522
Figure 5f
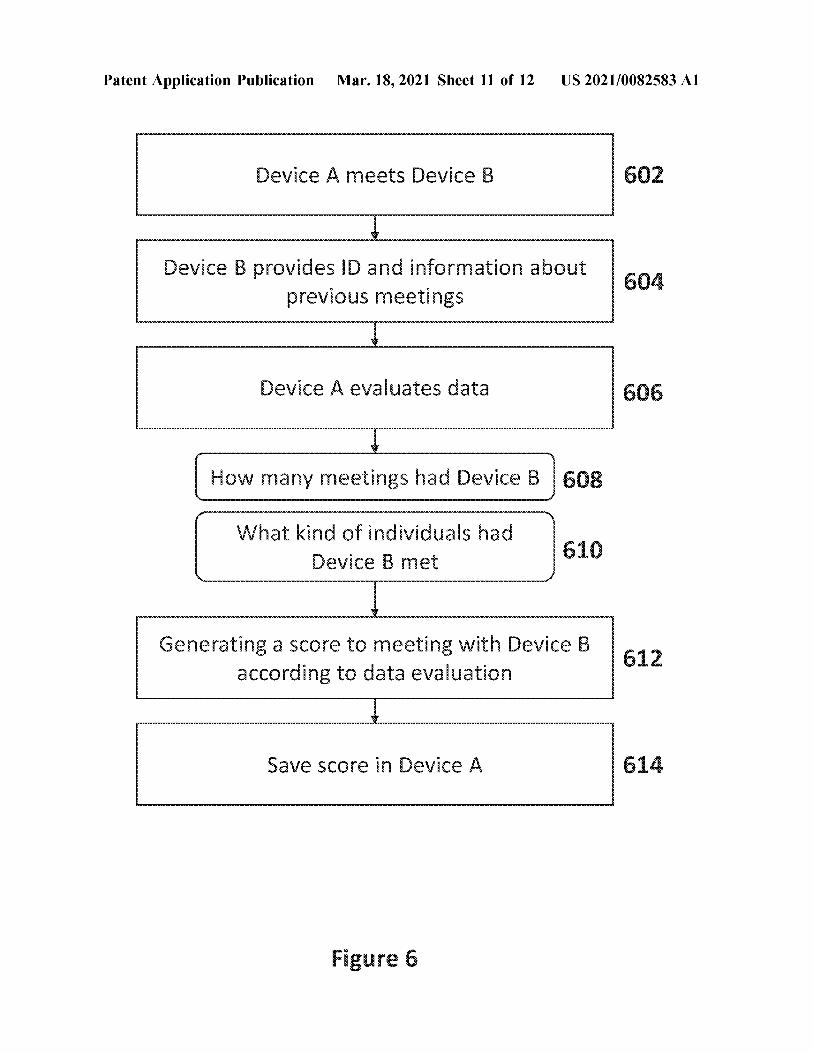
Patent Application Publication Mar. 18 , 2021 Sheet 11 of 12 US 2021/0082583 A1
Device A meets Device B 602
Device B provides ID and information about previous meetings
Device A evaluates data 606
How many meetings had Device B 608
What kind of individuals had Device B met 610
Generating a score to meeting with Device B according to data evaluation 612
Save score in Device A 614
Figure 6
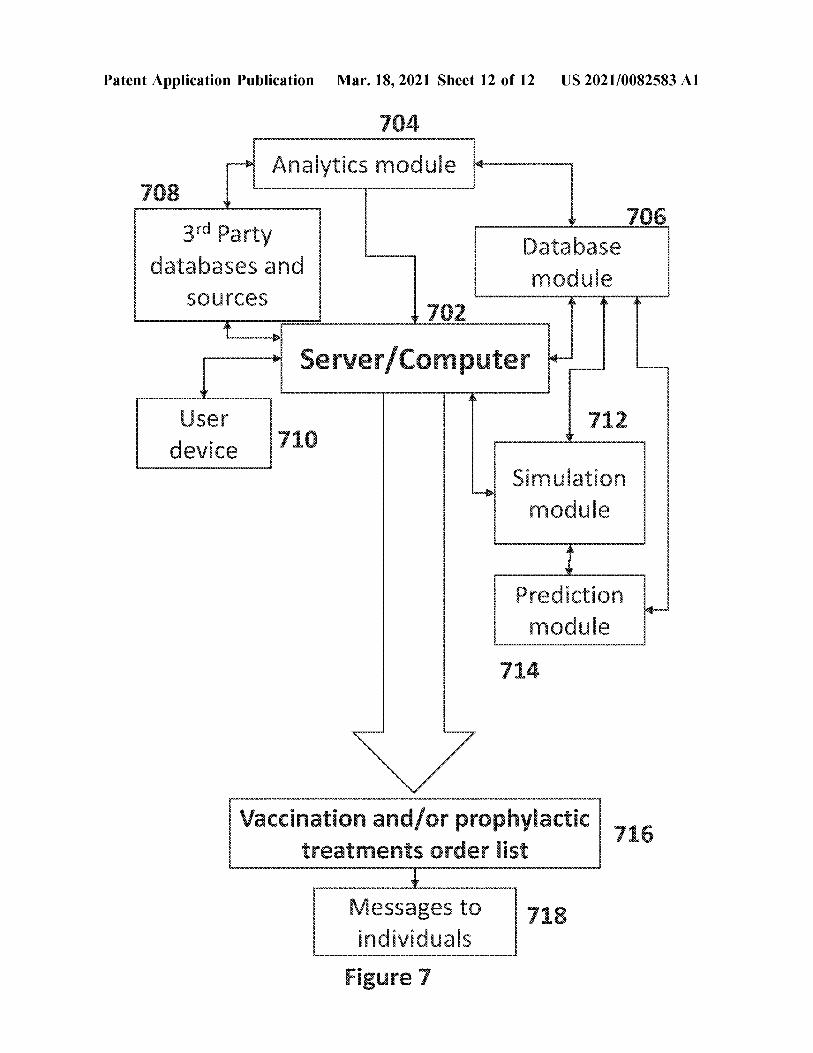
Patent Application Publication Mar. 18 , 2021 Sheet 12 of 12 US 2021/0082583 A1
Analytics module 708
3rd Party databases and
Database module
sources 702
Server / Computer 712 User
device 710
Simulation module
Prediction module
Vaccination and / or prophylactic treatments order list
Messages to individuals
Figure 7

US 2021/0082583 A1 Mar. 18 , 2021 1
METHODS AND SYSTEMS OF PRIORITIZING TREATMENTS ,
VACCINATION , TESTING AND / OR ACTIVITIES WHILE PROTECTING THE
PRIVACY OF INDIVIDUALS
RELATED APPLICATIONS [ 0001 ] This application claims the benefit of priority of Israel Patent Application No. 277083 filed on Sep. 1 , 2020 , Israel Patent Application No. 276665 filed on Aug. 11 , 2020 , and Israel Patent Application No. 276648 filed on Aug. 11 , 2020. The contents of the above applications are all incor porated by reference as if fully set forth herein in their entirety . [ 0002 ] This application is also related to United Arab Emirates Patent Application No. P6001304 / 2020 filed on Sep. 17 , 2020 , the contents of which are incorporated herein by reference in their entirety .
relationship between virally triggered inflammation , venous thromboembolism , and ARDS in COVID - 19 is still under investigation . Given that patients with severe COVID - 19 often present with shortness of breath and pulmonary infil trates , the diagnosis of PE may be overlooked in the context of an ARDS diagnosis . [ 0006 ] A research article by Straetemans et . al . called “ Prioritization strategies for pandemic influenza vaccine in 27 countries of the European Union and the Global Health Security Action Group : a review ” discussed vaccine priori tization strategies during pandemic times , but its conclu sions are limited to the critical groups , for example , health care providers ( e.g. , doctors , nurses , laboratories , hospitals , etc. ) , essential service providers ( e.g. , police , fire fighters , public sector personnel , governmental personnel , etc. ) and high risk individuals ( e.g. , people with high risk of compli cations , pregnant women , children , etc. ) . These obvious groups usually amount to less than 2-10 % of the total population , which still leaves the government with the question of what is the best order to vaccinate the rest of the population , namely prioritizing vaccinations . FIELD AND BACKGROUND OF THE
INVENTION SUMMARY OF THE INVENTION [ 0003 ] The present invention , in some embodiments
thereof , relates to methods and systems of prioritizing vaccinations \ treatments \ testing and , more particularly , but not exclusively , to method and systems of prioritizing vaccinations \ treatments \ testing in a pandemic situation , whereby vaccines are at short supply and while protecting the privacy of the individuals in the population . [ 0004 ] Coronavirus disease 2019 ( COVID - 19 ) is an infec tious disease caused by severe acute respiratory syndrome coronavirus 2 ( SARS - CoV - 2 ) . It was first identified in December 2019 in Wuhan , Hubei , China , and has resulted in an ongoing pandemic . The first confirmed case has been traced back to 17 Nov. 2019 in Hubei . As of 6 August 2020 , more than 18.7 million cases have been reported across 188 countries and territories , resulting in more than 706,000 deaths . More than 11.3 million people have recovered . The virus is primarily spread between people during close con tact , most often via small droplets produced by coughing , sneezing , and talking . The droplets usually fall to the ground or onto surfaces rather than travelling through air over long distances . However , the transmission may also occur through smaller droplets that are able to stay suspended in the air for longer periods of time in enclosed spaces , as typical for airborne diseases . Less commonly , people may become infected by touching a contaminated surface and then touching their face . It is most contagious during the first three days after the onset of symptoms , although spread is possible before symptoms appear , after they disappear and from people who show very mild or do not show symptoms at all . [ 0005 ] In addition , about 5 % of COVID - 19 patients expe rience complications including septic shock , acute respira tory distress syndrome ( ARDS ) , acute cardiac or kidney injury , and disseminated intravascular coagulation ( DIC ) . These complications are thought to be manifestations of the cytokine storm triggered by the host immune response of the virus . In critically ill patients , ARDS was the most common complication in 67 % of the patients with a 28 - day mortality of 61.5 % . DIC has been widely reported in COVID - 19 . Pulmonary embolism ( PE ) in COVID - 19 patients has been reported in a few studies . A recent study pointed to a higher incidence of PE with 23 % in severe COVID - 19 patients . The
[ 0007 ] Following is a non - exclusive list including some examples of embodiments of the invention . The invention also includes embodiments , which include fewer than all the features in an example , and embodiments using features from multiple examples , also if not expressly listed below . [ 0008 ] Example 1. An anonymized method of treating subjects against an infectious disease caused by a pathogen , comprising : [ 0009 ] a . providing an electronic device with proximity tracking circuitry for each of said subjects ; [ 0010 ] b . generating an ID for each said electronic device ; [ 0011 ] c . at a proximity event , when a particular said electronic device of a particular said subject is in proximity of one or more other of said electronic devices , one or both of transmitting said ID or an indication thereof to said one or more other devices and receiving an ID or indication thereof from said one or more other devices , by said particular electronic device ; [ 0012 ] d . generating , by said particular electronic device a score reflecting a propensity for proximity , according to a plurality of received IDs ; [ 0013 ] e . generating for said particular electronic device a prioritization of treatment based on said score ; [ 0014 ] f . treating said particular subject according to said prioritization . [ 0015 ] Example 2. The method according to example 1 , wherein said generating an ID comprises generating an ID having fewer than 100,000 potential values . [ 0016 ] Example 3. The method according to example 2 , wherein said generating an ID comprises generating a unique ID and also generating said ID as a portion of said unique ID [ 0017 ] Example 4. The method according to example 1 , further comprising changing said ID periodically . [ 0018 ] Example 5. The method according to example 1 , further comprising generating a second ID and transmitting said second ID or indication thereof together with said ID . [ 0019 ] Example 6. The method according to example 5 , wherein said transmitting a second ID is carried out only at a fraction of said proximity events .

US 2021/0082583 A1 Mar. 18 , 2021 2
[ 0020 ] Example 7. The method according to example 6 , wherein said transmitting comprises transmitting also sec ond IDs previously received from others of said electronic devices . [ 0021 ] Example 8. The method according to example 6 , comprising generating an indication of closeness of a popu lation met by said electronic device based on said received second IDs . [ 0022 ] Example 9. The method according to example 1 , wherein said score depends on an estimation of propensity of proximity of said one or more other devices . [ 0023 ] Example 10. The method according to example 1 , wherein said generating said score comprises counting the number of received IDs . [ 0024 ] Example 11. The method according to example 10 , wherein said counting comprises counting unique IDs . [ 0025 ] Example 12. The method according to example 10 , wherein said counting comprises counting IDs with a weighted parameter , said weighted parameter is generated by analyzing said exchanged second IDs . [ 0026 ] Example 13. The method according to example 1 , wherein said generating for said particular device comprises transmitting said score to a server and generating said prioritization on said server . [ 0027 ] Example 14. The method according to example 13 , wherein generating said prioritization comprises comparing scores by different ones of said electronic devices . [ 0028 ] Example 15. The method according to example 1 , wherein said generating for said particular device comprises generating said prioritization on said particular electronic device . [ 0029 ] Example 16. The method according to example 15 , wherein said generation comprises receiving form a server a list or a function indication prioritization according to score . [ 0030 ] Example 17. The method according to example 1 , comprising displaying treatment instructions on said par ticular electronic device based on said generated prioritiza tion .
[ 0031 ] Example 18. The method of example 1 , wherein said pathogen comprises a corona virus and wherein said treatment comprises a vaccination and wherein said priori tization is used to select subjects at greater risk of transmit ting the pathogen during a pandemic to be vaccinated sooner than subjects less likely to transmit the pathogen . [ 0032 ] Example 19. A system for anonymously selecting subjects for treatment against an infectious disease caused by a pathogen , comprising : [ 0033 ] a . a plurality of electronic devices configured to be carried around by said subjects and configured with instruc tions to :
[ 0034 ] i . generate an ID comprising for each said elec tronic device ;
[ 0035 ] ii . when in proximity of another such electronic device , one or both of transmit said ID or an indication thereof to said another electronic device and receive an ID or indication thereof from said another electronic device ;
[ 0036 ] iii . generating , a score based on a plurality of such received IDs ;
[ 0037 ] iv . receiving information from a server ; [ 0038 ] V. displaying relevant treatment instructions to
said subjects based on said received information ;
[ 0039 ] b . at least one server comprising a memory and a plurality of modules ; said memory - comprising instructions for :
[ 0040 ] vi . sending to said plurality of electronic devices information usable by a circuitry in said plurality of electronic devices to display said relevant treatment instructions ,
wherein said at least one server or said electronic devices comprise instructions to generate a prediction of likelihood of a subject transmitting said pathogen , based on a score of the subject . [ 0041 ] Example 20. The system according to example 19 , wherein said information comprises one or more of subject specific information . [ 0042 ] Example 21. The system according to example 19 , wherein said information comprises general information usable by a plurality of subjects and devices thereof . [ 0043 ] Example 22. The system according to example 19 , wherein said server is configured with instructions to receive anonymous scores for a plurality of said electronic devices and use said received scores to generate said general infor mation , said electronic devices configured to use said gen eral information to determine a relative treatment priority for their respective subjects . [ 0044 ] Example 23. The system according to example 19 , wherein said electronic devices comprises a proximity detecting module using one or more of : a . physical proximity data received by means of electronic positioning data of said subject ; b . a distance indicating sensor which indicates physical proximity of the location of a device in relation to the location of said another device ; and c . historical location data . [ 0045 ] Example 24. The system according to example 19 , wherein said at least one server or said electronic devices comprise instructions to determine a treatment prioritization based on said likelihood . [ 0046 ] Example 25. The system according to example 23 , wherein said determine a treatment prioritization further comprises one or more of : a . generating a score component based on a nature of a location where said physical proximity data is related ; b . generating a score component comprising health data of the subject of one or both electronic devices ; c . generating a score component comprising a profession of the subject of one or both electronic devices ; d . generating a score component reflecting relative health risk to said subject if said subject contracts said pathogen ; and e . generating a score component reflecting damage to soci ety if said subject contracts said pathogen . [ 0047 ] Example 26. The system according to example 23 , wherein when said physical proximity data is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0048 ] Example 27. The system according to example 19 , further comprising a vaccination server , which allocates vaccinations for a corona virus according to , said displayed treatment information . [ 0049 ] Example 28. The system according to example 27 , wherein said server comprises a simulation module config ured to perform one or both of :

US 2021/0082583 A1 Mar. 18 , 2021 3
( a ) predict the effect of vaccination on disease spread ; ( b ) predict the effect of an ID transmission probability on distinguishing between subjects who contact mainly sub jects in a same subpopulation . [ 0050 ] Example 29. The system of example 19 , wherein said electronic devices are configured to transmit a second ID and previously received second IDs , at a probability of less than 10 % and using said received second IDs to generate said score . Example 30. The system of example 19 , wherein said transmitted ID is a non - unique ID having fewer possible values than 10 % of the number of said devices . [ 0051 ] According to an aspect of some embodiments of the present invention there is provided a method of selecting subjects for being vaccinated / treated against an infectious disease caused by a pathogen , using personal physical proximity information of a subject , comprising : [ 0052 ] a generating , by circuitry , a predicted likelihood of said subject of transmitting said pathogen based on said physical proximity information , for a plurality of subjects ; [ 0053 ] b . selecting subjects of said plurality of subjects for vaccinating / treating based on a prediction that said vacci nating / treating said subjects will reduce a likelihood of spreading of said disease in said plurality of subjects , wherein said selecting is based on said generated predicted likelihood . [ 0054 ] According to some embodiments of the invention , said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0055 ] According to some embodiments of the invention , said disease is endemic or pandemic . [ 0056 ] According to some embodiments of the invention , said predicted likelihood of said subject of transmitting said pathogen comprises one or more score components used for generating a score . [ 0057 ] According to some embodiments of the invention , said score relates to a predicted likelihood of a group of subjects transmitting said pathogen based on said physical proximity information , and said physical proximity infor mation is a first score component used for said generating said score . [ 0058 ] According to some embodiments of the invention , said generating said score further comprises a score com ponent based on a nature of a location where said physical proximity information is related . [ 0059 ] According to some embodiments of the invention , said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non - ventilated indoor space and any combination thereof . [ 0060 ] According to some embodiments of the invention , when said physical proximity information is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0061 ] According to some embodiments of the invention , said physical proximity information is physical proximity data received by means of electronic positioning data of said subject . [ 0062 ] According to some embodiments of the invention , said physical proximity information is physical proximity data of the location of said subject in relation to the location of other subjects . [ 0063 ] According to some embodiments of the invention , said physical proximity data comprises one or more of
physical proximity distance data , duration of physical prox imity data and / or ambience of physical proximity data . [ 0064 ] According to some embodiments of the invention , said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects . [ 0065 ] According to some embodiments of the invention , said method further comprises generating a predicted like lihood of said subject contracting said pathogen based on said physical proximity data . [ 0066 ] According to some embodiments of the invention , said generating a score further comprises a second score component based on said predicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0067 ] According to some embodiments of the invention , said electronic positioning data is collected using one or more electronic devices . [ 0068 ] According to some embodiments of the invention , said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated elec tronic device . [ 0069 ] According to some embodiments of the invention , the method further comprising vaccinating / treating said sub jects according to said score . [ 0070 ] According to some embodiments of the invention , said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0071 ] According to some embodiments of the invention , said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0072 ] According to some embodiments of the invention , said electronic positioning data comprises geographical location data . [ 0073 ] According to some embodiments of the invention , said physical proximity information comprises historical location data . [ 0074 ] According to some embodiments of the invention , said generating said score further comprises a component comprising historical health data . [ 0075 ] According to some embodiments of the invention , said generating said score further comprises a component comprising a profession in record of said subject . [ 0076 ] According to some embodiments of the invention , said physical proximity information further comprises infor mation received from a third party . [ 0077 ] According to some embodiments of the invention , said physical proximity information is provided by said subject actively . [ 0078 ] According to some embodiments of the invention , said physical proximity information is provided by said subject passively by means of said one or more electronic devices . [ 0079 ] According to some embodiments of the invention , said pathogen is a virus . [ 0080 ] According to some embodiments of the invention , said virus is a corona virus . [ 0081 ] According to some embodiments of the invention , said virus is SARS - CoV . [ 0082 ] According to some embodiments of the invention , said virus is MERS - CoV .

US 2021/0082583 A1 Mar. 18 , 2021 4
[ 0083 ] According to some embodiments of the invention , said virus is SARS - CoV - 2 . [ 0084 ] According to some embodiments of the invention , said virus is an influenza virus . [ 0085 ] According to some embodiments of the invention , said disease results in influenza like symptoms . [ 0086 ] According to an aspect of some embodiments of the present invention there is provided a method of selecting subjects for being vaccinated / treated against an infectious disease caused by a pathogen , comprising : [ 0087 ] a . automatically collecting physical proximity information of a subject with other subjects ; [ 0088 ] b . generating a predicted likelihood of said subject of transmitting said virus based on said physical proximity information ; [ 0089 ] c . generating a score comprising a first score com ponent based on said predicted likelihood of said subject of transmitting said virus ; [ 0090 ] d . repeating steps b - c for a plurality of subjects ; and [ 0091 ] e . prioritizing vaccination / treatment of said sub jects according to said score . [ 0092 ] According to some embodiments of the invention , said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0093 ] According to some embodiments of the invention , said disease is endemic or pandemic . [ 0094 ] According to some embodiments of the invention , said generating said score further comprises a score com ponent based on a nature of a location where said physical proximity information is related . [ 0095 ] According to some embodiments of the invention , said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non - ventilated indoor space and any combination thereof . [ 0096 ] According to some embodiments of the invention , when said physical proximity information is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0097 ] According to some embodiments of the invention , said physical proximity information is physical proximity data received by means of electronic positioning data of said subject . [ 0098 ] According to some embodiments of the invention , said physical proximity information is physical proximity data of the location of said subject in relation to the location of other subjects . [ 0099 ] According to some embodiments of the invention , said physical proximity data comprises one or more of physical proximity distance data , duration of physical prox imity data and / or ambience of physical proximity data . [ 0100 ] According to some embodiments of the invention , said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects . [ 0101 ] According to some embodiments of the invention , said method further comprises generating a predicted like lihood of said subject contracting said pathogen based on said physical proximity data . [ 0102 ] According to some embodiments of the invention , said generating a score further comprises a second score
component based on said predicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0103 ] According to some embodiments of the invention , said electronic positioning data is collected using one or more electronic devices . [ 0104 ] According to some embodiments of the invention , said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated elec tronic device . [ 0105 ] According to some embodiments of the invention , the method further comprising vaccinating / treating said sub jects according to said score . [ 0106 ] According to some embodiments of the invention , said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0107 ] According to some embodiments of the invention , said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0108 ] According to some embodiments of the invention , said electronic positioning data comprises geographical location data . [ 0109 ] According to some embodiments of the invention , said physical proximity information comprises historical location data . [ 0110 ] According to some embodiments of the invention , said generating said score further comprises a component comprising historical health data . [ 0111 ] According to some embodiments of the invention , said generating said score further comprises a component comprising a profession in record of said subject . [ 0112 ] According to some embodiments of the invention , said physical proximity information further comprises infor mation received from a third party . [ 0113 ] According to some embodiments of the invention , said physical proximity information is provided by said subject actively . [ 0114 ] According to some embodiments of the invention , said physical proximity information is provided by said subject passively by means of said one or more electronic devices . [ 0115 ] According to some embodiments of the invention , said pathogen is a virus . [ 0116 ] According to some embodiments of the invention , said virus is a corona virus . [ 0117 ] According to some embodiments of the invention , said virus is SARS - CoV . [ 0118 ] According to some embodiments of the invention , said virus is MERS - CoV . [ 0119 ] According to some embodiments of the invention , said virus is SARS - CoV - 2 . [ 0120 ] According to some embodiments of the invention , said virus is an influenza virus . [ 0121 ] According to some embodiments of the invention , said disease results in influenza like symptoms . [ 0122 ] According to an aspect of some embodiments of the present invention there is provided a system for selecting subjects for being vaccinated / treated against an infectious disease caused by a pathogen , comprising :
US 2021/0082583 A1 Mar. 18 , 2021 5
[ 0123 ] a . at least one server comprising a memory ; [ 0124 ] b . an analytics module ; [ 0125 ] c . a database module ; [ 0126 ] d . a simulation module ; [ 0127 ] said memory in said at least one server comprising instructions , said instructions comprising :
[ 0128 ] i . generating , by circuitry , a predicted likelihood of said subject of transmitting said pathogen based on said physical proximity information , for a plurality of subjects ;
[ 0129 ] ii . selecting subjects of said plurality of subjects for vaccinating / treating based on a prediction that said vaccinating / treating said subjects will reduce a likeli hood of spreading of said disease in said plurality of subjects , wherein said selecting is based on said gen erated predicted likelihood .
( 0130 ] According to some embodiments of the invention , said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0131 ] According to some embodiments of the invention , said disease is endemic or pandemic . [ 0132 ] According to some embodiments of the invention , said predicted likelihood of said subject of transmitting said pathogen comprises one or more score components used for generating a score . [ 0133 ] According to some embodiments of the invention , said score relates to a predicted likelihood of a group of subjects transmitting said pathogen based on said physical proximity information , and said physical proximity infor mation is a first score component used for said generating said score . [ 0134 ] According to some embodiments of the invention , said generating said score further comprises a score com ponent based on a nature of a location where said physical proximity information is related . [ 0135 ] According to some embodiments of the invention , said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non - ventilated indoor space and any combination thereof . [ 0136 ] According to some embodiments of the invention , when said physical proximity information is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0137 ] According to some embodiments of the invention , said physical proximity information is physical proximity data received by means of electronic positioning data of said subject . [ 0138 ] According to some embodiments of the invention , said physical proximity information is physical proximity data of the location of said subject in relation to the location of other subjects . [ 0139 ] According to some embodiments of the invention , said physical proximity data comprises one or more of physical proximity distance data , duration of physical prox imity data and / or ambience of physical proximity data . [ 0140 ] According to some embodiments of the invention , said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects .
[ 0141 ] According to some embodiments of the invention , said method further comprises generating a predicted like lihood of said subject contracting said pathogen based on said physical proximity data . [ 0142 ] According to some embodiments of the invention , said generating a score further comprises a second score component based on said predicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0143 ] According to some embodiments of the invention , said electronic positioning data is collected using one or more electronic devices . [ 0144 ] According to some embodiments of the invention , said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated elec tronic device . [ 0145 ] According to some embodiments of the invention , the system further comprising vaccinating / treating said sub jects according to said score . [ 0146 ] According to some embodiments of the invention , said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0147 ] According to some embodiments of the invention , said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0148 ] According to some embodiments of the invention , said electronic positioning data comprises geographical location data . [ 0149 ] According to some embodiments of the invention , said physical proximity information comprises historical location data . [ 0150 ] According to some embodiments of the invention , said generating said score further comprises a component comprising historical health data . [ 0151 ] According to some embodiments of the invention , said generating said score further comprises a component comprising a profession in record of said subject . [ 0152 ] According to some embodiments of the invention , said physical proximity information further comprises infor mation received from a third party . [ 0153 ] According to some embodiments of the invention , said physical proximity information is provided by said subject actively . [ 0154 ] According to some embodiments of the invention , said physical proximity information is provided by said subject passively by means of said one or more electronic devices . [ 0155 ] According to some embodiments of the invention , said simulation module further comprises a prediction mod ule . [ 0156 ] According to some embodiments of the invention , said pathogen is a virus . [ 0157 ] According to some embodiments of the invention , said virus is a corona virus . [ 0158 ] According to some embodiments of the invention , said virus is SARS - CoV . [ 0159 ] According to some embodiments of the invention , said virus is MERS - CoV . [ 0160 ] According to some embodiments of the invention , said virus is SARS - CoV - 2 . [ 0161 ] According to some embodiments of the invention , said virus is an influenza virus .

US 2021/0082583 A1 Mar. 18 , 2021 6
[ 0162 ] According to some embodiments of the invention , said disease results in influenza like symptoms . [ 0163 ] Following is a second non - exclusive list including some examples of embodiments of the invention . The inven tion also includes embodiments , which include fewer than all the features in an example , and embodiments using features from multiple examples , also if not expressly listed below . [ 0164 ] Example 1. A method of selecting subjects for being vaccinated against an infectious disease caused by a pathogen , using personal physical proximity information of a subject , comprising : [ 0165 ] a generating , by circuitry , a predicted likelihood of said subject of transmitting said pathogen based on said physical proximity information , for a plurality of subjects ; [ 0166 ] b . selecting subjects of said plurality of subjects for vaccinating based on a prediction that said vaccinating said subjects will reduce a likelihood of spreading of said disease in said plurality of subjects , wherein said selecting is based on said generated predicted likelihood . [ 0167 ] Example 2. The method according to example 1 , wherein said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0168 ] Example 3. The method according to according to any one of examples 1-2 , wherein said disease is endemic or pandemic . [ 0169 ] Example 4. The method according to any one of examples 1-3 , wherein said predicted likelihood of said subject of transmitting said pathogen comprises one or more score components used for generating a score . [ 0170 ] Example 5. The method according to example 4 , wherein said score relates to a predicted likelihood of a group of subjects transmitting said pathogen based on said physical proximity information , and said physical proximity information is a first score component used for said gener ating said score . [ 0171 ] Example 6. The method according to any one of examples 4-5 , wherein said generating said score further comprises a score component based on a nature of a location where said physical proximity information is related . [ 0172 ] Example 7. The method of example 6 , wherein said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non ventilated indoor space and any combination thereof . [ 0173 ] Example 8. The method according to any one of examples 1-7 , wherein when said physical proximity infor mation is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0174 ] Example 9. The method according to any one of examples 1-8 , wherein said physical proximity information is physical proximity data received by means of electronic positioning data of said subject . [ 0175 ] Example 10. The method according to any one of examples 1-9 , wherein said physical proximity information is physical proximity data of the location of said subject in relation the location of other subjects . [ 0176 ] Example 11. The method according to any one of examples 9-10 , wherein said physical proximity data com prises one or more of physical proximity distance data , duration of physical proximity data and / or ambience of physical proximity data .
[ 0177 ] Example 12. The method according to any one of examples 9-11 , wherein said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects . ( 0178 ] Example 13. The method according to any one of examples 1-12 , wherein said method further comprises generating a predicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0179 ] Example 14. The method according to any one of examples 4-13 , wherein said generating a score further comprises a second score component based on said pre dicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0180 ] Example 15. The method according to any one of examples 9-14 , wherein said electronic positioning data is collected using one or more electronic devices . [ 0181 ] Example 16. The method of example 15 , wherein said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated elec tronic device . [ 0182 ] Example 17. The method according to any one of examples 4-16 , further comprising vaccinating said subjects according to said score . [ 0183 ] Example 18. The method according to any one of examples 4-17 , wherein said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0184 ] Example 19. The method according to any one of examples 4-18 , wherein said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0185 ] Example 20. The method according to any one of examples 9-19 , wherein said electronic positioning data comprises geographical location data . [ 0186 ] Example 21. The method according to any one of examples 1-20 , wherein said physical proximity information comprises historical location data . [ 0187 ] Example 22. The method according to any one of examples 4-21 , wherein said generating said score further comprises a component comprising historical health data . [ 0188 ] Example 23. The method according to any one of examples 4-22 , wherein said generating said score further comprises a component comprising a profession in record of said subject . [ 0189 ] Example 24. The method according to any one of examples 1-23 , wherein said physical proximity information further comprises information received from a third party . [ 0190 ] Example 25. The method according to any one of examples 1-24 , wherein said physical proximity information is provided by said subject actively . [ 0191 ] Example 26. The method according to any one of examples 1-25 , wherein said physical proximity information is provided by said subject passively by means of said one or more electronic devices . [ 0192 ] Example 27. The method according to any one of examples 1-26 , wherein said pathogen is a virus . [ 0193 ] Example 28. The method according to any one of examples 1-27 , wherein said virus is a corona virus . [ 0194 ] Example 29. The method according to any one of examples 1-28 , wherein said virus is SARS - CoV . [ 0195 ] Example 30. The method according to any one of examples 1-28 , wherein said virus is MERS - CoV .

US 2021/0082583 A1 Mar. 18 , 2021 7
[ 0196 ] Example 31. The method according to any one of examples 1-28 , wherein said virus is SARS - CoV - 2 . [ 0197 ] Example 32. The method according to any one of examples 1-27 , wherein said virus is an influenza virus . [ 0198 ] Example 33. The method according to any one of examples 1-32 , wherein said disease results in influenza like symptoms . [ 0199 ] Example 34. A method of selecting subjects for being vaccinated against an infectious disease caused by a pathogen , comprising : [ 0200 ] a . automatically collecting physical proximity information of a subject with other subjects ; [ 0201 ] b . generating a predicted likelihood of said subject of transmitting said virus based on said physical proximity information ; [ 0202 ] c . generating a score comprising a first score com ponent based on said predicted likelihood of said subject of transmitting said virus ; [ 0203 ] d . repeating steps b - c for a plurality of subjects ; and [ 0204 ] e . prioritizing vaccination of said subjects accord ing to said score . [ 0205 ] Example 35. The method according to example 34 , wherein said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0206 ] Example 36. The method according to any one of examples 34-35 , wherein said disease is endemic or pan demic . [ 0207 ] Example 37. The method according to any one of examples 34-36 , wherein said generating said score further comprises a score component based on a nature of a location where said physical proximity information is related . [ 0208 ] Example 38. The method according to any one of examples 34-37 , wherein said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non - ventilated indoor space and any combination thereof . [ 0209 ] Example 39. The method according to any one of examples 34-38 , wherein when said physical proximity information is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . Example 40. The method according to any one of examples 34-39 , wherein said physical proximity information is physical proximity data received by means of electronic positioning data of said subject . [ 0210 ] Example 41. The method according to any one of examples 34-40 , wherein said physical proximity informa tion is physical proximity data of the location of said subject in relation to the location of other subjects . [ 0211 ] Example 42. The method according to any one of examples 38-41 , wherein said physical proximity data com prises one or more of physical proximity distance data , duration of physical proximity data and / or ambience of physical proximity data . [ 0212 ] Example 43. The method according to any one of examples 38-42 , wherein said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects . [ 0213 ] Example 44. The method according to any one of examples 38-43 , wherein said method further comprises generating a predicted likelihood of said subject contracting said pathogen based on said physical proximity data .
[ 0214 ] Example 45. The method according to any one of examples 34-44 , wherein said generating a score further comprises a second score component based on said pre dicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0215 ] Example 46. The method according to any one of examples 38-45 , wherein said electronic positioning data is collected using one or more electronic devices . Example 47 . The method according to example 46 , wherein said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated electronic device . [ 0216 ] Example 48. The method according to any one of examples 34-47 , further comprising vaccinating said sub jects according to said score . [ 0217 ] Example 49. The method according to any one of examples 34-48 , wherein said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0218 ] Example 50. The method according to any one of examples 34-49 , wherein said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0219 ] Example 51. The method according to any one of examples 38-50 , wherein said electronic positioning data comprises geographical location data . [ 0220 ] Example 52. The method according to any one of examples 34-51 , wherein said physical proximity informa tion comprises historical location data . [ 0221 ] Example 53. The method according to any one of examples 34-52 , wherein said generating said score further comprises a component comprising historical health data . [ 0222 ] Example 54. The method according to any one of examples 34-53 , wherein said generating said score further comprises a component comprising a profession in record of said subject . [ 0223 ] Example 55. The method according to any one of examples 34-54 , wherein said physical proximity informa tion further comprises information received from a third party . [ 0224 ] Example 56. The method according to any one of examples 34-55 , wherein said physical proximity informa tion is provided by said subject actively . [ 0225 ] Example 57. The method according to any one of examples 34-56 , wherein said physical proximity informa tion is provided by said subject passively by means of said one or more electronic devices . [ 0226 ] Example 58. The method according to any one of examples 34-57 , wherein said pathogen is a virus . [ 0227 ] Example 59. The method according to any one of examples 34-58 , wherein said virus is a corona virus . ( 0228 ] Example 60. The method according to any one of examples 34-58 , wherein said virus is SARS - CoV . [ 0229 ] Example 61. The method according to any one of examples 34-58 , wherein said virus is MERS - CoV . [ 0230 ] Example 62. The method according to any one of examples 34-58 , wherein said virus is SARS - CoV - 2 . [ 0231 ] Example 63. The method according to any one of examples 1-57 , wherein said virus is an influenza virus . [ 0232 ] Example 64. The method according to any one of examples 1-63 , wherein said disease results in influenza like symptoms . [ 0233 ] Example 65. A system for selecting subjects for being vaccinated against an infectious disease caused by a pathogen , comprising :

US 2021/0082583 A1 Mar. 18 , 2021 8
[ 0234 ] a . at least one server comprising a memory ; [ 0235 ] b . an analytics module ; [ 0236 ] c . a database module ; [ 0237 ] d . a simulation module ; [ 0238 ] said memory in said at least one server comprising instructions , said instructions comprising : [ 0239 ] i . generating , by circuitry , a predicted likelihood of said subject of transmitting said pathogen based on said physical proximity information , for a plurality of subjects ; [ 0240 ] ii . selecting subjects of said plurality of subjects for vaccinating based on a prediction that said vaccinating said subjects will reduce a likelihood of spreading of said disease in said plurality of subjects , wherein said selecting is based on said generated predicted likelihood . [ 0241 ] Example 66. The system according to example 65 , wherein said pathogen is selected from the group consisting of a virus , a bacterium , a fungus and a protozoan . [ 0242 ] Example 67. The system according to any one of examples 65-66 , wherein said disease is endemic or pan demic . ( 0243 ] Example 68. The system according to any one of examples 65-67 , wherein said predicted likelihood of said subject of transmitting said pathogen comprises one or more score components used for generating a score . [ 0244 ] Example 69. The system according to example 68 , wherein said score relates to a predicted likelihood of a group of subjects transmitting said pathogen based on said physical proximity information , and said physical proximity information is a first score component used for said gener ating said score . [ 0245 ] Example 70. The system according to any one of examples 64-69 , wherein said generating said score further comprises a score component based on a nature of a location where said physical proximity information is related . [ 0246 ] Example 71. The system of example 70 , wherein said nature of the location is one or more of an open space , a closed space , indoor , outdoor , ventilated indoor space , non - ventilated indoor space and any combination thereof . [ 0247 ] Example 72. The system according to any one of examples 65-71 , wherein when said physical proximity information is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times . [ 0248 ] Example 73. The system according to any one of examples 65-72 , wherein said physical proximity informa tion is physical proximity data received by means of elec tronic positioning data of said subject . [ 0249 ] Example 74. The system according to any one of examples 65-73 , wherein said physical proximity informa tion is physical proximity data of the location of said subject in relation to the location of other subjects . [ 0250 ] Example 75. The system according to any one of examples 69-74 , wherein said physical proximity data com prises one or more of physical proximity distance data , duration of physical proximity data and / or ambience of physical proximity data . [ 0251 ] Example 76. The system according to any one of examples 69-75 , wherein said electronic positioning data is one or more of electronic geographical positioning data of said subject , electronic proximity positioning data of said subject relative to other subjects . [ 0252 ] Example 77. The system according to any one of examples 65-76 , wherein said method further comprises
generating a predicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0253 ] Example 78. The system according to any one of examples 64-77 , wherein said generating a score further comprises a second score component based on said pre dicted likelihood of said subject contracting said pathogen based on said physical proximity data . [ 0254 ] Example 79. The system according to any one of examples 69-78 , wherein said electronic positioning data is collected using one or more electronic devices . [ 0255 ] Example 80. The system according to example 79 , wherein said one or more electronic devices are one or more of a smartphone , a tablet , a smartwatch and a dedicated electronic device . [ 0256 ] Example 81. The system according to any one of examples 64-80 , further comprising vaccinating said sub jects according to said score . [ 0257 ] Example 82. The system according to any one of examples 64-81 , wherein said generating a score further comprises a third score component reflecting relative health risk to said subject if said subject contracts said pathogen . [ 0258 ] Example 83. The system according to any one of examples 64-82 , wherein said generating a score further comprises a fourth score component reflecting damage to society if said subject contracts said pathogen . [ 0259 ] Example 84. The system according to any one of examples 69-83 , wherein said electronic positioning data comprises geographical location data . [ 0260 ] Example 85. The system according to any one of examples 65-84 , wherein said physical proximity informa tion comprises historical location data . [ 0261 ] Example 86. The system according to any one of examples 64-85 , wherein said generating said score further comprises a component comprising historical health data . [ 0262 ] Example 87. The system according to any one of examples 64-86 , wherein said generating said score further comprises a component comprising a profession in record of said subject . [ 0263 ] Example 88. The system according to any one of examples 65-87 , wherein said physical proximity informa tion further comprises information received from a third party . [ 0264 ] Example 89. The system according to any one of examples 65-88 , wherein said physical proximity informa tion is provided by said subject actively . [ 0265 ] Example 90. The system according to any one of examples 65-89 , wherein said physical proximity informa tion is provided by said subject passively by means of said one or more electronic devices . [ 0266 ] Example 91. The system according to any one of examples 65-90 , wherein said simulation module further comprises a prediction module . [ 0267 ] Example 92. The system according to any one of examples 65-91 , wherein said pathogen is a virus . [ 0268 ] Example 93. The system according to any one of examples 65-92 , wherein said virus is a corona virus . [ 0269 ] Example 94. The system according to any one of examples 65-92 , wherein said virus is SARS - CoV . [ 0270 ] Example 95. The system according to any one of examples 65-92 , wherein said virus is MERS - CoV . [ 0271 ] Example 96. The system according to any one of examples 65-91 , wherein said virus is SARS - CoV - 2 . [ 0272 ] Example 97. The system according to any one of examples 65-91 , wherein said virus is an influenza virus .

US 2021/0082583 A1 Mar. 18 , 2021 9
[ 0273 ] Example 98. The system according to any one of examples 65-92 wherein said disease results in influenza like symptoms . [ 0274 ] Unless otherwise defined , all technical and / or sci entific terms used herein have the same meaning as com monly understood by one of ordinary skill in the art to which the invention pertains . Although methods and materials similar or equivalent to those described herein can be used in the practice or testing of embodiments of the invention , exemplary methods and / or materials are described below . In case of conflict , the patent specification , including defini tions , will control . In addition , the materials , methods , and examples are illustrative only and are not intended to be necessarily limiting . [ 0275 ] As will be appreciated by one skilled in the art , some embodiments of the present invention may be embod ied as a system , method or computer program product . Accordingly , some embodiments of the present invention may take the form of an entirely hardware embodiment , an entirely software embodiment ( including firmware , resident software , micro - code , etc. ) or an embodiment combining software and hardware aspects that may all generally be referred to herein as a “ circuit , ” “ module ” or “ system . ” Furthermore , some embodiments of the present invention may take the form of a computer program product embodied in one or more computer readable medium ( s ) having com puter readable program code embodied thereon . Implemen tation of the method and / or system of some embodiments of the invention can involve performing and / or completing selected tasks manually , automatically , or a combination thereof . Moreover , according to actual instrumentation and equipment of some embodiments of the method and / or system of the invention , several selected tasks could be implemented by hardware , by software or by firmware and / or by a combination thereof , e.g. , using an operating system . [ 0276 ] For example , hardware for performing selected tasks according to some embodiments of the invention could be implemented as a chip or a circuit . As software , selected tasks according to some embodiments of the invention could be implemented as a plurality of software instructions being executed by a computer using any suitable operating system . In an exemplary embodiment of the invention , one or more tasks according to some exemplary embodiments of method and / or system as described herein are performed by a data processor , such as a computing platform for executing a plurality of instructions . Optionally , the data processor includes a volatile memory for storing instructions and / or data and / or a non - volatile storage , for example , a magnetic hard - disk and / or removable media , for storing instructio and / or data . Optionally , a network connection is provided as well . A display and / or a user input device such as a keyboard or mouse are optionally provided as well . [ 0277 ] Any combination of one or more computer read able medium ( s ) may be utilized for some embodiments of the invention . The computer readable medium may be a computer readable signal medium or a computer readable storage medium . A computer readable storage medium may be , for example , but not limited to , an electronic , magnetic , optical , electromagnetic , infrared , or semiconductor system , apparatus , or device , or any suitable combination of the foregoing . More specific examples ( a non - exhaustive list ) of the computer readable storage medium would include the following : an electrical connection having one or more
wires , a portable computer diskette , a hard disk , a random access memory ( RAM ) , a read - only memory ( ROM ) , an erasable programmable read - only memory ( EPROM or Flash memory ) , an optical fiber , a portable compact disc read - only memory ( CD - ROM ) , an optical storage device , a magnetic storage device , or any suitable combination of the foregoing . In the context of this document , a computer readable storage medium may be any tangible medium that can contain , or store a program for use by or in connection with an instruction execution system , apparatus , or device . [ 0278 ] A computer readable signal medium may include a propagated data signal with computer readable program code embodied therein , for example , in baseband or as part of a carrier wave . Such a propagated signal may take any of a variety of forms , including , but not limited to , electro magnetic , optical , or any suitable combination thereof . A computer readable signal medium may be any computer readable medium that is not a computer readable storage medium and that can communicate , propagate , or transport a program for use by or connection with an instruction execution system , apparatus , or device . [ 0279 ] Program code embodied on a computer readable medium and / or data used thereby may be transmitted using any appropriate medium , including but not limited to wire less , wireline , optical fiber cable , RF , etc. , or any suitable combination of the foregoing . [ 0280 ] Computer program code for carrying out opera tions for some embodiments of the present invention may be written in any combination of one or more programming languages , including an object oriented programming lan guage such as Java , Smalltalk , C ++ or the like and conven tional procedural programming languages , such as the “ C ” programming language or similar programming languages . The program code may execute entirely on the user's computer , partly on the user's computer , as a stand - alone software package , partly on the user's computer and partly on a remote computer or entirely on the remote computer or server . In the latter scenario , the remote computer may be connected to the user's computer through any type of network , including a local area network ( LAN ) or a wide area network ( WAN ) , or the connection may be made to an external computer ( for example , through the Internet using an Internet Service Provider ) . [ 0281 ] Some embodiments of the present invention may be described below with reference to flowchart illustrations and / or block diagrams of methods , apparatus ( systems ) and computer program products according to embodiments of the invention . It will be understood that each block of the flowchart illustrations and / or block diagrams , and combina tions of blocks in the flowchart illustrations and / or block diagrams , can be implemented by computer program instructions . These computer program instructions may be provided to a processor of a general purpose computer , special purpose computer , or other programmable data pro cessing apparatus to produce a machine , such that the instructions , which execute via the processor of the com puter or other programmable data processing apparatus , create means for implementing the functions / acts specified in the flowchart and / or block diagram block or blocks . [ 0282 ] These computer program instructions may also be stored in a computer readable medium that can direct a computer , other programmable data processing apparatus , or other devices to function in a particular manner , such that the instructions stored in the computer readable medium pro

US 2021/0082583 A1 Mar. 18 , 2021 10
Overview duce an article of manufacture including instructions which implement the function / act specified in the flowchart and / or block diagram block or blocks . [ 0283 ] The computer program instructions may also be loaded onto a computer , other programmable data process ing apparatus , or other devices to cause a series of opera tional steps to be performed on the computer , other pro grammable apparatus or other devices to produce a computer implemented process such that the instructions which execute on the computer or other programmable apparatus provide processes for implementing the functions / acts specified in the flowchart and / or block diagram block or blocks . [ 0284 ] Some of the methods described herein are gener ally designed only for use by a computer , and may not be feasible or practical for performing purely manually , by a human expert . A human expert who wanted to manually perform similar tasks might be expected to use completely different methods , e.g. , making use of expert knowledge and / or the pattern recognition capabilities of the human brain , which would be vastly more efficient than manually going through the steps of the methods described herein .
BRIEF DESCRIPTION OF THE SEVERAL VIEWS OF THE DRAWINGS
[ 0285 ] Some embodiments of the invention are herein described , by way of example only , with reference to the accompanying drawings . With specific reference now to the drawings in detail , it is stressed that the particulars shown are by way of example and for purposes of illustrative discussion of embodiments of the invention . In this regard , the description taken with the drawings makes apparent to those skilled in the art how embodiments of the invention may be practiced . [ 0286 ] In the drawings : [ 0287 ] FIG . 1 is a schematic illustration of an exemplary definition of a superspreader , according to some embodi ments of the invention ; [ 0288 ] FIG . 2 is a flowchart of an exemplary embodiment of the invention , according to some embodiments of the invention ; [ 0289 ] FIG . 3 is a schematic flowchart of a method of calculating a weighted score , according to some embodi ments of the invention ; [ 0290 ] FIG . 4 is a schematic representation of an exem plary spreading network , according to some embodiments of the invention ; [ 0291 ] FIGS . 5a - f are flowcharts of exemplary methods for identifying superspreaders with high levels of anony mization , according to some embodiments of the invention ; [ 0292 ] FIG . 6 is a flowchart of a method of generating a score , according to some embodiments of the invention ; and [ 0293 ] FIG . 7 is a schematic representation of an exem plary system , according to some embodiments of the inven tion .
[ 0295 ] A broad aspect of some embodiments of the inven tion relates to reduce a pandemic by reducing a k value of infection in addition to and / or at the expense of reducing an RO value thereof . In some embodiments of the invention , this is achieved by identifying and vaccinating ( or otherwise preventing infection by ) persons who are potential super spreaders ( e.g. , people who , on the average , are expected to infect more than the average , for example , 1 , 2 , 3 or more or intermediate values of standard deviations from such aver age . This may result in effective lowering of RO and / or of effective herd immunity . Optionally , people are not mea sured by actual spreading , but rather by characteristics and / or behavior , which is expected to lead to greater spread ing than others . Optionally , such considerations also may be applied to below average in expected spreading , however , such people usually have a smaller overall effect on disease spread [ 0296 ] A broad aspect of some embodiments of the inven tion relates to using a prediction of individual behavior to decide on vaccination priority for that individual . In some embodiments of the invention , such prediction is based on past behavior of the individual . In some embodiments of the invention , an individual is given a score used for prioriti zation . In some embodiments of the invention , actual pri oritization may be based on a determination of the expected effect of such vaccination on spread of disease . Optionally , this determination is using a simulation of population dis ease spread . In some embodiments of the invention , how ever , people are evaluated as individuals . [ 0297 ] A broad aspect of some embodiments of the inven tion relates to soft - fail of vaccination prioritization , which avoids problems caused by imprecise automated tracking methods . In some embodiments of the invention , the use of imperfect information , which , on the one hand does not seriously damage the quality of scoring and , on the other hand , can be used to significantly increase privacy and / or ease of score collection is provided . It is noted that a mistake , for example , of 4 % , 8 % , 15 % or intermediate percentages in score of an individual or missing a potential super spreader will not have a significantly ( e.g. , a factor of 2 or more ) greater effect on a person ( e.g. , will not send such person into quarantine ) and / or the total efficacy of a vacci nation process . Also , even after such an effect , it is expected that the overall result is better than naïve or general classi fication - based vaccination prioritization . In some embodi ments of the invention , counting of contacts is allowed to be less precise . In some embodiments of the invention , identi fication of the quality of the contacts ( e.g. , indoor / outdoor , coughing behavior , actual proximity and / or existence of protective factors ) is allowed to be reduced and optionally carried out using less precise sensing means as provided , for example , by cellphones . Optionally or additionally , the identification of unique contacts is allowed to be less pre cise . [ 0298 ] An aspect of some embodiments of the invention relates to prioritizing vaccinations and / or prophylactic treat ments in a pandemic event by identifying potential super spreaders . In some embodiments , potential superspreaders are identified from a population before critical groups have been excluded . In some embodiments , potential super spreaders are identified from a population after critical groups have been excluded . In some embodiments , critical groups are for example , health care providers , essential
DESCRIPTION OF SPECIFIC EMBODIMENTS OF THE INVENTION
[ 0294 ] The present invention , in some embodiments thereof , relates to methods and systems of prioritizing vac cination / treatment and , more particularly , but not exclu sively , to methods and systems of prioritizing vaccination / treatment in a pandemic situation .
US 2021/0082583 A1 Mar. 18 , 2021 11
are
service provides and high - risk individuals . In some embodi ments , potential superspreaders are identified according to one or more of : their usual and / or expected level of activity , their usual and / or expected type of activity , their usual and / or expected health state , their belonging to a closed or open circle of connections , the kind of individuals a certain subject usually meets , the kind of individuals a certain subject has met and their actual sensed behavior . In some embodiments , the entire population ( with or without the critical groups ) , or a part of the population , such as a critical group or other group , are subjected to an analysis which provides each individual with a " superspreader score ” ( re ferred hereinafter just as “ score ” ) which reflects a likelihood of such a person acting as a superspreader and / or general expected ability of that person to spread the disease . In some embodiments , potential superspreaders identified according to a score in relation to other scores from the rest of the population . In some embodiments , potential super spreaders are identified according to a score in relation to a predetermined score generated by the system . In some embodiments , identified potential superspreaders having the highest score are vaccinated ( or provided with prophylactic treatments ) first . It should be appertained that the score may also be weighted with other information , such as criticality for infrastructure , social standing and / or risk form the dis ease or perceived risk to high - value members of society . [ 0299 ] An aspect of some embodiments of the invention relates to prioritizing vaccinations and / or prophylactic treat ments in a pandemic event according to a potential level of danger to the society . In some embodiments , the invention relates identification of individuals that , in case they were in a phase of infecting others with an infectious disease / virus / pathogen , it would potentially put everyone else in danger . For example , in the case where a subject is in potential contact with other people and those other people potentially meet a high number of individuals . For example , a subject that interacts face to face with health provider personnel , but does not belong to the health provides network . If that subject becomes infected , he / she can potentially infect a high number of health provider personnel , which will then , potentially , spread the infectious disease / virus / pathogen to a larger population . [ 0300 ] An aspect of some embodiments of the invention relates to protecting the privacy of individuals in a popula tion when their information is used for prioritizing vacci nations and / or prophylactic treatments in a pandemic event , optionally also according to a potential level of danger to the society . In some embodiments , actual names of individuals are encrypted and / or anonymized in the system . In some embodiments , only a device of an individual comprises the capabilities to translate between the actual name of the individual and the encrypted / anonymized user name . In some embodiments , the servers of the system comprise high levels of protection and / or encryption for the information stored therein . In some embodiments of the invention , even the device of the user stores a minimum of identifiable information , such as a score , but does not stores actual identities of persons met . [ 0301 ] In some embodiments of the invention , private information about a person's activity and / or persons they came in contact with and / or geolocations are maintained on that person's mobile device and used to determine a priority for that person ( e.g. , by assessing the number of contacts and overall risk of spreading disease due to typical behavior of
that person ) . Optionally , the mobile device is used to broad cast , optionally in an anonymous manner , the score , so that , it may be determined , for example , by a central computer , the distribution of scores across the population . It should be noted that the actual identification of the device and / or user is not needed , just the number of persons with each score , so this can be taken into account together with number and / or availability of vaccine doses , to plan a best dosing schedule . Optionally , the mobile device will receive a predetermined scale of scores from the system , which will be then used by the mobile device to translate the score in view of the scale of scores and communicate the user to get treatment and , optionally , the when and where . [ 0302 ] In some embodiments of the invention , once cal culated , such dosing schedule is broadcasted and each device can apply its score to the schedule to determine a priority , which is given to the device owner . Optionally , when arriving for a scheduled vaccination , the device owner is required to show that code and , optionally , proof that the telephone belongs to them . [ 0303 ] In one example , the local device calculates a score based on a user's medical information and behavior . Option ally is also receives behavior of those that person meets ( e.g. , transmitted to the device at proximity / contact of devices of those people ) . In some embodiments , the infor mation is stored without identification of source , except possibly a hash code , which , while can be used to detect that a certain device was “ met ” , it cannot be used to identify the device . In some embodiments , once this score ( e.g. , risk of contagion ) is calculated , the broadcasted information regarding number of vaccinations available and / or number of persons in each class is noted . In some embodiments , this data may be used to determine which vaccination priority the personal device score merits , for example , in the same manner as would be by a central computer ( e.g. , all scores above x , where there are y people with a score above x and y is the number of available vaccines ) . [ 0304 ] In some embodiments of the invention , broadcasts and data transmissions are digitally signed to prevent tam pering . This has a potential advantage of allowing more anonymous transmission method to be used ( e.g. , Tor ) . [ 0305 ] It should be noted that additionally or alternatively to a central processing , the calculation of the vaccine priority may be distributed between some or all of the mobile devices , for example , using parallelization methods known in the art , which optionally also prevent significant amount of information from passing through any particular device . [ 0306 ] In some embodiments of the invention , the device calculates the priority and determines when the device owner should be vaccinated , treated and / or tested . For example , the number and duration of persons in proximity to the device can be used to calculate a risk score . Optionally , medical information , such as susceptibility and / or risk of spreading by coughing is downloaded to the device . This is typically not a significant breach of anonymity , as the identity of the device is typically known to the medical record provider . In some embodiments of the invention , a person can apply to receive a rating , for example , based on importance , job ( e.g. , healthcare provider ) , being part of critical infrastructure and / or risk of death . Such rating may be provided in the form of a one - time code , which the person can enter into the device . In this manner , the device can

US 2021/0082583 A1 Mar. 18 , 2021 12
increase or decrease the risk score and / or priority of vacci nation , without any central authority being aware of the person's activities . [ 0307 ] In some embodiments of the invention , as the device calculates the person's score , it may generate warn ing to the device owner to avoid or reduce certain behavior . Optionally , such warning is tied to reduction in priority if not heeded . Optionally or additionally , the manually entered rating may affect such warnings . For example , socially promiscuous activity by a doctor may not merit such warn ing and / or may not reduce the doctor's score ( at least while activity is performed at an allowed location , such as a hospital , which location may be indicated as part of the rating ) , but will generate a warning or a sanction ( e.g. , if not heeded ) to a person without such rating . [ 0308 ] In some embodiments of the invention , when deciding if to allow entry of a person into a crowded location , such as a sports arena or a shopping mall , a user may be required to show their rating . [ 0309 ] A potential benefit of some embodiments of the invention is that rather than give out vaccination to critical workers , while placing the rest of society in a lockdown ( e.g. , complete or semi or otherwise restrictions ) , the total risk of spread may be reduced with a same or smaller number of vaccine doses . [ 0310 ] A potential benefit of some embodiments of the invention is self - policing . If a person does not install suitable software for tracking movements , such person may receive a lower priority of treatment / vaccination . Similarly , if a person leaves their device off , then such off - time can be noted and used to affect the score , or even can be used as an indication that that person is not at risk . [ 0311 ] In some embodiments of the invention , a process of using the method includes : [ 0312 ] ( a ) Learning the behavior of individuals . This may be done , for example , using existing contact tracking meth ods and / or using methods as discussed herein . [ 0313 ] Optionally , such learned behavior is maintained in privacy and / or collected in an anonymous manner or pro cessed as it is collected , to pr erve anonymity . [ 0314 ] ( b ) Scoring , which can be based , for example , on number , variety and / or quality of contacts , degree of bridg ing between subpopulations , risk to individual , risk to others the individual is in contact with other facts that affect spreading ( e.g. , chronic cough ) and / or existing immunity . [ 0315 ] ( c ) Inviting the individual to be vaccinated , option ally though software on an electronic device used for contact tracking . [ 0316 ] ( d ) Vaccination , optionally verified using the soft ware to identify the person being vaccinated . [ 0317 ] An aspect of some embodiments of the invention relates to identifying potential superspreaders without the use of personal data . In some embodiments , superspreaders are identified by providing an anonymous ID to each indi vidual , for example , when a dedicated application / software ( referred hereinafter as “ application ” or “ app ” ) is installed in an electronic device . In some embodiments , IDs are exchanged between electronic devices when in proximity to each other ( e.g. , to indicate a potentially infectious " meet ing ” of the device holders ) . In some embodiments , what is transmitted is only a part of such ID ( or an indication thereof ) , which potentially decreases the chances to identify the specific user . In some embodiments of the invention , even the partial IDs substantially unique ( e.g. , a random
number with more possibilities than the number of expected meetings ) . In some embodiments of the invention , the partial ID is selected to be non - unique , for example , including only 100 , 1000 , 10,000 or intermediate or smaller or greater possibilities . In some embodiments , prioritizing vaccina tions and / or prophylactic treatments in a pandemic event is performed according to a superspreader score calculated by the number of IDs collected by each user . [ 0318 ] An aspect of some embodiments of the invention relates to the quality of people an individual meets . In some embodiments of the invention , meeting with a person can be given a higher or lower weight , based on whether that person is himself a super spreader and / or tends to meet super spreaders and / or tends to meet others form many sub populations . In some embodiments of the invention , when two devices meet , they exchange their own score and / or number of contacts or other information , which is used to generate an indication of how much of a potential super spreader that person is . In some embodiments , such people may be given a higher weight . Optionally or additionally , persons who are from a same subpopulation and / or which have fewer contacts and / or which are met more often , are given a lower weight . [ 0319 ] An aspect of some embodiments of the invention relates to assessing the degree of contacts inside a subpopu lation and between subpopulations . Society often has bubbles ( subpopulations ) within which there is a lot of contact within the bubble but considerably less contact between bubbles . In such a context , a person who bridges between bubbles may be a greater threat of disease spread than a person with more overall contacts but most or all within the bubble . In some embodiments of the invention , a method is provided for assessing the degree to which a person is within bubbles and / or bridges between bubbles or between non - bubble subpopulations . For example , the method may be used to distinguish between a first person where 90 % of their contacts are within a strongly connected sub - group vs. a person where only 10 % of their contacts are to a same strongly sub - group vs a person where 90 % of contacts are to a strongly connected sub - group , but there are multiple ( exclusive ) such subgroups . [ 0320 ] In some embodiments of the invention , a distrib uted method of assessing the degree to which contacts of an individual are within a strongly connected or other type of bubble , is provided . An alternative view of such method is assessing a degree of diffusion , which may be correlated with a degree of propagation of disease . [ 0321 ] In some embodiments of the invention , some or all individuals are assigned a second ( or more ) ID which is transferred to people they meet at a probability lower than 100 % . Optionally , when two individuals meet they exchange not only their second ID , but also all second IDs they have collected . As with a regular ID , the second or further IDs may be more or less unique . When an individual device assesses the second IDs it collected , it will tend to have fewer IDs if it is within a bubble ( e.g. , because it will mainly have IDs within the bubble ) than if it interconnects bubbles ( e.g. , in which case it can have IDs from multiple bubbles ) . Optionally , the number of second IDs is used as a measure of diffusion of IDs in the contact network . In some embodi ments of the invention , the transfer of second IDs can be weighted ( and / or probability of transfer adjusted ) , for example , to better model the likely of transfer of disease , for example , weighted higher for IDs collected in closed spaces ,

US 2021/0082583 A1 Mar. 18 , 2021 13
at close distances or IDs received from a device owned by a person with a chronic cough and / or less if owner is known ( e.g. , recorded as such ) to be careful with facemasks or other protective gear . Such weighting may be used additionally or alternatively also for the other scores described herein . The score may be normalized to the period in which the score is collected . Such normalization may be alternatively or addi tionally applied to score based on the first ID . The normal ization may be non - linear ( e.g. , the score may increase faster at early times ) and may be different for different IDs and / or for different individual characteristic values . [ 0322 ] In some embodiments of the invention , the prob ability of transfer is preset ( e.g. , 0.01 % , 0.1 % , 1 % , 10 % or intermediate or smaller or greater percentages ) . Optionally or additionally , multiple additional IDs are provided , each one transferred at a different probability . Optionally , the preset probability is determined using a simulation . It is noted that with a very small transfer probability , there may not be sufficient diffusion of second ID values , while with a large probability , all individuals will collect all second IDs , given enough time . For example , a simulation of a contact network may be run with different preset transfer values to detect a value which allows to distinguish between typical sub - population sizes and / or which , within the measurement period , does not reflect diffusion of substantially all second IDs all over the network . Similarly , the degree of uniqueness of the second ID may be selected using such a simulation to ensure that the probability of a same second ID reaching an individual from two different subgroups is sufficiently low ( e.g. , below 10 % ) . [ 0323 ] An aspect of some embodiments of the invention relates to the political issues involved in vaccination priori tization . In some embodiments of the invention , using an objective measure of risk due to behavior allows vaccination selection without ( or less ) a political fiat of selecting groups and / or reducing political pressure applied to prefer a par ticular group , as the individuals are treated by prioritization software as individuals and do are not identified as or treated as belonging to particular groups . Also within a particular group , using an automated vaccination prioritization method can be used to reduce friction and argument . [ 0324 ] An aspect of some embodiments of the invention relates to encouraging users to use a dedicated application / software for tracking contacts ( and optionally identifying potential superspreaders either anonymized or not ) by pro viding vaccinations and / or prophylactic treatments first to those individuals that use the dedicated software . In some embodiments , individuals that use the dedicated software are those individuals that contribute to the overall benefit of the population , therefore are provided with vaccinations and / or prophylactic treatments before those who not . [ 0325 ] Before explaining at least one embodiment of the invention in detail , it is to be understood that the invention is not necessarily limited in its application to the details of construction and the arrangement of the components and / or methods set forth in the following description and / or illus trated in the drawings and / or the Examples . The invention is capable of other embodiments or of being practiced or carried out in various ways .
government must decide who will receive first the vaccine ! prophylactic treatment . According to studies , governments decide to provide the first doses of the treatment to the group of individuals that belong to : [ 0327 ] a ) Health care services , for example doctors , nurses , laboratories , hospitals , etc .; [ 0328 ] b ) Essential service services , for example police , fire fighters , public sector personnel , governmental person nel , etc .; and [ 0329 ] c ) High risk individuals , for example people with high risk of complications , pregnant women , children , etc. [ 0330 ] These individuals belong to a group called critical groups , due to the nature of their activity or due to their health status during pandemic times . Usually , critical groups amount to about 2 % to about 10 % of the total population of a country . [ 0331 ] After the critical groups have been vaccinated and / or provided prophylactic treatments , since the number of vaccinations / treatments is limited , there is the question who should be vaccinated / treated next . This is generally true also within a critical group or other group chosen for vaccination , for example , a group of less at risk individuals , such as males aged 50-60 . [ 0332 ] In some embodiments , the population is defined as a number of individuals between about 10 individuals and about 100 individuals , optionally between about 100 indi viduals and about 1,000 individuals , optionally between about 1,000 individuals and about 1,000,000 individuals , optionally up to 10,000,000 , optionally up to 100,000,000 , optionally up to the entire population of earth ( e.g. , 8 billion ) . Principals of Herd Immunity [ 0333 ] Before explaining the invention , the notion of herd immunity should be explained . Herd immunity ( also called herd effect , community immunity , population immunity , or social immunity ) is a form of indirect protection from infectious disease that occurs when a large percentage of a population has become immune ( resistant ) to an infection , whether through vaccination / prophylactic treatment or pre vious infections , thereby providing a measure of protection for individuals who are not immune . In a population in which a large proportion of individuals possess immunity , such people being unlikely to contribute to disease trans mission , chains of infection are more likely to be disrupted , which either stops or substantially slows the spread of disease . The greater the proportion of immune individuals in a community , the smaller the probability that non - immune individuals will come into contact with an infectious indi vidual , helping to shield non - immune individuals from infection . Individuals can become immune by recovering from an earlier infection or through vaccination / prophylac tic treatment . Some individuals cannot become immune because of medical conditions , such as an immunodefi ciency or immunosuppression , and for this group herd immunity is a crucial method of protection . Once a certain threshold has been reached , herd immunity gradually elimi nates a disease from a population . This elimination , if achieved worldwide , may result in the permanent reduction in the number of infections to zero , called eradication . For example , herd immunity created via vaccination / treatment contributed to the eventual eradication of smallpox in 1977 and has contributed to the reduction of the frequencies of other diseases . Herd immunity does not apply to all diseases ,
Definition of the Population [ 0326 ] During a pandemic , once a valid vaccine / prophy lactic drug becomes available , and the number of vaccines / drug doses is limited or not all available at the same time , the

US 2021/0082583 A1 Mar. 18 , 2021 14
( SSEVs ) took place in the context of ( 1 ) parties , ( 2 ) face to - face professional networking events and meetings , ( 3 ) religious gatherings , ( 4 ) sports events , ( 5 ) meat - processing facilities , ( 6 ) ships at sea , ( 7 ) singing groups , and ( 8 ) funerals .
Factors of Transmission
just those that are contagious , meaning that they can be transmitted from one individual to another . Tetanus , for example , is infectious but not contagious , so herd immunity does not apply . Herd immunity was recognized as a naturally occurring phenomenon in the 1930s when it was observed that after a significant number of children had become immune to measles , the number of new infections tempo rarily decreased , including among susceptible children . Mass vaccination / treatment to induce herd immunity has since become common and proved successful in preventing the spread of many infectious diseases . One of the main problems with achieving herd immunity is that there might be a limited number of vaccinations / treatments available to the population and mass vaccination / treatment is either not possible or it would take a long time to achieve herd immunity while the infectious disease continues to spread . [ 0334 ] It is a potential benefit of some embodiments of the invention to provide a method to resolve the problem of who to vaccinate / treat during a pandemic when a low amount of vaccine / treatment doses are available , while still providing an effective herd immunity , optionally by better targeting those individuals likely to pass on disease and vaccinating at least some of them , in a preferential manner .
[ 0343 ] Superspreaders have been identified who excrete a higher than normal number of pathogens during the time they are infectious . This causes their contacts be exposed to higher viral / bacterial loads than would be seen in the contacts of non - superspreaders with the same duration of exposure . This medical information may be available for at least some individuals , for example , if the epidemic is a recurring one , such as influenza . In addition , behavioral and medical attributes may also increase infectivity . For example , a chronic cough ( or one due to a temporary disease , which may be noted in a person's medical record ) may increase the degree to which an individual is conta gious . It is noted that coughs and sneezes ( and rate thereof ) can be detected automatically by a carried device , such as a cellphone , by signal analysis on an automatically and optionally continually ( or repeatedly discrete ) collected audio signal form the microphone . It is noted that an individual's cellphone or other electronic device may have access to a person medical records , by connecting to an EMR of that individual .
Basic Reproductive Number [ 0344 ] The basic reproduction number RO is the average number of secondary infections caused by a typical infective person in a totally susceptible population . The basic repro ductive number is found by multiplying the average number of contacts by the average probability that a susceptible individual will become infected , which is called the shed ding potential . The average number of contacts may further be weighed by quality of contact ( e.g. , length , repetition , distance , protective means and / or airflow quality )
RO = Number of contactsxShedding potential
Definition of Superspreaders [ 0335 ] A superspreader is an unusually contagious organ ism infected with a disease ( infectious disease / virus / patho gen ) . In the context of a human - borne illness , a super spreader is an individual who is more likely to infect others , compared with a typical infected person . [ 0336 ] Some cases of superspreading conform to the 80/20 rule , where approximately 20 % of infected individuals are responsible for 80 % of transmissions , although superspread ing can still be said to occur when superspreaders account for a higher or lower percentage of transmissions . In epi demics with such superspreader events ( SSEV ) , the majority of individuals infect relatively few secondary contacts . [ 0337 ] Although loose definitions of superspreader events exist , some effort has been made at defining what qualifies as a superspreader event ( SSEV ) . Lloyd - Smith et al . ( 2005 ) define a protocol to identify a superspreader event as fol lows : [ 0338 ] a . estimate the effective reproductive number , R , for the disease and population in question ; [ 0339 ] b . construct a Poisson distribution with mean R , representing the expected range of Z due to stochasticity without individual variation ; [ 0340 ] C. define an SSEV as any infected person who infects more than Z ( n ) others , where Z ( n ) is the nth percen tile of the Poisson ( R ) distribution . [ 0341 ] This protocol defines a 99th - percentile SSEV as a case , which causes more infections than would occur in 99 % of infectious histories in a homogeneous population . For example , during the SARS - CoV - 1 2002-2004 SARS out break from China , epidemiologists defined a superspreader as an individual with at least eight transmissions of the disease . Furthermore , superspreaders may or may not show any symptoms of the disease . In the methods described here , a threshold ( or scale ) for being a superspreader may be defined manually and / or determined by analyzing actual contact - transmission data collected manually and / or auto matically . [ 0342 ] Putting aside hospitals , private residences and old age homes , almost all of these superspreader events
Individual Reproductive Number [ 0345 ] The individual reproductive number represents the number of secondary infections caused by a specific indi vidual during the time that individual is infectious . Some individuals have significantly higher than average individual reproductive numbers and are known as superspreaders . Through contact tracing , epidemiologists have identified superspreaders in measles , tuberculosis , rubella , monkey pox , smallpox , Ebola hemorrhagic fever and SARS . Co - Infections with Other Pathogens [ 0346 ] Studies have shown that men with HIV who are co - infected with at least one other sexually transmitted disease , such as gonorrhea , hepatitis C , and herpes simplex 2 virus , have a higher HIV shedding rate than men without co - infection . This shedding rate was calculated in men with similar HIV viral loads . Once treatment for the co - infection has been completed , the HIV shedding rate returns to levels comparable to men without co - infection . Therefore , it could be hypothesized that in case of viral diseases transmitted through fluids , people with other pathologies , like chronic coughing , could also be defined as superspreaders and are

US 2021/0082583 A1 Mar. 18 , 2021 15
optionally so defined , or weighted accordingly in some embodiments of the invention .
Exemplary Pathogens
[ 0347 ] In some embodiments , a pathogen may be one or more of a virus ( in pl . viruses ) , bacterium ( bacteria ) , fungus ( fungi ) or a protozoan ( protozoa ) , for example coronavirus ( COVID - 19 , SARS - CoV - 1 , SARS - CoV - 2 , MERS - CoV ) . In some embodiments , the pathogen may be a virus , and said virus is an influenza virus . In some embodiments , the disease results in influenza like symptoms . It should be understood , that where referred to “ virus ” and / or “ patho gen ” , any one of an “ infectious disease ” , a “ generic or specific pathogen " , a " generic or specific virus " are included , and the use of the term “ virus ” and / or “ pathogen ” is just to facilitate the explanation and they should include them .
[ 0348 ] In some embodiments of the invention , the disease is transmitted by respiratory means , for example , aerosol and / or droplets . Optionally , an electronic device , such as a cellphone is used to detect contact which may be sufficient to transmit ( e.g. , detecting proximity for example , using Bluetooth power ; detecting physical activity for example , buy analysis of an audio trace recorded from such device ; detecting being indoors or outdoors based on geolocation or based on other sensors on the cellphone that are affected by being indoors ( e.g. , echoes in audio ) .
Vaccinations and Prophylactic Treatments [ 0349 ] In some embodiments , the term vaccination means the administration of a vaccine to help the immune system develop protection from a disease . In some embodiments , vaccines contain a microorganism or virus in a weakened , live or killed state , or proteins or toxins from the organism . In some embodiments , in stimulating the body's adaptive immunity , they help prevent sickness from an infectious disease . In some embodiments , as stated above , when a sufficiently large percentage of a population has been vac cinated , herd immunity results . [ 0350 ] In some embodiments , the term prophylactic treat ment means a preventive measure taken to fend off a disease or another unwanted consequence . [ 0351 ] In order to facilitate the explanation of the inven tion , the term " treatment ” will be used . It should be under stood that when the term " treatment ” is used it refers to both vaccinations and prophylactic treatment . [ 0352 ] In some embodiments , vaccines are all compounds as disclosed in in the website of the World Health Organi zation ( https : // www [ dot ] who [ dot ] int / publications / m / item / draft - landscape - of - covid - 19 - candidate - vaccines ) , which are all incorporated herein by reference , and which are option ally provided ( e.g. , as a kit ) with software such as described herein and / or provided with instructions for use targeting potential super spreaders detected , for example , using meth ods and apparatus as described herein , and include the following : 28 candidate vaccines in clinical evaluation
COVID - 19 Vaccine
developer manufacturer
Type of candidate vaccine
Vaccine platform
Number of
doses
Route of
Admin istration
Timing of
doses
Clinical Stage
Phase 1 Phase 1/2 Phase 2 Phase 3
ChAdOxl - S 1 IM 2020-001228-32 University of Oxford / AstraZeneca
Non Replicating
Viral
ISR CTN
89951424 Vector
PACTR 202006922165132 2020-001072-15
Interim Report
NCT04383574 NCT04352608
Chi
Sinovac Inactivated Inactivated 2 IM NCT 04456595
Chi Wuhan Inactivated Inactivated
0 , 14 days
0 , 14 or 0 , 21 days
2 IM CTR CTR
2000031809 2000034780
Inactivated Inactivated 2 IM Chi
Institute of Biological Products / Sinopharm Beijing
Institute of Biological Products / Sinopharm Moderna / NIAID
0 , 14 or 0 , 21 days
Chi CTR
2000032459 CTR
2000034780
RNA LNP 2 IM NCT NCT04405076 NCT04470427 0 , 28 days 04283461 encapsulated
mRNA Interim Report
RNA 3 LNP 2 IM NCT BioNTech / FosunPharma /
Pfizer
0 , 28 days
2020-001038-36 Chi mRNAS 04368728 CTR
2000034825 1 IM CanSino
Biological Inc./Beijing Institute of
Biotechnology
Non Replicating
Viral
Adenovirus Type 5 Vector
Chi CTR
Chi CTR
2000031781 Study Report
2000030906 Vector Study Report
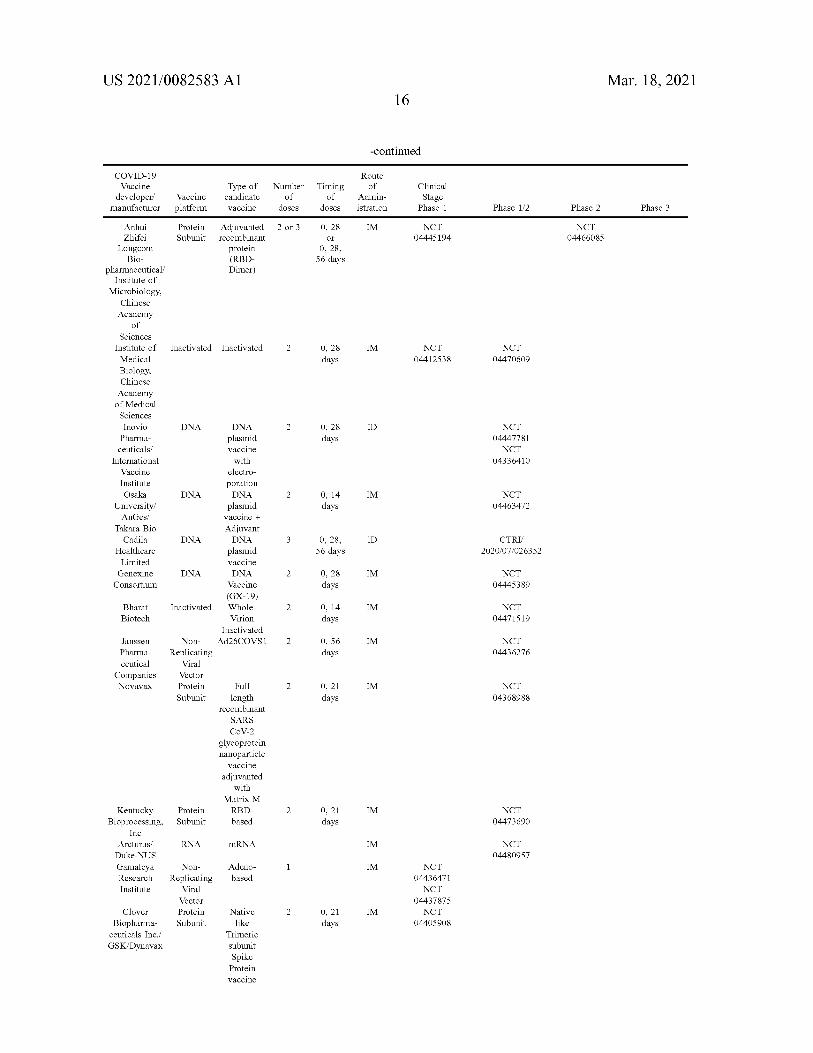
US 2021/0082583 A1 Mar. 18 , 2021 16
-continued
COVID - 19 Vaccine
developer manufacturer
Type of candidate vaccine
Vaccine platform
Number of
doses
Route of
Admin istration
Timing of
doses
Clinical Stage
Phase 1 Phase 1/2 Phase 2 Phase 3
2 or 3 IM Protein Subunit
0 , 28 or
0 , 28 ,
NCT 04445194
Adjuvanted recombinant
protein ( RBD Dimer )
NCT 04466085
56 days
Inactivated Inactivated 2 0 , 28 IM NCT 04412538
NCT 04470609 days
Anhui Zhifei
Longcom Bio
pharmaceutical / Institute of
Microbiology , Chinese Academy
of Sciences
Institute of Medical Biology , Chinese Academy of Medical Sciences Inovio Pharma ceuticals /
International Vaccine Institute Osaka
University / AnGes /
Takara Bio Cadila
Healthcare Limited Genexine Consortium
DNA 2 0 , 28 ID days
NCT 04447781 NCT
04336410
DNA 2 IM 0 , 14 days
NCT 04463472
DNA plasmid vaccine with
electro poration DNA
plasmid vaccine + Adjuvant DNA
plasmid vaccine DNA
Vaccine ( GX - 19 ) Whole Virion
Inactivated Ad26COVS1
DNA 3 0 , 28 , ID CTRI 2020/07/026352 56 days
DNA 2 0 , 28 IM NCT 04445389 days
Inactivated 2 0 , 14 IM Bharat Biotech
NCT 04471519 days
2 IM 0 , 56 days
NCT 04436276
Janssen Pharma ceutical
Companies Novavax
Non Replicating
Viral Vector Protein Subunit
2 IM 0 , 21 days
NCT 04368988
Full length
recombinant SARS COV - 2
glycoprotein nanoparticle
vaccine adjuvanted
with Matrix M RBD based
2 IM Protein Subunit
0 , 21 days
NCT 04473690
RNA mRNA IM
Kentucky Bioprocessing ,
Inc Arcturus / Duke - NUS Gamaleya Research Institute
NCT 04480957
1 IM Adeno based
Non Replicating
Viral Vector Protein Subunit
NCT 04436471 NCT
04437875 NCT
04405908 2 IM 0 , 21
days Clover
Biopharma ceuticals Inc./ GSK / Dynavax
Native like
Trimeric subunit Spike Protein vaccine
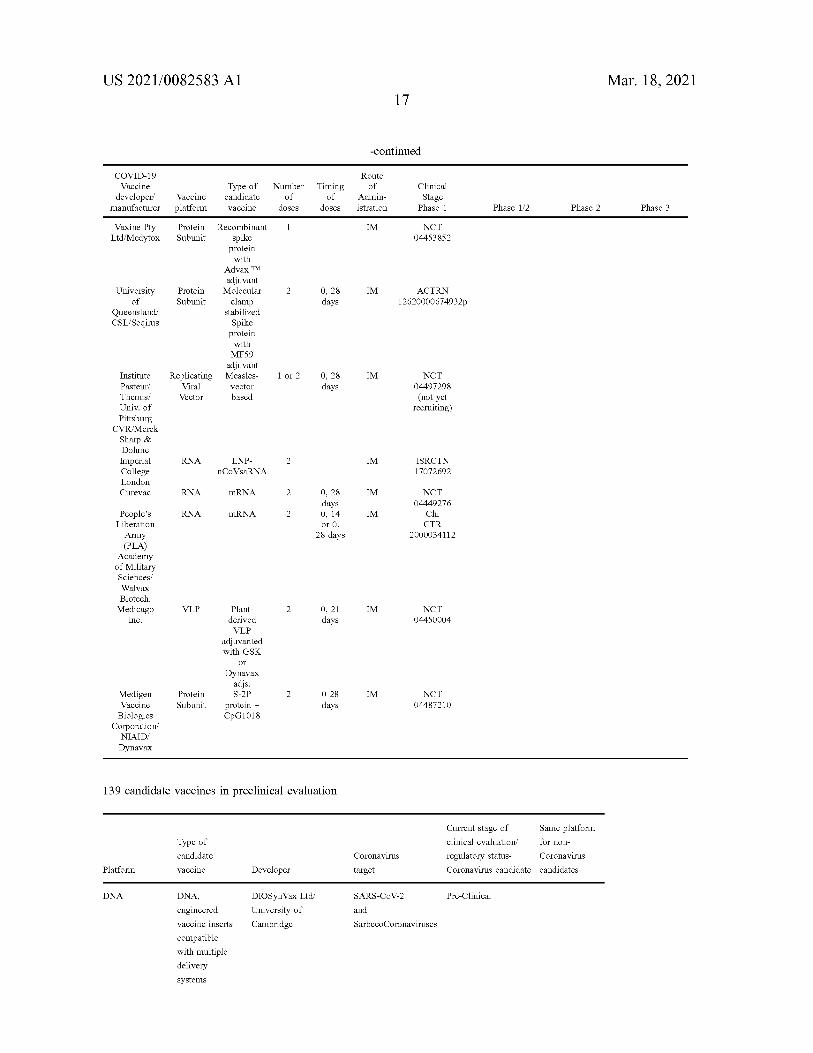
US 2021/0082583 A1 Mar. 18 , 2021 17
-continued
Type of COVID - 19 Vaccine
developer manufacturer
Vaccine platform
Route of
Admin istration
Number of
doses candidate vaccine
Timing of
doses
Clinical Stage
Phase 1 Phase 1/2 Phase 2 Phase 3
1 IM Vaxine Pty Ltd / Medytox
Protein Subunit
NCT 04453852
2 Protein Subunit
0 , 28 IM University of
Queensland / CSL / Seqirus
ACTRN 12620000674932p days
Recombinant spike
protein with
Advax TM adjuvant Molecular clamp
stabilized Spike protein with MF59
adjuvant Measles vector based
1 or 2 0 , 28 IM Replicating Viral Vector
days NCT
04497298 ( not yet
recruiting )
Institute Pasteur / Themis / Univ . of Pittsburg
CVR / Merck Sharp & Dohme Imperial College London Curevac
RNA 2 IM LNP nCoVsaRNA
ISRCTN 17072692
RNA mRNA 2 0 , 28 IM days
RNA mRNA 2 IM 0 , 14 or 0 ,
NCT 04449276
Chi CTR
2000034112 28 days
People's Liberation Army ( PLA )
Academy of Military Sciences / Walvax Biotech . Medicago
Inc. VLP 2 IM 0 , 21
days NCT
04450004 Plant derived VLP
adjuvanted with GSK
or Dynavax
adjs . S - 2P
protein + CpG1018
2 IM Protein Subunit
0 28 days
NCT 04487210
Medigen Vaccine Biologics
Corporation NIAID / Dynavax
139 candidate vaccines in preclinical evaluation
Type of Current stage of Same platform clinical evaluation for non regulatory status- Coronavirus Coronavirus candidate candidates
candidate Coronavirus
Platform vaccine Developer target
DNA SARS - CoV - 2 Pre - Clinical DIOSynVax Ltd University of Cambridge
and
SarbecoCoronaviruses
DNA , engineered vaccine inserts compatible with multiple delivery systems
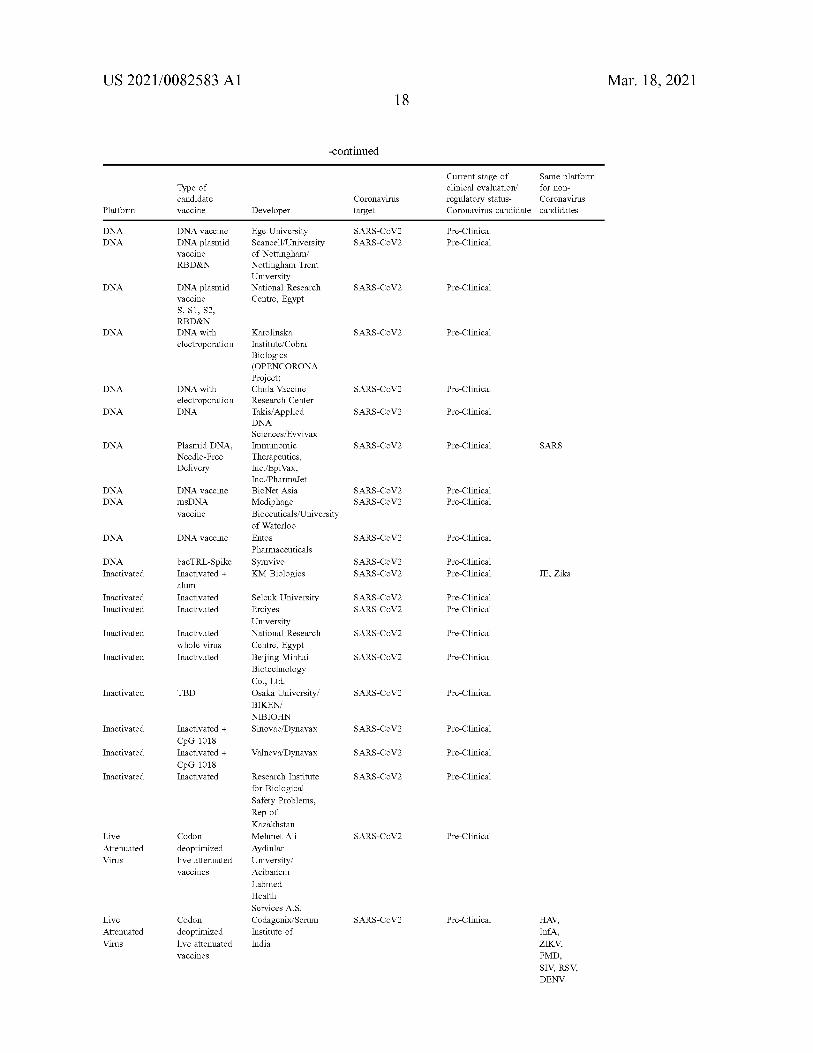
US 2021/0082583 A1 Mar. 18 , 2021 18
-continued
Type of Current stage of Same platform clinical evaluation for non regulatory status- Coronavirus Coronavirus candidate candidates
candidate vaccine
Coronavirus target Platform Developer
DNA DNA
SARS - CoV2 SARS - CoV2
Pre - Clinical Pre - Clinical
DNA vaccine DNA plasmid vaccine RBD & N
Ege University Scancell / University of Nottingham Nottingham Trent University National Research Centre , Egypt
DNA SARS - CoV2 Pre - Clinical DNA plasmid vaccine S , S1 , S2 , RBD & N DNA with electroporation
DNA SARS - CoV2 Pre - Clinical
DNA SARS - CoV2 Pre - Clinical DNA with electroporation DNA DNA SARS - CoV2 Pre - Clinical
DNA SARS - CoV2 Pre - Clinical SARS Plasmid DNA , Needle - Free Delivery
Karolinska Institute / Cobra Biologics ( OPENCORONA Project ) Chula Vaccine Research Center Takis / Applied DNA Sciences / Evvivax Immunomic Therapeutics , Inc./EpiVax , Inc./PharmaJet BioNet Asia Mediphage Bioceuticals / University of Waterloo Entos Pharmaceuticals Symvivo KM Biologics
DNA DNA
DNA vaccine msDNA vaccine
SARS - CoV2 SARS - CoV2
Pre - Clinical Pre - Clinical
DNA DNA vaccine SARS - CoV2 Pre - Clinical
DNA Inactivated
SARS - CoV2 SARS - CoV2
Pre - Clinical Pre - Clinical JE , Zika
bacTRL - Spike Inactivated + alum Inactivated Inactivated
Inactivated Inactivated
SARS - CoV2 SARS - CoV2
Pre - Clinical Pre - Clinical
Inactivated SARS - CoV2 Pre - Clinical Inactivated whole virus Inactivated Inactivated SARS - CoV2 Pre - Clinical
Selcuk University Erciyes University National Research Centre , Egypt Beijing Minhai Biotechnology Co. , Ltd. Osaka University BIKEN / NIBIOHN Sinovac / Dynavax
Inactivated TBD SARS - CoV2 Pre - Clinical
Inactivated SARS - CoV2 Pre - Clinical
Inactivated
Inactivated + CpG 1018 Inactivated + CpG 1018 Inactivated
Valneva / Dynavax SARS - CoV2 Pre - Clinical
Inactivated SARS - CoV2 Pre - Clinical Research Institute for Biological Safety Problems , Rep of
SARS - CoV2 Pre - Clinical Live Attenuated Virus
Codon deoptimized live attenuated vaccines
Kazakhstan Mehmet Ali Aydinlar University / Acibadem Labmed Health Services A.S. Codagenix / Serum Institute of India
SARS - CoV2 Pre - Clinical Live Attenuated Virus
Codon deoptimized live attenuated vaccines
HAV , InfA , ZIKV , FMD , SIV , RSV , DENV
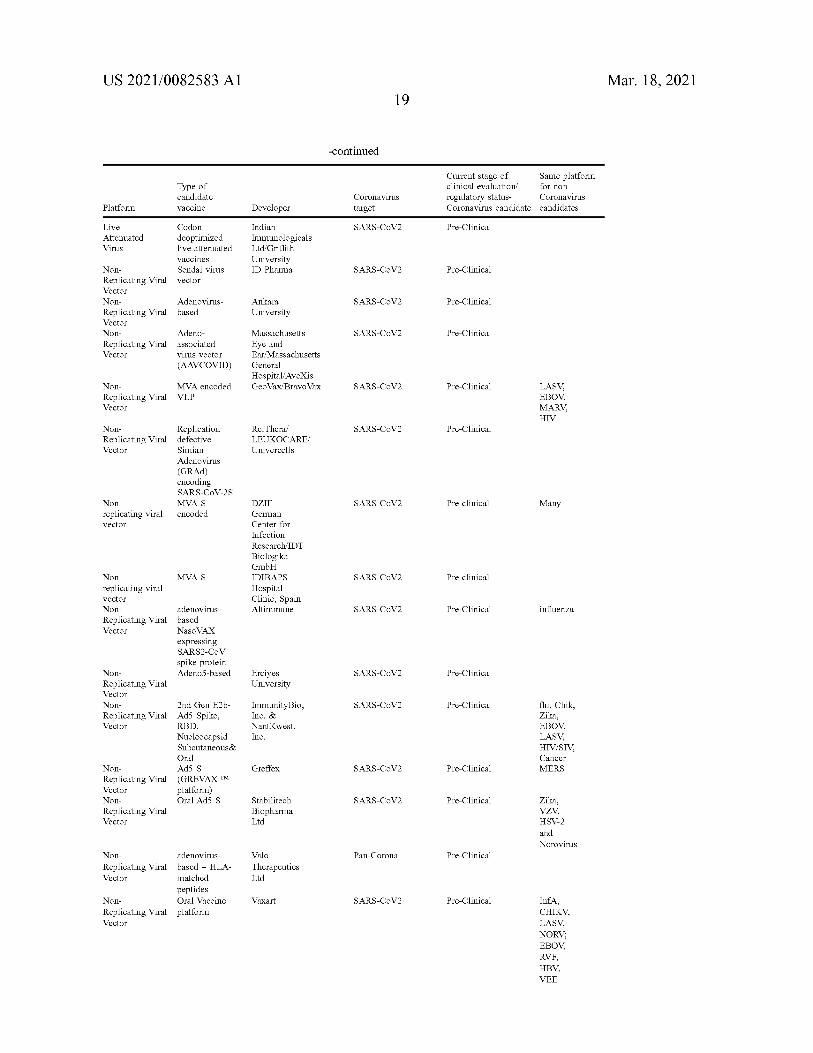
US 2021/0082583 A1 Mar. 18 , 2021 19
-continued
for non Type of candidate vaccine
Current stage of Same platform clinical evaluation regulatory status- Coronavirus Coronavirus candidate candidates
Coronavirus target Platform Developer SARS - CoV2 Pre - Clinical Live
Attenuated Virus
Codon deoptimized live attenuated vaccines Sendai virus vector
Indian Immunologicals Ltd Griffith University ID Pharma SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical
Non Replicating Viral Vector Non Replicating Viral Vector Non Replicating Viral Vector
Adenovirus based
Ankara University
Massachusetts SARS - CoV2 Pre - Clinical Adeno associated virus vector ( AAVCOVID )
Eye and Ear / Massachusetts General Hospital / AveXis Geo Vax / Bravo Vax SARS - CoV2 Pre - Clinical Non
Replicating Viral Vector
MVA encoded VLP
LASV , EBOV , MARV , HIV
SARS - CoV2 Pre - Clinical Non Replicating Viral Vector
ReiThera / LEUKOCARE / Univercells
Replication defective Simian Adenovirus ( GRAD ) encoding SARS - CoV - 2S MVA - S encoded
SARS - CoV2 Pre - clinical Many Non replicating viral vector
DZIF - German Center for Infection Research / IDT Biologika GmbH IDIBAPS Hospital Clinic , Spain Altimmune
MVA - S SARS - CoV2 Pre - clinical Non replicating viral vector Non Replicating Viral Vector
SARS - CoV2 Pre - Clinical influenza adenovirus based Naso VAX expressing SARS2 - COV spike protein Adeno 5 - based SARS - CoV2 Pre - Clinical Erciyes
University Non Replicating Viral Vector Non Replicating Viral Vector
SARS - CoV2 Pre - Clinical Immunity Bio , Inc. & NantKwest , Inc.
2nd Gen E2b Ad5 Spike , RBD , Nucleocapsid Subcutaneous & Oral Ad5 S ( GREVAX TM platform ) Oral Ad5 S
flu , Chik , Zika , EBOV , LASV , HIV / SIV , Cancer MERS Greffex SARS - CoV2 Pre - Clinical Non
Replicating Viral Vector Non Replicating Viral Vector
SARS - CoV2 Pre - Clinical Stabilitech Biopharma Ltd
Zika , VZV , HSV - 2 and Norovirus
Pan - Corona Pre - Clinical Valo Therapeutics Ltd
Non adenovirus Replicating Viral based + HLA Vector matched
peptides Non Oral Vaccine Replicating Viral platform Vector
Vaxart SARS - CoV2 Pre - Clinical InfA , CHIKV , LASV , NORV ; EBOV , RVF , HBV , VEE
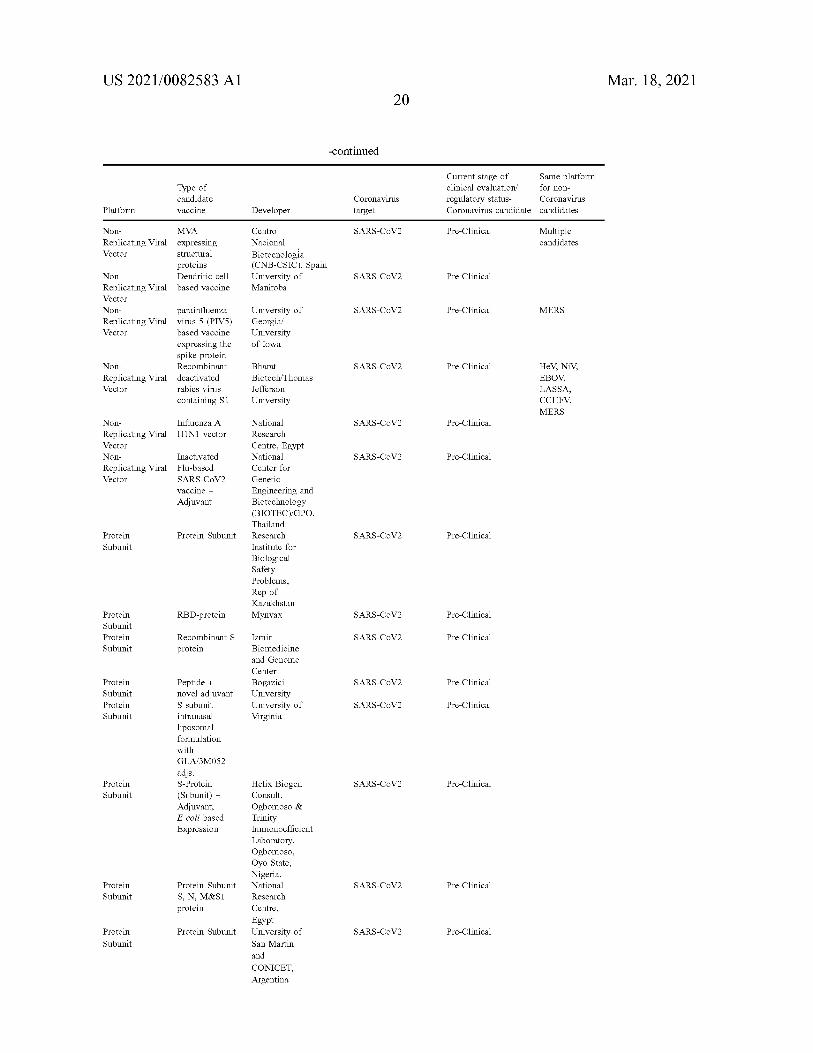
US 2021/0082583 A1 Mar. 18 , 2021 20
-continued
Type of Current stage of Same platform clinical evaluation / for non regulatory status- Coronavirus Coronavirus candidate candidates
candidate vaccine
Coronavirus target Platform Developer
SARS - CoV2 Pre - Clinical Multiple candidates
Centro Nacional Biotecnologia ( CNB - CSIC ) , Spain University of Manitoba
SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical MERS
Non MVA Replicating Viral expressing Vector structural
proteins Non Dendritic cell Replicating Viral based vaccine Vector Non parainfluenza Replicating Viral virus 5 ( PIV5 ) Vector based vaccine
expressing the spike protein
Non Recombinant Replicating Viral deactivated Vector rabies virus
containing S1
University of Georgia University of Iowa
SARS - CoV2 Pre - Clinical Bharat Biotech / Thomas Jefferson University
HeV , NIV , EBOV , LASSA , CCHFV , MERS
SARS - CoV2 Pre - Clinical Influenza A H1N1 vector
Non Replicating Viral Vector Non Replicating Viral Vector
SARS - CoV2 Pre - Clinical Inactivated Flu - based SARS - CoV2 vaccine + Adjuvant
National Research Centre , Egypt National Center for Genetic Engineering and Biotechnology ( BIOTEC ) / GPO , Thailand Research Institute for Biological Safety Problems ,
Protein Subunit . SARS - CoV2 Pre - Clinical Protein Subunit
Rep of Kazakhstan Mynvax RBD - protein SARS - CoV2 Pre - Clinical Protein
Subunit Protein Subunit
SARS - CoV2 Pre - Clinical Recombinant S protein
Izmir Biomedicine and Genome Center Bogazici University University of Virginia
SARS - CoV2 Pre - Clinical Protein Subunit Protein Subunit
SARS - CoV2 Pre - Clinical
Peptide + novel adjuvant S subunit intranasal liposomal formulation with GLA / 3M052 adjs . S - Protein ( Subunit ) + Adjuvant , E coli based Expression
SARS - CoV2 Pre - Clinical Protein Subunit
SARS - CoV2
Helix Biogen Consult , Ogbomoso & Trinity Immonoefficient Laboratory , Ogbomoso , Oyo State , Nigeria . National Research Centre , Egypt University of San Martin and CONICET , Argentina
Protein Subunit
Pre - Clinical Protein Subunit S , N , M & Si protein
Protein Subunit SARS - CoV2 Pre - Clinical Protein Subunit
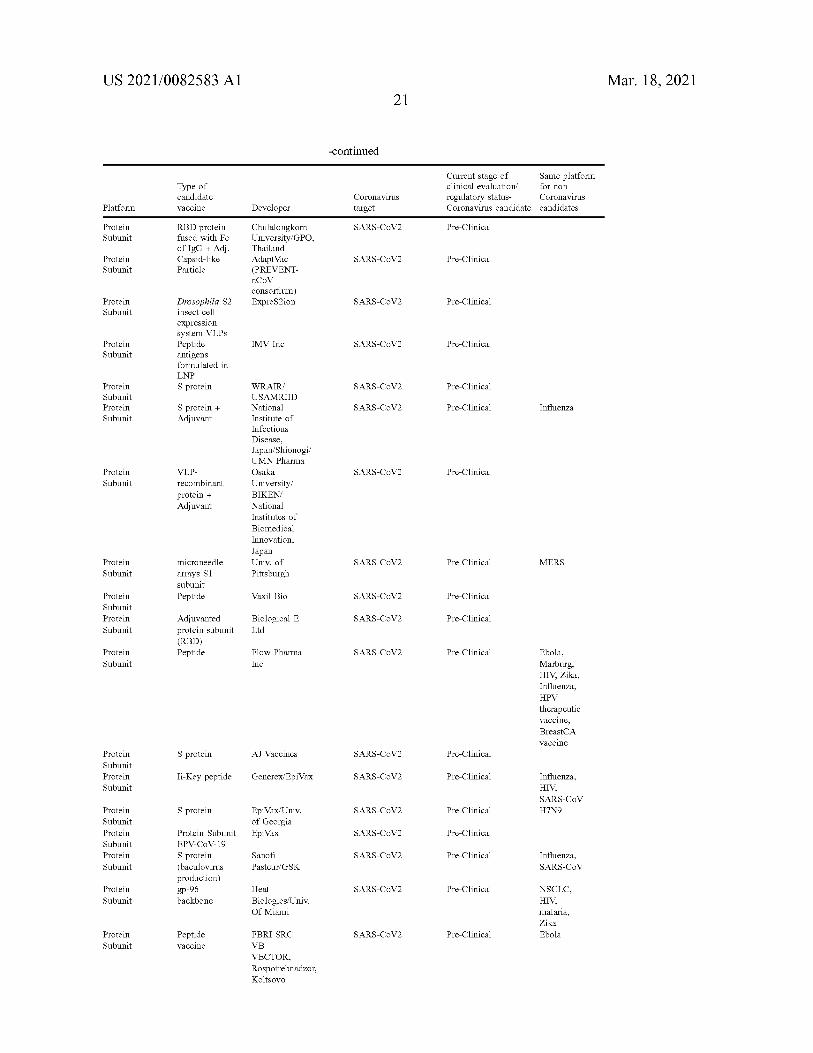
US 2021/0082583 A1 Mar. 18 , 2021 21
-continued
for non Type of candidate vaccine
Current stage of Same platform clinical evaluation regulatory status- Coronavirus Coronavirus candidate candidates
Coronavirus target Platform Developer SARS - CoV2 Pre - Clinical Protein
Subunit RBD protein fused with Fc of IgG + Adj . Capsid - like Particle
SARS - CoV2 Pre - Clinical Protein Subunit
Chulalongkorn University / GPO , Thailand AdaptVac ( PREVENT nCoV consortium ) ExpreS2ion SARS - CoV2 Pre - Clinical Protein
Subunit Drosophila S2 insect cell expression system VLPs Peptide antigens formulated in LNP S protein
IMV Inc SARS - CoV2 Protein Subunit
Pre - Clinical
SARS - CoV2 Pre - Clinical Protein Subunit Protein Subunit
SARS - CoV2 Pre - Clinical Influenza S protein + Adjuvant
SARS - CoV2 Pre - Clinical Protein Subunit
VLP recombinant protein + Adjuvant
WRAIR USAMRIID National Institute of Infectious Disease , Japan / Shionogi / UMN Pharma Osaka University / BIKEN / National Institutes of Biomedical Innovation , Japan Univ . of Pittsburgh
microneedle SARS - CoV2 Pre - Clinical MERS Protein Subunit arrays S1
subunit Peptide Vaxil Bio SARS - CoV2 Pre - Clinical Protein
Subunit Protein Subunit
SARS - CoV2 Pre - Clinical Biological E Ltd
Adjuvanted protein subunit ( RBD ) Peptide SARS - CoV2 Pre - Clinical Protein
Subunit Flow Pharma Inc
Ebola , Marburg , HIV , Zika , Influenza , HPV therapeutic vaccine , BreastCA vaccine
S protein AJ Vaccines SARS - CoV2 Pre - Clinical Protein Subunit Protein Subunit
Ii - Key peptide Generex / EpiVax SARS - CoV2 Pre - Clinical Influenza , HIV , SARS - CoV H7N9 S protein SARS - CoV2 Pre - Clinical EpiVax / Univ .
of Georgia EpiVax SARS - CoV2
Protein Subunit Protein Subunit Protein Subunit
Pre - Clinical
SARS - CoV2 Pre - Clinical
Protein Subunit EPV - CoV - 19 S protein ( baculovirus production ) gp - 96 backbone
Sanofi Pasteur / GSK
Influenza , SARS - CoV
SARS - CoV2 Pre - Clinical Protein Subunit
Heat Biologics / Univ . Of Miami
NSCLC , HIV , malaria , Zika Ebola SARS - CoV2 Pre - Clinical Protein
Subunit Peptide vaccine
FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo
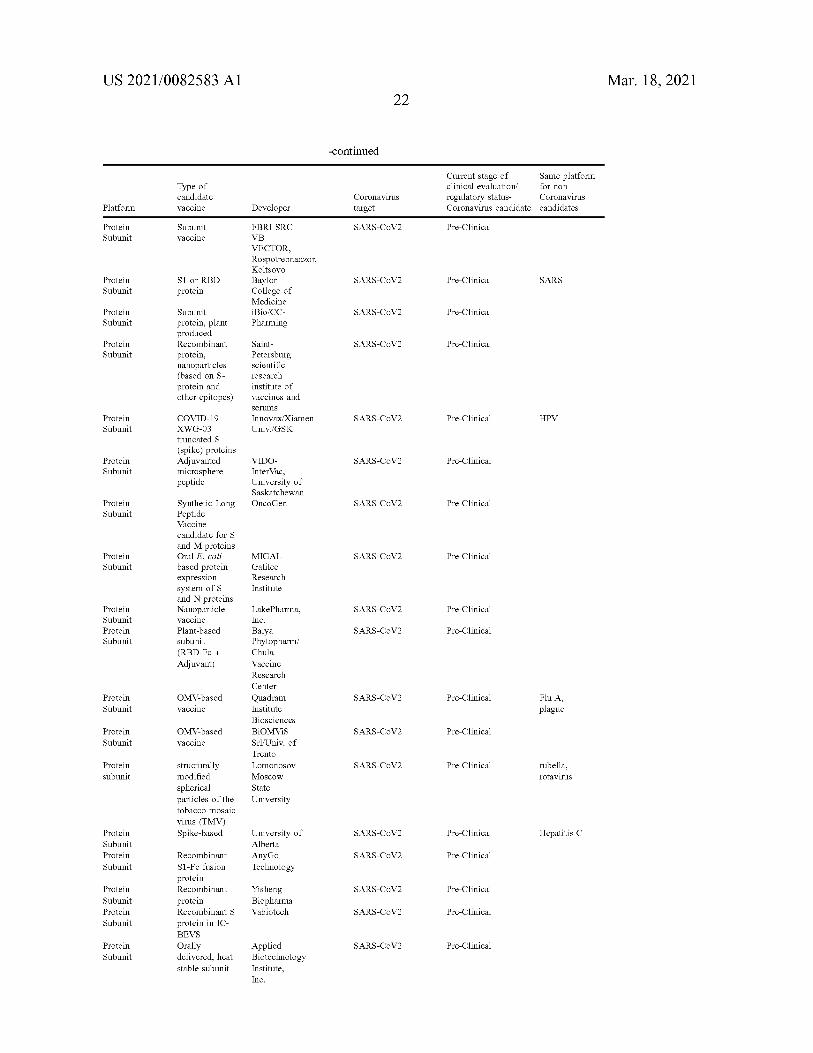
US 2021/0082583 A1 Mar. 18 , 2021 22
-continued
Type of for non Current stage of Same platform clinical evaluation regulatory status- Coronavirus Coronavirus candidate candidates
candidate vaccine Platform Developer
Coronavirus target
SARS - CoV2 Pre - Clinical Protein Subunit
Subunit vaccine
FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo Baylor College of Medicine iBio / CC Pharming
SARS - CoV2 Pre - Clinical SARS Protein Subunit
Si or RBD protein
SARS - CoV2 Pre - Clinical Protein Subunit
SARS - CoV2 Pre - Clinical Protein Subunit
Subunit protein , plant produced Recombinant protein , nanoparticles ( based on S protein and other epitopes )
Saint Petersburg scientific research institute of vaccines and serums
Innovax Xiamen Univ./GSK
SARS - CoV2 Pre - Clinical HPV Protein Subunit
COVID - 19 XWG - 03 truncated s ( spike ) proteins Adjuvanted microsphere peptide
SARS - CoV2 Pre - Clinical Protein Subunit
VIDO InterVac , University of Saskatchewan OncoGen SARS - CoV2 Pre - Clinical Protein
Subunit
SARS - CoV2 Pre - Clinical Protein Subunit
Synthetic Long Peptide Vaccine candidate for S and M proteins Oral E. coli based protein expression system of s and N proteins Nanoparticle vaccine Plant - based subunit ( RBD - Fc + Adjuvant )
MIGAL Galilee Research Institute
SARS - CoV2 Pre - Clinical Protein Subunit Protein Subunit
SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical Flu A , Protein Subunit
OMV - based vaccine
LakePharma , Inc. Baiya Phytopharm / Chula Vaccine Research Center Quadram Institute Biosciences BIOMVIS Srl / Univ . of Trento Lomonosov Moscow State University
plague
SARS - CoV2 Pre - Clinical Protein Subunit
OMV - based vaccine
SARS - CoV2 Pre - Clinical Protein subunit
rubella , rotavirus
structurally modified spherical particles of the tobacco mosaic virus ( TMV ) Spike - based SARS - CoV2 Pre - Clinical Hepatitis C Protein
Subunit Protein Subunit
University of Alberta AnyGo Technology
SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical Protein Subunit Protein Subunit
Recombinant S1 - Fc fusion protein Recombinant protein Recombinant S protein in IC BEVS Orally delivered , heat stable subunit
Yisheng Biopharma Vabiotech SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical Protein Subunit
Applied Biotechnology Institute , Inc.
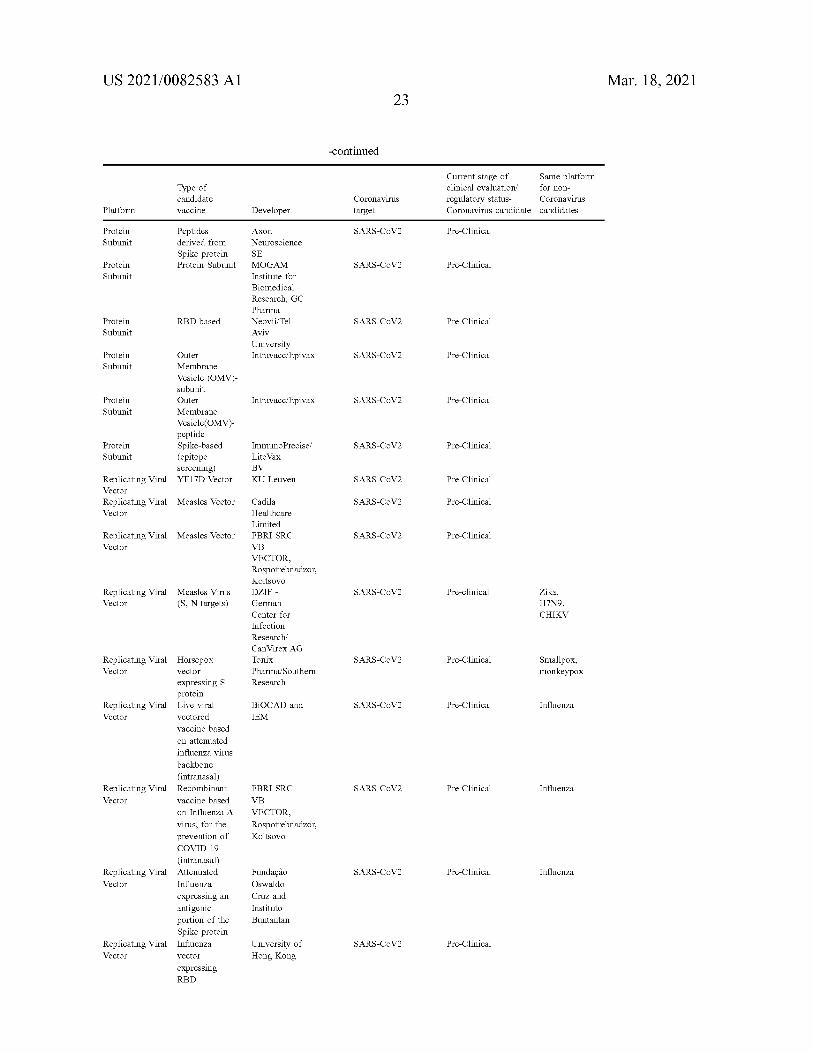
US 2021/0082583 A1 Mar. 18 , 2021 23
-continued
Type of candidate vaccine
Current stage of Same platform clinical evaluation for non regulatory status- Coronavirus Coronavirus candidate candidates
Coronavirus target Platform Developer
SARS - CoV2 Pre - Clinical Protein Subunit
Peptides derived from Spike protein Protein Subunit SARS - CoV2 Pre - Clinical Protein
Subunit
Axon Neuroscience SE MOGAM Institute for Biomedical Research , GC Pharma Neovii / Tel Aviv University Intravacc / Epivax
RBD - based SARS - CoV2 Pre - Clinical Protein Subunit
SARS - CoV2 Pre - Clinical Protein Subunit
Intravacc / Epivax SARS - CoV2 Pre - Clinical Protein Subunit
Outer Membrane Vesicle ( OMV ) subunit Outer Membrane Vesicle ( OMV ) peptide Spike - based ( epitope screening ) YF17D Vector
SARS - CoV2 Pre - Clinical Protein Subunit
ImmunoPrecise / Lite Vax BV KU Leuven SARS - CoV2 Pre - Clinical Replicating Viral
Vector Replicating Viral Vector
Measles Vector SARS - CoV2 Pre - Clinical
Measles Vector SARS - CoV2 Pre - Clinical Replicating Viral Vector
Replicating Viral Vector
SARS - CoV2
Cadila Healthcare Limited FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo DZIF German Center for Infection Research Can Virex AG Tonix Pharma / Southern Research
Measles Virus ( S , N targets )
Pre - clinical Zika , H7N9 , CHIKV
SARS - CoV2 Pre - Clinical Replicating Viral Vector
Smallpox , monkeypox
SARS - CoV2 Pre - Clinical Influenza Replicating Viral Vector
BioCAD and IEM
SARS - CoV2 Pre - Clinical Influenza Replicating Viral Vector
Horsepox vector expressing S protein Live viral vectored vaccine based on attenuated influenza virus backbone ( intranasal ) Recombinant vaccine based on Influenza A virus , for the prevention of COVID - 19
( intranasal ) Attenuated Influenza expressing an antigenic portion of the Spike protein Influenza vector expressing RBD
FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo
SARS - CoV2 Pre - Clinical Influenza Replicating Viral Vector
Fundação Oswaldo Cruz and Instituto Buntantan
SARS - CoV2 Pre - Clinical Replicating Viral Vector
University of Hong Kong
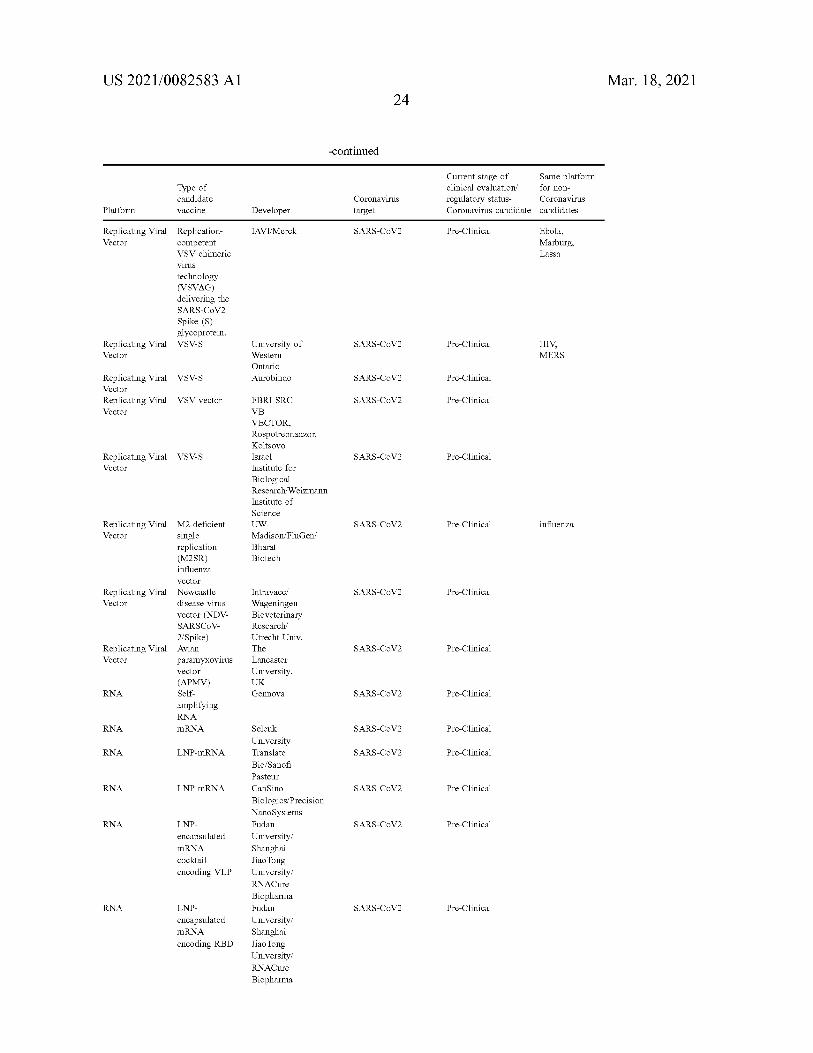
US 2021/0082583 A1 Mar. 18 , 2021 24
-continued
Type of Current stage of Same platform clinical evaluation for non regulatory status- Coronavirus Coronavirus candidate candidates
candidate vaccine
Coronavirus target Platform Developer
IAVI / Merck SARS - CoV2 Pre - Clinical Ebola , Marburg , Lassa
Replicating Viral Replication Vector competent
VSV chimeric virus technology ( VSVAG ) delivering the SARS - CoV2 Spike ( S ) glycoprotein .
Replicating Viral VSV - S Vector
SARS - CoV2 Pre - Clinical HIV , MERS
University of Western Ontario Aurobindo VSV - S SARS - CoV2 Pre - Clinical Replicating Viral
Vector Replicating Viral Vector
VSV vector SARS - CoV2 Pre - Clinical
VSV - S SARS - CoV2 Pre - Clinical Replicating Viral Vector
FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo Israel Institute for Biological Research / Weizmann Institute of Science UW Madison / FluGen / Bharat Biotech
SARS - CoV2 Pre - Clinical influenza
SARS - CoV2 Pre - Clinical
Replicating Viral M2 - deficient Vector single
replication ( M2SR ) influenza vector
Replicating Viral Newcastle Vector disease virus
vector ( NDV SARSCOV 2 / Spike )
Replicating Viral Avian Vector paramyxovirus
vector
( APMV ) RNA Self
amplifying RNA
RNA mRNA
Intravacc / Wageningen Bioveterinary Research / Utrecht Univ . The Lancaster University , UK Gennova
SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical
SARS - CoV2 Pre - Clinical
RNA LNP - mRNA SARS - CoV2 Pre - Clinical
RNA LNP - mRNA SARS - CoV2 Pre - Clinical
RNA SARS - CoV2 Pre - Clinical LNP encapsulated mRNA cocktail encoding VLP
Selcuk University Translate Bio / Sanofi Pasteur Can Sino Biologics / Precision NanoSystems Fudan University / Shanghai Jiao Tong University / RNACure Biopharma Fudan University / Shanghai Jiao Tong University RNACure Biopharma
RNA SARS - CoV2 Pre - Clinical LNP encapsulated mRNA encoding RBD
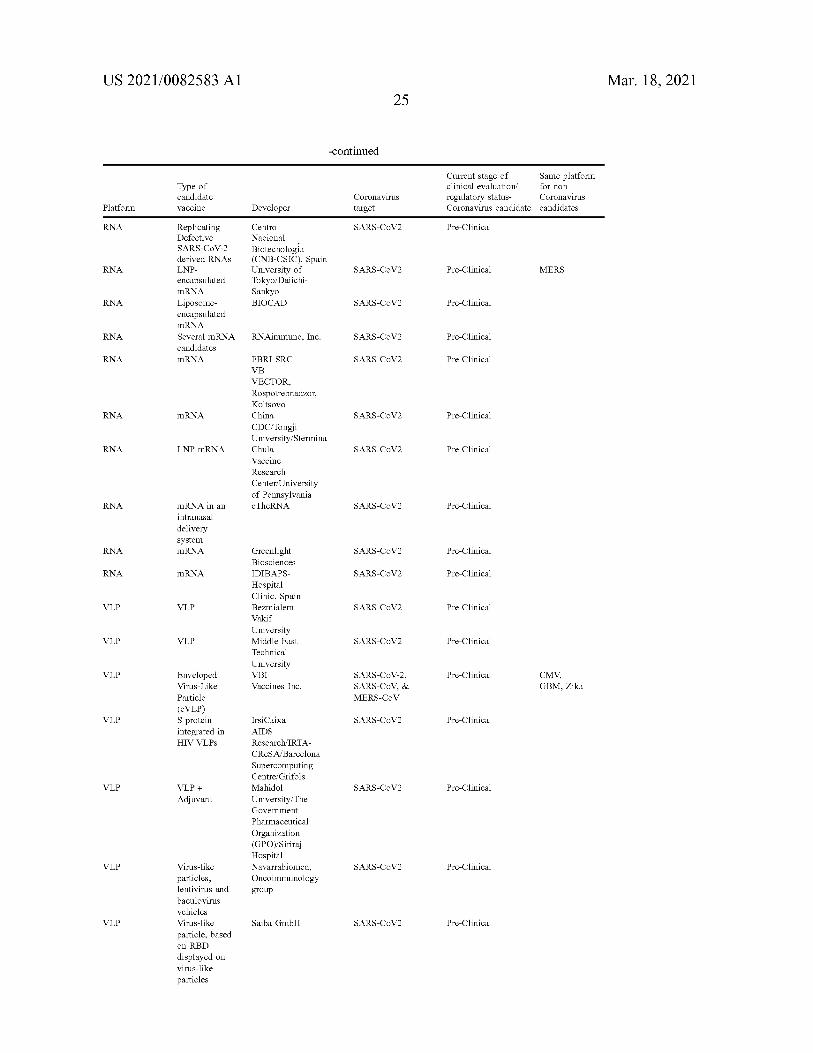
US 2021/0082583 A1 Mar. 18 , 2021 25
-continued
for non Type of candidate vaccine
Current stage of Same platform clinical evaluation regulatory status- Coronavirus Coronavirus candidate candidates
Coronavirus target Platform Developer
RNA SARS - CoV2 Pre - Clinical Centro Nacional Biotecnologia ( CNB - CSIC ) , Spain University of Tokyo / Daiichi Sankyo BIOCAD
RNA SARS - CoV2 Pre - Clinical
Replicating Defective SARS - CoV - 2 derived RNAS LNP encapsulated mRNA Liposome encapsulated mRNA Several mRNA candidates mRNA
MERS
RNA SARS - CoV2 Pre - Clinical
RNA RNAimmune , Inc. SARS - CoV2 Pre - Clinical
RNA SARS - CoV2 Pre - Clinical
RNA mRNA SARS - CoV2 Pre - Clinical
FBRI SRC VB VECTOR , Rospotrebnadzor , Koltsovo China CDC / Tongji University / Stermina Chula Vaccine Research Center / University of Pennsylvania eTheRNA
RNA LNP - mRNA SARS - CoV2 Pre - Clinical
RNA SARS - CoV2 Pre - Clinical mRNA in an intranasal delivery system mRNA RNA SARS - CoV2 Pre - Clinical
RNA mRNA SARS - CoV2 Pre - Clinical
VLP VLP SARS - CoV2 Pre - Clinical
Greenlight Biosciences IDIBAPS Hospital Clinic , Spain Bezmialem Vakif University Middle East Technical University VBI Vaccines Inc.
VLP VLP SARS - CoV2 Pre - Clinical
VLP Pre - Clinical SARS - CoV - 2 , SARS - CoV , & MERS - CoV
CMV , GBM , Zika
Enveloped Virus - Like Particle ( EVLP ) S protein integrated in HIV VLPs
VLP SARS - CoV2 Pre - Clinical
VLP SARS - CoV2 Pre - Clinical VLP + Adjuvant
IrsiCaixa AIDS Research / IRTA CReSA / Barcelona Supercomputing Centre / Grifols Mahidol University / The Government Pharmaceutical Organization ( GPO ) / Siriraj Hospital Navarrabiomed , Oncoimmunology group
VLP SARS - CoV2 Pre - Clinical
VLP
Virus - like particles , lentivirus and baculovirus vehicles Virus - like particle , based on RBD displayed on virus - like particles
Saiba GmbH SARS - CoV2 Pre - Clinical

US 2021/0082583 A1 Mar. 18 , 2021 26
-continued
Type of for non Current stage of Same platform clinical evaluation regulatory status- Coronavirus Coronavirus candidate candidates
candidate vaccine
Coronavirus target Platform Developer
VLP SARS - CoV2 Pre - Clinical ADDomerTM multiepitope display
Imophoron Ltd and Bristol University's Max Planck Centre Doherty Institute OSIVAX
VLP Unknown SARS - CoV2 Pre - Clinical
VLP VLP Pre - Clinical SARS - CoV1 SARS - CoV2 SARS - CoV2 VLP eVLP Pre - Clinical malaria ARTES
Biotechnology Univ . of Sao Paulo
VLP SARS - CoV2 Pre - Clinical VLPs peptides / whole virus
[ 0353 ] In some embodiments , vaccines are all compounds as disclosed in in the website of Clinical Trials.gov ( https : // clinicaltrials [ dot ] gov / ct2 / results ? cond = COVID - 19 ) , which are all incorporated herein by reference . Other vaccines may be used as well . [ 0354 ] In some embodiments , treatment can be the use of Hydroxychloroquine and azithromycin plus zinc . [ 0355 ] In some embodiments , vaccines include the vac cine developed by the Moscow - based Gamaleya Institute , named Sputnik - V . [ 0356 ] In some embodiments , providing a treatment as disclosed above to healthy subjects can be understood as prophylactic treatment and / or vaccination .
individual should receive the treatments . In some embodi ments , a potential advantage of vaccinating / treating indi viduals having the higher superspreading score is to block potential intersections where a higher number of individuals might be infected by the potential superspreaders , and this is done by vaccinating individuals with potentially and / or actual higher chances to meet other people , and optionally also in relation to other individuals ( for example by nor malization of the data ) . In some embodiments , a potential advantage of this method is that a population will potentially reach faster a state of herd immunity , as the provision of treatments continues . [ 0359 ] Referring now to FIG . 2 , showing a flowchart of an exemplary embodiment of the invention . In some embodi ments , the system and methods are based on the following : receiving information about a subject 202 , analyzing the received information 204 , generating a score 206 based on the information , optionally allocating the subject based to the score to a score group 208 , and providing treatment according to the score and / or according to the score group 210. As will be shown below , some or all of the receiving and generating may be performed on an electronic device of subject 202 .
Exemplary Classification of Superspreader [ 0357 ] Referring now to FIG . 1 , showing a schematic representation of a definition of superspreader , according to some embodiments of the invention . In addition to the notion that a superspreader might be identified as a person who excretes a higher than normal number of pathogens during the time they are infectious , a superspreader is a person who may excrete a normal ( or low ) number of pathogens during the time they are infectious but this person is potentially and / or effectively in contact with a high number of people , therefore potentially infecting the same or more number of people as a person who excretes a higher than normal number of pathogens , as schematically shown for example in FIG . 1. Following this logic , according to some embodiments of the invention , a superspreader is further identified according to the number of people he / she can potentially be in contact with , is expected or estimated to be in contact with ( e.g. , based on number he has been in contact with ) , no matter the level of excretion of said person .
Exemplary Factors Influencing the Score [ 0360 ] In some embodiments , the score is generated uti lizing one or more factors and / or components , each influ encing the final score by either adding or subtracting from the score . In some embodiments , the one or more factors can influence the score in a linear matter ( increasing / decreasing the score linearly , for example +1 to the score or -2 to the score ) and / or one or more factor can affect the score in a weighted matter , as will be further explained below . Exem plary factors and / or components are one or more of the following : Super - Spreading Potential Score
Profession in Record of the Individual [ 0358 ] In accordance with some embodiments of the invention , there are provided methods and systems of pro viding subjects in a population with a “ superspreading score ” , which will help to provide the order in which the subjects , optionally in groups of subjects , will receive treat ments . In some embodiments , the higher the score the higher the potential of each individual to spread the disease . In some embodiments , the higher the score , the earlier the
[ 0361 ] In some embodiments , the profession of the indi vidual is correlated with a potential number of people the person might be in contact with during a regular day of operation . In some embodiments , individuals that poten tially must meet many people due to their profession will receive a high score . For example , cashiers at the supermar

US 2021/0082583 A1 Mar. 18 , 2021 27
ket , vendors in markets , bus drivers , delivery people , tech nicians , librarians , etc. In some embodiments of the inven tion , the profession information is used to estimate a contact quality score , for example , doctors being more careful with PPE than teachers . It is a particular feature of some embodi ments of the invention , that differences within such a group , such as between different doctors , are determined . In some embodiments of the invention , a subject's score is modified according to the profession , for example , to compensate for criticality of the subject and / or to lack of control of the subject ( e.g. , a bus driver ) over number of contacts . [ 0362 ] In some embodiments of the invention , a subject provides profession information or other information used to adjust scoring by scanning a barcode ( or other machine readable item such as a barcode or RFID chip identity card ) which is optionally digitally signed with such information . Optionally , this allows the device to know the profession information , but may not allow the device and / or the infor mation provider to link the request for data to a particular individual . Thus potentially maintaining privacy .
[ 0368 ] In some embodiments , other factors that influence the increment or reduction of the likelihood of a subject transmitting a pathogen indoors are one or more of venti lation rate , use of natural ventilation , avoidance of air recirculation and use of air filters . [ 0369 ] In some embodiments , the system will comprise information on indoor locations related to the ventilation rate , use of natural ventilation , avoidance of air recirculation and use of air filters . In some embodiments , an indoor place comprising a high ventilation rate score will provide a lower score to the individual when compared to a place having a low ventilation rate score .
The Kind of Places Usually Visited by the Subject [ 0370 ] In some embodiments , subjects that are prone to frequent religious or secular events , like in a synagogue , a church or a mosque or a dancing venue , where the people are in close proximity to each other , and talk , pray , sing and / or breathe deeply and / or mingle more , will receive a higher score ( e.g. , for such a contact event ) than those who do not frequent religious events . In some embodiments , similarly to above , also subject that are prone to frequent sports events will receive a higher score . In some embodiments , places that are frequented regularly by a large quantity of individu als ( including public transportation , detectable for example , by geolocation and / or regular start - stop movement that matches a public transportation profile and / or base don payment activity using the tracking electronic device ) will be marked as points on interest for the potential spreading of the infectious disease / virus / pathogen , and subjects that fre quent those places will receive a higher score .
Characteristics of Population Potentially to Meet [ 0363 ] In some embodiments , the kind of population that a certain subject can potentially meet will either increase or decrease the score . For example , teachers that meet many children will be provided with a higher score , since if and once the children are infected by the teacher , the children return home and potentially infect their families . While for example , a doctor that works at a prison would potentially receive a lower score since the incarcerated people in the prison are not leaving and probably will not infect anyone else ( the infection is contained to the prison alone ) . [ 0364 ] Another example , if a certain subject meets only a certain number of individuals , and mainly only those indi viduals , for example a subject in a close community , then that subject will receive a lower score . Characteristics of Population that a Subject Actually Met [ 0365 ] In some embodiments , if a certain subject meets people that were identified as superspreaders , this will influence the score by increasing their score , also when compared to subjects that do not meet superspreaders and / or regular people . In some embodiments , the information regarding meeting a superspreader is performed between the mobile devices in an anonymous matter , for example , as will be further explained below .
The Length of Time at the Locations [ 0371 ] In some embodiments , the length that a subject stays in one place will contribute to the determination of the probability to infect others and / or to be infected by others . For example , a subject that visits many places but stays there just for a minute or two might receive a lower score ( e.g. , for a contact event ) than a person that stays for longer in a few places , since staying longer at one place potentially increases the chances to infect and / or be infected . Historical Geolocation Data of the Individual
The Nature of the Locations
[ 0366 ] In some embodiments , the nature of a location means if it is in a closed place , if it is in an open space , if it is indoors , if it is outdoors , quality of ventilation or any combination thereof . In some embodiments , the nature of the locations can drastically change the score given to a subject . It has been shown that a likelihood of a subject transmitting a pathogen increases by a factor of between about 10 times to about 100 times when the location is indoors and / or in a closed space . This is because the risk of infection is increased due to the possible buildup of the airborne pathogen - carrying droplets , the pathogen likely higher stability in indoor air , and / or a larger density of people . [ 0367 ] In some embodiments , if the location is indoors or in a closed location , then the score given to the subject for a contact will increase .
[ 0372 ] In some embodiments , historical data of the loca tion of an individual is used to assess the potential geolo cation activity of that specific individual . For example , Google Maps® data saved in servers , Waze data saved in servers , and other geolocation applications configured to save geolocation activity data . In some embodiments , indi viduals having a high volume of movement data ( and / or high usage of public transportation ) in their historical geo location data will receive a high score . In some embodi ments , the historical data is used to further assess a reliabil ity of change in behavior of a subject , for example to determine if to increase score in cases where the actual geolocation data changes drastically ( for example if there is a risk that a subject wants a higher score to receive the vaccine and increases his movements to achieve so ) .
Actual Geolocation Data of the Individual
[ 0373 ] In some embodiments , actual measured geoloca tion data of each individual is monitored to assess their potential to meet other people . In some embodiments ,

US 2021/0082583 A1 Mar. 18 , 2021 28
people which show high number movements during the day in areas where other people are located will receive a high score . In some embodiments , actual geolocation data of each individual is monitored using one or more of : 1. Electronic devices , for example the location provided by the GPS of their own cellphones ; 2. Using face recognition technology based on one or more of : a ) video surveillance data received from available sources , for example street cameras , ATM's , private surveil lance cameras in stores , buildings and houses , etc .; b ) social media . 3. Digital activity , for example credit card usage , IP address used while using a computer or an electronic device , anten nas that receive data while performing a phone call . [ 0374 ] Optionally or additionally , such actual geolocation data is used instead of or in addition to actually identifying contact between people .
some embodiments of the invention , already existing soft ware may be used , for example , both android and is based cellphones have software ( e.g. , as an operating system service ) which can detect proximity of others and such software may be used or improved to provide functionality as described herein . [ 0379 ] In some embodiments , such app can be used to provide information regarding how many unique people the user meets . For example , a certain user can meet many people but they are all the same people all the time . While another user can meet fewer people but each one is a different individual . In some embodiments , the second user may potentially receive a higher score and therefore receive treatment first . In some embodiments , such app and / or smart devices are also used to assess the progression of the vaccination procedures and the efficacy of the vaccination procedure . In some embodiments , individual data arriving from each user is coupled with their health information ( sick , vaccinated , recovered , etc. ) to further assess the progression of the vaccination procedures and the efficacy of the vaccination procedure . Optionally , if the persons met by a user are vaccinated or otherwise determined to be immune , such contacts may not count and / or be weighted lower . [ 0380 ] In some embodiments , the app will be also used to send personalized communication to the users , for example , to come and be vaccinated . In some embodiments , in view of the information received from the app , specific actions are taken , for example , send a communication to the user to enhance his awareness to behavioral rules during pandemic , to come and be vaccinated , to avoid certain locations , which are at high risk of contagion .
Historical Medical Data of the Individual
[ 0375 ] In some embodiments , historical medical data of each individual is assessed to provide a score . For example , as mentioned above , individuals with chronic coughing will receive a high score since they have potentially a higher chance to transmit the infectious disease / virus / pathogen . In some embodiments , individuals having a background con dition that enhances the chances of transmitting the disease will receive a high score . Actual Medical Data of the Individual
[ 0376 ] In some embodiments , during the pandemic , every new medical data concerning each individual is monitored to assess if the new data indicates a change in the medical status of the individual regarding their potential to infect others . Using the example above , if a person is diagnosed with chronic coughing it will increase their score ( e.g. , in general and / or per contact ) .
Dedicated Voluntary App [ 0381 ] In some embodiments , in view of the pandemic , the population is encouraged to install a dedicated app , where those that do install the app are rewarded . In some embodi ments , the reward is priority to receive treatment .
Third Party Information Regarding the Individual [ 0377 ] In some embodiments , third party information from individuals informing on others will be assessed to decide if the information needs to affect the score . For example , if a third party informs that a person that showed low movement data and received a low score is actually performing many movements , once the information is veri fied , the score will change accordingly . The contrary is also valid , for example , a third party informed that a person that showed high movement data and received a high score is actually staying at home , once the information is verified , the score may change accordingly .
Monitoring Behavior of Subject [ 0382 ] In some embodiments , the behavior of the subject is monitored in relation to safety features performed by the subject , for example , wearing a mask ( e.g. , analyzing images taken during calls or other looking at screen of cellphone ) , washing his hands ( e.g. , analyzing sounds of water running or movement by a smartwatch ) , keeping social distancing ( e.g. , based on Bluetooth power levels and / or NFC detection ) , moving between multiple locations , etc. In some embodiments , these are monitored using the same devices / methods as disclosed above .
Exemplary Scoring Method Dedicated Mandatory App [ 0378 ] In some embodiments , in view of the pandemic , the government may order the citizens to install a dedicated application on their smartphones ( or other smart devices like tablets , smart watches , smart glasses , etc. ) to help the government with the logistics of the vaccination procedures . In some embodiments , the government ( or other body ) provides the public with such dedicated smart devices . In some embodiments , the app and / or the smart device is configured to inform on the user's location at all times and to communicate with adjacent smart devices ( via Bluetooth for example ) to assess the interactions between users , for example vicinity between users , movement of users , etc. ) . In
[ 0383 ] In some embodiments , each individual in a popu lation ( e.g. , above 100 , 1000 , 10000 and / or 100000 indi viduals ) is provided with a score defining the potential level of superspreading of each individual . In some embodiments , scores are defined as number of contacts ( see herein ) , and the number of contacts that are counted are from about 10 to about 100 , optionally from about 100 to about 1000 , option ally from about 1000 to about 10000 , for example 100 , 400 , 1000 , 2000 , 10000 or intermediate or greater numbers . In some embodiments , a high score defines a high potential of superspreading , while a low score defines a low potential of superspreading . In order to facilitate the explanations of the

US 2021/0082583 A1 Mar. 18 , 2021 29
simulating the contact network and trying out various vac cination schemes and / or removal of various individuals and / or sets of individuals .
From Score to Treatment
[ 0391 ] In some embodiments , once the scoring of each individual is achieved , or optionally the scoring of a high number of individuals of the population , a list is created having the order in which each individual will receive the treatment . In some embodiments , the list is optionally divided by groups , for example , all the individuals that scored between 100 and 90 are grouped in group A , which will receive first the treatments . Then all the individuals that scored between 90 and 80 are grouped in group B , which will receive second the treatments , and so on .
Informing the Public [ 0392 ] In some embodiments , once the list is made , indi viduals will be informed on when and where to go and receive the treatments , for example , by means of emails , dedicated apps in their cellphones , over the media , etc.
invention , a scoring scale from 0 to 100 will be used . It should be understood that other scales can be used , like heat - map scoring , decimal order scales , etc. , all of which are included in the scope of the invention . In some embodiments of the invention , the score is open ended . In some embodi ments of the invention , the score is normalized , for example , to other scores . The normalization need not be linear . In some embodiments of the invention , the score is a scalar . In some embodiments of the invention , the score is multi dimensional , for example , including a superspreader poten tial dimension and a variability in behavior dimension ) [ 0384 ] In some embodiments , the score is calculated using weighted scoring models , in which one or more factors and / or components are assessed according to the received information data . Referring now to FIG . 3 , showing a schematic flowchart of a method of calculating a weighted score , according to some embodiments of the invention . In some embodiments , the system receives information data about a subject 302. In some embodiments , the information data is divided according to the source of the information data 304 , for example , electronic information 306 from smartphones , cameras , credit card information , etc. , geo graphical information 308 , for example from GPS or cell towers , governmental information 310 , for example from the census bureau or EMR ( electronic medical records ) , human information 312 , for example from other individuals calling an providing the information about other individuals , and one or more of the factors and / or components disclosed above . In some embodiments , the system then calculates a weighted score of each information , optionally according to a predetermined criterion 314. In some embodiments , the system then generates a total score from the different weighted scores , optionally according to a predetermined criterion 316. In some embodiments , the system then pro vides a list comprising an order of treatment , which is then used to actually treat the population 318 . [ 0385 ] In some embodiments , the score comprises a plu rality of components , for example predicted likelihood of a subject transmitting an infectious disease / virus / pathogen , predicted likelihood of a subject contracting an infectious disease / virus / pathogen , relative health risk to a subject if said subject contracts a infectious disease / virus / pathogen , damage to society if the subject contracts a infectious disease / virus / pathogen ; one or more of the above optionally in view of physical proximity data to other subjects . [ 0386 ] In some embodiments , physical proximity data of a subject with other subjects is calculated by including one or more of : [ 0387 ] 1. The number of subjects the subject potentially is in contact with ; [ 0388 ] 2. The potential and / or actual distance of the sub ject to the other subjects ; [ 0389 ] 3. The time length of the potential and / or actual encounter of the subject with the other subjects . [ 0390 ] In some embodiments of the invention , the score is updated for and / or after each contact event . In some embodi ments of the invention , update is at end of the day , which may allow aggregating multiple meetings with a same person . Optionally or additionally , the score is updated per a set of contact events . In some embodiments of the inven tion , the score is calculated after all contact events are collected , for example , based on an analysis of a contact network to identify individuals , which , if vaccinated , will best stop infection . Such analysis may be carried out by
Exemplary Simulations [ 0393 ] In some embodiments , models and simulations are run in dedicated computers , for example , to assess the potential progression of the treatments and the probable time to reach herd immunity and / or select values for various parameters . In some embodiments , simulations include the insertion of one or more of actual data received from individuals , simulated data of / from individuals ( in case is necessary to run probable scenarios ) . In some embodiments , evaluations and models utilize one or more of neural net works , machine learning and dedicated simulations . [ 0394 ] In some embodiments , the simulations take under consideration and model the probability of the treatments to work ( or not work ) on the individual . [ 0395 ] In some embodiments , the simulations take under consideration and model the kind of population that a certain subject can potentially meet and the potential population those individuals will potentially meet afterwards . For example , teachers that meet many children will be provided with a higher simulated score , since if and once the children are infected by the teacher , the children return home and potentially infect their families . While for example , a doctor that works at a prison would potentially receive a lower simulated score since the incarcerated people in the prison are not leaving and probably will not infect anyone else ( the infection is contained to the prison alone ) . [ 0396 ] In some embodiments , simulations are performed to evaluate parameter values used to identify a superspreader and possibly how to differentiate them from regular indi viduals .
Exemplary Spreading Network [ 0397 ] In some embodiments , before , during and / or receiving the information regarding the individuals in the whole population , a network 400 of the population is cre ated , as shown for example in FIG . 4. In some embodiments , the network is constantly updated by the system . In some embodiments , the network is used to determine the potential spreading of the infectious disease / virus / pathogen if a cer tain individual is infected . In some embodiments , when possible , clusters in the network are identified , for example

US 2021/0082583 A1 Mar. 18 , 2021 30
clusters 402 through 412 in network 400. In some embodi ments , when evaluating whom to provide treatments , the system assesses the individuals in the clusters and performs analysis and simulations to choose which individuals to treat ( e.g. , individuals that interconnect clusters ) . In some embodiments , this is performed in addition to the scoring performed and generated on each single individual . For example , it can be seen that individual 414 belongs to both clusters 402 and 404 , thereby creating a potential bottleneck ( or bridge ) between clusters . Therefore , it would be advan tageous to treat individual 414 to protect cluster 404 from potential infections coming from cluster 402. Same logic is applied to individual 416. Treating individual 416 can poten tially protect clusters 410 and 412 from potential infections coming from cluster 402. In some embodiments , the system identifies potential key individuals and / or potential key groups of individuals to treat first in order to potentially protect clusters of individuals . In some embodiments , the systems performs this assessment in view of the number of doses available to the population . For example , if there is a large number of doses , instead of treating the individuals located in the bottlenecks , it might be advantageous to treat first all individuals in the cluster 402 , thereby potentially protecting the rest of the clusters from infection . [ 0398 ] In one example , the system selectively removes individuals to identify which set of N individuals ( e.g. , where N is the number of doses to be used ) is best to remove . This can be done using brute force approaches , e.g. , of trying a plurality of sets . Optionally or additionally , this is done by selecting sets of individuals ( e.g. , based on some shared characteristic , such as profession or place in the network ) and seeing the effect of vaccinating these individuals . Optionally or additionally , a different search technique is used , e.g. , treating the problem as an optimization problem . Exemplary Use of the System and Methods for Testing [ 0399 ] In some embodiments , the system and methods are used to identify selected subjects to be tested for the disease . In some embodiments , the testing is used to assess one or more of the progress of the disease , the progress of the treatments , the progress of the herd immunity , etc. Exemplary Use of the System and Methods for Determining Who Will Receive a Certain Type of Vaccination [ 0400 ] In some embodiments , during the development of vaccines for a certain disease , different vaccines comprising different vaccine potencies are developed . In some embodi ments , vaccine potency is a quantitative measure of the specific ability of the vaccine product to achieve an intended biological effect defined in a suitable biological assay based on the attribute of the product that is linked to the relevant biological properties . In some embodiments , the system is used to identify which individuals will receive which types of vaccines in relation to their potency . For example , indi viduals that received and / or were identified as a high super spreading score by the system would be vaccinated with more potent vaccines , when compared with other individu als having lower superspreading scores . In some embodi ments , those individuals having lower superspreading scores might either receive later a vaccination or receive a vaccine having a lower potency . Exemplary Privacy Settings [ 0401 ] In some embodiments , the system comprises one or more layers of protection and / or privacy . In some embodi
ments , layers of protection include one or more of encryp tion algorithms and / or software . [ 0402 ] For example , encryption algorithms and / or soft ware convert the data into ciphertext to transform the original data to a non - readable format accessible only to authorized parties who can decrypt the data back to a readable format . The process of encrypting and decrypting messages optionally involves keys . The two main types of keys in cryptographic systems are symmetric - key and pub lic - key ( also known as asymmetric - key ) . [ 0403 ] Exemplary types of keys : Symmetric - keys : In sym metric - key schemes , the encryption and decryption keys are the same . Communicating parties must have the same key in order to achieve secure communication . Public Keys : In public - key encryption schemes , the encryption key is pub lished for anyone to use and encrypt messages . However , only the receiving party has access to the decryption key that enables messages to be read . In some embodiments , the length of the encryption key used in the system is one or more of 128 - bits , 256 - bits , 1024 - bits and 2048 - bits . [ 0404 ] In some embodiments , the privacy of the users that information is being collected is protected by anonymizing the user at the source . For example , when a cellular phone ! electronic device is used to collect the relevant data , the name of the owner of the electronic device is either encrypted and / or anonymized so any interaction with exter nal sources ( for example the servers of the systems ) will be managed without the use of the actual name of the user but using an encrypted and / or anonymized user name . In a practical example , electronic devices / cellphones are used to evaluate , quantify and qualify the interactions of the user with other people during the day . In some embodiments , the cellphone communicates with other cellphones to monitor the interactions ( distance , location , duration , etc. ) . In some embodiments , when collecting the data about the interac tions , the software in the electronic device will use encrypted and / or anonymized user names . For example , using the names as mentioned in the example below , John Doe , Jane smith and Mark Lite are three users , all having cellphones and optionally comprising a dedicated app for this purpose . In some embodiments , the software of the app in the electronic device will encrypt and / or anonymize the
to be , for example , John Doe = user 265498756124565526 , Jane smith = user 31678465923128 and Mark Lite = user 463212887036554. From this point on , all communications between their electronic devices and external sources will be performed using the encrypted and / or anonymized user names . Optionally , for example as described below , the user IDs or what is exchanged between telephones ) are non - unique . For example , provided at a ratio of , for example 1 : 100 , 1 : 1000 , 1 : 10000 , 1 : 100000 between codes and individuals . While this may mean a potential for confusion between individuals , such confusion may be small , while the increase in difficulty of identifying a use based on the tracked information can significantly increase . [ 0405 ] Furthermore , when assessing the order of receiving treatment , either individually or by groups , ( e.g. , at a server ) may comprise the parameters needed to enter a certain group ( for example , the first group to receive treatment , the second group to receive treatment , etc. ) . In some embodiments , the action of comparing between the parameters of each group and the collected data from the user will be performed inside and by the electronic device itself , thereby avoiding sending data to the servers . In some embodiments , the electronic
names

US 2021/0082583 A1 Mar. 18 , 2021 31
[ 0411 ] As an example , consider three types of systems having different levels of possible anonymization tech niques , in accordance with various exemplary embodiments of the invention : [ 0412 ] 1. A system that uses personal information but does not transmits that personal information about the individual ; [ 0413 ] 2. A system that uses personal information but does not transmits specific information that could be used to potentially identify the individual ; and [ 0414 ] 3. A system that does not require any personal information to work . [ 0415 ] In some embodiments , the anonymization tech niques described in the “ Exemplary Privacy Settings ” sec tion belong to the first type and / or the second type of technique , where relevant data ( positional data , personal data , etc. ) is used by the system but : a ) anything that is transmitted is either coded and / or anonymized when used , or b ) the necessary calculations are performed on the electronic device itself , thereby avoiding sending any personal data at all . [ 0416 ] In the following paragraphs , systems belonging to the third type of system comprising a method of identifying a superspreader that potentially does not require the use of any personal information will be explained .
device will contact the server to requests the parameters , the electronic device will perform the necessary calculations and will generate a score that will be sent back to the server in an anonymized matter ( as explained before ) . In some embodiments , additional information regarding each indi vidual user , as disclosed above , is also downloaded to the electronic device for use of calculations . Once the calcula tions are finished , the resulting data will be sent to the servers and , in response , the server will optionally send a notification to the user to go and receive treatment . [ 0406 ] It is a particular feature of some embodiments of the invention that information about a person's activities , locations , meetings , are not sent out of the device except as , for example , an overall score or a priority for treatment . In some cases , the behavior is sent out but is anonymized and / or condensed , for example , indicating a number ( e.g. , optionally not an exact number and / or time and / or date ) of people met and a number of large congregations attended ( optionally not an exact number and / or location ) , but with enough details removed so that identification of an identity of the device owner will be difficult or impossible . [ 0407 ] In some embodiments , whether the calculations are performed on the servers or on the electronic device , the encryption and / or anonymizing of the name of the user is always used . In some embodiments , the means to read between the encrypted / anonymized user name and the actual name will only be available in the user's electronic device . [ 0408 ] In some embodiments , the notification for getting treatment may or may not contain information regarding the results of the calculations . For example , an individual that was identified as a superspreader may or may not receive information about the fact that he / she was identified as such . In some embodiments , the potential advantage of not pro viding such information is to further enhance the privacy protection of the user . For example , an onlooker may not be able to tell if a user received a high score due to his own behavior , the behavior of those he meets and / or an under lying health condition , which may put them at higher risk . [ 0409 ] In some embodiments , dedicated codes , for example in the form of coupons , will be provided to indi viduals having important / relevant professions ( like doctors , police , etc. ) . In some embodiments , insertion of the codes into their personal electronic devices will inform the system that that encrypted / anonymized user needs a correction in their score . In some embodiments , the correction can be either increasing the score or decreasing the score . In some embodiments , when the electronic device detects certain behavior , like an increase in the movements of the user , the electronic device ( for example via the dedicated app ) will warn the user that his score will be changed if the behavior is not changed . In some embodiments , changing the score can be either increasing or decreasing the score . Exemplary Methods for Identifying Superspreaders with High Levels of Anonymization [ 0410 ] It has been shown that individuals are concerned that the authorities and / or companies are constantly collect ing data with or without their consent for a plurality of reasons . It is also scope of some embodiments of the invention to provide a method of identifying superspreaders without the need to collect data that could potentially be used to lead to the identification of the person in question .
Exemplary “ ID ” Based System for the Identification of Superspreaders [ 0417 ] In some embodiments , the system is based on the following assumptions : 1 ) all individuals comprise an elec tronic device of any kind ; 2 ) on each electronic device there is installed a dedicated application / app that runs the sys tem's software ( as will be explained in the following para graphs ) ; and 3 ) when individuals meet other individuals , information is passed between their electronic devices . [ 0418 ] Referring to FIGS . 5a - f , showing flowcharts of exemplary methods of identification of superspreaders , with an anonymization , according to some embodiments of the invention . In some embodiments , the method begins when a user downloads the software , in the form of an application ( or app ) into their electronic device 502. In some embodi ments , dedicated electronic devices comprising the software will be distributed to those individuals who either do not possess an electronic device or do not want the software downloaded into their electronic devices . In some cases , the device has such software preinstalled thereon . [ 0419 ] In some embodiments , when the individual opens the application , optionally , the individual will be requested to provide and / or insert an identification ( ID ) , optionally using alphanumeric digits 504 , optionally comprising a high number of digits , for example 10 digits , 20 digits , 40 digits . In some embodiments , the system will automatically pro vide an ID to the device ( e.g. , will be generated locally , for example , as a random number or as an encrypted version of the user ID . To facilitate the explanations below , a 20 digits ID will be assumed . It should be understood that other length of ID can be used , noting the difference between IDs that are expected unique and IDs that are not expected to be unique and within unique IDs , IDs that also a particular part thereof is long enough to be expected to be unique . [ 0420 ] At this point , all users have an electronic device with a software in the form and / or as part of an application in which an ID comprising 20 digits has been assigned to the device . It should be noted that the use of “ application ” , " app ” and “ software ” are interchangeable for the explana

US 2021/0082583 A1 Mar. 18 , 2021 32
tion of the following methods . From here , four different methods can be used , as will be further explained bellow . Anonymized Method 1 — Count [ 0421 ] Referring to FIG . 5b , showing a flowchart of exemplary anonymized method 1 , according to some embodiments of the invention . Following the letter “ A ” from FIG . 5a to FIG . 5b , in some embodiments , when an electronic device comes in proximity to another electronic device , the devices exchange full IDs 506 between each other , and the software saves the received ID in the appli cation itself . In some embodiments , after a certain period of time , for example , after one day , after 7 days , after 14 days , after 30 days , or intermediate or shorter times and / or on request by a central server , the application analyzes the IDs stored in the electronic device 508. In some embodiments , analyzing comprises one or more of counting the number of IDs that were received , the number of times that a specific ID was received and the number of IDs received in a day . In some embodiments of the invention , the counting is weighted so different IDs get a different weight , for example , IDs with a high score may be weighted higher , for example as described herein . In particular , IDs that are associated with contacting other suspected superspreaders may receive a higher score . In some embodiments , the software then generates a score based on the result of the analysis . [ 0422 ] At this point one of two different methods is optionally applied , a completely anonymous method and a semi - anonymous method 510 . [ 0423 ] In some embodiments , when the method is a com pletely anonymous method , the method continues following the letter " E ” back to FIG . 5a . [ 0424 ] In some embodiments , the application receives from the server a scale of scores 512. For example , con tinuing using the scale as above , from 1 to 100 , group 1 are those individuals having a score higher than 90 , group 2 are those individuals having a score from 80 to 90 , and so on . In some embodiments , the software then compares the score generated from the analysis with the scale of scores 514. In some embo nts , based on the result of the comparison , the software provides the user of the device with relevant information related the treatment to be received . For example , a predetermined date to receive vaccination ( infor mation received with the scale of scores from the server ) and / or the group number for receiving the vaccination . In some embodiments of the invention , the scale of scores is generated by the receiving information about the score distribution and selecting cutoff values optionally based on available vaccines . Optionally , the information comprises receiving scores form some or all devices . Optionally , only a statistical same of scores is used , for example , fewer than 10 % , 1 % , 0.1 % of available devices , for example , between 50 and 10,000 scores . It is noted that such scores may be delivered anonymously , for example , using an anonymous web service , optionally anonymized using anonymity tools such as Tor , so that the deliverer of each score is unknown . Optionally , the scores are digitally signed by the sender . [ 0425 ] Returning to FIG . 5b , in some embodiments , when the method is not a completely anonymous method , the method continues following the letter “ F ” to FIG . 5f . [ 0426 ] In some embodiments , after the software has gen erated a score based on the analysis , the software sends the score , together with the full ID ( here and in other examples , a full ID may be encrypted or Hashed or otherwise used to
generate a token , which , optionally , is not decipherable by the server ) , to the server to be used to evaluate if that specific individual is potentially a superspreader or not , when com pared to other users 518. In some embodiments , the server performs an evaluation by comparing the scores of the different IDs 520 and generates a treatment list according to the result of the evaluation . In some embodiments , the server then sends back notification regarding the vaccination pro cedures 522 , for example , when to go to receive a vaccina tion , the group number , etc. [ 0427 ] In some embodiments , optionally , the user can choose to respond to a series of personal questions presented by the application , which are then translated into factors that affect the score , for example as disclosed herein . [ 0428 ] In some embodiments , the user choses the level of anonymity that the system will work ( completely anony mous or partially anonymous ) , e.g. , different individuals may have different anonymity levels in a same vaccination prioritization system . Anonymized Method 2 – Count with Transmission of Partial Username [ 0429 ] Referring to FIG . 5c , showing a flowchart of exem plary anonymized method 2 , according to some embodi ments of the invention . Following the letter “ B ” from FIG . 5a to FIG . 5c , in some embodiments , when an electronic device comes in proximity to another electronic device , the devices exchange partial IDs , for example only the last 10 digits of the 20 digits of the ID 524 , and the application saves the received partial ID in the application itself . In some embodiments , the partial ID is a substantially unique partial ID . For example , the use of the last 10 digits of the 20 digits increases the chances that the partial ID is a substantially unique partial ID . In some embodiments , the partial ID is a substantially non - unique partial ID . For example , the use of the last 3 digits of the 20 digits increases the chances that the partial ID is a substantially non - unique partial ID , since there is an increased chance that the same last 3 digits appear in more than one ID . It should be understood that the word “ substantially ” in this context does not mean to be vague , but it is related to the statistical probabilities that a presented partial ID could be identical to another . [ 0430 ] In some embodiments , a potential advantage of exchanging only partial IDs is that it decreases the chances that the specific individual could be identified . It is also noted that , in some embodiments , transmitting partial ID might introduce errors to the analysis of the meeting between individuals since it increases the possibility that one or more individuals will transmit the same partial ID . Since the scope of the method is to protect the privacy of the individuals while contemporarily providing an indication of a potential superspreader , a certain margin of error is accept able . [ 0431 ] In some embodiments , when a received partial ID is stored in the application , it is stored ( or only transmitted that way ) by adding its own partial ID . In some embodi ments , a potential advantage of using this method is that if such pairs of partial ids are transmitted to a third party , such third party can track and count unique meetings . [ 0432 ] In some embodiments , after a certain period of time , for example , after 7 days , after 14 days , after 30 days ( or other times for as discussed in the previous method ) , the application analyzes the partial IDs stored in the electronic device 524. In some embodiments , analyzing comprises one

US 2021/0082583 A1 Mar. 18 , 2021 33
or more of counting the number of partial IDs that were received , the number of times that a specific partial ID was received and the number of partial IDs received in a day . In some embodiments , the software then generates a score based on the result of the analysis . In some embodiments of the invention , a repeat meeting with a same partial ID is not counted or given a lower weight . Other methods of counting as described herein may be used . In some embodiments of the invention , the count is otherwise normalized . For example , the distribution of counts may be used to recon struct an estimate of actual diversity of meetings , using statistical methods of distribution estimation , such as known in the art . Such methods may also be used if instead of always transmitting the ID the ID is only sometimes trans mitted . This statistical distribution may be used to estimate the percentage of unique meetings vs percentage of repeat meetings , for example , assuming a given distribution shape for repeat meetings . Such a given shape may be provided , for example , by a central server ( e.g. , based on real - time data collection ) or a priori . Optionally or additionally , such distribution may be created by sometimes applying method 1 of full ID transmission . [ 0433 ] At this point , one of two different methods is optionally applied , a completely anonymous method and a semi - anonymous method 528. In some embodiments , when the method is a completely anonymous method , the method continues following the letter “ E ” back to FIG . 5a . [ 0434 ] In some embodiments , when the method is not a completely anonymous method , the method continues fol lowing the letter “ F ” to FIG . 5f . These alternatives may be applied as above . Anonymized Method 3 — Count with Transmission of Partial Username and Username Changes Periodically [ 0435 ] In this method , which can be used as a variant of the last two methods , and is shown in FIG . 5d , the ID or partial ID used by the device is modified . [ 0436 ] In some embodiments , for example , after the cer tain period of time mentioned above for counting , the partial ID that is used for the transmission of IDs between is changed by the system and / or the individual itself 534. The actual ID may be changed or a different part of the ID transmitted . In some embodiments of the invention , the original ID is used as a seed to generate a series of pseudo random IDs to be used for transmission . In some embodi ments , for example , when the system changes the transmit ted partial ID , the system transmits instead of the last 10 digits of the ID , the first 10 digits of the ID ; or for example the first 5 digits together with the last 5 digits . It should be understood that the above - mentioned are only examples , and that other methods of randomizing the partial ID that is transmitted are also included in the scope of some embodi ments of the invention . In some embodiments , periodically changing the partial ID may further cause to errors since it further increases the possibility that one or more individuals will transmit the same partial ID . As mentioned above , a further certain margin of error is still acceptable . [ 0437 ] The method then continues with various options for acting on the score , for example , a completely anonymous method and a semi - anonymous method 536. In some embodiments , when the method is a completely anonymous method , the method continues following the letter “ E ” back to FIG . 5a .
[ 0438 ] In some embodiments , when the method is not a completely anonymous method , the method continues fol lowing the letter “ F ” to FIG . 5f . In this and other embodiments it is noted that other follow up activities may be provided in addition or instead , in particular , activity by a central server may be reduced . For example , a user may simply go to a vaccinating station and show their score and be given a vaccination or date therefore accordingly . Anonymized Method 4Complex Count with Transmission of Partial Username , at Least One Additional Number and Optionally Username Changes Periodically [ 0439 ] Referring to FIG . 5e , showing a flowchart of exem plary anonymized method 4 , according to some embodi ments of the invention . In some embodiments , a complex count method is used for probabilistically determining if a certain individual is a potential superspreader . In some embodiments , the complex count method comprises the use of two independent counts for the determination . [ 0440 ] Following the letter “ D ” from FIG . 5a to FIG . 5e , in some embodiments , when an electronic device is in proximity to another electronic device , the system is con figured to exchange not one , but at least two ID numbers as following : [ 0441 ] In some embodiments , the first number to be exchanged is the partial ID 538. In some embodiments , the exchange of the first number is as disclosed in method 1 , where the full ID is exchanged . In some embodiments , the exchange of the first number is as disclosed in either method 2 or method 3 , where a partial ID is exchanged . For the explanation of the method and as disclosed in FIG . 5e , the explanation will refer to the transmission of a partial ID . It should be understood that this method could also be applied when transmitting the full ID . [ 0442 ] In some embodiments , the first number is used to evaluate the number of contacts . [ 0443 ] In some embodiments , the second number to be exchanged is a different set of digits , either created by the system or inserted by the user itself 538. In some embodi ments , the actual second number to be exchanged is a partial second number , similar to what is done with the first number . [ 0444 ] In some embodiments , the second number is used to evaluate if the individual is meeting people from outside a limited subpopulation and / or track the general promiscu ousness ( optionally in a non - sexual sense ) of such individu als . [ 0445 ] In some embodiments , contrary to the first number that always is exchanged in an encounter , the second number is exchanged at a certain " rate of probability ” . In some embodiments , a rate of probability is , for example , a calcu lated number that responds to the question : what is the percentage rate necessary to separate between a super spreader and a non - superspreader . In some embodiments , the rate of probability is achieved by running a simulation , and checking for different probability rates the degree of discrimination . For example , a rate of probability can be 3 % , 5 % , 10 % , 20 % or smaller or intermediate values . In some embodiments , this means that , if the rate of probability is 3 % for example , an electronic device that encounters 100 elec tronic devices will exchange 100 times ( 100 % of the times ) the first number and 3 times ( 3 % of the times ) , in addition to the first number , will also exchange the second number . In some embodiments , the rate of probability is lower than 100 .

US 2021/0082583 A1 Mar. 18 , 2021 34
[ 0446 ] In some embodiments , from the moment the sys tem is activated , the electronic devices of the individuals will begin collecting first and second numbers as long as they continue to meet other electronic devices . [ 0447 ] In some embodiments , when a certain electronic device exchanges the second number ( under the rate of probability ) , the electronic device will exchange in addition to its second number , all second numbers that were collected until that moment . In some embodiments , potentially and probabilistically , an individual that is a superspreader will collect a high number of second numbers because he / she meets many different individuals , who themselves meet different individuals . While an individual “ trapped ” in a subpopulation may only collect at most as many numbers are there are persons in the subpopulation . Therefore , in some embodiments , when someone meets that super spreader , many second numbers will be potentially exchanged from that superspreader to that someone . In some embodiments , those second numbers collected from other individuals will later be used to indicate a specific meeting between an individual and a superspreader . [ 0448 ] In some embodiments , an individual that collects many second numbers , potentially and probabilistically , met a superspreader and / or is one themselves . In some embodi ments , this information is used to cause an effect ( e.g. , increase ) in the scoring of the individual and / or in the weight of the contact . [ 0449 ] The collected IDs may be counted after a time , e.g. , as described in the other methods ( 540 ) In some embodi ments , optionally , after the certain period of time mentioned above , the partial ID transmitted between devices is changed by the system and / or the individual itself 542 as disclosed above . [ 0450 ] Optionally , a method of follow - up is selected , for example , a completely anonymous method and a semi anonymous method 544. In some embodiments , when the method is a completely anonymous method , the method continues following the letter “ E ” back to FIG . 5a . [ 0451 ] In some embodiments , when the method is not a completely anonymous method , the method continues fol lowing the letter “ F ” to FIG . 5f , for example as described above . [ 0452 ] In any of the above methods , optionally , statistical information about collected first and / or second numbers ( e.g. , how many people had how many collected first and / or second numbers ) may be transmitted to the server to help generate a better picture of these statistics of the popula tion's collected information . In some embodiments of the invention , more than one second number is used . [ 0453 ] Optionally , each additional such number is trans mitted at a different probability . This allows different num bers to give information about different characteristics of subpopulations . It is noted that if only one number is used and its transmission rate not selected correctly , it may result is propagation of such second number over a significant part of the network of contacts , making it less useful for iden tifying more closed and more open parts of the network . [ 0454 ] In some embodiments of the invention , no addi tional second number is used . Rather the first number is optionally counted and / or transmitted using such probabi listic transmission rate . So , for example , during a contact , the second device will store the received ID of the first contact in a memory for storing and / or counting contacts with a first ID and also , with some probability store that
number in a second memory used for counting and / or tracking second numbers . Additional memories may be provided if more numbers are tracked . [ 0455 ] In some embodiments of the invention , a relatively small non - unique ID is used and this ID may be used as an index for the first and / or second memory . For example , when meeting an individual who passes a non - unique ID 234 , memory location 234 is increment ( optionally in a weighted manner ) . If a second ID list , say ( 123 , 456 , 789 ) is passed , the count in each of those indexes in the second memory is incremented ( optionally in a weighted manner ) . In some embodiments , only one bit ( or an equivalent thereof ) is saved for each ID in the second memory and it is either set or unset . Optionally , the second ID uses more bits than the first ID , for example , 2 , 3 , 4 , 5 times as many bits or an intermediate of smaller or greater number . This may allow preventing saturation of second ID tracking . Optionally or additionally , a statistical estimation of the actual number of second IDs is reconstructed using statistical methods and the number of second IDs received and optionally a count of at least a sample thereof . Optionally , an assumption is made about the expected shape of distribution of second IDs . [ 0456 ] Optionally or additionally , the number of second IDs collected is tracked as a function of time . Optionally , potential superspreaders ( and which get an increased score and / or contact weight ) are those who early on accumulate a larger number of second IDs ( e.g. , as compared to other persons an individual comes in contact with ) and / or those persons ( e.g. , with repeated contact ) whose second ID count asymptotes later or not at all . [ 0457 ] Regarding repeat meetings with an individual , it is noted that an individual is a sum of all his contacts , so that after a time , if and as that individual meets new contacts , the individual changes and should be weighted more heavily . Such tracking can be by time and / or can be by change in count of first and / or second IDs that an individual has , which count ( and / or a date of contact ) is optionally transmitted upon meeting and may be stored . Exemplary Effect of Meeting an Individual that has Met Potential Superspreaders [ 0458 ] Referring now to FIG . 6 , showing a schematic flowchart of an example of the effect caused when a certain individual meets another individual that had been in contact with possible superspreaders , according to some embodi ments of the invention . In some embodiments , as previously mentioned , when a Device A meets Device B 602 , IDs are exchanged and optionally also information regarding previ ous meetings 604. In some embodiments , for example , the software in Device A , that has just received the ID and previous meetings of Device B , will evaluate the received data 606. In some embodiments , evaluation of data com prises one or more of evaluating the number of meetings Device B has had 608 and the kind of individuals were met during those meetings 610. In some embodiments , since these operations were also previously performed by Device B during its meetings , the information about the possible meeting with a potential superspreader will be also delivered by Device B to Device A , when information is exchanged . In some embodiments , the software in Device A will gen erate a score to the meeting between Device A and Device B , also in view of the information regarding the kind of individuals that Device B has met 612. In some embodi ments , the score is then saved in Device A 614 to be used in the final score calculations , as previously described .

US 2021/0082583 A1 Mar. 18 , 2021 35
Exemplary Methods [ 0459 ] In some embodiments , an exemplary method of providing the order of treatments to a population comprises : 1. Collecting relevant data regarding each individual in the population , according to predetermined parameters . 2. Providing a superspreading score to each of the individu als according to a formula using the predetermined param eters .
3. Ordering each individual according to his or her super spreading score from high to low . 4. Optionally dividing all individuals in groups according to their superspreading score . [ 0460 ] In some embodiments , after the list is ready , optionally in groups : 5. Notifying the individuals with a location and a time to receive the treatments . 6. Treating the population according to their superspreading score , optionally by groups , where individuals and / or groups hiving the higher scores will receive first the treatments . In some embodiments of the invention , treatment is rather testing , as testing superspreaders may be a faster and more effective way of detecting a resurging pandemic . Exemplary System [ 0461 ] In some embodiments , the system comprises a computer network architecture optionally with machine learning and / or other artificial intelligence tools to allow for the automated prioritization of treatments in a pandemic event . In some embodiments , the system allows for priori tization of treatments using information regarding subjects in a population , disease process and progression , number of available treatment doses , and a plurality physical location attributes . In some embodiments , this potentially enables relevant authorities to measure , predict and / or improve their health - related performance during a pandemic . In some embodiments , this in turn enables relevant decision - making personnel and healthcare providers to get a true quantitative sense of what is possible to achieve with any given popu lation of patients , in view of the parameters that define each individual and the population . [ 0462 ] The following is an example of the workflow of a user experience with a system of the present invention : 1. A user makes a request for an analysis and list generation report to the system . 2. The system uses an analytics module ( A.M. ) to analyze the information of the population ( for example , information as disclosed above ) . 3. The system automatically issues a request to a Database Module ( DB.M ) to provide all relevant information and / or issues a request to external sources ( see above ) to provide the required information and / or issues a request to a simu lations module ( S.M ) to perform the necessary simulations . 4. The analytics module ( A.M. ) collates the results into a unified analysis response , based on any combination of the subjects in the population and factors and / or components data available . In some embodiments of the invention , the A.M includes a ML module ( optionally in the form of an analytic system or a neural network ) which is used to predict transmission and super - spreader potential of an individual based on their past behavior . Optionally , an initial model is provided for such mapping . Optionally , the ML module also receives actual infection information , for example , by auto mated collection from medical records or from epidemio
logical studies ( e.g. , of some or all infected people ) and uses this information to update the model , for example , using a machine learning method as known in the art , to generate a prediction of infectiveness ( and / or superspreader potential ) of an individual given his contacts and the superspreader potential of similar individuals . In some embodiments of the invention , statistical methods are used instead of or in addition to ML methods . Optionally or additionally , what is created is a classifier , which classifies an individual as a potential superspreader . Such a classifier can build a clas sification scheme given a set of individuals , each with behaviors and actual infectiveness as determined , for example , using epidemiological studies and / or contact track ing combined with disease detection in such tracked con tacts . Such classifier may be used ( or transmitted to indi vidual devices to be used instead of and / or in addition to counting for example as described herein ) to generate a general score for an individual based on the classification and optionally based on additional information , such as medical risk . [ 0463 ] Optionally or additionally , the AM includes one or more optimization tools which given the various inputs described herein and / or one or more goals , optimizes vac cine delivery and / or schedule to achieve a better approach to the goal . 5. The analytics module ( A.M. ) serves the response back to the system , and transmits the list to the user , and the list is now available to the relevant personnel . In some embodi ments , this potentially helps the relevant personnel to decide whom , when and where distribute the available doses to the population . [ 0464 ] Each and any of such modules may be imple mented , for example , using a central server , a distributed server and / or a cloud implementation . [ 0465 ] In some embodiments , the system may automati cally use the simulation models to select and apply a predictive model for the preferred deployment of the doses ( for example , the parameter may be number of available doses or the higher number of individuals protected by the act of vaccination and / or a total number of expected of deaths and / or time to reach a threshold where one or more limitations on society may be removed ) . In some embodi ments , the system may then predict the performance of an underperforming vaccination result ( if no changes are made to trend performance ) and predict the performance of the same treatment result if the requirements are met , and then compare the before and after predicted performance to show the impact of meeting the requirements . A report of the requirements and of the predicted impacts of meeting the requirements may then be prepared by the system , and transmitted to the user . [ 0466 ] FIG . 7 schematically illustrates components of an exemplary system comprising a computer network architec ture usable in some embodiments of the invention , compris ing at least one optional server 702 , an optional analytics module ( A.M. ) 704 , an optional Database Module ( DB.M ) 706 , and / or optional access to various third - party databases and sources 708 , and an optional simulations module 712 . [ 0467 ] In some embodiments , a user using a user device 710 accesses the at least one server 702. In some embodi ments , the user transmits a user request to the analytics module ( A.M. ) 704 for analysis of data and the generation of a list 716. In some embodiments , analytics module ( A.M. ) 704 accesses the Database Module ( DB.M ) 706 either

US 2021/0082583 A1 Mar. 18 , 2021 36
directly and / or via the server 702. In some embodiments , the analytics module ( A.M. ) 704 accesses through various iden tified third party and sources 708. In some embodiments , data accessed from third - party databases and sources 708 may be analyzed and stored in Database Module ( DB.M ) 706 , thus supporting the simulations module 712 , which performs machine - learning prediction activities . In some embodiments , the analytics module ( A.M. ) 704 may also access data received from the simulations module 712 and previously stored in the Database Module ( DB.M ) 706 , thus benefiting from the machine learning and artificial intelli gence of the simulations module 712 . [ 0468 ] In some embodiments , the system optionally com prises a prediction module 714 with a prediction generator and in communication with the simulation module 712 and with the database module 706 . [ 0469 ] Not shown is a vaccination management server , which is optionally a separate component of the system or be a separate system . In some embodiments of the invention , this server is used to manage distribution of vaccinations ( e.g. , locations and / or times ) and / or tracking of subjects that requested vaccination and / or received such vaccination . Optionally , this server manages the logistics of vaccine distribution using the information form the system indicat ing which subjects are to be vaccinated and in what order . In some embodiments of the invention , vaccinations are dis tributed based on population density and the vaccination management server is used to track subjects receiving vac cinations to ensure that they are not vaccinated out of turn , for example , by comparing prioritization data provided by the devices against a record of prioritization intentions . [ 0470 ] In some embodiments , the system allows automatic machine learning as new data sources are added , and new data is collected , and the predictive algorithms are recali brated and reselected using the expanded , and hence more reliable , data . In some embodiments , this may potentially enable users of the system to quickly realize the value of new data . [ 0471 ] In some embodiments , the system utilizes machine learning , optionally incorporated in predictive model algo rithms to execute predictive analytical operations . Learning may be supervised or unsupervised . In general , a predictive model analyzes historical data to identify patterns in the data . The patterns identified may include relationships between various events , characteristics , or other attributes of the data being analyzed . Modeling of such patterns may provide a predictive model whereby predictions may be made . Development of predictive models may employ math ematical or statistical modeling techniques such as curve fitting , smoothing , and regression analysis to fit or train the data . Such techniques may be used to model the distribution and relationships of the variables , e.g. , how one or more events , characteristics , or circumstances ( which may be referred to as “ independent variables ” or “ predictor vari ables ” ) relate to an event or outcome ( which may be referred to as a “ dependent variable ” or “ response ” ) . [ 0472 ] In some embodiments , a machine learning process may include developing a predictive model . For example , a dataset comprising observed data may be input into a modeling process for mapping of the variables within the data . The mapped data may be used to develop a predictive model . The machine learning process may also include utilizing the predictive model to make predictions regarding a specified outcome that is a dependent variable with respect
to the predictive model . The machine may then be provided an input of one or more observed predictor variables upon which the output or response is requested . By executing the machine - learning algorithm utilizing the input , the requested response may be generated and outputted . Thus , based on the presence or occurrence of a known predictor variable , the machine learning algorithm may be used to predict a related future event or the probability of the future event . [ 0473 ] It is noted that a most basic prediction may be used , e.g. , behavior in past predicts behavior in future . For example , if a person regularly meets 30 people a day for over 15 minutes each and within 2 meters and I a location that is closed ( e.g. , based on mapping data sources ) , it is assumed that may continue . Similarly , if a person attends a church of 200 people once a week , that may be assumed to continue . In addition , class behavior may be applied . For example , if the person is collage age , the system may be programmed with an expectation of a certain number and / or expected dates and / or expected probability of parties such a person might attend . Such information may also be generate by statistically analyzing the behavior of others in that person ' cohort . [ 0474 ] In some embodiments , once the treatment order list 716 is ready , individual messages 718 are sent to the specific individuals notifying them where and when they should go to be treated . [ 0475 ] The architecture of the system may depend on the implementation . For example , if the system is mainly anony mous , with scorings being generated on individual cell phones ( or other devices ) , the server may be used to generate information to be used by the cellphones and / or to collate results generate vaccination prioritization plans and / or invite individuals to be vaccinated . [ 0476 ] In such an example , the software of the electronic device may increase in relative importance . Such device may include a memory ( e.g. , as noted herein ) for storing actual IDs or partial IDs and / or counts thereof . Optionally or additionally , such device includes an ID generator . Option ally or additionally , such device includes communication software ( e.g. , addresses ) for making an anonymous drop of information and / or for receiving a general broadcast of information ( e.g. , from the server ) and / or for accessing an individual's EMR or other repository with relevant medical information . Optionally or additionally , such a device includes a count analysis and / or other module that applies a classification or scoring method for example , as described herein . Optionally or additionally , such a device includes a sensor an associated software for detecting infection related information , for example , being indoors , location , distance from other electronic devices , duration at such distance , coughing sounds and / or video or still analysis to detect mask wearing . Optionally or additionally , such a device includes a display and associated software for showing a vaccination invitation and / or a score . Optionally or additionally , such a device includes an input ( e.g. , a camera ) for receiving information form printed or other screens , for example , a user's occupation or special dispensation . Optionally or additionally , such device includes software , which generates behavior alerts to the user , for example , when the user engages in riskier behavior . [ 0477 ] Various embodiments and aspects of the present invention as delineated hereinabove and as claimed in the claims section below find calculated support in the following examples .
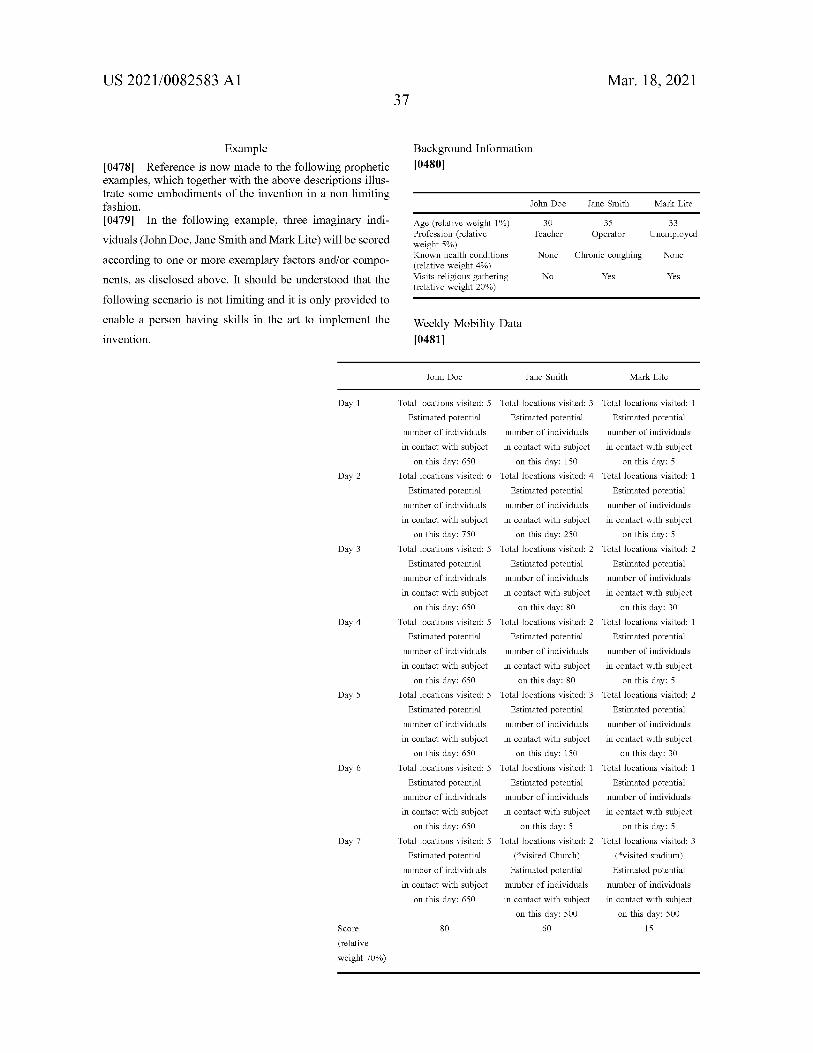
US 2021/0082583 A1 Mar. 18 , 2021 37
Background Information [ 0480 ]
John Doe Jane Smith Mark Lite
30 Teacher
35 Operator
33 Unemployed
Example [ 0478 ] Reference is now made to the following prophetic examples , which together with the above descriptions illus trate some embodiments of the invention in a non limiting fashion . [ 0479 ] In the following example , three imaginary indi viduals ( John Doe , Jane Smith and Mark Lite ) will be scored according to one or more exemplary factors and / or compo nents , as disclosed above . It should be understood that the following scenario is not limiting and it is only provided to enable a person having skills in the art to implement the invention .
Age ( relative weight 1 % ) Profession ( relative weight 5 % ) Known health conditions ( relative weight 4 % ) Visits religious gathering ( relative weight 20 % )
None Chronic coughing None
No Yes Yes
Weekly Mobility Data [ 0481 ]
John Doe Jane Smith Mark Lite
Day 1
Day 2
Day 3
Day 4
Total locations visited : 5 Total locations visited : 3 Total locations visited : 1 Estimated potential Estimated potential Estimated potential
number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 650 on this day : 150 on this day : 5 Total locations visited : 6 Total locations visited : 4 Total locations visited : 1
Estimated potential Estimated potential Estimated potential number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 750 on this day : 250 on this day : 5 Total locations visited : 5 Total locations visited : 2 Total locations visited : 2
Estimated potential Estimated potential Estimated potential number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 650 on this day : 80 on this day : 30 Total locations visited : 5 Total locations visited : 2 Total locations visited : 1
Estimated potential Estimated potential Estimated potential number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 650 on this day : 80 on this day : 5 Total locations visited : 5 Total locations visited : 3 Total locations visited : 2
Estimated potential Estimated potential Estimated potential number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 650 on this day : 150 on this day : 30 Total locations visited : 5 Total locations visited : 1 Total locations visited : 1
Estimated potential Estimated potential Estimated potential number of individuals number of individuals number of individuals in contact with subject in contact with subject in contact with subject
on this day : 650 on this day : 5 on this day : 5 Total locations visited : 5 Total locations visited : 2 Total locations visited : 3
Estimated potential ( * visited Church ) ( * visited stadium ) number of individuals Estimated potential Estimated potential in contact with subject number of individuals number of individuals
on this day : 650 in contact with subject in contact with subject on this day : 500 on this day : 500
80 60 15
Day 5
Day 6
Day 7
Score
( relative weight 70 % )

US 2021/0082583 A1 Mar. 18 , 2021 38
[ 0482 ] In view of the results of the Weekly mobility data alone , the order of the treatments will be John Doe , Jane Smith and then Mark Lite . [ 0483 ] The calculation of the overall score is :
criteria John Doe Jane Smith Mark Lite
50 80
50 0
Age Profession Known health conditions Visits religious gathering Mobility data
1 % 5 % 4 % 20 % 70 %
0
50 50 90 80 60
0 80 15 80
weighted scores 100 % 60.5 66.2 14.2
[ 0484 ] As can be seen , when taking under consideration all the information data , the order of the treatments will be Jane Smith , John Doe and then Mark Lite . [ 0485 ] It should be understood that the above numeric examples are just examples to help a person having skills in the art to understand the invention . It also should be under stood that different weight values , scores and methods of calculating a score could be used . [ 0486 ] It is expected that during the life of a patent maturing from this application many relevant parameters of scoring activity of individuals and methods of measuring said parameters will be developed ; the scope of the inven tion herein is intended to include all such new technologies a priori . [ 0487 ] As used herein with reference to quantity or value , the term “ about ” means " within + 20 % of ” . [ 0488 ] The terms “ comprises ” , “ comprising ” , “ includes ” , “ including ” , “ has ” , “ having ” and their conjugates mean “ including but not limited to ” . [ 0489 ] The term “ consisting of " means “ including and limited to " . [ 0490 ] The term “ consisting essentially of ” means that the composition , method or structure may include additional ingredients , steps and / or parts , but only if the additional ingredients , steps and / or parts do not materially alter the basic and novel characteristics of the claimed composition , method or structure . [ 0491 ] As used herein , the singular forms “ a ” , “ an ” and “ the ” include plural references unless the context clearly dictates otherwise . For example , the term “ a compound ” or “ at least one compound ” may include a plurality of com pounds , including mixtures thereof . [ 0492 ] Throughout this application , embodiments of this invention may be presented with reference to a range format . It should be understood that the description in range format is merely for convenience and brevity and should not be construed as an inflexible limitation on the scope of the invention . Accordingly , the description of a range should be considered to have specifically disclosed all the possible subranges as well as individual numerical values within that range . For example , description of a range such as “ from 1 to 6 ” should be considered to have specifically disclosed subranges such as “ from 1 to 3 ” , “ from 1 to 4 ” , “ from 1 to 5 ” , “ from 2 to 4 ” , “ from 2 to 6 ” , “ from 3 to 6 ” , etc .; as well as individual numbers within that range , for example , 1 , 2 , 3 , 4 , 5 , and 6. This applies regardless of the breadth of the range . [ 0493 ] Whenever a numerical range is indicated herein ( for example “ 10-15 ” , “ 10 to 15 " , or any pair of numbers linked by these another such range indication ) , it is meant to
include any number ( fractional or integral ) within the indi cated range limits , including the range limits , unless the context clearly dictates otherwise . The phrases “ range / rang ing / ranges between ” a first indicate number and a second indicate number and “ range / ranging / ranges from ” a first indicate number “ to ” , “ up to ” , “ until ” or “ through ” ( or another such range - indicating term ) a second indicate num ber are used herein interchangeably and are meant to include the first and second indicated numbers and all the fractional and integral numbers therebetween . [ 0494 ] Unless otherwise indicated , numbers used herein and any number ranges based thereon are approximations within the accuracy of reasonable measurement and round ing errors as understood by persons skilled in the art . [ 0495 ] It is appreciated that certain features of the inven tion , which are , for clarity , described in the context of separate embodiments , may also be provided in combination in a single embodiment . Conversely , various features of the invention , which are , for brevity , described in the context of a single embodiment , may also be provided separately or in any suitable subcombination or as suitable in any other described embodiment of the invention . Certain features described in the context of various embodiments are not to be considered essential features of those embodiments , unless the embodiment is inoperative without those ele ments . [ 0496 ] It is the intent of the applicant ( s ) that all publica tions , patents and patent applications referred to in this specification are to be incorporated in their entirety by reference into the specification , as if each individual publi cation , patent or patent application was specifically and individually noted when referenced that it is to be incorpo rated herein by reference . In addition , citation or identifica tion of any reference in this application shall not be con strued as an admission that such reference is available as prior art to the present invention . To the extent that section headings are used , they should not be construed as neces sarily limiting . In addition , any priority document ( s ) of this application is / are hereby incorporated herein by reference in its / their entirety . What is claimed is : 1. An anonymized method of treating subjects against an
infectious disease caused by a pathogen , comprising : a . providing an electronic device with proximity tracking
circuitry for each of said subjects ; b . generating an ID for each said electronic device ; c . at a proximity event , when a particular said electronic
device of a particular said subject is in proximity of one or more other of said electronic devices , one or both of transmitting said ID or an indication thereof to said one or more other devices and receiving an ID or indication thereof from said one or more other devices , by said particular electronic device ;
d . generating , by said particular electronic device a score reflecting a propensity for proximity , according to a plurality of received IDs ;
e . generating for said particular electronic device a pri oritization of treatment based on said score ; and
f . treating said particular subject according to said priori tization .
2. The method according to claim 1 , wherein said gener ating an ID comprises generating an ID having fewer than 100,000 potential values .

US 2021/0082583 A1 Mar. 18 , 2021 39
3. The method according to claim 2 , wherein said gener ating an ID comprises generating a unique ID and also generating said ID as a portion of said unique ID .
4. The method according to claim 1 , further comprising changing said ID periodically .
5. The method according to claim 1 , further comprising generating a second ID and transmitting said second ID or indication thereof together with said ID .
6. The method according to claim 5 , wherein said trans mitting a second ID is carried out only at a fraction of said proximity events .
7. The method according to claim 6 , wherein said trans mitting comprises transmitting also second IDs previously received from others of said electronic devices .
8. The method according to claim 6 , comprising gener ating an indication of closeness of a population met by said electronic device based on said received second IDs .
9. The method according to claim 1 , wherein said score depends on an estimation of propensity of proximity of said one or more other devices .
10. The method according to claim 1 , wherein said generating said score comprises counting the number of received IDs .
11. The method according to claim 10 , wherein said counting comprises counting unique IDs . 12. The method according to claim 10 , wherein said
counting comprises counting IDs with a weighted parameter , said weighted parameter is generated by analyzing said exchanged second IDs .
13. The method according to claim 1 , wherein said generating for said particular device comprises transmitting said score to a server and generating said prioritization on said server .
14. The method according to claim 13 , wherein generat ing said prioritization comprises comparing scores by dif ferent ones of said electronic devices .
15. The method according to claim 1 , wherein said generating for said particular device comprises generating said prioritization on said particular electronic device .
16. The method according to claim 15 , wherein said generation comprises receiving form a server a list or a function indication prioritization according to score .
17. The method according to claim 1 , comprising dis playing treatment instructions on said particular electronic device based on said generated prioritization .
18. The method of claim 1 , wherein said pathogen com prises a corona virus and wherein said treatment comprises a vaccination and wherein said prioritization is used to select subjects at greater risk of transmitting the pathogen during pandemic to be vaccinated sooner than subjects less likely
to transmit the pathogen . 19. A system for anonymously selecting subjects for
treatment against an infectious disease caused by a patho gen , comprising :
a . a plurality of electronic devices configured to be carried around by said subjects and configured with instruc tions to : i . generate an ID comprising for each said electronic
device ; ii . when in proximity of another such electronic device ,
one or both of transmit said ID or an indication thereof to said another electronic device and receive an ID or indication thereof from said another elec tronic device ;
iii . generating , a score based on a plurality of such received IDs ;
iv . receiving information from a server ; V. displaying relevant treatment instructions to said
subjects based on said received information ; b . at least one server comprising a memory and a plurality
of modules ; said memory comprising instructions for : vii . sending to said plurality of electronic devices
information usable by a circuitry in said plurality of electronic devices to display said relevant treatment instructions ,
wherein said at least one server or said electronic devices comprise instructions to generate a prediction of like lihood of a subject transmitting said pathogen , based on a score of the subject .
20. The system according to claim 19 , wherein said information comprises one or more of subject specific information .
21. The system according to claim 19 , wherein said information comprises general information usable by a plurality of subjects and devices thereof .
22. The system according to claim 19 , wherein said server is configured with instructions to receive anonymous scores for a plurality of said electronic devices and use said received scores to generate said general information , said electronic devices configured to use said general information to determine a relative treatment priority for their respective subjects .
23. The system according to claim 19 , wherein said electronic devices comprises a proximity - detecting module using one or more of :
a . physical proximity data received by means of electronic positioning data of said subject ;
b . a distance indicating sensor which indicates physical proximity of the location of a device in relation to the location of said another device ; and
c . historical location data . 24. The system according to claim 19 , wherein said at
least one server or said electronic devices comprise instruc tions to determine a treatment prioritization based on said likelihood .
25. The system according to claim 23 , wherein said determine a treatment prioritization further comprises one or more of :
a . generating a score component based on a nature of a location where said physical proximity data is related ;
b . generating a score component comprising health data of the subject of one or both electronic devices ;
c . generating a score component comprising a profession of the subject of one or both electronic devices ;
d . generating a score component reflecting relative health risk to said subject if said subject contracts said patho gen ; and
e . generating a score component reflecting damage to society if said subject contracts said pathogen .
26. The system according to claim 23 , wherein when said physical proximity data is related to a location that is either indoors or in a closed space , then said predicted likelihood of said subject of transmitting said pathogen increases by a factor of between about 10 times to about 100 times .
27. The system according to claim 19 , further comprising a vaccination server which allocates vaccinations for a corona virus according to said displayed treatment informa tion .

US 2021/0082583 A1 Mar. 18 , 2021 40
28. The system according to claim 27 , wherein said server comprises a simulation module configured to perform one or both of :
( a ) predict the effect of vaccination on disease spread ; ( b ) predict the effect of an ID transmission probability on
distinguishing between subjects who contact mainly subjects in a same subpopulation .
29. The system of claim 19 , wherein said electronic devices are configured to transmit a second ID and previ ously received second IDs , at a probability of less than 10 % and using said received second IDs to generate said score .
30. The system of claim 19 , wherein said transmitted ID is a non - unique ID having fewer possible values than 10 % of the number of said devices .
*
10/27/2021
Chairman Erickson and Committee Members
I don’t believe there should be state mandates. I believe it is a person’s choice. These
children that have to wear a mask or adults that have to wear a mask is not good for
someone to wear one 8 to 10 hours a day. With the vaccine people are still getting covid 19.
These vaccines have not been on the market long enough to know what the side effects will
be or could be. Again I believe this is a person’s choice, not anyone else’s to make for them.
Thank you for your time.
Brenda Schroeder
Lebo,KS 66856
Vaccine mandate
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Kansas government has no business telling us how to live you were not elected for this. President Biden needs to realize we don't work for him and he obviously doesn't work for United states either. This whole sham should have people hanging from ropeslike Fauchi he's no doctor or he would not be killing people do something about it
Sent from Yahoo Mail on Android
David Schroeder
October 27, 2021
Chair, Senator Renee Erickson Saturday, October 30, 2021, 10:00 AM Room 346-S Kansas Legislative Research Department, [email protected]
Position – Support COVID-19 Vaccination Mandates to Protect Public Health
Chair Erickson and Committee Members,
I’ll keep it brief and to the point. Society has had mandates for immunizations for years to protect individuals and society. This is based on science and years of public health experience. To change course now based on politics would be a grave (probably literally) mistake. Please support COVID-19, and all other scientifically recommended, vaccination mandates. Believe in science – it’s not perfect but the scientists have a much better grip on this situation than politicians.
Sincerely,
Robert Schwegler, M.D.
October 27, 2021
Dear Chairman Erickson and Committee Members,
It is my desire to express through this writing my strong position AGAINST government mandates for COVID-19 Vaccines. It has been my experience that people are capable, without force, coercion, or persuasion, of making decisions in regard to, and in favor of their personal health, their children’s health, all while not causing harm to others. Similarly, in my experience, these decisions are made to a degree of nuance that is unable to be upheld or replicated with sweeping mandates which only have a few recognized exemptions. People are born with rights that are not granted to them through governments. It is good for the government to recognize the rights of people, and better still for the people elected to positions within government to fight to uphold the inherent freedom of people. Further, it is my opinion that through history, governments mandating medical decisions upon the people they govern and ultimately using force to implement those medical decisions has come to no good end.
It would be my strong encouragement for you to choose with swift and decisive actions to uphold the sovereignty of the people for which you have been elected to protect. We are choosing to act as free people and you can choose to go along with us by defending us from government mandates at least in the areas of vaccines. Alternatively, I can choose to actively work with others to replace your positions with people who are willing to fight to uphold the inherent freedom of people.
Thank you for your time,
Mariah Scott
October 27,2021James Sharp
I will be unable to attend on 10/30/21 in Topeka, KS.
My COVID Experience
Chairman Erikson and Committee Members:
I am against the Covid-19 vaccination mandate.
I currently work for Ascension Via Christi in Wichita, KS. I have worked here for 27years. I enjoy my patients and working with my co-workers. We all strive to do our jobsto the best of our ability. That was all tested starting March of 2020. We never stoppedworking. I can say I only had to miss one day of seeing patients due to limiting ouraccess to seeing clients not knowing how the virus worked at that time. But we came towork every day. We knew that there may be unforeseen dangers, but we did our job aswe were asked to do. We were touted as heroes, but I did not see it that way. I saw itas just doing our jobs. Now, over a year later, I was told that despite dealing with covidpositive patients and family and friends. I would be mandated to get a shot. A shot thatI found out utilizes aborted fetal tissue in its development and or its testing for efficacy.My religious convictions do not allow me to take this shot. I informed my employer ofthis through the proper channels. My thought was that they would look at this on a caseby case basis and treat me fairly and justly. I knew that under Title VII of the Civil Rightsact I had certain freedoms and rights. But I got a letter that stated that my religiousexemption had been denied due to the fact that it would pose “undue hardship to theorganization”. And that I had until 11/12/21 to get the shot or lose my job. All of myfellow co-workers who I knew had the same convictions also got the same statement.
Thus now I wait as they play with my family's welfare and future. I have started a newjob search but I now run into the same issue. Businesses afraid to hire me or unwillingto grant a religious exemption due to Federal Government Mandates due to thepresident and his executive order. So they await OSHA standards to be written andOSHA takes its own sweet time in doing so. Thus I just wait. I have worked since I was
5 years old. I have always tried to glorify my Lord in everything I do so shine my light toothers. I am blessed to be born in a country with such potential.
But it is sad when a man can work, wants to work, and is told you can not, because youmust obey the State and not your Lord.
Thank you,James Sharp
Heather Simpson
Dear Chairman Erickson and committee members,
This is my written testimony only. I am very much against the COVID-19 vaccine mandates that
are in place. Personally, I have been given an ultimatum at my place of employment to be fully vaccinated
before December 8th, 2021, or I will lose my job.
Sincerely,
Heather Simpson
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Heather Sloan

Written testimony AGAINST government mandates of COVID-19 vaccines Dear Chairman Erickson and committee members, I am adamantly opposed to any and all government mandates in regards to COVID-19 mitigation strategy. Although we have all been deeply impacted by this crisis in many ways, relinquishing our God-given and constitutional rights to any governmental institution will only make the consequences even more dire for our children and future generations. If we don’t have bodily autonomy or rights as parents regarding the safety and well-being of our children, what else matters? I know my story is only one of millions and that I have been extremely fortunate compared to many. Dealing with the worries associated with any illness or outbreak (especially as a parent) is extremely stressful. However; historically when faced with this issue, people were able to make reasonable risk assessments based on their own family or medical history and could determine personal behavior based on those risks. I believe, when given the choice, most people will do the right thing especially when they are confident in the information presented to them by trustworthy sources. It has been extremely difficult for me to watch my 2 children (3rd grade and 7th grade at the time of government mandated shutdowns) deal with the trauma of being yanked out of school, taken away from their beloved teachers, being told they can’t see their friends, losing a year of meaningful instruction, being forced to wear masks when my little one is especially affected by facial expressions and nurturing, helping them through the frustrations of trying to catch up, and putting my own fears and stress to the side so that they would not be any more traumatized than they already were. In addition, I am considered an essential worker which means I was still expected to report to work in-person during the shutdown. I was only able to accomplish this by working split shifts around my children’s instruction time and sleeping for 3 hours per night during the entirety of remote and hybrid instruction. I know I am extremely fortunate that I was able to at least have that flexibility but it still did not come without its consequences. My job suffered because I was worried about my children, my children suffered because I was worried about my job, my marriage suffered because I was being pulled in impossible directions, and we all continue to experience trauma with each new local/school/state/federal mandate and pressure being placed on our family. The most recent upheaval we have been subjected to is the news that the Kansas Board of Regents has determined that Kansas State University employees fall under Joe Biden’s executive order requiring the COVID-19 vaccine for federal employees and contractors. Based on thorough research, sincere moral and religious objections, and risk assessments based on health history, we have made a family decision to not receive any of the COVID-19 vaccines. As a Kansas State University employee, I am now faced with a life-altering decision—do I relinquish my bodily autonomy and the right to my deeply-held moral and religious beliefs or do I lose my career of 20 years in which I have been an extremely loyal, dedicated employee and risk the livelihood of my family? It is abundantly clear that these mandates—whether economic or mask/vaccine-related—are not based on historically used methods of intense and thorough scientific scrutiny or backed by overwhelming, irrefutable data. As an alternative to vaccination, there actually are multiple treatments readily available that have been shown to be effective but are being demonized or ignored. The “experts” and “the science” we are expected to blindly follow have been so inconsistent and contradictory with “data” and messaging that it’s insulting. This “do what you’re told, or you are no longer allowed to participate in society” approach will only continue to erode the faith people have in every institution and to divide us

as a people. Most of us who have chosen to not be vaccinated are conscientious, hardworking, decent people who just want to mind our own business, take care of our families and enjoy the privilege of living in the greatest country on earth (for now), yet we are being portrayed as filthy, disgusting, unintelligent, and uncaring. As I mentioned before, if we are unable to maintain bodily autonomy along with all of the rest of our God-given rights, what else matters? In closing, I implore all representatives of the State of Kansas to do everything in their power to stop these illegal and unconstitutional mandates and guarantee that the working class of this state can continue to provide for themselves and their families during this unprecedented and difficult time. If we are forced to continue relinquishing our guaranteed rights one by one with ever-moving goalposts and ever-changing narratives, it will not end until they are all gone. Please, please help us to save this country before it is too late—she is too precious to give up without a fight. Thank you for your time and consideration.
1. Amy M. Sollock
2. Written testimony only
October 27, 2021
Dear Chairman Erickson and fellow committee members,
I am writing to you today to assertively express my position AGAINST any government mandate of COVID-19 vaccines. It is with absolute certainty, that this is a breech of our constitutional rights and a complete violation of our personal and religious freedoms.
As a little girl, I knew that Cooperative Extension work is my true calling and I’ve dedicated my entire career to the youth and communities of Kansas. I have worked for Kansas State University for 15 years and have received exemplary performance reviews the entire time of service. I work around the clock to further our land grant mission and to bring the University to the people of Kansas and have never given them reason to question my abilities, competencies or loyalty to their mission. It is absurd to me that the Kansas Board of Regents feels that it is within their authority to make decisions for my health and medical needs. A government mandate related to the covid-19 vaccine is a ridiculous overreach of their power.
This vaccine mandate has NOTHING to do with public health or safety. This defies logical science and research to every possible degree. If vaccinated people can still contract and spread the virus, then how does requiring a vaccine help the common good? If people with natural immunity and antibodies are proved to have a stronger resistance to the virus and its symptoms, than why isn’t that sufficient? If the KBOR has any integrity left, they’d place higher value on the importance of what real research and science is telling us. They recognize that this is a complete violation of our constitutional rights and political stunt tied to federal funding.
If you do not take action NOW against this mandate, K-State Research and Extension will suffer a STAGGERING loss of county agents and specialists. A loss of this magnitude would be catastrophic to not only our KSRE system, but to all 105 Kansas counties. I feel strongly that KSRE would not be able to recover. Not only will it impact the employees directly effected by termination, but our families and children across the state of Kansas. The ripple effect would be felt indefinitely, with the loss of programming around 4-H youth development, mental health, healthy aging, agronomy, financial management, master gardeners, just to name a few.
If we can’t depend on our Kansas legislators to fight for our constitutional rights, then you should ask yourselves how you got to where you’re at. You work for the hardworking, law abiding people of Kansas. Stand up for what you know is right. Stand up and fight to protect us and our jobs. It sickens me to think I will be terminated from a position that I love and am dedicated to. What’s even more sickening is that my employer thinks it is within their authority to require a medical “procedure” as a condition of my employment status.
I can’t believe that I find myself stuck in this miserable position and I can’t believe we have let our government get so far out of control that I am writing you this letter today. It baffles me that this is the United States of America, the greatest country in history, and that our personal liberties and constitutional rights are being stripped away.
It is time to ACT. I beg you to take action immediately to stop and retract this vaccine mandate. The people and communities of Kansas are depending on you.
Sincerely,
Amy M. Sollock
October 26, 2021
Chairman Erickson and Committee Members:
I respectfully urge you to do whatever you can do hold true to your oath to defend the Constitution, especially the inalienable, individual rights of Kansas citizens. It is not right that the federal government step in and impose a medical procedure on anyone if it is against their conscience or religion. All medical decisions must be left solely with the individual with the help and guidance from a respected medical professional of their choosing.
It is not the place of any government, whether federal, state or local, to impose upon individuals a requirement to inject or alter their body in any way in order to earn a living. I urge you to do your job to represent the people of this state and not let any form of government get in the way of the people and their God-given rights.
Thank you for your time.
Becca Sowers
October 27, 2021
Chairman Erickson and Committee Members:
I had Covid last year. I have natural immunity. I am absolutely against the Covid-19 vaccine mandate! I have been at my job for nearly 20 years and to think that I may be forced to leave because the government wants me to inject myself with a substance that carries a risk that may leave me disabled and unable to provide for my family is absolutely infuriating! Isn’t this supposed to be a free country? Why does it feel more like what I learned of Nazi Germany lately?
You have been elected to represent me, my family and my co-workers that simply want to provide for our families without the threat of government overreaching further than they already have for decades. If you don’t stand up and find backbone that the first settlers in Kansas had, I will work to replace you with others who will.
Thank you.
Joel Sowers
From: Keri Spencer To: Chairman Erickson and Committee Members Subject: Written Testimony to STOP Government Overreach COVID-19 Mandate Written Testimony: As a nurse practitioner serving people in Kansas who are in Hospice care, it is an honor to share my concerns about Covid-19 vaccine mandates. Not only am I a healthcare provider I am a mother of two daughters ages 19 and 15. My husband works in a large factory setting and I have a mother with COPD. I am AGAINST Covid-19 vaccine mandates in the State of Kansas. A vaccine of any type is a treatment and medication that is administered by way of injection. I educate people daily about their right to decline or accept medical treatments and/or medications. These are individuals who deserve to be informed about potential side effects, long and short-term outcomes and the course of care for the prescribed treatment. Each one of us is an individual and we should not be expected or forced to take an injection of anything just because the government, healthcare establishment, insurance companies, pharmaceutical companies or religious communities say we should. Choice is a God given right. Those I am concerned about the confusing information that comes from our government leaders. This has led to distrust and hesitancy for many. It is no secret that money talks in the world of Big Pharma. It exists and not addressing the financial veins that inhabit government and drug companies is dangerous. I am concerned about package insert storage instructions for the Covid-19 vaccines. If these instructions are not followed with precision is the vaccine rendered in-effective yet still given in this high-vaccine push in clinics and health departments across the state? I am concerned that asymptomatic spreaders of Covid-19 were labeled as the lethal in our society prior to the vaccine availability and now the vaccinated are spreading it to those who were vaccinated but are not protected due to vaccine resistance and those who cannot be or choose not to be vaccinated. It is concerning, the healthcare workers who have worked tirelessly to take care of those with Covid-19 and got the virus and recovered then went back into the care facilities and hospitals to continue providing care to the sick are being treated terribly by their employers because they choose not to get the vaccine. It is imperative that the power of the Human Immune System be recognized for what it is. Powerful and protective. The “New Segregation” that has developed over the past 2 years is now swarming the individuals that do not want to be forced to take the vaccine. People are being guilted into getting an injection that is not making the virus go away like government has touted. Never has a vaccine been so blindly pushed than with the Covid-19 vaccine. People who believe to be fully vaccinated are still getting it and passing it on with knowing. Never before did we hear that people vaccinated with smallpox, mumps or polio were contracting these diseases.
This testimony of concern is only a partial list of concerns: quarantine, school closings, isolation of our elderly, parent’s rights and mask mandates. Much more is at stake regarding rights of Kansans. My request for Kansas leaders recognizes and uphold each person’s individual right to accept or decline the Covid-19 vaccine. NO Person should be pushed, coerced or guilted into receiving a treatment or medication. I ask that this vaccine not be MANDATED IN THE STATE OF KANSAS. Thank you and God Bless each of You as you protect the rights of all Kansans. Keri Spencer
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
Briana Stephenson
Chairman Erickson and Committee members,
I will not be able to be in-person. This is my written testimony. I am completely against government mandates of COVID-19 shots (vaccines if that is what you must call them, even though they aren’t vaccines). I believe it is up to each individual person/parent to decide what is best for them and their family.
The Government should have no say in whether or not I receive a vaccine.
Sincerely,
Briana Stephenson
Ryan Storrer
Written Testimony
Chairman Erickson and committee members,
I am completely against any and all COVID vaccine mandates. Every US Citizen has the birth right to decide what is put into our bodies. These individual rights have been exercised by those who have chosen to receive the COVID shot. While we defend their right to receive the vaccine, we are also defending our right to refuse it without coercion. These rights cannot exist without each other. Those who feel comfortable with this treatment, may not be comfortable with the next vaccine decision used at that time. It is also with this in mind, that we must protect that right to make all of our own medical decisions without coercion.
The current vaccines available is merely a vaccine study, and does not involve a time-tested product. Having reviewed the FDA, Moderna, and Pfizer websites and their posted statements, it appears that the product being used in the United States is not the same product that the FDA authorized. Moderna clearly states that the product in use, will remain under the EUA. While we reserve our birth right to choose, many people would likely be more confident in a medical treatment that has been around for ten or more years. The CDC is ignoring their own VAER system, which is showing very large numbers of injuries. This means their data is incomplete and their conclusions are suspect. Also, the fact that the industry pushing this, has been proven to put wealth ahead of safety, is a huge red flag concerning the safety of this new treatment. Every pharmaceutical drug that has been removed from the market for injuries, was approved by the FDA in order to be put on the market.
In regards to natural immunity, since when does that not play into our defense against illnesses? The government is ignoring the most important defense function that we have. Being infected and recovered has been proven to create, as good or better, antibodies than any vaccine. When necessary, a safe and effective vaccine merely stimulates our own immune systems, but it is our own immune systems that do the work. Even the vaccine manufacturers have clearly and repeatedly stated that the vaccines do not stop the carrying and transmission of this virus. Individual studies have confirmed this to be true. Therefore, arguing that an individual’s vaccination is protecting others, is purely ignorant.
For myself, I have been watching the communities that I live and work in. Those communities change frequently as my work locations change. I have not seen any of those communities being ravaged by this virus, contrary to what media has reported about those very communities. People have, for the most part, continued on with their daily lives while doing their best to navigate through the panic and fear driven by the media. Without wearing any mask, I have been directly exposed to at least three different people with COVID at different times, last year and this year. These individuals were very symptomatic and had positive tests, yet, I never got sick. I’ve never had a flu shot, yet I don’t get the flu. Even though the illness has been in our home, only one person became ill, and they fully recovered. We are fine and have no reason to live in fear of something that is less likely to harm us than being in a traffic accident.
Our jobs have been considered to be essential, but these jobs are now being held hostage by tyrants who make claims of safety and efficacy, without having any factual proof. Whose “science” is correct, the scientists on the drug company and/or government payroll, or other scientists that have reached

opposite conclusions? Obvious motives definitely call the industry/government scientists’ reliability into question. Several other industries and emergency services have already lost many experienced and skilled workers because of these mandates, regardless of the source of those mandates. Those jobs are not filled the next day, week, month, or many times, years. It takes lots of time and resources for companies to replace skilled workers. Literally replacing a workforce is a very costly prospect. If Kansas allows these overreaching mandates to happen, it is creating a lose-lose situation for everyone. If Kansas does not pass legislation to protect their workers from government overreach, is likely the state will lose workers and their families as they look for jobs in states that have already passed legislation. This will cost all Kansans, as those income and consumer sales taxes will leave with them. On the other hand, Kansas could see an influx of residents from tyrannical states should our state government protect individual rights, thereby securing our jobs. Simply put, it is the duty of our government to secure our rights and not hold them hostage. Securing those rights could increase our tax base, but following tyrants will reduce that tax base.
10/27/2021
Chairman Erickson and Committee Members:
I stand in opposition to any mandate for the COVID “vaccine.” Some of Kansas’ biggest employers are
mandating the vaccine now. This legislative body had a chance to stop that last spring. It’s time to
correct that now. But I’m afraid by the time you are able to correct the oversight from last spring, it will
be too late for these employees.
K-State is standing in direct opposition to Kansas law. You must come down HARD on this violation. Joe Biden saying he was going to have an executive order enforced by OSHA is not even an executive order. And those are not laws! No jab, no job is not a choice. It’s clearly coercion.
May I also point out that EUA medications cannot be forced on anyone. The approved “vaccine” is not
available in the United States. Ingredients in the EUA trio are not disclosed.
Yesterday, the FDA approved the Pfizer vaccine under EUA for kids ages 5-11. One of the voting
members said, and I quote, “We’re never gonna learn about how safe the vaccine is until we start giving
it. That’s just the way it goes.” These people are evil.
This “vaccine” has had more adverse effects and deaths in NOT EVEN ONE YEAR than the entire history
of the VAERS system. 818,042 adverse events, 83,412 hospitalizations, 26,199 disabled, 2,631
miscarriages and 17,128 deaths. It is estimated that only 10% (I’ve even seen 8%) of adverse events are
reported. We can see where this is going. The government is after our children. Mandates are coming to
participate in sports, go to school, and YOU IN THE LEGISLATURE are our last defense. Don’t let them
shut down small businesses. Don’t let them have our kids. Don’t let them mandate our freedom. Stand
for liberty. This is your moment. The people of Kansas are counting on you. And I still think we need an
immediate special session.
Thank you for your time.
Sincerely,
Melissa Stramel
Chairman Erickson and Committee Members –
My name is Joanna Struble and I am a resident of Lenexa, KS. I am writing you today to state that I am
strongly against government mandates of COVID-19 vaccines. The response to COVID vaccine has
already cost the livelihood of countless small business owners. Several members of my family are
currently facing termination because of the federal overreach. Yet, the overreach continues. To
mandate a vaccine that neither stops infection nor transmission is unethical and nonsensical. To make
the statement that it’s for my own good is unethical and nonsensical. To make the statement that it is
to protect those already vaccinated is, you guessed it, unethical and nonsensical.
I am a healthy 33 year old woman. The NIH spent millions of dollars to study the impact of the vaccines
on women’s reproductive health. These studies are not going to be completed for at least a year. Does
my reproductive health no longer matter? Recently, several countries are pulling specific vaccines away
from young men because of the increased risk of myocarditis. Meanwhile, many teenagers and young
men had to be hospitalized before this was admitted. Does the health of our youth no longer matter?
This is a failure to the highest degree – please do not create an economic crisis, mental health crisis and
exacerbate the unemployment crisis by supporting these mandates. We urge you as Kansans and fellow
humans to do the right thing.
Thank you,
Joanna Struble
Cheryl Stucky
_
Written Testimony to stop government over reach tovid-19 Mandate
.. �
Position: Against the Mandate
Written Testimony Only
To Chairman Erickson and Committee Members,
I do not agree with the MANDATE.
I am 45 years old. I am educated and I have a great job that I enjoy every day. I was raised in a
Christian, blue-collar, middle class home. I appreciate the sacrifices that were made for this
great nation and for our freedoms. I am worried and frankly sacred that the mandate is the
start of losing my personal freedoms.
I do not agree with the mandate. It is my body and I should have the right (within reason) to
choose what I want to do with it, inject into it, and subject it to.
The argument for the mandate, is similar to the argument for abortion. If a woman wanting an
abortion, can say, it's "her body" and her choice ... Why is it not the same for "my body" and
my choice?
We work hard, we pay taxes, we support our service men and police department, we attend
church, we serve in our community, and we are blessed to live and thrive in this great nation.
For all practical purposes, we are quality members of society. We don't want to fight the
system, there is good in government ... But we do not believe the government should have
complete control over Her people or mandate their freedoms. We believe in freedom and the
right to choose whether or not we want the vaccine.
I will support my husband, should he be fired over this mandate. His firing will be our way of
taking a stand for what we believe in. It is our way of fighting for our rights, freedom and
liberty. We are hopeful many others will take a stand as well. We believe this mandate is just
the beginning of "government infringing" on our freedom and our liberty.
Thank you for your time and consideration!
Cheryl Stucky
Jay Stucky
Written Testimony to stop government over reach Covid-19 Mandate
Position: Against the Mandate
Written Testimony Only
To Chairman Erickson and Committee Members,
I would like to say I am against this mandate and against giving up our freedom and our rights. I
am a journeyman lineman for Evergy and have been considered and essential worker for the
last year and half. Now I am faced with the decision to either get vaccinated or to lose my job
and income to support my family. How did we go from being essential workers to not being
needed if we don't receive the shot?
Do I believe Covid-19 is real? Yes, but I also believe we have been lied to over and over again by
our government and the media. According to the data over 700,000 people have died from
Covid. This data is false. 700,000 people did not die from Covid, they died with Covid.
We have been told this mandate is all about saving lives. If the government is so worried about
saving lives that it can give a free vaccine for Covid-19, then why isn't insulin free? Why is
Narcan free to a drug addict who made a choice to overdose on drugs but an epi-pen cost
$350.00 to someone that has no choice? Why aren't cancer treatments free? According to the
American Heart Association, in 2017 868,662 people died from heart disease, more deaths than
Covid. Why isn't every fast food restaurant in the U.S. shut down? Instead of shutting them
down, we can go in and place an order, and "super-size" it.
This mandate is not about saving lives, it is about control. It's about taking away our freedom
to choose for ourselves. It is only the beginning of the government trying to strip away our
freedoms.
When any medication, other than the Covid-19 vaccine, is advertised, they start by telling you
the name of the drug. Then you are told about all the great things it does, followed by all of the
side effects. When the Covid-19 vaccine is advertised we are told the name, then how great it
is, but the side effects are left out. WHY?
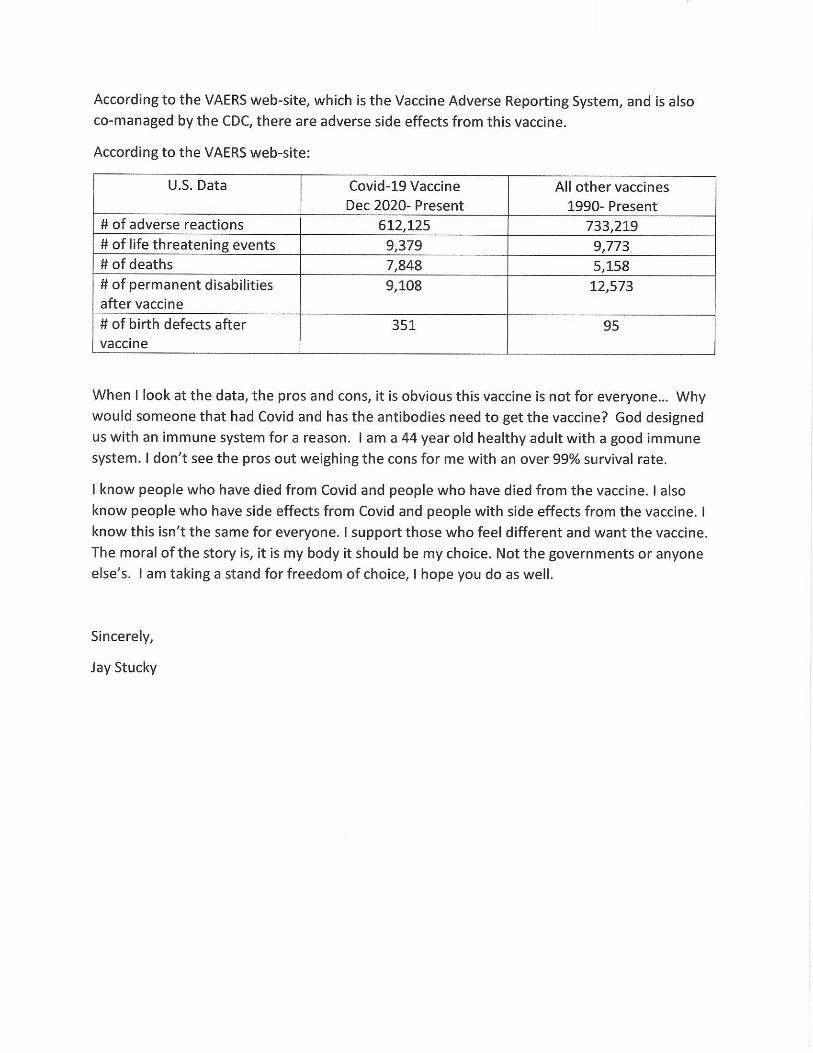
Dear Chairman Erickson and Committee Members,
My name is Mandy Swift. I have been a Registered Nurse since 2006 and graduated from Washburn University School of Nursing. I have a very strong opinion of the current covid 19 mandates happening throughout the U.S. and in particular, in Kansas. I will NOT be giving an in-person testimony but only a written testimony. I am AGAINST government mandates & overreach of the COVID-19 vaccines.
My testimony comes after MUCH research regarding the vaccines, the safety & efficacy of the vaccines, and the economic, mental, spiritual and physical hardships this will bring to thousands and thousands of individuals.
First, we have already seen that the efficacy of these vaccines wanes after just 6 months, quite possibly less time. We are seeing thousands and thousands of counts of side effects and reactions to these vaccines, ranging from heart attacks, seizures, blood clots, myocarditis, pericarditis, blindness, Guillian Barre Syndrome, early miscarriage, pre-term labor, & still births. The list is extensive and if we were really looking into these issues arising after vaccinations from the mRNA and J&J vaccines, we SHOULD have stopped them a LONG time ago! So, not only does the vaccine efficacy wane in just 6 months, but the safety has NOT in fact been established in adequate animal testing prior to mass distribution on the public. This is reckless, foolish and NOT what healthcare professionals gave an oath to get behind. At the very best, we should have only offered these vaccines to those that had comorbidities that made them high-risk to covid in the first place AFTER giving them INFORMED CONSENT regarding the risks and benefits to each vaccine.
Secondly, we are NOT giving any credibility to natural immunity and we ABSOLUTELY should be. At this point in time, 20 months into the pandemic, we have reason to believe that a large majority of people have natural immunity to covid-19. Testing whether antibodies exist in individuals and checking antibody levels would tell us SO much about where we are in reference to herd immunity. Studies are already showing that individuals with vaccine immunity are 13x more likely to get covid again than those with natural immunity! We are seeing breakthrough cases in our vaccinated individuals as early as 6 months post full vaccination dates. The vaccine mandates are not taking into account all the people that now have natural immunity to covid. People are having to prove their positive test result was within the last 6 months, when we know full well that natural immunity is lasting FAR LONGER! Most places are not even accepting natural immunity as a basis for not getting vaccinated. If this is really about the HEALTH of our community and state, we would be looking at natural immunity to get our state back to normalcy as quickly and safely as possible. Because the reality is that those with natural immunity are FAR safer and are not seeing the breakthrough cases like the vaccinated.
Third, as someone that has helped over 40+ people in Topeka and across the U.S. with religious exemptions, it's clear how the mandates are causing undue hardships on some of the most involved and dedicated people that have served this entire pandemic. Looking at one of our own local hospitals in Topeka, Kansas, prior to the mandates they were already short over 350 nurses. The overwhelm that existed was largely due to the lack of staffing, NOT covid admissions. In hearing testimony from local nursing staff and doctors, many patients coming in for healthcare were largely NOT covid related. And we most definitely have NOT seen a huge influx of pediatric covid hospitalizations and deaths. Kansas is still sitting at 3 pediatric covid deaths in the last 20 months. The vaccination mandates will place our local healthcare facilities in a MAJOR predicament. While still in the middle of a pandemic, we will be firing our most dedicated and educated staff. While in a HUGE nursing shortage, we will be firing some of the very best. MANY of these healthcare professionals sat next to covid positive dying patients when their family was not allowed by their bedside. MANY of these nurses risked their own health, donned PPE each day, and worked tirelessly to keep complete strangers alive. They did this without prejudice. They did this without questioning these individuals' prior health history that could have very easily made them more susceptible to covid-19. They went to work, laying down their own fears to save the next person. They worked 14 months without a vaccine, SAVING LIVES and LAYING DOWN THEIR OWN. Now, we aren't even considering their reasons for not wanting the vaccines. We trusted them to save lives but we don't trust them to make their own medical decisions. They have become disposable. Many of these people (not just healthcare workers) have served endlessly while placing their own families at risk. People should not have to choose between providing financially for their loved ones and getting a vaccine that is proving to only be effective for 6 months with unknown long term safety. This is not a CHOICE. This is COERCION and unconstitutional.
If we as Kansans want to do the right thing, we would encourage high-risk individuals to seriously consider the vaccine after informed consent is given. We would NOT mandate a vaccine that is still in trial phases. We would NOT threaten an individual's job and livelihood. We would NOT mandate or even encourage those that are young, healthy and low-risk to dying of covid to be vaccinated. Our children are our future. We, as parents, are entrusted to protect our children and Kansas needs to be the place known for placing children's health and safety first. Children are at a very, very low risk of dying from covid. Many children won't even have symptoms that make it necessary to seek medical attention. If those that are high risk are vaccinated (at their OWN choosing), children getting covid will not be a threat.
President Biden's mandate on businesses is a complete overreach of power and unconstitutional. I would expect and hope that the state of Kansas would fight these mandates for the betterment of their people. I believe that Kansas has the ability to do this and will make the right decision.
Thank you for hearing my personal testimony and stance on the covid-19 vaccines.
Mandy Swift

Written Testimony to STOP Government overreach COVID 19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
To Chairman Erickson and committee members: My name is Sandra Temple of 215 Chestnut St., Wamego, KS 66547. My phone number is785-640-1159. This is my written Testimony to STOP Government overreach COVID 19 Mandates. I am a Registered Nurse, having beenemployed in the medical profession for 42 years. I have been forced to resign a job that I love and leave the nursing profession due to mybeliefs and choice of not receiving the vaccine. I am currently unemployed and searching for any job that will allow me to be a productivemember of society. It has brought financial and emotional strain on my family and me. For the last year and half I have worked on thefrontline in an ER. I have seen people that have received the vaccine and those that have not. Both types of clients have come down withthe virus. Both types have had casualties and successes in fighting the virus. Both types of clients have been carriers. I have first hand seenside effects from the shot be as minor as a sore arm to severe endocarditis, blood clots and neurological reactions. I have chosen not toreceive the vaccine and continue to wear a mask. The point is to allow each individual the right to govern their own health. Let theindividual decide. The mandates are creating forced unemployment, staff shortages, and hardship and division to this country and state. Letus all take a deep breath and use reasonable common sense. Mandates are forcing people to take a vaccine that does not allow themrestitution if a side effect debilitates them. Why is that? If the vaccine works so wonderfully, why are vaccinated persons still getting thedisease? And, why is the Federal Government threatening hospitals that don’t have 100% vaccine compliance with employees? I believe theFederal Government has overreached its power with this mandate. It is my understanding that the 10th amendment of the Bill of Rights waswritten to define the balance of power between federal and state governments. Please fight for your constituents. Push back and stop thecoercion. Thank you for your time. Sincerely, Sandra L. Temple

To Chairman Erickson and committee members,
We have illegals pouring into our country (over 2 million in just the past Biden Administration) who are not mandated to be
vaccinated or tested, while the American citizens are being mandated to be vaccinated and if not, lose their jobs over this. This to
me, is an overreach and unconstitutional. It also is a violation of the Equal Rights Amendment when Americans are MANDATED to
get the vaccination, while illegals are not.
I just received an email from my employer on Monday (10/25/21) saying we as employees need to either get the vaccination or
“voluntary termination”, which is not a voluntary termination, in my eyes as we are not voluntarily leaving our jobs. I’ve been
with the company for over 13 years and due to this mandate, I could lose my job, not by my choice. This is a forced termination
and unjust. The unemployment rates are skyrocketing, and all this is going to do is make matters worse.
This overreach on mandates are destroying the lives of American People who have dealt with enough on the lockdowns and
mandatory vaccination or lose their jobs.
It’s time to stand up and say ENOUGH is ENOUGH. Let AMERICANS decide, as we’ve done in the past. Please STOP this overreach.
Thank you,
Casey Theel

WRITTEN Testimony to STOP Government Overreach COVID-19 MANDATES
To Chairman Erickson and committee members:
When illegals are pouring into our country by the thousands per day not mandated vaccinated or
tested, why should Americans be expected to give up our rights and be exposed by the sick from other
countries? Employee shortages have now grown by a substantial amount due to forced vax mandates.
Our health care professionals constitutional rights and liberties are BEING VIOLATED as are all Americans
rights to decide for themselves and their children.
People who do not wish to be vaccinated should be allowed not to be. My husband and I had COVID
in August 2021 and were hospitalized. We have NATURAL IMMUNITY now, so we would not want to be
vaccinated. People who work out of their homes should be allowed to opt out. Those vaccinated are
getting covid just as fast and are ending up In the hospitals as much as the unvaccinated. As of the first
of October we had more cases of Covid after the vaccines then last year without. We need to respect
the rights given to us by our constitution. We have crossed the line into communism which is apparently
what is happening. This is not the law and must be stopped. NO MANDATES!
Thank you Janie Theel

WRITTEN TESTIMONY TO STOP GOVERNMENT OVERREACH COVID-19 MANDATES
To Chairmen Erickson and Committee Members
I am against the mandates to require vaccinations for Covid before we are allowed to dine, travel, work
at our jobs and live in peace and harmony. Mandates destroy optimism which is essential to individual
achievement. We need more freedom not less. The right to choose for oneself is protected by the
constitution. I have had covid, as have so many, and have been assured this is better than vaccines
which must be repeated every 6-12months. Vaccinations are personal and should be decided by noone
other then an individual and doctor. Thank you for considering my ideas.
Kenneth Theel
Dear Chairman Erickson and committee members! I appreciate you having this event, and thank you for listening to me.
Covid-19 never bothered me. Period. What the government has done in response to Covid-19, however, the lockdowns, shutdowns, mask, mask mandates, social distancing, stay at home order, quarantine, testing, vaccine, vaccine mandates, and vaccine passports, has effected me a LOT!!!!!!!! It has effected everybody a lot.
Mandates aren’t constitutional. The first amendment of the United States constitution, says ‘Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the of the people peaceably to assemble, and to petition the Government for a redress of grievances’.
Mandates violated almost the entire first amendment. Mandates forcing you to stay at home, and prohibiting people from going to church. And anywhere else. Freedom of religion, gone. Freedom of assembly, gone. Facebook, twitter, youtube banning people that oppose these new restrictions. Freedom of speech, gone. Youtube/google/Facebook/twitter taking down media companies that oppose their view point. Freedom of press, gone.
My personal experience with mandates is this. In February 2020 I was in a theater production at the Lawrence arts center. It was fun, amazing, cool and I wanted to do it again. I was also enrolled in tap dancing, and art at the Lawrence arts center.Then; lockdown, masks, social distancing. Suddenly, everything was also online. I wasn’t able to adapt to online dance class, so I stopped that. Art class was also online, but after one semester, I had to stop that as well. As for theater productions, the were now performed on zoom. I didn’t even bother with that one. All of a sudden my life was very empty. My piano class was on Skype, we stopped seeing as many friends, and, really my life not only was not empty, I felt empty. I know I could have done things on zoom, but there is no replacement for reality.And I know for a fact, that children, like me, really, really, need their social life. Thats life.Then mask mandates were really enforced. If you go here, you’ll need a mask. If you go there you’ll need a mask. Masks became a part of everyday life. Sometimes I would get heartburn after I wore a mask. But if I refused to wear one, I could be kicked out of wherever I was.

However, I should be responsible for my health choices. Hence the name my health. The only other people that can have a say in my health are my parents. Period.So, masks became enforced. It didn’t stop there.Enter vaccines/injection/jab/shot.I knew my family and I wouldn’t get it, from the beginning, so when they rolled it out I didn’t really think about it that much. Then came the vaccine mandates. New York, NYIf you have the vaccine, you can do whatever you want. Eat in a restaurant, watch a broadway show etc…. If you don’t, you can do almost nothing.THAT IS SEGREGATION!!!!!!If you’re not a Jew, you’re good. If you are, then you are a lower class of the human race. Therefore you can not; eat in a restaurant, enjoy entertainment venues, use the transportation system etc…. This is coming true.Only, the “bad” people this time, are the unvaccinated.Thankfully, its not as bad here in Kansas as it is in New York. But it is getting to be that way.The arts center in Lawrence, which I mentioned earlier, now requires the vaccine for anything that has to do with them. If you qualify for a religion exemption, however, you can still enjoy in the activities there, if, you get tested. Basically the vaccinated get it easy and the unvaccinated get it hard.Hospitals(in Kansas) have the “right” to now reject unvaccinated from any treatment. Even in life or death situations.THAT IS COMPLETE AND TOTAL DISCRIMINATION AGAINST THE UNVACCINATED!!!!!!
What I want to see in Kansas, is laws that protect the rights of every Kansan, vaccinated and unvaccinated alike. I want laws, that allow unvaccinated to participate in the same activities that the vaccinated participate in. I want laws that allow every Kansan to decide for their own, their own health choices.I want Kansas to mandate freedom. No more masks required signs, no more vaccination required signs, no more social distancing signs. And no more segregation against the unvaccinated.We all matter.And finally, I want the Kansas government to acknowledge that 17,000+ people have died of the Covid-19 vaccine. It says so on VAERS.
No more discrimination.
No more segregation. Just freedom.
Thats all I want.
Respectfully, Benjamin Thoennes
October 26, 2021 Dear Chairman Erickson and Committee Members: Although I hope to be present on Saturday for the hearing, I want to submit my written testimony to strongly oppose the current COVID-19 “vaccine” mandate. I am a wife, mom of four children, homemaker and home educator. Even though my job is not in jeopardy of being taken away from me, I am writing to convey to you how I have been affected by this mandate. Below are the stories of people I know personally. Some of them may have already submitted testimony to you, however many, I am sure, have not. Their stories have broken my heart, and they need to be heard. All of these individuals have something in common. For various reasons, they do not want to inject into their bodies a substance that has NOT been fully tested or approved, is still in the experimental stages, does NOT prevent the spread OR contraction of COVID-19 (a virus with a very high survival rate for these healthy individuals) AND they will all likely lose their livelihoods if they do not comply with this overreaching government mandate. It is difficult to believe we live in America after writing that last sentence. Here are their stories:
• My husband is awaiting status of his religious exemption, but if denied he will lose his job at a major aircraft company located in Wichita on December 8th. He has been a proficient engineer for over twenty years and has hardly missed a day of work because of his incredible work ethic. As I mentioned, we have four children, and he is the sole provider of our family.
• My daughter is eighteen years old. She recently graduated high school and is currently working toward a bachelor’s degree. She is a 4.0 honor student and accepted a summer internship at a major aircraft company in Wichita and was offered a great part time job afterward. She was excited to have a good paying job to pay her way through college but now is afraid to be interrogated for submitting a religious exemption and does not want to be fired from her first real job. She will likely submit her two-week notice and quietly leave, forced to find a lower paying job to avoid college debt.
• Our neighbor is a hard-working physician’s assistant in the medical industry. She is also the sole provider for her family with three children. Her religious exemption was recently denied, and she is facing the reality of losing a career that she has worked extremely hard for and has done for many years.
• We know another man who works in the local aircraft industry whose wife is pregnant and is due to deliver their (long-awaited, after many miscarriages) baby in December. If he does not comply, he may lose his job and health insurance the same month his baby is born.
• Two people we know personally will retire early though their plan was to continue working for a few more years. They will miss out on possible early buyout incentives from their company and will not be as financial stable as they had hoped to be because they feel forced take an intravenous medication they do not feel comfortable with.
• Several men we attend church with feel very coerced into receiving the shot that they do not want injected into their bodies. One man is in the military with a wife and five children. He could retire in three years but does not have another way to provide for his family.
• One man my husband works with has been losing sleep over the decision to be inoculated. He is in conflict with his wife over the decision and is in constant worry.
• My cousin is a home health care nurse. She is a single mom of one in college and another in high school. She has already had the virus. She does not want or need the injection but will face losing her job soon if she does not receive it.
I know there are thousands of more stories just like these. I hope you really stop to listen to each and every one of them. These people want to work! They want to be contributing members of the society and to the local economy, and they want to provide for their families. They do not want to be unemployed. They have the right to life, liberty and the pursuit of happiness. And the role of government is to uphold and honor that right given to us by GOD alone. You have an obligation and a responsibility to do the right thing for the people of Kansas. I ask that you hear these voices and act accordingly and please act swiftly. Thank you, Yolanda Thomas
October 27, 2021 Chairman Erickson and committee members, My name is Amanda Thompson, a Kansas resident residing in Olathe, KS. I am submitting my written testimony for your review and consideration. My family and I are completely against government mandates related to COVID-19 vaccines and forced masked mandates. Requiring individuals at any age to inject something into their body or wear something that restricts oxygen from entering the body against their will is not only unlawful but unethical. It goes against who we are as a country and a people and we should all be highly outraged regardless of how you personally feel about masks or vaccines. If you choose to wear a mask or inject yourself with an EUA shot then I respect your decision. My family and I should be extended the same courtesy. My body, my choice! We have three children and we know at least one of them has a vaccine injury. Our son is autistic but our government has given a pass to any vaccine manufacturer/company so they cannot be held accountable. Is there any other industry that isn't held accountable? My husband also experienced difficulties after being required to get a series of vaccines before an extended work trip to India. Our family is not anti-vaccine. We are anti- the stabilizing agents they put in them and the combination of vaccines they insist on giving children at such a young age. We did what most people did when we were younger and raising small children, we trusted our doctor's and government that they would be informed and recommend safe, researched options for our family. Sadly, we learned the hard way and are now living in a country where we can no longer take people at their word and assume that those that should have our best interest at heart actually do. The mandatory mask mandates in our county and in our schools is unconstitutional. My 11-year-old son, with autism, came home multiple days last year with active mold in his masks. Thankfully, we were able to get a mask exemption for him which led to other issues like isolation and being bullied. Look around, these masks are being sat on the floor during lunchtime and athletic games when kids are in the game, touched by peers, left in cars and used day after day without washing or being sanitized... the toxic bacteria is harmful and doesn't promote good health or hygiene, in fact it is making our kids sicker. Have you looked on the package or box of mask lately? It literally says, does not prevent transmission of bacteria/viruses yet they are required to wear them. It is proven that the oxygen levels significantly decrease when wearing a mask for any length of time. What do our brains need to develop, learn and grow, oxygen! That doesn't even take into consideration the injustice we are doing to our kids due to lack of facial expression and connections. My kids social/emotional health has taken a huge hit and they continue to struggle with anxiety, social issues and fear of what might happen. They are losing connections with their peers and teachers and for what? It makes no sense that schools are required to mask but they can literally go anywhere else outside of the school day unmask.
My middle daughter has unilateral hearing loss and under normal circumstances struggles to hear her teachers and peers. You put a mask on them and that becomes a much bigger challenge which further isolates her. The official county mandate in Johnson County states that if a person interacts with a deaf or hard of hearing person then they are exempt from mask wearing but you won't find a school district or teacher that will stand up and actually allow this to occur. It's discrimination and under normal circumstances would not be tolerated. Who is fighting for my kids, kids like my kids? Is anyone listening? We feel strongly that given the data (actual numbers) and experiencing Covid ourselves, that our natural immune system is more than capable to fight it off. The alarming side effects as well as the uncertainty of how these chemicals will react in the body in the coming years is not worth the risk. We need to be asking the question of who is getting paid for these vaccines, why the insistent push literally at every turn to get them and why the shaming, censoring and guilting of a large part of the population (those of us that choose otherwise) is being tolerated? People's livelihoods are at stake due to the recent mandates from employers to require their staff to be fully vaccinated. We are conditioning the people of the USA to turn away from our countries values and turn on one another. This is weakening our country and will have lasting implications if something is not done to right this wrong. Sadly, our family has experienced great loss at the hands of COVID-19 and the current narrative in this country. Both my father-in-law and husband's aunt passed away in hospitals this year due to limited available treatment and further government overreach. They were not allowed treatment that has been researched, proven effective and available in other parts of the country/world by doctors who are being censored and losing their jobs because they will not follow the narrative. Remdesivir and ventilators were the only allowed treatments which essentially led to kidney failure and ultimately death. My husband begged the physician in charge of my father-in-law's treatment to treat with ivermectin and was told it wasn't an option because it wasn't approved by the CDC. The same doctor for a time refused to talk with my husband about his father's care. My husband was the next of kin and had a medical power of attorney. It is criminal and they need to be held accountable. Sadly, we are not the only ones that experienced this and it could have been prevented. Living in a country that is supposed to be for the people, governed by the people does not look like this. You know it and I know it. Our country has been hijacked. Every day more and more information becomes available about what is happening (before it gets censored) and we must take a stand. You have been elected by the people for the people to do what is best for the people of this great state and country. Now is your time to take a stand and make an impact that can save us all! With great power, comes great responsibility. I implore you to do the right thing for all people! Thank you for your time and for standing up for what matters most, FREEDOM! Sincerely, Amanda Thompson
Chairman Erickson and committee members,
My name is Shad Thompson, a Kansas resident residing in Olathe, KS. I am submitting my written testimony for your review and consideration.
My family and I are completely against government mandates related to COVID-19 vaccines and forced masked mandates. Requiring individuals at any age to inject something into their body or wear something that restricts oxygen from entering the body against their will is not only unlawful but unethical. It goes against who we are as a country and a people and we should all be highly outraged regardless of howyou personally feel about masks or vaccines. If you choose to wear a mask or inject yourself with an EUA shot then I respect your decision. My family and I should be extended the same courtesy. My body, my choice!
We have three children and we know at least one of them has a vaccine injury. Our son is autistic but our government has given a pass to any vaccine manufacturer/company so they cannot be held accountable. Is there any other industrythat isn't held accountable? I also experienced difficulties after being required toget a series of vaccines before an extended work trip to India. Our family is not anti-vaccine. We are anti- the stabilizing agents they put in them and the combination of vaccines they insist on giving children at such a young age. We did what most people did when we were younger and raising small children, we trusted ourdoctor's and government that they would be informed and recommend safe, researched options for our family. Sadly, we learned the hard way and are now living in a country where we can no longer take people at their word and assume that those that should have our best interest at heart actually do.
The mandatory mask mandates in our county and in our schools is unconstitutional. My11-year-old son, with autism, came home multiple days last year with active mold in his masks. Thankfully, we were able to get a mask exemption for him which led to other issues like isolation and being bullied. Look around, these masks are being sat on the floor during lunchtime and athletic games when kids are in the game, touched by peers, left in cars and used day after day without washing or being sanitized... the toxic bacteria is harmful and doesn't promote good health or hygiene, in fact it is making our kids sicker. Have you looked on the package or boxof mask lately? It literally says, does not prevent transmission of bacteria/virusesyet they are required to wear them. It is proven that the oxygen levels significantly decrease when wearing a mask for any length of time. What do our brains need to develop, learn and grow, oxygen!
That doesn't even take into consideration the injustice we are doing to our kids dueto lack of facial expression and connections. My kids social/emotional health has taken a huge hit and they continue to struggle with anxiety, social issues and fear of what might happen. They are losing connections with their peers and teachers and for what? It makes no sense that schools are required to mask but they can literallygo anywhere else outside of the school day unmask. My middle daughter has unilateralhearing loss and under normal circumstances struggles to hear her teachers and peers. You put a mask on them and that becomes a much bigger challenge which furtherisolates her. The official county mandate in Johnson County states that if a person interacts with a deaf or hard of hearing person then they are exempt from mask
wearing but you won't find a school district or teacher that will stand up and actually allow this to occur. It's discrimination and under normal circumstances would not be tolerated. Who is fighting for my kids, kids like my kids? Is anyone listening?
We feel strongly that given the data (actual numbers) and experiencing Covid ourselves, that our natural immune system is more than capable to fight it off. The alarming side effects as well as the uncertainty of how these chemicals will react in the body in the coming years is not worth the risk. We need to be asking the question of who is getting paid for these vaccines, why the insistent push literallyat every turn to get them and why the shaming, censoring and guilting of a large part of the population (those of us that choose otherwise) is being tolerated? People's livelihoods are at stake due to the recent mandates from employers to require their staff to be fully vaccinated. We are conditioning the people of the USA to turn away from our countries values and turn on one another. This is weakening our country and will have lasting implications if something is not done toright this wrong.
Sadly, our family has experienced great loss at the hands of COVID-19 and the current narrative in this country. Both my Dad and my aunt passed away in hospitals this year due to limited available treatment and further government overreach. They were not allowed treatment that has been researched, proven effective and available in other parts of the country/world by doctors who are being censored and losing their jobs because they will not follow the narrative. Remdesivir and ventilators were the only allowed treatments which essentially led to kidney failure and ultimately death. I begged the physician in charge of my Dad's treatment to treat with ivermectin and was told it wasn't an option because it wasn't approved by the CDC. The same doctor for a time refused to talk with me about my Dad's care. I was the next of kin and had a medical power of attorney. It is criminal and they need tobe held accountable. Sadly, we are not the only ones that experienced this and it could have been prevented. Living in a country that is supposed to be for the people, governed by the people does not look like this. You know it and I know it.
Our country has been hijacked. Every day more and more information becomes availableabout what is happening (before it gets censored) and we must take a stand. You havebeen elected by the people for the people to do what is best for the people of this great state and country. Now is your time to take a stand and make an impact that can save us all! With great power, comes great responsibility. I implore you to do the right thing for all people!
Thank you for your time and for standing up for what matters most, FREEDOM!
Sincerely,
Shad Thompson
Dear Chairman Erickson and Committee Members:
I write to you today to state my position against government mandates of Covid-19 vaccines. I have recently l earned that my husband’s j ob may be affected by the mandate. He i s an electrical foreman for the IBEW 271 based i n Wichita. The company he works for has sent a letter to their employees stating that they would l ike to protect the medical privacy and religious beliefs of their employees, but due to vaccine mandates, they may not have a choice. He recently completed the electrical component of the runway j ob at the Wichita Eisenhower Airport on time, under budget with praise from his company supervisors. He l oves his j ob and takes pride i n his work. However, i f required to get the vaccine i n order to continue his employment, he will quit. Kansans have the right to be employed or terminated based upon their j ob performance not their personal beliefs.
This i ssue i s not an argument about the merits of the vaccine, but rather an i ssue of whether or not the government can mandate personal health choices for i ts citizens. Health i s an i ndividual responsibility, not a community responsibility. We have been on a slippery slope from “two weeks to slow the spread”, to expanding l ockdowns, then mask mandates. All have been an infringement on our personal l iberties i n the name of safety. If I could sum up the vaccine mandate i n one word, that word would be “communism.” The American government was set up to serve “We the People” not the other way around.
On a related but slightly different note, can we please consider banning mask mandates i n schools? My two oldest children are 6 and 7 years old. Their risk of dying from Covid-19 i s statistically ZERO. Furthermore, any concerned adults they come i n contact with have had every opportunity to receive the vaccine. I have been unable to find any scientific studies proving mask efficacy, particularly i n children. Masking should be a personal choice.
Finally, thank you for your service to the citizens of our state of Kansas. In particular, I appreciate your service as a committee for this hearing.
God Bless, Joslynn Toon

10/27/21
Chairman Erickson and Committee Members:
I have been a nurse for nearly 15 years. One of the first things we learn in nursing school is the
importance of critical thinking. Sadly, this is lacking today.
I work with young people. It is so sad to watch them be "muzzled" all day, every day. They are generally
not severely affected by this virus, yet the psychological effects of masks and isolation have been awful.
Kids are required to wear masks when they perform in concerts and plays, while practicing sports, and in
all their classes. I saw a group of middle schoolers light up when they got to see each other without
masks for the first time in months. People are made to make connections with one another, and that
involves facial expressions—especially smiling. Many kids have not seen a peer without a mask for
months. When will it end?
Not only are kids expected to wear a mask all day, but now they are also going to be offered (or
required) to get an injection of an experimental vaccination. We have no idea how it will affect adults
long term, let alone children! There have been concerns with these injections, yet they are being
downplayed. I know of a young person who was “vaccinated” and within a week had to go to the
hospital twice due to chest pain. As a rule, vaccines and medications take years to come to market. Are
you going to require a vaccine after such a short time?
As of today, I have not had to choose between my job and this unproven, unnecessary “vaccine”.
Unfortunately, I know many who have been forced to make this choice. Some are leaving careers they
love to protect their health, others to stand for their freedom. And why should they have to choose?
This “vaccine” does not prevent the immunized from catching COVID. It does not prevent the
immunized from spreading COVID. It is simply to artificially placate those who are afraid. Please do not
let any more hard-working Kansans make this horrible choice.
The people of the State of Kansas need you to think critically. Stop mandates for masks and vaccines.
Allow us to make our own choices for ourselves and our children. Stand for freedom and common sense.
Thank you for your consideration!
Lynnette Toutges
Written Testimony to Stop Government Overreach COVID 19 Mandates
Robyn Trussel
Written testimony, will try to be in person
Chairman Erickson and Committee Members
I am against the government mandates of COVID19 Vaccines.
I am in a position where by December 8th I have to make a decision to leave behind a 20 year job that I truly love OR put a mandated vaccine in my body that I don’t truly believe is the answer to COVID. My options are a religious exemption or a medical exemption. In which I don’t feel either will make it through the review process. Actually, it is neither of these that I want. I want an exemption that says “My body, my choice”. I’m against this vaccine for work, personal and tax payer reasons.
I work for Kansas State Research and Extension, a job that has Research in the name. A job where I can’t share with our clientele the way my grandma canned tomatoes, yet I need to share the Food Safety, researched proven methods that have been handed down from our Food Science division and Ball Canning. This is the method that is covered by our liability. This is the method we share because it has been researched and PROVEN. Now that same company is asking me to put a vaccine in my body that has not been researched long enough to be a proven manner of protection, or there is not enough research to know what the side effects of the vaccine is.
Another routine that happens in my job is that all flyers, publications, presentations and such have to include the statement of Equal Employment Opportunity which says that we do not discriminate against a job applicant or an employee because of the person's race, color, religion, sex (including pregnancy, transgender status, and sexual orientation), national origin, age (40 or older), disability or genetic information. Yet, here we are discriminating against those who are not vaccinated versus those who are.
My personal beliefs against this vaccine mandate are that our government is using their dictatorship to mandate a vaccine into my body, yet we have a south border open wide letting anyone and everyone in and there is no mandate on any of the millions of people coming into America. We have no idea if they have Covid, or any other diseases that are freely being allowed to enter out communities. I have worked through this pandemic every day. I did not receive any government handouts to help me in any way. I think our government needs to put our taxes to the best use to improve America not tear us apart.
I appreciate you listening to my thoughts and know that I am not the only one that feels this way, please take into consideration all the blue collar worker in America that this is effecting and what you will be doing to the workforce of America if you continue to force this upon the hard working people of America.
Sincerely, Robyn R Trussel
TO: The Special Committee on Government Overreach and Impact of COVID-19 Mandates
FROM: Oksana Tyshlek DATE: October 29, 2021 RE: Written testimony against government mandates of COVID-19 vaccines. Dear Chairman Erickson and Committee Members, My name is Oksana Tyshlek; I have been a resident of Kansas for the last 20 years. This testimony is to support in writing my strongest opposition to government mandates for COVID-19 vaccines. In the past few months, we learned that none of the available on the market Covid-19 vaccines offer a complete immunity as was promised when these vaccines were rolled out. The immunity goes down significantly with time and new variants. Israel was the first country on Earth to fully vaccinate an absolute majority of its citizens against COVID-19. In August-September, when over 80% of the population was fully vaccinated, the country had one of the world's highest daily infection rates — an average of nearly 7,500 confirmed cases a day. Similar examples exist in large quantities across American states, cities, and organizations. We also learned that people with Covid (either vaccinated or unvaccinated) might spread the virus to others. That means there are no societal benefits from forced vaccination of everyone. On the other hand, we all know that the design, approval, and release of all three available Covid-19 vaccines were expedited and done via emergency protocols. All vaccines are less than a year old and have been produced using the new technologies. Due to such a short life span, none of the vaccines have been tested over time, so we cannot tell today what long-term health consequences people will develop because of vaccination. Here are previous examples in world history when we rolled out the drugs or procedures that later were discovered to cause serious side effects. In the mid-1950s, a drug called "Thalidomide" was licensed and widely used in Europe. The drug came with the guarantee that it could be "given with complete safety to pregnant women and nursing mothers without any adverse effect on mother and child." This drug was later calculated to cause 90,000 miscarriages, and over 10,000 children were born with severe deformities before it was pulled off the shelves. It was sold to the public through 1962, so it took public and regulatory agencies 5-6 years to figure out the sideffects.1. Another example is the procedure that is now believed to be wildly unethical, but at a time, it was considered highly effective and safe by medical professionals across the globe. This procedure in 1949 got the Nobel Prize in physiology and medicine. I am describing a lobotomy that was widely used in mentally ill, depressed, or people with learning disabilities. The procedure was famous for sending the patients into a vegetative state.
One more example from our recent history: one year ago, no one could tell that Covid-19 mRNA vaccines cause myocarditis in young males. Just like no one could know that we will see blood clotting, thrombosis, and strokes in patients vaccinated with Covid-19 vector vaccines. I could continue with real-life examples here; the main point is that only time will show the long-term consequences that these vaccines cause. The same people who encourage all of us to believe in science are not following the science themselves. They openly ignore or deny natural immunity, the concept that has been known to every doctor and listed in every medical textbook for the last couple of centuries. It's like we've collectively have forgotten basic immunology. Recent studies from Israel with over 700,000 participants showed that natural immunity is significantly stronger than vaccine-induced immunity.2 Several studies showed it is 13-27 times stronger and lasts for years. Moreover, people who had Covid are much more likely to have side effects from vaccines. Involuntary vaccination denies the benefits of natural immunity and exposes people with innate immunity to additional unjustified risks with limited or no benefits. The same concept applies to young and healthy individuals with minimal or no comorbidities. Study after study shows the risk of getting very sick or dying from Covid-19 is low for these people. I personally or through my family members know more than one hundred people who had Covid-19. The majority of them barely noticed they were sick at all; the only way some of them found out they had the disease was through testing. These people should have the right to decide with their doctor what is a greater risk for them – known and unknown vaccine side effects or Covid-19 itself. The definition of medical fascism by Oxford dictionary (from 1980th): "The attempted regulation of others' behavior in the interest of their health, perceived as intrusively authoritarian or as an infringement of civil liberties." 3 We see across the nation today the federal government and private companies are firing people and ruining family and community livelihoods based on the vaccination status. Numerous stores, theaters, concert halls, airlines do not allow unvaccinated people to get in. These actions de-facto segregate US citizens into two groups based on their medical status: one with rights and privileges, another one with no privileges, and, apparently, no rights. Knowing that vaccines don't protect people from getting sick, don't prevent the spread of the virus, and their safety is not yet proven with time, will Kansas Senate, House, and the Special Committee on Government Overreach remain silent and do nothing to stop this unequal treatment and deprivation of rights of Kansas citizens based on their vaccination status? Will the members of the Senate, House, and the Special Committee be complacent witnesses that observe and allow the advancement of real-life medical fascism?
1. https://www.abc.net.au/austory/a-bitter-pill/10875902 2. https://www.youtube.com/watch?v=6v5VrpgXPm4 3. https://www.lexico.com/en/definition/health_fascism
Dear Chairman Erickson and Committee Members:
Thank you for meeting to discuss government overreach and the impact of COVID-19 mandates. I truly appreciate the time the committee is taking to discuss this issue and listen to the voices of the people. I am firmly against any government mandates of COVID-19 vaccines.
Any order forcing vaccination of individuals is a direct assault against the freedoms our founders set down in the Constitution that our brave servicemen and women have died defending. For over 200 years, our democracy has been a light to the world, a beacon of hope to those in oppressive regimes. When our sitting president makes an executive order demanding vaccination, even going so far as to say, “it’s not about freedom,” he has lost the compass of liberty our nation has long held dear. Nowhere in the Constitution does our president have any authority to force such a mandate on the people. Our founders knew first-hand the dangers of a monarch, and they crafted our Constitution very carefully to ensure that the American people would not be subject to the orders of one person. It is disturbing to watch other states and government institutions forcing compliance, as well as private companies. We are praying for the employees of Spirit AeroSystems as they stand strong for the right to make personal health choices. We are a democracy, not a dictatorship. We must stop this tyranny.
I spent a year teaching English in a communist country. Suffice it to say, I came home with a new respect for our nation and our flag. I never met the wife of one of our staff members; she was in hiding the whole year I was there for breaking a law that is nonexistent in our country. In addition, our school janitor was removed from her home and taken by force to a hospital for a mandatory medical procedure that violates human rights. When I expressed my shock and outrage to my students, they simply shrugged and told me she disobeyed the law. I was floored and angered at the lack of human rights.
Perhaps that is why this issues is so urgent to me. I have seen first-hand the effects of government control of healthcare. I cannot emphasize enough the importance of personal choice. Our freedom is at stake. Please defend our rights as Kansans to make our own health choices. Please do not allow the President’s executive order to have any jurisdiction in Kansas. My husband works at a company of over 100 people, so this will directly affect us. This mandate fails to take into account natural immunity, as well as the fact that vaccine manufacturers are not held liable for any adverse reactions.
We are Kansans. We want to live and work in freedom in this great state, with no danger of harassment or coercion or loss of job or dignity because of our personal health choices. We do not want a totalitarian regime that pushes mandates down our throats. There are plenty of other places in the world we can move to if we want that. Please stand strong and defend our rights for personal choice.
Sincerely,
Julie Vallier
October 27, 2021
To Chairman Erickson and Committee Members: I am an Associate Educator of Music Education and Placement Coordinator at Wichita State University. I coordinate the placement of all music student teachers and supervise them during their student teaching semester. It is a ,50 unclassified non-tenured position. This is my eleventh year in this position and I am planning on retiring at the end of the 2021-22 school year next June.
I received this communication from WSU President Dr. Richard Muna on Friday, October 22. In
summary it states that ALL employees at Wichita State University are mandated to be vaccinated
by December 8 unless eligible for a medical or religious exemption. This is a condition of
employment. I meet student teachers on campus once a week during their student teaching
semester unless otherwise designated. This amounts to about 10 times throughout the
semester. I office mainly from my home but I do spend time in area public schools observing
and consulting with these future music educators. I wear a mask in public schools requiring a
mask.
I have included the complete memo for your information:
October 22, 2021
Update on vaccination and masking requirements at WSU
Shocker family, I know many of you are aware of President Biden’s recent executive order regarding COVID practices and protocols relating to vaccines, masking and physical distancing for federal contractors, and have had questions as to if — and how — this order might apply to WSU. After a thorough internal review of the order and its implementing guidance — and in consultation with state and federal partners, our fellow Kansas research institutions, and the president of the Kansas Board of Regents — we have determined that the order applies to the entire WSU workforce. What does this mean for you? In accordance with the executive order, there are several COVID safety protocol requirements that will impact our community: vaccines, masks and physical distancing. All employees (including part-time, full-time and student employees) will be required to be fully vaccinated by December 8, 2021, unless eligible for a medical or religious exemption. The mandatory vaccination obligations apply even to those covered employees who are working remotely (as long as they are working on or in connection with a covered contract). Given the short timeframe for implementation and the
length of vaccination protocols (in some cases, taking up to six weeks), unvaccinated employees should seek their first vaccine dose immediately. Get more information on vaccination schedules. Compliance with the vaccine requirement is a condition of employment. Employees who are not fully vaccinated or do not receive approval for a medical or religious exemption will be prohibited from engaging in work after December 8, 2021. Further failure to comply will be addressed consistent with university policies and procedures, which may include corrective action up to and including separation. Additionally, absent an exemption, all individuals on campus — employees, students and visitors – regardless of vaccination status, will be required to wear masks and physically distance (to the extent required in the order). This includes indoor and outdoor spaces, classrooms, labs and social events. This masking and physical distancing requirement is effective Monday, October 25, 2021. What are the next steps in complying with this order? We are asking all employees to please not submit your vaccination card (or other proof of your vaccination status) to your supervisor or Human Resources at this time. Employees will be able to upload proof of their vaccination status through a secure online portal shortly; more details are coming on how to do that. Also, please do not submit requests for vaccine exemptions to your supervisor or HR at this time. More information will be forthcoming regarding the exemption request process. We have put together a list of frequently asked questions to help answer some of your immediate questions. More information will be distributed as it becomes available. As I have said before, vaccines remain the most effective way for us to combat this virus. Our top priority has been and remains the health, safety and well-being of our entire campus community. I call upon each of you — as a critical and valuable part of our Shocker family — to do your part in this fight not only for yourself, but also for your family, your friends, your neighbors and your colleagues. Vaccination of our campus not only ensures compliance with our federal obligations, thereby continuing to secure millions of dollars in federal funding that support and fund research, employment and educational efforts, it also gives us the best chance at keeping our classrooms and campus open. As a reminder, all WSU students, faculty and staff can receive the vaccine, free of charge, through Student Health Services. Additionally, in partnership with the Sedgwick County Health Department, WSU is hosting two weekly public walk-in vaccination clinics. See the walk-in vaccination schedule.
If you have additional questions, email [email protected]. Thank you for all you have done and continue to do for our university! Sincerely, President Rick Muma
I received the following memo from the Dean of Fine Arts on Monday, October 25, repeating President Muna's information with more clarification:.
• On Oct 25, 2021, at 3:43 PM, Miller, Rodney <[email protected]> wrote:
Dear Colleagues, By now, each and every one of you should be aware that Wichita State – as of today – is under a new mandate originating with President Biden’s Executive Order. This email is my attempt (emphasis on attempt!) to clarify what this order means for CFA. I will do so with a series of bullet points.
PART I – EMPLOYEE RESPONSIBILITY
Who is affected? - All employees (including part-time, full-time and student employees) will be required to be fully vaccinated by December 8, 2021, unless eligible for a medical or religious exemption. This includes adjuncts, GTAs, and student workers. It also applies to those who are working remotely. When do I have to decide whether to comply? – Immediately. Given the length of vaccination protocols (in some cases, taking up to six weeks), you should get your first vaccine dose immediately. What happens if I decide NOT to get vaccinated? – You will be subject to termination. Compliance is a condition of employment. Employees who are not fully vaccinated or do not receive approval for
a medical or religious exemption will be prohibited from engaging in work after December 8, 2021. Further failure to comply will be addressed consistent with university policies and procedures, which may include corrective action up to and including separation. How do I prove I’ve been vaccinated? – Don’t worry about that yet. Employees will be able to upload proof of their vaccination status through a secure online portal shortly; more details are coming on how to do that. How do I get an exemption for religious or medical reasons? – Don’t worry about that yet. More information will be forthcoming regarding the exemption request process. ---------
PART II – IMPACT ON CFA PRESENTATIONS/PERFORMANCES
What is the new Mask Policy? - Absent an exemption, all individuals on campus will be required to wear masks and physically distance (to the extent required in the order). This includes indoor and outdoor spaces, classrooms, labs and social events. Who is affected? - All employees, students, and visitors to campus regardless of vaccination status. When does it go into effect? – IMMEDIATELY! This masking and physical distancing requirement is effective TODAY - Monday, October 25, 2021. How does it impact CFA Performances/Presentations? - "At this point in time" performers whose performance would be compromised (singers, actors, wind players, etc.) would NOT have to wear a mask while on stage. Performers who wouldn't (pianists, strings, etc.) should wear one. Support staff (technicians, ushers, etc.) would be expected to wear a mask. And, of course, audience members will now be required to wear a mask.
What happens if an audience member refuses to wear a mask? - Absent proof of an exemption, they will not be admitted to the performance. Who is responsible for policing this mask policy? – The faculty/staff of the School. [Please Note!]: We will not be asking/requiring student workers or volunteers to police the audience. We feel this would simply be inappropriate. This is what has been decided (at this point in time) regarding the enforcement of the Mask Mandate announced last Friday:
o Masks will be made available to patrons, both at the Box Office and at the door.
o We will have signs that say “Until further notice, masks are required for entry to the venue” at the box office window, and at entry doors.
o Enforcement of mask use will be by house managers/ushers, to a point. If a patron is proving to be difficult, Dr. Tim Shade will be available tomorrow night for the orchestra concert. For Performing Arts events there will be a faculty member (uncertain who it will be at this time) to perform the same function. Dr. Shade will delegate for future SOM performances.
o Mask use is required by all technicians, box office personnel, house management, and most performers. Performers that require free breathing, i.e., singers, horns, woodwinds, brass, and such like, may not be required, but should wear them backstage. Enforcement of performers will be done by ensemble directors or faculty, not by Performance Facilities personnel.
o Common sense should prevail, if you’re around people, wear a mask. If you’re in your office alone, you can take it off.
Dr. Rodney E. Miller
Dean, College of Fine Arts
Wichita State University
(316) 978-3389 – Office
(316) 978-6174 – Direct (316) 680-0539 – Mobile
[email protected] And finally, the Director of the School of Music sent out the following information
If you have not read the entire Strategic Communications email sent at 12:11pm on Friday, I urge you to
do so for some important information regarding the updated Vaccination and Masking policies. To summarize: All WSU Employees (full-time, part-time, and student) will be required to be fully vaccinated by
December 8, 2021. Compliance with the vaccine mandate is a condition of employment. Employees who
are not fully vaccinated or do not receive approval for medical or religious exemption will be prohibited
from engaging in work after December 8, 2021. Further failure to comply will be addressed consistent
with university polices and procedures, which may include corrective action up to and including
separation. PLEASE DO NOT send notice of your vaccination status to the School of Music Administration or HR.
An online portal will be setup for you to submit your information and exemption requests. Beginning today, October 25th, we will need to abide by the requirement that masks are worn at all times
on campus for faculty, students, and visitors. • This includes all of our rehearsals, lessons, and performances. • Audience members will be required to wear masks as well as guest artists. • Instructors, no matter how far from your students, must be masked. • Face shields are not permitted in place of masks. • An ending date to this mandate has not been specified.
Regarding Social Distancing: At this point, I have not found any guidance requiring us to be socially
distanced indoors. Therefore, no new distancing guidelines are in place for the School of Music. If you have any further questions, please do not hesitate to stop by or call the School of Music office. Timothy M. Shade | D.M.A.
Director, School of Music
Director of Bands
Wichita State University
Wichita Youth Symphony Wind Ensemble Conductor
(316)-978-3500 – Office
(614)-499-3798 – Cell
Information for medical and religious exemptions are forthcoming. I will be seeking a religious
exemption per directives.
Our universities in Kansas receive federal monies for outstanding programs. Liberty Counsel,
Matt Staver, director, has filed a class action law suit against Joe Biden the Department of
Defense, and the Department of Homeland Security on behalf of a group of military members,
federal employees, and civil employees of federal contractors. Our university personnel fall
under civil employees of federal contractors. Liberty Counsel is also seeking a Temporary
Restraining Order that would stop similar mandates if granted. I do not know the status of this
TRO. I certainly hope it is successful because the constitutionality and legality of these
mandates could be decided in the courts.
So a part time music teacher who makes $28.000 a year and who is planning on retiring in the
spring is caught in the web of coercion of an executive order. I have many doubts about the
safety and the side effect from this inoculation and do not want to subject myself to those
dangers. I see a bias on a daily basis of pro-inoculation propaganda. II see a highly politically
charged bias throughout the conversations and the silencing, de-platforming, censoring of
opposing views and even opposing conversations. For example, I strongly object to the use of
aborted fetal tissues in the development and/or dispensing of the three main formula. I
understand that the federal government could pull millions of dollars of contracts, grants, and
programs if universities do not capitulate to the demands described in the above
memos. However, that federal money came from TAX PAYERS, like me and you. It should
NOT be a Quid Pro Quo. Employment is a choice, at least for now. But easily eroded into the
private sector.
The public cannot go to a college performance or sporting event without wearing a mask! This
certainly is not throughout our public and private schools or our professional events! It's about
the federal money and control.
One final point: CoVid Cases at WSU are DOWN! Covid Cases in Sedgwick County are
DOWN! It is NOT about Covid! It is about control and about the money made from
vaccinations. I am sure you have several sources being thrown at you that if listed here would be
redundant. VAERS can give you reactions, OSHA is no longer requiring reactons to be reported. Reporting is skewed, etc.....
I consider this an overreach of great magnitude and if it is not stopped at this level, more areas of
overreach will occur. Please do what YOU can do to stop the erosion of our freedoms without
extortion without coersion
Jeanne Shoemaker

Written Only testimony to STOP government overreach Covid-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
I am a Christian. I have very strong religious beliefs. I wrote a religious exemption to my employer, Hanes Brands, located in Lenexa Kansas. They denied my request and gave me a few weeks to get the vaccine or be terminated. I am a very healthy person. I take good vitamins and eat healthy to keep a good healthy immune system. I was terminated Oct 18th, 2021. I was an over achiever on my job. I worked there for 14.5 years. They don't require the vaccine on the production floor. I had worked on a machine at over 100% for 8 years. They said I couldn't take a demotion and let me go. I am 100% against mandates. They are against the peoples right.
Paulene Vandeputte
Sent on my Samsung Galaxy S20 FE 5G.
Pam Vetter
October 27, 2021
Chairman Erickson and Committee Members,
We are at a precipice right now. You as committee members and legislators have the authority to keep many Kansans from falling in to this precipice of destruction.
The overreach of the federal and state governments have to cease! We all see the signs of a socialistic regime coming to power. What are you going to do to stop it? We as Kansans are here today to take a stand together to show our legislators that we are united. We stand together hoping that you as legislators will stand together as well. Why are government officials not willing to take the bull by the horns and do something to stop the mandates that are surely to devastate individuals and their rights to choose what they put into their bodies. Kansans are being coerced and forced to make a decision that they should never have had to make in the first place according to the Constitution and the Nuremberg Code.
We are at a place that you as legislators could have prevented. You could have supported SB212, and SB213. There are no excuses that you can make at this point that would justify the loss of health freedoms that Kansans face.
What will come next if legislation is not passed to protect Kansans and they either get fired, quit, or get the jab and suffer the consequences of that choice with an adverse, lifelong, damaging health event? Who will be held responsible?
I would like to remind you that KDHE still has the power to add vaccines and or experimental injections to the childhood schedule. The FDA just approved the jab for children yesterday. Do you think that Lee Norman will not adhere to, or recommend the Covid jab for our children? Predictably, he will.
Dr. Richard Malone MD, creator of the mRNA technology and Dr. Geert Vanden Bossche DMV,PhD, are both strongly speaking out that in order to get out of this viral spread and mutations, we must NOT give the jab to children and stop injecting adults. They would know the true science. The science, that is being suppressed right now, due to the agenda that is being pushed by the FDA, CDC, NIH and big Pharma.
Another concern of mine is the legislation passed in 2020. I assure you that most Kansans do not even know that this statute exists, and if they did, they would be very alarmed because of the environment we are living in today.
It is Article 1.- Secretary of Health and Environment Activities:
65-129b. Infections or contagious diseases: authority of local health officer or secretary; evaluation or treatment orders, isolation or quarantine orders; enforcement
(C) if a competent individual of 18 years of age or older or an emancipated minor refuses vaccination, medical examination, treatment or testing under this section, may require the individual to go to and remain in a place of isolation or quarantine until the local health officer or the secretary determines that the individual no longer poses a substantial risk of transmitting the disease or condition to the public: and
(D) if, on behalf of a minor child or ward, a parent or guardian refuses VACCINATION, medical examination, treatment or testing under this section, may require the minor child or ward to go to and remain in a place or isolation or quarantine and must allow the parent or guardian to accompany the minor child or ward until the local health officer or the secretary determines that the minor child or ward no longer poses a substantial risk of transmitting the disease or condition to the public; and may order any sheriff, deputy sheriff or other law enforcement office of the state or any subdivision to assist in the execution of enforcement of any order issued under this section.
This is next! Please do not think for one minute that this cannot happen in the state of Kansas. It can and it will if you don’t do something now!
I am praying for you all, knowing that you are accountable before God, as we all are, for your decisions. May the Lord give you the wisdom and discernment you need as you make these very important choices that affect so many people’s lives.
Pam Vetter
WRITTEN Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Kristina Vezilich
27 October 2021
Dear Chairman Er ickson and Commit tee Members,
I am providing wr i t ten test imony to STOP government mandates of COVID-19 vaccines.
I personal ly know of many people who have contracted Covid-19 and quickly recovered. I know of no one who has truthful ly d ied of just Covid-19, and I know a lot of people. From al l of my f i rst hand exper ience there is absolutely no reason to be vaccinated, even i f these shots are actual ly “vaccines”. In real i ty no one real ly knows exact ly what they are and what they contain. Why so much mystery? Our so-cal led heal th agencies have completely contradicted themselves every step of the way and have shown no transparency when legi t imately quest ioned, the CDC is now claiming that they don’ t even know what k ind of r isks these shots pose to chi ldren. I personal ly know of many people who have died short ly af ter being jabbed…this is a HUGE RED FLAG!
Not only is a mandatory jab Un-Const i tut ional i t is exact ly what was warned against and made global ly i l legal at the Nuremburg Tr ia ls….PLEASE THINK!!
Also the human body has what is known as an immune system…natural immunity is a Scient i f ic Proven FACT. These jabs are pure and total human exper imentat ion. I f you al low these mandates to go forward you are compl ic i t in Cr imes Against Humanity as per the Nuremburg Codes. Don’ t Be a Nazi . Please.
Kind Regard,
Kr ist ina

Dear Chairman Erickson & Committee Members, We are against government mandates of COVID-19 vaccines. We really feel that these issues are for the family and their healthcare provider and not government intervention. There are so many areas that the counties need help with instead of so much focus on the COVID-19 issues. Freedom is very important to us. Thank you for your time. Blessings, Mark & Michele Volz
Revised Written Testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Chairman Erickson and committee members,
I am writing today to voice my opinion on the COVID-19 Mandates. We farm in Norton County, a farm that has been here for over 100years. We have many local businesses that are running the risk ofloosing valuable employees due to these mandates. A lot of theseemployees have been there for many years and have the knowledgeand experience that it takes to keep the local economy moving.I do not believe that the government has the authority to mandate avaccine that has not been proven to prevent Covid-19. A lot of theseemployees are healthy individuals that are not in the high riskcategories. Therefore, taking the vaccine without knowing thelongterm affects is an individual choice that you should not make forthem. And by doing so, you are taking away their rights and possiblyloosing some very valuable and experienced employees. If you mandate this vaccine it will affect EVERY business. It will takeyears for these businesses to replace all the employees they will loose. There is no way of knowing how much productivity will be lost. EveryAmerican is affected in some way with this mandate. What happened
to our rights?I pray that you stop these mandates and help the working Americanpeople.
Jim and Cindy Voss

Written testimony to STOP Government Overreach COVID-19Mandates
EXTERNAL: This email originated from outside the organiza�on. Do not click any links or open any a�achments unless you trust thesender and know the content is safe.
Chairman Erickson and Commi�ee Members:
I am very against government mandates of the COVID-19 vaccines.
As a business owner I have witnessed and experienced first-hand, the detrimental effects of government shut downs and overreach. I believe every individual should have the right to choose what is best for them, and that a government en�ty should not make decisions for me on health issues. I believe in medical freedom of choice.
As an individual that experiences tremendous nega�ve side effects from any and all vaccine, I believe that I should have the right to choose what goes into my body.
As a mother, I will not support a system that takes away freedoms from my children.
Thank you for addressing my concerns,
Melanie Voss
Let’s Go Brandon
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
The subject line reflects my opinion on the issue on proposed legislation
Sent from my iPhone
Walker Voss
Covid -19 Written Testimony
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
10/27/21
Written Testimony only to the Special Committee on Government Overreach and Impact of COVID-19 Mandates
Attention: Chair, Senator Renee Erickson, Kansas Legislative Research Department
It is important to me personally as an elderly person in the state for us to mandate masks and vaccines in public places. Until we get this Covid -19 epidemic behind us by having a more fully vaccinated public then all of us will continue to be endangered as the longer the virus circulates and evolves, the more danger we all face.
We are just getting students back to the classroom and we want to continue that trend. We want to be able to safely go out and shop and dine and work but we cannot do it until more of us are vaccinated. So mandates are vital. Just recently a friend of mine suffered a break through Covid infection caught from a co-worker who could not be bothered to ensure the safety of those with whom she worked. She unfortunately passed Covid on to her two adult children before she knew she was contagious with it.
What we seem to lack right now is enough empathy to care for others in this pandemic - a pandemic that should be fought with common sense, compassion and science. What would our world be like if we hadn't discovered, tested and used other vaccines that have prevented millions of deaths in this country.
Thank you for letting me submit this testimony. Nancy Wagner
Chairman Erickson and committee members,
I am writing today in strong opposition of vaccine mandates! I’m a lifelong Kansas resident and homeschooling mother of three precious girls. My husband works hard for our family and is now faced with losing his job because of his very well-researched and educated choice not to inject himself with an experimental injection when he has a 99.99% survival rate. We are a single-family income and this would be devastating for our family but we will not comply with tyrannical mandates!
In the last 1.5 years, I’ve watched so many people suffer - and only very few from covid itself. Most of the suffering has come from lockdowns, closure of businesses, job losses, children suffering with mental illnesses from isolation, special needs children failing to receive services, crippling adverse reactions from the vaccine, and stress. WE, the people, are suffering and we need you to step in and do your jobs as elected officials which is only to protect our rights and freedoms! We don’t need a government to keep us “safe” from any of the trillions of viruses in existence. We don’t need to be told how to medically care for ourselves or our children. We are smart, respectable, Godly beings and deserve to choose how we want to live. We need you to protect our rights so we can decide for ourselves!! Kansas has been quiet. Many other states, like Florida, Texas, South Dakota, etc, have boldly promised to protect their people. Kansas has been SILENT! Please make a stand! Lead the way for our beautiful country that is quickly deteriorating. We are the majority even when the mainstream news and Biden administration want us to feel isolated and alone. Please be a leader and do everything in your power to ban vaccine mandates!! HOME OF THE FREE BECAUSE OF THE BRAVE. Thank you for your time and service.
Sincerely,
Keely Waller
Chairman Erickson and committee members,My name is Luke Waller and I am AGAINST government mandates of COVID-19 vaccines. I will bethere on Saturday, but will only be giving my written testimony here.
Just like everyone, our family has been very affected by all the mandates and quarantines. Thegovernment has no business forcing individuals to inject an experimental drug that we haven’t evenseen be effective.
It is absolutely wrong to make getting a vaccine a requirement to simply be employed and takeprovide for your family.
My phone number is 785-215-7018. I live in Lawrence and my address is 2040 W 31st St, Suite G#235.
Luke
Ext. 1020
LegacyAccel Marketing Pieces are HERE
For LIFE resources, marketing materials and much more: www.advisorsexcel.com/life
Luke Waller, J.D.VP of Life Insurance
E: [email protected] P: 866.363.9595
A: 2950 SW McClure Rd., Topeka, KS 66614
For LIFE product updates, materials, and events stay connected with us atwww.advisorsexcel.com/life
10/27/2021
To Chairman Erickson and Committee members:
I will be submitting my written testimony against government mandates for Covid-19 vaccines.
Ever since the beginning of the Covid-19 pandemic, we have been told WHAT to THINK aboutit, and WHAT to DO about it. We have not been trusted with the FACTS and allowed toconsider for ourselves. This has been especially true in the arena of the healthcare industry inwhich I work for Ascension Via Christi, though only for a few more days. Since July, we havebeen harassed with e-mails up to 3 times a DAY urging us to get the shot. Some includeso-called experts in white lab coat repeating the same tired mantra that the vaccine is “safe andeffective”, mostly because they are ALL assumed to be. No true evidence was given. No data.No references cited, unless perhaps to the CDC website which constantly spouts circularreasoning. We are just supposed to believe this person because they are a doctor and claim tohave this higher knowledge.
Furthermore, when Ascension made the decision to require the covid-19 vaccination BEFOREFDA approval, they said that it was for concern over employee and patient safety, and theirjustification was that millions of doses have already been given. That was it. Not that millionswere followed and it was found to be safe, not that long-term results were positive, just that thedoses were given, and that was “good enough” for them. Well, it’s not good enough for me.
I work in a relatively small department, of less than 15 colleagues. Since the shot has beenadministered, 2 have started having migraines, one has come down with a severe auto-immunedisorder, another has had a chronic illness get so much worse she had to quit and find a remotejob instead. In addition, I have had patients that have had strokes, heart arrhythmias, covid-19itself and death shortly after receiving the shot. This is by my own observation. No one canprove or disprove whether this is from the injection, but I should have the choice whether to takethat risk or not.
When the FDA did release their “approval”, it was in a very confusing and perhaps evenunderhanded way, with changing the name to Comirnity, or that the approved one was notwidely available, which is misleading to the public either way. It is also highly suspicious thatsome of the higher-ups in the FDA left their roles soon after this so-called “approval.”
When there was still resistance, Ascension changed tactics to Spiritual abuse and manipulation,quoting the Pope saying it is a “moral obligation” and an “act of love” to receive this injection, indirect opposition to a statement from The National Catholic Bioethics Center which states that“vaccination is not, as a rule, a moral obligation and that, therefore, it must be voluntary.” Still,the incessant e-mails continued, with bribery, guilt-tripping, emotional manipulation, and finally,threats to employment. Those who were not vaccinated were essentially shunned and pointedout because others were not required to wear masks, but we were, violating our privacy. We
were not approved to attend meetings in person. We were not allowed to do any businesstravel.
The organization would not sign the waiver I requested taking responsibility for wages lost,damages or disability were incurred related to the Covid-19 vaccine.
We were told that unless approved a medical or religious exemption, we would be “voluntarilyresigning” if we did not receive both doses of vaccination by . The exemptionNov 12, 2021forms themselves were violating, and felt as if I was throwing myself under the bus. We wererequired to watch their video. Required to check a box that we agreed to “voluntary resignation”if not approved, with inability to make caveat or comment. We were required to check a box thatwe would abide by whatever “accommodations” were asked of us, without definition of WHATthose accommodations would be, again, without ability to make caveat or comment. Then,questions about church attendance and doctrines that the shot violated, and how you live thisout in your daily life to prove that it is a “sincerely held” belief. We would then be required tosubmit these exemptions for approval yearly. These were supposedly reviewed by up to 3committees. (The larger question is, who has the right to judge whether someone’s religiousbelief is “valid” or not? And if they can, does that mean we have State approved religions andunapproved religions? This is a dangerous precedent to losing religious freedoms.) Medicalexemptions had to have written approval by a physician, however, of the four physicians Icontacted, they said they were “not giving exemptions”, or they were “advised by legal not toapprove exemptions”. In other words, there was no discussion about whether or not the doctoragreed with not taking the shot due to a specific condition or not, they just made it a policy not tosign off on them at all. Ascension had to know that. So really, no such thing as a medicalexemption was available. I submitted my religious exemption request with a pastoral supportletter only after previously submitting my resignation letter, because I did not feel comfortablewith the request form, but wanted to know if it would be approved in the future if I wanted toreturn to working for Ascension. It was denied. What looked like an automated response formletter stated that both flu and covid vaccine exemption requests were denied due to the “natureof your role” and that accommodations would present an “undue hardship” to the company.This, even though my role is 99% virtual, with no face-to-face interaction with patients sinceprior to the pandemic. Even fully remote employees received this response. All the colleaguesthat I know of who submitted exemption requests received the exact same response. Managersreceived this response. I have been in contact with many nurses, and in many support groupsand have not heard of one single request being approved. This essentially makes exemptionrequests an illusion of choice, when the only “choice” is jab or unemployment. Oh, but wait, wealready signed away our unemployment benefits because we “voluntarily resigned”. The rulesin place only support the corporate companies, which want the image of safety, but does notensure it. It is sickening that an industry that spouts ethics of “patient autonomy and right tochoose” does not respect those same ethics in regards to their employees. Having been anurse for over 12 years, I expected more of my employers and my medical colleagues. My lastday with Ascension, and perhaps as a nurse, will be November 2nd. I am devastated to bepotentially being forced out of my chosen career. However, I have long told my patients not toconsent to any medicine or medical procedure that they did not want or were not comfortable
with. Now is the time for me to take my own advice and advocate for myself, but also forpatients and my colleagues! There are now being requirements put forth for the patients, suchas for kidney transplants at a health system in Colorado. I also grieve for my colleagues left tobear large and heavy assignments, which is not sustainable for staff, and is dangerous for bothstaff and patients. Who knows how long they will be able to tolerate that work load before theybreak? The current policies are creating a healthcare environment that is not safe for caregiverOR patient. The violation of our bodily autonomy will not stop until we say no. Our bodies donot belong to the state or our employer, but are gifts to us from God. They are ours alone inwhich to live out our beliefs and convictions. We must retain the human right to bodilyautonomy, because if the government “grants” this freedom, that means they can take it away.Regardless of whether the vaccine is “safe and effective”, it is totally unethical and unacceptablefor any vaccines to be anything other than voluntary. What is currently being allowed by thegovernment and acted out by corporations will have ramifications beyond what we canimmediately see, but will long suffer from.
Thank you,
Cassandra Drummond, RN BSN
Vaccine mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Please protect our freedom to choose whether or not we take the Covid injection without stripping us of our unalienable rights as would beinfringedupon if you supported Vaccine Passports or Vaccine Mandates in ANY legislative form.
My family has already suffered consequences of the shot they fere forced to take in order to continue working in the schools, as a department head in a State position and as a nursing student in our state educational institution! Heart problems to the extent Md's thought he was having a heart attack initially and now, months later, dealing with new heart issues! 41 years old! ...husband and father of 4!!!!
Please take your constituents' voice to the vote. We do not want or deserve to be controlled, completely dominated by such legislation.
Thank you for your voice and service to Kansans!
Sincerely and most respectfully yours,
Jan Weishaar
Topeka mother, grandmother, 70 year old concerned voting citizen and Election Board Worker, and business owner
Written testimony to Stop Government Overreach Covid-19 Mandates
Lorna Weixelman
Written testimony only
Dear Chairman Erickson and committee members,
I am against government mandates of Covid-19 vaccines. If a person chooses to
be vaccinated that is their choice.
I am a Registered Nurse with a Bachelor of Science in Nursing. I have a current
Kansas nursing license. I have previously worked in Intensive Care and am not
currently employed. For the last 40 years I have been a lactation specialist as a
volunteer and have worked with over 10,000 mothers and their babies. I am a
wife, mother to 8 daughters, and grandmother to 11. I have been a volunteer all
of my life and have given 400-500 hours of service each year.
Since February 2020 I have spent much time nearly every day reading and
studying information about Covid, the Covid vaccine, and mandates. Across the
United States and the world brave scientists have risked their lives to expose
information about the disease and the vaccine. Because the survival rate of
Covid is over 99% I don’t believe it is necessary for everyone to be vaccinated. Dr.
Robert Malone, the inventor of the mRNA technology, believes the use of this
particular vaccine is driving the creation of new variants. Covid is not going away.
Dr. Harvey Risch,Professor of Epidemiology at Yale University recently stated:
“The unvaccinated should be afraid of the vaccinated…it is well-known that it is
the vaccinated people that generate the mutant strains and not the unvaccinated
people. And the corruption of the medical establishment saying the unvaccinated
are generating the mutants is an absolute falsehood; it is exactly the opposite.
This has been known for a hundred years. It is vaccinated people that are more
prone to generate mutant strains.”(Coffee & Covid, Oct. 25, 2021, Jeff Childers)
I also object to the use of vaccines created with the use of aborted fetal cells. The
three Covid vaccines available all have been created through the use of aborted
fetal cells (which were obtained from the tissue of living fetuses prior to being
aborted) either in the testing of the vaccine or in the vaccine itself. This is wrong
and the religious beliefs of people who object to the vaccines should be
respected.
Enough time has elapsed and researchers have been able to show that the
immunity gained from having had Covid is durable and long lasting. Studies from
Israel and many doctors like Dr. Peter McCullough, an esteemed cardiologist from
Dallas, Texas supports this. I agree with Senator Rand Paul that people who have
had Covid do not need to be vaccinated. Data has shown that some people who
have had Covid and then receive the vaccine are at greater risk for adverse
reactions. I do not believe it is right to ignore the herd immunity that we now
have achieved from so many people having already had the virus.
Not enough testing has been done to know how safe the Covid vaccine is. The
truth is that all of the people getting the vaccine are the test cases and we won’t
know the long term effects of the vaccines for months to years. The Covid vaccine
has been created in too little time with not enough evidence that it will protect
the people. I am appalled that an FDA committee member recently voted to
approve the Covid vaccine for children ages 5 – 11 and stated that we wouldn’t
know how well it will work for children unless we try it.
A growing number of physicians and health care professionals including Dr. Peter
McCullough, Dr. Vladimir Zelenko, Dr. Ryan Cole, Dr. Piere Kory, Dr. Simone Gold
have shown that there are supplements and current drugs available that can help
to prevent and treat Covid. They have successfully treated large numbers of
people with Covid. Our government has done a disservice to the population by
not having public service campaigns to alert people about the use of these
supplements and drugs which could prevent and treat Covid.
As a nurse and mother it has amazed me that from the beginning of the Covid
pandemic that people with positive covid tests have been told to go home and
treat their illness like the flu but have not been given treatment until they were so
sick that they were admitted to the hospital and for many it was too late.
American doctors who were invested in the health of their patients have
persisted and saved a great many of the sick by using their knowledge of current
medications and supplements to treat the public. These frontline doctors have
been heroes.
I don’t believe it is right for anyone to coerce another person to have medication
that they do not want to be injected into their bodies. There isn’t proof the use of
the vaccine is necessary for the greater good of the society. It is wrong to
mandate this vaccine and force a sizeable part of the workforce to give up their
livlehoods and way of supporting themselves and their families because they are
following their conscience in making the decision to refuse the covid vaccines.
Our society is going to be in great danger from the loss of this part of our
workforce. I have friends and family who are now approaching vaccination
deadlines and I fear for their families. We are all experiencing great anxiety.
I find it frightening that so many scientists, health care professionals, and citizens
have been threatened and silenced because their information is informing the
public but disagrees with the current government or pharmaceutical
recommendations. We should all have the opportunity to use our critical thinking
skills to determine what information we will use to make the important decisions
we have to make. The freedom of speech is in danger in America.
Unvaccinated health care workers and first responders chose to go to work to
serve the people in 2020 at great risk. They were heroes. Now in 2021 those
same people who choose to remain unvaccinated will be fired by hospitals and
governments. They are all capable of weighing the benefits vs the risk of the
Covid vaccine and their rights should be protected to make that decision.
We have seen the upheaval of our American society over the last year and a half
and it has caused great anxiety in our lives. I am asking the Kansas legislators to
protect the rights of Kansans from forced vaccination mandates. We are
depending on you.
Sincerely,
Lorna Weixelman
Written testimony to Stop Government Overreach Covid-19 Mandates (Natalie)
Natalie Weixelman
Written testimony only
Dear Chairman Erickson and Committee members,
I believe that everyone should have the right to choose if they want a Covid-19
vaccine or not. We have the right to choose in this free land that we live in.
I have family members and a boss who will be affected by a vaccine mandate. This
will adversely affect my life.
Sincerely,
Natalie Weixelman

WELLS WRITTEN TESTIMONY
Tina Wells
Dear Chairman Erickson and Committee Members:
I’d like to thank you all for taking the time to discuss this matter. I am sadly missing the gathering in
the flesh, but wish to submit this written testimony.
In regards to the current governmental COVID-19 vaccine mandates, I’d like to make it known that I am
against such things.
My husband and I run a chiropractic office and don’t feel comfortable with the direction in which these
mandates are heading, particularly in respect to medical facilities & their staff. It is a core belief that
personal health choice belongs to the individual and not to government.
I would ask that you please listen to the voice of the people and uphold our constitutional rights by
keeping this government over reach out of our great state.
God Bless,
Tina Wells
Good afternoon I am writing this for my written testimony against vaccine and mask mandates.
I firmly believe we should always have a choice in our health. Through this pandemic we never talk about health and how people should take care of themselves. The TV commercials are fast food and medications. Big Pharmaceutical companies had increased their wealth by billions.
People are living in fear of a man made virus that was released. I believe on purpose to damage the American people. I have never been against vaccines until this pandemic happened now I have no faith in western medicine. We have never worn a mask during any other flu season why are we masking our children and keeping people separated. I believe along with choices for adults parents should get to choose for their children and not be forced to vaccinate their children.
I also never see any reports of how many people have died and or been injured because of the Covid vaccines. I do know the numbers but why aren’t these even considered by the State of Kansas?! Please stop wasting money on scare tactics with your current ads about Covid!! Such over reach by the government.
Thank you for your time and please fight for our rights and the rights of our children.
I am against government mandates of Covid-19 vaccines.
Suzy Wempe
Covid Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Dear Congress People,
Please do not mandate the Covid vaccine. This is my life and body and I feel I should have a choice if I put somethingexperimental trig in it. I have had Covid and should have natural immunity to it. I have no problem with people choosing tohave the vaccine, but I think it should be a choice NOT A MANDATE. This is a complete over reach of government!Thank you for your time concerning this matter!!Betty Wenger
Sent from my iPhone
10/27/2021 To: Chairman Erickson and Committee Members Position: Against government mandates of COVID-19 vaccinations Thank you for hearing our testimony. We have spoken twice before to the House Committee on Health and Human Services with regard to insurance companies being required to pay for PANS, PANDAS, and autoimmune encephalitis treatments. All to say, we are not strangers to some of the members of the Kansas Congress and we fully appreciate the process. Both years we gave our testimony, we did our best to describe the truly indescribable years that two of our kids suffered from autoimmune encephalomyelitis. Our son has been dealing with his illness, including the tormenting symptom of suicidality, for ten years now (having had a recent setback starting in April of 2020). Our daughter suffered for three years and has entered remission. Our family has taken an enormous financial hit, too – one that would be far beyond your wildest nightmares. But we didn’t tell the rest of the story, as it didn’t relate to our purpose at the time. Summer of 2017, the first summer that both of the kids were diagnosed (as I write, recalling one memory I have of their having seizures at the same time in our living room), and one of our other sons was beginning to show early symptoms of the same illness, our youngest was getting ready to enter kindergarten. Her name is Brenna, and she was probably the happiest, most docile, enjoyable, cooperative little girl we have ever known. Of course, Brenna needed vaccines to enter kindergarten, and we were happy to comply. We were pro-vaccine (and we continue to be pro-vaccine). But unfortunately, within 24 hours of her shots, a destructive, multi-system pathway was triggered in her body that created dysregulation in her nervous system and inflammation in her brain. In other words, overnight, she had had an onset of the same illness as her siblings. Of course, Brenna’s illness was not yet as severe as the other two, but we knew that illness progression was inevitable. The two diagnosed had been at her level of severity at one point and had progressed into debilitating severity. Obviously, the experience of watching our daughter become vaccine injured made us strongly consider the possibility that our other kids had been vaccine injured, as well (without their regression being as sudden as hers). The continued bad news is that she continued to go downhill for the next 18 months. The good news is that the treatments we finally discovered were able to clear her out and bring her back to functioning. However, she still has the dysregulation at times and likely will the rest of her life (once autoimmune, always autoimmune). That said, though we are not against vaccines, we are terrified to use them for our family anymore. Our family is fully vaccinated except for the most recent school vaccine requirements, but we have chosen exemption from this point forward (unless of course, the benefits outweigh the risks). What you have to understand is that the current concern centers around that fact that medical exemptions are impossible to get based on parental testimony. Also - many doctors still expect vaccine-injured people to get vaccines even when they, themselves, have seen the effects of the injuries in these patients! We rely on autonomy to keep our family healthy. We can no longer allow the risk that a vaccine could trigger the torturous, “brain-on-fire” illness in our kids, and we cannot go through more financial devastation. We respectfully and desperately ask that you please consider – comprehensively – all the consequences that vaccine mandates can cause to families, and fight against government mandates for the sake of our families. Also, for all vaccines, we ask that you continue the allowance of medical exemptions and religious exemptions in Kansas, and to please add general exemptions for schools and workplaces. Micaela Widman and Jerad Widman, MD
October 27, 2021Chairman Erickson and Committee Members,
First, I want to thank you for taking the time to meet about this grave issue, the federal COVID vaccinemandate. I believe that the constitution was made for such a time as this. Currently, we have the most totalitarian presidential administration this country has ever endured. We must leverage the power of the people and the states to counterbalance this tyranny. We the people of Kansas demand that Kansas boldly oppose this abuse of power. It is obvious why the government should not force its citizens to take any drug or vaccine. We have examples from history of a government forcing people to undergo medical procedures and the results were horrific. Need I mention Josef Mengele?
Next, I would like to explain how the mask and vaccine mandates have personally impacted me. I am a Speech Language Pathologist in a public school and performing my job while the children and myself are masked is completely ineffective. I am unable to hear the children talking and I cannot see their mouth to properly assess what sounds they are making. Children are more wary of a stranger who has most of their face covered up. I have seen first hand how very young children are less responsive to a masked face. I have also witnessed young children who are developmentally delayed and have been unable to socialize this past year because their parents are afraid of taking them out due to the constant media propaganda. By now, those of us who absorb actual research know that children are not the ones affected by the actual virus.
My sister-in-law was recently notified by her job that she has until January 1st to get the vaccine or become unemployed. She recently obtained her Physical Therapist Assistant License, something that she worked very hard to achieve, and will now have to give up her career. My husband, who works remotely, was just notified that he must show proof of vaccination by December 8th or quit his job. A medical or religious exemption is available, as long as it doesn’t cause “undo burden” on his company. He is still debating whether or not to apply for a religious exemption. It seems like it is enabling his company to make a poor decision and is also allowing them to discriminate against his fellow coworkers who aren’t religious. People should be able to refuse the vaccine because of basic common sense. I have another friend who just had her first baby and who works in a nursing home. Her company is also mandating the vaccine and she doesn’t want to get it, but needs the income to care for herself and her new daughter.
Finally, let us hearken back to when members of the Biden administration proclaimed they couldn’t mandate a vaccine. Around a year ago, a liberal acquaintance of mine emphatically stated that I had nothing to worry about regarding a mandate. It took less than a year for the idea of a vaccine mandate to go from unacceptable to reality. Based on my observation, it seems that the majority of common people, conservative, liberal, or politically uninvolved, disagree with the mandate. Many of them don’t want to be political and won’t raise a respectful ruckus. However, rest assured that opposing these mandates is the will of the people.
Thank you for your time,
Callie Williams

Written testimony to stop government vaccine madates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
Hello,My name is Ricky J Woelk. This will be an email only testimony.
Chairman Erickson and Committee members:I have worked Bethesda Nursing Home in Goessel Kansas for just over 25 years first in Maintenance and then as Technology Manager. There have been many challenges throughout those years, but none as menacing as this government vaccine mandate. There is currently a staffing crisis where I work caused by a variety of factors, mostly the hassles of working with a facility with so many regulations and a lower pay scale. This unfair and unprecedented vaccine mandate (which includes no provision for religious or medical exemptions) will likely cause the nursing home where I work to close, and it's residents to have to move out of the facility and community that they love. Although the flu vaccine is pretty much required, we can still refuse it and wear a mask during flu season. In the case of this mandate, noncompliance would cause my nursing home to lose funding for around 75% of our residents because they are there through Medicaid funds. This mandate is unconstitutional and heartless. Please do all you can to stop it! Thank you!
WRITTEN Testimony to STOP Government Overreach COVID-19 Mandates
To Chairman Erickson and committee members,
Thank you for meeting out of session for this urgent matter and for reading and listening to our
testimonies. As a native-born Kansas wife, mother and activist I’m writing to voice my grave concern and
opposition to all COVID-19 mandates and particularly against COVID-19 vaccine mandates imposed by
government or employers. My family has been significantly affected mentally, physically and
emotionally by the COVID-19 lockdowns, forced mask requirements, and now vaccine mandates. We
have been shamed and ridiculed for choosing to breathe freely and ejected from private restaurants and
shopping centers as well as public attractions including the Flint Hills Discovery Center. I’ve had to teach
my children that it’s okay to disobey certain rules if they infringe on our religious beliefs or can cause us
harm. Never in my life have I been a rule-breaker and I’ve always raised my 6 children to obey authority,
but that’s just one more change that COVID-19 mandates have brought about.
I oppose all vaccine mandates, especially for this ridiculous excuse of a vaccine which couldn’t
even pass animal safety studies. My entire extended family and I agree we will never receive this vaccine
for both religious and health reasons. Unsurprisingly, our federal government is now attempting to force
small businesses to mandate the vaccine to their employees. My husband’s employer does not want to
enforce this mandate, but they will abide by whatever comes down from the Biden administration and
OSHA. My husband is at a very real risk of losing his job for the first time in his 25-year career. He has
provided for our family day in, and day out during that time and never once have we needed
government assistance in the form of welfare, food stamps or Medicaid type insurance. All of that will
certainly change if he loses his job and we’ll be forced to become a drain on our incredible state rather
than contributing to the benefit of others. I’m asking that you as Kansas senators and representatives
act immediately and pass legislation that will stop the COVID-19 vaccine mandate. I pray to God that
you’ll make the best decision for the Kansans you represent rather than the pharmaceutical companies
who are trying to pay you off. Remember, I didn’t get paid one cent to write this, but every piece of pro-
vaccine propaganda, publicity or PR originates from a paid pharma employee.
Sincerely,
Sonja Woods
OCTOBER 27, 2021
Dear Chairman Erickson and committee members,
I am against government mandates of COVID-19 vaccines. First, a mandate is not a law. Just because the current
administration wants to be a dictator does not mean he can rewrite the meaning of the law. A law needs to be passed.
As far as I have seen there is nothing that has been officially written saying it is a law. So, employers should not have
to comply. It is unlawful and against our Constitutional rights.
Second, I do not understand why no one is considering the protection from natural immunity. Before this virus
became political, the science was that the antibodies created form contracting an actual virus are typically way more
effective than that of a shot. It is also proven that the shots efficacy diminishes quite a lot after a period of 3 months.
The studies I have seen show that the natural infection antibodies are lasting a lot longer.
Third, the shot is not working. People who get it can still contract the virus, spread the virus, and die from the virus. If
you look at studies in Israel, India, and Great Britain you will see evidence of this. Our leaders are suppressing
information leading to even more widespread distrust.
Fourth, this virus has a very high survival rate. With the adverse effects a person can have from the shot should
concern anyone who is considering taking it. We should not be forced. It is again, against our Constitutional rights.
and coercion is unacceptable.
I am more concerned of the effect of the shot than from contracting and dying from the virus. I have a 99.8% chance of
survival. I will not take a shot as I have already had the virus and I don’t need one. I have antibodies. My child will not
be taking the shot. He has more of a chance to die from getting hit by a meteor that dying from this virus. Yet our
schools insist on targeting them with masks. I am sure they are going to target them for the shot. The fact that the
FDA, so called, approved this for anyone in asinine and negligent. There is not enough data and someone just telling
me it is safe is unacceptable. I want proof. I want studies. I want a lot of it.
Regards,
AimeeWoofter
Aimee Woofter
Testimony to STOP Government Overreach COVID-19 Mandates
EXTERNAL: This email originated from outside the organization. Do not click any links or open any attachments unless youtrust the sender and know the content is safe.
To chairman Erickson
I am writing to you to let you know that I am one of those millions of people that are against covid mandate.
Just like others my reasons are the same, and the most important is my freedom
I don't like to be vaccinated and I don't need to be forced to do it.
Aileen
Sent from Yahoo Mail on Android
Yessaminyen Yessa

Chairman Erickson and committee members,
My name is Melinda Young. I am AGAINST Government Mandates of Covid-19 Vaccines.
First, a little bit about myself. I am the wife of a County Extension Single Agent who works long hours to serve the community in a number of different ways. I’m the mother to three children. My two daughters are aged 8 and 5 and attend a small private Christian school. My son is just two months old, which is why I chose not to be with you today. But I wanted to send a testimony in support of all of you. I’m with you in spirit because I strongly believe that if we don’t fight for freedom, our kids won’t have any.
The freedom I’m talking about is the freedom to choose how we live our lives. I believe each and every one of us deserves to live and work the way we want to without being forced something we don’t want. Every day we have choices to make. Soon we may not get to have choices. That’s what we need to stand together and fight for today.
My family and I have lived our lives the best we could during the past year and a half. We have worked and tried to raise our kids in a good environment as fear and anxiety free as possible. Luckily, we’ve been able to enjoy most luxuries pre-Covid and none of us have gotten Covid.
My husband is an Extension Agent and works hard. He values his job so much that he is willing to get the shot to keep it even though it is not aligned with his beliefs. He feels like he’s caught in a corner between doing the right thing and protecting his family. I am concerned over Vaers reports of vaccine injury. I have seen too many reports of injury and death from these vaccines. I have family members who have gotten blood clots or have gotten very sick after receiving these vaccines. It’s enough to make me question the safety of them and I’m writing today to defend my husband and many others who are facing these forced jabs.
I’m here in spirit with you because I want to be a voice for everyone who wants or needs to have a voice because if I don’t then who will? I’m hoping that the mandate will be lifted and not enforced so that good workers will not have to make this decision that will affect their livelihood.
It all started with the masks. Our small Christian school requires them (but the church does not for some reason – How Ironic!). My older daughter and I have had Respiratory infections after wearing masks. She has to wear one at her school, which has caused problems to which she takes Chloro tablet each day to help prevent respiratory issues at school. I quit wearing masks after a bout of Bronchitis/Pneumonia for over a month. I did not Covid – I recently had the antibody test, which came back negative. With the encouragement of several friends in the area, I have not worn a mask since.
You might be wondering: How did you get through your pregnancy without wearing one mask? Well, I just never wore it. They would give me one at the door and I would either put it in my pocket or put it on my chin. I never put it over my nose and face again. No one in the clinics or hospital ever told me I needed to put it on correctly.
So, my hospital visits during my pregnancy were very normal. One thing that did surprise me though was when I asked my Doctor about whether to get or not to get the Covid vaccines during pregnancy. He blatantly said: “I’m not recommending it during pregnancy but it’s your choice to me.” That’s when I knew that if he’s not truly recommending it, then it must not be safe. If it was safe for me to get it, he would have said I SHOULD GET IT.
Sadly, I’ve known several pregnant friends who have gotten the vaccine, and some have had miscarriages. One vaccinated friend had her baby around the same time as me and her baby was born with a heart defect. He had to have surgery and probably must see a pulmonologist for the rest of his life. That is why I believe that this Covid vaccine should not be mandatory for all because it’s not one size fits all. A woman can have a healthy pregnancy without the vaccine – I’m proof of that.
So, my friends in Extension who are being forced to get the shots while pregnant are at risk of miscarriages and postnatal issues. That is not okay. Pregnant women should be able to make that choice.
I don’t think healthy people should be forced to have the vaccine. For one thing, THERE IS NO FDA approved vaccine. The vaccine that we thought the FDA approved is actually not available in our country. So, the vaccine being required is going to be an Emergency Use Only shot. It is against our Civil Right to mandate an Emergency Use Only Shot.
What’s in the shot? Well, one ingredient that has been verified to be in the shot is Graphene Oxide, which is poison to humans. Another ingredient is aborted fetal baby tissue. If you’re a Christian like me, that information may disgust you. It’s devilish. Which reminds me. A third ingredient in the Vaccine is called Luciferase. Lucifer is Devil’s Name. Why would the ingredient be named something that is supposed to be good for us?
This is a virus with a 99% Recovery rate and a cure. Hydroxychloroquine and Ivermectin does work when given. There’s no need for a Mandatory Vaccine that ruins your God Given immune system. He made us perfectly. There’s no need for the mandate to change how he made us with an mRNA substance. This should be a choice. If you want the mRNA, then you have it for free! But if you don’t, then you have the freedom to make that decision as well.
Where am I getting my information? Doctors all over the world. Real Doctors who have spoken out and lost their jobs or left their jobs because of speaking out. Hundreds of them have spoken out and the information is out there for us to find. There are several Patriots I follow to get news and information. You can find them all on Rumble.com.
A mandate is not a law. A mandate of this shot is a violation of our Civil and Religious Rights to Freedom. There’s a lot of people counting on your committee to make the right decision. Please remember that this should NOT BE a one sized fits all decision.
I pray that you have a good day and God Bless You All!
Melinda Young
RE: Written Testimony to STOP Government Overreach COVID -19Mandates
EXTERNAL: This email originated from outside the organiza�on. Do not click any links or open any a�achments unless you trust thesender and know the content is safe.
A�en�on: Chairman of The Special Commi�ee on Government Overreach and Impact of COVID-19 Mandates – Erickson and commi�ee members.
I value my liberty and freedom and am not in favor of these mandates that are being imposed on the ci�zens of Kansas and the United States. Please consider my voice in the wri�en no�ce to the special commi�ee on Government Overreach and Impact of COVID-19 Mandates. I vote no on the Mandates. This means I am NOT in favor of these mandate. If someone wants to get the vaccine, that is their choice and am thankful it is available for those who want it. But by no means should this be forced on anyone. This is The United States of American, land of the FREE!
Agnes T Zimmerman
Sent from Mail for Windows
To: Chairman Erickson and committee members I am submitting my written testimony to you in opposing vaccine mandates for COVID 19. I don’t believe that the government nor private business working at the behest of the federal government has the right to force an individual to take an experimental gene therapy injection without proper informed consent which cannot be obtained without long-term, unbiased data regarding the safety and efficacy of these drugs. Recent studies as well as real time data is showing that these vaccines are “leaking”, which not only means that they do not prevent the fully vaccinated from contracting and spreading the virus but may also mean that it is likely causing the
virus to mutate which could actually prolong the pandemic. Naturally acquired immunity is far more robust, yet there is no exemption for those who have already contracted and recovered from the virus. Why? When we have more than 50 studies showing that naturally acquired immunity has longer lasting and much broader protection than the narrowly focused spike protein mechanisms of the vaccines. Another big issue is the way they are smearing any doctor or patient who attempts to treat COVID 19 early with the numerous drugs that have decades of safety data and are cheap and readily available (or at least were before being politicized) and are proving in real time to be highly effective at keeping people out of the hospitals and
preventing death. I have had numerous pharmacies refuse to fill a prescription from a board certified physician for a drug that is safer than Tylenol and has received the Nobel prize as recently as 2015! How is it possible for a pharmacist to get between me and my doctor and make the decision to refuse to fill a prescription? I was astonished to discover that in the state of Kansas not only is this legal but the language of the law actually encourages this behavior!In most states this considered practicing medicine without a license and is forbidden by law. KS statute 65-1637 is failing us and needs to be changed. Furthermore, even though we are being told that the Pfizer vaccine has full FDA approval, to my knowledge ALL of the
COVID 19 vaccines available in the U.S. are still under E.U.A. meaning that there is NO legal recourse for an individual who is harmed by taking the injection. Threatening our jobs and ability to provide for our families is blatant coercion. I believe this violates the Nuremberg code and denies the individual of their God-given right to bodily integrity and personal autonomy. As many Americans are being forced to make one of the most difficult decisions of their lives, I am asking you to do the same for the thousands of Kansans like myself who choose not to get the jab for whatever reason, religion, ethics, risk vs. benefits etc… we feel trapped. Forced by powerful politicians and bureaucrats in Washington D.C. to inject something we
do not want into our bodies or be shunned from society. You have the power to stop this! It won’t be easy but big things in life rarely are. Courage is contagious and with Iowa passing SF 193 through the senate subcommittee now is the time for Kansas to act! Before it’s too late. If we let them succeed with this mandate you can believe your children and grandchildren will be next, schools will be mandating the vaccines and booster shot after booster shot…
Loren Zody





























