Embed Size (px)
Citation preview

SEPSIS BIOMARKERS UPDATES
DR.MAGDY KHAMES ALY
CRITICAL CARE MEDICINE
ZMH AL BATAYEH
NOV 2017
OBJECTIVES
• Simplifying the understanding of sepsis biomarkers role.
• Identify the best biomarker for sepsis diagnosis
• Define the role of each biomarker in sepsis
• Define the best model to diagnose sepsis early
INTRODUCTION
• Sepsis is one of the most common causes of death in severely injured patients worldwide. The early detection of sepsis still has to be solved in clinical practice.
• The delayed diagnosis often contributes to inappropriate antimicrobial treatment and subsequent high mortality.
• Sepsis biomarkers are produced during the host response to infection.
• Traditional biomarkers are polypeptides and/or proteins derived from this response.
• Omics-based biomarkers are screening out from all kinds of molecules of host response while high-throughout omics technologies are emerging.
OMICS
Technologies that measure some characteristic of a large family of cellular molecules, such as genes, proteins, or small metabolites, have been named by appending the suffix “-omics,” as in “genomics.” Omics refers to the collective technologies used to explore the roles, relationships, and actions of the various types of molecules that make up the cells of an organism.
ROLES OF BIOMARKERS
• Diagnosis
–Identifying or ruling out sepsis.
–Identifying patients who may benefit from
specific therapies.
• Follow up the response to therapy.
• Prognosis.
THE PERFECT SEPSIS BIOMARKER
• Should be highly sensitive and specific for sepsis to allow the differentiation between infectious and non-infectious causes of inflammation, organ dysfunction and shock.
• Linked to the main underlying processes
–Inflammation
–Coagulation
–Tissue damage
–Tissue repair
• Should be present at the onset or even before the appearance of the clinical signs of sepsis to have prognostic value.
• Should be easy and safe to measure with low cost for the patients and for the hospital.
• Should be biologically plausible.
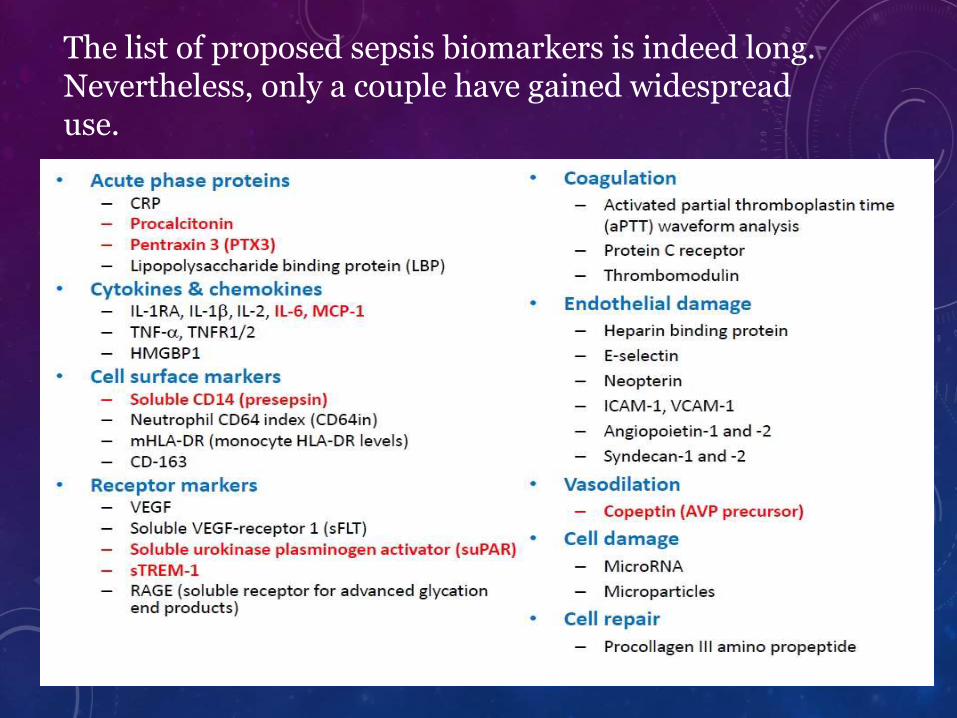
The list of proposed sepsis biomarkers is indeed long. Nevertheless, only a couple have gained widespread use.
QUESTIONS TO BE ANSWERED
• Does the biomarker aid diagnosis?
• Does it provide additional prognostic info?
–For outcome
–For progression/decline
• Better than scoring systems?
THE ROC CURVE• The ROC curve is a widely used tool for comparing diagnostic tests.
The curve is constructed by plotting the diagnostic sensitivity and specificity values for every individual cut-off on a graph with 1-specificity on the x-axis and sensitivity on the y-axis.
• The shape of an ROC curve and the area under the curve (AUC) helps estimate the discriminative power of a marker. The closer the curve is located to the upper left-hand corner and the larger the AUC, the better the marker is at discriminating between septic and non-septic patients.
• A perfect biomarker has an AUC of 1, whereas a non-discriminating marker has an area of 0.5.
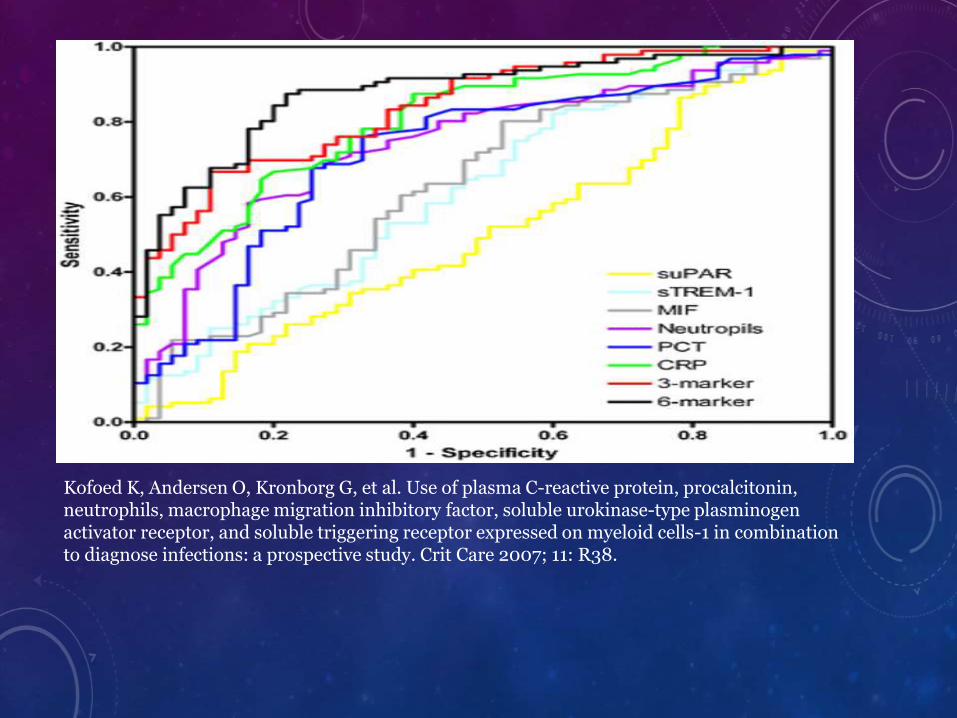
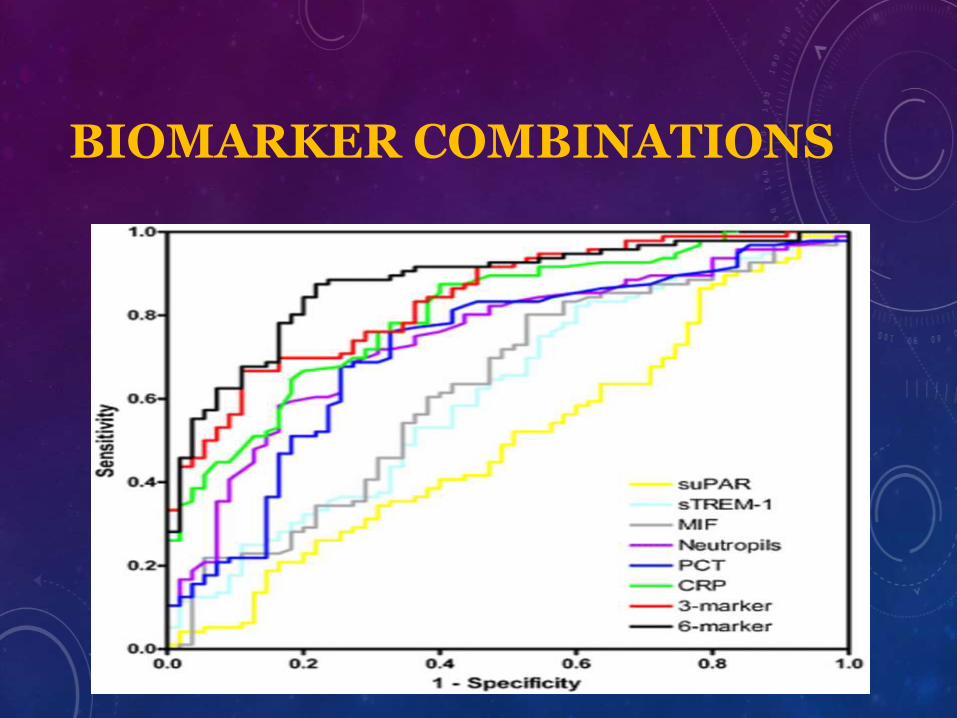
Kofoed K, Andersen O, Kronborg G, et al. Use of plasma C-reactive protein, procalcitonin, neutrophils, macrophage migration inhibitory factor, soluble urokinase-type plasminogen activator receptor, and soluble triggering receptor expressed on myeloid cells-1 in combination to diagnose infections: a prospective study. Crit Care 2007; 11: R38.
Displayed are ROC curves comparing:
• Soluble urokinase-type plasminogen activator receptor (suPAR),
• Soluble triggering receptor expressed on myeloid cells (sTREM)-1,
• Macrophage migration inhibitory factor (MIF),
• Neutrophil count,
• Procalcitonin (PCT),
• C-reactive protein (CRP),
• Combined three-marker and Six-marker tests for detection of
bacterial versus non-bacterial causes of systemic inflammation.
• The six-marker combination is the best-performing marker
model (ROC-AUC 0.88)
C-REACTIVE PROTEIN (CRP)
• Acute phase protein
• Synthesized in liver
• IL-6 (and IL-1 and TNFα) stimulate synthesis
• Binds bacterial polysaccharide/ chromatin
– Activates the classical complement pathway
– Increase the immune inflammatory response in bacteria infection
CLINICAL SIGNIFICANCE (CRP)
Diagnostic use:
• CRP is used mainly as a marker of inflammation.
• Normal concentration in healthy human serum is between 5 and 10 mg/L, increasing with aging
• Higher levels are found in late pregnant women, mild inflammation and viral infections (10–40 mg/L),
active inflammation, bacterial infection (40–200 mg/L),
severe bacterial infections and burns (>200 mg/L).
Follow/up treatment:
• Measuring and charting CRP values can prove useful in determining disease progress or the effectiveness of treatments.
Limitations
CRP is a non‐specific marker of inflammation so does not indicate the
organ or organs affected.
CRP measurements can only be used to assess cardiovasular risk status if they are made in the absence of acute inflammation.
CLINICAL SIGNIFICANCEPROCALCITONIN
Diagnostic:
• To aid in the diagnosis and risk stratification of bacterial sepsis.
• To aid in the diagnosis of renal involvement in children with urinary tract infection.
• To aid in distinguishing bacterial from viral infections, including meningitis.
• To monitor therapeutic response to antibacterial therapy and reduce antibiotic exposure.
• To aid in the diagnosis of systemic secondary infection after surgery and in severe trauma, burns, and multiorgan failure.
• To aid diagnosis of infected necrosis and associated systemic complications in acute pancreatitis.
Prognostic:
Proposed applications of serum procalcitonin measurement include the following:
• To aid the choice and timing of the initiation of antibiotic treatment (Procalcitonin Algorithm)
• To assist with elucidating prognosis of severe localized infections (eg, pneumonia)
• To aid with elucidating prognosis of critically ill patients with systemic infection
• Predicting the need of antibiotic treatment in sepsis and to shorten the duration of antibiotics required
• Use as independent predictor of graft failure late after renal transplantation
PROCALCITONIN (PCT)• REFERENCE VALUES (EXCEPT NEWBORN)
SIGNIFICANTLY LOWER IN LEUKOPENICPATIENTS
• < 0.05ng/ml
• 0.5-2ng/ml
• >2ng/ml
• Healthy individuals Probability of sepsis is low, local infection possible
• Grey zone, recheck 6-12hrs later
• Probability of sepsis is high
LIMITATIONS• Procalcitonin, although useful in bacterial sepsis, has no
value in the assessment of fungal or viral infections and shows no response to intracellular microorganisms (ie, Mycoplasma) or in local infections with no systemic response.
• Similar to CRP, clinical conditions associated with high baseline procalcitonin levels include burns, major surgery, and systemic inflammatory processes.
• To date, the use of procalcitonin, both as an indicator of severe infection and predictor of antibiotic choices/duration, has been center-specific, with insufficient data from multicenter/multinational studies to support its use as a routine laboratory marker in clinical practice.
PROCALCITONIN VERSUS C-REACTIVE PROTEIN
• Studies investigating the use of PCT and CRP have found
the diagnostic performance of CRP and PCT to be rather
similar. With regard to diagnosing bacteremia in particular,
PCT have shown excellent diagnostic ability; this is in
accordance with the suggested notion that PCT is superior to
CRP in diagnosing systemic infection.
• What makes PCT particularly interesting is that several
well-designed studies have proven that algorithms based on
PCT concentrations as the main guide can shorten the length
of antibiotic treatment and decrease the use of antibiotics.
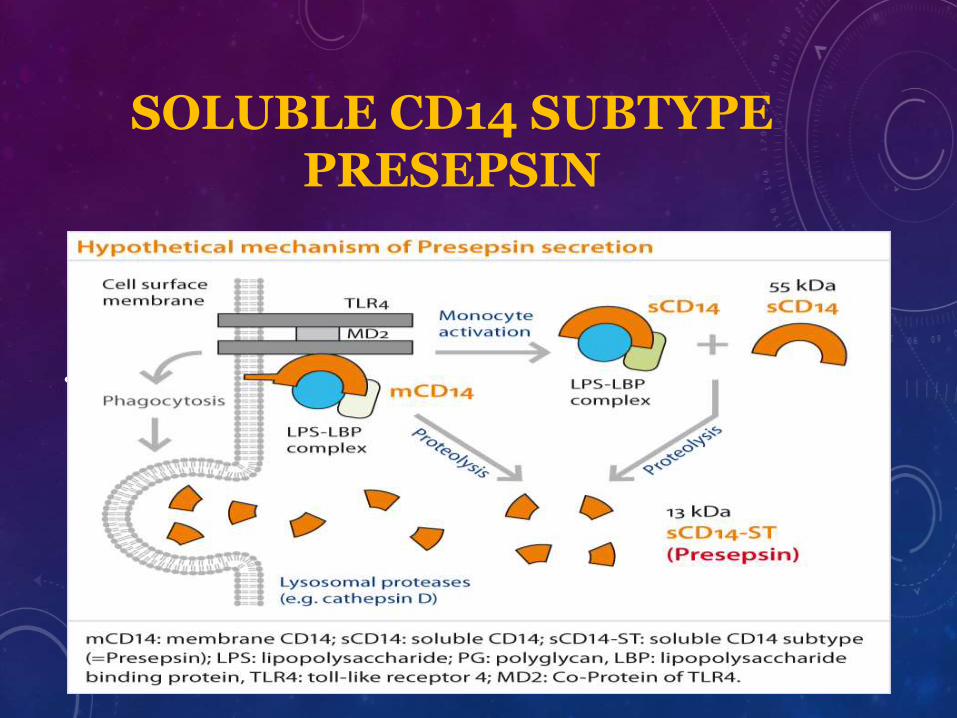
SOLUBLE CD14 SUBTYPE PRESEPSIN
• In 2004, a new biomarker sCD14-subtypes (presepsin) was found and its value was shown in the diagnosis and evaluation of sepsis
PRESEPSIN• In 2004, a new biomarker sCD14-subtypes (presepsin)
was found and its value was shown in the diagnosis and evaluation of sepsis.
• CD14 acts as a co-receptor (along with the Toll-like receptor TLR 4 and MD-2) for the detection of bacterial lipopolysaccharide (LPS).
• By activating a proinflammatory signaling cascade on contact with infectious agents, CD14 has a role as a recognition molecule in the innate immune response against microorganisms.
• During inflammation, plasma protease activity generates soluble CD14 (sCD14) fragments. One of them, called sCD14 subtype (sCD14-ST), or presepsin.
PRESEPSIN VS PCT
In comparison with PCT
Diagnostic accuracy:
• The best diagnostic cutoff for presepsin was 600 pg/ml. At that level, sensitivity and specificity were 78.95% (95% CI, 69.4 to 86.6)
• The best diagnostic cutoff in terms of sensitivity and specificity for PCT was 0.18 ng/ml, corresponding to 89.47% sensitivity (range, they actually were 95% CI 81.5% to 94.8%) and 75.90% specificity (range, 65.3% to 84.6%)
PRESEPSIN VS PCT
• The receiver operating characteristic (ROC) curves were designed including those patients with a definitive diagnosis of sepsis or severe sepsis/septic shock.
• The results were significant for both biomarkers. The areas under the curve (AUCs) calculated from the ROC curve were 0.701 (95% confidence interval (CI), 0.63 to 0.77; P < 0.001,) for presepsin and 0.875 (95% CI, 0.82 to 0.92; P < 0.001) for PCT, respectively. The difference between the two AUCs was significant (P < 0.001)
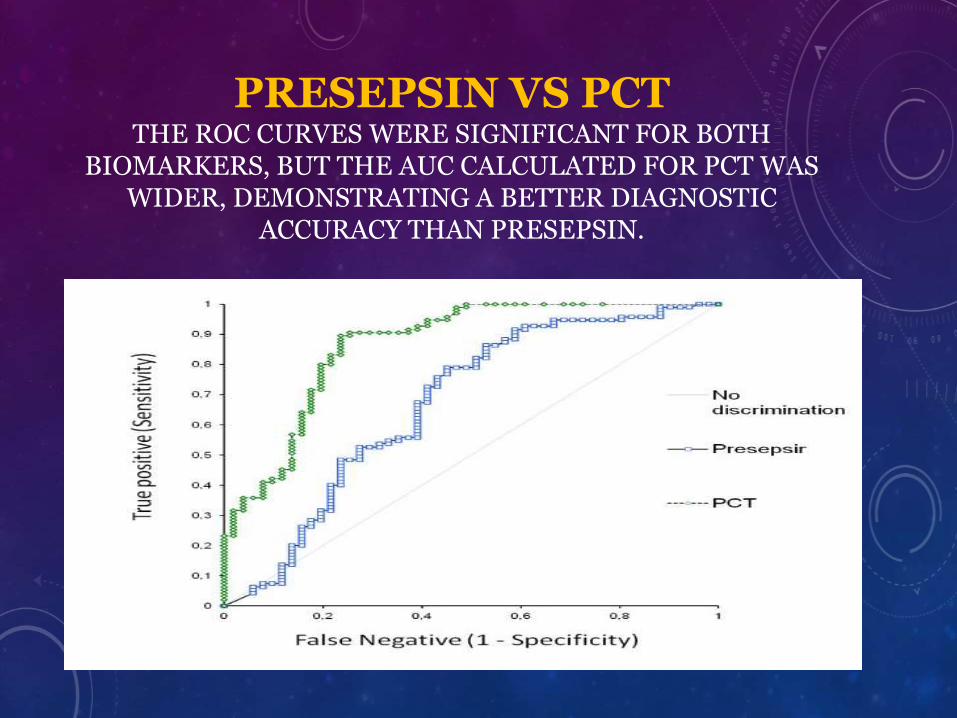
PRESEPSIN VS PCTTHE ROC CURVES WERE SIGNIFICANT FOR BOTH
BIOMARKERS, BUT THE AUC CALCULATED FOR PCT WAS WIDER, DEMONSTRATING A BETTER DIAGNOSTIC
ACCURACY THAN PRESEPSIN.

PRESEPSIN VS PCT
Prognostic role
• Analysis of 60-day mortality showed the superiority of presepsin compared to PCT. Presepsin concentrations at the first evaluation in the ED were higher in nonsurvivorseptic patients than in survivors. No significant correlation was found between PCT values and 60-day mortality. These results pointed out the possible prognostic role of presepsinin predicting in-hospital mortality and promptly identifying high-risk patients.
• The close correlation between presepsin initial values and in-hospital mortality suggests its potential usefulness for the early recognition of high-risk septic patients, who could benefit from a more aggressive approach starting in the ED.
FUTURE SEPSIS BIOMARKERS
Triggering receptor expressed on myeloid cells-1(TREM-1)
• TREM-1 is expressed mainly on macrophages and neutrophils, and has been identified as an amplifier of the immune response that strongly enhances leukocyte activation in the presence of microbial products
• A soluble TREM-1 variant (sTREM-1) has been detected in several body fluids
• Initially, sTREM-1 was only found in fluids from patients with microbial infections, but recent studies have found elevated sTREM-1 plasma levels in patients with non-infectious conditions, such as inflammatory bowel disease and chronic obstructive pulmonary disease, and in patients undergoing cardiac surgery
• The latter results suggest that sTREM-1 can be released by a broad spectrum of inflammatory stimuli.
TRIGGERING RECEPTOR EXPRESSED ON MYELOID CELLS-1(TREM-1)
• The first promising result of the use of sTREM-1 in plasma to diagnose sepsis in ICU patients [31] indicated that sTREM-1 might be that perfect diagnostic sepsis biomarker that everybody had been looking for.
• A recently published meta-analysis of the diagnostic value of sTREM-1 concluded that sTREM-1 represents a reliable biological marker of bacterial infection
• But because of deficient studies and the heterogeneity in study design and setting, and the limited size of the studies published make it impossible to draw firm conclusions on the diagnostic accuracy of sTREM-1.
CYTOKINES
• Based on our present knowledge, measurements of single cytokines will not have great impact on the future diagnosis of sepsis. However, it is plausible that real-time monitoring of a panel of cytokines and receptors will be important to determine the level of dysregulation of the innate immune system and to guide future sepsis treatments.
PENTRAXIN-3
• Pentraxin-3 (PTX-3) is an acute-phase protein involved in inflammatory and infectious processes.
• Specifically for the presence of at least sepsis. In addition, PTX-3 correlated with disease severity and degree of organ dysfunctions as assessed by clinical scores such as the SOFA score, as has also been described in earlier studies
• Circulating PTX3 concentrations are elevated in sepsis and even higher in septic shock
• Consistent with the current observations, multiple previous studies presented significant and valuable AUCs for discriminating sepsis or septic shock from healthy controls

PENTRAXIN-3
• The diagnostic superiority of PTX-3 over PCT or CRP is still under debate, as different studies so far have been inconsistent regarding their diagnostic capacity in patients with sepsis and septic shock, applying different criteria and definitions of the sepsis syndrome. No study is currently available applying the newest Sepsis-3 definitions for novel biomarker analyses.
• In summary, PTX-3 valuably discriminates the different stages of sepsis severity during the first week of intensive care treatment according to latest Sepsis-3 definitions.
BIOMARKER COMBINATIONS
• No single marker may be able to have the high accuracy needed for fast and accurate guidance of treatment of sepsis patients.
• Therefore, the search for a single “magic bullet” marker might ultimately be fruitless, but a combination of markers could improve diagnosis, prognosis and treatment efficacy, and thereby survival. Instead of a single marker, a combination of markers may be the right approach to crack the “sepsis code”.
• A combination of the three best-performing markers (CRP, PCT and neutrophil count) and all six markers were found to be more accurate in detecting inflammatory response caused by bacterial infection than individual markers alone with an ROC-AUC of 0.88

BIOMARKER COMBINATIONS
• Shapiro et al published results from a multicenter study of ED patients with suspected sepsis . Nine biomarkers were assayed and multivariable logistic regression was used to identify an optimum combination of biomarkers to create a panel. Among the nine biomarkers tested, the optimum three-marker panel was neutrophil gelatinase-associated lipocalin, protein C and interleukin-1 receptor antagonist.
• The ROC-AUC for the accuracy of the sepsis score derived from these three biomarkers was 0.80 for severe sepsis, 0.77 for septic shock and 0.79 for death. In the future, multimarker panels will probably add to the diagnostic accuracy and risk assessment in sepsis.
BIOMARKER COMBINATIONS
CONCLUSIONS
• Accurate and timely diagnosis of infection and monitoring of treatment effects are very important for patient outcomes.
• Current evidence suggests that CRP will remain an important marker of inflammation and infection, and that PCT will enhance the clinicians’ ability to diagnose infection in critically ill patients and probably guide therapy. Thus I foresee that PCT will be measured in more patients in the future.
• A sepsis biomarker that has attracted a lot of attention during the last years is sTREM-1. On the one hand there are studies showing that sTREM-1 is the ideal sepsis biomarker, and on the other hand there are studies showing that sTREM-1 is as accurate as a toss of a coin.
• Given the complexity and variability of sepsis it is understandable that no single biomarker possesses all of the “perfect biomarker” qualities. Combining information from several sepsis markers is simple and may facilitate diagnosis and risk assessment in septic patients.

THANK YOU


















![Review Article An Update on Sepsis Biomarkers...sequential organ failure assessment (SOFA) score [4], recommended for assessing organ dysfunction in sepsis criteria-3 [1], runs the](https://img.dokumen.tips/doc/110x75/5f32800362b92645966bf002/review-article-an-update-on-sepsis-biomarkers-sequential-organ-failure-assessment.jpg)










