Embed Size (px)
Citation preview
Dr Teh-Kuang Sun
Section of cardiology
Puli Christian Hospital
Taiwan
Patient’s profile
Mr Wu , 48 y/o male
Past Hx :
HTN since age of 30, irregular compliance to medical control
Obesity ( BH 152 cm, BW 68kg, BMI 27.2)
Heavy smoker ( 1-2 ppd) since age of 18
Hepatitis B
PUD
FH : father HTN / IHD, mother HTN
Present illness
On the day of admission, angina since 7:00
AM, associated symptoms are diaphoresis,
nauceas and dyspnea.
At arrival to ER:
Intermittent bradycardia ( HR 35-50 bpm),
hypotension ( SBP around 70-100 mmHg)
ECG: limb leads II III AVF ST elevation.
inferior wall STEMI impressed.
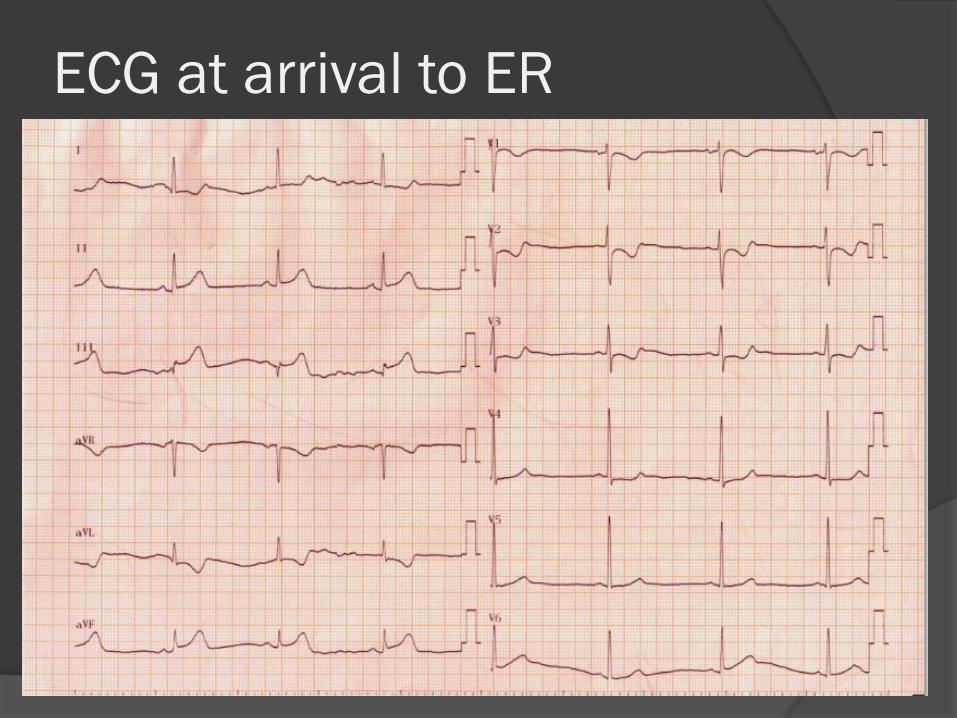
ECG at arrival to ER
Primary PCI
Pre-medications at ER :
Heparin sulfate 4000 u, iv stat.
Aspirin 300 mg and clopidogrel 300 mg, po
stat.
Morphine 3 mg, iv , for pain control
O2 by nasal prong, 2-3 l/min
IV fluid: normal saline 100 ml/hour
At cath-lab:
For bradycardia: Temporary pacemaker ,
via right femoral vein
Additional Heparin sulfate 3000 u, iv stat,
immediately prior to initiate PCI, to keep
ACT > 250 sec.
Patient had vomited once in cathroom.
Metoclopramide HCL 10 mg iv st was
given
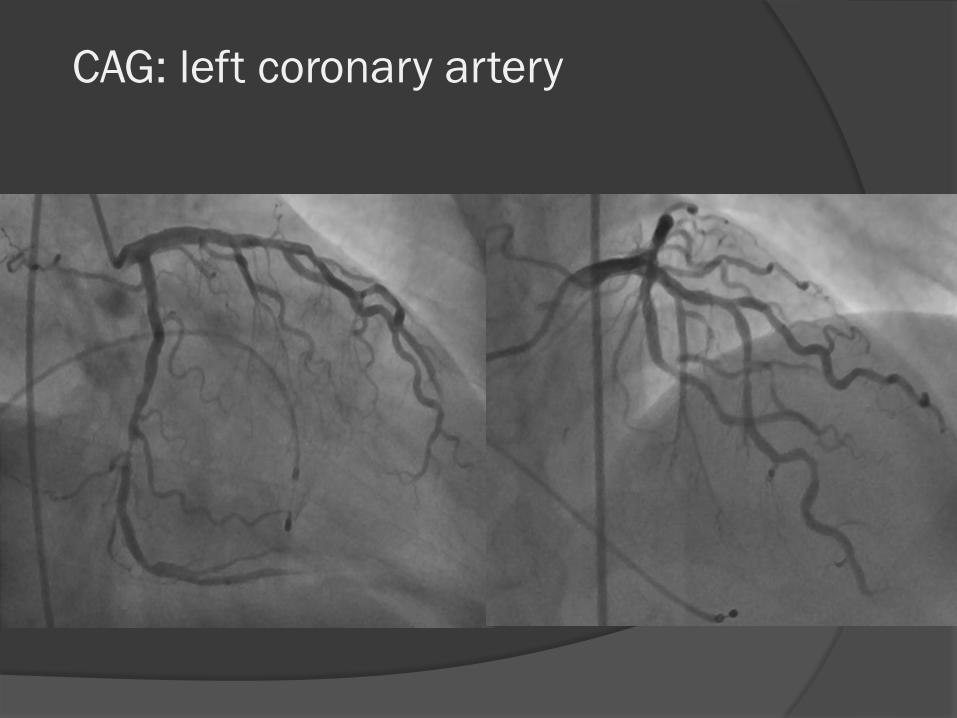
CAG: left coronary artery
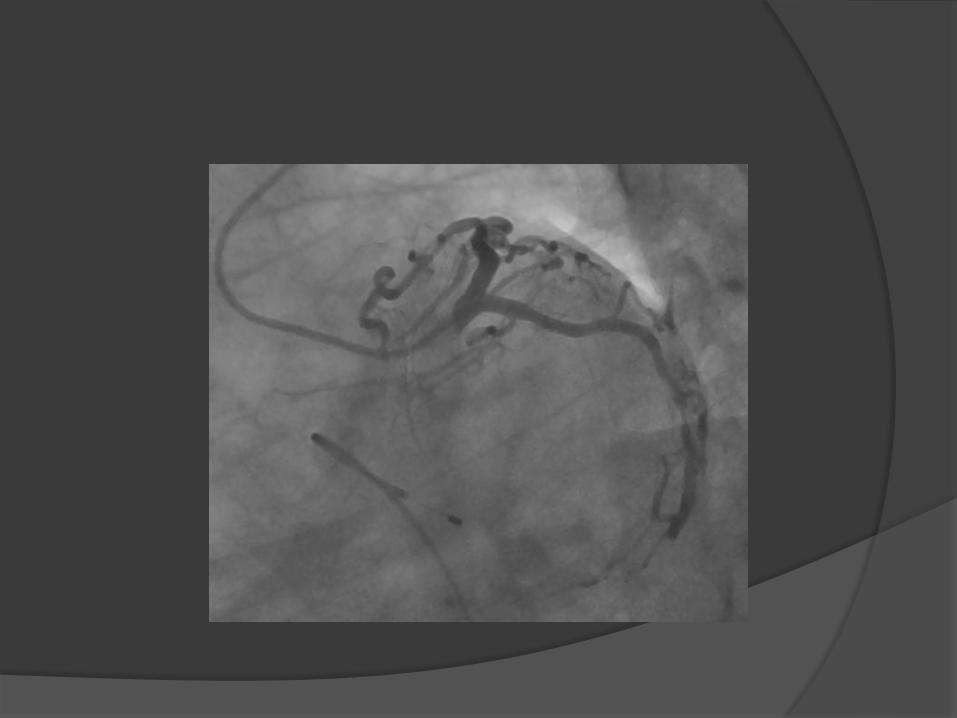
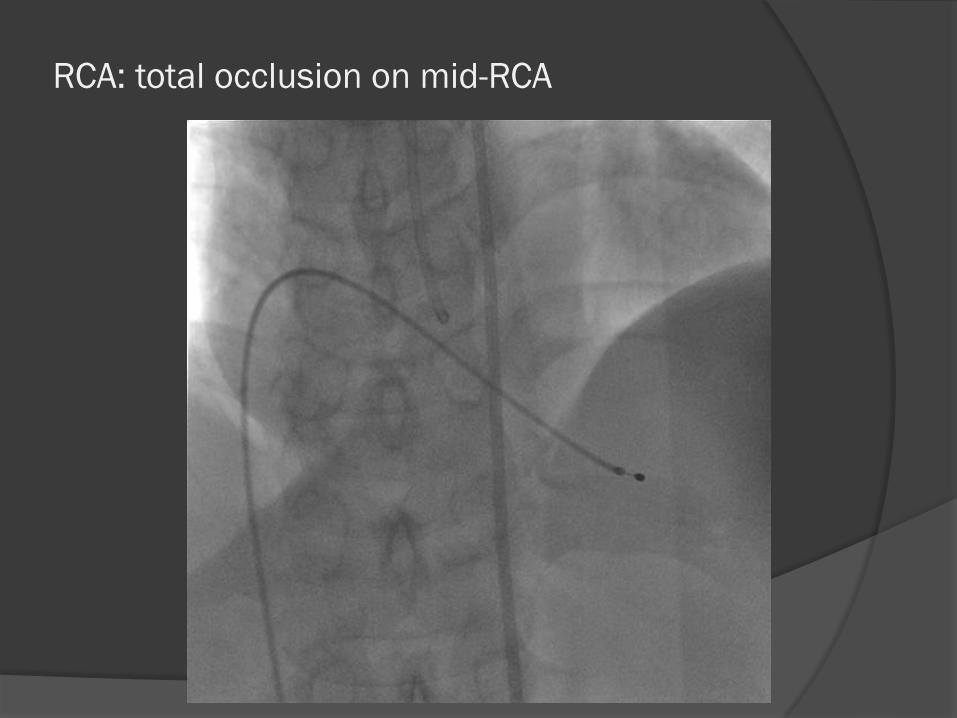
RCA: total occlusion on mid-RCA
Target lesion: mid-RCA total occlusion
Catheter: 7Fr, JR 4.0
PTCA wire: 0.014 Fielder FC wire
PTCA balloon: Terumo Ryujin 2.75x15
mm
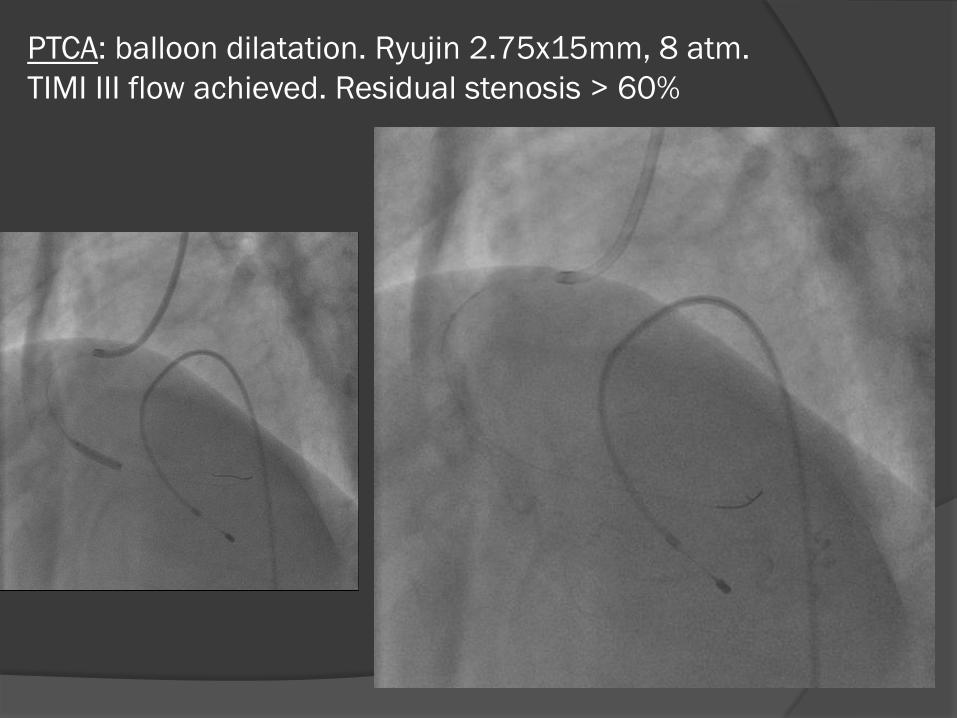
PTCA: balloon dilatation. Ryujin 2.75x15mm, 8 atm.
TIMI III flow achieved. Residual stenosis > 60%
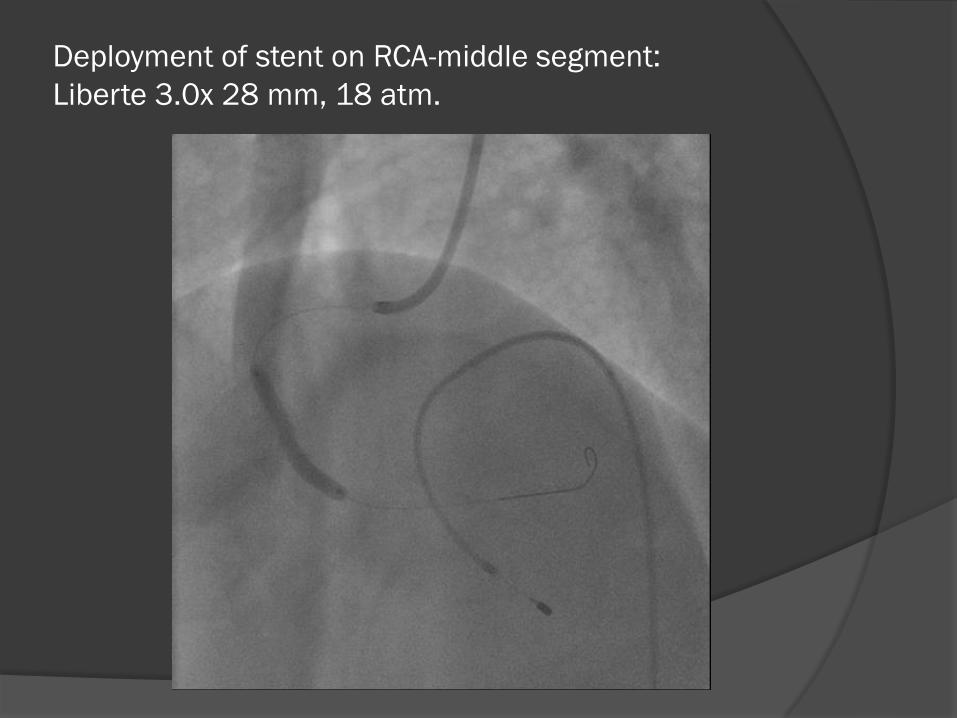
Deployment of stent on RCA-middle segment:
Liberte 3.0x 28 mm, 18 atm.
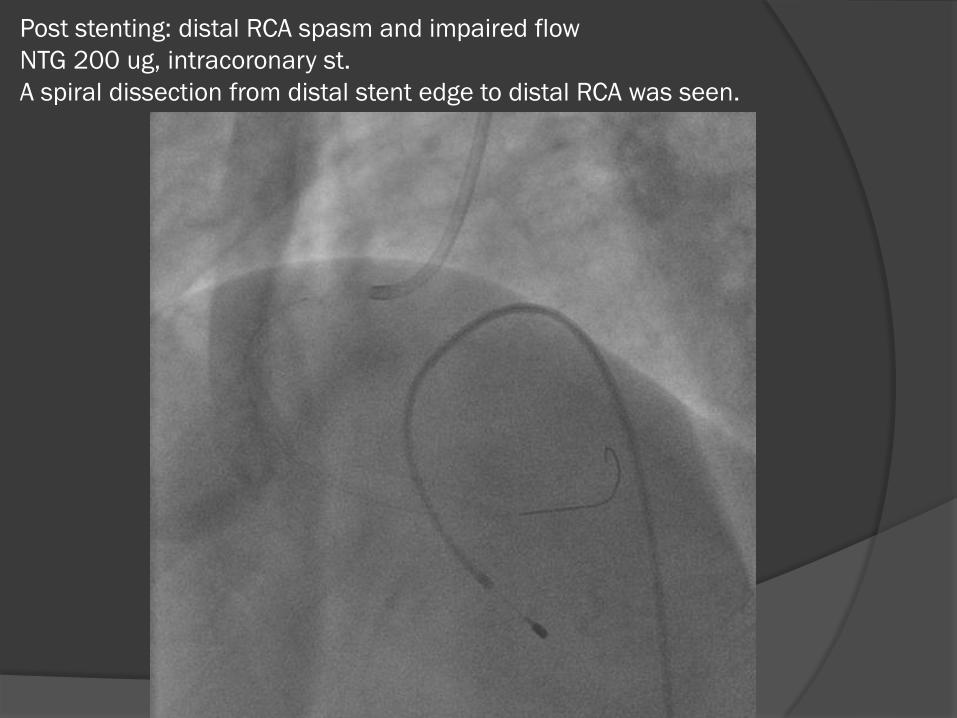
Post stenting: distal RCA spasm and impaired flow
NTG 200 ug, intracoronary st.
A spiral dissection from distal stent edge to distal RCA was seen.
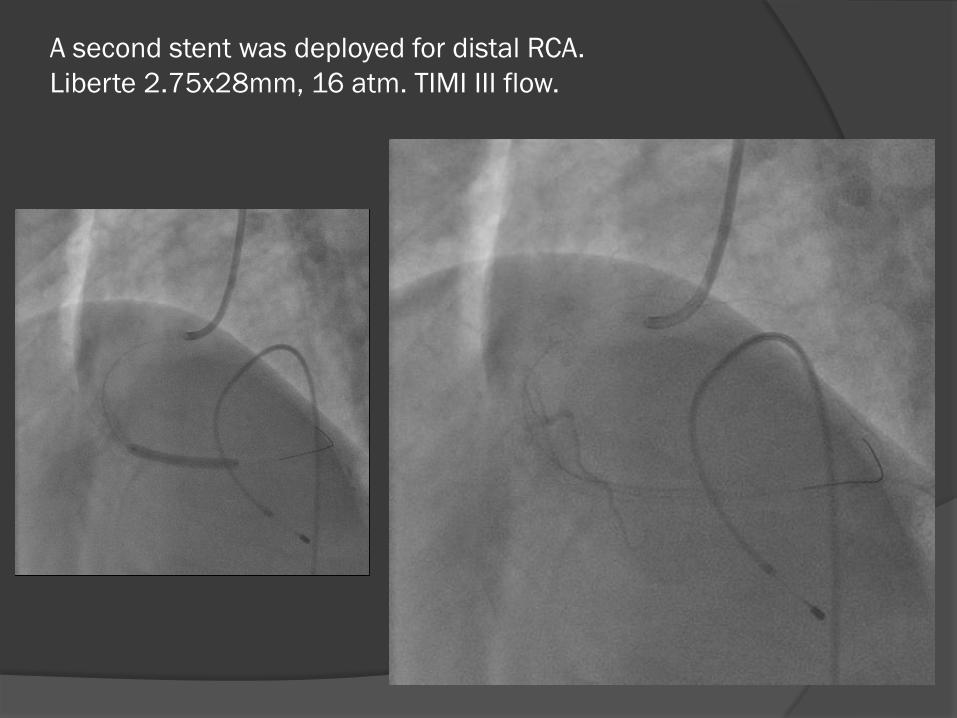
A second stent was deployed for distal RCA.
Liberte 2.75x28mm, 16 atm. TIMI III flow.
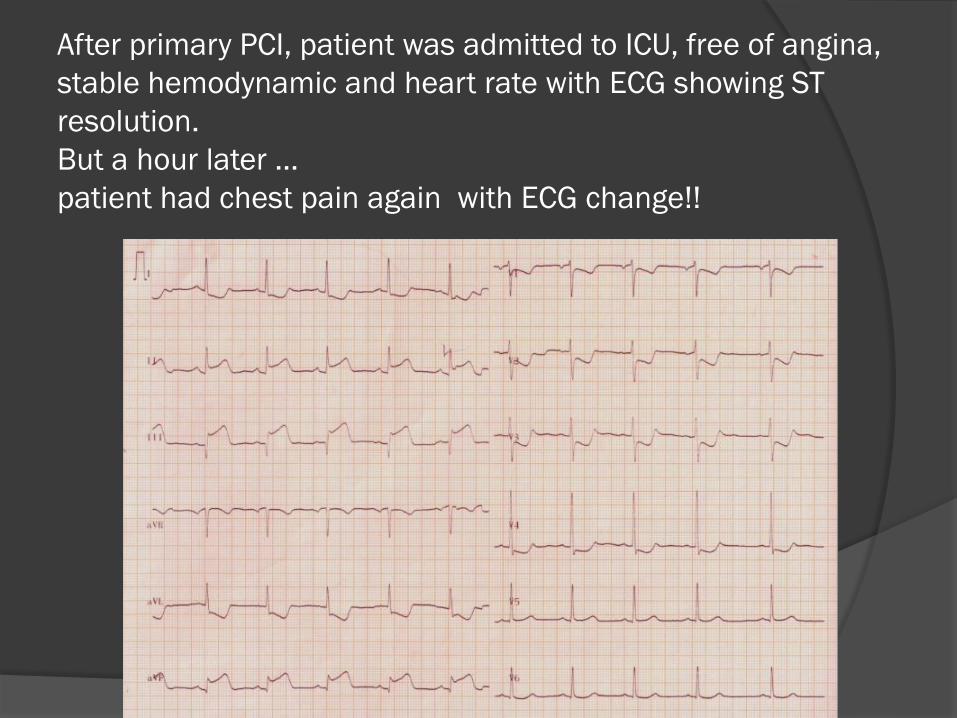
After primary PCI, patient was admitted to ICU, free of angina,
stable hemodynamic and heart rate with ECG showing ST
resolution.
But a hour later …
patient had chest pain again with ECG change!!
A glycoprotein IIbIIIa ( GP IIbIIIa)
antagonist Tirofiban intravenous loading
infusion and then continue infusion was
started , in addition to Heparin sulfate iv
infusion.
Morphine 3 mg iv for pain control
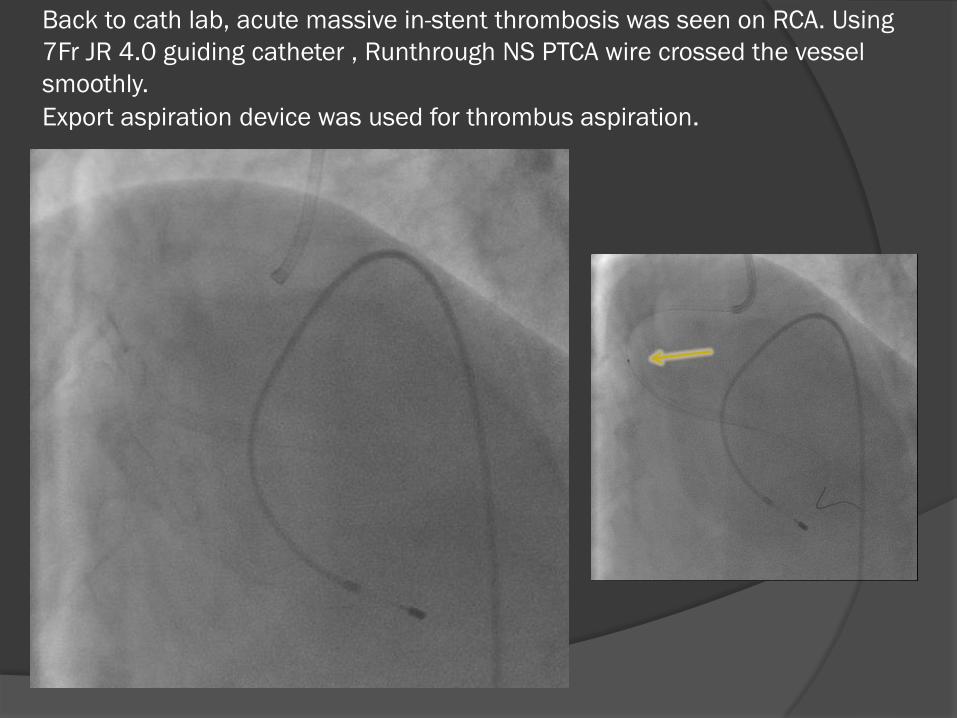
Back to cath lab, acute massive in-stent thrombosis was seen on RCA. Using
7Fr JR 4.0 guiding catheter , Runthrough NS PTCA wire crossed the vessel
smoothly.
Export aspiration device was used for thrombus aspiration.
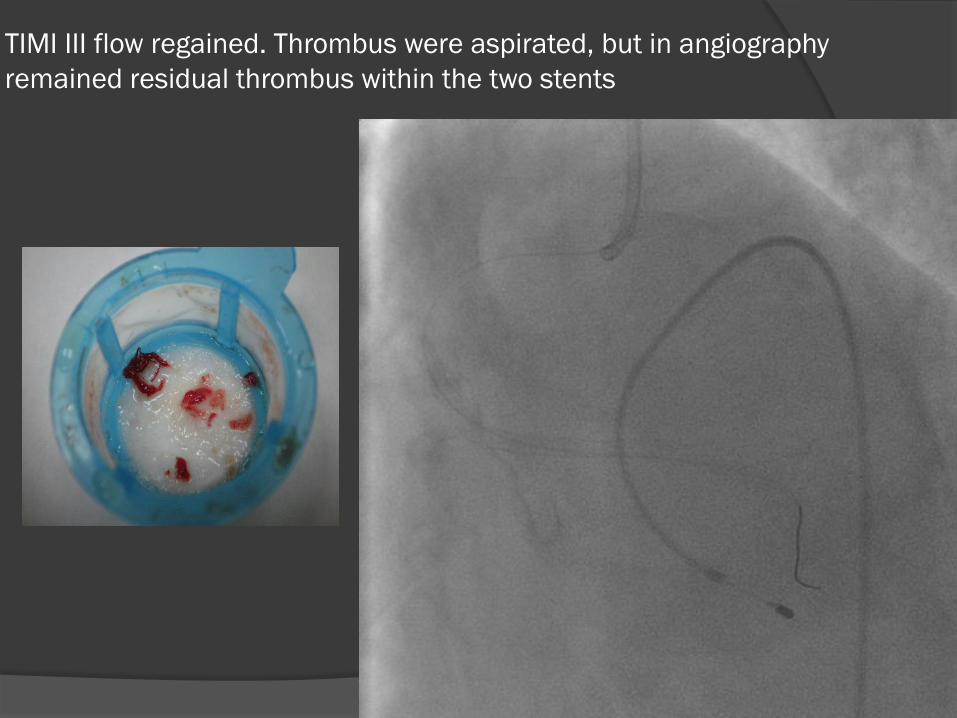
TIMI III flow regained. Thrombus were aspirated, but in angiography
remained residual thrombus within the two stents
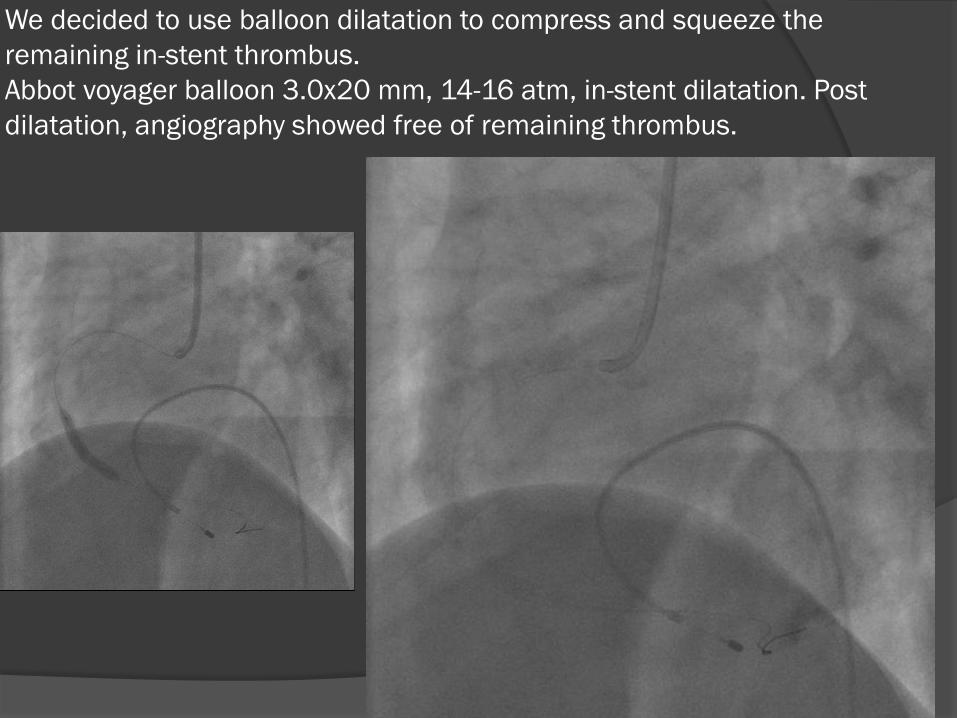
We decided to use balloon dilatation to compress and squeeze the
remaining in-stent thrombus.
Abbot voyager balloon 3.0x20 mm, 14-16 atm, in-stent dilatation. Post
dilatation, angiography showed free of remaining thrombus.
Lessons to learn from this experience …
Post stenting distal vessel spiral dissection.
Maintain the wire across the lesion
If the dissection is long and the flow is
impaired, with vessel diameter > 2.5mm, the
lesion should be stented promptly in its full
length.
If the stent edge dissection is minor, with
residual lumen > 50%, without impairment of
flow, there’s no need of further treatment.
Anticoagulation during PCI
Loading dose of oral aspirin with either clopidogrel or GP IIb IIIa antagonist are indicated ( class I indication)
Use unfractionated heparin ( Class I indication)
This patient had vomited … is this the reason that full antiplatelet effect had not achieved, after the oral loading dose of dual antiplateletdrugs?
It’s reasonable to start GP IIbIIIa antagonist ( tirofiban / eptifibatide) at time of primary PCI in selected patient ( Class IIa indication).
Management of acute in-stent thrombosis
Remember the risk factors for acute thrombosis are:
undersized stent, dissection, TIMI flow post MI, CAD > 50% stenosis proximal to the culprit lesion, malignancy, no aspirin at time of PCI, and LVEF< 30%.
Emergency PCI is the treatment of choice, back to cath-lab as soon as posible, the strategy is same as used in STEMI.
Thrombus aspiration device is a useful
tool.
Concomitant antiplatelet medication with
use of glycoprotein IIbIIIa antagonist is
indicated by the present guidelines ( II
a ).
Full anticoagulation is essential.
What to do if you have done all above and still remain
some residual thrombus?
May consider use of balloon dilatation to
compress and squeeze residual thrombus
against the deployed stent and vessel wall.
But… It’s a dangerous move!
It only can be done if most of the thrombus
are removed by thrombus aspiration device
or distal protection devices like GuardWire,
and no remaining thrombus are are seen on
bifurcations / nearby branches





























