Embed Size (px)
Citation preview

Hemodialysis in AKI
Dr. Sherif M. Shaaban
Specialist, internal medicine
and nephrology
Port Fouad General Hospital

Hemodialysis
A form of renal replacement therapy (RRT).
An extracorporeal therapy that is prescribed to reduce the
signs and symptoms of uremia and to replace partially a
number of key functions of the kidneys when kidney
function is no longer sufficient to maintain the patient well-
being or life.
Other forms of RRT include peritoneal dialysis (PD) and renal
transplantation (RTx).

Functions Of The Kidneys
Maintenance of body composition: regulation of body fluid
volume, osmolality, acidity, electrolyte content (sodium,
potassium, magnesium, chloride, phosphate, calcium), and
concentration.
Excretion of metabolic end-products and foreign
substances: most notably urea, some toxins and drugs.
Production and secretion of enzymes and hormones: renin,
erythropoietin, 1,25 (OH)2 D3.
Metabolic functions: elimination of insulin, gluconeogenesis.





Dialysis
Dialysis is a process whereby the solute composition of a
solute A, is altered by exposing solute A to a second solute,
B, through a semi-permeable membrane.

Dialysis
Water molecules and low-molecular-weight solutes in the
two solutions can pass through the membrane pores and
intermingle, but larger solutes (such as proteins) cannot
pass through the semi-permeable barrier, and the
quantities of high-molecular-weight molecules on either
side of the membrane will remain unchanged.

Mechanisms of solute transport
Convection
(ultrafiltration; UF)
Diffusion

Diffusion
Due to random molecular motion.
The larger the molecular weight of a solute, the
slower will be its rate of transport through a semi-
permeable membrane even if they fit into the
ports of the membrane, and vice versa.

Convection (UF)
Occurs when water driven by hydrostatic or osmotic force
is pushed through the membrane.
Solutes that can pass easily through the membrane pores
are swept along with the water (i.e., solvent drag).
The water being pushed through the membrane is
accompanied by such solutes at close to their original
concentrations.

Hemodialysis Apparatus
Blood circuit.
Dialysis solution circuit.
Both meet at the dialyzer.



Blood Circuit
Begins at the vascular access.
Blood is pumped from the access through the ‘arterial
blood line’ into the dialyzer.
Blood is returned from the dialyzer to the patient via a
‘venous blood line’.
Various chambers, side ports, and monitors are connected
to the inflow and outflow blood lines. They are used to
infuse heparin or saline, measure pressures and detect the
presence of air.

Blood Circuit
Blood is moved through the dialyzer by a spring-loaded
roller pump which moves blood by totally occluding a
segment of the tubing then rolling the occluded
segment forwards (like milking a straw).
The blood flow through the dialyzer is a function of the
roller pump rotation rate and the diameter and the
length of the blood line roller pump segment.

Dialysis Solution Circuit
Includes the dialysis solution
(dialysate) supply system,
which makes dialysate by
online mixing of treated
water with concentrated
dialysis solutions.
The final dialysate is pumped
through the dialysate
compartment of the
dialyzer.



Dialysis Solution Circuit
The dialysis solution circuit includes various
monitors that ensure that the dialysate has the
right temperature ad a safe concentration of
dissolved components.
A blood leak detector ensures detection of blood
products in the outflow dialysate.

Dialyzer
Is where the blood
and dialysis fluid
interact and where
the movement of the
molecules between
dialysis solution and
blood across a semi-
permeable
membrane occurs.


Dialyzer Efficiency and Flux
The ability of the dialyzer to remove small-
molecular-weight solutes is a function of its
surface area multiplied by the permeability of the
membrane to urea.

Dialyzer Efficiency
A high efficiency dialyzer is a dialyzer with a large
surface area that has a high ability to remove
urea.
High-efficiency dialyzers have large or small pores
and thus can either have a high or low clearance
of large-molecular-weight molecules such as B2-
microglobulin and Vitamin B12.

Dialyzer Flux
High-flux dialyzers are those with large pores that
allow larger molecules, e.g., B2 microglobulin, to
pass through.
High-flux membranes also have high water
permeability.

Vascular Access In the acute setting, venous catheters are commonly used in
the following situations:
1. AKI
2. HD or hemoperfusion for overdose or toxication.
3. Late stage CKD patients requiring urgent dialysis.
4. ESRD patients who don’t have vascular access or who have
lost their permanent access (e.g., infection, thrombosis).
5. RTx patients who need temporary HD during episodes of
rejection.
6. PD patients in episodes of peritonitis.
7. HF

Types of catheter types
1. Uncuffed
2. Cuffed




Selected factors favoring different temporary
(non-tunneled) hemodialysis catheterinsertion sites
E G Clark,J H Barsuk. Temporary hemodialysis catheters: recent advances. Kidney International (2014) 86, 888–895; doi:10.1038/ki.2014.162

Anticoagulation
Exposure of blood to tubing, dialyzer, drip chambers and air
predisposes to clotting.
Thrombosis may cause occlusion or malfunction of the
extracorporeal circuit, causing loss of dialyzer and tubing as
well as 100 – 180 ml of blood.
Heparin is the most common anticoagulant used. LMWH is
also used.
Heparin-free dialysis in patients with high risk of bleeding
e.g., AKI patients.

AKI: Classification


AKI: Classification Over the last few decades, more than 35 different
definitions have been used to define acute kidney injury(AKI). Many of those definitions were complex.
The more commonly used were based on urine output (UO)
and/or serum creatinine (SCr) criteria.
An increase in basal SCr of at least 0.5 mg/dL, a decrease
in Cr clearance of at least 50% or the need for renal
replacement therapy (RRT) were the most frequent
definitions used for AKI in clinical practice.
Where UO has been used to define AKI, it is generally
considered that a value less than 400–500 mL/day could bean indicator.
J A Lopez, S Jorge. The RIFLE and AKIN classifications for acute kidney injury: a critical and comprehensive review. Clin Kidney J (2013) 6 (1): 8:14.

AKI: Classification
RIFLE (Risk, Injury, Failure, Loss of kidney function, and
End-stage kidney disease) classification for AKI
definition emerged, which was published in May
2004 in Critical Care.

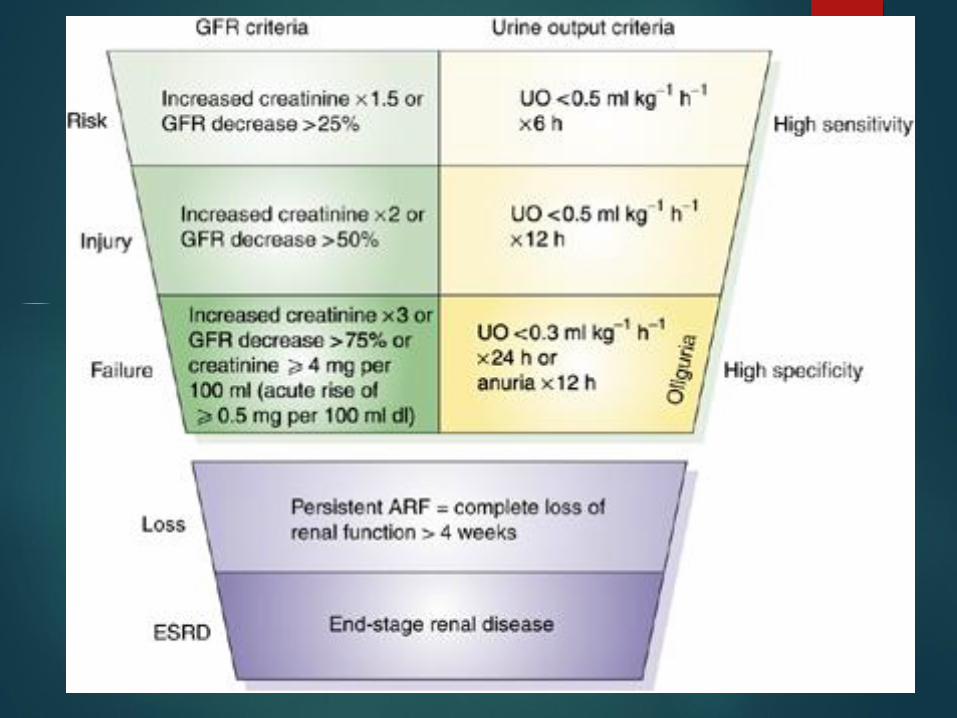

eGFR



RIFLE classification: Strengths
Largely validated in terms of determining the
incidence of AKI and its prognostic stratification in
several settings of hospitalized patients.
Facilitated the identification of a large proportion of
AKI patients.
An independent and stepwise increase in mortality as
AKI severity increased.

RIFLE classification: Strengths
Enables monitoring of the progression of AKI
severity during hospitalization. RIFLE classes are
strongly associated with increased lengths of stay,
RRT requirement, renal function recovery and
discharge from hospital to a care facility.

RIFLE classification: Limitations
Baseline SCr is necessary to define and classify AKI; this
baseline value is frequently unknown in clinical practice.
In this situation, the ADQI work group propose estimating
the baseline SCr using the MDRD equation, assuming a
baseline GFR of 75 mL/min/1.73m2.
In CKD patients, baseline SCr determined assuming a GFR
of 75 mL/min/1.73m2 has a low correlation with the real
value of SCr and results in an overestimation of AKI
incidence.

RIFLE classification: Limitations
The MDRD formula has been validated in CKD
patients with stable renal function, not in AKI
patients.
RIFLE classification: LimitationsSCrDetermination of renal function using SCr has
several other limitations:
S.Cr is influenced by multiple factors, namely
age, gender, diet, and muscle mass;
10 to 40% of Cr elimination is performed bytubular secretion and this mechanism is amplified
as the GFR diminishes, thus, overestimating renal
function in AKI patients;
many medications inhibit tubular secretion of Cr
(i.e. trimethoprim, cimetidine), causing a
temporary increase in SCr;


RIFLE classification: LimitationsSCr
various factors can interfere with SCr
determination (i.e. acetoacetate accumulated in
diabetic ketoacidosis can interfere with the
alkaline picrate method), causing a false
elevation in SCr.
Cr is a marker of renal function, and not of renal
lesion.

RIFLE classification: Limitations UO
Decrease in the UO is sensitive and frequent in AKI;
however, it also has some important limitations indefining and staging AKI:
Sensitivity and specificity of UO can be
significantly changed by the use of diuretics, andthis issue is not specifically considered in the RIFLE
classification;
the UO can only be determined in patients with abladder catheter in place, which, despite being
common in ICU patients, is not frequent in otherhospitalized patients;

RIFLE classification: LimitationsUO
It is possible that the predictive ability of UO could
be inferior to that of SCr, which can explain the
difference in terms of mortality between the same
classes defined by each one of those criteria,
observed in studies that utilized both criteria to
define and classify AKI.

RIFLE classification: Limitations
The aetiology of AKI and the requirement for RRT
are not considered in the RIFLE classification.

AKIN Classification
Published in March 2007 in Critical Care.
It is a later version of the RIFLE classification with some
modifications:
the diagnosis of AKI is only considered after achieving an
adequate status of hydration and after excluding urinary
obstruction;
only relies on SCr and not on GFR changes;
baseline SCr is not necessary, and
it requires at least two values of SCr obtained within a periodof 48 h.

AKIN Classification
These modifications were based on the cumulative
evidence that even small increases in SCr are associated
with a poor outcome
The advantages of the RIFLE modifications have not
been proven.
In fact, the AKIN classification compared with the RIFLE
classification did not exhibit a better prognostic acuity in
terms of in-hospital mortality, although it enabled the
identification of more AKI patients.




RRT in AKI
Early detection and accurate prediction of
patients that ultimately will require RRT may allow
earlier initiation in those who need it and, at the
same time, prevent harm in those who do not.





RRT in AKI
The optimal timing of dialysis for AKI is not defined.
In current practice, the decision to start RRT is based most
often on clinical features of volume overload and
biochemical features of solute imbalance (azotemia,
hyperkalemia, severe acidosis).
However, in the absence of these factors there is
generally a tendency to avoid dialysis as long as
possible, a thought process that reflects the decisions
made for patients with CKD Stage 5.

RRT in AKI
Clinicians tend to delay RRT
when they suspect that patients may recover on their own,
and
because of concern for the well-known risks associated with
the RRT procedure, including hypotension, arrhythmia,
membrane bio-incompatibility, and complications of vascular
access and anticoagulant administration.

RRT in AKI
There is also some concern that RRT may compromise
recovery of renal function, and increase the progression of
CKD. Whether these risks outweigh the potential benefits of
earlier initiation of RRT is still unclear.
Palevsky PM, Baldwin I, Davenport A, et al. Renal replacement therapy and
the kidney: minimizing the impact of renal replacement therapy on recovery
of acute renal failure. Curr Opin Crit Care 2005; 11: 548–554.

RRT in AKI
The treatment of AKI with RRT has the following goals:
i) to maintain fluid and electrolyte, acid-base,and solute homeostasis;
ii) to prevent further insults to the kidney;
iii) to permit renal recovery; and
iv) to allow other supportive measures (e.g.,
antibiotics, nutrition support) to proceed withoutlimitation or complication.

RRT in AKI
5.1.1: Initiate RRT emergently when life-threatening
changes in fluid, electrolyte, and acid-base balance
exist. (Not Graded).
5.1.2: Consider the broader clinical context, the
presence of conditions that can be modified with RRT,
and trends of laboratory tests—rather than single BUN
and creatinine thresholds alone—when making the
decision to start RRT. (Not Graded)

RRT in AKI
While no RCTs exist for dialysis for life-threatening
indications, it is widely accepted that patients with
severe hyperkalemia, severe acidosis, pulmonary
edema, and uremic complications should be dialyzed
emergently.

Timing
Only one RCT has evaluated the effect of timing of
initiation of RRT on outcome. Bouman et al. randomized
106 critically ill patients with AKI to early vs. late initiation
of RRT.
The early initiation group started RRT within 12 hours of
oliguria (<30 ml/h for 6 hours, not responding to diuretics or
hemodynamic optimization), or CrCl<20 ml/min.
The late-initiation group started RRT when classic
indications were met.

Timing
The study did not find differences in ICU or hospital
mortality, or in renal recovery among survivors, but was
clearly too small to allow for definitive conclusions.

Timing The remaining data come from observational studies.
A prospective multicenter observational cohort study
performed by the Program to Improve Care in Acute
Renal Disease (PICARD) analyzed dialysis initiation—as
inferred by BUN concentration—in 243 patients from five
geographically and ethnically diverse clinical sites.
Adjusting for age, hepatic failure, sepsis,
thrombocytopenia, and SCr, and stratified by site and
initial dialysis modality, initiation of RRT at higher BUN (>76
mg/dl) was associated with an increased risk of death (RR
1.85; 95% CI 1.16–2.96).

Timing
The most recent study on this subject is the analysis of
surgical ICU patients with AKI, showing that late
initiation of RRT (defined as RIFLE-I or -F) was an
independent predictor of mortality (HR 1.846; CI 1.07–
3.18).
Shiao CC, Wu VC, Li WY, et al. Late initiation of renal replacementtherapy is associated with worse outcomes in acute kidney injuryafter major abdominal surgery. Crit Care 2009; 13: R171.

Metabolic Acidosis and RRT
Metabolic acidosis is a frequent clinical problem
in patients with severe AKI.
Metabolic acidosis associated with AKI can
usually be corrected with bicarbonate and should
rarely require urgent dialysis if not accompanied
by volume overload or uremia.
Gauthier PM, Szerlip HM. Metabolic acidosis in the intensive care unit. Crit Care Clin 2002; 18: 289–308.

Metabolic Acidosis and RRT
As the pH and bicarbonate values to initiate dialysis for
metabolic acidosis are not supported by evidence, no
standard criteria for initiating dialysis for acidosis exist.
A variety of poisons, drug overdoses, and toxic
compounds (e.g., salicylates, ethylene glycol,
methanol, metformin) can contribute to acid-base
problems and also lead to AKI. In these circumstances,
RRT may also facilitate removal of the offending drug.

Fluid overload
There is increasing evidence that fluid overload in critical
illness and AKI is associated with adverse outcomes.
Data from the PICARD group examining 396 ICU patients
with AKI requiring RRT further supports these findings.
Survivors had lower fluid accumulation at dialysis initiation
compared to non-survivors (8.8% vs. 14.2% of baseline body
weight. The adjusted OR for death associated with fluid
overload at dialysis initiation was 2.07 (95% CI 1.27–3.37).
These data suggest that fluid overload should be further
evaluated as parameter to guide the initiation of RRT.

Other factors that might influence the decision of
when to start RRT are:
• the severity of the underlying disease (affecting the
likelihood of recovery of kidney function),
• the degree of dysfunction in other organs (affecting the
tolerance to e.g., fluid overload),
• the prevalent or expected solute burden (e.g., in tumor lysis
syndrome), and
• the need for fluid input related to nutrition or drug therapy .

Dialysis As A Form Of Renal Support
It may be more appropriate to consider dialytic
intervention in the ICU patient as a form of renal
support rather than renal replacement.
For instance, massive volume overload resulting from
volume resuscitation may be an indication for RRT
even in the absence of significant elevations in BUN
or SCr.

Thank You


























