Embed Size (px)
Citation preview

The National Health Board in New Zealand: Delivering Better, Sooner,
More Convenient Healthcare
Professor Gregor CosterUniversity of Auckland
22 September 2010

Overview
• Purpose of this paper is to discuss the rationale for setting up the National Health Board (NHB, Board)
• legislative framework in brief• board accountabilities; how the role of Ministers has changed• how the Board was set up in practice; how it is intended to
operate; the role, if any, of the public in the Board’s workings• how the Board’s impact will be assessed • overlapping roles, including with the body responsible for new
technology assessment• comparison between NZ National Health Board and UK NHS
Commissioning Board• lessons that can be gained from the New Zealand experience.

Arrangements until 2009
• Health Funding Authority till 2000• health reforms shifted from a single purchaser to 21 District
Health Boards (DHBs) 2000/01• DHBs responsible for planning and funding of all services in
district except some services e.g. disability• provide hospital services• democratically elected boards, with some appointed members• intended to ensure local needs are met• evaluations found that intended devolution did not occur
– central control continued– local autonomy difficult to achieve– prioritisation of services limited by level of control by central
government over services (Coster, 2010)

Arrangements until 2009
‘The reforms involved a shift away from a ‘quasi’-market model to a more collaborative set of arrangements for purchasing and providing health and disability support services with a stronger community voice in relation to decision making about health and disability support services’ (Mays et al., 2007).

National Party manifesto

Expenditures in $US PPP
(purchasing power parity)
Netherlands is estimated
OECD Health Data, 2009
NZ = $2,454
Australia = $3,357
USA = $7,290
Davis et al 2010 The Commonwealth Fund

30
40
50
60
70
80
1998 2000 2002 2004 2006 2008 2010 2012 2014
$ billion
Year ended 30 June
Core Crown Revenue & Expenses
Budget 2010 Expenses Budget 2010 Revenue
FORECAST

Growth in health expenditure 1950-2010

Assuming that relative health spend will remain at about 20% of total Government expenditure, then the maximum tolerable increase in the health budget will be about 40% between now and 2020.
Growth in health expenditure 1950-2010

NZ Population Projections by Age Cohort (Assuming medium population growth)Source: NZIER (2005)
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,0000-
4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80-8
4
85-8
9
90+
2001 2011 2021

Age Distribution of Population
Statistics New Zealand, March 2006

Ministerial Review Group Report 2009
‘… we must find a way to deliver these public services within a more sustainable and, therefore, slower path for health expenditure growth… Bureaucracy, waste, and inefficiencies must be reduced and resources moved to the front-line as spending growth slows. We must focus on quality which will deliver better patient outcomes and on ensuring better access to health services through smarter planning and resource utilisation, at regional and national levels.’ (Ministerial Review Group, 2009) p.3.

MRG recommendations (1)
• Stronger clinical leadership in decision-making • accelerating improvements in quality and safety • higher system performance and secure future
sustainability • improved national and regional service planning and
decision-making • minimising administrative costs and reducing
bureaucracy and waste.

MRG recommendations (2)
• The MRG considered that the complexity of the current roles of the Ministry made it difficult to focus on its core responsibility of policy development. They believed that a much clearer focus on the Ministry’s core policy and regulatory functions was required, along with reduced bureaucracy and a smaller Ministry of Health.
• Foremost among the recommendations was a proposal that a new National Health Board be created by revamping the Crown Health Funding Agency to manage national capacity and service planning, to plan and fund national services, and to fund and monitor DHBs i.e. to establish a separate Crown Entity.

Cabinet decisions
• Rejected the notion of a separate Crown Entity –established a NHB within MoH with a GM– Chair of NHB reports directly to Minister– Take over funding and planning of certain national services
(paediatric oncology, clinical genetics, major burns)– Infrastructure planning for IT, Capital, Health Workforce
• Establish Shared Service Organisation• Strengthen regional cooperation in service planning
and delivery• Devolve funding of $2.5b to DHBs, where appropriate

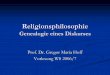
Minister of Health
National Health Board
Shared Service Organisation
Health Workforce New Zealand
National Health Committee
Health Quality and Safety Commission
Pharmac
National Health Information
Technology Board
District Health Boards
Director General
of Health
Regional consortia
Ministerial CommitteesCrown Entities
Accountability arrangements in the New Zealand health system in 2010

Reconfiguration of the Ministry
• National Health Board Business Unit (750 staff) – National Director – reports regularly to NHB
• Health Workforce New Zealand Business Unit (50-60 staff) –Director – reports regularly to HWNZ
• Ministry residuum => policy and regulatory functions, plus service delivery responsibilities (e.g. disability) (600 staff)
• split ministry• public accountability for MACs through State Sector
accountability framework => MoH SOI, information supporting the Estimates, and Annual Output Plan.

Role of the Minister
• Retains significant powers • minimal devolution • NHB may be directed => remains accountable to Minister• may direct DHBs, regional consortia of DHBs, and numerous
Ministerial Committees and Crown entities in order to achieve the government’s objectives for health
• requires DHBs to prepare plans that address local, regional and national needs for health services as directed
• has power to intervene and resolve disputes between DHBs• contrasts with UK where the government proposes to establish
an independent and accountable NHS Commissioning Board limiting the powers of Ministers over day-to-day NHS decisions

Empowering legislationThe Bill, which is expected to be passed: • amends the objectives and functions of DHBs to ensure that DHBs work
together for the most effective and efficient delivery of health services to meet national, regional, and local needs.
• amends planning requirements for DHBs in order to provide for a planning and accountability framework that takes account of national, regional, and local requirements
• amends regulation-making powers in the current Act relating to arbitration and mediation to enable these powers to have wider application, particularly where there are disputes between DHBs about how national, regional, and local requirements are best provided for
• provides that the Minister may give a direction to all DHBs to comply with stated requirements for the purpose of supporting government policy on improving the effectiveness and efficiency of the health and disability system.

NHB
“Anybody holding the NHB National Director’s role would be wise to come up with a process of developing recommendations to the Minister that will incorporate and involve not only the Ministry’s view but that of the NHB as well.”– Chai Chuah, new National Director of the NHBBU

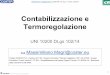
Minister of Health
National Health Board
District Health Boards
Director General
of Health
Regional consortia
Planning arrangements in the New Zealand health system in 2010
National Health Plan
Regional Health Plan
District Health Plan
Annual, five year and ten year health plans Service
Configurations and Models of
Care
ITCapital
Workforce

NHB Annual Plan 2010/11- eight priorities
The programme includes the following priority areas:• developing an approach to long-term service planning that is
more effective and unified • identifying, planning, funding and monitoring the delivery of
national health services• supporting the ongoing development and implementation of
regional service plans by DHBs• DHB funding and planning, and improving DHB performance• ensuring workforce, information technology and capital
requirements support future service plans• encouraging clinical leadership and engagement• reducing waste and bureaucracy and improving the
productivity of the health and disability system• devolving relevant non-departmental expenditure to the
regional and district level.

Comparison of New Zealand and UK Plans for NHBs
NHB NHSCBMinisterial Advisory Committee Statutory commissioning board
Responsible for national funding, monitoring and planning of health services
Lead on the achievement of health outcomes, allocate and account for NHS resources
Deciding which services should be planned, funded and provided at national, regional and local levels
Ensuring the development of GP commissioning consortia
Planning and funding of designated national services
Commissioning responsibility for national and regional specialised services
Management of certain national services Promoting and extending public and patient involvement and choice
Oversight of regional service planning and funding, including arbitration of disputes
Ensure commissioning decisions are fair and promote competition
Strategic planning and funding of future capacity (IT, facilities, workforce)
Determining health data standards for collection and transfer of information
[Improve quality and safety – Health Quality and Safety Commission]
Lead on quality improvement
Promote equality and tackle inequalities in access to healthcare

Do we need a NHS Agency?
“The evidence is mounting that reforms of this sort rarely if ever produce the expected benefits. Devolution can be pursued without setting up a new agency. It is a matter of the centre determining what it will and will not seek to control and direct. A less disruptive approach would be simply to pass legislation restricting the scope of business that the Secretary of State could be legitimately be expected to be responsible for to Parliament.”
Nicholas Mays. ‘Should the NHS be freed from political control?’ J Health Serv Res Policy Vol 9 No 1 January 2004.

Do we need a NHS Agency?
“It is time for the health sector to catch up with modern governance practices and establish an independent agency to manage the NHS. The greatest advantage would be that it would free government ministers and Parliament to provide leadership in health policy rather than just NHS policy or, worse still, policy on how best to look after Rose Addis.”
Nick Black. ‘Should the NHS be freed from political control?’ J Health Serv Res Policy Vol 9 No 1 January 2004.

Key themes of the new arrangements
• ‘Devolution’ to a new agency
• Few new Crown entities
• New accountabilities
• Future change is possible

Effectiveness of the new arrangements in NZ
• Indications are that NHB is already showing stronger engagement with clinicians in decision-making, and more focussed planning of national and regional services than previously
• better regional collaboration between DHBs is being achieved
• amalgamation is possible in order to achieve greater regionalisation
• relative invisibility of the NHB will need to be addressed, along with providing both the public and health sector with a clearer explanation of the interrelationships between various committees and components of the revamped health sector.

Potential for overlapping roles
• Policy-setting – NHB vs ‘Ministry’• health workforce – HWNZ vs ‘Ministry’• priority-setting (medical devices, new technologies,
disinvestment decisions) – National Health Committee vs Pharmac vs NHB
• health quality and safety – HQSC vs NHB vs DHBs

How will the NHB’s impact be assessed?
• ‘Better, sooner, more convenient’ – achieving the aspirational goals
• greater economic efficiency• reduction in growth of health expenditure (capital and
operational)• improving health and performance indicators• achievement against NHB annual plan• greater clinical involvement in decision-making• less bureaucracy • reduction in health committees• co-ordinated regional planning• But not decided yet

Lessons from the New Zealand experience• Avoid dual accountabilities for the NHS Commissioning Board
• ensure clear pathways and responsibility for provision of Ministerial advice in policy and administrative matters from the Department and the NHS Commissioning Board
• legislate clearly the powers and functions of the NHS Commissioning Board, and the ability of the Minister to hold the board to account
• clarify the accountabilities for the Care and Quality Commission, Monitor and other statutory bodies in relationship to the NHS Commissioning Board
• commissioning by GP Consortia may run the risk of inhibiting the development of partnership relationships with other non-government providers if there are no controls on commissioning behaviour
• New Zealand can learn from the model of promoting and extending public and patient involvement and choice.