Embed Size (px)
Citation preview
HERNIAS DIAFRAGMÁTICAS
TRAUMÁTICASManuel Sebastián Páez
UPTC
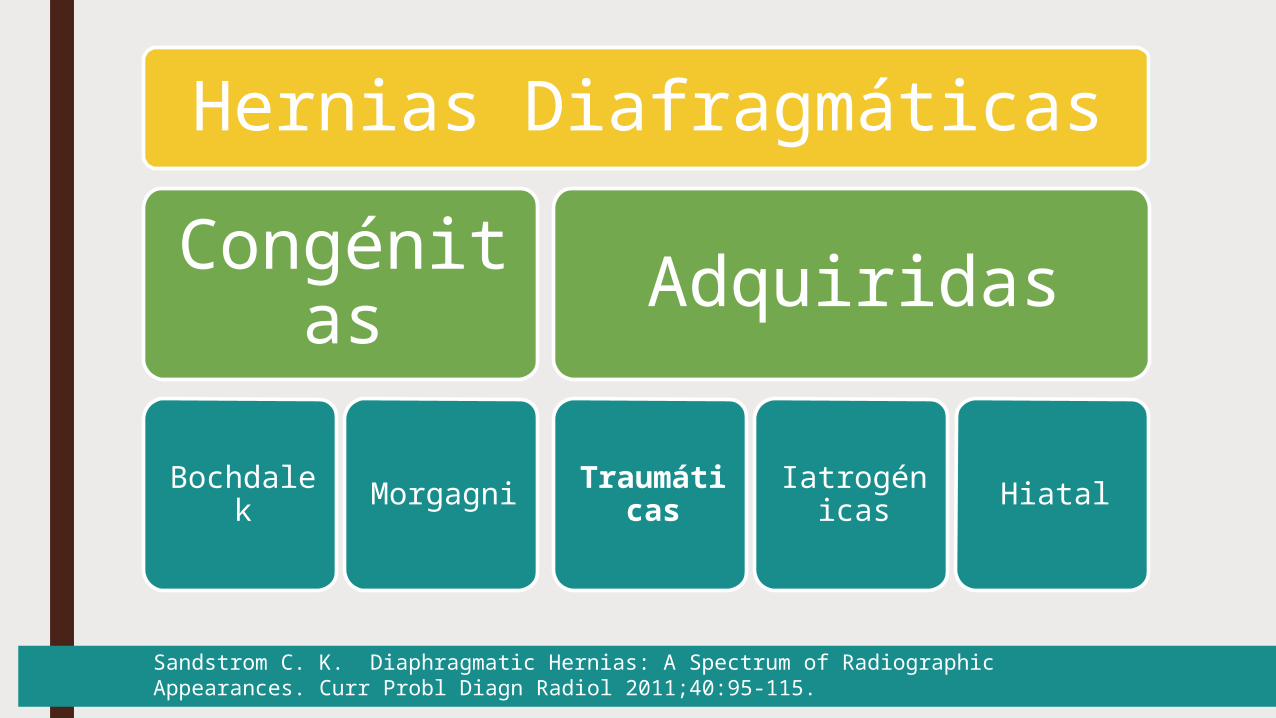
Hernias DiafragmáticasCongénit
asBochdale
k Morgagni
Adquiridas
Traumáticas
Iatrogénicas Hiatal
Sandstrom C. K. Diaphragmatic Hernias: A Spectrum of Radiographic Appearances. Curr Probl Diagn Radiol 2011;40:95-115.
Reseña histórica■ Sennertus, en 1541: Primera Descripción■ Ambroise Paré: Reporte de primer caso 1579■ Riolfi, 1886: Primero en repararla ■ Naumann 1888 Dx Clínico, imposible reducir estomago
herniado muerte■ Walker 1889, reparo por laparotomía y sutura de
Diafragma por tronco
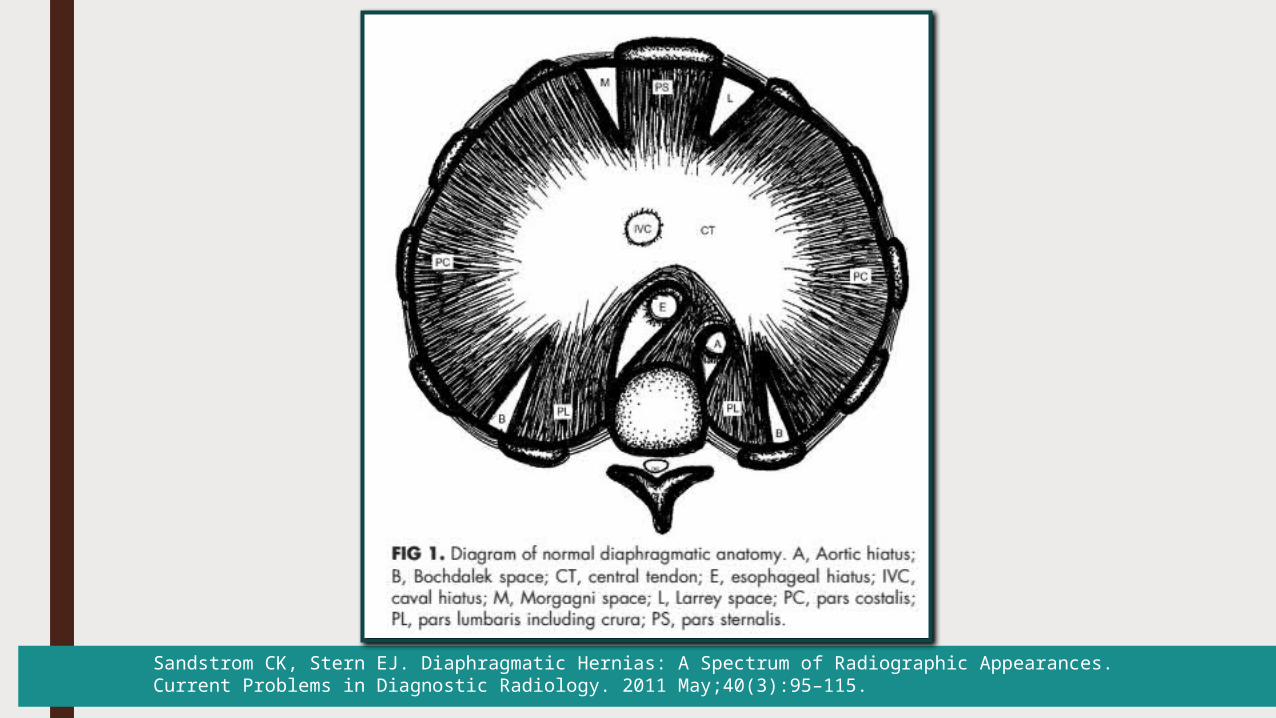
Sandstrom CK, Stern EJ. Diaphragmatic Hernias: A Spectrum of Radiographic Appearances. Current Problems in Diagnostic Radiology. 2011 May;40(3):95–115.
DEFINICIÓN
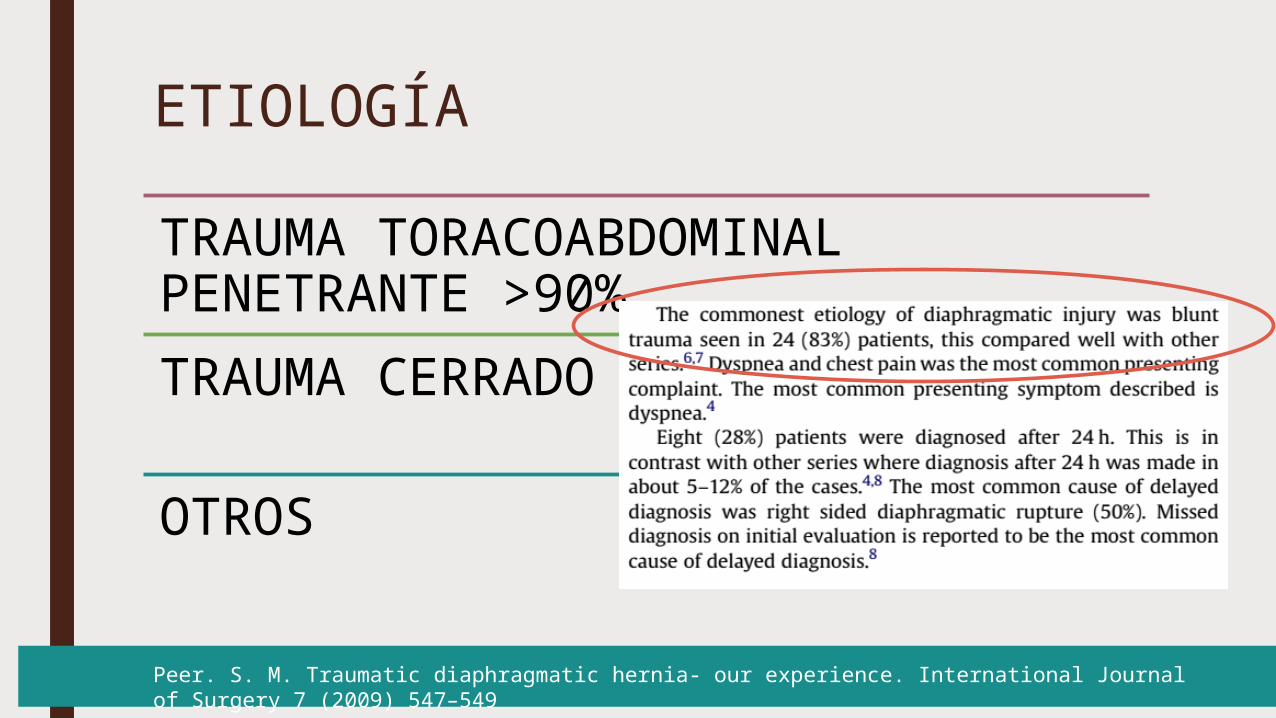
ETIOLOGÍA
TRAUMA TORACOABDOMINAL PENETRANTE >90%TRAUMA CERRADO
OTROS
Peer. S. M. Traumatic diaphragmatic hernia- our experience. International Journal of Surgery 7 (2009) 547–549
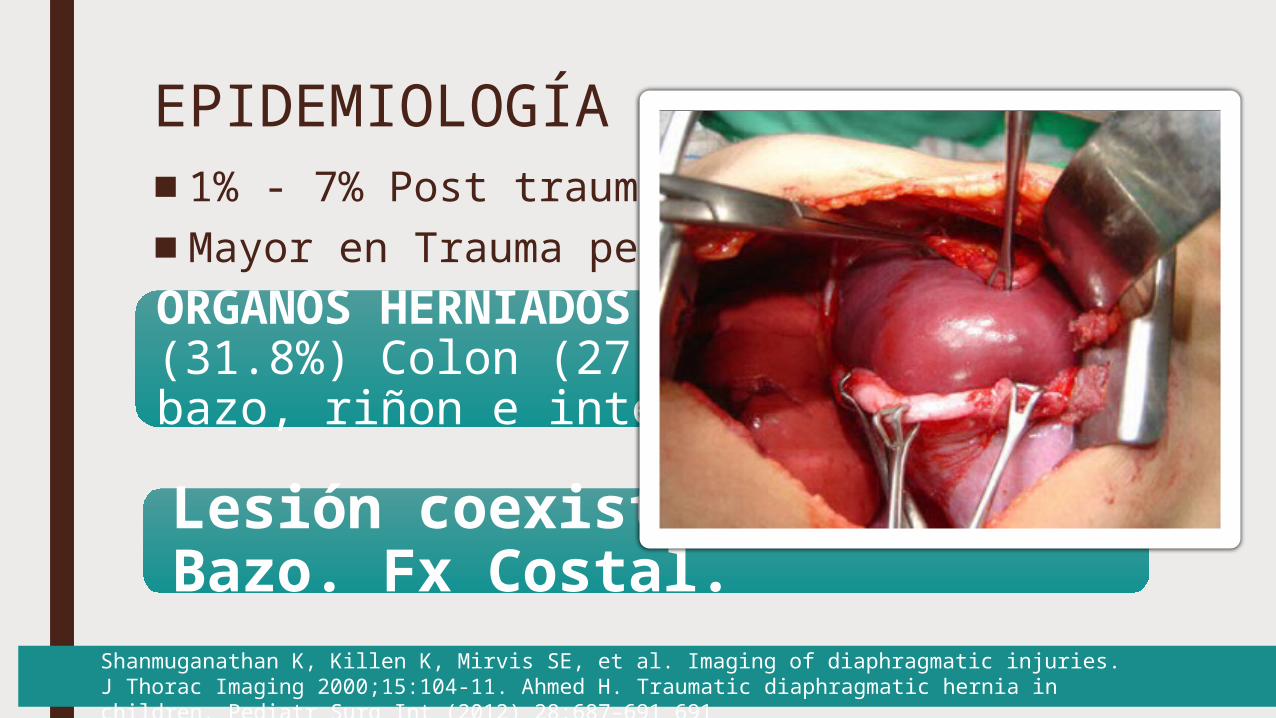
EPIDEMIOLOGÍA■1% - 7% Post trauma Abdominal cerrado■Mayor en Trauma penetrante
Shanmuganathan K, Killen K, Mirvis SE, et al. Imaging of diaphragmatic injuries. J Thorac Imaging 2000;15:104-11. Ahmed H. Traumatic diaphragmatic hernia in children. Pediatr Surg Int (2012) 28:687–691 691
Lesión coexistente: Lx Bazo. Fx Costal.
ORGANOS HERNIADOS: Estomágo (31.8%) Colon (27.2%), hígado, bazo, riñon e intestino delgado
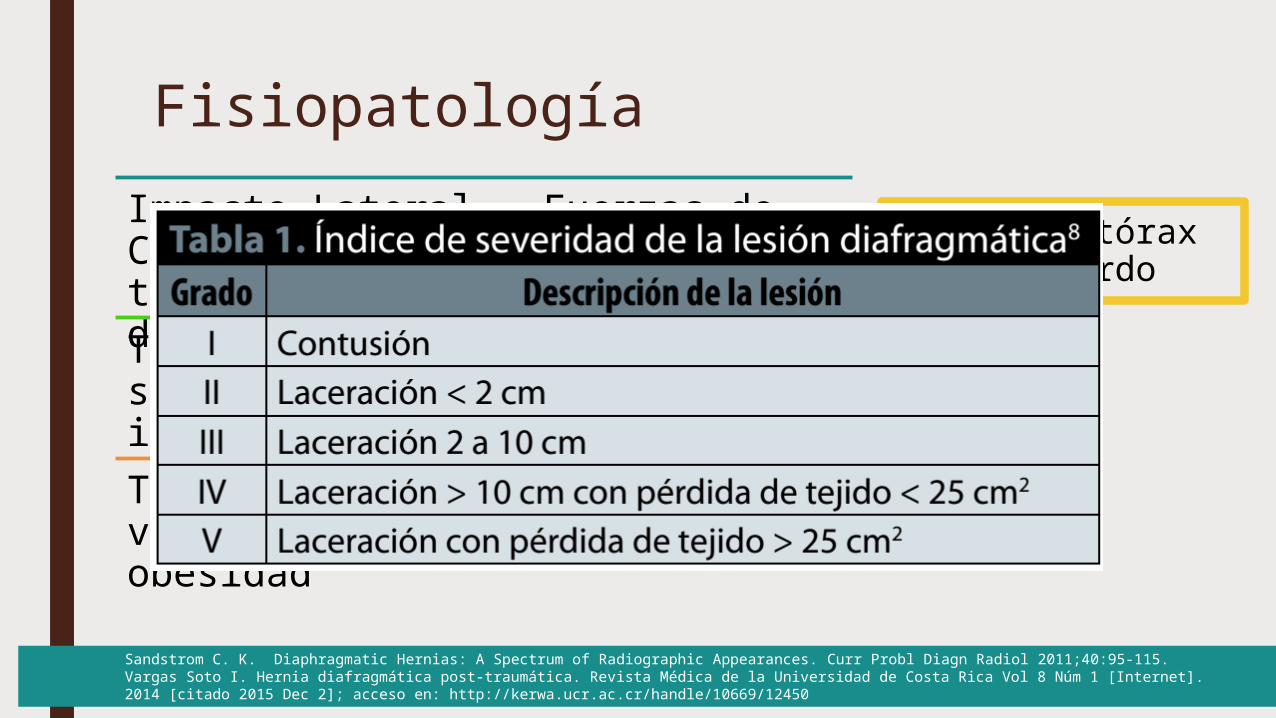
FisiopatologíaImpacto Lateral = Fuerzas de Cizallamiento en pared torácica y uniones diafragmáticasTx Frontal Directo = Aumento súbito de Presión intraabdominal
Traumas menores repetidos: Tos violenta, multiparidad, y obesidad
90% hemitórax izquierdo
Sandstrom C. K. Diaphragmatic Hernias: A Spectrum of Radiographic Appearances. Curr Probl Diagn Radiol 2011;40:95-115.Vargas Soto I. Hernia diafragmática post-traumática. Revista Médica de la Universidad de Costa Rica Vol 8 Núm 1 [Internet]. 2014 [citado 2015 Dec 2]; acceso en: http://kerwa.ucr.ac.cr/handle/10669/12450
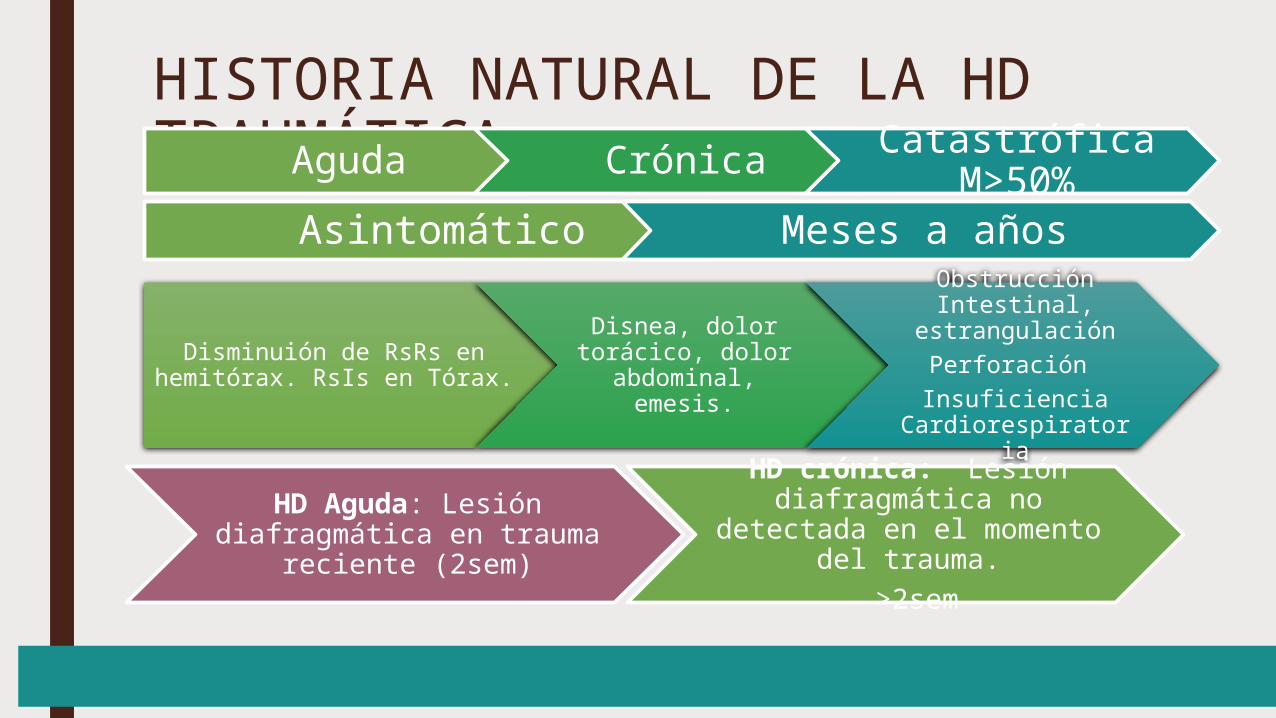
HISTORIA NATURAL DE LA HD TRAUMÁTICAAguda Crónica Catastrófica
M>50%Asintomático Meses a años
Disminuión de RsRs en hemitórax. RsIs en Tórax.
Disnea, dolor torácico, dolor
abdominal, emesis.
Obstrucción Intestinal,
estrangulaciónPerforación Insuficiencia
Cardiorespiratoria
HD Aguda: Lesión diafragmática en trauma
reciente (2sem)
HD crónica: Lesión diafragmática no detectada en el momento del trauma.
>2sem
DIAGNÓSTICO:SE REQUIERE UN ALTO INDICE DE SOSPECHA!!Pacientes con Trauma cerrado de abdomen, trauma toracoabdominal penetrantePacientes con antecedente de herida por arma cortopunzante que reconsultan con síntomas respiratorios, cardiovasculares o gastrointestinales. ■ Rx Tórax■ TAC■ Laparoscopia / Toracoscopia Diagnóstica (y terapeutica)
Liao. C. H. Factors affecting outcomes in penetrating diaphragmatic trauma. International Journal of Surgery 11 (2013) 492e495
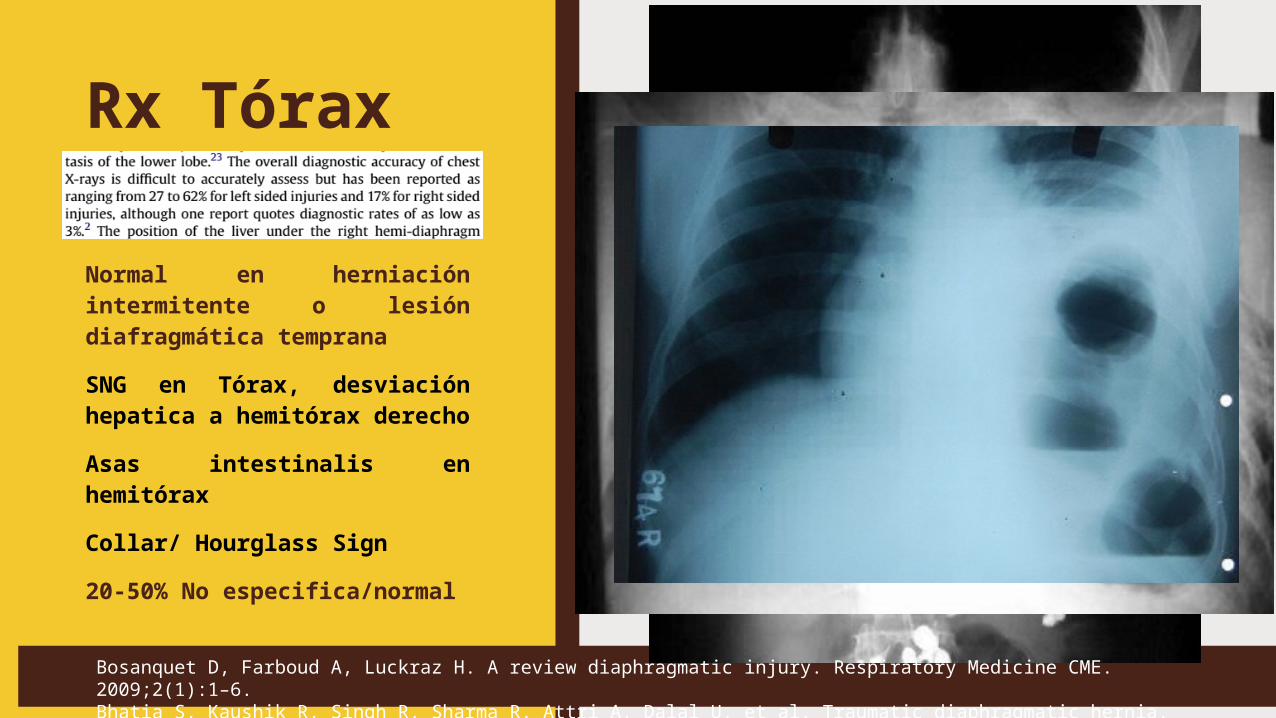
Rx Tórax
Normal en herniación intermitente o lesión diafragmática temprana
SNG en Tórax, desviación hepatica a hemitórax derecho
Asas intestinalis en hemitórax
Collar/ Hourglass Sign
20-50% No especifica/normal
Bosanquet D, Farboud A, Luckraz H. A review diaphragmatic injury. Respiratory Medicine CME. 2009;2(1):1–6.Bhatia S, Kaushik R, Singh R, Sharma R, Attri A, Dalal U, et al. Traumatic diaphragmatic hernia. Indian Journal of Surgery.2008;70(2):56–61.
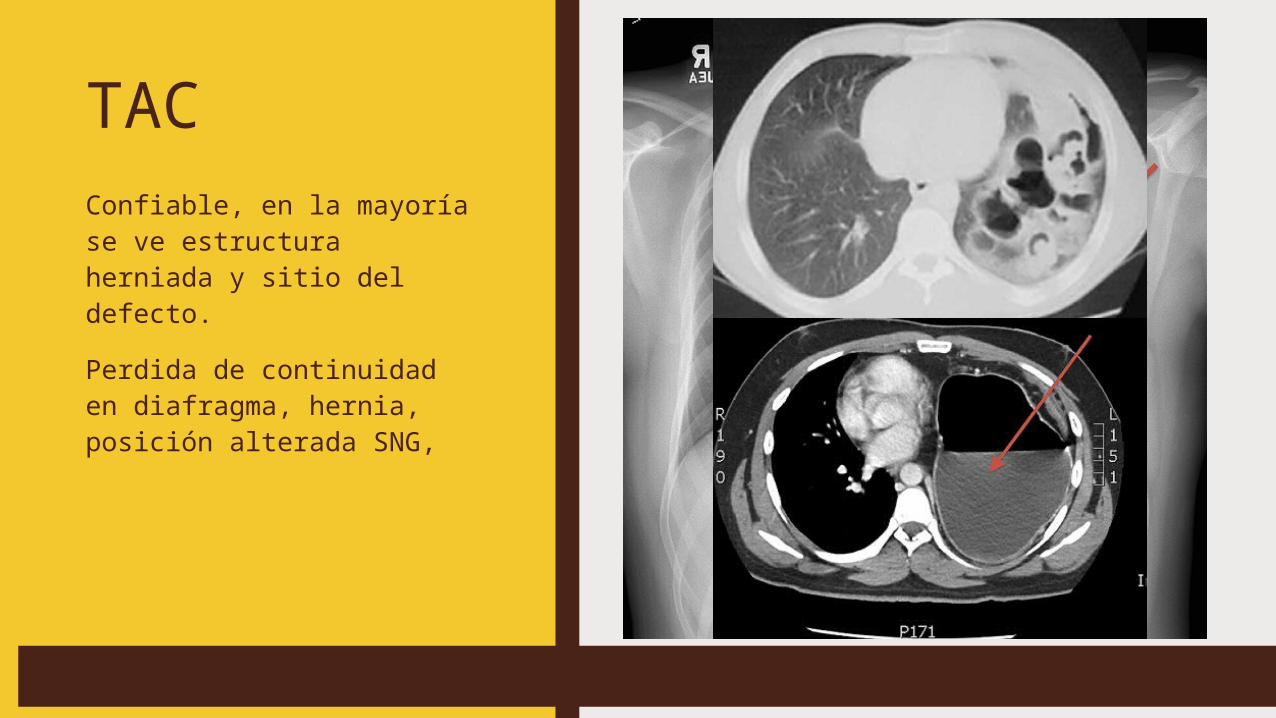
TACConfiable, en la mayoría se ve estructura herniada y sitio del defecto.Perdida de continuidad en diafragma, hernia, posición alterada SNG,
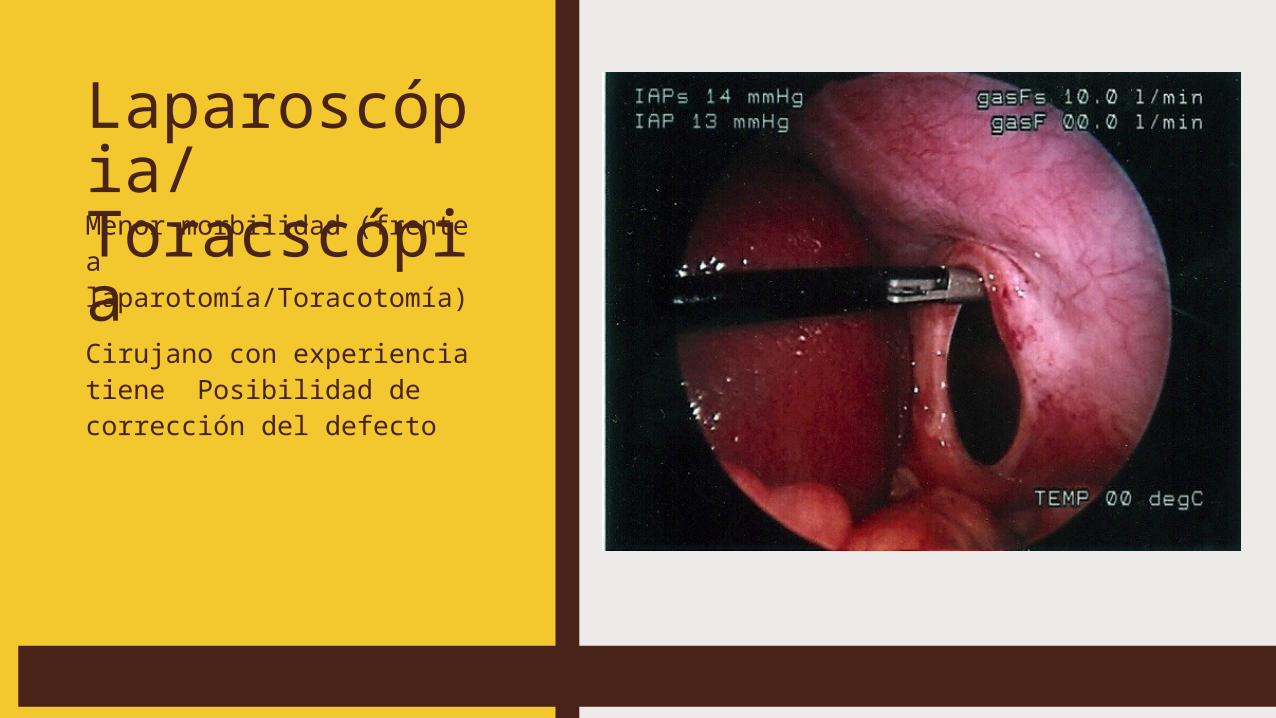
Laparoscópia/ToracscópiaMenor morbilidad (frente a laparotomía/Toracotomía)Cirujano con experiencia tiene Posibilidad de corrección del defecto
TRATAMIENTO = QUIRÚRGICO Reconstrucción de HD traumática aguda por laparoscopia con colocación de malla de polipropileno. DIAFRAGMA SOPORTA LAS SUTURASTransabdominal o transtorácico (dependiente de otras lesiones) Desgarros diafragmáticos asintomáticos■ Agudas: Abordaje Abdominal preferido, permite corregir lesiones
coexistentes. ■ Crónicas. Más adherencias, procedimiento más complejo y de más
riesgo. (Aumenta mortalidad hasta un 66%!)■ Asintomáticos: Programar pronto, riesgo de encarcelación y
estrangulación
Fiscon V et al.: Laparoscopic repair of intrathoracic liver herniation after traumatic rupture of the diaphragm. Surg Endosc 2011;25:3423–3425. Eren S. Diaphragmatic hernia: diagnostic approaches with review of the literatura. European Journal of Radiology 54 (2005) 448–459
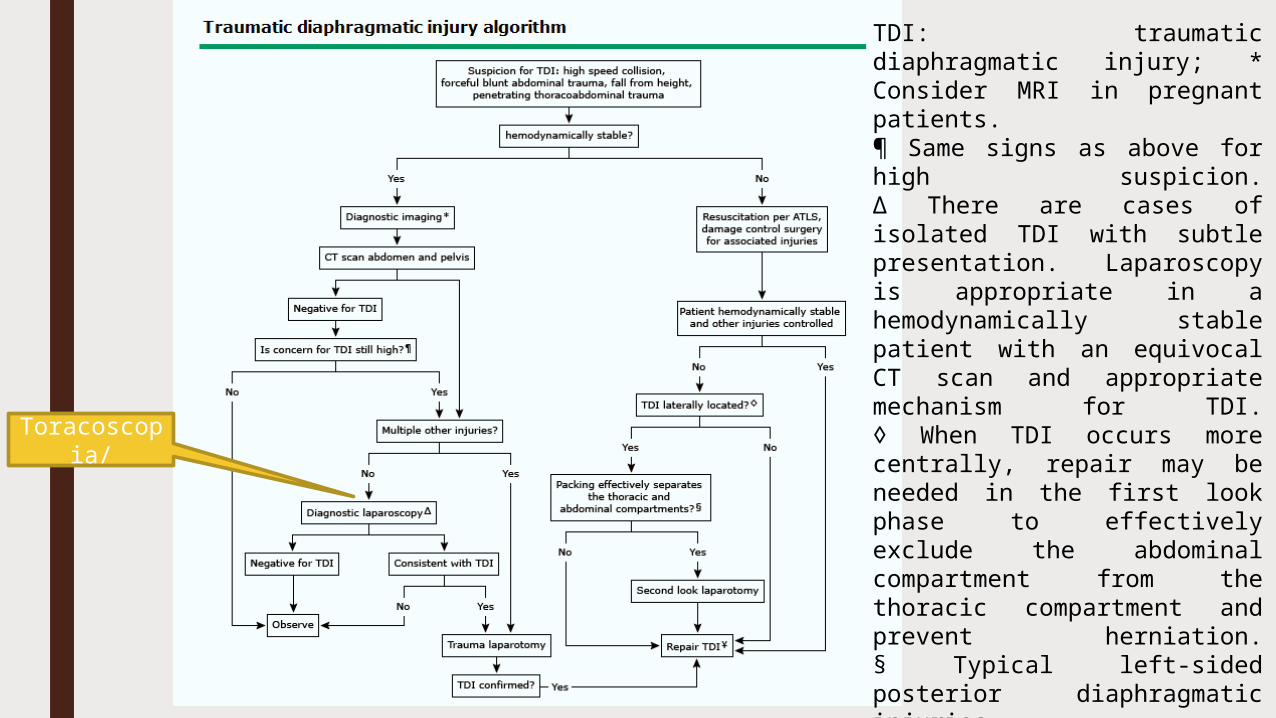
Toracoscopia/
TDI: traumatic diaphragmatic injury; * Consider MRI in pregnant patients.¶ Same signs as above for high suspicion.Δ There are cases of isolated TDI with subtle presentation. Laparoscopy is appropriate in a hemodynamically stable patient with an equivocal CT scan and appropriate mechanism for TDI.◊ When TDI occurs more centrally, repair may be needed in the first look phase to effectively exclude the abdominal compartment from the thoracic compartment and prevent herniation.§ Typical left-sided posterior diaphragmatic injuries.¥ The need to place mesh in the setting of associated organ injury should prompt careful evaluation to rule out bowel injury and ensure control of all other injuries. A second look should be considered.}
PARA RECORDAR:El alto índice de sospecha es clave para el diagnóstico de las hernias diafragmáticas traumáticas
DESCARTAR LESIÓN DIAFRAGMÁTICA EN TODO PACIENTE CON TRAUMA TORACOABDOMINAL PENETRANTE Y/O TRAUMA ABDOMINAL CERRADOSu diagnóstico temprano tiene importancia porque las Hernias diafragmáticas crónicas tienen mortalidad hasta de 66%, muy elevada a comparación de las agudas.Pacientes con antecedente de herida por arma cortopunzante que reconsultan con síntomas respiratorios, cardiovasculares o gastrointestinales. Manejo definitivo es Quirúrgico. Reparación del defecto con colocación de malla de polipropileno, abierta o por laparoscopia
REFERENCIAS1. Sandstrom C. K. Diaphragmatic Hernias: A Spectrum of Radiographic
Appearances. Curr Probl Diagn Radiol 2011;40:95-115.2. Peer. S. M. Traumatic diaphragmatic hernia- our experience.
International Journal of Surgery 7 (2009) 547–5493. Fiscon V et al.: Laparoscopic repair of intrathoracic liver herniation
after traumatic rupture of the diaphragm. Surg Endosc 2011;25:3423–3425.
4. Eren S. Diaphragmatic hernia: diagnostic approaches with review of the literatura. European Journal of Radiology 54 (2005) 448–459
5. Liao. C. H. Factors affecting outcomes in penetrating diaphragmatic trauma. International Journal of Surgery 11 (2013) 492e495





























