Embed Size (px)
Citation preview

Stevens-Johnson syndrome
• A form of TEN, life- threatening skin condition, medical emergency.
• Extensive widespread necrosis, causing epidermis to separate from the dermis.
By: Arravindh Vivekananthan

Pathophysiology
Hypersensitivity reaction• Type III (IC rxn)• Type IV ( cytotoxic CD8+ T lymphocyte)

Severe Cutaneous
Adverse Reaction
Erythema multiforme
SJS
SJS/TEN
TEN

SJS : with bullae, + mucous membrane involvement
when <10% is called Steven Johnson Syndromewhen 10-30% bullae called Steven Johnson
Syndrome-Toxic Epidermal-Necrolysis (SSJ-TEN)when the bullae> 30% is called Toxic Epidermal
Necrolysis (TEN).








SSSSsparing of mucous membranes and risk factors,such as drug history and clinical suspicion of staphylococcal infection.

• SKIN BIOPSY: non-inflammatory superficial splitting of the epidermis
• Blood Culture


Stevens-Johnson syndrome
• Etiology– Drug-induced (60%)– Infection (20%)– Idiopathic (20%)


– InfectionsPaeds : EBV, enterovirus, URTIViral : HSV, HIV, mumpsBacterial : Group A B-Haemolytic, diphteria, M.pneumonieFungal : coccidioidomycosis, dermatophytosis, and histoplasmosis

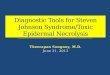
Clinical Manifestation
• Prodromal symptoms (1- 14 days):– Non- specific symptoms : fever, headache, sore
throat, cough, malaise and/or burning of the eyes followed by the appearance of mucocutaneous lesions.
– Mucous membrane– Diffuse rash, flaccid blistering. ( + Nikolsky’s sign)

• Ocular sequelae – Corneal ulceration, anterior uveitis, blepharitis– Vision loss, severe dry eye ( 1-3%)
• Esophagus, small bowel, colon involvement – Esophageal strictures, impair enteral nutrition, absorption of oral medications.
• Tracheobronchial mucosa shedding – Respiratory failure 20% mechanical ventilation
• Vaginal stenosis and penile scarring
• PTSD in survivors
• Renal complications (rare)


History
• Cutaneous lesions develops abruptly:– typically are non-pruritic, but are painful
hemorrhagic erosions
• The rash begin as macules; develops into vesicles, bullae.
• Later rupture, leaving denuded skin. – Susceptible to secondary infection

Investigations
• FBC may reveal – Normal WBC count or leukocytosis– Highly elevated WBC count indicates a
superimposed bacterial infection

• Histological analysis of Skin Biopsy under direct immunofluorescence – Typical full- thickness epidermal necrolysis.– Due to extensive keratinocyte apoptosis.

full-thickness epidermal necrosis and separation of dermis and epidermis

full-thickness epidermal necrosis and separation of dermis and epidermis

necrotic keratinocytes within the entire epidermis and vacuolar degeneration at the dermal-epidermal junction resulting in subepidermal separation of the epidermis.

• Offending drugs must be stopped.• Refer to Burn Units/ ICU. Warm environment, I/V
analgesics.
• Supportive management, nutrition.• I/V fluids with 0.7mL/kg per % of BSA
• NG/ parenteral feeding.• Oral lesions : Analgesic mouth rinse for mouth ulcer.• Ocular involvement : referral to ophthalmologist
( ophthalmic steroid/ local antibiotics)• Denuded areas : non-adhesive dressings with silver
nitrate.