Embed Size (px)
Citation preview

BYPROF/ GOUDA ELLABBAN

• Wounds may be defined as disruption of the normal continuity of bodily structure due to trauma, which may be penetrating or non-penetrating

• Incised wound: caused by sharp instruments, if
there is associated tearing of tissue it is called lacerated wound
• Abrasion: result from friction damage to the
body surface and it characterized by superficial bruising and loss of various thickness of skin and underlying tissue

• Crush injury: These are due to severe pressure, even
though skin may not be breached there can massive tissue destruction also there is massive edema which may prevent wound closure
• Degloving injury: Result from sharing forces that cause
parallel tissue plane to move against each other, e.g.: when a hand is caught between roller or in moving machinery. Large areas of apparently intact skin may be deprived of their blood supply by rapture of feeding vessels.

• Gunshot wounds: May be low or high velocity. Bullets
fired from high velocity cause massive tissue destruction.
• Burn: These are caused by heat,
electricity, irradiation and chemicals.

• Classification:Surgical procedure can be classified according
to the likelihood of contamination and wound infection into:
1- Clean procedure : Those in which wound contamination is not
expected and should not occur. e.g. incision for a clean elective procedure when there is no infective focus is encountered and no viscus is entered ( hernia repair, thyroidectomy). Wound infection rate is less than 1%
WWW.SMSO.NET

c
2- Clean – contaminated procedure:There is no focus of infection is encountered
but significant risk is still present may be because of the opening of viscus such as colon. Infection rate is > 5%.
3- Contaminated:When there is obvious spillage or obvious
inflammatory disease, e.g. a gangrenous appendix. Infection rate 15-20%.
4- Dirty wounds:When there is a frank pus or gross soiling.
E.g. perforated large bowel or drainage of subphrenic abscess. Infection rate is up to 40%.
WWW.SMSO.NET

• The principle causes of wound infection are the penicillin-resistant staph.aureus, together with strept. Faecalis, pseudomonas, coliform bacteria and other bowel bacteria including bacteriodes.
• With continuous use antibiotics, more resistant strains of organisms are appearing, such as methicillin-resistant staph.aureus (MRSA) and the vancomycin-resistant enterococcus (VRE).
WWW.SMSO.NET

Preoperative factors:Local factors: pre-existing infection. e.g.
a perforated appendix or infected compound fracture.
General factors: nasal carrier of staphylococci or having skin infection, malnourishment and immunosuppression (Children – elderly – HIV patients – cancer patients – diabetics).
Risk factors of wounds infection
WWW.SMSO.NET

Operative factors:1- Failure of adequate sterilization of instruments, surgeon’s
hands or dressings.2- Nasal or skin carriers of staphylococci among the nursing and
surgical staff.3- Site of wound: • common when alimentary, biliary or urinary tract is opened
allowing bacterial contamination to occur.• Wounds placed on poorly vascularized tissue, such as in
amputation because necrotic tissue is a good medium for bacterial growth and a good supply is necessary to provide access for the inflammatory cells.
Postoperative factors:1- cross-infection from elsewhere on the patient’s body or from
other infected cases in the ward during dressing change or wound inspection.
2- new infection due to contamination of the wound from the nose or hands of the surgical or nursing staff.
WWW.SMSO.NET

Clinical features• It usually become evident 3-4 days after operation.• 1st sign is cellulitis around the margin of the wound,
or swelling of the wound with discharge from between the sutures.
• Fluctuation can be elicited when there is an abscess or liquefying hematoma.
• Crepitus may be present if gas-forming organisms are involved.
• The patient may have pyrexia and increase wound tenderness
• General effect of infection (malaise, anorexia, vomiting)
WWW.SMSO.NET

Managements • Established infection is treated by drainage,
antibiotics are given if there is spreading cellulitis.
• A wound swab or specimen is sent routinely for bacteriological culture and sensitivity determination.
• The state of immunity against tetanus is assessed and appropriate action taken.
• Area of redness is mapped out so that its extent can be monitored.
WWW.SMSO.NET

Prevention • Careful patient preparation• Isolation of infected cases.• Elimination of carriers with colds or
septic lesions among the medical and nursing staff.
• Prophylactic use of antibiotic in high risk patients
• Meticulous attention to good operating theatre and dressing techniques
WWW.SMSO.NET

• It is the disruption of the continuity of an epithelial surface .
• It follows traumatic removal or death and desquamatation by disease of the whole or part of an epithelium.
WWW.SMSO.NET

Features of an ulcer1- Edge:It is the junction between healthy and
diseased tissueTypes:A- slopping edge:• Reddish-purple an consist of new healthy
epithelium growing over the base of the ulcer.
• Example: traumatic, venous ulcer, healing ulcer
WWW.SMSO.NET
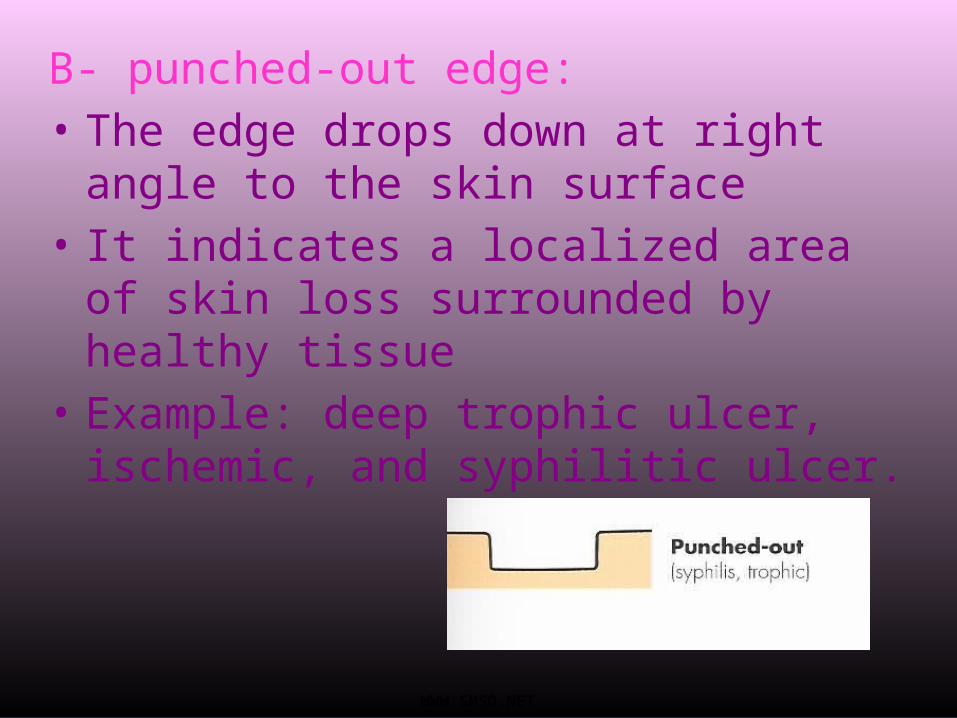
B- punched-out edge:• The edge drops down at right
angle to the skin surface• It indicates a localized area of
skin loss surrounded by healthy tissue
• Example: deep trophic ulcer, ischemic, and syphilitic ulcer.
WWW.SMSO.NET
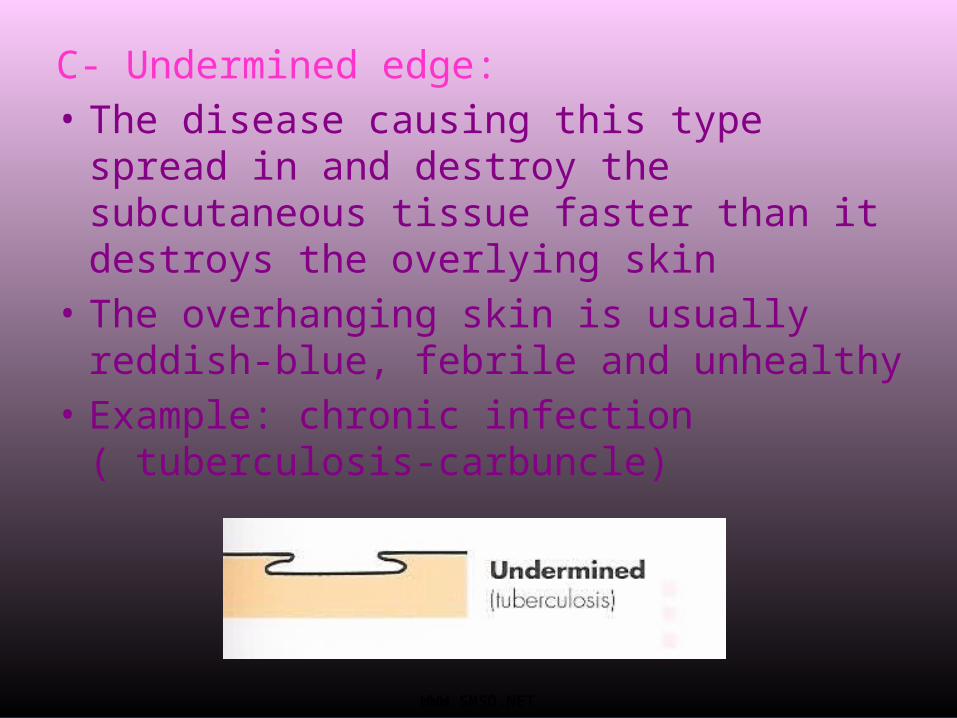
C- Undermined edge:• The disease causing this type spread
in and destroy the subcutaneous tissue faster than it destroys the overlying skin
• The overhanging skin is usually reddish-blue, febrile and unhealthy
• Example: chronic infection ( tuberculosis-carbuncle)
WWW.SMSO.NET

D- Rolled edge:• It is necrotic at its center but
grows quite quickly at its periphery so that it rises above the surface of the skin.
• Example: basal cell carcinoma
WWW.SMSO.NET

E- everted edge:• Caused by a fast growing infiltrating
cellular disease. The growing portion at the edge of ulcer goes up and spills over the normal skin to produce an everted edge
• Example: sequamous cell carcinoma, ulcerated adenocarcinom
WWW.SMSO.NET

2- The base:• It consist of 3 types of tissue:1-granulation tissue:1st stage of healing process.2-dead tissue:It is also called slough3-malignant tissue:It is maybe slightly vascular or necrotic but
never develop granulation tissue
WWW.SMSO.NET

3- Discharge:• May be serous, purulent,
offensive, copious or so slight which dries into scab
• It should be cultured to determine the nature of infective organisms.
WWW.SMSO.NET

Deferential diagnosis of leg ulcers
• Venous ulcer complicating venous insufficiency.• Ischemic ulcer due to impaired arterial blood supply.• Neuropathic ulcer; particularly common in diabetics
where they are often compounded by ischemia due to diabetics micro-angiopathy.
• Malignant ulcer; a squamous carcinoma, often arising on a pre-existing chronic ulcer, or an ulcerated malignant melanoma.
• Ulcer complicating systemic disease, e.g.: acholuric jaundice, ulcerative colitis and rheumatoid arthritis.
• Arteriovenous fistula-associated ulcer.• Repetitive self-inflected injury.• Gummatous ulcer of syphilis.
WWW.SMSO.NET

• Ulceration due to venous hypertension is due to deep veins incompetence although incompetence of superficial vein may be present.
• Usually seen in patients 40-60 years old but severe disease can cause ulceration in young adult and it can appears in children with congenital venous malformation.
• Women affected more than men.• Usually the patient has a history of deep venous
thrombosis, childbirth or immobilization in bed for any reason.
WWW.SMSO.NET

• The patient usually suffered from aching pain, discomfort and tenderness of the skin, pigmentation and eczema for months before an ulcer appears.
• At 1st it is painful then it settles down and become chronic. It is rarely very painful.
WWW.SMSO.NET

Site:• Usually it occurs around the medial malleoli not in the foot
because in this area the subcutaneous tissue is less well supported than in foot.
• The surrounding tissue shows signs of chronic venous hypertension (indurations, pigmentation, warmth, redness, and tenderness)
Edge:• It can be of any shape and size. • The edge is sloping and pale purple-blue in color.Base:• The base is usually covered with pink granulation tissue
but in chronic ulcer there maybe fibrous tissue more than granulation tissue.
• It is shallow and flat, and fixed to the deep tissueDischarge:• The discharge is serropurulent with a trace of blood
sometimes.
WWW.SMSO.NET

Investigation:• Full blood count, blood glucose
determination.• Duplex ultrasound to defined
nature and distribution of disease
• Ascending venography
WWW.SMSO.NET

Treatment:• Medical:If patient have co-morbidity, but it doesn’t
increase healing.• Dressing. • Compression therapy:- elastic, multiple or graduated.- After healing, compression stocking to reduce
chance of recurrence. • Surgery:- split-skin grafting to spread up ulcer healing.- Correction of superficial venous reflux by
short and long saphenous surgery.- Ligating medial calf perforating vein either
endoscopicaly or by open surgery.
WWW.SMSO.NET

• It is caused by an inadequate blood supply.• Common in elderly with symptoms of
coronary or cerebral vascular disease but can occur in the young.
• It is very painful and they can cause rest pain.
• It can be of any size.• There is no signs of heeling and often they
get deeper and larger slowly.• The pulse maybe absent.
WWW.SMSO.NET

causes:1- Large-artery obliteration :Atherosclerosis, embolism.
2- small-artery obliteration:Raynaud’s disease, Scleroderma,
Buerger’s disease, embolism, diabetes, radiation, trauma, electrical burn
WWW.SMSO.NET

• Site:- usually it found at the tip of toes and over the pressure
area.- Surrounding tissue are cold, pale, atrophic because also
they are ischemic . If it is warm. It suggest that the ulcer is due to local factor.
• Edge:- The edge is punched-out and if heeling does begin the
edge becomes slopping.• Base:- It may contain grey-yellow sloughing tissue and is often
infected.- Often it is deep penetrating down to bone and
underlying joints. • Discharge:- It doesn’t bled but discharge a thin serous exudates
which is sometimes purulent.
WWW.SMSO.NET

Investigation:• Angiography to reveal the filling of
leg vessels.• Duplex.• X-ray shows gas in the tissue
indicates anaerobic infection, an may shows bony destruction if osteomylitis occur.
Angiogram showing irregularity of outline with stenosis in left superficial femoral artery
WWW.SMSO.NET

Treatment:1- necrotic tissue; debridement abscess; incision, drainage gangrene; amputation 2- Dry dressing.3- antibiotic should be administered
if there is associated infection.4- surgical arterial bypass or
angioplasty.
WWW.SMSO.NET

Clinical features
Ischemic ulcer Venous ulcer
Gender Men > women Women > men
Age Usually presents > 60 years Typically develops 40-60 years
Risk factors Smoking, diabetes, hyperlipidemia and hypertension
Previous DVT, thrombophilia, varicose vein
Symptoms Severe pain unless there is diabetic neuropathy
Pain but not severe, relieved by elevation
Site Pressure area (heel, metatarsal head and base)
Medial and lateral malleoli
Edge Regular, punched out Irregular, with neo-epithelium
Base Deep, green (sloughy) or black (necrotic) with no granulation tissue, may involve tendon, bone and joint
Pink and granulating
Surrounding skin
Shows signs of ischemia (cold, pale, atrophic….)
Varicose eczema, indurations, pigmentation, redness.
Veins Empty Full, usually varicosed
Swelling Usually absent Often present
WWW.SMSO.NET
• Caused by local ischemia due to lack of sensation in the tissue.
• They are deep penetrating ulcer. Similar to ischemic ulcer occur in pressure area but the surrounding tissue are healthy and have a good circulation.
• The foot is well nourished, healthy and often has hair.
• Good dorsalis pedis and posterior tibial pulses.
• It is warm, deep penetrating ulcer.
WWW.SMSO.NET

Diagnostic feature:1- They are painless.2- The surrounding tissue areunable to appreciate pain.3- The surrounding tissue is healthy and have a normal blood supply.
WWW.SMSO.NET

Causes:1- Peripheral nerve injury:Diabetes, nerve injury, leprosy.
2- Spinal cord lesions:Spina bifida, tabes dorsalis,
syringomyelia.
WWW.SMSO.NET

• DM can be associated with true ischemic ulcer due to large vessels atherosclerosis, also it can be associated with neuropathic ulcer due to peripheral neuritis.Neuropathic ulcer Ischemic ulcer
PainlessNormal arterial pulseLoss of sensationWarm footPlanter ulcerationNo intermittent claudication
PainfulReduced arterial pulseVariable sensory findingCold footToe ulcerationIntermittent claudicationWWW.SMSO.NET

Investigations:1- blood glucose level.2- CBC; leukocytosis.3- swab for culture and sensitivity.4- biopsy.5- nerve conduction test to confirm
diagnosis of neuropathy.6- arteriogram.7- LFT, PT, PTT to prepare for surgery.
WWW.SMSO.NET

Treatment:1- control of diabetes.2- incision and removal of dead tissue.3- dry dressing.4- antibiotic if infected.5- skin graft.6- follow-up and education.7- if failed; amputation
WWW.SMSO.NET

1- squamous ulcer carcinoma (Marjolin’s ulcer):
• Arise in a long standing benign ulcer or scar.• The commonest ulcer to become malignant is a
longstanding venous ulcer.• The scar that is most often associated with
malignant change is the scar of an old burn.• It has the same characteristics of ordinary
squamous carcinoma but the edge is not always raised and everted.
• This type is not so invasive, slower growing and slightly less malignant
WWW.SMSO.NET

2- Malignant melanoma:Because the tumor cells multiply,
so the overlying epithelium become anoxic and either ulcerates spontaneously or break after minor injury.
WWW.SMSO.NET

WWW.SMSO.NET

![Magnesium Sulphate Powder in the Treatment of …...March, 1942] TREATMENT OF WOUNDS AND ULCERS : ANDREASEN 129 Original Articles Magnesium sulphate powder in the treatment of wounds](https://img.dokumen.tips/doc/110x75/5e8e2523c09d3945c554d5d4/magnesium-sulphate-powder-in-the-treatment-of-march-1942-treatment-of-wounds.jpg)



























