Embed Size (px)
Citation preview
Ventilator Education
Presentation by Rachelle Solum CRT 2014
Objectives: After this presentation you should be able to :
• Define key ventilator terms
• Understand 3 common vent modes and settings used on ventilators
• Identify the 2 vents we use, find patient data and setting data on them
• Identify 3 common vent alarms and be able to troubleshoot problems and know what actions to take associated with those alarms
• Identify a clinometer and HME and their uses
• Identify LTV1200 exhalation port and sensors
DEFINITIONS
This section will define some commonly used terms when discussing ventilators

Definitions
Tidal Volume (Vt)
Rate/frequency
PEEP
FiO2
Pressure Support
When the vent cycles it is set to give a specific amount of Oxygen enriched air.
If the vent has a set Tidal Volume (Vt) of 500ml, every breath given by the vent is about 500ml.
It sometimes is a little more or less depending on how much effort there is from the patient, pressure in the lungs and other factors, but usually near 500ml.
DefinitionsTidal Volume (Vt)
Rate/frequency
PEEP
FiO2
Pressure Support
How many breaths the patient is breathing per minute based on time between the beginning of 2 breaths. This number can change with every breath a patient takes.

DefinitionsTidal Volume (Vt)
Rate/frequency
PEEP
FiO2
Pressure Support
Positive End-Expiratory Pressure
Air is pulled by the lungs into tiny little air sacs called alveoli, which are wet inside.
Coughing, mucous production and suctioning of the lungs can collapse the alveoli and make them resistant to re-opening.
PEEP is a constant pressure inside the patient's lungs that minimizes the collapse of the alveoli and helps recruit collapsed alveoli.
DefinitionsTidal Volume (Vt)
Rate/frequency
PEEP
FiO2
Pressure Support
Fraction of Inspired Oxygen
It's the oxygen setting on the vent expressed as a percent.
The range is 21% (room air) to 100%
DefinitionsTidal Volume (Vt)
Rate/frequency
PEEP
FiO2
Pressure Support
It is an extra push of pressure to help with each breath.
It increases the volume of breath and works with PEEP to increase the number of full alveoli and helps patient get a breath with less work.

Ventilator Modes and Settings
This section will explain the different vent modes and settings we use most commonly

Ventilator Modes Assist Control (AC)
Synchronized Intermittent Mechanical Ventilation (SIMV)
Pressure Support (PS)
These are the most common vent modes used
The settings used in the examples are not always the numbers used.
They are all tailored to each patient depending on their needs.

Assist Control (AC) This is the highest support available on the vent.
Example: AC12, 500, 30%, +5 means that the rate is set at 12, tidal volume (Vt) is set at 500, FiO2 is 30% and PEEP is +5.
The very least the patient gets is 12 full breaths per minute with a Vt of 500ml.
If the patient takes more than 12 breaths, the vent senses their inspiratory effort and gives them the full Vt of 500ml with each breath over 12.

Synchronized Intermittent Mechanical Ventilation (SIMV) Example: SIMV12, 500, 30%, +5, +15 means that the rate is
set at 12, tidal volume (Vt) is set at 500, FiO2 is 30%, PEEP is +5, and the pressure support (PS) is +15.
Again, like AC, the very least the patient gets is 12 full breaths per minute with a Vt of 500ml.
If the patient takes more than 12 breaths, the vent senses their inspiratory effort and gives them a breath with a PS of +15 to help boost the volume. Those breaths are more work and start to exercise the diaphragm and lungs.
This is a mode that we use to start the weaning process. Often we reduce the rate gradually (example: SIMV rate is lowered 1 breath per day) to wean the patient.

Pressure Support (PS) Example: PS15, 30%, +5 means that pressure support is set
at +15, FiO2 is 30% and PEEP is +5.
There is no set rate and no set tidal volume(Vt).
ALL the patients breaths are at their own volume with a pressure support behind them of +15.
Pressure Support helps overcome the increased work of breathing with an artificial airway and the resistance of the vent circuit.
This mode is usually used before trach mask trials begin.
This is technically & sometimes referred to as CPAP mode.

Vent Changes ONLY a Respiratory Staff member is allowed to change ANY
ventilator settings on the vent.
Parameters that we are NOT allowed to change without a Doctor’s order: • Mode(AC, SIMV, PS)• Rate• Tidal Volume (Vt)• PEEP • Pressure Support(PS)
Our protocol allows us to titrate the FiO2 to maintain a Pulse Oximetry (POX) level of 90% or above. This includes giving 100% O2 when patient will be placed in a supine position, exerting effort or being suctioned, when it is indicated.
Our Ventilators
This section will show you where to read the actual patient data and where to read the vent settings on
each of the vents we are currently using
We have 2 ventilatorsPuritan Bennett 760
(PB760)
Sometimes referred to as:
Big vent or old vent
Viasys LTV1200
(LTV1200)
Sometimes referred to as:
Small vent or new vent

Patient informationWhere to see what the patient is actually doing on the vent
PB760 – RED circle is Pt info LTV1200 – RED circle is Pt info
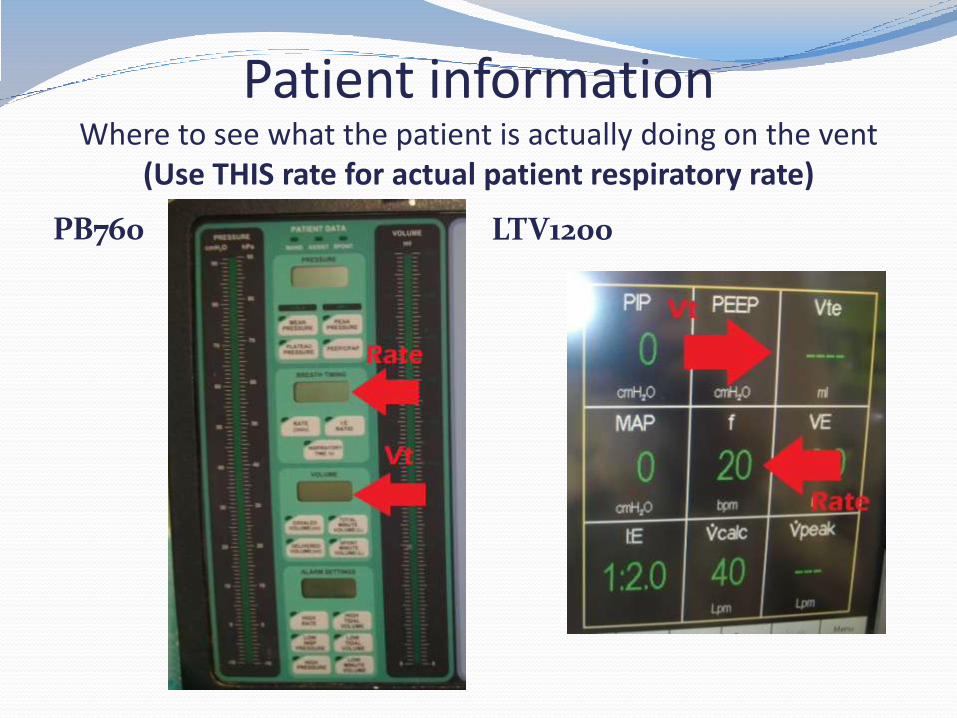
Patient informationWhere to see what the patient is actually doing on the vent
(Use THIS rate for actual patient respiratory rate)
PB760 LTV1200

Ventilator SettingsWhere to find vent settings
PB760 LTV1200

Ventilator Settings Where to Find the SettingsPB760
LTV1200 -#’s are red if active

100% FiO2How to give patient 100% FiO2 for suctioning or distress
PB760 LTV1200 bottom display
Alarms
This section will explain some common alarms, and how YOU can troubleshoot ventilator alarms
Common Alarms
High Pressure
High Rate/Frequency
Disconnect, Low Volume or Low Pressure

High Pressure Usually this alarm is activated when patient COUGHS
or NEEDS SUCTIONING.
Action: Suction patient
Sometimes activated when vent circuit is compressed.
Action: Check vent circuit for kinks or compressions and straighten out vent circuit.
Lungs are not compliant with current vent settings, patient “fighting” vent settings, or alarm set to low.
Action: Contact Respiratory Staff

High Rate/Frequency This alarm is activated when patient breathes more
times per minute than the alarm is set for, usually 40 breaths per minute. It may be due to anxiety, pain or fatigue.
Action: Contact Respiratory Staff, especially if patient is weaning, diaphoretic or appears to be struggling with breathing.
Action: Check if patient needs anxiety or pain medication.
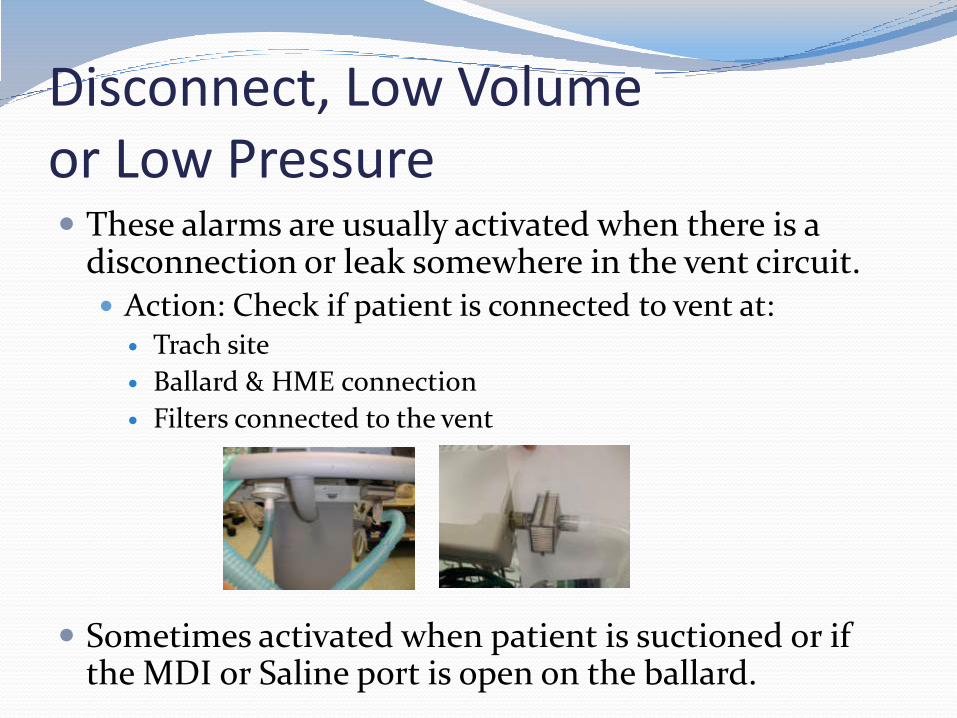
Disconnect, Low Volume or Low Pressure These alarms are usually activated when there is a
disconnection or leak somewhere in the vent circuit. Action: Check if patient is connected to vent at: Trach site
Ballard & HME connection
Filters connected to the vent
Sometimes activated when patient is suctioned or if the MDI or Saline port is open on the ballard.
Other Alarm Information There are many other alarms that may be activated. If
you can hear or see an alarm that you are unfamiliar with, please contact Respiratory Staff.
There is no need to worry if an alarm warning is on the vent, but there is no audible alarm. The vents will display the last alarm activated.
Notify Respiratory Staff immediately after checking patient if a vent is alarming in room, but no hallway light or alarm is activated!
Additional Information
This section will provide some items you need to be aware of when caring for our ventilated patients

Head Of BedALWAYS make sure that ANY artificial airway patient has their head elevated to 30 degrees or greater. Please use the clinometers to check the elevation.

HME – Heat Moisture Exchanger
HME’s keeps heat and moisture in the air that the patient breathes in. Because we do not use humidifiers or heaters on our vents, these must be in place.
Insure the HME is slightly elevated (an inch or two) above the artificial airway so that it does not fill with secretions.
If you notice an HME filled with secretions or moisture, please contact Respiratory Staff so that it can be changed.
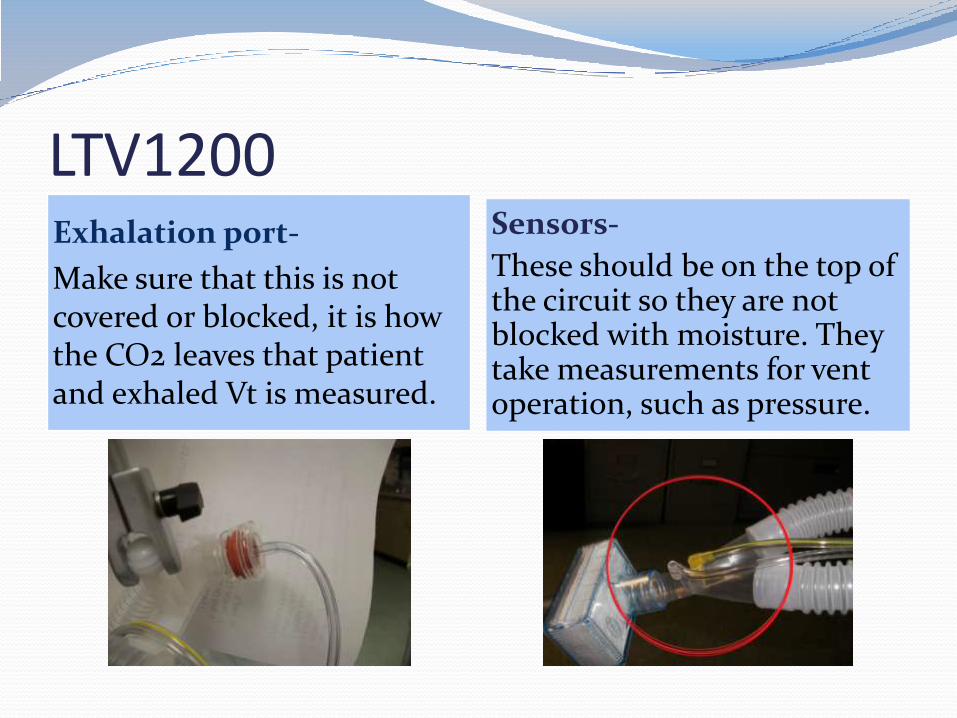
LTV1200 Exhalation port-
Make sure that this is not covered or blocked, it is how the CO2 leaves that patient and exhaled Vt is measured.
Sensors-
These should be on the top of the circuit so they are not blocked with moisture. They take measurements for vent operation, such as pressure.

For more information Please ask any Respiratory Staff member





























