Embed Size (px)
Citation preview
SMALL BOWEL OBSTRUCTION
Dr abdul rub Pgy3 mem
OVERVIEW:
•CLASSIFICATION •COMMON CAUSES OF OBSTRUCTION•CLINICAL FEATURES•INVESTIGATION•TREATMENT
What are our objectives?
we should be able to address the following questions1. Is this bowel obstruction or ileus?2. What is my immediate treatment plan?3. Is this a small or large bowel obstruction?4. Is this proximal or distal obstruction?5. What is the cause of this obstruction?6. Is this a complex or simple obstruction?7. How should I start investigating my patient?8. What is the role of other supportive investigations?9. What are the indications for surgery?
Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt
assessment, resuscitation and intensive monitoringObstruction A mechanical blockage arising from a
structural abnormality that presents as physical barrier the progression of gut contentsIleus :is a paralytic or functional variety of
obstruction
Obstruction is: Partial or complete Dynamic or a dynamic
Simple or strangulated
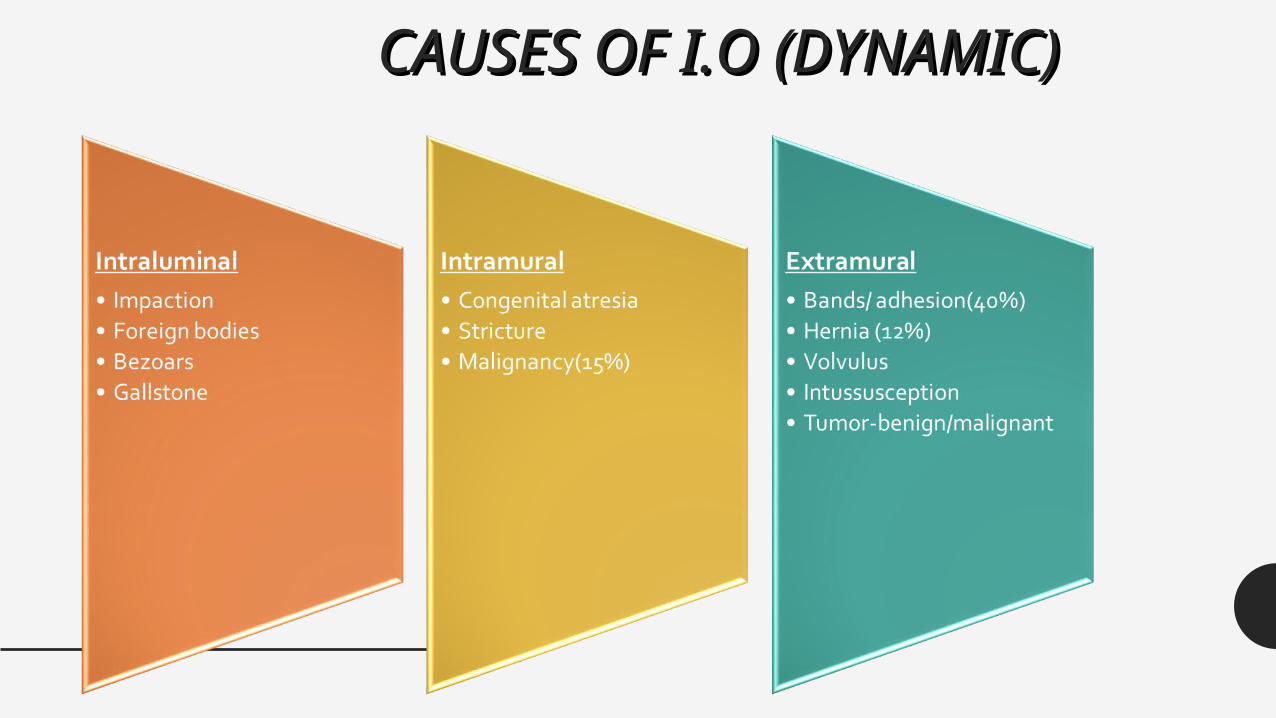
CAUSES OF I.O (DYNAMIC)CAUSES OF I.O (DYNAMIC)
Patho-physiology I 8L of isotonic fluid received by the small intestines (saliva,
stomach, duodenum, pancreas and hepatobiliary ) 6L absorbed 2L enter the large intestine and 200 ml excreted in the
faeces Air in the bowel results from swallowed air ( O2 & N2) and
bacterial fermentation in the colon ( H2, Methane & CO2), 600 ml of flatus is released Enteric bacteria consist of coliforms, anaerobes and
strep.faecalis. Normal intestinal mucosa has a significant immune role
Distension results from gas and/ or fluid and can exert hydrostatic pressure.
In case of BO Bacterial overgrowth can be rapid If mucosal barrier is breached it may result in translocation of
bacteria and toxins resulting in bactaeremia, septaecemia and toxaemia.
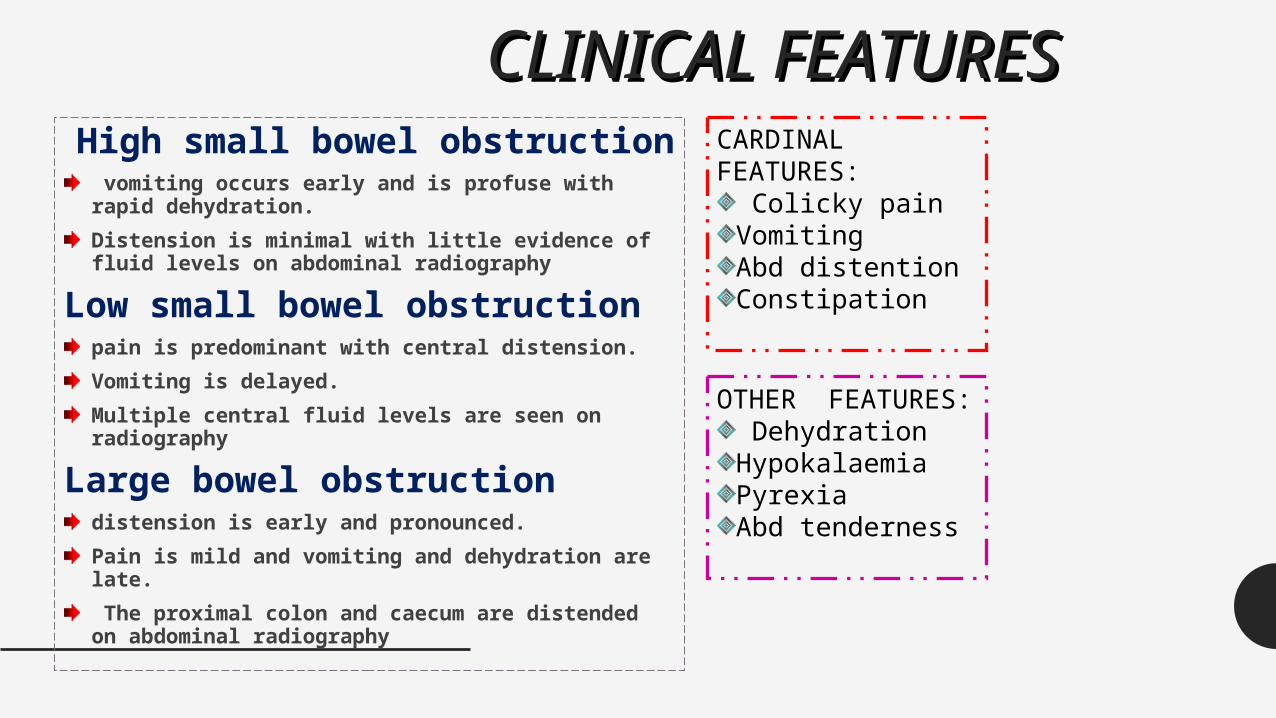
CLINICAL FEATURESCLINICAL FEATURES High small bowel obstruction
vomiting occurs early and is profuse with rapid dehydration. Distension is minimal with little evidence of fluid levels on abdominal radiography
Low small bowel obstructionpain is predominant with central distension.Vomiting is delayed.Multiple central fluid levels are seen on radiography
Large bowel obstructiondistension is early and pronounced. Pain is mild and vomiting and dehydration are late. The proximal colon and caecum are distended on abdominal radiography
CARDINAL FEATURES:
Colicky painVomitingAbd distentionConstipation
OTHER FEATURES: DehydrationHypokalaemiaPyrexiaAbd tenderness
Clinical Findings2. Examination
General
•Vital signs: P, BP, RR, T, Sat•dehydration•Anaemia, jaundice, LN•Assessment of vomitus if possible•Full lung and heart examination
Abdominal
•Abdominal distension and it’s pattern•Hernial orifices•Visible peristalsis•Cecal distension•Tenderness, guarding and rebound•Organomegaly•Bowel sounds
–High pitched–Absent
•Rectal examination
Others
Systemic examination If deemed necessary.•CNS•Vascular•Gynaecological•muscuoloskeltal
How to initially investigate your patient• Lab:
• CBC (leukocytosis, anaemia, hematocrit, platelets)• Clotting profile• Arterial blood gasses• U& Crt, Na, K, Amylase, LFT and glucose, LDH• Group and save (x-match if needed) • Optional (ESR, CRP, Hepatitis profile
• Radiological:• Plain xrays• USS ( free fluid, masses, mucosal folds, pattern of paristalsis,
Doppler of mesenteric vasulature, solid organs)• Other advanced studies (CT, MRI, Contrast studies……senior
decision)
• ECG and other investigations for co-morbid factors
Diagnosis
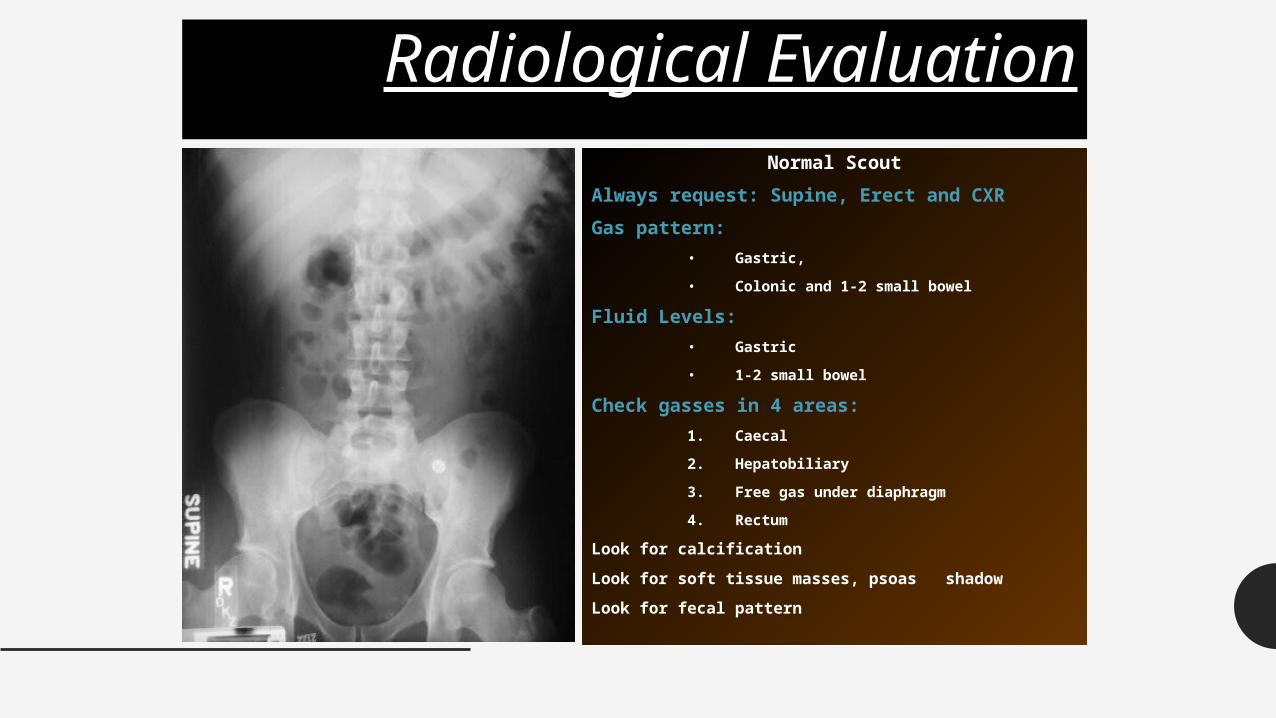
Radiological EvaluationNormal Scout
Always request: Supine, Erect and CXRGas pattern:
• Gastric,
• Colonic and 1-2 small bowel
Fluid Levels:• Gastric
• 1-2 small bowel
Check gasses in 4 areas:1. Caecal
2. Hepatobiliary
3. Free gas under diaphragm
4. Rectum
Look for calcification
Look for soft tissue masses, psoas shadow
Look for fecal pattern
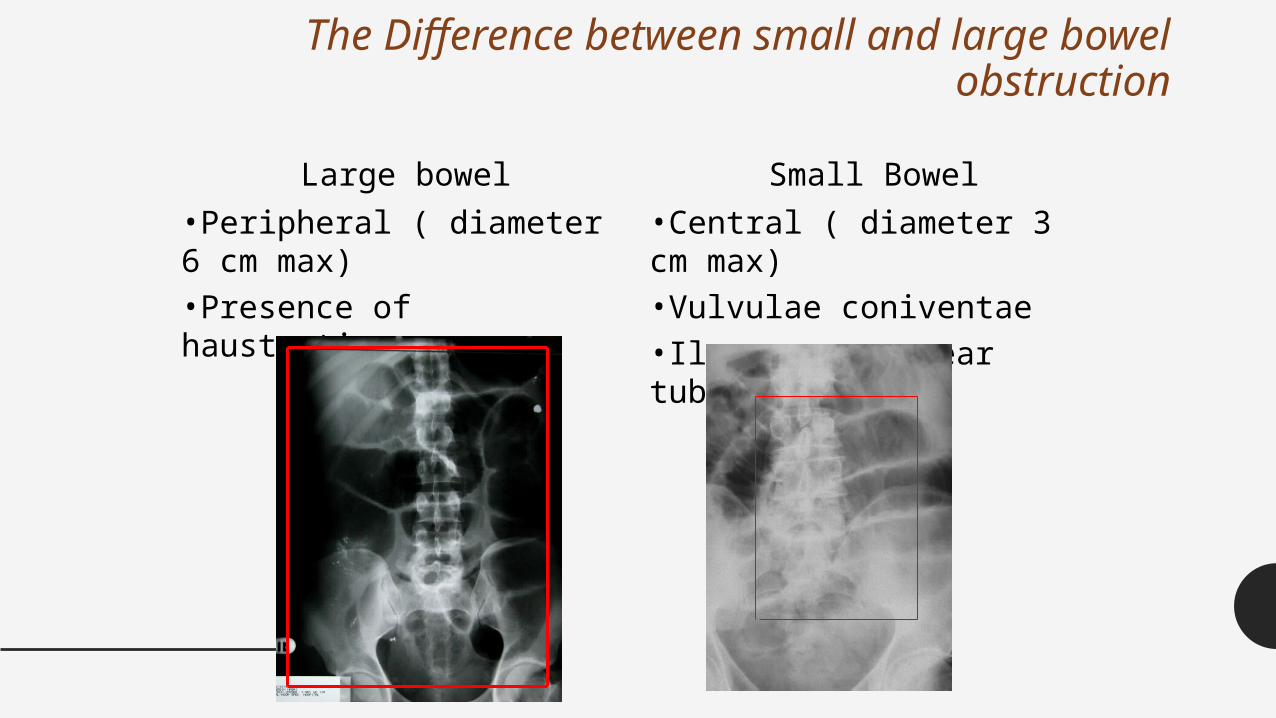
The Difference between small and large bowel obstruction
Large bowel Small Bowel•Peripheral ( diameter 6 cm max)•Presence of haustration
•Central ( diameter 3 cm max)•Vulvulae coniventae•Ileum: may appear tubeless
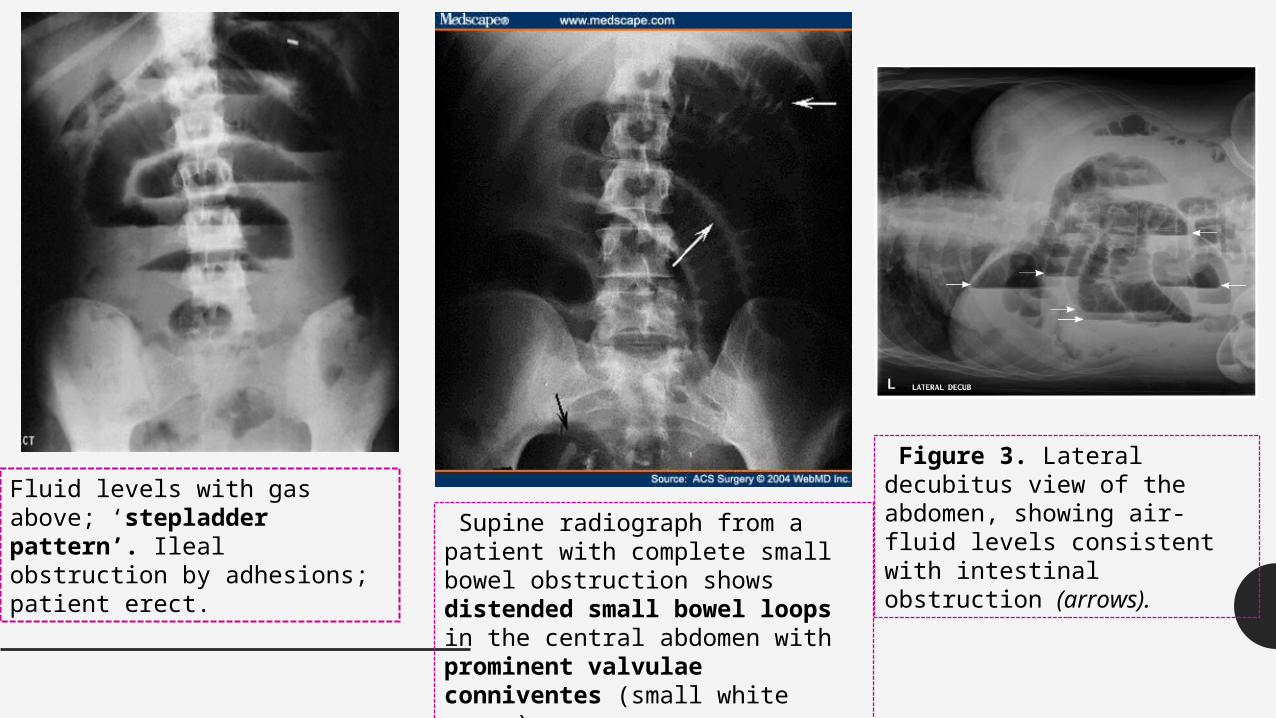
Fluid levels with gas above; ‘stepladder pattern’. Ileal obstruction by adhesions; patient erect.
Supine radiograph from a patient with complete small bowel obstruction shows distended small bowel loops in the central abdomen with prominent valvulae conniventes (small white arrow)
Figure 3. Lateral decubitus view of the abdomen, showing air-fluid levels consistent with intestinal obstruction (arrows).
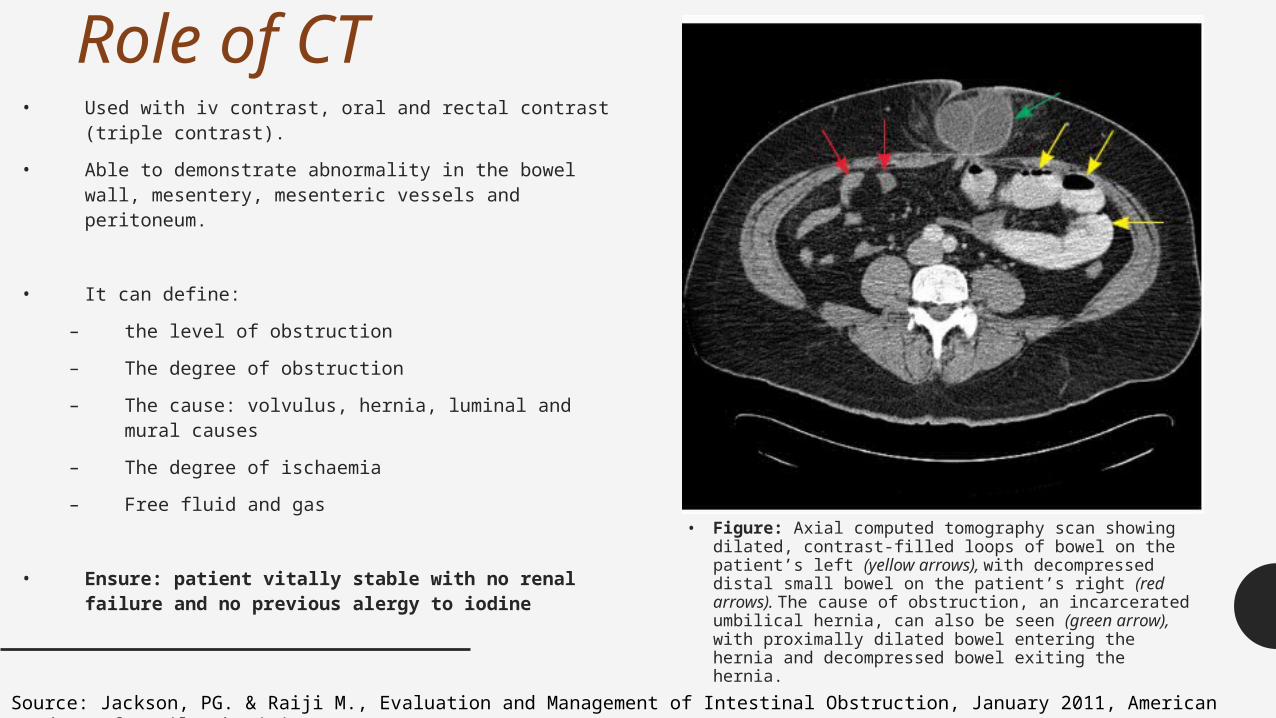
Role of CT• Used with iv contrast, oral and rectal contrast (triple contrast).
• Able to demonstrate abnormality in the bowel wall, mesentery, mesenteric vessels and peritoneum.
• It can define:
– the level of obstruction
– The degree of obstruction
– The cause: volvulus, hernia, luminal and mural causes
– The degree of ischaemia
– Free fluid and gas
• Ensure: patient vitally stable with no renal failure and no previous alergy to iodine • Figure: Axial computed tomography scan showing
dilated, contrast-filled loops of bowel on the patient’s left (yellow arrows), with decompressed distal small bowel on the patient’s right (red arrows). The cause of obstruction, an incarcerated umbilical hernia, can also be seen (green arrow), with proximally dilated bowel entering the hernia and decompressed bowel exiting the hernia.
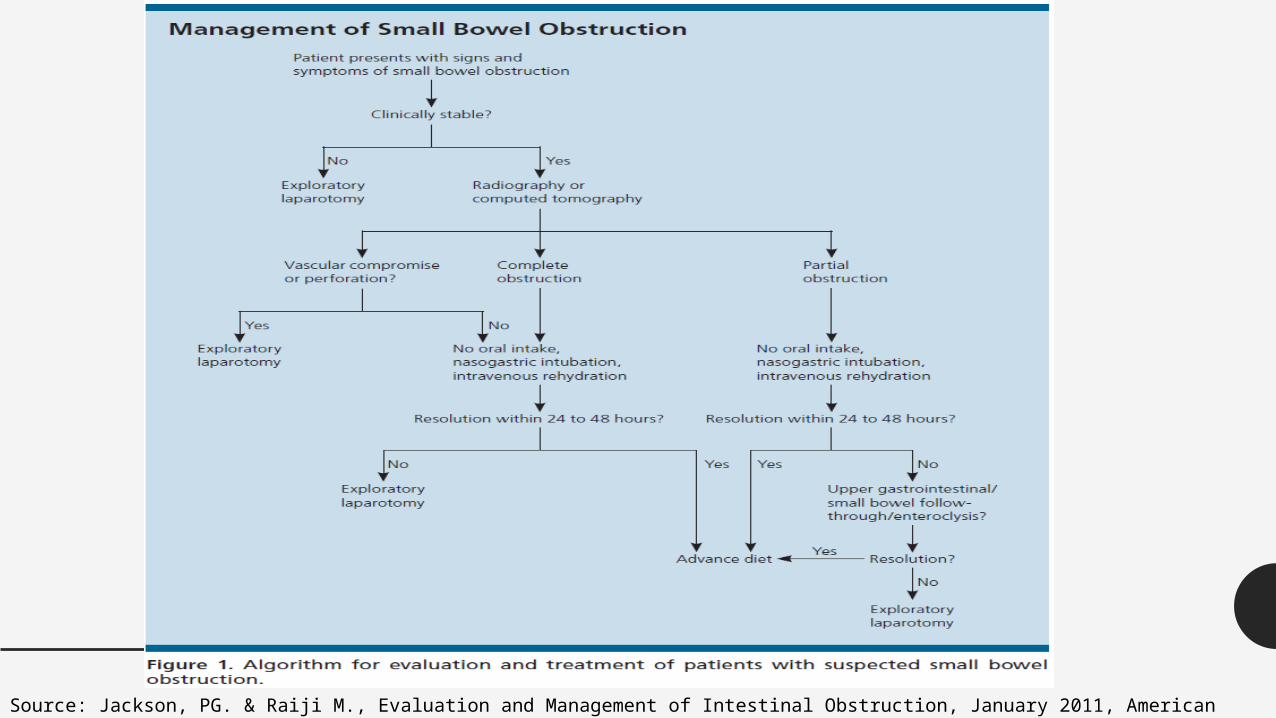
Source: Jackson, PG. & Raiji M., Evaluation and Management of Intestinal Obstruction, January 2011, American Academy of Family Physicians (AAFP), 83: 2 (160-164)
Small Bowel Adhesions• Accounts for 60-70% of All SBO• Results from peritoneal injury, platelet activation and fibrin
formation.• Associated with starch covered gloves, intraperitoneal sepsis,
haemorrhage and wash with irritant solutions iodine and other foreign bodies.
• As early as 4 weeks post laparotomy. The majority of patients present between 1-5 years
• Colorectal Surgery 25%• Gynaecological 20%• Appendectomy 14%
• 70% of patients had a single band• Patients with complex bands are more likely to be readmitted• Readmission in surgically treated patients is 35%
TREATMENT OF ADHESIVE OBSTRUCTION
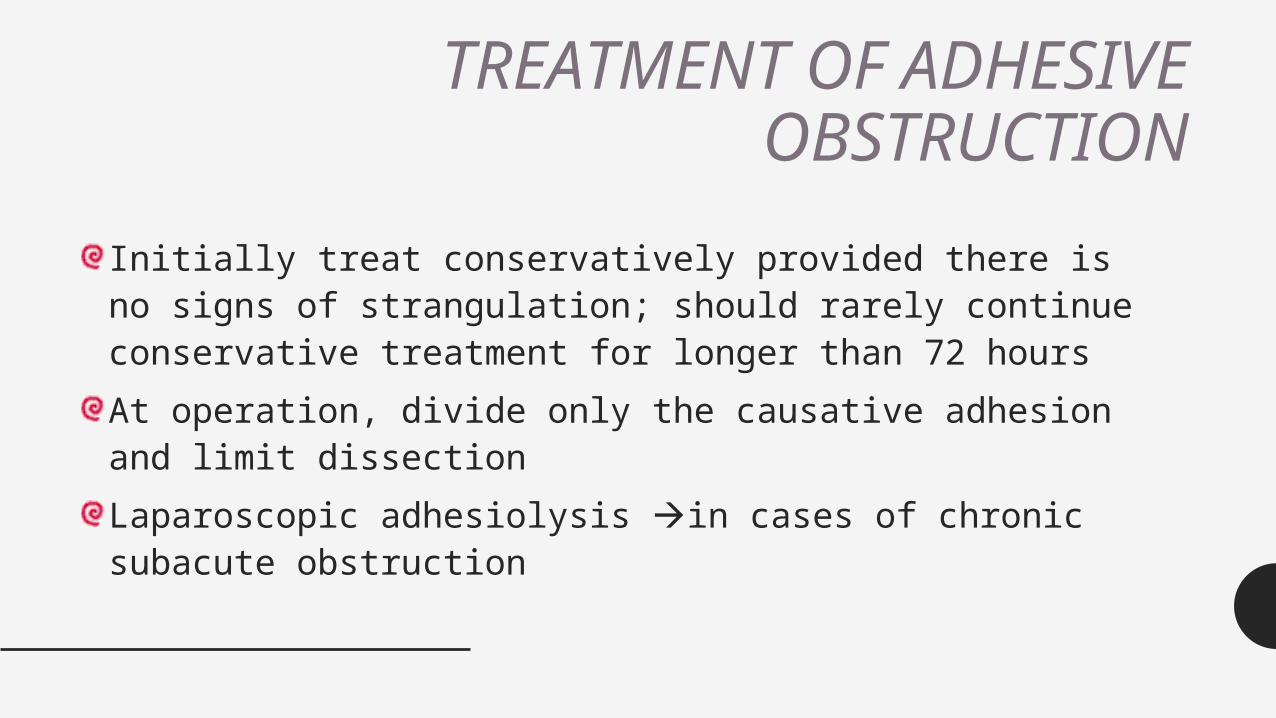
Initially treat conservatively provided there is no signs of strangulation; should rarely continue conservative treatment for longer than 72 hoursAt operation, divide only the causative adhesion and limit dissectionLaparoscopic adhesiolysis in cases of chronic subacute obstruction
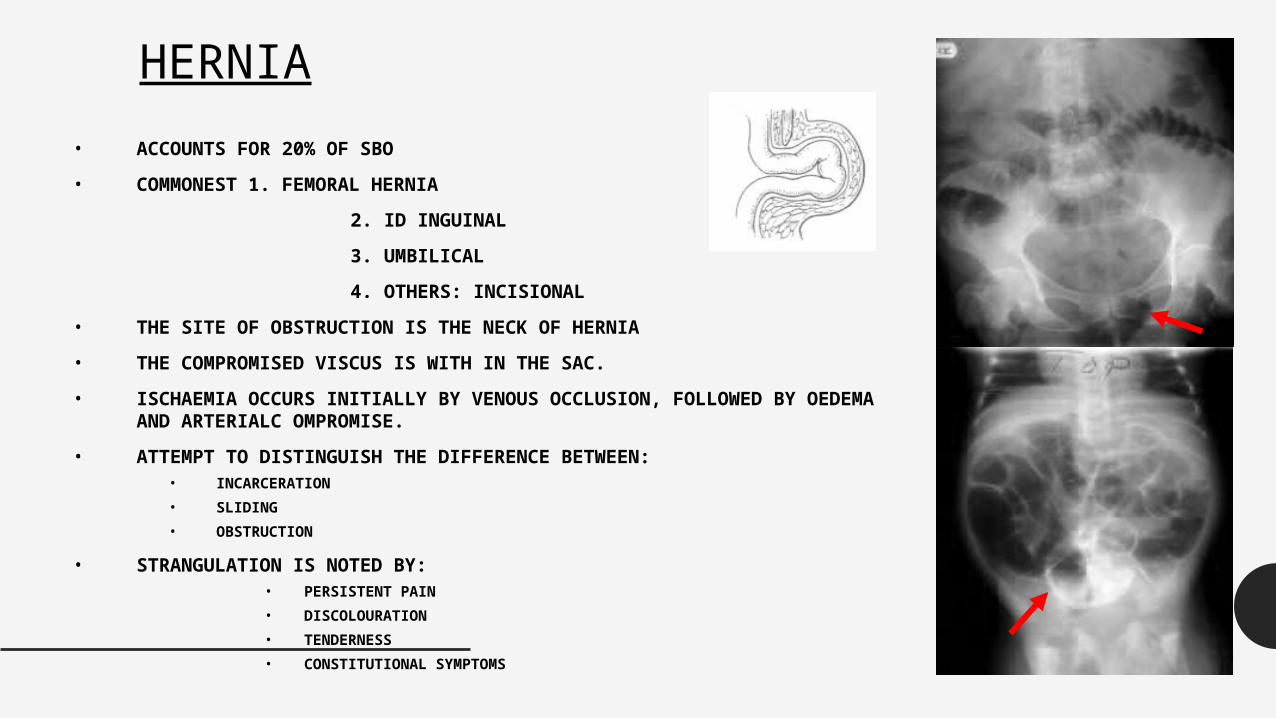
HERNIA• ACCOUNTS FOR 20% OF SBO
• COMMONEST 1. FEMORAL HERNIA
2. ID INGUINAL
3. UMBILICAL
4. OTHERS: INCISIONAL
• THE SITE OF OBSTRUCTION IS THE NECK OF HERNIA
• THE COMPROMISED VISCUS IS WITH IN THE SAC.
• ISCHAEMIA OCCURS INITIALLY BY VENOUS OCCLUSION, FOLLOWED BY OEDEMA AND ARTERIALC OMPROMISE.
• ATTEMPT TO DISTINGUISH THE DIFFERENCE BETWEEN:• INCARCERATION• SLIDING• OBSTRUCTION
• STRANGULATION IS NOTED BY: • PERSISTENT PAIN• DISCOLOURATION• TENDERNESS• CONSTITUTIONAL SYMPTOMS
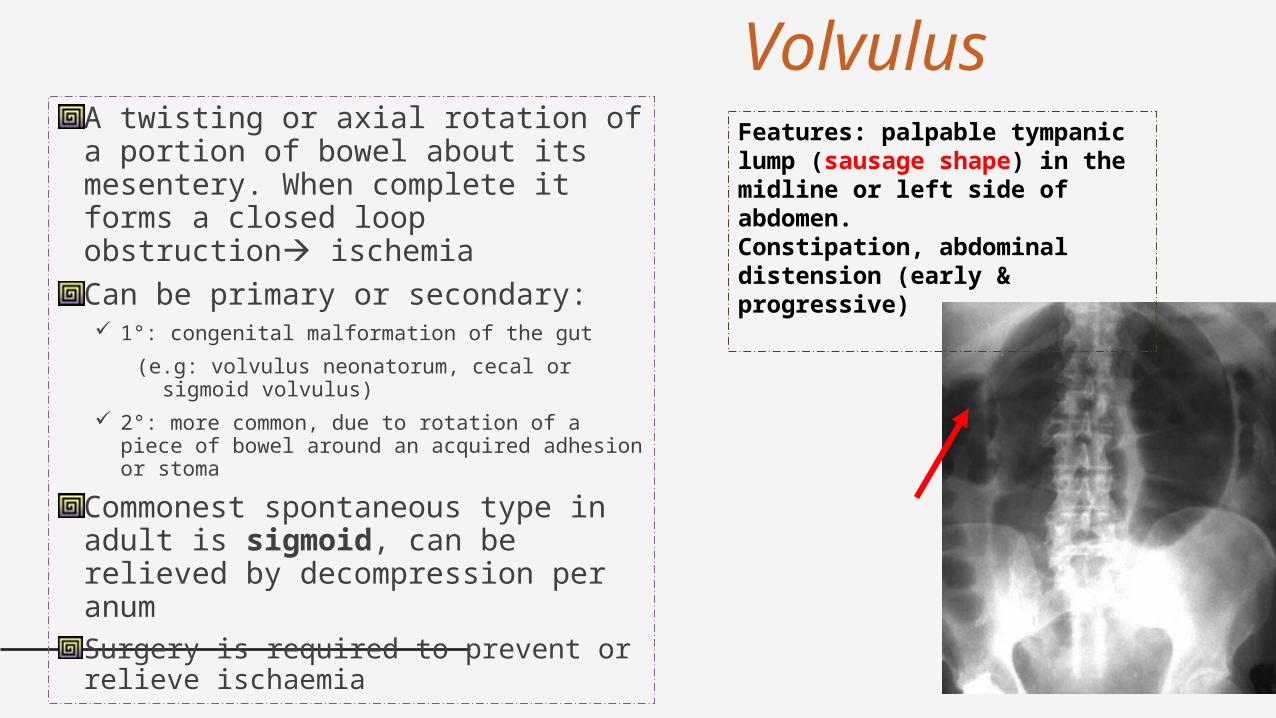
VolvulusA twisting or axial rotation of a portion of bowel about its mesentery. When complete it forms a closed loop obstruction ischemiaCan be primary or secondary: 1°: congenital malformation of the gut
(e.g: volvulus neonatorum, cecal or sigmoid volvulus)
2°: more common, due to rotation of a piece of bowel around an acquired adhesion or stoma
Commonest spontaneous type in adult is sigmoid, can be relieved by decompression per anumSurgery is required to prevent or relieve ischaemia
Features: palpable tympanic lump (sausage shape) in the midline or left side of abdomen. Constipation, abdominal distension (early & progressive)
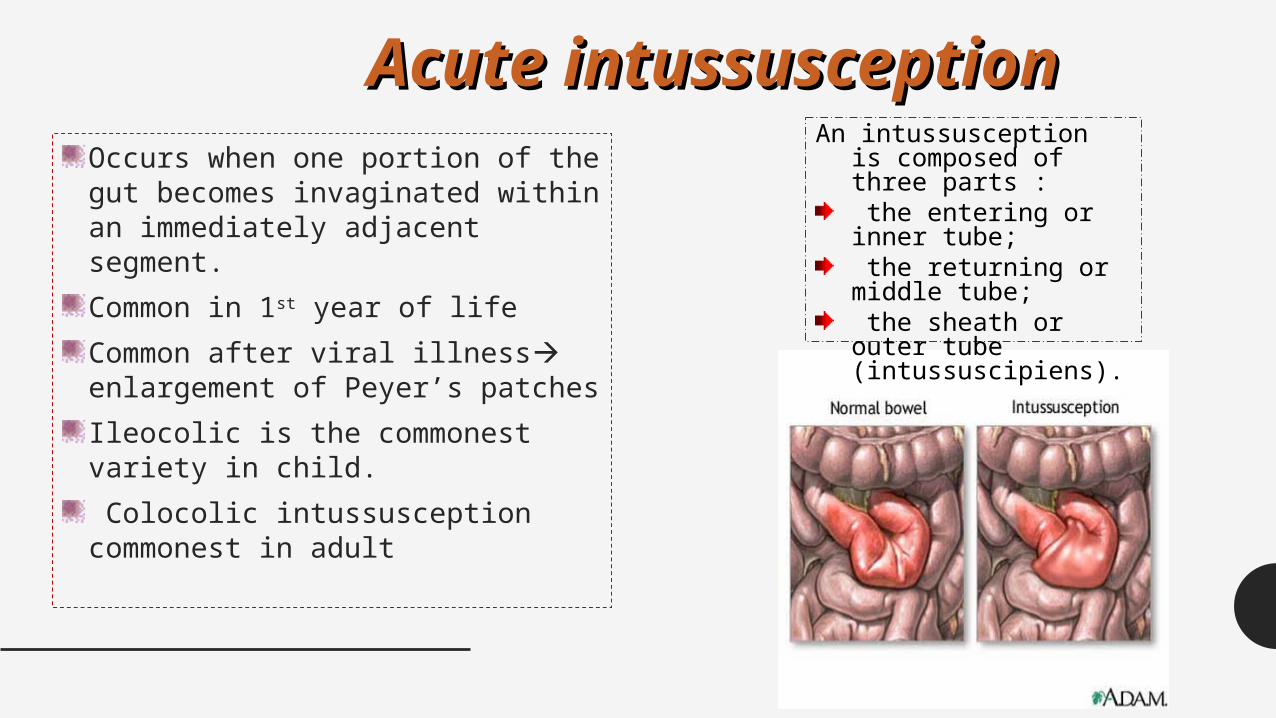
Acute intussusceptionAcute intussusceptionOccurs when one portion of the gut becomes invaginated within an immediately adjacent segment.Common in 1st year of lifeCommon after viral illness enlargement of Peyer’s patchesIleocolic is the commonest variety in child. Colocolic intussusception commonest in adult
An intussusception is composed of three parts : the entering or inner tube; the returning or middle tube; the sheath or outer tube (intussuscipiens).
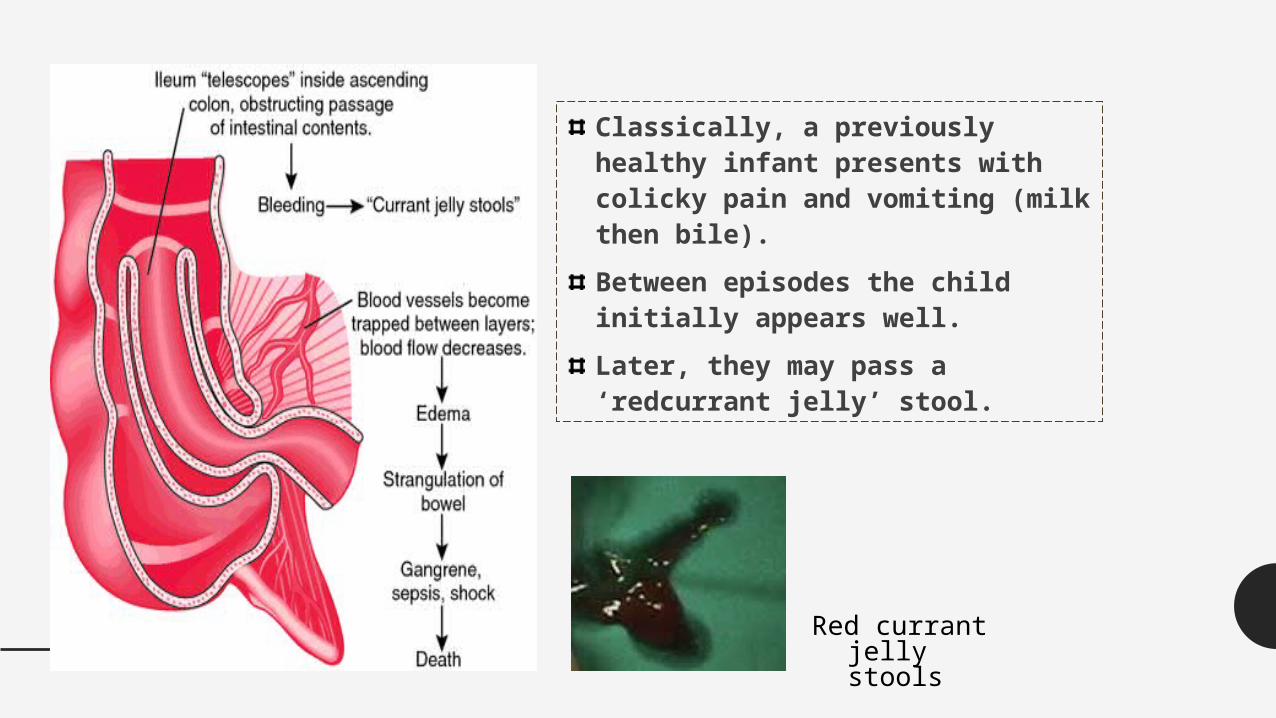
Classically, a previously healthy infant presents with colicky pain and vomiting (milk then bile). Between episodes the child initially appears well. Later, they may pass a ‘redcurrant jelly’ stool.
Red currant jelly stools
Acute Mesenteric Occlusion• Acute ischemic of mesenteric vessel. Commonly SMA
• Causes: AF, mural thrombosis, atheromatous plaque from aortic aneurysm and valave vegetation from endocarditis
• Features: -Sudden onset of severe abd. pain in pt with AF and atherosclerosis-Persistent vomiting and defecation then passage of altered blood-Hypovolumic shock
• Investigations: - Neutrophil leukocytosis - Abd Xray: Absence of gas in thickened small intestines
• Treatment: - Anti-coagulant - Embolectomy - Revascularization - Colectomy
PARALYTIC ILEUSA state in which there is a failure of transmission of peristaltic waves 2° to neuromuscular failure ( in Auerbach’s and Meissner’s plexuses)Stasis leads to accumulation of fluid and gas within bowel a/w distension, vomiting, absence of bowel sound and absolute constipationVarieties factors: postoperative, infection, reflex ileus and metabolicRadiological: gas filled loops of intestines with multiple fluid levels
Ileus• Associated with the following conditions:
• Postoperative and bowel resection• Intraperitoneal infection or inflammation• Ischemia• Extra-abdominal: Chest infection, Myocardia infarction• Endocrine: hypothyroidism, diabetes• Spinal and pelvic fractures• Retro-peritoneal haematoma• Metabolic abnormalities:
• Hypokalaemia• Hyponatremia• Uraemia• Hypomagnesemia
• Bed ridden• Drug induced: morphine, tricyclic antidepressants
Is this an ileus or obstruction
Clinical features• Is there an under lying cause?• Is the abdomen distended but tenderness is not marked.• Is the bowel sounds diffusely hypoactive.
Radiological features:• Is the bowel diffusely distended• Is there gas in the rectum• Are further investigasions (CT or Gastrografin studies) helpful in showing an
obstruction.
Does the patient improve on conservative measures
Management:Essence of treatment prevention with use of nasogastric suction and restriction of oral intake until bowel sound and passage of flatus returnMaintain electrolyte balanceSpecific treatment:
• Removed primary cause• Decompressed GI distension• If prolong paralytic ileus , consider laparotomy exclude hidden cause
and facilitate bowel decompression
Small intestinal pseudo-obstruction
Colonic pseudo-obstruction (Ogilvie’s syndrome, )
This condition may be primary (i.e. idiopathic or associated withfamilial visceral myopathy) or secondary. The clinical picture consists of recurrent subacute obstruction. The diagnosis is made by the exclusion of a mechanical cause.Treatment consists ofinitial correction of any underlying disorder. Metoclopramide anderythromycin may be of use.
This may occur in an acute or a chronic form.
presents as acute large bowelobstruction.
Abdominal radiographs show evidence of colonic obstruction, with marked caecal distension being a commonfeature.
AXR shows colonic obstruction with marked caecal distension
Confirmation of absence mechanical cause by colonoscopy or single contrast water soluble barium enema or CT.
Once confirmed, treated by colonoscopic decompression
Initial Management in the ER• Resuscitate:
• Air way (O2 60-100%)
• Insert 2 lines if necessary
• IVF : Crytloids at least 120 ml/h. (determined by estimated fluid loss and cardiac function). Add K+ at 1mmmol/kg
• Draw blood for lab investigations
• Inform a senior member in the team.• NPO.• Decompress with Naso-gastric tube and secure in position
• Insert a urinary catheter (hourly urinary measurements) and start a fluid input / output chart
• Intravenous antibiotics (no clear evidence)• If concerns exist about fluid overloading a central line should be inserted
• Follow-up lab results and correction of electrolyte imbalance
• The patient should be nursed in intermediate care
• Rectal tubes should only be used in Sigmoid volvulus.
Source: Jackson, PG. & Raiji M., Evaluation and Management of Intestinal Obstruction, January 2011, American Academy of Family Physicians (AAFP), 83: 2 (160-164)
INDICATIONS FOR SURGERY• Absolute
– Generalised peritonitis– Localised peritonitis– Visceral perforation– Irreducible hernia
• Relative– Palpable mass lesion– 'Virgin' abdomen– Failure to improve
• Trial of conservatism– Incomplete obstruction– Previous surgery– Advanced malignancy– Diagnostic doubt - possible ileus
Source: http: Surgical Tutor.co.uk
Indications for SurgeryImmediate intervention:• Evidence of strangulation (hernia….etc)• Signs of peritonitis resulting from perforation or ischemia
In the next 24-48 hours• Clear indication of no resolution of obstruction ( Clinical,
radiological).• Diagnosis is unclear in a virgin abdomen
Intermediate stageThe cause has been diagnosed and the patient is stabalised
THANKSQuestions???????????????????????????????????????????????????
?????????????