Embed Size (px)
Citation preview
HUMAN PAPILLOMA-
VIRUS VACCINE (DO WE
NEED IT IN EGYPT)
Moustapha Ramadan
2010
Epidemiology of cancer cervix
WorldWide
2nd most frequent cancer among women
490 000 women diagnosed annually with invasive cervical
cancer
3rd leading cause of death among cancer ( after cancer
breast and cancer lung) with 270 000 annually death
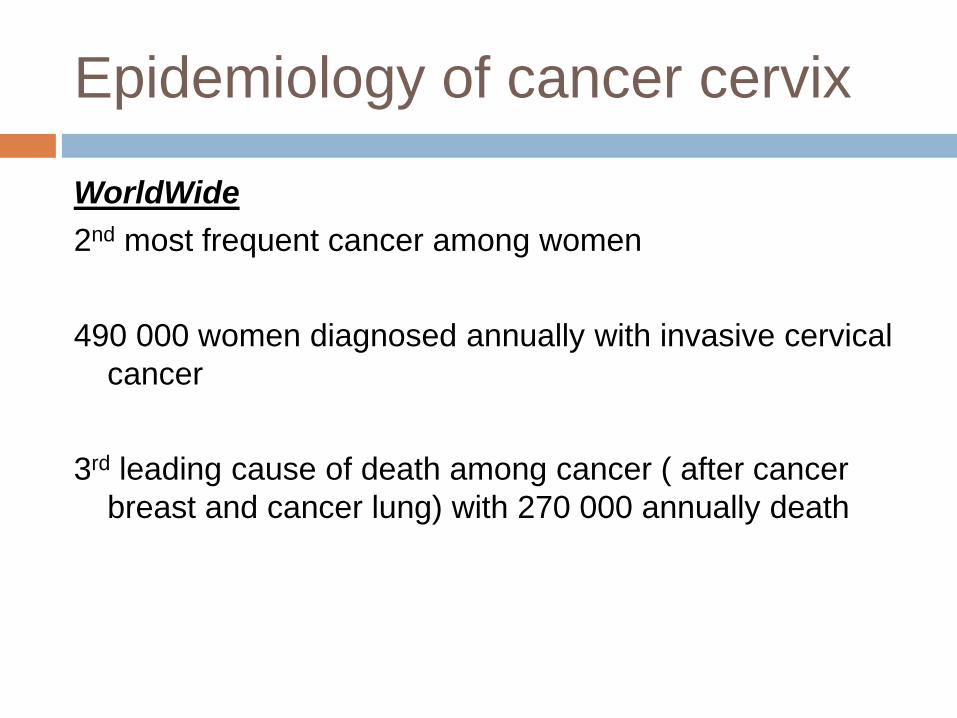
Worldwide incidence of cervical
cancer per 100000 females (2005)
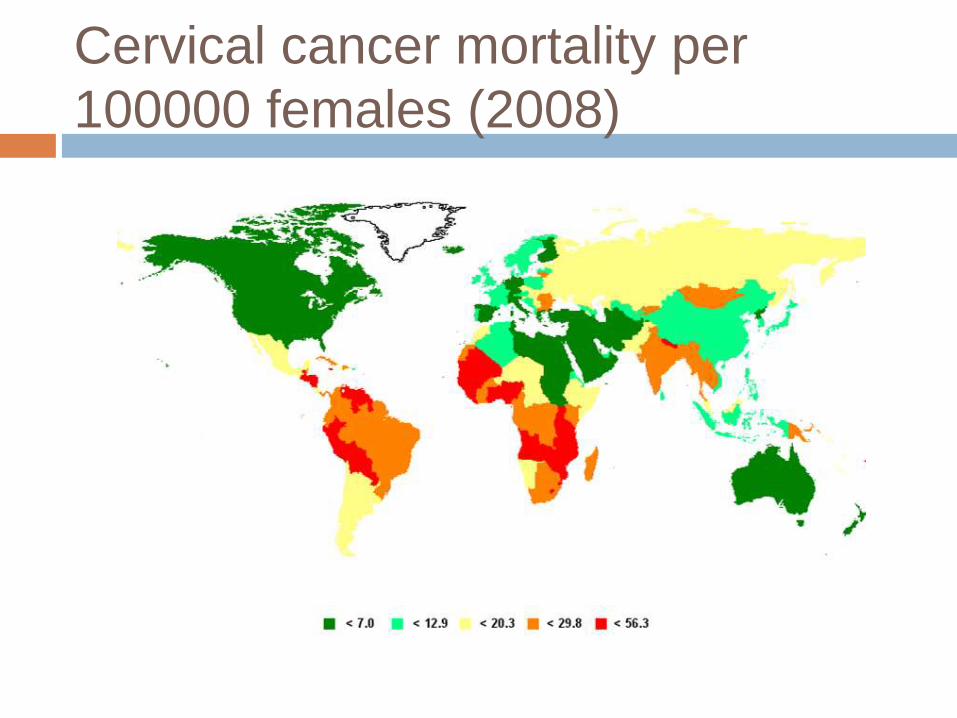
Cervical cancer mortality per
100000 females (2008)
Human papilloma-virus
characteristics
1. Double stranded, enveloped DNA virus
2. Over 100 characterized serotypes
3. Grouped into three categories
4. At least 40 serotypes infect human mucosa
5. At least 14 serotypes are considered high risk‟ for
malignancy
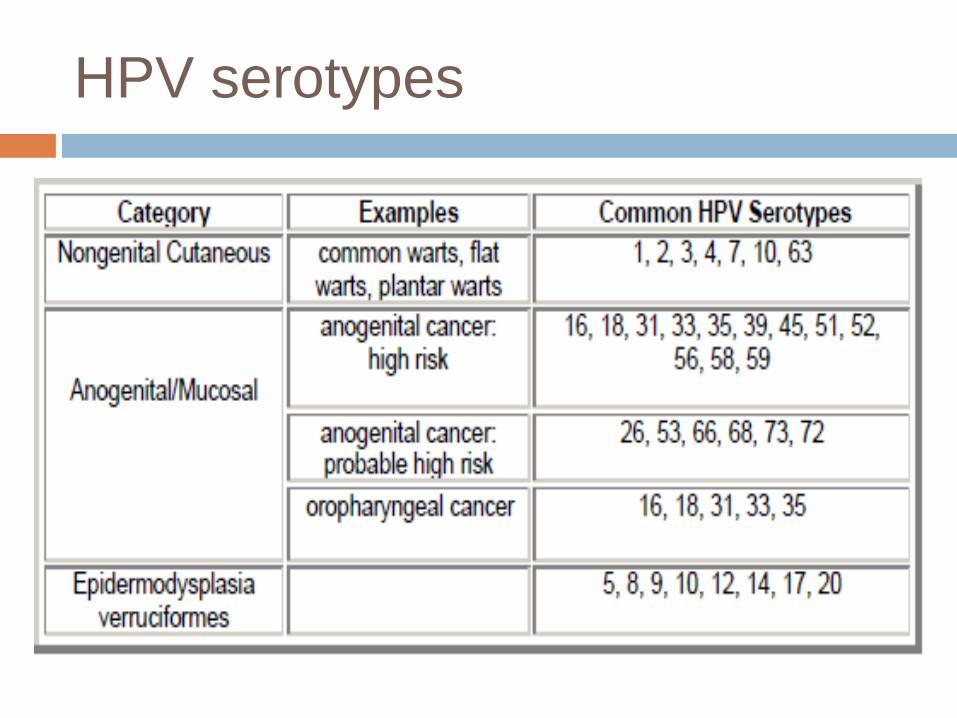
HPV serotypes
Epidemiology of HPV
1.Most common sexually transmitted disease in the United
States
2. Estimated 6.2 million people infected annually
3. 80% of women are infected during their lifetime
4. More than 50% of women are infected within first three
years of sexual debut
5. In women HPV has a bimodal distribution
a. Peaks in early 20s (20 to 24)
b. Progressively declines
c. Increases sharply in late 40s and early 50s (45 to 55)
6. HPV is responsible of about 70% of cervical cancer
worldwide
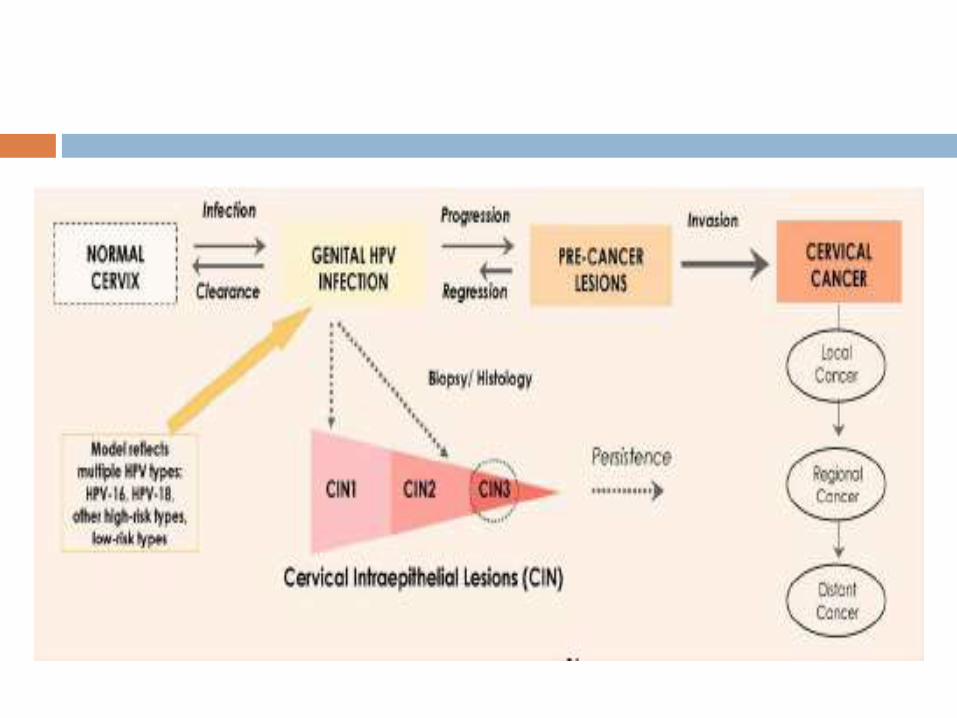
Pathophysilogy
HPV enters epithelial tissues through microabrasions in host mucosa
Viral reproduction in bloodless epithelial cells allows HPV to efficiently evade the host immune system
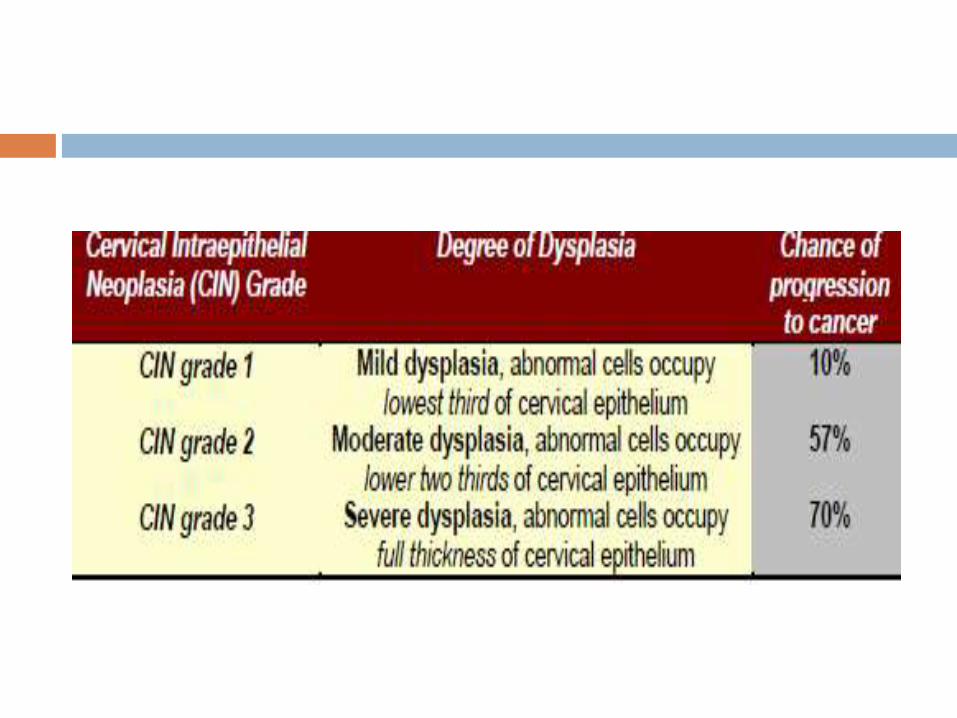
Cervical intraepithelial neoplasia (CIN) is cell dysplasia caused by HPV infection
CIN is categorized by level of severity; CIN 2 and 3 are widely accepted surrogate markers for cancer

HPV vaccine
Administration
3 doses (Now,1,6) intramuscularly (IM)
Contraindicated in anyone with a history of an immediate
hypersensitivity to yeast
Can be administered at same visit as other vaccines
Quadrivalent Vaccine (Gardasil) contains HPV serotypes 6,
11, 16, 18
Bivalent Vaccine (Cervarix) contains HPV serotypes 16 and
18
Vaccination in females 9 to 26 years of age (before first
intercourse)
Adverse effects:
94% non-serious: dizziness, syncope, nausea, rash pain,
erythema, swelling at injection site, headache, fatigue,
myalgia.
6% serious: Guillain-Barre, venous thromboembolism,
death. Do no appear to be causally linked to
vaccine.
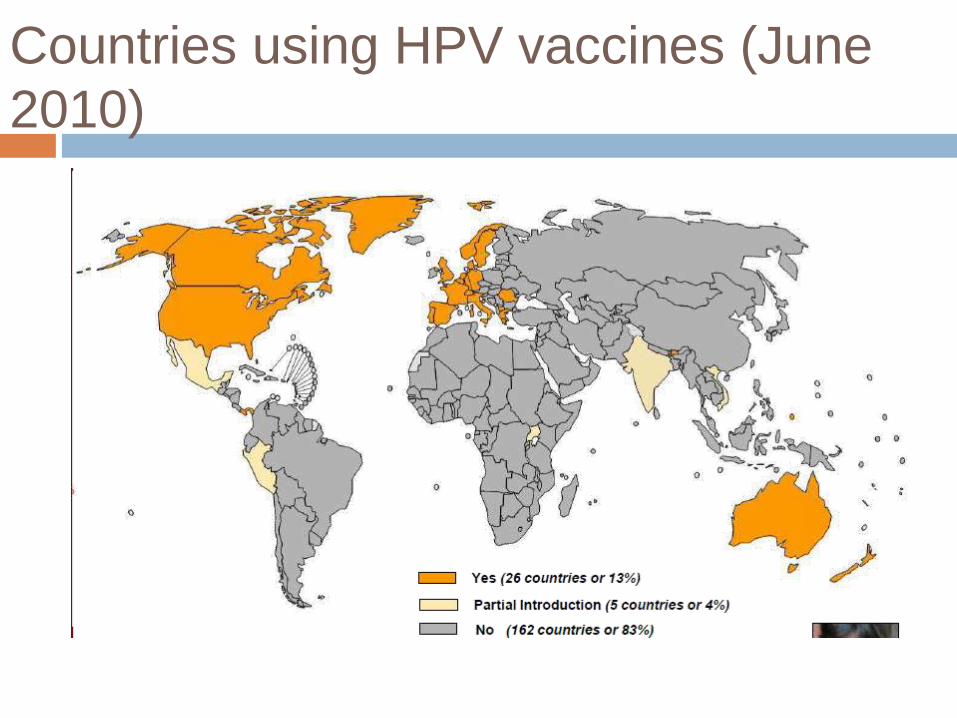
Countries using HPV vaccines (June
2010)
STUDIES
Paavonen J, Naud P, Salmeron J, et al. Efficacy of
human papillomavirus (HPV)-16/18 ASO4 –adjuvanted
vaccine against cervical infection and precancer caused
by oncogenic HPV types (PATRICIA): final analysis of a
double-blind, randomized study in young women. Lancet,
2009. 25;374(9686):301-14

Methodolgy
Multi-center, randomized, double-blind, placebo-controlled trial
18,644 women aged 15 to 25 years (92% had the full dose
schedule)
Between May2004, and June 2005, at 135 centres in 14
countries in Asia Pacific, Europe, Latin America, and North
America
Inclusion criteria: not pregnant at time of enrollment, < 6 lifetime
sexual partners, no previous colposcopy, no autoimmune
disease or immunodeficiency
Subjects received HPV 16/18 vaccine at 0, 1, and 6 months and were asked to use effective birth control during vaccination period
Cervical biopsy samples taken every 6 months for HPV DNA typing of 14 oncogenic HPV strains
Blood samples gathered at months 0, 7, and 24 for HPV 16/18 antibodies

Two study cohorts:
Total vaccinated- naive cohort (TVC-N): women receiving all doses of vaccine who had no virologic evidence of infection with HPV 16/18 through 1 month after third dose of vaccine (represent girls before sexual debut)
Total vaccinated cohort (TVC): all women including those who had evidence of HPV 16 or 18 infection (represent the general population of young women)

Follow-up visits every 12 months for Papanicolaou smear
(and colposcopy if necessary) based on a standardized
treatment algorithm
CIN grade 2 or 3, adenocarcinoma in situ, or invasive
cancer associated with HPV 16/18
CIN associated with other oncogenic HPV types
Results
Mean follow-up time was 34.9 months after third dose
Seroconversion at 36 months: HPV-16 100%, HPV-18 100%
Vaccine efficacy in preventing CIN 2+ lesions caused by HPV 16/18:
TVC-naïve cohort: 98.1% (CI, 88.4 to 100%)
TVC cohort: 30%: (CI, 21.5 to 38%)
Significant cross-protection against HPV 31, 33, 45, 52 and 58
Vaccine efficacy in preventing CIN 2+ lesions caused by any HPV type TVC-N: 68.2% (CI, 54 to 80.9%)
Conclusion
Bivalent HPV vaccine significantly lowers incidence of
high-grade CIN related to HPV 16/18 in women without
previous HPV 16/18 infection
Vaccine does not appear to alter the course of HPV 16/18
infection or lesions already present
Vaccine provides cross protection against HPV 31, 33, 45,
52, 58
Helen Saxenian, International AIDS vaccine initiative,
PATH. HPV vaccine adoption in developing countries:
Cost and Financing issues. December 2007
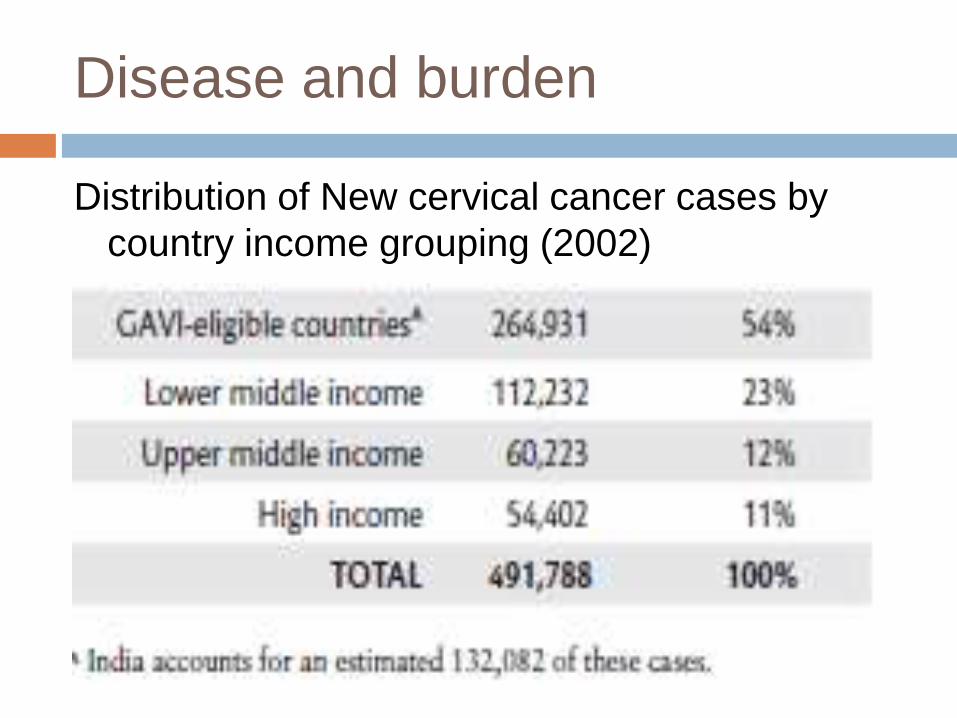
Disease and burden
Distribution of New cervical cancer cases by
country income grouping (2002)
About 6.6 million 11-year-old girls are in
industrialized countries in 2010 and about 52
million girls in developing countries.
The cost of quadrivalent vaccine is 120 USD/
dose.
Additional cost should be considered, wastage,
cold chain etc…
Developing Countries found that the population-
weighted mean cost per fully immunized child in
27 developing countries was about 17 USD,
with a range from 3 USD to 31 USD
Costs varied considerably by region, given
variation in labor costs and in delivery strategies
Cost-effectiveness models have been used to
compare the net cost of HPV vaccination with
the potential benefits, expressed as years of life
saved (YLS) or quality-adjusted life years
(QALYs)
At a cost of ID 50, the cost-effectiveness ratio
was about ID 300 per YLS with a reduction of
about 43% in the lifetime risk of cancer
Combined vaccination and screening at costs of
ID 75, 100, and 450 per vaccinated girl resulted
in cost-effectiveness ratios of about ID 1,100,
1,700, and 9,600 per YLS compared to
screening alone.
GDP per capita, estimated in current
international dollars, was 9,500 for that year
SITUATION IN EGYPT
Egypt has a population of 25.76 millions women
ages 15 years and older who are at risk of
developing cervical cancer.
Current estimates indicate that every year 514
women are diagnosed with cervical cancer and
299 die from the disease.
Cervical cancer ranks as the 14th most frequent
cancer among women in Egypt, and the 12th
most frequent cancer among women between
15 and 44 years of age.
About 10.3% of women in the general population
are estimated to harbor cervical HPV infection at
a given time.
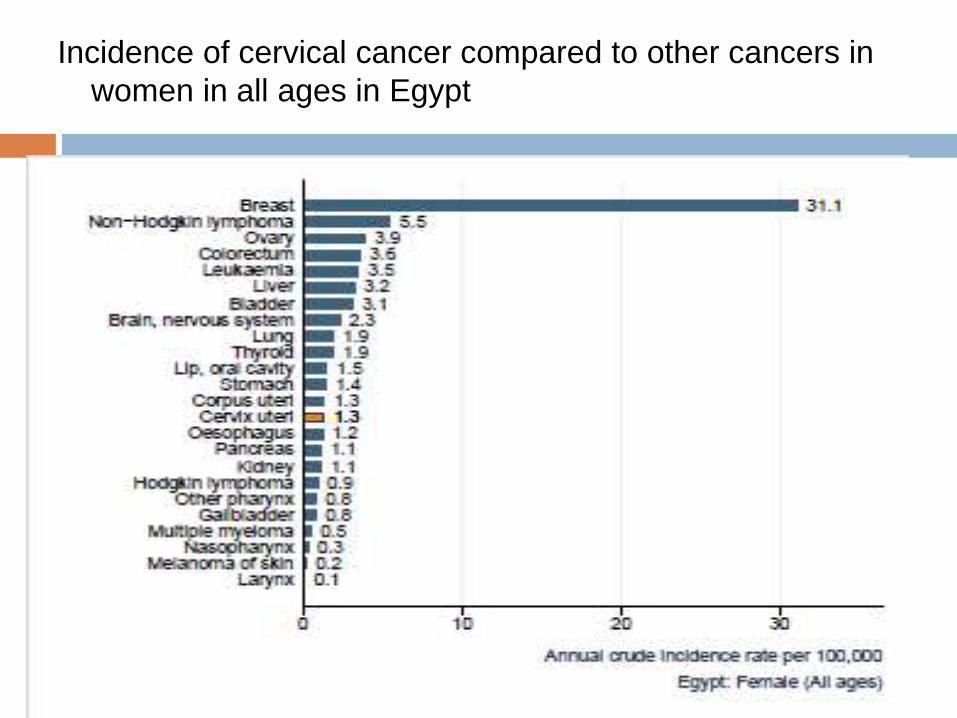
Incidence of cervical cancer compared to other cancers in
women in all ages in Egypt
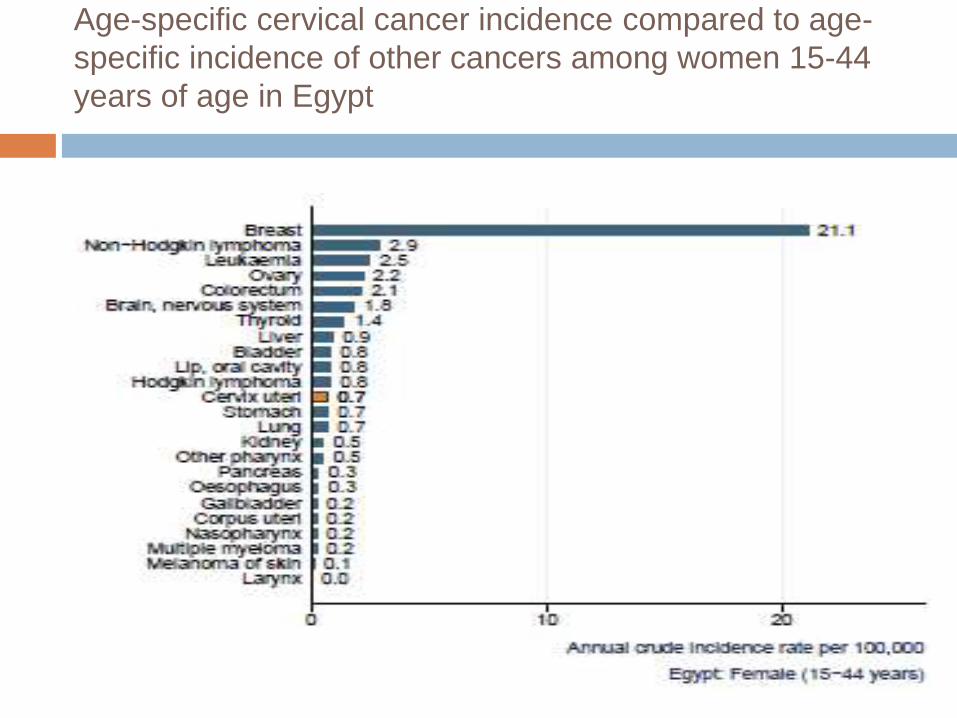
Age-specific cervical cancer incidence compared to age-
specific incidence of other cancers among women 15-44
years of age in Egypt
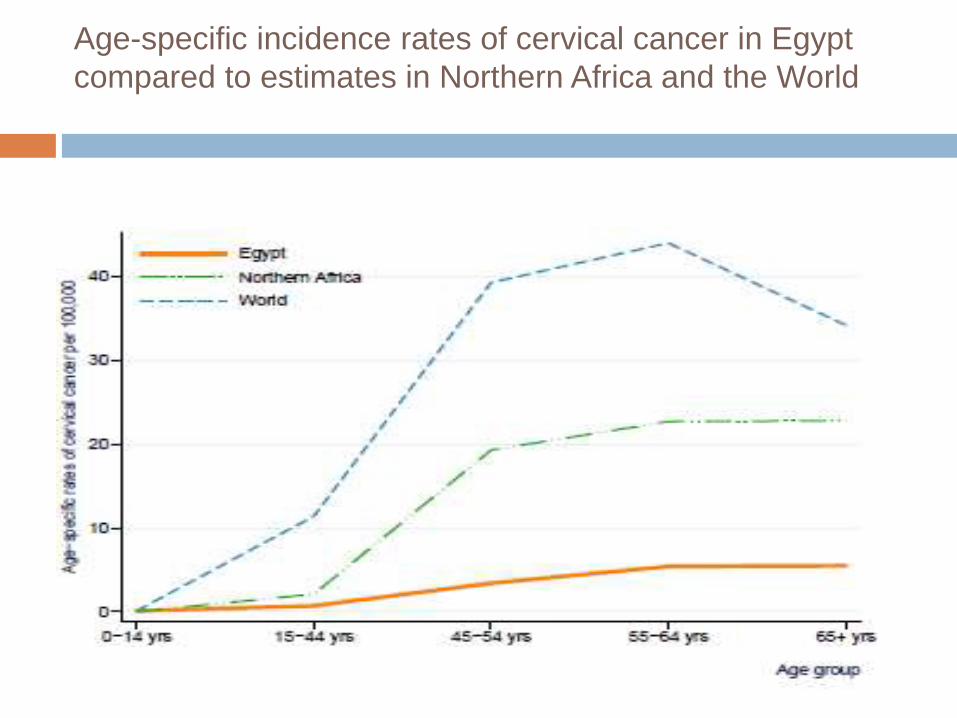
Age-specific incidence rates of cervical cancer in Egypt
compared to estimates in Northern Africa and the World
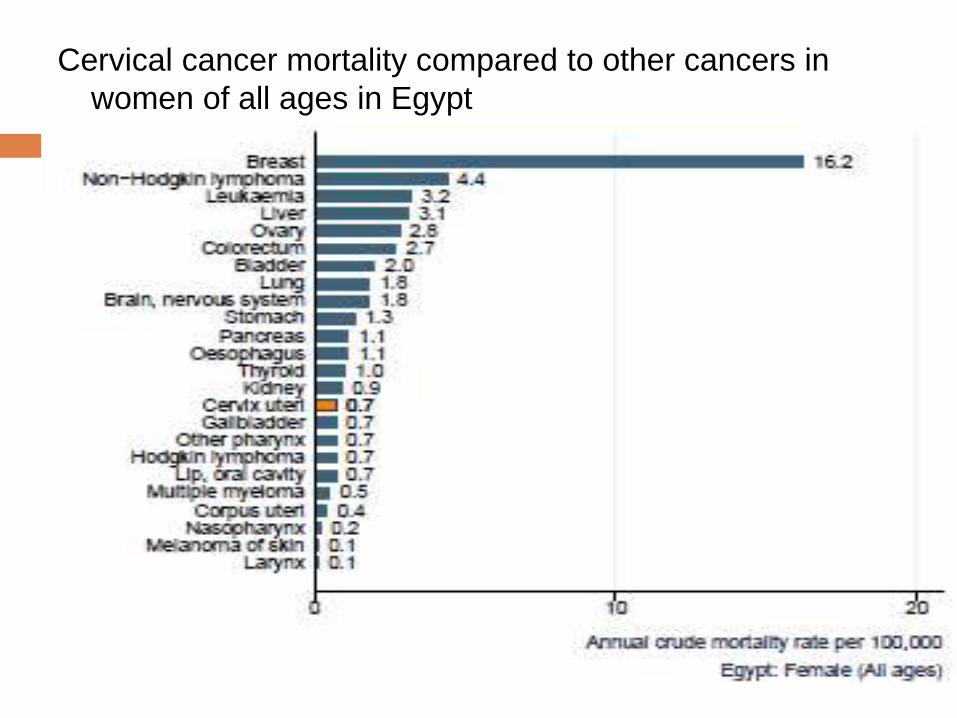
Cervical cancer mortality compared to other cancers in
women of all ages in Egypt
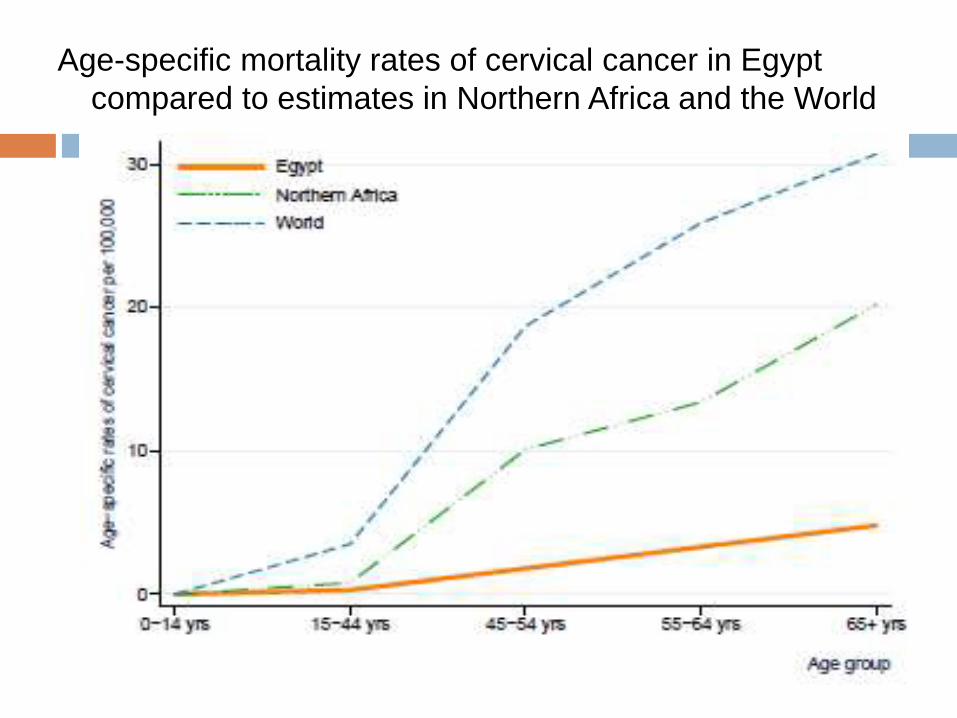
Age-specific mortality rates of cervical cancer in Egypt
compared to estimates in Northern Africa and the World

Human papilloma virus situation in
Egypt
HPV prevalence with normal cytology 10.3%
HPV type distribution among women with normal
cytology, precancerous cervical lesions and
cervical cancer ------
HPV prevalence among men -----
Human papilloma virus vaccine in
Egypt
Licensure status of current HPV vaccines in Egypt
2009
Country recommendations on the inclusion of HPV
vaccines in national immunization program -----
National decision-making process for new vaccine
introduction
Policy issues: Public health priority
Disease burden
Economic burden Vaccine cost-effectiveness Vaccine quality, efficacy and safety Vaccine cost, financing options, sustainability
Operational issues: Vaccine presentation, vial size, cold chain
requirements Reliable vaccine supply Adequate program capacity

Constrains against introduction of HPV
vaccine
Social factors
1- Rumors about new vaccine
2- Beliefs and traditions
Economic factors
1- High cost of the vaccine which may increase the rumors
2- Absence of surveillance for HPV incidence among
females, males and its relations in developing cancer
3- Absence of effective cancer cervix screening program
Overcoming the constraints
1- Launching cancer cervix screening program
2- Launching surveillance program for Human papilloma
virus
3- Health insurance system could cover part of vaccine
cost
4- Cost-effectivness studies as regards induction of Human
papilloma virus vaccine to prevent Cancer cervix and not
human papilloma infection.