Embed Size (px)
Citation preview
PERINATAL ASPHYXIA (HYPOXIC ISCHEMIC (ENCEPHALOPATHYDR. TAI AL AKAWY
Perinatal asphyxia
Perinatal asphyxia, more appropriately known as hypoxic-ischemic encephalopathy, is characterized by clinical and laboratory evidence of acute or subacute brain injury due to asphyxia.
The primary causes of this condition are systemic hypoxemia and/or reduced cerebral blood flow (CBF).
Birth asphyxia causes 23% of all neonatal deaths worldwide.
Severe hypoxia results in anaerobic glycolysis and lactic acid production first in the peripheral tissues (muscle and heart) and then in the brain.
Ischemia (lack of sufficient blood flow to all or part of an organ) is both a cause and a result of hypoxia.
Hypoxia and acidosis can depress myocardial function, leading to hypotension and ischemia.
Ischemia can impair oxygen delivery, causing further compromise, as well as disrupt delivery of substrate and removal of metabolic and respiratory by-products (eg, lactic acid, carbon dioxide).
TIMING OF INJURY
Asphyxia can occur before, during, or after birth. Based on a review of multiple studies that have examined the temporal relationship of obstetric events and neonatal outcomes, predominantly HIE in term infants, the proportion of conditions that occurs in each time period can be estimated
Antepartum events, such as maternal hypotension or trauma, account for 4 to 20 percent of cases.
Intrapartum events, such as placental abruption or umbilical cord prolapse, are seen in 56 to 80 percent.
In approximately 10 percent of cases, a postnatal insult occurs, usually caused by severe cardiopulmonary abnormalities or associated with prematurity.
However, the timing of injury often is difficult to establish for an individual infant
Neonatal encephalopathy is a heterogeneous syndrome characterized by signs of central nervous system dysfunction in newborn infants

Clinical suspicion of neonatal encephalopathy should be considered in any newborn exhibiting an abnormal level of consciousness, seizures, tone and reflex abnormalities, apnea, aspiration and feeding difficulties
"Neonatal encephalopathy" has emerged as the preferred term to describe central nervous system dysfunction in the newborn period
The terminology does not imply a specific underlying pathophysiology since the nature of brain injury causing neurologic impairment in a newborn is poorly understood.
While neonatal encephalopathy was once automatically ascribed to hypoxia-ischemia
It is now known that hypoxia-ischemia is only one of many possible contributors to neonatal encephalopathy.
Whether a particular newborn's encephalopathy can be attributed to hypoxic-ischemic brain injury is often unclear.
Some investigators require stringent criteria for using the term neonatal encephalopathy, such as two or more symptoms of encephalopathy lasting over 24 hours ,while others require no more than a low five minute Apgar score
However, the use of Apgar scores alone is problematic, as Apgar scores may be low due to maternal analgesia or prematurity, or can be normal in the presence of acute hypoxia-ischemic injury.
Given that the underlying nature of brain injury causing neurologic impairment in a newborn is often poorly understood, "neonatal encephalopathy" has emerged as the preferred terminology to describe central nervous system dysfunction in the newborn period, as it does not imply a specific underlying pathophysiology
The incidence of neonatal encephalopathy depends on how the syndrome is defined, but varies between two to nine per 1000 term births
As the term “neonatal encephalopathy” has become increasingly favored, it has been shown that the diagnosis of "birth asphyxia" has declined over the past decade
Despite major advances in monitoring technology and knowledge of fetal and neonatal pathologies, perinatal asphyxia or, more appropriately, hypoxic-ischemic encephalopathy (HIE), remains a serious condition that causes significant mortality and long-term morbidity.
Pathophysiology
Brain hypoxia and ischemia due to systemic hypoxemia, reduced cerebral blood flow (CBF), or both are the primary physiological processes that lead to hypoxic-ischemic encephalopathy
The initial compensatory adjustment to an asphyxial event is an increase in CBF due to hypoxia and hypercapnia.
This is accompanied by a redistribution of cardiac output to essential organs, including the brain, heart, and adrenal glands.
A blood pressure (BP) increase due to increased release of epinephrine further enhances this compensatory response.
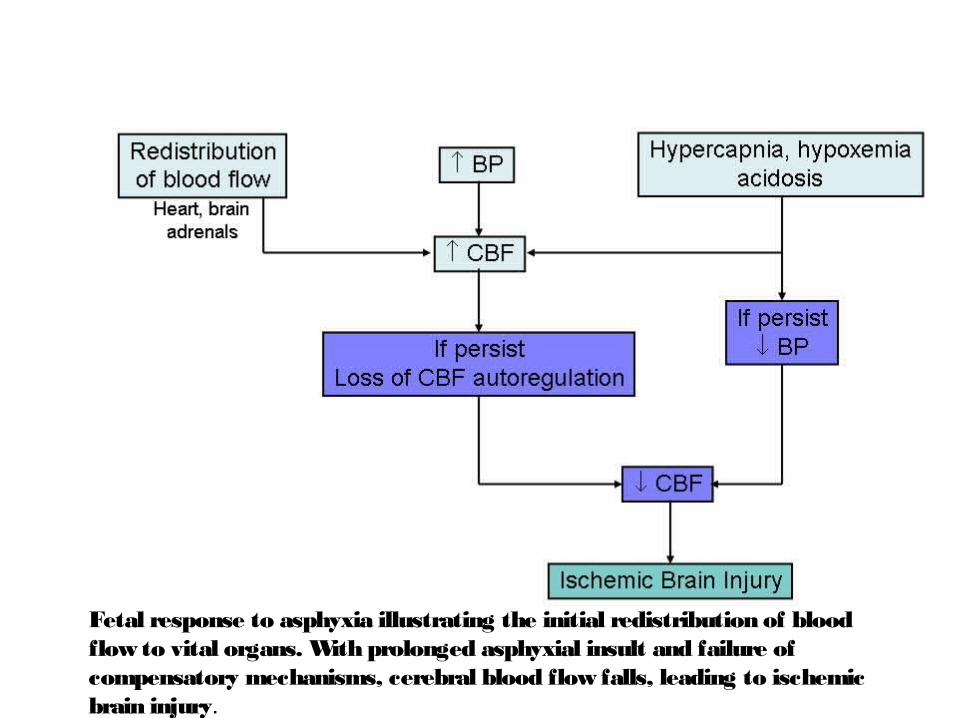
Fetal response to asphyxia illustrating the initial redistribution of blood flow to vital organs. With prolonged asphyxial insult and failure of compensatory mechanisms, cerebral blood flow falls, leading to ischemic brain injury.
In adults, CBF is maintained at a constant level despite a wide range in systemic BP.
This phenomenon is known as the cerebral autoregulation, which helps maintain cerebral perfusion
In human adults, the BP range at which CBF is maintained is 60-100 mm Hg.

Limited data in the human fetus and the newborn infant suggest that CBF is stable over much narrower range of BPs
Some experts have postulated that, in the healthy term newborn, the BP range at which the CBF autoregulation is maintained may be only between 10-20 mm Hg (compared with the 40 mm Hg range in adults)
In addition, the autoregulatory zone may also be set at a lower level, about the midpoint of the normal BP range for the fetus and newborn.
However, the precise upper and lower limits of the BP values above and below which the CBF autoregulation is lost remain unknown for the human newborn.
In the fetus and newborn suffering from acute asphyxia, after the early compensatory adjustments fail, the CBF can become pressure-passive, at which time brain perfusion depends on systemic BP
As BP falls, CBF falls below critical levels, and the brain injury secondary to diminished blood supply and a lack of sufficient oxygen occurs.
This leads to intracellular energy failure.
During the early phases of brain injury, brain temperature drops, and local release of neurotransmitters, such as gamma-aminobutyric acid transaminase (GABA), increase.
These changes reduce cerebral oxygen demand, transiently minimizing the impact of asphyxia.
At the cellular level, neuronal injury in hypoxic-ischemic encephalopathy is an evolving process.
The magnitude of the final neuronal damage depends on duration and severity of the initial insult combined to the effects of reperfusion injury, and apoptosis.
At the biochemical level
Excitatory amino acid (EAA) receptor overactivation plays a critical role in the pathogenesis of neonatal hypoxia-ischemia.
During cerebral hypoxia-ischemia, the uptake of glutamate (the major excitatory neurotransmitter of the mammalian brain) is impaired.
This results in high synaptic levels of glutamate and EAA receptor overactivation, including N-methyl-D-aspartate (NMDA), amino-3-hydroxy-5-methyl-4 isoxazole propionate (AMPA), and kainate receptors.
NMDA receptors are permeable to Ca++ and Na+, whereas AMPA and kainate receptors are permeable to Na+
Accumulation of Na+ coupled with the failure of energy dependent enzymes such as Na+/ K+ -ATPase leads to rapid cytotoxic edema and necrotic cell death.
Activation of NMDA receptor leads to intracellular Ca++ accumulation and further pathologic cascades activation.
EAAs accumulation also contributes to increasing the pace and extent of programmed cell death through secondary Ca++ intake into the nucleus.
Finally, developing oligo/dendroglia is uniquely susceptible to hypoxia-ischemia, specifically excito-toxicity and free radical damage.
This white matter injury may be the basis for the disruption of long-term learning and memory abilities in infants with hypoxic-ischemic encephalopathy.
During the reperfusion period, free radical production increases due to activation of enzymes such as cyclooxygenase, xanthine oxidase, and lipoxygenase.
Free radical damage is further exacerbated in the neonate because of immature antioxidant defenses..
Free radicals can lead to lipid peroxidation as well as DNA and protein damage and can trigger apoptosis.
Finally, free radicals can combine with nitric oxide (NO) to form peroxynitrite a highly toxic oxidant
This excessive NO production plays an important role in the pathophysiology of perinatal hypoxic-ischemic brain injury.
Inflammatory mediators (cytokines and chemokines) have been implicated in the pathogenesis of HIE and may represent a final common pathway of brain injury.
Following the initial phase of energy failure from the asphyxial injury, cerebral metabolism may recover following reperfusion, only to deteriorate in a secondary energy failure phase.
This new phase of neuronal damage, starting at about 6-24 hours after the initial injury, is characterized by mitochondrial dysfunction, and initiation of the apoptotic cascade.
This phase has been called the "delayed phase of neuronal injury."
The duration of the delayed phase is not precisely known in the human fetus and newborn but appears to increase over the first 24-48 hours and then start to resolve thereafter.
In the human infant, the duration of this phase is correlated with adverse neurodevelopmental outcomes at 1 year and 4 years after insult.
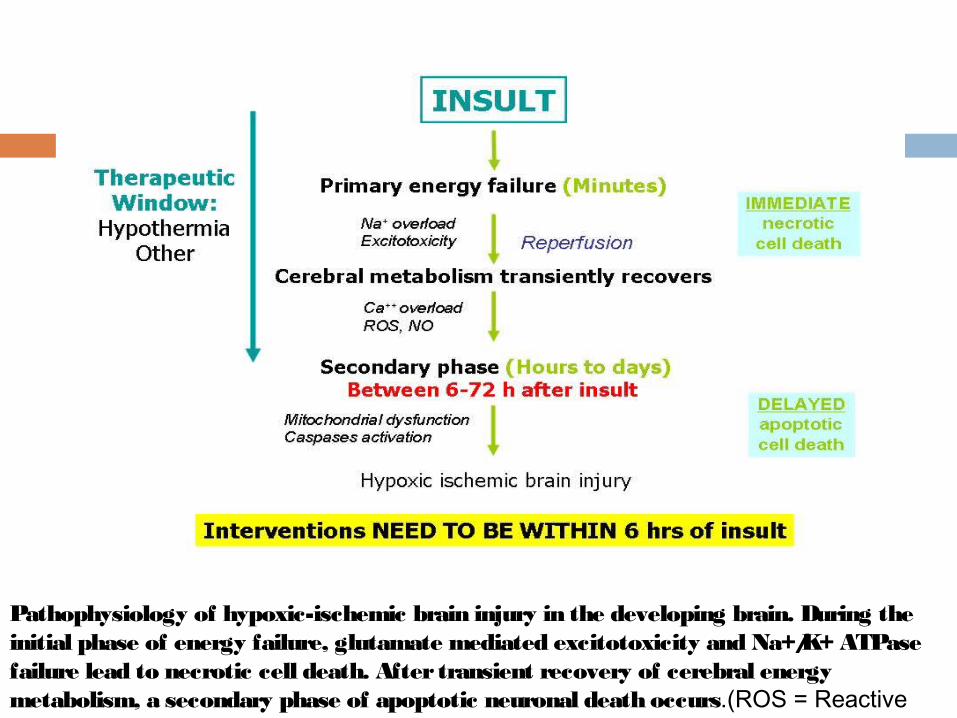
Pathophysiology of hypoxic-ischemic brain injury in the developing brain. During the initial phase of energy failure, glutamate mediated excitotoxicity and Na+/K+ ATPase failure lead to necrotic cell death. After transient recovery of cerebral energy metabolism, a secondary phase of apoptotic neuronal death occurs.(ROS = Reactive oxygen species).
Frequency
In the United States and in most advanced countries, the incidence of hypoxic-ischemic encephalopathy is 1-8 cases per 1000 births.
The incidence of HIE is reportedly high in countries with limited resources; however, precise figures are not available.
Birth asphyxia is the cause of 23% of all neonatal deaths worldwide.
Mortality/Morbidity
In severe hypoxic-ischemic encephalopathy, the mortality rate is reportedly 25-50%. Most deaths occur in the first week of life due to multiple organ failure.
Some infants with severe neurologic disabilities die in their infancy from aspiration pneumonia or systemic infections.
80% of infants who survive severe hypoxic-ischemic encephalopathy develop serious complications,
10-20% develop moderately serious disabilities, and
as many as 10% are healthy.
History
The 1996 guidelines from the AAP and ACOG for (HIE) indicate that all of the following must be present for the designation of perinatal asphyxia severe enough to result in acute neurological injury:
Profound metabolic or mixed acidemia (pH < 7) in an umbilical artery blood sample, if obtained
Persistence of an Apgar score of 0-3 for longer than 5 minutes
Neonatal neurologic sequelae (eg, seizures, coma, hypotonia)
Multiple organ involvement (eg, kidney, lungs, liver, heart, intestines)
CNS Manifestations
Mild hypoxic-ischemic encephalopathy Muscle tone may be slightly increased and
deep tendon reflexes may be brisk during the first few days.
Transient behavioral abnormalities, such as poor feeding, irritability, or excessive crying or sleepiness, may be observed.
The neurologic examination findings normalize by 3-4 days of life.
Moderately severe hypoxic-ischemic encephalopathy The infant is lethargic, with significant
hypotonia and diminished deep tendon reflexes.
The grasping, Moro, and sucking reflexes may be sluggish or absent.
Occasional periods of apnea. Seizures may occur within the first 24 hours of
life. Full recovery within 1-2 weeks is possible and
is associated with a better long-term outcome.
An initial period of well-being or mild hypoxic-ischemic encephalopathy may be followed by sudden deterioration, suggesting ongoing brain cell dysfunction, injury, and death; seizure intensity might increase.
Severe hypoxic-ischemic encephalopathy Stupor or coma is typical. The infant may not
respond to any physical stimulus. Breathing may be irregular, and the infant
often requires ventilatory support. Generalized hypotonia and depressed deep
tendon reflexes are common. Neonatal reflexes (eg, sucking, swallowing,
grasping, Moro) are absent.
Disturbances of ocular motion. The pupils may be dilated, fixed, or poorly reactive to light
Seizures occur early and often and may be initially resistant to conventional treatments.
The seizures are usually generalized, and their frequency may increase during the 24-48 hours after onset, correlating with the phase of reperfusion injury
As the injury progresses, seizures subside and the EEG becomes isoelectric or shows a burst suppression pattern.
At that time, wakefulness may deteriorate further, and the fontanelle may bulge, suggesting increasing cerebral edema.
Irregularities of heart rate and blood pressure (BP) are common , as is death from cardiorespiratory failure.
Infants who survive severe hypoxic-ischemic encephalopathy The level of alertness improves by days 4-5 of
life. Hypotonia and feeding difficulties persist,
requiring tube feeding for weeks to months.
Multiorgan Dysfunction
Multiorgan systems involvement is a hallmark of hypoxic-ischemic encephalopathy.
Heart (43-78%) May present as reduced myocardial
contractility, severe hypotension, passive cardiac dilatation, and tricuspid regurgitation.
Lungs (71-86%) Patients may have severe pulmonary
hypertension requiring assisted ventilation.
Renal (46-72%)Renal failure presents as oliguria, leading to
significant water and electrolyte imbalances. Liver (80-85%)Elevated liver function test results,
hyperammonemia, and coagulopathy can be seen.
Necrotizing enterocolitis is rare

Hematologic (32-54%) Disturbances include increased nucleated
RBCs, neutropenia or neutrophilia, thrombocytopenia, and coagulopathy.
Neurologic Findings
Cranial nerves Lack of reflex activity mediated by the cranial
nerves can indicate brainstem dysfunction. Neurologic examination may be difficult in the
small premature infant, but weakness of the lower extremities sometimes reflects the neuropathologic substrate of periventricular leukomalacia
The pupil starts reacting to light around 30 weeks, but the light reflex is not consistently assessable until the gestational age of 32-35 weeks. Pupillary reflexes are reliably present at term.
Patients with mild HIE often have mydriasis. Progression of the disease may produce miosis responsive to light, and in severe cases (stage 3 of Sarnat classification), the pupils are small or midpositioned and poorly reactive to light, reflecting sympathetic or parasympathetic dysfunction.
The lack of pupillary, eye movement, corneal, gag, and cough reflexes may reflect damage to the brainstem, where the cranial-nerve nuclei are located.
Decreased respiratory drive or apnea can be from lesions of the respiratory center or medullary reticular formation.
Ventilatory disturbances in HIE may manifest as periodic breathing apnea or just decreased respiratory drive.
Motor function Begin the motor examination of an infant with
suspected HIE by qualitatively and quantitatively observing his posture and spontaneous movements.
Specific patterns of motor weakness indicate cerebral injury patterns
Se iz ure s
HIE is often reported to be the most frequent cause of neonatal seizures
They usually occur 12-24 hours after birth and are difficult to control with anticonvulsants.
Tonic, unilateral, or focal seizures consistently have an EEG signature.
Subtle seizures may be a part of the HIE picture
Sarnat Staging System
The staging system proposed by Sarnat in 1976 is often useful in classifying the degree of encephalopathy.
Stages I, II, and III correlate with the descriptions of mild, moderate, and severe encephalopathy

Causes
Badawi et al investigated risk factors of neonatal encephalopathy in the Western Australian case control study.
Of the 164 infants with moderate-to-severe neonatal encephalopathy, preconceptual and antepartum risk factors were identified in 69% of cases;
24% of infants had a combination of antepartum and intrapartum risk factors,
whereas only 5% of infants had only intrapartum risk factors.
In this study, 5% had no identifiable risk factors.
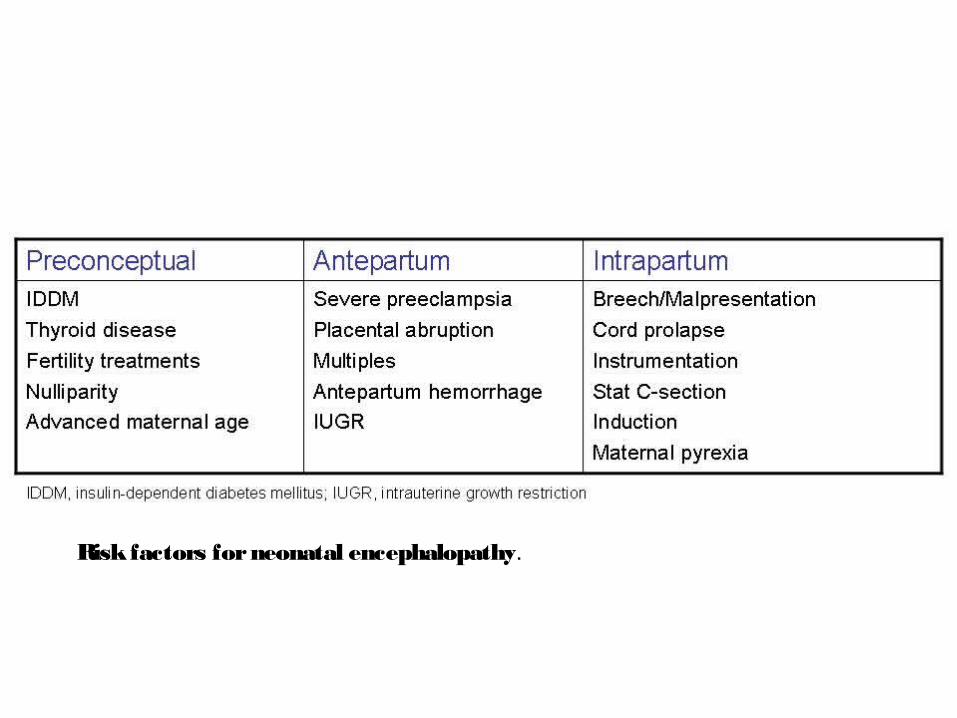
Risk factors for neonatal encephalopathy.
Laboratory Studies
There are nor specific tests to confirm or exclude a diagnosis of hypoxic-ischemic encephalopathy (HIE) because the diagnosis is made based on the history, physical and neurological examinations, and laboratory evidence
As always, the results of the tests should be interpreted in conjunction with the clinical history and the findings from physical examination.
Serum electrolyte levels In severe cases, daily assessment of serum
electrolytes are valuable until the infant's status improves.
Markedly low serum sodium, potassium, and chloride levels in the presence of reduced urine flow and excessive weight gain may indicate acute tubular damage or syndrome of inappropriate antidiuretic hormone (SIADH) secretion, particularly during the initial 2-3 days of life.
Renal function studies Serum creatinine levels, creatinine clearance,
and BUN levels suffice in most cases. Cardiac and liver enzymes These values are an adjunct to assess the
degree of hypoxic-ischemic injury to these other organs.
Coagulation system evaluation This includes prothrombin time, partial
thromboplastin time, and fibrinogen levels. ABG Blood gas monitoring is used to assess acid-
base status and to avoid hyperoxia and hypoxia as well as hypercapnia and hypocapnia.
Medical Care
Following initial resuscitation and stabilization, treatment of (HIE) is largely supportive and should focus on adequate ventilation and perfusion,
careful fluid management, avoidance of hypoglycemia and
hyperglycemia and treatment of seizures. Intervention strategies
aim to avoid any further brain injury in these infants.

Supportive Care in Patients with Hypoxic-ischemic Encephalopathy Most infants with severe hypoxic-ischemic
encephalopathy need ventilatory support during first days of life.
Hypocapnia in particular may lead to severe brain hypoperfusion and cellular alkalosis and has been associated with worse neurodevelopmental outcomes.
Of note, recent evidence indicates that increased FiO2 in the first 6 hours of life is a significant risk factor for adverse outcomes
Infants with hypoxic-ischemic encephalopathy are also at risk for pulmonary hypertension and should be monitored.
Perfusion and Blood Pressure Management Studies indicate that a mean blood pressure
(BP) above 35-40 mm Hg is necessary to avoid decreased cerebral perfusion.
Hypotension is common in infants with severe HIE and is due to myocardial dysfunction, capillary leak syndrome, and hypovolemia; hypotension should be promptly treated.
Dopamine or dobutamine can be used to achieve adequate cardiac output
Fluid and Electrolytes Management Because of the concern for acute tubular
necrosis (ATN) and syndrome of inappropriate antidiuretic hormone (SIADH) secretion, fluid restriction is typically recommended for these infants until renal function and urine output can be evaluated.
However, fluid and electrolyte management must be individualized on the basis of clinical course, changes in weight, urine output, and the results of serum electrolyte and renal function studies.

The role of prophylactic theophylline, given early after birth, in reducing renal dysfunction after HIE has been evaluated in 3 small randomized controlled trials
A single dose of theophylline (5-8 mg/kg) given within 1 hour of birth resulted in (1) decreased severe renal dysfunction (2) increased creatine clearance; (3) increased glomerular filtration rate (GFR); and (4) decreased b2 microglobulin excretion.
Fluid and glucose homeostasis should be achieved.
Avoid hypoglycemia and hyperglycemia because both may accentuate brain damage
Hyperthermia management : Hyperthermia has been shown to be
associated with increased risk of adverse outcomes in neonates with moderate-to-severe HIE
Treatment of Seizures
Hypoxic-ischemic encephalopathy is the most common cause of seizures in the neonatal period.
Seizures are generally self-limited to the first days of life
Current therapies include phenobarbital, phenytoin, and benzodiazepines
Hypothermia Therapy
Extensive experimental data suggest that mild hypothermia (3-4°C below baseline temperature) applied within a few hours (no later than 6 h) of injury is neuroprotective
The neuroprotective mechanisms are not completely understood.
Possible mechanisms include (1) reduced metabolic rate and energy
depletion; (2) decreased excitatory transmitter release; (3) reduced alterations in ion flux; (4) reduced apoptosis due to HIE; and (5) reduced vascular permeability, edema, and
disruptions of blood-brain barrier functions
The clinical efficacy of therapeutic hypothermia in neonates with moderate-to-severe hypoxic-ischemic encephalopathy has been evaluated in 7 randomized controlled trials
Inclusion criteria))RCT
Near-term infants Evidence of acute event around the time of
birth - Apgar score of 5 or less at 10 minutes after birth
Evidence of moderate to severe encephalopathy at birth - Clinically determined
at least 2 of the following:
lethargy, stupor, or coma; abnormal tone or posture; abnormal reflexes [suck, grasp, Moro, gag,
stretch reflexes]; decreased or absent spontaneous activity; autonomic dysfunction [including bradycardia,
abnormal pupils, apneas]; and clinical evidence of seizures, moderately or
severely abnormal amplitude (aEEG)
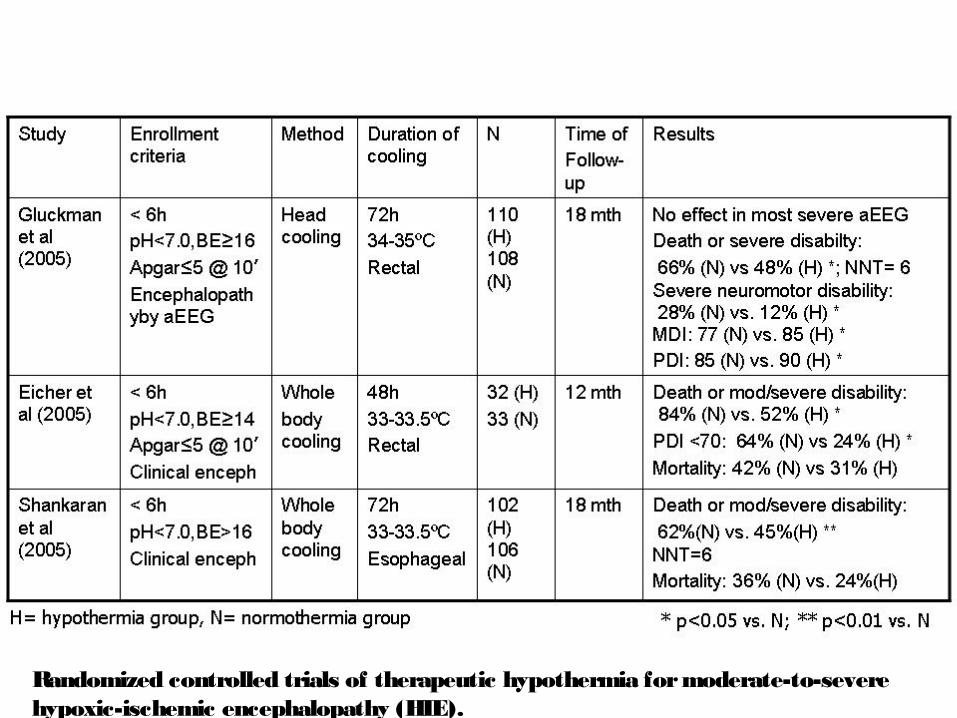
Randomized controlled trials of therapeutic hypothermia for moderate-to-severe hypoxic-ischemic encephalopathy (HIE).
the results of the trials
No difference in composite outcome of death or severe disability were noted between the groups.
However, the study found that moderate hypothermia for 72 hours improved neurologic outcomes in survivors.
Surviving infants who were cooled were more likely to be free of neurologic abnormalities
These clinical studies have been reassuring regarding safety and applicability of hypothermia therapy
Therapeutic hypothermia when applied within 6 hours of birth and maintained for 48-72 hours is a promising therapy for mild-to-moderate cases of HIE
hypothermia and its side effects
include coagulation defects, leukocyte malfunctions, pulmonary hypertension, worsening of metabolic acidosis, and abnormalities of cardiac rhythm, especially
during rewarming.

What is the optimal timing of initiation of hypothermia therapy? Cooling must begin early, within 6 hours of
injury. However (the earlier the better ) Simplified method using widely available
icepacks is an effective way to provide hypothermia therapy in referring centers while awaiting transfer to a tertiary NICU
6 hr ???!!!>
On the other hand, a favorable outcome may be possible if the cooling begins beyond 6 hours after injury.
A current National Institute of Child Health and Human Development (NICHD) study is evaluating the efficacy of delayed hypothermia therapy for infants presenting at referral centers beyond 6 hours of life or with evolving encephalopathy.
What is the optimal duration of hypothermia therapy? The greater the severity of the initial injury, the
longer the duration of hypothermia needed for optimal neuroprotection.
The optimal duration of brain cooling in the human newborn has not been established
What is the best method?
Two methods have been used in clinical trials: selective head cooling and whole body cooling.
selective head cooling
In selective head cooling, a cap (CoolCap) with channels for circulating cold water is placed over the infant's head, and a pumping device facilitates continuous circulation of cold water.
Rectal temperature is then maintained at 34-35°C for 72 hour
whole body hypothermia
In whole body hypothermia, the infant is placed on a commercially available cooling blanket, through which circulating cold water flows, so that the desired level of hypothermia is reached quickly and maintained for 72 hours.

What is the optimal rewarming method? Rewarming is a critical period. In clinical trials, rewarming was carried out
gradually, over 6-8 hours.
Does hypothermia therapy result in long-term benefits?
Several meta-analysis have been conducted and indicate that therapeutic hypothermia is beneficial to term newborns with hypoxic-ischemic encephalopathy
In a Cochrane review, Jacobs et al found that therapeutic hypothermia results in significant reduction in the following:
Combined outcome of mortality or major neurodevelopmental disability at age 18 months
Mortality Neurodevelopmental disability in survivors
They also found a significant increase in thrombocytopenia, although it was not clinically significant.
Benign sinus bradycardia
Hypothermia therapy should be conducted under strict protocols and reserved to regional referral centers offering comprehensive multidisciplinary care and planning to conduct long-term neurodevelopmental follow-up.

NEUROPROTECTIVE STRATEGIES
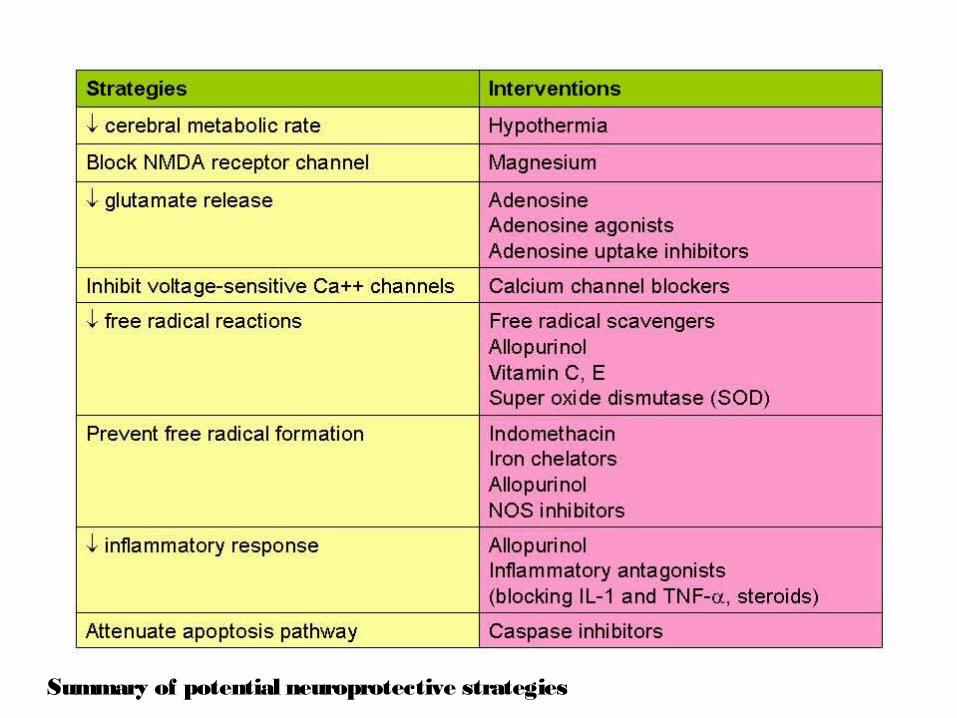
Summary of potential neuroprotective strategies
Promising avenues include the following:
Prophylactic barbiturates: high-dose phenobarbital (40 mg/kg) was given over 1 hour to infants with severe hypoxic-ischemic encephalopathy.
Treated infants had fewer seizures Treated infants also had fewer neurological
deficits at age 3 years
Erythropoietin: In a recent study, low-dose erythropoietin (300-500 U/kg) administered for 2 weeks starting in the first 48 hours of life decreased the incidence of death or moderate and severe disability at age 18 months
Subgroup analysis indicated that only infants with moderate disability benefited from this therapy.
Allopurinol: Slight improvements in survival and cerebral blood flow (CBF) were noted in a small group of infants tested with this free-radical scavenger in one clinical trial.
Excitatory amino acid (EAA) antagonists: (MK-801, an EAA antagonist), has shown promising results in experimental animals and in a limited number of adult trials.
However, this drug has serious cardiovascular adverse effects
Medication Summary
Providing standard intensive care support, correcting metabolic acidosis, close monitoring of the fluid status, and seizure control are the main elements of treatment in patients with (HIE).
Anticonvulsants are the only specific drugs used often in this condition.
Further Inpatient Care
Close physical therapy and developmental evaluations are needed prior to discharge in patients with (HIE).
References Ferriero DM. Neonatal brain injury. N Eng l J Me d . Nov 4 2004;351(19):1985-95. [Medline]. Perlman JM. Brain injury in the term infant. Se m in Pe rina to l. Dec 2004;28(6):415-24. [Medline]. Grow J, Barks JD. Pathogenesis of hypoxic-ischemic cerebral injury in the term infant: current
concepts.Clin Pe rina to l. Dec 2002;29(4):585-602, v. [Medline]. Srinivasakumar P, Zempel J, Wallendorf M, Lawrence R, Inder T, Mathur A. Therapeutic
hypothermia in neonatal hypoxic ischemic encephalopathy: electrographic seizures and magnetic resonance imaging evidence of injury. J Pe d ia tr. Aug 2013;163(2):465-70. [Medline].
Shankaran S. The postnatal management of the asphyxiated term infant. Clin Pe rina to l. Dec 2002;29(4):675-92. [Medline].
Stola A, Perlman J. Post-resuscitation strategies to avoid ongoing injury following intrapartum hypoxia-ischemia. Se m in Fe ta l Ne o na ta l Me d . Dec 2008;13(6):424-31. [Medline].
Laptook A, Tyson J, Shankaran S, et al. Elevated temperature after hypoxic-ischemic encephalopathy: risk factor for adverse outcomes. Pe d ia tric s . Sep 2008;122(3):491-9. [Medline]. [Full Text].
[Guideline] American Academy of Pediatrics. Relation between perinatal factors and neurological outcome. In: Guidelines for Perinatal Care. 3rd ed. Elk Grove Village, Ill: American Academy of Pediatrics; 1992:221-234.
[Guideline] Committee on fetus and newborn, American Academy of Pediatrics and Committee on obstetric practice, American College of Obstetrics and Gynecology. Use and abuse of the APGAR score.Pe d ia tr. 1996;98:141-142. [Medline].

References Papile LA, Rudolph AM, Heymann MA. Autoregulation of cerebral blood flow in the preterm fetal lamb.Pe d ia tr
Re s . Feb 1985;19(2):159-61. [Medline]. Rosenkrantz TS, Diana D, Munson J. Regulation of cerebral blood flow velocity in nonasphyxiated, very low birth
weight infants with hyaline membrane disease. J Pe rina to l. 1988;8(4):303-8. [Medline]. Pacher P, Beckman JS, Liaudet L. Nitric oxide and peroxynitrite in health and disease. Phys io l Re v . Jan
2007;87(1):315-424. [Medline]. Roth SC, Baudin J, Cady E, Johal K, Townsend JP, Wyatt JS. Relation of deranged neonatal cerebral oxidative
metabolism with neurodevelopmental outcome and head circumference at 4 years. De v Me d Child Ne uro l. Nov 1997;39(11):718-25. [Medline].
Berger R, Garnier Y. Pathophysiology of perinatal brain damage. Bra in Re s Bra in Re s Re v . Aug 1999;30(2):107-34. [Medline].
Rivkin MJ. Hypoxic-ischemic brain injury in the term newborn. Neuropathology, clinical aspects, and neuroimaging. Clin Pe rina to l. Sep 1997;24(3):607-25. [Medline].
Vannucci RC. Mechanisms of perinatal hypoxic-ischemic brain damage. Se m in Pe rina to l. Oct 1993;17(5):330-7. [Medline].
Vannucci RC, Yager JY, Vannucci SJ. Cerebral glucose and energy utilization during the evolution of hypoxic-ischemic brain damage in the immature rat. J Ce re b Blo o d Flo w Me ta b . Mar 1994;14(2):279-88.[Medline].
de Haan HH, Hasaart TH. Neuronal death after perinatal asphyxia. Eur J O bs te t G yne c o l Re p ro d Bio l. Aug 1995;61(2):123-7. [Medline].
McLean C, Ferriero D. Mechanisms of hypoxic-ischemic injury in the term infant. Se m in Pe rina to l. Dec 2004;28(6):425-32. [Medline].
Bryce J, Boschi-Pinto C, Shibuya K, Black RE. WHO estimates of the causes of death in children. La nc e t. Mar 26-Apr 1 2005;365(9465):1147-
THANK YOU
Case presentation
A male , post term (42)W , NVD, AGA , BW 3.625, admitted to our NICU at 12:15 am with a diagnosis of HIE.
The mother is a 34yr old multipara G3 P2 A1,low socioeonomic status and suferred from raised blood pressure and UTI during the last trimester for which she received oral therapy .
Iron deficieny anaemia started during 2nd trimester and 3rd for which she received oral iron tab
Natal History
Spontaneous vaginal delivery , spont. Rupture of memb.,clear amnion , vertex presentation , fetal monitoring : absent +ve data.
APGAR score 1st min is 1 and immediat resuscitation started in the delivery room , drying ,warming , positioning and AMBU bag vetilation .
5 min and 10 min apgar was 5 , intubation and transfere to NICU
ABG cord blood result: PH 6.8 Pco2 : 72 Po2 : 27 Hco3 BE -14
Whole body cooling was started at 12:30 am (within 15 min of birth)
Monitoring of pulse, temp, bl press and ECG cardiac monitor and other aspect of incubator care were started prompetly
IV fluid , broad spectrum antibiotic and complete panil of initial investigations including CBC , electrolyte , pt, ptt, liver enz , BUN and creatinin together with CK and LDH
COOLING for 72hr
On D 2 : prolonged PT 50 sec and PTT 2 min for which plasma trnsfusion was given
Erythropoietin inj. are Started (neuroprotection)
Convulsion occured , generalized colonic , phenobarbiton inj was given (loading and maintenance)
D3: convulsions un controlled , add Epanutin D4: Gradual rewarming was started
D5: significant apnea attacks , PTV was given then NCPAP ( peep 5 , fio2 30%)
Hypoactive , poor reflexes BP monitoring showed rising MAP :88 , 72, 90.
D7: nasal pronge ( stop NCPAP) Full fontanelle: CSF analysis (bloody tap) Cr U/S : free MRI : pic. Of cerebral oedema and hypoxic
changes Reduced total fluid intake with gradual
introduction of NG feeding
D8: ECG monitor multiple premature ventricular contractions associated with generalized tonic convulsions treated with IV lidocaine
D11 : Off o2 D24: stable , transfered to bed , nasogastric
full feeding , stop IV fluid and antibiotics Convulsions controlled , maintenance
sominaletta and epanutin orally Oral Topiramate
Discharge plan: Educate the parent about NG feeding with
gradual stimulation of oral suckling ( pacifiers) Follow up at Neonatal outpt clinic and blood
pressure management Gradual withdrawal of anti convulsant under
supervision of ped. Neurology clinic F/u of MRI after 3 month of discharge Cont. care and support in pediat outpt clinic
Fundus exam and hearing assessment to exclude potential handicap
Follow up of developmental mile stones




![Acute Kidney Injury in Asphyxiated neonates admitted into a ......with perinatal asphyxia. Perinatal Asphyxia ranks as the second most important cause of neonatal death[1]. Major risk](https://img.dokumen.tips/doc/110x75/61110be6b93f5b0fcd11cc91/acute-kidney-injury-in-asphyxiated-neonates-admitted-into-a-with-perinatal.jpg)
























