Embed Size (px)
Citation preview
Classification of Pelvic Fractures
Zahid AskarFCPS(Ortho), FRCS (Ortho)
Prof of Orthopaedics & TraumaKhyber Medical College, Peshawer

Value Of classification
• Mechanism of injury
• Treatment options
• Prognosis
• Records/communications
It should also be :-Easily ReproducibleHave good Intra- & Interobservor reliabilityEasily remembered/applied
Historical Background
• First attempt by Malgaigne in 1859
– Described without radiographs of the so-called “double vertical fracture”
Malgaigne I. F.: Traite des Fractures et desLuxations, Paris, J. B. Bailliere, 1855.
Historical classification
• Watson-Jones
• Connolly & Hedberg
• Huttinen & Slatis
• Trunkey
• Looser & Crombie
• Present classification systems started with the ground-breaking work by Pennal
• Classified Injuries as APC/LC/VS
Pennal GF, Sutherland GO. Fractures of the Pelvis. Park Ridge, IL: American Academy ofOrthopedic Surgeons, 1961.
Pennal, G. F., and Sutherland, G. 0.: Fractures of the Pelvis. Motion picture in AAOS film library, 1961.
Classification Systems
• Letournel
• Bucholz,
• Tile
• Young & Burgess
• OTA/AO -research
Commonly used Classification systems:-Tile ClassificationYoung & Burgess Classification
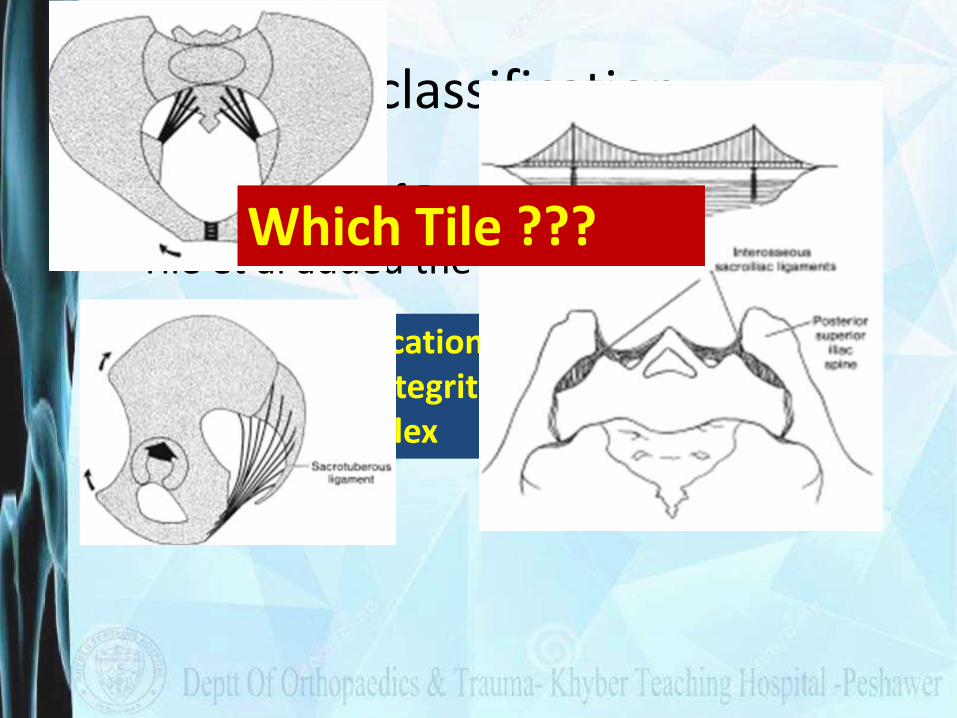
Tile classification
• Modification of Pennal Idea
• Tile et al added the concept of stability
The Tile classification system is mainly based on the integrity of the posterior sacroiliac complex
Which Tile ???
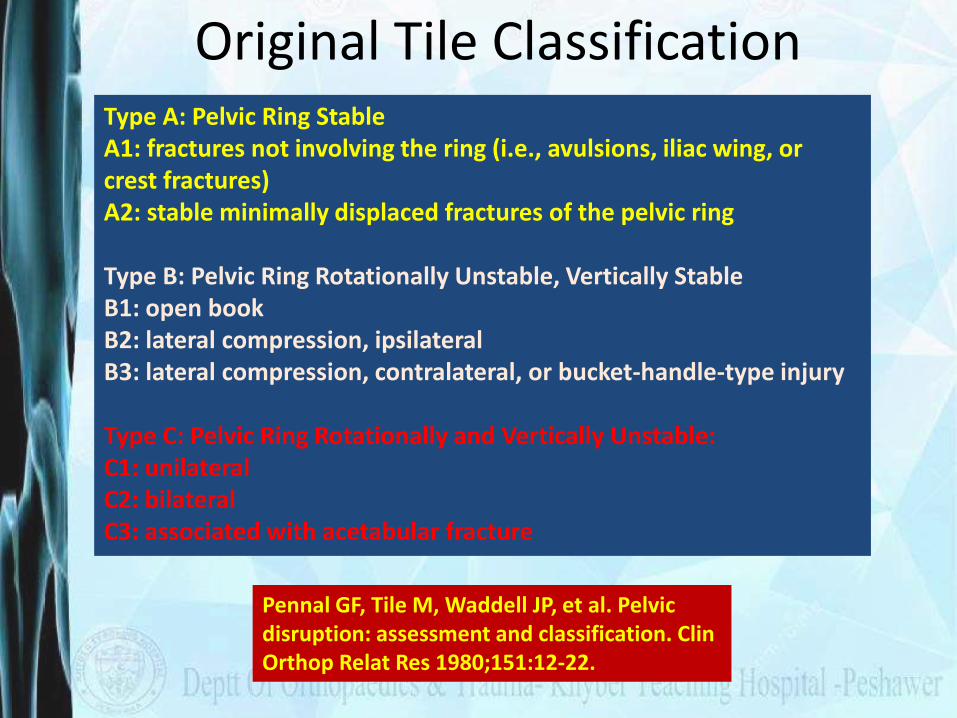
Original Tile Classification
Pennal GF, Tile M, Waddell JP, et al. Pelvic disruption: assessment and classification. ClinOrthop Relat Res 1980;151:12-22.
Type A: Pelvic Ring StableA1: fractures not involving the ring (i.e., avulsions, iliac wing, or crest fractures)A2: stable minimally displaced fractures of the pelvic ring
Type B: Pelvic Ring Rotationally Unstable, Vertically StableB1: open bookB2: lateral compression, ipsilateralB3: lateral compression, contralateral, or bucket-handle-type injury
Type C: Pelvic Ring Rotationally and Vertically Unstable:C1: unilateralC2: bilateralC3: associated with acetabular fracture
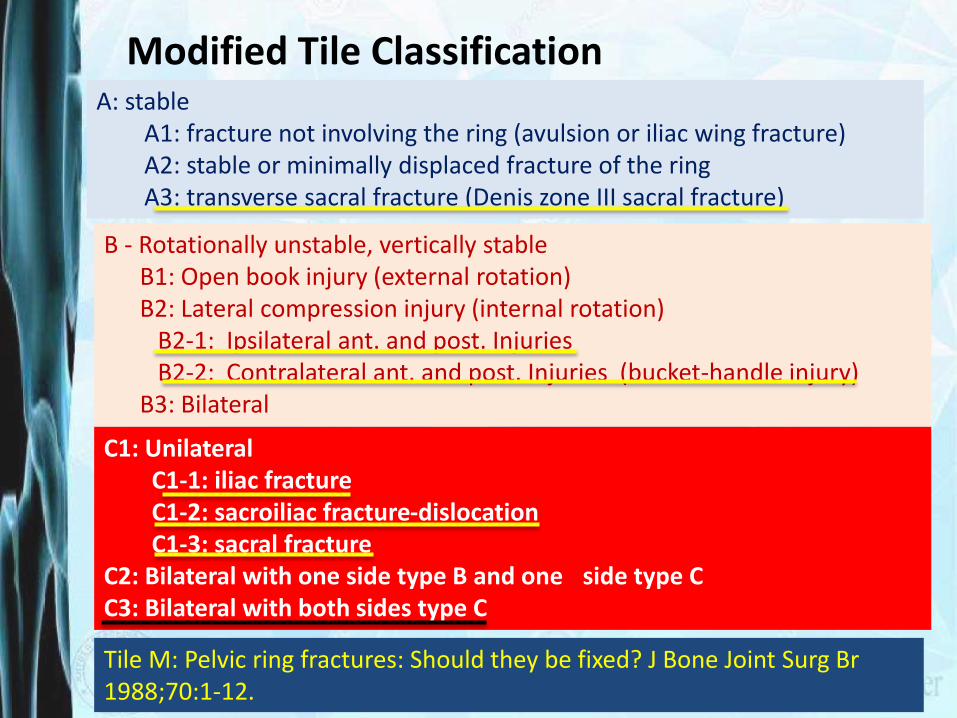
C1: UnilateralC1-1: iliac fractureC1-2: sacroiliac fracture-dislocationC1-3: sacral fracture
C2: Bilateral with one side type B and one side type CC3: Bilateral with both sides type C
B - Rotationally unstable, vertically stableB1: Open book injury (external rotation)B2: Lateral compression injury (internal rotation)
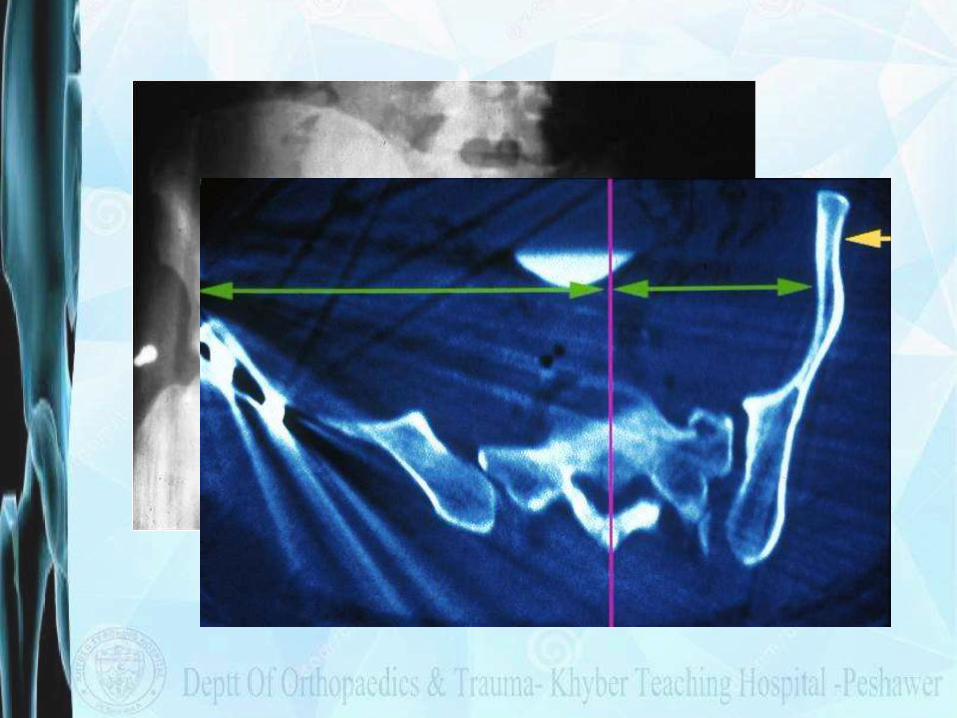
B2-1: Ipsilateral ant. and post. Injuries B2-2: Contralateral ant. and post. Injuries (bucket-handle injury)
B3: Bilateral
A: stableA1: fracture not involving the ring (avulsion or iliac wing fracture)A2: stable or minimally displaced fracture of the ringA3: transverse sacral fracture (Denis zone III sacral fracture)
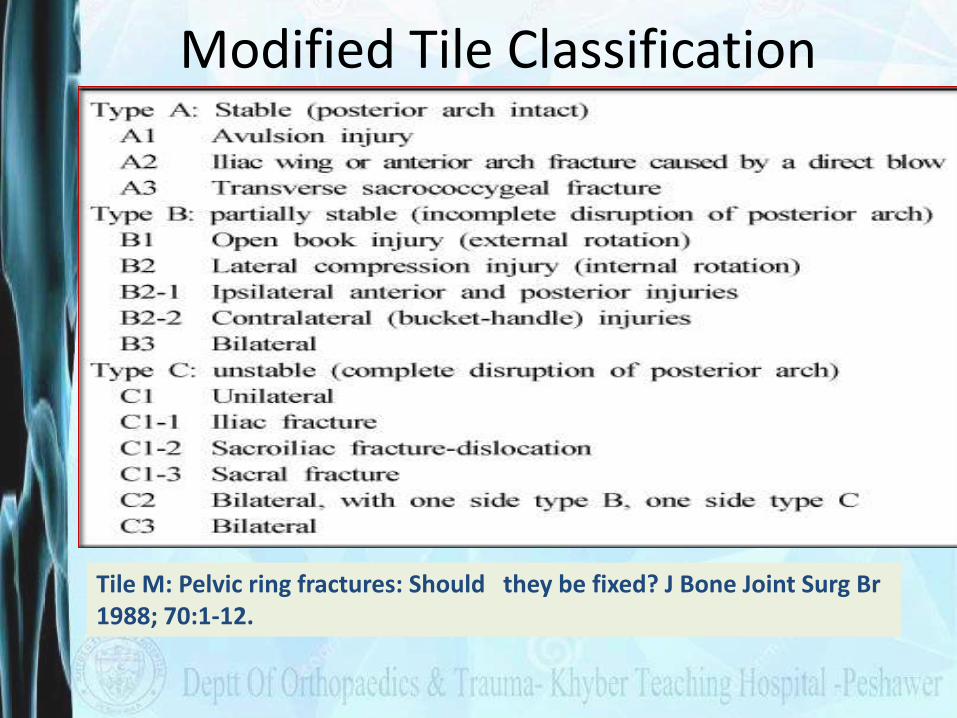
Modified Tile Classification
Tile M: Pelvic ring fractures: Should they be fixed? J Bone Joint Surg Br 1988;70:1-12.
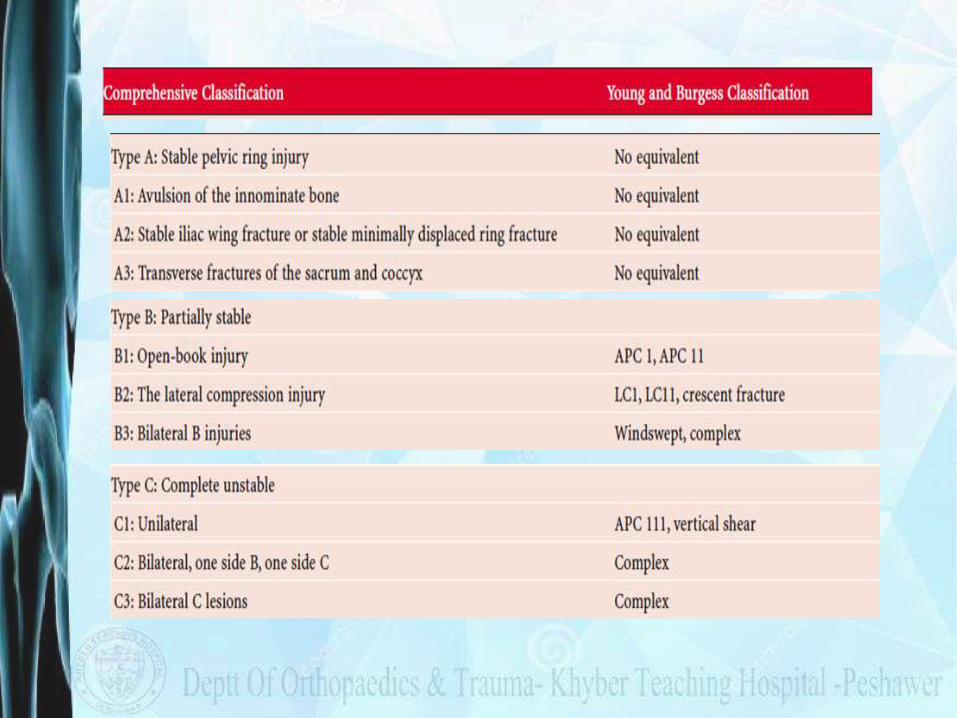
• Comprehensive Classification
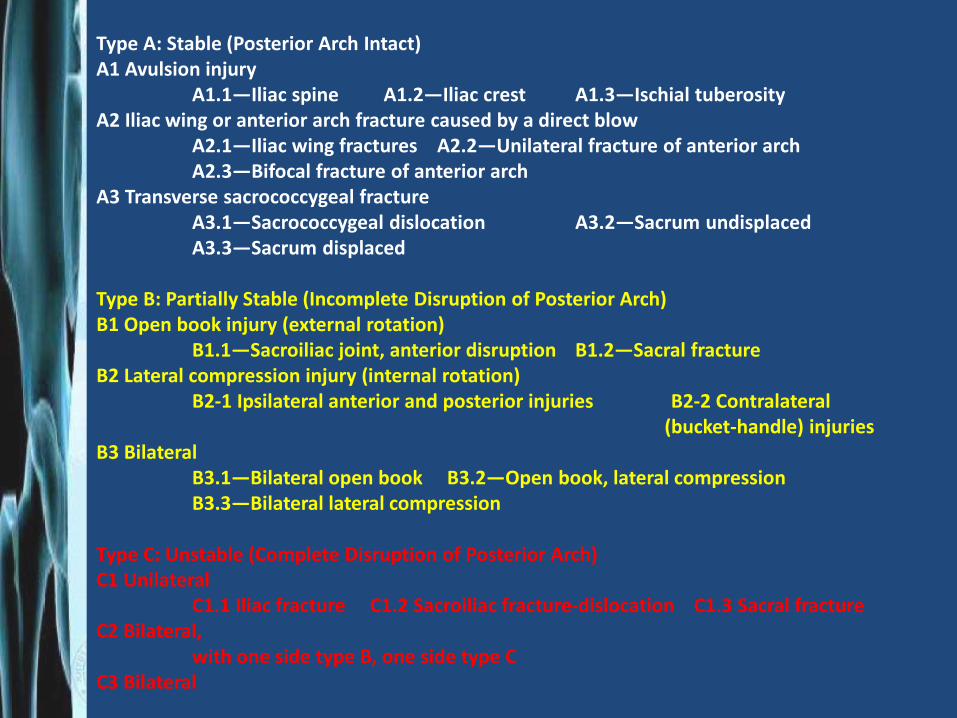
Type A: Stable (Posterior Arch Intact)A1 Avulsion injury
A1.1—Iliac spine A1.2—Iliac crest A1.3—Ischial tuberosityA2 Iliac wing or anterior arch fracture caused by a direct blow
A2.1—Iliac wing fractures A2.2—Unilateral fracture of anterior archA2.3—Bifocal fracture of anterior arch
A3 Transverse sacrococcygeal fractureA3.1—Sacrococcygeal dislocation A3.2—Sacrum undisplacedA3.3—Sacrum displaced
Type B: Partially Stable (Incomplete Disruption of Posterior Arch)B1 Open book injury (external rotation)
B1.1—Sacroiliac joint, anterior disruption B1.2—Sacral fractureB2 Lateral compression injury (internal rotation)
B2-1 Ipsilateral anterior and posterior injuries B2-2 Contralateral(bucket-handle) injuries
B3 BilateralB3.1—Bilateral open book B3.2—Open book, lateral compressionB3.3—Bilateral lateral compression
Type C: Unstable (Complete Disruption of Posterior Arch)C1 Unilateral
C1.1 Iliac fracture C1.2 Sacroiliac fracture-dislocation C1.3 Sacral fractureC2 Bilateral,
with one side type B, one side type CC3 Bilateral
Modified Tile Classification
Tile M: Pelvic ring fractures: Should they be fixed? J Bone Joint Surg Br 1988; 70:1-12.
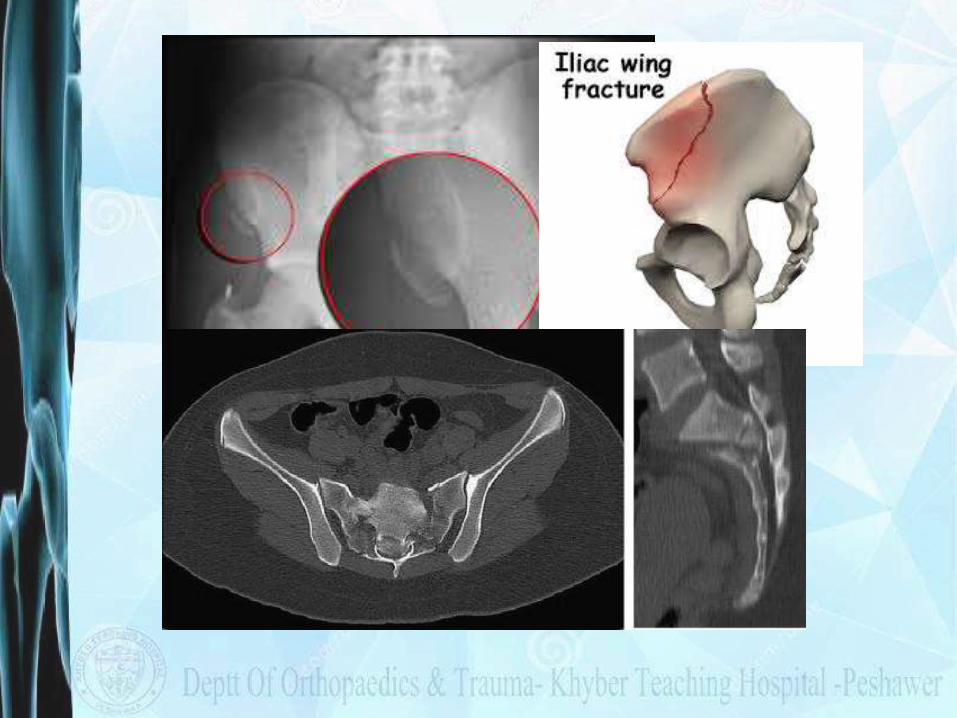
Tile Type A fractures
• The SI Joint is completely stable( Rotationally & vertically)
• Fractures are outside the pelvic ring !! A: stableA1: fracture not involving the ring (avulsion or iliac
wing fracture)
A2: stable or minimally displaced fracture of the ring
A3: transverse sacral fracture (Denis zone III sacral fracture)
Tile Type B Fractures
• Partial Instability of the SI Joint Complex
• Rotationally Unstable while Vertically stable
B - Rotationally unstable, vertically stable
B1: Open book injury (external rotation)
B2: Lateral compression injury (internal rotation)B2-1: with anterior ring rotation/displacement
through ipsilateral ramiB2-2-with anterior ring rotation/displacement
through contralateral rami (bucket-handle injury)
B3: Bilateral
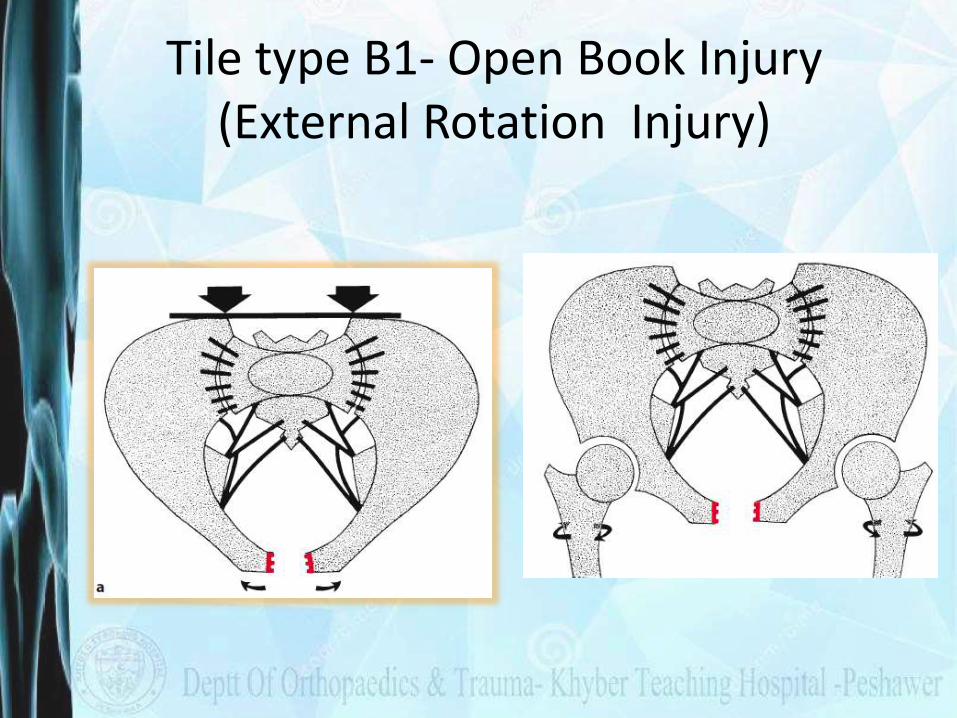
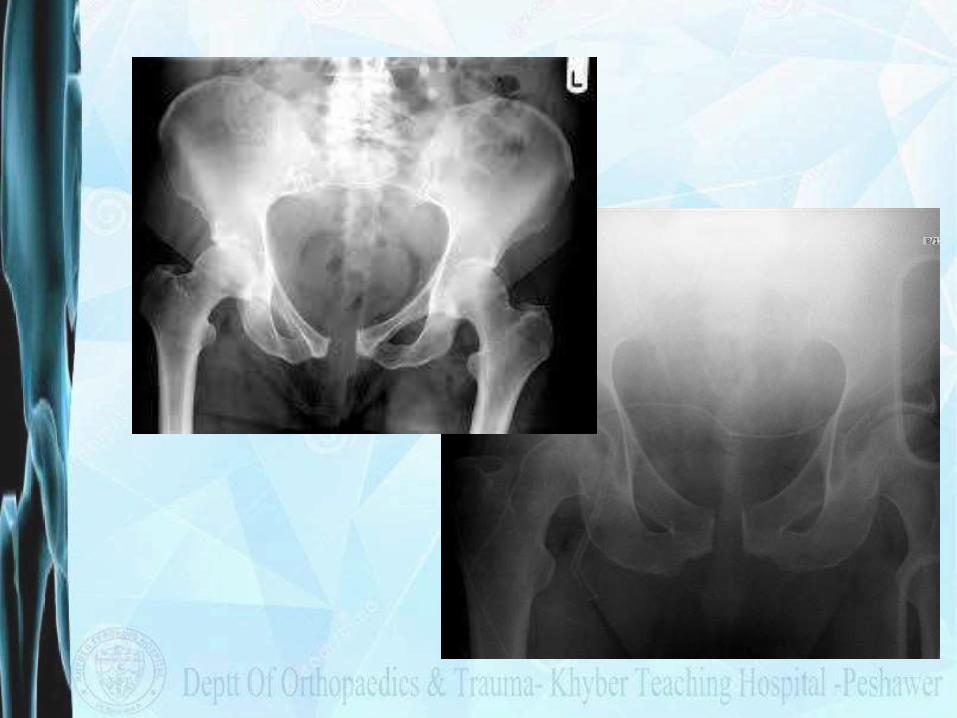
Tile type B1- Open Book Injury(External Rotation Injury)
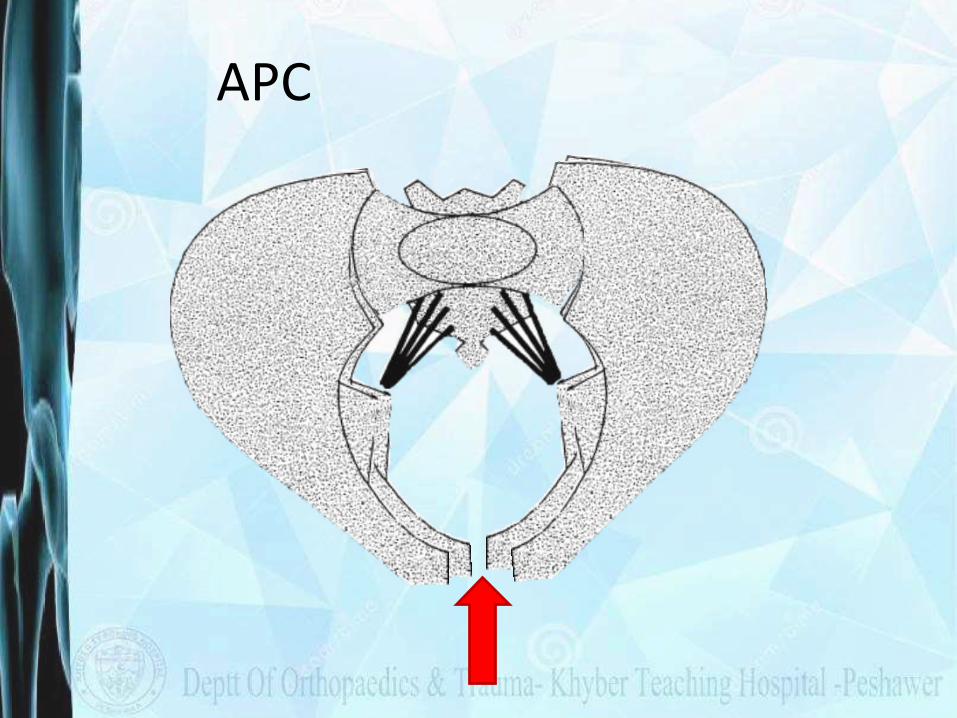
APC
B2- Lateral Compression Injury
B2: lateral compression injury (internal rotation)
B2-1: with anterior ring rotation/displacement through ipsilateral rami
B2-2: with anterior ring rotation/displacement through contralateral rami (bucket-handle injury)
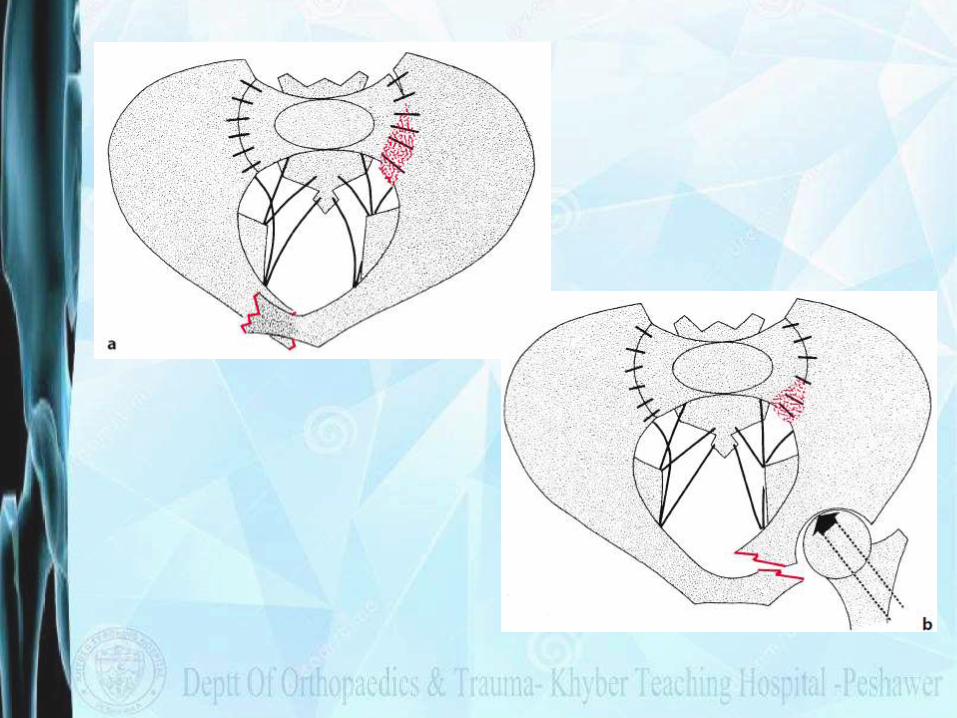

B2: lateral compression injury (internal rotation)
B2-1: Ipsilateral Ant/Post Injuries
B2-2-Contralateral Ant/Post Injuries (bucket-handle injury)
B2.1 B2.2

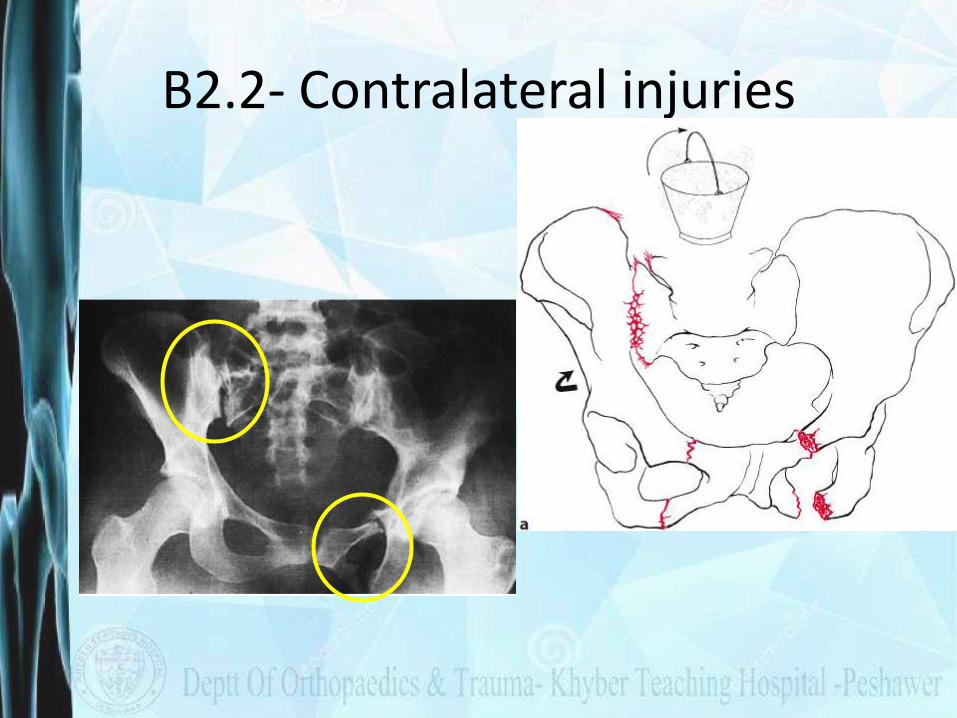
B2.2- Contralateral injuries

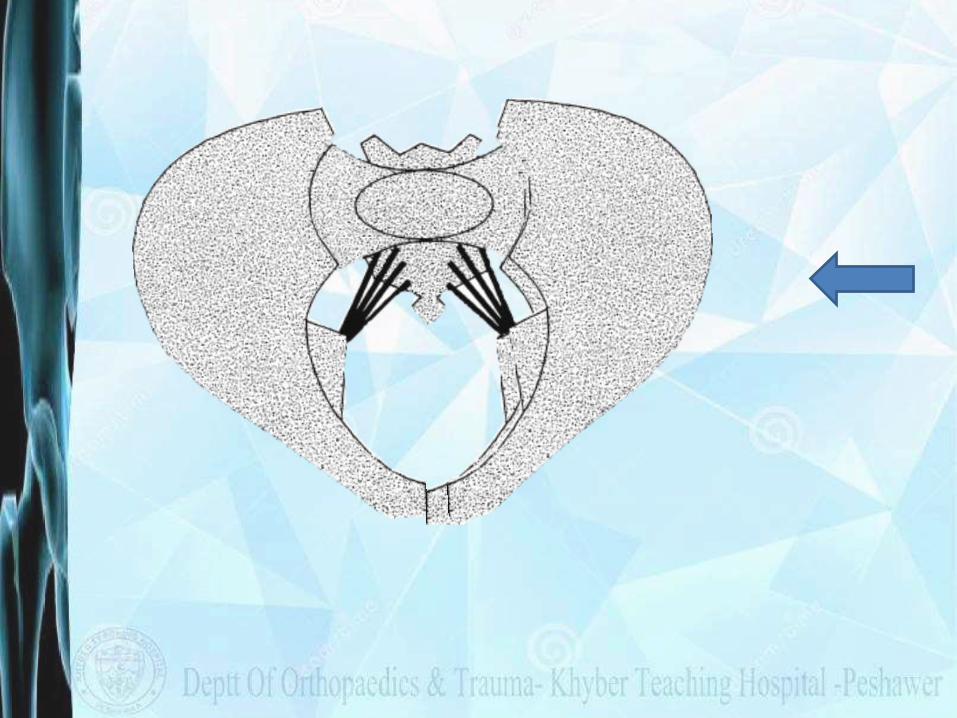
B3- Bilateral
The B3 bilateral injuries can be bilateral open book type One side B1 and one side B2 or Bilateral B2 .
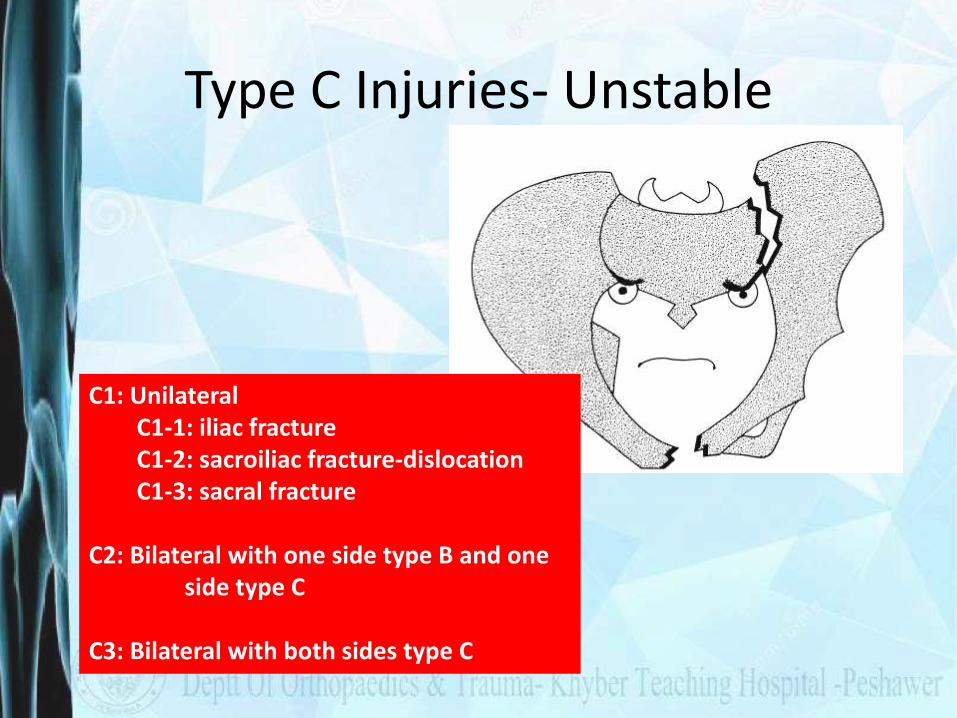
Type C Injuries- Unstable
C1: UnilateralC1-1: iliac fractureC1-2: sacroiliac fracture-dislocationC1-3: sacral fracture
C2: Bilateral with one side type B and one side type C
C3: Bilateral with both sides type C
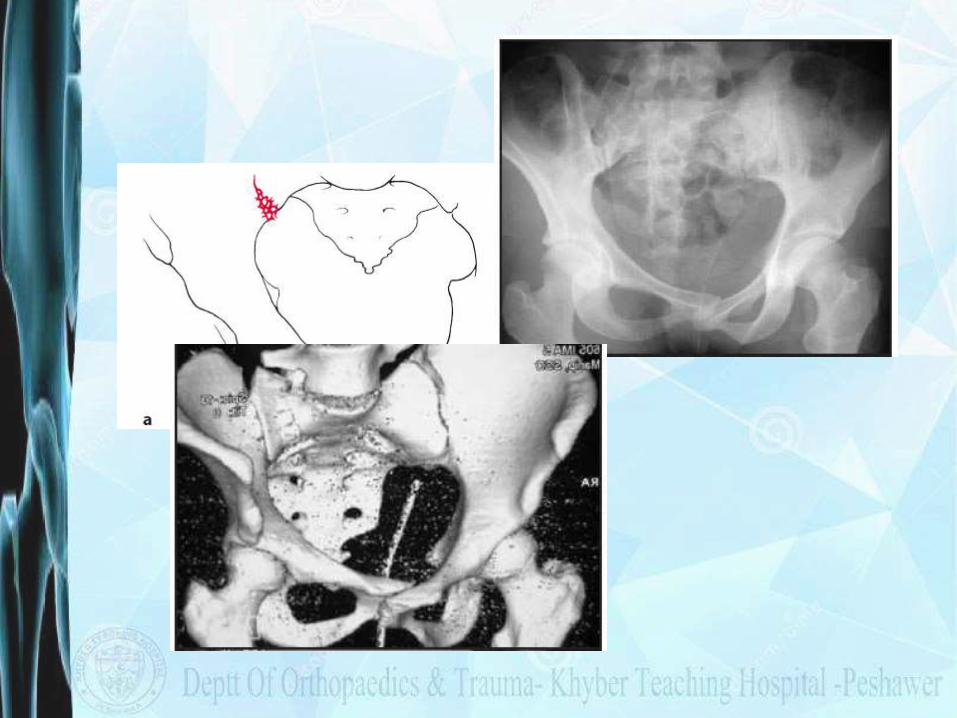
C1- Unilateral Injuries
C1: UnilateralC1-1: iliac fractureC1-2: sacroiliac fracture-dislocationC1-3: sacral fracture


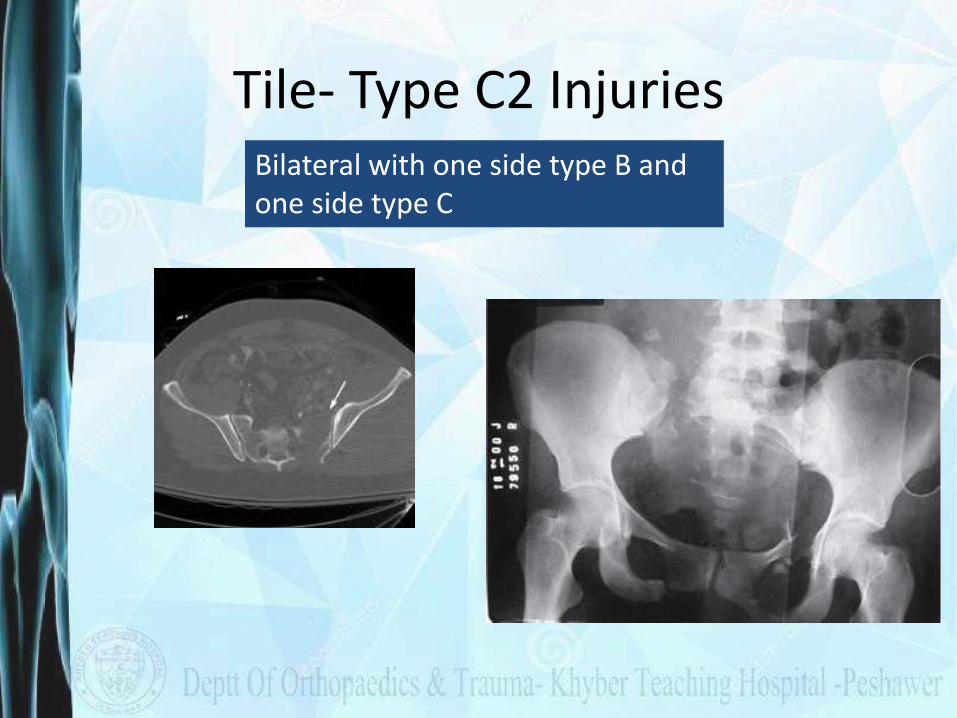
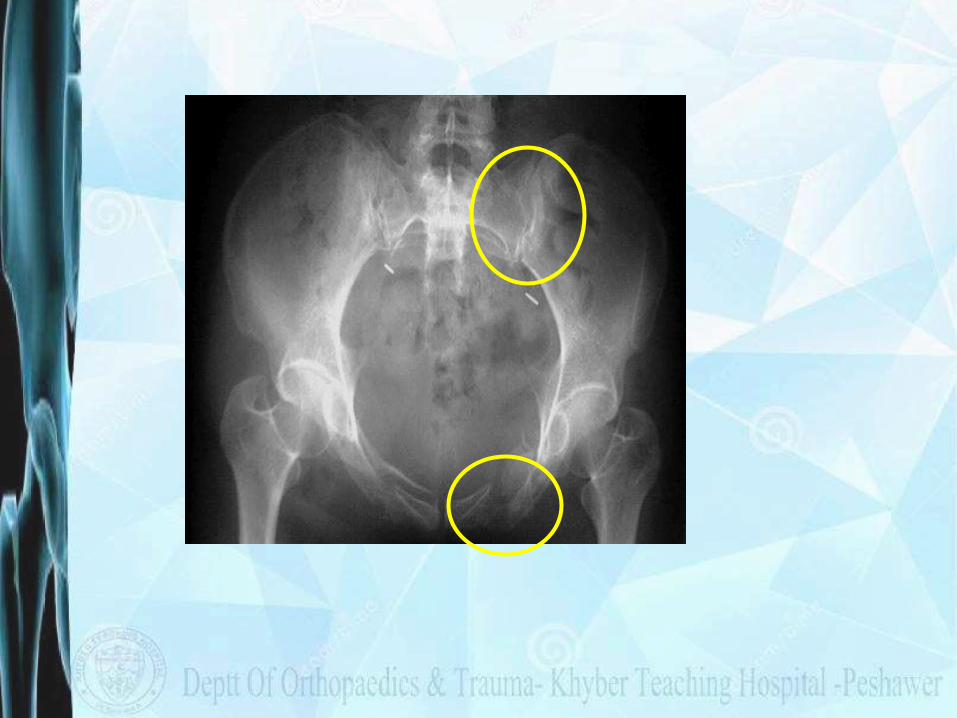
Tile- Type C2 InjuriesBilateral with one side type B and one side type C
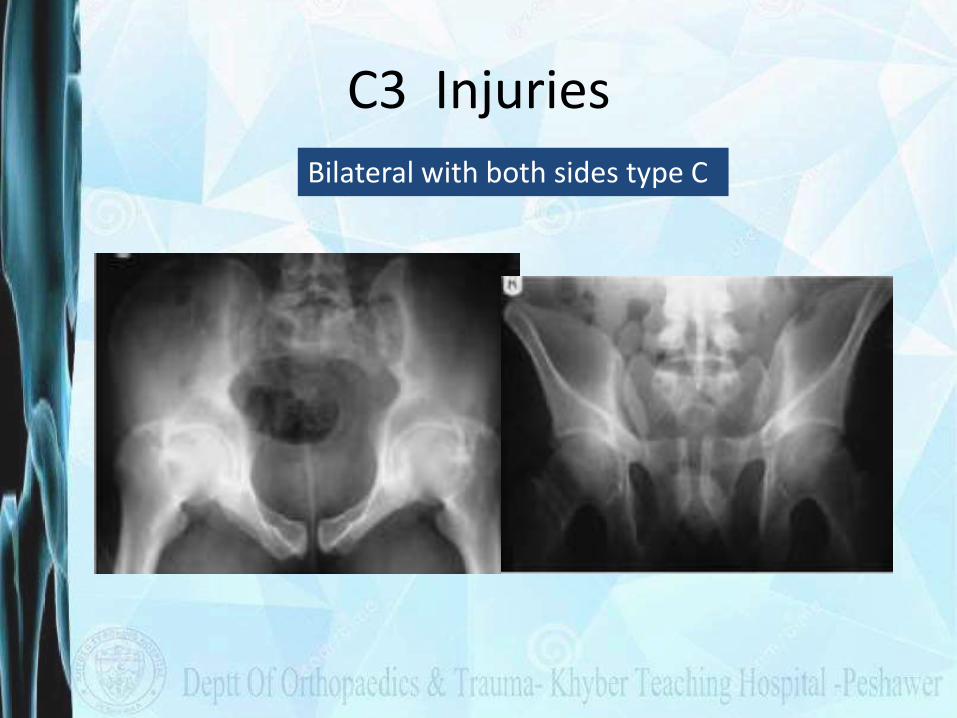
C3 Injuries
Bilateral with both sides type C

Young and Burgess Classification
• Based on the direction of forces causing fracture, associated instability of pelvis
• Original Work of Pennal
Young JW, Burgess AR, Brumback RJ, Poka A. Pelvic fractures: Value of plain radiography in early assessment and management. Radiology 1986;160:445-51.
Burgess AR, Eastridge BJ, Young JW, et al. Pelvic ring disruptions: effective classification system and treatment protocols. J Trauma. Jul 1990;30(7):848-56.
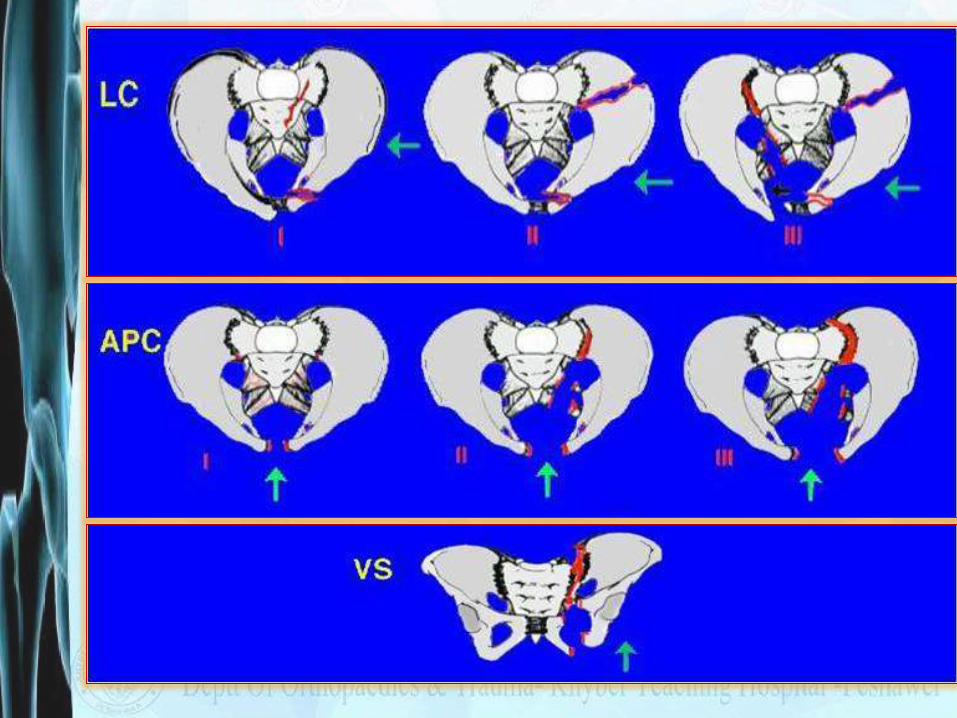
Young and Burgess classification
• Four Injury Patterns
• Lateral compression (LC)
• Anteroposterior compression (APC) (external rotation)
• Vertical shear (VS)
• Combined Mechanism (CM)
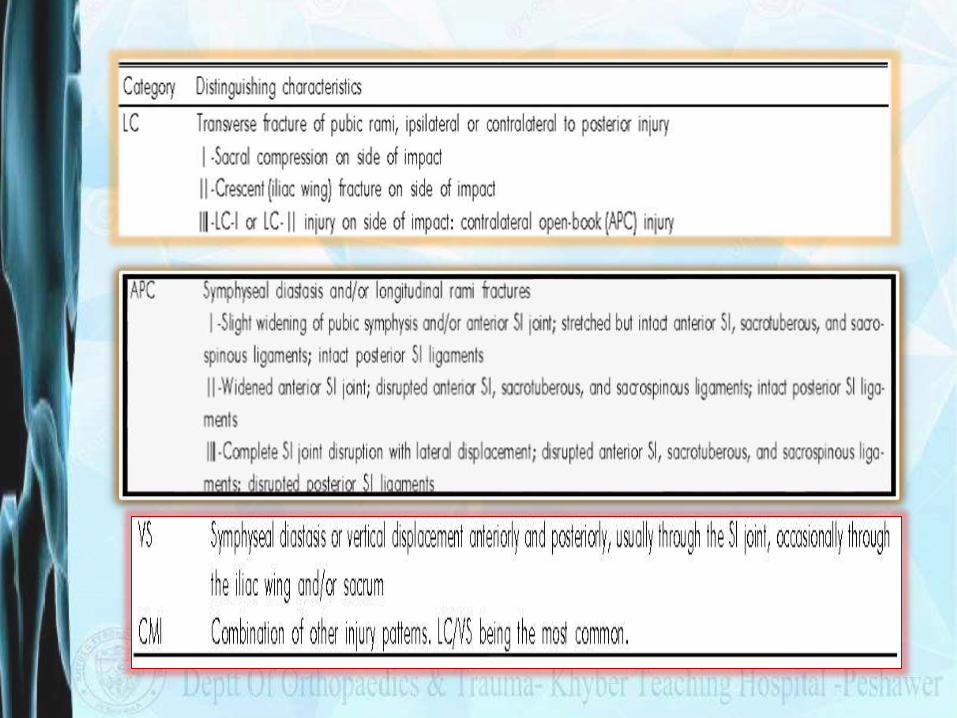
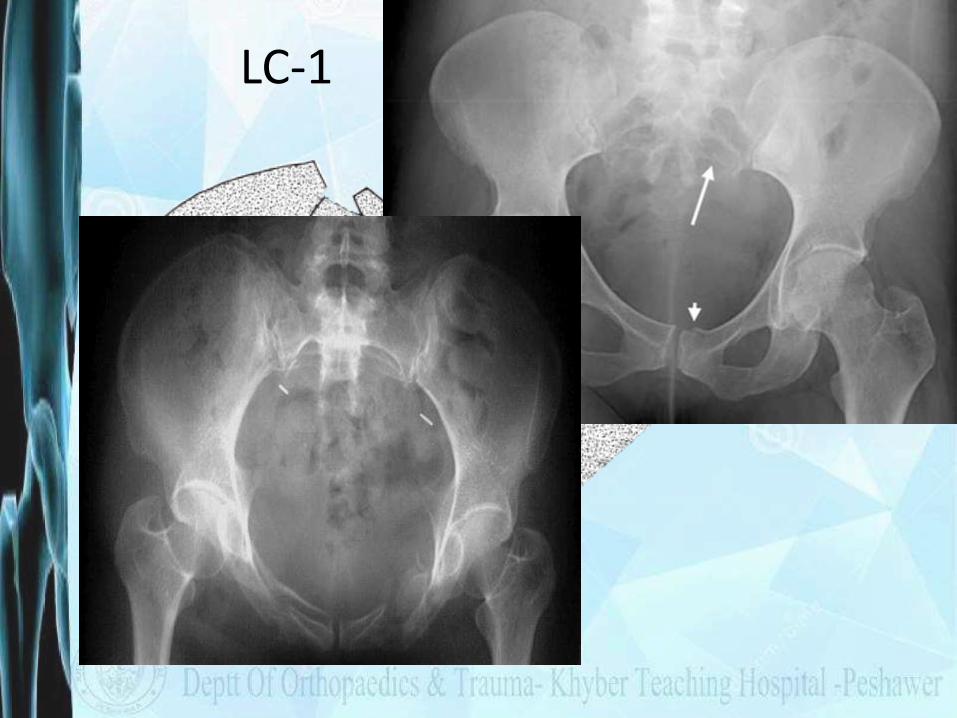
LC-1
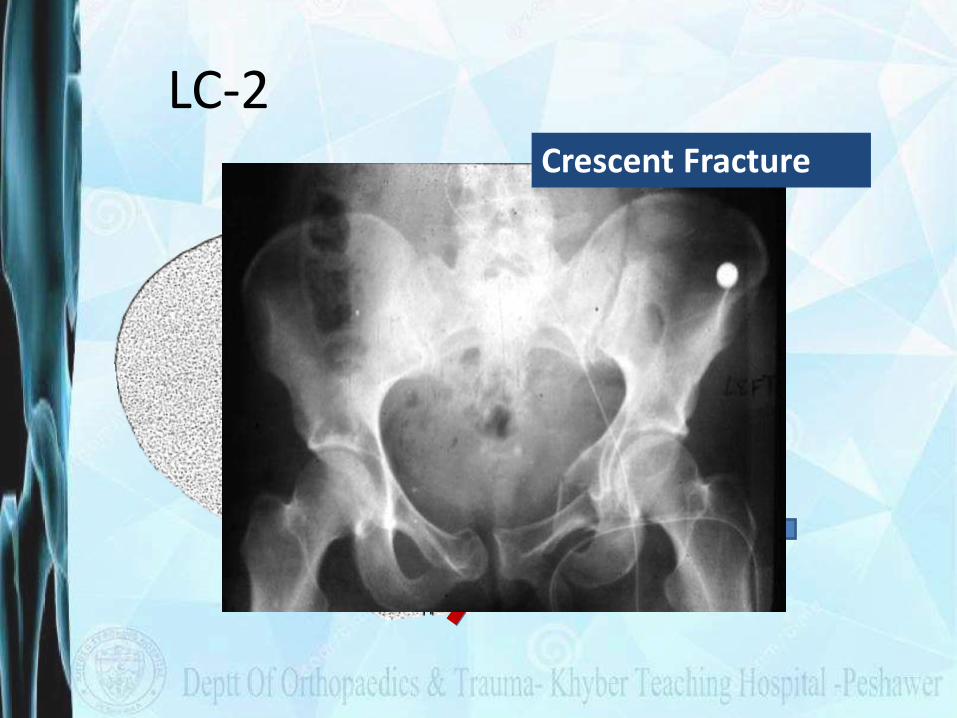
LC-2Crescent Fracture
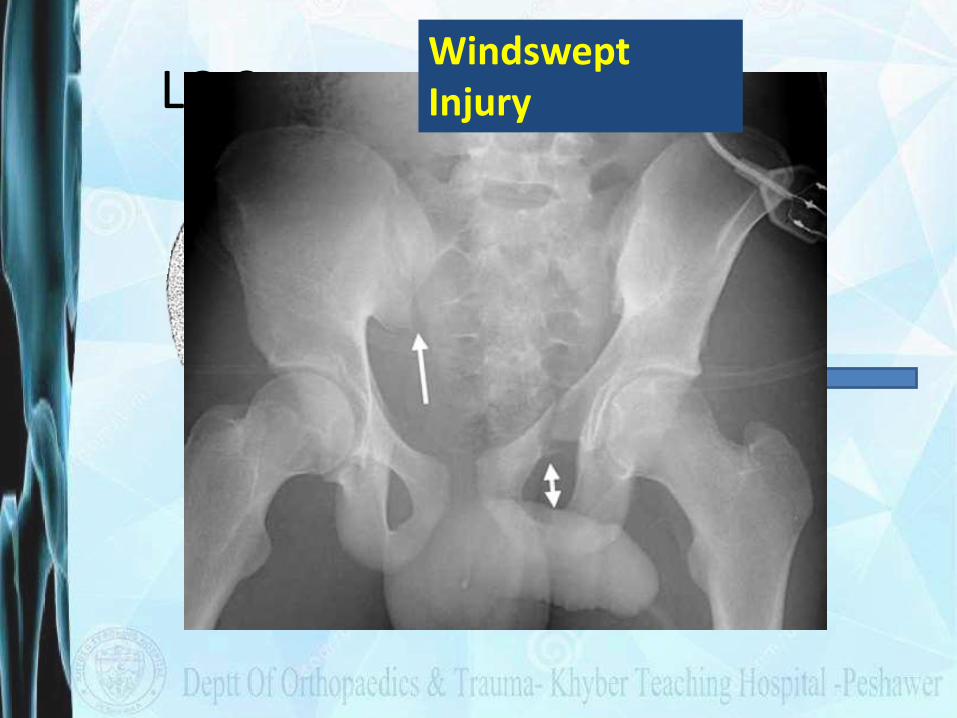
LC-3Windswept Injury
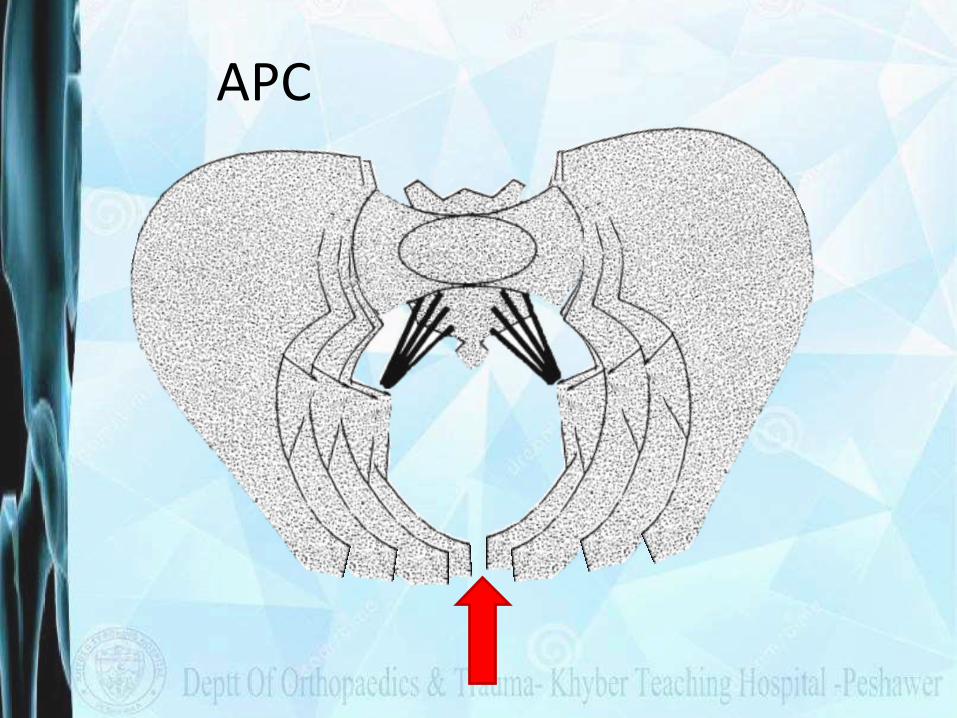
APC
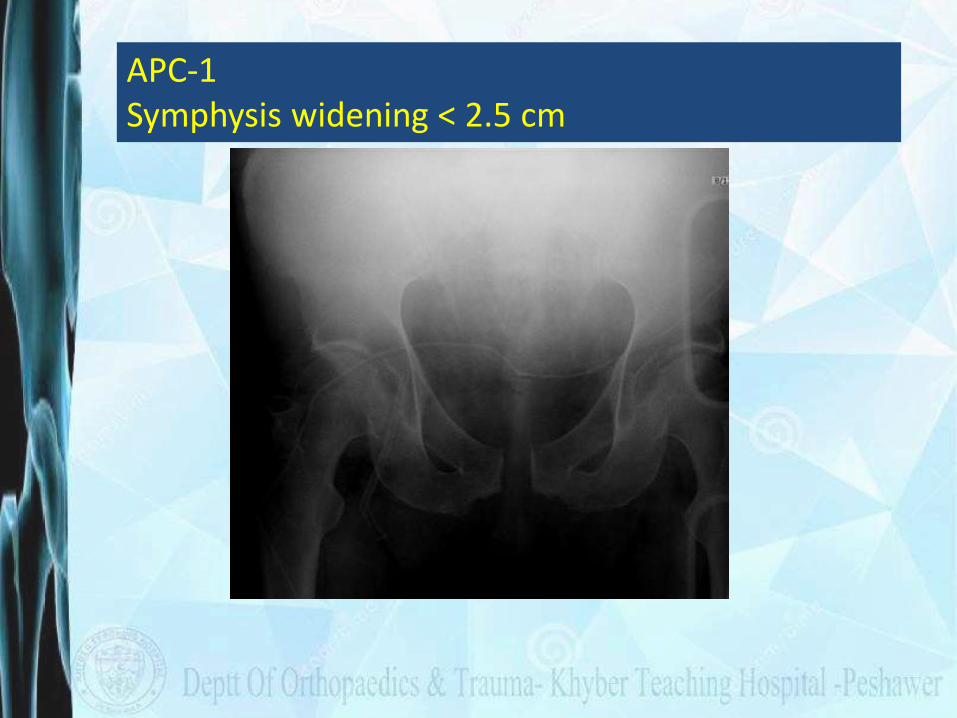
APC-1Symphysis widening < 2.5 cm

APC-2
Symphysis widening > 2.5 cm. Anterior SI joint diastasis .
Posterior SI ligaments intact. Disruption of sacrospinous
and sacrotuberous lig
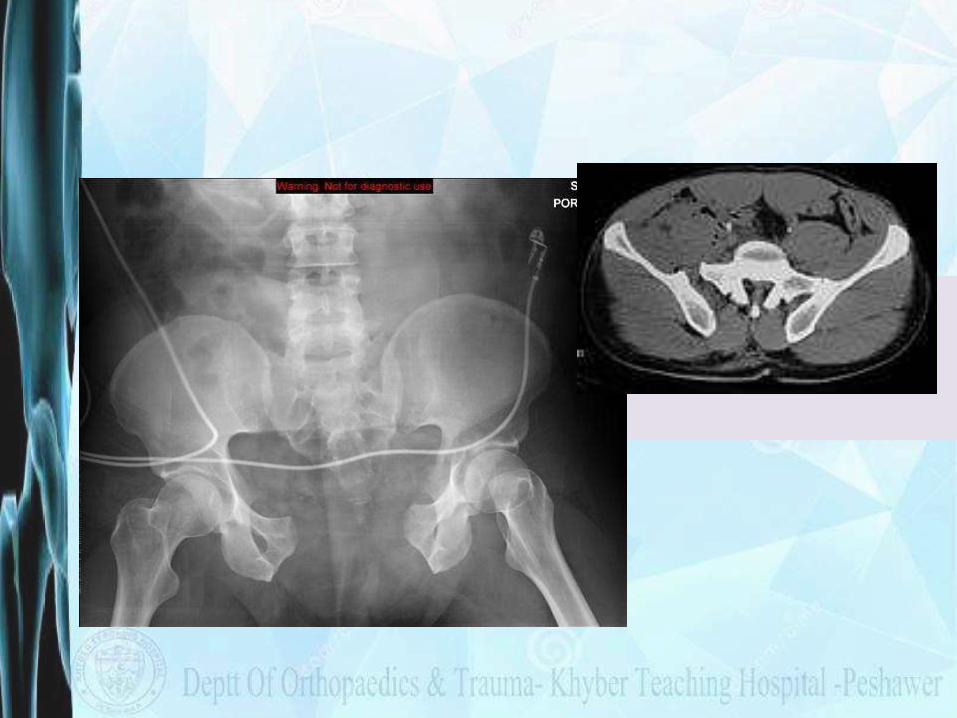
APC-3Disruption of anterior and posterior SI ligaments (SI dislocation). Disruption of sacrospinous and sacrotuberousligaments.
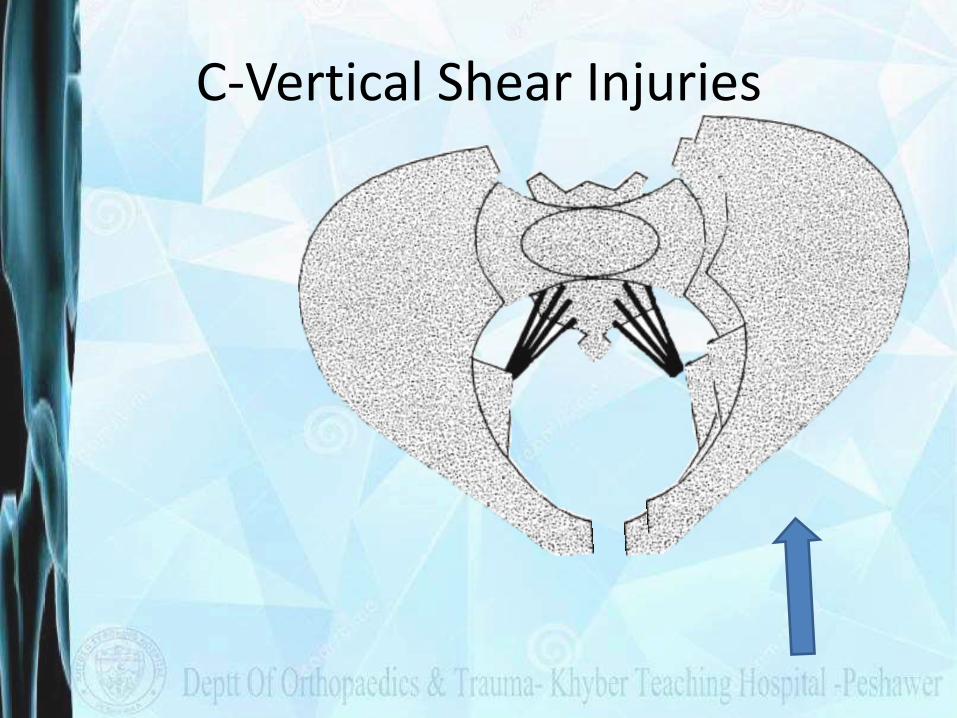
C-Vertical Shear Injuries

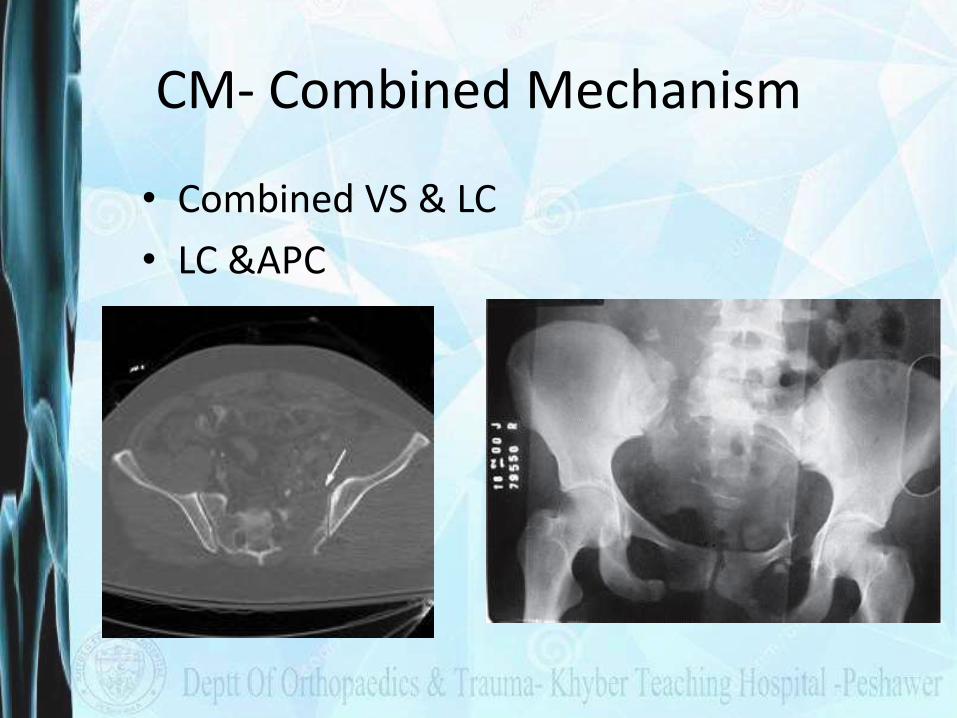
CM- Combined Mechanism
• Combined VS & LC
• LC &APC
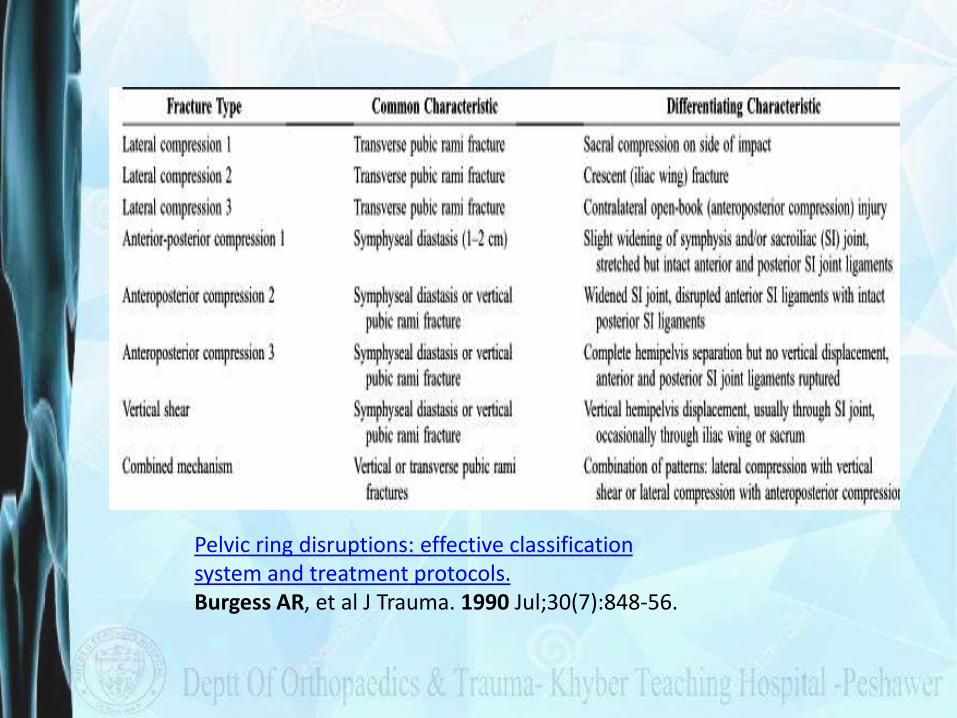
Pelvic ring disruptions: effective classification system and treatment protocols.Burgess AR, et al J Trauma. 1990 Jul;30(7):848-56.

Which one is better ???
• Easily reproducible
• Inter observor Agreement
• Relationship to prognosis/treatment
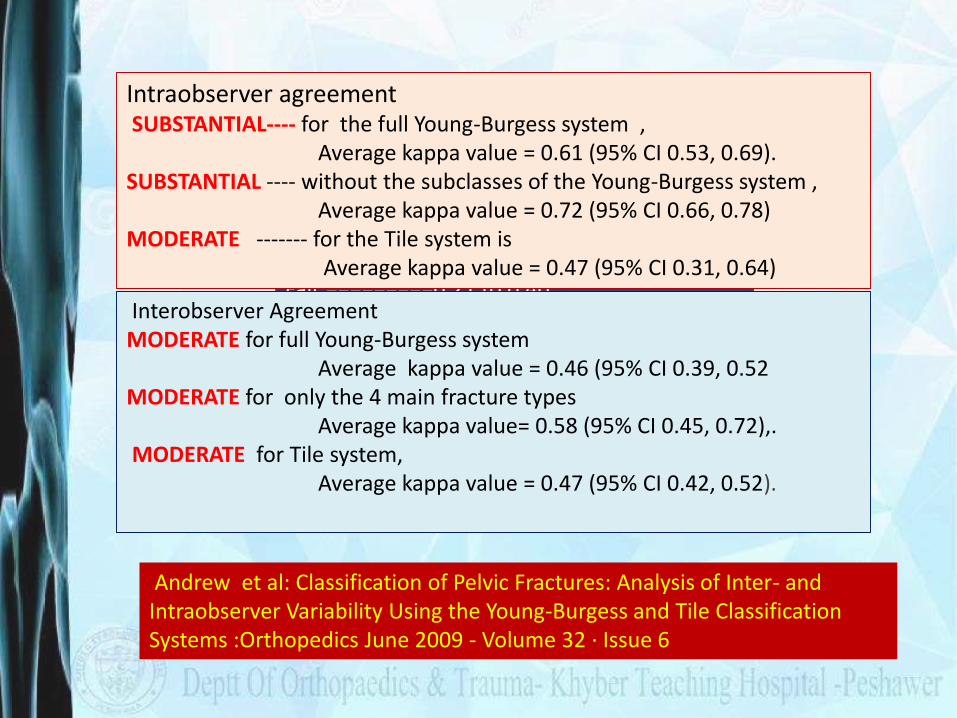
Kappa values ( Agreement grades)Poor ======= =0 to 0.20 ,Fair =========0.21 to 0.40 , Moderate ====0.41 to 0.60 Substantial ===0.61 to 0.80 Perfect ====== >0.80
Intraobserver agreement SUBSTANTIAL---- for the full Young-Burgess system ,
Average kappa value = 0.61 (95% CI 0.53, 0.69). SUBSTANTIAL ---- without the subclasses of the Young-Burgess system ,
Average kappa value = 0.72 (95% CI 0.66, 0.78)MODERATE ------- for the Tile system is
Average kappa value = 0.47 (95% CI 0.31, 0.64)
Andrew et al: Classification of Pelvic Fractures: Analysis of Inter- and Intraobserver Variability Using the Young-Burgess and Tile Classification Systems :Orthopedics June 2009 - Volume 32 · Issue 6
Interobserver AgreementMODERATE for full Young-Burgess system
Average kappa value = 0.46 (95% CI 0.39, 0.52MODERATE for only the 4 main fracture types
Average kappa value= 0.58 (95% CI 0.45, 0.72),.MODERATE for Tile system,
Average kappa value = 0.47 (95% CI 0.42, 0.52).
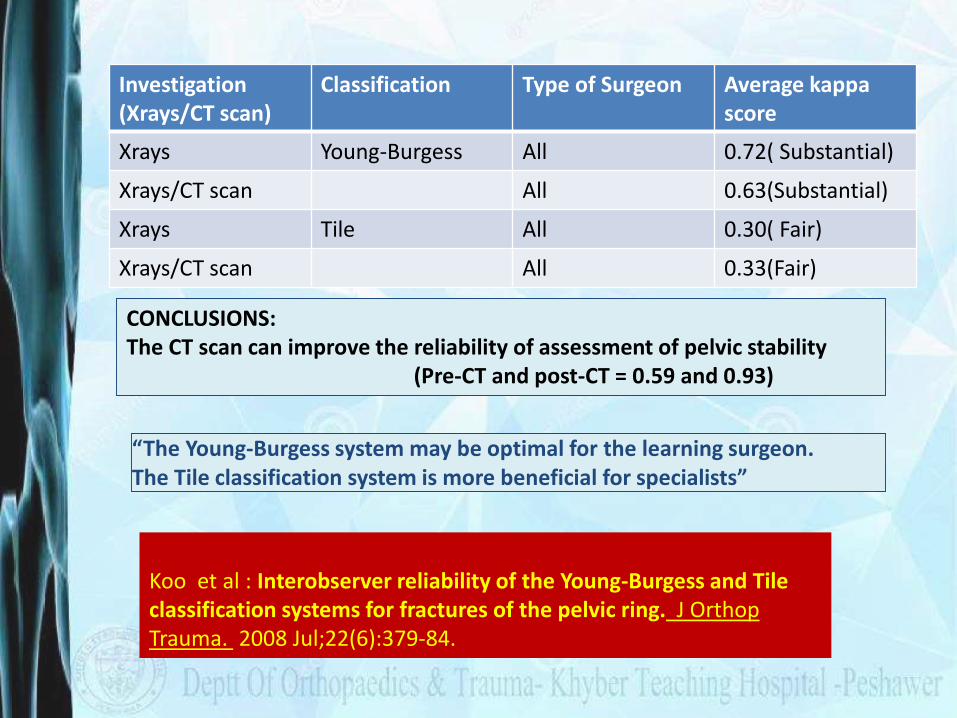
Koo et al : Interobserver reliability of the Young-Burgess and Tile classification systems for fractures of the pelvic ring. J OrthopTrauma. 2008 Jul;22(6):379-84.
CONCLUSIONS:The CT scan can improve the reliability of assessment of pelvic stability
(Pre-CT and post-CT = 0.59 and 0.93)
Investigation (Xrays/CT scan)
Classification Type of Surgeon Average kappa score
Xrays Young-Burgess All 0.72( Substantial)
Xrays/CT scan All 0.63(Substantial)
Xrays Tile All 0.30( Fair)
Xrays/CT scan All 0.33(Fair)
“The Young-Burgess system may be optimal for the learning surgeon. The Tile classification system is more beneficial for specialists”
Osterhoff et al : Comparing the predictive value of the pelvic ring injury classification systems by Tile and by Young and Burgess. Injury 2014 Apr;45(4):742-7
Conclusions“In this first direct comparison of both classifications, we found no clinical relevant differences with regard to their predictive value on mortality, transfusion/infusion requirement and concomitant injuries.”
Predictive Value ???
Guthrie HC, Owens RW, Bircher MD.Fractures of the pelvis: J Bone Joint Surg Br. 2010
Nov;92(11):1481-8
“We recommend using the Young and Burgess classification which is derived from the initial anteroposterior (AP) radiograph and is based predominantly on the mechanism of injury and severity of pelvic fracture.”
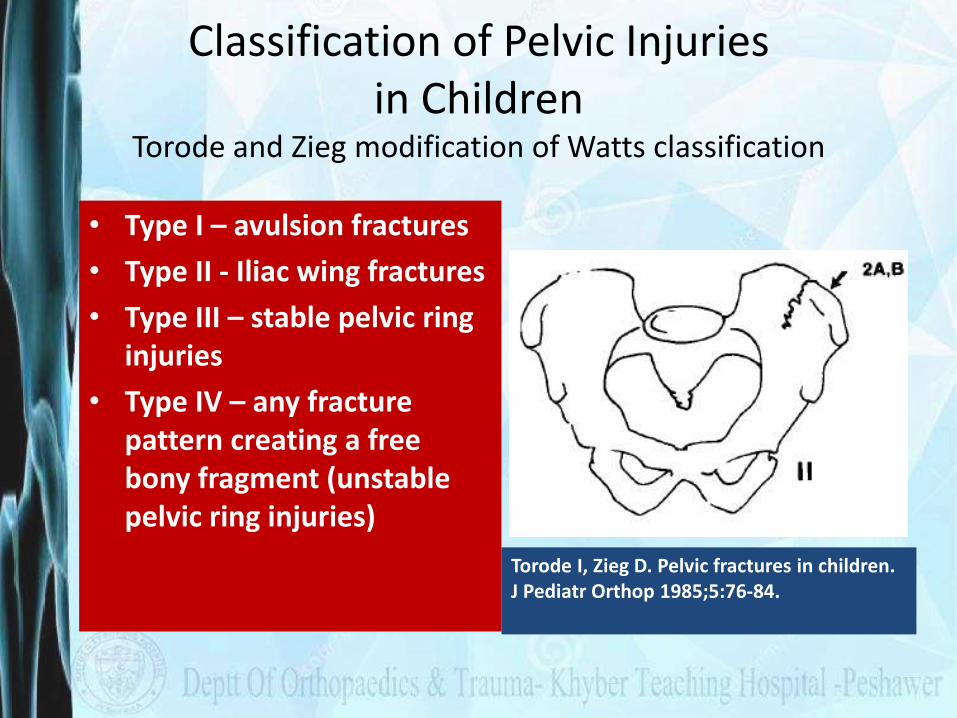
Classification of Pelvic Injuries in Children
Torode and Zieg modification of Watts classification
• Type I – avulsion fractures
• Type II - Iliac wing fractures
• Type III – stable pelvic ring injuries
• Type IV – any fracture pattern creating a free bony fragment (unstable pelvic ring injuries)
Torode I, Zieg D. Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84.
Open pelvic fractures
Accounting for 2% to 4% of all pelvic ring fractures. High rate of mortality (25–50%) and significant morbidity
An open pelvic fracture is defined by a communication to lesions of the integument or the gastrointestinal and urogenital tracts.
Class 1: Stable open pelvic ring fractures (low mortality)
Class 2: Unstable open pelvic ring fractures without rectal injury (about 33% mortality)
Class 3: Unstable open pelvic ring fractures in combination with rectal injury (upto 50% mortality)
Jones Classification for Open Pelvic Fractures
Jones AL, Powell JN, Kellam JF, et al. Open pelvic fractures: a multicenter retrospective analysis. Orthop Clin North Am 1997; 28:345–350.
Bircher and Hargrove Classification of Open Pelvic Fractures
Soft tissue injury was divided into three main alphanumerical categories, which were assigned to Tile’s classification of pelvic ring fractures. Subsets were defined by the primary skin lesion and associated soft tissue damage.
Bircher M, Hargrove R. Is it possible to classify open fractures of the pelvis? Eur J Trauma 2004; 30:74–79.
Bircher and Hargrove Classification of Open Pelvic Fractures
Type A1: Penetrating trauma, for example, by a bullet. Tile/AO type A fracture.
Type A2: “Outside in” injury of the iliac crest, with minimal soft tissue damage.Tile/AO type A fracture.
Type A3: “Outside in” injury of the iliac crest, with extensive soft tissue damagerequiring surgery for soft tissue coverage. Tile/AO type A fracture.
Type B1: “Inside out” injury caused by lateral compression and showing littleexternal damage but possible injury to the genitourinary system (i.e., tiltfracture). Tile/AO type B2 fracture (LC).
Type B2: “Inside out” injury, caused by lateral compression and representingmoderate tissue damage. An example would be a rotationally unstablepelvic fracture in combination with extensive degloving (Morel–Lavalle´syndrome). Tile/AO type B2 fracture (LC).
Type B3: “Perineal split” following APC injury. Tile/AO type B1 fracture (“openbook”).

Type C1: “Perineal split” and/or “sacral shear/split” injury with moderate toextensive skin loss, complete genitourinary disruption, and rectal lesionswith subsequent fecal contamination. Tile/AO type C fracture.
Type C2: “Hemipelvic destabilization” injury with severe tissue damage, complete urogenital and bowel injury combined with extensive contamination of all tissue layers. Tile/AO type C fracture.
Type C3: “Pelvic crush” with bilateral complex pelvic instability and massivedamage to soft tissues and intrapelvic organs. Tile/AO type C fracture.
Soft tissue injury was divided into three main alphanumerical categories, which were assigned to Tile’s classification of pelvic ring fractures. Subsets were defined by the primary skin lesion and associated soft tissue damage.
Bircher M, Hargrove R. Is it possible to classify open fractures of the pelvis? Eur J Trauma 2004; 30:74–79.
Summary
• Tile and Burgess & Young Classifications are the most commonly used classifications
• Burgess & Young seems to be more easily remembered and reproduced
• The prognostic values of both are comparable
• Certain fractures may not be classifiable in either systems

Thanks for your attention !!!