Embed Size (px)
Citation preview

South TynesideIntegrated Community Teams
3rd March 2015


South Tyneside - Who are weOver reliance on
hospital services Population 150,000
28 GP Practices
1 Foundation Trust
1 Local Authority
Growing elderly
population
Clinical
Variation
Fragmented
Services
Risk
taking
behaviour
Poor
Mental
Health

Integration Principles
We will impose a person
perspective throughout our
work
We will manage the organisational consequences of
being person-centred
Our staff will not automatically
reach for traditional solutions
We will develop our staff jointly, not separately
“I can promote my own health and wellbeing by planning my care & support with people who work together to understand
me and my carers, allow me control and bring together services to achieve the outcomes important to me”
Our vision for integration

Aim of Integrated Community Teams
The vision is to develop existing community services into integrated locality teams providing
joined up health and social care support to residents of South Tyneside

To have services delivered slickly around the needs of the patient

Current provision
Many different teams, individuals and providers delivering a range of health & social care tasks
Mental health Palliative care
Diagnostics
Therapy/Equipment
Assessment
LTC Management
Social and personal care
Medication
Welfare rights
Nursing care
Dietetics
Moving and handling
Complex wound management
SALT
Housing
Acute Care team

Current provision
• Workforce capacity;
– 150 WTE Community Nurses
– 11 Home Care Providers
– 60 WTE Social Care Staff
– 28 GP Practices
• Hand offs, fragmentation, duplication, limited information sharing
• Opportunity to improve patient experience

Patient & Partner
GP
Cons. Memory
Cons. Geriatrician
DN
CM
ICTACT
SW
Care Provider
Age UK
Alzheimer's Society
What is integration?
• ADD SAMS STORY

So what are we doing about this?• We have a model – eventually!
• Prototyped it for 3 months involving 3 GP practice populations in Hebburn
• Scaling up to 9 practices in Jarrow and Hebburn in March
• We are continually developing the model, bringing in more services over time and increasing the services provided by the team
• We are committed to action learning and developing the model together!

West hubHebburn/Jarrow
East hubSouth Shields
No. of delivery
teams TBC
South hubWhitburn/
Cleadon/Boldon
Prototype
Phased Implementation
Delivery Team 1
Hebburn
Delivery Team 2 Jarrow
Practices (See below)
Practices
Delivery Team 1
The Park
Ellison View
The Glen
No. of Practices TBC
No. of Practices TBC
No. of delivery
teams TBC
In place from
17th
November
2014
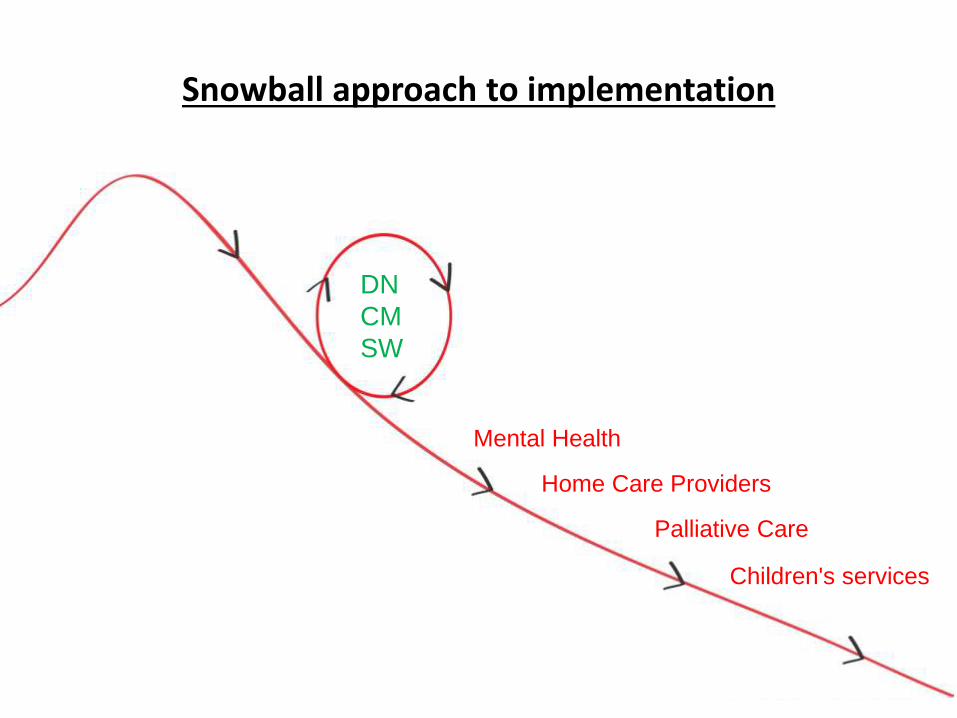
Snowball approach to implementation
DN
CM
SW
Mental Health
Home Care Providers
Palliative Care
Children's services

Patient & Partner
GP
Cons. Memory
Cons. Geriatrician
ICT
ACT
Care Provider
Age UK
Alzheimer's Society
Patient & partner now have just 2 main points of contact as the Care Coordinator delivers, manages and liaises with the community services, and the GP role is strengthened through these streamlined relationships
Integrated Team – Care Coordinator

Social Worker
Social Navigator
District Nurse
GP
District Nurse
Community Matron

Patient Stories: Community Matron

Day 1- 17th November
• Prevent duplication of services!
• Information sharing
• Clinical handover
• Practicalities
– Duty board
• Blurring of the roles

Pre Go-Live Guide• Pre –meet and greet• Case load identification, transfer, allocation and
identification of care coordinator• Access to the building!
– Swipe cards
• Access to IT – Access to STFT log on– Hardware– Software (SWIFT)– Printers
• Office set up– Integrated seating– Duty Board

Post Go-Live Guide
• Information sharing processes remains ongoing
• Ways of working with practices– Integrated approach to MDTs
• Establish regular structured hub meeting
• Captured lessons learnt
• Develop Skill matrix
• Consider OD offer (staff led!)

Patient storiesDistrict Nurse
Pre integration Patient story
Not integrated!Fragmented care & communicationTime delays in referral processIndirect referrals
38 year old ladyMultiple health and social care needs
Post integration Patient story
Direct referral processJoined up serviceJoint visits/reduction in visits Information sharingBlurring of roles/crossing organisational boundariesOne stop shop for patientsImproved patient outcomes
81 year old gentlemanMultiple LTCs and social care needs

Patient stories
Social workerPre integration Patient story
Unable to accept direct referralsReferrals going outside of the ICTInformation gathering
82 year old gentlemanDementia
Post integration Patient story
Information sharingAble to accept internal referralsCompletion of joint visits
80 year old gentlemanLung CA

Impact of integrated teams
• The impact of the prototype team is being measured in the following key areas:
Service user and carer experience
GP and staff satisfaction
Reliance on hospital and residential services
Team operational metrics (e.g. no and types of visits, inter-team referrals etc)

Our journey
• NHSIQ support
Workshop facilitation: getting our partners working together
Support to generate whole system commitment to the change process
Practical tools and techniques
Guided the local team through the journey from inception to implementation through a bottom-up approach
• The highs
Genuine partnership working
Focus on improving services for patients
Enthusiasm from front line delivery teams
GP practices have wanted small local teams aligned to them for years
Bottom-up approach from all disciplines and skill mixes
Voluntary Sector part of core teams
Going live!
Our journey

• The challenges
Significant work between workshops
Large resource commitment
Overcoming organisational boundaries
Small operational issues having a big impact

1. Commit operational and managerial time to the change process from all organisations – don’t underestimate this
2. Understand the power of actual patient voices and examples of the care they are experiencing pre and post change
3. Make sure that teams and GP practices have funded time out to learn, input and ultimately own the model
Our journey Reflections and Top Tips

4. Importance of going through the journey not jumping to the conclusion – support from NHSIQ invaluable
5. Don’t let IT and system incompatibility get in the way. Think of practical ways to work round it. The IT can catch up over time and it’s not a deal breaker

Final message from the team…
Remember why we’re doing this:
– It’s better for the patient!
– It’s better for the professionals!
– Its just better!!
• We have one Team of professionals meeting the needs of a practice population
• Embrace Change
• All Issues have Solutions !





























