Embed Size (px)
Citation preview
BYDR. MARWA A. MAHROUS
ASSISTANT LECTURER SOHAG UNIVERSITY HOSPITAL
2015
Traumatic brain injury
Sources of this lecture: The Brain Trauma Foundation The American Association of Neurological Surgeons The Joint Section on Neurotrauma and Critical Care Traumatic Brain Injury By: Erin Engnell ICU Protocols Kasr Al-Aini Hospital Anesthesia Department
Cairo University TRAUMATIC BRAIN INJURY By: Dr.Gihan Seif El Nasr
Professor of Anaesthesia & ICU guidelines prepared by the Department of Surgical
Education, Orlando Regional Medical Center 2014.
Topics
-definition-causes
-pathophysiology-severity
-diagnosis-complications
-management
Definition of TBI
“An insult to the brain, not of degenerative or congenital nature caused by an external physical force that may produce a diminished or altered state of consciousness, which results in an impairment of cognitive abilities or physical functioning. It can also result in the disturbance of behavioral or emotional
functioning”.
Causes
An outside force impacts the head causing the brain to move
A direct blow to the head
A rapid acceleration and deceleration of the head
Traumatic brain injury (TBI) is the leading cause of death for all age groups, contributing to over 60% of trauma-related deaths .
The primary goals of management in TBI are to minimize cerebral edema, intracranial pressure (ICP), and to optimize cerebral perfusion pressure (CPP) thereby decreasing the incidence of secondary injury
Pathophysiology
TBI may be divided into primary injury and secondary injury.
Primary injury is induced by mechanical force and occurs at the moment of injury.
Secondary injury is not mechanically
induced. It may be delayed from the moment of impact, and it may superimpose injury on a brain already affected by a mechanical injury.
Primary injury:
The 2 main mechanisms that cause primary injury are:
Contact (as an object striking the head or the brain striking the inside of the skull)
Acceleration-deceleration.
Primary injury due to contact may result in; injury to the scalp, fracture to the skull and surface contusions.
Contusions are distinct areas of swollen brain tissue,typically found on the poles of the frontal lobes, the inferior aspects of the frontal lobes, the cortex above and below the operculum of the sylvian fissures, and the lateral and inferior aspects of the temporal lobes.
Primary injury due to acceleration-deceleration results from unrestricted movement of the head and leads to shear, tensile, and compressive strains.
These forces can cause intracranial
haematoma or diffuse axonal injury (injury to cranial nerves and the pituitary stalk.
Intracranial haematoma is the most common cause of death and clinical deterioration after TBI. Haematomas may be:
Epidural haematomas caused by fracture of the temporal bone and rupture of the middle meningeal artery, clotted blood collects between the bone and the dura.It can grow quickly creating pressure against the brain tissue.
Subdural haematomas are usually caused by rupture of the bridging veins in the subdural space. They can grow large enough to act as mass lesions, and they are associated with high morbidity and mortality rates.
Subarachnoid haematomas result from damage to blood vessels in the posterior fossa stalk.

Diffuse axonal injury (DAI) is one of the most common and important pathologic feature of TBI.
It constitutes mostly microscopic damage, and it is often not visible on imaging studies.
The main mechanical force that causes DAI is rotational acceleration of the brain, resulting in unrestricted head movement.
Rotational acceleration produces shearing and tensile forces, and axons can be pulled apart at the microscopic level.
Microscopic evaluation of the brain tissue often shows numerous swollen and disconnected axons.
Rapid stretching of axons is thought to damage the axonal cytoskeleton and, therefore, disrupt normal neuron function.
Secondary injury:It may occur hours or even days after the
inciting traumatic event. Injury may result from impairment or local
declines in CBF after TBI as a result of local edema, haemorrhage or increased ICP.
As a result of inadequate perfusion, cellular ion pumps may fail, causing a cascade involving intracellular calcium and sodium which may contribute to cellular destruction.
Excessive release of excitatory amino acids, such as glutamate and aspartate, exacerbates failure of the ion pumps.
As the cascade continues, cells die, causing free radical formation, proteolysis, and lipid peroxidation.
These factors can ultimately cause neuronal death.
To summarize causes of secondary brain injury: Hypotension Hypoxaemia Hypercarbia Hyperthermia Hyperglycaemia Hypoglycaemia Hyponatraemia Seizures Infection
Severity
Head injuries can be classified into mild, moderate, and severe.
The Glascow Coma Scale (GCS),is the most commonly used system for classifying TBI severity;
TBI with a GCS of 13 or above is mild, 9–12 is moderate, and 8 or below is severe.
Other classification systems are also used to help determine severity; duration of post-traumatic amnesia (PTA), and loss of consciousness (LOC).
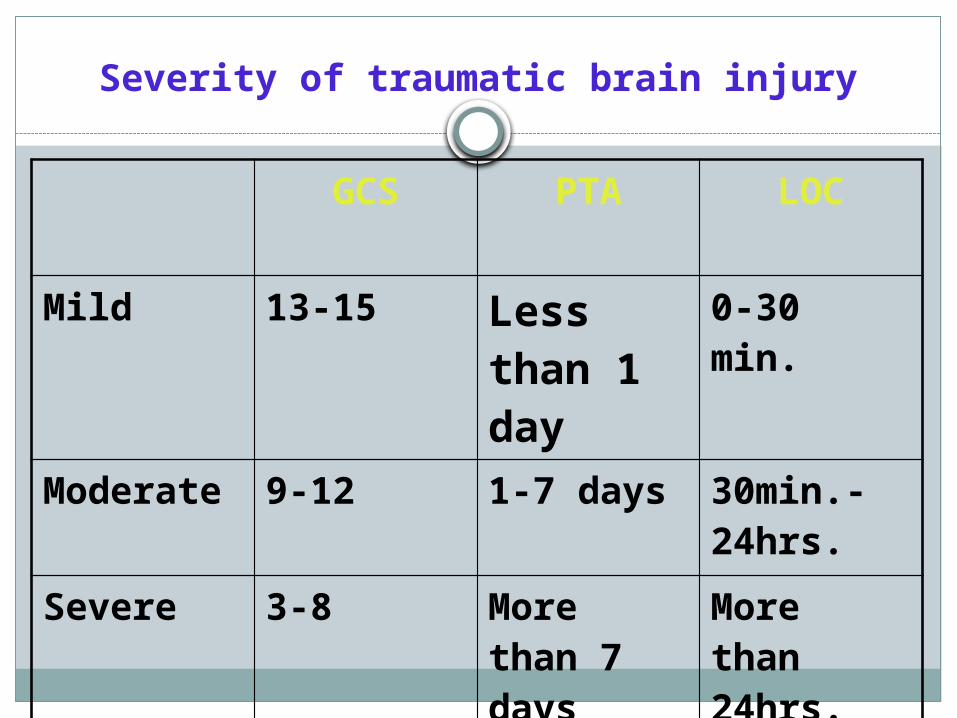
Severity of traumatic brain injury
GCS PTA LOC
Mild 13-15 Less than 1 day
0-30 min.
Moderate 9-12 1-7 days 30min.- 24hrs.
Severe 3-8 More than 7 days
More than 24hrs.
Signs and symptoms
Symptoms are dependent on the injury's severity:
• With mild TBI, the patient may remain conscious or may lose consciousness for a few seconds or minutes.
• Other symptoms of mild TBI include; headache, vomiting, nausea, lack of motor coordination, dizziness, difficulty balancing, lightheadedness, blurred vision or tired eyes, ringing in the ears, bad taste in the mouth, fatigue or lethargy, and changes in sleep patterns.
• Cognitive and emotional symptoms include; behavioral or mood changes, confusion, and trouble with memory, concentration, attention, or thinking.
A person with a moderate or severe TBI may have a headache that
does not go away, repeated vomiting or nausea, convulsions, an
inability to awaken,dilation of one or both pupils,slurred speech,
aphasia , dysarthria, weakness or numbness in the limbs, loss of
coordination, confusion, restlessness, or agitation.
Common long-term symptoms of moderate to severe TBI are
changes in appropriate social behaviour, deficits in social
judgment, and cognitive changes, especially problems with
sustained attention, processing speed, and executive functioning.

When the pressure within the skull,ICP rises too high, it can be deadly.
Signs of increased ICP include decreasing level of consciousness, paralysis or
weakness on one side of the body, and a blown pupil, one that fails to
constrict in response to light .
Cushing's triad, a slow heart rate with high blood pressure and
respiratory depression is a classic manifestation of significantly raised ICP.
Anisocoria, unequal pupil size, is another sign of serious TBI.
Abnormal posturing, a characteristic positioning of the limbs caused by severe
diffuse injury or high ICP, is an ominous sign.
Small children with moderate to severe TBI may have some of these symptoms.
Other signs seen in young children include persistent crying, inability to be
consoled, listlessness, refusal to nurse or eat and irritability.
Diagnosis
Neurological examination and assigning a GCS Score.
Neuroimaging helps in determining the diagnosis and prognosis and proposed treatment.
The preferred radiologic test in the emergency setting is computed tomography (CT): it is quick, accurate, and widely available.
Followup CT scans may be performed later to determine whether the injury has progressed.
Magnetic resonance imaging (MRI) can show more details than CTas detecting injury characteristics such as diffuse axonal injury. However, MRI is not used in the emergency setting.
X-rays are still used for head injuries that are so mild that they do not need imaging or severe enough to merit the more accurate CT.
Angiography may be used to detect blood vessel pathology.
Electroencephalography and transcranial doppler may also be used.
Complications
Posttraumatic seizures; frequently occur after moderate or severe TBI, they are usually general or partial.
Immediate seizures occur in the first 24 hours. Early seizures occur in the first 2-7 days.Late seizures occur after 7 days. Temkin showed that prophylactic use of phenytoin
is effective during the first week after TBI.He recommended discontinuation after 1 week if
no seizures develop because of its lack of effect in preventing late seizures.
Hydrocephalus
Hydrocephalus is characterized as communicating or noncommunicating; Noncommunicating hydrocephalus occurs secondary to an obstruction in the ventricular system before the point at which CSF exits the fourth ventricle.
Communicating hydrocephalus is the most common form after TBI and occurs when the obstruction is in the subarachnoid space.
Deep vein thrombosis
-DVT is common in persons with TBI, with an incidence as high as 54%.
-Risk factors for DVT include; immobility, lower extremity fracture, paralysis, and disruption in coagulation and fibrinolysis.
-DVT may cause pulmonary embolism, postthrombotic syndrome or recurrence.
-DVT best detected by venous Doppler ultrasonography and contrast-enhanced venography.
-Prophylaxis for DVT should be started as soon as possible.
Heterotopic ossification is described as ectopic bone formation in the soft tissue surrounding the joints,in TBI, its incidence is 11-76%.
-It causes joint pain and decreases range of motion ,it is often associated with low-grade fever, peri-articular swelling, peri-articular warmth, and peri-articular erythema.
-The risk of heterotopic ossification is greatest during the first 3-4 months after injury.
Spasticity is defined as velocity-dependent increase in tone.
It is found in an estimated 25% of patients with TBI.
-First-line treatment for spasticity is correct positioning of the involved body segment and exercises.
-Second-line treatment include splinting, casting and other modalities.
GIT and urinary tract complications remain among the most common sequelae in patients with TBI.
-Most frequent GIT complications are; stress ulcers, dysphagia, bowel incontinence, and elevated levels of liver function tests. -Urinary tract complications include; urethral strictures, infections, and urinary incontinence.
Posttraumatic agitation is common after TBI. Furthermore, aggression was consistently associated with depression.
Insomia is common in TBI patients. They may have nighttime awakenings and longer sleep-onset latency.
Posttraumatic headache in 38%.Posttraumatic depression in 40% after TBI, it is
further associated with cognitive decline, anxiety disorders, substance abuse, dysregulation of emotional expression, and aggressive outbursts.
management
Initial Evaluation All patients who present with suspected TBI should
undergo a rapid primary and secondary survey with thorough evaluation of their airway, breathing, and circulation.
Airway patency and adequate oxygenation and ventilation are paramount to avoiding secondary brain injury .
The patient’s cervical spine should be immobilized until cervical spine injury is ruled out. Urgent intubation to secure the patient’s airway should be considered in any patient who presents with a GCS < 8 or in those who are unable to protect their airway.
Intravenous access should be rapidly established
. Bedside glucose testing should be performed in all unconscious patients and hypoglycemia rapidly treated if present. Thiamine (100 mg) should be administered in patients at risk for nutritional deficiency.
If opioid toxicity is suspected (e.g., history of illicit drug use, apnea, bradypnea, small pupils), naloxone 0.4 mg IV should be administered and repeated as necessary, up to 4 mg.
Appropriate laboratory tests [serum electrolytes, CBC with platelets, coagulation studies, arterial blood gas, urinalysis, and urine toxicology / alcohol level (as appropriate)] should be performed.
If definitive neurosurgical care cannot be provided at the initial presenting institution, transfer to a higher level of care should be facilitated in a rapid fashion to preserve the “Gold Hour” and optimize the patient’s outcome. Certain key resuscitative interventions should initiated at the referring facility however to minimize secondary cerebral injury

Management
Monitoring: This is essential in severe TBI. It includes; ECG, invasive arterial blood
pressure, pulse oximetry, central venous pressure, urinary catheter, naso-gastric vs oro-gastric tube (in case of base skull fracture), frequent neurological examination, temperature and capnography.
Resuscitation of Blood Pressure& Oxygenation
GuidelineHypotension (SBP < 90 mm Hg) or hypoxia
(apnea of cyanosis in the field or a PaO2 < 60 mm Hg)must be scrupulously avoided, if possible, orcorrected immediately.
Hypotension (SBP < 90 mm Hg) occurred in 35%of patients and was associated with a two fold increase in mortality.OptionThe mean arterial pressure should be maintained
above 90 mm Hg throughout the patient’s course.
Maintenance of cerebral perfusion pressure(CPP):
This is achieved by maintaining MAP above 90mmHg and preventing increases in ICP,to be between
20-25mmHg. CPP = MAP – ICPCerebral Perfusion PressureCerebral Perfusion Pressure should be
maintained at a minimum of 70 mm Hg.
Maintaining MAPTreating hypovolaemia by 0.9% NaCl/ colloids/P-RBCs/FFP as indicated.Avoid glucose containing fluids unless there is hypoglycaemia (blood sugar should be between 4-7 mmols).Start early enteral feeding as,TBI patients have induced hypermetabolic
and hypercatabolic state resulting in increased energy and protein.Use inotropes (noradrenaline- dopamine), if other causes of hypotension are treated.
Initial Management
OptionThe first priority for the head injured patient
is complete and rapid physiologic resuscitation.No specific treatment should be directed at intracranial hypertension in the absence of signsof transtentorial herniation or progressiveneurologic deterioration not attributable to extracranial explanations.
Indications for ICP Monitoring
GuidelineICP monitoring is appropriate in severe head injury
patients with an abnormal CT, or a normal CT scan if 2 or more of the following are noted on admission: SBP < 90 mm Hg Age > 40 years Uni-/Bilateral motor posturing
Risk of intracranial hypertension (with normal CT) increased to 60% if two or more of the following were noted: 1) Age over 40 years 2) SBP < 90 mm Hg 3) motor posturing
Monitoring of increase in ICP
CT scan should be done on admission and repeated whenever there is change in symptoms or signs.Frequent neurological examination is essential. Hourly recording of GCS, hourly recording of pupil size and reaction.Monitoring ICP if available.
ICP Monitoring Technology
RecommendationIn the current state of technology, the
ventricular catheter connected to an external strain gauge isthe most accurate, low cost, and reliable methodof monitoring ICP. It also allows therapeuticCSF drainage.
ICP transduction via fiberoptic or strain gauge devices placed in ventricular catheters provide similar benefits but at a higher cost.

Controlling ICP
ICP Treatment ThresholdGuidelineICP treatment should be initiated at an upper
threshold of 20 - 25 mm Hg.
Raised ICP leads to secondary brain injury.It is treated by; osmotherapy, analgesia,
sedation, optimal ventilation, surgical and positioning of patient.
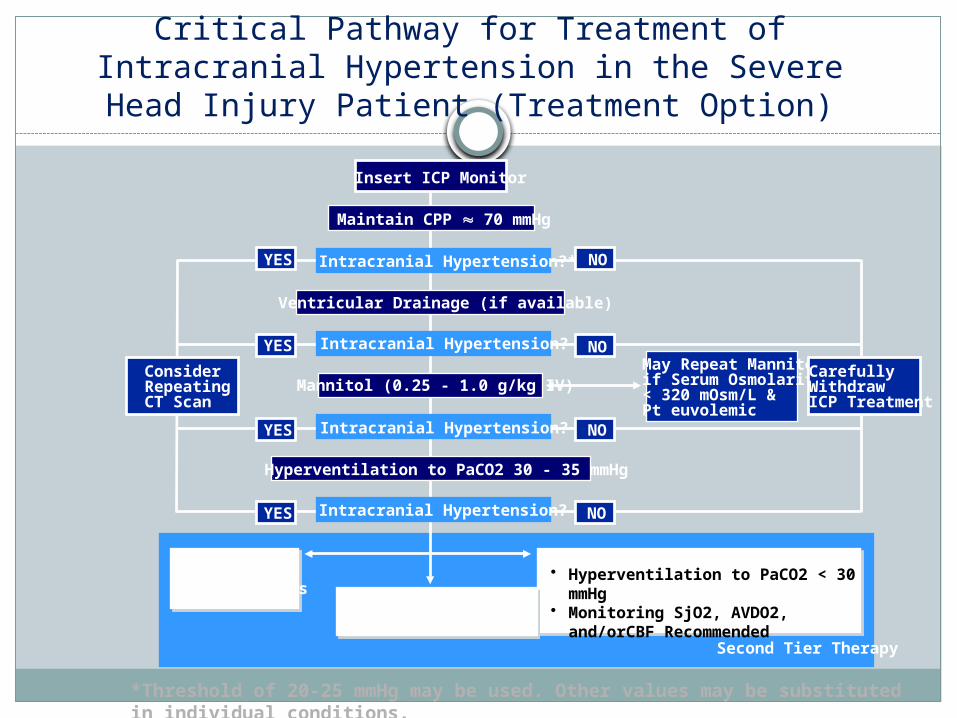
Critical Pathway for Treatment of Intracranial Hypertension in the Severe Head Injury Patient
(Treatment Option)
*Threshold of 20-25 mmHg may be used. Other values may be substituted in individual conditions.
May Repeat Mannitolif Serum Osmolarity< 320 mOsm/L &Pt euvolemic
High DoseBarbiturate therapy
• Hyperventilation to PaCO2 < 30 mmHg• Monitoring SjO2, AVDO2, and/orCBF
Recommended
Other SecondTier Therapies
NO
YES NO
YES NO
YES NO
CarefullyWithdrawICP Treatment
ConsiderRepeatingCT Scan
YES
Second Tier Therapy
Intracranial Hypertension?
Hyperventilation to PaCO2 30 - 35 mmHg
Intracranial Hypertension?
Mannitol (0.25 - 1.0 g/kg IV)
Intracranial Hypertension?
Ventricular Drainage (if available)
Intracranial Hypertension?*
Maintain CPP 70 mmHg
Insert ICP Monitor
Osmotherapy
Mannitol induces changes in blood rheology and increases cardiac output, leading to improved CPP and cerebral oxygenation.
Improvements in cerebral oxygenation induce cerebral artery vasoconstriction and subsequent reduction in cerebral blood volume and ICP.
Mild dehydration after osmotherapy is desirable and may improve cerebral edema.
Also it decreases CSF production by up to 50%, lead to prolonged ICP decrease.
Mannitol
GuidelineMannitol is effective for control of raised ICP
after severe head injury.
OptionEffective doses range from 0.25 - 1.0 gm/kg
body weight.
Mannitol has several limitations;• Hyperosmolality is a common problem, and a
serum osmolarity >320 mOsmol/L is associated with adverse renal and central nervous system effects.
• Accumulation of mannitol in cerebral tissue may lead to a rebound phenomenon and increased ICP.
• The indications for the use of mannitol prior to ICP monitoring are signs of transtentorial herniation or progressive neurological deterioration not attributable to systemic pathology.
The most promising solution investigated as possible substitute for mannitol; is hypertonic saline (HTS). Serum Na is maintained between 145 and 155 mmol/L in all patients with TBI. To start osmotherapy,250-mL bolus of 3% HTS is administered through a central venous cannula. This dose is repeated until ICP is controlled or a Na level of 155 mmol/L is achieved. The serum Na is maintained at this level until ICP has stabilized and then gradually allowed to normalize.
The permeability of the BBB to sodium is low.HTS produces an osmotic
gradient between the intravascular and intracellular compartments,
leading to shrinkage of brain tissue (where BBB is intact) and therefore
reducing ICP.
The selectivity of the BBB to NaCl is more than that of mannitol making
it potentially a more effective osmotic drug.
HTS augments volume resuscitation and increases circulating BV, MAP,
and CPP.
HTS restores the neuronal membrane potential, maintains BBB
integrity, and modulates the inflammatory response by reducing
adhesion of leukocytes to endothelium.
If ICP control is still problematic after 3–4 days of HTS therapy, boluses of furosemide are administered in an effort to mobilize tissue Na.
Serum sodium and potassium concentrations are monitored four hourly on a blood gas analyzer.
Analgesia and Sedation
Morphine or fentanyl can be used for analgesia but with caution for their respiratory depression in case patient is spontaneously breathing.
Remifentanyl can be used in ventilated patients.
Propofol is sedative of choice especially in first 48 hours. It causes cerebral metabolic suppression and has neuroprotective effect. Using propofol in doses more than 5mg/Kg and for longer than 48hrs;
Midazolam should replace propofol for sedation. (for fear of propofol infusion syndrome).
Barbiturates
GuidelineHigh-dose barbiturate therapy may be
consideredin hemodynamically stable salvagable severe head injury patients with intracranial hypertension refractory to maximal medical and surgical ICP lowering therapy.
Barbiturate Coma
High-dose barbiturates are used to control intracranial hypertension in selected patients. ICP is decreased due to decrease in CBV due to vasoconstriction caused by increase in cerebrovascular resistance.Indications:1. Potentially survivable head injury2. No surgically treatable lesion accounting for intracranial hypertension
(except when used for preparation for surgery)3. Other conventional therapies of controlling ICP have failed (posture,
hyperventilation, osmotic and tubular diuretics, corticosteroids)4. ICP > 20 to 25 mmHg for more than 20 min, or >40 mmHg at any time5. Unilateral cerebral hemispheric edema with significant (>.7 mm) shift of
midline structures shown on CT6. A low Glasgow Coma score
Takeko Toyama, MD Assistant Professor of Anesthesiology University of Miami, Miami, FL
Goals1. Maintenance ICP < 20 mmHG2. Therapeutic EEG response: burst
suppression or cortical electrical silence (with preservation of SSEP and BAEF)
Benefits:1. Decrease in cerebral metabolic rate (CMRO2), caused by decrease in
synaptic transmission, presumably by affecting GABA transmission2. Decrease in cerebral blood volume and ICP, due to increase in
cerebrovascular resistance, due vasoconstriction -Both CMRO2 and CBF are decreased in a dose dependent fashion: About 50% decrease at a dose sufficient to produce isoelectric EEG
3. Promote or induce hypothermia4. Increase in IC glucose, glucagon, and phosphocreatine energy store5. Decrease in nitrogen excretion following acute head injury6. Shunt blood from regions of normal perfusion to those of reduced
CBF due to vasoconstriction7. Anticonvulsant prophylaxis8. Stabilization of lysosomal membranes9. Decrease in excitatory neurotransmitters and IC calcium10. Free radical scavenging ( thiopental only)
Risks:1. Direct myocardial depressant2. Increase in venous capacitance, due to
central and peripheral sympatholytic action3. Impaired gastrointestinal motility Increased
hepatic microsomal activity4. Direct CNS depressant, resulting in
unreliable neurological examination5. Possible allergic reaction Impaired
lymphocyte immune response and function
Dosing RegimensPentobarbital: High dose:
Loading:30-40 mg/Kg over 4 hours (~2500mg/70Kg) Maintenance: 1.8-3.3mg/Kg/hr (~175mg/70Kg)
Mid-level dose: Loading: 10mg/Kg over 30min, 20-25mg/Kg over 4hrmaintenance: 5mg/Kg/hr for 3hrs,then 2-2.5mg/Kg/ with 5mg/Kg bolus prn if serum level < 3mg/dl
Low dose: Loading: 3-6mg/Kg over 30min Maintenance: .3- 3mg/Kg/hr
Therapeutic serum level: 2.5-4 mg/dl ( 6 mg/dl may be needed )Thiopental:
Loading: 3mg/Kg bolus, followed by 10-20mg/Kg over 1 hr Maintenance: 3-5 mg/Kg/hr Therapeutic serum level: 6-8.5 mg/dl Weaning: dosage is halved q 12 hr.
MonitoringCardiovascular1. A-line: arterial BP, blood gases2. PA catheter: CO, CI, SV, SVR, PVR, right heart filling pres., PCWP3. Bladder catheter: urine outputCerebrovascular and neurophysiological4. ICP: maintain < 25 mmHg, preferably less5. CPP: maintain > 70 mmHg6. EEG: burst suppression, or cortical electrical silence optional7. Brain temperature8. Jugular bulb O2 monitor/ oxymeter catheter9. Somatosensory or brainstem auditory evoked potentials (SSEP, BAEF)Other monitoring10. Core body temperature: NP, TM, E: 32 to 35 degrees C is acceptable11. Serum barbiturate levels12. nasogastric catheter: pH and output13. intake and outputTherapy may be required for 7-14 days or longer, may be weaned after 3-6
days
1. Therapeutic end points
2. Success:1. ICP < 20 mmHg for at least 48 hours, at a minimum2. Resolution of intracranial mass effects or midline shift, preferably3. ICP must remain controlled with conventional therapies
3. Failure:1. Diagnosed brain death2. Uncontrollable ICP despite adequate serum levels, EEG burst-3. Suppression, or electrical silence4. Intolerable side effects;
1. Hypotention not responsive to cardiac inotropes, peripheral vaso- pressors, or intravenous fluid therapy (cardiac isotopes: dopamine, dobutamine, epinephrine) (peripheral vasopressors: ephedrine, phenylephrine)
2. (IV fluids: packed RBCs, albumine, hetastarch, LR)3. Progressive pulmonary dysfunction4. Sepsis
Steroids
StandardThe use of steroids is not recommended for
improving outcome or reducing intracranial pressure in patients with severe head injury.
Multiple prospective, randomized studies have demonstrated no benefit in lowering ICP or improvement in patient outcome through the use of high-dose corticosteroids in acute TBI .
The use of methylprednisolone in patients with moderate to severe TBI has been demonstrated to increase mortality and is contraindicated.

Mechanical ventilation
In TBI patients, hypoxia, hypercarbia / hypocarbia should be prevented.PaO2 should be above 100mmHg and SpO2 above 95%. Mechanical ventilation should be started at GCS 8. PaCO2 in first 24hrs should be 34-38mmHg and mild hyperventilation can be started for PaCO2 to be 32-35mmHg in case of increased ICP.Monitor end tidal CO2 and perform blood gases 15-20 min. after any change in ventilatory parameters.
Hyperventilation
Standard In the absence of increased intracranial pressure (ICP), chronic
prolonged hyperventilation therapy (PaCO2 of 25 mm Hg or less)should be avoided after severe traumatic brain injury (TBI).
Guideline The use of prophylactic hyperventilation (PaCO2 < 35 mm Hg)
therapy during the first 24 hours after severe TBI should be avoided because it can compromise cerebral perfusion during a time when cerebral blood flow (CBF) is reduced.
Option Hyperventilation therapy may be necessary for brief periods
when there is acute neurologic deterioration, or for longer periods if there is intracranial hypertension refractory to sedation, paralysis, cerebrospinal fluid (CSF) drainage, and osmotic diuretics.
Hypercapnea is a potent cerebral vasodilator and should be avoided in patients with cerebral edema and elevated ICP.
Hyperventilation reduces ICP by causing cerebral vasoconstriction and reducing cerebral blood flow.
Aggressive hyperventilation has been used for years in the treatment of elevated ICP, but has been demonstrated to have a deleterious outcome
Hyperventilation should be avoided in the first 24 hours post-injury when cerebral blood flow is often critically reduced.
Hyperventilation may have a role as a temporizing measure in the acute reduction of elevated ICP.
When hyperventilation is used for more than a brief period of time, monitoring of cerebral oxygenation using either jugular venous bulb oximetry (SjvO2) or brain tissue oxygen tension (PbrO2) should be considered.
Neuromuscular blockade
May be considersd to facilitate endotracheal intubation.
In cases of difficult ventilation inspite of adequate sedation/analgesia.
Use of neuromuscular blockade may mask seizure activity, increase risk of pneumonia and cause critical illness neuropathy.
Patient positioning
Patient head should be in neutral position with head of bed elevated 15-30 degree.
Neck collar should be applied whenever there is doubt of cervical spine injury.

Surgical Intervention
Whenever decided by neurosurgeon to decrease intracranial hypertension.
Surgery can be performed on mass lesions or to eleminate objects that penetrated the brain.
Mass lesions are like contusions or haematomas causing significant shift of intracranial structures.
Maintenance of haematological parameters
Monitor HCT or haemoglobin level as CBF is influenced by blood viscosity which increases by increase in HCT.CBF is reduced by HCT levels above 50% and increased by HCT levels below 30%. HTC of 30-34% is suggested to be best for optimal oxygen delivery to brain tissue.
Antiseizure Prophylaxis
StandardProphylactic use of phenytoin,
carbamazepine, phenobarbital or valproate is not recommendedfor preventing late post-traumatic seizures.
Control of seizures
Seizure activity in TBI patients may cause secondary brain damage as a result of increased metabolic demands, raised ICP and excess neurotransmitter release.Benzodiazepines should be started together with phenytoin . Adequate sedation with propofol reduces seizure activity and raises seizure threshold.
Fever
Elevated body temperature increases the patient’s inflammatory response by elevating levels of pro-inflammatory cytokines and neutrophils. This can increase sympathetic tone, resting energy expenditure, oxygen consumption, heart rate, and minute ventilation.
While fever occurs in 30-45% of the non-neurologically injured, it may be seen in up to 70% of those with TBI. In these patients, an infectious etiology is present less than 50% of the time, with the remainder being classified as “central fever.”
Central fever is believed to be due to direct damage to the thermoregulatory centers of the brain, which are found in the preoptic nucleus of the hypothalamus and focal centers of the pons. Severe damage to these centers can also result in profound hypothermia, which can result in coagulopathy, cardiac arrhythmias, or depressed immune function.
Early fever following TBI has been associated with lower GCS, presence of diffuse axonal injury, cerebral edema, hypotension, hypoglycemia, and leukocytosis .
Fever within the first week is associated with increased intracranial pressure, neurologic impairment, and prolonged ICU stay
Hypothermia is also associated with worse outcomes in TBI.
Aggressive efforts to control temperature in the TBI patient should be implemented including early intravenous and enteral antipyretic medications, control of room temperature, and cooling blankets or pads.
Due to the deleterious effect of temperature on brain parenchyma, therapy should be initiated when patient temperature exceeds 37˚ Celsius rather than waiting until the traditional definition of fever has been reached.
Therapeutic Hypothermia
Therapeutic hypothermia has been demonstrated to improve neurologic outcome following witnessed arrest from ventricular fibrillation or pulseless ventricular tachycardia.
Data supporting its use following TBI has been less convincing.
While normothermia has few potential side effects, the potential complications of therapeutic hypothermia include hypotension, arrhythmia, electrolyte disorders, impaired coagulation, shivering, hyperglycemia, and increased risk of infection.
Therapeutic hypothermia may have a role in the treatment of patients with severe TBI and refractory ICP, but should only be used after consultation between the attending intensivist and neurosurgeon.
When therapeutic hypothermia has been initiated, therapy should be continued until ICP < 20 mmHg for 48 hrs at which time patients may be rewarmed at a rate not to exceed 0.1˚ Celsius per hour with close monitoring for the development of rebound intracranial hypertension.
Shivering management When body temperature is lowered, the physiologic response is to
prevent further heat loss through vasoconstriction. When vasoconstriction is no longer effective, shivering occurs to counterbalance heat loss.
In the context of induced hypothermia, shivering is undesirable because it causes patient discomfort, increases body temperature, increases metabolic / oxygen demand, and increases intraocular and intracranial pressures.
A step-wise approach to the prevention of shivering appears appropriate. Pharmacologic options for the control of shivering include: meperidine, morphine, fentanyl, propofol, magnesium, benzodiazepines, and neuromuscular blockers .
It is important to consider that data on pharmacologic interventions for shivering control are based upon experience with either health volunteers or in the postoperative setting (20-23). Therefore, the effect of repetitive dosing and prolonged use of these agents in therapeutic hypothermia is lacking (i.e. CNS toxicity associated with merperidine).
Targeted Temperature Management
With the deleterious effects of fever and hypothermia established for TBI patients, many modalities of achieving either normothermia or therapeutic hypothermia have been described .
Conventional cooling methods include skin exposure, ice, cold packs, infused cold fluid, peritoneal lavage, and antipyretics. There are also many commercially available cooling devices available. The Blanketrol (Cincinnati Subzero, Cincinnati, OH) is a water-circulating blanket system that utilizes two large cooling blankets, one beneath and one on top of the patient, to maintain the desired patient temperature.
The Arctic Sun (Medivance, Jugenheim, Germany) circulates water through gel pads that are applied to the patient’s back, abdomen, and thighs, automatically controlled by a rectal thermometer. Several intravascular cooling systems are also commercially available. These systems infuse cold fluids via a closed-loop central venous catheter to maintain the desired body temperature.
In a prospective study of ICU patients, Hoedemakers et al found superior temperature control using water-circulating blankets, gel-pads, and intravascular cooling as compared to conventional cooling techniques and air-circulating blankets /
Nutrition
GuidelineReplacement of 140% of Resting Metabolic
Expenditure in non-paralyzed patients and 100% Resting Metabolic Expenditure inparalyzed patients using enteral or parenteral formulas containing at least 15% of calories as protein by the seventh day after injury.
Prospective trial in 38 patients randomly assigned to receive total parenteral nutrition (TPN) or standard enteral nutrition (SEN).
The TPN group got full nutritional support by 7 days whereas the SEN group did not. There were significantly more deaths in the group that did not receive full caloric replacement by the 7th day after injury.
J. Neurosurg 58:907-912, 1983
Monitoring renal function
Urine output should be 0.5-1ml/Kg/min.Diabetes insipidus should be suspected if urine output is more than 250ml/hr, for more than 3hrs. and specific gravity less than 1005,confirmed by serum and urine osmolalities. If confirmed , start desmopressin.
TIERS OF THERAPY
TIER ZERO TIER ONE TIER TWO TIER THREE
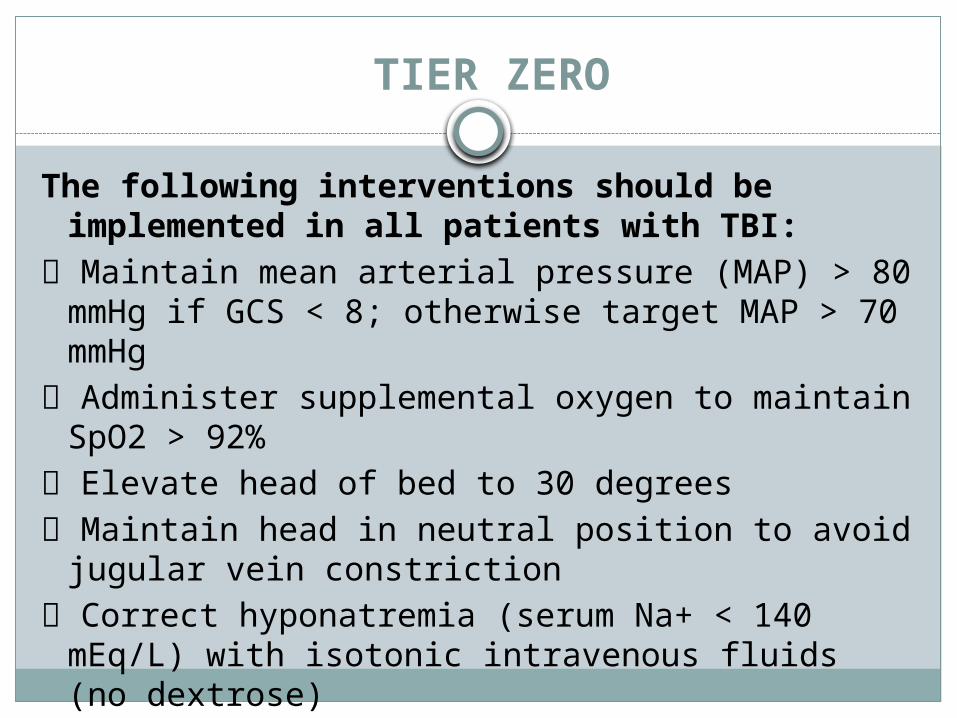
TIER ZERO
The following interventions should be implemented in all patients with TBI:
Maintain mean arterial pressure (MAP) > 80 mmHg if GCS < 8; otherwise target MAP > 70 mmHg
Administer supplemental oxygen to maintain SpO2 > 92%
Elevate head of bed to 30 degrees Maintain head in neutral position to avoid
jugular vein constriction Correct hyponatremia (serum Na+ < 140 mEq/L)
with isotonic intravenous fluids (no dextrose)
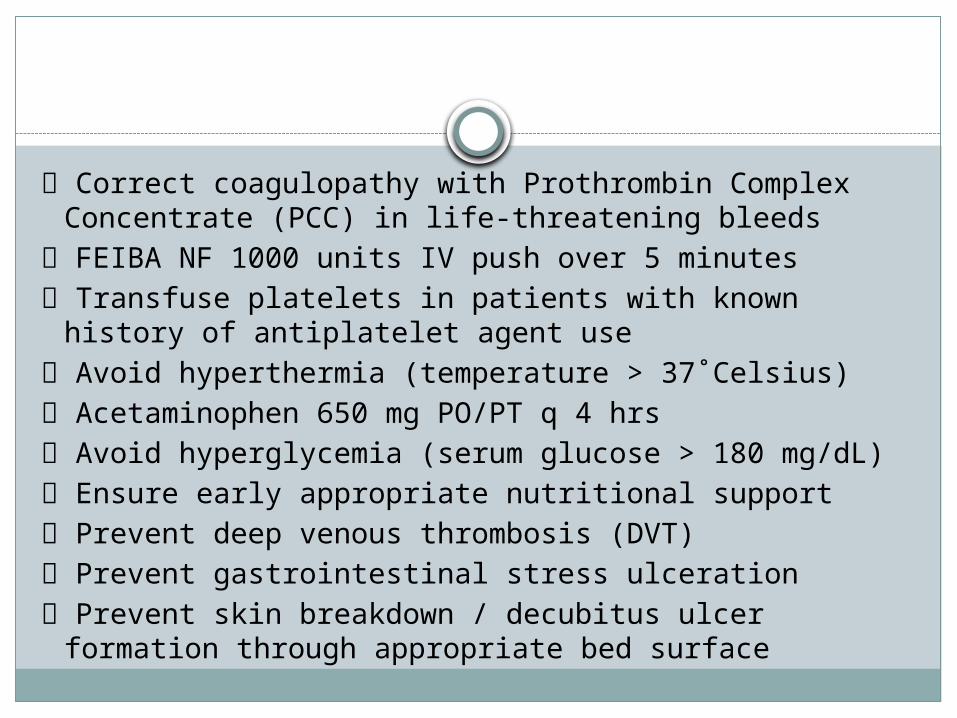
Correct coagulopathy with Prothrombin Complex Concentrate (PCC) in life-threatening bleeds
FEIBA NF 1000 units IV push over 5 minutes Transfuse platelets in patients with known history of
antiplatelet agent use Avoid hyperthermia (temperature > 37˚Celsius) Acetaminophen 650 mg PO/PT q 4 hrs Avoid hyperglycemia (serum glucose > 180 mg/dL) Ensure early appropriate nutritional support Prevent deep venous thrombosis (DVT) Prevent gastrointestinal stress ulceration Prevent skin breakdown / decubitus ulcer formation
through appropriate bed surface
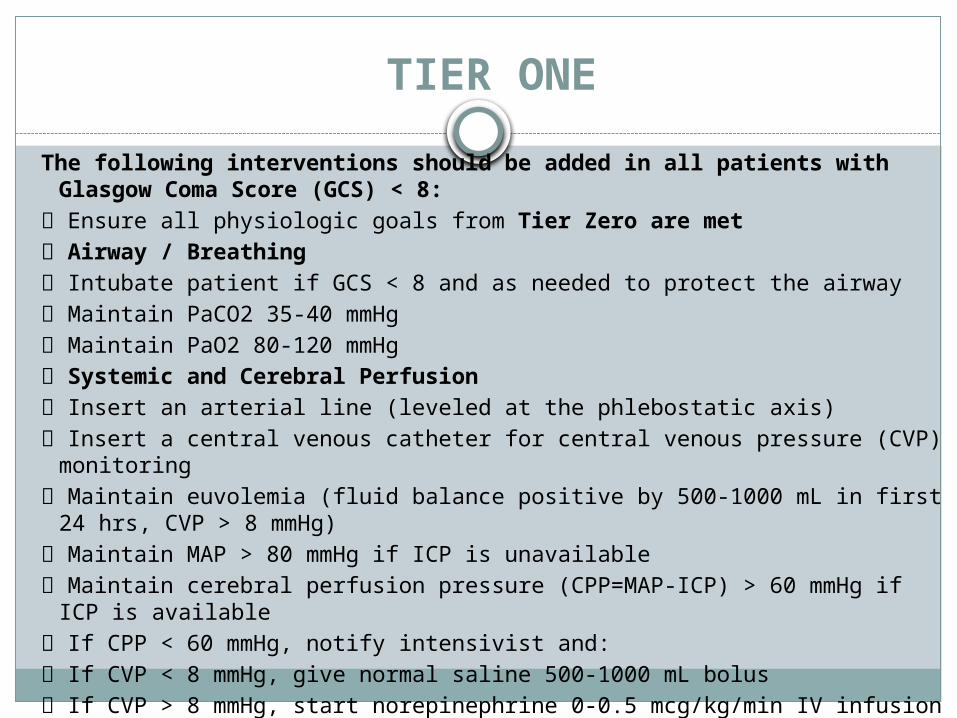
TIER ONE The following interventions should be added in all patients with Glasgow
Coma Score (GCS) < 8: Ensure all physiologic goals from Tier Zero are met Airway / Breathing Intubate patient if GCS < 8 and as needed to protect the airway Maintain PaCO2 35-40 mmHg Maintain PaO2 80-120 mmHg Systemic and Cerebral Perfusion Insert an arterial line (leveled at the phlebostatic axis) Insert a central venous catheter for central venous pressure (CVP) monitoring Maintain euvolemia (fluid balance positive by 500-1000 mL in first 24 hrs,
CVP > 8 mmHg) Maintain MAP > 80 mmHg if ICP is unavailable Maintain cerebral perfusion pressure (CPP=MAP-ICP) > 60 mmHg if ICP is
available If CPP < 60 mmHg, notify intensivist and: If CVP < 8 mmHg, give normal saline 500-1000 mL bolus If CVP > 8 mmHg, start norepinephrine 0-0.5 mcg/kg/min IV infusion to
maintain CPP
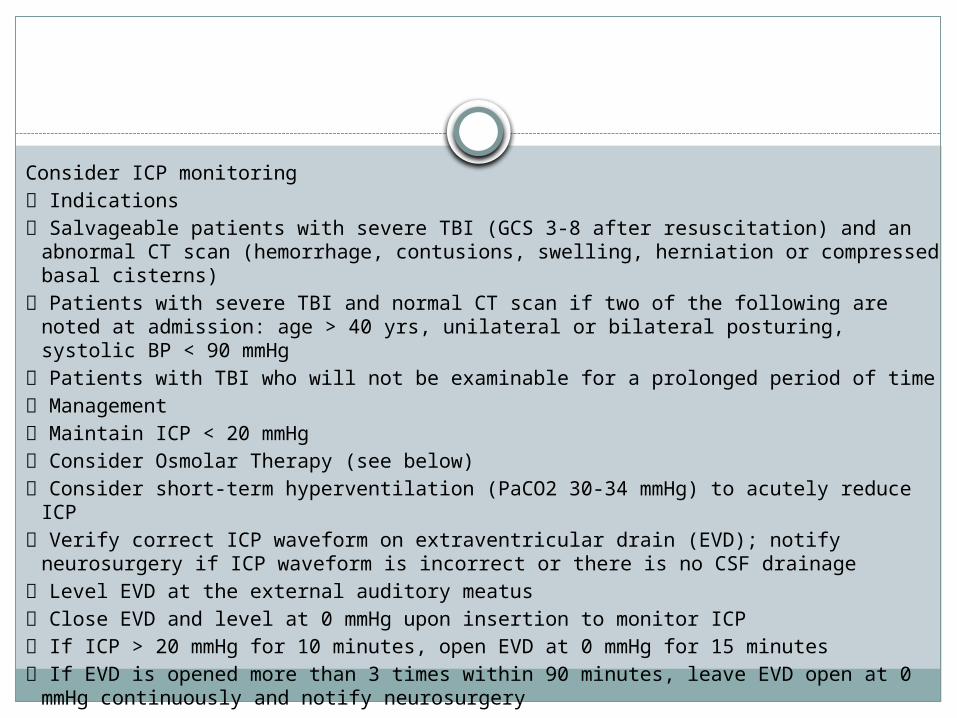
Consider ICP monitoring Indications Salvageable patients with severe TBI (GCS 3-8 after resuscitation) and an
abnormal CT scan (hemorrhage, contusions, swelling, herniation or compressed basal cisterns)
Patients with severe TBI and normal CT scan if two of the following are noted at admission: age > 40 yrs, unilateral or bilateral posturing, systolic BP < 90 mmHg
Patients with TBI who will not be examinable for a prolonged period of time Management Maintain ICP < 20 mmHg Consider Osmolar Therapy (see below) Consider short-term hyperventilation (PaCO2 30-34 mmHg) to acutely reduce ICP Verify correct ICP waveform on extraventricular drain (EVD); notify neurosurgery
if ICP waveform is incorrect or there is no CSF drainage Level EVD at the external auditory meatus Close EVD and level at 0 mmHg upon insertion to monitor ICP If ICP > 20 mmHg for 10 minutes, open EVD at 0 mmHg for 15 minutes If EVD is opened more than 3 times within 90 minutes, leave EVD open at 0 mmHg
continuously and notify neurosurgery

Osmolar Therapy First line therapy 3% normal saline IV bolus 100-250 mL q 2 hrs prn ICP >
20 mmHg for > 10 minutes Alternate therapy Mannitol 0.25-1.0 gm/kg IV q 6 hrs prn ICP > 20 mmHg Measure serum osmolality and electrolytes q 6 hrs Notify intensivist if serum Na changes by > 3 mEq/L from
previous measurement Hold hypertonic saline therapy for serum Na > 160 mEq/L Hold mannitol therapy for serum osmolality > 320 mOsm
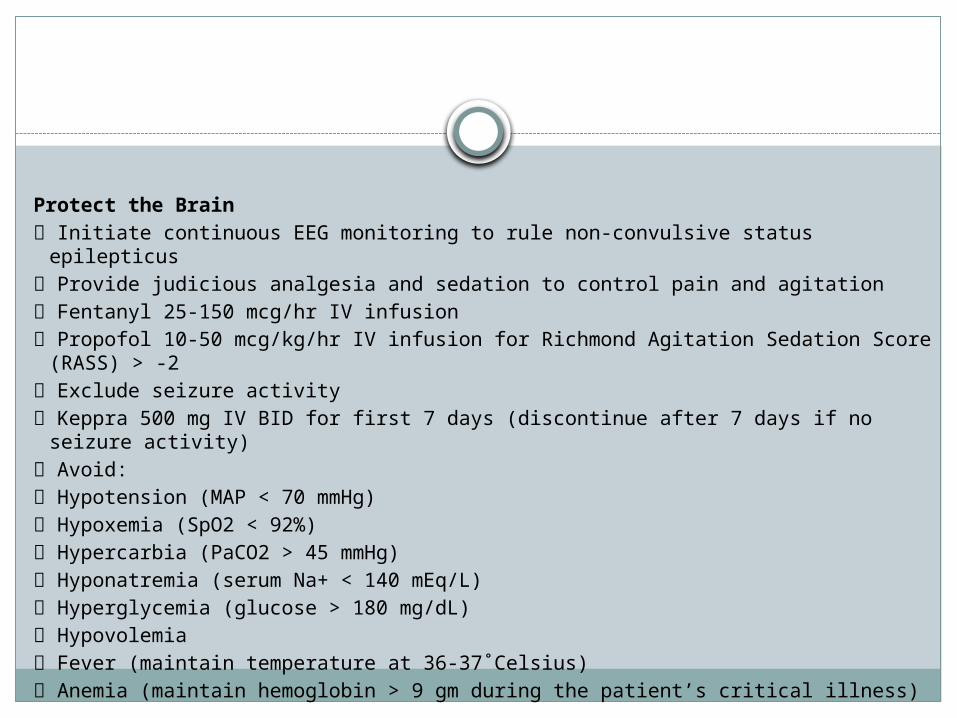
Protect the Brain Initiate continuous EEG monitoring to rule non-convulsive status epilepticus Provide judicious analgesia and sedation to control pain and agitation Fentanyl 25-150 mcg/hr IV infusion Propofol 10-50 mcg/kg/hr IV infusion for Richmond Agitation Sedation Score (RASS)
> -2 Exclude seizure activity Keppra 500 mg IV BID for first 7 days (discontinue after 7 days if no seizure activity) Avoid: Hypotension (MAP < 70 mmHg) Hypoxemia (SpO2 < 92%) Hypercarbia (PaCO2 > 45 mmHg) Hyponatremia (serum Na+ < 140 mEq/L) Hyperglycemia (glucose > 180 mg/dL) Hypovolemia Fever (maintain temperature at 36-37˚Celsius) Anemia (maintain hemoglobin > 9 gm during the patient’s critical illness)
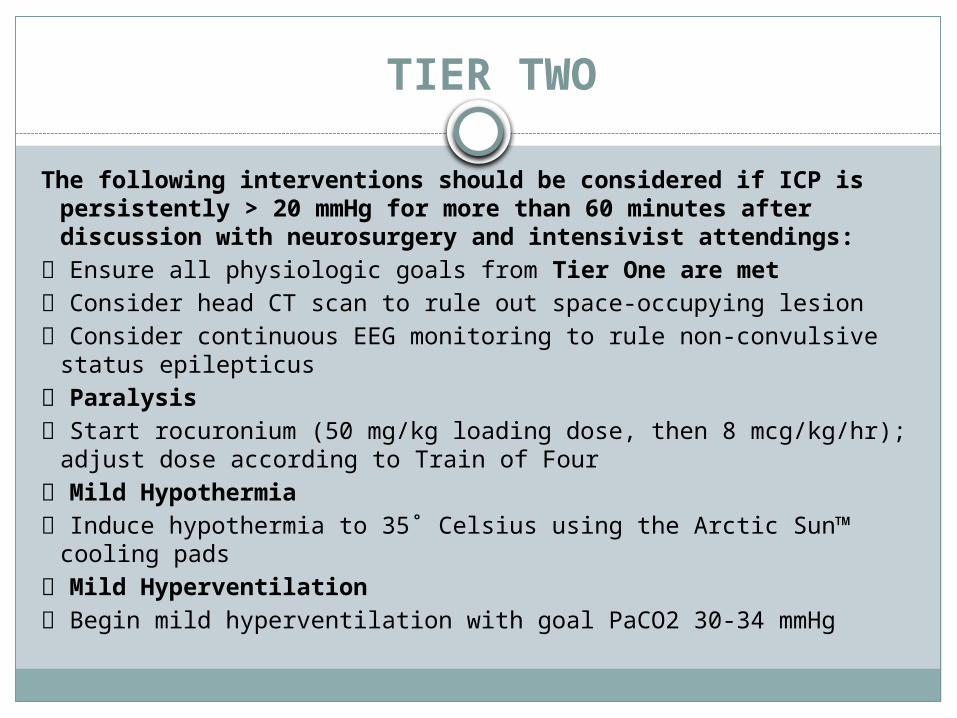
TIER TWO
The following interventions should be considered if ICP is persistently > 20 mmHg for more than 60 minutes after discussion with neurosurgery and intensivist attendings:
Ensure all physiologic goals from Tier One are met Consider head CT scan to rule out space-occupying lesion Consider continuous EEG monitoring to rule non-convulsive status
epilepticus Paralysis Start rocuronium (50 mg/kg loading dose, then 8 mcg/kg/hr); adjust
dose according to Train of Four Mild Hypothermia Induce hypothermia to 35˚ Celsius using the Arctic Sun™ cooling pads Mild Hyperventilation Begin mild hyperventilation with goal PaCO2 30-34 mmHg
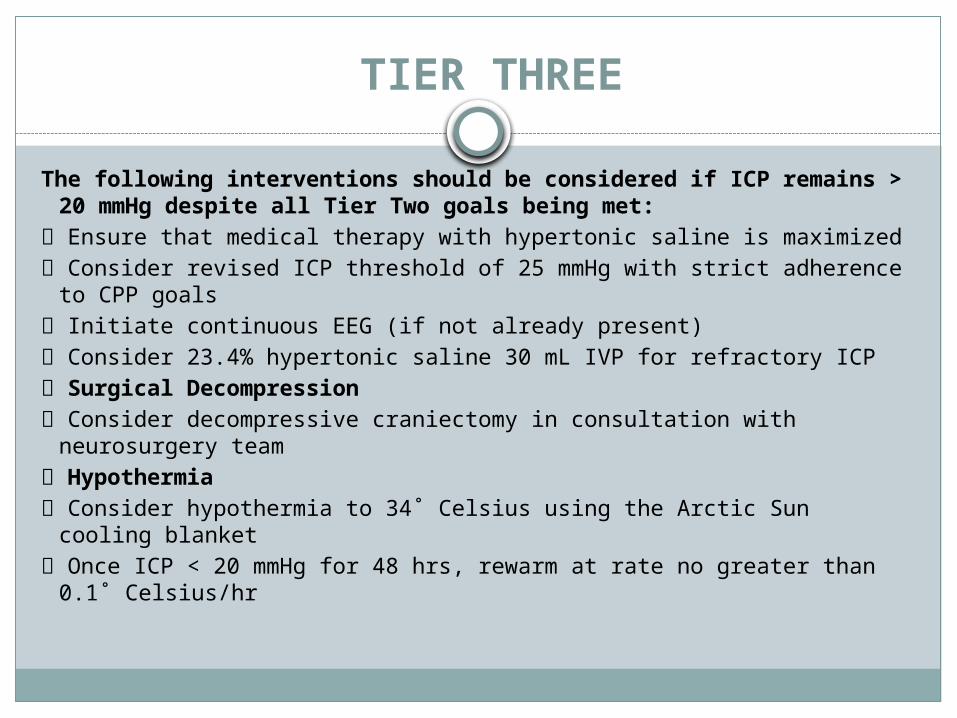
TIER THREE
The following interventions should be considered if ICP remains > 20 mmHg despite all Tier Two goals being met:
Ensure that medical therapy with hypertonic saline is maximized Consider revised ICP threshold of 25 mmHg with strict adherence to
CPP goals Initiate continuous EEG (if not already present) Consider 23.4% hypertonic saline 30 mL IVP for refractory ICP Surgical Decompression Consider decompressive craniectomy in consultation with
neurosurgery team Hypothermia Consider hypothermia to 34˚ Celsius using the Arctic Sun cooling
blanket Once ICP < 20 mmHg for 48 hrs, rewarm at rate no greater than 0.1˚
Celsius/hr
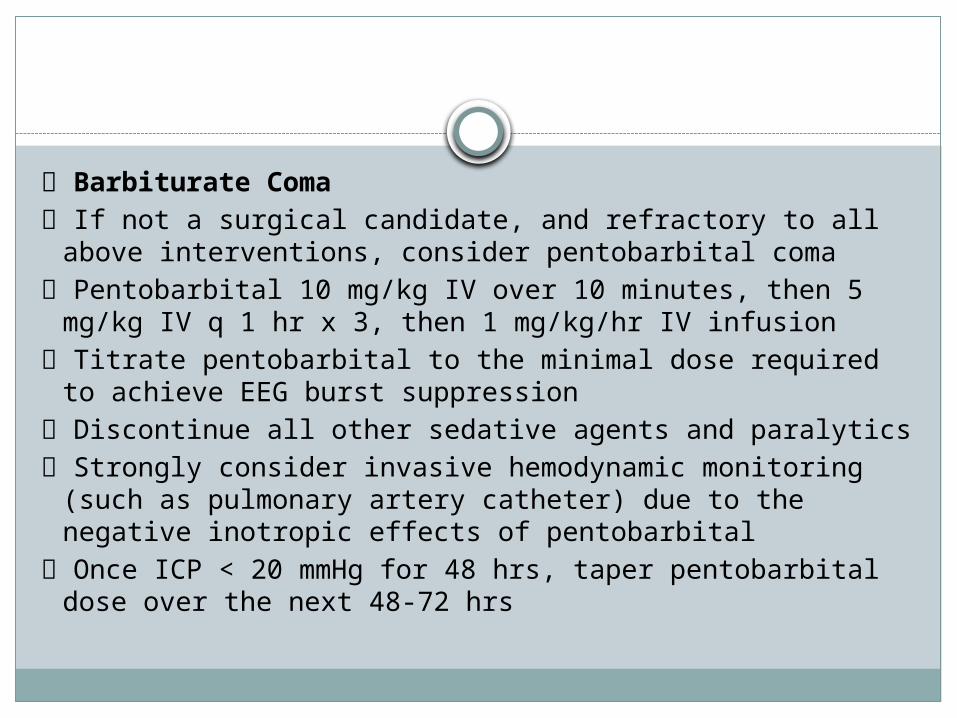
Barbiturate Coma If not a surgical candidate, and refractory to all above
interventions, consider pentobarbital coma Pentobarbital 10 mg/kg IV over 10 minutes, then 5 mg/kg
IV q 1 hr x 3, then 1 mg/kg/hr IV infusion Titrate pentobarbital to the minimal dose required to
achieve EEG burst suppression Discontinue all other sedative agents and paralytics Strongly consider invasive hemodynamic monitoring (such
as pulmonary artery catheter) due to the negative inotropic effects of pentobarbital
Once ICP < 20 mmHg for 48 hrs, taper pentobarbital dose over the next 48-72 hrs
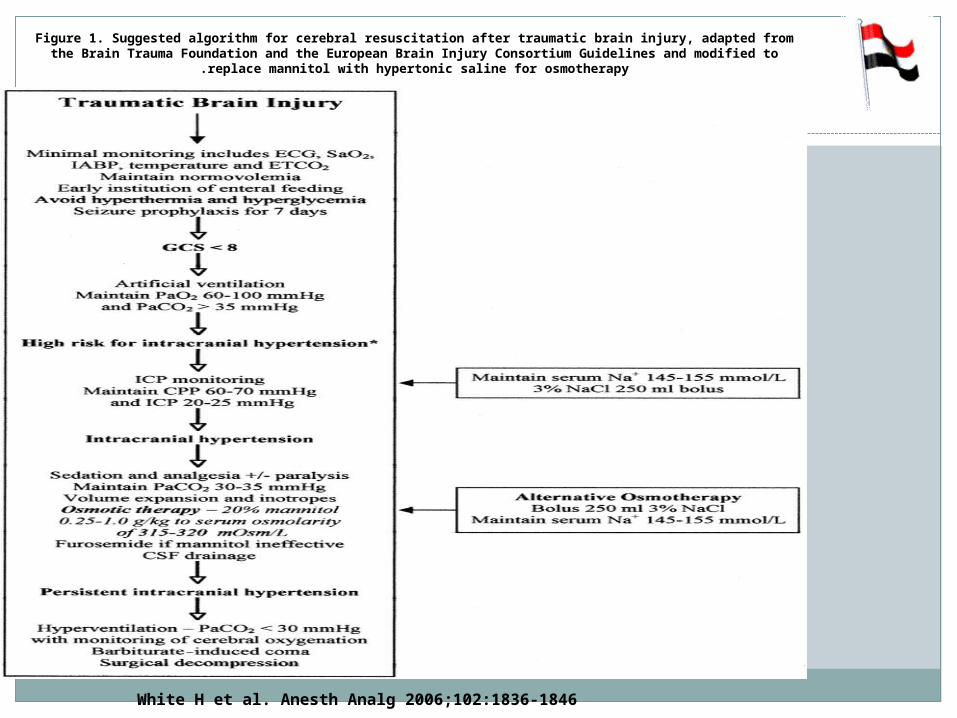
Figure 1. Suggested algorithm for cerebral resuscitation after traumatic brain injury, adapted from the Brain Trauma Foundation and the European Brain Injury Consortium Guidelines and modified to replace
mannitol with hypertonic saline for osmotherapy.
White H et al. Anesth Analg 2006;102:1836-1846



















