Embed Size (px)
Citation preview
WHO/Polio/04.02


World Health Organization
G l o b a lP o l i o
E r a d i c a t i o nI n i t i a t i v e
Progress 2003
WHO/Polio/04.02
� iv
Ordering code: WHO/Polio/04.02Printed: May 2004
Copies may be requested from: World Health Organization
CH-1211 Geneva 27, SwitzerlandFax: +41 22 791 1571
E-mail: [email protected]
© World Health Organization, 2004
All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination,World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857;email: [email protected]). Requests for permission to reproduce or translate WHO publications - whether for sale or for
noncommercial distribution – should be addressed to Publications, at the above address(fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinionwhatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or ofits authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommendedby the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions
excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete and correctand shall not be liable for any damages incurred as a result of its use.
Photographs on the cover, from left to right, are the copyright of: WHO
Design & Layout: L’IV Com Sàrl, Morges, Switzerland

v �
Progress 2003
Executive summary 1
Polio eradication – major developments in 2003 2Highlights 2003 2Challenges 2003 2
Interrupting transmission of polioviruses 4
Polio eradication: Areas of work 8Intensification of supplementary immunization activities 8Certification-standard surveillance 13Containment of wild poliovirus stocks 16Development of post-certification immunization policy 18Strengthening of routine immunization services 19
Polio financing 21The funding gap 21New fundraising initiatives 22Donor support 22
Advocacy 25
The Future: Strategic Plan 2004–2008 28
Abbreviations and acronyms 31
Table of contents


1 �
� � �
The Global Polio Eradication Initiativeachieved strong progress in 2003. By the end of 2003, only 6 countries in theworld were still polio-endemic, the lowestnumber ever: Nigeria, India, Pakistan,
Niger, Afghanistan and Egypt.
Of particular note is the progress achieved inSomalia, which was taken off the endemic coun-try list, and in India, Egypt and Pakistan, whichrecorded lowest-ever levels of transmission duringthe second half of 2003, the traditional “high sea-son” for transmission. At the end of 2003, theworld had an unprecedented opportunity to finishthe job in 2004.
Despite this progress, however, an acute cashshortage in early 2003 led to a major tactical shift,forcing the scaling back and reprioritization ofactivities for the year. As increased emphasis wasplaced on the remaining endemic countries and“high risk” areas, most polio-free countries ceasedto conduct preventive immunization campaigns,leaving their populations vulnerable to potentialpoliovirus importations.
The risks due to this increasing vulnerability wereunderlined in 2003, when a new polio outbreakoriginating in northern Nigeria re-infected 8 pre-viously polio-free countries across west and centralAfrica. The outbreak occurred following the suspension of immunization campaigns in northern states of Nigeria in August, due to concerns by some public figures regarding thesafety of oral polio vaccine (OPV). For the firsttime ever, the number of countries suffering“importation” cases (9 countries) was greater thanthe number of actual endemic countries (6 countries).
In late 2003, the Global Polio EradicationInitiative launched the new Strategic Plan2004–2008, outlining the revised activitiesrequired to interrupt wild poliovirus transmission,the new target date to achieve global certification,products required to stop OPV and activities tomainstream the Global Polio EradicationInitiative. Of particular note, the new StrategicPlan outlines activities required to stop the routine use of OPV as soon as possible after global eradication, a policy decision taken at a sci-entific meeting of experts at WHO in September.
To interrupt wild poliovirus transmission asquickly as possible, endemic countries must inten-sify polio immunization campaigns throughout2004, and the international donor communitymust fill the global funding gap of US$ 130 million (as at January 2004) for activitiesthrough 2005.
The world is very close to becoming polio-free, aswild poliovirus transmission is now restricted geographically. Approximately 90% of all globalcases were found in Nigeria, India and Pakistan in2003. However, as 2003 ended, the polio out-break in west and central Africa was continuing tospread to additional countries, in some of whichthe quality of polio activities had been compro-mised by the acute cash shortage earlier that year.It was increasingly evident that this outbreakcould require a much larger, multi-country “emer-gency response” in 2004. It is time for the finalpush against polio, with the goal of interruptingtransmission by the end of 2004. ■
Executive summary
Progress 2003

Global Polio Eradication Initiative
� 2
Polio eradication –major developments in 2003
Highlights 2003� Somalia passed a full calendar year without
polio, reporting its last case in October 2002.Somalia’s success in eradicating polio is test-imony to the soundness of the polio eradicationstrategies, which work even in the mostchallenging country-settings.
� By the end of 2003, only 6 countries in theworld were still polio-endemic, the lowest-ever number: Nigeria, India, Pakistan, Niger,Afghanistan and Egypt. In 1988, the year theGlobal Polio Eradication Initiative waslaunched, more than 125 countries wereendemic.
� In 2003, 784 polio cases were reported world-wide, a significant reduction over 2002, when 1 918 polio cases were reported. Of the 784 cases, approximately 90% were found injust three countries: Nigeria, India andPakistan.
� Following an epidemic of 1 600 cases in 2002,India achieved the lowest number of cases everin 2003, by dramatically accelerating immu-nization activities, increasing both the qualityand quantity of immunization campaigns. Thecountry launched the largest-ever health campaign in history, immunizing more than165 million children in just six days in February2003.
� Rotary International raised US$ 119 millionfrom its membership in a 12-month campaign to help close the funding gap.Rotary’s total contribution to polio eradicationhas exceeded US$ 500 million, and by the timethe world is certified polio-free, donations willreach US$ 600 million.
� The Organization of the Islamic Conference(OIC) and the African Union (AU) adoptedresolutions to eradicate polio from theirMember States. The G8 reaffirmed its commitment to eradicating polio at its Summitin Evian, France.
Challenges 2003� An acute cash shortfall in early 2003, and a
changing epidemiology, prompted a major,unprecedented tactical shift in the Global PolioEradication Initiative, forcing a scaling backand reprioritization of activities for the year.Increased emphasis was placed on the remain-ing endemic countries and “high-risk” areas,but many countries were left increasingly vul-nerable as preventive immunization campaignscould no longer be conducted (55 countriesconducted preventive campaigns in 2003, com-pared to 93 countries in 2002).
� � �
Phot
o: Se
phi
A child receives polio vaccine during a National Immunization Day in India

3 �
Progress 2003
� In Nigeria, a number of northern states suspended polio immunization campaigns inAugust 2003, following concerns by some public figures regarding the safety of the poliovaccine. Subsequently, a new outbreakoccurred, originating in the state of Kano, and reinfecting previously polio-free areas withinNigeria (including Lagos), as well as eight previously polio-free countries across west andcentral Africa.
� For the first time ever, the number of countriessuffering polio due to imported virus wasgreater than the number of countries actuallyendemic. Importations will continue to be arisk until wild poliovirus transmission is inter-rupted everywhere. 52 cases of polio followingimportations into previously polio-free countries were reported in 2003.
� Despite an increase in programme costs of morethan US$ 100 million between May 2003 andJanuary 2004 due to the intensification of polioimmunization activities in priority countries,the Global Polio Eradication Initiative receivedmore than US$ 200 million in new fundingover that period. However, a global funding gap of US$ 130 million (as at January 2004) foractivities through 2005 continues to threatenthe goal of a polio-free world. ■
Phot
o: JM
Gibo
ux/R
otar
y In
terna
tiona
l
Polio immunization in Nigeria
� � �
Global Polio Eradication Initiative
� 4
Interrupting transmission of polioviruses
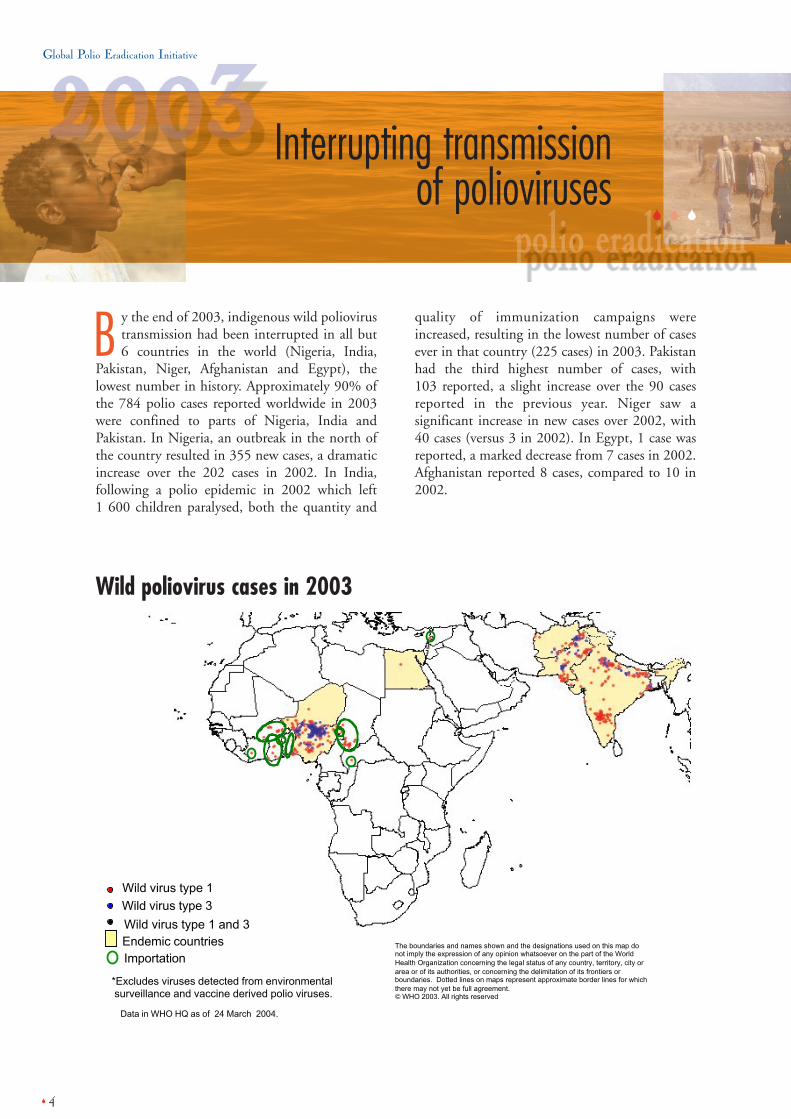
B y the end of 2003, indigenous wild poliovirustransmission had been interrupted in all but 6 countries in the world (Nigeria, India,
Pakistan, Niger, Afghanistan and Egypt), thelowest number in history. Approximately 90% ofthe 784 polio cases reported worldwide in 2003were confined to parts of Nigeria, India andPakistan. In Nigeria, an outbreak in the north ofthe country resulted in 355 new cases, a dramaticincrease over the 202 cases in 2002. In India,following a polio epidemic in 2002 which left 1 600 children paralysed, both the quantity and
quality of immunization campaigns wereincreased, resulting in the lowest number of casesever in that country (225 cases) in 2003. Pakistanhad the third highest number of cases, with 103 reported, a slight increase over the 90 casesreported in the previous year. Niger saw asignificant increase in new cases over 2002, with40 cases (versus 3 in 2002). In Egypt, 1 case wasreported, a marked decrease from 7 cases in 2002.Afghanistan reported 8 cases, compared to 10 in2002.
Data in WHO HQ as of 24 March 2004.
*Excludes viruses detected from environmental surveillance and vaccine derived polio viruses.
The boundaries and names shown and the designations used on this map donot imply the expression of any opinion whatsoever on the part of the WorldHealth Organization concerning the legal status of any country, territory, city orarea or of its authorities, or concerning the delimitation of its frontiers orboundaries. Dotted lines on maps represent approximate border lines for whichthere may not yet be full agreement. WHO 2003. All rights reserved
Endemic countries
Wild virus type 1
Wild virus type 3
Importation
Wild virus type 1 and 3
Wild poliovirus cases in 2003

5 �
Progress 2003
For the first time ever, the number ofcountries suffering importations wasgreater than the number of polio-endemic countries. In January, a childwas paralysed by polio in Lebanon, thefirst case seen in that country since1994. Genetic sequencing confirmedthat the virus had been imported fromIndia. A new outbreak originating innorthern Nigeria (see text box) spreadacross west and central Africa, re-infecting previously polio-free areaswithin that country (including Lagos),and 8 previously polio-free countries(Benin, Burkina Faso, Cameroon,Central African Republic, Chad, Côted’Ivoire, Ghana and Togo).Additionally, in the first quarter of2004, a case of polio originating innorthern Nigeria was reported inBotswana.
Wild poliovirus incidence 2002 vs. 2003
Wild poliovirus incidence by country in 2003 Number of reported polio cases 2003
355225103408121121251811
NigeriaIndiaPakistanNigerAfghanistanEgyptBeninBurkina FasoCameroonCentral African RepublicChadCôte d’IvoireGhanaLebanonTogo
Endemic countries
Importation countries*
Country
*For the first time ever, the number of countries suffering polio importations was greater thanthe number of actual polio endemic countries.
1000
800
400
200
600
1200
1600
1800
1400
Numb
er o
f cas
es
Nigeria India Pakistan Niger Afghanistan Egypt0
Reported polio cases 2002 Reported polio cases 2003
Nigeria – new outbreak spreads across regionIn August 2003, following concerns by public figures in northernNigeria regarding the safety of oral polio vaccine (OPV), polioimmunization activities were suspended in some states, most notablyKano. Subsequent to the suspension of the polio campaigns and theresulting decrease in population immunity levels, a new outbreakoccurred, reinfecting previously polio-free areas within Nigeria(including Lagos), and 8 neighbouring countries (Benin, Botswana,Burkina Faso, Cameroon, Central African Republic, Chad, Côte d’Ivoire,Ghana and Togo). Mass emergency immunization campaigns to protectchildren across west and central Africa from the spreading outbreakhad to be conducted in October, November and December, at a cost ofUS$ 25 million. Further campaigns will need to be conductedthroughout 2004 and 2005. The outbreak underlines the increasingvulnerability of populations to polio.

Global Polio Eradication Initiative
� 6
Disclaimer - The boundaries and names shown and the designations used on this map donot imply the expression of any opinion whatsoever on the part of the World HealthOrganization concerning the legal status of any country, territory, city or area or of itsauthorities, or concerning the delimitat ion of its frontiers or boundaries. Dotted lines onmaps represent approximate border lines for which there may not yet be full agreement. WHO 2003. All rights reserved
India: Wild poliovirus 2002 vs. 2003
India 2003: 225 polio cases
Disclaimer - The boundaries and names shown and the designations used on this mapdo not imply the expression of any opinion whatsoever on the part of the World HealthOrganization concerning the legal status of any country, territory, city or area or of itsauthorities, or concerning the delimitation of its front iers or boundaries. Dotted lines onmaps represent approximate border lines for which there may not yet be full agreement. WHO 2003. All rights reserved
India 2002: 1600 polio cases

7 �
Progress 2003
Increasingly vulnerable world as cashshortage prompts cessation of preventiveimmunization campaigns
The world is increasingly vulnerable to polioimportations, which will remain a risk until poliois eradicated everywhere. The acute cash shortageand changing epidemiology which prompted amajor tactical shift as available resources werefocused on endemic and high-risk areas, meantthat preventive immunization campaigns ceasedin most polio-free countries, leaving the popula-tions increasingly vulnerable to poliovirus.Consequently, rapidly eradicating the final polioreservoirs in 2004 became an urgent internationalpublic health issue.
For 2004 – interrupt wild poliovirustransmission and fill the funding gap
On 15 January 2004, an emergency meeting ofhealth ministers of the remaining polio-endemiccountries was convened at the World Health
Organization (WHO) in Geneva, Switzerland.Delegates presented data on the status of eradica-tion activities in their countries, alongside plans torapidly interrupt poliovirus transmission by theend of 2004. With polio transmission at the low-est-ever levels in key countries such as India,Pakistan and Egypt, the ministers concluded thatthe world has a rare opportunity in 2004 to haltthe spread of the virus. The ministers unveiledbold new plans to immunize 250 million childrenmultiple times in an accelerated polio immuniza-tion campaign schedule throughout 2004.Delegates at the meeting publicly committed tothe plan by signing the Geneva Declaration for theEradication of Poliomyelitis.
A global funding gap of US$ 130 million (as atJanuary 2004) for activities in 2004 and 2005continues to threaten the goal of a polio-freeworld, and must urgently be filled. ■
� � �
Global Polio Eradication Initiative
� 8
Intensification ofsupplementaryimmunization activities
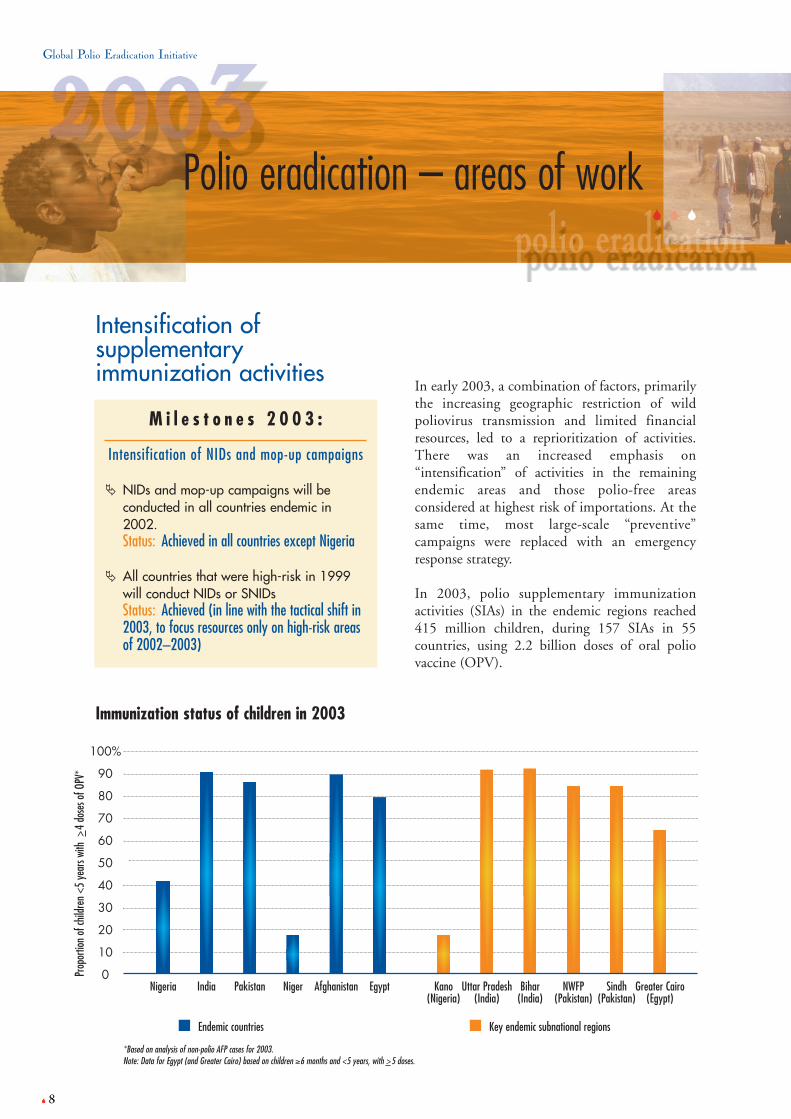
In early 2003, a combination of factors, primarilythe increasing geographic restriction of wildpoliovirus transmission and limited financialresources, led to a reprioritization of activities.There was an increased emphasis on“intensification” of activities in the remainingendemic areas and those polio-free areasconsidered at highest risk of importations. At thesame time, most large-scale “preventive”campaigns were replaced with an emergencyresponse strategy.
In 2003, polio supplementary immunizationactivities (SIAs) in the endemic regions reached415 million children, during 157 SIAs in 55countries, using 2.2 billion doses of oral poliovaccine (OPV).
� 8
M i l e s t o n e s 2 0 0 3 :
Intensification of NIDs and mop-up campaigns
� NIDs and mop-up campaigns will beconducted in all countries endemic in2002. Status: Achieved in all countries except Nigeria
� All countries that were high-risk in 1999will conduct NIDs or SNIDs Status: Achieved (in line with the tactical shift in2003, to focus resources only on high-risk areasof 2002–2003)
Polio eradication – areas of work
Immunization status of children in 2003
50
40
20
10
30
60
80
90
100%
70
Prop
ortio
n of
child
ren
<5 y
ears
with
>4
dose
s of O
PV*
*Based on analysis of non-polio AFP cases for 2003.Note: Data for Egypt (and Greater Cairo) based on children ≥6 months and <5 years, with >5 doses.
Nigeria India Pakistan Niger Afghanistan Egypt Kano(Nigeria)
Uttar Pradesh(India)
Bihar(India)
NWFP(Pakistan)
Sindh(Pakistan)
Greater Cairo(Egypt)
0
Endemic countries Key endemic subnational regions

9 �
Progress 2003
Number of SIAs in 2003
0 NIDs5 SNIDs2 NIDs4 SNIDs4 NIDs4 SNIDs2 NIDs3 SNIDs4 NIDs2 SNIDs4 NIDs4 SNIDs
2 NIDs0 SNIDs2 NIDs0 SNIDs0 NIDs2 SNIDs2 NIDs0 SNIDs1 NID2 SNIDs2 NIDs0 SNIDs2 NIDs0 SNIDs4 NIDs0 SNIDs2 NIDs0 SNIDs
Polio case count2003
355
225
103
40
1
8
3
11
2
1
25
1
8
1
1
Endemic countriesNigeria
India
Pakistan
Niger
Egypt
Afghanistan
Importation countriesBenin
Burkina Faso
Cameroon
Central African Republic
Chad
Côte d'Ivoire
Ghana
Lebanon
Togo
CountryNumber of SIAs
in 2003
2 NIDs1 SNIDs2 NIDs0 SNIDs0 NIDs2 SNIDs0 NIDs4 SNIDs2 NIDs0 SNIDs2 NIDs5 SNIDs0 NIDs5 SNIDs
Polio case count2003
0
0
0
0
0
0
0
Recently-endemic countriesAngola
Bangladesh
Democratic Republic of the CongoEthiopia
Nepal
Somalia
the Sudan
Country
Supplementary Immunization Activities (SIAs) in 2003
Phot
o: Na
sir M
irza
Polio immunization activity in Pakistan

Global Polio Eradication Initiative
� 10
India – a model response to the 2002epidemic
In India, the number of polio cases decreaseddramatically in 2003, with 225 cases reported forthe year.
In 2002, India suffered an epidemic of polio caseswhich left 1 600 children paralysed. Indiainstigated a model response to this epidemic, as it accelerated its immunization activities,dramatically increasing the number and quality of large-scale immunization campaigns – from 3 campaigns in 2002, to 6 campaigns in 2003.
Social mobilization and communication activitieswere enhanced, in efforts to reach all childrenunder the age of 5 years, regardless of socio-economic background. A particular focus wasplaced on the remaining under- or un-immunizedgroups of children in the state of Uttar Pradesh. Inclose collaboration with the Government of India,UNICEF India deployed 4 000 individuals toassist national health workers with communitymobilization activities to reach Muslim children –the group which represented a disproportionate59% of new polio cases in 2002. As a result of thissocial mobilization effort, the proportion ofMuslim children receiving three or more doses oforal polio vaccine (OPV) in India increased from61% in 2002 to 85% in 2003.
As a result of this intensification of SIAs in 2003,India had both the lowest number of cases and thelowest ever levels of transmission during the late2003 “high season”. In 2004, India has thegreatest opportunity for success in stoppingtransmission of wild poliovirus.
Non-polio AFP cases (Muslim children age ≥6 months ≤5 years) by OPV status, Uttar Pradesh
India National Immunization Day – not your typical week!
Did you know what is involved in a 6-day immunizationcampaign in India? Here are just some of the basicfacts…� 640 000 vaccination booths� 2.3 million vaccinators� 1.1 million vaccination teams� 137 000 supervisors, with 137 000 vehicles (cars,
motorcycles, mopeds, bicycles, boats, whatever ittakes)
� 200 million doses of polio vaccine, carried around thecountry in 2 million vaccine carrier bags
� 6.3 million ice-packs to keep all those doses of poliovaccine in the 2 million vaccine carrier bags cold
� 191 million homesvisited
� 169 million childrenimmunized in just 6 days!
And that’s just one forone, single NID! In 2004, India will conduct5 such NIDs, and 1 Sub-National ImmunizationDay (SNID) targeting 100 million children.
After being immunized with OPVduring a National Immunization Daycampaign, a young child gets itsfingers marked to ensure that everychild under five has been vaccinated.
Phot
o: ©
Seph
i
≥4 doses61%
0 dose11%2002
(N=450)
0 dose1%
1-3 doses14%
2003(N=336)
Data as of 10 January 2004
���1-3 doses
28%≥4 doses
85%

11 �
Progress 2003
Nigeria – suspension of campaigns innorth of country leads to outbreak
In Nigeria, the number of polio cases increasedsignificantly, with 355 cases reported in 2003 (thehighest number worldwide), compared to 202 cases the year before.
The primary reason for this marked increase wasthe suspension of SIAs in key northern states ofthe country, particularly Kano. The suspensionoccurred as a result of concerns among somecommunity leaders regarding the safety of oralpolio vaccine (OPV).
Health authorities tried to counter the lack of nationwide activities by conducting up to 5 Sub-National Immunization Days (SNIDs) inareas which were participating. However, theintense transmission of poliovirus in the north ofthe country and inconsistent SNID coverage ledto the re-infection of previously polio-free areas within Nigeria (including Lagos), as well as8 previously polio-free countries across west andcentral Africa.
Pakistan and Afghanistan – strongprogress in second half of the year
In Pakistan, although the number of polio casesincreased to 103 in 2003, from 90 in the previousyear, by the end of 2003 the level of poliovirustransmission during the “high season” was at itslowest ever.
The progress in late 2003 was due to the highnumber of SIAs conducted, with 4 NIDs and 4 SNIDs conducted during the year. Asimportantly, the quality of the SIAs continued toimprove throughout the year, with 87% of non-polio acute flaccid paralysis (AFP) cases havingreceived 3+ doses of OPV by the end of 2003.
Afghanistan – which shares a cross-borderpoliovirus reservoir area with Pakistan – reported8 polio cases in 2003, compared to 10 in 2002.Afghanistan maintained its SIA schedule andsynchronized its campaigns with Pakistan.Activities were intensified by increasing SIAquality, with 87% of non-polio AFP casesreceiving at 3+ doses of OPV.
OPV safety: Ongoing controversy in Nigeria highlights the risks of “invalid” tests
In August 2003, as a result of concerns among some community leaders regarding the safety of the oral poliovaccine (OPV), polio immunization campaigns were suspended in several northern states, most notably Kano.Specifically, some leaders suggested that estrogen was introduced into OPV in an effort to depopulate Nigeria'spopulation.
Both state and federal authorities in Nigeria have been working tirelessly to resolve the ongoing controversy,repeatedly testing OPV to demonstrate its safety. All of the analyses that were conducted with “valid” testsdemonstrated the absence of estrogen. Some analyses conducted with invalid tests have suggested“false–positive” signals of estrogen at the margins of the tests' detectability. Regrettably, these “false–positive”signals have been misinterpreted widely in some national media outlets, and thereby added to the confusion.
To investigate these concerns, the Federal Government of Nigeria established the “Joint Committee on OPVSafety”, consisting of federal and state authorities, including two delegates from Kano state, under thechairmanship of the Shehu of Dikwa, Kyari Ibn Umar El-Kanemi. Although estrogens are not used in theproduction of OPV and are not present in the finished product, the Committee recommended “gold standard”testing in at least two independent laboratories to demonstrate the vaccine's safety.
On 15 March 2004, the Committee filed its report with H. E. Eyitayo Lambo, the Minister of Health ofNigeria, who presented the findings to H. E. President Olusegun Obasanjo two days later. In its report, theCommittee unanimously re-affirmed the safety of OPV.
Key to the rapid resolution of the ongoing controversy will be the engagement of all key stakeholders inNigeria, and particularly Kano, in ensuring that full confidence in the safety of OPV is re-established among allcommunities.
Global Polio Eradication Initiative
� 12
Egypt – strong progress throughout theyear
Egypt dramatically reduced the number of poliocases in 2003 compared to 2002, with just 1 casereported for the entire year, in June (compared to7 cases in the previous year). Furthermore, thenumber of wild poliovirus positive environmentalsamples continued to decline markedly (from55% in 2001, to just 4% in 2003 – the mostrecent positive environmental sample wasreported on 6 January 2004).
The country intensified its immunizationactivities in 2003, as one additional NID wasconducted over the previous year, for a total of 4 NIDs and 2 SNIDs. The quality of SIAscontinued to improve throughout the year underthe leadership of the new Minister of Health. Bythe end of 2003, 89% of non-polio AFP cases hadreceived at least 5 doses of OPV, up from 74% in2002.
As a result of this strong progress, Egypt is ontrack to eradicate polio in 2004.
Niger – higher quality campaignsrequired
Niger saw a marked increase in new cases in 2003,with 40 new cases reported (compared to 3 in2002).
Although the country conducted 3 SNIDs and 2 NIDs in 2003, the quality of these activitiesmust urgently improve, if wild poliovirustransmission is to be interrupted. Surveillancedata suggested that as many as 82% of childrenwere still under- and un-immunized (receivingless than 4 doses).
As a result of the suboptimal polio campaignquality in 2003, and compounded by theoutbreak of new cases in the shared borderreservoir with Nigeria, wild poliovirustransmission remains extensive throughout allparts of Niger.
West and central Africa –intensified synchronized SIAs inresponse to Nigeria outbreak
Throughout west and central Africa, 51 cases ofpolio were reported in 2003 in 8 previously polio-free countries: Benin, Burkina Faso, Cameroon,Central African Republic, Chad, Côte d’Ivoire,Ghana and Togo. All cases were as a result ofimported poliovirus which was genetically linkedto Nigeria.
To respond to the ongoing threat caused by theNigerian outbreak, emergency synchronizedNIDs were conducted in late 2003, at aninternational cost of US$ 25 million.
The campaigns involved hundreds of thousands ofvolunteers and health workers, to reach 25 millionchildren under the age of 5 years across the region.Particular effort was placed on enhancingtechnical support and social mobilization toengage traditional and religious leaders in everycountry to counter the rumours concerning OPVsafety spreading out of Nigeria.
Children in these countries will continue to be atrisk of permanent polio paralysis until theoutbreak spreading from Nigeria is stopped.Emergency response campaigns will need tocontinue throughout 2004 and 2005.
� 12
Phot
o: H
Ever
ts/WH
O
National Immunization Day in Niger

13 �
Progress 2003
Certification-standardsurveillance
Surveillance for poliomyelitis and poliovirus reliesprimarily on reporting and laboratory investigationof cases of acute flaccid paralysis (AFP),supplemented in specific circumstances bycomplementary systems, such as environmentaland/or enterovirus surveillance. The quality of AFPsurveillance – its ability to detect ongoingtransmission of wild poliovirus in a country – isevaluated through three key indicators:
1) rate of reported AFP cases not due to wildpoliovirus (“non-polio AFP rate”) of at least 1 case of non-polio AFP per 100 000population aged < 15 years;
2) collection of “adequate” stool specimens fromat least 80% of reported AFP cases;
3) analysis of all AFP stool specimens (100%) inlaboratories accredited by WHO.
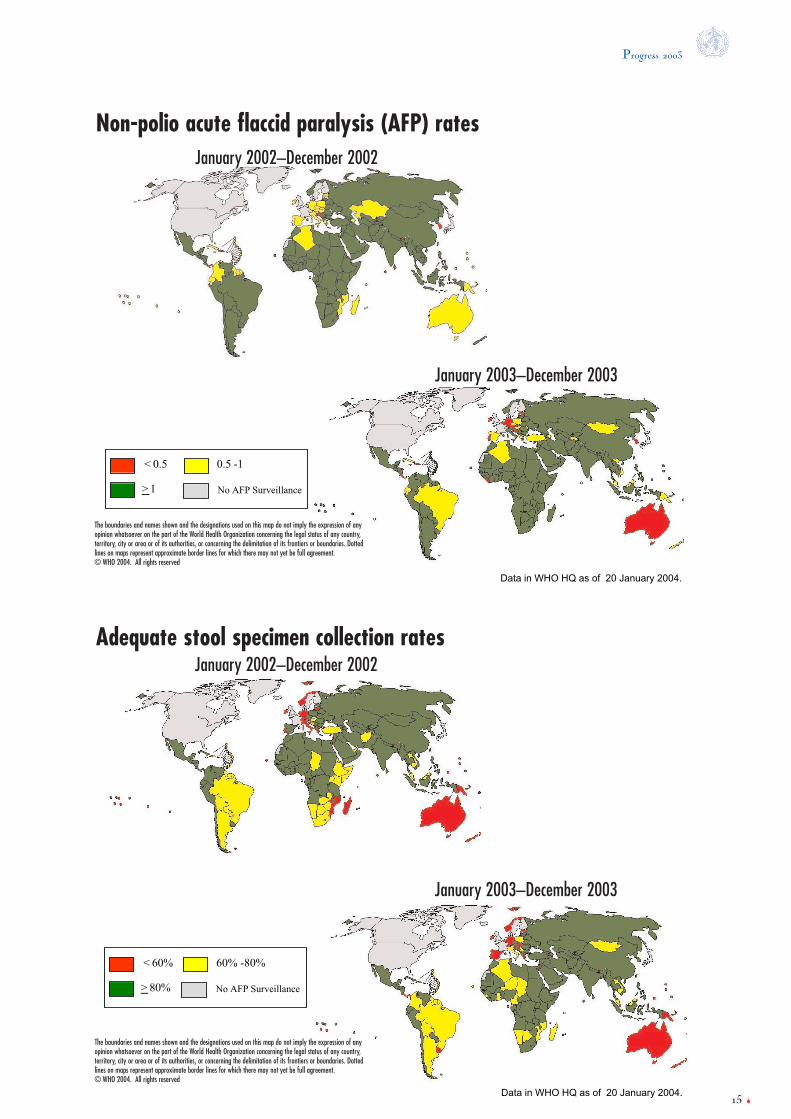
The timeliness and completeness of AFPreporting and collection of adequate stoolspecimens continued to be at the level of qualityrequired for polio-free certification in all WHOregions in 2003. The overall number of AFP casesreported globally decreased slightly from 2002 to2003 (mainly as a result of the large polio
outbreak in India in 2002); however, non-polioAFP rates remained at levels considerably above1/100 000 globally (1.9) and in all WHO regions(ranging from 1.22 in the European Region to2.60 in the African Region). The proportion ofAFP cases with adequate specimens increasedslightly, from 84% in 2002 to 86% in 2003,mainly as a result of improvements in specimencollection rates in two endemic WHO regions:the African Region (from 81% to 88%) and theEastern Mediterranean Region (from 88% to90%). All specimens (100%) were processed inWHO-accredited laboratories.
All countries endemic at mid-2003 maintained orachieved certification-quality surveillance,including Somalia. International AFP surveillancereviews continued to provide specific guidance tocountries on how to further improve the quality ofAFP surveillance. As recommended by the globaltechnical oversight body, the Technical ConsultativeGroup for the Global Eradication of Poliomyelitis(Global TCG), reviews were conducted inAfghanistan, Cameroon, Kenya, Madagascar, Maliand Mozambique. In an attempt to identify andclose subnational gaps in surveillance sensitivity,several key endemic countries continued (Pakistan)or began (India) to conduct formal internal AFPreviews at provincial or state level.
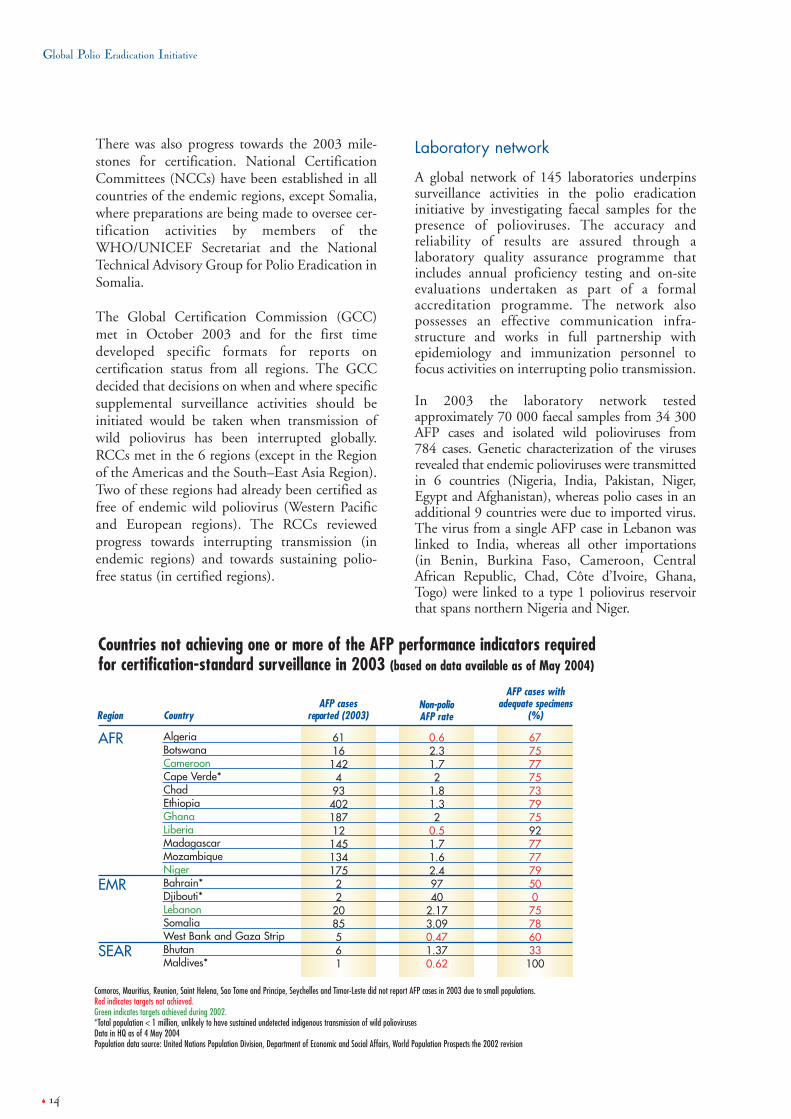
Progress in AFP surveillance is also monitored bythe number of countries in endemic regions notreaching certification-standard surveillance, whichdecreased from 19 in 2002 to 18 in 2003. Ofthese, 11 are in the African Region (including 9 countries with sample collection rates just below80%), 5 are small countries or areas in the EasternMediterranean Region (Bahrain, Djibouti,Lebanon, West Bank and Gaza) and 2 are smallcountries in the South-East Asia Region (Bhutan,Maldives).
Surveillance gaps which persisted until late 2002in southern and eastern Africa are beginning toclose. Four of the seven recently polio-endemiccountries in southern and eastern Africa whichhad lagged behind in AFP surveillance up to theend of 2002 have now reached certification-standard (Namibia, South Africa, Zambia andZimbabwe), leaving Madagascar, Mozambiqueand Botswana where sample collection rates werejust below the 80% target.
M i l e s t o n e s 2 0 0 3 :
� The Global Certification Commission(GCC) will have defined supplementarydata that will be needed for globalcertification from all previously certifiedregions.Status: Achieved (in progress)
� Supplemental surveillance will be initiatedas recommended by the GCC.Status: Ongoing
� Certification mechanisms will beestablished for all countries/areas lackingaccess to a national commission.Status: Achieved
� All AFR countries will have a NationalCertification Committee.Status: Achieved
Global Polio Eradication Initiative
� 14
There was also progress towards the 2003 mile-stones for certification. National CertificationCommittees (NCCs) have been established in allcountries of the endemic regions, except Somalia,where preparations are being made to oversee cer-tification activities by members of theWHO/UNICEF Secretariat and the NationalTechnical Advisory Group for Polio Eradication inSomalia.
The Global Certification Commission (GCC)met in October 2003 and for the first timedeveloped specific formats for reports oncertification status from all regions. The GCCdecided that decisions on when and where specificsupplemental surveillance activities should beinitiated would be taken when transmission ofwild poliovirus has been interrupted globally.RCCs met in the 6 regions (except in the Regionof the Americas and the South–East Asia Region).Two of these regions had already been certified asfree of endemic wild poliovirus (Western Pacificand European regions). The RCCs reviewedprogress towards interrupting transmission (inendemic regions) and towards sustaining polio-free status (in certified regions).
Laboratory network
A global network of 145 laboratories underpinssurveillance activities in the polio eradicationinitiative by investigating faecal samples for thepresence of polioviruses. The accuracy andreliability of results are assured through alaboratory quality assurance programme thatincludes annual proficiency testing and on-siteevaluations undertaken as part of a formalaccreditation programme. The network alsopossesses an effective communication infra-structure and works in full partnership withepidemiology and immunization personnel tofocus activities on interrupting polio transmission.
In 2003 the laboratory network testedapproximately 70 000 faecal samples from 34 300AFP cases and isolated wild polioviruses from 784 cases. Genetic characterization of the virusesrevealed that endemic polioviruses were transmittedin 6 countries (Nigeria, India, Pakistan, Niger,Egypt and Afghanistan), whereas polio cases in anadditional 9 countries were due to imported virus.The virus from a single AFP case in Lebanon waslinked to India, whereas all other importations (in Benin, Burkina Faso, Cameroon, CentralAfrican Republic, Chad, Côte d’Ivoire, Ghana,Togo) were linked to a type 1 poliovirus reservoirthat spans northern Nigeria and Niger.
CountryAFP cases
reported (2003)
611614249340218712145134175222085561
Non-polio AFP rate
0.62.31.72
1.81.32
0.51.71.62.49740
2.173.090.471.370.62
AFP cases withadequate specimens
(%)
677577757379759277777950075786033100
AlgeriaBotswanaCameroonCape Verde*ChadEthiopiaGhanaLiberiaMadagascarMozambiqueNigerBahrain*Djibouti*LebanonSomaliaWest Bank and Gaza StripBhutanMaldives*
Countries not achieving one or more of the AFP performance indicators requiredfor certification-standard surveillance in 2003 (based on data available as of May 2004)
Region
Comoros, Mauritius, Reunion, Saint Helena, Sao Tome and Principe, Seychelles and Timor-Leste did not report AFP cases in 2003 due to small populations.Red indicates targets not achieved.Green indicates targets achieved during 2002.*Total population < 1 million, unlikely to have sustained undetected indigenous transmission of wild poliovirusesData in HQ as of 4 May 2004Population data source: United Nations Population Division, Department of Economic and Social Affairs, World Population Prospects the 2002 revision
AFR
EMR
SEAR
Progress 2003
< 0.5 0.5 -1
> 1 No AFP Surveillance
Data in WHO HQ as of 20 January 2004.
< 60% 60% -80%
> 80% No AFP Surveillance
Data in WHO HQ as of 20 January 2004.
Non-polio acute flaccid paralysis (AFP) rates
Adequate stool specimen collection rates
January 2002–December 2002
January 2003–December 2003
January 2002–December 2002
January 2003–December 2003
15 �
The boundaries and names shown and the designations used on this map do not imply the expression of anyopinion whatsoever on the part of the World Health Organization concerning the legal status of any country,territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dottedlines on maps represent approximate border lines for which there may not yet be full agreement.© WHO 2004. All rights reserved
The boundaries and names shown and the designations used on this map do not imply the expression of anyopinion whatsoever on the part of the World Health Organization concerning the legal status of any country,territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dottedlines on maps represent approximate border lines for which there may not yet be full agreement.© WHO 2004. All rights reserved

Global Polio Eradication Initiative
� 16
Containment of wildpoliovirus stocks
Progress towards laboratory containment of wildpolioviruses continues worldwide. In WHOregions certified as polio-free (AMR, EUR,WPR), all countries have appointed a nationaltask force responsible for overseeing the Phase Iactivities – laboratory survey and inventory. 95% of these countries (128/135) have started anational survey of laboratories and 70%(91/135) have completed the survey andcompiled a national inventory of laboratoriesholding wild poliovirus materials.
Of considerable note was the completion of thePhase I activities in a number of industrializedcountries of western Europe and North America,particularly as these countries have long historiesof biomedical research and laboratory contactsworldwide. Belgium, Denmark, Germany,Ireland, Italy, Portugal and Sweden all reportedcompletion of national surveys in 2003. France,
Switzerland and the United Kingdom are in thefinal stages and expect to finish in 2004. In AMR,the United States of America reported completionof a national survey of over 100 000 laboratories,having identified 178 facilities with wildpoliovirus materials.
In WHO regions not yet certified as polio-free(AFR, EMR, SEAR), non-endemic countries havealso started containment activities. In EMR andSEAR, 12/28 (43%) polio-free countries havereported completion and compilation of anational inventory along with one country in AFR(Botswana).
As more than 100 countries in the world havenow completed the survey and inventoryactivities, in 2003 the process of evaluating thequality of the process began with results fromWPR, EUR and EMR expected in 2004. Thefinal reports generated from the qualityassessment of Phase I will serve as the basis forfuture containment activities after theinterruption of poliovirus transmission.
The publication of the Global Polio EradicationInitiative Strategic Plan 2004-2008 and the policyto stop routine use of OPV as soon as possibleprovides new direction to future containmentactivities and alters the milestones previously setfor 2003. Activities for Phase II containment andglobal certification will officially begin one yearafter the last documented episode of wildpoliovirus transmission anywhere in the world.The revised timeline for interruption oftransmission, as outlined in the new StrategicPlan, has shifted the milestone for implementingPhase II containment activities. Work continuesto focus on completing Phase I in all WHOregions and preparing the containment plans forcessation of routine OPV use. A third edition ofthe Global Action Plan for the LaboratoryContainment of Wild Polioviruses will bedeveloped, outlining the strategy to minimize therisk of reintroducing polioviruses from alaboratory to a community after interruption ofwild poliovirus circulation and cessation of OPVuse. Containment of all live polioviruses will beconsidered in the plan, which will be available in2005.
M i l e s t o n e s 2 0 0 3 :
� AMR and EUR will attain globalcertification containment requirements.Status: Ongoing EUR: 48/51 countries completed “survey andinventory” phase AMR: 40/47 countries started “survey andinventory” phase, with 9 countries completingthis phase
� National inventories and containment ofwild poliovirus infectious and potentiallyinfectious materials will be achieved underBSL-2/polio conditions in all countries ofAFR, EMR and SEAR.Status: Delayed due to ongoing endemic wildpoliovirus transmission
� Preparations will begin to establish finalglobal wild poliovirus repository(ies).Status: Ongoing

17 �
Progress 2003
Polio endemic
Survey not yet started
Conducting surveyReporting completion of surveyand inventory of laboratorieswith polio materials
AFR (48 countries) 27 1 1 1
AMR (47 countries) 47 40 40 9
EMR (22 countries) 17 15 15 9
EUR (52 countries) 52 52 52 49
SEAR (11 countries) 9 9 9 3
WPR (37countries and areas) 36 36 36 34
Progress with the “survey and inventory” phase of laboratory containment activities (Phase I)
Appointed a national coordinator Member States in each region which have:
Startedconductingsurvey of
laboratories
Begun compiling listof biomedical
facilities tobe surveyed
Submittedfinalized national
inventory oflaboratories
Laboratory containment 2003 – Progress with the “survey and inventory”

Global Polio Eradication Initiative
� 18
Development of post-certification immunizationpolicy
In September 2003, a meeting of scientific expertswas convened at WHO on immunization policiesfollowing the global eradication of wildpoliovirus. As a result of this meeting andincreasing scientific and programme data, thefollowing 3 landmark policy decisions were taken:
1. Cessation of oral polio vaccine (OPV):Since 2000, polio outbreaks caused by vaccine-derived polioviruses (VDPVs) have conclusivelydemonstrated that the continued use of OPV forroutine immunization could compromise the goalof eradicating all paralytic disease due tocirculating polioviruses.
To minimize the long-term risks associated withOPV, the decision was taken to stop the routineuse of this vaccine as soon as possible aftereradication, while surveillance sensitivity andpopulation immunity are high.
2. No universal introduction of inactivated poliovaccine (IPV):Based on the increasingly understood risks ofpolio re-introduction following OPV cessation,
and the plans of many OPV-using countries,WHO will not recommend universalintroduction of IPV. This is a decision eachcountry must make individually. Every countrymust plan for the cessation of OPV use, anddecide whether or not to introduce IPV; countriesdeciding to introduce IPV must makearrangements for its procurement. WHO and itspartners will continue to support individualcountries in the decision-making process, and willprovide technical assistance during OPVcessation, and, if requested, during theintroduction of IPV.
3. Strategies for the safe cessation of OPV:A road map for the safe cessation of OPV hasalready been developed, and published in the GlobalPolio Eradication Initiative Strategic Plan 2004-2008. This roadmap outlines the specific activitieswhich will need to be implemented, and include:■ the interruption of wild poliovirus transmission
globally;■ the appropriate containment of all laboratory
and vaccine manufacturing stocks of poliovirus,including Sabin strains;
■ licensing of monovalent OPV (mOPV) andmanufacture of IPV from Sabin strains (S-IPV);
■ maintenance of surveillance and laboratorycapacity to detect VDPVs that might circulateafter cessation of OPV;
■ establishment of a global OPV stockpile, andmanagement mechanisms thereof, in the eventthat it be required after routine use of OPV hasbeen stopped.
It is anticipated that in 2004, most researchrelevant to OPV cessation will be completed,including an analysis of stockpile options andstrategies. Guidelines for national decision-making on OPV cessation will be completed,outlining:
a) rationale for OPV cessation;b) risks of polio in the post-OPV era;c) surveillance requirements;d) post-OPV stockpile and response; ande) implications of IPV introduction.
A third edition of the Global Action Plan for theLaboratory Containment of Wild Polioviruses(GAP III) will be developed.
M i l e s t o n e s 2 0 0 3 :
Data Generat ion
� All scientific research data required forpolicy development is being collected.Status: Achieved
Pol i cy Deve lopment
� At least one forum is held with key policy-makers in each geopolitical block toreceive comments on the risk frameworkand post-certification immunization policyoptions.Status: Achieved (EPI manager meetings)

19 �
Progress 2003
Strengthening of routineimmunization services
The Global Polio Eradication Initiative waslaunched with the dual goals of interrupting wild poliovirus transmission globally andstrengthening of health systems, particularlyroutine immunization services. The milestones ofthe programme for the years 2001–2004 werereviewed by the Technical Consultative Group forthe Global Eradication of Poliomyelitis (GlobalTCG) and subsequently revised to focus on threeactivities:
1) strengthening routine immunization; 2) expanding surveillance; and 3) improving partnership management.
During 2003, the programme continued to focuson strengthening immunization services in thenon-endemic and recently-endemic countries.Major progress in the development andimplementation of the “Reaching Every District”(RED) approach was achieved, which has fourelements for improving immunization services atthe district level. These are:
a) re-establishment of outreach services; b) supportive supervision; c) establishing community links with service
delivery; and d) monitoring and use of data for planning
and managing resources.
As the RED approach is based upon polioexperiences and maximizes the use of the humanand material resources of the Global PolioEradication Initiative, it forms a strongfoundation for strengthening routineimmunization. The programme collaborated with the Global Alliance for Vaccines andImmunization (GAVI) and other partners whichprovided funds for immunization systemsstrengthening in Bangladesh, the DemocraticRepublic of the Congo, Ethiopia, Pakistan and theSudan. In these countries, polio-funded staff wereinstrumental in the planning, implementationand monitoring of activities for immunizationsystems strengthening. All these activities were
coordinated through the InteragencyCoordinating Committee (ICC) mechanism thathad been initially set up for polio eradication, butnow coordinates all immunization activities. Keyfeatures included the adoption of multi-yearExpanded Programme on Immunization (EPI)plans by the ICCs (Angola and Ethiopia),expansion of the Terms of Reference (TORs) andworkplans of polio-funded staff, or recruitment ofnational staff to supervise and coordinate EPIactivities at sub-national level (Bandgladesh andEthiopia), provision of supportive supervisionduring AFP surveillance visits, use of the poliosurveillance network to channel monitoring dataincluding district level coverage information,monitoring of reporting of priority diseasesurveillance data (the Sudan), and monitoring theuse of immunization systems strengthening fundsat the province or district levels.
Furthermore, countries which conductedsupplementary immunization activities formeasles control (Ethiopia) also used polio-fundedAFP surveillance officers to plan, implement andevaluate the activities. In many instances, theplanning was linked to that for poliosupplementary immunization activities, therebystrengthening the link between the Global PolioEradication Initiative and other disease controlactivities.
In late 2003, GAVI, in collaboration with WHOand UNICEF, initiated the “enhanced efforts inlarge population countries” of the GAVIframework, under which seven countries(Bangladesh, the Democratic Republic of theCongo, Ethiopia, India, Indonesia, Nigeria andPakistan) are undertaking renewed efforts tostrengthen routine immunization services. Morethan 35 million un-immunized children live inthese countries, and in 2004, additional fundingto support technical staff and immunizationstrengthening activities will be dispersed, toensure the RED approach is implemented.
The activities in 2003 show progress instrengthening routine immunization programmesthrough use of the polio surveillanceinfrastructure and collaboration with otherimmunization partners. In 2004, polioeradication-recruited staff, especially provincial
Global Polio Eradication Initiative
� 20
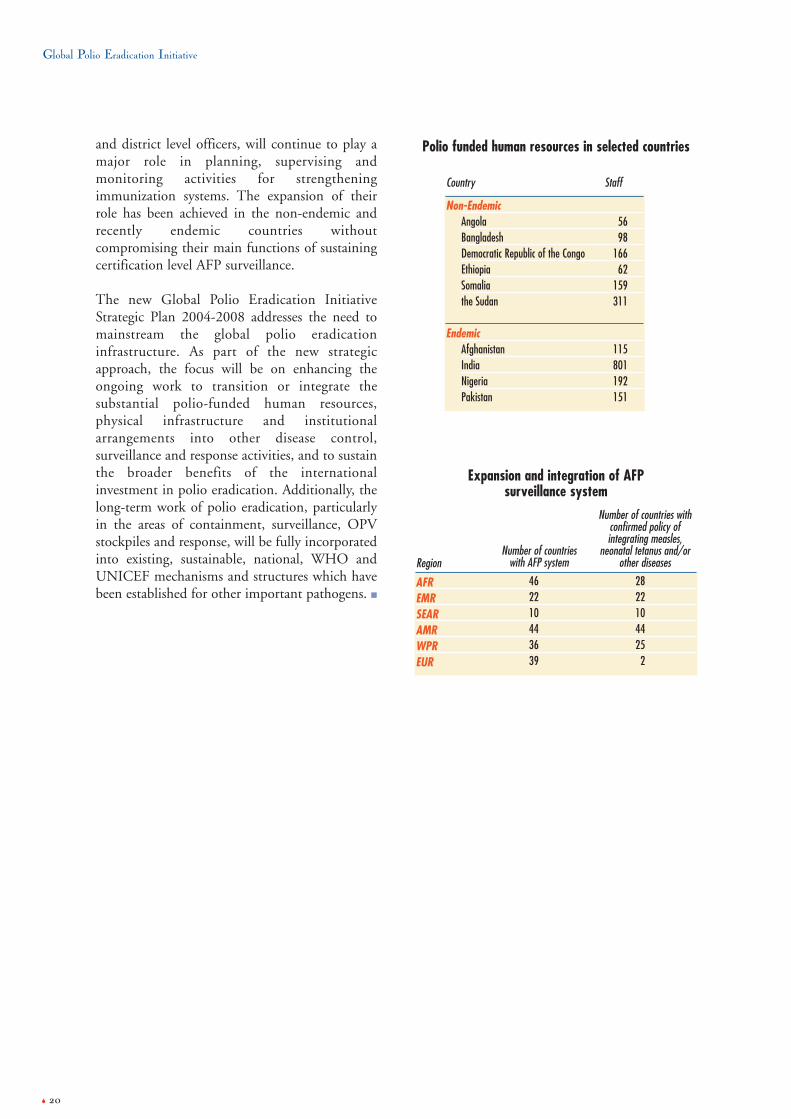
and district level officers, will continue to play amajor role in planning, supervising andmonitoring activities for strengtheningimmunization systems. The expansion of theirrole has been achieved in the non-endemic andrecently endemic countries withoutcompromising their main functions of sustainingcertification level AFP surveillance.
The new Global Polio Eradication InitiativeStrategic Plan 2004-2008 addresses the need tomainstream the global polio eradicationinfrastructure. As part of the new strategicapproach, the focus will be on enhancing theongoing work to transition or integrate thesubstantial polio-funded human resources,physical infrastructure and institutionalarrangements into other disease control,surveillance and response activities, and to sustainthe broader benefits of the internationalinvestment in polio eradication. Additionally, thelong-term work of polio eradication, particularlyin the areas of containment, surveillance, OPVstockpiles and response, will be fully incorporatedinto existing, sustainable, national, WHO andUNICEF mechanisms and structures which havebeen established for other important pathogens. ■
Non-EndemicAngolaBangladeshDemocratic Republic of the CongoEthiopiaSomaliathe Sudan
EndemicAfghanistanIndiaNigeriaPakistan
5698
16662
159311
115801192151
Polio funded human resources in selected countries
StaffCountry
Expansion and integration of AFP surveillance system
AFREMRSEARAMRWPREUR
462210443639
2822104425
2
Number of countrieswith AFP systemRegion
Number of countries withconfirmed policy ofintegrating measles,
neonatal tetanus and/orother diseases

21 �
� � �
The Funding Gap
International community responds tofunding gap
The global community responded to the acutefunding crisis experienced by the Global PolioEradication Initiative in early 2003, by providing additional resources of more than US$ 200 million between May 2003 and January2004.
Despite this extremely encouraging internationalsupport, the Global Polio Eradication Initiative still faced a critical funding gap of US$ 130 million for 2004 and 2005 (as at January2004), against projected costs of US$ 765 millionfor planned activities to interrupt transmissionglobally. The funding gap is a result of the increase
in the programme costs for 2004–2005 by morethan US$ 100 million to respond to poliovirusimportations in west and central Africa and theintensification of immunization activities in thepriority countries. At this time, flexible multi-yearfunding is essential to ensure that the funding gapof US$ 130 million can be met, and emergingprogramme needs can be responded to in a timelymanner.
At the end of 2003, with the assistance of coredonors and new fundraising initiatives, a total ofUS$ 635 million had been confirmed or projectedto be received for activities in 2004–2005. Majorcontributions for 2003 came from Canada, theEuropean Commission, France, Japan, Norway,the Russian Federation, Rotary International, the World Bank, the United Kingdom and theUnited States.
OthersUSAID
France
Gates Foundation
WB/Gates/Rotary/UNF
UK
Netherlands
EuropeanCommission
World Bank/India
Rotary International
UN Foundation
DenmarkGermany
JapanCanada
“Other” includes: the Governments of Australia, Belgium, Finland, Ireland, Italy, Luxembourg, Malaysia, New Zealand, Norway, Oman, Republic of Korea, Russian Federation, Switzerland, Saudi Arabia, the UnitedArab Emirates; Aventis , De Beers, Inter-American Development Bank, International Federation of Red Cross and Red Crescent Societies, Millennium Fund, Oil for Food Programme, OPEC Foundation, Smith KlineBiologicals , UNICEF National Committees, UNICEF Regular Resources, Saudi Arabian Red Crescent Society, United Arab Emirates Red Crescent Society, WHO Regular Budget and Wyeth.
Private Sector20%
Public Sector65%
Multilateral Sector15%
2004-2005 Funding Gapfor planned activities
US$ 130 million
USCDC
Polio financing
Funding Gap US$ 3 billion budget, 1988–2005*
* as at January 2004

Global Polio Eradication Initiative
� 22
All funding information is outlined in detail inthe Global Polio Eradication Initiative EstimatedExternal Financial Resource Requirements 2004-2008.
New fundraising initiativesRotary International polio eradication
fundraising campaignRotary International successfully concluded anextraordinary polio fundraising drive among itsmembership. The aim of the campaign was toraise US$ 80 million from 1.2 million Rotariansin 163 countries to help close the funding gap.Rotarians responded very generously once againand provided a truly remarkable amount of US$ 119 million. The results were announced atthe Rotary International Convention in Brisbane,Australia in June. Since 1985, RotaryInternational has contributed more than US$ 500 million to global polio eradication. Bythe time the world is certified polio-free, Rotary’scontributions will reach US$ 600 millon. Of evengreater significance has been the huge volunteerarmy mobilized by Rotary. Hundreds ofthousands of volunteers at the local level areproviding support at clinics or mobilizing theircommunities for immunization or polioeradication activites.
G8 Africa Action PlanAt the June 2003 G8 Summit in Evian, France,G8 leaders reiterated their commitment,originally expressed at the Summit in Kananaskis,Canada in 2002, to provide the necessary fundingto eradicate polio by 2005. As part of this pledge,France made a first-time commitment to the PolioEradication Initiative of US$ 35.5 million for2004–2006 and Russia committed US$ 4 millionfor 2003–2005.
Organization of the Islamic ConferenceAt the 10th Islamic Summit of the Organization ofthe Islamic Conference (OIC) in October 2003,OIC Member States adopted a landmark polioresolution that called on the internationalcommunity, OIC Member States, and Islamicphilanthropic institutions to provide financialassistance to eradicate polio. With the strong
support of the OIC Secretariat, polio partners arenow working to identify and engage all OICMember States, especially the Gulf CooperationCouncil countries.
World Bank/Gates Foundation/Rotary –United Nations Foundation Investment
Partnership for PolioThe World Bank joined forces with the Bill andMelinda Gates Foundation, Rotary Internationaland the United Nations Foundation (UNF) tocreate an innovative financing mechanism that hasprovided US$ 49 million to help fill the2003–2005 funding gap for OPV in Nigeria andin Pakistan. The collaboration sees the GatesFoundation and Rotary International/UNFbuying down to zero World Bank loans togovernments for OPV, in effect turning the loansto countries into grants. Vaccines are beingpurchased through UNICEF.
Donor supportAustralia
In 2003, Australia provided US$ 1.5 million inglobal funds to the Global Polio EradicationInitiative.
Aventis PasteurAventis Pasteur is the Global Polio EradicationInitiative’s longest standing corporate partner witha total donation of 110 million doses of OPV. The company committed an additional US$ 1.41 million in OPV to the Global PolioEradication Initiative.
Bill and Melinda Gates FoundationThe Foundation collaborated with Rotary International in a unique public/privatesector partnership along with the World Bank andthe UN Foundation, to provide OPV to Nigeriaand Pakistan. The Gates Foundation had previ-ously contributed US$ 50 million to the GlobalPolio Eradication Initiative.
CanadaIn 2003, Canada provided additional support ofUS$ 32.88 million in response to the G8’scommitment to provide the resources necessary to

23 �
Progress 2003
eradicate polio in Africa by 2005. Canadacontinues to be a strong supporter of the GlobalPolio Eradication Initiative and has contributed atotal of more than US$ 65 million to theprogramme.
US Centers for Disease Control andPrevention (CDC)
In addition to its role as a core technical spear-heading partner, CDC provided US$ 87.20 mil-lion for OPV, operational costs and programmesupport through its Atlanta-based headquarters.CDC supported the costs of more than 125 tech-nical personnel to assist WHO and UNICEF inglobal polio eradication efforts, laboratory sup-port to the 145 members of the global polio labo-ratory network, and scientific assistance on devel-oping products for the cessation of OPV.
DenmarkDenmark provided US$ 1.75 million to India’spolio eradication effort in 2003 as it concluded itssix-year US$ 30 million-plus commitment topolio eradication in India.
European Commission (EC)The EC provided US$ 39 million for polioeradication activities in Nigeria and in India.Funds were used for operational costs of NIDsand vaccine procurement.
FinlandFinland provided US$ 80,000 for the FinnishPolio Reference Laboratory.
FranceFrance, in support of the G8 commitment toprovide financial resources to eradicate polio,made a commitment of US$ 35.5 million to theGlobal Polio Eradication Initiative for 2004–2006activities in Africa.
GermanyGermany continued its commitment to theprogramme in India by providing US$ 8.8 millionfor OPV.
ItalyIn addition to a US$ 1 million contribution topolio eradication in India, Italy provided US$ 300 000 in global funding, as well assupporting activities in the Sudan and Somalia.
IrelandIreland provided US$ 900 000 in unspecifiedfunds for polio eradication.
JapanA key, major long-term donor to the programme,Japan contributed over US$ 30 million for OPV,cold chain and logistics in several countries in2003, bringing its total contribution to more thanUS$ 230 million. It also supported the polioeradication research agenda and containment andcertification activities.
The NetherlandsIn follow up to its US$ 110 million in globalcontributions in 2000–2001, the Netherlandsprovided support to the AFP surveillance systemin Bangladesh.
New ZealandNew Zealand provided US$ 1 million in globalfunds to the Global Polio Eradication Initiative,through Rotary, WHO and UNICEF.
NorwayNorway continued its strong support to the globalpolio eradication effort with a US$ 7 millionunspecified contribution in 2003.
Rotary InternationalRotary International, the largest private sectordonor to the Global Polio Eradication Initiative,continued its outstanding commitment byproviding US$ 25 million in 2003 to countries inall the remaining endemic regions, andconcluding a US$ 119 million fundraisingcampaign. Rotary International’s totalcontribution to the polio eradication effort since1985 has exceeded US$ 500 million, and willreach US$ 600 million when the world is certifiedpolio-free. Rotary International also joined forceswith the World Bank, the Bill and Melinda GatesFoundation, and the UN Foundation in aninnovative financing collaboration to help fill the2003–2005 funding gap for OPV in Nigeria andin Pakistan.

Global Polio Eradication Initiative
� 24
Russian FederationTo support the G8’s pledge to fund polioeradication, the Russian Federation committedUS$ 4 million over three years and provided thefirst instalment of US$ 1 million in 2003.
US Fund for UNICEF “Trick-or-Treat”campaign
The Trick-or-Treat for UNICEF campaignorganized by the US Fund for UNICEFcontributed US$ 3 million.
UNICEF National CommitteesIn 2003, the UNICEF National Committee inCanada provided US$ 50 000 for activities inHaiti.
United Arab EmiratesThrough the Red Crescent Society, the UAEprovided US$ 200 000 for polio eradicationactivities in Iraq.
United Kingdom’s Department ofInternational Development (DFID)
DFID continued its strong commitment with2003 funding of US$ 53.5 million. Funding wasprovided both at the global level, and bilaterally,to India, Nepal and Myanmar. The UK continuedto play a critical role in encouraging other donors,including the G8, to fulfil their commitment andprovide support to the Global Polio EradicationInitiative.
United Nations Foundation (UNF)The UN Foundation continued its criticalsupport to strengthen the Global PolioEradication Initiative’s fundraising capacity. It alsocollaborated with the Rotary International PrivateSector campaign, joined The World Bank/Gates/Rotary-UNF Investment Partnership forPolio.
The US Agency for InternationalDevelopment (USAID)
USAID continued its support for global polio eradication activities by providing US$ 27.5 million in 2003. USAID is the largestdonor to the Global Polio Laboratory Networkand supports the work of surveillance officers inAfrica and South Asia. It also supported vaccinedelivery in key countries, and helped raiseawareness to increase community-levelparticipation.
World Bank/Government of IndiaThe World Bank and the Government of Indiasigned a US$ 83 million credit agreement forpolio eradication activities in India.
Wyeth PharmaceuticalsThe pharmaceutical company Wyeth entered intothe second year of its second US$ 1 millioncommitment to the African Regional PolioLaboratory Network. ■

25 �
� � � � � �
��G8 pledges financial supportFollowing statements of support by G8 leaders atthe 2002 Summit in Kananaskis, Canada, G8leaders again re-affirmed their commitment to apolio-free world at the Summit in Evian, France,pledging to provide the necessary financialresources to eradicate polio from Africa. Canada,France, Japan, the Russian Federation, the UnitedKingdom and the United States are the G8countries which have so far followed through onthe collective pledge and provided funding.
��African Union adopts resolution toeradicate polio At the African Union Summit in Maputo,Mozambique in July, Member States unanimouslyadopted a resolution to do the necessary toeradicate polio and ensure that all African childrenare protected from the crippling disease forever.
��Organization of Islamic Conference(OIC) pledges to do the necessary to stop polio
With 5 of 6 remaining endemic countries beingMember States of the OIC, the importance ofinterrupting wild poliovirus transmission wasrecognized at the 10th Session of the IslamicSummit Conference in Malaysia in October,when Member States unanimously passed aresolution to eradicate polio from its MemberStates. 52 of the OIC’s 57 Member States arealready polio-free.
��Prince of Wales backs India’s fight againstpolio
On 31 October, HRH The Prince of Wales visiteda north Indian village to meet children beingimmunized against polio as part of the targetednational campaign to eradicate the disease by the end of 2004. The Prince’s visit to Kutail Gamriin Haryana state raised awareness ahead of crucialimmunization campaigns.
Advocacy
Phot
o: ©
Dr W
ong,
Prot
ocol
Divis
ion o
f the
Mini
stry
of Fo
reign
Affa
irs, M
alays
ia
Heads of State from 57 countries adopted the new resolution, which waspresented by the Government of Malaysia and other OIC Members, on thelast day of the 10th Session of the Islamic Summit Conference in Putrajaya,Malaysia.
Phot
o: ©
Kiro
n Pa
srich
a
Dr Jay Wenger, WHO, explains the benefits of using OPV to the Prince ofWales during a national immunization campaign in Kutail Gamri, India

Global Polio Eradication Initiative
� 26
��New WHO Director-General steps upglobal polio eradication effort
Immediately upon taking office, the new WHODirector-General Dr LEE Jong-wook announcedplans to rapidly step up the global effort toeradicate polio, calling it a “top priority”. “I wantto see this disease gone once and for all,” Dr Leesaid, as he announced an immediate upgrade ofWHO’s capacity to support the remainingendemic countries in their efforts to immunizeevery child against polio. Dr Lee’s office tookdirect oversight of polio eradication activities, andhe appointed Dr David Heymann – who led theteam which stopped the SARS outbreak – as hisRepresentative for Polio Eradication.
��Thousands of Rotary members volunteertime to protect children from polioRotary members worldwide continued tovolunteer their time and personal resourcestoward a polio-free world. Thousands of Rotaryclub members, including those that traveled fromthe United States, Canada, Europe and Australiato join their counterparts in India and West Africa, helped to immunize more than 200 million children against polio.
Rotary member Dave Groner from Michigan,USA, led a team of almost 200 volunteers fromthe United States and Canada to various cities inthe state of Uttar Pradesh, India. Groner said thatconnecting with the mothers of children receivingthe vaccine was a moving experience. “The look intheir eyes said the words ‘Thank you’. This
tremendously exhilarating experience has let meknow that my life is meaningful.” JonathanMajiyagbe, President of Rotary International andresident of Kano, Nigeria said: “The dedicationshown by Rotary members is not only inspiring,but it is also a fundamental component of ourfight against polio.”
��Pakistan President takes personaloversight of final push to eradicate polio inPakistan
Pakistan’s President General Pervez Musharrafannounced he would take personal oversight of
Phot
o: ©
JM G
iboux
, Rot
ary
Inter
natio
nal
Rotarian Dave Groner immunizes children in Uttar Pradesh, IndiaPhot
o: ©
WHO
/P.Vi
rot
Dr JW Lee, new Director-General and veteran of polio eradication activities
Phot
o: ©
WHO
/EMR
O
Regional Director WHO Regional Office for the Eastern Mediterranean, Dr Hussain A. Gezairy, called on President General Pervez Musharraf atRawalpindi on 12 September 2003

27 �
Progress 2003
the final push to eradicate polio from Pakistan, ata meeting with Dr Hussein A. Gezairy, RegionalDirector, WHO Regional Office for the EasternMediterranean. President Musharraf appealed togovernors, chief ministers, district Nazims andcivil servants across the country to ensure that thedisease is eradicated from Pakistan and that everychild is protected from polio once and for all.
��India’s biggest film star AmitabhBachchan fights polio as UNICEF GoodwillAmbassador
Amitabh Bachchan, India’s biggest film star, raisedcrucial awareness of polio eradication activities asUNICEF Goodwill Ambassador. Mr Bachchan hasa tremendous appeal to people from all walks oflife, and his support to polio eradication has beencritical to the strong progress achieved throughoutthe year. “India is closer than ever to eradicatingpolio,” Mr Bachchan said. “Let’s finish the job andrid our country of this terrible disease forever.”
��World-renowned photographer con-tinues to highlight global fight against polioSebastião Salgado, the globally-acclaimedphotographer, continued to advocate for a polio-free world throughout 2003. Salgado’sphotographs were featured in a number ofnewspapers and magazines, as well as in publicexhibits. Salgado also published The End of Polio:A Global Effort to End a Disease, an inspiring andpoignant chronicle of the global initiative toeradicate polio.
��Carol Bellamy, Executive Director,UNICEFIn 2003, UNICEF Executive Director CarolBellamy continued to make polio eradication apriority for UNICEF. Polio was the key topic ofher visits to endemic countries such as Nigeria andPakistan, where she participated in NIDs and metwith government representatives, religious leadersand traditional rulers to discuss the campaign’sprogress. During her keynote address to Heads ofState at the ECOWAS Summit in Ghana, sheemphasized the urgency of stopping the spread ofpolio across Africa. She also urged other globalleaders to become more actively involved in thefight to end polio, including Secretary-GeneralKofi Annan; the SG’s Special Adviser on Africa,Professor Ibrahim Gambari; and former Secretary-General Boutros Boutros Ghali.
��Strong start into 2004: Ministers ofhealth launch “final push” to eradicate poliowithin 12 months
At a high-level meeting at WHO in Geneva on 15 January 2004, ministers of health from theremaining endemic countries committed toeradicating polio by the end of 2004, and unveileda bold new plan to immunize 250 millionchildren multiple times during a series of massive,intensified polio immunization campaigns. Theministers publicly committed to do the necessaryto finish the job in 2004, by the signing of theGeneva Declaration for the Eradication ofPoliomyelitis. ■
Phot
o: ©
WHO
/P V
irot
Professor Eyitayo Lambo, Minister of Health, Nigeria, signs the GenevaDeclaration for the Eradication of Poliomyelitis
TV spots featuring Indian movie star Amitabh Bachchan helped raiseawareness of polio campaigns in India
� 28
� � �
The Future:Strategic Plan 2004–2008
A significant project in 2003 was thedevelopment of the new Global PolioEradication Initiative Strategic Plan 2004-
2008. The rationale for the development of thenew Strategic Plan was the tactical shift in 2003 tofocus resources on endemic and high-risk areas,the revised timeline for the target of globalcertification, and the increased knowledge base fordevelopment of polio vaccination policy followingglobal eradication.
The new Strategic Plan focuses on the followingfour objectives:
1. interruption of poliovirus transmission;2. achievement of certification of global
polio eradication;3. development of products for the cessation
of OPV; and4. mainstreaming of the Global
Polio Eradication Initiative.
The Global Polio Eradication Initiative StrategicPlan 2004–2008 replaces and updates theStrategic Plan 2001–2005, and therefore alsoreplaces the previous milestones, initially set outfor 2001 to 2005 (see following pages for themilestones of the new Strategic Plan, in relation toeach of the Plan’s 4 objectives). The greatest risk toachieving the annual milestones is ongoing wildpoliovirus transmission in any of the 6 remaining endemic countries, and an increasedfrequency of polio outbreaks due to vaccine-derived polioviruses.
Implementing the full activities of the StrategicPlan requires continued technical support from astrong polio eradication partnership, and ongoinggenerous financial support from the internationaldonor community. ■
*Available in electronic format on www.polioeradication.org, or by email [email protected] for printed copies.
**The Global Polio Eradication Initiative Estimated External Financial Resource Requirements 2004–2008 outlines the resources required to implement the fullactivities. This document is also available in electronic format on www.polioeradication.org, or by email [email protected] for printed copies.
Global Polio Eradication Initiative
S t ra t e g i c P l a n
2 0 0 4 – 2 0 0 8
WHO
Partners in the Global Polio Eradication Initiative
Global Polio EradicationInitiative
Estimated external financial resourcerequirements 2004-2008as of December 2003
WHOPartners in the Global Polio Eradication Initiative
Global Polio EradicationInitiative Strategic Plan2004–2008*
Estimated External FinancialResource Requirements 2004–2008**

29 �
Progress 2003
≤5
100%
30%
80%
85%
2 0 0 4
1*
100%
40%
90%
90%
2 0 0 5
0
100%
50%
100%
100%
2 0 0 6
0
NA
60%
100%
100%
2 0 0 7
0
NA
70%
100%
100%
2 0 0 8I n d i c a t o r s
Number of endemic countries
Percentage of planned SIAs
implemented in highest risk
polio-free areas
Percentage of countries
achieving GAVI targets for
DTP3/OPV3**
Percentage of emergency
mop-ups begun within 4
weeks of case confirmation
Percentage of non-certified
countries with certification-
standard surveillance
¸
O b j e c t i v e 1 : I n t e r r u p t P o l i o v i r u s T r a n s m i s s i o nI n d i c a t o r s a n d M i l e s t o n e s
G l o b a l P o l i o E r a d i c a t i o n I n i t i a t i v eS t r a t e g i c P l a n 2 0 0 4 – 2 0 0 8
O b j e c t i v e s a n d M i l e s t o n e s
* As of end-2003, one country is at particular risk of ongoing transmission into the first half of 2005.** Based on the rate of progress which would be required to achieve the GAVI target: by 2010 or sooner, all countries will have routine immunization coverage at90% nationally with at least 80% coverage in every district.
M i l e s t o n e s
85%
100%
50%(phase I)
NA
60%(regional
certification)
2 0 0 4
90%
100%
75%(phase I)
NA
70%(regional
certification)
2 0 0 5
100%
100%
100%(phase I)
NA
85%(regional
certification)
2 0 0 6
100%
100%
100%(phase II)
60%
100%(regional
certification)
2 0 0 7
100%
100%
100% (phase II+)
100%
100%(global
certification)
2 0 0 8I n d i c a t o r s
Percentage of non-certified
countries with certification-
standard surveillance
Percentage of AFP specimens
processed in a WHO-
accredited laboratory
Percentage of countries
completing each laboratory
biocontainment phase
Percentage of manufacturers
producing wild-type IPV under
BSL-3/polio
Percentage of countries
submitting “final” certification
documentation
O b j e c t i v e 2 : A c h i e v e C e r t i f i c a t i o n o f G l o b a l P o l i o E r a d i c a t i o nI n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s
Global Polio Eradication Initiative
� 30
Guidelines and
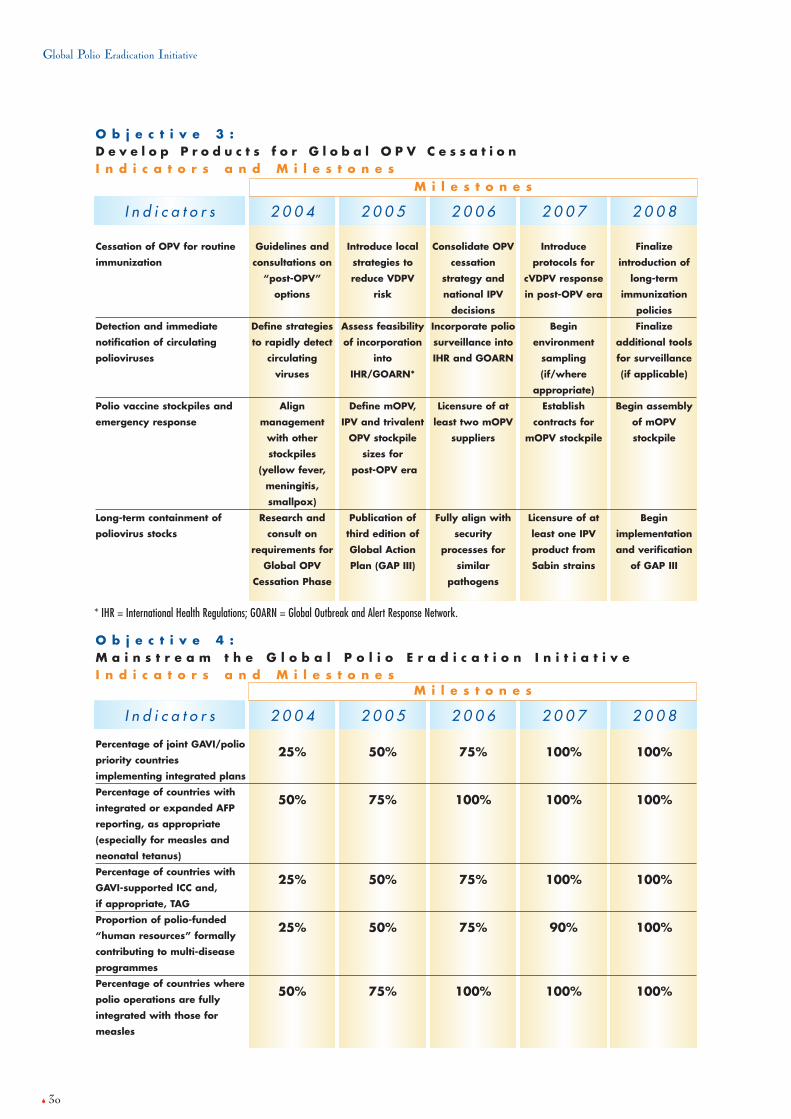
consultations on
“post-OPV”
options
Define strategies
to rapidly detect
circulating
viruses
Align
management
with other
stockpiles
(yellow fever,
meningitis,
smallpox)
Research and
consult on
requirements for
Global OPV
Cessation Phase
2 0 0 4
Introduce local
strategies to
reduce VDPV
risk
Assess feasibility
of incorporation
into
IHR/GOARN*
Define mOPV,
IPV and trivalent
OPV stockpile
sizes for
post-OPV era
Publication of
third edition of
Global Action
Plan (GAP III)
2 0 0 5
Consolidate OPV
cessation
strategy and
national IPV
decisions
Incorporate polio
surveillance into
IHR and GOARN
Licensure of at
least two mOPV
suppliers
Fully align with
security
processes for
similar
pathogens
2 0 0 6
Introduce
protocols for
cVDPV response
in post-OPV era
Begin
environment
sampling
(if/where
appropriate)
Establish
contracts for
mOPV stockpile
Licensure of at
least one IPV
product from
Sabin strains
2 0 0 7
Finalize
introduction of
long-term
immunization
policies
Finalize
additional tools
for surveillance
(if applicable)
Begin assembly
of mOPV
stockpile
Begin
implementation
and verification
of GAP III
2 0 0 8I n d i c a t o r s
Cessation of OPV for routine
immunization
Detection and immediate
notification of circulating
polioviruses
Polio vaccine stockpiles and
emergency response
Long-term containment of
poliovirus stocks
* IHR = International Health Regulations; GOARN = Global Outbreak and Alert Response Network.
O b j e c t i v e 3 : D e v e l o p P r o d u c t s f o r G l o b a l O P V C e s s a t i o nI n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s
25%
50%
25%
25%
50%
2 0 0 4
50%
75%
50%
50%
75%
2 0 0 5
75%
100%
75%
75%
100%
2 0 0 6
100%
100%
100%
90%
100%
2 0 0 7
100%
100%
100%
100%
100%
2 0 0 8I n d i c a t o r s
O b j e c t i v e 4 : M a i n s t r e a m t h e G l o b a l P o l i o E r a d i c a t i o n I n i t i a t i v e I n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s
Percentage of joint GAVI/polio
priority countries
implementing integrated plans
Percentage of countries with
integrated or expanded AFP
reporting, as appropriate
(especially for measles and
neonatal tetanus)
Percentage of countries with
GAVI-supported ICC and,
if appropriate, TAG
Proportion of polio-funded
“human resources” formally
contributing to multi-disease
programmes
Percentage of countries where
polio operations are fully
integrated with those for
measles

31 �
Progress 2003
AFP acute flaccid paralysisAFR WHO African RegionAMR WHO Region of the AmericasCDC US Centers for Disease Control and Prevention (USA)DFID Department for International Development (United Kingdom)EC European CommissionEMR WHO Eastern Mediterranean RegionEUR WHO European RegionEPI Expanded Programme on ImmunizationGAVI Global Alliance for Vaccines and ImmunizationGCC Global Commission for the Certification of the Eradication of PoliomyelitisICCs Interagency Coordinating CommitteesIPV inactivated polio vaccinemOPV monovalent OPVNCCs National Certification CommitteesNIDs National Immunization DaysOIC Organization of the Islamic ConferenceOPV oral polio vaccineRCCs Regional Certification CommissionsSEAR WHO South-East Asia RegionSIAs Supplementary Immunization ActivitiesSNIDs Subnational Immunization DaysTCG Technical Consultative Group for the Global Eradication of PoliomyelitisUN United NationsUNF United Nations FoundationUNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentVDPVs vaccine-derived poliovirusesWHO World Health OrganizationWPR WHO Western Pacific Region
Abbreviations and acronyms






























