Embed Size (px)
Citation preview

Nutritional Rickets
Dr. Siddharth GuptaSenior resident
Chacha Nehru Bal Chikitsalya, Delhi

THE JOURNAL CLUB


Definition
Nutritional rickets
Disorder of defective chondrocyte differentiation and mineralization of
the growth plate and defective osteoid mineralization
Osteomalacia
Osteomalacia is abnormal matrix mineralization in established bone, and
although present in children with rickets, it is used to describe bone
mineralization defects after completion of growth

CALCIUM VITAMIN D

Diagnosis
• The diagnosis of Nutritional rickets is
made on the basis of :
• History
• Physical examination
• Biochemical testing
• Confirmed by radiographs

LAB/BIOCHEMICAL
• Biochemical testing alone is not sufficient to diagnose NR
and may not differentiate whether the primary cause of NR
• Combined deficiencies are common
• Dietary history

Increasing vs Decreasing
• Serum PTH
• Alkaline phosphatase (ALP)
• Urinary phosphorus levels
• 25-hydroxyvitamin D
(25OHD)
• Serum phosphorus
• Serum calcium
• Urinary calcium

How to assess serum Vit D? Vitamin D status is assessed by measuring blood
levels of total 25OHD which has been classified by the panel as follows:
0 20 40 60
Sufficient(>50)
Insufficient(30-50)
Deficient(<30)
25OHD(nmol/L)
Vit d(nmol/L)
In healthy children, routine 25OHD screening is not recommended
Why 25OHD?
NR does not include rickets associated with heritable disorders
of vitamin D metabolism, including 1-α-hydroxylase
deficiency and vitamin D receptor defects, or congenital or
acquired hypophosphatemic rickets

Symptomatic Deficiency
• NR may not occur with very low 25OHD concentrations but is
more likely to occur with deficiency sustained over time, i.e.
chronic deficiency--------Duration is important
• Most children with vitamin D deficiency are asymptomatic
Reason CALCIUM VITAMIN D

Recommendations • 25OHD level at 30–34 nmol/l is the critical
cutoff below which NR is more likely to occur• PTH starts increasing when 25OHD levels
drop below 34 nmol/l• Seasonal variations in 25OHD
maintaining 25OHD levels >50 nmol/l (i.e. sufficient)

Dietary Calcium Intake to Prevent Rickets
AGE (Months) DOSE (Mg/ day)
<6 200
6-12 260
>12 Atleast 300
Sufficient >500
Insufficient 300-500
Deficient <300
“For children over 12 months of age, dietary calcium intake of <300 mg/d increases the risk of rickets independent of serum 25OHD levels”
Vitamin D Deficiency and Fractures
• Children with radiographically confirmed rickets have an increased risk of fracture
• Children with simple vitamin D deficiency are not at an increased risk of fracture.

Prevention and Treatment of Nutritional Rickets and Osteomalacia-Vitamin D Supplementation
AGE (Months) DOSE (IU/DAY)
<12 400
>12 600
Infants and toddlers with 25OHD < 50nmol/L
50-100 000 every 3 months
“Among infants and toddlers with 25OHD levels < 50 nmol/L for whom daily vitamin D supplementation may not be ideal, intermittent bolus doses of 50 to 100 000 IU every 3 months hold promise”


How to prevent risk factors?
Candidates for vitamin D supplementation
• Children with a history of symptomatic vitamin D deficiency
requiring treatment
• Children and adults at high risk of vitamin D deficiency with
factors or conditions that reduce synthesis or intake of
vitamin D
• Pregnant women
Dose of Vitamin D and Calcium for the Treatment of Nutritional Rickets
• The minimal recommended dose of vitamin D is 2,000 IU/day
(50 μg) for a minimum of 3 months
• Oral calcium, 500 mg/day, either as dietary intake or
supplements, should be routinely used in conjunction with
vitamin D in the treatment regardless of age or weight
“ Combined treatment is justified because studies have shown that the diet of children and adolescents with NR is generally
low in both vitamin D and calcium”
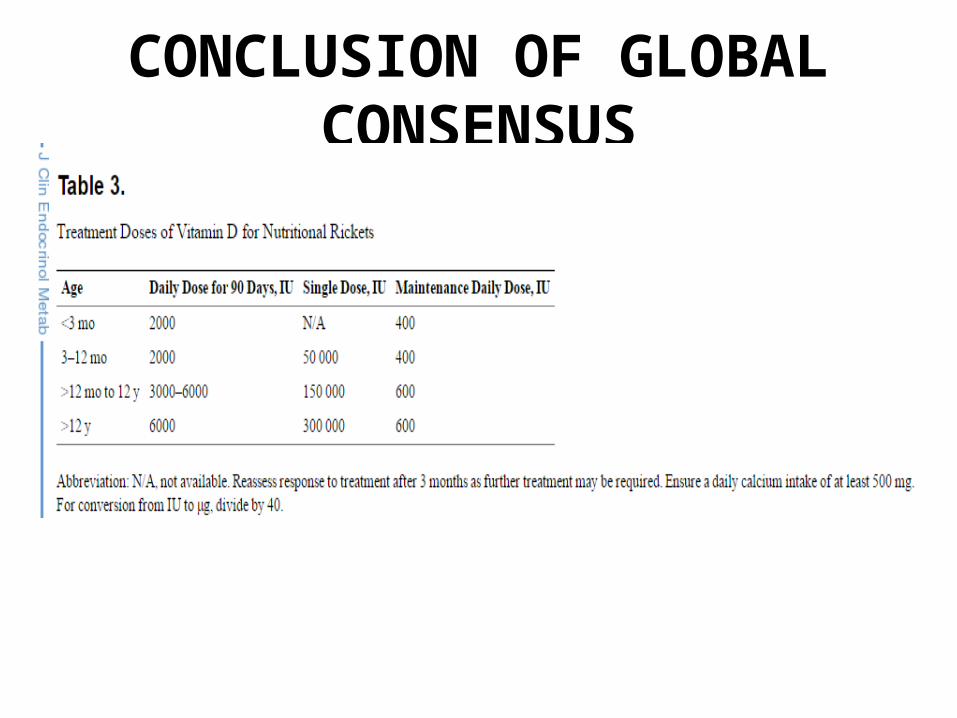
CONCLUSION OF GLOBAL CONSENSUS
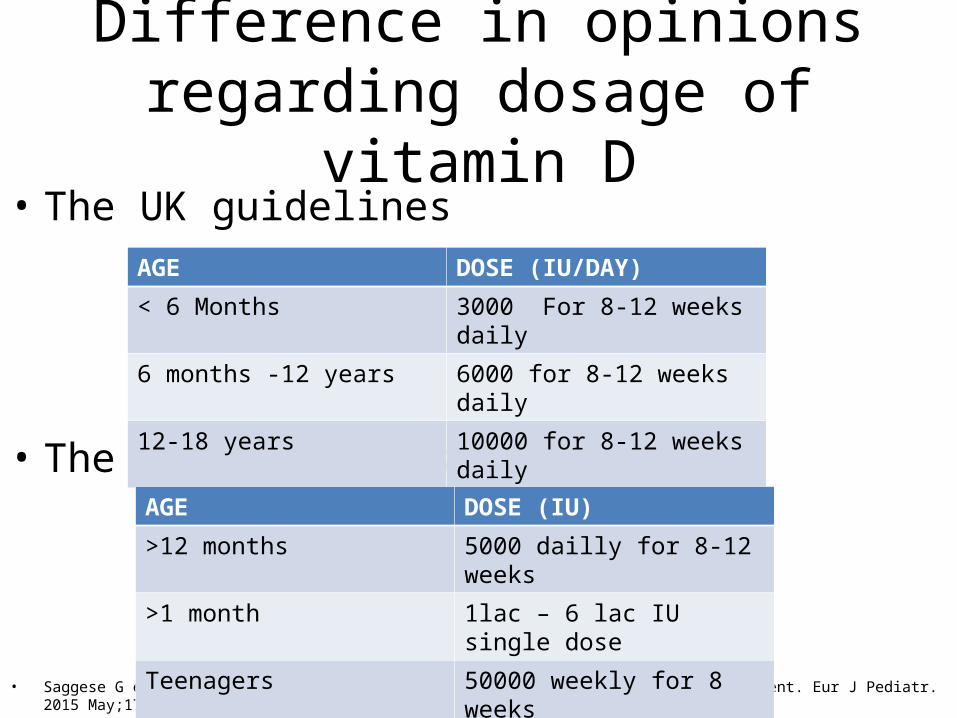
Difference in opinions regarding dosage of vitamin D
• The UK guidelines
• The US guidelines
• Saggese G et al Vitamin D in childhood and adolescence: an expert position statement. Eur J Pediatr. 2015 May;174(5):565-76. doi: 10.1007/s00431-015-2524-6. Epub 2015 Apr 2.
AGE DOSE (IU/DAY)
< 6 Months 3000 For 8-12 weeks daily
6 months -12 years 6000 for 8-12 weeks daily
12-18 years 10000 for 8-12 weeks daily
AGE DOSE (IU)
>12 months 5000 dailly for 8-12 weeks
>1 month 1lac – 6 lac IU single dose
Teenagers 50000 weekly for 8 weeks

What we follow IAP
Vitamin D Deficiency in Childhood – A Review of Current Guidelines on Diagnosis and Management
S Balasubramanian, K Dhanalakshmi and Sumanth AmperayaniFrom Kanchi Kamakoti CHILDS Trust Hospital, The CHILDS Trust Medical Research Foundation, 12-A, Nageswara Road,
Nungambakkam, Chennai 600 034, Tamil Nadu, India

THE STOSS REGIMEN

The Stoss therapy
• The administration of a large dose given as a single dose or in
divided doses over several days
• This approach has been advocated for ease of use and
compliance • 3lac – 6lac IU as a single dose
• Risk of hypercalcemia
• Hence should be limited to children who have evidence of
symptomatic vitamin D deficiency

What is the end point of treatment?
Endpoint of an ALP level < 350 U/L and radiographic evidence
of near-complete healing of rickets was seen in a higher
percentage of patients who received a combination of calcium
and vitamin D (58%) or calcium alone (61%) than in those who
received vitamin D alone (19%)
Thacher TD, Fischer PR, Pettifor JM, et al. A comparison of calcium, vitamin D, or both for nutritional rickets in Nigerian children. N
Engl J Med. 1999;341(8):563–568
ORAL OR INTRAMUSCULAR• Oral treatment: restores 25OHD levels faster than
intramuscular (IM) treatment
• For daily treatment, both D 2 and D 3 are equally effective
• When single large doses are used, D 3 appears to be
preferable compared to D 2 because the former has a longer
half-life
• Duration : minimum of 12 weeks, recognizing that some
children may require a longer treatment duration

Vitamin D synthesis(Mankin part 1)
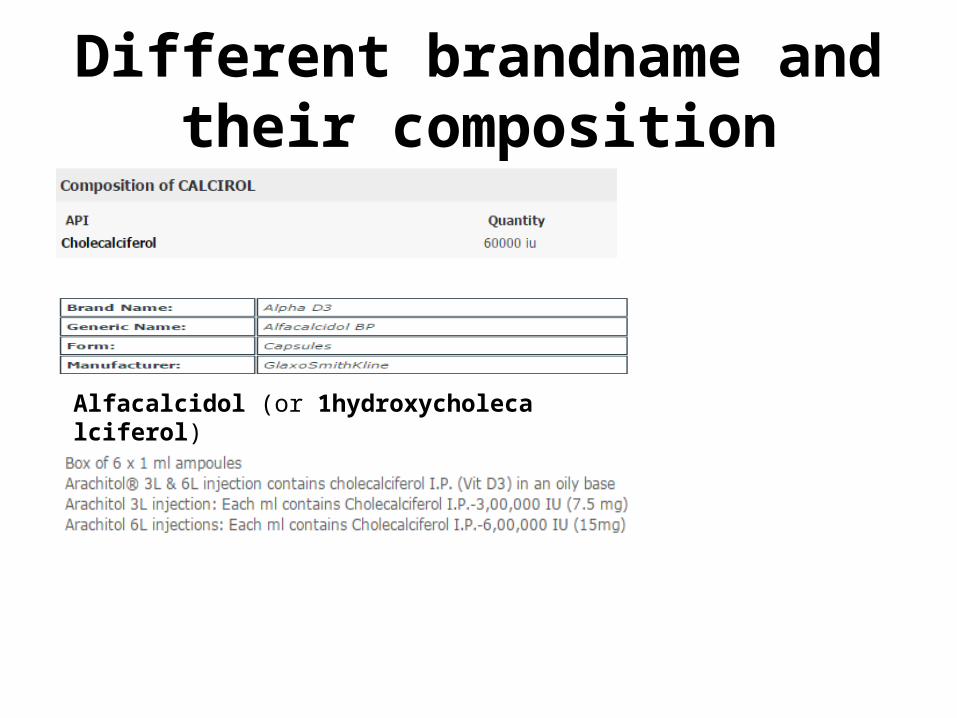
Different brandname and their composition
Alfacalcidol (or 1hydroxycholecalciferol)
The sunlight
• No exact studies done yet as it is multifactorial
• UVB (290-315 nm) is preferable
• The more oblique rays are absorbed by ozone so less role
before 10 am and after 3 pm“A healthy adult in a bathing suit exposed to
an amount of sunlight that causes a minimal erythema (lightpinkness to the skin 24 h after exposure; 1 MED) is equivalent
to ingesting approximately 20,000 IU of vitamin D”

Factors affecting solar vitamin D
• Latitude• Pigmentation• Age• Use of sunscreen SPF 30• Glass• Time of day
Prevention of Osteomalacia During Pregnancy and Lactation and Congenital
Rickets• Pregnant women should receive 600 IU/d of supplemental
vitamin D
• Pregnant women do not need calcium intakes above
recommended nonpregnant intakes to improve neonatal bone
• Advantages of taking supplementation during pregnancy: 1.Prevention from large fontenelle 2.Avoids neonatal hypocalcemia 3.Prevention from congenital rickets 4.Improve dental enamel formation

• Maternal calcium intake during pregnancy or lactation is not
associated with breast milk calcium concentrations
• Lactating women should not take high amounts of vitamin D
as a means of supplementing their infant
• Lactating women should ensure they meet the dietary
recommendations for vitamin D (600 IU/d)
Influence of calcium or vitamin D supplementation in pregnancy or lactation on breast milk calcium or vitamin D