Embed Size (px)
Citation preview


-Definition of PC
-Historical view
-PC Importance
-PC Goals & Benefits
-Q & A regarding PC
-PC Tools
-PC for Men
-PC in Iraq

A set of prevention and management interventions that aim to identify and modifybiomedical , behavioral, and social risks to a woman’s health or pregnancy outcome.




To limit assessments to this population is likely to result in missed opportunities for prevention education because nearly half (49.2%) of all pregnancies in the United States occur to women who were not intending to become pregnant at the time they did. These pregnancies, which are termed unintended, occur in all subgroups of sexually active women; rates vary by age and socioeconomic and marital status. The highest ratesare for women younger than 20 years and women older than 40 years, but the largest number of unintended pregnancies occur in women aged 20–24 years. Among married women, 31% of pregnancies are self-reported as unintended.

As approximately half of all pregnancies in the United States are unplanned.
In 1995, Conway and associates studied the type of preconceptional counseling likely to be offered to women of reproductive age by 140 internal medicine and 42 family practice residents at Cook County Hospital. Residents were asked to answer an anonymous, self-administered questionnaire. During a 2-week period, 115 of 140 (82%) internal medicine residents and 28 of 42 (67%) family practice residents completed the questionnaire. The knowledge score consisted of a total of 46 items in a true-or-false format. Hypothetical patients and recommended management decisions were presented relating to rubella immunization, potential for congenital anomalies in diabetic patients, and management of chronic hypertension. More than 40% of the residents failed to indicate that they would provide a healthy woman information about rubella immunization, family planning, or counseling on sexually transmitted disease and safer sex.

Adverse pregnancy outcomes remain a prevalent health problem
–12% of babies are born premature, 8% with low birth weight
–3% have major birth defects
–31% of women giving birth suffer pregnancy complications
•Risk factors for adverse pregnancy outcomes remain prevalent among woment of reproductive age
–Smoking, obesity, teratogenic drugs, preexisiting medical conditions (diabets)




Is preconception care best targeted to the general population or to specific subsets?
Should it always be offered as a routine component of well-woman care or delegated to a special visit?
Do all potentially fertile women want preconception services?
Is preconception care cost-effective?
Must preconception risk assessment and related education be provided in a clinical setting?
How do multiple providers avoid competing or conflicting recommendations?
What strategies best encourage busy providers to incorporate a prevention emphasis into routine encounters?



HistoryMedical History
Reproductive History
Nutrition
Family History
Social History
Laboratory tests

Medical HistoryIs the patient under current or former treatment for:
*Diabetes mellitus?*Thyroid disorders?*Hyperphenylalaninemia?*Asthma?*Heart disease?*Chronic hypertension?*Deep venous thrombosis?*Kidney disease?*Systemic lupus erythematosus?*Epilepsy?*Hemoglobinopathies?*Cancer?

Medical history*Does the patient have occupational exposure to the blood or bodily secretions of others?*Does the patient engage in high-risk behaviors for
exposure to the human immunodeficiency virus?*Does the patient handle feline litter boxes or eat raw
or very rare meat?*Does the patient routinely or occasionally take any
prescribed medications?*Does the patient routinely or occasionally take any
over-the-counter medications?

Reproductive HistoryHas the patient had:
*Uterine or cervical abnormalities?*Two or more pregnancies ending in first trimester
miscarriage without an intervening successful gestation?*One or more fetal deaths?*One or more preterm deliveries?*One or more small-for-gestational-age infants?*One or more infants requiring care in a neonatal
intensive care unit?*One or more infants with a birth defect?

NutritionDoes the patient:
*Folic acid supplement?
*Practice vegetarianism?*Eat a special diet?*Have a history of bulimia or anorexia?*Use vitamin supplements in excess of the RDA*Have a history of pica?*Weight < 85% or > 135% of the ideal for height?

Family HistoryDoes the patient, her partner, any of their offspring, or
any members of their families have:
*Hemophilia?*Thalassemia?*Tay-Sachs trait or disease?*Sickle cell disease or trait?*Phenylketonuria?*Cystic fibrosis?*Birth defects?*Mental retardation?

Social HistoryDoes the patient
*Drink beer, wine, or hard liquor?*Smoke cigarettes or use other tobacco products?*Use marijuana, cocaine, or any similar drugs?*Use lead or chemicals at home or at work?*Participate in activities that could result in
overheating (e.g. saunas, hot tubs, demanding exercise in hot, humid conditions)?*Have evidence of current or former physical, sexual,
or psychological abuse?*Have a plan for spacing and timing her pregnancies?*Have maternity benefits in her insurance program
that cover her and a future neonate?*Know her employer’s policies around pregnancy and
birth?

Laboratory tests :*Hematocrit*Rubella serology, immunization if indicated*Varicella titer, immunization if indicated*Syphilis serology***Screenings
*Toxoplasmosis*Hepatitis B surface antigen*Chlamydia*Gonorrhea*Tuberculosis*Human immunodeficiency virus*Tay-Sachs disease*Cystic fibrosis*Sickle cell*Pap smear




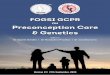
(C. Savona-Ventura et al : Int. J Risk Safety Med , 2007, 19:229-236)



In a study of 22 women who delivered infants with this syndrome in four Southern California counties, 57% of the women had 22 known missed opportunities, such as induced and spontaneous abortion.

Each year in the United States more than 4000 pregnancies are complicated by NTDs, and between 2500 and 3000 infants are born with the condition.
Because the research indicated that 50–70% of NTDs could be prevented by adequate periconceptional folic acid intake, the US Public Health Service (USPHS) released a landmark recommendation in 1992 that read: “All women of childbearing age in the United States who are capable of becoming pregnant should consume 0.4 mg of folic acid per day for the purpose of reducing their risk of having a pregnancy affected with spina bifida or other neural tube defects


Little attention has been given to men’s preconception health and health care
•In the US, there has been a steady increase in research and programs on men’s health
“ Men as Partners in reproductive health”

Why Preconception care for men is important?
–Improving family planning and pregnancy outcomes, enhancing the reproductive health and health behavior of their female partners, and preparing men for fatherhood
–Offer an opportunity for disease prevention and health promotion in men




















![Preconception counselling directed on nutrition and ... counseling nutrition...DHF TS THF Methyl acceptor Methylated acceptor [vitamin B6] NO // Derangements in one carbon pathway](https://img.dokumen.tips/doc/110x75/5e3ae9506718b4411c1e314f/preconception-counselling-directed-on-nutrition-and-counseling-nutrition.jpg)