Embed Size (px)
Citation preview

Pharmacotherapy of Hypertension
Ankita MishraJNMCH
AMU,ALIGARH

Chronic sustained elevation of systemic arterial blood pressure.
JNC 8 Recommendation
• Definitions of HTN and prehypertension not addressed, but thresholds for pharmacologic treatment are defined.
Introduction

Depending on methods of patient ascertainment
• Essential hypertension: ~80–95% • Secondary hypertension: 5–20%

Physiological regulation of BP overlapping mechanism
• Neural: • Baroreceptor, Chemoreceptor reflexes, RVLM
• Hormonal:• Catecholamines, RAAS, Vasopressin
• Renal body fluid control system:• Pressure natriuresis, diuresis


Principles of Antihypertensive Therapy Arterial pressure = cardiac output X peripheral vascular resistance. • BP lowered by actions on TPR, CO, or both.
• CO -decreased by inhibiting myocardial contractility or by decreasing ventricular filling pressure.
• Reduction in ventricular filling pressure - by actions on venous tone or on blood volume via renal effects.
• TPR –decreased by acting on smooth muscle to cause relaxation of resistance vessels.
• Or by interfering with activity of systems that produce constriction of resistance vessels (sympNS, RAAS).

Classification of Antihypertensive Drugs by Their Primary Site or Mechanism of Action

• Diuretics • Thiazides & related agents (hydrochlorothiazide, chlorthalidone,
chlorothiazide, indapamide, metolazone)• Loop diuretics (furosemide, bumetanide, torsemide, ethacrynic acid)• K+-sparing diuretics (amiloride, triamterene, spironolactone)
• Sympatholytic drugs • β receptor antagonists (metoprolol, atenolol, betaxolol, bisoprolol,
carteolol, esmolol, nadolol, nebivolol, penbutolol, pindolol, propranolol, timolol)
• α receptor antagonists (prazosin, terazosin, doxazosin, phenoxybenzamine, phentolamine)
• Mixed α-β receptor antagonists (labetalol, carvedilol)• Centrally acting adrenergic agents (methyldopa, clonidine)

• Ca2+ channel blockers Verapamil, diltiazem, felodipine, nicardipine, isradipine, amlodipine, clevidipine, nifedipine
• Angiotensin-converting enzyme inhibitors Captopril, enalapril, lisinopril, ramipril, fosinopril, moexipril, perindopril, trandolapril
• AngII receptor antagonists Losartan, candesartan, irbesartan, valsartan, telmisartan, eprosartan, olmesartan)
• Direct Renin Inhibitor Aliskiren
• Vasodilators 1.Arterial(hydralazine) 2.Arterial and venous (nitroprusside)

Diuretics• THIAZIDE:• Hydrochlorothiazide prototype drug.
• Exact mechanism of BP reduction is not certain.
• Initially decreases ECV by interacting with thiazide-sensitive NaCl co-transporter (NCC) in DCT, enhancing Na+ excretion in urine, leading to fall in CO.
• Long-term effect due to decreased vascular resistance;
• Thiazides directly or indirectly promote vasodilation.

• DOSE-12.5 mg- 25 mg daily of chlorthalidone or hydrochlorothiazide. • Most patients respond within about 4-6 wks.
• ADRs- Hypokalemia, Hyperuricemia, Hypercalcaemia, Hyperglycaemia, Hyperlipidaemia, Hypersensitivity reaction.

• OTHER DIURETIC ANTIHYPERTENSIVE AGENTS
• Thiazide diuretics more effective antihypertensive than loop diuretics.
• Not preferred in mild to moderate HTN.
• Efficacy of loop diuretics in producing a rapid and profound natriuresis can be detrimental for HTN.
• Useful in patients with azotemia or with pulmonary edema.

• Amiloride [K+-sparing diuretic] has some efficacy in lowering BP.
• Spironolactone, lowers BP but has significant ADRs, especially in men (e.g., erectile dysfunction, gynecomastia, benign prostatic hyperplasia).
• Should be used cautiously with frequent measurements of K+ concentrations in plasma.
• Renal insufficiency is a relative contraindication to the use of K+-sparing diuretics.
• Concomitant use of an ACEI or an ARA magnifies risk of hyperkalemia.

Sympatholytic Agents• β RECEPTOR ANTAGONIST• MOA- Reduction in myocardial contractility, HR and CO ; blockade of JG
complex β receptor, reducing renin secretion- diminishing production of circulating AngII; nebivolol and celiprolol promotes endothelial cell dependent vasodilation via activation of NO pathway.
• PHARMACOLOGICAL EFFECTS• Vary in selectivity for β 1 receptor, presence of ISA and vasodilating
capacity. • Drugs without ISA - initial reduction in CO and a reflex-induced rise in TPR ,
no net change in BP. • Drugs with ISA -lesser decreases in HR and CO;

• THERAPEUTIC USES- Provide effective therapy for all grades of HTN.
• Once- or twice-daily administration.
• Elderly and African-Americans show less response.
• The combination of a β antagonist, a diuretic, and a vasodilator is effective if third drug required.
• Highly preferred for hypertensive patients with MI, IHD, CHF.
• ADRs- Bradycardia, cold extremities, sleep disturbance, bronchoconstriction, hypoglycaemia, rebound HTN (withdrawal).

• α1 ADRENERGIC RECEPTOR ANTAGONISTS
• PHARMACOLOGICAL EFFECTS• Initially, reduce arteriolar resistance and increase venous capacitance and
cause a sympathetically mediated reflex increase in HR and plasma renin activity.
• Long-term therapy- vasodilation persists, but CO, HR, and plasma renin activity return to normal.
• Retention of salt and water occurs in many patients during continued administration- attenuates the postural hypotension.
• Reduce triglycerides, LDL and increase HDL.

• THERAPEUTIC USES• Not recommended as monotherapy.
• Used with diuretics, β blockers, and other antihypertensive agents.
• Use for hypertensive patients with BPH, because they also improve urinary symptoms.
• ADRs- Postural hypotension, impotence, nasal congestion, Na+ and water retention.

• COMBINED α1 AND β ADRENERGIC RECEPTOR ANTAGONISTS
• LABETALOL- α1antagonist, nonselective β antagonist with partial agonist activity.
• Can reduce BP sufficiently rapidly to be useful for the treatment of hypertensive emergencies.
• CARVEDILOL- is a β antagonist with α1 antagonist activity.• Approved for hypertension and symptomatic HF. • Reduces mortality in patients with CHF when used as an adjunct to
therapy with diuretics and ACE inhibitors.• Not be given in decompensated HF.

• METHYLDOPA• Centrally acting agent; Prodrug• Analog of DOPA- metabolized by a.a decarboxylase – methyldopamine-
converted to -methylnorepinephrine -Stored in secretory vesicles of adrenergic neurons, substituting for NE.
• Inhibit adrenergic neuronal outflow in CNS.• Agonist at presynaptic α2 adrenergic receptors in brainstem, attenuating NE
release.
• THERAPEUTIC USE- HTN during pregnancy; effective and safe for mother and fetus.
• Dose is 250 mg twice daily.• Single daily dose at bedtime minimizes sedative effects, twice daily is
required for some.

• ADRs- Sedation, depression, dryness of the mouth, diminished libido, parkinsonian signs, hyperprolactinemia, gynecomastia and galactorrhea, hepatotoxicity, hemolytic anemia.

• α 2 RECEPTORS AGONIST-• Clonidine prototype.
• Stimulate α 2A subtype of α 2 receptors in brainstem, resulting in a reduction in sympathetic outflow from CNS.
• At higher doses, these drugs can activate α 2B subtype on vascular smooth muscle cells.
• THERAPEUTIC USE- Not a leading option for monotherapy of HTN.
• Effectively lower BP in some patients who have not responded to other agents.

• Used in hypertensive for diagnosis of pheochromocytoma. [lack of suppression of plasma concn. of NE to >500 pg/mL 3 hours after oral dose of 0.3 mg of clonidine suggests tumor presence].
• ADRs- • Sedation, xerostomia (parotid gland swelling and pain), postural
hypotension, sleep disturbances, restlessness, depression, bradycardia and sinus arrest, contact dermatitis(transdermal).
• Sudden discontinuation of clonidine α2 adrenergic agonists may cause a withdrawal syndrome.

Ca2+ Channel Antagonists
• Bind to α1 subunit of L-type Ca2+ channels and reduce Ca2+ flux through voltage sensitive channel.
• PHARMACOLOGICAL EFFECTS-
• Actions in Vascular Tissue- relax arterial smooth muscle, less effect on venous beds, do not affect cardiac preload.
• Verapamil less potent vasodilator than dihydropyridine.
• Actions in Cardiac Cells- Verapamil-direct negative chronotropic, dromotropic & inotropic effects; less with DHP
• Greater degree of peripheral vasodilation seen with DHP- sufficient increase in symp. tone reflexly to overcome negative inotropic effect.

• THERAPEUTIC USE- given alone or in combination with other drugs for HTN.
• Can achieving BP control as monotherapy in elderly subjects and African-Americans.
• May be preferred in patients with isolated systolic HTN.
• ADRs- GERD, Urinary retention, Rash, Elevations of liver enzymes.
• Nifedipine- Tachycardia, Worsening of angina, Headache, Hypotension, Fluid retention.
• Verapamil- Bradycardia, Transient asystole, HF exacerbation, Constipation.

Angiotensin-Converting Enzyme Inhibitors
• Captopril was first agent to be developed for treatment of HTN. • Blocks the conversion of ANG I to ANG II.• Also inhibit degradation of bradykinin.
• THERAPEUTIC USE- ACEI lower BP to some extent in most patients.
• Response more in young and middle-aged Caucasian patients.
• Preferred initial agent in diabetic and CRD patients.
• Patients with hypertension and IHD are candidates for ACEI.
• ADRs- Dry cough, Hyperkalemia, Renal failure, Angioneurotic oedema, Teratogenic, altered taste sense

AT1 Receptor Antagonists
• By antagonizing AngII, these agents relax smooth muscle and promote vasodilation, increase renal salt and water excretion, reduce plasma volume, and decrease cellular hypertrophy.
• Also theoretically overcome some disadvantages of ACEI.
• THERAPEUTIC USES- Appear to be as effective as ACEI in HTN.
• Full effect on BP typically not until abt 4 wks.
• If BP is not controlled by AT1 antagonist alone, a second drug acting by a different mechanism (e.g., a diuretic or Ca2+ channel blocker) may be added.
• ADRs- Hypotension, Hyperkalemia, Renal failure, Teratogenicity.

Direct Renin Inhibitors
• Aliskiren- the first orally effective agent.
• Directly and competitively inhibits catalytic activity of renin.
• Inhibit capacity of renin to produce AngI from angiotensinogen.
• THERAPEUTIC USES- Can be given as monotherapy with dose-dependent increasing efficacy at 150-300 mg/day.
• Action appears to persist for 24 hrs.
• Combination with hydrochlorothiazide -greater lowering of BP.

• Long-term outcome studies—including assessments of target organ damage in heart, brain, kidneys—important in establishing its role.
• Concerns of higher ADRs and lesser benefit recently.
• ADRs- Diarrhea, Cough, Angioedema, Teratogenic, hyperkalemia.

Vasodilators
• HYDRALAZINE- no major role with introduction of newer agents.
• Hydralazine directly relaxes arteriolar smooth muscle.
• Do not relax venous smooth muscle.
• PHARMACOLOGICAL EFFECTS- Vasodilation associated with powerful stimulation of SNS, due to baroreceptor-mediated reflexes-
• Increased HR & contractility, increased renin activity, fluid retention;
• These effects counteract the antihypertensive effect of hydralazine.

• THERAPEUTIC USES- No longer a first-line drug –unfavorable ADR profile.
• May have utility in treatment of severe HTN.
• Can be useful in HTN emergencies in pregnant women (preeclampsia).
• Usual oral dosage of is 25-100 mg BD.
• ADRs- Headache, Nausea, Hypotension, Palpitations, Tachycardia, Angina pectoris, MI
• Drug-induced lupus syndrome, Serum sickness, Hemolytic anemia, Vasculitis, Rapidly progressive glomerulonephritis.

• SODIUM NITROPRUSSIDE- nitrovasodilator that acts by releasing NO. • NO activates guanylyl cyclase–cyclic GMP–PKG pathway, leading to
vasodilation • Mimick production of NO by vascular endothelial cells.• Mechanism of NO release not clear. • Tolerance does’nt develop to nitroprusside.
• PHARMACOLOGICAL EFFECTS- Nonselective vasodilator • Regional distribution of blood flow not affected by drug. • Renal blood flow and GFR maintained.• Modest increase in HR and overall reduction in myocardial O2 demand.

• THERAPEUTIC USES- • Used primarily to treat hypertensive emergencies.
• Lower BP during acute aortic dissection;
• Improve CO in HTN with pulmonary edema not responding to other treatment.
• Used to induce controlled hypotension during anesthesia -reduce bleeding in surgical procedures.

• Unstable molecule- decompose under alkaline conditions or when exposed to light.
• Given by continuous IV infusion. • Onset of action within 30 secs; peak effect within 2 min, effect disappears
within 3 minutes.
• Administered as controlled continuous infusion;• Available in vials that contain 50 mg. • Contents dissolved in 2-3 mL of 5% dextrose in water. • Added to 250-1000 mL of 5% dextrose in water giving 50-200 microg/mL.• Fresh sol. should be used, bottle covered with an opaque wrapping. • Majority respond to an infusion of 0.25-1.5 g/kg/min.

• ADRs- Hypotension;
• Cyanide accumulation leading to lactic acidosis-
• Occurs when sodium nitroprusside is infused at a rate >5 microg/kg/min or in patients receiving doses ~2 microg/kg/min for a prolonged period.
• Mismatching of ventilation with perfusion.


Lifestyle Modifications to Manage Hypertension
• Weight reduction; Attain and maintain BMI <25 kg/m2 .
• Dietary salt reduction; no more than 2,400 mg/day.
• Adapt DASH type dietary plan; Rich in fruits, vegetables, reduced content of saturated and total fat.
• Moderation of alcohol consumption.
• Smoking cessation.
• Physical activity; Regular aerobic activity, e.g., brisk walking for 30 min/d.

Strategies to Dose Antihypertensive Drugs (JNC8)
Strategy Description A Start one drug, to maximum dose, and then add a second drug. B Start one drug, then add a second drug before achieving max dose of first. C Begin 2 drugs at same time, as separate pills or combination pill. Initial combination therapy is recommended if BP is greater than 20/10mm Hg above goal.

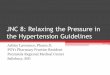
JNC 8 Hypertension Guideline Algorithm