Embed Size (px)
Citation preview
PATIENT-CENTERED CARE
By Dr. Smruti Nikumbh- HavalM.B.B.S.D.N.B.(Family medicine)
1950 – Michael Balint explored ‘illness-centered’ medicine, conventional method inadequate to reach deep understanding of patient illness.
1964 – Balint dev. Concepts of ‘attentive’ listening and responding to patient offers.
1970 – Ian R. Mc Whiney – patient-centered care medical model
1986 – Levenstein et al evaluated and formulated patient centered as clinical method
HISTORY
The intuitive mind is a sacred gift, and
the rational mind is a faithful servant. We
have created a society in which we honor
the servant and have forgotten the gift.
Albert Einstein
PATIENT-CENTERED CARE:
Defined as ‘a philosophy of care that encourages:
(a) shared control of the consultation, decisions about intervention or management of the health problems with the patient, and/or
(b) a focus in the consultation on the patient as a whole who has individual preferences situated within social context’ (in contrast to a focus in the consultation on a body part or disease)
.
c)“treating patients as partners, involving them in planning their health care and encouraging them to take responsibility for their own health”
d)help your patients become medical decision makers who take an active role in their own care’
Cochrane review, issue 2, 2003 & Lowes R. 1998. Patient-centered care for better patient adherence. Fam. Prac. Management
THE SCIENCE OF PATIENT CENTERED CARE
It expands on the ‘disease-oriented’ model by incorporating the patient’s experience of illness, the psychosocial context & sharing decision making with patient and his family.
“The process of healing depends on knowing the patient as a person, in addition to accurately diagnosing their disease.”
Ronald M, J. Fam. Pract 2000, no 49

1) Bio-psycho-social perspective
2) Patient as person
3) Sharing power and responsibility
4) Therapeutic alliance
5) Doctor as person
Peter C et al: Analysis of large cohort BMJ 2002;325:691-692
It has been in noticed in manycountries that Doctors nearingcompleting 3 years of postgraduatetraining in specialized branches, while ingeneral practice they showed onlylimited ability to achieve patient-centered outcomes.
Primary Care Physician Is The
Captain Of Ship
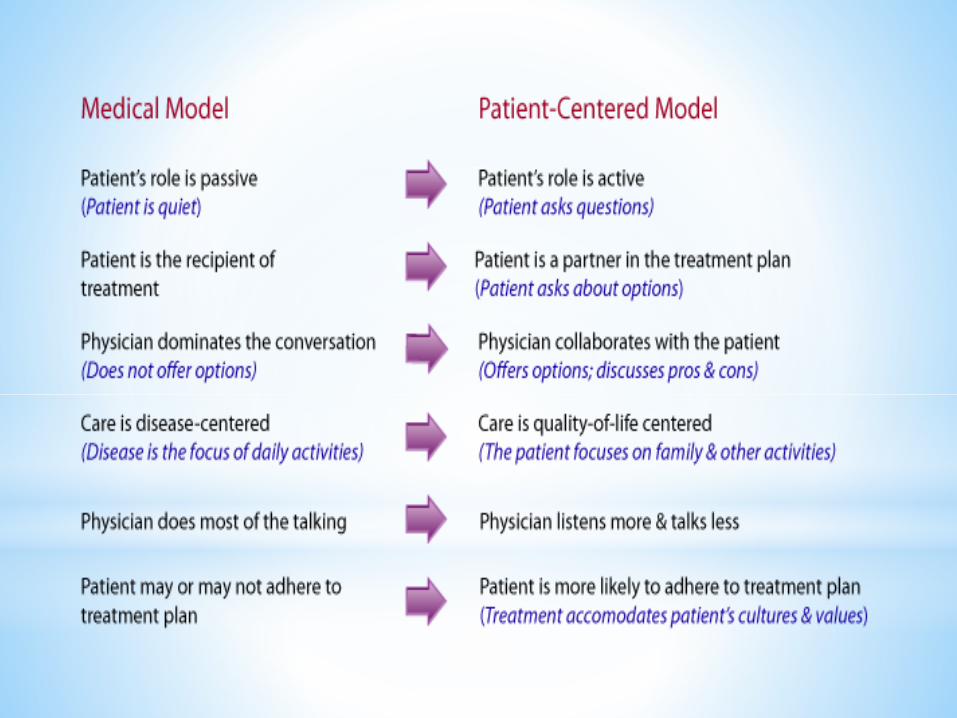
PATIENT CENTERED MODEL
•A conceptual framework to guide the practitioners to be more caring, it provides description of specific behaviors needed to be learned and when/how to use them with patients.
•Simplifies complexity of doctor’s job without distorting it.
•Provides a framework for research.
• ‘method’ operationalize this model
PATIENT-CENTERED METHOD :
Six interactive components:
1) Exploring both the disease and the illness experience.
2) Understanding the whole person.
3) Finding common ground regarding management.
4) Incorporating prevention and health promotion.
5) Enhancing the patient-doctor relationship.
6) Being realistic.

1)EXPLORING BOTH THE DISEASE AND
THE ILLNESS EXPERIENCE
• Assess the two model of ill health: disease and illness
• Dimension of disease
• Assess the disease process by history, examination
& the differential diagnosis
• The dimension of illness
–How patient feels about being ill, what the patient’s ideas about
the illness, what impact the illness has on the patient’s function,
what he or she expects from the physician
Disease-Theoretical construct terms of abnormality structure/ function of body organ/systems including physical & mental disorder.
It is diagnostic explains what a disease has in common with others.
Established by conventional method.
Illness-Patient personal experience of ill health.
Unique in each patient.
Need additional approach.
4 principles dimension of patient illness:1) Their ideas of what is wrong with them
2) Their feelings especially fears about being ill
3) The impact of their problems on functioning
4) Their expectations of what should be done.
Requires skill in interviewing to enable doctor to ‘enter into the patient’s world’
2)UNDERSTANDING THE WHOLE PERSON
Integrate the concept of disease and illness with an
understanding of the whole person.
Includes an awareness of the patient’s position in the life
cycle and the social context in which they live
The family and anyone else involved in or affected by
the patient’s illness; the physical environment
Cultural beliefs & attitudes also influences care
3)FINDING COMMON GROUND
Mutual definition of the problems and priorities
Mutual definition of the goals of management/
treatment
Mutual exploring of the roles to be assumed by
the patient and the doctor in the management
Required areas doctor and patient to agree :
1)The nature of the problems and priorities.
E.g – tumor & migraine.
2)The goals of treatment- negotiate reasonably.
E.g- FBS in diabetic pt.
3)The roles of the doctor & the patient.

4)INCORPORATING PREVENTION AND
HEALTH PROMOTION
“Use each visit as an opportunity for prevention and
health promotion”
Health enhancement
Risk reduction policies
Early detection of disease
Ameliorated the effects of disease
Health enhancement:
Doctor & patient monitor areas in patient’s live that
need improvement for long term physical & emotional
health.
Risk reduction & early detection :
Doctor monitor, recognized problems and screen
unrecognized disease.
Doctor collaborate with other health professionals
implementing health promotion & screening.
5)ENHANCING THE PATIENT-DOCTOR
RELATIONSHIP
• Characteristics of the therapeutic relationship
– Each encounter with patient should be used to develop the
doctor-patient relationship
– Caring and healing approach
– Transference and countertransference
• To develop trust and respect
– Sharing power
– Self awareness
• This has impact on other components of the method
Doctor seeing same patient, with variety of problems, acquire personal knowledge that may help in future.
Every visit develope continuity of care and effective long term relationship.
Different patient needs different approaches.
i. e.g.– praise patient who follows their treatment plans properly.
ii. supports those having difficulty in reaching goals.iii. asking about their feelings and opinion shows that
their input is important.
6)BEING REALISTIC
Throughout the process, physician have to be realistic
in terms of time, availability of resources and the
amount of emotional and physical energy needed
Time: Manage time efficiently for maximum benefit of
patient.
Resources : Develops skills of priority setting,
resource allocation, teamwork.
Team building : Doctors also must respect their own
limits of emotional energy and not expect too much of
themselves.
Patient centered care is ….
1. Not a strictly defined process, sequential stages,
standardized procedures or interviewing styles
2. Though presented separately, reality – interwoven.
3. Varies from patient to patient.
4. Learning is different from acquiring the process.
5. When performing focally aware of the whole process,
not the components


WHY PRACTICE PATIENT-
CENTERED CARE?
Improved satisfaction for patient and service provider.
Patient-centered approach have positive relationship with patient
recovery, emotional health, physical function and physiologic
outcome and treatment satisfaction.
Improved adherence. Research shows patients more likely to take their pills, lay off
sour cream, show up for appointment thus a better patient adherence.
Evidence that patient-centered communication skills promote adherence.
Functional outcome improvement.
Research shows fewer limitations imposed by the disease on patient functional ability.
Decreased litigation
Studies demonstrated that physicians behave like devaluing patients views, delivering information poorly, failing to be attentive to patients perspective often face malpractice claims.
Common questions regarding patient-centered care1.Conflict between patient expectation and medical assessment?
Physician try to reconcile the two conflicting views.
E.g – refused admission when unnecessary,
pt. demand narcotic drugs.
2. Risk of invading privacy?
Allows and encourage expression without forcing.
3. Always necessary to use the method?
We don’t know unless we ask.
4. Time consuming?
average length of office visit plus physical examination is 21
min either conventional or patient centered.
Lots of time get waste in doctor-centered visits because the Doctor goes on and on about medical information that doesn’t address what’s on the patient mind.
In patient-centered visits, the Doctor talk less and the patient says more.”