Embed Size (px)
Citation preview



Dr. Mohammad Amiri , ODDepartment of Optometry ,Faculty of RehabilitationShahid Beheshti Medical Sceince UniversityVision Care of MeniconKeratoconusAnd specialty contact lens fitting of irregular corneas

Keratoconus• Is a progressive disorder in which the cornea has irregular
shape• Onset: around puberty • Autosomal dominant• Usually bilateral; but assymetrical• Systemic association: e.g. Down syndrome; Turner syndrome;
Marfan syndrome• Ocular association: e.g. retinitis pigmentosa; vernal
keratoconjunctivitis;

• According to morphology can be classified into • Nipple cones: small size 5mm; steep
curvature; the apex of the cone is central or infero-nasally

• Oval cones: 5-6mm size; ellipsoid (oval) & displaced inferotemporally

• Globus cones: the largest >6mm

• Presentation: visual impairment due to progressive myopia & astigmatism (usually reported for one eye); changes in spectacle Rx; decrease tolerance to contact lens wear;
• Signs: central or paracentral stromal thinning; apical protrusion; irregular astigmatism; steepening of the cornea graded according to keratometry readings (mild <48D, moderate 48-54D, severe >54D)
Early in the disease: oil droplet reflex on ophthalmoscopy; irregular scissor reflex on retinoscopy; Vogt lines (i.e. deep vertical stromal striae) on slit-lamp exam; irregular astigmatism on keratometry; abnormal corneal topography

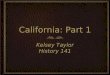
Vogt striae (i.e. line) in keratoconus

Late in the disease: Munson sign (i.e. bulging of the lower lid on downgaze); visual acuity worsens; watering; oedema; stromal scarring after beaks healing;
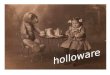
Munson sign in keratoconus

Keratoconus
• What have the years taught us?

Keratoconus Characteristics
Non-inflammatory. Central or para-central corneal thinning. Corneal steepening or protrusion. Increased astigmatism and possibly myopia. Loss of best spectacle corrected visual acuity. Corneal striae and scarring. Corneal hydrops (inflammatory).

Keratoconus
• Non-Inflammatory Ectasia• Stromal Thinning• Disruption of Bowman’s
Membrane
• Corneal Ectasia• Myopia• Irregular Astigmatism
• Optical Correction• Spectacles– early• Contact Lenses– later

Keratoconus
• Demographics• Estimates vary from 50 to
170 per 100,000
• Obscure Etiology• Heredity• Allergies, Eye Rubbing

Why Does the Cornea Bulge in Keratoconus?
• Corneal tissue is abnormal• Too elastic?• Abnormal cross-linking
of collagen?
• Loss of structural integrity of Bowman’s Layer?
• Keratocyte apoptosis• Trauma (eye rubbing)
• Corneal tissue bulges because it is too thin?

Pathology of Keratoconus
Loss of Bowman’s Layer.
Stromal Thinning.
Apoptosis.
Increased Enzyme Activity.
Enlarged Prominent Corneal Nerves.

Causes of Keratoconus
• Heredity vs. Mechanical
• Cellular
• Tissue
• Genetic

Cellular Changes
• Keratoconus cells are hypersensative.• Increased enzyme activity, lack of enzyme
inhibitors.• Matrix substrate instability in response to
environmental stress factors.• mtDNA damage and exaggerated oxidative
response causing cellular damage.

Tissue Changes
Loss of Bowman’s layer.
Lamellar slippage.
Lack “anchoring” lamellar fibrils.
Apoptosis of the stroma causing anterior thinning.

Heredity vs. Mechanical
• Does eye rubbing cause Keratoconus?• 2 out of 250 doctors feel that rubbing is a
cause.• KC patients do rub their eyes more often than
those without KC.• What is it that makes KC patients rub their
eyes?

Genetics
• Autosomal dominant w/variable penetrance.• SOD1, an antioxidant enzyme, is abnormal in
some KC corneas.• No single gene responsible.• 10 different chromosomes have been
associated with KC.• Most likely multiple genes involved.

Additional Information
Male to Female Ratio = 3:1 Approximately 20% result in PKP. 90% are diagnosed by optometrists. Mean age of diagnosis is 22.88 years. Visual outcome with RGP is better than PKP. More prevalent in certain ethnic groups (4x
higher in Asians from Indian sub-continent regions than White Europeans).

Progression and Prognosis
Age is a big factor. The younger the diagnosis, the poorer the
prognosis. Less likely to progress to the point of a
transplant if diagnosed in the 30’s. 20% of Keratoconus patients result in corneal
transplants. 35 to 45% of all transplants are due to
Keratoconus.

Possible Aggravating Factors
• UV exposure.
• Allergies.
• Vigorous eye rubbing.
• Poorly fitting contact lenses.
• Inflammation.

Types of Keratoconus
• Nipple/Oval cone - central or mildly para-central localized thinning and steepening.
• Keratoglobus - Large generalized thinning and steepening.
• PMD (pellucid marginal degeneration) – peripheral thinning and steepening.
• Keratoconus Fruste – Less progressive and less manipulative.

Nipple/Oval Cone
• Central Steepening• Steepest form

Keratoglobus
• Wider – 75 to 90% of cornea.• Not as steep.

Pellucid Marginal Degeneration
• Peripheral Thinning

Orbscan Analysis




How to Treat Keratoconus Spectacles Contacts
Soft StandardSoft CustomRGP StandardRGP CustomHybrid
SurgeryIntacsPenetrating Keratoplasty
Riboflavin/UV treatment

When to Intervene?
• Best Spectacle/Soft CL Acuity 20/30 or better?– Good tolerance of acuity.– Corneal health is not compromised.– “If it aint broke, don’t fix it.”
• Best Spectacle/Soft CL Acuity worse than 20/30?– Specialized contact lenses.– My opinion, use RGP lenses.

Which RGP Design?
• Early Keratoconus– Standard RGP– KC RGP
• Mid-stage Keratoconus– KC RGP– Custom KC RGP
• Advanced Keratoconus– Custom KC RGP– Intra-limbal or Scleral RGP

My “GO TO” Lens – Rose K
• Developed by Dr. Paul Rose.• Designed to fit the irregular cornea.• “Very forgiving lens”• Multiple designs to fit all shapes of corneas
and corneal conditions.• Blanchard is very good to work with and has
staff to assist with very difficult cases.

Nipple/Oval Cone Fitting
• Most common form of KC.• Early stages - simple RGP or KC RGP• Later stages – KC RGP usually small and steep.• The steeper the cone, the smaller the lens
diameter.

Rose K2
• Rose K vs. Rose K2• 72% of patients notice an increase in acuity
with aspheric, aberration control.• Lens to be centered on the cone.• Reduce excessive movement (1 to 2mm).

Fitting the Rose K2
• Too high – tighten edge liftreduce OADsteepen base curve
• Too low – increase edge liftincrease OADflatten base curve

Fitting the Rose K2
• Centrally fitting thelens on a nipplecone better insuresoptimal acuity and comfort.

Rose K2IC
• IC stands for irregular cornea• Larger diameter• Larger optic zone• Aspheric for aberration control• Reverse geometry design

• PMD
• Keratoglobus
• LASIK induced ectasia
• Corneal transplants

Corneal Dystrophies
Traumatic Corneas with Scars
Post RK
Irregular Astigmatism or Corneal Warpage

What is That?


Asymmetric Corneal Technology
• ACT.

ACT – Continued…

Using ACT ( Asymmetric Corneal Technology)
• 3 standard grades available • Option also to specify degree of tuck in 0.1 steps from 0.4 to 1.5mm
Grade 1 ( 0.7mm steeper)
Grade 2 (1.0mm steeper)
Grade 3 (1.3mm steeper)
Fitting with ACT

NO ACT WITH ACT
ACT - Improved comfort , lens stability and vision
Fitting with ACT

Toric Peripheral Curves

Fitting Pearls
Tendency to tighten after initial fitting. Light central touch will increase acuity. Avoid central staining. Movement is necessary but slight movement is
usually sufficient. Pay attention to tear flow beneath lens. The steeper the lens, the smaller OAD and less
movement. Don’t change too many parameters at once.

Penetrating KeratoplastyWhen to refer?
Acuity is 20/50 or worse. Patient intolerance to visual decrease. Scars within the visual axis. Multiple episodes of Hydrops. Contact lens intolerance. Unable to get adequate/healthy CL fit. Consider OD to OD referral. Give reasonable expectations.

Post PKP Management
• How soon can you fit with lens? • Why are the curvatures so strange?• Do you have to wait for all sutures to be
removed?• Corrective options.– Spectacles– RGP contact lenses.– LASIK

Rose K2 Post Graft

PKP Topography

Rose K2 Post Graft
Much more difficult to fit than KC.
Patients are less tolerable to CL.
Eyes are more dry.
Ill-fitting contact lenses can lead to graft
rejection.
Lens design is crucial to success.

K2PG Fitting Pearls
• Don’t be intimidated!• Watch tear flow!• Also good lens for ectasia patients.• Stay with your fitting basics– Fit base curves.– Adjust diameter.– Adjust peripheral curves.– Use ACT or Toric PC if needed.

Post Graft – Too Steep

Post Graft – Too Flat

Post Graft – Good Fit

Watch Vasculature

The Difficult Ones
• Nothing is comfortable.
• Acuity isn’t improving..
• Eyes are too dry. (Sjogren’s Syndrome)
• Cornea is too irregular for any lens to fit
properly or in a healthy manner.

What Do You Do?