Embed Size (px)
Citation preview
Definition of psychiatric disorderHistory. Classification. Prevalence. Comorbidity. Epidemiology.
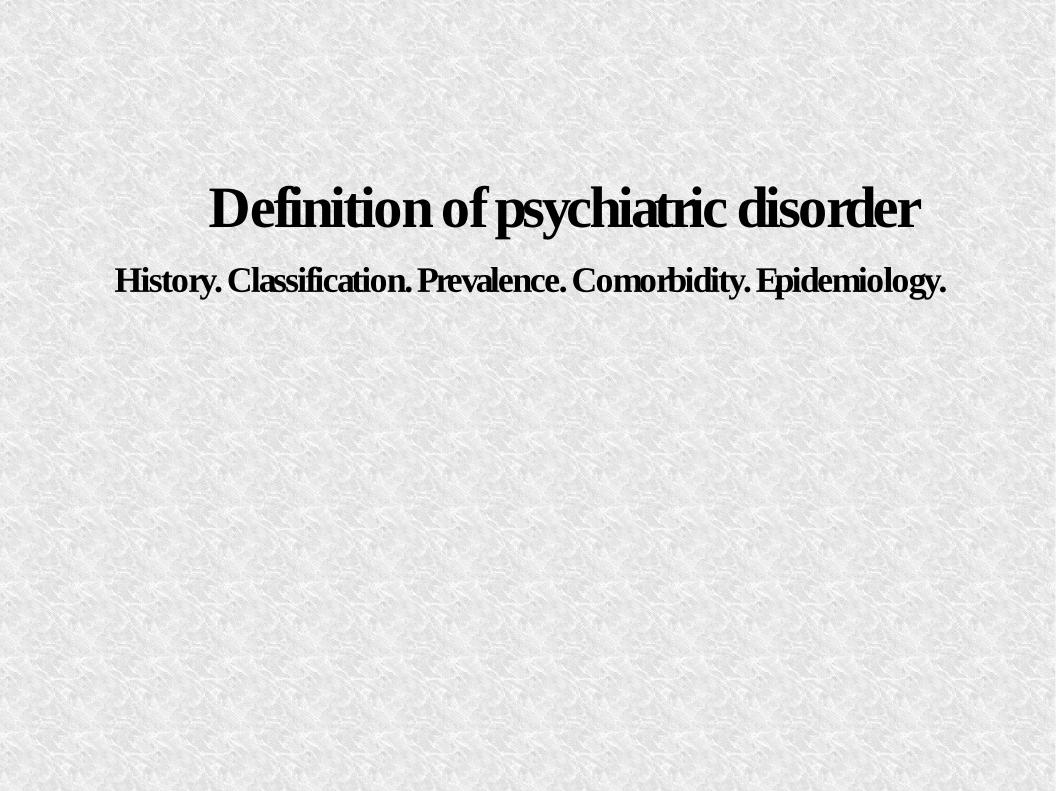
DefinitionDSM criteria of abnormal behavior: “A behavior is considered as abnormal if it is statistically rare, deviates from society's unwritten rules (norms), it is counter-productive to the individual and affects individual's mental well-being”
Statistically rare behaviorDeviates from the normIt's counter-productiveAffects the mental well-being
Normal
Statistically rare behaviorDeviates from the normIt's counter productiveAffects the mental well-being
Abnormal
Statistically rare behaviorDeviates from the normIt's counter productiveAffects the mental well-being
Normal
Definition
Neuroscience: “Mental disorders are a diverse group of brain disorders that primarily affect emotion, higher cognition and executive function”
Philosopher: “There is no such thing as mental illness in any culture, and that there could not be, because the very notion of mental illness is based on a fundamental mistake or set of mistakes.”
Wikipedia: “Mental disorder or mental illness are terms used to refer to a psychological or physiological pattern that occurs in an individual and is usually associated with distress or disability that is not expected as part of normal development or culture”
DSM criteria of abnormal behavior: “A behavior is considered as abnormal if it is statistically rare, deviates from society's unwritten rules (norms), it is counter-productive to the individual and affects individual's mental well-being”
Diagnostic Systems
Diagnostic and Statistical Manual of Mental Disorders (DSM)
D
Publisher: American Psychiatric Association
Last Version: IV-TR
Covers only Mental Disorders
International Classification of Diseases (ICD)
I
Publisher: World Health Organization
Last Version: 10
Covers all medical diagnosis (chapter 5: mental disorders)
C
ICD-10[International Statistical Classification of Diseases and Related Health Problems]
International Classification System. Coding of all kind of diseases and mental disorders.
22 Categories
Examples:
Certain infectious and parasitic diseases
Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism
Endocrine, nutritional and metabolic diseases
Mental and behavioural disorders
Diseases of the nervous system
Diseases of the eye and adnexa
Diseases of the ear and mastoid process
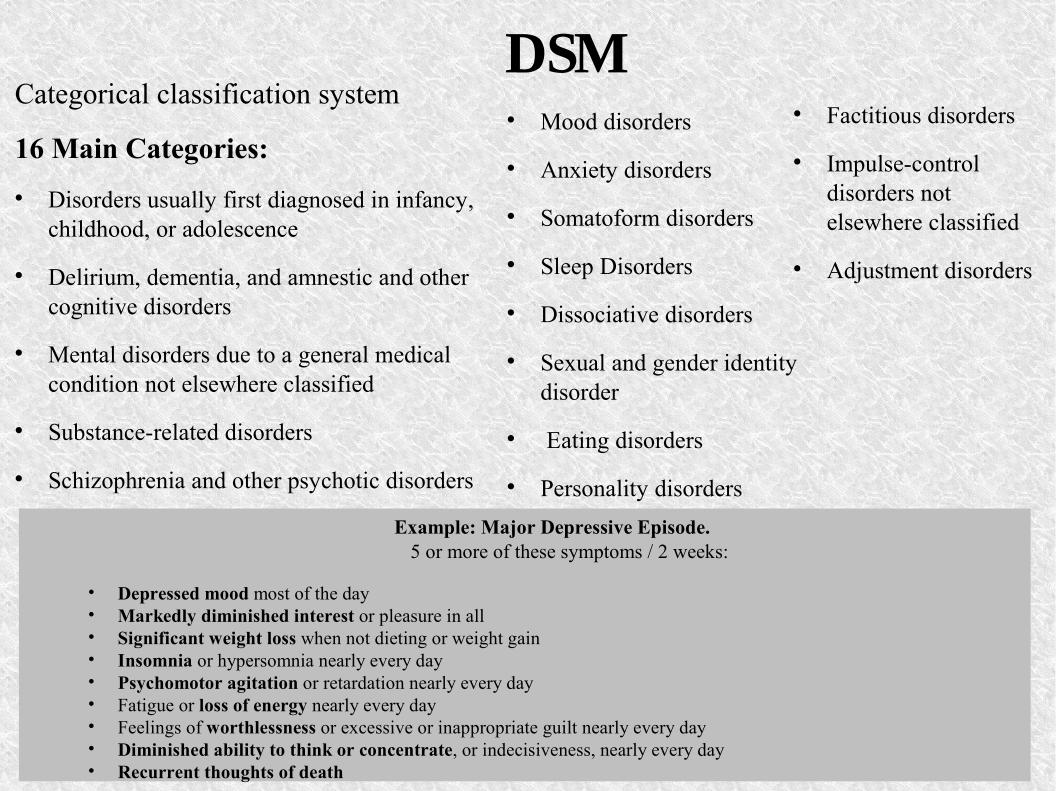
DSMCategorical classification system
16 Main Categories: Disorders usually first diagnosed in infancy,
childhood, or adolescence
Delirium, dementia, and amnestic and other cognitive disorders
Mental disorders due to a general medical condition not elsewhere classified
Substance-related disorders
Schizophrenia and other psychotic disorders
Example: Major Depressive Episode. 5 or more of these symptoms / 2 weeks:
• Depressed mood most of the day• Markedly diminished interest or pleasure in all• Significant weight loss when not dieting or weight gain • Insomnia or hypersomnia nearly every day • Psychomotor agitation or retardation nearly every day • Fatigue or loss of energy nearly every day • Feelings of worthlessness or excessive or inappropriate guilt nearly every day • Diminished ability to think or concentrate, or indecisiveness, nearly every day • Recurrent thoughts of death
Mood disorders
Anxiety disorders
Somatoform disorders
Sleep Disorders
Dissociative disorders
Sexual and gender identity disorder
Eating disorders
Personality disorders
Factitious disorders
Impulse-control disorders not elsewhere classified
Adjustment disorders
Diagnostic Systems
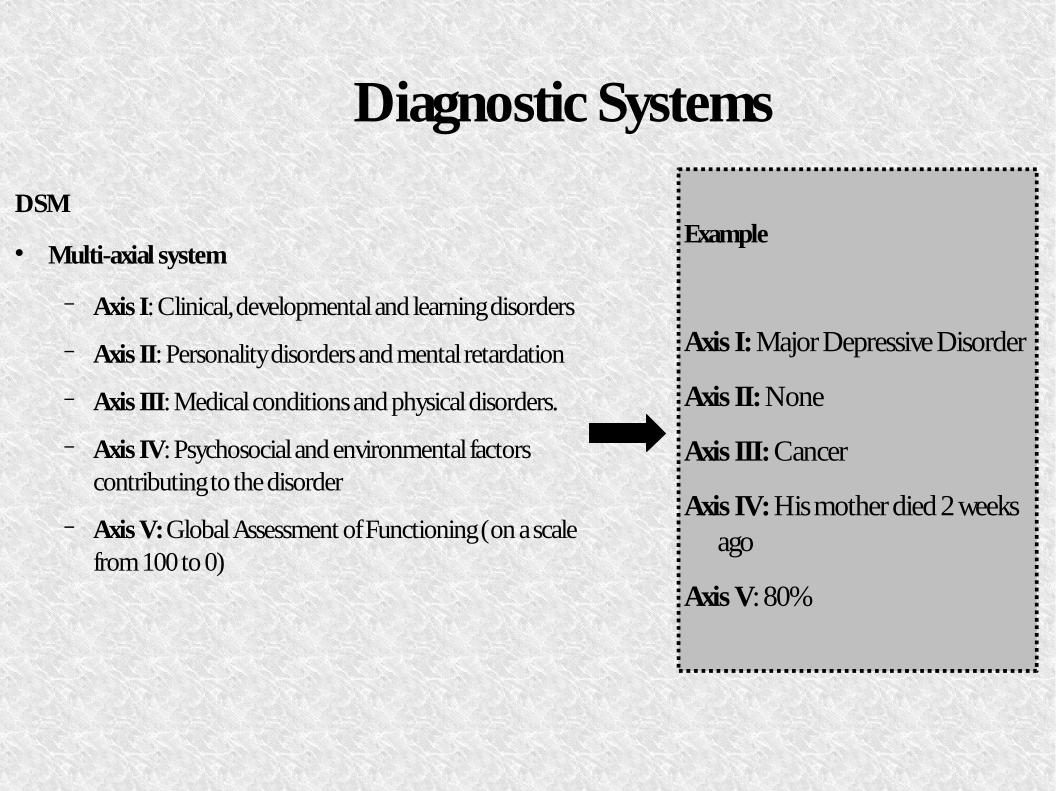
DSM
Multi-axial system
− Axis I: Clinical, developmental and learning disorders
− Axis II: Personality disorders and mental retardation
− Axis III: Medical conditions and physical disorders.
− Axis IV: Psychosocial and environmental factors contributing to the disorder
− Axis V: Global Assessment of Functioning (on a scale from 100 to 0)
f
Example
Axis I: Major Depressive Disorder
Axis II: None
Axis III: Cancer
Axis IV: His mother died 2 weeks ago
Axis V: 80%
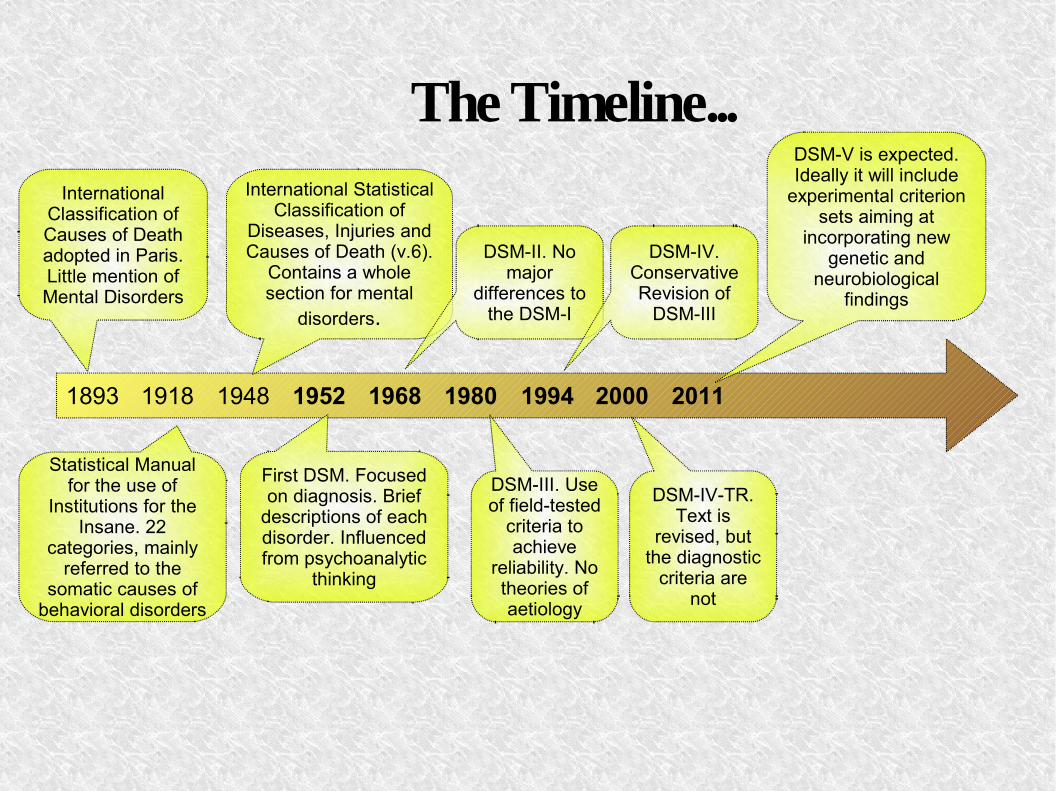
The Timeline...
1893 1918 1948 1952 1968 1980 1994 2000 2011
International Classification of Causes of Deathadopted in Paris. Little mention of Mental Disorders
International Statistical Classification of
Diseases, Injuries and Causes of Death (v.6).
Contains a whole section for mental
disorders.
Statistical Manual for the use of
Institutions for the Insane. 22
categories, mainly referred to the
somatic causes of behavioral disorders
First DSM. Focused on diagnosis. Brief
descriptions of each disorder. Influenced from psychoanalytic
thinking
DSM-II. No major
differences to the DSM-I
DSM-III. Use of field-tested
criteria to achieve
reliability. No theories of aetiology
DSM-IV. Conservative Revision of
DSM-III
DSM-IV-TR. Text is
revised, but the diagnostic
criteria are not
DSM-V is expected. Ideally it will include
experimental criterion sets aiming at
incorporating new genetic and
neurobiological findings
Criticism of DSM
Use of categoriesDSM uses categories, but drugs do not respect the boundaries of the disorders.Many disorders are better conceptualized as dimensional traits.
Normal Abnormal/ Mental Disorder
Different levels of symptoms. More or less severe cases.“Not Otherwise Specified” category is used very often!
Co-morbidityA large fraction of patients qualifies for multiple diagnoses.
Possible explanations:Shared genetic risk factorsErrors in splitting symptoms between different disorders
Mental Disorders and Neuroscience
Need for integration of Neuroscience into DSM-V Arbitrary boundaries between mental and neurological disorders. Overlapping practice patterns between neurology and psychiatry. Use of neurological techniques in order to treat mental disorders (e.g. deep brain stimulation) Both treat higher brain functions (e.g. autism, Alzheimer's disease, ADHD)
B
Biological basis of many mental disorders (e.g. schizophrenia, bipolar disorder)
B
Need to build a new dimensional diagnostic system. Ultimate goal: a diagnostic classification system for mental disorders based not only on symptomatology but also on aetiology and pathophysiology of the disorders.
How can Neuroscience help?
Neurogenetics Significant influence of genes (twin
studies/ adoption studies etc)
s
Many studies tried to identify the role of genetic factors in development of disorders.
Interaction between multiple genetic factors that cause a common symptom in different mental disorders (e.g. gene catechol-O-methyltransferase => metabolism of neurotransmitters like dopamine=> schizophrenia-like symptoms)
d
New technologies will provide complete information about the exact genetic factors
How can Neuroscience help?
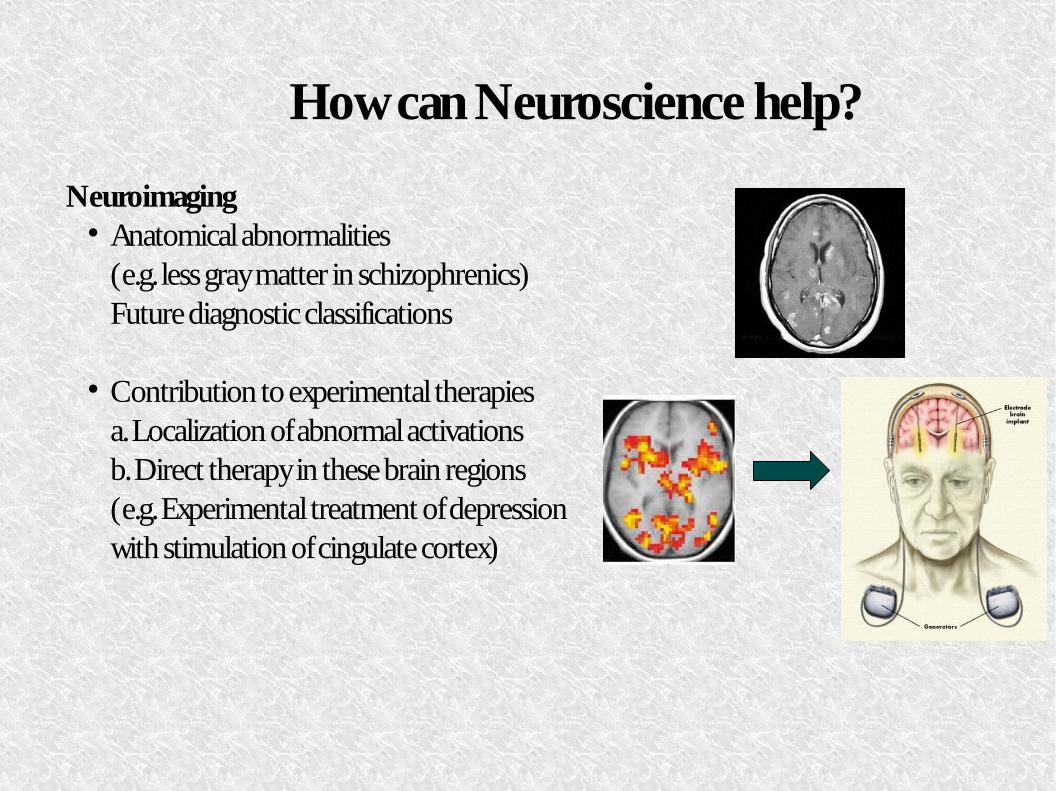
Neuroimaging Anatomical abnormalities
(e.g. less gray matter in schizophrenics)Future diagnostic classifications
Contribution to experimental therapiesa. Localization of abnormal activationsb. Direct therapy in these brain regions(e.g. Experimental treatment of depression with stimulation of cingulate cortex)
w
How can Neuroscience help?
Example: Phenylketonuria [1 in 15,000 births]autosomal recessive genetic disorder deficiency in the PAH enzyme→
Discovery of phenylketones in urine of some mentally retarded individualsAnatomical differences (brain size ~80% of normal)
A
1950: More specific reports White matter abnormalities (spongy change)
W
Pallor of myelin staining Demyelination
Demyalination is caused after the birthMore accurate detection of PKUDietary Therapy (low in phenylalanine)
D
Today: Animal Models
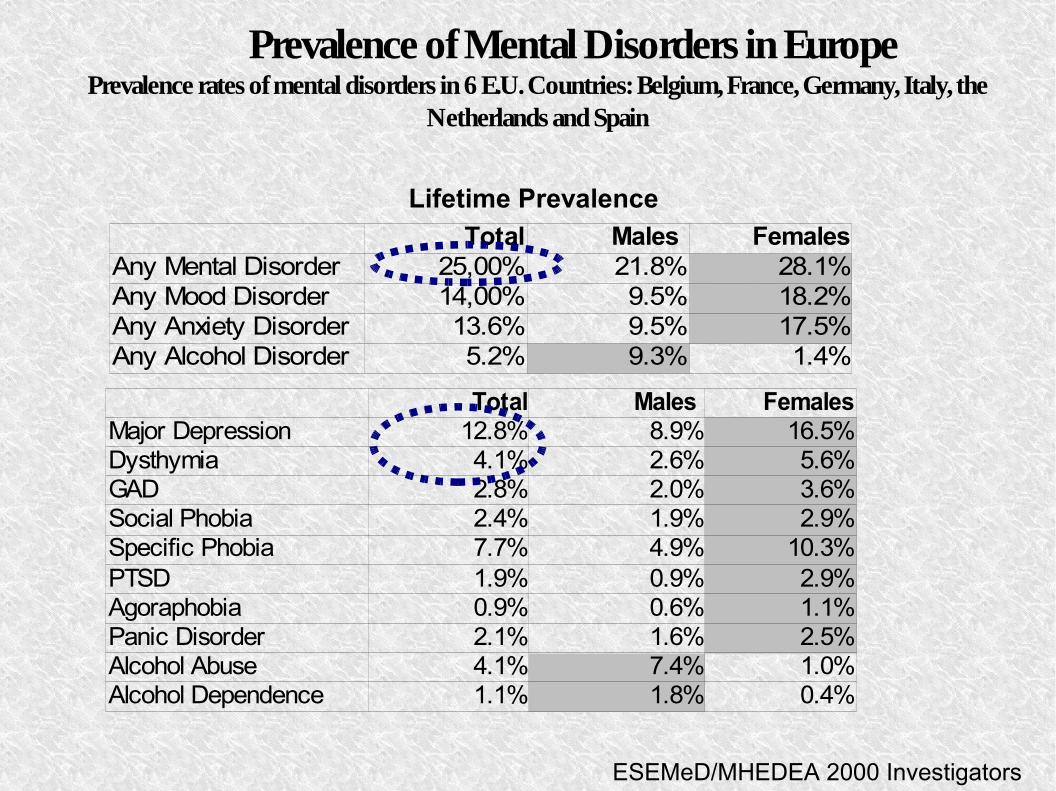
Prevalence of Mental Disorders in EuropePrevalence rates of mental disorders in 6 E.U. Countries: Belgium, France, Germany, Italy, the
Netherlands and Spain
Total Males FemalesAny Mental Disorder 25,00% 21.8% 28.1%Any Mood Disorder 14,00% 9.5% 18.2%Any Anxiety Disorder 13.6% 9.5% 17.5%Any Alcohol Disorder 5.2% 9.3% 1.4%
Lifetime Prevalence
Total Males FemalesMajor Depression 12.8% 8.9% 16.5%Dysthymia 4.1% 2.6% 5.6%GAD 2.8% 2.0% 3.6%Social Phobia 2.4% 1.9% 2.9%Specific Phobia 7.7% 4.9% 10.3%PTSD 1.9% 0.9% 2.9%Agoraphobia 0.9% 0.6% 1.1%Panic Disorder 2.1% 1.6% 2.5%Alcohol Abuse 4.1% 7.4% 1.0%Alcohol Dependence 1.1% 1.8% 0.4%
ESEMeD/MHEDEA 2000 Investigators
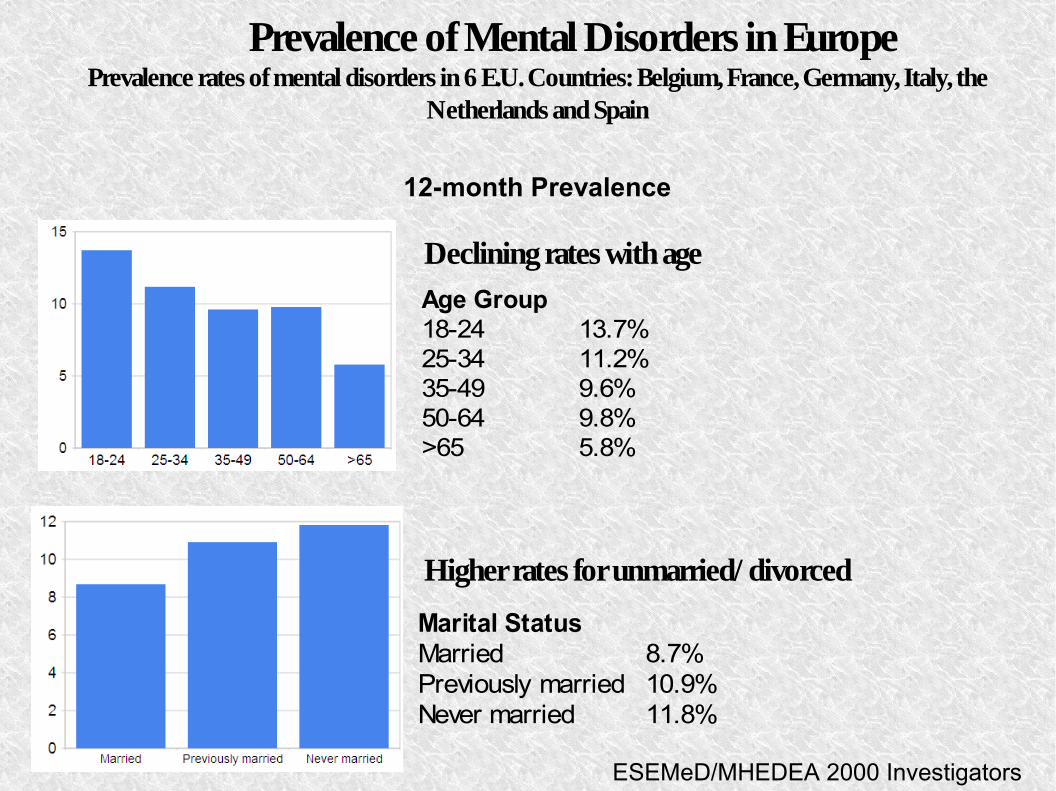
Prevalence of Mental Disorders in EuropePrevalence rates of mental disorders in 6 E.U. Countries: Belgium, France, Germany, Italy, the
Netherlands and Spain
Declining rates with ageAge Group18-24 13.7%25-34 11.2%35-49 9.6%50-64 9.8%>65 5.8%
Higher rates for unmarried/ divorced
Marital StatusMarried 8.7%Previously married 10.9%Never married 11.8%
12-month Prevalence
ESEMeD/MHEDEA 2000 Investigators
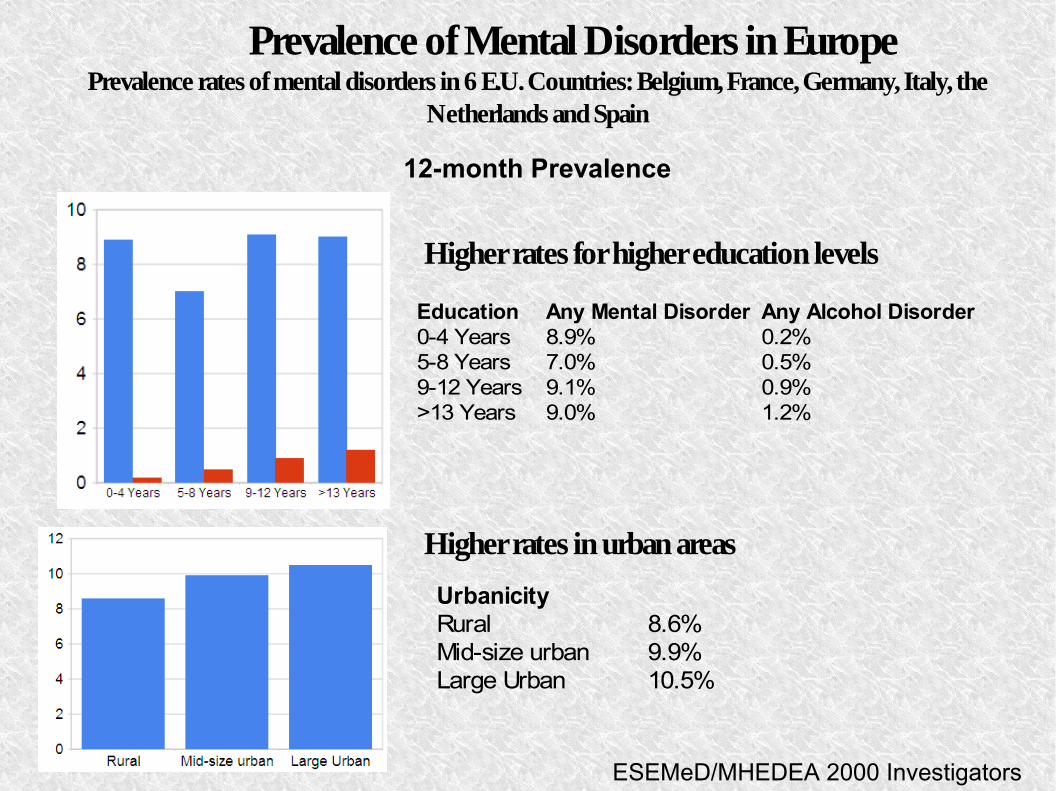
Prevalence of Mental Disorders in EuropePrevalence rates of mental disorders in 6 E.U. Countries: Belgium, France, Germany, Italy, the
Netherlands and Spain
Higher rates for higher education levels
Higher rates in urban areas
Education Any Mental Disorder Any Alcohol Disorder0-4 Years 8.9% 0.2%5-8 Years 7.0% 0.5%9-12 Years 9.1% 0.9%>13 Years 9.0% 1.2%
12-month Prevalence
ESEMeD/MHEDEA 2000 Investigators
UrbanicityRural 8.6%Mid-size urban 9.9%Large Urban 10.5%

Prevalence of major psychiatric disorders
Example: DepressionDepression ranks 5th across women and 7th across men as a cause of morbidity (World Bank, 1993)
a
WHO: in 2020 depression will be the second most important cause of disability.The cultural background is likely to determine whether depression will be experienced and expressed in psychological and emotional terms or in physical terms.
Bhugra & Mastrogianni, 2004
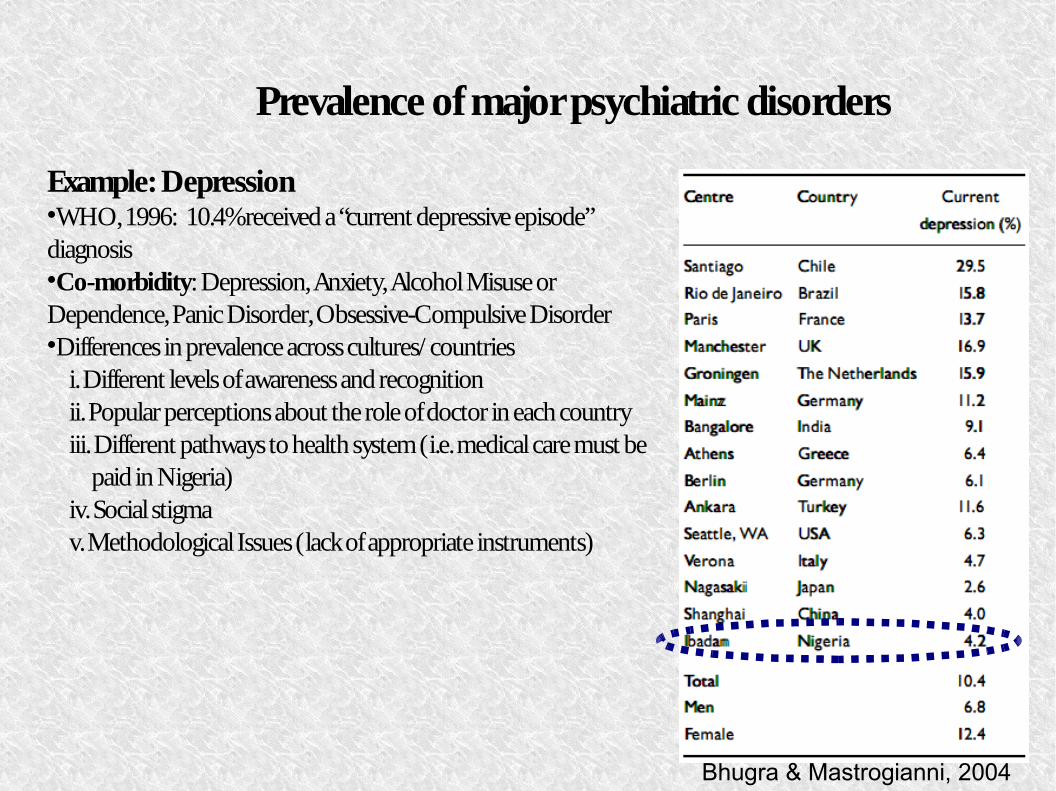
Prevalence of major psychiatric disorders
Example: DepressionWHO, 1996: 10.4% received a “current depressive episode” diagnosisCo-morbidity: Depression, Anxiety, Alcohol Misuse or Dependence, Panic Disorder, Obsessive-Compulsive DisorderDifferences in prevalence across cultures/ countries
i. Different levels of awareness and recognitionii. Popular perceptions about the role of doctor in each countryiii. Different pathways to health system (i.e. medical care must be
paid in Nigeria)iv. Social stigmav. Methodological Issues (lack of appropriate instruments)
v
Bhugra & Mastrogianni, 2004
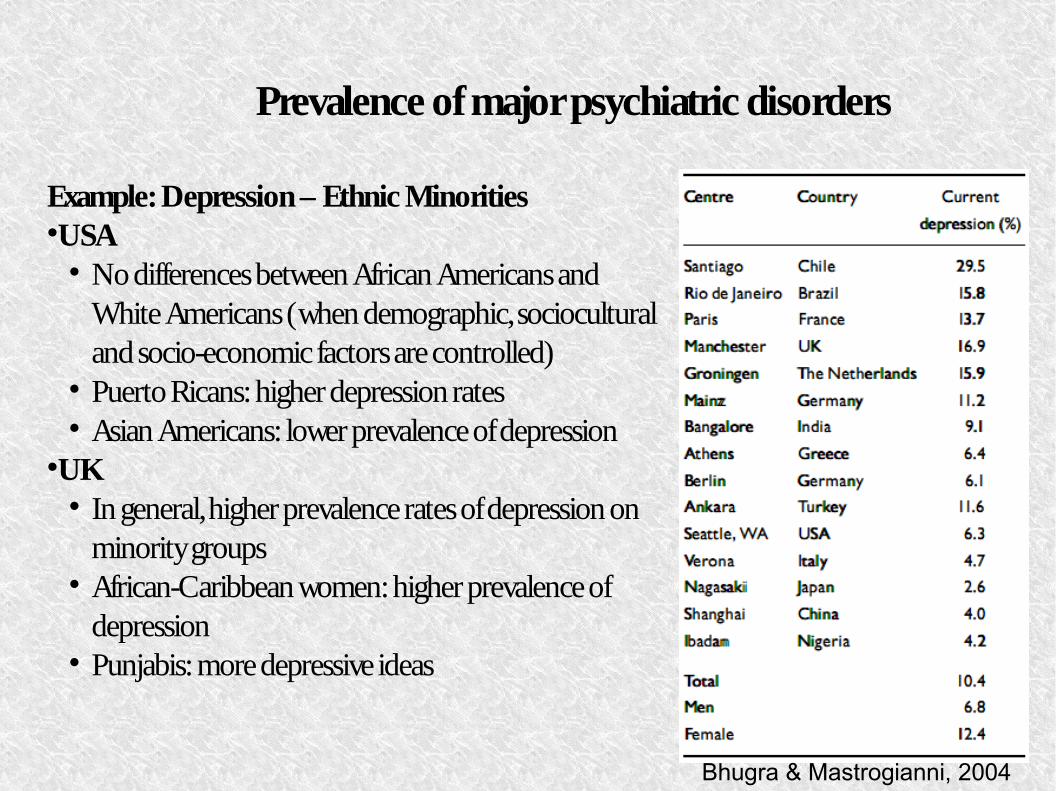
Prevalence of major psychiatric disorders
Example: Depression – Ethnic MinoritiesUSA
No differences between African Americans and White Americans (when demographic, sociocultural and socio-economic factors are controlled)
a
Puerto Ricans: higher depression rates Asian Americans: lower prevalence of depression
UK In general, higher prevalence rates of depression on
minority groups African-Caribbean women: higher prevalence of
depression Punjabis: more depressive ideas
Bhugra & Mastrogianni, 2004
Prevalence of major psychiatric disorders
Example: Depression – DiagnosisDepression is under-recognized throughout the world. Primary care physicians detect only 50% of the casesUK
Asians: visit their practitioner more frequently, but is less likely to have their psychological difficulties identified (complaints about somatic symptoms)
i
Indian women: 17% recognitionUSA
Physicians are less likely to detect depression among African American and Hispanic patientsAustralia
Asians: lower rate of diagnosis (similar rate of self-reported symptoms)
A
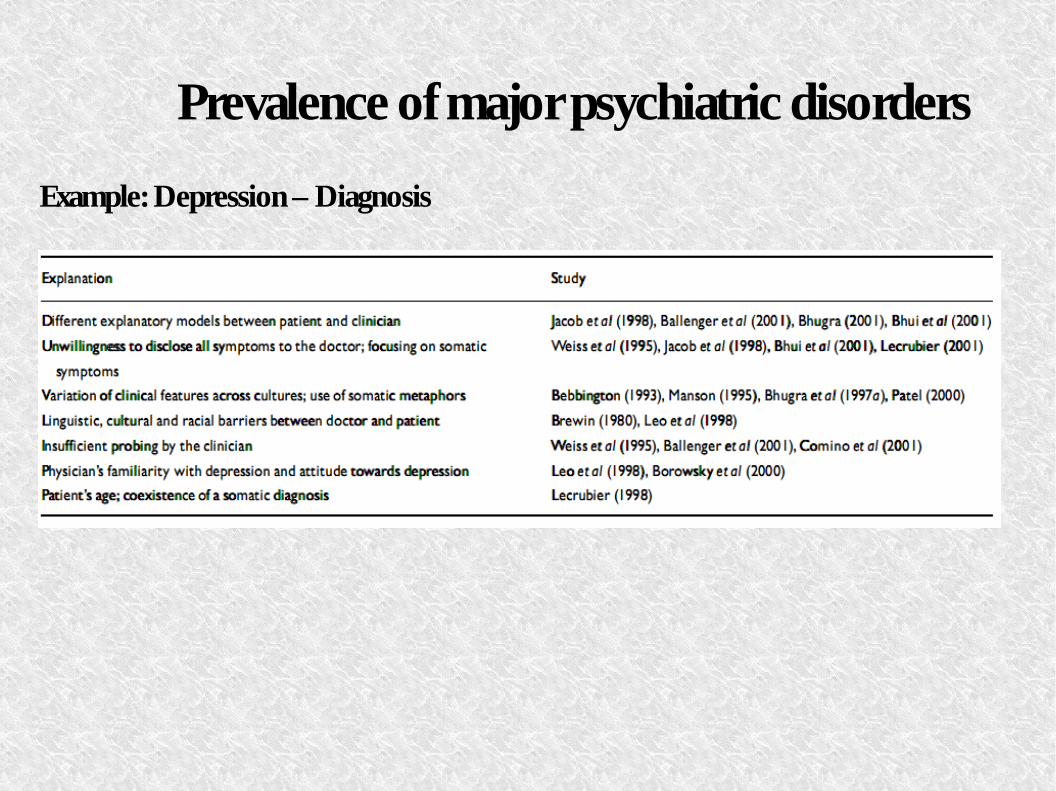
Prevalence of major psychiatric disorders
Example: Depression – Diagnosis
SummaryTwo main categorical systems:DSM (mental disorders)ICD (diseases and mental disorders)
Need for integration of Neuroscience in the future versions of these categorical systemsDiagnosisTreatmentFuture Studying
Prevalence & Epidemiology450 million people suffer from mental disordersMost common: mood disordersMore women than menDevelopment during youthUrban Areas > Rural AreasDifferent rates around the worldSocial factors (culture, language, minorities etc)