Embed Size (px)
Citation preview

D R V I S H W A N A T H H E S A R U R
J N M C , B E L G A U M
TRUNCUS ARTERIOSUS

FORMATION OF CONOTRUNCAL SEPTUM


Single outflow tract from the heart• Improper formation of truncal ridges & aorticopulmonary
septum such that aorta & pulmonary trunk are not fully divided• 1-2% of all CHDs

DEFECT OF CONOTRUNCAL SEPTATION

TRUNCUS ARTERIOSUS
Truncus arteriosus is one of the least common cynotic
congenital heart disease.
1-2.5 % in all CHD.
Frequently syndromic as 22q 11 deletion syndrome.
DiGeorge’s syndrome.

DiGeorge’s syndrome

Definition
It is congenital cardiac malformation in which one great
artery arises from the base of the heart by a way of single
semilunar valve (truncal valve),it gives origin to systemic
arteries,coronary arteries and pulmonary arteries.
History – Wilson – 1st described in 1798.
Buchanan – clinical and autopsy reports in 1864.
Collett and Edwards –classification in 1949.
Van praagh- alternative classification in 1965.
McGoon – 1st repair with homograft in 1967.

Echocardiography
It starts with situs –visceral situs ,atrial situs
Atrioventricular concordance.
Two balanced ventricles are usually present & separated by large VSD.
Very rare form with discordant atrioventricular connection.
Truncal valve continuity with the anterior leaflet of mitral valve.



Truncal valve
It is best seen in parasternal short axis view.
It can be tricuspid – 60-67 %.
Quadricuspid – 25- 31%
Bicuspid – 8%
Pentacuspid -0.3%
Valve leaflet can be normal or may be stenotic or
regurgitant.

Truncal valve

Classification of truncus arteriosus
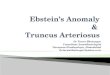
I) Edward & Collett classification-
Type I – main pulmonary trunk arises from truncus
arteriosus and gives rise to RPA & LPA.
Type II- RPA & LPA arteries arises directly and lying
close to one another.
Type III- RPA & LPA arises from separate ostium lying at
some distance from one another.
Type IV-absence of branch of PA ,pulmonary blood flow
is derived from aortopulmonary collaterals.

EDWARD AND COLLETT CLASSIFICATION-1949

Van praagh classification-1965
Type A1-corresponds to type I of collett & Edward.
Type A2- corresponds to Type II and Type III of collett &
Edward.
Type A3-Absence of truncus origin of one of the
pulmonary Artery.
Type A4- Hypoplasia of Aorta.


Differential diagnosis
A)Pulmonary atresia-pulmonary ateries are small with
continues flow being seen in branch PA either from PDA
or collateral flow.
B) very rarely this large great vessel may be PA in
patient’s of aortic atresia.(Imp – identify Aorta).
C) anomalous origin of RPA from posterior aspect of
aorta.

2D-Parastenal long axis view
Common arterial trunk arising predominantly from LV –
4-6%
Truncus arteriosus with biventricular origin – 69%
Right ventricular origin – 11 – 29 %
Truncal override –
It is discontinuity between IVS and anterior truncal wall.


Large ventricular septal defect
In truncus arteriosus large VSD is commonly seen.
It developes due to absence or deficiency of infundibular
septum.
Restrictive VSD or no VSD is very rare.


Short MPA with RPA & LPA arising frm left lateral aspect of TR
NO MPA –direct RPA & LPA arising from posterior aspect of TR
Parasternal short axis view

Apical view


Suprasternal long axis view

Regurgitant truncal valve
Causes-
1) Thickening , dysplastic cusps.
2) Prolapsed cusps.
3) unequal cusps.
4) truncal root dilation.

Stenotic truncal valve
By using colour and continues doppler gradient across
pulmonary arteries and stenotic truncal valve can be
recorded.
Stenosis and regurgitant gradient is frequently
overestimated across truncal valve bz both the ventricular
output has to pass across it.
Gradient up to 40 – 50 mmHg have been documented.
Significant stenosis of origin of branch of pulmonary
artery is the presence of diastolic spill on doppler.


Coronary artery anomalies

Associated anomalies
Right aortic arch- 25 to 35 %
Coarction of aorta.-10 to 15 %
Patent ductus arteriosus-10%
Interrupted aortic arch- 10 to 15 %
Ostium secundum ASD-10 %
Left SVC draining into coronary sinus- 10%
TAPVC / PAPVC

Surgical correction