Embed Size (px)
Citation preview

04/12/2023 FOUAD[NCI] 1
Limited liver resection with limited mobilization:
A preferred surgical technique in cirrhotic patients with hepatocellular carcinoma
Fouad A. Fouad M.D ., Tarek k.Saber M.D

04/12/2023 FOUAD[NCI] 2
INTRODUCTION
• Hepatocellular carcinoma (HCC) is the fifth most common cancer.
• The third leading cause of cancer death worldwide.
• Surgical treatment is an effective treatment for HCC.

04/12/2023 FOUAD[NCI] 3
THE AIM OF THE THIS STUDY
• We aimed to evaluate if • Limited hepatic ligaments dissection and • Limited hepatic volume resection
Decreased risk of operative and post operative morbidity , mortality and hospital stay.

04/12/2023 FOUAD[NCI] 4
METHODS
• Data of twenty nine patients with HCC on a background of cirrhosis were studied during the period from January 2002, to December 2009.
• Patients were operated upon in the department of surgical oncology in the National Cancer Institute Cairo University.

04/12/2023 FOUAD[NCI] 5
METHODS
• Group (A) included sixteen patients in whom wide anatomical hepatic resection of more than one hepatic segments done and needed hepatic mobilization.
• Group (B) included thirteen patients who underwent limited hepatic resection inform of resection of the lesion regardless of segmental or lobar anatomy and did not need hepatic mobilization.

04/12/2023 FOUAD[NCI] 6
• ELIGIBILITY CRITERIA for patient inclusion in the study were: Patients selected with a single tumor 5 cm or smaller and two tumors each 3 cm or less.
• EXCLUSION CRITERIA :Extra hepatic metastases, and inferior vena cava or main portal vein tumor thrombus precluded curative hepatic resection.

04/12/2023 FOUAD[NCI] 7
TECHNIQUE
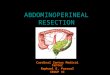
• Anatomical resection: was defined as the systematic removal of a hepatic segment confined by cancer-bearing portal tributaries and needed hepatic mobilization in which resection of more than one Couinaud segments.

04/12/2023 FOUAD[NCI] 8
COUINAUD SEGMENTS

04/12/2023 FOUAD[NCI] 9
TECHNIQUE
• Limited non anatomical resection was defined as the resection of a lesion regardless of segmental or lobar anatomy without hepatic mobilization.

04/12/2023 FOUAD[NCI] 10

04/12/2023 FOUAD[NCI] 11

04/12/2023 FOUAD[NCI] 12
Clinicopathological and
surgical data for 29 HCC patients
Variable Group(A)Anatomical resection+ hepatic mobilization(NO.=16)
Group(B)Limited non-anatomical resection(NO.=13)
P value
Age Years (mean±SD)
56±13 61±11 0.2802
Sex(M:F) 11:5 9:4 0.312Hepatitis c virus 100% 100%
Child-Pugh score 5.7±o.5 6.1 ±o.4 0.1271
Liver cirrhosis Present/absent
16/0 13/0 1.000
Tumor size cm (mean ± SD)
5.1 ± 0.9 4.7 ± 1.1 0.2906
a-fetoprotein (ng/ml) ± SD
590±150 630±o213 0.5771

04/12/2023 FOUAD[NCI] 13
Operative data of hepatic resection for 29 HCC patients
Variable Group(A)Anatomical resection+ hepatic mobilization(NO.=16)
Group(B)Limited non-anatomical resection(NO.=13)
P value
Operative time (min.)
113.3±38.4 107.8±31.7 0.6504
Blood loss (mean ± SD) ml
253±87.3 145.1±25 0.0002
Hepatic ligaments cutting (yes/no)%
(16/16)% 1/130.005
Surgical margin mm (mean ± SD)
8.3 ± 5.9 7.4 ± 5.4 0.6748

04/12/2023 FOUAD[NCI] 14
Post operative mortality and
morbidity for 29 HCC patientsVariable Group(A)
Anatomical resection+ hepatic mobilization(NO.=16)
Group(B)Limited non-anatomical resection(NO.=13)
P value
Mean hospital stay(days) 7±6.3 3±2.4 0.0399
Operative mortality (one month death)
1/16(6.5%) 0/13% 0.567
Postoperative Morbidity(total)
10/16(62.5%) 1/13(7.5%) 0.036
Bleeding Jaundice
1/161/16
0 /130/13
Ascites Mild Moderate Severe Encysted ascites
8/164/162/161/61/16
1/131/130/130/130/13

04/12/2023 FOUAD[NCI]
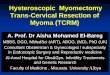
Kaplan-Meier survival curve for 29 patients with HCC
0 10 20 30 40 50 60 70
0
20
40
60
80
100
Time
Surviv
al probability (
%)
GROUPAB
15
P = 0.9291
The overall survival 3-years and 5-years survival in: group A patients was 68% ;39% and in group B was 65%; 33%.

04/12/2023 FOUAD[NCI] 16
CONCLUSIONS• Surgical treatment of HCCs, the balance
between curability and hepatic function preservation is important.
• Limited liver resection with limited mobilization is the preferred technique for HCC in cirrhotic patients.
• Anatomical resection with hepatic mobilization did not improve the overall survival compared with limited hepatic resection.

04/12/2023 FOUAD[NCI] 17
CONCLUSIONS
• Increased risk of operative morbidity were identified in patients who had, resection of :
• A large volume of functioning liver parenchyma • Extensive hepatic mobilization and dissection of the
hepatic ligaments increase post operative morbidity especially ascites due to increase lymphatic transudation ; increase portal hypertension.

04/12/2023 FOUAD[NCI] 18