Embed Size (px)
Citation preview
Closed Fractures of the Tibial Diaphysis
David Templeman, MDRobert Cantu, MD
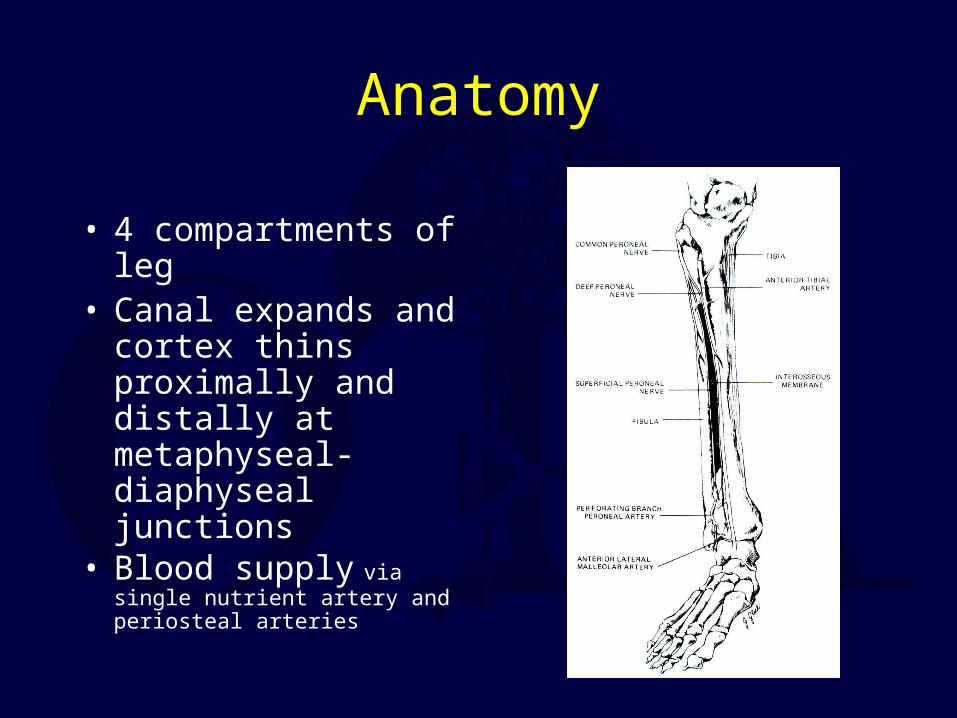
Anatomy
• 4 compartments of leg• Canal expands and
cortex thins proximally and distally at metaphyseal-diaphyseal junctions
• Blood supply via single nutrient artery and periosteal arteries
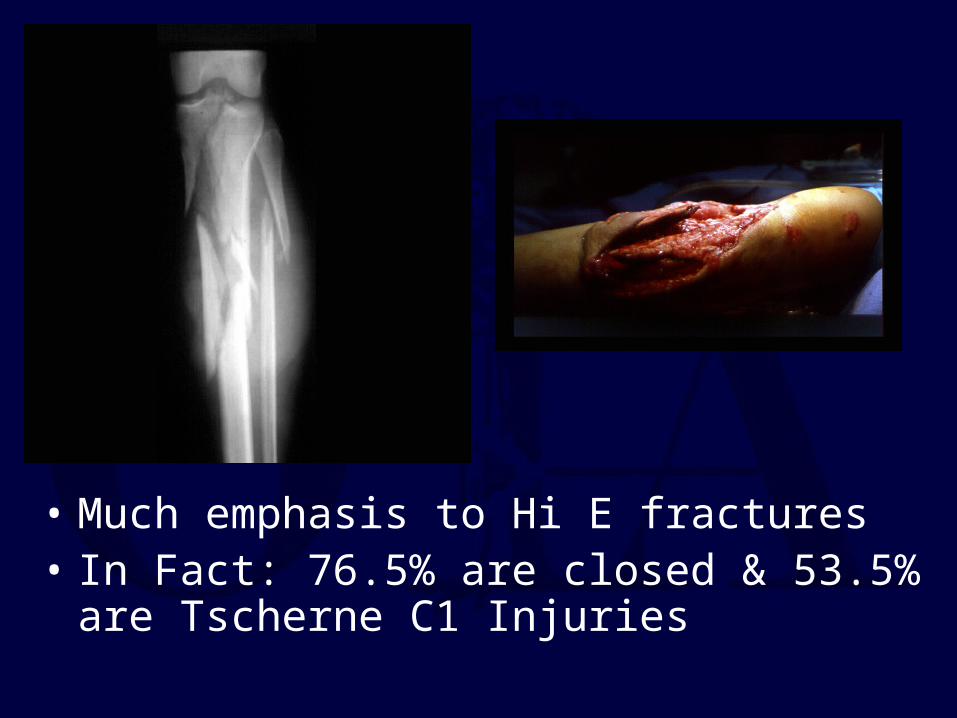
• Much emphasis to Hi E fractures• In Fact: 76.5% are closed & 53.5% are Tscherne
C1 Injuries
Tibial Fractures
• 492,000 per year (incidence)• 100,000 nonunions per year (prevelance)
Physical Exam
• Pain, inability to bear weight, and deformity may be seen
• Local swelling and edema variable
• Careful inspection of soft tissue envelope necessary, including compartment swelling
• Thorough neurovascular assessment including motor/sensory exam and distal pulses
Physical Exam
• Soft tissue injury with high-energy crush mechanism may take several days to fully declare itself
• Repeated exam often necessary to follow compartment swelling
Radiographic Evaluation
• AP and Lat views of entire tib/fib required from knee to ankle
• Oblique views can be helpful in follow-up to assess healing
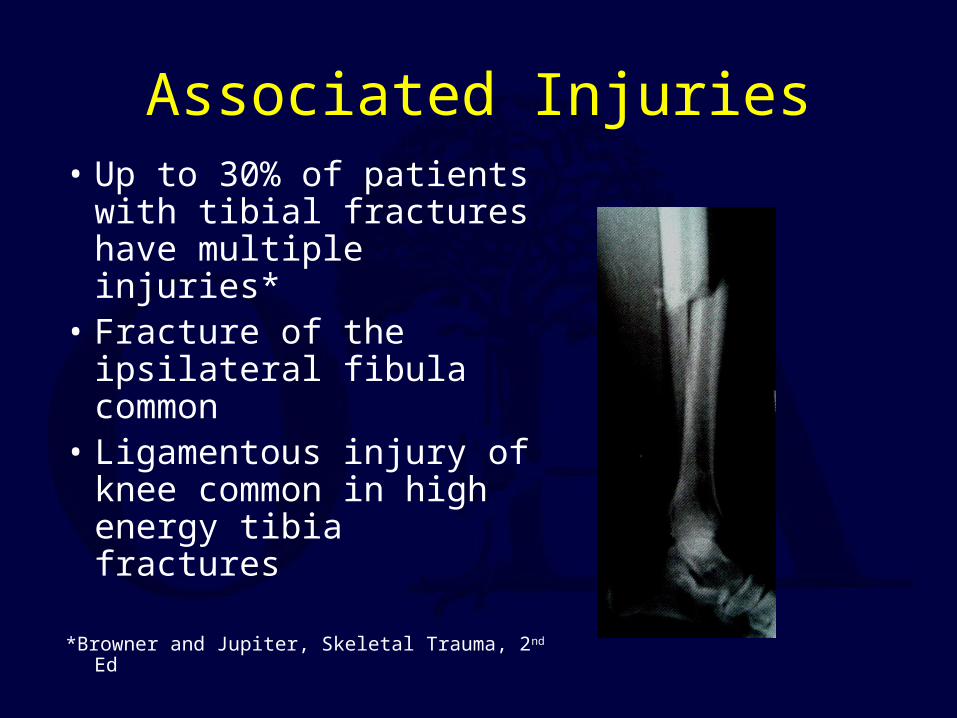
Associated Injuries• Up to 30% of patients
with tibial fractures have multiple injuries*
• Fracture of the ipsilateral fibula common
• Ligamentous injury of knee common in high energy tibia fractures
*Browner and Jupiter, Skeletal Trauma, 2nd Ed
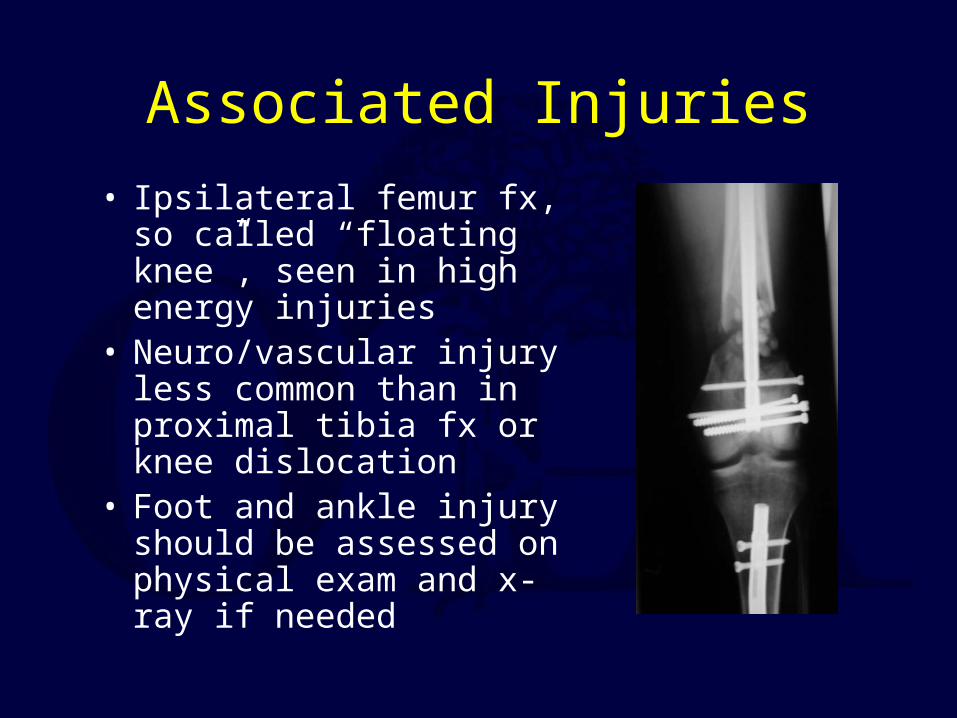
Associated Injuries• Ipsilateral femur fx, so
called “floating knee”, seen in high energy injuries
• Neuro/vascular injury less common than in proximal tibia fx or knee dislocation
• Foot and ankle injury should be assessed on physical exam and x-ray if needed
Classification
• Numerous classification systems have been proposed
• Important variables are pattern and location of fracture, associated fibula fracture, extent of comminution, and degree of soft tissue injury
Johner and Wruh’s Classification
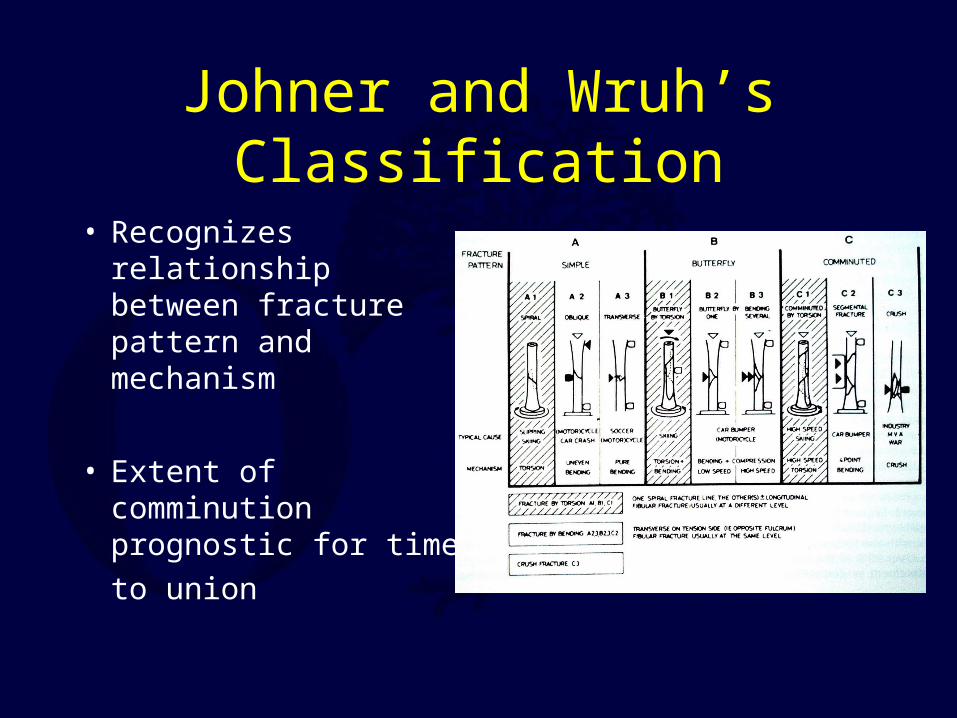
• Recognizes relationship between fracture pattern and mechanism
• Extent of comminution prognostic for time to union
Henley’s Classification
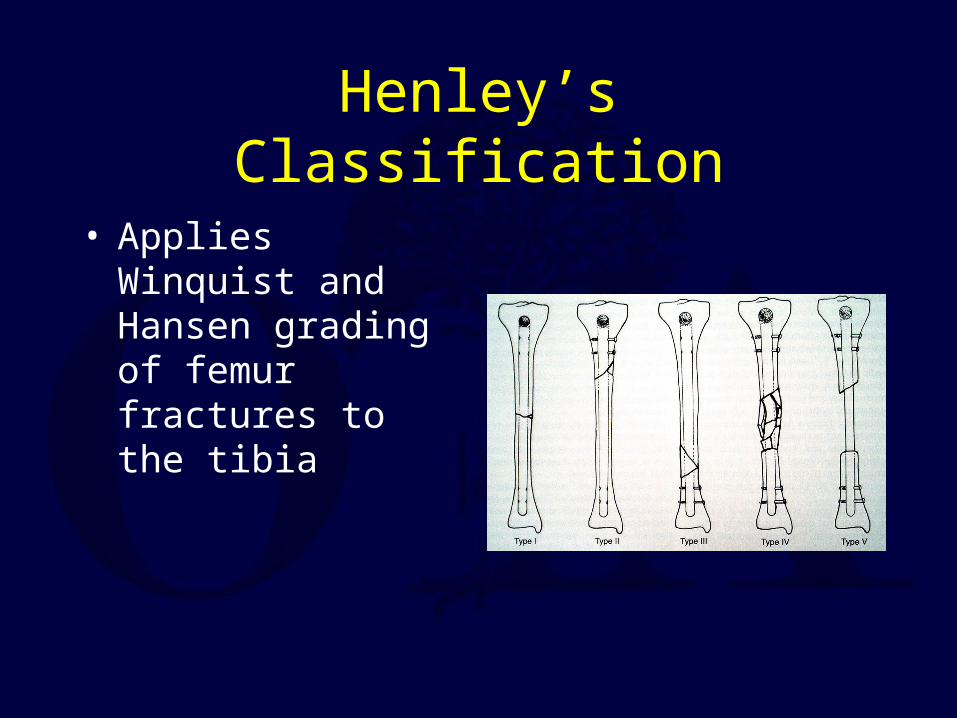
• Applies Winquist and Hansen grading of femur fractures to the tibia
Tscherne Classification of Soft Tissue Injury
• Grade 0- negligible soft tissue injury• Grade 1- superficial abrasion or contusion• Grade 2- deep contusion from direct trauma• Grade 3- Extensive contusion and crush injury
with possible severe muscle injury
Compartment Syndrome
• 5-15%• HISTORY
Hi-EnergyCrush
Nerve is the Tissue most Sensitive to Ischemia
• PAIN first Symptom• PAIN with Passive Stretch first Sign
Each Compartmenthas Specific Innervation
• Ant Comp Deep- - Peroneal• Lateral -Sup Peroneal N.• Deep Post. - Tibial N.• Sup Post. - Sural N.
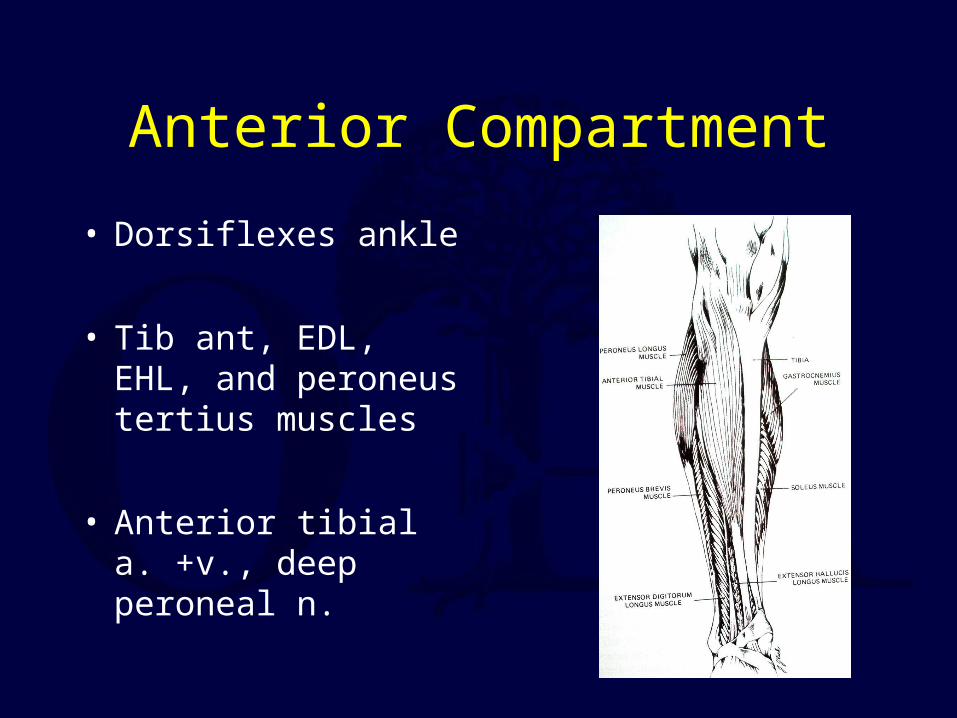
Anterior Compartment
• Dorsiflexes ankle
• Tib ant, EDL, EHL, and peroneus tertius muscles
• Anterior tibial a. +v., deep peroneal n.
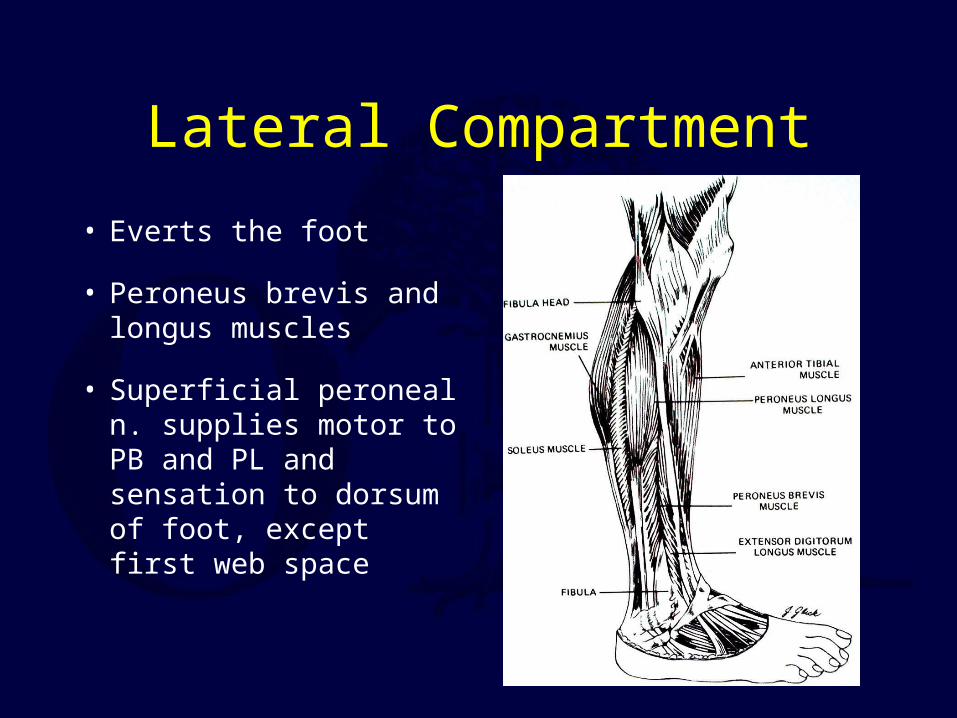
Lateral Compartment
• Everts the foot
• Peroneus brevis and longus muscles
• Superficial peroneal n. supplies motor to PB and PL and sensation to dorsum of foot, except first web space
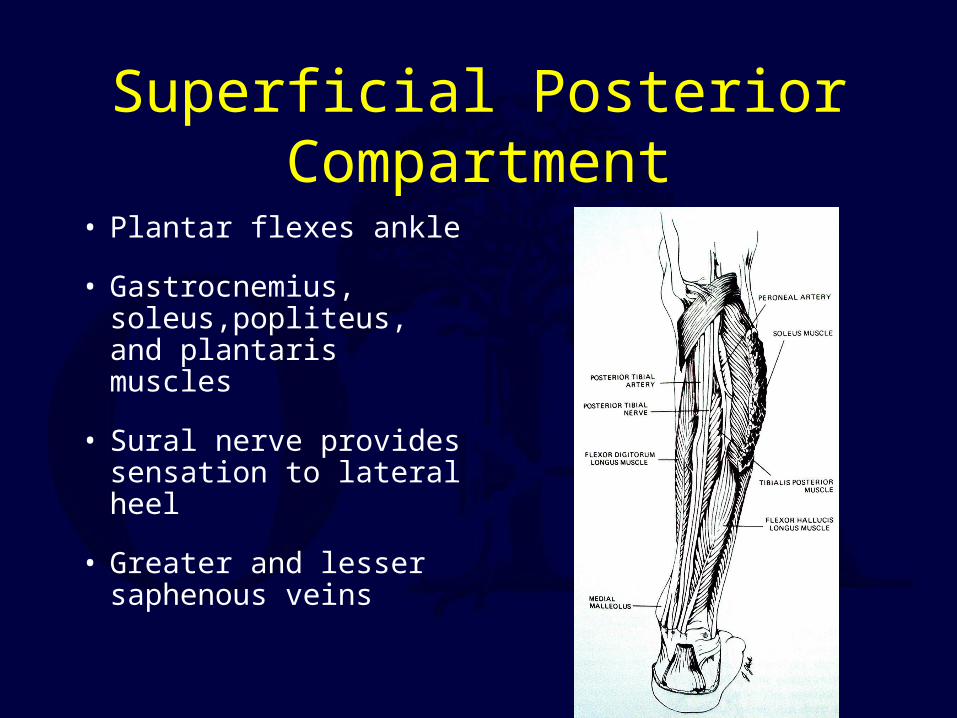
Superficial Posterior Compartment
• Plantar flexes ankle
• Gastrocnemius, soleus,popliteus, and plantaris muscles
• Sural nerve provides sensation to lateral heel
• Greater and lesser saphenous veins
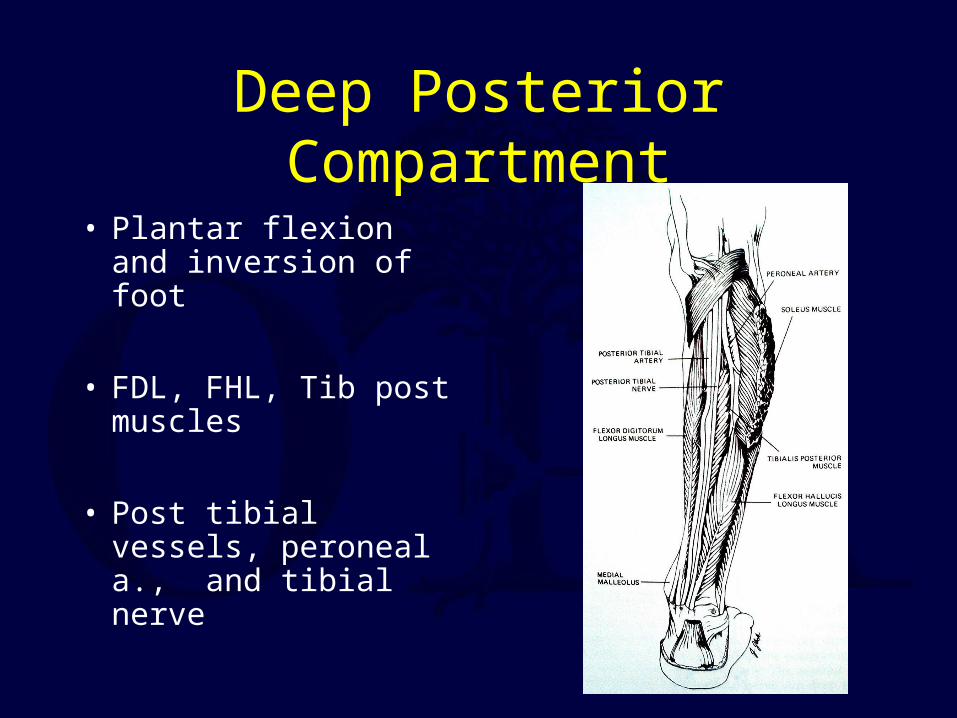
Deep Posterior Compartment
• Plantar flexion and inversion of foot
• FDL, FHL, Tib post muscles
• Post tibial vessels, peroneal a., and tibial nerve
Fundamental Problem
• ? Pressure Of Ischmia• Aerobic - Anaerobic • Clinical Need to Obtain Tissue Pressures
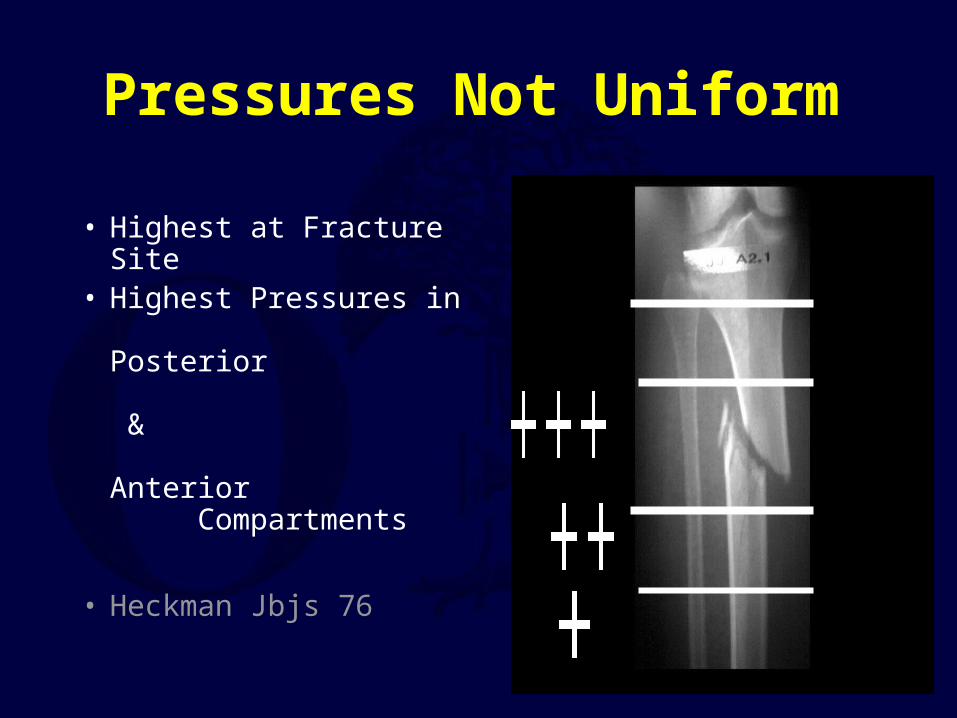
Pressures Not Uniform
• Highest at Fracture Site• Highest Pressures in
Posterior & Anterior Compartments
• Heckman Jbjs 76
Compartment Syndrome is a Clinical Diagnosis
Pressure Measurement are Helpful
• Delta P• Diastolic BP - Compartment Pressure• > 30 is considered ‘Safe’
Clinical Monitoring
• Need Close Observation• Repetitive Exams• Some instances repetitive Pressure
measurements
Compartment Pressures
• Various ThresholdsP = 30P = 45∆ P < 30
∆ P
• Difference between diastolic BP & Compartment Pressure
• When less than 30 + clinical findings perform fasciotomy
Goals of Fasciotomy
• Decompress The Compartment• Fixation• Closure• Do Not Strip Muscle From The Bone
Single vs. two Incisions
• Wide Release• Arterial Injury to the Anterior Tibial Artery
Closed Tibial Shaft Fractures
• Broad Spectrum of Injures No Single Treatment
• Dependent on Mechanism of Injury

Extensive Soft Tissue InjuryDue to Crushing Mechanism of Injury
Natural History
• Studies Indicate that angular deformities tolerated without associated Knee or Ankle Arthrosis

• Kristensen >10-deg F/U: 20-29 yr
• Merchant F/U 29 yrs. No assoc. with ang., site, immob. (37/108)
Nonoperative Treatment
• Casts• Functional Bracing• Nondisplaced & Low Energy Injuries
Sarmiento
• Closed Functional TreatmentAbout 1,000 Tibial Fractures
• 60% Lost to F/u• No Report on Rom
Initial shortening should < 1.4mm.
• Union 98.5%• Time 18.1 Wks.• Short >20mm 1.4%
Angulation
• No clear scientific proof that angulation causes arthrosis of knee or ankle in these 2 studies

Ankle Motion
• 25% patients with 25% loss of ankle-ROM
Surgical Options
• Intramedullary nail
• ORIF with plate
• External Fixation
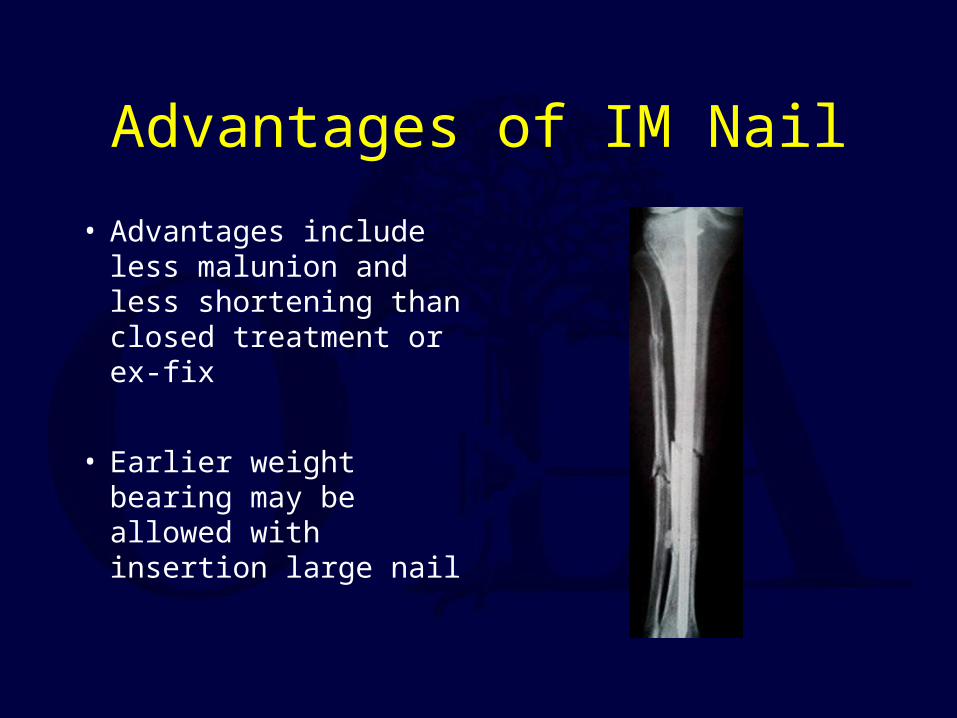
Advantages of IM Nail
• Advantages include less malunion and less shortening than closed treatment or ex-fix
• Earlier weight bearing may be allowed with insertion large nail

Hooper
• In a prospective study found that when displacement >50% and angulation >10 deg.
• Nails superior to cast treatment
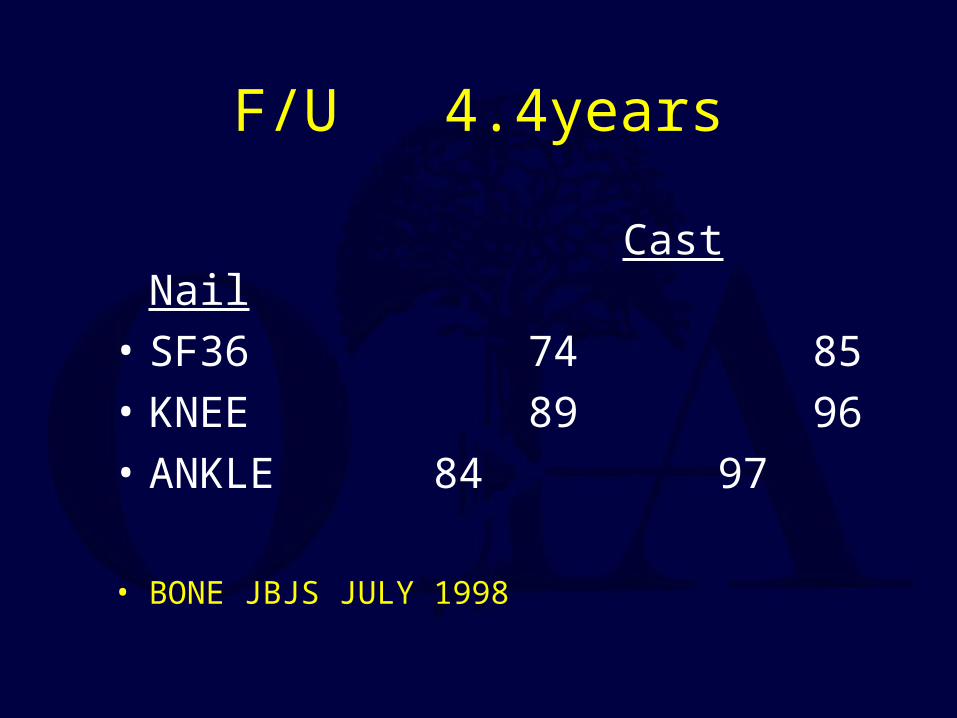
F/U 4.4years
Cast Nail• SF36 74 85• KNEE 89 96• ANKLE 84 97
• BONE JBJS JULY 1998
Reamed vs. Nonreamed IM Nailing
for Displaced Tibial Fractures
Variables
• Reamings (osteogenic)• Larger Nails (bolts)
• Studies Comparing reamed vs. nonreamed also compare nail diameters and stronger constructs

Reamed vs. Nonreamed
Nail Size
0
5
10
15
20
25
30
8 9 10 11 12 13 14
Nail Diameter
No. Used
Reamed
Unreamed

Stability

When To Interlock?
Loss of Alignment without Interlocking Nails
• Spiral 7/22• Transverse 0/27• Metaphyseal 7/28• Templeman CORR 1997
Expanded Indications
• Proximal 1/3• Distal 1/3• Increased Problems
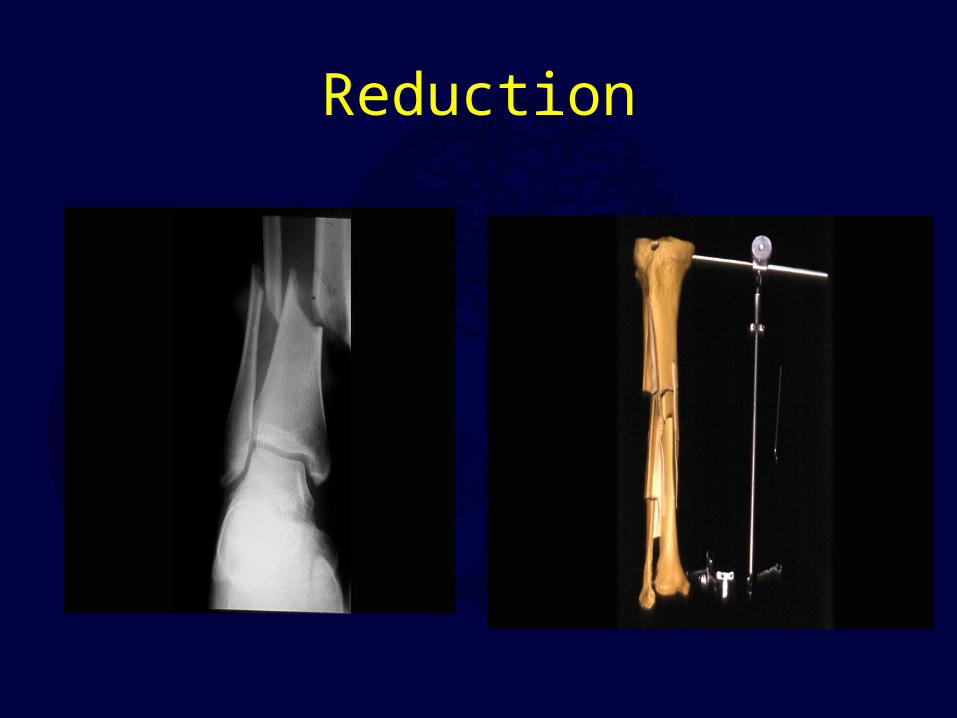
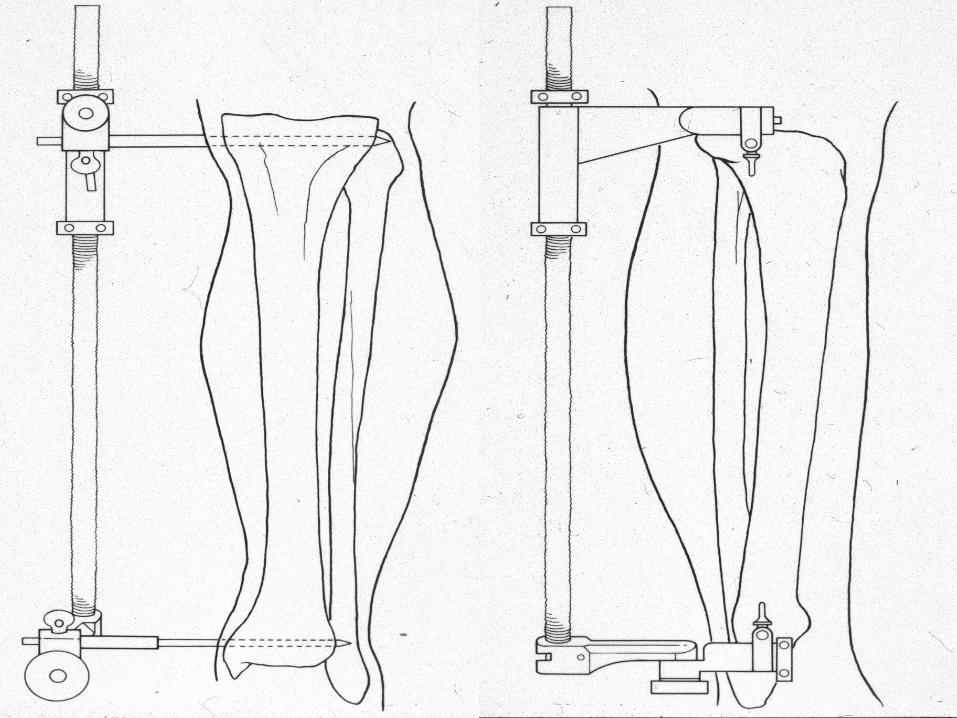
Reduction

• Proximal Fractrues are technically more challenging
• Prone to Valgus & • Pro-curvatum deformities


Technique
• Screws placed on concave side of deformity.
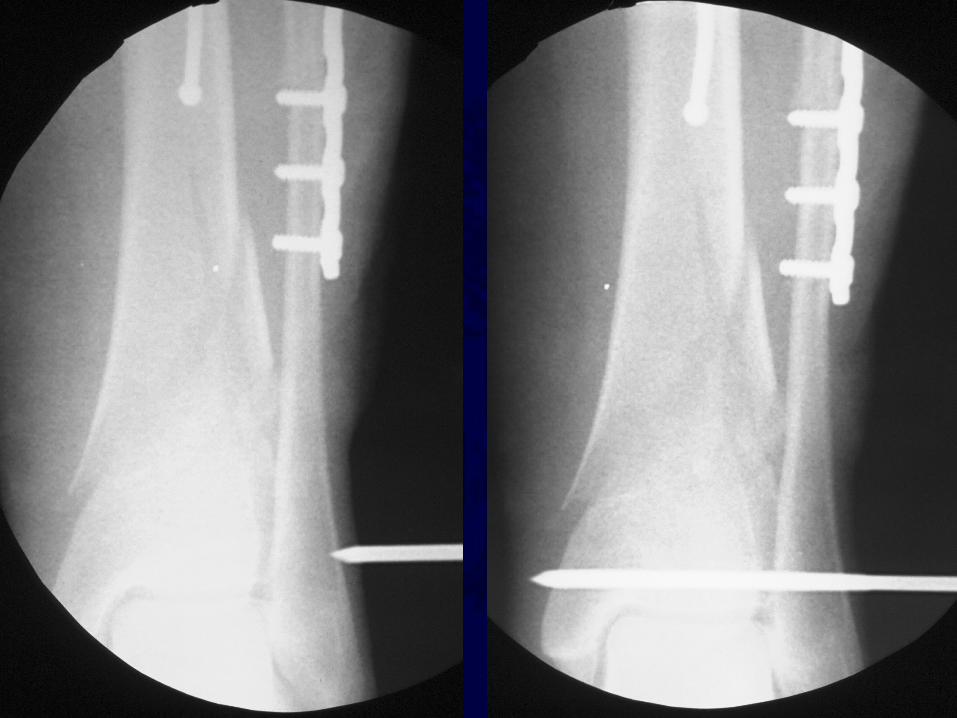
Blocking (Poller) Screws
• Functionally narrow im canal• Increase strength and rigidity of fixation
The Use of Poller Screws as Blocking Screws in Stabilising Tibial Fractures
Treated with Small Diameter Nails
• 21 patients• All healed within 3-12 months• Mean alignment 1 degree valgus, antecurvatum 2
degrees.
Krettek C, et al. JBJS 81B: 963, 1999

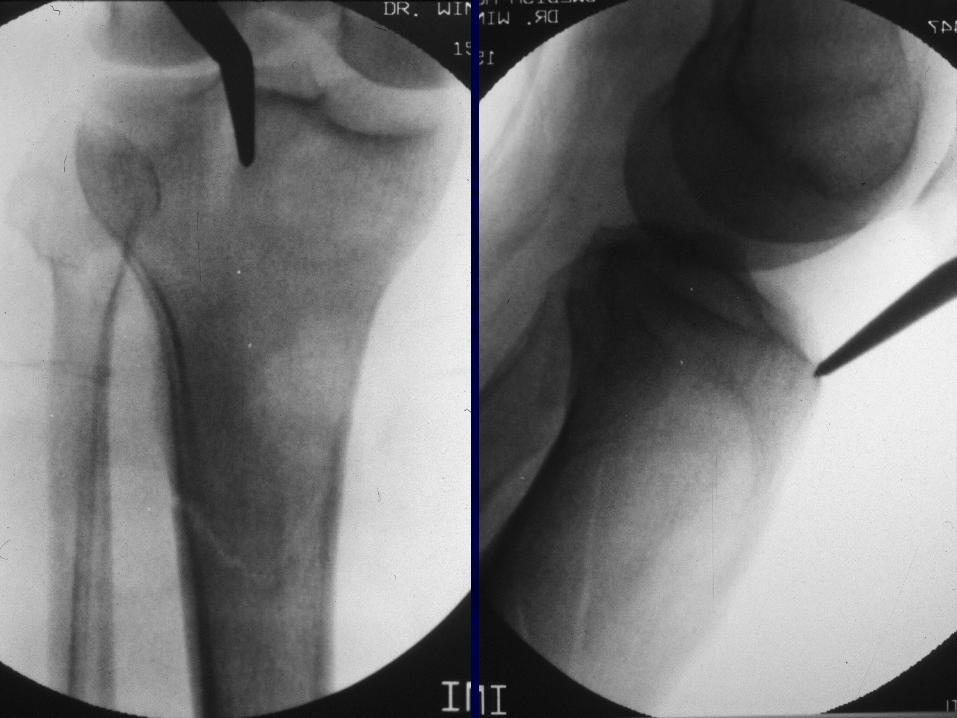
• Entry Site for Proximal fractures Critical
• Reference is Lateral Tibial Spine
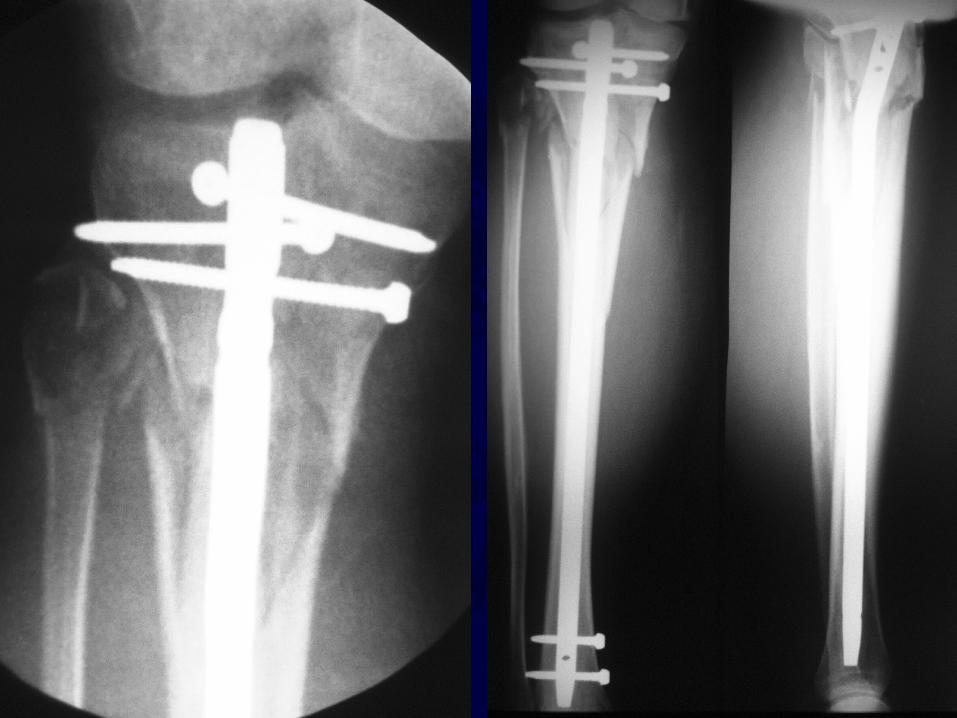

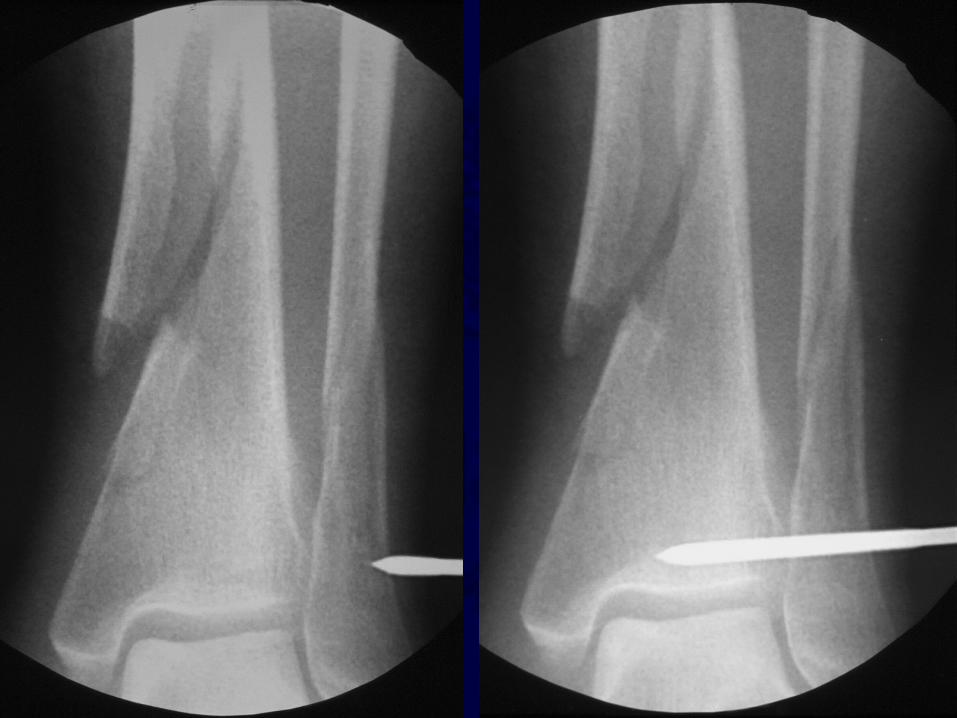
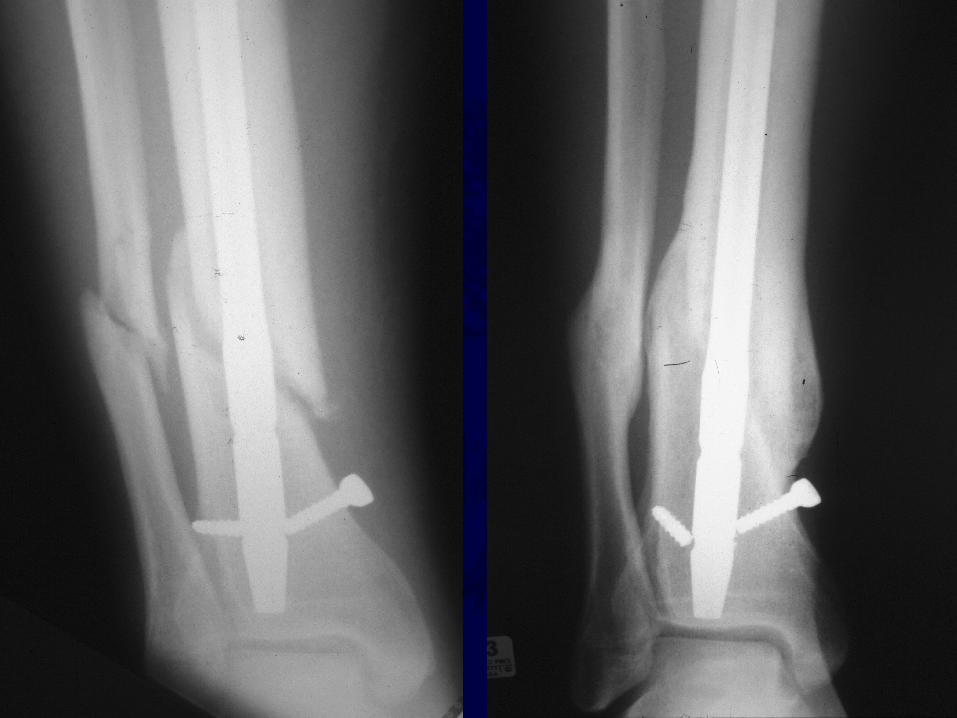
NailingDistalTibia
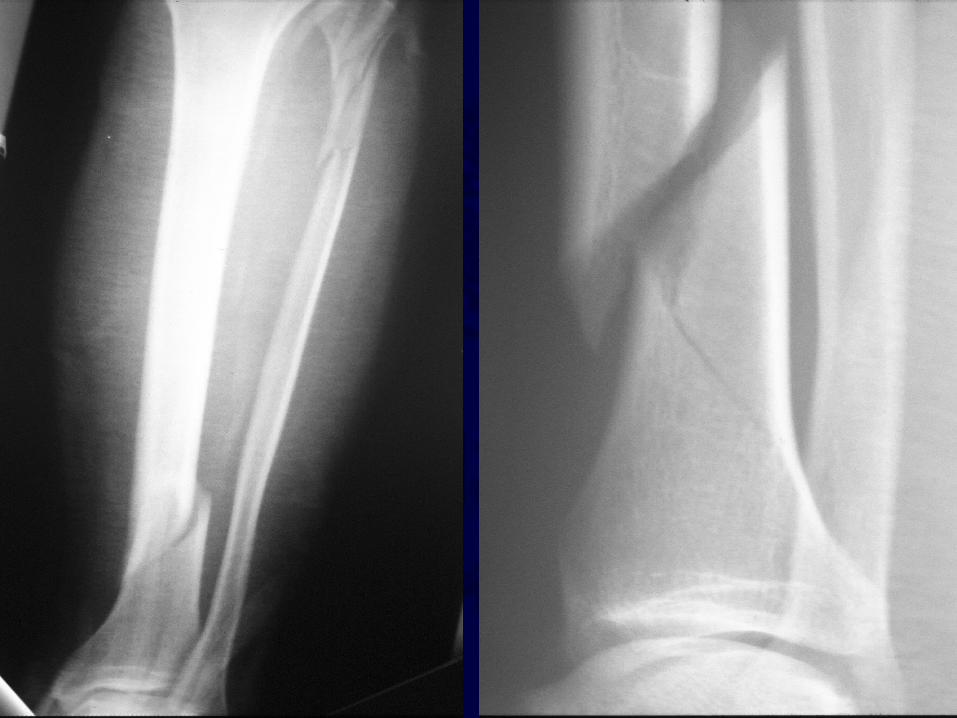
Reduction of Distal Tibial Fractures
• Distractor• Joy Stick• Fibular Plating• Calcaneal Traction




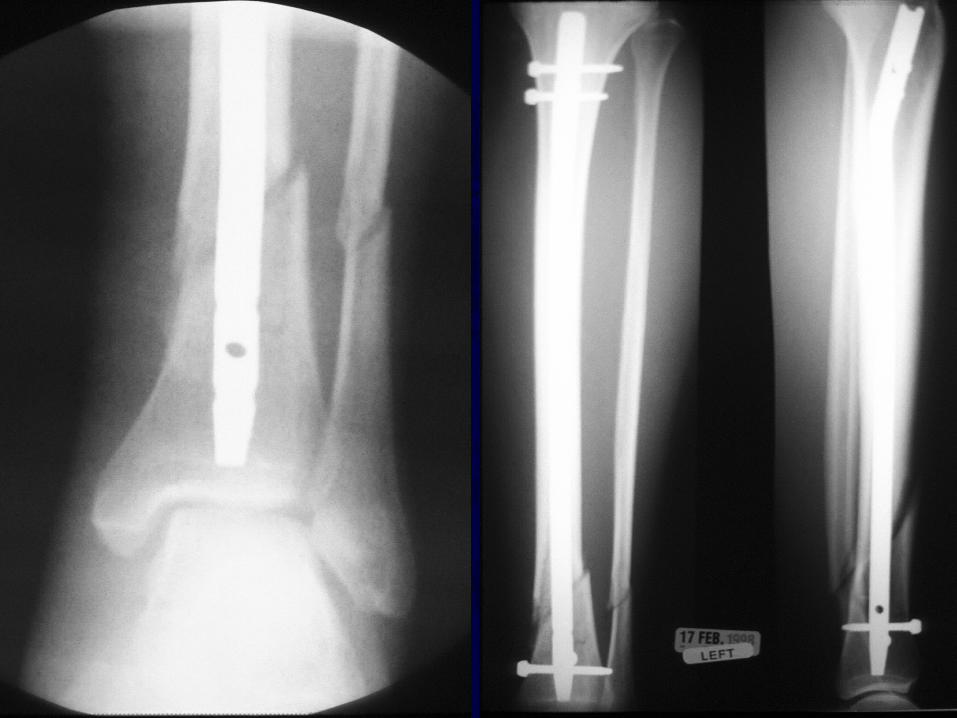
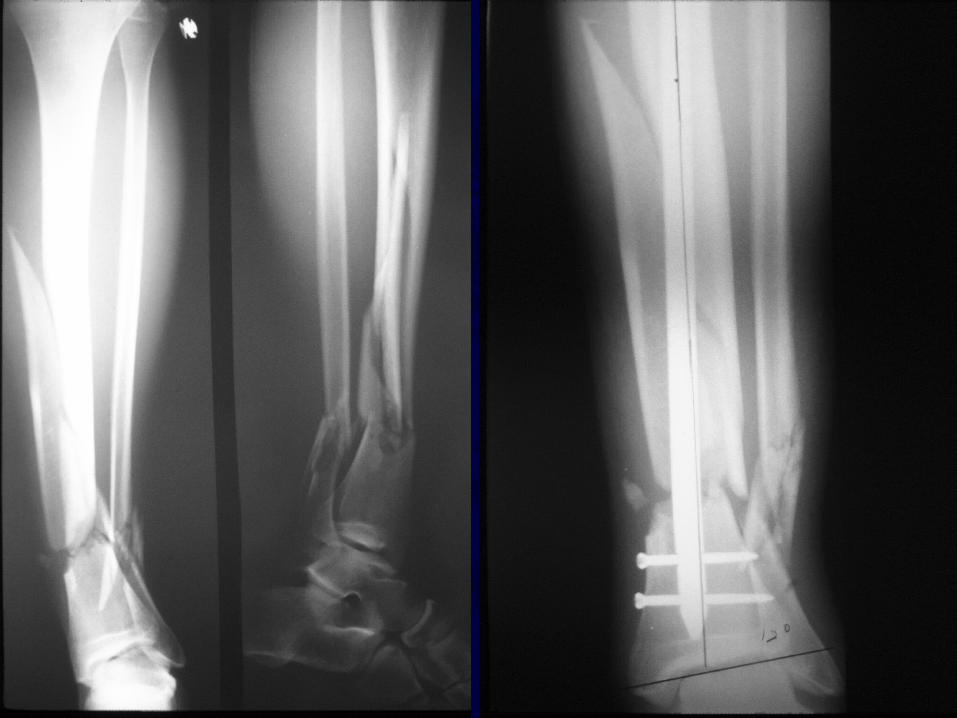

Pin//
Ankle

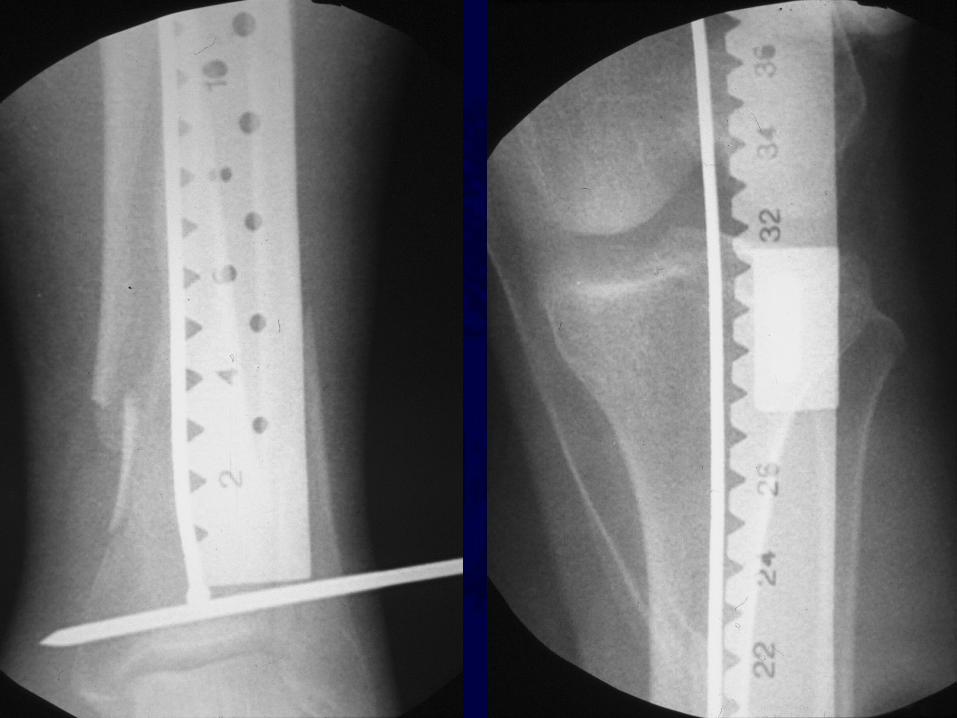


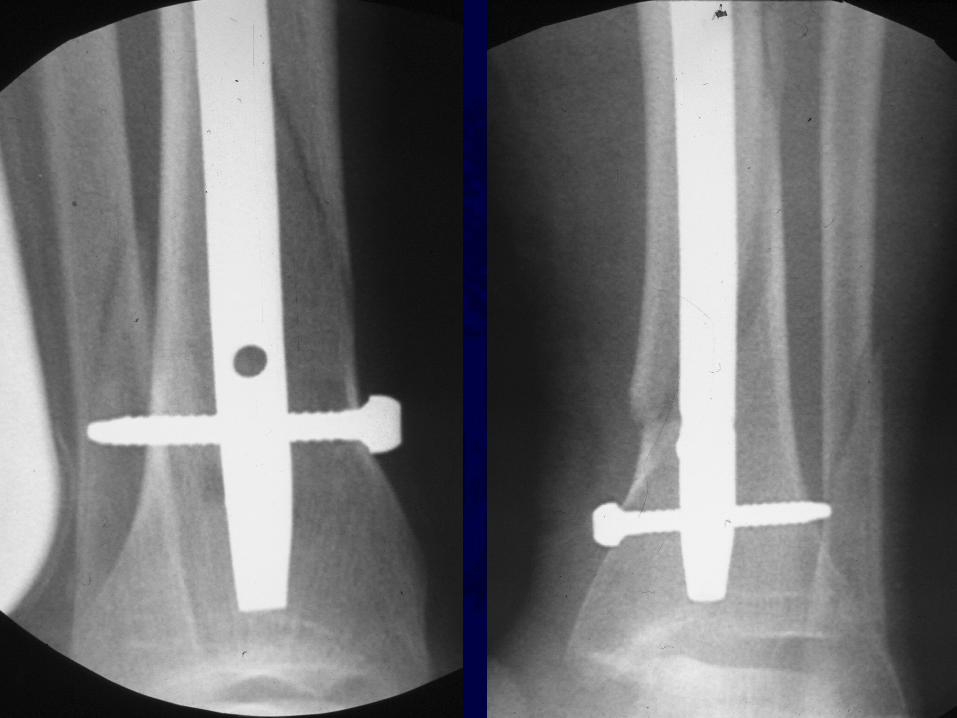
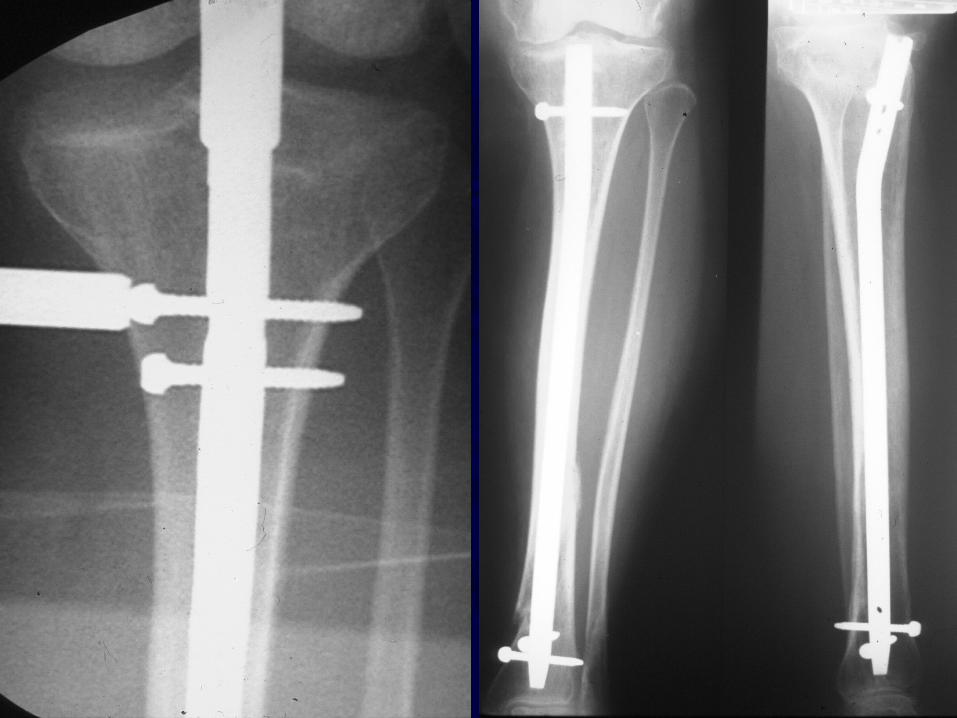

PlateFibula
+ Alignment- Dynamization



Proximal and Distal Cases Courtesy of
R. Winquist M.D.Seattle, Wa.

Results
Reamed and Nonreamed techniques are comparable; more bolt breakage with
smaller nonreamed implants

Blachut JBJS 79A
+R -R 73 63N/U 4% 11%Mal. 4% 3%Screws 3% 16%
Complications
• Infection 1-5%• Union >90%• Knee Pain
Common
Anterior Knee Pain
• Severe 9%• Moderate 22%• Mild 68%

Knee Pain
• Severe 9%• Moderate 22%• Mild 68%
• Kneeling 92%• Running 57%• Rest 37%
Nail Removal
• Resolved 27%• Marked improv 69%
• Complete 44%• Partial 34%• No - 20%

Iaquinto 1998
Epidural 4.1 X
Neurological Complications

Disadvantages of IM Nail
• Disadvantages include anterior knee pain (up to 56.2% *), risk of infection, increased hardware failure with unreamed nails
*Court-Brown et al. JOT 97
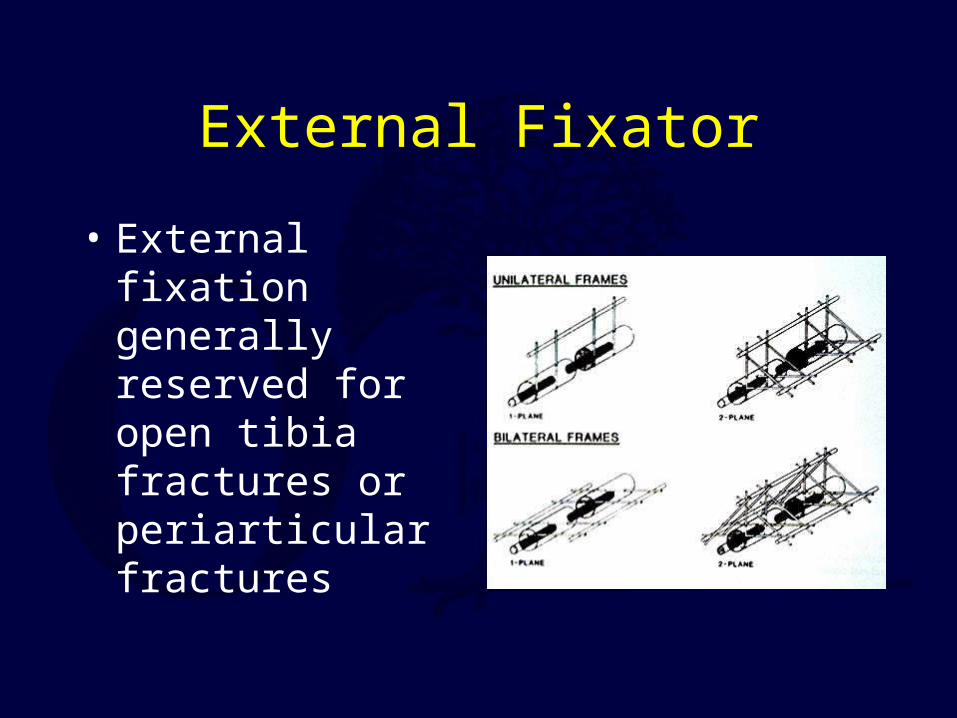
External Fixator
• External fixation generally reserved for open tibia fractures or periarticular fractures
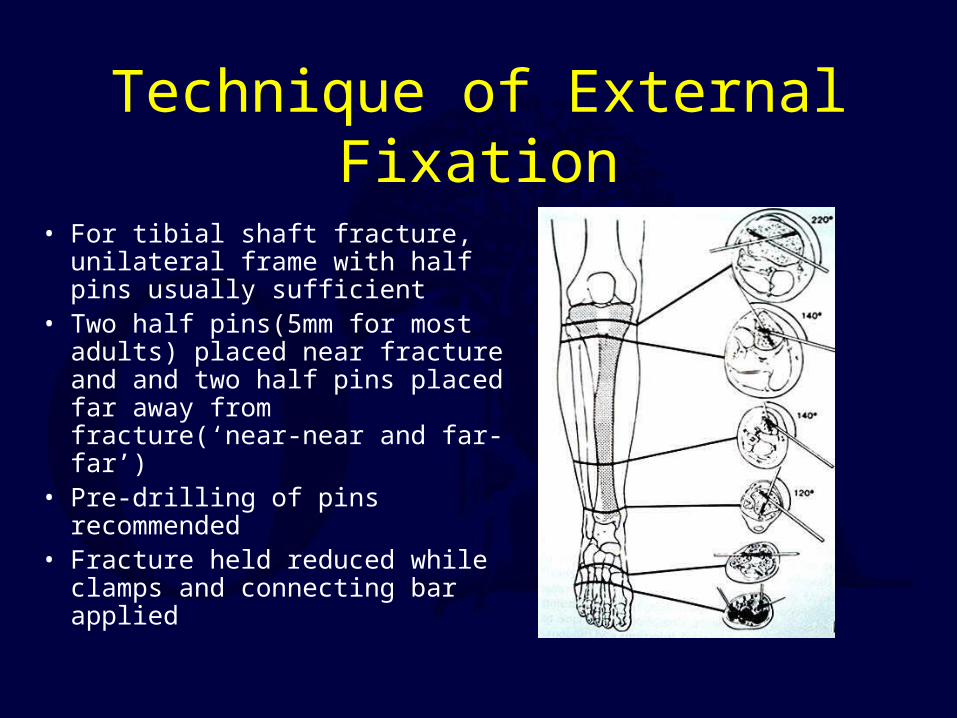
Technique of External Fixation
• For tibial shaft fracture, unilateral frame with half pins usually sufficient
• Two half pins(5mm for most adults) placed near fracture and and two half pins placed far away from fracture(‘near-near and far-far’)
• Pre-drilling of pins recommended• Fracture held reduced while clamps
and connecting bar applied
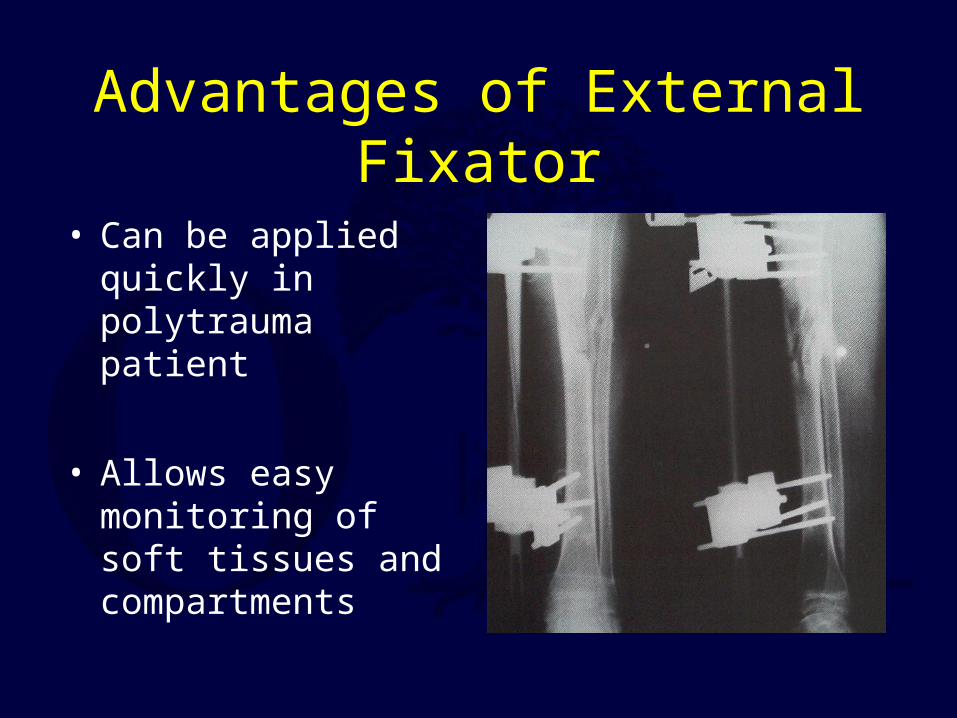
Advantages of External Fixator
• Can be applied quickly in polytrauma patient
• Allows easy monitoring of soft tissues and compartments
Disadvantages of External Fixator
• Increased incidence of malunion compared to IM nail
• Risk of pin tract infection, cellulitis
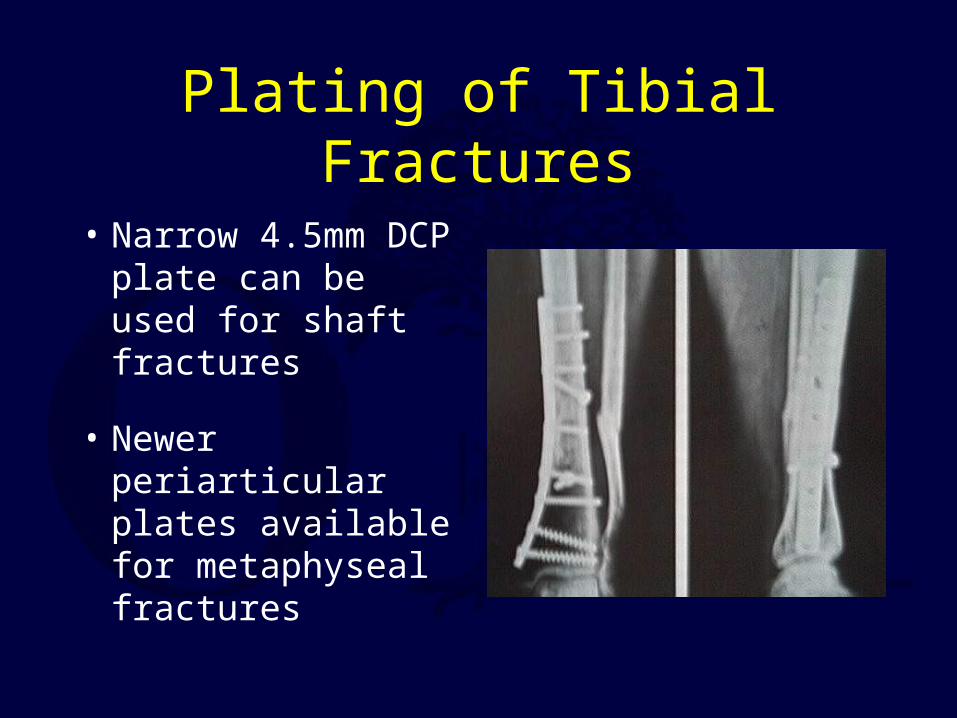
Plating of Tibial Fractures
• Narrow 4.5mm DCP plate can be used for shaft fractures
• Newer periarticular plates available for metaphyseal fractures

Technique of Tibial Plating• Anterior longitudinal incision allows placement of plate on
medial border of tibia• 4.5mm LCDCP plate secured to bone on distal fragment• Butterfly fragment can be secured with interfragmentary
screw• The AO articulating tension device can be secured to
proximal part of plate to aid reduction• With fracture reduced, screws placed through plate on
either side of fracture
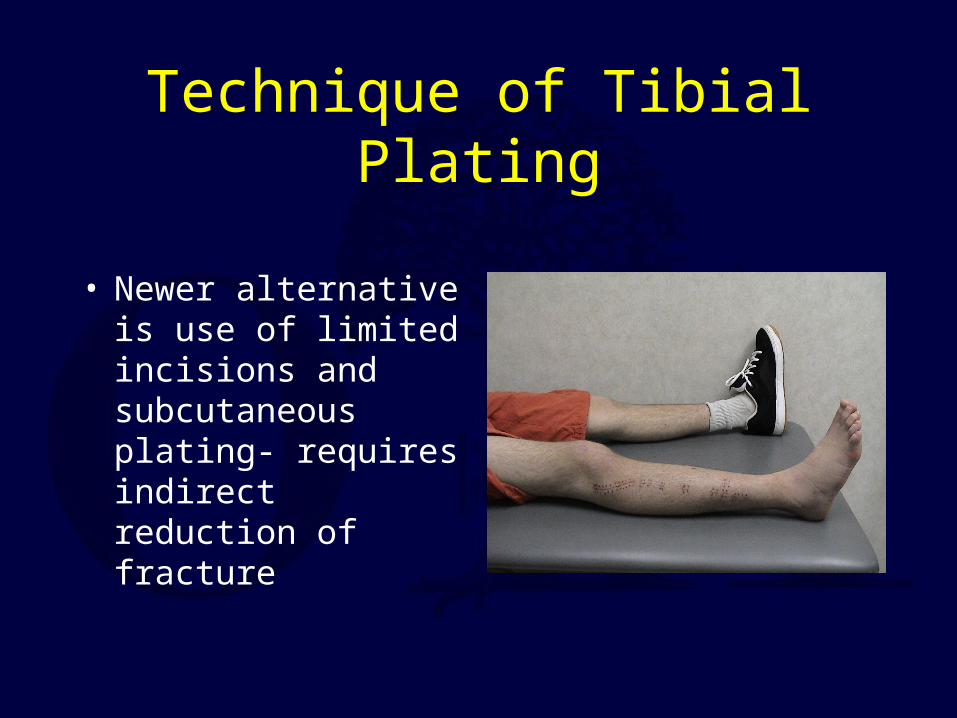
Technique of Tibial Plating
• Newer alternative is use of limited incisions and subcutaneous plating- requires indirect reduction of fracture

Advantages of Plating
Anatomic reduction usually obtained
In low energy fractures 97% very good/good results have been reported*
*Ruedi et al. Injury vol 7
Disadvantages of Plating
• Increased risk of infection and soft tissue problems, especially in high energy fractures
• Higher rate hardware failure than IM nail
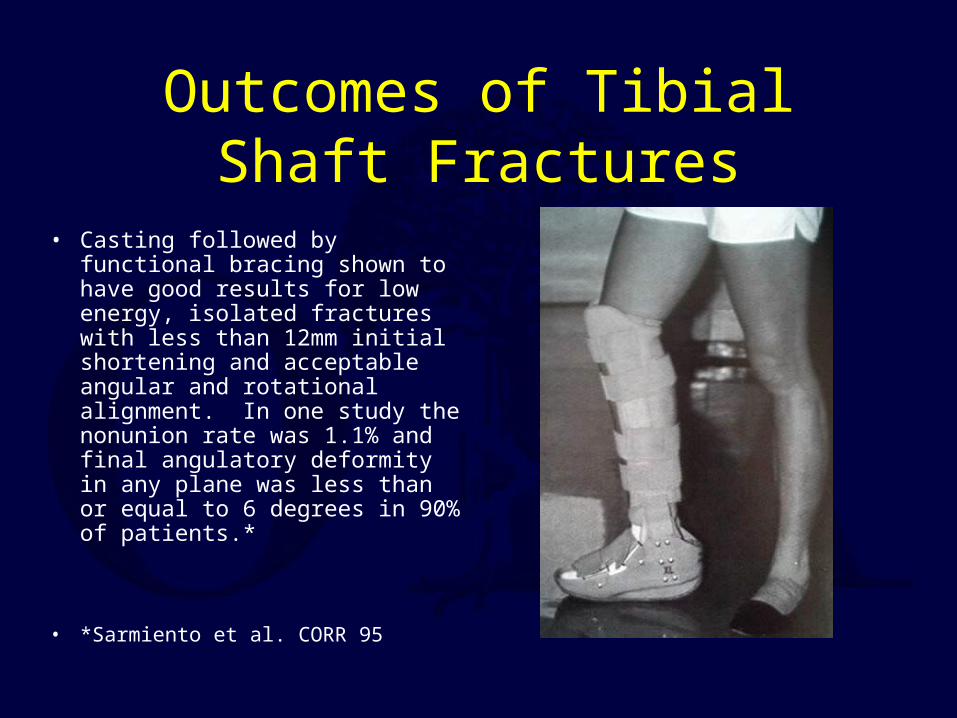
Outcomes of Tibial Shaft Fractures
• Casting followed by functional bracing shown to have good results for low energy, isolated fractures with less than 12mm initial shortening and acceptable angular and rotational alignment. In one study the nonunion rate was 1.1% and final angulatory deformity in any plane was less than or equal to 6 degrees in 90% of patients.*
• *Sarmiento et al. CORR 95

Outcomes of Plate Fixation• For low energy tibial fractures 97% ‘very good/good’
results have been reported, although most studies not this favorable*
• Complications such as hardware failure and infection have been as high as 48% after plating comminuted fractures**
*Ruedi et al. Injury,7,252-257**Johner and Wruhs, Clin Orthop 1983
Outcomes of External Fixation
• 95% union rate has been reported for group of closed and open tibia fractures, but 20% malunion rate*
• Most common complications are pin track infections and malunion**
• Loss of reduction associated with removing frame prior to union
*Anderson et al. Clin Orthop 1974**Edge and Denham JBJS[Br] 1981
Outcomes of IM Nailing
• In a study of 200 closed, low-energy tibia fractures treated with cast versus IM nail, the results for nailing were: union rate=98%, malunion rate=0, infection=3.3%. The results of casting were: union rate=90%, malunion rate=4.3%, and infection=1.4%*
* Puno et al. Clin Orthop 1986
Outcomes of IM Nailing
• Another large group of tibia fractures treated with reamed IM nail had 98% union rate and 3% infection rate*
• Most common complication after IM nailing remains anterior knee pain **
*Williams et al. JOT 1995** Court-Brown et al. JBJS 1990
Return to Lower Extremity
Index


























](https://img.dokumen.tips/doc/110x75/577cdc6e1a28ab9e78aa86df/l10-closed-tibia-fracture1.jpg)

