Embed Size (px)
Citation preview

From PHR to NHR? An UCD challenge
Giampaolo Armellin, Dario Betti, Stefano Bussolon,
Annamaria Chiasera, Manuela Corradi, Jovan Stevovic
Personal Health Records and patient-oriented infrastructures

Declaratio terminorum (1)
2
Dictionary by By jwyg on http://www.flickr.com/photos/jwyg/3745559121/

Declaratio terminorum (2)
3
Personal Health Records vs. Electronic Medicals vs. Electronic Health Records
Dictionary by By jwyg on http://www.flickr.com/photos/jwyg/3745559121/
Infrastructures for interoperability
4
Regional/national/international-wide infrastructures to enable data exchange and sharing among EMRs and EHRs.
Beyond the boundaries
5
putting into action eHealth interoperability
Border-USA-Mexico by By `David on http://www.flickr.com/photos/david_ludwig/386317095/

What's about PHRs?
6
Can we name them NHRs (Networked Health Records)?
Could be NHR the european way to UHRs (Universal Health Records)?
Border-USA-Mexico by By `David on http://www.flickr.com/photos/david_ludwig/386317095/
Who uses it? What is its relationship to EHRs? What is thetechnical architecture to connect PHRs? What strategies canbe employed to overcome the technical, societal, and organi-zational barriers that impede dissemination and use of PHRs?This paper summarizes the discussions that occurred at thesymposium.
Definitions and Characteristics of a PersonalHealth RecordThe Markle Foundation’s Connecting for Health collabora-tive, a public-private endeavor working toward an interoper-able health information infrastructures defined PHR in theirreport on the subject as:
‘‘An electronic application through which individuals canaccess, manage and share their health information, and thatof others for whom they are authorized, in a private, secure,and confidential environment.’’2
Although this definition represents a good starting point,more clarity is necessary to understand how PHRs mightfunction to benefit individuals, their caregivers, and theirhealth care providers.
A PHR includes health information managed by the individ-ual. (Often the term patient is used when referring to stake-holders of PHRs, but we prefer to use the term individual toemphasize that the PHR is a tool that can be helpful in main-taining health and wellness as well as a tool to help withillness that the term patient implies.)
This can be contrasted with the clinician’s record of patientencounter–related information (a paperchart or EHR, alsoknown as an electronic medical record or the computer-basedpatient record), which is managed by the clinician and/orhealth care institution. Over time, we envision an environ-ment in which health information about an individual canflow seamlessly among systems used by authorized healthprofessionals, caregivers, and the patient, when the patientauthorizes such sharing.
There are several possible approaches to creating a functionalPHR (Fig. 1).3 In the first approach, an individual may createhis or her PHR using commercially available applications,ranging from stand-alone systems to Web-based applications.The patient can enter and access his or her health data throughsuch systems. In its simplest form, the PHR is a stand-alone ap-plication that does not connect with any other system. At theother end of the spectrum, PHR functionality can be providedby allowing patients to view their own health information thatis stored in their health care provider’s EHR. The EHR-based
systems may include additional functionality, such as allow-ing the patient to request appointments and prescriptionrenewals and providing a communication channel toclinicians.4–7 In some cases, patientsmay add supplemental in-formation that may or may not subsequently be incorporatedinto the provider’s EHR. Although there are not good dataavailable that quantify current use of PHR systems, we believethat themajority of consumers using a PHR today use one thatis integrated with the provider’s EHR in some way. Somehybrid PHR systems can connect to various health care datasources to acquire and transmit data. This latter approachovercomes the limitations that result from using a PHR inte-grated in a single health care provider or organization, but ismuch more complex. Figure 1 illustrates the spectrum ofPHR models. As part of the symposium agenda, the Collegeconducted a formal debate to discuss the relative advantagesand disadvantages of each model.
In the discussions following the debate, symposium at-tendees considered the merits of stand-alone PHRs, includingthose supplied on ‘‘smart cards,’’ USB drives, and CDs.Although the stand-alone nature of such devices providesmore individual control over access to the data contained inthe PHR, the attendees were concerned that, except for themost highly motivated, it is unlikely that individuals wouldkeep records in a stand-alone PHR up to date. In addition,it is unlikely that a stand-alone PHR that depends solely onpatient input can act as a trusted conduit for transmissionof medical record data among clinician offices or health careinstitutions. A PHR system must serve as more than a repos-itory for an individual’s health information. While patient-entered segments are desirable for some information andonly patients can provide some types of health data, cliniciansmust also have access to their own past considerations and in-terpretations, as well as reliable objective data, if they are todepend on records for clinical decision making. The reliabilityof patient-entered data depends on the nature of the informa-tion per se, the patient’s general and health literacy, and thespecific motivations for recording the data. For example,patient reports are usually reliable for symptoms and easy-to-measure objective parameters, such as height, weight,and temperature by thermometer. However, most patientscannot reliably report specific laboratory values such as theirspecific cholesterol level or hemoglobin A1c.8
Although there are specific advantages for each type of PHR,symposium participants concluded that PHRs integratedwith EHRs, either through tethering or interconnectivity, pro-vide much greater benefits than stand-alone PHRs. The inte-grated PHR-EHR approach can convey much more relevantdata to the patient. In addition, because EHRs generally areequippedwithmore robust backup systems, in a natural disas-ter such as that experienced during Hurricane Katrina, it ismore likely that patient data in PHR-EHR systems will sur-vive. The ability of the Veteran’s Health Administration torestore patient data within days illustrates this benefit. Inaddition, the business case for such integrated systems is easierto make (see discussion below). The remainder of this paperconsiders the integrated PHR model as the preferred model.
Data SourcesIdeally, the PHR should include as much relevant data aspossible over the individual’s lifetime, from multiple sources,including health care facilities as well as the individual. The
F i g u r e 1 . Range of complexity in various approaches topersonal health records (PHRs).
122 TANG ET AL., PHRs: Definition to Adoption Strategies
group.bmj.com on December 9, 2011 - Published by jamia.bmj.comDownloaded from
from: Tang PC, Ash JS, Bates DW, Overhage JM, Sands DZ. Personal health records: definitions, benefits, and strategies for overcoming barriers to adoption. J Am Med Inform Assoc.2006

At least two big issues
7
- the semantic gap on the data flowing from EMRs and EHRs into NHRs - the privacy control on the data flowing from PHRs into NHRs
Flow by By Yogendra174 on http://www.flickr.com/photos/yogendra174/5980718184

8
How to address?
It is necessary to involve the citizens- patients in designing the modalities in which their PHRs merge in the NHRs.

The semantic gap
9
“Both terminology and data presentation must be adapted to the individual using the PHR, so that they realize optimal benefits". (Tang et al., 2006)
The New York Times on the New Art of Flick by By Thomas Hawk on http://www.flickr.com/photos/thomashawk/2442371176/

The semantic gap: the terminology issue/1
10
Many relevant works have been done on the problem of the linguistic gap between consumer-oriented vocabularies and specialized medical terminologies
(Soergel et al., 2004, Zeng et al. 2006, Rosembloom et al., Keselman et al., 2007) by machine-automated analysis and mapping.

The semantic gap: the terminology issue/2
11
The hybrid approach: machine-automated tools plus the direct involvement of lay people (Cardillo et al., 2009, 2010)
The semantic gap: the data presentation issue/1
12
To avoid information overload, patients need individualized view on their health data. (Knaup␣et al., 2007)

The semantic gap: the data presentation issue/2
13
Which data are relevant to patients?
How to organize them?

The semantic gap: the Trentino case study
14
Event oriented architecture (EDA) is an architectural pattern widely used in the design of the interoperability infrastructures in the healthcare domain
(National Institutes of Health, 2006).

The semantic gap: the Trentino case study
15

The semantic gap: beyond linguistic mapping
16
yellow crowd by twose on http://www.flickr.com/photos/twose/887903401/
Which events are relevant to patients?
Which data should these events delivery to PHRs?

The privacy control
17
Safe by rpongsaj on http://www.flickr.com/photos/pong/288491653/

Different privacy regulations
18
Safe by rpongsaj on http://www.flickr.com/photos/pong/288491653/
The patient under European Data Protection Directives
The data producers under HIPAA
Who is the data owner?

Our previous work: data filtering rules
19
A purpose-based access control with sub-document level granularity
To specify which documents and which parts can be used for which purposes
To allow organizations to gain complete control over data sharing
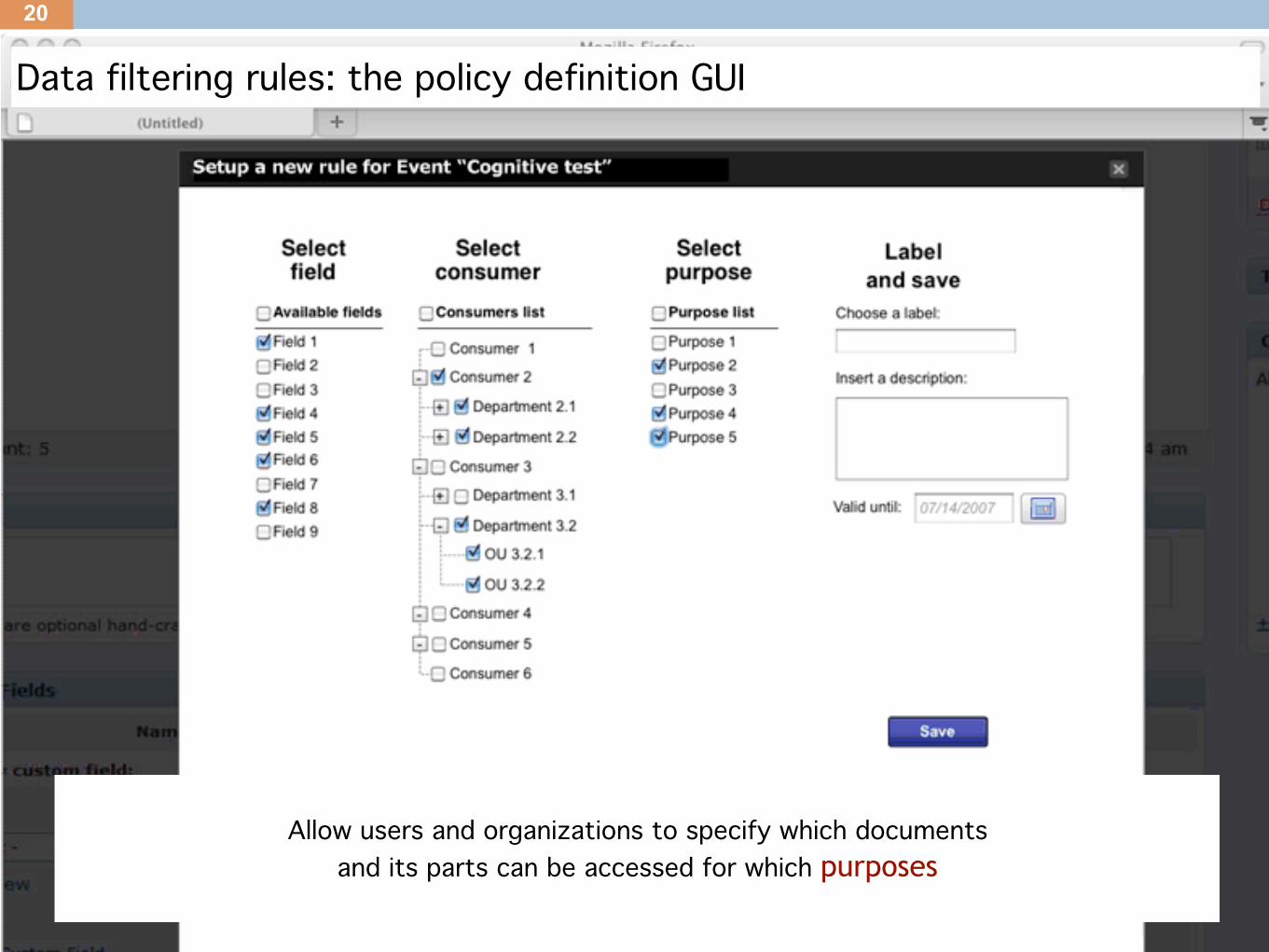
Data filtering rules: the policy definition GUI
20
Allow users and organizations to specify which documents and its parts can be accessed for which purposes

Different regulations
21
Which are the patient rights under each different regulation?

Patient vs. Organization produced data
22
How to provide GUIs that allow flexible policy definition?
Patients have different rights on different records

Crossing country boundaries
23
How to share data across organizations belonging to different regulations?
US-EU Safe Harbor privacy principle
By DeusXFloridam on http://farm3.staticflickr.com/2430/3976943870_8f3a033bd0_b.jpg

Lessons learned
24
Crucial role of citizens/patients to successfully create an NHR: beyond linguistic mapping, towards process mapping
Methodology for tight and incremental control on the access and dissemination of sensitive information
A purpose-based access control mechanism that is suitable for data sharing in health care

Future work
25
On-field experimentation of UCD techniques in a real example of evolution of a PHR in NHR for an empirical evaluation of the effectiveness of the patients involvement
Analysis of different regulations and requirements
Design flexible user interfaces to satisfy mentioned problems

Questions?
{garmellin, dbetti, achiasera, mcorradi, jstevovic}@cr-gpi.it
Thanks!




![NHR-7 NHR-7B › files › pam › pam_nhr7.pdfI I NHR-15 NHR-11 NHR-15B 00175-000236 00175-000180 p ; 00175-000237 p ; p ; ¢ ] k£ ¢ ] k£ ¢ ] k£ O 37.8 kg O 39.1 kg O 28.0 kg](https://img.dokumen.tips/doc/110x75/5f18eb357c52714c15267512/nhr-7-nhr-7b-a-files-a-pam-a-pamnhr7pdf-i-i-nhr-15-nhr-11-nhr-15b-00175-000236.jpg)
























