Embed Size (px)
Citation preview

Polycystic Ovarian
Syndrome

Polycystic Ovarian Syndrome (PCOS)Overview
Polycystic ovarian syndrome (Stein-Leventhal syndrome) is a complex endocrine disorder affecting women in their reproductive years.It is characterized by increased androgen production and disordered gonadotropin secretion, which results in chronic anovulation.
It is the leading cause of anovulatory infertility and hirsutism.PCOS is also associated with disorders of reproduction, metabolism, and general health, including increased risk of miscarriage, insulin resistance, hyperlipidemia, cardiovascular disease, and endometrial cancer.
Obesity is common but not universal in women with PCOS.Women with PCOS have high rate of type 2 diabetes; these women have hyperlipidemia and a greatly increased risk of cardiovascular disease.

INTRODUCTION
• Most common cause of infertility in women
• Classic syndrome originally described by Stein and Levanthal
• Hyperandrogenism• Menstrual irregularity• Polycystic ovaries• Central adiposity
• Syndrome, not a disease—multiple potential etiologies with variable clinical expression

Why is PCOS important?
• Affects 4-12% of women of reproductive age
• Significant association between obesity, insulin resistance, and PCOS.
• Huge impact on the reproductive, metabolic, and cardiovascular health of affected women.

Clinical Features of PCOSMenstrual Irregularity
• May appear at puberty with a delayed menarche followed by the onset of irregular periods or as the breakdown of a previously regular cycle
• Anovulation is usually chronic and presents as oligomenorrhea or amenorrhea

Clinical Features of PCOSHyperandrogenism
• Symptoms may include hirsutism, acne,
male pattern balding, and/or male
distribution of body hair
Hirsutism Acne

Pathogenesis
1. Hyperandrogenism
2. Insulin resistance

Common Endocrine Abnormalities in PCOS
• Elevated luteinizing hormone (LH)• Increased LH/follicle-stimulating
hormone (FSH) ratio• Elevated androgen levels• Decreased sex hormone binding
globulin levels


In PCOS, discovered increased pulse frequency of GnRH (2/2 abnml pulse generator), resulting in relatively increased pulse frequency of LH, over FSH. Increased frequency of LH pulses in PCOS. Progesterone administration can restrain rapid pulse frequency. Increased LH results in increased production of androgens by ovarian theca cells.
INSULIN acts synergistically with LH to enhance androgen production. INSULIN suppresses SHBG (the key protein that binds testosterone), resulting in increased free testosterone. TESTOSTERONE inhibits and estrogen stimulates hepatic synthesis of Sex hormone-binding globulin (SHBG).

Pathogenesis: Hyperandrogenism
• Symptoms of androgen excess
• Reduced sex-hormone-binding globulin (SHBG) more free testosterone conversion of androstenedione in adipose tissue
• Insulin insensitivity
• Lipid abnormalities
• Abdominal obesity

Metabolic Abnormalities in PCOS
• Hyperinsulinemia and insulin resistance• Insulin resistance may be independent of the
effect of obesity• Decreased peripheral insulin sensitivity and
consequent hyperinsulinemia may play an important role in the pathogenesis of PCOS

Lipid and Lipoprotein Abnormalities in PCOS
• Elevated LDL cholesterol• Elevated triglycerides • Decreased HDL cholesterol• Decreased apolipoprotein A-I• Impaired fibrinolytic activity

Pathogenesis: Insulin resistance
• Favors anovulation, androgen excess, reduced SHBG
• Metabolic syndrome
• Abdominal obesity


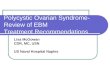
Abnormal Pituitary Function—Altered Negative Feedback Loop
• Increased GnRH from hypothalamus• Excessive LH secretion relative to FSH by pituitary
gland• LH stimulates ovarian thecal cells-- androgen
production • Ineffective suppression of the LH pulse frequency
by estradiol and progesterone• Androgen(such as testosterone or androsterone)
excess increases LH by blocking the hypothalamic inhibitory feedback of progesterone

hypothalamus
pituitary
ovary
GnRH
LH
androgens
Androgens block inhibitory effect of progesterone
X

Abnormal steroidogenenesis
• Intraovarian androgen excess results in excessive growth of small ovarian follicles
• Follicular maturation is inhibited
• Excess androgen causes thecal and stromal hyperplasia

HYPERINSULINEMIA
• Excess insulin production and insulin resistance
• Genetic link
• Hyperandrogenism vs. hyperinsulinemia– Which came first?

DIAGNOSTIC CRITERIA
AND
CLINICAL MANIFESTATIONS

– Menstrual irregularity due to anovulation or oligo-ovulation
– Evidence of clinical or biochemical hyperandrogenism
• Hirsutism, acne, male pattern baldness
• High serum androgen levels
– Exclusion of other causes (CAH, tumors, hyperprolactinemia)
DIAGNOSTIC CRITERIA

MENSTRUAL DYSFUNCTION
• Oligo or amenorrhea– Menstrual irregularity typically begins in the peripubertal
period– Delayed menarche
• Reduction in ovulatory events leads to deficient progesterone secretion
• Chronic estrogen stimulation of the endometrium with no progesterone for differentiation—intermittent breakthrough bleeding or dysfunctional uterine bleeding
• Increased risk for endometrial hyperplasia and/or endometrial CA


HYPERANDROGENISM
• Hirsutism, acne, male pattern balding, alopecia
• 50-90% patients have elevated serum androgen levels
• Free testosterone levels most sensitive
• Rare: increased muscle mass, deepening voice, clitormegaly (should prompt search for underlying neoplasm)

Diagnosis
1. Hyperandrogenism (cont’d) Laboratory features
Elevated total testosterone Most values in PCOS <150 ng/dl (if >200 ng/dl, consider ovarian or
adrenal tumor) Free testosterone assays not reliable yet
DHEA-S Most normal or slightly high in PCOS If >800 mcg/dl, consider adrenal tumor
LH/FSH ratio Levels vary over menstrual cycle, released in pulsatile fashion,
affected by OCPs (contraceptives) LH/FSH ratio >2 has little diagnostic sensitivity

Diagnosis
2. Oligoovulation or anovulation Oligomenorrhea or amenorrhea Dysfunctional uterine bleeding Infertility
30-50% 1st trimester miscarriage rate
3-fold increased risk endometrial carcinoma

Diagnosis
3. Polycystic Ovaries Criteria by ultrasound
Increased ovarian area (>5.5 cm2) or volume (>11 ml) w/ presence of >12 follicles measuring 2-9 mm in diameter
Polycystic ovaries not specific for PCOS > 20% normal women have incidental
polycystic ovaries

OVARIAN ABNORMALITIES• Thickened sclerotic cortex
• Multiple follicles in peripheral location
• 80% of women with PCOS have classic cysts




INFERTILITY
• Intermittent ovulation or anovulation
• Inherent ovarian disorder—studies show reduced rated of conception despite therapy with clomid

Diagnosis
4. Absence of other disorders to account for these symptoms.
Pregnancy pregnancy test Hypothyroidism TSH Hyperprolactinemia prolactin Late onset congenital adrenal hyperplasia 17-
hydroxyprogesterone (r/o if <200 ng/dl) Ovarian tumor total testosterone (esp if >200 ng/dl)– Adrenal tumor DHEA-S (esp if > 800 mcg/dl)– Cushing’s syndrome salivary cortisol, 24 hr urine
cortisol

Diagnosis5. Supportive of insulin resistance
“Syndrome XX”: 3 or more of the following criteria:
• Waist circumference > 88 cm• Triglycerides > 150 mg/dl• HDL <50 mg/dl• BP > 130/85• Fasting glucose >110 mg/dl
ACOG and ADA suggest screening all women w/ PCOS for glucose intolerance, type 2 DM.
Oral glucose tolerance test more sensitive than fasting glucose.
Personal or family history of DM Acanthosis nigricans

OBESITY AND INSULIN RESISTANCE
• ½ patients with PCOS are obese
• > 80% are hyperinsulinemic and have insulin resistance (independent of obesity)
• Hyperinsulinemia contributes to hyperandrogenism through production in the theca cell and through its suppressive effects on sex hormone binding globulin production by the liver

ASSOCIATED MEDICAL CONDITIONS
• Increased risk of developing Type 2 Diabetes and Gestational diabetes
• Low HDL and high triglycerides• Sleep apnea• Nonalcoholic steatohepatitis• Metabolic syndrome—43% of PCOS
patients (2 fold higher than age-matched population)
• Elevated CRP and heart disease• Advanced atherosclerosis

DIFFERENTIAL DIAGNOSIS
1. Hyperprolactinemia– Prominent menstrual dysfunction
– Little hyperandrogenism
2. Congenital Adrenal Hyperplasia– morning serum 17-hydroxyprogesterone
concentration greater than 200 ng/dL in the early follicular phase strongly suggests the diagnosis
– confirmed by a high dose (250 mcg) ACTH stimulation test: post-ACTH serum 17-hydroxyprogesterone value less than 1000 ng/dL

3. Ovarian and adrenal tumors– serum testosterone concentrations are always
higher than 150 ng/dL– adrenal tumors: serum DHEA-S
concentrations higher than 800 mcg/dL– LOW serum LH concentrations
4. Cushing’s syndrome
5. Drugs: danazol; OCPs with high androgenicity

TESTING
• Serum HCG
• Serum prolactin
• Thyroid panel
• FSH: r/o ovarian failure
• Serum luteinizing hormone (LH)—elevated
• Serum estradiol—normal
• Serum estrone—elevated

TESTING
• Fasting glucose: elevated
• 2 hour OGTT: elevated
• Fasting insulin: elevated
• Free testosterone: elevated
• DHEA-S: normal
• 17-hydroxyprogesterone: normal
• Pelvic US
• Lipids

TREATMENT
Management
– Immediate/Acute issues– Hirsutism
– Regulation of menses
– Fertility issues
– Long-term issues– Insulin resistance
– Cardiovascular risk
– Malignancy risk

WEIGHT LOSS
• Weight loss
• Weight loss
• Weight loss

Management:Immediate/Acute Issues
• Regulation of menses• Oral contraceptives
• Periodic progesterone withdrawal– Medroxyprogesterone 10 mg/day x 7-10 days,
every 3 months (approx 4 menses annually)
• Lifestyle modification/weight loss
• Metformin- ie., hitting the “root cause”– 500-1000 mg bid, 6 month trial reasonable for
improvement of menses

Oligomenorrhea
• Combination estrogen-progestin pill first line when fertility is not desired– Decrease in LH secretion and decrease in
androgen production– Increase in hepatic production of sex-
hormone binding globulin– Decreased bioavailablity of testosterone– Decreased adrenal androgen secretion– Regular withdrawal bleeds– Prevention of endometrial hyperplasia

Management:Immediate/Acute Issues no fertility desired
• Monophasic antiandrogenic OCP– ON 1/35 (norethindrone)– Orthocyclen (norgestimate)– Desogen or Orthocept (desogestrel)– Yasmin
Fertility issues– Metformin– Thiazolidinediones

INFERTILITY TREATMENT
• Metformin– 500 mg daily– Increase by 500 mg each week until:
• Normal menses
• Reached max dose
• Side-effects
• Clomid– 50 mg days 3-7 for 3 months– 100 mg days 3-7 for 3 months

METFORMIN
• Decreases hepatic glucose production
• Reduces need for insulin secretion
• Improves insulin sensitivity (increases peripheral glucose uptake and utilization)
• Antilipolytic effect—reduces fatty acid concentrations and reduces gluconeogenesis

Infertility• Weight loss—reduction in serum testosterone
concentration and resumption of ovulation• Clomid: 80% will ovulate, 50% will conceive• Metformin: when added to clomid, improves
ovulatory rates • FSH injections• Laparoscopic surgery: wedge resections,
laparoscopic ovarian laser electrocautery• IVF=Vitro Fertilization

Management:Long-Term Issues
• Insulin resistance– Metformin
• Function– Lowers hepatic glucose production by reducing
gluconeogenesis
– Increases peripheral glucose uptake by skeletal muscle and adipose tissue
– Reduces intestinal glucose absorption
• Outcomes– Estimated 31% reduction in development of type II DM
over mean period 3 years
– Taken during pregnancy, reduction in gestational diabetes and major fetal complications

Management:Long-Term Issues
• Insulin resistance– Thiazolidinediones
• Function– Selective ligands of the nuclear transcription PPARγ,
expressed in adipose tissue, pancreatic beta cells, vascular endothelium, macrophages, HPO axis.
– “fatty acid steal” hypothesis» Promote fatty acid uptake and storage in adipose
tissue, sparing other tissues (muscle, liver) from harmful metabolic effects of free fatty acids (high levels in PCOS)
– Increased expression of adiponectin (adipocytokine with an insulin sensitivity effect)
– Decreased expression of 11β-hydroxysteroid dehydrogenase type 1 (enzyme converts inactive cortisone to active cortisol)

Management:Long-Term Issues
• Cardiovascular Risk– Increased prevalence of HTN– Dyslipidemia (↑ TG, ↓ HDL, ↑ LDL)– Predisposition to macrovascular disease and
thrombosis– Aggressive management…”CHAMP”?

Management:Long-Term Issues
• Risk for malignancy– 3X increased risk endometrial carcinoma
in PCOS– Increased risk of ovarian and breast
cancer– Warrants regular screening, low threshold
for endometrial biopsy


Diet and Exercise
In patients with PCOS who are obese, endocrine-metabolic parameters markedly improve after 4-12 weeks of dietary restriction.
Their SHBG levels rise and free testosterone levels fall by 2-fold.
Serum insulin and IGF-1 levels also decrease.
Weight loss in patients with PCOS who are obese is associated with a reduction of hirsutism and a return of ovulatory cycles in 30% of women.

Diet and Exercise A moderate amount of daily exercise increases of levels of IGF-
1 binding protein and decreases IGF-1 levels by 20%.
Modest weight loss of 2-5% of total body weight can help restore ovulatory menstrual periods in obese patients with PCOS.
A daily 500-1000 calorie deficit with 150 minutes of exercise per week can cause ovulation.
The Androgen Excess and Polycystic Ovary Syndrome Society recommends lifestyle management as the primary therapy in overweight and obese women with PCOS for the treatment of metabolic complications.