Embed Size (px)
Citation preview

NURSES BURNOUT: IMPLICATIONS FOR NURSING LEADERSHIPSTEVE IDUYEDALHOUSIE UNIVERSITY
OUTLINE
INTRODUCTION TO BURNOUT SYNDROME AMONG NURSES
CAUSES THEORETICAL FRAMEWORK STAGES OF BURNOUT
IMPACTS OF BURNOUT BURNOUT CYCLE HOW TO ADDRESS BURNOUT MEASUREMENT AND EVALUATION
APPROACH RECOMMENDATIONS
A VIDEO EXCERPT ON NURSES BURNOUT

A VIDEO EXCERPT ON NURSES BURNOUT
What can you say about Jimmy?
INTRODUCTION TO NURSES BURNOUT
World Health Organization reported a shortage of 4.3 million healthcare workers globally, and estimated that over the next two decades this figure would increase by 20%(Laschinger, Grau, Finegan, & Wilk, 2010).
In Canada As more nurses become eligible for retirement each year than those
graduating from nursing education programs, and with the alarmingly high rates of turnover intentions, the ability of the nursing workforce to sustain itself is severely threatened (Laschinger, Grau, Finegan, & Wilk, 2010).
INTRODUCTION TO NURSES BURNOUT
CNA (2009) warns that Canada may suffer a shortage of 60,000 full-time equivalent RNs by 2022 (Canadian Nurses Association, 2009).
The new graduated nurses who represent the future of the profession are not encouraged to stay. Several studies have shown that new graduates’ working conditions are stressful and have resulted in increased levels of burnout (Cho et al. 2006, Gustavsson et al. 2010).
Evidence suggest that the first two years of practice influences new nurses’ desire to leave the profession due to burnout (Beecroft et al., 2008).

INTRODUCTION TO NURSES BURNOUT
A recent study of 309 new nurses in Quebec found that 43% reported a high level of psychological distress.
The same study revealed that 62% of respondents intended to quit their present jobs for other jobs in nursing, and 13% intended to leave the profession entirely
(Lavoie-Tremblay, O’Brien-Pallas, Desforges & Marchionni, 2008)

WHAT IS BURNOUT
International Classification of Diseases ICD-10 defines Burnout as a clinical condition or a work-related neurasthenia with the following symptoms. A persistent and distressing complaints of exhaustion after a
minor mental effort, or a persistent and distressing complaints of fatigue and bodily weakness after minimal physical effort.
At least two out of the following six distress symptoms: muscular aches and pain, dizziness, tension headaches, sleep disturbance, inability to relax, or irritability
WHAT IS BURNOUT
The patient is unable to recover from the symptoms by means of rest
The duration of the disorder is at least three months The criteria for any more specific disorders do not apply. SCHAUFELI & ENZMAN, 1998
WHAT IS BURNOUT
Diagnostic and Statistical Manual of Mental Disorders DSM-IV describes Burnout as a mental adjustment disorder which are characterized by “the development of clinically significant emotional or behavioral symptoms in response to an identifiable psychosocial stressor or stressors.
The two definitions provide three hallmarks or characteristics of burnout Mental Exhaustion Depersonalization Lack of Career accomplishment
(Schaufeli & Enzman, 1998)

WHAT BURNOUT IS NOT
Burnout has often been mistaken for Stress, Depression or Post-Traumatic Disorder due to similarities in their symptoms.
IN STRESS Stress produces urgency and hyperactivity. Burnout, on the
other hand, produces helplessness. (Burisch, 2006) Emotions associated with stress are over-reactive, those
associated with burnout are more blunted.( Burisch, 2006)

WHAT BURNOUT IS NOT
IN DEPRESSION Depression may extend over every life domain (e.g., work, family, leisure).
Burnout, however, is specific to work context (Maslach et al., 2001).
IN POST-TRAUMATIC DISORDER Post traumatic stress disorder (PTSD) is “caused by the exposure to a
traumatic event or extreme stressor that is responded to with fear, helplessness, or horror”.
Burnout, on the other hand, is caused mainly by interpersonal and emotional stressors in the workplace and is characterized by different reactions e.g emotional exhaustion. (Mealer, Burnham, Goode, Rothbaum & Moss, 2009, p. 1118).

CAUSES OF BURNOUT

THEORETICAL FRAMEWORK
Structural Empowerment Theory (Kanter, 1977 & 1993) theory of structural empowerment in organizations
conceptualizes empowering conditions as social structures in the workplace that enable employees to accomplish their work in meaningful ways.
The empowering conditions are derived from the ability of the leadership to mobilize human and material resources to accomplish work and is attained through access to information, support and resources in the work setting.
According to Kanter (1993), when employees have access to these working conditions, they will be empowered to accomplish their work in meaningful ways.
Moreover, the absence of this structural empowerment in a workplace creates a toxic environment for nurses.
Laschinger,Grau, Finegan,& Wilk,(2010).

THEORETICAL FRAMEWORK
A Dualistic Model (Passion and Harmonious Theory)
This model posits that obsessive passion produces conflict between work and other life activities because the person cannot let go of the work activity. Conversely, harmonious passion is expected to prevent conflict while positively contributing to work satisfaction.
With obsessive passion, one displays rigid persistence attitude toward work and cannot let go of one’s work involvement. This is expected to lead to conflict between work and other life activities and consequently to burnout.
(Vallerand, Paquet, Philippe, & Charest, 2010).

THEORETICAL FRAMEWORK
A Dualistic Model (Passion and Harmonious Theory)
Whereas, in harmonious passion, the individual maintains control over the passionate activity, and can physically and mentally disengage from the work activity when needed
Because of this sense of balance in harmonious passion, the person is protected from the experience of conflict between work and other life activities, one is also protected from the experience of mental and emotional staleness, and from burnout.
This explains why in the same organization, one individual is thriving well, whereas another one is experiencing burnout symptoms.
(Vallerand, Paquet, Philippe, & Charest, 2010).
THEORETICAL FRAMEWORK To test the proposed Dualistic Model in France Hospitals. A study
using cross-sectional design with experienced registered nurses was carried out.
It was posited that obsessive passion would positively predict conflict between work and other life activities.On the other hand, harmonious passion was expected to positively predict work satisfaction.
Vallerand et al, 2010

THEORETICAL FRAMEWORK
Method A total of 97 nurses working in France hospitals took part in the study. Most of them were female nurses (90 women, 6 men, and 1 missing
value) Their ages range between 21 and 57 years (M 34.07 years, SD 9.95
years). The nurses were working on average of 34.15 hr per week (SD 4.16 hr)
and had been working as nurses for an average of 11.21 years (SD 10.12 years
Vallerand et al, 2010

THEORETICAL FRAMEWORK
Instrumentation The Passion Scale: is composed of two subscales of six items
each, assessing harmonious (HP) and obsessive (OP) passion.
Each item is responded to a 7-point Likert scale ranging from 1 (do not agree at all) to 7 (completely agree).
Vallerand et al, 2010

THEORETICAL FRAMEWORK
Maslach Burnout Inventory is composed of 22 items assessing burnout with three subscales tapping emotional exhaustion, depersonalization, and diminished personal accomplishment
The Satisfaction at Work Scale (SAWS)assesses work satisfaction. The SAWS contains five items responded to on a 7-point Likert scale (1 = do not agree at all, 5= completely agree)
Vallerand et al, 2010

THEORETICAL FRAMEWORK
Result As predicted, with significant p-value for 0P and HP, OP
predicted conflict that was in turn associated with burnout. while, HP positively predicted satisfaction at work.
The former playing a facilitative role and the latter a protective role in burnout.
Vallerand et al, 2010
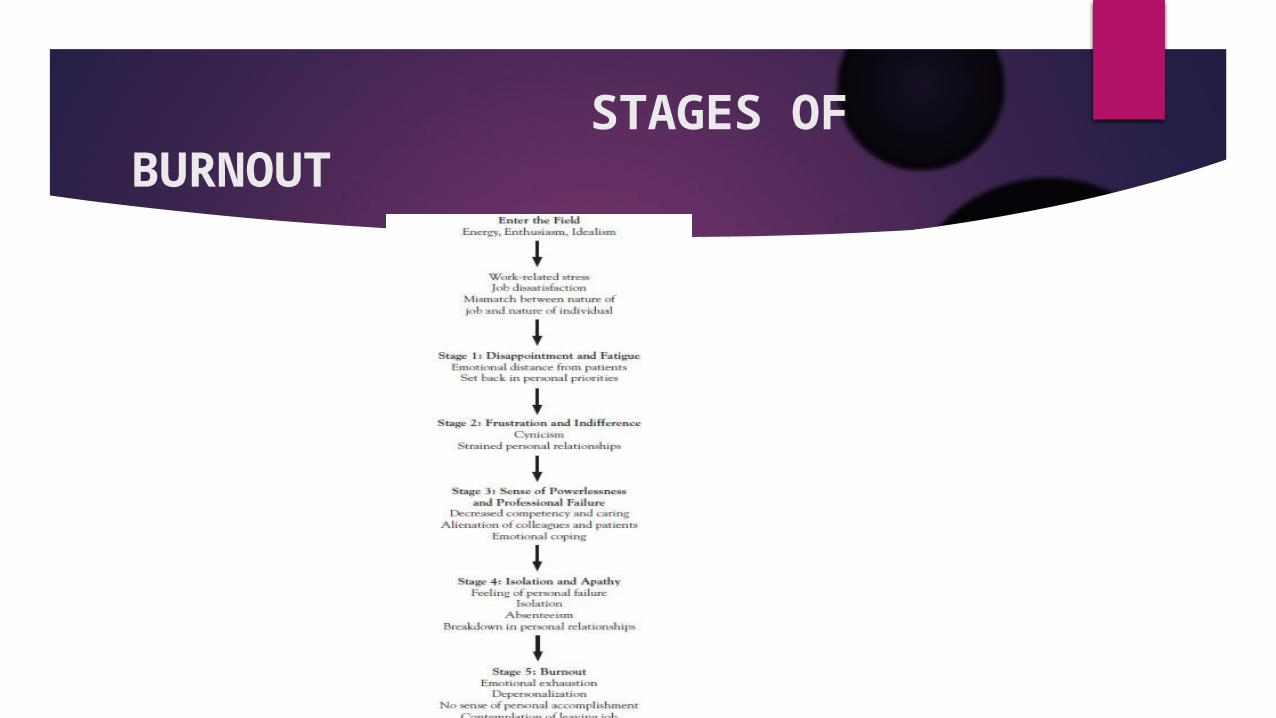
STAGES OF BURNOUT
SIGNS & SYMPTOMS OF BURNOUTAffective signals: • Depressed mood / changing moods • Tearfulness • Emotional exhaustion • Increased tension / anxiety Cognitive signals: • Helplessness / loss of meaning and hope • Feelings of powerlessness / feelings of being “trapped” • Sense of failure • lack of career fulfillment• Guilt • Inability to concentrate / forgetfulness / difficulty with complex tasks Schaufeli and Enzman (1998)

SIGNS & SYMPTOMS OF BURNOUT
Behavioral signals: • Hyperactivity / impulsivity • Increased consumption of: caffeine, tobacco, alcohol, illicit drugs • Abandonment of recreational activities • Compulsive complaining / denial Motivational signals: • Loss of zeal / loss of idealism • Resignation • Disappointment • Boredom Schaufeli and Enzman (1998)
SIGNS & SYMPTOMS OF BURNOUT
Physical signals: • Headaches • Nausea • Dizziness • Muscle pain • Sleep disturbances • Ulcer / gastro-intestinal disorders • Chronic fatigue Schaufeli and Enzman (1998)
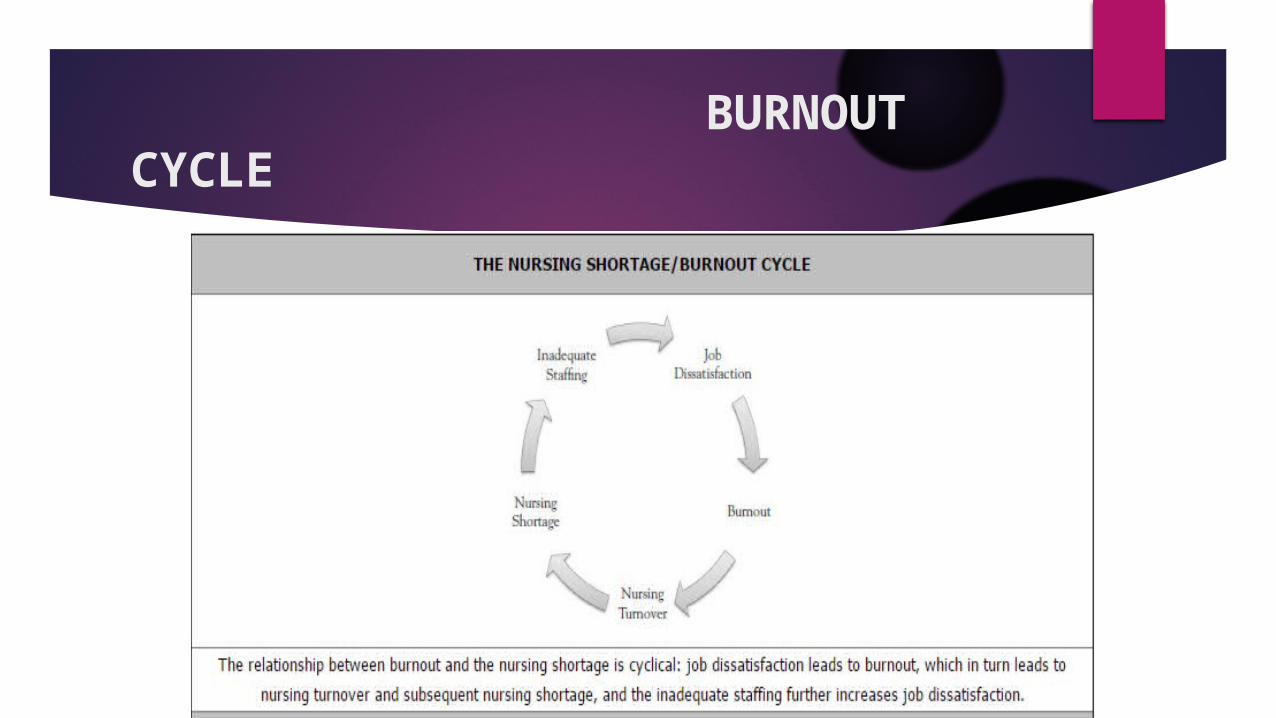
BURNOUT CYCLE

IMPACTS OF BURNOUT
The nursing shortage has far-reaching effects on the quality of care and patient safety (Alexandra, 2015). A lot of studies have demonstrated the nurses shortage often leads to burnout with resultant effects:On Nurses Inadequate staffing and continuous overtime for nurses Decrease quality of care The potential for medication errors
IMPACTS OF BURNOUT
On Patients
Medication adverse effects for patients and patient mortality. Increase patients neglect, cross infections or complications Patient Dissatisfaction

IMPACTS OF BURNOUT
On Management
High rates of employee turnover Increased employee absenteeism due to clinical symptoms of diseases It creates a hostile and toxic work environments and increases lawsuits
for the management.

HOW TO ADDRESS BURNOUT
MEASUREMENT & EVALUATION
The criterion standard for measuring burnout is the MBI (Maslach Burnout Inventory), a self-assessment tool first published in 1981 by Maslach and Jackson
The tool has been shown to be reliable, valid, and easy to administer and has been translated into several languages for use around the world.
The MBI is often used in conjunction with other assessments to evaluate the relationship between burnout and organizational policies, productivity, and social support
Maslach C, Jackson SE. (1981) Maslach Burnout Inventory.

MEASUREMENT & EVALUATION
The MBI addresses the three defining aspects of burnout syndrome with 22 statements in three subscales
Emotional exhaustion: Nine statements to measure feelings of being emotionally overextended and exhausted by one's work
Depersonalization: Five statements to measure an unfeeling and impersonal response to the recipients of one's services, care treatment, or instruction
Personal accomplishment: Eight statements to measure feelings of competence and successful achievement in one's work
Maslach C. (2003) Burnout: The Cost of Caring
MEASUREMENT & EVALUATION
Another useful tools is The General Health Questionnaire in conjunction with the MBI which can help professionals gain a better understanding of the sources of stress for individuals.
The General Health Questionnaire has been translated into several languages and is available in a variety of versions. the version with 28 items (GHQ-28) has been used most often in workplace settings.
A score of 0 to 3 is assigned to four possible responses ("not at all," "no more than usual," "rather more than usual," and "much more than usual")
Jackson C. (2007)The General Health Questionnaire. Occup Med.

MEASUREMENT & EVALUATION
Another tool for measuring burnout is the Burnout Risk Survey.
This tool is designed to demonstrate the probability of mismatches between an individual and his or her work environment.
A "yes" response to three or more of these items indicates a risk of burnout and a "yes" response to four or more items indicates a high risk.
Pfifferling JH. (2015) Burnout Risk Appraisal.

RECOMMENDATIONS
Lifestyle Modification Approach Take Care of Yourself First Nurses are trained to put the care of others ahead of themselves. It is important
for nurses to recognize that self-care is not equivalent to selfishness; rather, self-care is essential for energizing, restoring, and maintaining the physical and emotional stamina to reduce fatigue and manage stress.
Nurses should also seek outside activities that will help them disengage from their professional routine and provide enjoyment, such as yoga, music, art, reading, journaling, sports, and volunteerism.
Maslach C. (2003) Burnout: The Cost of Caring

RECOMMENDATIONS
Quick identification of the signs and symptoms of stress overload and burnout should be a continuous process, and individuals should remain alert to the use of unhealthy and ineffective coping mechanisms, such as excessive use of caffeine, alcohol, or prescription medication; overeating or undereating; smoking; inactivity; or social withdrawal ( Carr, 2006)
Individual should focus on changing one behavior at a time and seek help from professional counseling if necessary (American Psychological Association,2015)
RECOMMENDATIONS
Enhance Interpersonal and Social Relationships by remaining connected to a positive social network of people
Grief Well: Grieving well involves accepting the reality of the loss, experiencing the pain of grief, adjusting to the absence, and moving on with life (Worden, 1991).
Become an advocate for changes in the work environment can help nurses increase a sense of control (Maslach, 2003)
RECOMMENDATIONS
Structural Empowerment in Organizational culture An integral step in preventing burnout is to survey staff about important aspects of the
organizational culture Organizations can protect nurses from burnout by creating an organizational culture of trust,
support, and open communication and fostering a healthy work environment through1. Appropriate staffing2. Meaningful recognition3. True collaboration4. Skilled communication5. Effective decision making6. Authentic leadership (AACN, 2015)

RECOMMENDATIONS
Improve Issues Related to Staffing and Work Hour: how?Employers should stop using mandatory overtime as a staffing solution
Employers should adopt official policy that gives RNs the "right to accept or reject a work assignment" to prevent risks from fatigue. The policy should be clear that rejecting an assignment under these conditions is not patient abandonment and that RNs will not be retaliated against or face negative consequences for rejecting such an assignment
Alexandra 2015
RECOMMENDATIONS
Let bring humanity back to our workplaces

QUESTIONS?
Questions Clarifications Contributions Answers
THANK YOU FOR LISTENING

References
Alexandra, L (2015) Burnout: Impact on Nursing and Quality of Care. Retrieved on the 8th June, 2016 from http://www.netce.com/coursecontent.php?courseid=1167
A video excerpt on nurses burnout (2015) retrieved https://www.youtube.com/watch?v=0ILcmfHmpfI Borgogni, L, Consiglio, G. Alessandri, W.B. Schaufeli (2012) Don’t throw the baby out with the bathwater! Interpersonal
strain at work and burnout. Eur. J. Work Organ. Psychol., 21 (6) (2012), pp. 875–898 Burisch, M. (2006). Das Burnout-Syndrom: Theorie der inneren Erschöpfung [The Burnout- Syndrome: A Theory of inner
Exhaustion]. Heidelberg: Springer Medizin Verlag. American Association of Critical-Care Nurses. AACN Standards for Establishing and Sustaining Healthy Work
Environments. Available athttp://www.aacn.org/wd/hwe/docs/hwestandards.pdf. Last accessed June 6, 2016 Canadian Nurses Association (2002) Planning for the Future: Nursing Human Resource Projections. Canadian Nurses
Association, Ottawa. Carr JL (2006) Healthy Nurse: Escape Burnout and Discover the Ultimate Life/Work Balance. Columbus, IN: Matilda
Publishing; 2006. Cho J., Laschinger H.K.S. & Wong C. (2006) Workplace empowerment, work engagement and organizational commitment
of new graduate nurses. Nursing Leadership 19(3), 43–60. Gustavsson J.P., Hallsten L. & Rudman A. (2010) Early career burnout among nurses: modelling a hypothesized process
using an item response approach. International Journal of Nursing Studies 47(7), 864–875. Laschinger, H. S., Grau, A. L., Finegan, J., & Wilk, P. (2010). New graduate nurses' experiences of bullying and burnout in
hospital settings. Journal Of Advanced Nursing, 66(12), 2732-2742 11p. doi:10.1111/j.1365-2648.2010.05420.x
References
Maslach C. (2003) Burnout: The Cost of Caring. Cambridge, MA: Malor Books. Maslach C, Jackson SE. (1981) Maslach Burnout Inventory. Palo Alto, CA: Consulting Psychologists Press. Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397-422.
doi:10.1146/annurev.psych.52.1.397 Mealer, M., Burnham, E. L., Goode, C. J., Rothbaum, B. & Moss, M. (2009). The prevalence and impact of post traumatic stress disorder
and burnout syndrome in nurses. Depression & Anxiety, 26, 1118-1126. Pfifferling JH. Burnout Risk Appraisal. Available at http://www.cpwb.org/burnout_information.htm. Last accessed June 12, 2016 Vallerand, R., Paquet, Y., Philippe, F., & Charest, J. (2010). On the Role of Passion for Work in Burnout: A Process Model.Journal of Personality, 78(1),
289-312. Worden JW. (1991)Grief Counseling and Grief Therapy: A Handbook for the Mental Health Professional. 2nd ed. New York, NY: Springer. Spinetta JJ, Jankovic M, Ben Arush MW, et al. Guidelines for the recognition, prevention, and remediation of burnout in health care
professionals participating in the care of children with cancer: report of the SIOP Working Committee on Psychosocial Issues in Pediatric Oncology. Med Pediatr Oncol. 2000;35(2):122-125.
Schaufeli, W. B. & Enzman, D. (1998). The burnout companion to study & practice. London: Taylor & Francis.





























