Embed Size (px)
Citation preview

Standards in health informatics– Problem, clinical models and terminologies
Silje Ljosland Bakke / Information architect, Nasjonal IKT HF / Co-lead, openEHR Foundation Clinical Models Program
E-mail: [email protected] / Twitter: @siljelb

2

An ongoing problem…“In attempting to arrive at the truth, I have applied everywhere for information but in scarcely an instance have I been able to obtain hospital records fit for any purpose of comparison.”
“If they could be obtained, they would enable us to decide many other questions besides the one alluded to. They would show subscribers how their money was being spent, what amount of good was really being done with it or whether the money was not doing mischief rather than good.”
- Florence Nightingale, 1863
Credit: Heather Leslie

Why is health IT so hard?
•Banks are acing it; why isn’t health?
–Complex and dynamic domain
–Lifelong records
–Clinical diversity
–Confidentiality
–Mobile population
Credit: Heather Leslie

Complexity
•Both the number of concepts and the rate ofchange is high•Health is big, and continually growing…
– In breadth– In depth– In complexity
•Clinical knowledge is continually changing
Credit: Heather Leslie

How have we been dealing with this?
•Free text(Specialist and administrative systems have more structured data, but generic electronic health recordsare still mainly free text)

So what do we need structure for?
•Avoid repetition and shadow records
•Retrieval and overview
•Reuse of record info
•Clinical decision support
•Quality indicators
•Management data

Longitudinal information access
•How long are you planning to live?
•Do you expect your health record to survivethat long?
•Even if it does survive, willit be readable for futuresystems and users?
Credit: Ricardo Correia

Celsius
Ear measurement
IR aural thermometer
Environment: 5° C
Wet clothing Space blanket
temperatureBodyStructuring health is hard
Credit: Bjørn Næss

Structuring identically is even harderExample: Smoking status in national registries: • 9 different variations on
“Smoking status” in 26 different forms
• Additionally: number of cigs per day, month quit smoking, number of months since quitting date, etc.
Brandt, Linn (2016). Report from REGmap February 2016 – Complete mapped register set - Preliminary analysis.

Structure is not the Messiah
•Structured data is not a goal in itself
•Structure where clear value can be identified
• It must be possible to add nuances using free text
•Sometimes free textis adequate/best suited for purpose
11

Semantic interoperability
•[…] the ability of computer systemsto exchange data with unambiguous, shared meaning
•A Holy Grail of health informatics
•Requires (amongst other things)shared information modelsand terminologies
12
NCOIC, "SCOPE", Network Centric Operations Industry Consortium, 2008
«Information model»?
•A definition of the structure and content of theinformation that should be collected or shared– A "minimal dataset"
– A message or interface definition
• Internally all applications have some sort ofinformation model
•Sharing information requires developing sharedinformation models
Credit: Ian McNicoll

How have we been doing infomodelling?
•Locked into each product
•In ways that clinicians don’t understand
•Few clinicians participating
•Technicians are left to interpret
•New requirements?

Clinicians must participate!•They’re the ones who know the domain
•Garbage in ⇒ garbage out
•Minimise wronginterpretations

Semantic interoperability* requiresidentical data models
Clinical information modelling is difficult andexpensive, and should be done once
⇒ Information models should be shared and governed strictly
* Level 4 semantic interoperability; Walker et al. (2005); http://www.ncbi.nlm.nih.gov/pubmed/15659453


National governance
•Managed by Nasjonal IKT
•Goal: Sharing quality information models
•Online collaboration tools:
–http://arketyper.no
–https://kilden.sykehusene.no/display/KLIM/
•More than 400 clinicians and health informaticiansparticipating
18

• Specification for structured health records
• openEHR Foundation (openehr.org)
• Free (as in beer AND speech)
• International community
• Two level modelling
• Not an open source application
• Not a downloadable app
Illustration: https://wolandscat.net/2011/05/05/no-single-information-model/

openEHR reference model
• EHR structure
• Security
• Versioning
• Participants, dates/times,data types
NO CONTENT
Credit: Heather Leslie

openEHR reference model
Domain
Core
RM

Archetypes
• Implementable specification for one clinical concept
• Comprehensible for non-techies
• Maximum datasets (aspirational)
• Reusable
THE STANDARDISED CONTENTCredit: Heather Leslie

Archetypes
23

Templates
• Combinations of constrained archetypes
• Data sets for forms, messages, interfaces, etc
• For specific use cases
• NOT user interfaces
THE USECASE SPECIFIC CONTENTCredit: Heather Leslie

Templates
25

Are information models enough?
•Sure, if we’re okay with making 100k models, one for each diagnosis, lab result, symptom, …
•Sure, if we never want a list of all the patientswho had viral lung diseases
•We need something more: Terminologies
30

Terms/knowledge abouthealth and healthcare:
TerminologiesVocabularies, classifications,
ontologies; ICD-10, SNOMED CT, ICF
Framework for informationabout single individuals:
Informationmodels
Information structure;openEHR archetypes, FHIR
resources
Rules to be applied to recorded information:
Inference modelsRules and knowledge bases
used in decision support and alert systems.
Some overlap
The things that actuallyhappen in healthcare:
Process models

Terminologies?
•Controlled vocabularies
•Classifications
•Ontological thesauri
32

Controlled vocabularies
•Flat lists of coded concepts
•Examples: code sets from hl7.org or volven.no
33

Classifications
•Hierarchies
•Examples: ICD-10, ATC
34

Ontological thesauri
•Polyhierarchies with associated attributes
•Synonyms
•Some are combinatorial
•Examples: SNOMED CT,ICNP
35

36

Terminologies vs information models
Information models can be said to describe the "questions"
Terminologies can give (some of) the"answers"
Complementary concepts
ICD_10::L40.0::Psoriasis vulgaris
and
SCT_2015::74757004::Skin structure of elbow
SCT_2015::6736007::Moderate
???

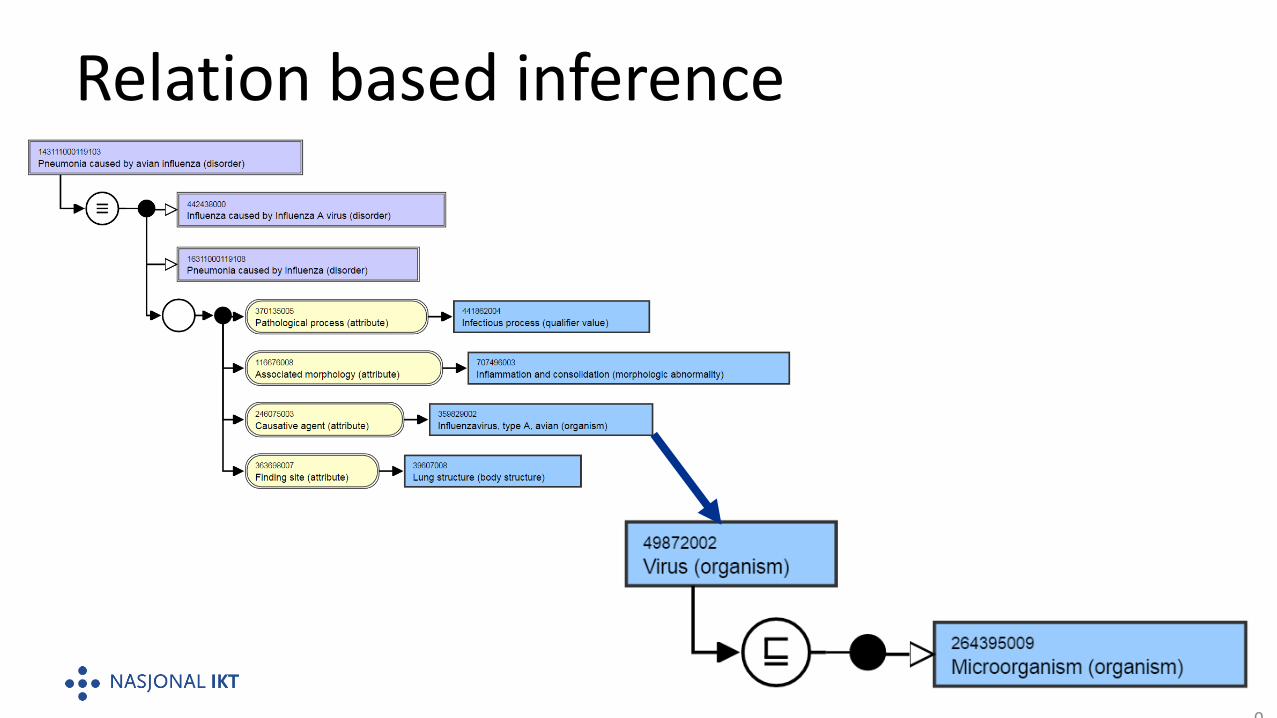
Where terminologies shine
•Hundreds of thousands of concepts
–Diagnoses, symptoms, lab results, body structures, organisms, procedures, …
•Inference based on relations between concepts
38

Relation based inference
39
Relation based inference
40

Where terminologies don’t shine
•Context
•Quantitative data types
•Complex concepts
41
Context
• "Let’s just chuck the codesin here so we can bill for thiscancer treatment!"
• 15 years later, from the brand new Dr. Google:– "Ma’am, I’m sorry to tell you you have ovarian cancer."– "What!? They were taken out 15 years ago!”
• Diagnosis code had no date to show when it was valid…
42

Quantitative data types
•«Wouldn’t it be really nice to just have a codefor the number of the pregnancy the woman is in…?"
•"Yeah. 10 ought to beenough for anybody."
Famous last words…
43

Complex concepts
•Combinatorial explosion
–"Every kind of rash for every skin area"
–Every combination of oral glucose challenge⇒ 601 LOINC "glucose" codes:
•Postcoordination maymitigate, but beware…
44
Grey areas
•Small value sets
•Some contextual information
–Actual diagnosis vs. tentative vs. risk vs. exclusionvs. family history
•Consistent use is hard, and not always appropriate
–Different use cases will have different requirements
45

Summary
• Structure is important, but not always appropriate
• Clinicians must drive clinical modelling
• Information models must be shared
• Terminologies are necessary additions to information models
• Grey areas -> pragmatic choice based on requirements
More info:
• Videos of one day seminar in Sweden 2015: http://goo.gl/6Ibbkf





























