Embed Size (px)
Citation preview

Revolutionizing the Fight
Against Cancers and
Infectious Diseases
Dr. J. Joseph KimPRESIDENT & CEO NASDAQ: INO
It’s All About the T-Cells
Forward Looking Statement
Our commentary and responses to your questions may containforward-looking statements, including comments concerningclinical trials and product development programs, evaluation ofpotential opportunities, the level of corporate expenditures,the assessment of Inovio’s technology by potential corporatepartners, capital market conditions, timing of events, cashconsumption and other subjects. Information concerningfactors that could cause actual results to differ materially fromthose set forth in our Annual Report on Form 10-K for the yearended December 31, 2014, our Form 10-Q for the quarterended June 30, 2015, and other regulatory filings from time totime.
2
3
Licensing agreement and R&D collaboration • MedImmune acquired the rights to INO-3112
• Inovio retains the rights to VGX-3100• INO-3112 will be evaluated in combination with immune-oncology
molecules• Joint research on two additional DNA-based cancer vaccine products not in
Inovio’s pipeline
Financial Terms:• Upfront payment of $27.5 million• Development and commercial milestone payments amounting to $700
million• Up to double-digit tiered royalties on INO-3112 product sales• MedImmune will pay all developments costs
Further validation of the potential of Inovio’s DNA immunotherapies to fight cancer
Validating Partnership with MedImmune
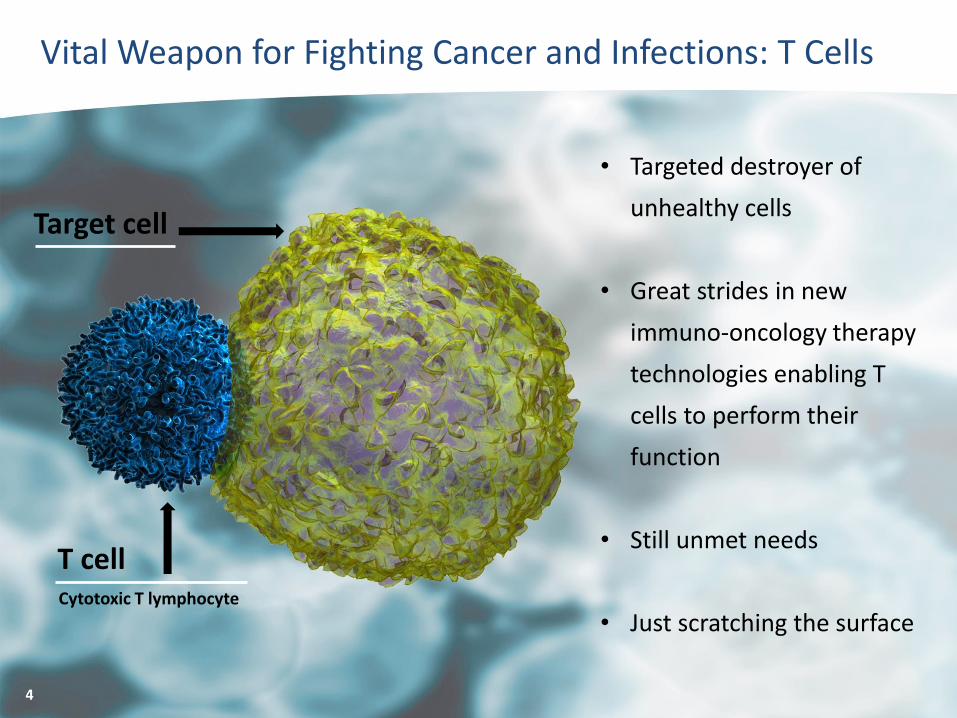
Vital Weapon for Fighting Cancer and Infections: T Cells
Cytotoxic T lymphocyte
T cell
Target cell
4
• Targeted destroyer of
unhealthy cells
• Great strides in new
immuno-oncology therapy
technologies enabling T
cells to perform their
function
• Still unmet needs
• Just scratching the surface
5
An “Ideal” T Cell-Generating Immunotherapy?
Attributes
• Activate targeted, antigen-specific T cells
• Functional, with “killing tools” granzyme and perforin
• Robust in magnitude
• Persistent and durable over time
• In vivo (in the body) rather than ex vivo production
• No unwanted immune response against a vector
• No toxic inflammatory response
• Capable of breaking immune system tolerance to a
cancer

Inovio DNA Immunotherapies: T Cells by Design
IT’S ALL ABOUT THE
T CELLS
Identify pertinent disease-specific antigen(s)
Encode one or more DNA plasmids with genetic code for individual antigens
Deliver plasmids into cells, enabling them to produce antigen(s)
T cells eliminate cells displaying disease-specific antigen
Immune system responds to antigens; activates antigen-specific T cells
Effective, efficient, safe in vivo T cell activation
Cellular machinery uses DNA code to produce encoded disease antigens
ANTIGENIC PROTEINS
5

7
• Activate disease-specific CD8+ killer T cells and antibodies
Antigen targeting immunotherapies &
vaccines
• Enhance immune response activation
• Impact durability of immune responses
• Drive immune responses to sites of infectionImmune activators
• Simplified design, product stability, better manufacturing, dosing, and cost effectiveness
• Rapidly activates robust antibody responses
• Target infections or cancers (checkpoint inhibitors)
DNA-Based Monoclonal Antibodies
(dMAbs)
DNA Immunotherapy Platform: Multiple Applications
8
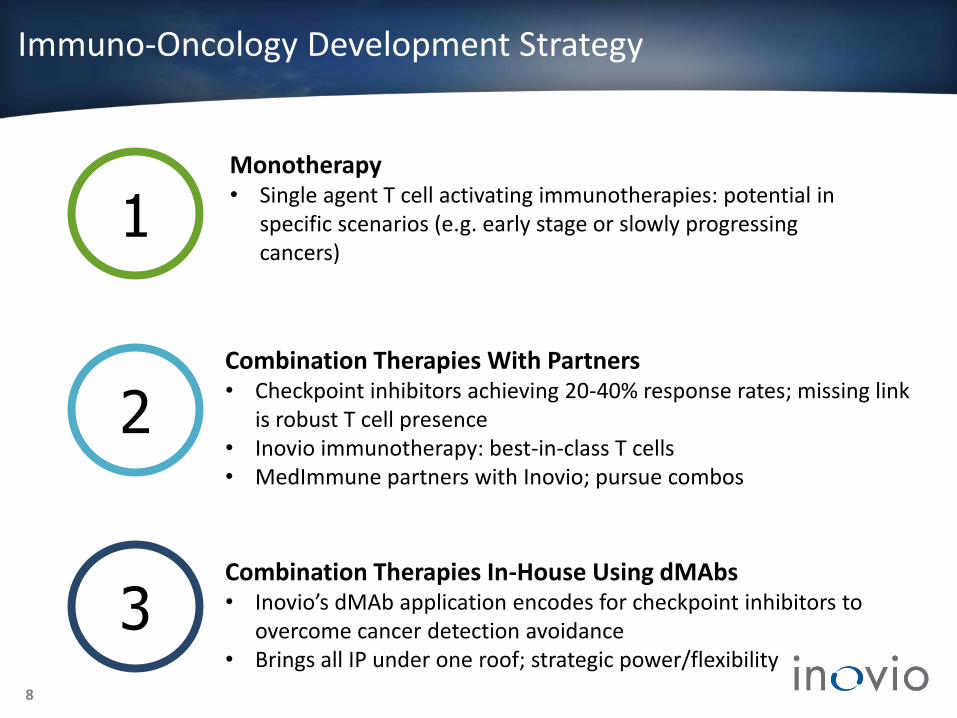
Immuno-Oncology Development Strategy
1
2
3
Monotherapy• Single agent T cell activating immunotherapies: potential in
specific scenarios (e.g. early stage or slowly progressing cancers)
Combination Therapies With Partners• Checkpoint inhibitors achieving 20-40% response rates; missing link
is robust T cell presence • Inovio immunotherapy: best-in-class T cells• MedImmune partners with Inovio; pursue combos
Combination Therapies In-House Using dMAbs• Inovio’s dMAb application encodes for checkpoint inhibitors to
overcome cancer detection avoidance• Brings all IP under one roof; strategic power/flexibility

Inovio Immuno-Oncology Pipeline
Product Name Indication Preclinical Phase I Phase II
Vgx-3100
Ino-5150
Ino-1400
Phase III
9
INO-3112
INO-3112
Breast/lung / Pancreatic
cancers
Prostate cancer
Head & Neck Cancer
Cervical Cancer
Cervical dysplasia
Aerodigestive CancerINO-3106

10
Cervical Dysplasia: Schiffman et al. Arch Pathol Lab Med (2003), Public Health England Cervical Cancer Screening Programme, Stoler et al. Anatomic Path (2011), Castle et al. JNCI (2005), Mayrand et al. NEJM (2007)Cancers: CDC, www.hpvcentre.net, WHO IARC
HIGH GRADE
CERVICAL
DYSPLASIA
(CIN2/3)
US:220,000 –270,000
EU5:
260,000
High Grade
Vulvar
Neoplasia
(VIN)
US:4,400 -27,000
EU5:6,500
High grade
Anal
Neoplasia
(AIN)
US:13,400
EU5:13,400
ORO-
PHARYNGEAL
CANCER
US:14,410
EU5:33,330
CERVICAL
CANCER
Annual incidences: US and EU5
HPV-Caused Pre-Cancers & Cancers
US: 12,900
EU5: 43,670
HPV driven cancers

Phase II: Study Design
• 148 subjects: 18-55 year old females with high-grade cervical dysplasia (CIN2/3)
• HPV 16 and/or 18 positive
• 6 mg VGX-3100 or placebo(IM followed by EP) at weeks 0, 4, and 12
Placebo-Controlled, Randomized, Double
Blind
• Regression of CIN2/3 to CIN1 or normal at six months post third dose (Week 36)Primary Endpoint
• Regression of CIN2/3 to CIN1 or normal and
• Clearance of HPV 16 and/or 18 genotype detected during screen
Secondary Endpoint
11

0
10
20
30
40
50
60
Phase II: Regression of Cervical Lesions to CIN 1 or Normal
Pre-Specified 1° Endpoint: HistopathologicRegression of CIN2/3 to CIN1 or Normal
30.6%(11/36)
Statistically significant difference(p=0.017; strata-adjusted)
Post-Hoc Analysis: Regression of CIN2/3 to Normal
0
10
20
30
40
50
60
40.2%(43/107)
16.7%(6/36)
Perc
ent
VGX-3100 Placebo VGX-3100 Placebo
Statistically significant difference(p=0.006; strata-adjusted)
Overall Histopathologic Regression Incidence
Per-Protocol Population (N=143)
12
49.5%(53/107)
Perc
ent
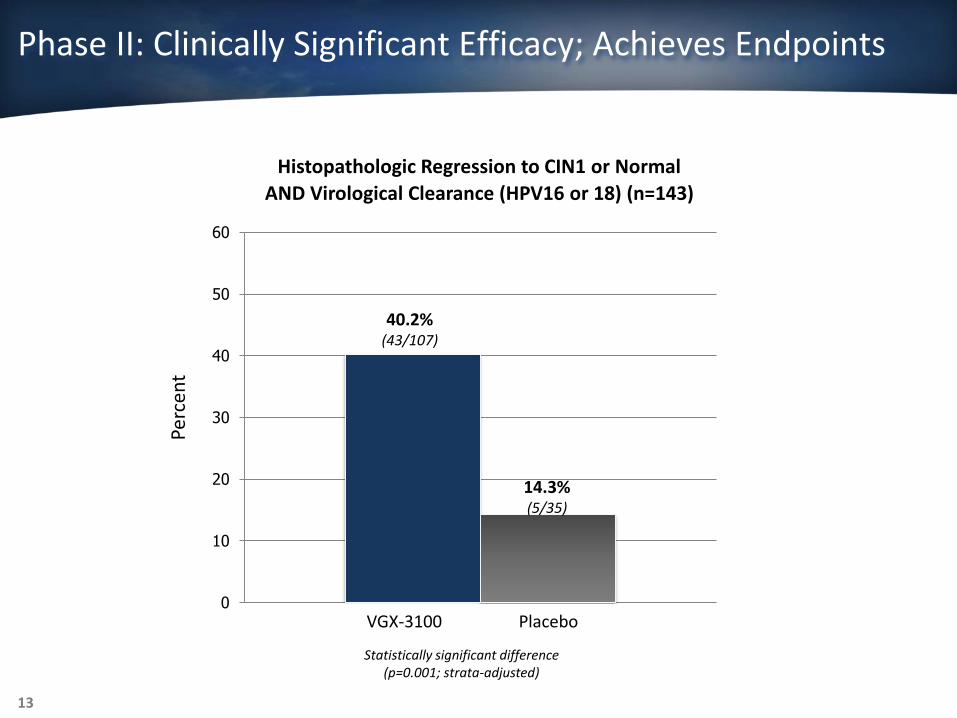
Phase II: Clinically Significant Efficacy; Achieves Endpoints
49.5%(53/107)
30.6%(11/36)
Histopathologic Regression to CIN1 or Normal
AND Virological Clearance (HPV16 or 18) (n=143)
0
10
20
30
40
50
60
40.2%(43/107)
14.3%(5/35)
Perc
ent
VGX-3100 Placebo
Statistically significant difference(p=0.001; strata-adjusted)
13

VGX-3100 Generates HPV-16 and HPV-18 T Cell Responses
14
N=140
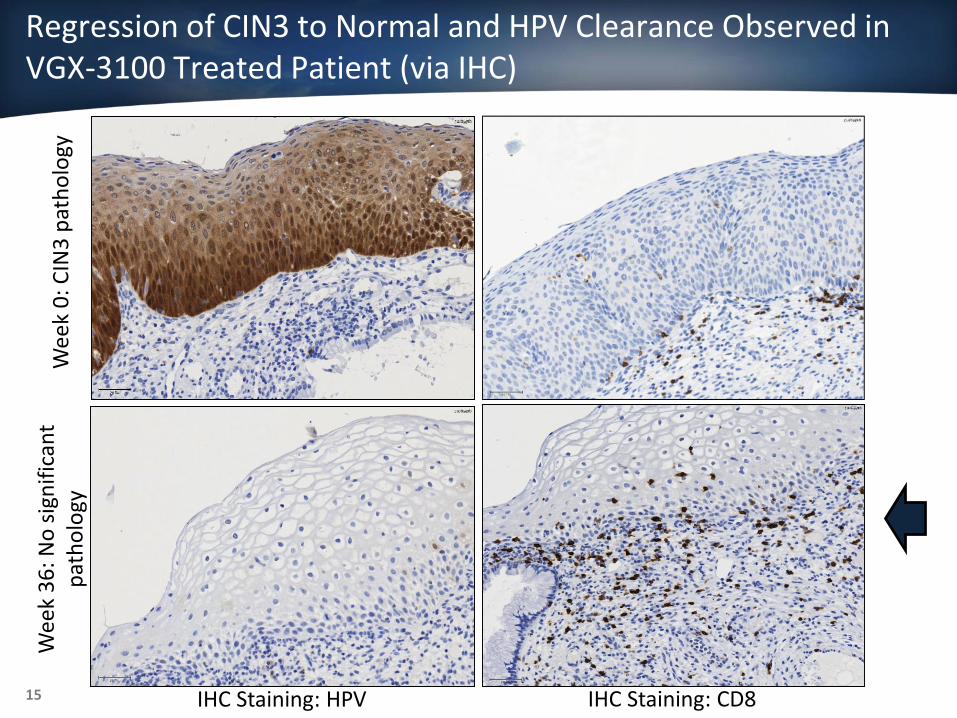
Regression of CIN3 to Normal and HPV Clearance Observed in VGX-3100 Treated Patient (via IHC)
Wee
k 0
: CIN
3 p
ath
olo
gy
IHC Staining: HPV
Wee
k 3
6: N
o s
ign
ific
ant
pat
ho
logy
IHC Staining: CD815
Powerful Impact of VGX-3100 Phase II T Cell & Efficacy Data
• Simple 3 monthly injections generated antigen-specific CD8 killer T cells• Measured in blood• Observed in cervical tissue (tissue infiltrating T cells)• Direct correlation found between CD8 T cells and efficacy
• Demonstrated phase II efficacy and safety• Regressed disease to normal• Cleared virus which caused the disease
• Non-surgical option for the treatment of CIN2/3 • Proof of principle regarding all HPV-related antigens and diseases • Advance other anti-cancer therapies (lung, breast, pancreas, prostate)• Virus (HPV) clearance supports other anti-viral therapies (HBV, HCV, HIV)
16
Phase II results facilitate strategic cancer vaccine collaboration and license with MedImmune and support advancement into phase III HPV precancer trial

VGX-3100: Next Steps
EXPANSION OF HPV PROGRAM TO RELATEDCANCERS AND PRE-CANCERS• HPV cancers licensed to MedImmune for use in combination therapies• Inovio to pursue HPV pre-cancers
SCIENTIFIC PAPER IN PEER REVIEWED JOURNAL• Completed immunological analysis to characterize T cell subsets.
Phase II data adds to phase I data, which was extensively characterized (Bagarazzi, et al. Sci Transl Med 2012)
• Manuscript accepted in top-tier journal
PHASE III PLANNING FOR EARLY 2016 LAUNCH• Clinical and regulatory• Scale up immunotherapy production• Market research
• Supply chain strategy• EP device production• Pricing & reimbursement
17

• 20 men/women • Safety, tolerability, immunogenicity • Anti-tumor effects & progression free survival• Arm #1: treat before/after tumor resection• Arm #2: treat after chemoradiation
HPV-Associated Head & Neck Cancer Studies: INO-3112
Phase I/IIa clinical trialINO-3112 (VGX-3100 + IL-12 DNA immune activator)
HPV 16/ 18 related disease
18
Head & Neck Squamous Cell Carcinoma
Being advanced as part of MedImmune’s license and combination strategy development plan with Inovio

• 126 women with cervical carcinoma• Safety & progression free survival at 18
months• INO-3112 administered during standard
chemo-radiotherapy (CRT) or during and after standard CRT as an adjuvant
• Funded by the EORTC
• 20 women with cervical carcinoma• Safety, tolerability, immunogenicity• Cervical histology • Treat after chemoradiation
HPV-Associated Cervical Cancer Studies: INO-3112
Two clinical trials for cervical cancer: INO-3112 (VGX-3100 + IL-12 DNA immune activator)
HPV 16/ 18 related disease
19
Phase I/II Cervical Cancer Phase II Cervical Cancer
Being advanced as part of MedImmune’s license and combination strategy development plan with Inovio

Phase I: INO-1400 +/- IL-12 DNA immune activator
Human telomerase reverse transcriptase (hTERT), associated with cancer cell survival
hTERT-Associated Cancers Study: INO-1400
• hTERT overexpressed in 85% of cancers - potential “universal” cancer therapy • 54 patients• Safety, tolerability, immunogenicity• Anti-tumor effects and progression free survival • Trial launched: 4Q 2014
20
Breast, Lung, or Pancreatic Cancers

• Men with biochemically relapsed prostate cancer• Safety, tolerability, and immunogenicity of INO-5150 alone or in combination with
DNA-based IL-12 immune activator• Evaluating changes in PSA levels • Study initiated 3Q 2015
Prostate Cancer Study: INO-5150
Phase I clinical trialINO-5150 or INO-5150 + IL-12
Targeting PSA & PSMAProstate cancer
21
Prostate Cancer
22
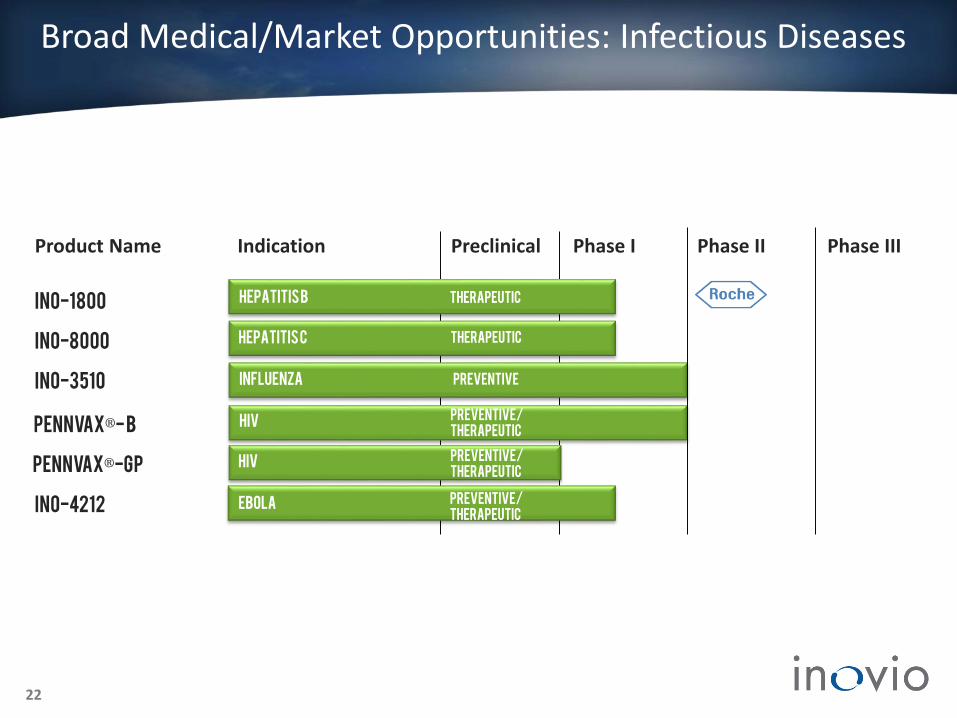
Ino-3510
ino-1800Hepatitis B Therapeutic
influenza
EbolaINO-4212
Preventive
Pennvax®- B hiv
Pennvax®-GP hiv
Preventive/
Therapeutic
Preventive/
Therapeutic
Ino-8000 Hepatitis C Therapeutic
Product Name Indication Preclinical Phase I Phase II Phase III
Broad Medical/Market Opportunities: Infectious Diseases
Preventive/
Therapeutic

• 126 patients• Safety, tolerability, immunogenicity • Trial started: 2Q 2015• Roche paying all development costs plus milestones• 240M+ global market opportunity
23
Hepatitis B Study: INO-1800
Phase I: INO-1800 +/- IL-12 DNA immune activator
Multi-antigen: HBV pan-clade surface antigens & core antigens
Chronic Hepatitis B Virus

Louis Pasteur
Peter KiesCFO• Ernst & Young
• Experience with growth companies
Mark L. Bagarazzi, MDCMO• Clinical research experience incl. Merck
• Led clinical/regulatory for shingles and rotavirus vaccines; DNA vaccine expert
J.Joseph Kim, PhDPresident & CEO
• Decades of biotechnology/ pharma management
• Merck: hepatitis A and B vaccines manufacturing; HIV
vaccine (Ad5) R&D
Niranjan Y. Sardesai, PhDCOO
• Extensive biotech management and product development
experience
• Led diagnostics development for mesothelioma, bladder
cancer, and ovarian cancer for Fujirebio Diagnostics
Management
24

J. Joseph Kim, PhD• President & CEO, Inovio
Adel Mahmoud, PhD• Professor, Princeton University
• Former President, Merck Vaccines
• Responsible for Gardasil®, Zostavax®, Proquad® and Rotateq®
Morton Collins, PhD• General Partner, Battelle
Ventures and Innovations Valley Partners
Simon X. Benito• Former Senior Vice President,
Merck Vaccine Division
Angel Cabrera, PhD• President, George Mason University
• Former President, Thunderbird School of Global Management
Avtar Dhillon, MD Chairman, BOD
• Former President & CEO, Inovio Biomedical
Board of Directors
25
Nancy Wysenski , MBA• Former COO of Endo
Pharmaceuticals and Vertex Pharmaceuticals

Louis PasteurStanley A. Plotkin, MD• Developed rubella and rabies vaccines
• Oversaw Sanofi flu vaccine
• Emeritus Professor, Wistar Institute & University of Pennsylvania
Philip Greenberg, MD• Expert in T cell immunology
• Head, Immunology Program, Fred Hutchinson Cancer Research Center
26
Anthony W. Ford-Hutchinson, PhD
• Former SVP, Vaccines R&D, Merck
• Oversaw development: Singulair®, Januvia®, Gardasil®, Zostavax®,
Proquad® and Rotateq®
David B. Weiner, PhDChairman
•“Father of DNA vaccines”
• Dept. of Pathology & Laboratory Medicine, University of Pennsylvania
Scientific Advisory Board

Financial Information
Cash & short-term investments2 $ 154.6 M
Debt2 0 M
Cash runway 4Q 2018
Shares outstanding2 71.8 M
Recent share price1 $8.19
Market cap1 $ 588.0 M
NASDAQ: INO
27
1Aug 10, 2015 2June 30, 2015 3 Payable in Q3, 2015
Upfront payment: MedImmune 3 $ 27.5 M

INTERNALLY FUNDED EXTERNALLY FUNDED
Ino-14002016Report interim data
Breast, Lung, And
Pancreatic Cancer
Vgx-31002015 Publish data in med journalEarly 2016 Initiate phase IIICervical dysplasia
28
Value Drivers
INO-3112 Phase I/II studies progressingHead & Neck and
Cervical Cancer
Ino-80002015Report interim phase I data
Hepatitis C
Ino-18002Q 2015Initiated phase I
Hepatitis B
Ebola2Q 2015Initiated phase I
INO-4212
Ino-51503Q 2015Initiated phase I
Prostate cancer
PennVAX® 3Q 2015 Initiate PENNVAX-GP phase I
HIV
INO-31122016Initiate phase II with EORTCCervical Cancer
Best-in-class immune
responses to fight cancers
and infectious diseases
Targeting broad range of billion dollar disease
markets
Breakthrough in vivo T cell generating technology Validating
partnerships with
MedImmune & Roche
Lead product achieved phase
II efficacy endpoints
Investor Highlights
29





























