Embed Size (px)
Citation preview
Dr Vikash(Junior Resident 2nd year)
Moderator-Dr. Amrita Ghosh
Kar(Associate Prof)
Depatment of Pathology,IMS BHU
Recent advances In Colorectal
Carcinoma
Introduction
Epidemiology
Etiology
Molecular Pathogenesis
Clinical features
Diagnostic Modalities
Staging and Grading
Spread and Metastasis
Treatment
Prognosis
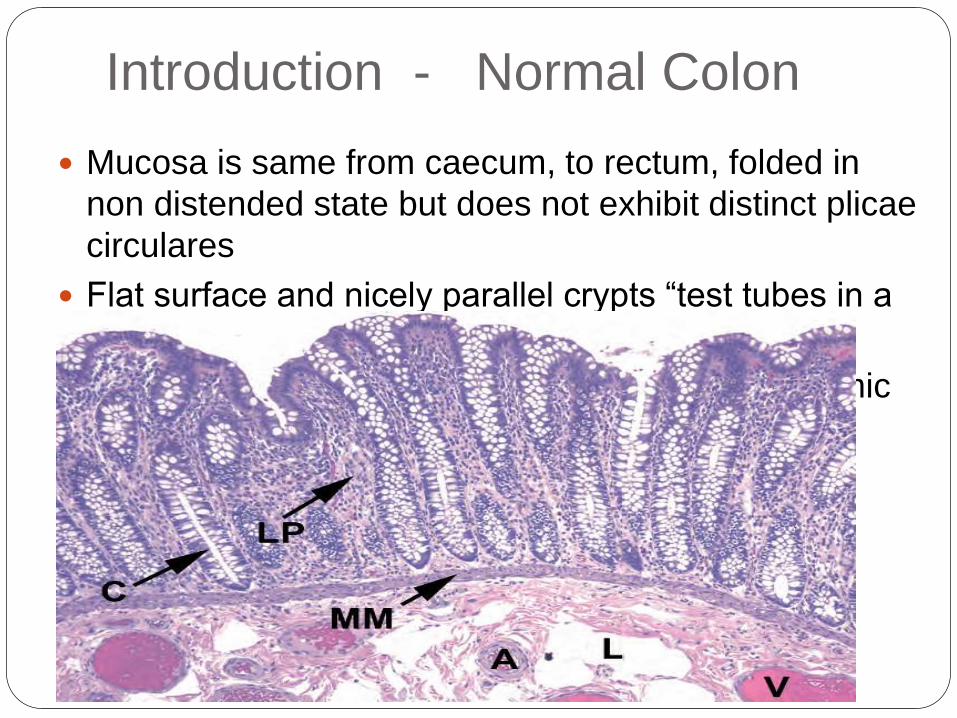
Introduction - Normal Colon
Mucosa is same from caecum, to rectum, folded in
non distended state but does not exhibit distinct plicae
circulares
Flat surface and nicely parallel crypts “test tubes in a
rack.”
Muscularis mucoa is prominent feature –for rhythmic
contactions
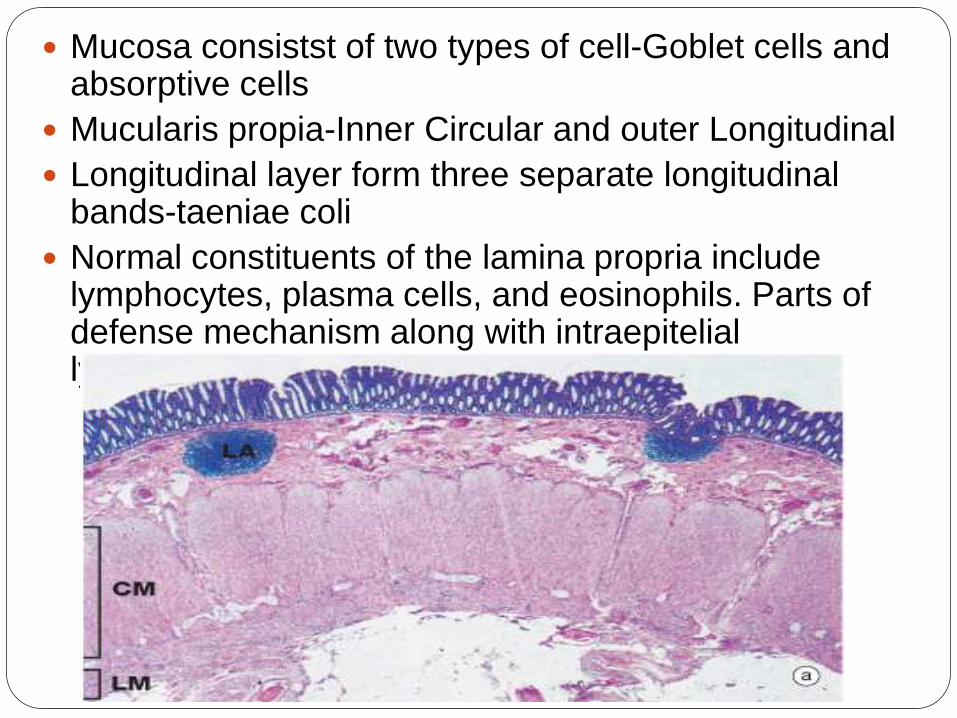
Mucosa consistst of two types of cell-Goblet cells and absorptive cells
Mucularis propia-Inner Circular and outer Longitudinal
Longitudinal layer form three separate longitudinal bands-taeniae coli
Normal constituents of the lamina propria include lymphocytes, plasma cells, and eosinophils. Parts of defense mechanism along with intraepiteliallymphocytes and lymphoid aggregates
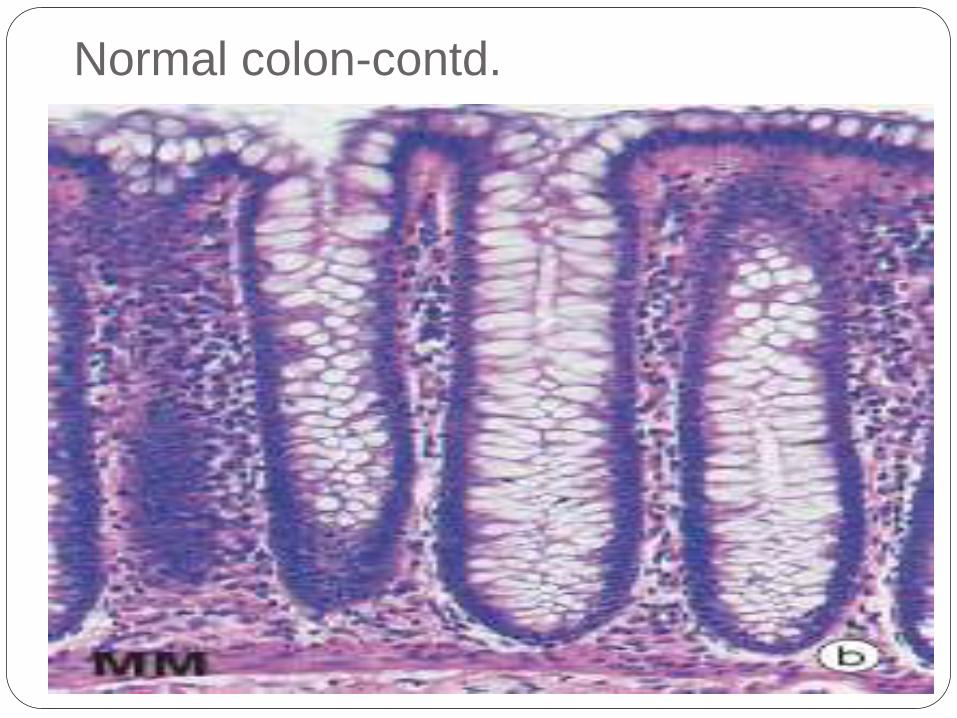
Normal colon-contd.
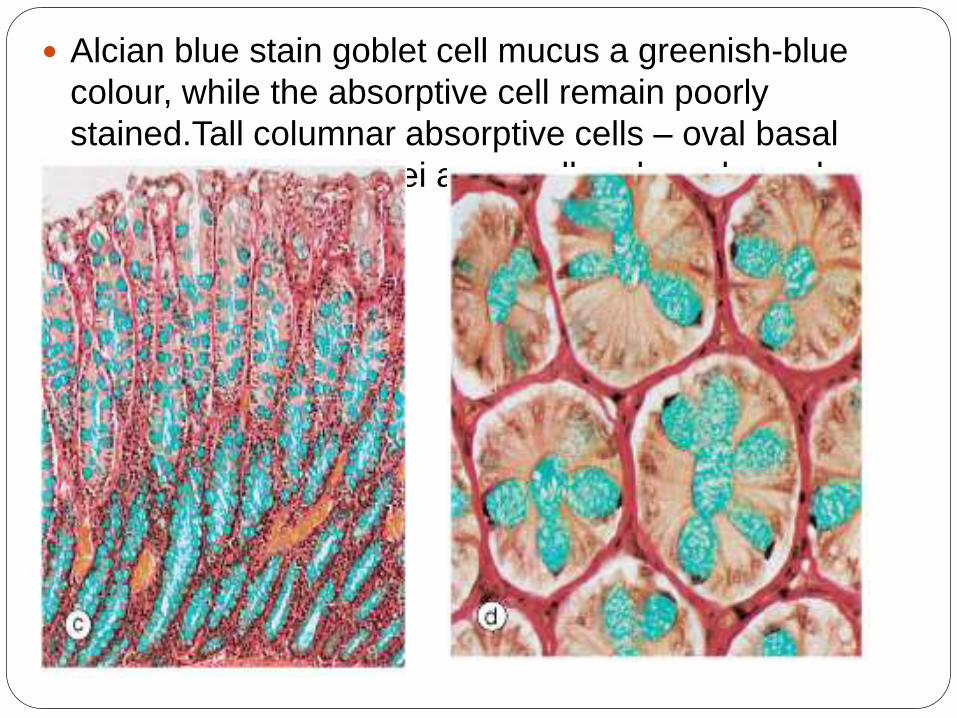
Alcian blue stain goblet cell mucus a greenish-blue
colour, while the absorptive cell remain poorly
stained.Tall columnar absorptive cells – oval basal
nuclei, Goblet cell nulei are small and condensed.
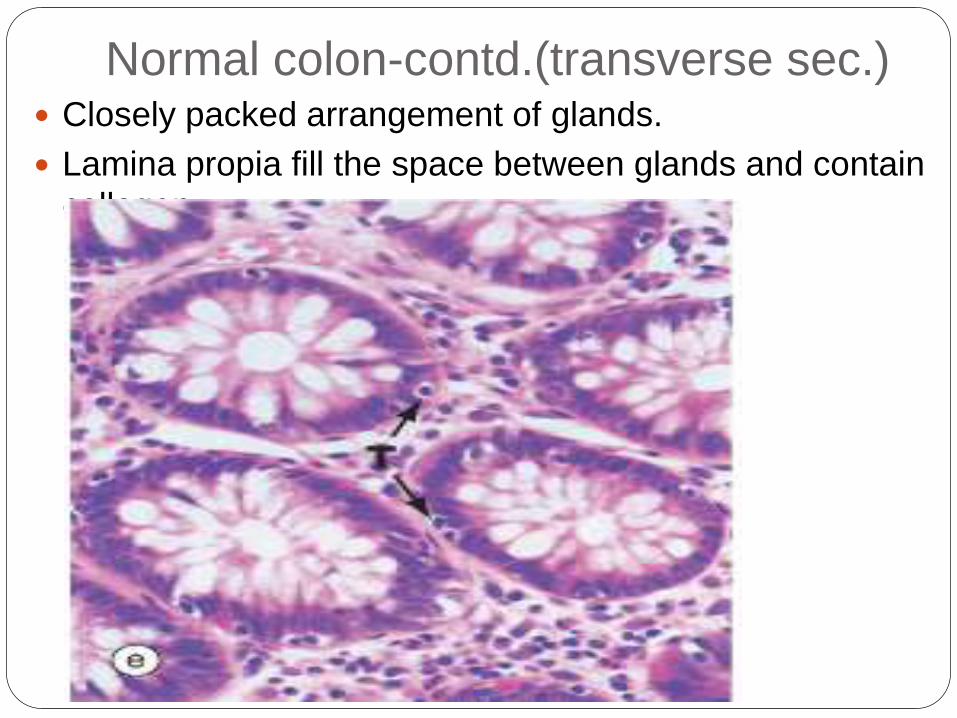
Normal colon-contd.(transverse sec.) Closely packed arrangement of glands.
Lamina propia fill the space between glands and contain
collagen
Epidemiology Third most common cancer in USA after prostate
and lung.
Most curable form of carcinoma of the g.i.t tract.
Non cancerous polyp that can be overtime
become cancerous lesion.
98% of all cancers in large intestine almost
always arise in adenomatous polyp,generally
curable by resection.
Males and females are equally affected.
Mean age -62 year
Although right sided colonic cancer has been
increasing,Rectum is commonest site.
Asian Pacific journal of Cancer prevention ;
vol13,2012
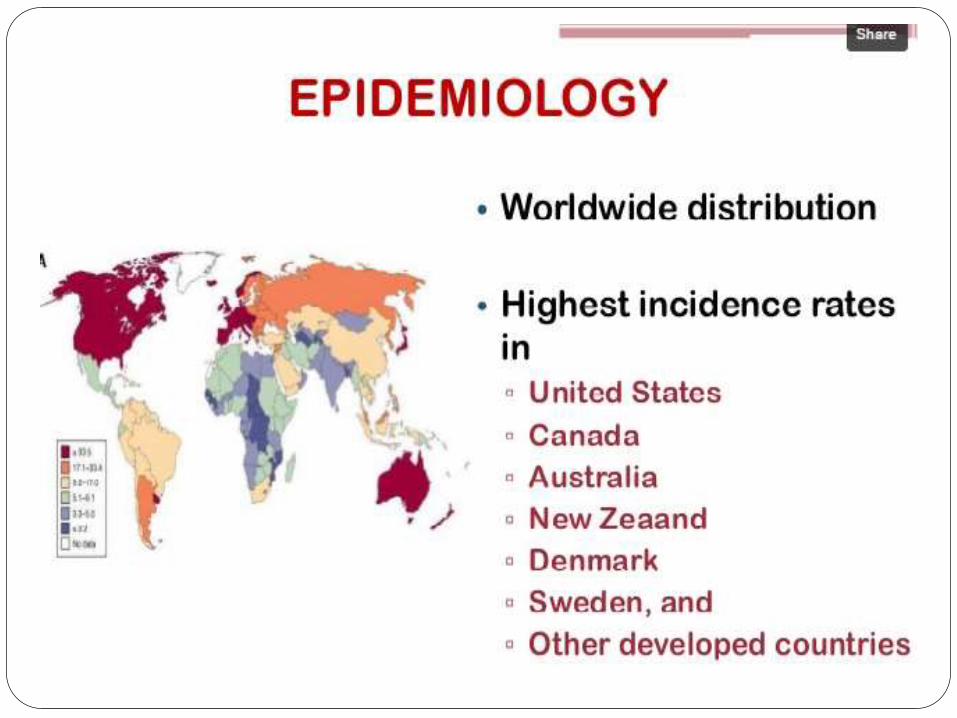
Risk factors Age(Most common)
Dietary factor
High animal fat diet
Low fibre diet
Alcohol
• Inflammatory Bowel disease (UC,
Crohn’s)
• Smoking
• Pelvic irradiation
• Acromegaly
• UreteroSigmoidostomy
• Streptococcus Bovis Bacteremia
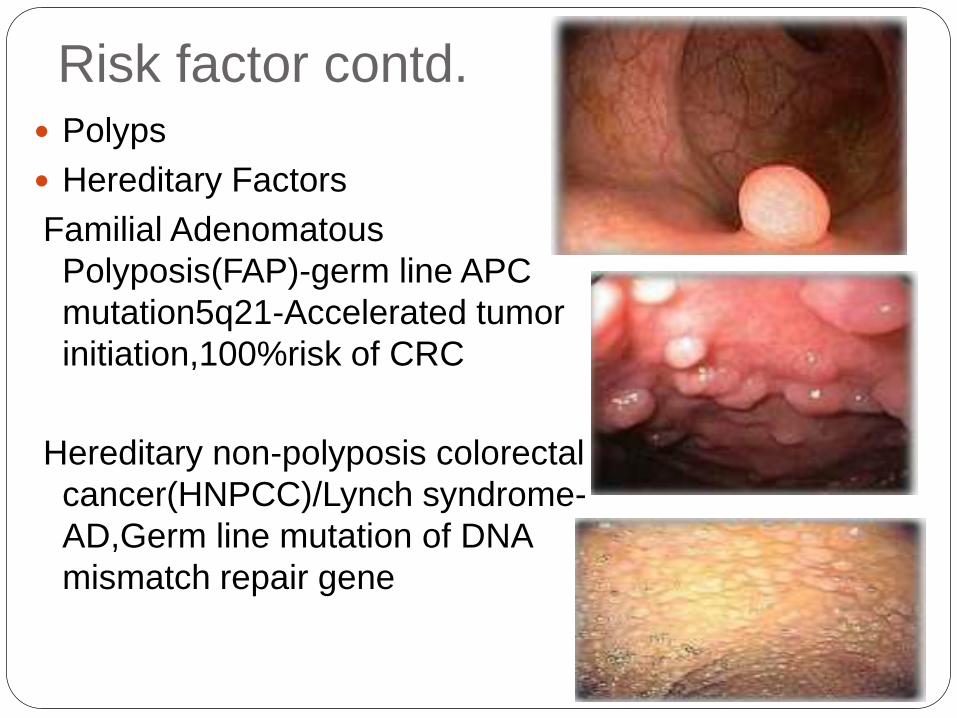
Risk factor contd. Polyps
Hereditary Factors
Familial Adenomatous
Polyposis(FAP)-germ line APC
mutation5q21-Accelerated tumor
initiation,100%risk of CRC
Hereditary non-polyposis colorectal
cancer(HNPCC)/Lynch syndrome-
AD,Germ line mutation of DNA
mismatch repair gene
Risk factor-Adenoma( Neoplastic
lesion)
Clonal lesions that shows at least low grade
dysplasia.
Cells lining the crypts and the surface-Tall and
dark (because of depleted mucin)
Nuclei- cigar-shaped and/or pseudostratified
Hyperchromatic nuclei. Overall look blue on
slide
If it will remain untreated-Adenoma ca seq-
Invasive Adenocarcinoma
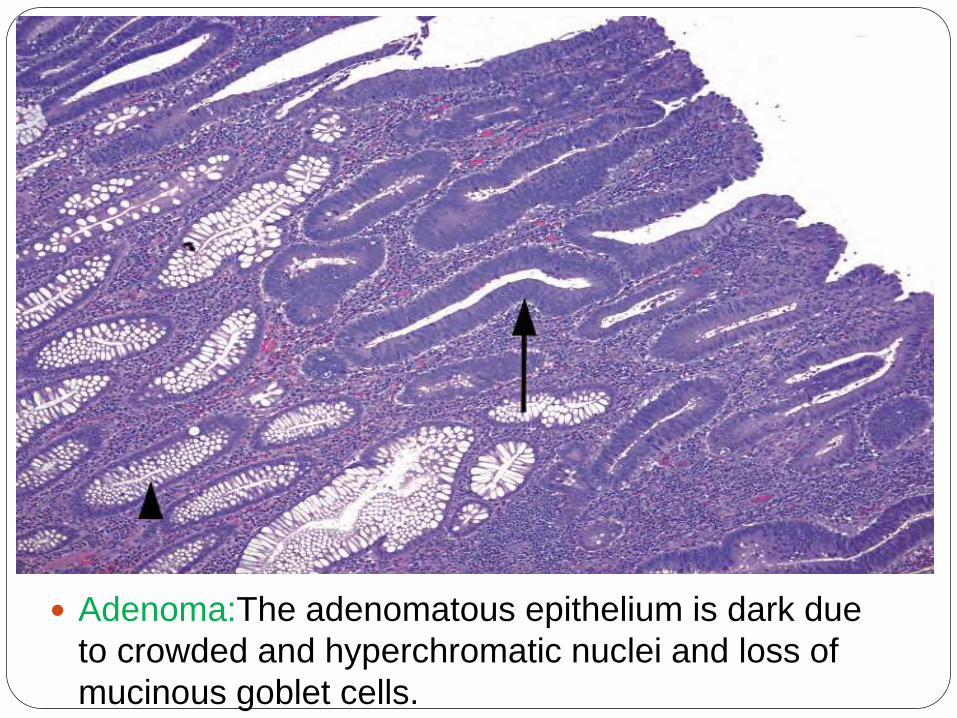
Adenoma:The adenomatous epithelium is dark due
to crowded and hyperchromatic nuclei and loss of
mucinous goblet cells.
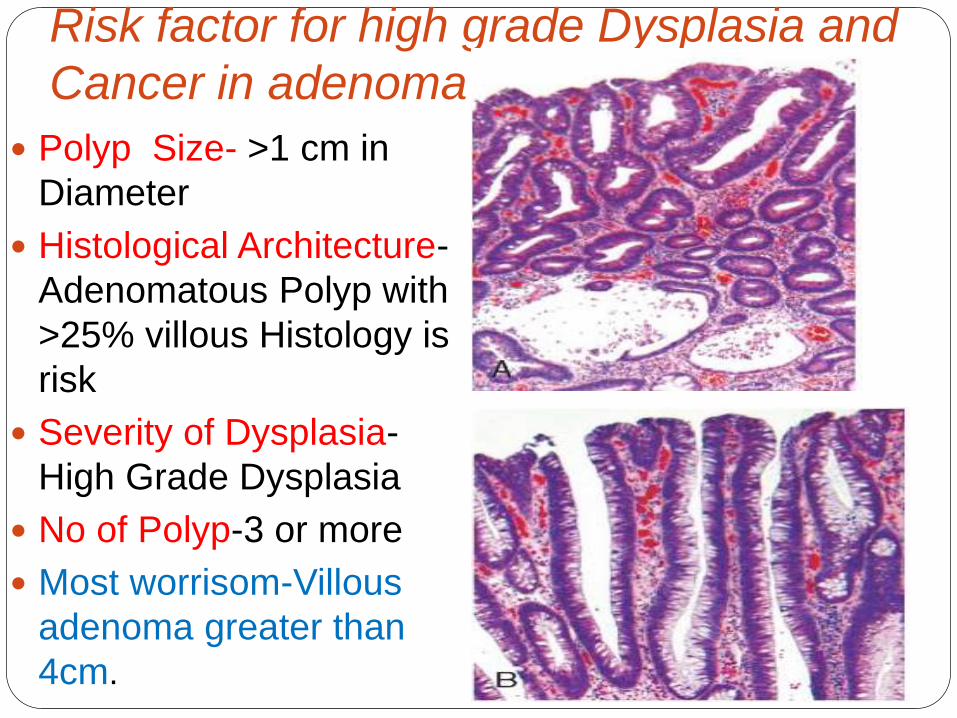
Risk factor for high grade Dysplasia and
Cancer in adenoma
Polyp Size- >1 cm in
Diameter
Histological Architecture-
Adenomatous Polyp with
>25% villous Histology is
risk
Severity of Dysplasia-
High Grade Dysplasia
No of Polyp-3 or more
Most worrisom-Villous
adenoma greater than
4cm.
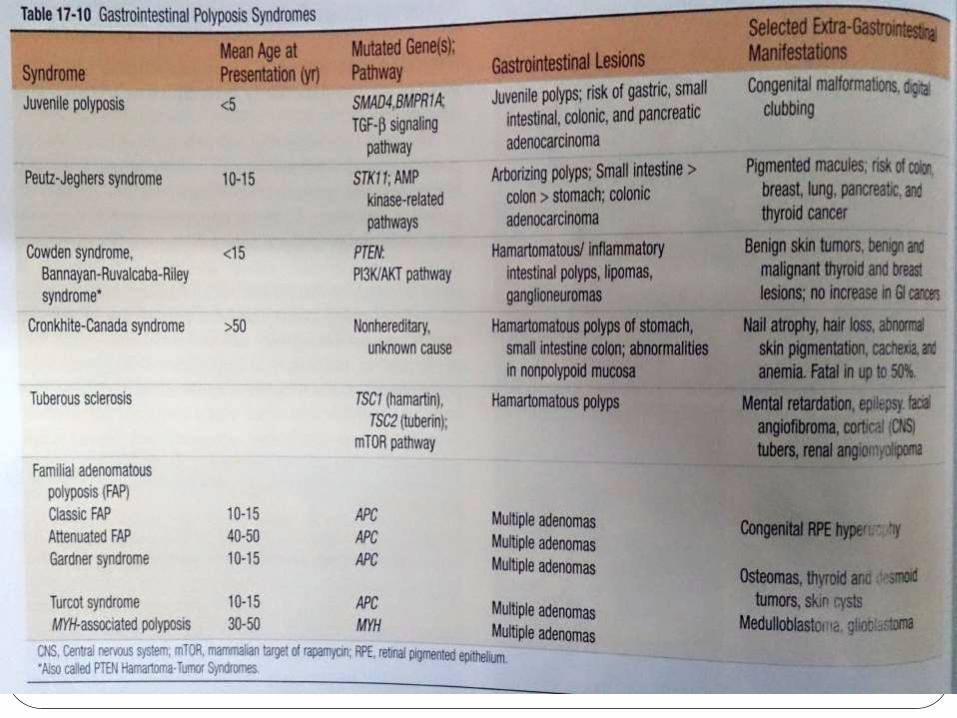
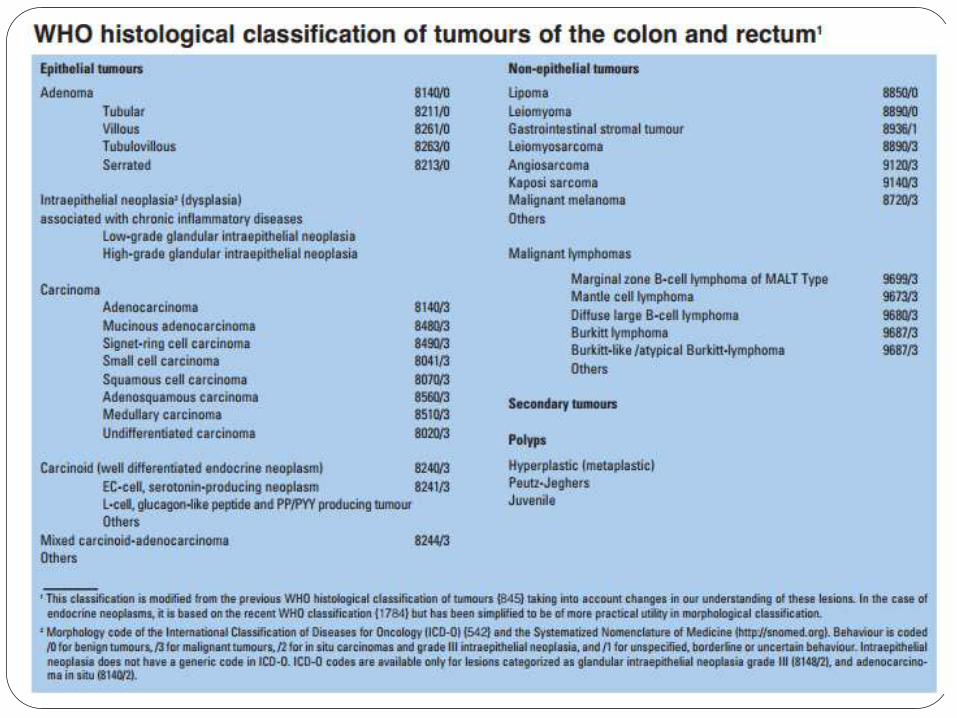
Classification of Tumors of colon Non neoplastic (Benign) Polyps
Hyperplastic polyps
Hamartomatous polyps
-Juvenile polyps
-Peutz-Jeghers polyps
Inflammatory polyps
Lymphoid polyps
Neoplastic epithelial Lesions
- Adenomas
Malignant
-Adenocarcinoma
-Carcinoid tumor
-Anal zone Carcinoma
-Lymphoma
Mesnchymal tumors
GIST
Other benign lesions-Lipoma, Neuroma ,Angioma
Basic Overview of Classification Polyp- Tumerous mass, Protude in lumen,Sessile or
Pedunculated
Non-Neoplastic polyps----No malignant potential per
se
Abnormal Mucosal maturation and decrease
turn over-Hyperplastic polyp
Due to inflammation regenerating mucosa-
Inflammatory polyp/Pseudopolyp
Malformation of gland and Stroma-
Harmatomatous Polyp
Adenomatous Polyp/Adenoma- Neoplastic, Due to
proliferation and Dysplasia
Precursors of carcinoma
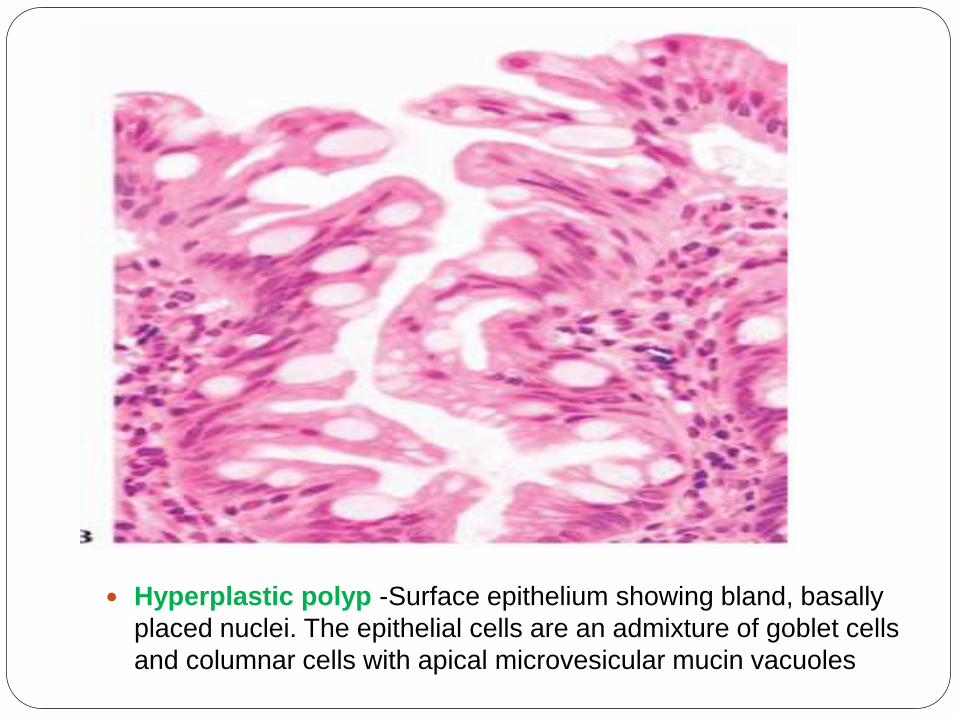
Hyperplastic polyp -Surface epithelium showing bland, basally
placed nuclei. The epithelial cells are an admixture of goblet cells
and columnar cells with apical microvesicular mucin vacuoles
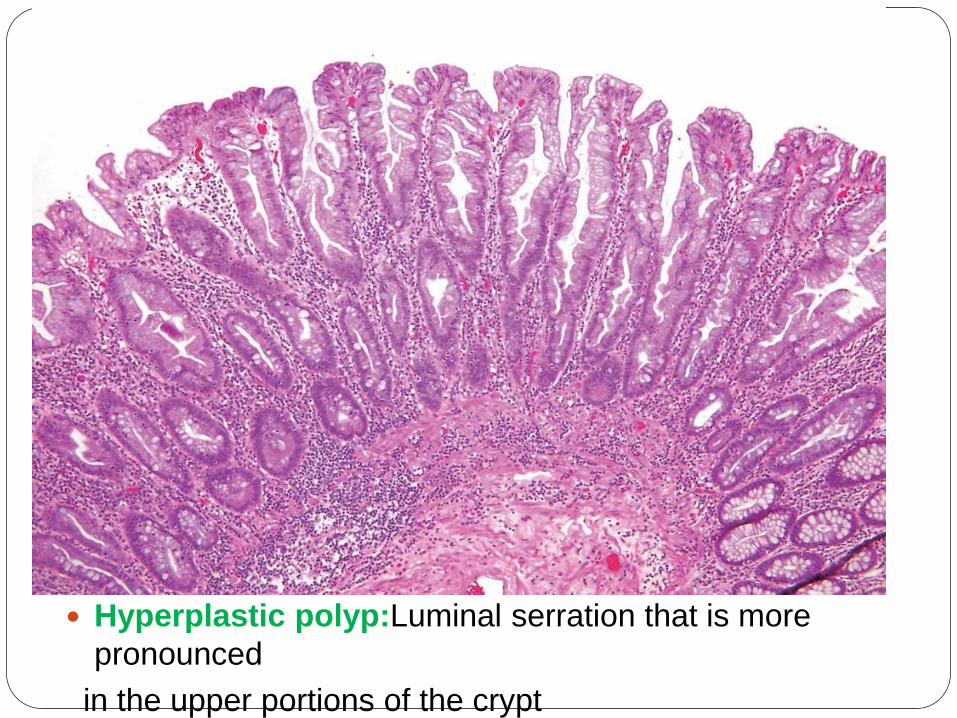
Hyperplastic polyp:Luminal serration that is more
pronounced
in the upper portions of the crypt
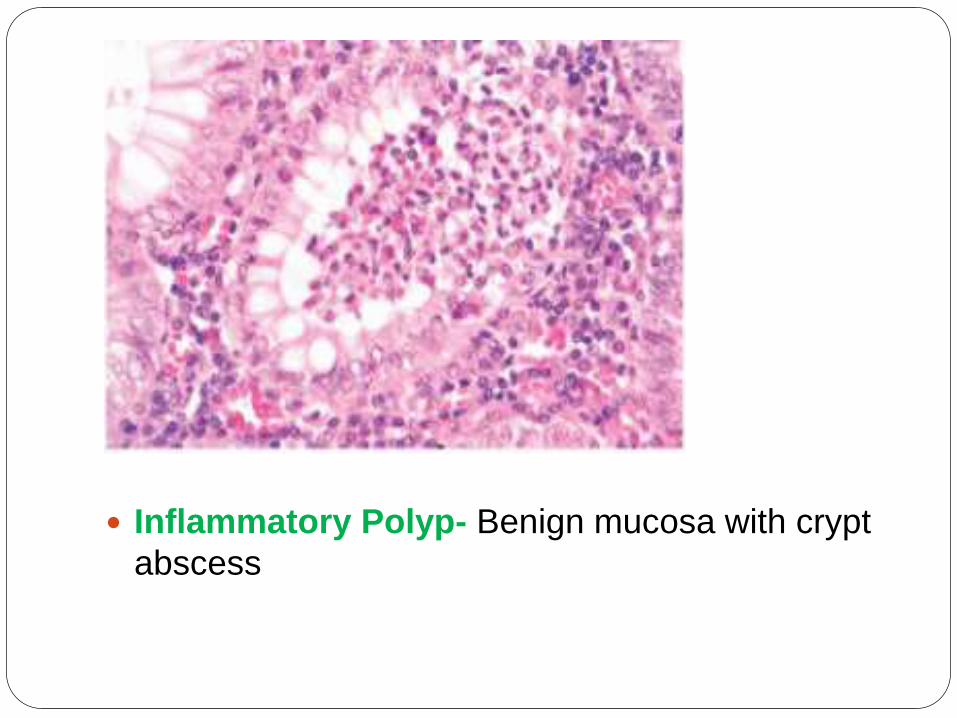
Inflammatory Polyp- Benign mucosa with crypt
abscess
Hamartomatous polyp-Juvenile Polyps(50 to 100 polyps)
-Peutz-Jeghers Polyps(melanotic mucosal
lesion)
Occurs singly and no malignant potential
But, Some rare Autosomal Syndromes occurs in
Hamartomatous polyp
-Juvenile Polyposis Syndrome-SMAD4 or
BMPRA gene
-Peutz-Jeghers Syndrome-LKB1/STK11 germline
mut.
-Cowden Syndrome(acral keratoses, oral
papilloma)
-Cronkhite-Canada Syndrome(Non-hereditary)
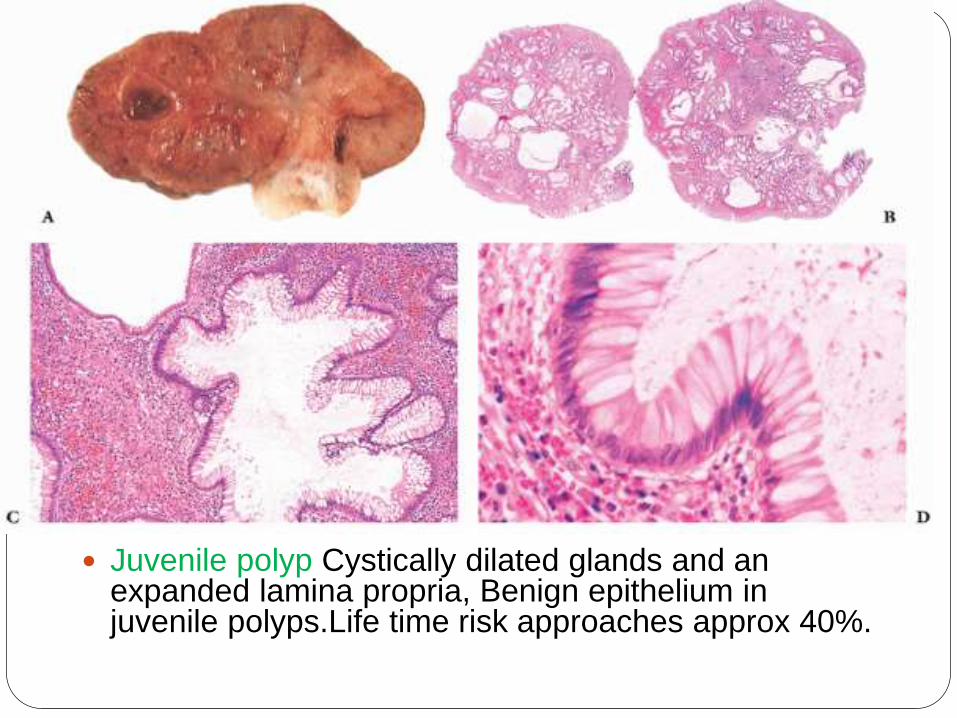
Juvenile polyp Cystically dilated glands and an expanded lamina propria, Benign epithelium in juvenile polyps.Life time risk approaches approx 40%.
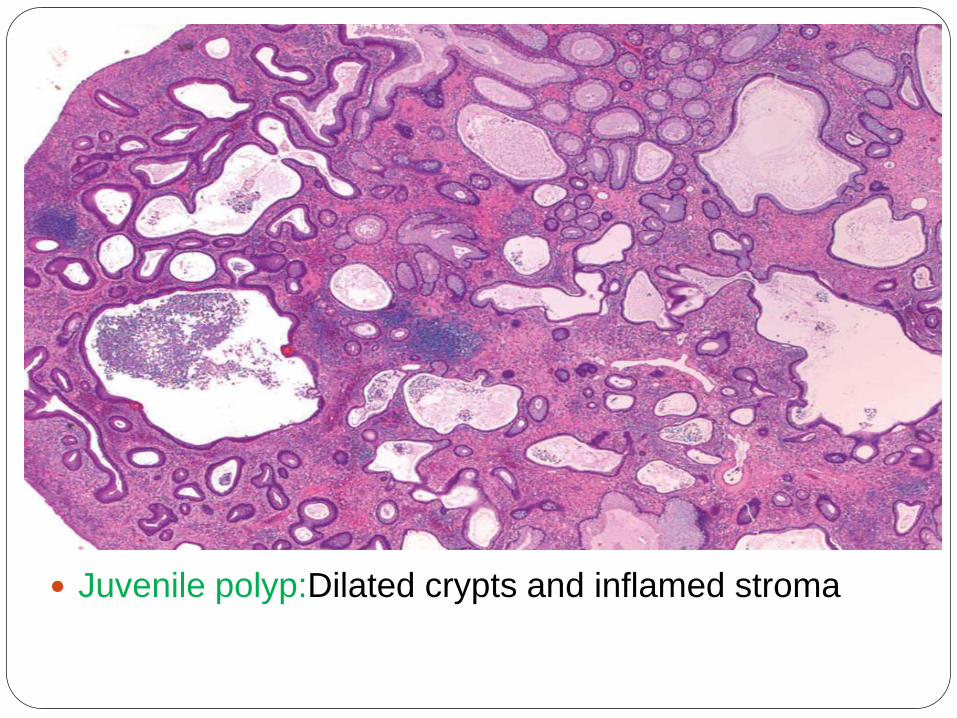
Juvenile polyp:Dilated crypts and inflamed stroma
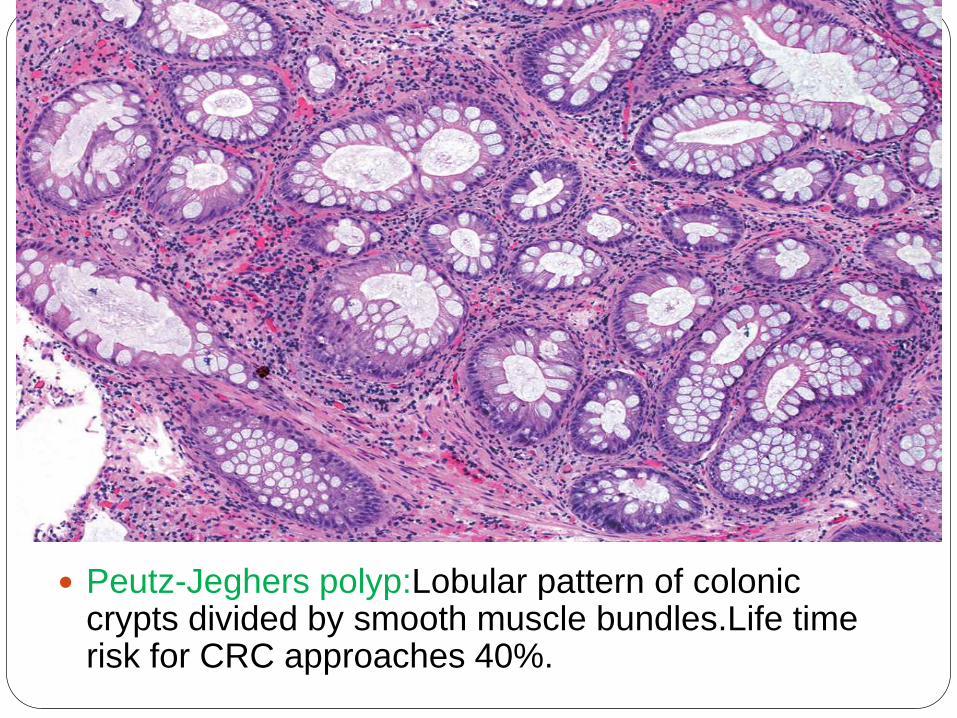
Peutz-Jeghers polyp:Lobular pattern of colonic crypts divided by smooth muscle bundles.Life time risk for CRC approaches 40%.
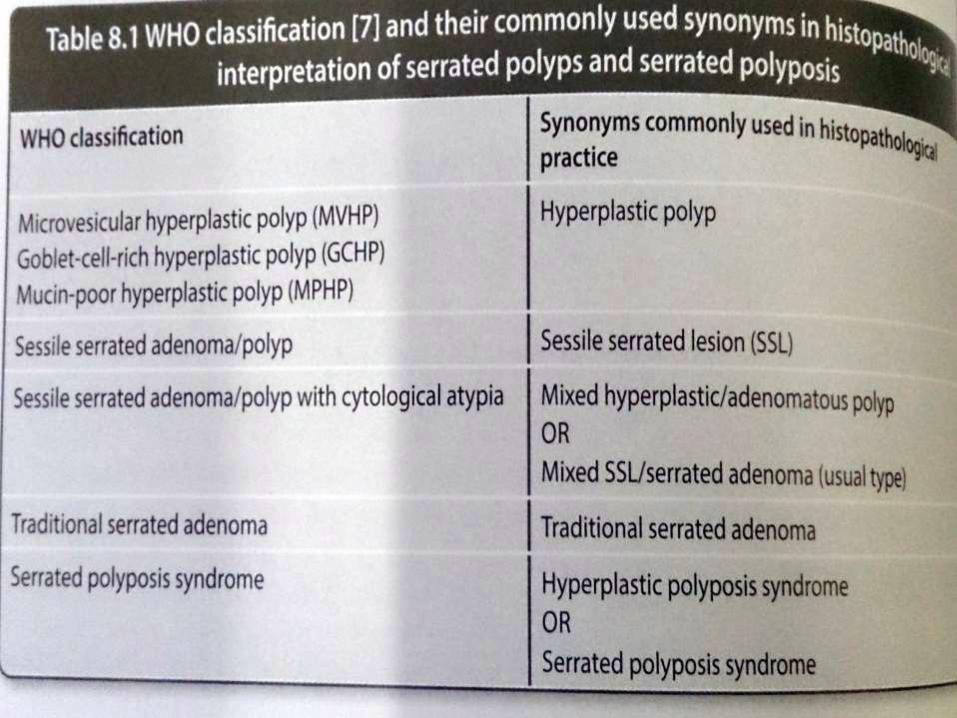
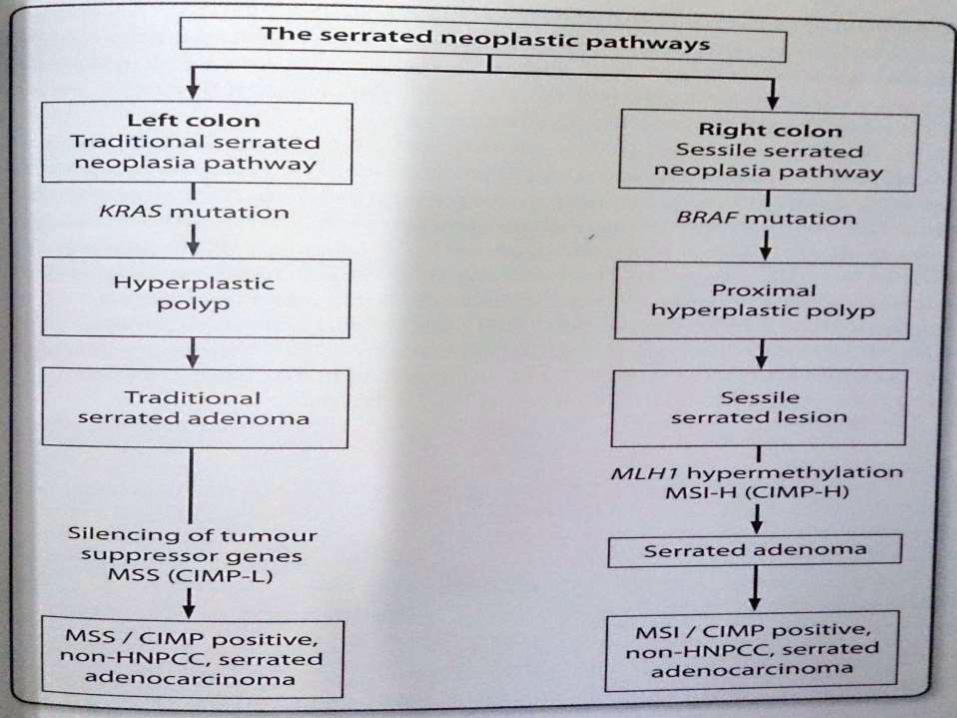
Serrated polyps
Newer term
General term for any polyp that shows
serrrated(sawtooth or stellate)
architecture.
Heterogenous Group
Hyperplastic Polyp
Sessile serrated Adenoma/Polyp
Traditional serrated adenomaBelived to be precursor lesions for cancer that have CpG island
methylator phenotype(CIMP) Pathway mutation and MSI
pathway mutation
Sessile serrated
Adenoma/Polyp
Currently used interchangeably
Proximal colon & female
Histologically
Exaggerated crypt serration
Serration throughout crypt length
Hypermucinous epithelium
Crypt Dilatation, Branching
Horizantal Crypt extension
Lack dysplastic nuclear that characterize
conventional adenomas.
Relatively new entity that used to be classified
as HP in past
SSA/Ps –Precursor lesion for
CRC with MSI and prob. Also
for CpG island methylated
carcinoma.
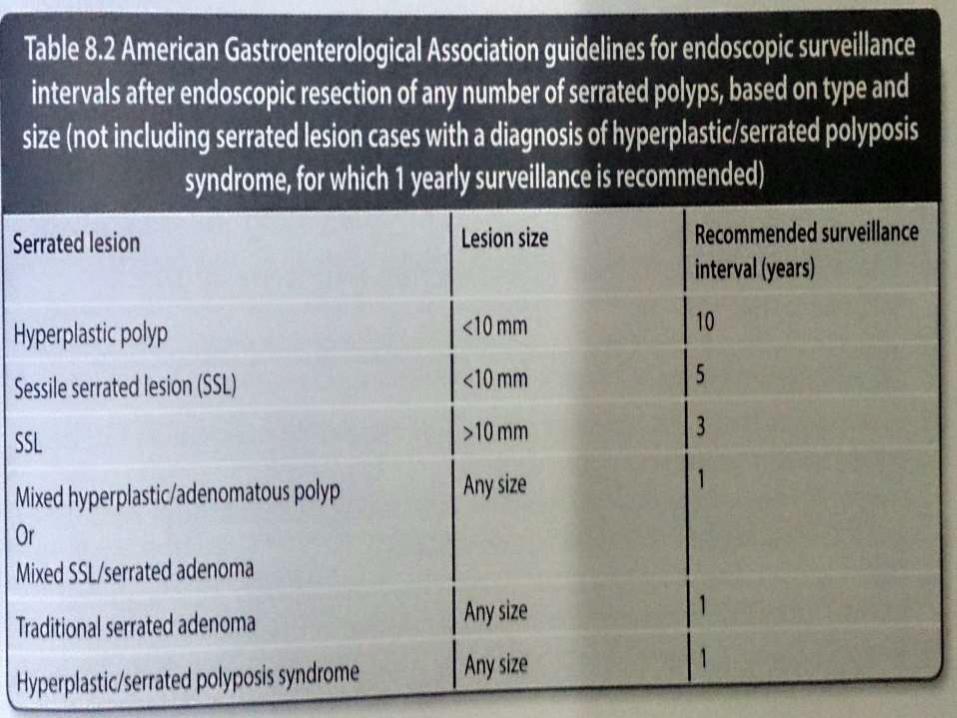
Serrated Polyposis
New term used by WHO
Historically called Hyperplastic polyposis
Defined by
-5 serrated polyps proximal to sigmoid
colon with 2 or more polyps >1cm.
-Any number of serrated polyp proximal to
sigmoid colon who has a 1st degree relative
having serrated polyposis
->20 serrated polyps of any size
throughout colon.
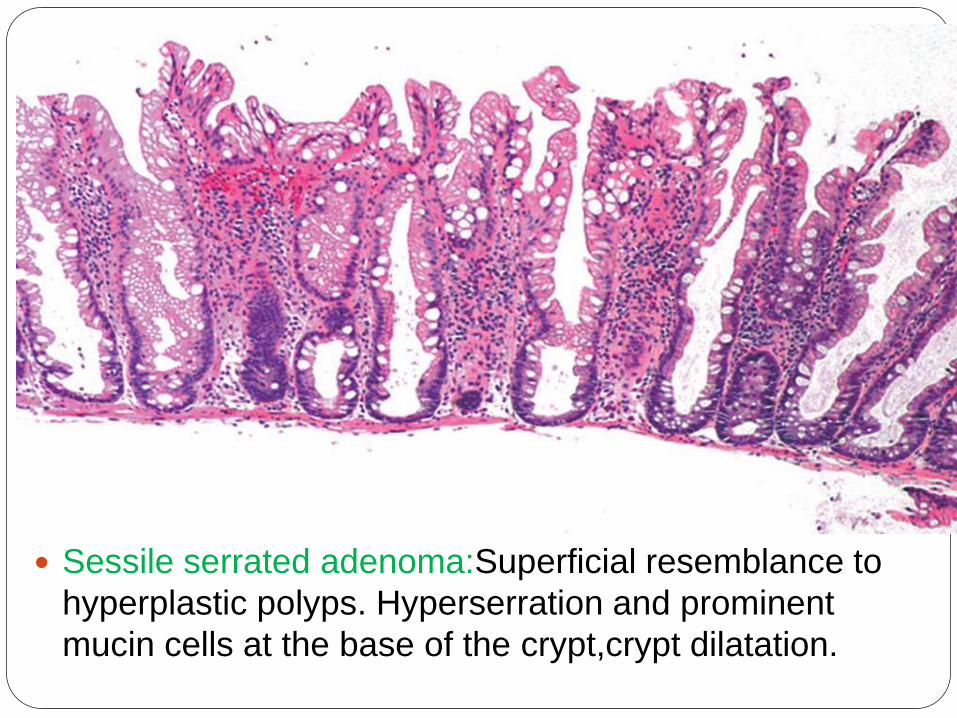
Sessile serrated adenoma:Superficial resemblance to
hyperplastic polyps. Hyperserration and prominent
mucin cells at the base of the crypt,crypt dilatation.
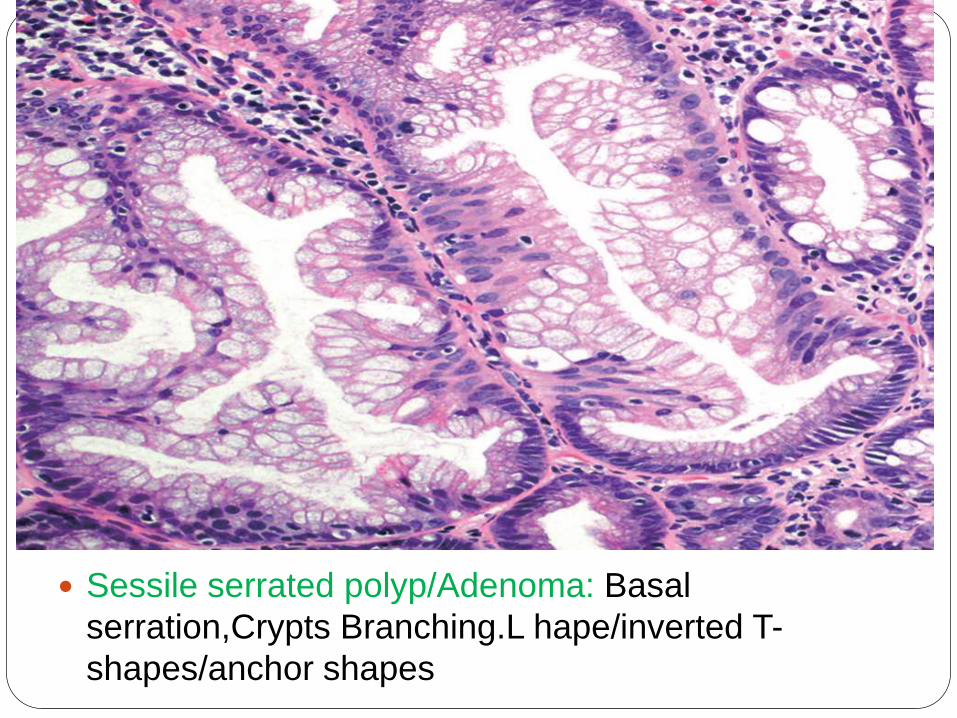
Sessile serrated polyp/Adenoma: Basal
serration,Crypts Branching.L hape/inverted T-
shapes/anchor shapes
Traditional serrated
Adenoma(TSA)
Uncommon type of true adenoma.
Low grade nuclear dysplasia similar to that
seen for conventional
adenoma
Shows a serrated architecture similar to
that seen for HP and SSA/P.
Prominent cytoplasmic eosinophilia and a
villous growth pattern are characteristic
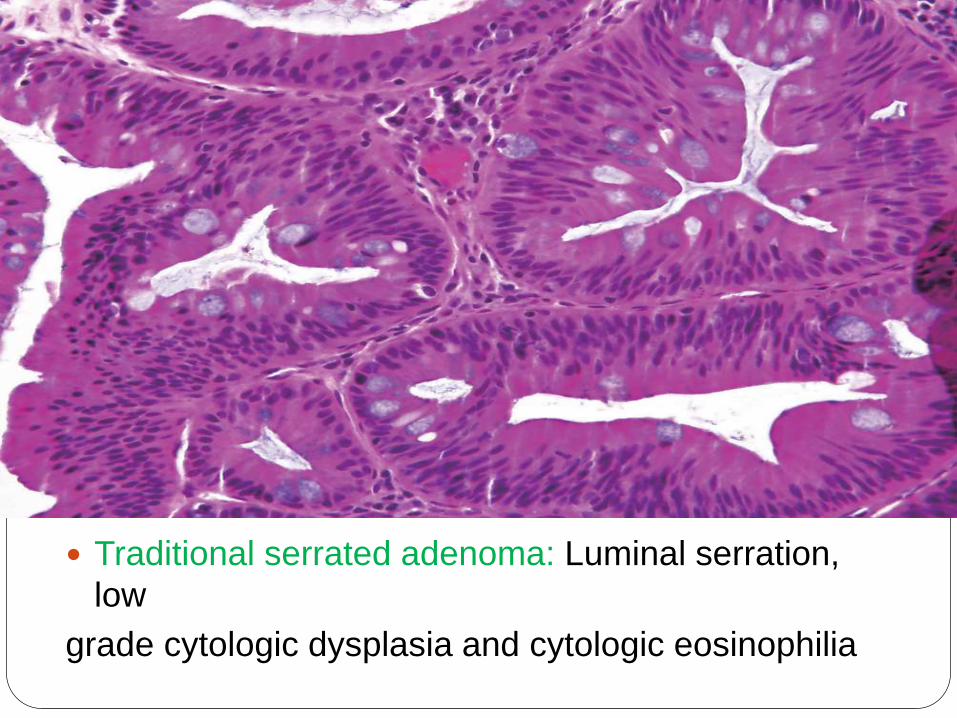
Traditional serrated adenoma: Luminal serration,
low
grade cytologic dysplasia and cytologic eosinophilia
Neoplastic Polyp-
Adenoma/Adenomatous polyp
Adenocarcinoma –approx 5% of all adenoma.
Also depend on size and histological type-
Invasive cancer is found in 0.5% of adenoma < 1 cm
5.0% - 1 to 1.9 cm
10% > 2 cm
Tubular- 2 to 3%
Tubulovillous-6 to 8%
Villous- 10 to 18%
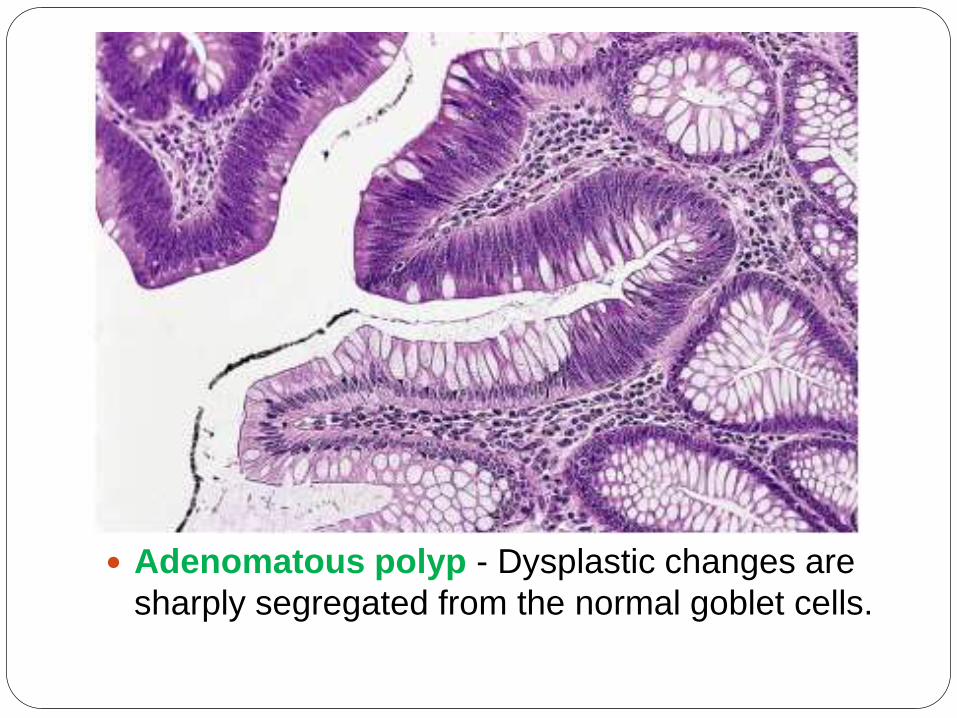
Adenomatous polyp - Dysplastic changes are
sharply segregated from the normal goblet cells.
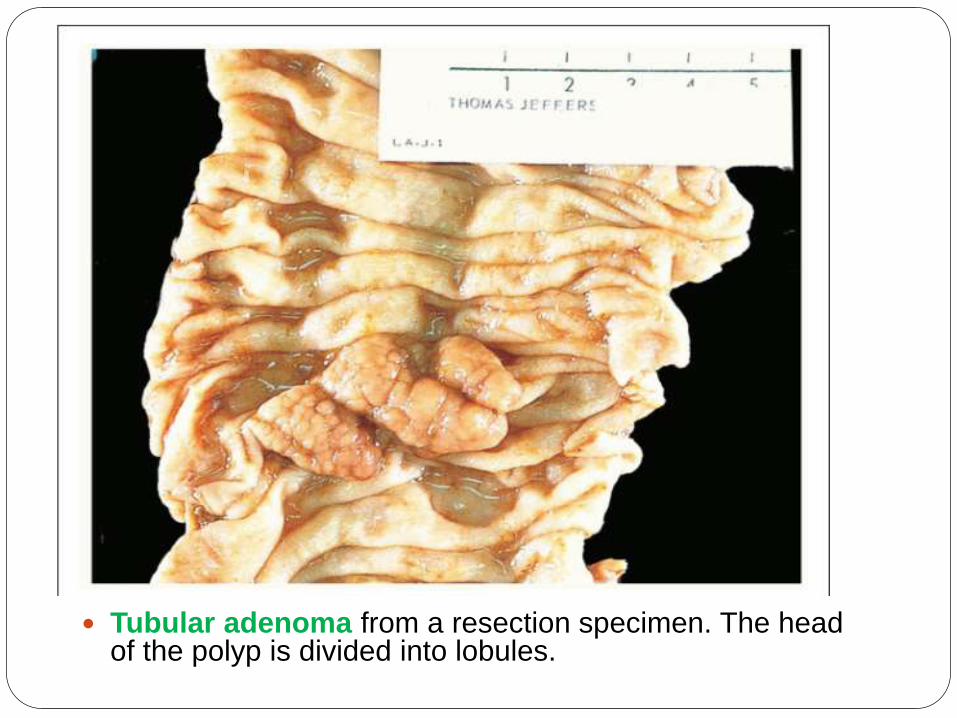
Tubular adenoma from a resection specimen. The head of the polyp is divided into lobules.
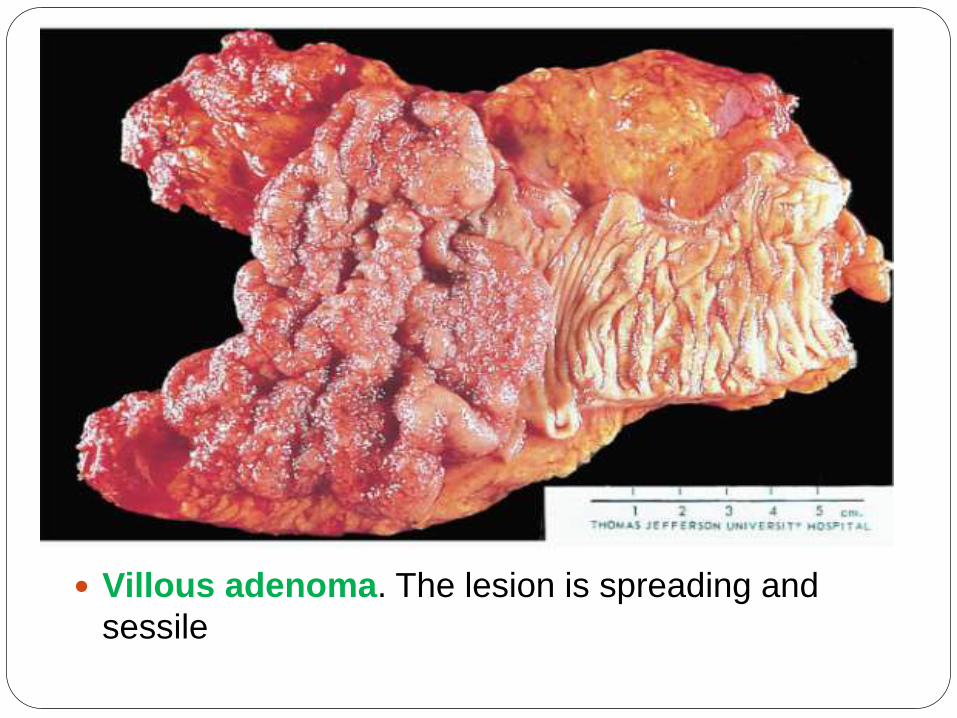
Villous adenoma. The lesion is spreading and
sessile
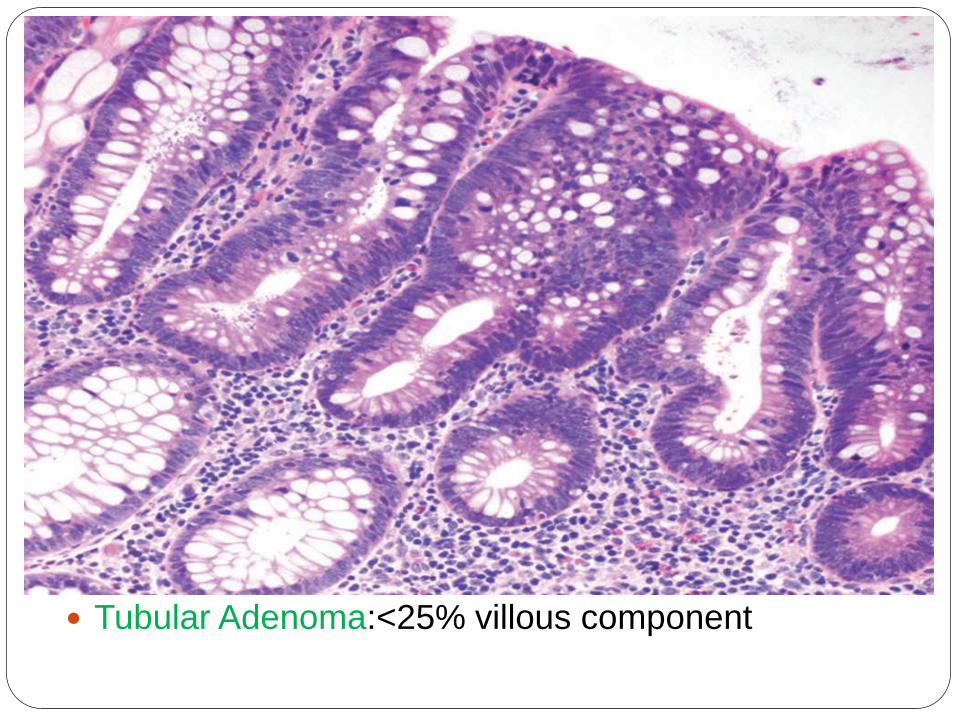
Tubular Adenoma:<25% villous component
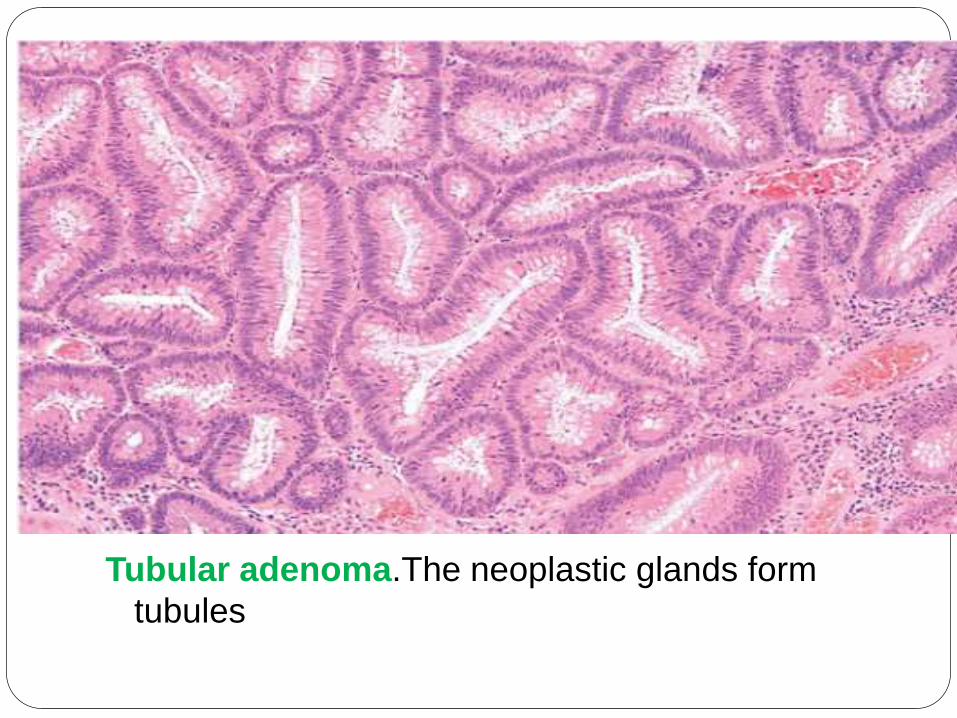
Tubular adenoma.The neoplastic glands form
tubules
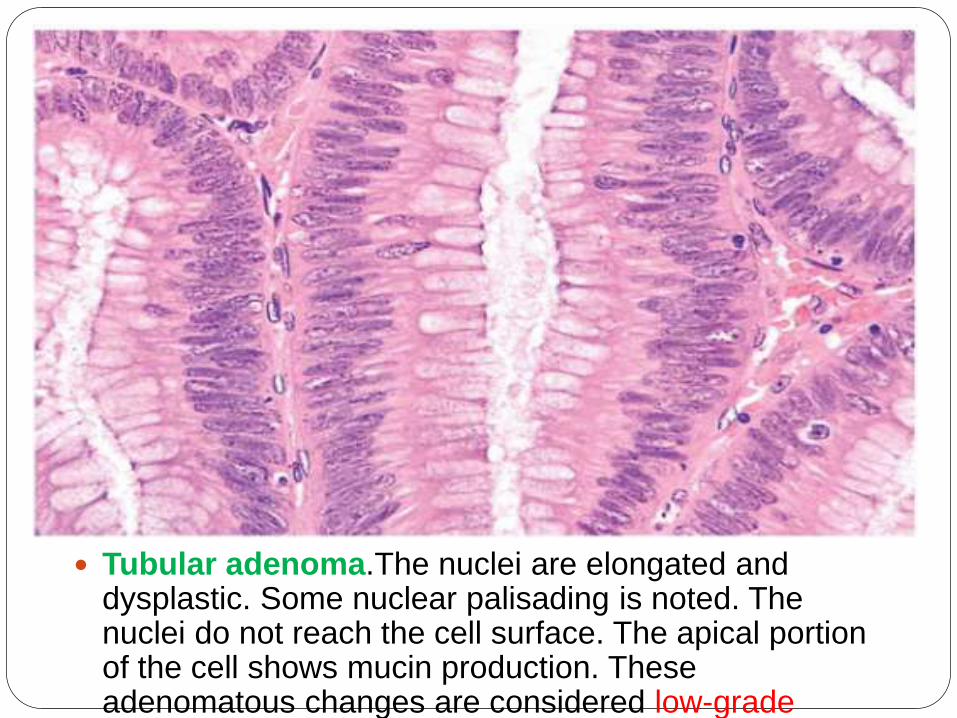
Tubular adenoma.The nuclei are elongated and dysplastic. Some nuclear palisading is noted. The nuclei do not reach the cell surface. The apical portion of the cell shows mucin production. These adenomatous changes are considered low-grade dysplasia.
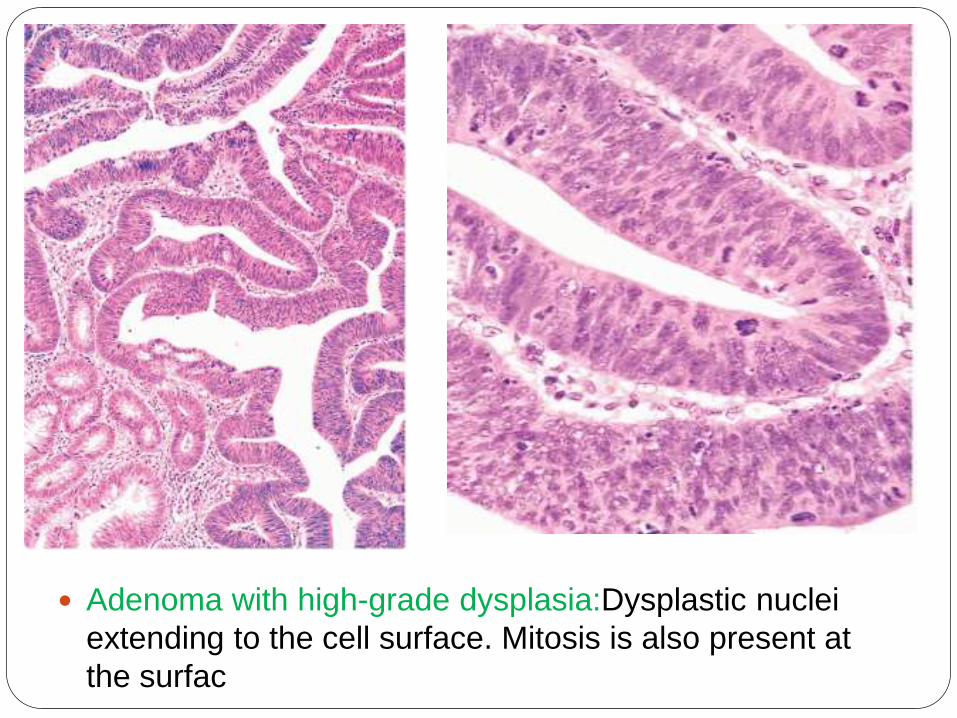
Adenoma with high-grade dysplasia:Dysplastic nuclei
extending to the cell surface. Mitosis is also present at
the surfac
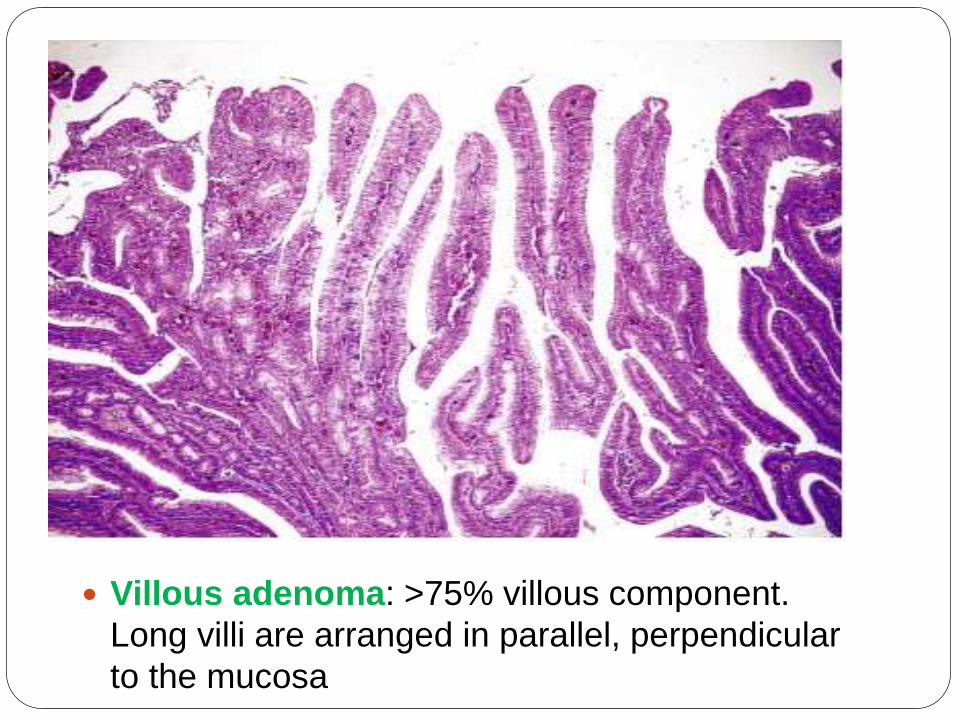
Villous adenoma: >75% villous component.
Long villi are arranged in parallel, perpendicular
to the mucosa
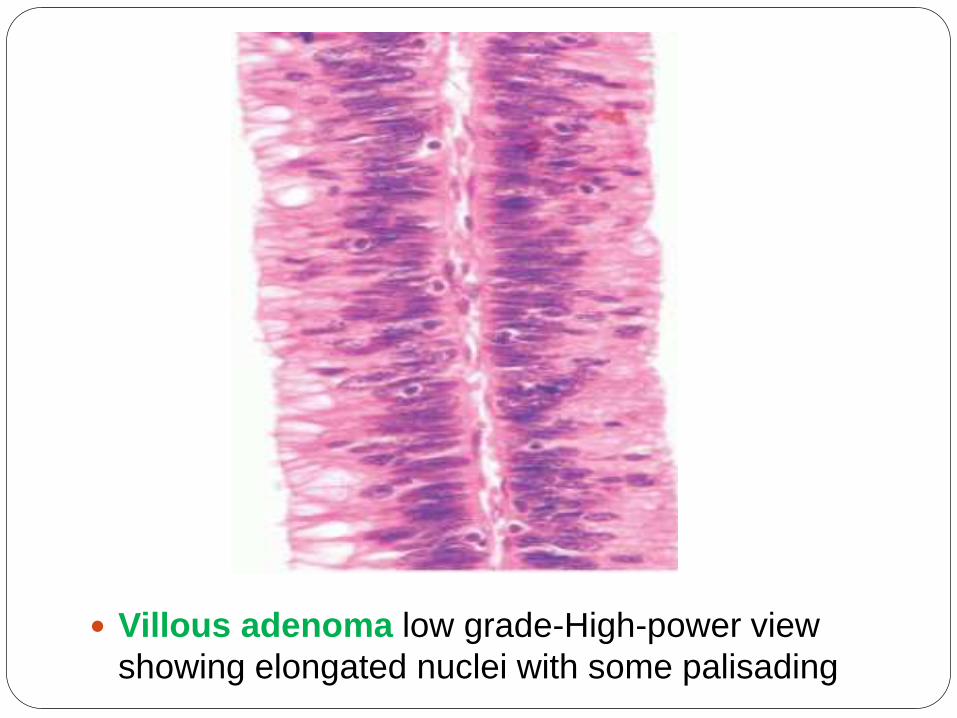
Villous adenoma low grade-High-power view
showing elongated nuclei with some palisading
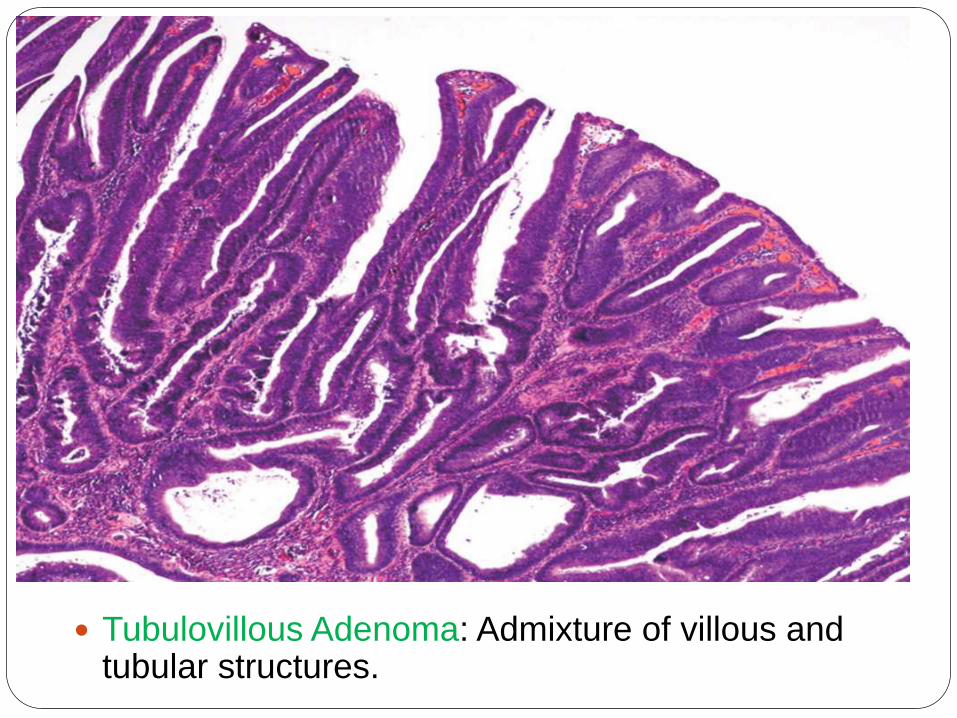
Tubulovillous Adenoma: Admixture of villous and tubular structures.
Pitfall in assessment of
Adenomatus polyp
Adenomatous elements misplaced/herniated into
the submucosa
Secondary to traumatization(Twisting and torsion of
the stalk)
Distinguished form true invasion-
-Lobular configuration of herniated elements
-Lack of overt high grade atypia
-Inflammatory cells around entrapped elements
-Lack of desmoplastic reaction
-Presence of hemosiderin or hemorrhage
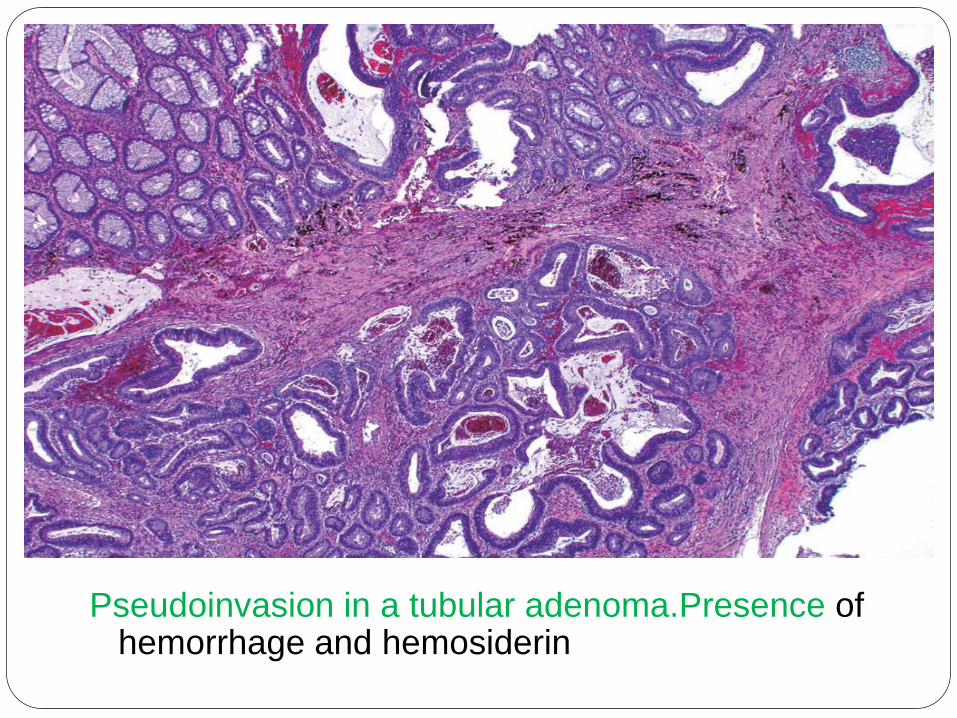
Pseudoinvasion in a tubular adenoma.Presence of hemorrhage and hemosiderin
Familial Syndromes Uncommon Autosomal dominant disorders
Importance-Propensity for malignant
transformation
Provide insight in the Molecular Pathogenesis
Peutz-Jeghers Syndrome-
Hamartomatous polyp
Juvenile Polyposis Syndrome
Cowden Syndrome
Familial Adenomatous polyp(FAP)-
Adenoma
HNPCC/Lynch syndrome-Adenoma-
Familial Adenomatous
Polyposis(FAP)
APC mutation on chromosme 5q21
Autosomal dominant disorder in which patients develop
numerous colorectal adenomas as teenagers.
At least 100 polyps are necessary for a diagnosis of classic
FAP, and as many as several thousand may be present
Adeno ca develop in 100% of untreated pt below 30 yr.
Prophylactic colectomy
Extaintestinal manifestation-congenital hypertrophy RPE
Some FAP patients without APC loss have mutations of the
base-excision repair gene MUTYH/MYH
MUTYH gene prevent mutation
following oxidative DNA damage.
Attenuated form of FAP/MUYTH
polyposis
•Delayed polyp development,
•Presence of fewer than 100 adenomas,
•Delay appearance of colon carcinoma >50
year or above
•Life time risk of cancer around 50%
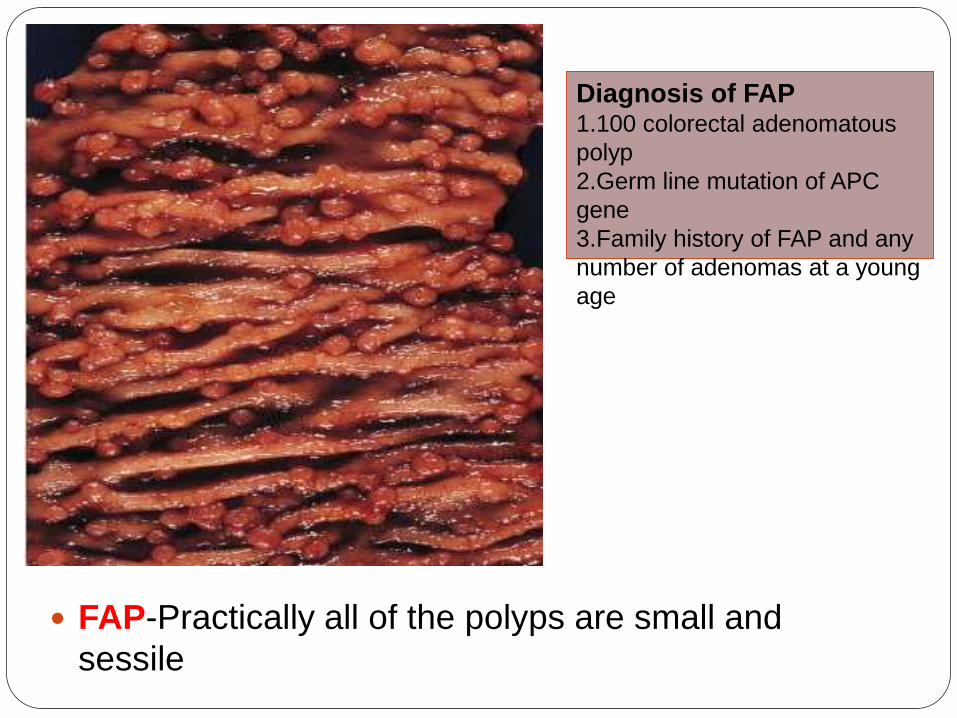
FAP-Practically all of the polyps are small and
sessile
Diagnosis of FAP1.100 colorectal adenomatous
polyp
2.Germ line mutation of APC
gene
3.Family history of FAP and any
number of adenomas at a young
age
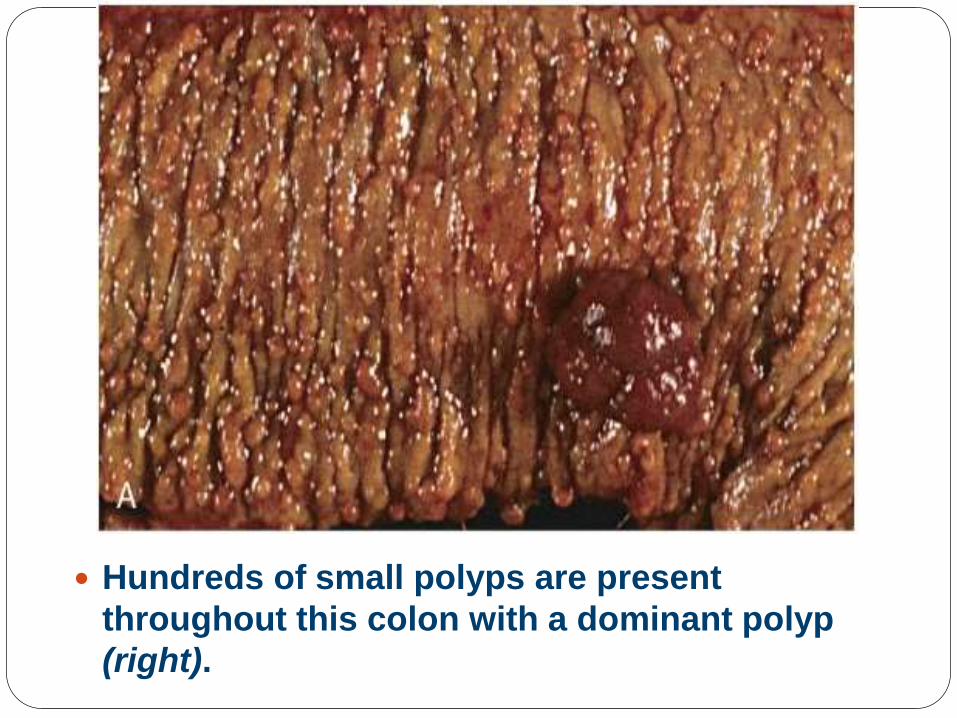
Hundreds of small polyps are present
throughout this colon with a dominant polyp
(right).
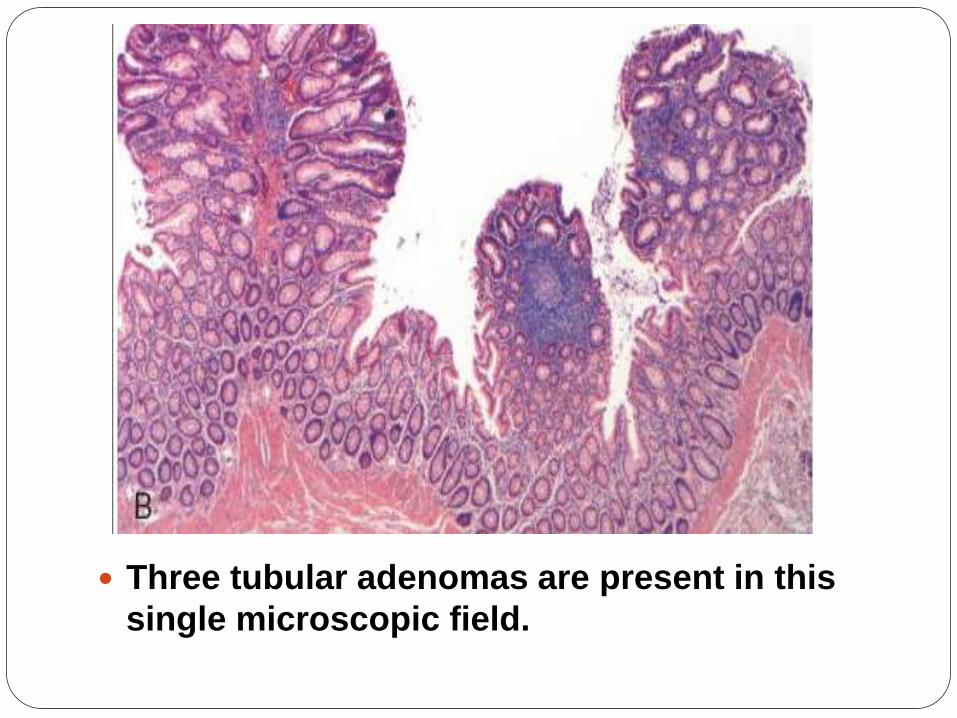
Three tubular adenomas are present in this
single microscopic field.
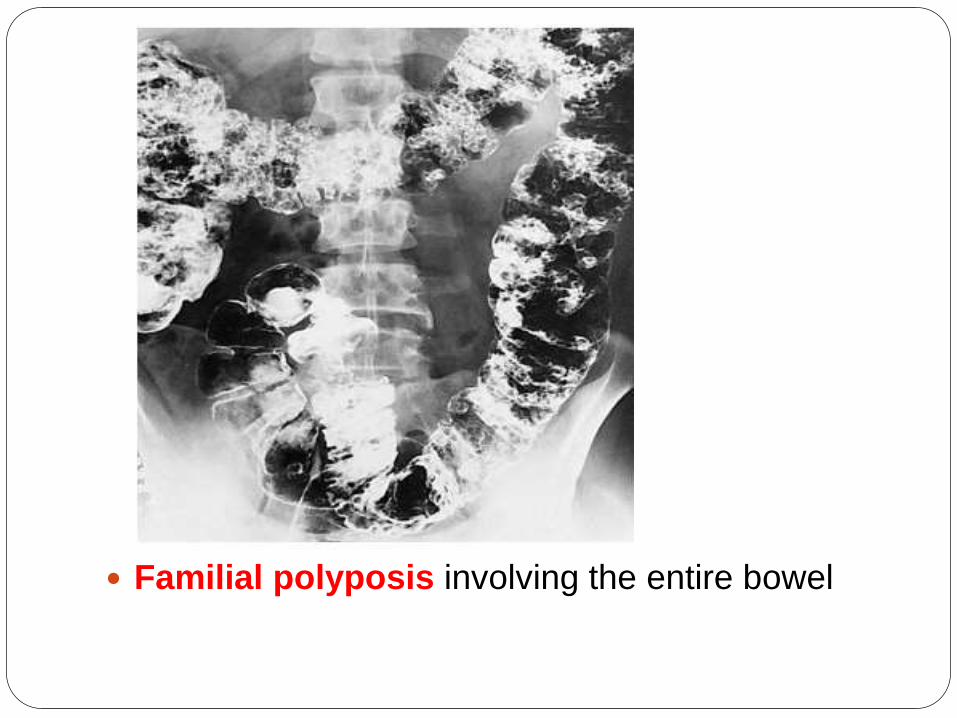
Familial polyposis involving the entire bowel
Other variants of FAP Gardner syndrome-
-Intestinal Adenoma
-Osteoma of mandible,skull,long bones
-Epidermal cysts
-Desmoid tumor
-Thyroid tumor
-Dental abnormalities(Supenumerary teeth,unerupted
teeth)
Turcot Syndrome-
-Intestinal adenomas
-CNS abnormality(medulloblastoma/glioblastoma)
Two third have APC mutation and rest one third have DNA
mismatch repair gene defect
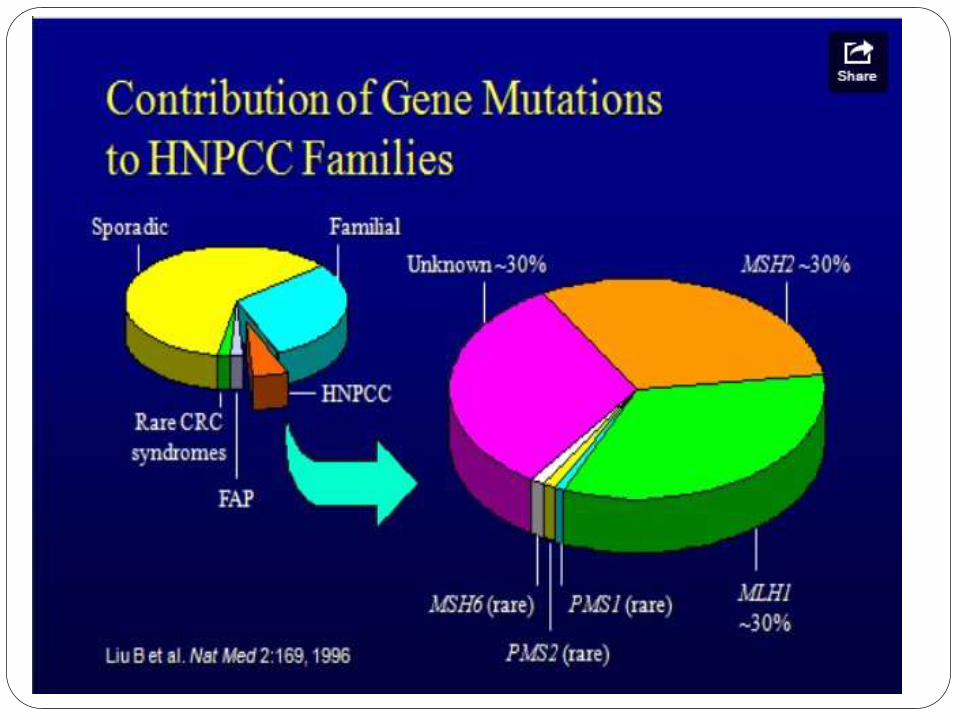
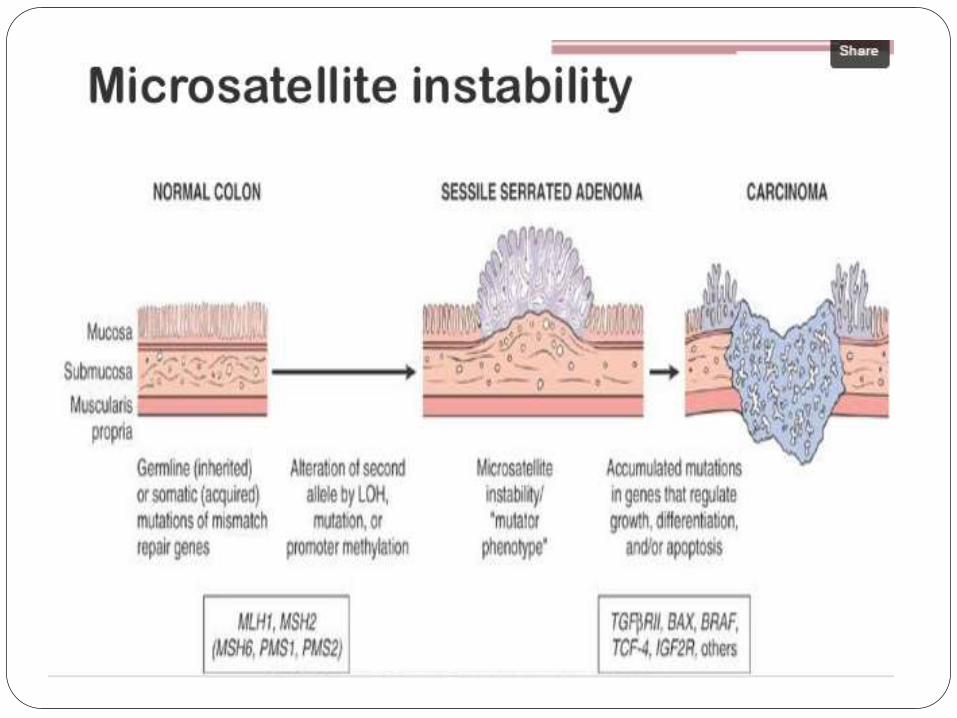
HNPCC/Lynch syndrome Inherited mutations in genes that encode proteins
responsible for the detection, excision, and repair of
errors that occur during DNA replication(Mismatch
repair gene).
Life time risk of cancer-66% for men and 43% for
women
MSH2 and MLH1 (Mainly).Others mismatch repair
genes are PMS1,PMS2,MSH6
Inherit one mutated DNA repair gene and one
normal allele
Familial clustering of cancers at several sites-
colorectum,endometrium,Stomach,Ovary,Uterus,Br
ain,Small bowel,skin
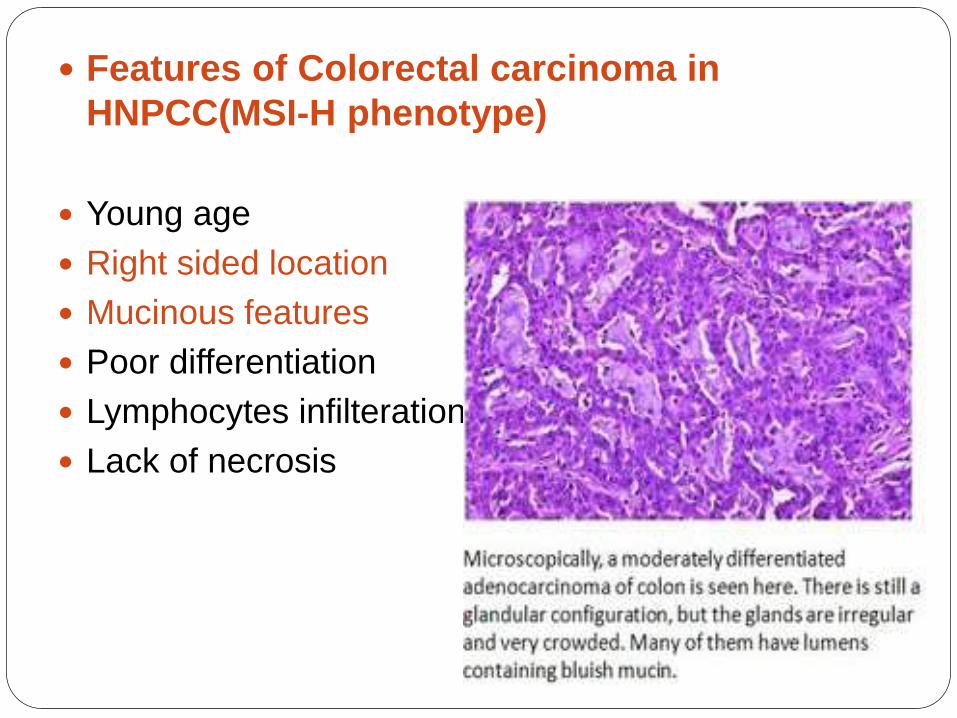
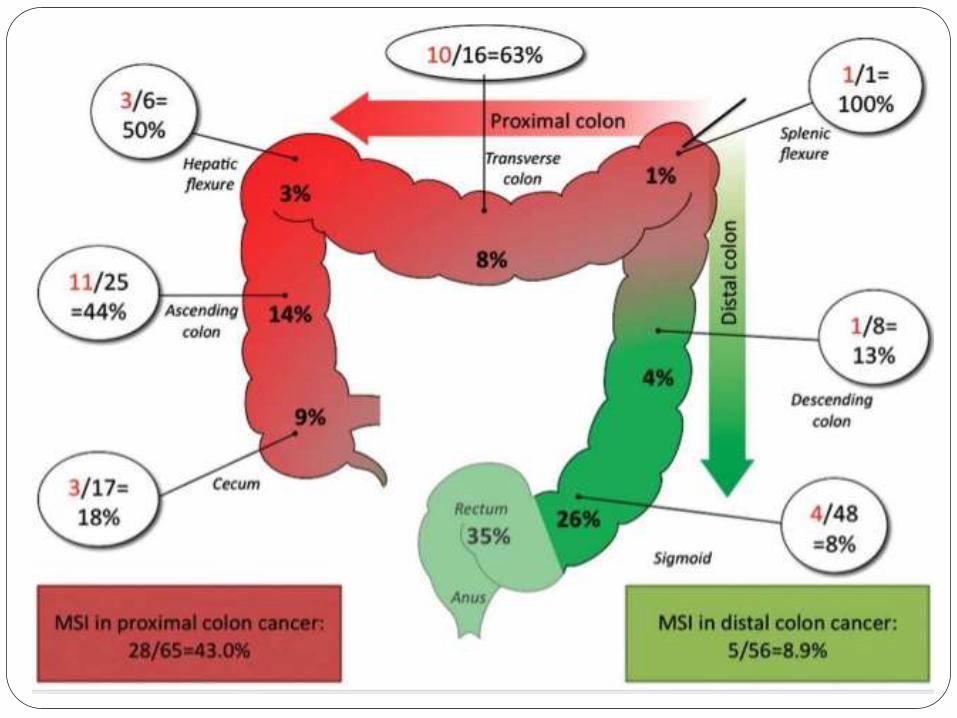
Features of Colorectal carcinoma in
HNPCC(MSI-H phenotype)
Young age
Right sided location
Mucinous features
Poor differentiation
Lymphocytes infilteration
Lack of necrosis
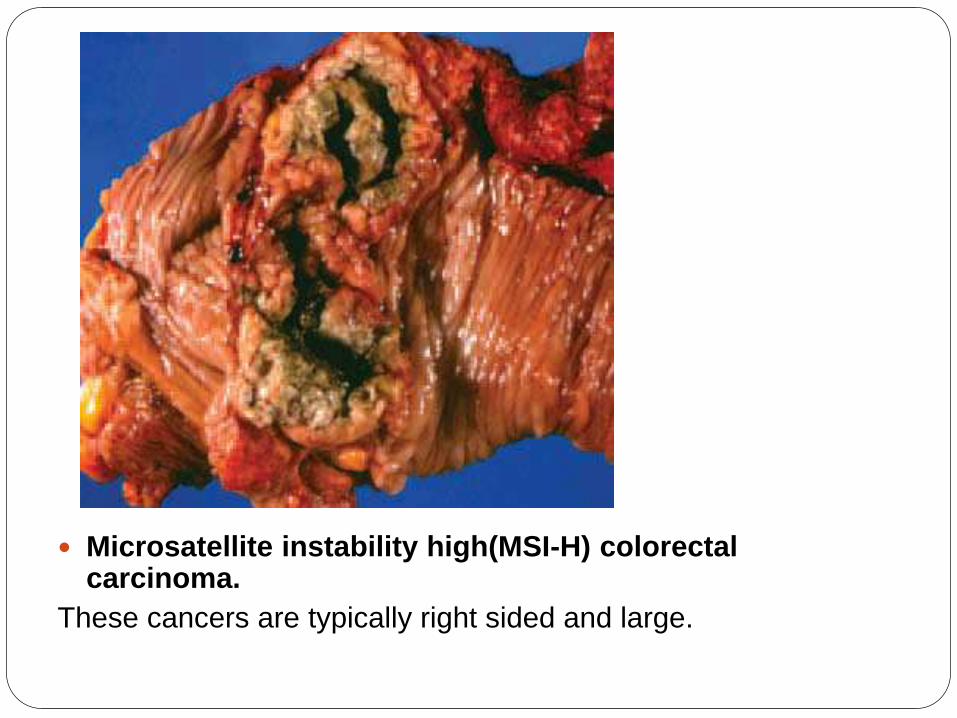
Microsatellite instability high(MSI-H) colorectal carcinoma.
These cancers are typically right sided and large.
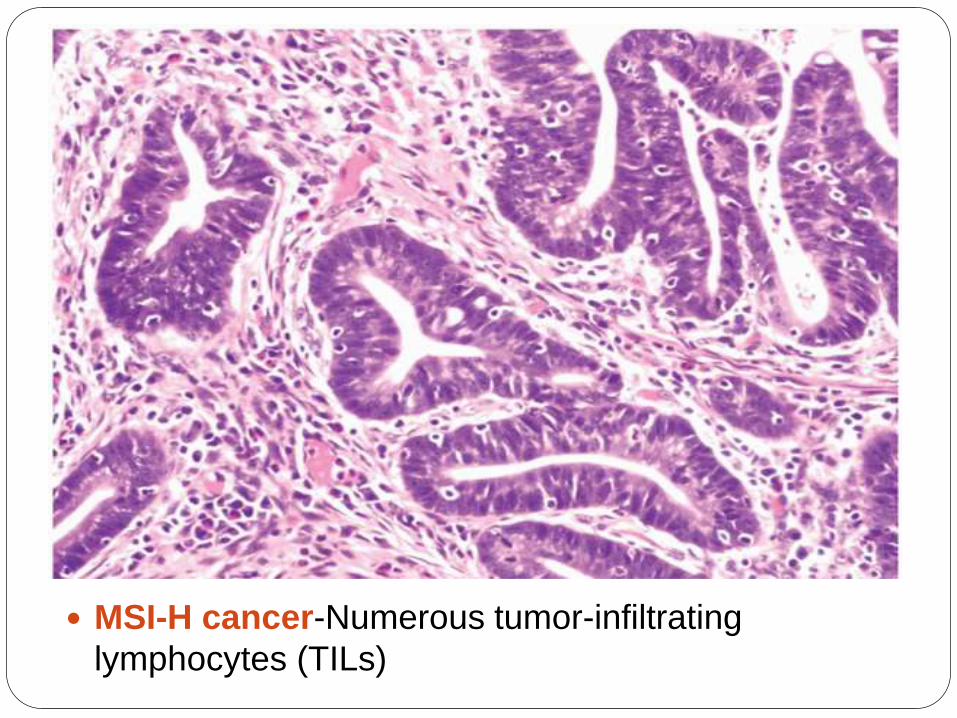
MSI-H cancer-Numerous tumor-infiltrating
lymphocytes (TILs)
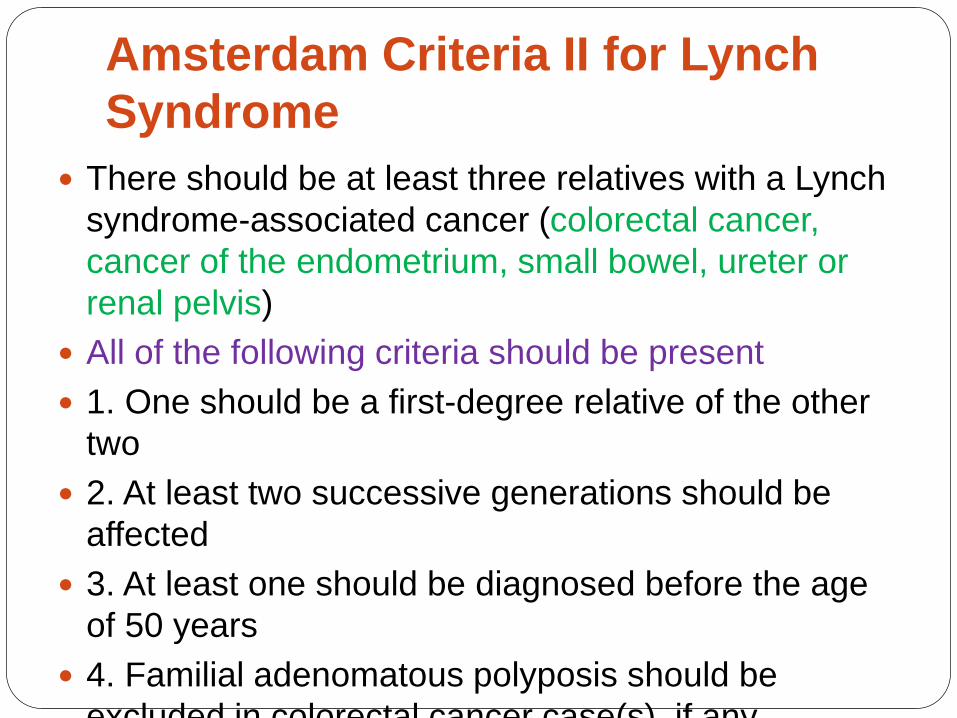
Amsterdam Criteria II for Lynch
Syndrome
There should be at least three relatives with a Lynch
syndrome-associated cancer (colorectal cancer,
cancer of the endometrium, small bowel, ureter or
renal pelvis)
All of the following criteria should be present
1. One should be a first-degree relative of the other
two
2. At least two successive generations should be
affected
3. At least one should be diagnosed before the age
of 50 years
4. Familial adenomatous polyposis should be
excluded in colorectal cancer case(s), if any
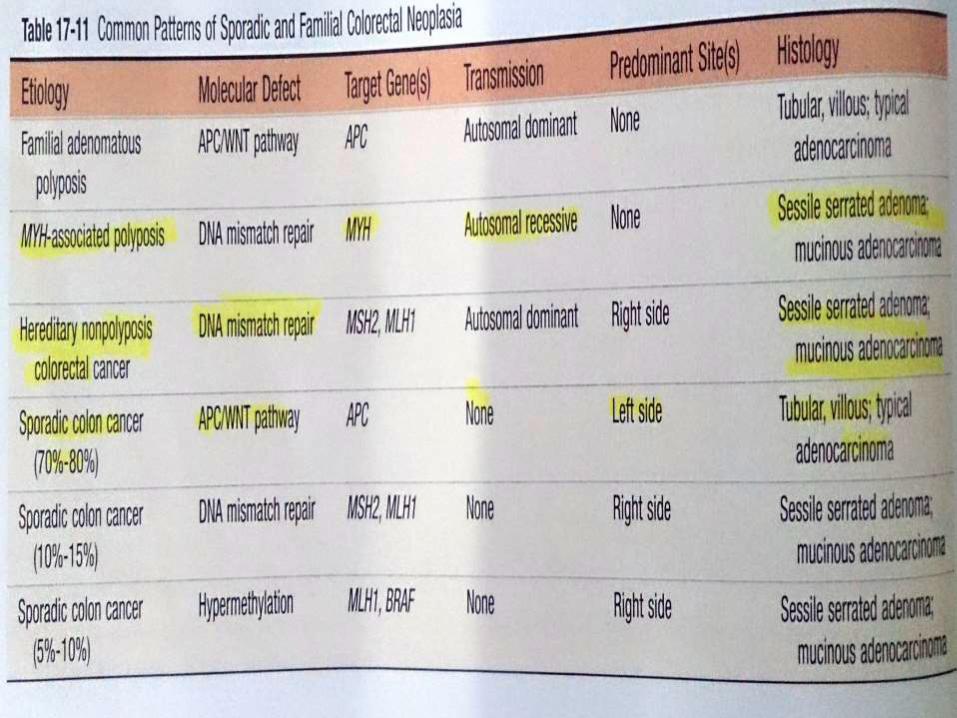
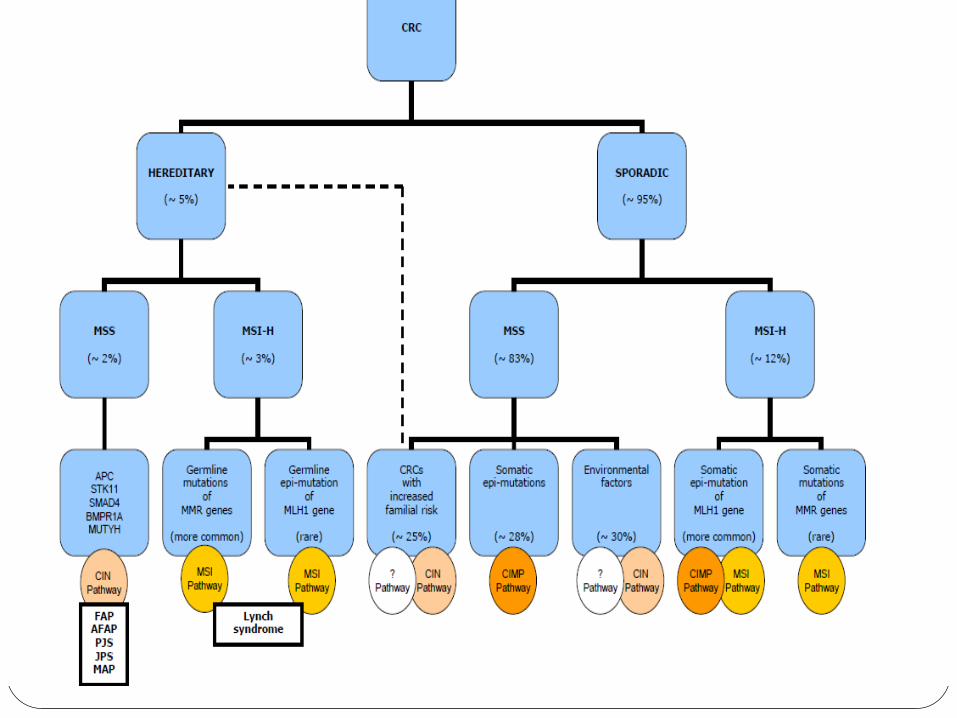
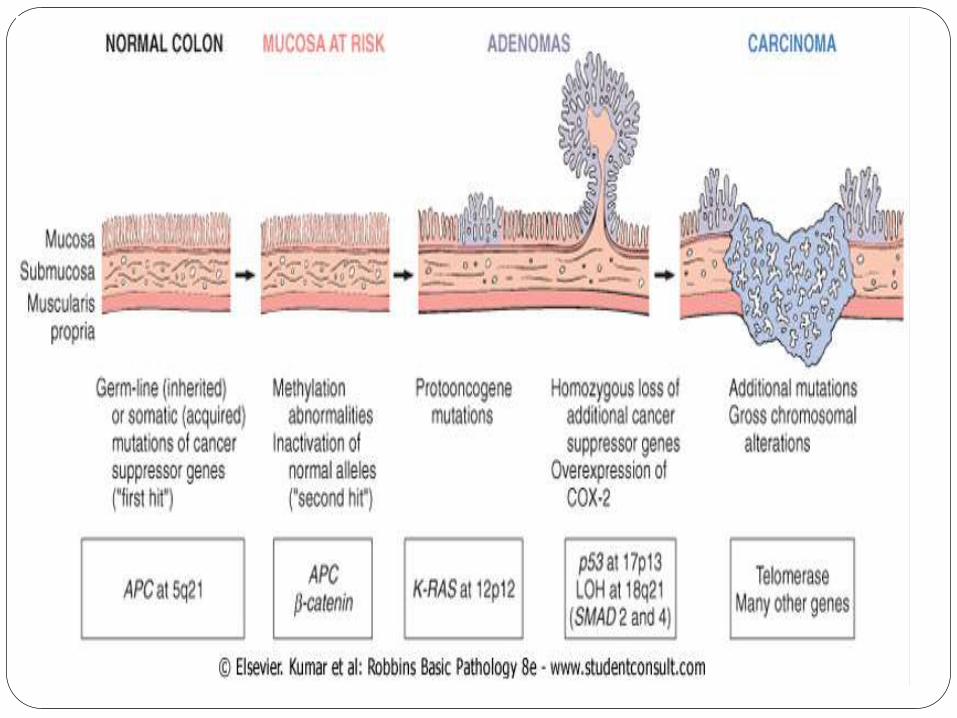
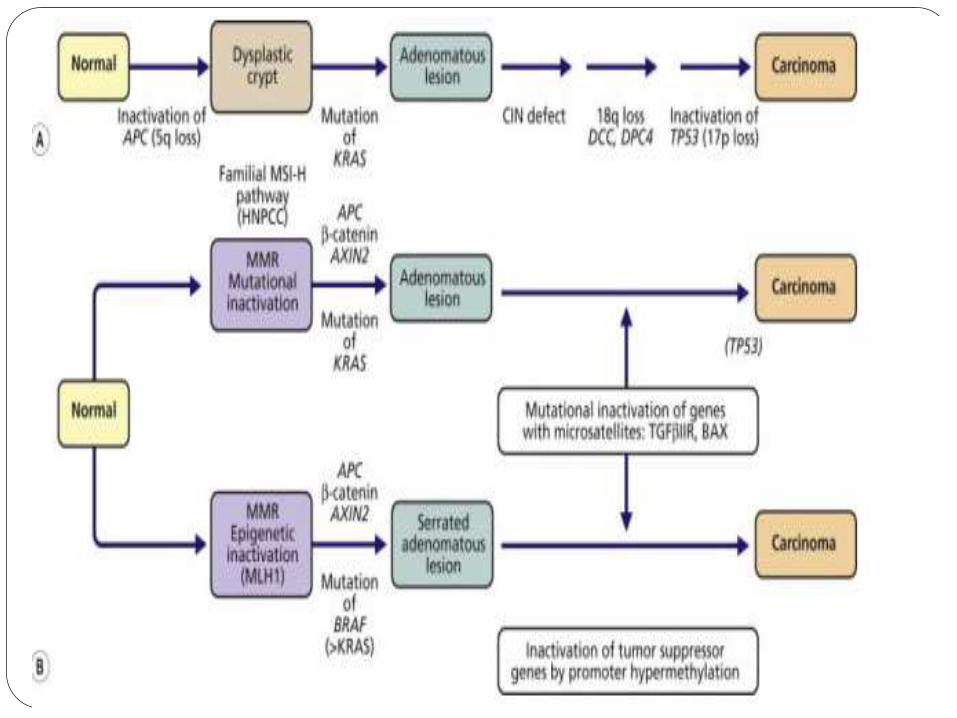
Carcinogenesis and Molecular
Pathogenesis Two distinct genetic pathway
1.APC/β catenin pathway
Associated with WNT signaling pathway and the
chromosomal instability pathway(CIN).
2.Microsatellite instability pathway(MSI pathway)
Associated wuth defect in DNA mismatch repair gene
Overview of Molecular
Pathogenesis
Clasical adenoma-carcinoma sequence-
80% of sporadic-Typically include mutation
of APC early in neoplastic process.
In patient with DNA mismatch repair def. ,
Mutation accumulate in Microsatellites
repeats- Codition referred as –Microsatellite
instability(MSI)-MSI high or MSI-H tumors-
Mutation in TGFβ(inhibit cell prolif) and
proapop BAX
A subset of microsatellite unstable colon
cancer without mutation in DNA mismatch
repair gene-CpG island hypermeth.
Phenoty(CIMP)-MLH1 promoter region
hypermethylation and its repair fn. And
activating mutation in oncogene BRAF
A small group display increased CpG island
hypermethylation in absence of
microsatellite instability associated with
KRAS mutation
Overview Both MSI and CIN describes pathogenesis—Loss of
function of tumor suppressor gene and/or gain of
function of Oncogenes.
Last decade epigenetic instability has gained
attention.
Implicated in pathogenesis of almost one third of
colorectal cancers.
Epigenetic Modification includes—
-DNA methylation
-Histone alteration
-Chromatin remodelingBest characterized epigenetic modification is silencing of
genes (tumor suppressor and/or MMR genes) through
hypermethylation of their promotor region.
Epigenetic instability
Promoter Hypermethylation of MLH1
gene –demonstrated in majority of CRC
with a MSI phenotype.
Methylation of cytosine residue in CpG
island is a common phenomenon—
cause loss of function of tumor
suppresor gene without mutations.
CIMP pathway occurs in some MSI-H or
MSS tumor
APC/β Catenin pathway
APC Tumor suppresor gene (5q21)
Downregulate Growth promotimg Signals (β-catenin)
Component of WNT Signaling Pathway
Catenins—Proteins found in complexes with cadherin cell adhesion molecule.
β- catenin participate in the WNT signaling pathways as a growth promoting signals.
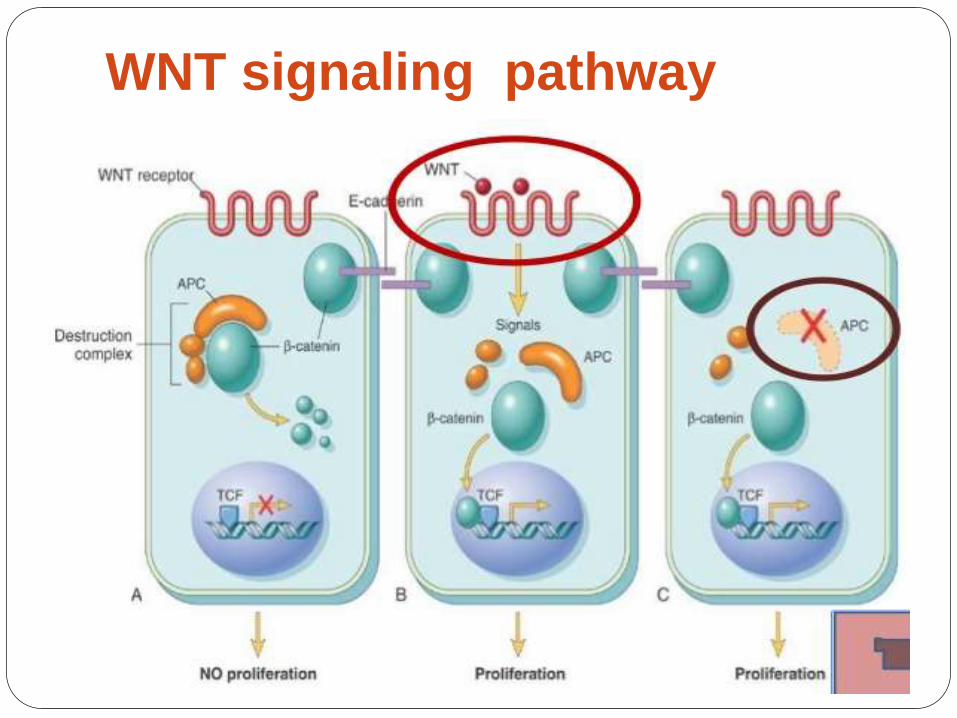
WNT signaling pathway
WNT signaling pathway
Passes signals from cell surface
receptors to the nucleus through
cytoplasm
Causes expression of target genes (
transcription regulator genes-cMYC and
Cyclins).
Major role in controlling cell
fate,adhesion and cell polarity during
embryonic development
WNT signaling is also require for self
Chromosomal instability
pathway(CIN)
Incresed rate of chromosome
missegregation in mitosis
Due to
--Gain/loss of
chromosome(Aneuploidy)
--Gross chromosomal rearrangment
Earliest event involved in CIN is APC gene
mutation(80%)
-K-RAS mutation
-p53 gene mutation
Late event – DCC (deleted in colonic
carcinoma) gene mutation
Advance event-DPC4/SMAD4 mutation
(18q21)
CIN forms the basis of
Adenoma- Carcinoma
sequence
MICROSATELLITE INSTABILITY
Pathway (MSI)
Satellite DNA?
Microsatellite DNA?
Why it is more liable to be unstable?
How this instability leads to colorectal
carcinoma?
Satellite DNA
Satellite DNA is composed of tandemly repeating DNA (non-coading regions)
Tandem repeats occur in DNA where a pattern of two or more nucleotides is repeated .
A-T-T-C-G-A-T-T-C-G-A-T-T-C-G
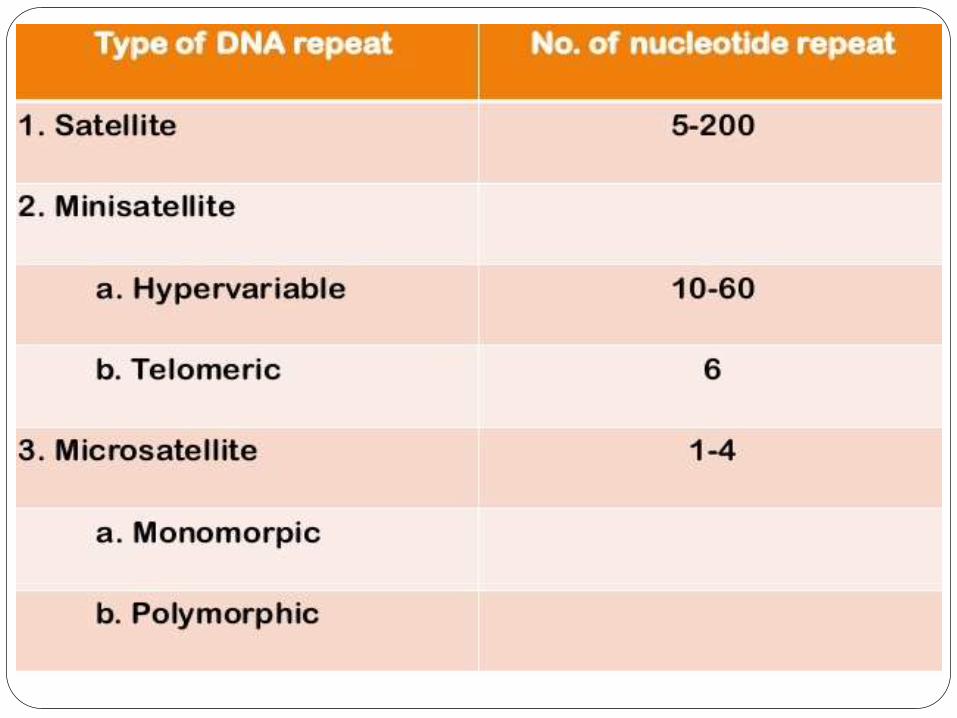
Microsatellite DNA
If the number of nuleotide repeat is 1-4
Dinuleotide repeat
When exactly two nuleotide are
repeated.eg-ACACACAC
Such region in DNA are commonly affected
in HNPCC.
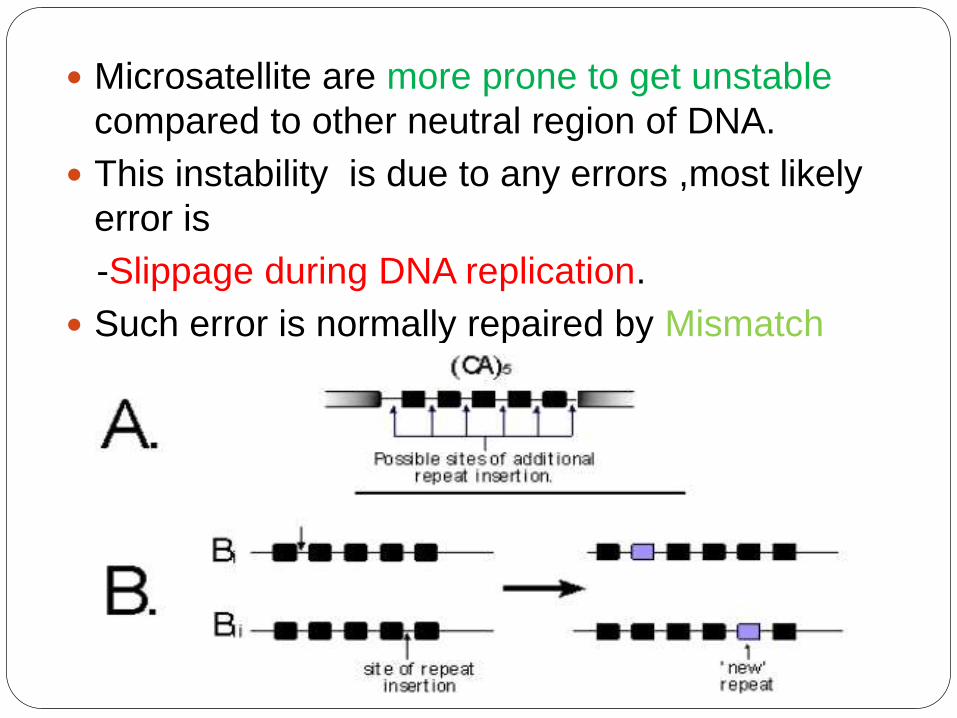
Microsatellite are more prone to get unstable
compared to other neutral region of DNA.
This instability is due to any errors ,most likely
error is
-Slippage during DNA replication.
Such error is normally repaired by Mismatch
repair enzymes which are encoaded by
Mismatch repairs genes.
Defect in MMR gene
Reduced capacity of cells to repair
specific types of DNA damage
Increased rate of mutation
accumulation in
microsatellite DNA
Colorectal Carcinoma(CRC)
Mismatch repair genes(MMR)
MSH2(2p21)
,MSH3,MSH4,MSH5,MSH6
MLH1(3p21.3), MLH2,MLH3
PMS1,PMS2
As majority of microstaellite are
located in non-coding region, these
mutations are generally silent
Some microsatellite which are present
in the coding region of the gene are
involved in the regulation of cell
growth, like thoe encoading
Type II TGF-β receptor
Proapoptotic protein BAX
Defect in MMR gene
Mutation—HNPCC
CpG island Hypermethylation
in MMR Gene---Sporadic
Colorectal Carcinoma
CpG Island Hypermethylation
What is CpG?
Term like CpG site and Cpg Island?
What is methylation?
What is Hypermethylation?
How Hypermethylation leads to Carcinoma?
CpG Sites
Region of DNA where a cytosine occurs next
to a guanine.
DNA methylation occurs at these sites by an
enzyme –DNA methyltransferase
In Humans, 80 to 90% of all CpGs are
Methylated.
This methylation results in conversion of
cytosine to 5- Methylcytosine
The remaining 10%
nonmethylated CpGs are
grouped in a cluster forming
CpG island, and is usually
located in the promoter region
toward 5’ end.
The unique property of Cpg
island is that it is unmethylated
in germ line.
Methylation of CpG island
within the promoters of gene
Silencing of tumor suppressor
gene Colorectal cancer
Susceptible Tumor Supressor genes which
shows ‘CpG island methylator phenotype’
positivity(CIMP+) –
MLH1
p16
MGMT
IGF2
RUNX3
SOCS1
NEUROG1
Ref – Recent advances in histopathology 23rd
edition

The Bethesda Guidelines
MSI testing is recommended in people with any of
the following features-
1.Colorectal cancer diagnosed in a patient who is less than
50 years of age
2. Presence of synchronous colorectal, or other Lynch
syndrome-related tumors,regardless of age
3. Colorectal cancer with the MSI-H histology,diagnosed in
a patient who is less than 60 years of age
4. Colorectal cancer diagnosed in one or more first-degree
relatives with a Lynch syndrome-related tumor, with one of
the cancers being diagnosed under age 50 years
5. Colorectal cancer diagnosed in two or more first- or
second-degree relatives with Lynch syndrome-related
tumors,regardless of age
MSI Testing
~15% of CRCs
Detected by PCR amplification of microsatellite loci in DNA extracted from CRC specimen.
Newer tests-Nuclei acid flourescencelabelling,laser scanning,Flourscence PCR PCR amplification
To identification of risk of hereditary cancer cancer and predict the outcome of CRC.
To detect MLH1 And MSH2 germlinemutation.
Test is PCR based and done on formalin fixed paraffin-
embedded tissues.
Done by Bethesda panel
Sensitivity-55-84% Specificity-90% (PCR)
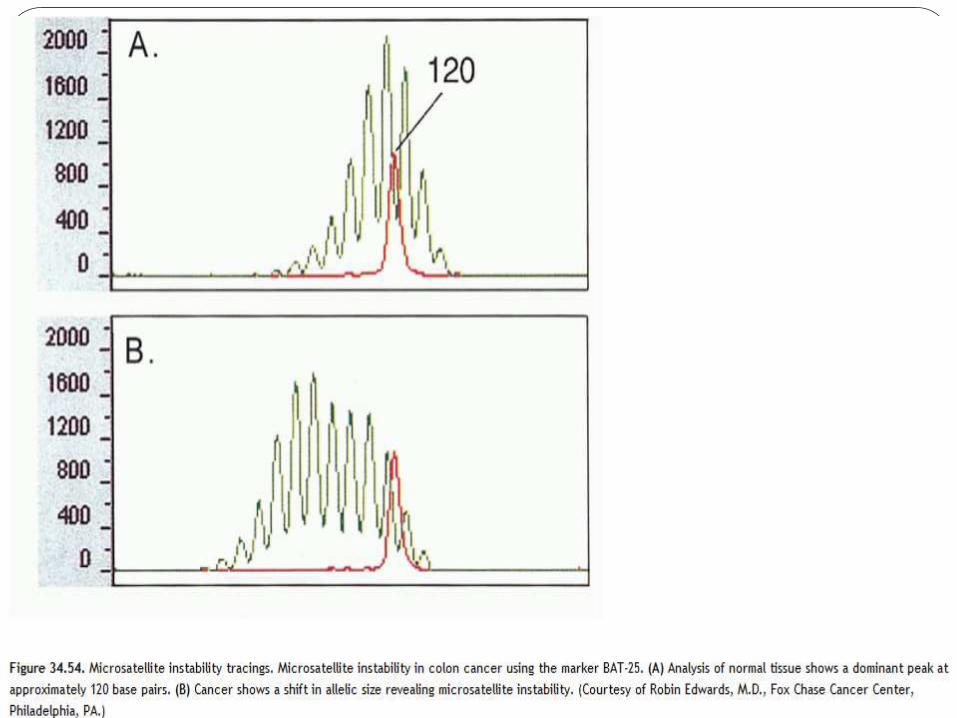
Analyzing two mononucleotide repeats(BAT-25 and BAT-
26) and three dinuleotide repeats(D2S123,D5S346 and
D17S250).
MSI-H-Two or more(>40%) of five microsatellite marker
show instability.
MSI-Low-only one marker show instability
MSS-No marker
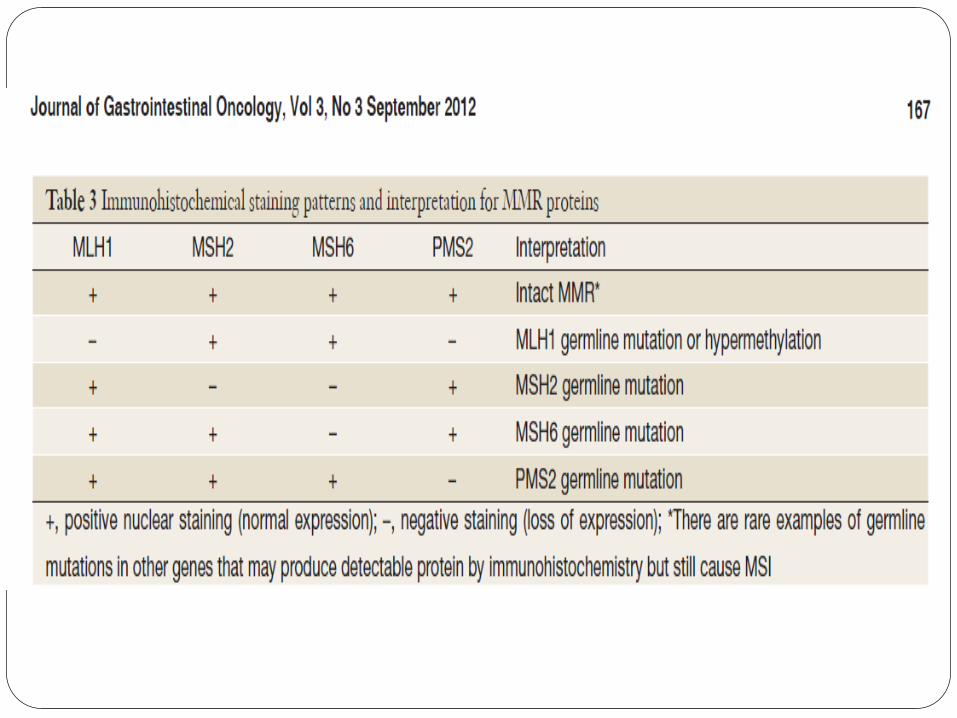
Indirect analysis can be done by IHC stain of MMR
proteins(90%).
Does not discriminate germline from epigenetic and may
miss rare mutation.
M.Fleming et al;J gastro oncol sept 2012:3(3):153-173
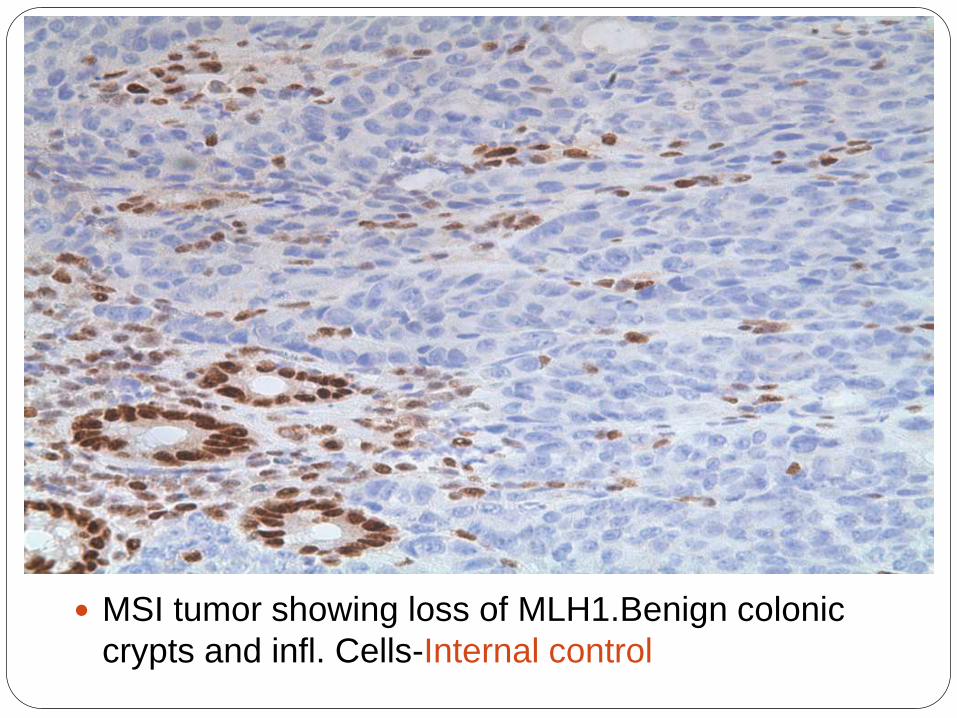
MSI tumor showing loss of MLH1.Benign colonic
crypts and infl. Cells-Internal control
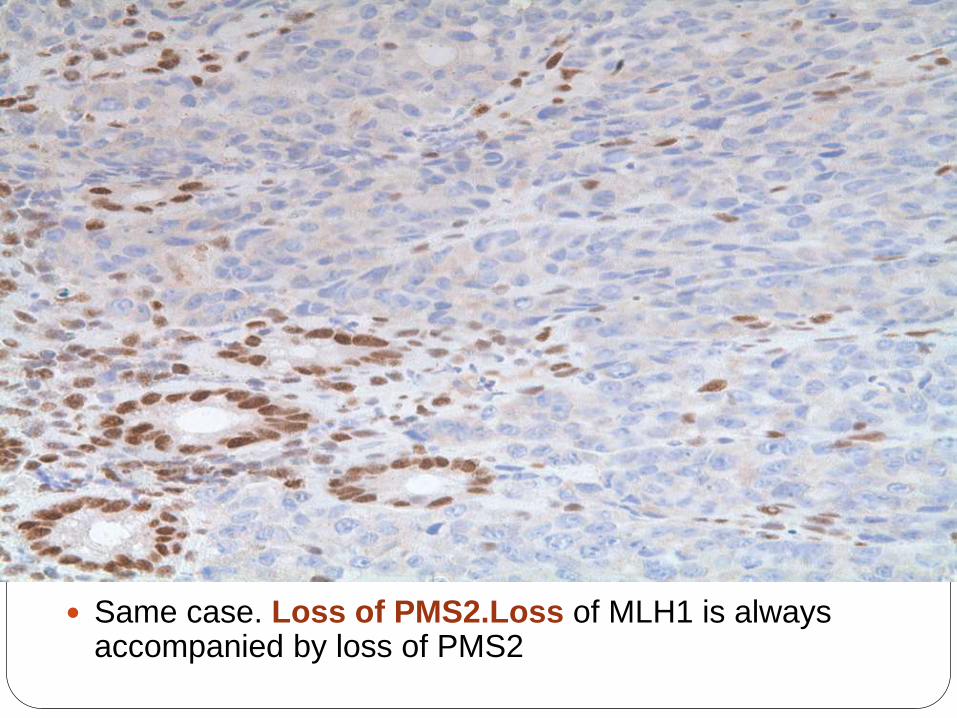
Same case. Loss of PMS2.Loss of MLH1 is always accompanied by loss of PMS2
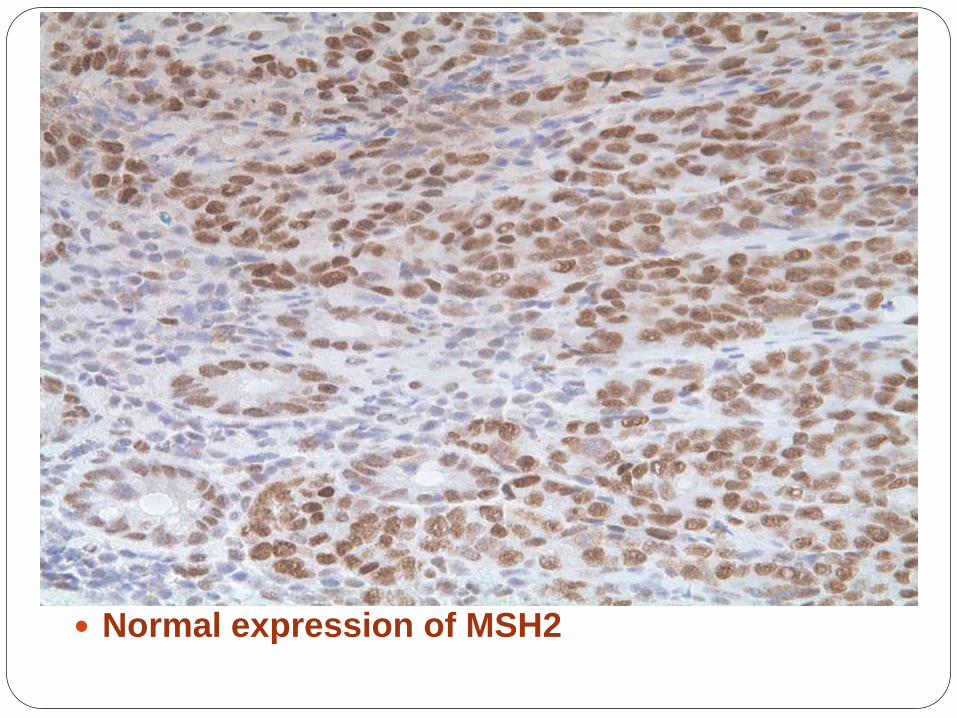
Normal expression of MSH2
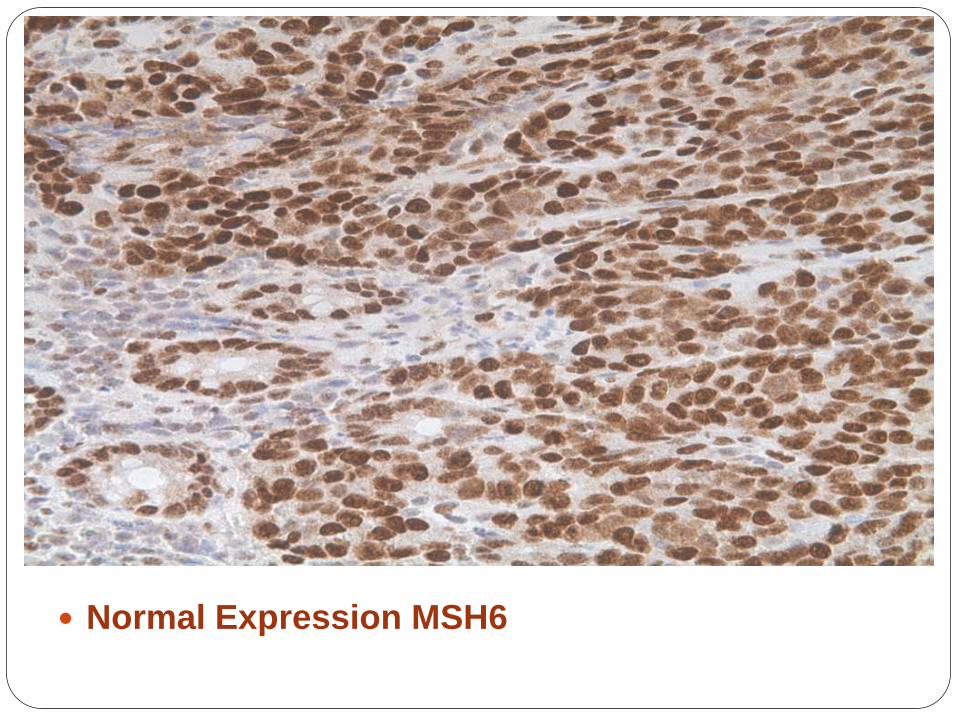
Normal Expression MSH6
MSI testing is done because-
Survival advantage for MSI-H Carcinoma
over MSI-Low and MSI stable cancer.
MSI-H predict poor response to fluorouracil-
based chemotherapy regimens; better
response to irinotectan based chemotherapy
regimen.
M.fleming et al ;J gastointes oncol.Sept 2012;3(3):153-173
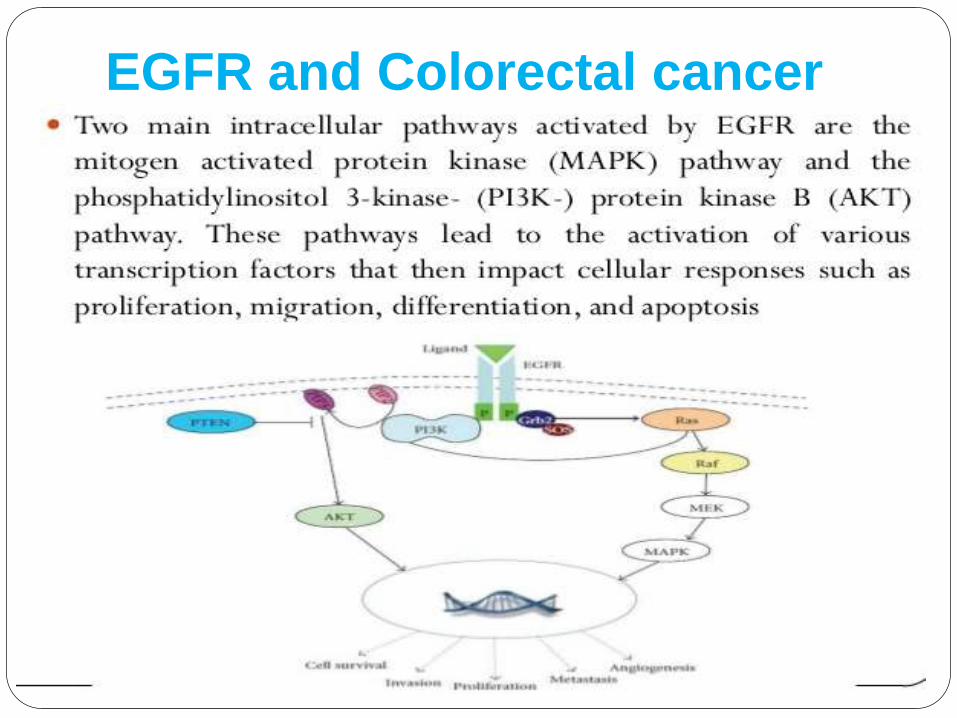
EGFR and Colorectal cancer

EGFR protein Expression
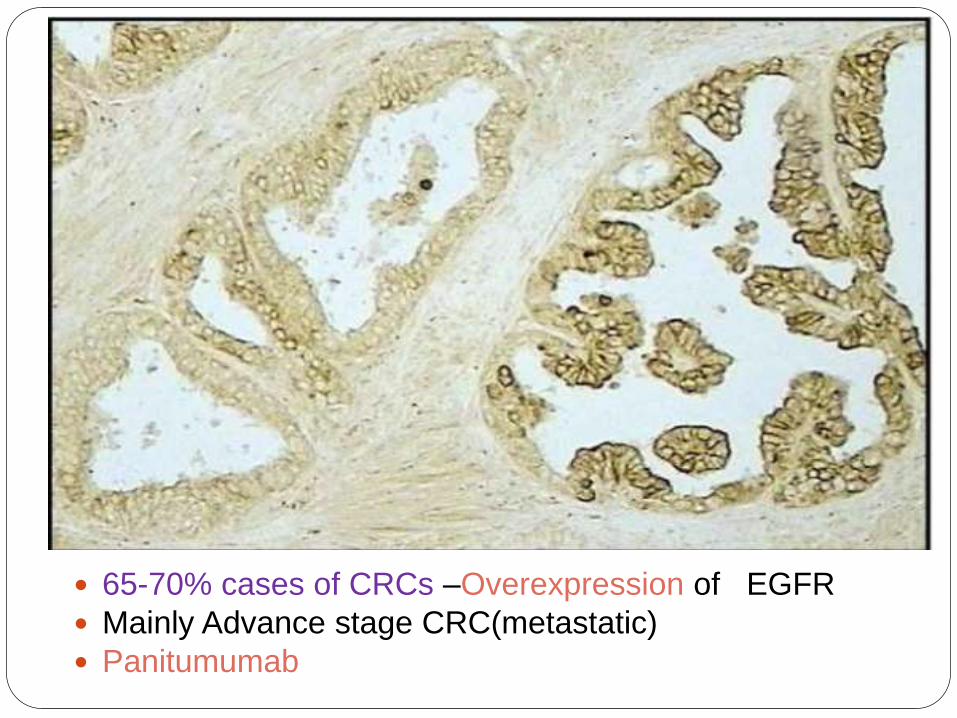
65-70% cases of CRCs –Overexpression of EGFR
Mainly Advance stage CRC(metastatic)
Panitumumab
Clinical Features Asymptomatic for years.
Left Side colonic carcinomas
Occult bleeding
Change n bowel habit
Crampy left lower quadrant discomfort
Right sided colonic carcinomas
Fatigue
Weakness
Iron deficiency anaemia
Fe def. anaemia in an older man means git
cancer until proven otherwise
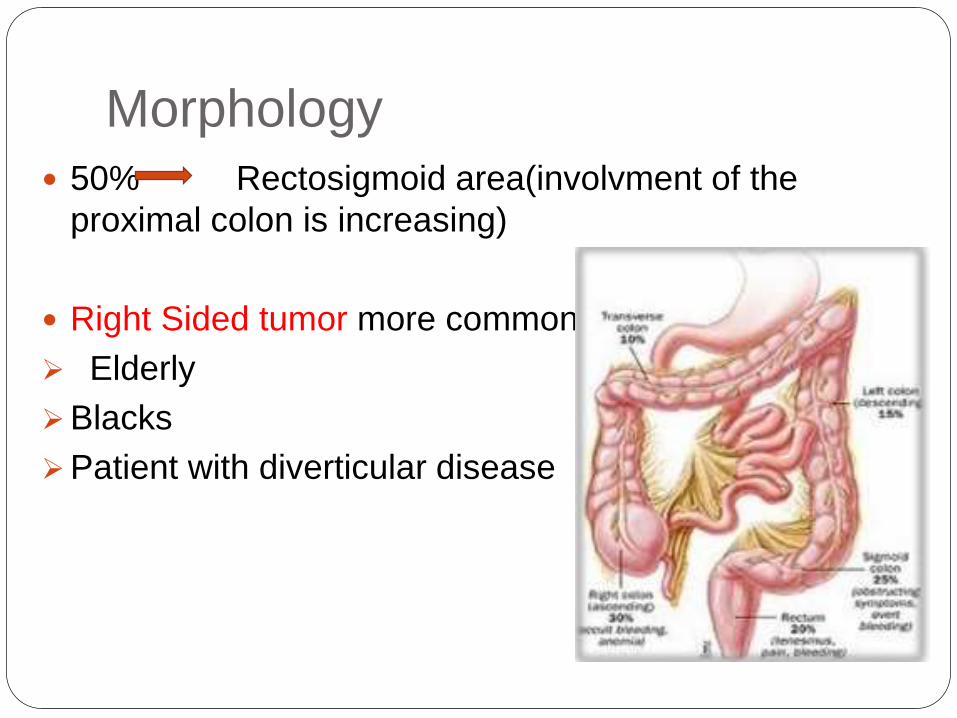
Morphology
50% Rectosigmoid area(involvment of the
proximal colon is increasing)
Right Sided tumor more common in the
Elderly
Blacks
Patient with diverticular disease
Gross A. Proximal colon
Polypoid
Bulky mass, well defined/rolled margin
and a sharp dividing line with the normal
bowel
Ulcerative
Less elevated surface and is centrally
ulcerated
These tumor rarely cause obstruction
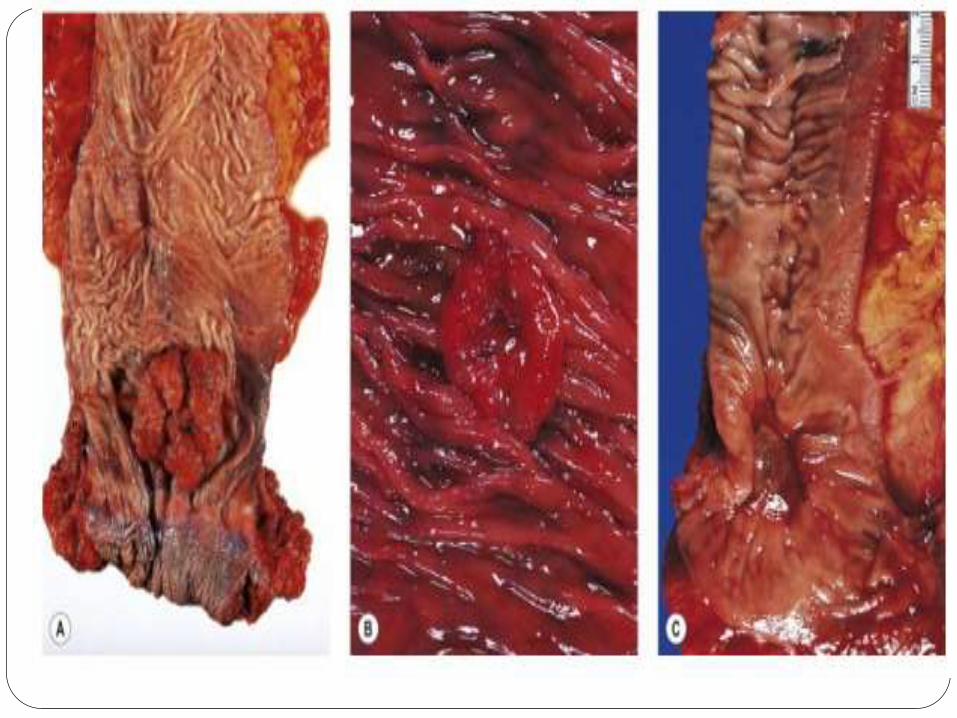
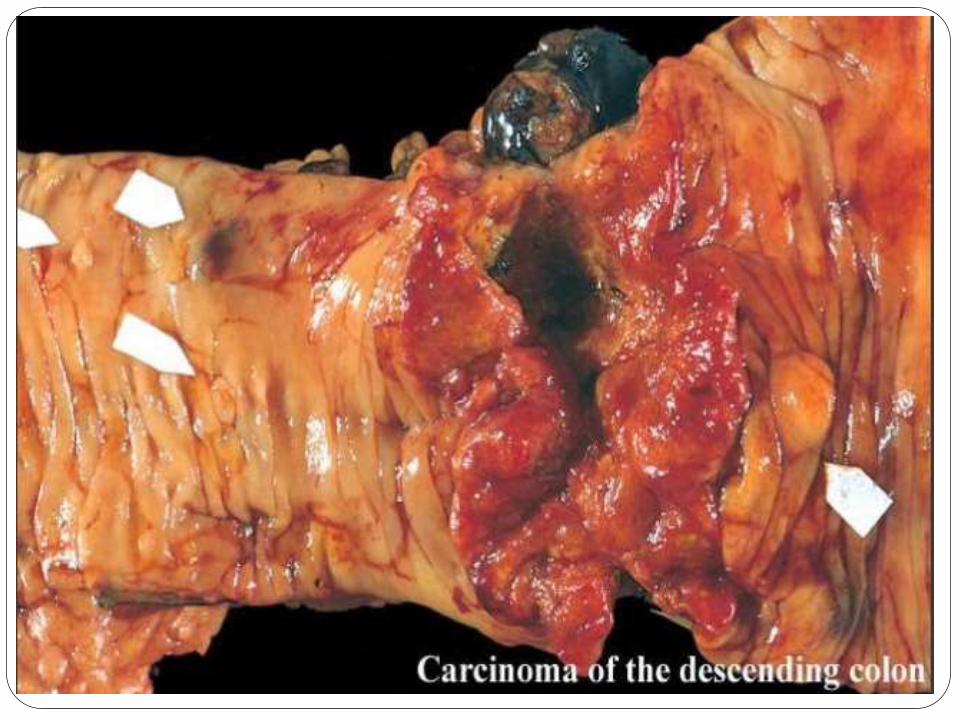
B.Distal Colon
Annular lesion producing
“Napkin-ring” constrictions and
luminal narrowing.
These tumor can cause
obstruction.
MICROSCOPIC Adenocarcinoma
Infiltration of glands of variable differentiation lined by anaplastic
epithelial cells
Lining cells are fully stratified and have large hyperchromatic nuclei
and prominent nucleoli
Prominent mitotic activity often with atypical forms
Invasion promotes a characteristic robust desmoplastic tissue
reaction and necrosis.
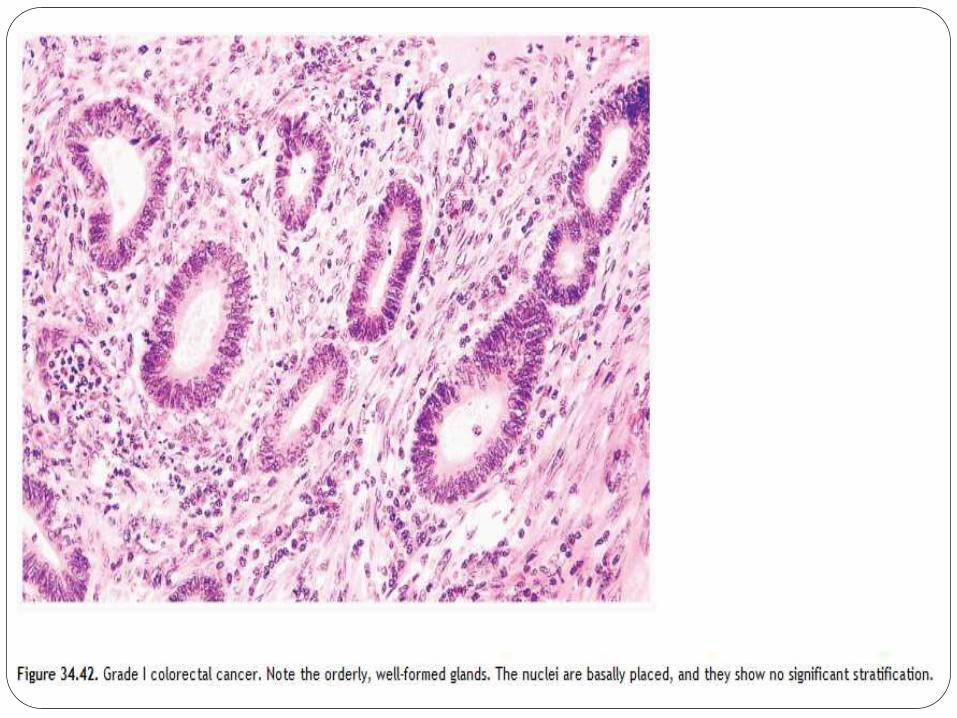
---Grade I
◆ Composed predominantly of well-formed glands
in a desmoplastic stroma
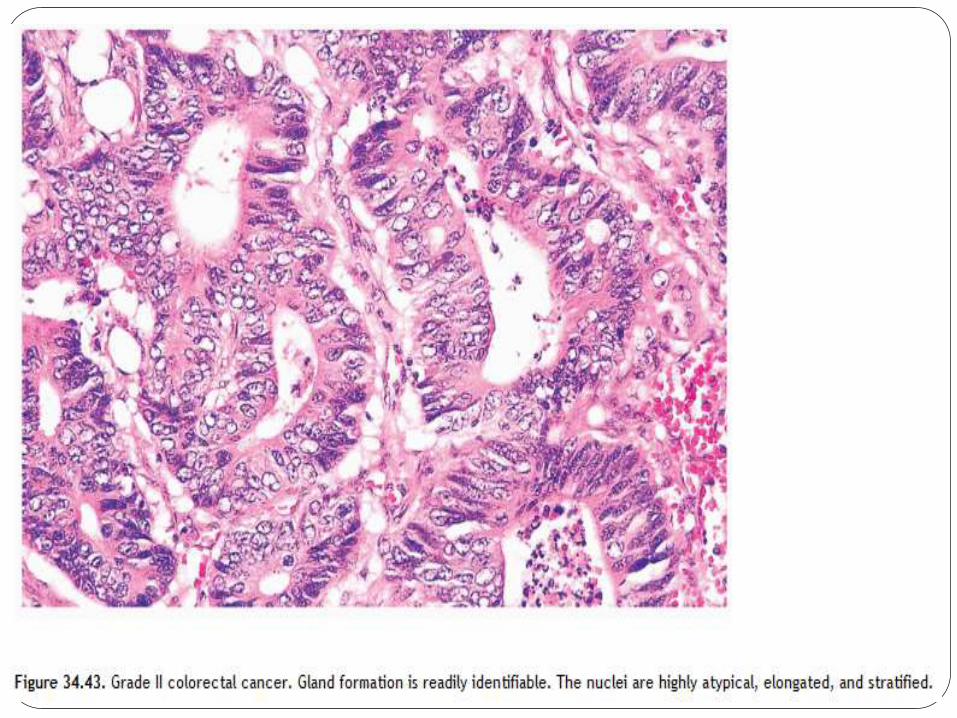
— Grade II
◆ Less well-formed glands with focal cribriform
architecture
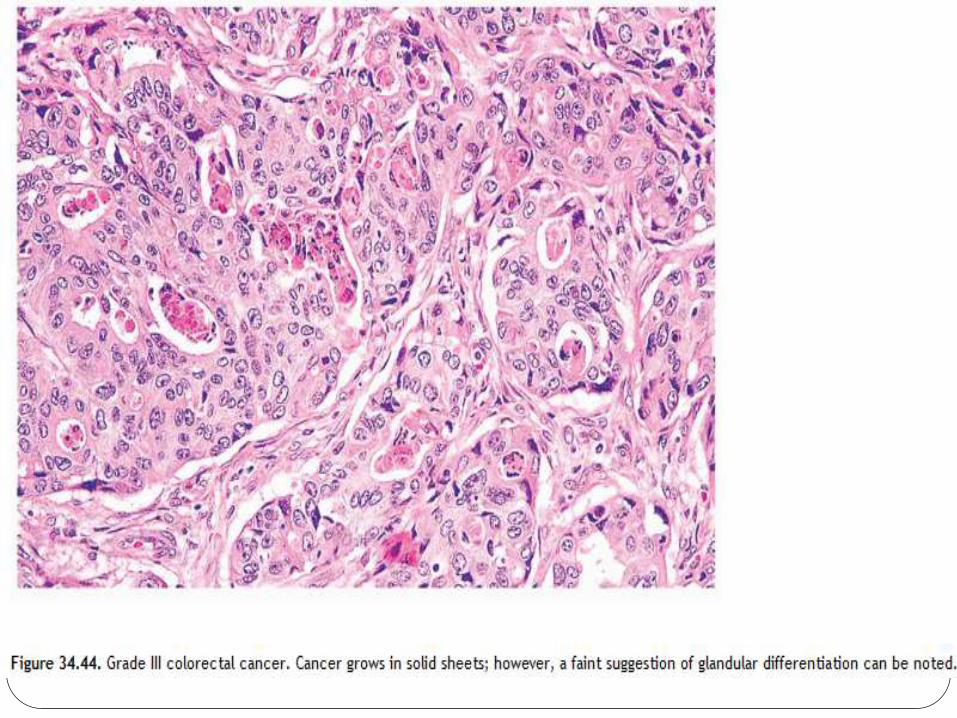
— Grade III
◆ Tumor grows in solid sheets with no distinct
gland formation
Well diferentiated->95%
gland forming
Moderately differntiated-
50-95%
Poorly differntiated-
<50%
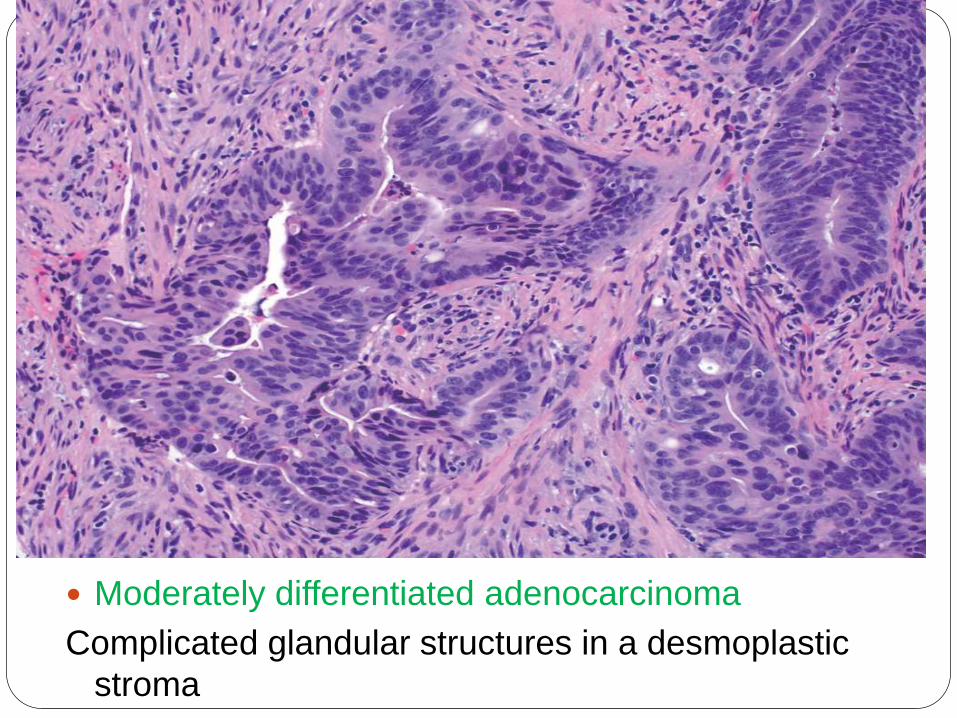
Moderately differentiated adenocarcinoma
Complicated glandular structures in a desmoplastic
stroma
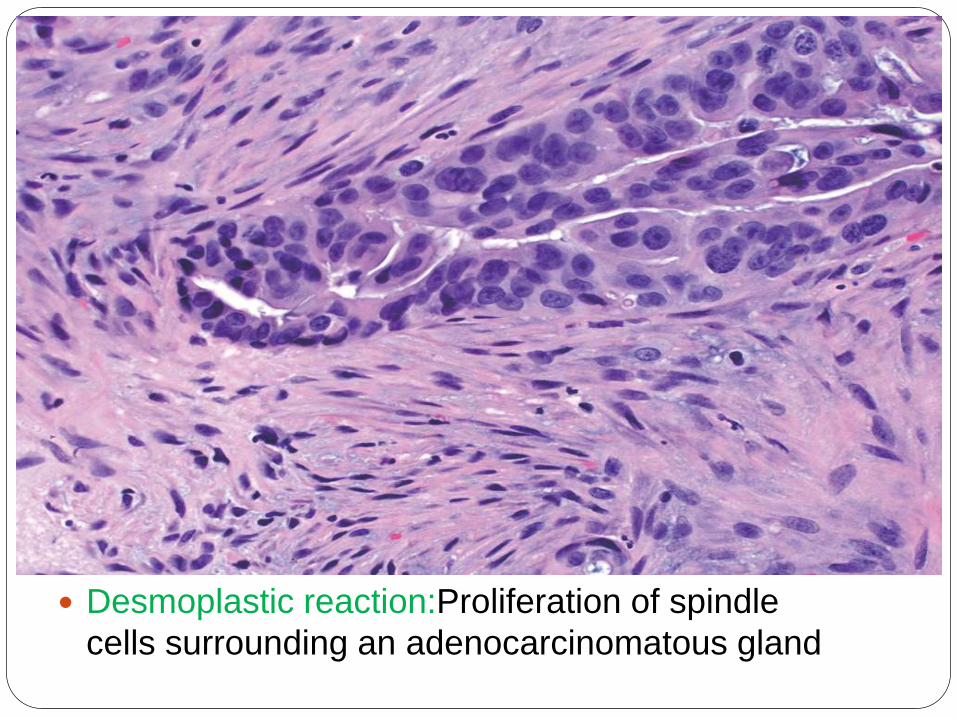
Desmoplastic reaction:Proliferation of spindle
cells surrounding an adenocarcinomatous gland

Necrotic debris (“dirty necrosis”) within the lumina
of adenocarcinomatous glands
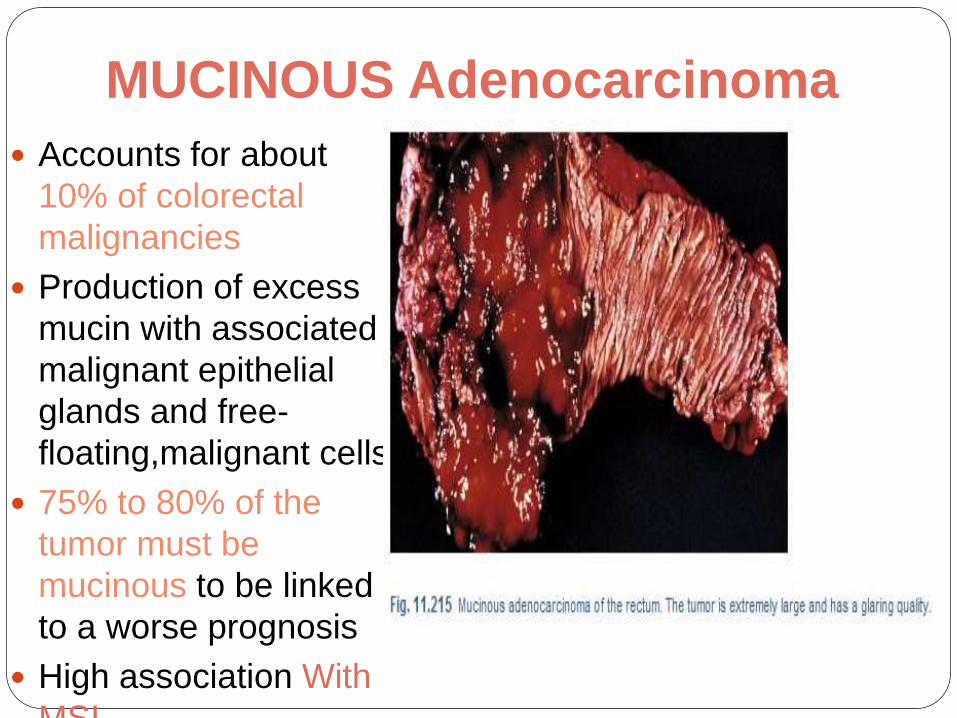
MUCINOUS Adenocarcinoma
Accounts for about
10% of colorectal
malignancies
Production of excess
mucin with associated
malignant epithelial
glands and free-
floating,malignant cells
75% to 80% of the
tumor must be
mucinous to be linked
to a worse prognosis
High association With
MSI.
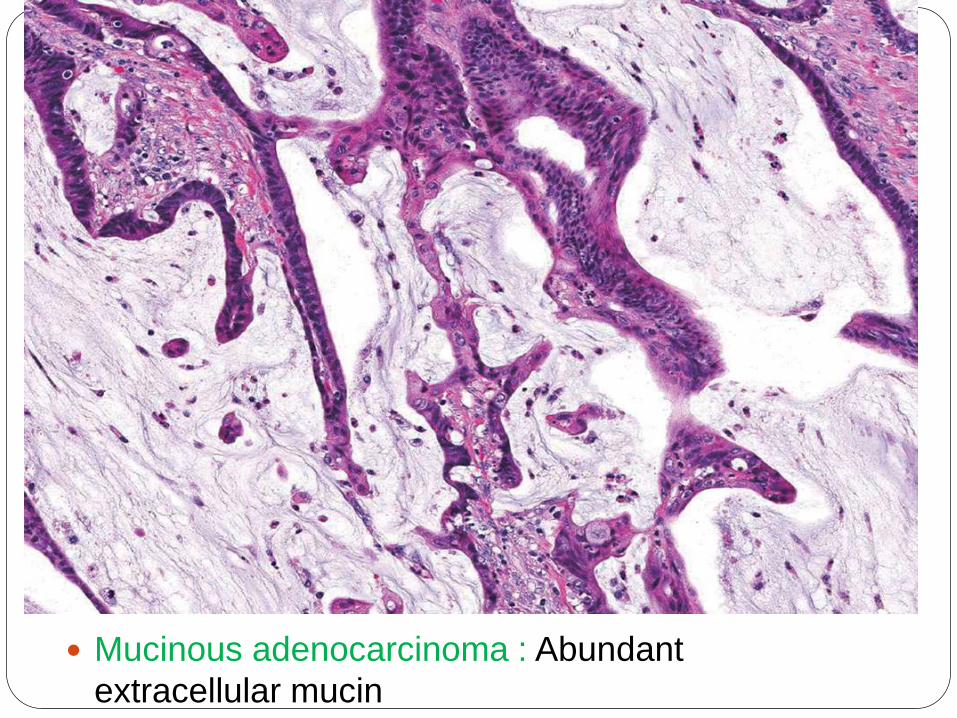
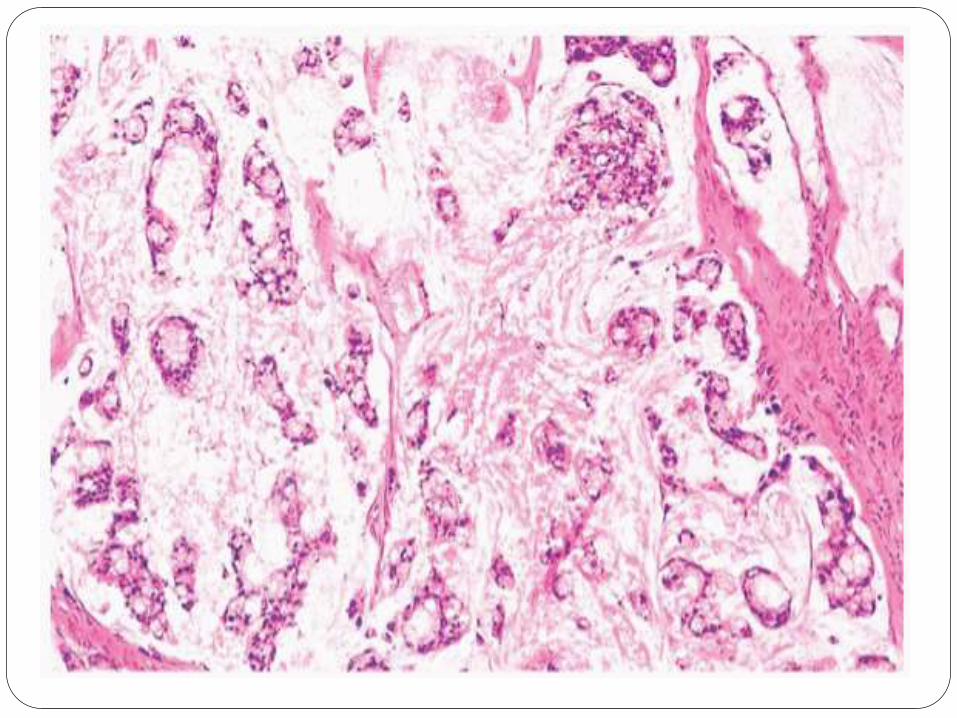
Mucinous adenocarcinoma : Abundant
extracellular mucin

Mucinous adenocarcinoma with signet-ring cells
and extracellular mucin pools.
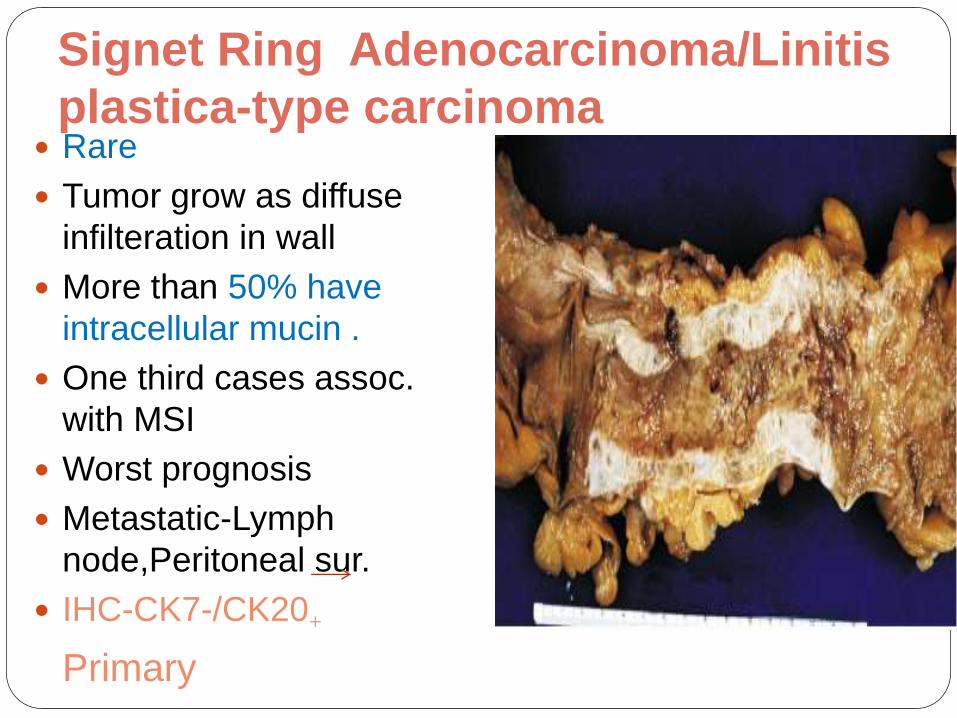
Signet Ring Adenocarcinoma/Linitis
plastica-type carcinoma Rare
Tumor grow as diffuse
infilteration in wall
More than 50% have
intracellular mucin .
One third cases assoc.
with MSI
Worst prognosis
Metastatic-Lymph
node,Peritoneal sur.
IHC-CK7-/CK20+
Primary
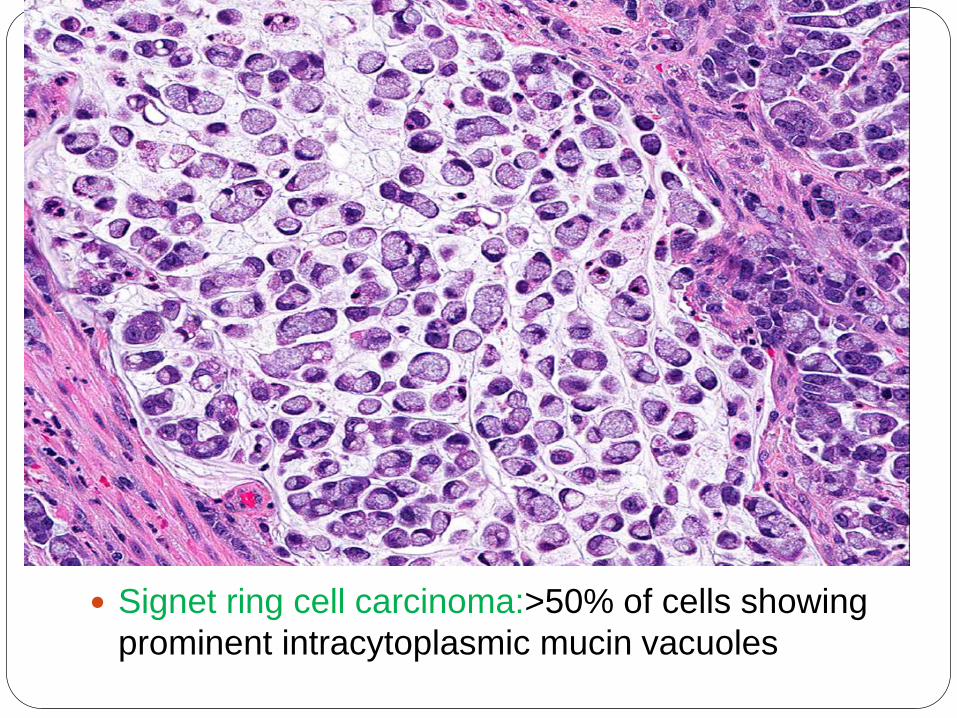
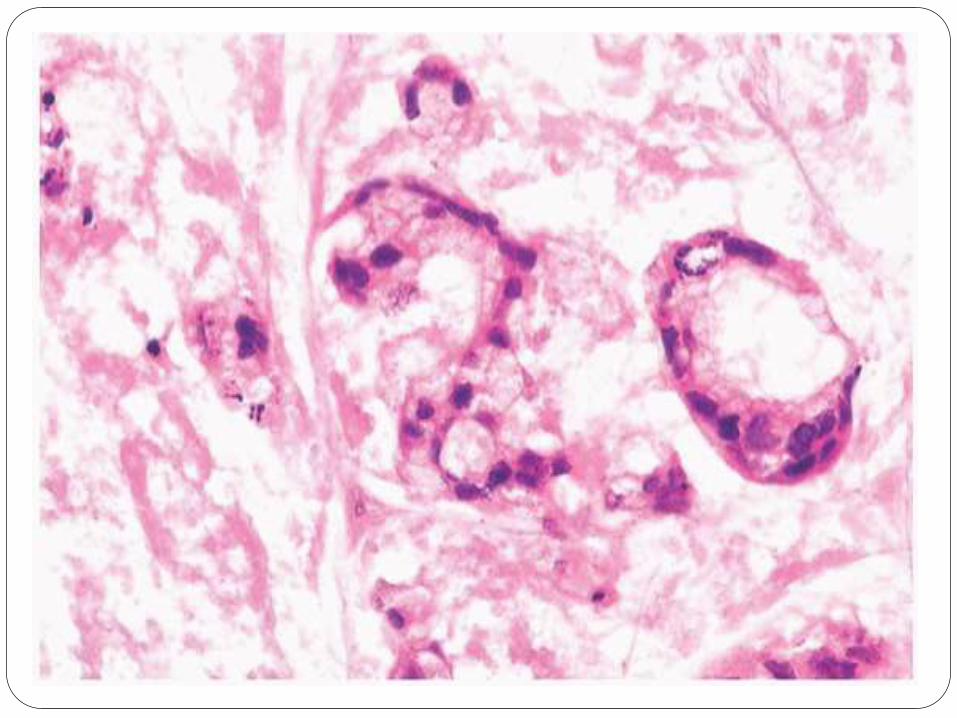
Signet ring cell carcinoma:>50% of cells showing
prominent intracytoplasmic mucin vacuoles
MEDULLARY carcinoma Rare
Common in Proximal colon
Female Prdominance
Tumor cells have eosinophilic or
amphophilic cytoplasm with rounded nuclei
with prominent nucleoli
Closely packed, trabecular or solid patterns
Invariably associated with MSI
Good prognosis
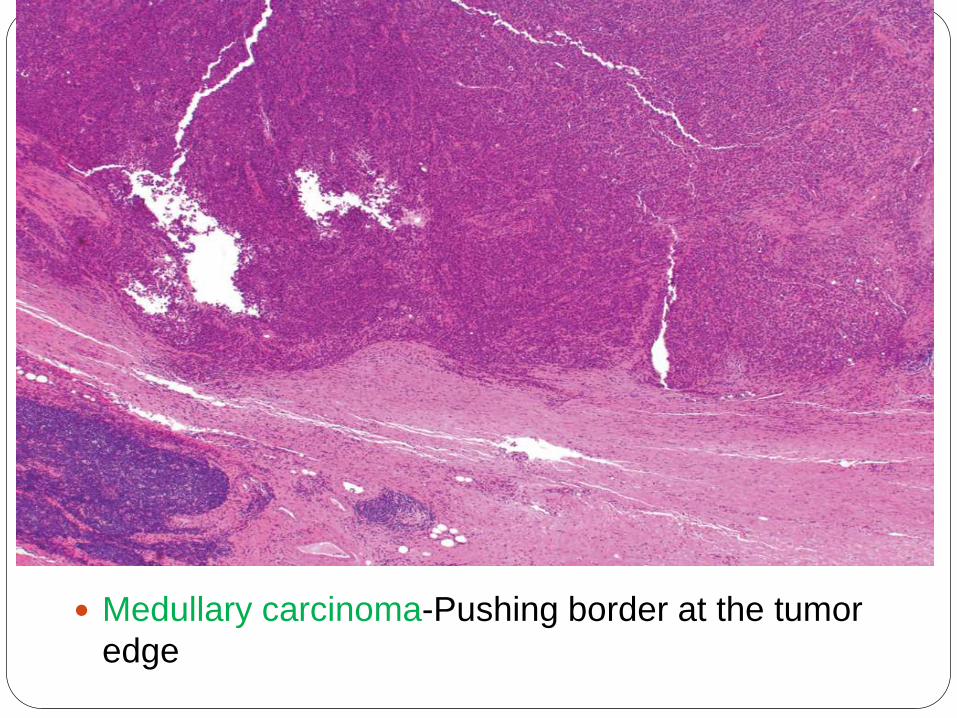
Medullary carcinoma-Pushing border at the tumor
edge
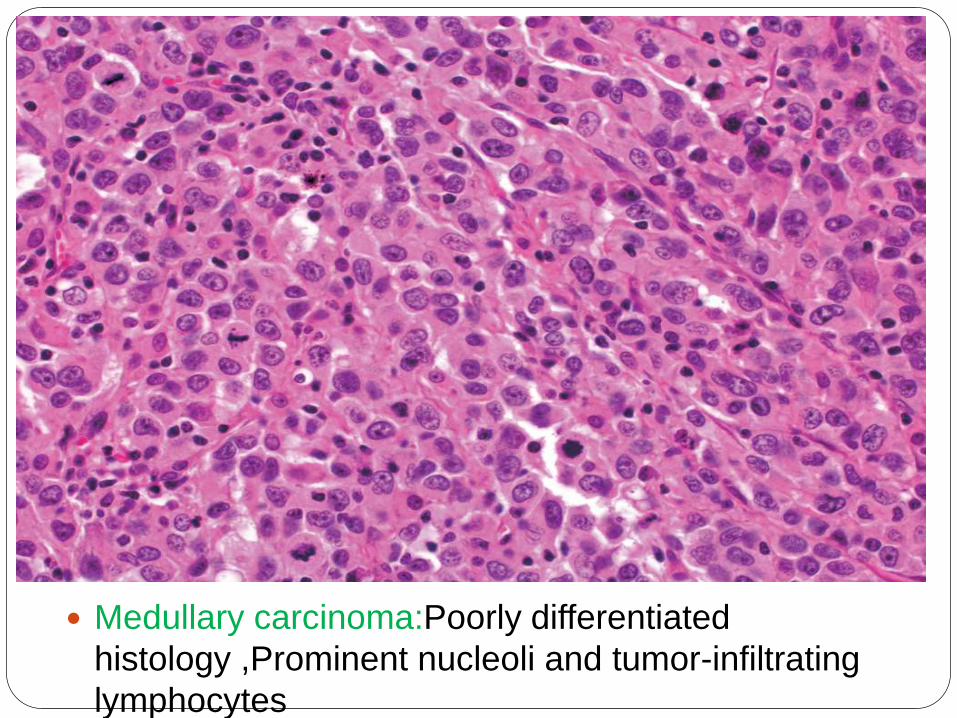
Medullary carcinoma:Poorly differentiated
histology ,Prominent nucleoli and tumor-infiltrating
lymphocytes
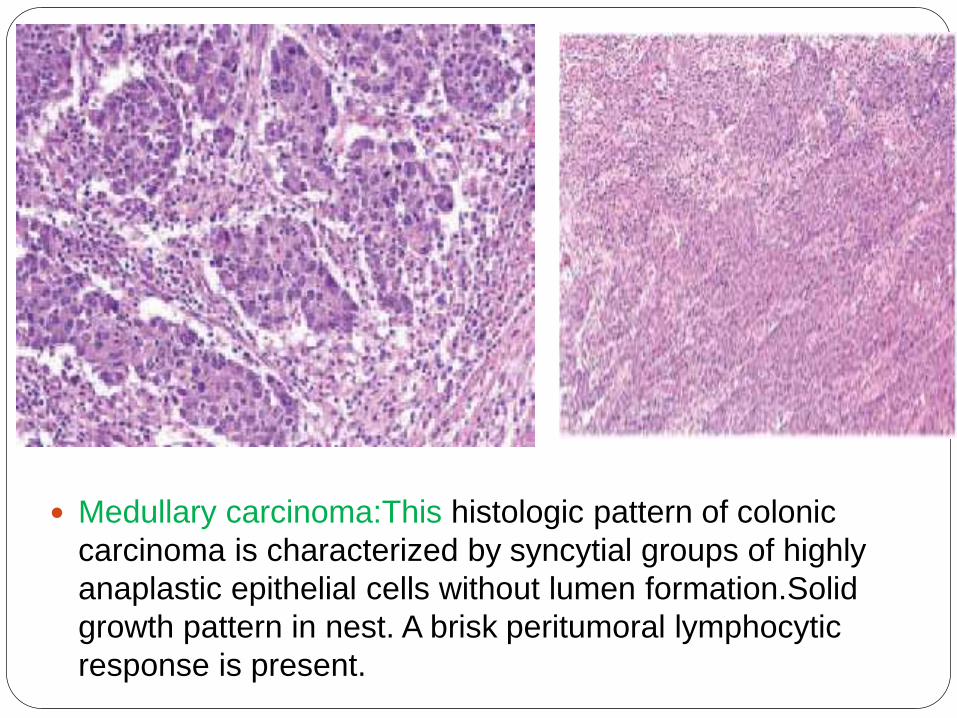
Medullary carcinoma:This histologic pattern of colonic
carcinoma is characterized by syncytial groups of highly
anaplastic epithelial cells without lumen formation.Solid
growth pattern in nest. A brisk peritumoral lymphocytic
response is present.
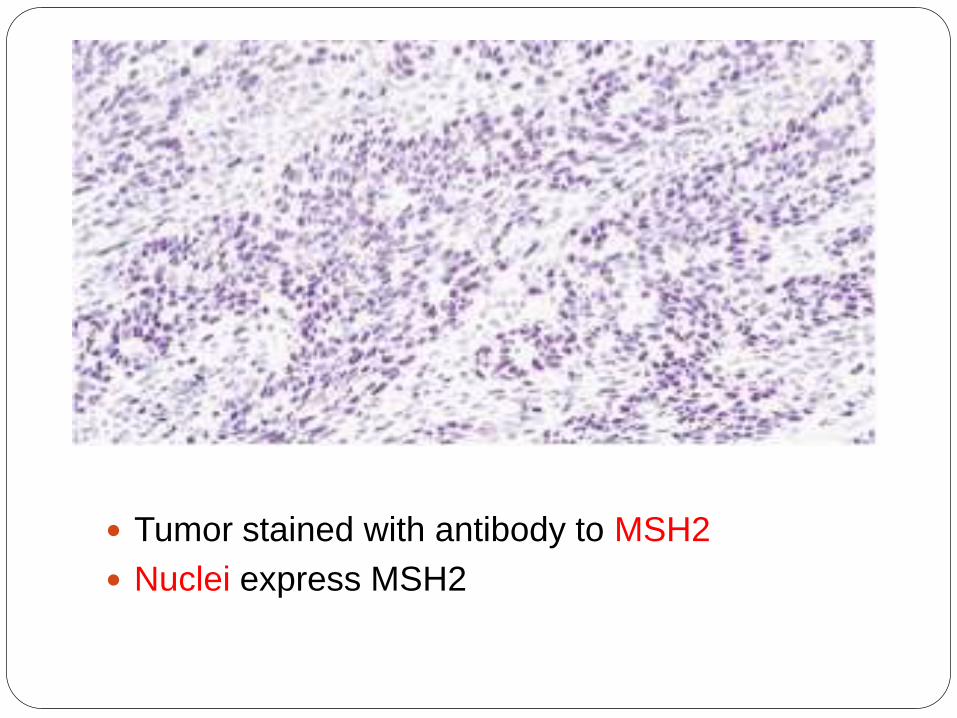
Tumor stained with antibody to MSH2
Nuclei express MSH2
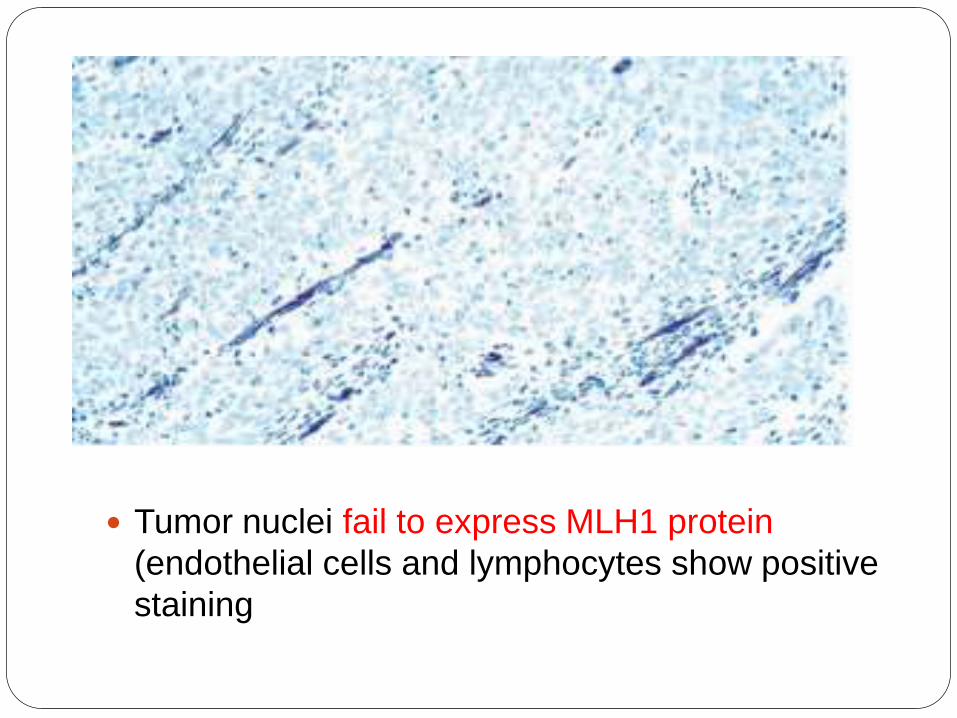
Tumor nuclei fail to express MLH1 protein
(endothelial cells and lymphocytes show positive
staining
SERRATED Adenocarcinoma
Newly described entity
7.5% of all CRC and 17.5% of proximal carcinoma
Common in proximal colon
Derived from serrated adenoma
MICROSCOPIC
Serrated, Mucinous or Trabecular pattern of growth
Abundant eosinophillic cytoplasm,Vesicularnuclei and Prominent nucleoli
Preseved polarity
No necrosis
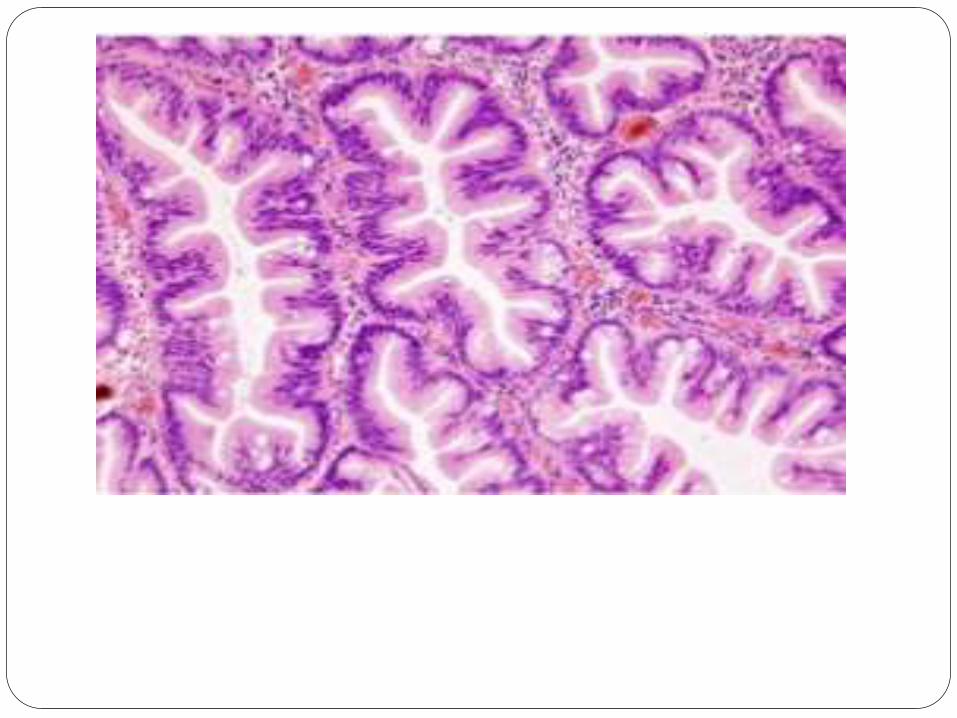
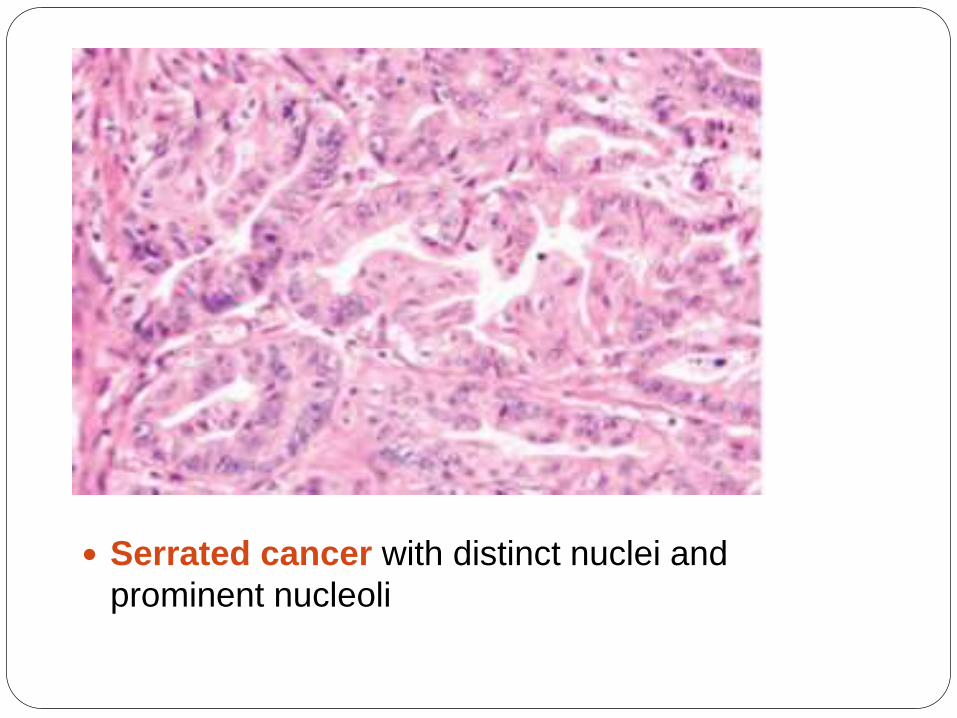
Serrated cancer with distinct nuclei and
prominent nucleoli
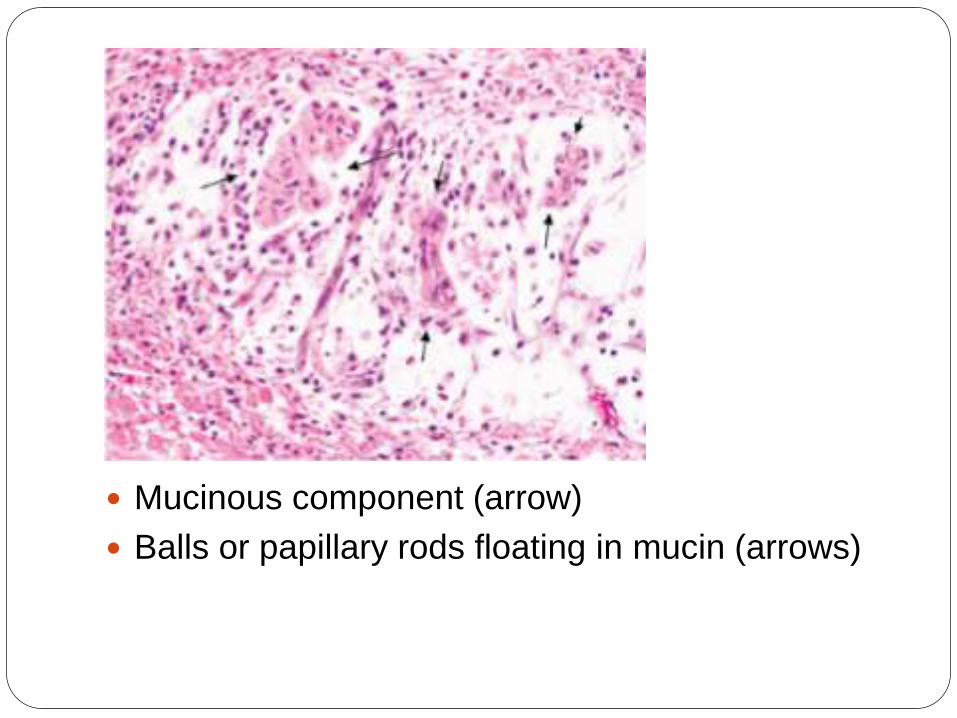
Mucinous component (arrow)
Balls or papillary rods floating in mucin (arrows)
SQUAMOUS Differentiation
Common in Proximal colon.
Usually associated with glandular
elements(adenosquamous
carcinoma)
Occasionally seen in pure
form(squamous cell carcinoma)
Evidence of Human Papilloma virus
16 involvement in the pathogenesis
of some rectal cases.
IMMUNOHISTOCHEMICAL
Features Conventional Adenocarcinoma of colon
express MUC1 and MUC3
Mucinous carcinoma express MUC2
CRCs invariably positive for
cytokeratin(CK)-positive for CK20 and
negative for CK7.-Primary
Positive for CEA
Poitive for CDX2,in majority of CRCs.
Tumor associated glycoprotein(TAG-72) is
present in 100% of invasive colorectal
carcinoma.
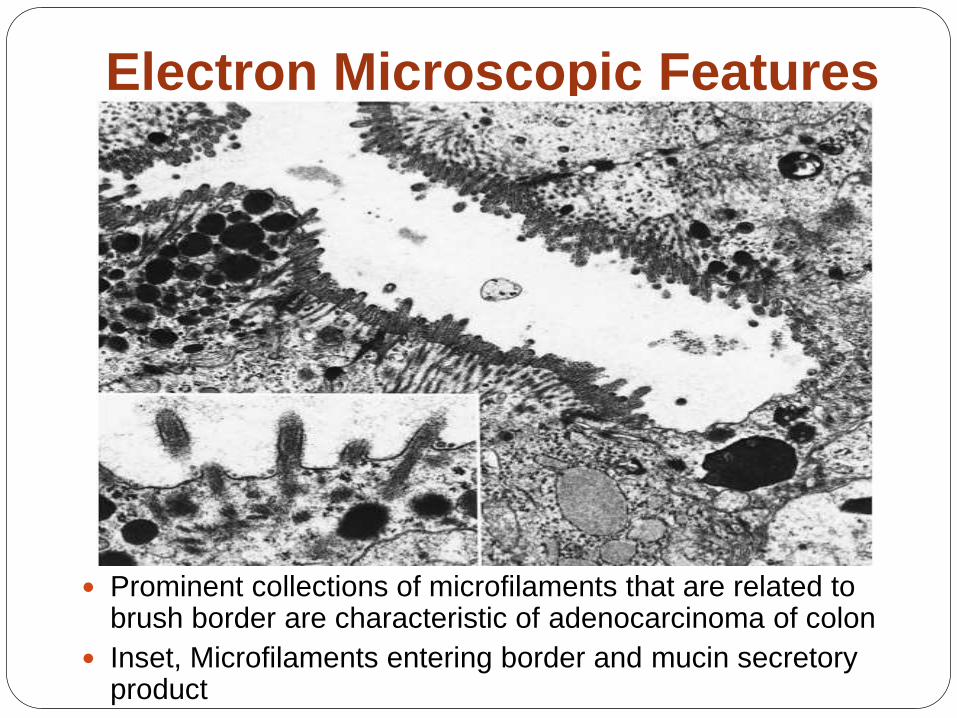
Electron Microscopic Features
Prominent collections of microfilaments that are related to brush border are characteristic of adenocarcinoma of colon
Inset, Microfilaments entering border and mucin secretoryproduct
DIAGNOSTIC MODALITIES
CYTOLOGY
Its an accurate way of diagnosing CRC.
Little Practical value
Low-lying rectal lesions can be easily
sampled.
Brush cytology can also be performed
via the fiberoptic scope.
It is a sensitive technique , perhaps
even more so than than endoscopic
biopsy,but it has not yet found
widespread acceptance.
BIOPSY
There is a need of POSITIVE BIOPSY
before radical urgery for CRC.
In large lesions, several biopsies should
be taken from diverse areas.
Biopsy from center—Only granulation
tissue
Biopsy from the very Periphery—Only
hyperplastic colonic epithelium
VARIOUS SCREENING
MODALITIES
Colonoscopy
Virtual Colonoscopy
Sigmoidoscopy
Fecal occult blood test
Double contrast barium enema
Digital rectal examination
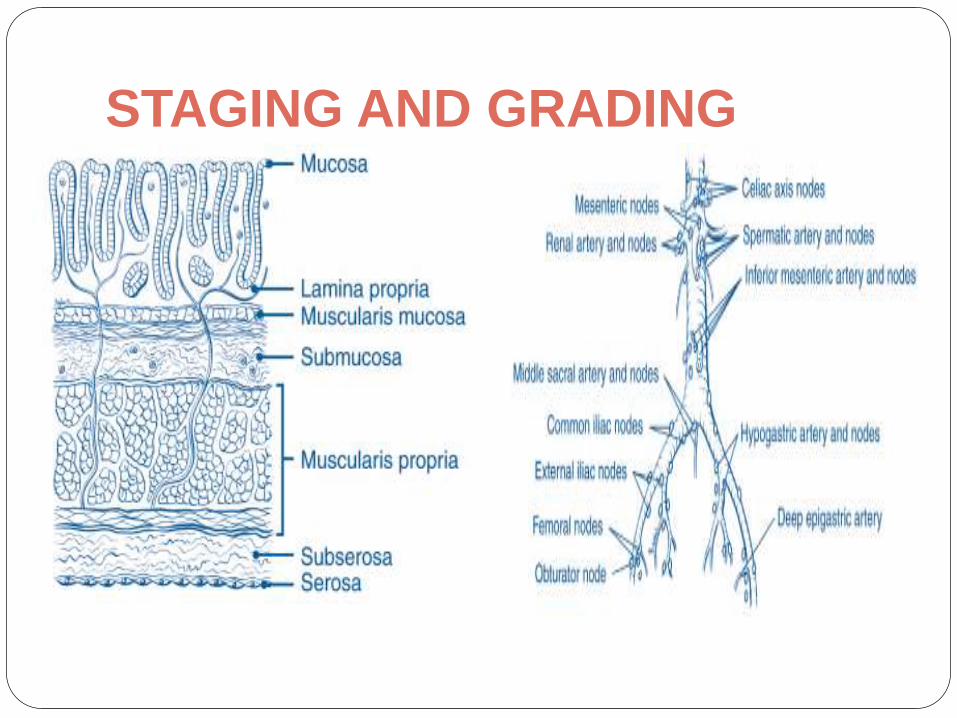
STAGING AND GRADING
STAGING AND GRADING
In 1937, DUKES proposed staging for
rectal carcinoma
In 1954, Astler and Coller proposed
different staging system
American joint committee on
Cancer(AJCC)
The union Internationale Countre Le
Cancer(UJCC)
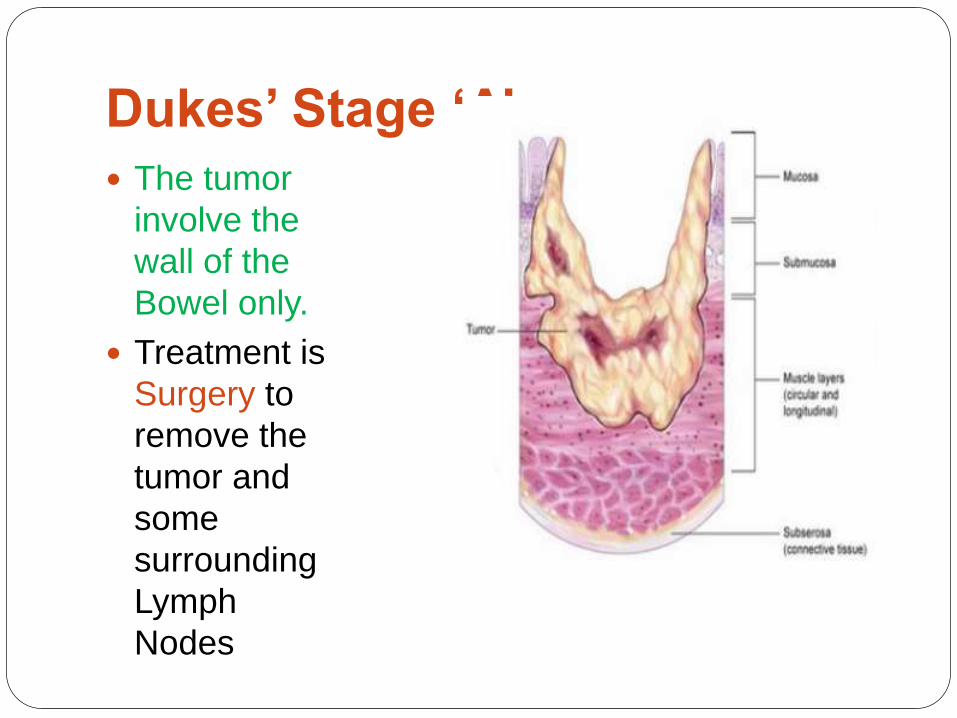
Dukes’ Stage ‘A’
The tumor
involve the
wall of the
Bowel only.
Treatment is
Surgery to
remove the
tumor and
some
surrounding
Lymph
Nodes
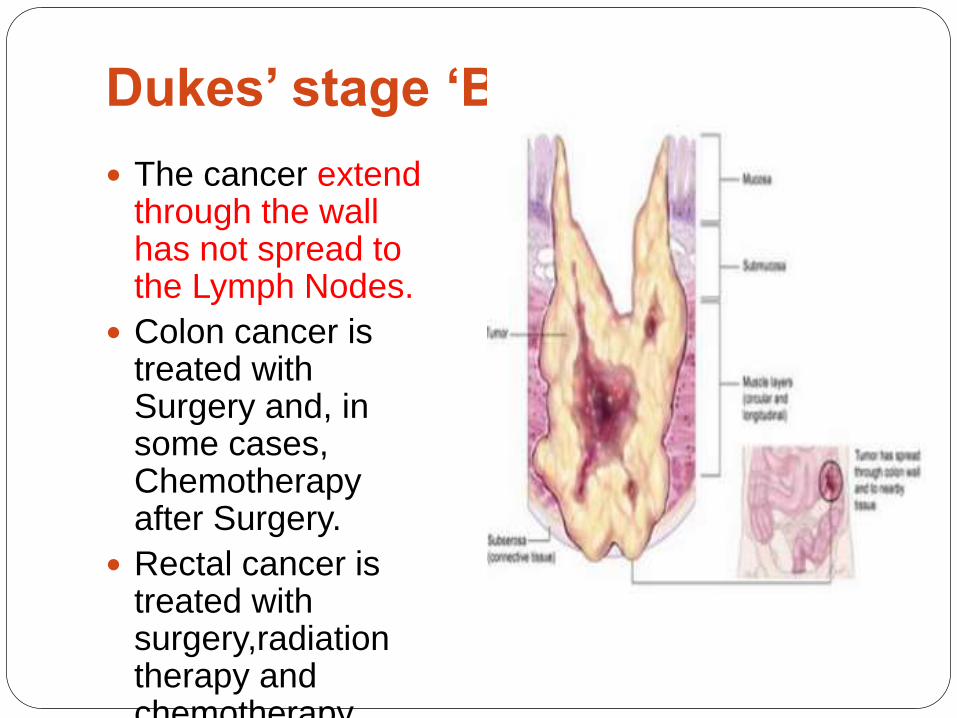
Dukes’ stage ‘B’
The cancer extend through the wall has not spread to the Lymph Nodes.
Colon cancer is treated with Surgery and, in some cases, Chemotherapy after Surgery.
Rectal cancer is treated with surgery,radiationtherapy and chemotherapy
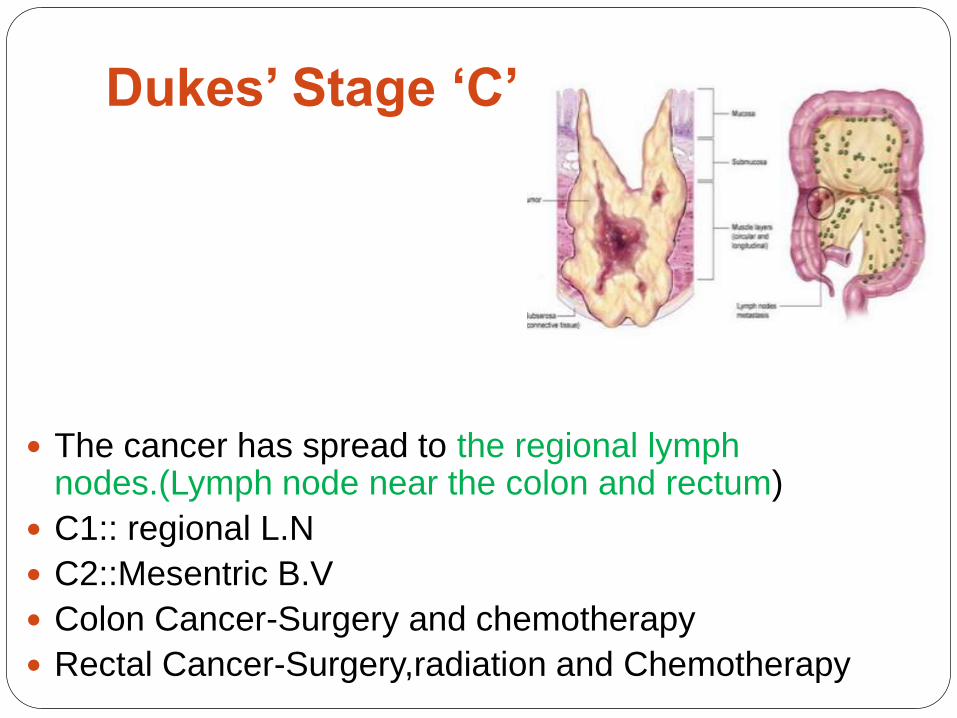
Dukes’ Stage ‘C’
The cancer has spread to the regional lymph nodes.(Lymph node near the colon and rectum)
C1:: regional L.N
C2::Mesentric B.V
Colon Cancer-Surgery and chemotherapy
Rectal Cancer-Surgery,radiation and Chemotherapy
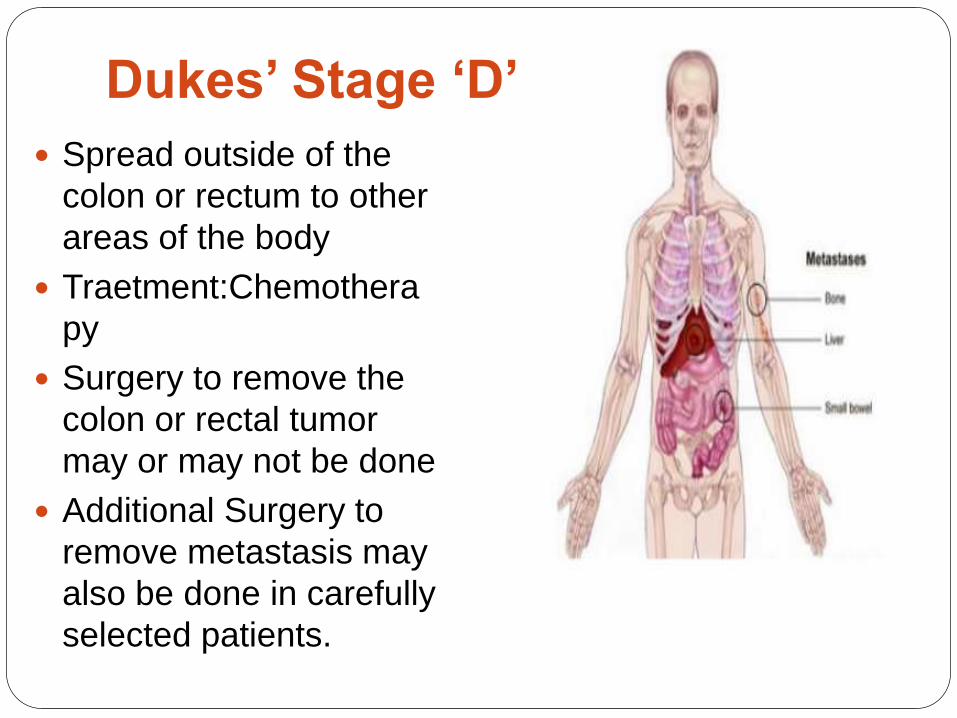
Dukes’ Stage ‘D’
Spread outside of the
colon or rectum to other
areas of the body
Traetment:Chemothera
py
Surgery to remove the
colon or rectal tumor
may or may not be done
Additional Surgery to
remove metastasis may
also be done in carefully
selected patients.
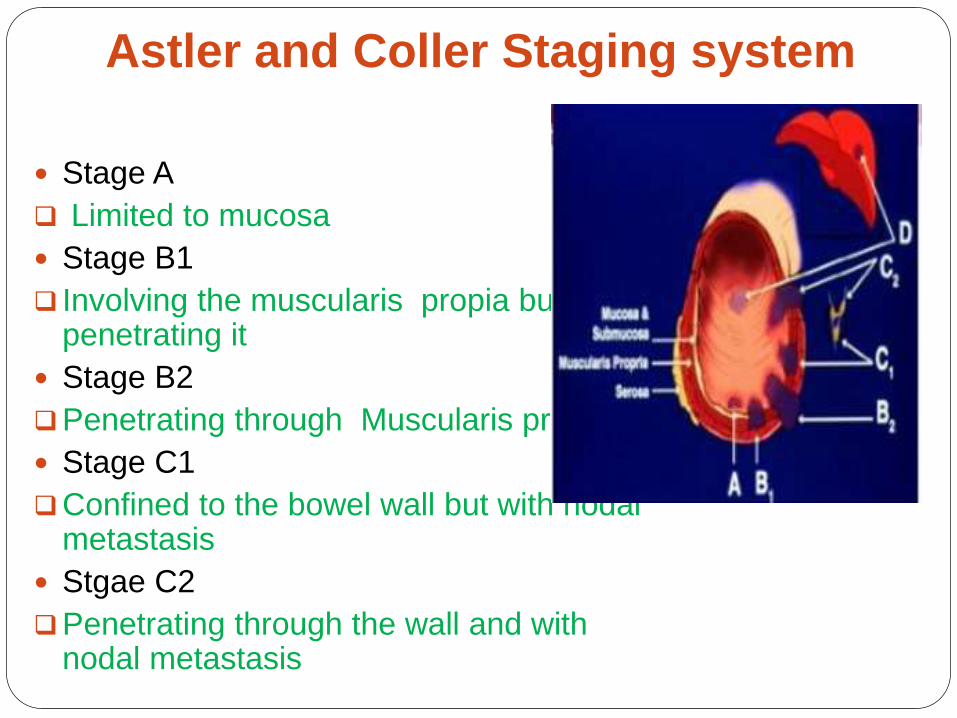
Astler and Coller Staging system
Stage A
Limited to mucosa
Stage B1
Involving the muscularis propia but not penetrating it
Stage B2
Penetrating through Muscularis propia
Stage C1
Confined to the bowel wall but with nodal metastasis
Stgae C2
Penetrating through the wall and with nodal metastasis
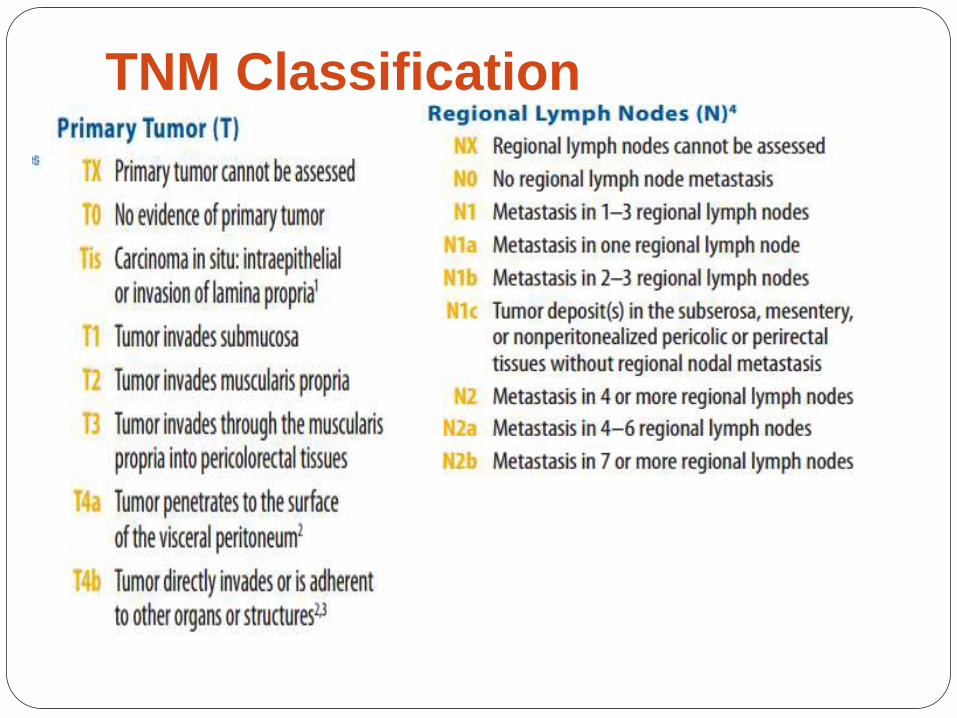
TNM Classification
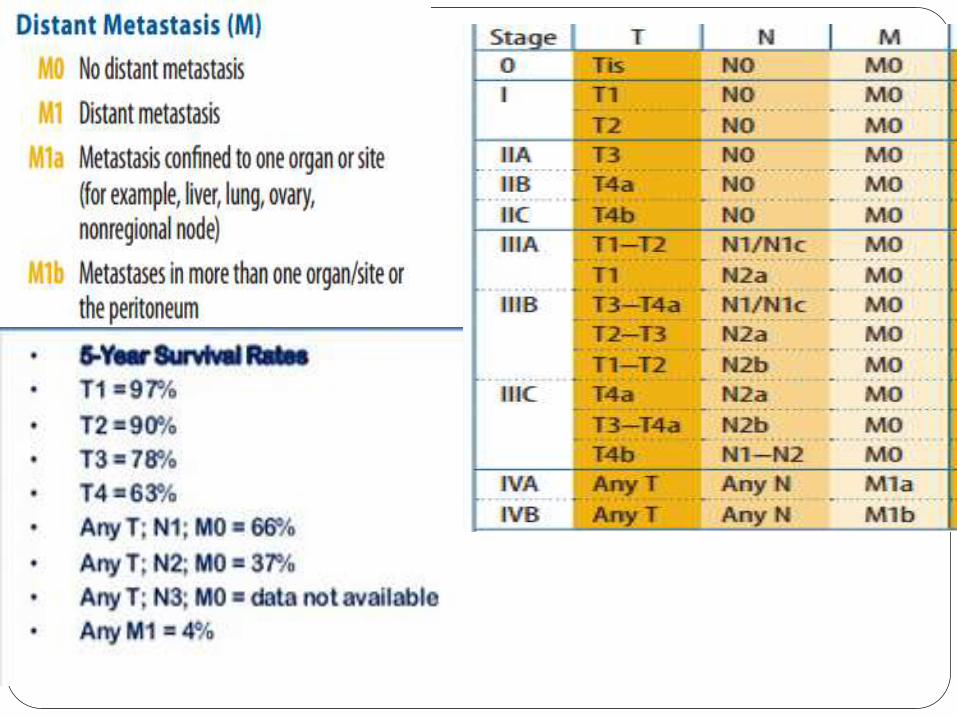
Spread and Metastasis
Common site
Regional lymph nodes
Liver
Other relative common site –
Peritoneum,Lung,Ovaries
Minimum no. of nodes recovered from a
surgical specimen of colorectal carcinoma
should be 14 or 15.
Liver Metastasis-More common in the tumor
showing evidence of blood vessels invasion.

Treatment
Chemotherapy
Radiotherapy
Photodynamic Therapy
Radical Surgery
Gene Therapy
Immunotherapy-Cetuximab (anti-
EGFR)-use in colon cancer
Prognosis The 5 year survival rate after curative
resection for CRC range between 40% and
60%.
Local recurrence and/or regional lymph
node metastasis occur in over 90% of the
faliure cases.
Over two-thirds of the recurrences are
evident within the first 2 year and 91% by 5
years.
The prognosis of colorectal carcinoma is
related to a number of clinical and
pathologic parameters.
Prognosis
Stage III cancers treated with a fluorouracil
adjuvant regimen, MSS cancers with loss
of heterozygosity of 18q –Worse survival
MSI-H cancers have been associated with
improved 5-year survival compared with
MSS and MSI-L cancers .
THANK YOU
To download this Presentation use following gmail
address
User id- [email protected]
Password- pathseminar14





























