Embed Size (px)
Citation preview
Legg – Calve – Perthes Legg – Calve – Perthes DiseaseDisease
Presenter – Dr. Maulik T PatelPresenter – Dr. Maulik T PatelOrthopedic surgeonOrthopedic surgeon
DefinitionDefinition
It is a self limiting disorder of the hip It is a self limiting disorder of the hip produced by ischemia and varying produced by ischemia and varying degrees of necrosis of the femoral head.degrees of necrosis of the femoral head.

SynonymsSynonyms
Coxa PlanaCoxa PlanaPseudocoxalgia (Calve)Pseudocoxalgia (Calve)Arthritis deformans juvenilis (Perthes)Arthritis deformans juvenilis (Perthes)Osteochondroses of the hipOsteochondroses of the hipCoronary disease of the hipCoronary disease of the hip

HISTORYHISTORY
Reidel in 1890 presented the first case of Reidel in 1890 presented the first case of osteochondritis dessecans in the hip.osteochondritis dessecans in the hip.
Preiser in Germany presented a patient Preiser in Germany presented a patient with osteoartritis deformans.with osteoartritis deformans.
HISTORYHISTORY
Waldenstorm In 1909 described the Waldenstorm In 1909 described the disorder in 10 children . He thought it to be disorder in 10 children . He thought it to be tubercular in origin and named it “Der tubercular in origin and named it “Der Obere Tuberculose Collumherd”Obere Tuberculose Collumherd”
In 1910 this disorder was recognised as In 1910 this disorder was recognised as an independent entity by three men…an independent entity by three men…
HISTORYHISTORY Arthur LeggArthur Legg of the of the
United StatesUnited States

HISTORYHISTORY Jacques CalveJacques Calve of of
FranceFrance
HISTORYHISTORY Georg PerthesGeorg Perthes of of
GermanyGermany
HISTORYHISTORY In the Early years treatment consisted on In the Early years treatment consisted on
non weight bearing with Ischial weight non weight bearing with Ischial weight bearing Caliperbearing Caliper
Parker started the use of broomstick cast in Parker started the use of broomstick cast in 1929.1929.
Eyre-Brook introduced traction in bed for 18-Eyre-Brook introduced traction in bed for 18-24 months.24 months.
In 1966 Salter induced avascular necrosis in In 1966 Salter induced avascular necrosis in Pig model and proved that best result was Pig model and proved that best result was with weightbearing with hips held in with weightbearing with hips held in abduction.abduction.

Blood supply to femoral headBlood supply to femoral head Retinacular arteriesRetinacular arteries Metaphyseal arteriesMetaphyseal arteries Artery of the teres Artery of the teres
ligamentligament

Blood supply to femoral headBlood supply to femoral head
Infants Infants 1.1. Medial ascending cervical or inferior Medial ascending cervical or inferior
metaphyseal arteries of trueta.metaphyseal arteries of trueta.2.2. Lat epiphysealLat epiphyseal3.3. Lig teres – insignificantLig teres – insignificant
4 mts – 4 years4 mts – 4 years1.1. Lat epiphysealLat epiphyseal2.2. Med epiphyseal decrease in number.Med epiphyseal decrease in number.

Blood supply to femoral headBlood supply to femoral head
4 yrs to 7 years4 yrs to 7 yearsEpiphyseal plate forms a barrier to metaphyseal Epiphyseal plate forms a barrier to metaphyseal
vessels.vessels. Pre-adolescentPre-adolescent
After 7 yrs arteries of lig teres become more After 7 yrs arteries of lig teres become more prominent and anastomose with the lateral prominent and anastomose with the lateral epiphyseal vessels.epiphyseal vessels.

IncidenceIncidence Male : Female = 4-5:1Male : Female = 4-5:1 2.5:1 in India2.5:1 in India Age of onset earlier in females.Age of onset earlier in females. Age – Age – Range – 2-13 years.Range – 2-13 years. Most common 4-8 years.Most common 4-8 years. Average – 6 years.Average – 6 years. Bilateral in 10-12 %Bilateral in 10-12 % Incidence more in Caucasians compared to Incidence more in Caucasians compared to
Negroid, mongoloid, Polynesians.Negroid, mongoloid, Polynesians. In India it is most prevalent in the west coast In India it is most prevalent in the west coast
especially in Udupi district.especially in Udupi district.

EtiologyEtiology
The exact etiology of Legg Calve Perthes The exact etiology of Legg Calve Perthes disease in not known but many factors disease in not known but many factors related to etiology of this disease have related to etiology of this disease have been mentioned.been mentioned.

EtiologyEtiology Coagulation disorders.Coagulation disorders. Arterial status of femoral head.Arterial status of femoral head. Abnormal venous drainage.Abnormal venous drainage. Abnormal growth and development.Abnormal growth and development. Trauma.Trauma. Hyperactivity or attention deficit disorder.Hyperactivity or attention deficit disorder. Genetic component.Genetic component. Environmental influences.Environmental influences. As a sequel to synovitis.As a sequel to synovitis.

Coagulation disordersCoagulation disorders Glueck et al showed that 75% of their series of Glueck et al showed that 75% of their series of
children with perthes disease had abnormalities of children with perthes disease had abnormalities of coagulation (protein C or S deficiency, thrombophilia, coagulation (protein C or S deficiency, thrombophilia, increased lipoprotein a, hypofibrinolysis)increased lipoprotein a, hypofibrinolysis)
-- JBJS Am Jan 1996-- JBJS Am Jan 1996 Valder Aruda et al reported factor 5 leiden mutation Valder Aruda et al reported factor 5 leiden mutation
in children with Perthesin children with Perthes -- Journal of paed orthopedics-- Journal of paed orthopedics Jan/feb 1999Jan/feb 1999

Coagulation disordersCoagulation disordersKaeley et al found no causal relationshipKaeley et al found no causal relationship -JBJS Br July 2000-JBJS Br July 2000Vinod Balasa, Charles Glueck et al found Vinod Balasa, Charles Glueck et al found
causal relationship between Factor 5 Leiden causal relationship between Factor 5 Leiden mutation, Anticardiolipin antibodies in Perthes mutation, Anticardiolipin antibodies in Perthes disease.disease.
--JBJS Am Dec 2004--JBJS Am Dec 2004Mc Dougall also found no linkMc Dougall also found no linkClearly more studies are needed to resolve Clearly more studies are needed to resolve
this issue.this issue.

Arterial status of femoral headArterial status of femoral head Angiographic studies have shown obstruction of Angiographic studies have shown obstruction of
superior capsular arteries and decreased flow in superior capsular arteries and decreased flow in medial circumflex femoral arteries in Perthes disease.medial circumflex femoral arteries in Perthes disease.
The intracapsular ring has been found to be The intracapsular ring has been found to be incomplete more often in males than females.incomplete more often in males than females.
In Negroid infants the major source of blood supply to In Negroid infants the major source of blood supply to the femoral head is from the inferior gluteal artery the femoral head is from the inferior gluteal artery which could be a reason why Perthes is uncommon in which could be a reason why Perthes is uncommon in negroid race.negroid race.

Abnormal venous drainageAbnormal venous drainageVenous drainage normally flows through the Venous drainage normally flows through the
medial circumflex femoral vein.medial circumflex femoral vein. In patients with perthes ,there is increased In patients with perthes ,there is increased
venous pressure in the femoral neck and venous pressure in the femoral neck and associated congestion in the metaphysis, and associated congestion in the metaphysis, and venous outflow obstruction has been found .venous outflow obstruction has been found .
In a dog model obstruction of venous outflow In a dog model obstruction of venous outflow has reproduced the features of AVN.has reproduced the features of AVN.

Abnormal growth and developmentAbnormal growth and developmentA delay in Bone age of 1.5 to 2 years A delay in Bone age of 1.5 to 2 years
has been seen in children with perthes has been seen in children with perthes disease.disease.
Low birth weight has been seen in Low birth weight has been seen in patients with Perthes Disease.patients with Perthes Disease.
Boys with Perthes have been found to Boys with Perthes have been found to be 1 inch shorter and girls 3 inch be 1 inch shorter and girls 3 inch shorter than their peers.shorter than their peers.
Some investigators have found low Some investigators have found low levels of growth factor Somatomedin C.levels of growth factor Somatomedin C.
TraumaTrauma
In the developing femur , the major lateral In the developing femur , the major lateral epiphyseal artery must course through a epiphyseal artery must course through a narrow passage ,which could make it narrow passage ,which could make it susceptible to disruption in case of susceptible to disruption in case of trauma.trauma.

Hyperactivity or attention deficit Hyperactivity or attention deficit disorderdisorder
A high prevalence of this disorder has A high prevalence of this disorder has been seen in patients with Perthes been seen in patients with Perthes Disease.Disease.
But Its precise role has not been defined.But Its precise role has not been defined.

Genetic componentGenetic component
Familial association has been reported.Familial association has been reported.
Burch et al have found a X-Linked Burch et al have found a X-Linked recessive inheritance in a few cases.recessive inheritance in a few cases.

Environmental influencesEnvironmental influences
Low socioeconomic status has been seen Low socioeconomic status has been seen to be associated with Perthes Disease.to be associated with Perthes Disease.

Sequel to synovitisSequel to synovitis
Synovitis of the hip occurs early in LCPSynovitis of the hip occurs early in LCP
A controversial school of thought says that A controversial school of thought says that the increased pressure in synovitis may the increased pressure in synovitis may cause a tamponade effect on the cause a tamponade effect on the vasculaturevasculature

Truetta’s HypothesisTruetta’s Hypothesis
He postulated that the solitary blood He postulated that the solitary blood supply in the age group 4-8 yrs makes supply in the age group 4-8 yrs makes them suceptible to ischemia.them suceptible to ischemia.
Compression of Lat epiphyseal arteries by Compression of Lat epiphyseal arteries by ext.rotators.ext.rotators.

Caffey’s HypothesisCaffey’s Hypothesis
Intraepiphyseal compression of blood Intraepiphyseal compression of blood supply to ossification centersupply to ossification center

PATHOGENESISPATHOGENESIS
LOSS OF BLOOD SUPPLY PRODUCES LOSS OF BLOOD SUPPLY PRODUCES
AVN OF THE EPIPHYSEAL OSSCIFICATION AVN OF THE EPIPHYSEAL OSSCIFICATION
CENTRE FOLLOWED BY RESORPTION OF CENTRE FOLLOWED BY RESORPTION OF
DEAD BONE AND REPLACEMENT WITH DEAD BONE AND REPLACEMENT WITH
NEWLY FORMED IMMATURE BONE.NEWLY FORMED IMMATURE BONE.
THE PROCESS IS DESCRIBED IN STAGESTHE PROCESS IS DESCRIBED IN STAGES

ICIPIENT OR SYNOVITIS ICIPIENT OR SYNOVITIS STAGESTAGE
LAST 1-3 WEEKS . SYNOVIUM IS LAST 1-3 WEEKS . SYNOVIUM IS
SWOLLEN , HYPEREMIC AND SWOLLEN , HYPEREMIC AND
EDEMATOUS. EDEMATOUS. JOINT FLUID JOINT FLUID
IS INCREASED ANDIS INCREASED AND ABSENCE OF ABSENCE OF
IMFLAMMATORY CELLS.IMFLAMMATORY CELLS.

Increase joint space

STAGE OF AVNSTAGE OF AVN AVN INVOLVES PORTION OF OSSIFIC NUCLEUS AVN INVOLVES PORTION OF OSSIFIC NUCLEUS
SITUATED ANTERIORLY AMORPHOUS SITUATED ANTERIORLY AMORPHOUS
DEBRIES FILLS THE MARROW SPACES. TRABACUALES DEBRIES FILLS THE MARROW SPACES. TRABACUALES
ARE CRUSHED INTO MINUTE FRAGMENTS AND COMPRESSED ARE CRUSHED INTO MINUTE FRAGMENTS AND COMPRESSED
INTO A COMPACT BONE ACCOUNTING FOR INTO A COMPACT BONE ACCOUNTING FOR
INCREASED DENSITY ON RADIOGRAPH.INCREASED DENSITY ON RADIOGRAPH.
THE INCREASED OPACITY IS CONTRASTED THE INCREASED OPACITY IS CONTRASTED
MARKED DIMINIRALISATION OF ADJACENT METAPHYSIS MARKED DIMINIRALISATION OF ADJACENT METAPHYSIS
RESULT OF HYPERVASCULARITY RESULT OF HYPERVASCULARITY
CONSTITUTES PREPARATION FOR INVASION CONSTITUTES PREPARATION FOR INVASION
VASCULAR CONNECTIVE TISSUE TOWQRDS NECROTIC BONE. VASCULAR CONNECTIVE TISSUE TOWQRDS NECROTIC BONE.
THE CARTILAGE IS VIABLE NUTRITION IS THE CARTILAGE IS VIABLE NUTRITION IS
DERIVED FROM SYNOVIAL FLUID. DERIVED FROM SYNOVIAL FLUID. STAGE LAST STAGE LAST
6 MONTHS TO 1 YEAR.6 MONTHS TO 1 YEAR.


STAGE OF STAGE OF FRAGMENTATION OR FRAGMENTATION OR
REGENERATIONREGENERATION RADIOGRAPHIC FRAGMENTED APPEARANCE RADIOGRAPHIC FRAGMENTED APPEARANCE RESULTS MANY TOUNGE LIKE RESULTS MANY TOUNGE LIKE
SUBCHONDRAL FRACTURES OF NECROTIC SUBCHONDRAL FRACTURES OF NECROTIC BONE BONE MULTIPLE MINUTE MULTIPLE MINUTE TRABECULAR FRAGMENTS TRABECULAR FRAGMENTS COMPRESSED TOGETHER. CARTILAGE REMAINS COMPRESSED TOGETHER. CARTILAGE REMAINS NORMAL .NORMAL .
THE COUNTOR OF THE NEWLY FORMED SOFT THE COUNTOR OF THE NEWLY FORMED SOFT
BONE DEVELOPS IN RESPONSE TO THE BONE DEVELOPS IN RESPONSE TO THE EXTERNAL FORCES. EXTERNAL FORCES. STAGE EXTENTS OVER STAGE EXTENTS OVER 2-3 YEARS.2-3 YEARS.

HEALED OR RESIDUAL HEALED OR RESIDUAL STAGESTAGE
FORMATION OF NORMAL BONE ALONGSIDE FORMATION OF NORMAL BONE ALONGSIDE REPLACING SLOWLY RESORBING BONE. REPLACING SLOWLY RESORBING BONE. NEWLY FORMED BONE IS IMMATURE NEWLY FORMED BONE IS IMMATURE FORMED OF SLENDER TRABECULAE AND EASILY FORMED OF SLENDER TRABECULAE AND EASILY COMPRESSED TOGETHER WITH NECROTIC COMPRESSED TOGETHER WITH NECROTIC FRAGMENTSFRAGMENTS
THE COMPRESSION IS LIMITED THE COMPRESSION IS LIMITED ANTERIOR PORTION OF HEAD CREATING A ANTERIOR PORTION OF HEAD CREATING A CUP SHAPED DEFECT SEEN ON FROG CUP SHAPED DEFECT SEEN ON FROG LEG VIEW THE OSSIFIC NUCELUS LEG VIEW THE OSSIFIC NUCELUS ASSUMES A MUSHROOM SHAPED COUNTOR. ASSUMES A MUSHROOM SHAPED COUNTOR.

APPERANCE OF GREATER APPERANCE OF GREATER
TROCHANTERTROCHANTER :- IT BECOMES :- IT BECOMES
STRIKINLY LARGE IN SOME CASES. SINCE STRIKINLY LARGE IN SOME CASES. SINCE
LONGITUDINAL GROWTH OF THE FEMORAL LONGITUDINAL GROWTH OF THE FEMORAL
NECK MAY CEASE COMPLETELY AT 12 -14 NECK MAY CEASE COMPLETELY AT 12 -14
YEARS OF AGE , WHEREAS GROWTH OF THE YEARS OF AGE , WHEREAS GROWTH OF THE
GREATER TROCHANTER CONTINUES UNTILGREATER TROCHANTER CONTINUES UNTIL
17 -18 YEARS, A DISCERPANCY IN GROWTH 17 -18 YEARS, A DISCERPANCY IN GROWTH
NECK AND THE GREATER TROCHANTER NECK AND THE GREATER TROCHANTER
MAY RESULT.THE ELEVATION IMPAIRS THE MAY RESULT.THE ELEVATION IMPAIRS THE
POWER OF PELVITROCHANTERIC POWER OF PELVITROCHANTERIC
ABDUCTER MUSCLES, MANIFESTED BY ABDUCTER MUSCLES, MANIFESTED BY
POSITIVE TRENDELBERG SIGN.POSITIVE TRENDELBERG SIGN.

Avascular necrosisAvascular necrosis
Temporary cessation of growthTemporary cessation of growthOf epiphysisOf epiphysis PotentialPotentialRevascularisation from periphery PerthesRevascularisation from periphery Perthes
Resumption of ossificationResumption of ossification
Pathological fracturePathological fracture
Resorption of underlying boneResorption of underlying bone
Replacement by biologically TrueReplacement by biologically TruePlastic bone Perthes Plastic bone Perthes
SubluxationSubluxation
DeformityDeformity
CLINICAL FEATURESCLINICAL FEATURESSYMPTOMSSYMPTOMS
MOST CHILDERN PRESENT WITH MILD AND MOST CHILDERN PRESENT WITH MILD AND
INTERMITTENT PAIN IN THE THIGH OR A LIMP OR INTERMITTENT PAIN IN THE THIGH OR A LIMP OR
BOTH.BOTH.
THE ONSET OF PAIN MAY BE ACUTE OR INSIDIOUS THE ONSET OF PAIN MAY BE ACUTE OR INSIDIOUS
THE CLASSICAL PRESENTATION IS DESCRIBED AS A THE CLASSICAL PRESENTATION IS DESCRIBED AS A
“PAINLES LIMP” THE CHILD LIMPS BUT DOES NOT “PAINLES LIMP” THE CHILD LIMPS BUT DOES NOT
COMPLAINS OF DISCOMFORT.COMPLAINS OF DISCOMFORT.
PAIN IS AGRRAVATED BY MOVEMENT OF HIP AND PAIN IS AGRRAVATED BY MOVEMENT OF HIP AND
RELIVED BY REST.RELIVED BY REST.
H/O OF TRAUMA USUALLY A MILD IS PRESENTH/O OF TRAUMA USUALLY A MILD IS PRESENT..
EXAMINATION:-EXAMINATION:- ANTALGIC GAIT ANTALGIC GAIT
MUSCLE SPASM SECONDARY TO IRRITABLE HIP.MUSCLE SPASM SECONDARY TO IRRITABLE HIP.
LIMITATION OF ABDUCTION AND INTERNAL LIMITATION OF ABDUCTION AND INTERNAL
ROTATIONROTATION
FFD IS PRESENTFFD IS PRESENT
AXIS DEVIATION IS PRESENT due to central collapse AXIS DEVIATION IS PRESENT due to central collapse
DIFFERENTIAL ROTATION .DIFFERENTIAL ROTATION .
TRENDELENBERG TEST POSITIVE TRENDELENBERG TEST POSITIVE

InvestigationInvestigation
X-Ray –AP & Frog leg Lat viewX-Ray –AP & Frog leg Lat viewUSGUSGArthrographyArthrographyBone ScanBone ScanCTCTMRIMRI
RADIOGRAPHIC STAGESRADIOGRAPHIC STAGES
FOUR WALDENSTROM STAGES:FOUR WALDENSTROM STAGES:
1) INITIAL STAGE1) INITIAL STAGE
2) FRAGMENTATION STAGE2) FRAGMENTATION STAGE
3) REOSSIFICATION STAGE3) REOSSIFICATION STAGE
4) HEALED STAGE4) HEALED STAGE

INITIAL STAGEINITIAL STAGE EARLY RADIOGRAPHIC EARLY RADIOGRAPHIC
SIGNS:SIGNS: FAILURE OF FEMORAL FAILURE OF FEMORAL
OSSIFIC OSSIFIC NUCLEUS TO GROWNUCLEUS TO GROW
WIDENING OF MEDIAL WIDENING OF MEDIAL JOINT SPACEJOINT SPACE
““CRESCENT SIGN”CRESCENT SIGN” IRREGULAR PHYSEAL IRREGULAR PHYSEAL
PLATEPLATE BLURRY/ RADIOLUCENT BLURRY/ RADIOLUCENT
METAPHYSISMETAPHYSIS

X-RayX-Ray Cresent Sign or Cresent Sign or
Salters sign or Salters sign or Caffey’s signCaffey’s sign
FRAGMENTATION STAGEFRAGMENTATION STAGE
BONY EPIPHYSIS BONY EPIPHYSIS BEGINS TO BEGINS TO FRAGMENTFRAGMENT
AREAS OF AREAS OF INCREASED INCREASED LUCENCY AND LUCENCY AND DENSITYDENSITY
EVIDENCE OF EVIDENCE OF REPAIR ASPECTS REPAIR ASPECTS OF DISEASEOF DISEASE

X-RayX-Ray Fragmentation of Fragmentation of
epiphysisepiphysis

REOSSIFICATION STAGEREOSSIFICATION STAGE
NORMAL BONE NORMAL BONE DENSITY RETURNSDENSITY RETURNS
ALTERATIONS IN ALTERATIONS IN SHAPE OF FEMORAL SHAPE OF FEMORAL HEAD AND NECK HEAD AND NECK EVIDENTEVIDENT

X-RayX-Ray
Metaphyseal Metaphyseal widening and cystic widening and cystic changes in femoral changes in femoral neckneck

X-RayX-Ray Lateral extrusion of Lateral extrusion of
femoral head and femoral head and changes in changes in acetabulum.acetabulum.
X-RayX-Ray
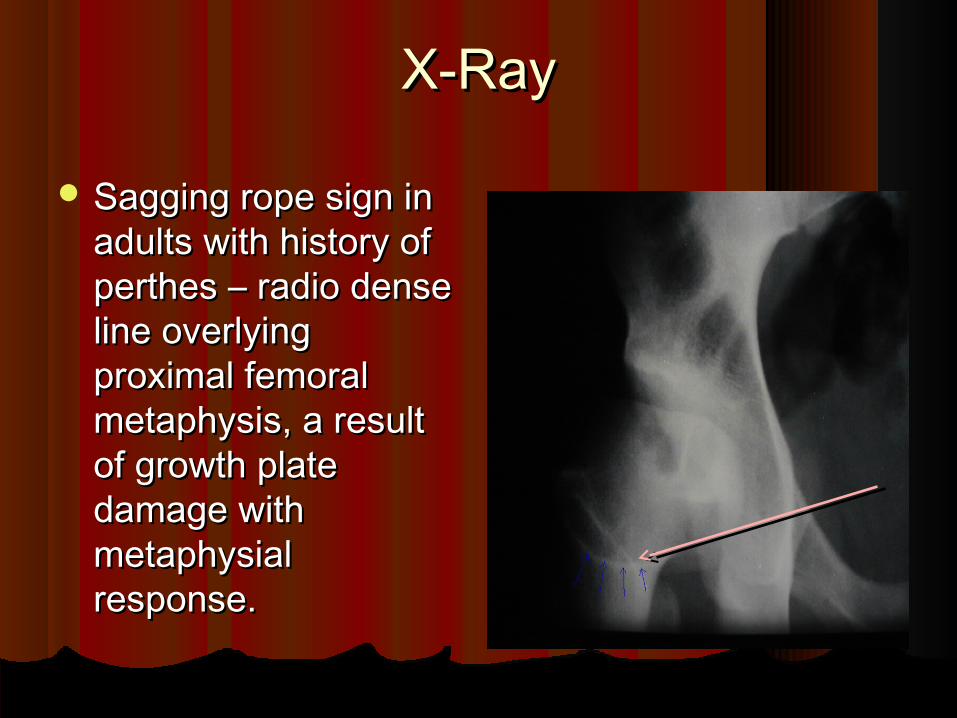
Sagging rope sign in Sagging rope sign in adults with history of adults with history of perthes – radio dense perthes – radio dense line overlying line overlying proximal femoral proximal femoral metaphysis, a result metaphysis, a result of growth plate of growth plate damage with damage with metaphysial metaphysial response.response.
ArthrographyArthrography
Indicated to know the contour of head Indicated to know the contour of head and congruity of articular surface and congruity of articular surface
Shows the configuration of the femoral Shows the configuration of the femoral head and its relation with the acetabulum.head and its relation with the acetabulum.
Provides reliable information regarding Provides reliable information regarding containment.containment.
We can assess congruity of hip in many We can assess congruity of hip in many different positions.different positions.
Not routinely used .Not routinely used .

Bone ScanBone Scan
Indicated to diagnose in early stages and Indicated to diagnose in early stages and to classify the severity.to classify the severity.
Diagnosis possible months before signs Diagnosis possible months before signs appear on X-Ray.appear on X-Ray.
Avascular areas show cold spots.Avascular areas show cold spots.Revascularisation can be detected much Revascularisation can be detected much
before radiographic evidence.before radiographic evidence.
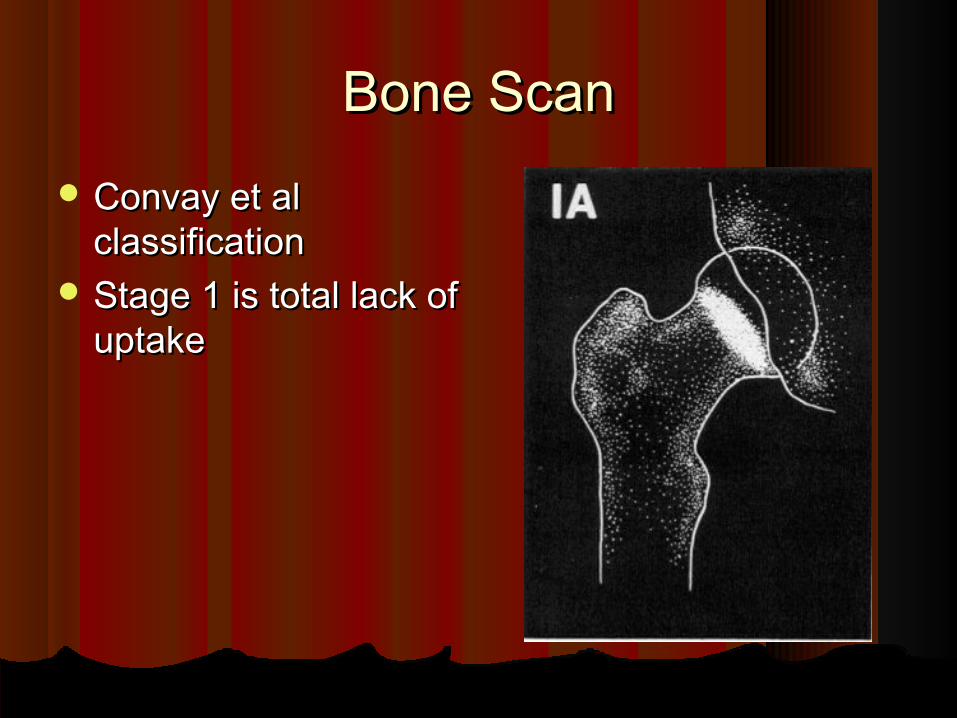
Bone ScanBone Scan Convay et al Convay et al
classificationclassification Stage 1 is total lack of Stage 1 is total lack of
uptakeuptake

Bone ScanBone Scan Revascularisation at Revascularisation at
lateral columnlateral column Failure to revascularise Failure to revascularise
at lat column is a grave at lat column is a grave signsign
Also called “scintigraphic Also called “scintigraphic head at risk sign”head at risk sign”
Precedes radiographic Precedes radiographic head at risk sign by 2-3 head at risk sign by 2-3 mthsmths
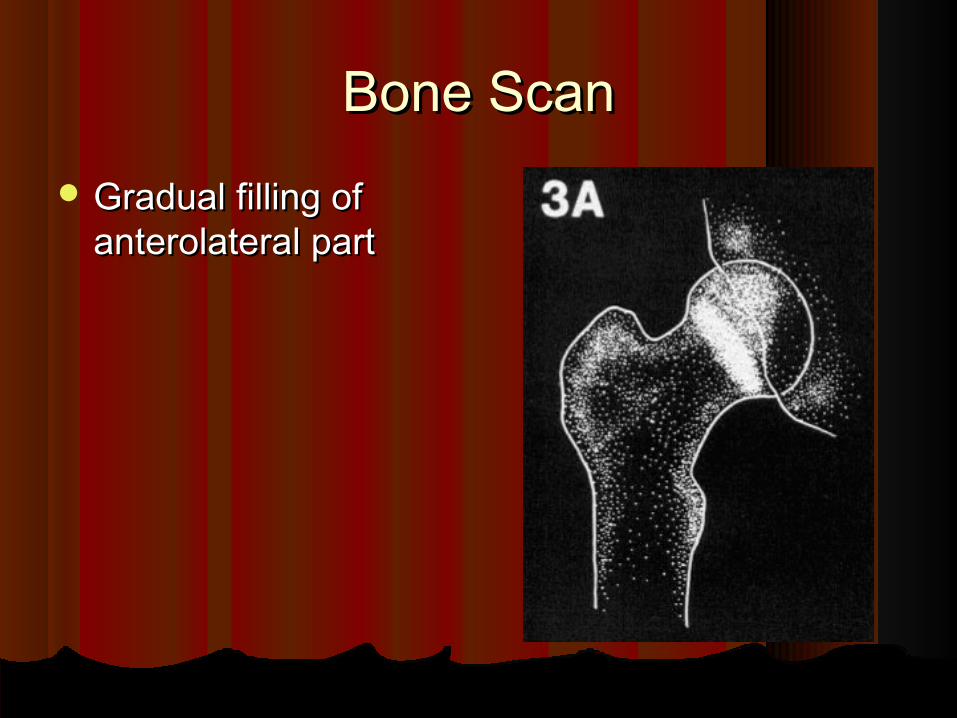
Bone ScanBone Scan Gradual filling of Gradual filling of
anterolateral partanterolateral part

Bone ScanBone Scan Return to normalReturn to normal

MRIMRI
Accurate in early diagnosis.Accurate in early diagnosis.Shows congruity, containment, synovial Shows congruity, containment, synovial
hypertrophy well.hypertrophy well.Subtraction MRI shows ischemia as well Subtraction MRI shows ischemia as well
as scintigraphy and also allows early as scintigraphy and also allows early recognition of reperfusion.recognition of reperfusion.

ClassificationClassification
Waldenstroms classification.Waldenstroms classification.Catterall classification. Catterall classification. Salter classificationSalter classificationHerrings lateral pillar classification.Herrings lateral pillar classification.Modified Elizabethtown classification.Modified Elizabethtown classification.

Waldenstroms classificationWaldenstroms classification
1.1. Incipient stage – 1-3 wksIncipient stage – 1-3 wks2.2. Avascular stage – upto 1 yrAvascular stage – upto 1 yr3.3. Regenerative stage Regenerative stage 4.4. Residual stageResidual stage Not scientifically valid.Not scientifically valid.
Catterall classification (1971)Catterall classification (1971) I – only anterior portion of epiphysis I – only anterior portion of epiphysis affected.affected. II – anterior segment involved central II – anterior segment involved central sequestrum presentsequestrum present III – most of epiphysis sequestered withIII – most of epiphysis sequestered with unaffected portions located medial unaffected portions located medial and lateral to central segmentand lateral to central segment IV – all of epiphysis sequestered.IV – all of epiphysis sequestered.
Catterall described head at risk factors to Catterall described head at risk factors to predict prognosis:predict prognosis:
1- lat. subluxation of femoral head1- lat. subluxation of femoral head3- Calcification lat. to epiphysis3- Calcification lat. to epiphysis4- Horizontal physeal line4- Horizontal physeal line5- gage sign5- gage sign6- exetensive metaphyseal involvement6- exetensive metaphyseal involvement

Gage’s signGage’s sign Rarefaction in the Rarefaction in the
lateral part of the lateral part of the epiphysis and epiphysis and subjacent subjacent metaphysis.metaphysis.
Salter ClassificationSalter Classification
Type A = I & II CatterallType A = I & II CatterallType B = III & IV Catterall.Type B = III & IV Catterall.

Herring Lat PillarHerring Lat Pillar Group-A hips are defined as those with no Group-A hips are defined as those with no
involvement of the lateral pillar, with no density involvement of the lateral pillar, with no density changes and no loss of height of the lateral pillarchanges and no loss of height of the lateral pillar
Group-B hips have lucency in the lateral pillar Group-B hips have lucency in the lateral pillar and may have some loss of height , but not and may have some loss of height , but not exceeding 50% of the original height.exceeding 50% of the original height.
Group-C hips are those with more lucency in the Group-C hips are those with more lucency in the lateral pillar and >50% loss of heightlateral pillar and >50% loss of height

Lateral Pillar group ALateral Pillar group A
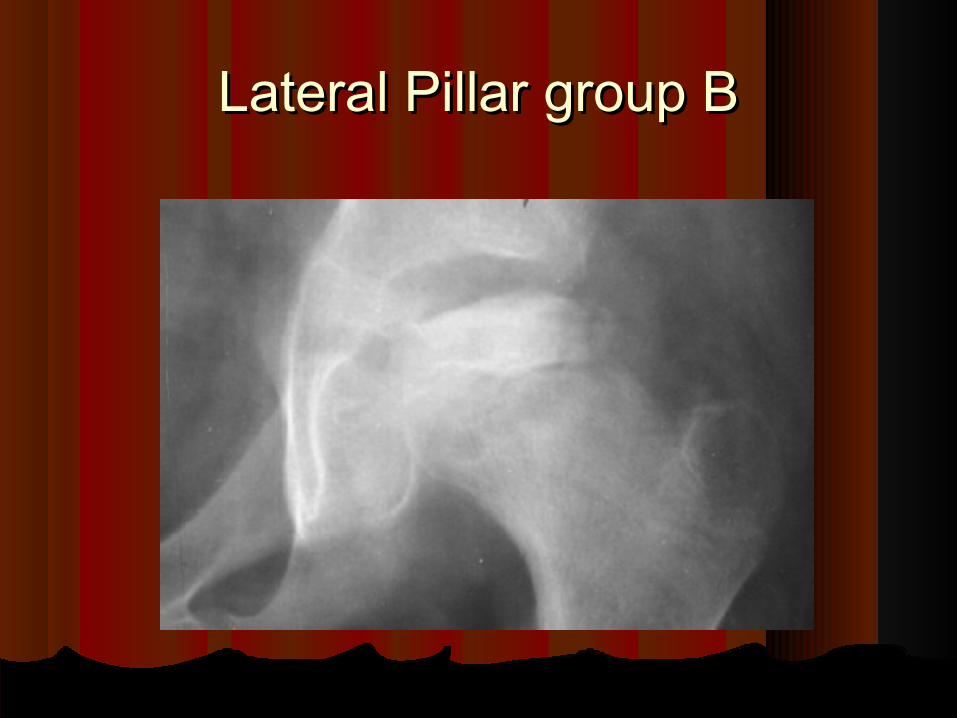
Lateral Pillar group BLateral Pillar group B

Lateral Pillar group CLateral Pillar group C
Modified Elizabethtown Modified Elizabethtown classificationclassification
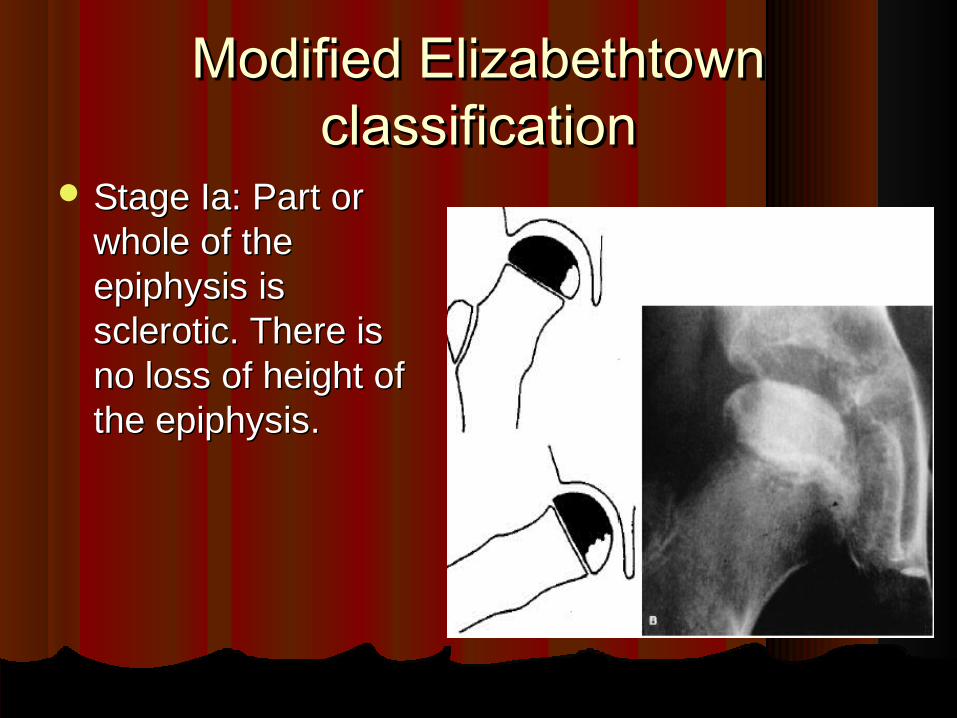
Stage Ia: Part or Stage Ia: Part or whole of the whole of the epiphysis is epiphysis is sclerotic. There is sclerotic. There is no loss of height of no loss of height of the epiphysis.the epiphysis.

Modified Elizabethtown Modified Elizabethtown classificationclassification
Stage Ib: The Stage Ib: The epiphysis is epiphysis is sclerotic and sclerotic and there is loss of there is loss of epiphyseal epiphyseal height. There is height. There is no evidence of no evidence of fragmentation of fragmentation of the epiphysis.the epiphysis.
Modified Elizabethtown Modified Elizabethtown classificationclassification
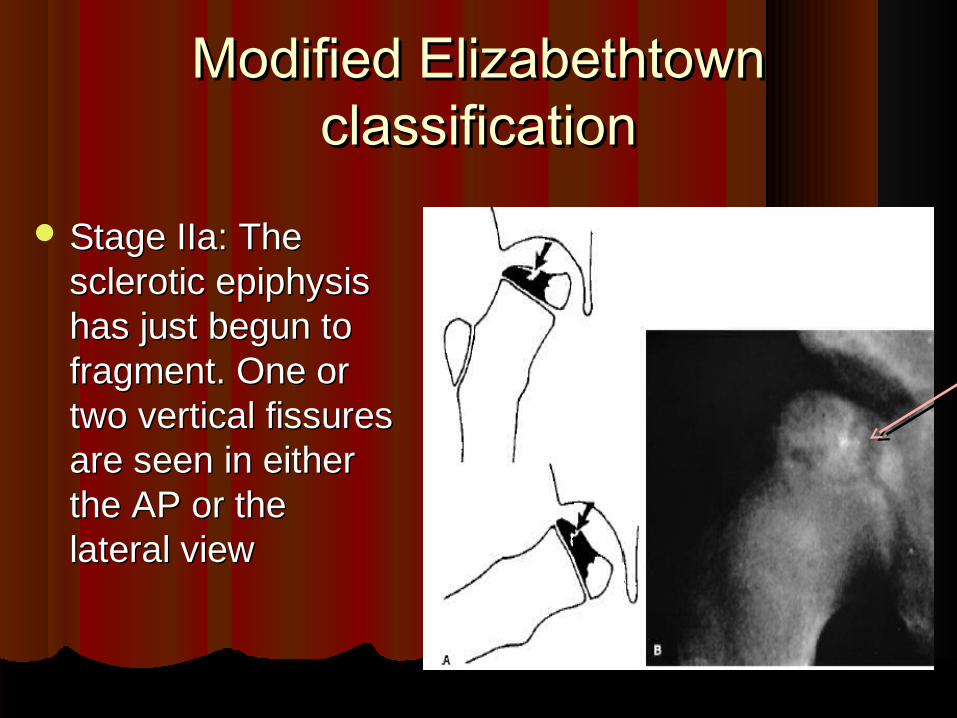
Stage IIa: The Stage IIa: The sclerotic epiphysis sclerotic epiphysis has just begun to has just begun to fragment. One or fragment. One or two vertical fissures two vertical fissures are seen in either are seen in either the AP or the the AP or the lateral viewlateral view

Modified Elizabethtown Modified Elizabethtown classificationclassification
Stage IIb: Stage IIb: Fragmentation is Fragmentation is advanced. No new advanced. No new bone is visible bone is visible lateral to the lateral to the fragmented fragmented epiphysis.epiphysis.
Modified Elizabethtown Modified Elizabethtown classificationclassification
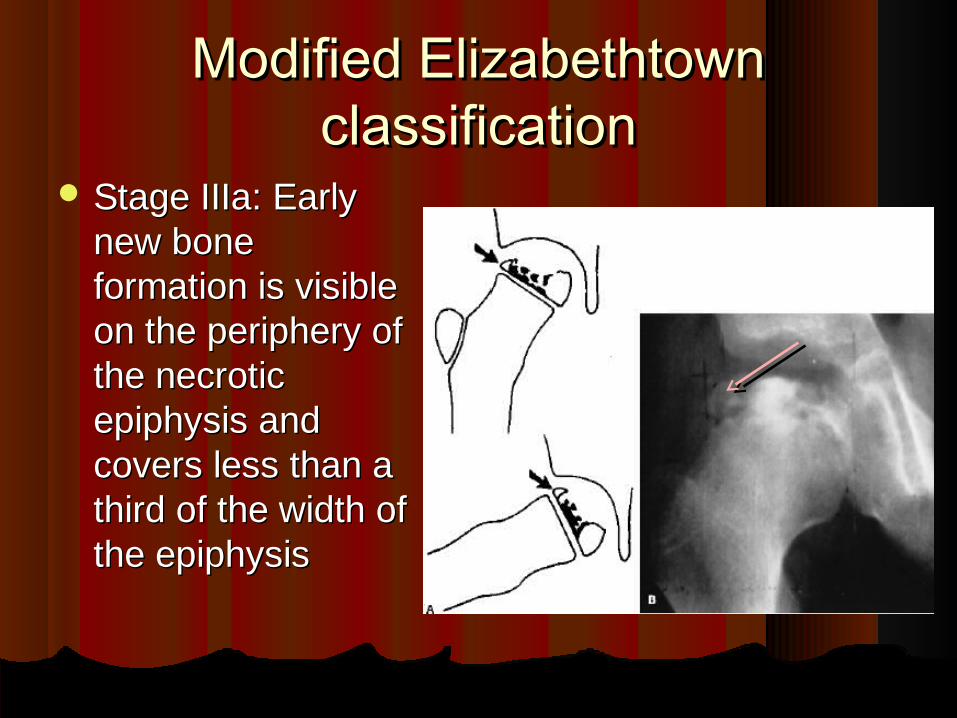
Stage IIIa: Early Stage IIIa: Early new bone new bone formation is visible formation is visible on the periphery of on the periphery of the necrotic the necrotic epiphysis and epiphysis and covers less than a covers less than a third of the width of third of the width of the epiphysisthe epiphysis

Modified Elizabethtown Modified Elizabethtown classificationclassification
Stage IIIb: The Stage IIIb: The new bone is of new bone is of normal texture normal texture and has grown and has grown over a third of the over a third of the width of the width of the epiphysis.epiphysis.

Modified Elizabethtown Modified Elizabethtown classificationclassification
Stage IV the healing is complete and there is Stage IV the healing is complete and there is no radiologically identifiable avascular bone.no radiologically identifiable avascular bone.

Prognostic FactorsPrognostic Factors1.1. Age at diagnosisAge at diagnosis2.2. Extent of involvementExtent of involvement3.3. SexSex4.4. Catterall “head at risk” clinical signsCatterall “head at risk” clinical signs
ClinicalClinical1.1. Progressive loss of hip motionProgressive loss of hip motion2.2. Increasing abduction contractureIncreasing abduction contracture3.3. Obese childObese child

Classification of PrognosisClassification of PrognosisUniplanar methodsUniplanar methods - CE angle of Weiberg.- CE angle of Weiberg. - Salters extrusion Index.- Salters extrusion Index. - Epiphyseal index.- Epiphyseal index. - Epiphyseal quotient. - Epiphyseal quotient. Biplanar methodsBiplanar methods - Stulberg classification.- Stulberg classification.

CE angle of WeibergCE angle of Weiberg Indicator of acetabular depth It is Indicator of acetabular depth It is
the angle formed by a the angle formed by a perpendicular lines through the perpendicular lines through the midportion of the femoral head midportion of the femoral head and a line from the femoral head and a line from the femoral head center to the upper outer center to the upper outer acetabular margin. acetabular margin.
Normal = 20 to 40 degrees, with Normal = 20 to 40 degrees, with an average of 36 degrees. an average of 36 degrees.
This angle may be slightly larger This angle may be slightly larger in women and in older persons.in women and in older persons.
Angle >25 = good, 20-25= fair, < Angle >25 = good, 20-25= fair, < 20 = poor20 = poor

Salters extrusion IndexSalters extrusion Index If AB is more If AB is more
than 20% of CD than 20% of CD it indicates a it indicates a poor prognosis poor prognosis
Epiphyseal index & quotientEpiphyseal index & quotientEpiphyseal index = greatest height of the Epiphyseal index = greatest height of the
epiphysis divided by its width.epiphysis divided by its width.
Epiphyseal quotient = Epiphyseal index of Epiphyseal quotient = Epiphyseal index of involved hip divided by the index for involved hip divided by the index for uninvolved hip.uninvolved hip.
>0.6 = good>0.6 = good 0.4-0.6 = fair0.4-0.6 = fair <0.4 = poor<0.4 = poor
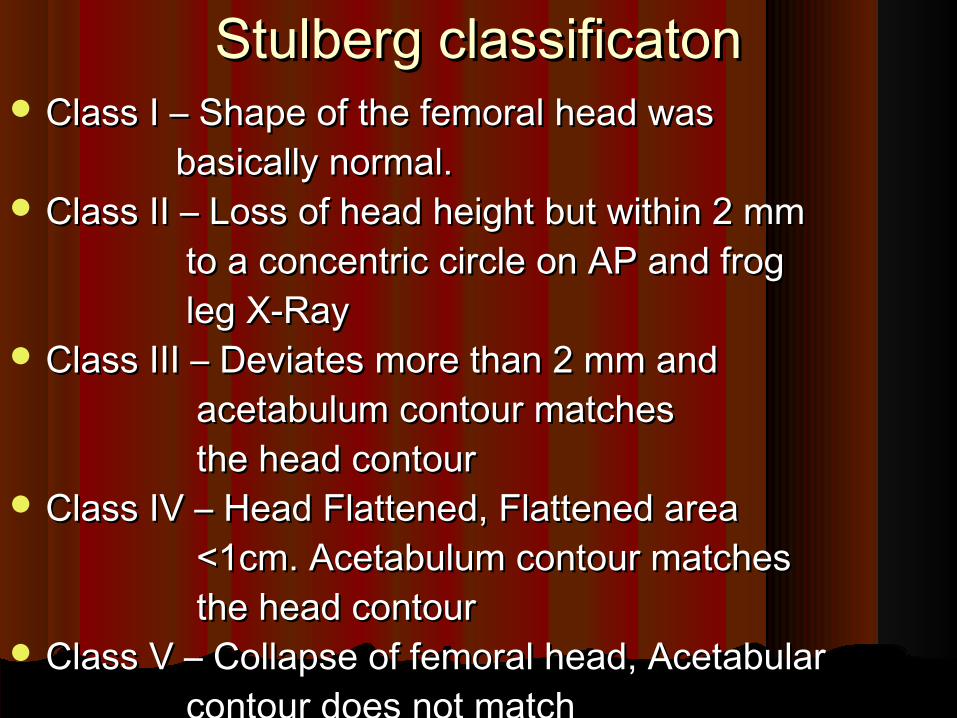
Stulberg classificatonStulberg classificaton Class I – Shape of the femoral head wasClass I – Shape of the femoral head was basically normal.basically normal. Class II – Loss of head height but within 2 mmClass II – Loss of head height but within 2 mm to a concentric circle on AP and frogto a concentric circle on AP and frog leg X-Rayleg X-Ray Class III – Deviates more than 2 mm andClass III – Deviates more than 2 mm and acetabulum contour matchesacetabulum contour matches the head contourthe head contour Class IV – Head Flattened, Flattened area Class IV – Head Flattened, Flattened area <1cm. Acetabulum contour matches<1cm. Acetabulum contour matches the head contourthe head contour Class V – Collapse of femoral head, AcetabularClass V – Collapse of femoral head, Acetabular contour does not matchcontour does not match

Stulberg classificatonStulberg classificaton Class I Class I
Shape of Shape of the femoral the femoral head is head is basically basically normal.normal.

Stulberg classificatonStulberg classificaton Class II Class II
Loss of Loss of head head height but height but within 2 within 2 mmmm

Stulberg classificatonStulberg classificaton Class III Class III
Deviates Deviates more than more than 2 mm 2 mm

Stulberg classificatonStulberg classificaton Class IV Class IV
Head Head FlattenedFlattened

Stulberg classificatonStulberg classificaton Class V Class V
Collapse of Collapse of femoral femoral head, head, Acetabular Acetabular contour contour does not does not change and change and not matchenot matche

Differential diagnosisDifferential diagnosis
Tuberculosis of the hipTuberculosis of the hipSCFESCFETransient synovitisTransient synovitisSpondylodysplasiaSpondylodysplasiaAVN due to leukemia, lymphoma, AVN due to leukemia, lymphoma,
gauchers disease, Hemoglobinopathies gauchers disease, Hemoglobinopathies etcetc

TreatmentTreatmentObjectivesObjectives - To produce a normal femoral - To produce a normal femoral head and neckhead and neck - To produce a normal acetabulum- To produce a normal acetabulum - A congruous hip which is fully - A congruous hip which is fully mobilemobile - To prevent degenerative arthritis - To prevent degenerative arthritis of the hip later in lifeof the hip later in life

TreatmentTreatmentGOAL :GOAL :Treatment efforts are directed towardsTreatment efforts are directed towards - Restoration and maintenance of - Restoration and maintenance of full mobility of the hipfull mobility of the hip - Containment of the femoral- Containment of the femoral head.head. - Resumption of weight bearing- Resumption of weight bearing and full activity as soon as and full activity as soon as possiblepossible

TreatmentTreatment
Caterall group 1 andCaterall group 1 and
group 2 ( < 7 years)group 2 ( < 7 years) No activeNo active Herring group 1 &Herring group 1 & TreatmentTreatment
group 2 (< 6 years)group 2 (< 6 years)

TreatmentTreatmentTreatment is divided into 3 phasesTreatment is divided into 3 phases
Initial Phase – restore & maintain mobilityInitial Phase – restore & maintain mobility
Active Phase – Containment and Active Phase – Containment and maintainance of full mobility.maintainance of full mobility.
Reconstructive phase – correct residual Reconstructive phase – correct residual deformities.deformities.
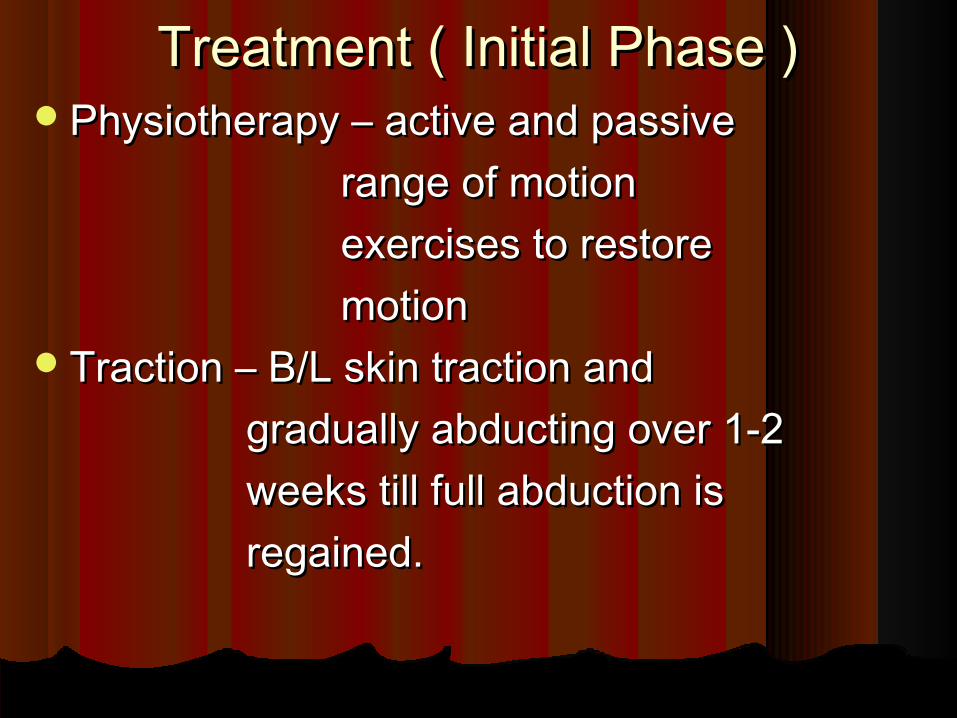
Treatment ( Initial Phase )Treatment ( Initial Phase )Physiotherapy – active and passive Physiotherapy – active and passive range of motionrange of motion exercises to restoreexercises to restore motionmotionTraction – B/L skin traction and Traction – B/L skin traction and gradually abducting over 1-2 gradually abducting over 1-2 weeks till full abduction isweeks till full abduction is regained.regained.

Treatment ( Active Phase )Treatment ( Active Phase )
Consists of containment of the femoral Consists of containment of the femoral head within the acetabulum. This can be head within the acetabulum. This can be achieved by achieved by
orthosis orthosis or byor by surgerysurgery

Treatment (Orthosis)Treatment (Orthosis) Non Ambulatory weight releivingNon Ambulatory weight releiving
1.1. Abduction broomstick plaster castAbduction broomstick plaster cast2.2. Hip spica castHip spica cast3.3. Milgram hip abduction orthosisMilgram hip abduction orthosis
Ambulatory Both limbs includedAmbulatory Both limbs included1.1. Petrie Abduction castPetrie Abduction cast2.2. Toronto orthosisToronto orthosis3.3. Newington orthosisNewington orthosis4.4. Birmingham braceBirmingham brace5.5. Atlanta Scotish Rite Brace Atlanta Scotish Rite Brace
Ambulatory unilateralAmbulatory unilateral1.1. Tachdjian trilateral socket orthosisTachdjian trilateral socket orthosis

Treatment (Orthosis)Treatment (Orthosis) Atlanta Scotish Rite Atlanta Scotish Rite
BraceBrace

Atlanta Scotish Rite BraceAtlanta Scotish Rite Brace

Newington orthosisNewington orthosis
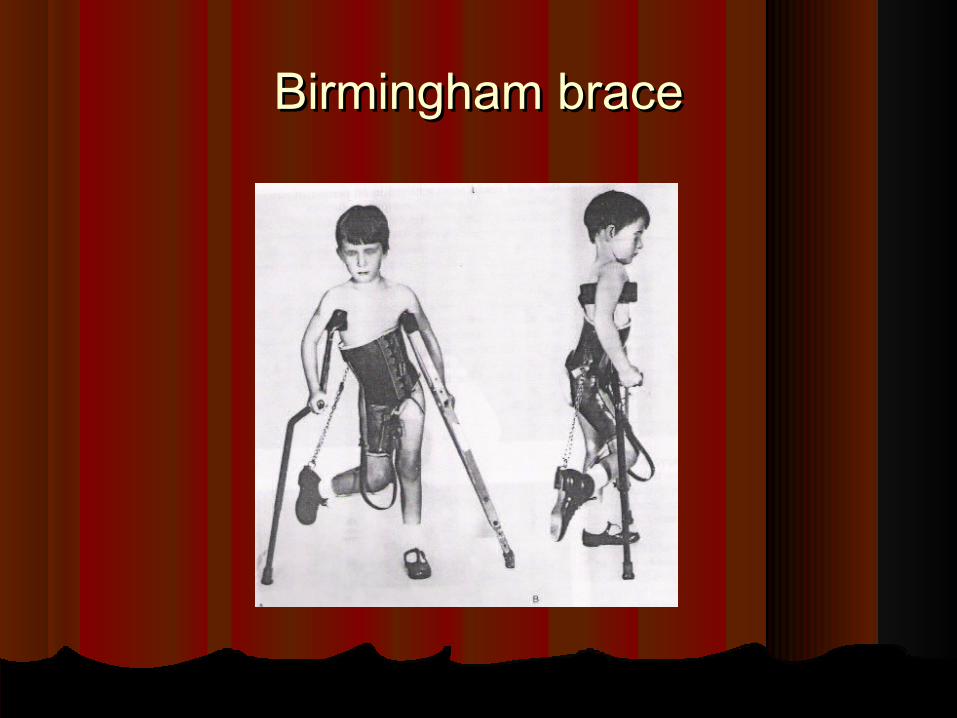
Birmingham braceBirmingham brace

Toronto BraceToronto Brace
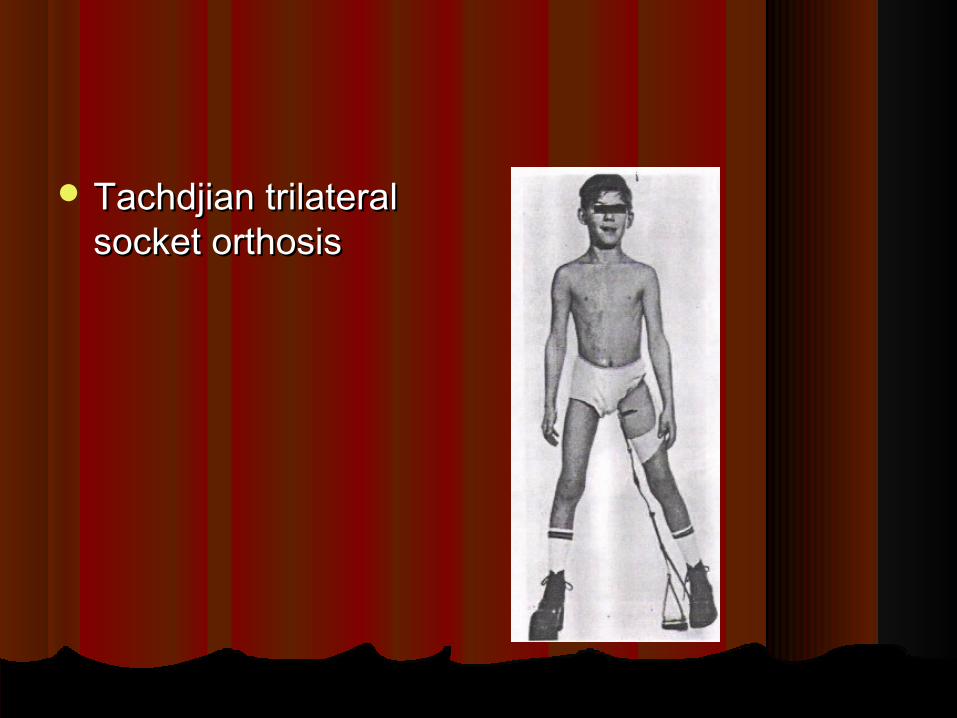
Tachdjian trilateral Tachdjian trilateral socket orthosissocket orthosis

Treatment (Orthosis)Treatment (Orthosis) Orthotic treatment is discontinued when the Orthotic treatment is discontinued when the
disease enters the reparative phase and healing disease enters the reparative phase and healing is established.is established.
The radiographic evidence of healing areThe radiographic evidence of healing are1.1. Appearance of regular ossification in the Appearance of regular ossification in the
femoral head.femoral head.2.2. Increased density of femoral head should Increased density of femoral head should
disappear.disappear.3.3. Metaphyseal rarefaction involving the lateral Metaphyseal rarefaction involving the lateral
cortex of the metaphysis should ossify.cortex of the metaphysis should ossify.4.4. There should be intact lateral column.There should be intact lateral column.5.5. There should be normal trabecular bone in the There should be normal trabecular bone in the
epiphysis.epiphysis.

Treatment ( Surgical)Treatment ( Surgical)Femoral varus osteotomy.Femoral varus osteotomy. Inominate osteotomy.Inominate osteotomy.Combined femoral and inominate Combined femoral and inominate
osteotomyosteotomyValgus osteotomyValgus osteotomyShelf arthroplastyShelf arthroplastyChiari osteotomyChiari osteotomyCheilectomy.Cheilectomy.Trochanteric advancement or arrest.Trochanteric advancement or arrest.

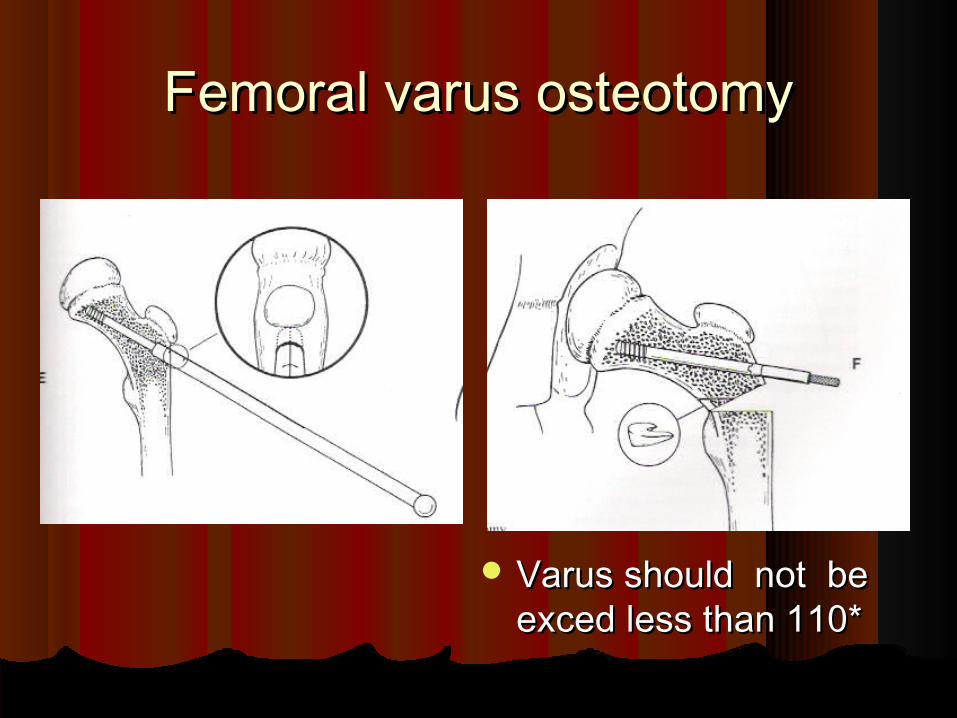
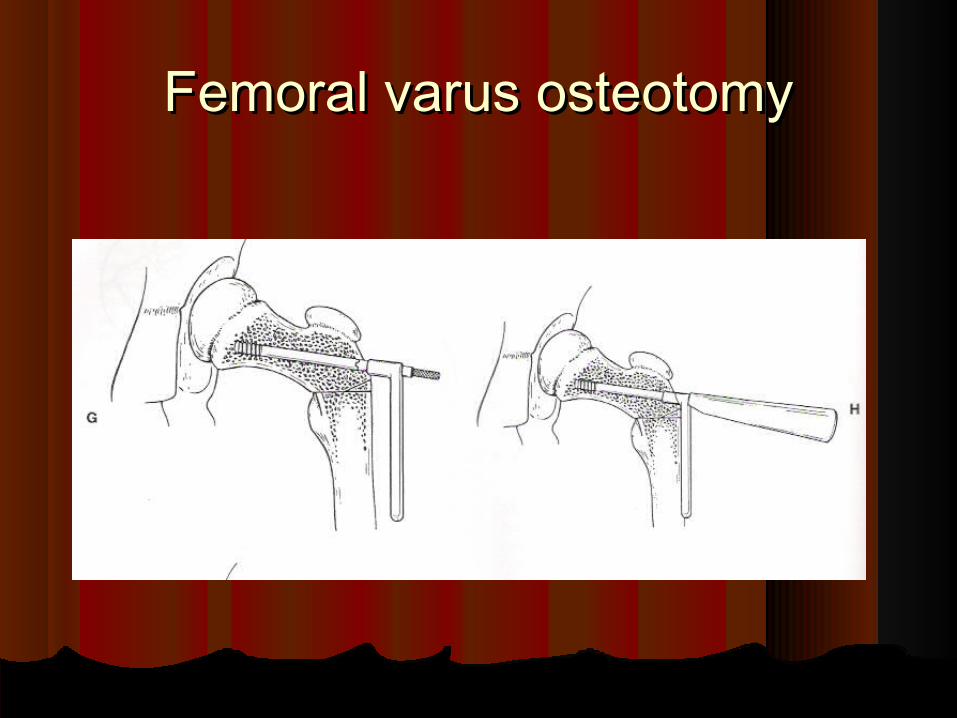
Femoral varus osteotomyFemoral varus osteotomy
IndicationsIndications: 1.>6yrs of age: 1.>6yrs of age 2.hip with normal or near normal 2.hip with normal or near normal hiphipComplicationsComplications:1.excessive post op varus:1.excessive post op varus2.Persistant ext.rotation2.Persistant ext.rotation3.Shortening of extremity3.Shortening of extremity4.Incresed abductor lurch4.Incresed abductor lurch5.Trochanteric over growth5.Trochanteric over growth6.Delayed or non union6.Delayed or non union

Femoral varus osteotomyFemoral varus osteotomy

Femoral varus osteotomyFemoral varus osteotomy
Femoral varus osteotomyFemoral varus osteotomy
Varus should not be Varus should not be exced less than 110* exced less than 110*
Femoral varus osteotomyFemoral varus osteotomy

Femoral varus osteotomyFemoral varus osteotomy

Femoral varus osteotomyFemoral varus osteotomy
Inominate osteotomyInominate osteotomy IndicationsIndications::1.>6 yrs1.>6 yrs2.mod. Or severely affected head with loss of 2.mod. Or severely affected head with loss of
containmentcontainment
RequirementRequirement::Able to abduct 45 deg. And femoral head to be Able to abduct 45 deg. And femoral head to be
contained in positioncontained in position
ComplicationsComplications :loss of fixation, leg-lengthening ,dec. hip :loss of fixation, leg-lengthening ,dec. hip flx. And jt.stiffness, second procedure for k wire flx. And jt.stiffness, second procedure for k wire remavalremaval



Valgus OsteotomyValgus Osteotomy
Indication:hinged Indication:hinged abduction of hipabduction of hip
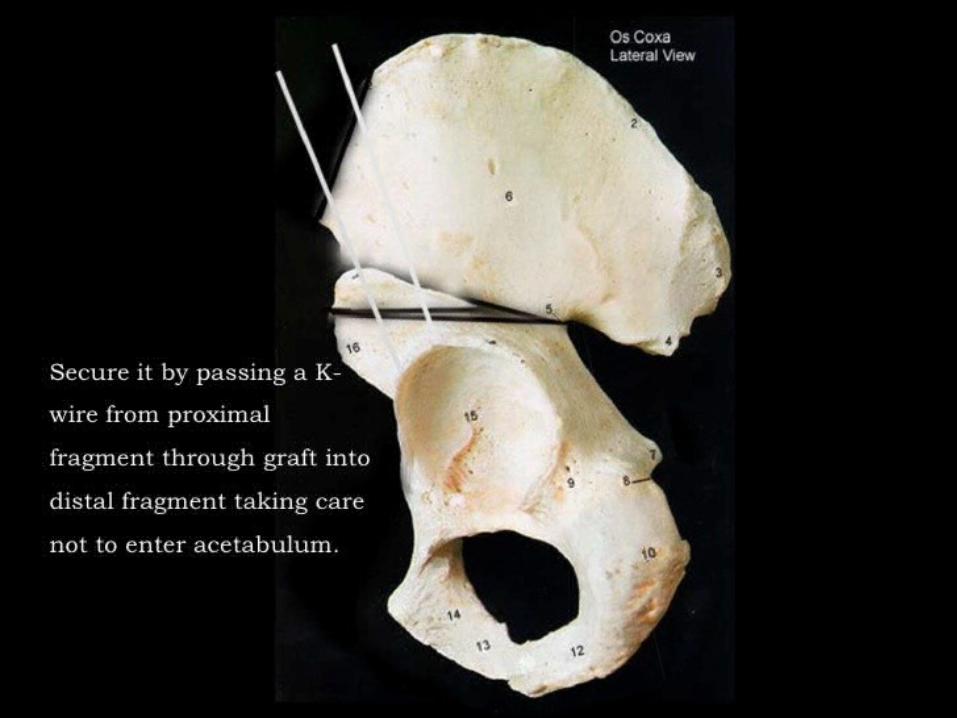
Shelf ArthroplastyShelf Arthroplasty
Performed to enlarge the volume of Performed to enlarge the volume of acetabulum.acetabulum.
Indication:A deficient acetabulum cannot Indication:A deficient acetabulum cannot be corrected by pelvic osteotomybe corrected by pelvic osteotomy
Contra indication: Dysplastic hip with Contra indication: Dysplastic hip with spherical congruity spherical congruity

Shelf ArthroplastyShelf Arthroplasty

Chiari osteotomyChiari osteotomy Capsular interpositional Capsular interpositional
arthroplastyarthroplasty
Deepens the deficient Deepens the deficient acetabulum by medial acetabulum by medial displacement of distal displacement of distal pelvic fragment and pelvic fragment and improves sup.lat.femoral improves sup.lat.femoral coverage.coverage.
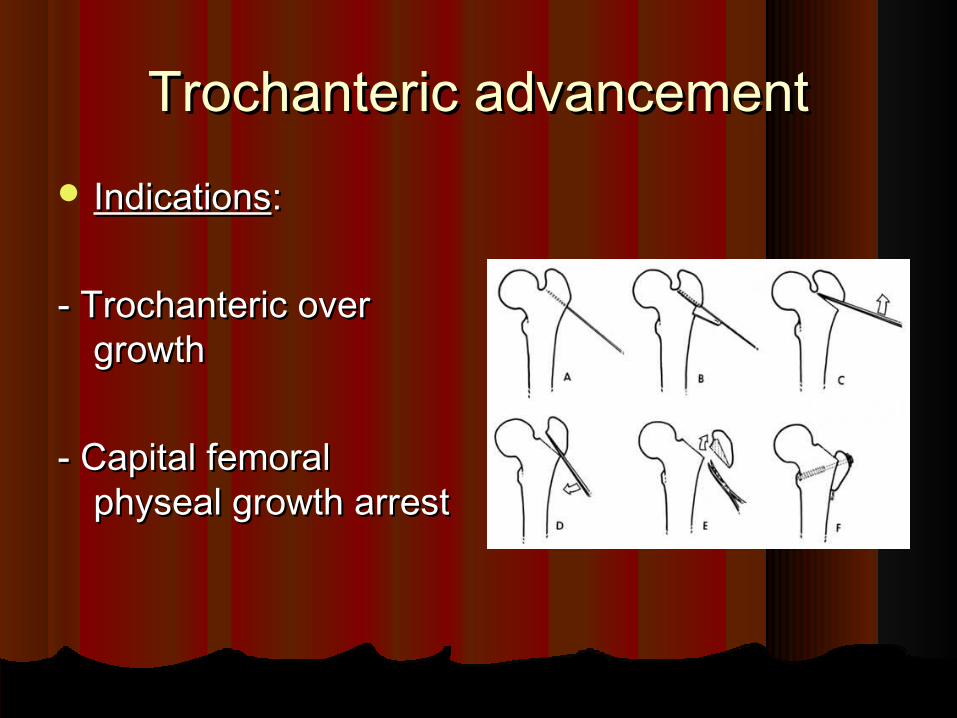
Trochanteric advancementTrochanteric advancement IndicationsIndications::
- Trochanteric over - Trochanteric over growthgrowth
- Capital femoral - Capital femoral physeal growth arrestphyseal growth arrest
Recommended Indications for diff. Recommended Indications for diff. surgeriessurgeries
Hinged abduction - valgus subtrochanteric Hinged abduction - valgus subtrochanteric osteotomyosteotomy
Severly Mal formed femoral head – Severly Mal formed femoral head – cheilectomycheilectomy
Coxa magna – shelf augmentationCoxa magna – shelf augmentationA large malformed femoral head with A large malformed femoral head with
lat.subluxation – Chiari’s pelvic osteotomylat.subluxation – Chiari’s pelvic osteotomyCapital femoral physeal arrest – Capital femoral physeal arrest –
Trochanteric advancementTrochanteric advancement


Recent AdvancesRecent Advances
AnticoagulantAnticoagulantBotulinum toxinBotulinum toxin Ibadronate :this has shown there Ibadronate :this has shown there
importance in rat model by increase importance in rat model by increase spericity of femoral headspericity of femoral head
Still lot more work to do in this fieldsStill lot more work to do in this fields

References References
Campbell’s operative Orthopaedics – 10Campbell’s operative Orthopaedics – 10 thth editionedition
Tachdjian’s paediatric orthopaedics – 3Tachdjian’s paediatric orthopaedics – 3 rdrd editionedition
Mercer’s Orthopaedic surgery – 9Mercer’s Orthopaedic surgery – 9 thth edition editionJournals of bone and joint surgeryJournals of bone and joint surgery InternetInternet

Thank you for your patient l istening





























![The acetabulum in Perthes’ disease: a prospective study of 123 … · 2017. 4. 6. · Perthes’ disease leads to typical anatomic changes of the femoral head [1–3]. In 1950,](https://img.dokumen.tips/doc/110x75/5ff8d15fc672a5217871fc27/the-acetabulum-in-perthesa-disease-a-prospective-study-of-123-2017-4-6-perthesa.jpg)