Embed Size (px)
Citation preview

الرحيم الرحمن الله بسم

Hypertension and Kidney
Dr. Ramadan Arafa; MSc, MRCPI, PG Dip DM (Leicester, UK)Specialist A Physician; Fujairah Hospital


Objectives • BP control and role of the kidney
• Epidemiology of HTN
• Epidemiology of CKD
• Effect of hypertension in the kidney
• Effect of CKD on BP
• BP targets in CKD
• Anti-HTN medications and possible side effects of the kidney
• Take home message

Normal Blood Pressure Control

Indian J Endocrinol Metab. 2011 Oct; 15(Suppl4): S281–S288.
BP control
Local mechanisms
Acute VDAcute VC
Ch. VDCh. VC
Global neural mechanisms
C.O.PA.N.S
Renal – endocrine
system

Regulation of blood pressure
• Short-term changes in BP are regulated by SNS and RAAS
• Long-term BP control is controlled by the kidney.
• Sympathetic regulation also plays a role in long-term BP regulation
• The most important stimulus to renin release in the juxtaglomerular
apparatus is through renal sympathetic nerves.

• High pressure baroreceptors in the carotid sinus and aortic arch
respond to acute elevations in systemic BP by causing a reflex vagal
bradycardia and inhibition of sympathetic output from the CNS.
• Low pressure cardio pulmonary receptors in the atria and ventricles
likewise respond to increases in atrial filling by causing tachycardia,
increasing ANP release and inhibiting vasopressin release.


Rossier BC et al. Physiological Reviews Jan 2015, 95 (1) 297-340
GHTSH
ACTH


Objectives • BP control and role of the kidney
• Epidemiology of HTN
• Epidemiology of CKD
• Effect of hypertension in the kidney
• Effect of CKD on BP
• BP targets in CKD
• Anti-HTN medications and possible side effects of the kidney
• Take home message

• Globally, the overall prevalence of HTN in adults aged > 18 around 22% in
2014.
• It is highest in Africa, where it was 30% for both sexes combined as well as for
men and women separately.
• The lowest prevalence of HTN was in Americas at 18% for both sexes (21% for
men and 16% for women).
• In all WHO regions, men have slightly higher prevalence of HTN than women.
• The prevalence of HTN was higher in low-income countries compared to
middle-income and high-income countries.WHO, Global Health Observatory Data 2014

High Blood Pressure in the United States
• About 70 million American adults (29%) have high blood pressure.
• About 1 in 3 American adults has prehypertension.
• Only 52% of people with high BP have their condition under control.
• High BP was a primary or contributing cause of death for more
than 360,000 Americans in 2013—that's nearly 1,000 deaths each
day.
• High BP costs the nation $46 billion each year.



Epidemiology of HTN according to country income
Income Level of Country
No. (%) of Participants
Overall Aware Treated ControlledProportion With
BP<140/90 mm Hg Among Those Receiving Treatment
HIC 6263 49 46.7 19 1189 (40.7)UMIC 18 123 52.5 48.3 15.6 2833 (32.3)LMIC 23 269 43.6 36.9 9.9 2314 (26.9)LIC 10 185 40.8 31.7 12.7 1298 (40.2)All included countries 57 840 46.5 40.6 13.2 7634 (32.5)
Chow et al. JAMA. 2013;310:959–968.

UAE in 2009
Dubai Household Health Survey 2009

Dubai Household Health Survey 2009

both sexes female male
24.321.5
25.526.323.3
27.5
Hypertension in UAE in 2010 and 2014
2014 2010 http://apps.who.int/gho/data

USA Canada Egypt Algeria KSA Oman Qatar Kuwait Iraq UAE SumaliaMauritania
15.9 15.7
25.628.1 28 27 27
29.1 2825.5
34 35
Hypertension in other countries

Objectives • BP control and role of the kidney
• Epidemiology of HTN
• Epidemiology of CKD
• Effect of hypertension in the kidney
• Effect of CKD on BP
• BP targets in CKD
• Anti-HTN medications and possible side effects of the kidney
• Take home message

Chronic Kidney Disease (CKD)• CKD is defined as abnormalities of kidney structure or function, present for > 3
months, with implications for health. Criteria for CKD (either of the following present for > 3 months)
KDIGO guidelines 2012
Markers of kidney damage (one or more)
Albuminuria (AER > 30 mg /24h, ACR > 30 mg/gm or 3mg/mmol
Urine sediments abnormalities
Electrolytes and other abnormalities due to tubular disorders
Abnormalities detected by histology
Structural abnormalities detected by imaging
History of kidney transplantation
Decreased GFR GFR < 60 ml/min/1.73 m2


New Cases of renal failure by Primary Diagnosis-2011
United States Renal Data System

34
58
13
16 15

6.411
23
49
15.6

13.5
15.914.7

Prevalence of CKD by CKD Stage and YearYear unmeasured eGFR 90+ CKD II CKD III CKD IV CKD V Dialysis TX
2005 29.39% 16.47% 39.02% 13.62% 0.91% 0.22% 0.23% 0.15%
2006 33.29% 16.84% 35.59% 12.79% 0.85% 0.13% 0.37% 0.14%
2007 25.01% 16.31% 41.69% 15.42% 0.88% 0.12% 0.43% 0.14%
2008 27.77% 18.92% 38.90% 12.92% 0.80% 0.14% 0.40% 0.16%
2009 32.13% 19.63% 35.38% 11.41% 0.77% 0.11% 0.42% 0.15%
2010 33.59% 21.08% 33.37% 10.61% 0.69% 0.11% 0.41% 0.14%
2011 33.93% 21.96% 32.54% 10.24% 0.67% 0.11% 0.41% 0.14%
2012 30.01% 25.04% 33.48% 10.13% 0.68% 0.11% 0.41% 0.14%


• The incidence of CKD is
increasing most rapidly in
people ages 65 and older.
• The incidence of recognized
CKD in people ages 65 and
older more than doubled
between 2000 and 2008.
• The incidence of recognized
CKD among 20- to 64-year-olds
is less than 0.5 %. kidney-disease-statistics-united-states.



Prevalence of other comorbid conditions in SEEK study
Singh et al. BMC Nephrology 2013


Hypertension and Renal Disease

Hypertensive Nephropathy

• The term hypertensive nephrosclerosis has been used to describe a clinical
syndrome characterized by long-term essential HTN, hypertensive
retinopathy, LVH, minimal proteinuria, and progressive renal insufficiency.
• Most of the literature dedicated to hypertensive nephrosclerosis is based
on the assumption that progressive renal failure in a patient with long-
standing HTN, moderate proteinuria, and no evidence suggesting an
alternative diagnosis characterizes hypertensive nephrosclerosis.

• The atherosclerotic, hypertension-related vascular lesions in the
kidney primarily affect the preglomerular arterioles, resulting in
ischemic changes in the glomeruli and postglomerular structures.
• Glomerular injury may also be a consequence of direct damage to
the glomerular capillaries due to glomerular hyperperfusion.
• Glomerular pathology progresses to glomerulosclerosis, and
eventually the renal tubules may also become ischemic and
gradually atrophic.

• The renal lesion associated with malignant hypertension consists of
fibrinoid necrosis of the afferent arterioles, sometimes extending
into the glomerulus, and may result in focal necrosis of the
glomerular tuft.
• Clinically, macroalbuminuria (a random urine ACR >300 mg/g) or
microalbuminuria (a random urine ACR 30–300 mg/g) are early
markers of renal injury. These are also risk factors for renal disease
progression and for cardiovascular disease.

Hypertensive nephrosclerosis

Hypertensive nephrosclerosis (continued)

• The paradoxical results of increasing incidence of renal failure despite
wider antihypertensive drug therapy and reduction in hypertensive target
events, such as stroke and cardiovascular disease, raises questions about
the causal role of hypertension in this disorder.
• Unlike morbidity and mortality of stroke and coronary disease, incident
cases of ESRD attributed to hypertension continue to increase. Some
authors suggest that many of these cases are more likely related to other
factors, including small vessel injury related to aging, diabetes, or obesity -
related kidney injury.Fervenza FC 2015

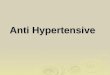
• SBP has strong association with ESRD
• Patients with SBP > 210 mmHg have 22 – fold risk for ESRD compared with
SBP< 120 mmHg
• DBP was a weaker predictor than SBP.
• The relative risk for a 20 mm Hg higher SBP was 2.1 versus 1.5 for DBP.
• There is a graded and continuous relationship between baseline SBP and
risk of ESRD, adjusted for other covariates.
• An 85% to 95% of patients with stage 3-5 CKD have HTN. Klag et al. N Engl J Med. 1996;334:13–18HSU et al. Arch Intern Med.2005;165:923–928Botdorf et al. Cardiorenal Med. 2011;1:183–192.
.

The Relationship Between Pretreatment Systolic Blood Pressure Level and the Subsequent Occurrence of ESRD.
Nat Rev Neph, 2010, Nature Publisher

Genetic predisposition and hypertensive nephropathy• Discovery of an association between MYH9 polymorphisms and kidney disease in 2009
• The current theory purports that MYH9 polymorphisms result in products that disrupt normal
podocyte function, causing podocyte injury, which ultimately leads to glomerulosclerosis.
• The presence of genetic polymorphisms that lead to intrinsic kidney injury suggest that the
failure of strict BP control to prevent CKD progression does not relate to BP alone, but rather
relates to factors intrinsic to the kidney that are yet to be defined.
• This hypothesis might partially explain why blood-pressure control alone cannot reverse
existing kidney damage or stop progressive kidney damage, as was observed in the African
American Study of Kidney Disease (AASK).

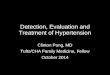
• Presence of stage 3 CKD or higher seems to independently aggravate HTN.
• CKD is associated with impaired function of endogenous vasodilators, increased
sympathetic activity and increased salt retention.
• The ability of the normal kidney to handle variations in dietary sodium intake and sodium
excretion is governed by the pressure-natriuresis curve: increased sodium intake is
associated with increased blood pressure, increased GFR and, ultimately, increased
sodium excretion to match the increased intake of sodium.
• In advanced parenchymal kidney damage, the ability to achieve complete sodium balance
is blunted by the decrease in GFR. Thus, the pressure-natriuresis curve shifts to the left
and sodium balance is only achieved at the expense of an increase in blood pressure.


Nat Rev Neph. 2010@ Nature Publishing

• Benign nephrosclerosis.
• Majority of cases
• Slow progression to renal failure: 1-5% develop ESRD
• Malignant nephrosclerosis.
• Medical emergency.
• Usually complicates malignant HTN
• May present as AKI
• Requires rapid and aggressive intervention to save the kidneyKhawaja Tahir et al / J Biomed Sci and Res., 2010
Varieties of hypertensive nephrosclerosis

Manifestations of hypertensive nephropathy:
1. Frequent urination at night: at least 3 times a night.
2. Changed urine color: dark orange, tea-color and even red.
3. Bubbles in urine.
4. Edema.
5. Hypoproteinemia.
6. Hyperlipidemia

Investigations
(1) Identifying other cardiovascular
risk factors,
(2) Exclude secondary hypertension
(3) Evaluating for evidence of end
organ damage.
A. ECG
B. CXR
C. Echocardiography
D. Laboratory investigations:
• CBC
• Dialysis and renal profile
• eGFR
• Blood glucose studies
• Lipid profile
• Urine routine exam and ACR
• Minerals.
JNC 7

Features suggesting hypertensive nephrosclerosis
Black race
Hypertensive retinal changes
Left ventricular hypertrophy
Long-standing or very severe HTN
Proteinuria less than 0.5 g/d
Hypertension diagnosed prior to the
onset of proteinuria
Hypertension preceding renal
dysfunction
No evidence of another renal
disease
Biopsy findings compatible with the
diagnosis
Fervenza; 2015

Management strategies of HTN in CKD patients
Based on KDIGO guidelines 2012Kidney International Supplements (2012) 2, 341–342;

GENERAL STRATEGIES
2.1: Individualize BP targets and agents according to age, co-existent
cardiovascular disease and other co-morbidities, risk of progression of CKD,
presence or absence of retinopathy (in CKD patients with diabetes) and
tolerance of treatment. (Not Graded)
2.2: Inquire about postural dizziness and check for postural hypotension
regularly when treating CKD patients with BP-lowering drugs. (Not Graded)

Lifestyle modification2.3: Encourage lifestyle modification in patients with CKD to lower BP and improve
long-term cardiovascular and other outcomes:
2.3.1: We recommend achieving or maintaining a healthy weight (BMI 20 to 25). (1D)
2.3.2: We recommend lowering salt intake to <90 mmol (<2 g) per day of sodium
(corresponding to 5 g of sodium chloride), unless contraindicated. (1C)
2.3.3: We recommend undertaking an exercise program compatible with cardiovascular
health and tolerance, aiming for at least 30 minutes 5 times per week. (1D)
2.3.4: We suggest limiting alcohol intake to no more than two standard drinks per day
for men and no more than one standard drink per day for women. (2D)

BP management in CKD ND patients without DM
3.1: We recommend that non-diabetic adults with CKD ND and urine albumin
excretion <30 mg per 24 hours (or equivalent*) whose office BP is consistently >140
mmHg systolic or > 90 mmHg diastolic be treated with BP-lowering drugs to
maintain a BP that is consistently < 140mmHg systolic and < 90mmHg diastolic. (1B)
3.2: We suggest that non-diabetic adults with CKD ND and urine albumin excretion
of 30 to 300 mg per 24 hours (or equivalent*) whose office BP is consistently > 130
mmHg systolic or > 80mmHg diastolic be treated with BP-lowering drugs to
maintain a BP that is consistently <130 mmHg systolic and < 80 mmHg diastolic.
(2D)

3.3: We suggest that non-diabetic adults with CKD ND and urine albumin excretion
> 300 mg per 24 hours (or equivalent*) whose office BP is consistently >130 mmHg
systolic or > 80 mmHg diastolic be treated with BP-lowering drugs to maintain a BP
that is consistently < 130 mmHg systolic and < 80 mmHg diastolic. (2C)
3.4: We suggest that an ARB or ACE-I be used in non-diabetic adults with CKD ND
and urine albumin excretion of 30 to 300 mg per 24 hours (or equivalent*) in whom
treatment with BP-lowering drugs is indicated. (2D)
3.5: We recommend that an ARB or ACE-I be used in non-diabetic adults with CKD
ND and urine albumin excretion >300 mg per 24 hours (or equivalent*) in whom
treatment with BP-lowering drugs is indicated. (1B)

BP management in CKD ND patients with DM
4.1: We recommend that adults with diabetes and CKD ND with urine albumin
excretion <30 mg per 24 hours (or equivalent*) whose office BP is consistently
>140 mm Hg systolic or >90 mm Hg diastolic be treated with BP lowering drugs
to maintain a BP that is consistently <140 mm Hg systolic and < 90 mm Hg
diastolic. (1B)
4.2: We suggest that adults with diabetes and CKD ND with urine albumin
excretion >30 mg per 24 hours (or equivalent*) whose office BP is consistently
>130 mm Hg systolic or >80 mm Hg diastolic be treated with BP lowering drugs
to maintain a BP that is consistently < 130 mm Hg systolic and <80 mm Hg
diastolic. (2D)




RRR 20%P <0.001

4.3: We suggest that an ARB or ACE-I be used in adults with diabetes
and CKD ND with urine albumin excretion of 30 to 300 mg per 24 hours
(or equivalent*). (2D)
4.4: We recommend that an ARB or ACE-I be used in adults with
diabetes and CKD ND with urine albumin excretion >300 mg per 24
hours (or equivalent*). (1B)

BP management in kidney transplant recipients (CKD T)
5.1: We suggest that adult kidney transplant recipients whose office BP is
consistently >130 mm Hg systolic or >80 mm Hg diastolic be treated to maintain
a BP that is consistently <130 mm Hg systolic and <80 mm Hg diastolic,
irrespective of the level of urine albumin excretion. (2D)
5.2: In adult kidney transplant recipients, choose a BP-lowering agent after
taking into account the time after transplantation, use of calcineurin inhibitors,
presence or absence of persistent albuminuria, and other co-morbid conditions.
(Not Graded)

BP management in elderly persons with CKD ND
7.1: Tailor BP treatment regimens in elderly patients with CKD ND by carefully
considering age, co-morbidities and other therapies, with gradual escalation of
treatment and close attention to adverse events related to BP treatment,
including electrolyte disorders, acute deterioration in kidney function, orthostatic
hypotension and drug side
effects. (Not Graded )
The Work Group does not believe that the evidence is sufficiently strong to
support a lower target BP level for all patients with diabetes and CKD.

ADA recommendations 2016

ADA recommendations 2016 … continued

Renovascular hypertension (RVHT)

Prevalence • Renal artery stenosis (RAS) prevalence in free – living black and white
Americans older than 65 years is 7% (1)
• RAS prevalence increases to 20-45% of patients older than 50 years
who have had peripheral or coronary artery disease (2).
• Progressive renal disease occurs in 10% of patients over 5 years.
• Not all patients with RAS are hypertensive.
(1) Hansen et al. J Vasc Surg. 2002 Sep. 36(3):443-51(2) Fervenza; Medscape 2015

Clinical manifestations of atherosclerotic RAS
• Hypertension especially at young age
• Renal failure (ischemic nephropathy)
• Recurrent episodes of CCF, and flash pulmonary edema.
• Sudden worsening of renal function in a patient who is hypertensive and
who was started on an ACE-I is also suggestive of renal vascular disease.

Pathophysiology • Renal artery occlusion creates ischemia, which triggers the release of renin
and a secondary elevation in blood pressure.
• Hyperreninemia promotes conversion of angiotensin I to angiotensin II,
causing severe vasoconstriction and aldosterone release.
• The ensuing cascade of events varies, depending on the presence of a
functioning contralateral kidney.


The evolution of RVHT has three stages or phases:
• Renin-angiotensin–dependent phase
• Salt-retention phase
• Systemic renin-angiotensin–independent phase

Investigation
• Doppler ultrasound scanning: can be highly accurate when stenosis
is present but it has many false negative results.
• MRA using gadolinium: test of choice. It has a risk of NSF
• CT angiography, or intra-arterial renal angiography.
• Captopril renogram: less sensitive


Treatment • ACE-Is / ARBs
• Diuretics, beta blockers, CCB
• Renal revascularization: Percutaneous transluminal angioplasty with
stenting
• Surgery: surgical reconstruction and nephrectomy
• To date, no RCTs has shown a survival benefit for either
endovascular or surgical revascularization compared with medical
management in patients with RAS.Schmidt; Medscape 2015

Anti-HTN Agents for Patients With CKD and HTN
Classification of Patients With CKD First Line Second Line Third Line Fourth Line
Diabetic CKD +/- HTN ACE inhibitor or ARB Thiazide or loop
diuretics / ND-CCB ND-CCB Aldosterone antagonist
Nondiabetic CKD + HTN + proteinuria ACE inhibitor or ARB Thiazide or loop
diuretics / ND-CCB ND-CCB Aldosterone antagonist
Nondiabetic CKD + HTN without proteinuria (<200 mg/g)
No agents preferred; consider a diuretic
ACE inhibitor or ARB or CCB
Aldosterone antagonist NA
K/DOQI clinical practice guidelines. Am J Kidney Dis. 2004;43(suppl 1):S1-S290.Navaneethan etal. Clin J Am Soc Nephrol. 2009;4:542–551.

CCB in CKD

Suggested Goals for CKD Patients esp. with DM and HTN• Lifestyle modifications (no obesity, regular exercise)• BP 130/80 mmHg or lower, esp in diabetes or proteinuria) • Maximal reduction of proteinuria (<1 g/d)• Multiple BP lowering meds(3-4 meds or more, if needed)• ACEIs, ARBs, Diuretics, Non-Dihydropyridine-CCBs • HbA1c at <7% (in diabetics)• Dietary protein restriction (0.6 - 0.8 kg/d)• Dietary sodium restriction (<2-3 g/d sodium)• Lipid-lowering therapy (diet, statins)

Take home message
• The incidence of ESRD has increased by 18% between 2000 and 2007, but
current data show a plateau in this rise
• Rates of BP control have improved dramatically over the past decade, which
might explain the plateau in ESRD rates
• HTN is clearly associated with chronic kidney disease progression; however,
existing data have demonstrated that the current recommended blood-
pressure goal (<130/80 mmHg) slows, but does not stop, CKD progression

• Sustained increases in serum creatinine level reflect renal
parenchymal damage and, potentially, irreversible kidney injury
• Identifying early hypertension-associated kidney injury is
necessary to prevent progression ro ESRD.
• Volume removal leads to a consistent lowering of blood
pressure, suggesting that maintaining euvolemia is an
important strategy in achieving target blood-pressure levels in
patients with CKD

Thank you